1
Fifth stage
Surgery-Ortho
Lec-12
د . هشام
1/1/2014
DISSICANS AND FOOT DEFORMITY AND KNEE
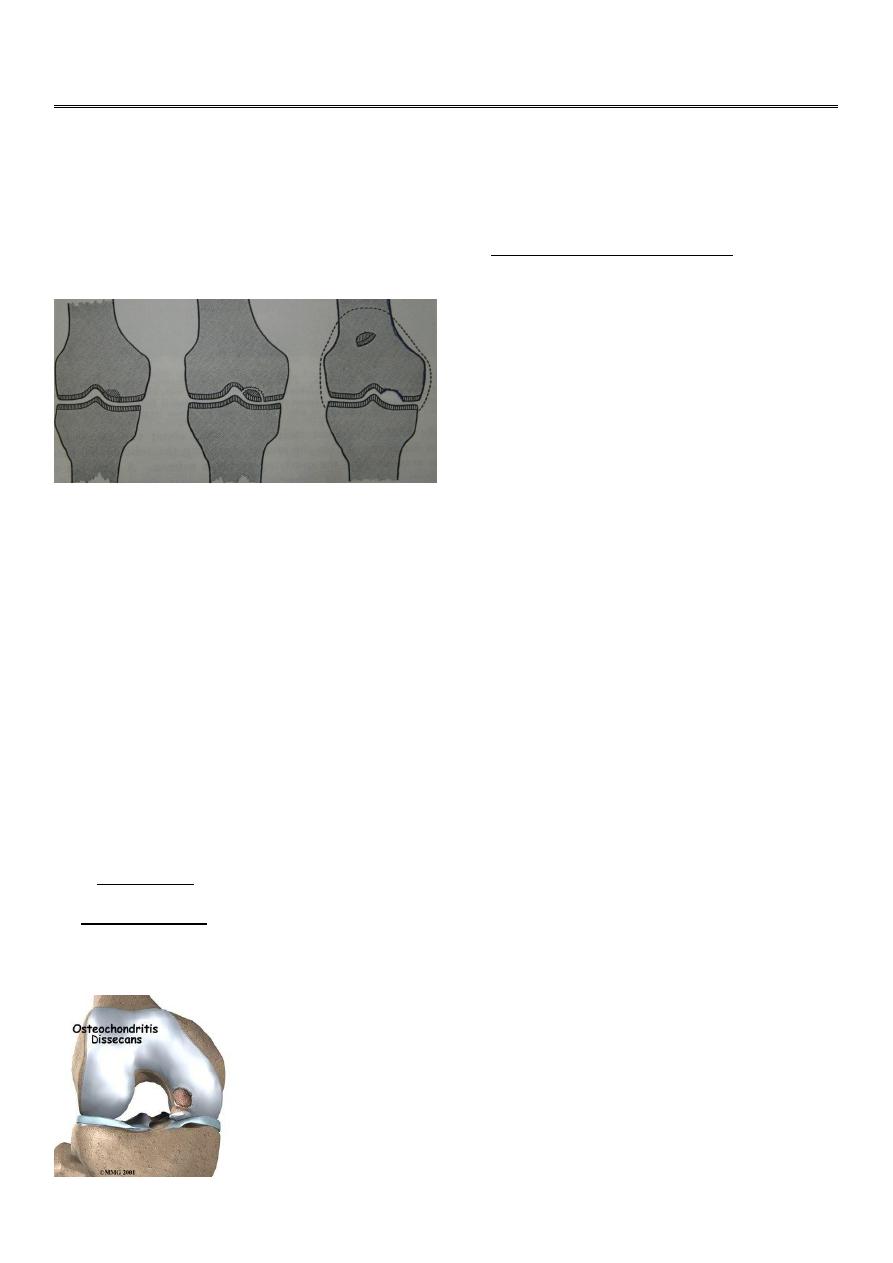
Osteochondritis dissecans
A small well demarcated avascular fragment of bone and overlying cartilage sometimes
separated from one of the femoral condyle and appears as a loose body in the joint
A etiology:
Either single impact trauma
Or repeated micro trauma
Clinical features:
Male patient usually 15-20 years Presented with intermittent ach or swelling.
Later attacks of giving way ,locking may occur.
Waisted quadriceps muscle
Joint effusion
Soon after the attack there are two signs almost diagnostic
1.tenderness localizes to one femoral condyle.
2.wilsons sign positive (the knee is flexed to 90 degree rotated medially and then
gradually straightened pain is felt). repeating the test with the knee rotated laterally is
painless.
2
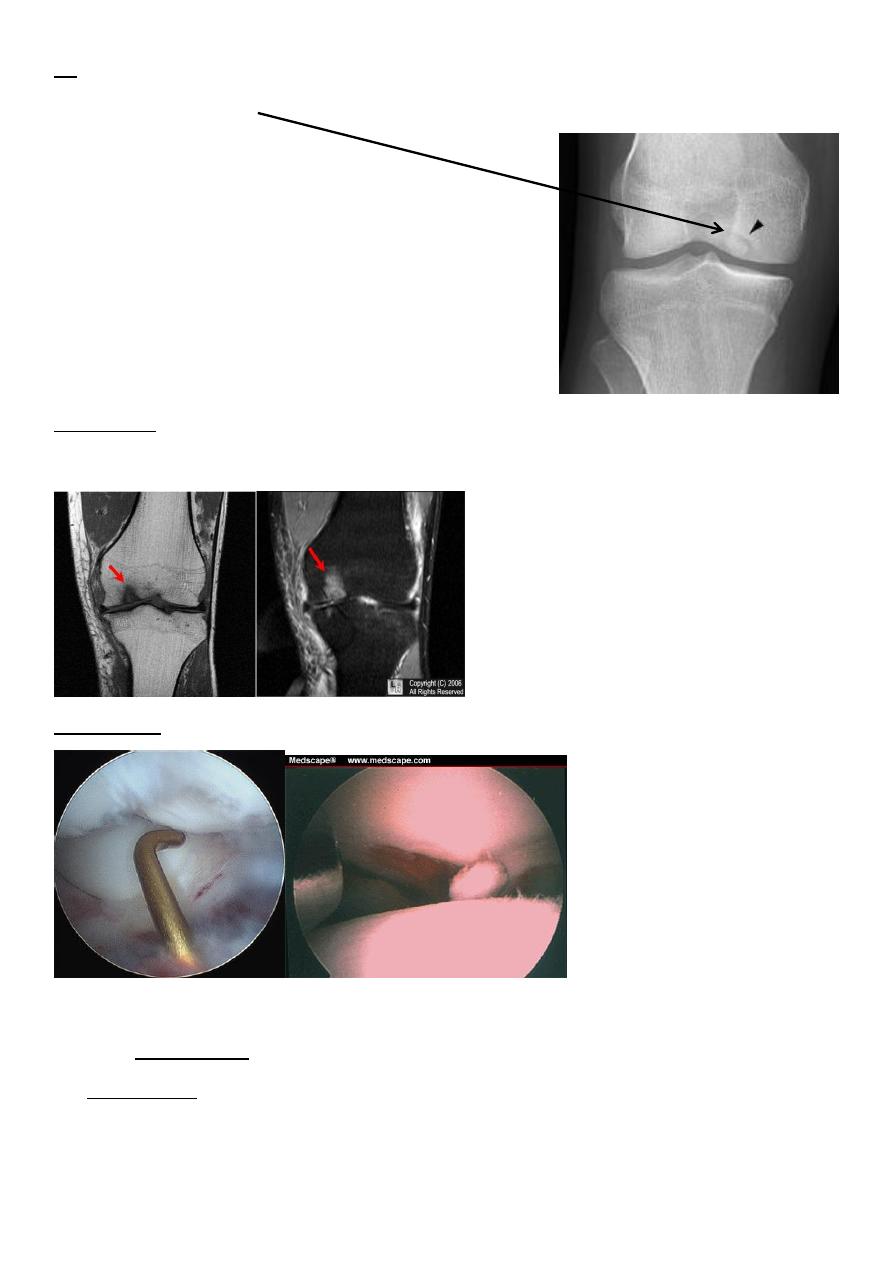
XR show aline of demarcation or an empty hollow.
