1
Fifth stage
Surgery-Ortho
Lec-5
د.هشام القطان
19/10/2015
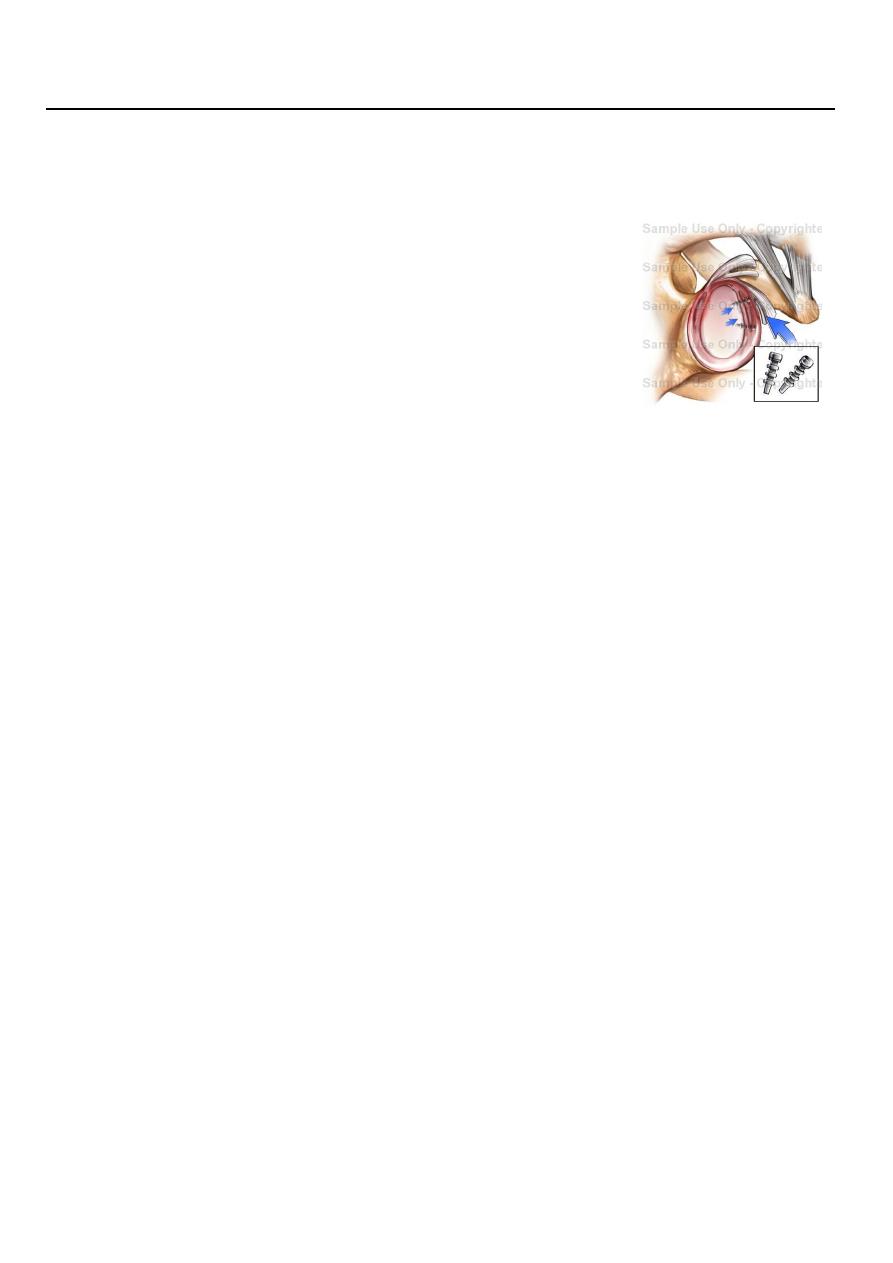
Review Anatomy Of The Shoulder
The shoulder consists of four joints:
Glenohumeral.
Acromioclavicular
Scapulothoracic
Labrum around edge of saucer Capsule and capsular ligaments
Dynamic “cuff” of muscles
Subscapularis anterior
Supraspinatus superior
Infraspinatus posteriorsuperior
Teres minor posterior
Long head of biceps intra-articular
Examination
The patient should always be examined from the front and from the behind.
Both upper and the chest must be visible.
Examination of the shoulder must include a full examination of the neck and vice
versa.
