
1
Fifth stage
Pediatric
Lec-2
.د
أ
ثل
1/1/2016
DIARRHOEA in INFANCY & CHILDHOOD
Objectives of Lec.2
A/ correction of dehydration
To differentiate between the types of dehydration.
How you can correct different types of dehydration & how you manage the emergency?
To know the types of oral & I.V. fluid.
B/ Prevention of GE
How you can decrense the occurance of GE
C/ Complication of GE
To enumerate the complication of GE.
TYPES OF DEHYDRATION
ISOTONIC (ISONATRAEMIC). S . Na
5
4
1
-
5
3
1
=
mmol/L
HYPERTONIC (HYPERNATRAEMIC).
S . Na >
145
(
151
)
mmol/L
HYPOTONIC(HYPONATRAEMIC). S . Na < (135)130 mmol/L.
CORRECTION OF DEHYDRATION
ORAL REHYDRATION THERAPY
Mild to moderate dehydration from diarrhea of any cause can be treated
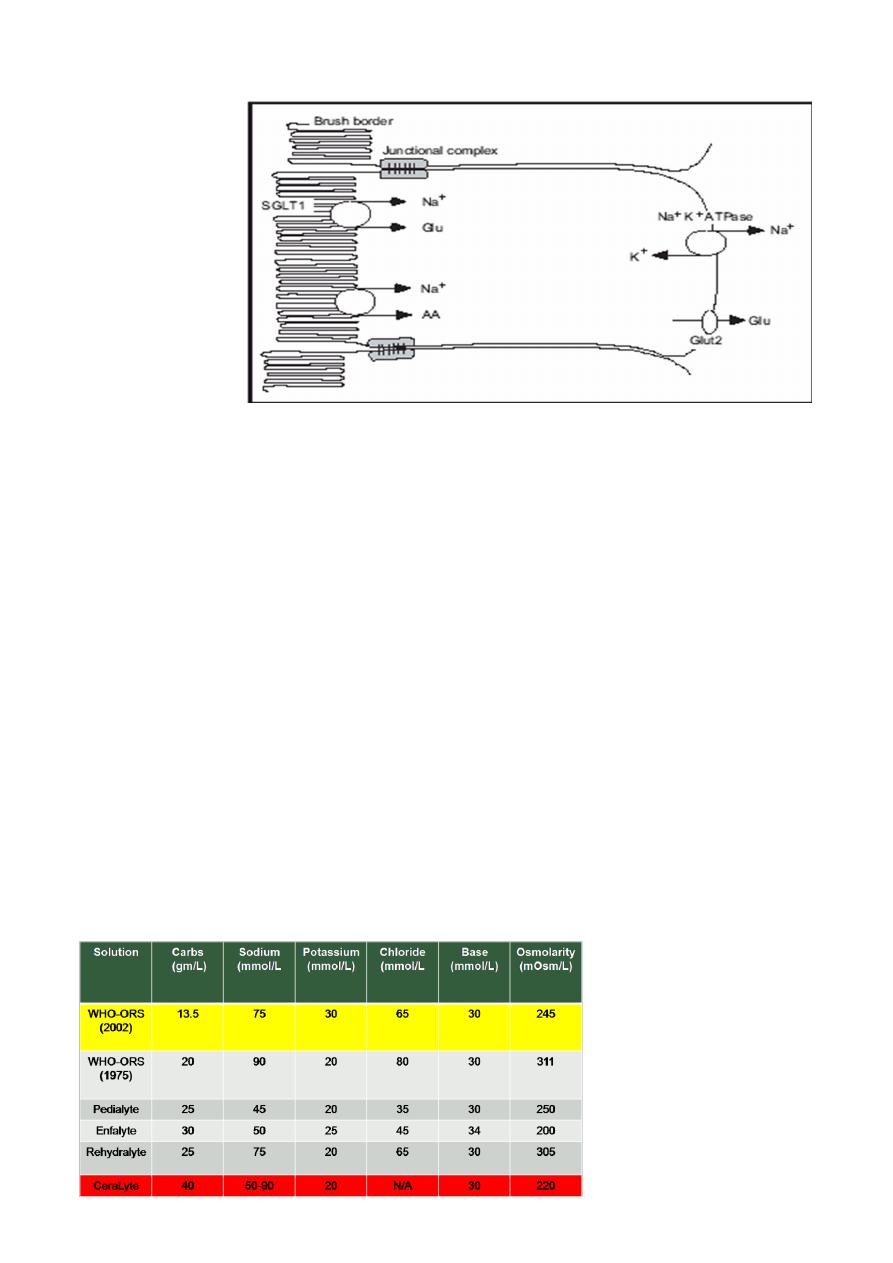
effectively using a simple, oral rehydration solution (ORS) containing glucose and
electrolytes. The ORS relies on the coupled transport of sodium and glucose in the
intestine (Facilitated transport of SODIUM by absorption of GLUCOSE )
ORT is less expensive than IV therapy and has a lower complication rate.