Loose body in the joint
Radioactive isotopes increase activity around the lesion.
M R I
Arthroscopy.
Treatment:
In the earliest stage
(stable lesion) activity curtailed for 6-12 months.
If the fragment unstable
If small removed.
3
Large >1 cm fixed in situ.
If the fragment is completely detached in one piece
Refixation
If fragment in pieces
(discarded and drilling bed).
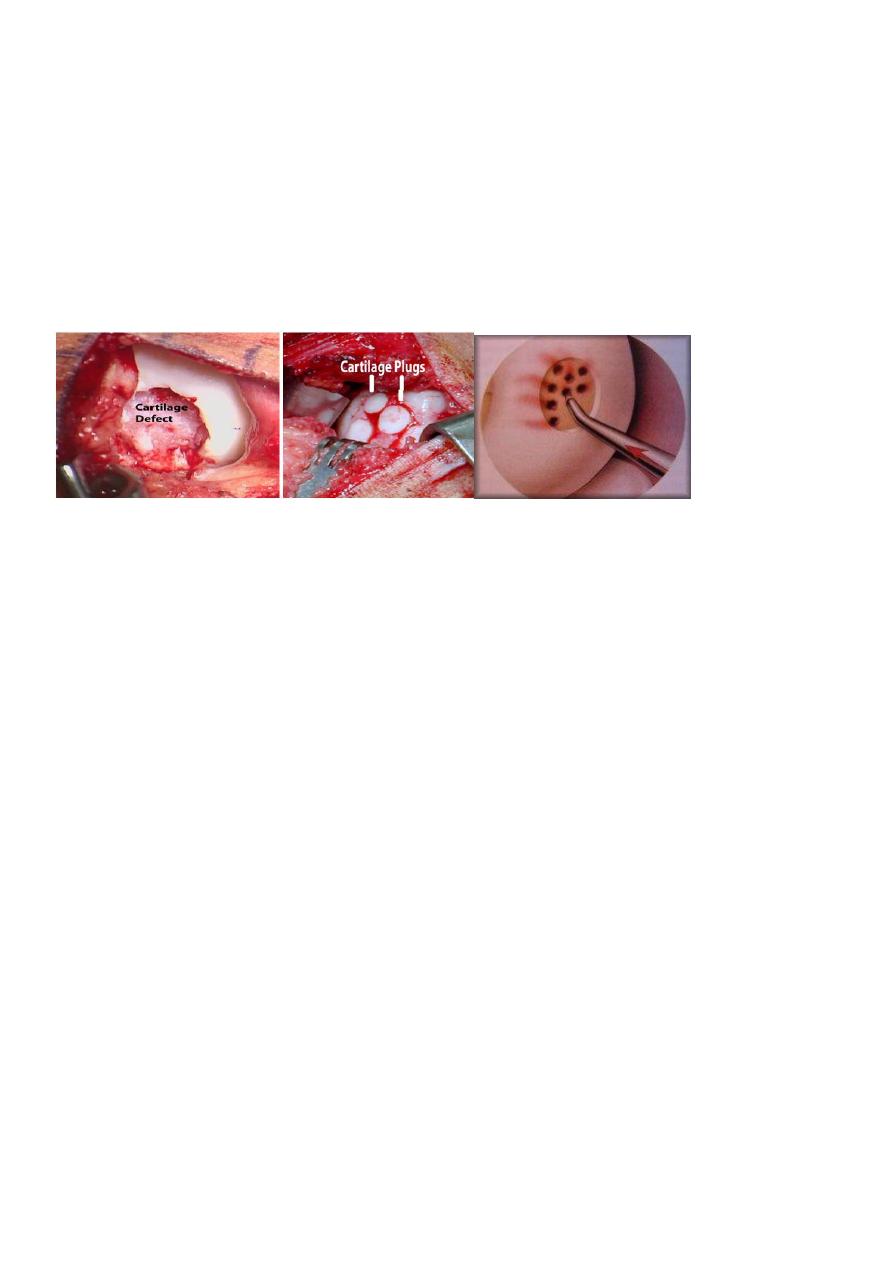
Recently
articular cartilage transplantation.
Loose bodies
A etiology:
Injury.
Osteochondritis dissecans.
OA.
Charcots' disease.
Synovial chondromatosis.
Clinical features
May be symptom less.
Usually complaint is attack of sudden locking without injury.
Patient may be aware of some thing popping in and out of the joint.
Loose body may be felt during palpation.