Basic Examination; Inspection
General: Swelling, Erythema, Joint Deformity, Muscle wasting
Front: Sternoclavicular Joint prominence, Clavicle deformity, Acromioclavicular joint
prominence
Side: Swelling
Behind: Scapula shape and situation, Webbing of the skin, Winging
Above: Clavicle, Supraclavicular fossa, Swelling
2
Basic Examination; Palpation
Heat
Crepitations
Bony tenderness
Humeral head and shaft
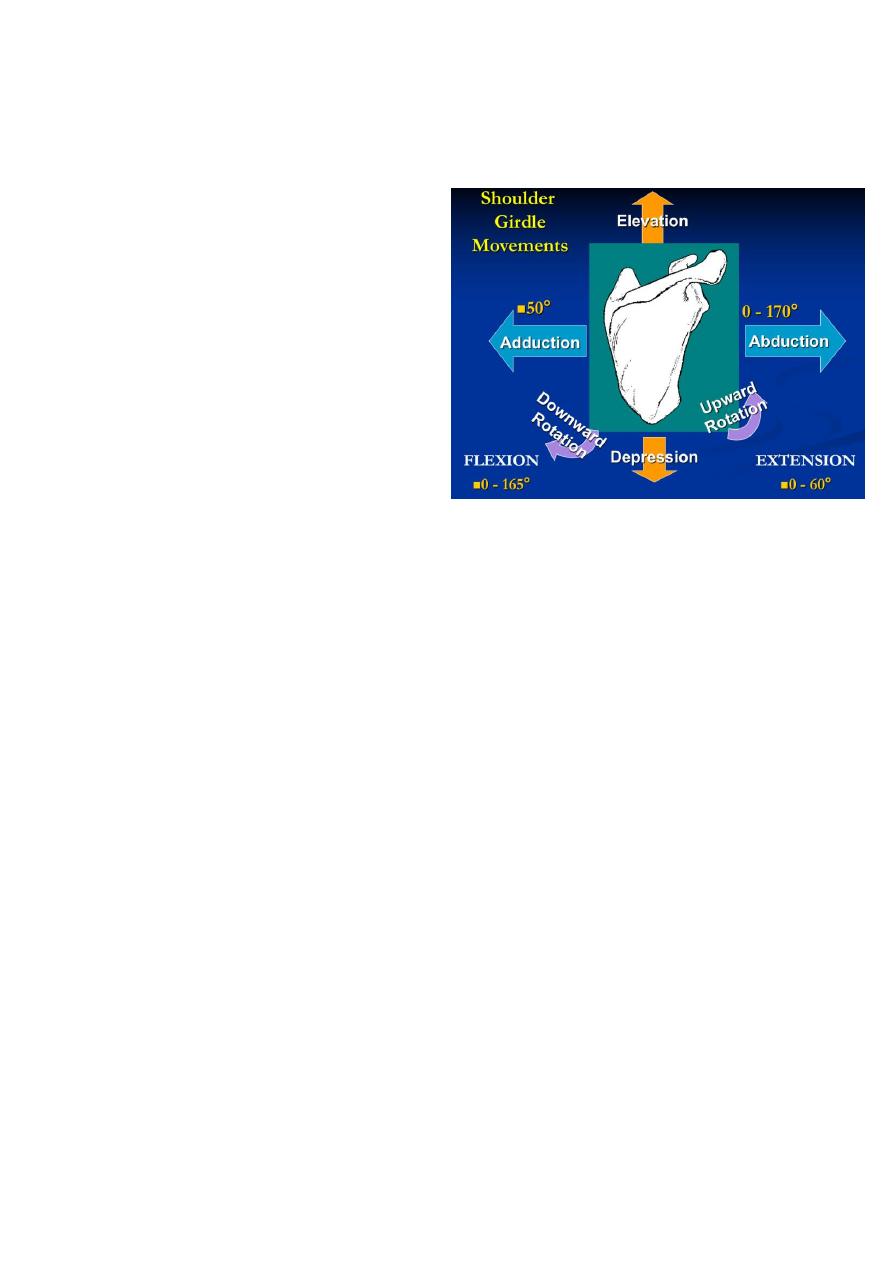
Basic Examination; Movement
Active before passive
Internal rotation in abduction - 70°
External rotation in extension - 70°
Drop Arm Test Supraspinatus
Weakness
Speed’s Test Bicep Tendon Irritation
Apprehension tests
Investigations
X-ray
WBC
ESR
Blood Culture
Aspiration of the Joint
CAT
MRI
Arthroscopy
Arthography
Examination under anesthetic
Disorder of the rotator cuff
A acute tendinitis.
Chronic tendinitis (Impingement Syndrome).
Rotator Cuff Tears.
Frozen Shoulder.

3
Supraspinatus Tendinitis
acute calcific tendinitis
Pain is caused by inflammation of the tendon and subacromial bursa.
Age of onset is 43
Men being more commonly affected.
Clinical features
Rapid onset without Warning. Disturbance of sleep.
Severe pain.
Apprehension to move the arm.
Acute localised tenderness.
Shoulder Impingement Tests
Hawkins-Kennedy Test.
Neer’s Test
X-ray :
calcium deposit close to insertion of the Supraspinatus tendon.
Treatment
mild cases :
Rest with sling
Anti-inflammatories
Severe cases :
1.long acting steroid injections (methylprednisolone 40-80 mg).
with local anaesthetic (lignocaine 1%).
2.If symptom not relieved surgery for removal calcific material.