IV therapy still may be required for patients with severe dehydration; patients
with uncontrollable vomiting; patients unable to drink because of extreme
fatigue, stupor, or coma; or patients with gastric or intestinal distention.
2
Physiologic Basis of ORT
ORS
NaCl: 3.5 gm
NaHCO3: 2.5 gm
KCl: 1.5 gm
Glucose: 20 gm
Add 1 Liter of pure water
ORS ( WHO 2005)
[Na] 75mmol/L
[Cl] 65mmol/L
[HCO3] 10mmol/L
[K ] 20mmol/L
Glucose 13.5 g/L
Osm 245 mosm/L
Choices of ORS
3
ORT
REHYDRATION PHASE
For MILD Dehydration :
50 cc /Kg/ 4 Hr.
For MODERATE Dehydration:
100 cc /Kg/ 4 Hr
MAINTENANCE PHASE
MILD Diarrhea : 100 cc /Kg/24Hr
SEVERE Diarrhea : 10-15 cc /Kg/ Hr
in addition to milk feeds until diarrhea stops
.
INTRAVENOUS REHYDRATION
ONGOING LOSS
MAINTENANC
E
INTRAVENOUS
REHYDRATION
DEFICIT
4
DEFICIT
Calculated According to The Clinical Assessment For Severity of Dehydration
Water Deficit
Percent dehydration × weight
Resuscitation Phase
The child with dehydration requires acute intervention to ensure that there is
adequate tissue perfusion. This resuscitation phase requires rapid restoration of
the circulating intravascular volume. This restoration should be done with an
isotonic solution, such as normal saline or Ringer's lactate. Blood is an appropriate
fluid choice for a child with acute blood loss.
The child is given a fluid bolus, usually 20 mL/kg of the isotonic solution, over
about 20 minutes. A child with severe dehydration may require multiple fluid
boluses and may need to receive fluid at a faster rate.
The initial resuscitation and rehydration is complete when the child has an
adequate intravascular volume. Typically the child has some general clinical
improvement, including a lower heart rate, normalization of the blood pressure,
improved perfusion, and a more alert affect.
Potassium is not usually included in the intravenous fluids until the patient voids.
NOTE
The resuscitation phase (treatment of shock state ) is same in iso, hypo, &
hypernatremic dehydration
MAINTENANCE
Maintenance fluids are composed of a solution of water, glucose, sodium
potassium, and chloride. This solution replaces electrolyte losses from the urine
and stool and water losses from the urine, stool, skin, and lungs. The glucose in
maintenance fluids provides approximately 20% of the normal caloric needs of the

5
patient. This percentage is enough to prevent the development of starvation
ketoacidosis and diminishes the protein degradation that would occur if the
patient received no calories. Glucose also provides added osmoles, avoiding the
administration of hypotonic fluids, which may cause hemolysis.
Maintenance fluids do not provide adequate calories, protein, fat, minerals, or
vitamins. Because of inadequate calories, a child on maintenance IV fluids loses
0.5% to 1% of real weight each day. Patients should not remain on maintenance
therapy indefinitely; parenteral nutrition should be used for children who cannot
be fed enterally for more than a few days. Parenteral nutrition is especially
important in a patient with underlying malnutrition.
Goals of Maintenance Fluids
Prevent dehydration
Prevent electrolyte disorders
Prevent ketoacidosis
Prevent protein degradation
Body Weight Method for Calculating Daily Maintenance Fluid Volume
First 10 Kg 100 cc /Kg/24Hr
Second 10 Kg 50 cc /Kg/24Hr
> than 20 Kg 20 cc /Kg/24Hr
NOTE: The maximum total fluid per day is normally 2,400 mL.
