
1
Fifth stage
Surgery-Ortho
Lec-4
.د
يقضان
29/11/2015
BONE INFECTION
micro-organism may reach the bone and joint either directly through a break in the skin e.g.
. Wound, pinprick, open fracture . Or indirectly through blood stream from distant site any
source of infection in the body .
According to the type of micro-organism, site of infection and host response the result may
be pyogenic osteomyelitis,arthritis, chronic granulomatus reaction e.g. T.B , fungal infection
or parasitic infestation.e.g.hydatid .
INFECTION :is a condition in which pathogenic M.O. multiply and spread within the body
tissue , this will give rise to acute or chronic inflammatory reaction which is the body way of
defense to kill the M.O. the sign of inflammation are redness, swelling , heat , pain and loss
of function
ACUTE HAEMATOGENOUS OSTEOMYELITIS
It is almost a disease of children ; if it affect adult it may be due to low resistance for any
cause .
Trauma may predispose to this disease by heamatoma or fluid collection in the bone .
The causal M.O. is usually staph. Aureus , less often strepto coccal pyogen or pnemonae .
In children under 4 years haemophilous inflauanzae is common .
E.Coli , proteus , pseudomonas seen in heroin addict .
Patients with sickle cell disease are prone to infection by salmonella
Pathogenesis
The M.O. is blood born , it come from any source of infection any where in the body,inter
the bone via the nutrient artery and reach the metaphysis where infection start , lead to
pus formation which escape outside the cortex to become under the periosteum lead to
periosteial reaction and new bone formation(envolicurum) , then the pus escape through
the clawaka to open to the skin as a discharging sinus .
The dead bone called sequestrum .
2
Pathology
Five steps
1- inflammation .
2- suppuration .
3- necrosis .
4- reactive bone formation .
5- resolution .
Clinically
The pt. is usually a child presented with sever pain , malaise , loss of function of the limb
and fever .
In neglected cases the child is dehydrated toxic and in advanced neglected cases the child
may presented with septicemia (septic shock)
3
On examination
The pt. look acutely ill feverish , dehydrated , pulse rate above 100 b/min .
Local ex. : acute tenderness near one of the large joint , even gentle manipulation is painful
, joint movements is restricted .
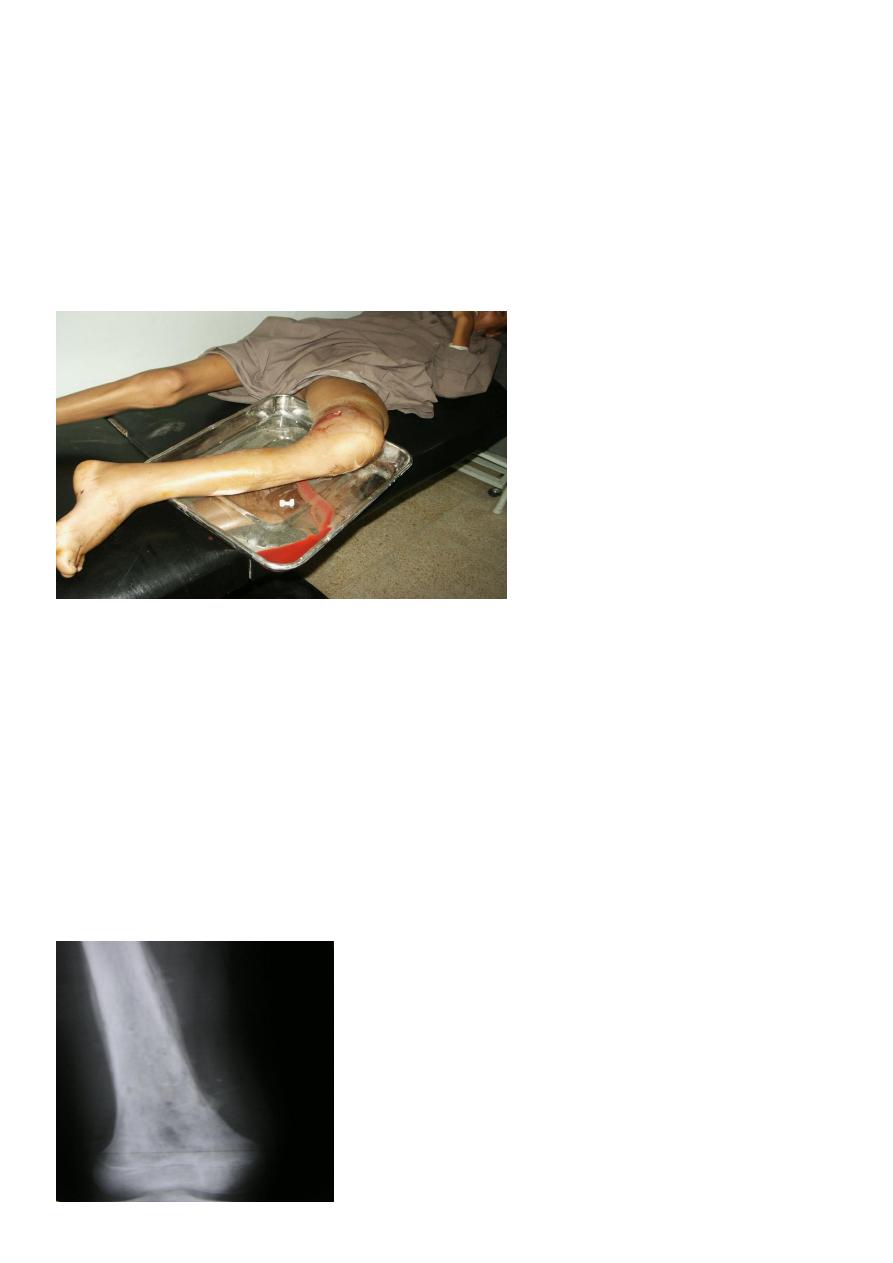
Later on redness , swelling , hotness will be present and these signify that pus is escape
