1
4th stage
Surgery
Lec-1
Dr.Ahmed
16/4/2016
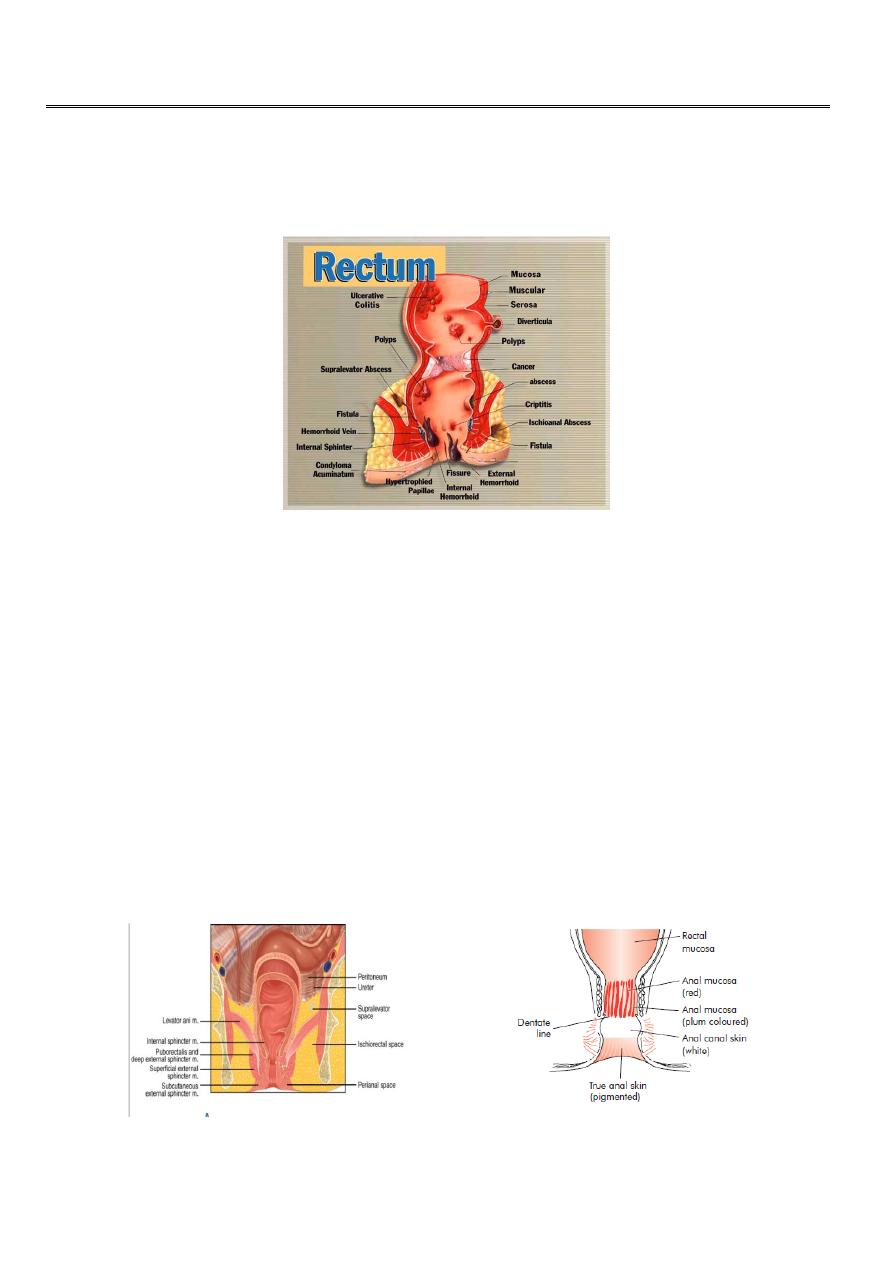
Anal conditions
Anorectal diseases :
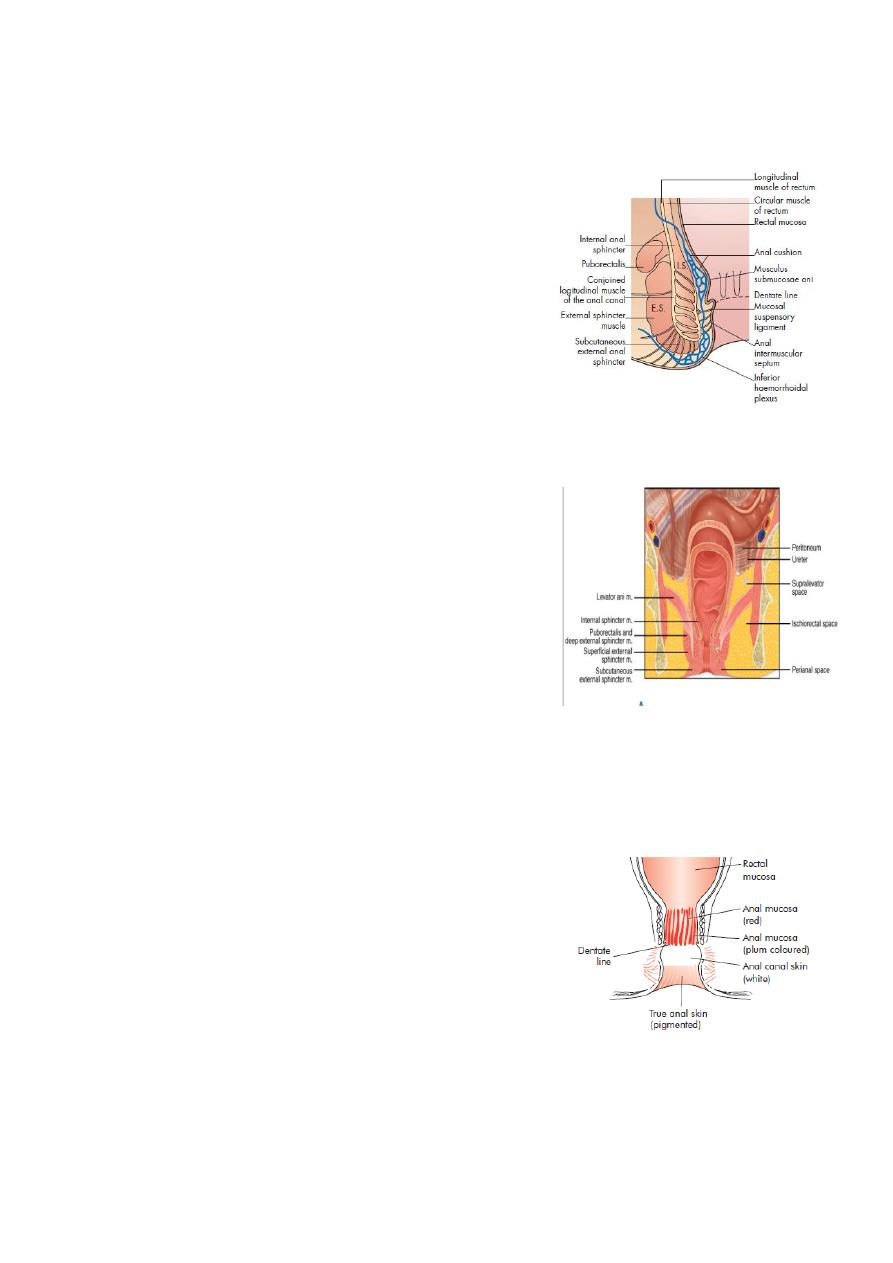
Surgical anatomy of the anal canal :
Terminal part of G.I.T.
3-4 cm in length.
The anal canal commences at the level where the rectum passes through the pelvic
diaphragm and ends at the anal verge.
The muscular junction between the rectum and anal canal can be felt clearly with the
finger as a thickened ridge the anorectal bundle or ‘ring’ especially on its posterior
and lateral aspects.