XR can detect the loose body
There might be underlying factors

4
Treatment:
Loose body causing symptom should remove by arthroscopy
The ankle and foot congenital deformities
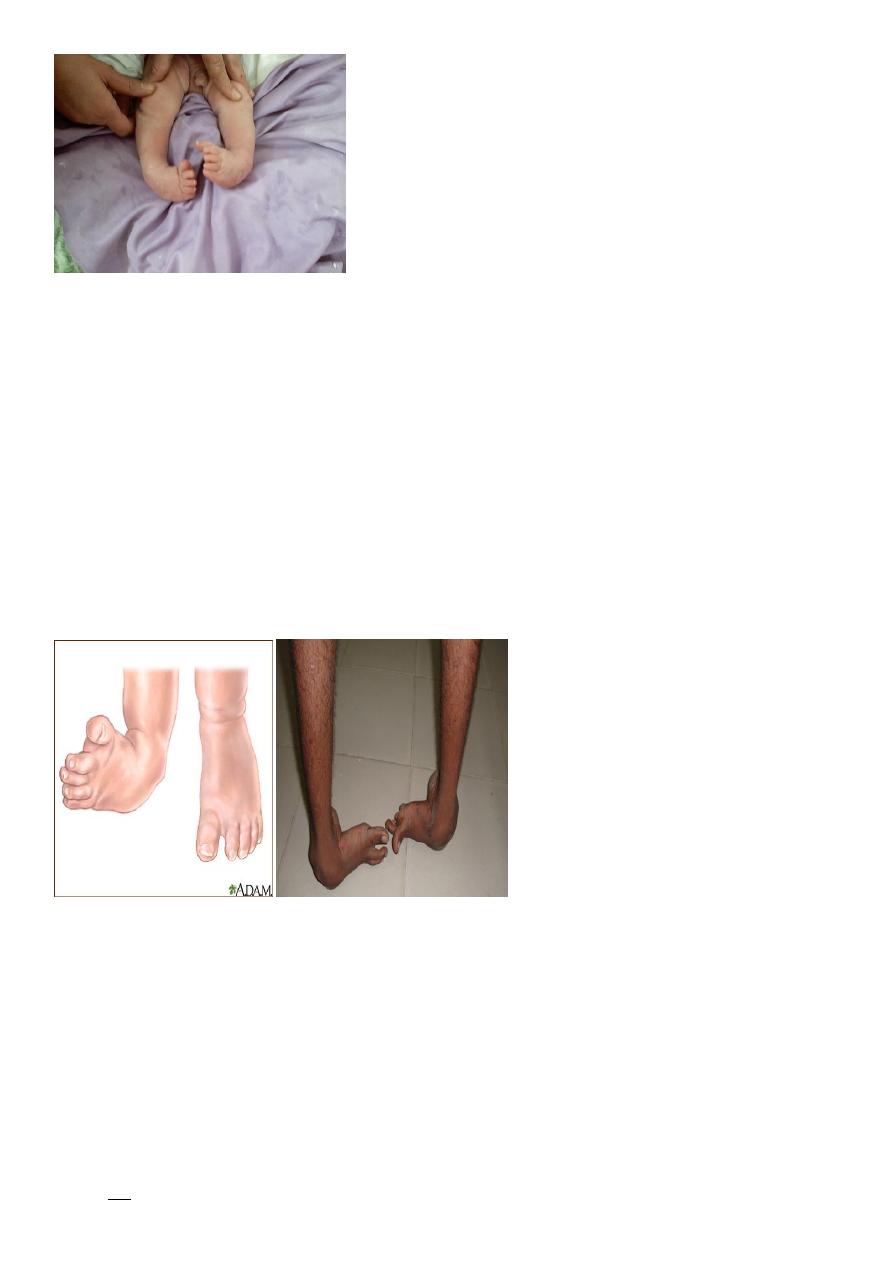
Talipes equinovarus
idiopathic club foot
Talipes is derived from talus
Pes foot
The heel is in equines .
hind foot in Varus mid foot .
forefoot adducted and supinated.
It is common 1-2 \1000 births
Male 2:1 female
1\3 is bilateral
5
A etiology:
Genetic.
arrested development.
neuromuscular disorder.
Clinical features:
At birth obvious deformity in which the foot is both turned and twisted so the sole
faces posteriomedial
Heel inverted
Forefoot adducted and supinated
Talus protrude on posteriolateral surface.
Heel small and high.
Deep creases appear medially.
Calf abnormal thin.
On examining foot movement dorsiflexion and eversion were resisted to varying
degree.
The infant must examined for other associated anomalies e.g. hip and spine disorder.