Maintenance requirements of electrolytes:
Sodium: 2 - 3 mEq/kg/day
Potassium: 1 - 2 mEq/kg/day.

6
Composition of Maintenance fluids:
Child WT < 10Kg:
D5 + ¼ NS (38.5mEq/L) + 20 mEq/L of [K]
Child WT > 10Kg:
D5 + ½ NS (77mEq/L) + 20 mEq/L of [K]
NOTE: These guidelines assume that there is no disease process present that would require
an adjustment in either the volume or the electrolyte composition of maintenance fluids
ONGOING LOSSES
Calculated CC for CC and mmol for mmol and added to the rehydrating solution.
Replacement solutions should have approximately the same electrolyte
composition as the fluid that is lost. Electrolyte content can be measured directly,
or a solution can be selected based on the typical electrolyte composition of
diarrhea or gastric losses
REPLACEMENT OF LOSSES
< 10Kg BW: 60-120 mL ORS for each diarrheal stool or vomiting episode
>10 kg BW: 120-240 mL ORS for each diarrheal stool or vomiting episode
if unable to drink, administer through nasogastric tube or administer 5% dextrose
in normal saline with 20 mEq/L potassium chloride IV
Fluid Management of Dehydration
Restore intravascular volume
Normal saline: 20 mL/kg over 20 min (repeat until intravascular volume restored)
(maximum = 1 L over 2 hr)
Calculate 24-hr water needs
Calculate deficit water
Calculate maintenance water
Select an appropriate fluid (based on total water and electrolyte needs)
Administer half the calculated fluid during the first 8 hr, first subtracting any boluses
from this amount
Administer the remainder over the next 16 hr
Replace ongoing losses as they occur
7
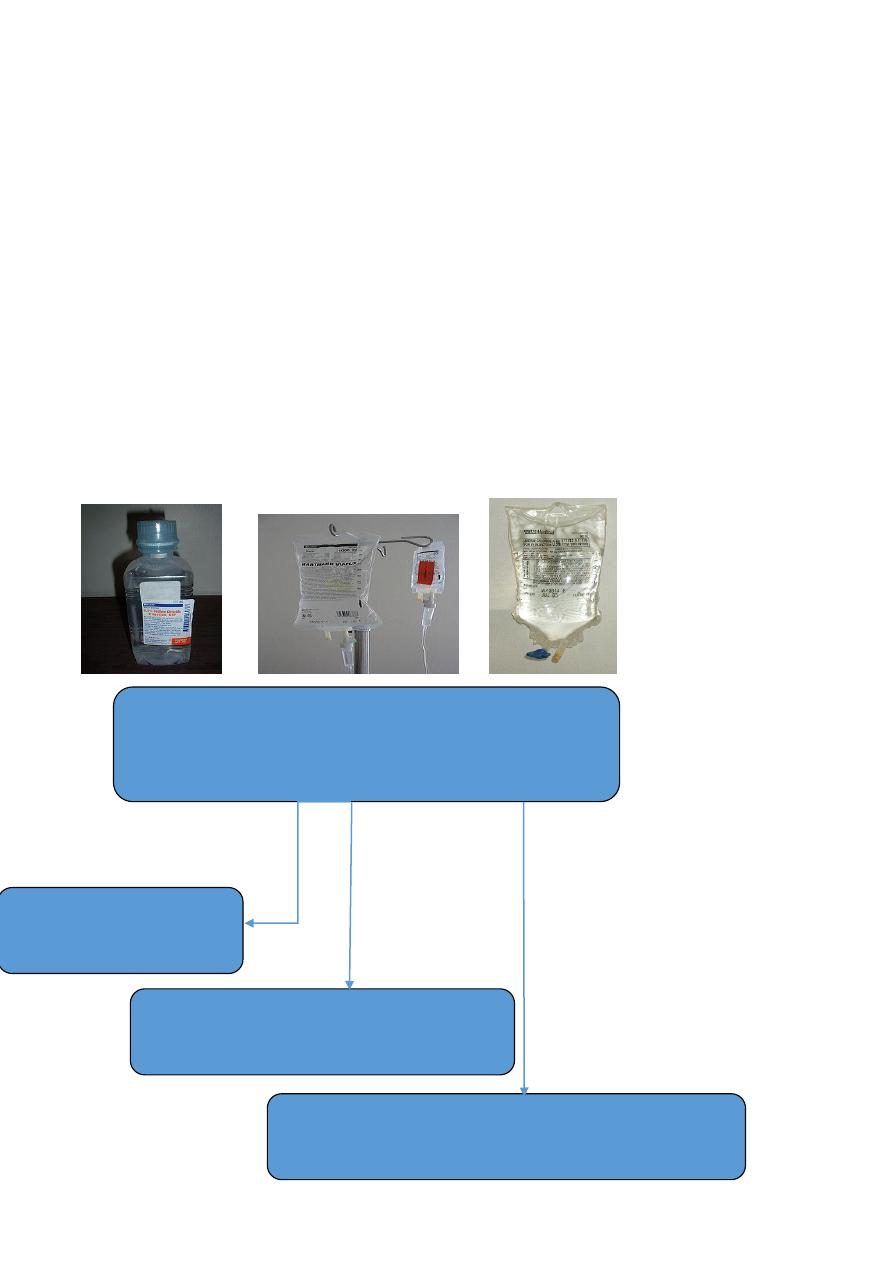
TYPES OF IV FLUID
HYPONATREMIC DEHYDRATION
Hyponatremic dehydration produces more substantial intravascular volume depletion
due to the shift of water from the extracellular space into the intracellular space. In
addition, some patients have symptoms, predominantly neurologic, as a result of
hyponatremia
Treatment
Treatment of hypovolemic hyponatremia requires administration of IV fluids with
sodium to provide maintenance requirements and deficit correction and to
replace ongoing losses
solution
Glucose (g/l)
Na+
K+
Ca+2
Cl-
Lactate
D5W
50
0
0
0
0
0
D10w
100
0
0
0
0
0
NS
0
154
0
0
154
0
½ NS
0
77
0
0
77
0
¼ NS
0
38.5
0
0
38.5
0
D5NS
50
154
0
0
154
0
D5 ½
NS
50
77
0
0
77
0
0.2 NS
0
31
0
0
31
0
3%NaCl
0
513
0
0
513
0
LR
0
130
4
3
109
28

8
Most patients with hyponatremic dehydration do well with the same basic
strategy for correction of Isonatremic dehydration.