from the bone to the soft tissue .
If antibiotic is given , these signs will be modified
Investigation
X-RAY :
It is normal during the first 10 days apart from soft tissue swelling .
At the end of the 2
nd
week there will be periosteal reaction ; later on the periosteal reaction
become more thick (new bone) .
Areas of cortical destruction shown as osteolytic lesion ( black lesions) mainly in the
metaphysis it is called moth eaten lesions .
Late sign is patches of rarefaction(area of decrease density) and patches of increase density
.

4
ULTRASOUND : it may detect subperiosteal collection of fluid in the early stage of the
disease .
RADIO SCINTIGRAPHY(BONE SCAN) :
Tc99 , Ga67 , In 111 show increase perfusion phase and bone phase in early stage of the
disease .
MRI : it is extremely sensitive
Blood investigations :
C.B.P and ESR :show increase ESR , increase wbc count (mainly polymorph) .
C – reactive protein increase .
Blood culture is positive in 50% of the cases .
Anti staphylococcal anti body titer may be increased .
Aspiration by needle (most certain)
Differential diagnosis
1- cellulitis .
2- acute suppurative arthritis .
3- acute rheumatism .
4- sickle cell crises .
Treatment
In osteomyelitis fluid(pus)and blood are taken from the patient for culture and sensitivity
before any drug is administered and then the treatment is started immediately .
Four important aspect of the treatment :
A- supportive treatment for pain and dehydration .
B- splintage of the affected limb .
C- antibiotic .
D- surgical drainage .
Antibiotics
Immediately started after aspiration of blood and fluid for culture and sensitivity .
5
For staph. Aureus : flucloxaciliine and fucidic acid are used .
In children before 4 years old when heamophilous inflauanzae is suspected ,
cephalosporine is indicated .
Pt. with sickle cell disease when salmonilla is suspected , chloramphinicol , cotrimoxazol ,
amoxil with clavulonic acid (amoxyclave) is indicated
I.V. antibiotic should be continued until c-reactive protein return to normal level (usually
take 1-2 weeks) , and then change to oral antibiotic for 3-6 weeks .
Surgical drainage : if after 36 hours of conservative treatment there is no improvement and
there is sign of pus collection , then it should be drained .
Rehabilitation
Once the infection is subside , movement is encouraged and the child is allowed to walk
with aid of crutches .
Full weight bearing is allowed after 3-4 weeks
Complication
1- metastasis of infection locally and systemically .