XR AP & Lateral
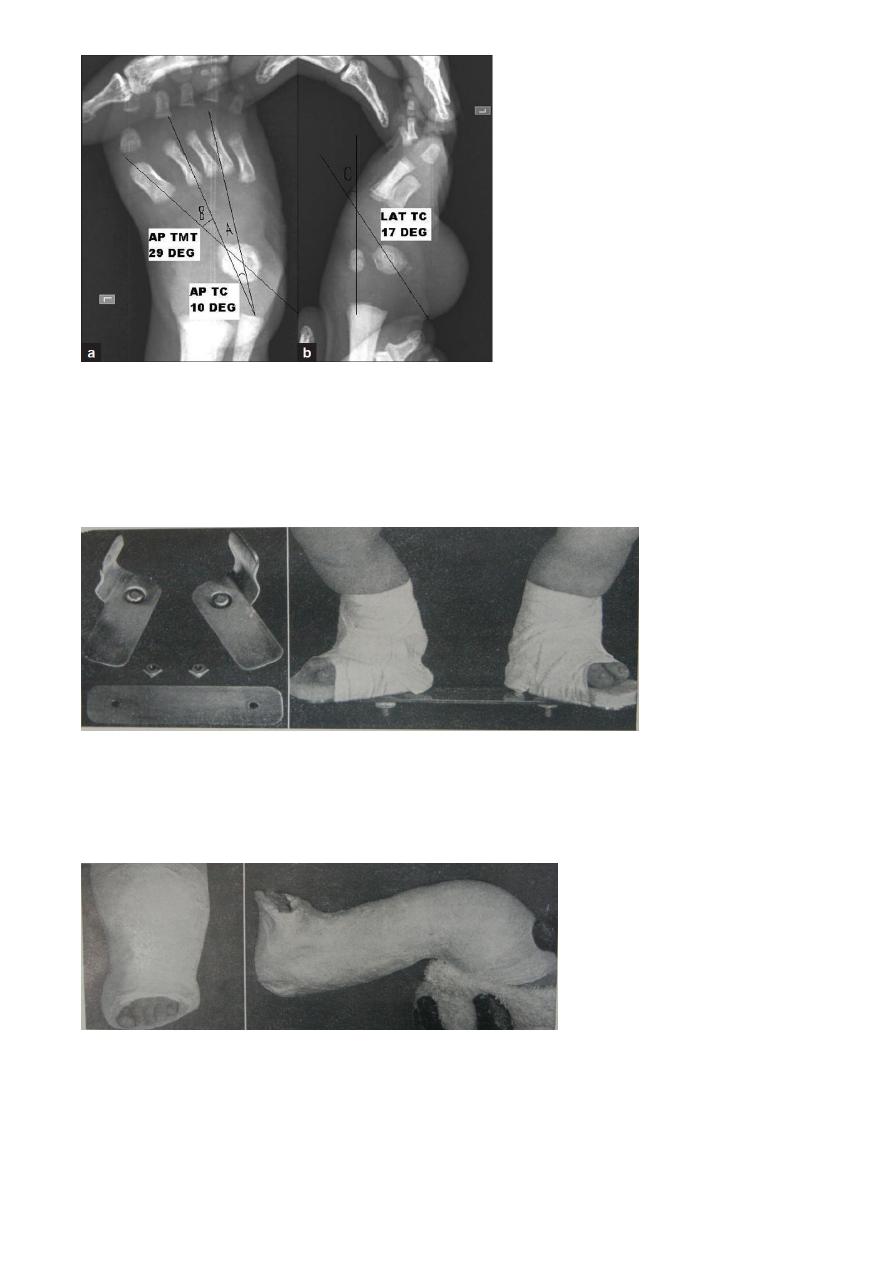
6
Rx:
conservative
1.1-2 day after delivery repeated manipulation and adhesive strapping by the relative
or physiotherapist.
2. Or pop
3. Conservative continue for 8-12 weeks (PONSENTI ) METHOD OF POP.
Either to continue or shift TO SURGERY
to surgery
Better until the child is near walking age
Soft tissue release.
7
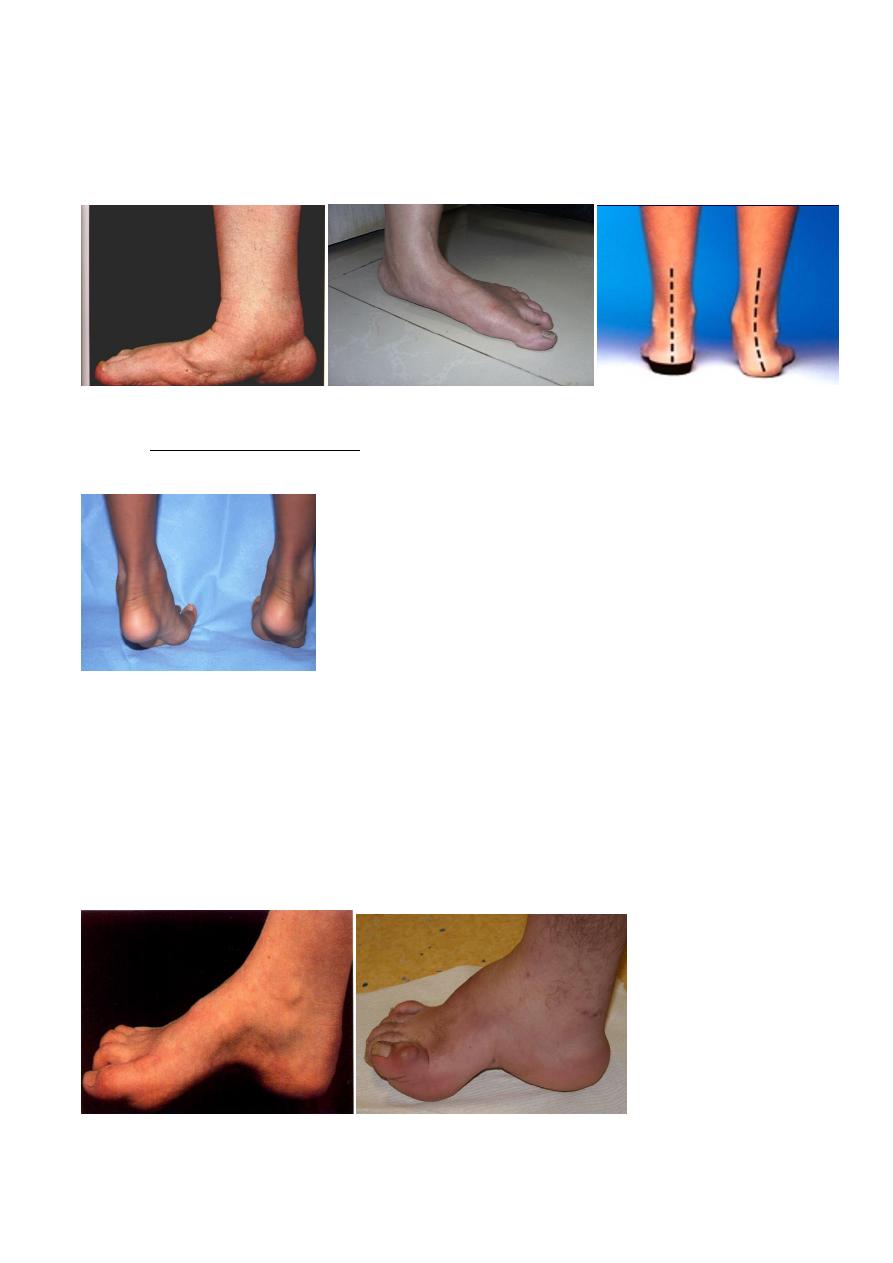
Flat foot:
The apex of the arch has collapsed and medial border if the foot is in contact or
nearly contact with the ground.
The heel become valgus and the foot pronated at subtalar –mid tarsal complex.
Flat foot may be flexible (the arch simply restored by sampling dorsiflexion of the great
toe, OR STANDING ON THE TOES Or might be rigid flat foot (deformity cannot corrected
passively. as in RA. (subtalar joint).
Rx : either conservative
Rx :Under lying cause.
Or Surgery.