Division of the anorectal ring results in permanent incontinence of faeces like in case
of surgery for high anal fistula.
2
The anal canal continues downwards and backwards surrounded by three concentric
cylinders of muscles,
these are the internal and external sphincters, with the thin longitudinal muscle layer
between them.
On either side of the anal canal there is the fat filled space named the ischiorectal
fossa.
The Dentate line :
important landmark surgically it separates
:
Above
• columnar epithelium;
•autonomic nerves (insensitive);
•portal venous system;
Below
•from squamous epithelium;
•from spinal nerves (very sensitive);
•from systemic venous system.

3
Anal canal lining:-
Above dentate line lined by columnar epithelium.
Below dentate line lined by squmous epith.
Arterial supply:-
Superior haemorrhoidal A.from inferior mesenteric A.
Middle haemorrhoidal a. from int. iliac A.
Inferior haemorrhoidal a. from int. iliac A.
Venous drainage:-
The superior and middle haemorrhoidal veins drains the upper half of the anal canal
& they drain via the inferior mesenteric vein into the portal system.
The inferior haemorrhoidal veins drain the lower half of the anal canal and the
subcutaneous perianal veins:
they eventually join the external iliac vein on each side.
Lymphatic drainage:-
Above dentate line to para aortic lymph nodes.
Below dentate line to inguinal lymph node.
The Anal Glands :
Found in the submucosa and intersphincteric space,number up to10 .
Their function is unknown although they secrete mucin which perhaps lubricates the
anal canal to ease defecation.
The importance of intersphincteric anal glands is that they are widely considered to
be the potential source of anal sepsis, either acute, presenting as perianal,
ischiorectal or pelvic sepsis, or chronic, presenting as a cryptoglandular (non-specific)
anal fistula.

4
Examination of the anus :
The examining couch should be of sufficient height to allow easy inspection and
access for any necessary maneuvers.
A good light is mandatory.
The Sims (left lateral) or the lithotomy position is satisfactory, the lithotomy is less
convenient for an elderly patient and can cause social embarrassment to young
women.
A protective glove should be worn.
The patient should be relaxed and able to cooperate.
A few quiet words from the doctor can prevent many loudones from the patient.
Inspection :
With the buttocks opened, the anus is inspected.
The patient is asked to strain down before inspection is concluded.
inspect any lesions, e.g. inflammatory skin changes, haemorrhoids, fissure(‘sentinel
pile’) or fistula.
Digital Examination With Index Finger :
A good lubricant is necessary neither too little nor too much.
Any secretions should be sampled before applying lubricant to the anal verge.
Extreme gentleness should be the rule so that pain is not caused.
Painful spasm of the anal sphincters is confirmation of a hidden fissure if the history
is suggestive.
The examination check normal, and abnormal, structures as follows:
Intraluminal:
normal: faeces.
abnormal: polyp or carcinoma.
Intramural:
normal: sphincter muscles and anorectal angle.
abnormal: carcinoma .
Extramural:
normal: perianal structures.
abnormal: abscess.
Before withdrawing the finger, the patients asked again to strain down, and a note is
made regarding the prostate in a male patient and the cervix, uterus and pouch of
Douglas in a female.
5
Discharge
After withdrawal, the finger is examined for mucus, pus, blood and abnormal fecal
material.
Proctoscopy :
This examination is of great importance.
Either the Sims position with the buttocks elevated on a small cushion, or the knee-
elbow position may be used.
The lower third of the rectum, the anorectal junction and the anal canal can be
inspected as the instrument is withdrawn slowly.
Minor procedures can be carried out through this instrument, e.g. treatment of
haemorrhoids by injection or banding and biopsy.
Sigmoidoscopy :
This examination of the rectum and lower sigmoid colon, should be carried out even
when an anal lesion has been confirmed.