Impingement Syndrome
The pain is due to irritation of the Supraspinatus tendon.
Commonly caused by repeated overhead movements which cause pinching of the
tendon.
The clinical featuresPatient age 40-60 years.
Onset usually insidious .
But can be sudden after overuse.
Painful lateral aspect of upper arm( over the deltoid muscle).
Worse at night.
4
can not lie on affected arm.
The shoulder looks normal.
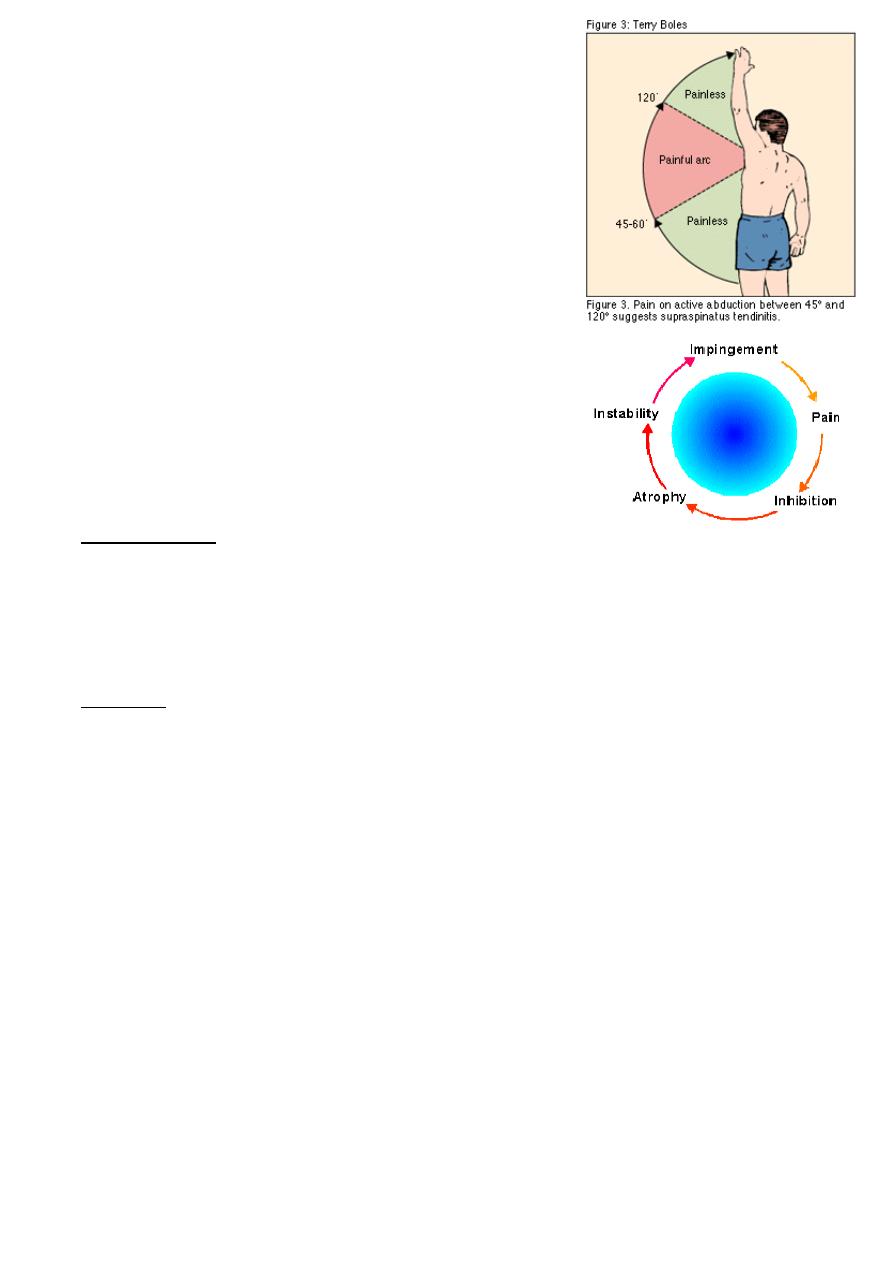
pain on overhead and behind the back m ovements.
Repeating the movement with the arm in full external
rotation may be easier and painless
(pathognomonic of Supraspinatus tendinitis)
Crepitus or clicking during movement.
In long standing cases wasting of the muscles
Loss of power
Treatment
Rest in the younger patient, modification of activity
(i.e. not playing golf/ racket sports).
In chronic cases
Physiotherapy.
analgesics and sometimes steroid and local anaesthetic injections become necessary.
If symptoms keep recurring, operation is advisable by decompressing the
coracoacromial ligament (now a day done by arthroscopy)
Operative
Acromioplasty
Coracoacromial ligament
Release
Rotator Cuff Tear
Minor In minor tears the Supraspinatus muscle is still able to function.
Major In a major tear there is no activity of the Supraspinatus muscle.
Clinical features
The patient is usually aged 45-75.