The initial goal in treating hyponatremia is correction of intravascular volume
depletion with isotonic fluid (NS or LR).
An overcorrection in the serum sodium concentration (>135mMol/L) is associated
with an increased risk of central pontine myelinolysis (CPM).
The risk of CPM also increases with overly rapid correction of the serum sodium
concentration, so it is best to avoid increasing the sodium by >12 mEq/L each 24
hr.
Emergency treatment of symptomatic hyponatremia, such as seizures, uses IV
hypertonic saline to increase the serum sodium concentration rapidly, which leads
to a decrease in brain edema.
Each 1 ml/Kg of 3% sodium chloride increases the serum sodium by approximately
1 mEq/L.
A child often improves after receiving 4 to 6 mL/kg of 3% sodium chloride.
The aim should be to increase the serum sodium concentration to not more than
130 mEq/L.
HYPERNATREMIC DEHYDRATION
Hypernatremic dehydration is the most dangerous form of dehydration due to
complications of hypernatremia and of therapy.
Hypernatremia can cause serious neurologic damage, including central nervous system
hemorrhages and thrombosis. This appears to be secondary to the movement of water
from the brain cells into the hypertonic extracellular fluid, causing brain cell shrinkage
and tearing blood vessels within the brain

9
Clinical Manifestations
Children with hypernatremic dehydration often appear less ill than children with a
similar degree of isotonic dehydration. Urine output may be preserved longer, and there
may be less tachycardia. Children with hypernatremic dehydration are often lethargic
and irritable when touched. the pinched abdominal skin has a "doughy" feel.
Hypernatremia may cause fever, hypertonicity, and hyperreflexia.
More severe neurologic symptoms may develop if cerebral bleeding or thrombosis
occurs.
Treatment
Too rapid treatment of hypernatremic dehydration may cause significant morbidity
and mortality.
Idiogenic osmoles are generated within the brain during the development of
hypernatremia. These idiogenic osmoles increase the osmolality within the cells of
the brain, providing protection against brain cell shrinkage secondary to movement
of water out of cells into the hypertonic ECF. They dissipate slowly during correction
of hypernatremia.
With rapid lowering of the extracellular osmolality during correction of
hypernatremia, there may be a new gradient created that causes water movement
from the extra-cellular space into the cells of the brain, producing cerebral edema.