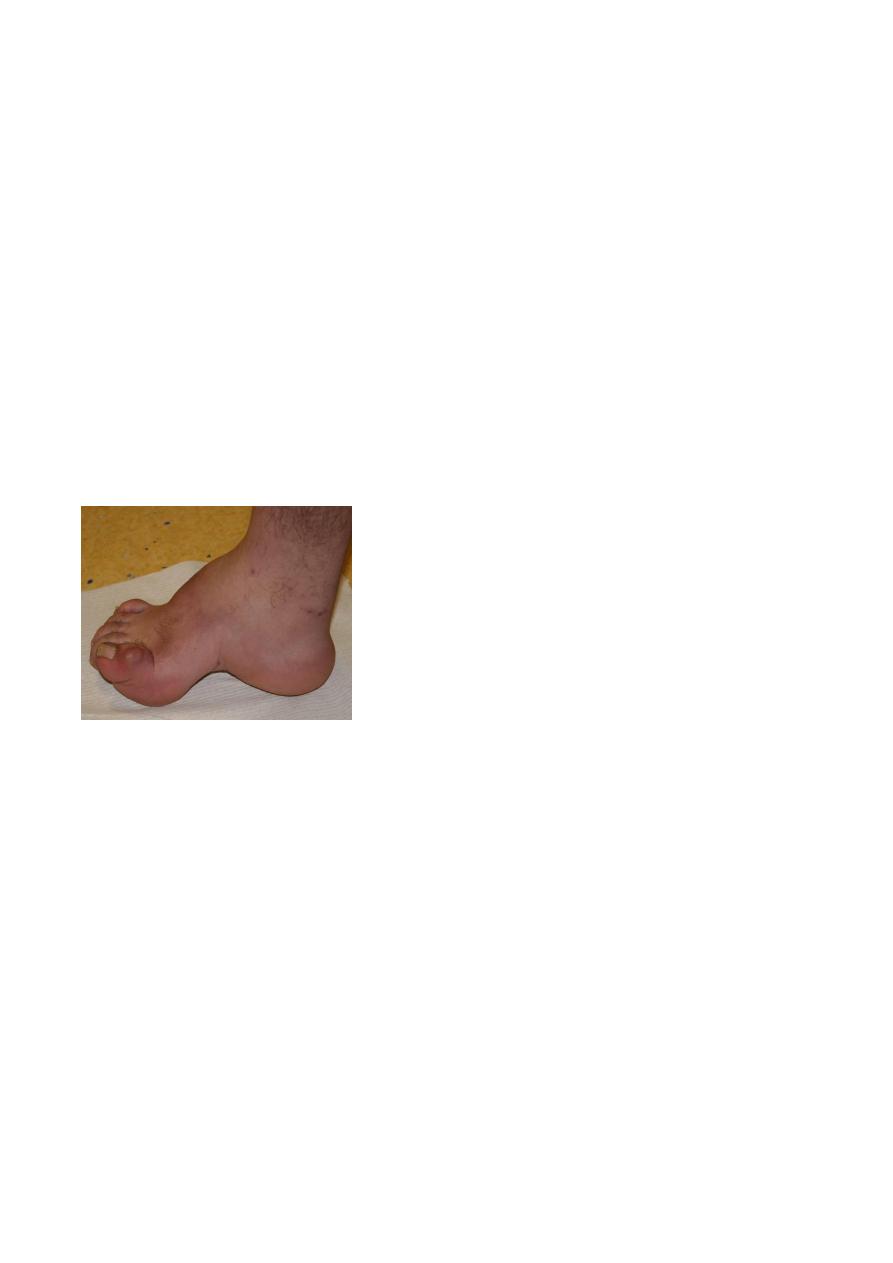
High –arched feet (pes cavus)
The arch is higher than normal and often there is also clawing of the toes.
8
Causes:
Neurological disorder
Congenital causes.
Acquired neuromuscular disorder
Miscellaneous (trauma, burn, compartment syndrome)
Clinical features
8-10 years at school
there might be family history a spinal disorder.
Pain at metatarsal head
Callosities.
Examination
deformity obvious Over flexion at IP joint. Hyperextension at MP joint. Drop metatarsal
head
High arch mid foot
Neurological examinations important
XR different measurements.
Treatment
Often no rx , If symptom present surgery is recommended (bony soft tissue or tendon
transfer ).
Hallux valgus
H V is the commonest of the foot deformities and probably of the musculoskeletal
deformities ,in which the Angulation of the big toe is excessive .

9
A etiology:
Metatarsus primus.
Elderly people with loss of the muscle tone.
RA
Positive family history in
60
%
Clinical features:
Most common in women 50-70
Bilateral
In those appear in adolescence has strong familial tendency
No symptom apart from deformity.
Some time pain due to either pressure shoe
Metatarsalgia.
deformity lesser toes.
OA 1
st
metatarsal joint.
Deformity obvious, bunion swollen.