While lifting a weight or protecting himself from falling, he 'sprains' his shoulder.
Pain is felt immediately.
Unable to lift his arm sideways.
The appearance is usually normal.
but in longstanding cases there is Supraspinatus wasting.
5
Tenderness may be diffuse or may be localized to just below the tip of the acromion
process.
With a recent injury, active abduction is grossly limited and painful.
To distinguish between partial and complete tears, pain is abolished by injecting a
local anesthetic.
if active abduction is now possible, the tear must be only partial.
Weeks later
Two types are easily differentiated.
With a complete tear.
Pain has by then subsided.
Active abduction is impossible .
Passive abduction is full and once the arm has been lifted above a right angle, the
patient can keep it up by deltoid (the abduction paradox).
When he lowers it sideways it suddenly drops (the drop-arm sign).
With a partial tear.
abduction slowly recovers.
Investigations
The diagnosis may be confirmed by ultrasonography.
Arthroscopy
Frozen Shoulder
The term frozen shoulder should he reserved for, ((((a well-defined disorder
characterized by progressive pain and stiffness which usually resolves spontaneously
after about 18 months))).
The patient, aged 40-60.
May give a history of trauma, often trivial.
Pain gradually it increases in severity and
Prevents sleeping on the affected side.
After several months it begins to subside.
But as it does so, stiffness becomes more and more of a problem.
Untreated, stiffness persists for another 6-12 months. Gradually movement is
regained, but may not return to normal.
Usually there is nothing to see except slight wasting.
There may also be some tenderness.

6
But movements are always limited and in a severe case the shoulder is extremely
stiff.
Stages:
Freezing Moderate diffuse pain, normal but painful motion.
Frozen Pain subsides, leaving stiffness and severe decrease in function.
Thawing Return to normal function gradually.
X-rays
Show decreased bone density in the humerus.
Arthrography shows a contracted joint.
Treatment
Freezing: Try to abort in the inflammatory stage, local heat , NSAIDs, cortisone
injection locally sometimes help , physiotherapy.
Frozen or Thawing:
Manipulation under GA if no progress with physio
Arthroscopic release for resistant cases
Elbow
EXAMINATION
Both upper limbs must be complete." exposed and it is essential to look for the back
as well the front.
The neck ,shoulder and hands should also be examined.
Look
Looking at the patient from the front,
with his or her arms outstretched alongside the body and the palms facing forwards,
the elbows are seen to be held in 5-10 degrees of valgus;
this is the normal 'carrying angle'.
Anything more, especially if unilateral, is regarded as a valgus deformity.
Varus deformity is less obvious.
The most common swelling is in the olecranon bursa at the back of the elbow.
Feel
Important bony landmarks are the medial and lateral condyle ,and the tip of the
olecranon.
These are palpated to determine whether the joint is correctly positioned.

7
Superficial structures are examined for warmth and subcutaneous nodules.
The joint line (including the radioulnar joint
depression is located and palpated for synovial thickening.
Tenderness can usually be localized to a particular structure.
The ulnar nerve is fairly superficial behind the medial condyle and here it can be
tolled under
Movement
Flexion and extension are compared on the two sides.
the radioulnar joints are : pronation and supination
General examination
symptoms and signs do not point clearly to a local disorder,
other parts are examined:
the neck for cervical disc lesions),
the shoulder (for cuff lesions)
the hand (for nerve lesions)
Radiological examination
position of each bone is noted.
then the joint line and space.
Next, the individual bones are inspected for evidence of old injury or bone
destruction.
Finally, loose bodies .
ELBOW DEFORMITIES
CUBITUS VARUS (or 'gun-stock') deformity
is most obvious when the elbows are extended and the arms are elevated.
The most common cause is malunion of a supracondylar fracture.
The deformity can be corrected by a wedge Osteotomy of the lower humerus.
CUBITUS VALGUS
The most common cause

8
is non-union of a fractured lateral condyle; this may give gross deformity and a bony
knob on the inner side of the joint.
The importance of valgus deformity is the liability for delayed ulnar palsy to develop;
years after the causal injury,
the patient notices weakness of the hand with numbness and tingling of the ulnar
fingers.
The deformity itself needs no treatment.
but for delayed ulnar palsy the nerve should be transposed to the front of the elbow
'TENNIS ELBOW'
The cause of these common disorders is unknown.
Most cases follow minor trauma or repetitive strain on the tendon aponeuroses
attached to the lateral .
Pain is probably due to a vascular repair process similar to that of rotator cuff
tendinitis around the shoulder.
Often there is a history of occupational stress or unaccustomed activity.
1. such as house painting,
2. carpentry or
3. other activities that involve strenuous wrist movements and forearm muscle
contraction
Clinical features
pain is felt over the outer side of the elbow.
in severe cases it may radiate widely.
It is initiated or aggravated by movements such as pouring out tea.
turning a stiff door-handle.
shaking hands or.
lifting with the forearm.