Symptoms of the resultant cerebral edema can produce seizures, brain herniation,
and death.
To minimize the risk of cerebral edema during correction of hypernatremic
dehydration, the serum sodium concentration should not decrease more than 12
mEq/L every 24 hours. The deficits in severe hypernatremic dehydration may need to
be corrected over 2 to 4 days
the initial resuscitation-rehydration phase of therapy remains the same as for other
types of dehydration.
Typical fluids:
D5 in ¼ NS ( ½ NS) + 20 mEq/L [K]
Seizures are the most common manifestation of cerebral edema from an overly
rapid decrease of the serum sodium concentration during correction of
hypernatremic dehydration
Acutely, increasing the serum concentration via an infusion of 3% sodium chloride
can reverse the cerebral edema.

11
Monitoring Therapy
Vital signs:
o Pulse
o Blood pressure
Intake and output:
o Fluid balance
o UOP & specific gravity
Physical examination:
o Weight
o Clinical signs of depletion or overload
Electrolytes
DRUG THERAP
ANTIMICROBIALS
Campylobacter Erythromycin
Clostredia difficle Vancomycin, Metronidazol
Salmonella Amp, TMP-SMZ ,Chloram,3rd GCS
Shigella Co-TMZ,Nalidixic acid, 3rd GCS
V cholerae Tetracycline,Co-TMZ
G lambilia Metronidazole
E histolytica Metronidazole
Nitazoxanide
,
an anti-infective agent, has been effective in the treatment of a wide
variety of pathogens including G. lamblia, E. histolytica, C. difficile, and rotavirus.
Although preliminary data suggest that nitazoxanide may be of use in nonspecific acute
secretory diarrhea, these data need replication in further studies.
Medications that slow gut motility diphenoxylate, loperamid & anticholinergics are
COTRAINDICATED
Racecadotril,
an enkephalinse inhibitor, has inconsistently been shown to reduce stool
output in patients with diarrhea. Experience with this drug in children is limited, and for
the average child with acute diarrhea it may be unnecessary.
Antiemetic
agents such as the phenothiazines are of little value and are associated with
potentially serious side effects (lethargy, dystonia, malignant hyperpyrexia). Nonetheless,
ondansetron is an effective and less-toxic antiemetic agent. Because persistent vomiting
can limit oral rehydration therapy, a single sublingual dose of an oral dissolvable tablet of

11
ondansetron (4 mg 4-11 yr and 8 mg for children >11 yr [generally 0.2 mg/kg]) may be
given.
However, most children do not require specific antiemetic therapy; careful oral rehydration
therapy is usually sufficient.
Probiotic
The use of probiotic nonpathogenic bacteria for prevention and therapy of diarrhea has
been successful in developing countries. In addition to restoring beneficial intestinal flora,
probiotics can enhance host protective immunity.
A variety of organisms (Lactobacillus, Bifidobacterium) have a good safety record.
Enteral Feeding and Diet Selection
Continued enteral feeding in diarrhea aids in recovery from the episode, and a continued
age-appropriate diet after rehydration is the norm.
Once rehydration is complete, food should be reintroduced while oral rehydration can be
continued to replace ongoing losses from emesis or stools and for maintenance. Breast-
feeding or nondiluted regular formula should be resumed as soon as possible. Foods with
complex carbohydrates (rice, wheat, potatoes, bread, and cereals), lean
meats, yogurt,
fruits, and vegetables are also tolerated. Fatty foods or foods high in simple sugars (juices,
carbonated sodas) should be avoided.
COMPLICATIONS
Renal Failure
o Dehydration
o Acute Tubular Necrosis
o Haemolytic-Uraemic Synd.
o Renal Vein Thrombosis
Hypokalaemia and Paralytic Ileus.
Secondary Lactose Intoleranc
Fluid Overload and Pulmonary Edema
Convulsions
o Fever.
o Hypoglysemia.
o Hypocalcemia.
o Hyponatremia.
o Hypernatremia.
o Hypomagnesemia.

12
o Meningitis.
o
Cerebral Vascular Thrombosis.
Prevention
Promotion of Exclusive Breast-feeding
Improved Complementary Feeding Practices
Rotavirus Immunization
Improved Water and Sanitary Facilities and Promotion of Personal and Domestic
Hygiene
Improved Case Management of Diarrhea