Forefoot is too wide
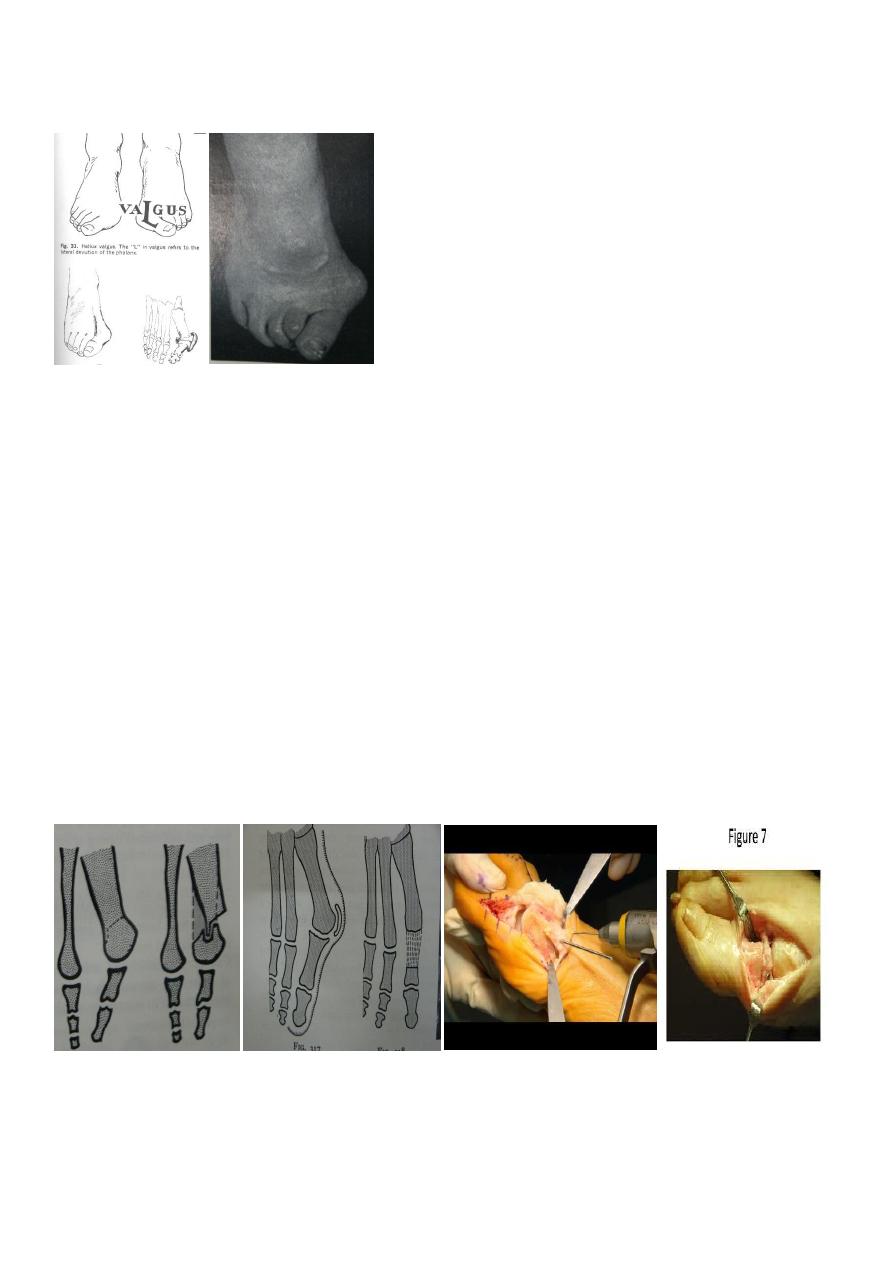
11
Great toe valgus position.
2nd toe is crowded and hammer toe deformities are common
old shoes will show the traces of long standing pressure.
Good range of joint movement
XR to measure the degree between the first and 2nd metatarsals.
Treatment:
Adolescents
(conservative by proper shoe).
If failure with frank deformity surgery is indicated.
By different osteotomy.
Adult:
Surgery by different osteotomy
Exscion arthroplasty.
Painful feet
My feet are killing me This is
common complaint
Pain due to
11
mechanical pressure (deformed foot)
joint inflammation
a localized bone lesion
peripheral ischemia.
Muscular strain
May be part of general disorder (diabetes).
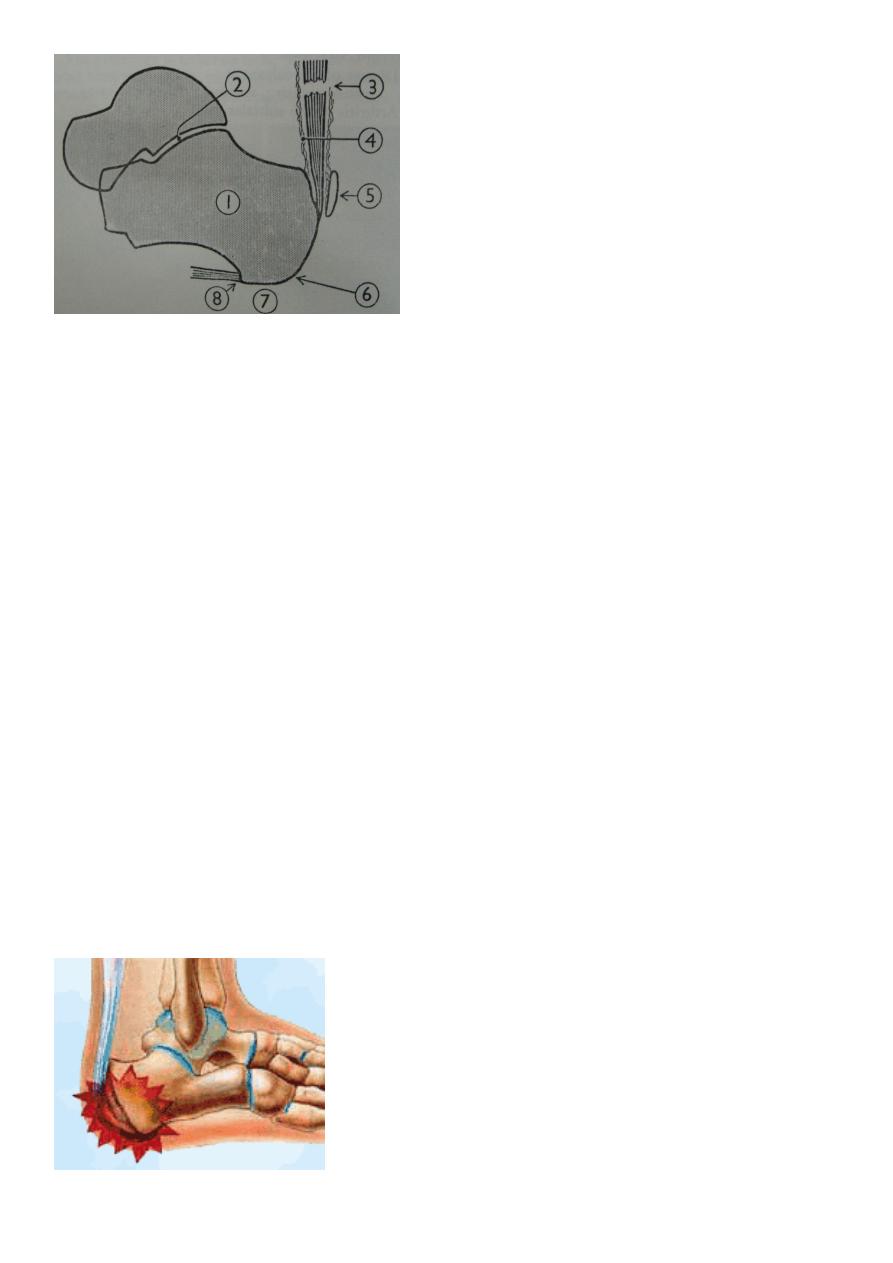
Posterior heel pain
Sever's disease
Calcaneal bursitis
Plantar fascitis
Painful fat pad
Nerve entrapment.