The elbow looks normal and flexion and extension are full and painless.
Tenderness is localized to a spot just below the lateral epicondyle, and pain is
reproduced by getting the patient to extend the wrist against resistance.
Or simply by passively flexing the wrist so as to stretch the common extensors.
Treatment
Rest and analgesia.
9
If pain is severe. the area of maximum tenderness is injected with a mixture of
corticosteroid and local anaesthetized .
Persistent pain
surgery with detachment origin at the humeral epicondyle
'GOLFER'S ELBOW'
Similar symptoms occur around the medial epicondyle and, owing to involvement of
the common tendon of origin of the wrist flexors.
pain is reproduced by passive extension of the wrist.
Treatment
Rest, or avoiding the precipitating activity, allow the lesion to heal.
If pain is severe, the area 0f maximum tenderness is injected with a mixture
corticosteroid and local anaesthetic.
Persistent pain which fails to respond conservative measures may call for operative
treatment.
(((The affected common tendon on the medial side of the elbow is detached from its
origin at the humeral epicondyle))).
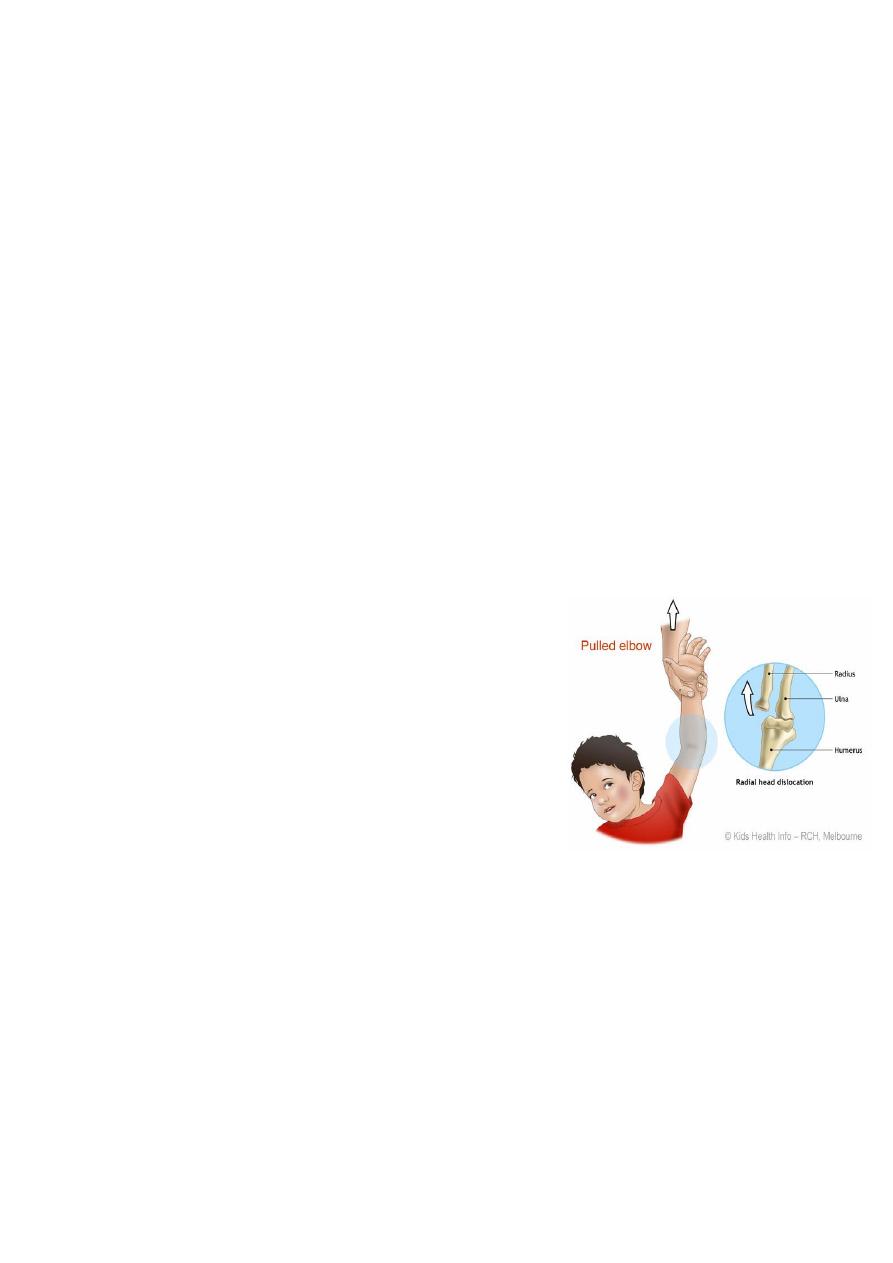
PULLED ELBOW “Nursemaids Elbow”
is due to the radial head stretching the ligament
and slipping out from under its cover.
It occurs in children in the 2-6 age group,
and is a common in young chil
dren between 1 and
4 years of age.
