Tumours of the Spines (Spinal Tumours)
Tumours of the SpinesAs in the brain, any space occupying lesion around the soft encaged spinal cord will produce the same symptoms, signs and even radiological appearance of a tumour.
Spinal Tumours
15 % of primary CNS tumors are intraspinal.Most of the primary CNS spinal tumors are benign.
Most present by compression rather than invasion.
Sites of Spinal Tumours
ExtraduralIntradural: which may be either:
Extramedullary (i.e. outside the cord)
Intramedullary (i.e. inside the cord, within the substance of the cord)
• Extradural Tumours:
Pathological Types:Metastatic tumours (secondary deposits)
Sarcoma
Chordoma
Neurofibroma
Metastatic tumours (secondary deposits)
These are the most common tumours of the spine, accounting for 98% of all spine lesions.
Although metastatic lesions may be found in each group, they are usually extradural.
Areas involved in frequency are dorsal, cervical, lumbar and sacral.
These are also the commonest extradural tumours.
Metastatic tumours (secondary deposits)
• The most common sites of origin usually from the following organs in order of frequency:Breast (21%)
Lung (14%)
Prostate (7.5%)
Renal (5%)
Gastrointestinal (5%)
Thyroid (2.5%)
Metastatic tumours (secondary deposits)
Methods by which metastatic disease spreads to the spines:Embolisation through the venous system (Batson's plexus): this is the most frequent pathway.
Embolasation through the arterial system.
Direct extension.
Lymphatic spread.
Neurofibroma
Neurofibroma may be "dumb-bell" in shape, the smaller part lies within the neural canal while the larger part projects through an intervertebral foramen and encroaches on the thorax.
Clinical Features of Extradural spinal tumours
These tumours present with symptoms and signs of irritation of nerve roots preceding the signs of pressure on the cord.Differential diagnosis of Extradural Spinal Tumours
Prolapsed intervertebral disc in the lumbar and less commonly in the cervical regions, may produce identical symptoms.Intradural Tumours
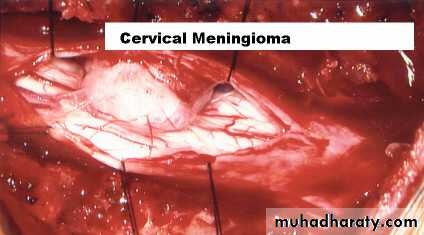
• I. Intradural Extramedullary Tumours:Pathological Types: the most important are
Meningiomas
Neurofibromas
Clinical Features of Extramedullary Tumours
Sensory and motor weakness. The anterior or posterior roots tend to be involved first; the proximal level of the sensory and motor changes depends on the site of the tumour.Symptoms due to pressure on the cord itself occur later, there may be the Brown-Sequard hemisection phenomenon, with weakness and loss of vibration sense on the same side as the lesion and loss of pain on the opposite side. Paraplegia will follow if pressure is not relieved.
Intradural Intramedullary tumours
Pathological types: Intramedullary tumours are usually:Ependymomas.
Astrocytomas (Gliomas).
Clinical features of Intramedullary Tumours
Cord signs present first, while root pains tend to occur later.
Paralysis may occur on both sides, or sometimes may be of the crossed type, where there is anaesthesia on one side and paralysis and hyperaesthesia on the other.
Dissociated sensory loss may occur.
Urinary incontinence usually appears early.
Investigations of Spinal Tumours
Plain X-ray of the spines should be done in anteroposterior, lateral and oblique views.• Erosion of bone or some other bony abnormalities is seen nearly 50% of patients with spinal tumours.
2. CT scan and MRI of the spines will show the lesion clearly.
3. Myelography has been largely superseded by CT scan and MRI.
MRI

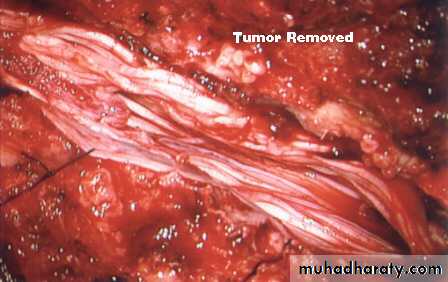
Treatment of Spinal Tumours
Laminectomy is performed and if possible the tumour is removed.Removal of the tumour and laminectomy help in decompression of the cord.
Acute paraplegia demands an emergency operation.
Treatment of Spinal Tumours
If the vertebral body pathology with anterior compression, a corpectomy done with fusion and fixation.
Intradural Tumour
Intradural Tumour

Intradural Tumour