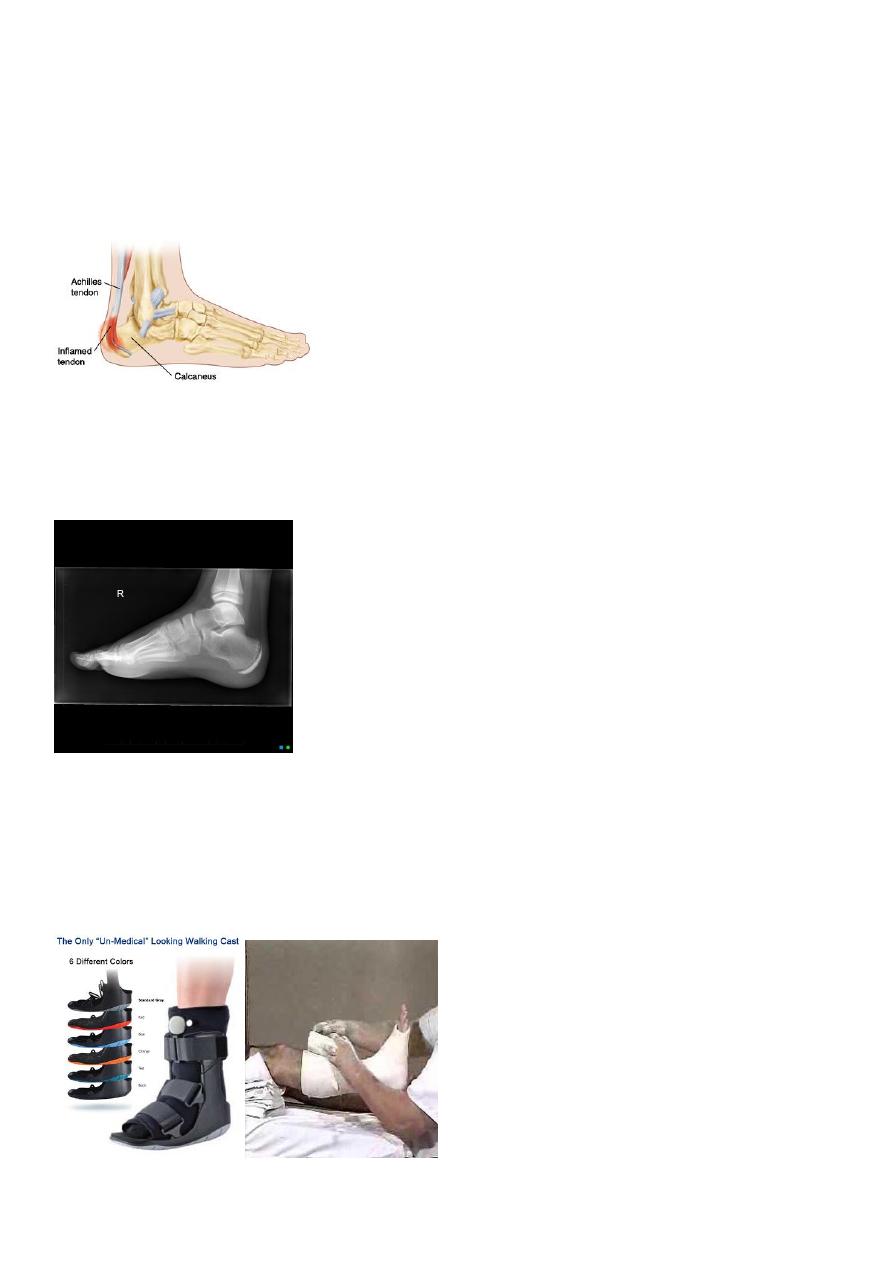
Sever's disease
Harmless condition ocur in children ,during active period of growth.
Now it is consider as strain at the attachment of the posterior apophysis of
calcaneum.from pull of achilles tendon
12
Clinical features
Age 8-13 years.
Pain behind the heal, slight limping.
O/E tenderness over the lower part of the tuberosity.
Radiographs
Usually fail to show any alteration.
Sometimes show fragmentation of the calcaneal apophysis.
Treatment
Most cases not required.
It is gardually subside.
If in pain few weeks below –knee walking plaster
13
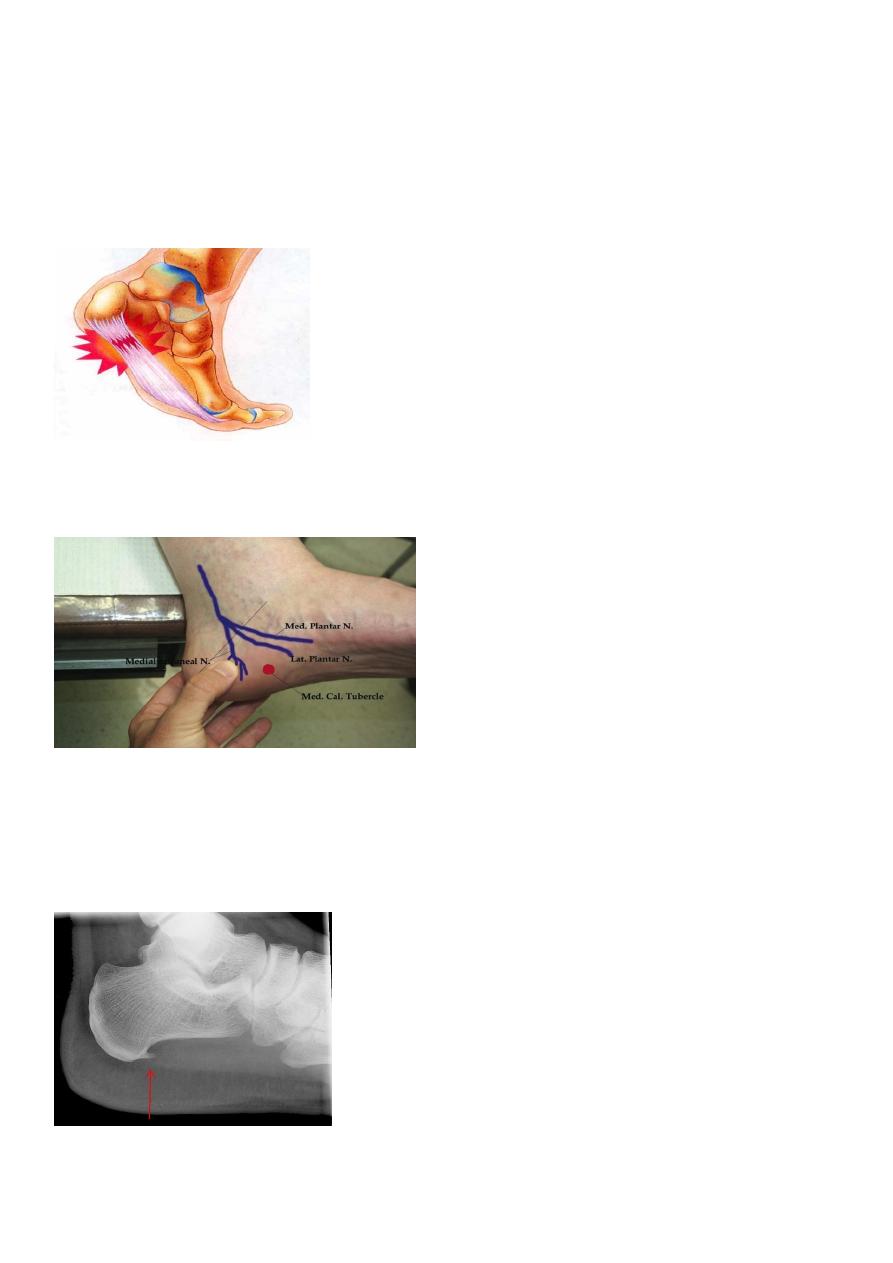
Plantar fasciitis
believed to be inflammatory, there is pain in the anterior part of the calcaneus.
