1
Fifth stage
Medicine
Lec-1
د . منوع
1/1/2014
Acute poisoning
Common medical emergency
Its incidence varies in different countries
Substances involved in poisoning vary as well
Paracetamol poisoning is very common in UK (48% of all cases of poisoning), while it is
rare in Iraq.
Organophosphorus poisoning on the other hand is very common in developing countries
including Iraq.
Assessment of an acutely poisoned patient :
First aid measure
History taking
Standard clinical examination
Laboratory investigation
First aid measure
First aid measure should ensure that:
Airway is clear
Breathing is adequate
Circulation is not compromised
History taking
History taking should include:
Establishing the diagnosis of poisoning
Calculating the duration since exposure to the toxic substance
Identification of the drug or substance abused
Asking about the cause of poisoning
Considering the symptoms since poisoning
Asking about past medical and psychiatric history
2
Clinical examination
Start standard clinical examination esp. considering:
State of consciousness (better assessed by Glasgow coma scale)
Most cases of poisoning can lead to disturbance of consciousness, but this is
especially true in case of psychotropic drugs.
In an unconscious patient, carefully exclude stroke, hypoglycemia, diabetic
ketoacidosis, CNS infection (meningitis and encephalitis), uraemia, hepatic
encephalopathy, and brain injury.
Pupil size:
Small (miosis): Opioids (narcotics)
OP (organophosphorus)
Large (midriasis): Anticholenergics
TCAD
Alcohol
Antihistaminics
Respiratory rate:
Reduced: Opioids
Benzodiazapines
Increased Salicylates
Blood pressure:
Hypotension TCAD
Salicylates
Phenthiazines
Hypertension
agonists
3
Heart rate:
Tachycardia (or tachyarrhythmia): TCAD,
Digoxine
Theophylline
Anticholenergics
Antihistamines
Bradycardia (or bradyarrhythmia): Digoxine
CCB (calcium channel blockers)
Blockers
Opioids
Temperature:
Fever: Anticholenergic
Salicylates
SSRI
Hypothermia: CNS depressants
Phenthiazines
Cerebellar signs (esp. nystgmus): Anticonvulsants
Alcohol
Extrapyramidal signs: Phenthiazines
Metoclopromide
Convulsions: TCAD
Theophylline
Anticonvulsants
NSAIDs
Sweating: Salicylates
OP

4
Cyanosis: CNS depressants
Methaemoglobinaemia
Jaundice: Paracetamol
Needle tracts: Drug abuse
Toxicology study
Urea, creatinine and electrolytes should be measured in most patients.
Arterial blood gases and acid base balance should be checked in those with
significant respiratory or circulatory symptoms and when the poison is likely to affect
acid base balance
Toxicology laboratory is needed for
The measurement of serum level of paracetamol (and to a lesser extent of aspirin) to
plan subsequent management.
Other types of poisoning are diagnosed by urine or gas chromatography (only in
difficult cases and for medico-legal indications).
General management of acute poisoning
A. Prevention of further absorption
B. Supportive care
C. Antidotes
D. Psychiatric consultation
A. Prevention of further absorption
Removal of clothing and skin washing with soap and water in case of contamination by
chemicals or pesticides.
Eye irrigation by normal saline for 15 min. in case the eye is contaminated.
Patients breathless or wheezy because of inhaling toxic gases or fumes should receive
oxygen and bronchodilator nebulization
Ingested poisons are removed by:
Gastric lavage
5
Activated char coal
Whole bowel irrigation
Urinary alkalization
Haemodialysis and haemoperfusion
Gastric lavage:
◦ Only if potentially life threatening amounts are ingested (not to be used for
acids, alkalis, or petroleum distillates poisoning).
◦ No gastric lavage should be attempted in unconscious patient unless the
airways are protected by cuffed endotracheal tube.
Activated charcoal:
◦ it adsorbs most toxins and is the method of choice to prevent further drug
absorption.
◦ For patients poisoned within one hour, 50 gm is given orally.
◦ The dose can be repeated every 4 hours for carbamazepine, theophylline
poisoning.
◦ For patients with disturbed consciousness or those who can not swallow,
activated charcoal is administered through nasogastric tube and the airway
should be protected to avoid aspiration pneumonitis.
◦ If multiple doses are needed, a laxative (like sorbitol) is given to avoid intestinal
obstruction.
◦ Certain poisons are not adsorbed by charcoal, including iron, lithium, acids,
alkalis, ethanol, methanol and petroleum distillates
Whole bowel irrigation:
◦ Polyethylene glycol is administered orally for potentially toxic ingestion of iron,
lithium, and theophylline.
◦ One litre is ingested every hour until the rectal effluent is clear.