It is rare beyond the age of 6 years
condition that young children often get from being swung around while being held by
the lower arms It.
commonly occurs when being grabbed suddenly by the wrist, e.g. to prevent a child
running into the road, or when a child falls while his hand is being held.
jerky pressure on the elbow joint can pop the radial head out from under the
ligament.
This is not a considered a dislocation of the elbow, which
is extremely rare in young children.
A child will begin to cry right after the injury, and cannot
move the affected forearm because of the pain.
The arm is slightly bent at the elbow, and the forearm is usually held in front of the
stomach.

11
The patient’s history and distinct posture of the affected forearm make the diagnosis.
An X-ray is not usually required.
Investigation
X rays are unnecessary if there is a typical history and no visible swelling or
deformity.
If the child has a pulled elbow the X ray is normal.
The child may have normal use of the arm on return from radiology since positioning
by the radiographer may solve the problem.
Management
A pulled elbow is corrected by a specific manipulation, which is uncomfortable for a
moment, a click is often felt as the radial head pops back under the ligament.
The child will start using the arm soon afterwards.
If the elbow is not corrected with manipulation,
the arm is rested in a sling as spontaneous correction usually occurs within 48 hours.
You may wish to give your child pain relief.
HOW TO PREVENT THIS FROM HAPPENING AGAIN
Avoid lifting or pulling a child by the hands, wrist or forearms.
Avoid swinging a child around by their wrists or forearms.
Use upper arms or arm-pits to lift the child
OLECRANON BURSITIS
The olecranon bursa sometimes becomes enlarged as a result of pressure or friction.
When it is also painful, the
Cause is more likely to be infection. gout or rheumatoid arthritis.
Treatment
The underlying disorder must be treated.
Septic bursitis may need local drainage.
Occasionally a chronically enlarged bursa has to be excised.
11
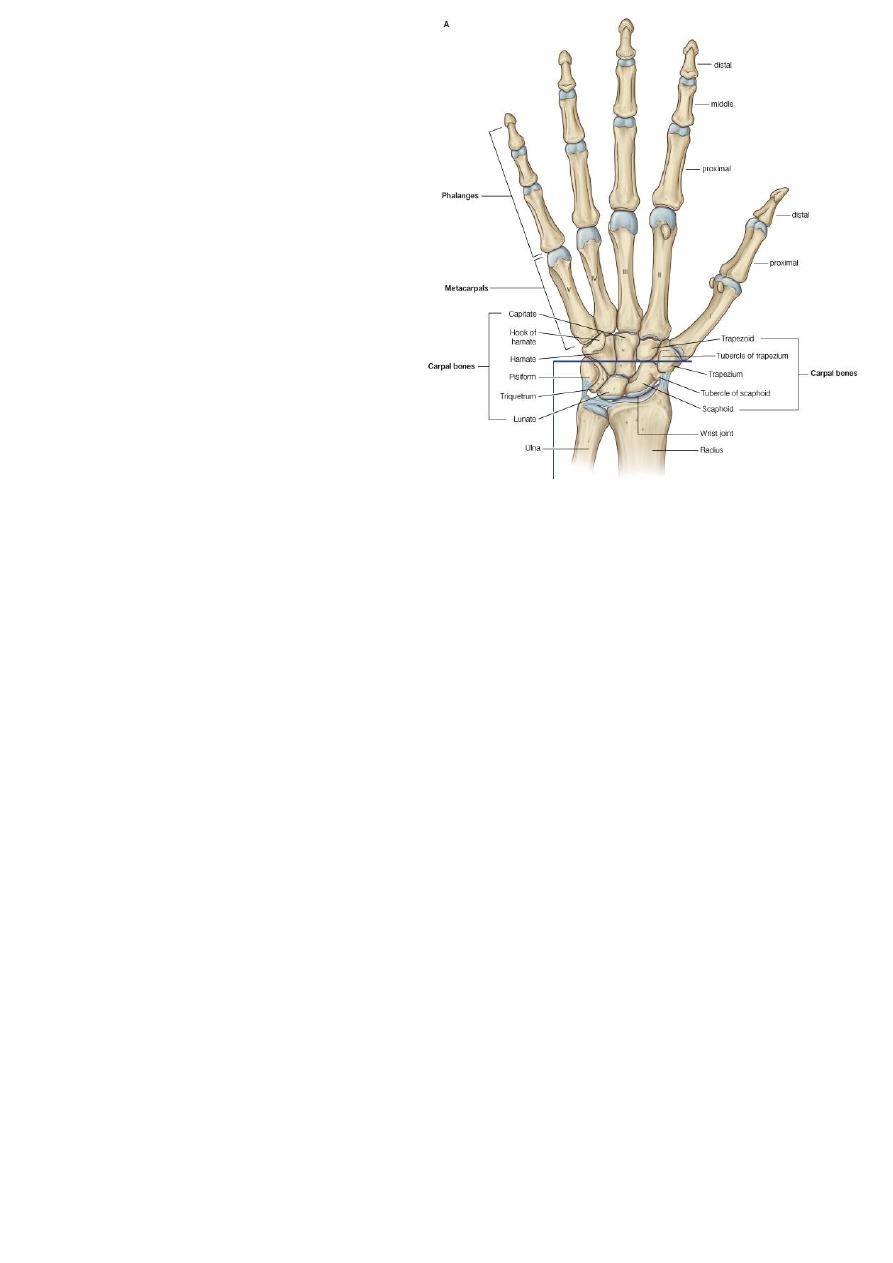
Wrist and hand
WRIST DEFORMITIES
CONGENITAL DEFORMITIES
Radial club-hand
The infant is born with the wrist in
marked radial deviation.