Clinical features.
The complaint is of pain beneath the heel on or walking; the pain extends medially and
into the sole
On examination
tenderness over the site of attachment of the plantar fascia to the calcaneus
Radiographs
usually do not show any abnormality.
A sharp spur projecting forwards from the tuberosity of the calcaneus is sometimes
found.

14
Treatment.
Conservative treatment
: message
Rolling pin excercise
The heel should be protected by a resilient cushion on an insole.
Anti inflamatory drugs
If fail go to Local injection corticosteroid
Pain over mid foot Kohler disease.
15
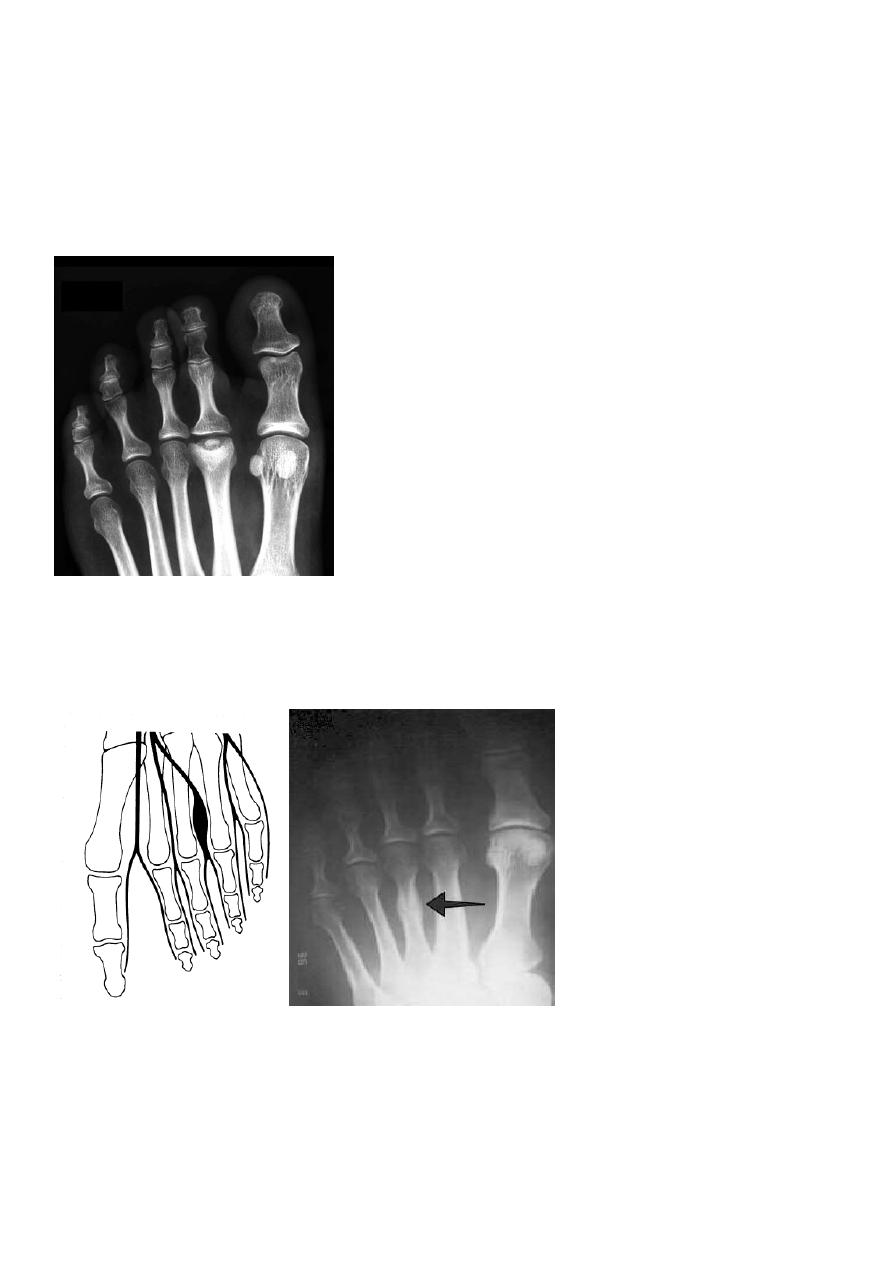
Pain in the forefoot
Metatarsalgia (flattening metatarsal arch).
RA in MP joint
Sesamoiditis.
Freiberg's disease (crushing type of Osteochondritis of 2nd metatarsal head)
Stress fracture (2nd 3rd metatarsal )
Interdigital nerve compression
Tarsal tunnel syndrome.