◦ Contraindications include GI bleeding or ulceration
Urinary alkalinization:
◦ Indicated for severe salicylate poisoning
Haemodialysis or haemoperfusion:
◦ Effective methods of treating severe poisoning by salicylate, theophylline,
carbamazepine, and methanol
6
B. supportive care
1. Unconscious patients are better treated in intensive care units with general treatment of
comatose patient provided. Regular recording of Glasgow coma scale is important.
2. Convulsions are treated with IV diazepam 10mg IV repeated as necessary.
3. If cardiac complications are present or expected, the patient is put under continuous
ECG monitoring.
4. Ventilatory support may be needed for those with respiratory depression.
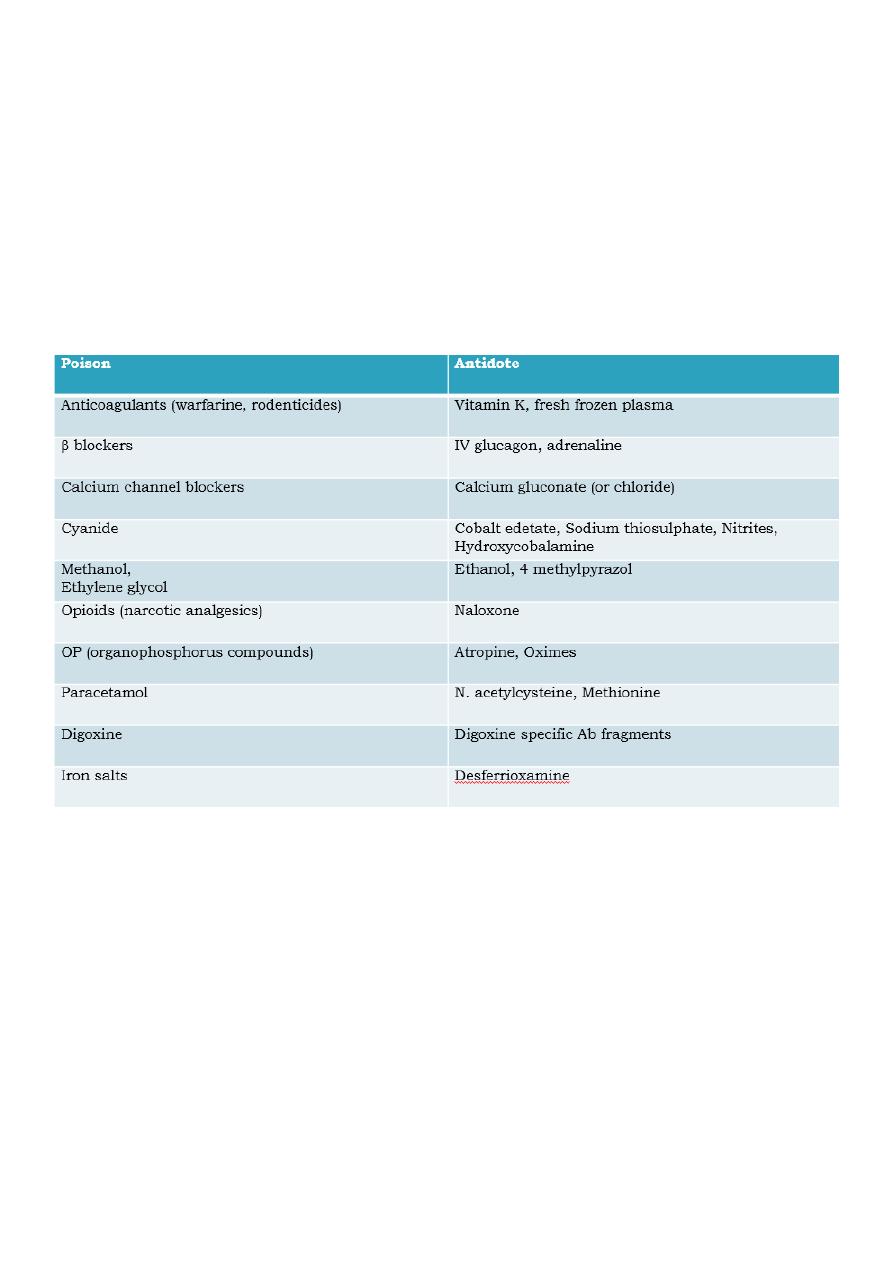
C. Antidotes
D. psychiatric consultation
This is essential for patients who have attempted suicide.
The psychiatrist should be consulted as soon as the patient recovers.
Substances of low toxicity
Certain substances are of very low toxicity even if ingested in high doses. Examples include:
most antibiotics (except antiTB, and tetracyclines)
antiulcer drugs (H2 blockers and PPIs)
oral contraceptive pills
chalk
paper glue
washing liquids