There is absence of the whole or
part of the radius, and usually also
the thumb.
Treatment
In the neonate consists of gentle manipulation and splintage.
If function deteriorates, centralization of the carpus over the ulna is recommended,
preferably before the age of 3 years
Madelung's deformity
The carpus is deviated forwards, leaving the ulnar head projecting on the back of the
wrist.
Deformity is seldom marked before the age of 10 years.
function is usually excellent.
in the worst cases the deformity may have to be corrected by Osteotomy
RHEUMATOID ARTHRITIS
Wrist
After the metacarpophalangeal joints.
the wrist is the most common site of rheumatoid arthritis.
Pain.
swelling and tenderness may at first be localized to the radioulnar joint.
or to one of the tendon sheaths.

12
Sooner or later the whole wrist becomes involved and tenderness is much more ill-
defined.
In late cases the wrist is deformed and unstable ulnar deviation
Hand and fingers
To start synovitis of the proximal joints and tendon sheaths; later, joint and tendon
erosions.
final stage, joint instability and tendon rupture cause progressive deformity and loss
of function.
Pain and stiffness of the fingers are early symptoms.
As the disease progresses, deformities begin to appear
Ulnar deviation of the fingers and subluxation of the Mp joints, often associated with
boutonniere deformities
Swan-neck deformity
Extensor tendons may rupture where they cross the dorsum of the wrist. causing one
or more of the fingers to drop into flexion
Dropped finger.
Ruptured extensor pollicis longus
X ray
The characteristic features are osteoporosis and bony erosions.
Narrowing joint space. small periarticular erosions appear
Treatment
Management in the early stage consists of splintage.
local injection of corticosteroids.
Combined with systemic treatment.
At late stage surgery different type.
KIENBOCK'S DISEASE
After injury or stress.
The lunate bone may develop a patchy avascular necrosis.
A predisposing factor: may be relative shortening of the ulna . which could result in
excessive stress being applied to the lunate where it is squeezed between the distal
surface of the (overlong) radius and the second row of carpal bones.

13
The patient, usually a young adult.
Complains of ache and stiffness.
Tenderness is localized to the centre of the wrist on the dorsum.
wrist extension may be limited.
Imaging
The earliest signs of osteonecrosis can be detected only by MRI.
Typical x-ray signs are increased density in the lunate.
later osteoarthritis of the wrist.
Treatment
During the early stage, while the shape of the lunate is more or less normal,
osteotomy of the distal end of the radius may reduce pressure on the bone and
thereby protect it from collapsing.
In late cases, partial wrist arthrodesis may be the only option.
DECUERVAIN'S DISEASE
Tenovaginitis of the first dorsal compartment is usually seen in women between the
ages of 30 and 50 years.
There may be a history of unaccustomed activity,
such as pruning roses,
cutting with scissors or
wringing out clothes.
Clinical features
Pain.
and sometimes swelling, is localized to the radial side of the wrist.
The tendon sheath feels thick and hard.
Tenderness is most acute at the very tip of the radial styloid.
The pathognomonic sign :
is elicited by Finkelsteins test..
Hold the patient's hand firmly, keeping the thumb tucked in close to the palm, then
turn the wrist sharply towards the ulnar side.
A stab of pain over the radial styloid is a positive sign. Repeating the movement with
the thumb left free is relatively painless.
14
Treatment
In early cases, symptoms can be relieved by ultrasound therapy .
Or a corticosteroid injection into the tendon sheath.
Sometimes combined with splintage of the wrist.
Resistant cases need an
Operation, which consists of slitting the thickened tendon sheath.
Care should be taken to prevent injury to the dorsal sensory branches of the radial
nerve, which may cause intractable dysaesthia.
GANGLION
The ubiquitous ganglion:
is seen most commonly on the back of the wrist.
It arises from cystic degeneration in the joint capsule or tendon sheath.
The distended cyst contains a glairy fluid
The patient, often a young adult.
presents with a painless lump.
usually on the back of the wrist.
Occasionally there is a slight ache.
The lump is well defined, cystic and not tender.
It may be attached to one of the tendons.
Treatment
The ganglion often disappears after some months, so there should be no haste about
treatment.