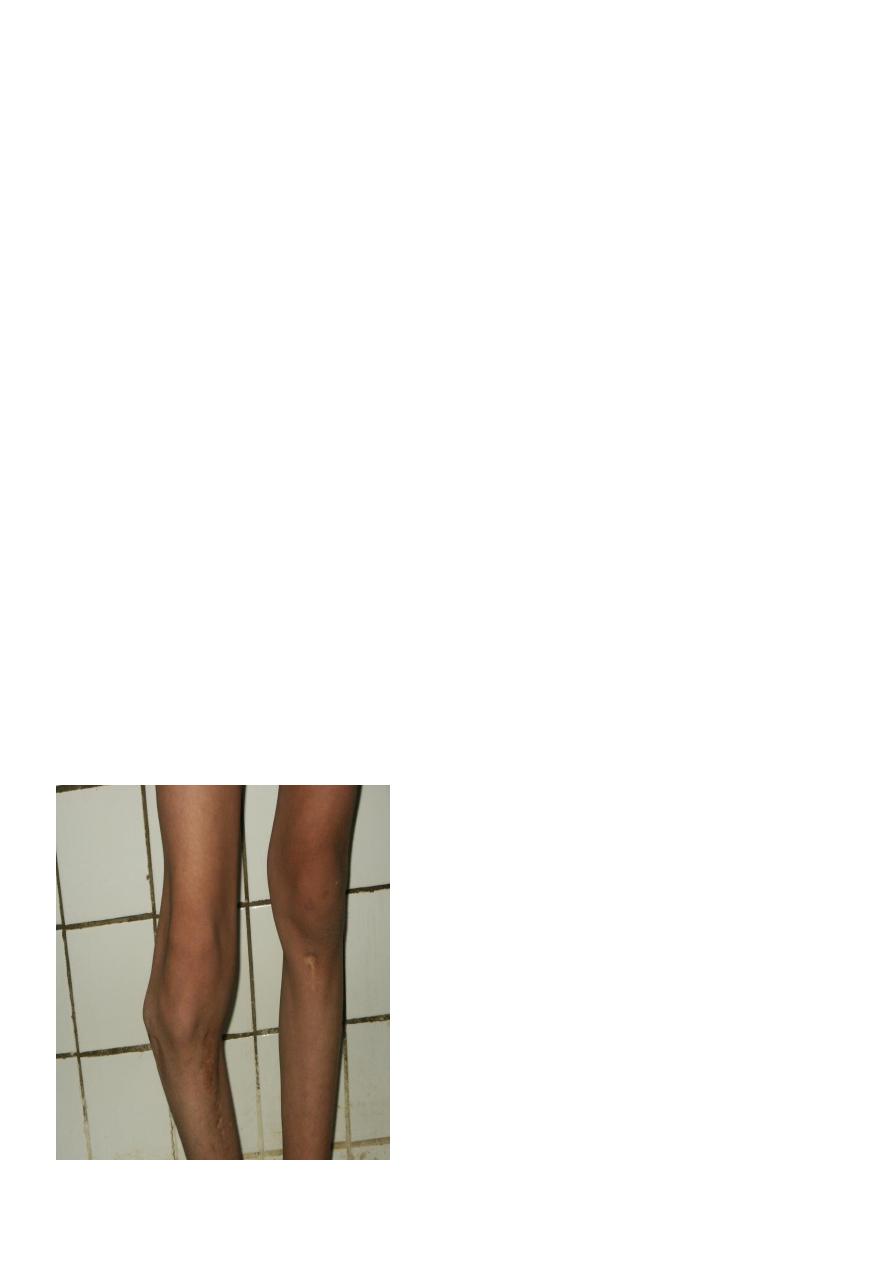
2- altered bone growth (due to damage to the growth plate of the bone) e.g. varus
deformity of the knee (genu varum)
3- chronic osteomyelitis .
Genu varum deformity late complication of acute osteomyelitis

6
Sub acute osteomyelitis
Metaphyseal osteolytic lesion surrounded by area of sclerosis called (brodies absces) .
The patient usually has long standing pain , swelling , local tenderness , but no fever
Sclerosing osteomyelitis of Garrie’s
Non suppurative sclerosing osteomyelitis affecting young adult .
Patient has chronic pain .
X-ray show increase bone density .
Treatment : by excision of the sclerosed bone