If the lesion continues to be troublesome, it can be aspirated.
if it recurs, excision is justified, bur the patient should be told that there is a 30 per
cent risk of recurrence, even after careful surgery .
CARPAL TUNNEL SYNDROME
This is the commonest and best known of all the nerve entrapment syndromes.
In the normal carpal tunnel there is barely room for all the tendons and the median
nerve .
Any swelling is likely result in compression and ischaemia of the nerve.
Common in women at the menopause, in rheumatoid arthritis, in pregnancy and in
myxoedema.

15
Clinical features
The usual age group is 40-50 years
The history is most helpful in making the diagnosis.
Pain and paraesthesia occur in the distribution of the median nerve in the hand.
Night after night the patient is woken with burning.
Patients tend to seek relief by hanging the arm over the side of the bed or shaking
the arm.
helpful test (Tinels sign) : sensory symptoms can often be reproduced by percussing
over the median nerve.
Phalens test: Holding the wrist fully flexed for a minute or two .
In late cases there is wasting of the thenar muscles.
weakness of thumb abduction and sensory dulling in the median nerve territory.
Electrodiagnostic tests. which show slowing of nerve conduction across the wrist.
Treatment
Light splints that prevent wrist flexion can help those with night pain or with
pregnancy-related symptoms.
Steroid injection into the carpal canal, likewise, provides temporary relief .
Endoscopic carpal tunnel release offers an alternative with slightly quicker
postoperative rehabilitation.
Open surgical division of the transverse carpal ligament usually provides a quick and
simple cure.
Alternative therapies. Acupuncture . have benefited some patients but their
effectiveness remains unproved.
ACUTE INFECTIONS OF THE HAND
Infection of The hand is frequently limited or one of several well-defined
compartments:
Nail fold (paronychia).
The pulp space (whitlow).
Subcutaneous tissues elsewhere.
A tendon sheath.
One of the deep fascial spaces or a joint.
Almost invariably the cause is a Staphylococcus which has been implanted by trivial
or unobserved injury.
16
Pathology
Acute inflammation and suppuration in small closed compartments (e.g. The pulp
space or tendon sheath) may cause an increase in pressure to levels at which the
local blood supply is threatened.
In neglected cases tissue necrosis is an immanent risk.
Even if this does not occur, the patient may end up with a stiff and useless hand
unless the infection is rapidly control.
Clinical features
Usually there is a history of trauma, but it may have been so trivial as to pass
unnoticed.
A thorn prick can be as dangerous as a cut Within a day or two, the finger (or hand)
becomes painful and swollen.
The patient may feel ill.
feverish and the pain becomes throbbing.
obvious redness and tension in the tissues.
exquisite tenderness over the site of infection.
Finger movements may be markedly restricted.
Principles of treatment
Antibiotics
As soon as the diagnosis is made and specimens have been taken for microbiological
investigation, antibiotic treatment is started - usually with
flucloxacillin and, in severe cases, with fusidic acid
or a cephalosporin as well.
This may later be changed when bacterial sensitivity is known.
Rest and elevation
In a mild case the hand is rested in a sling.
In a severe case the arm is elevated in a roller towel.
while the patient is kept in hospital under observation.
Analgesics are given for pain.
Drainage
If there are signs of an abscess (throbbing pain, marked tenderness and toxaemia).
the pus should drained.
A tourniquet and either general or regional block anaesthesia are essential.
17
The incision should be made at the site of maximal tenderness, but never across a
skin crease.
Necrotic tissue is excised and the area thoroughly washed and cleansed.
The wound is either left open or lightly sutured and then covered with non-stick
dressings.
A pus specimen is sent for microbiological investigation.
Splintage
splint should be applied always with the joints in the position of safe.
Specific types of Infections
Paronychia
Pulp-space infection (felon)
Tendon-sheath infection
Deep fascial space infection
Human bites
M . O .
(including anaerobes) are encountered,
the commonest being Staphylococcus aureus,
Streptococcus group .
such wounds should be assumed to be infected.
Treatment
Surgery to clean the infected tissue.
Antibiotic .
TRIGGER FINGER
Intermittent 'deformity'. usually of the ring or middle finger.
The patient complains that, when the hand is clenched and then opened, the finger
(or thumb) gets stuck in flexion; with a little more effort, it suddenly snaps into fulI
extension
Causes is:
thickening of the fibrous tendon sheath
similar entrapment may occur due to a bulky
Tenosynovitis.

18
Treatment
Either healed spontaneously.
Local injection steroid
Surgery
DUPUYTREN'S CONTRACTURE
This is a nodular hypertrophy and contracture of the palmar aponeurosis.
The patient - usually a middle-aged man complains of a nodular thickening in the
palm.
If the subcutaneous cords extend into the fingers, they may produce flexion
deformities at the MP and PIP joints.
Operation is indicated if the deformity is progressive and interferes with function.
Photos www.muhadharaty.com/lecture/2831