Rectal pathology, e.g. colitis or carcinoma, is frequently the cause of an anal lesion,
e.g. fissure or hemorrhoids.
Not infrequently, rectal pathology is found that is independent of the anal lesion and
which requires treatment.
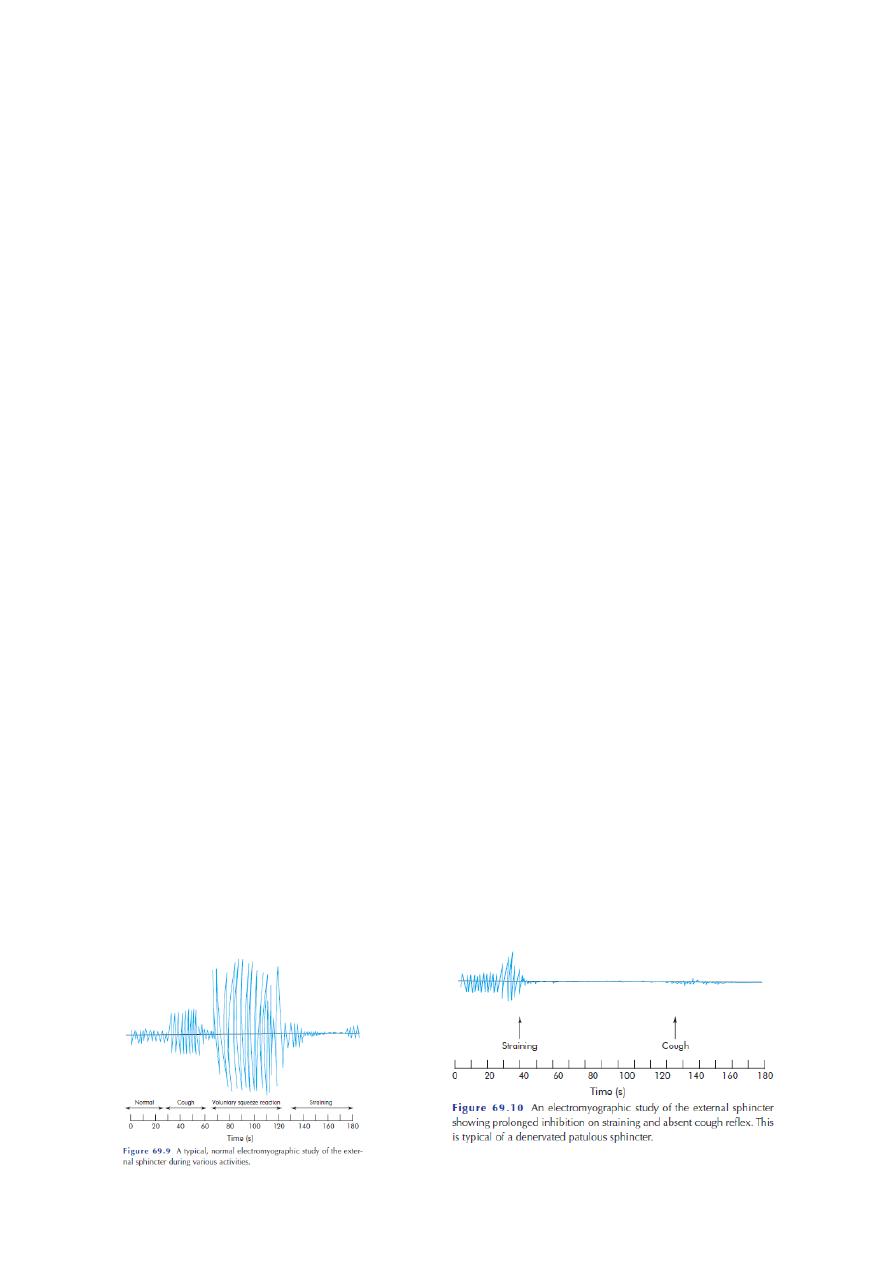
Special Investigation :
Manometry
Proctography
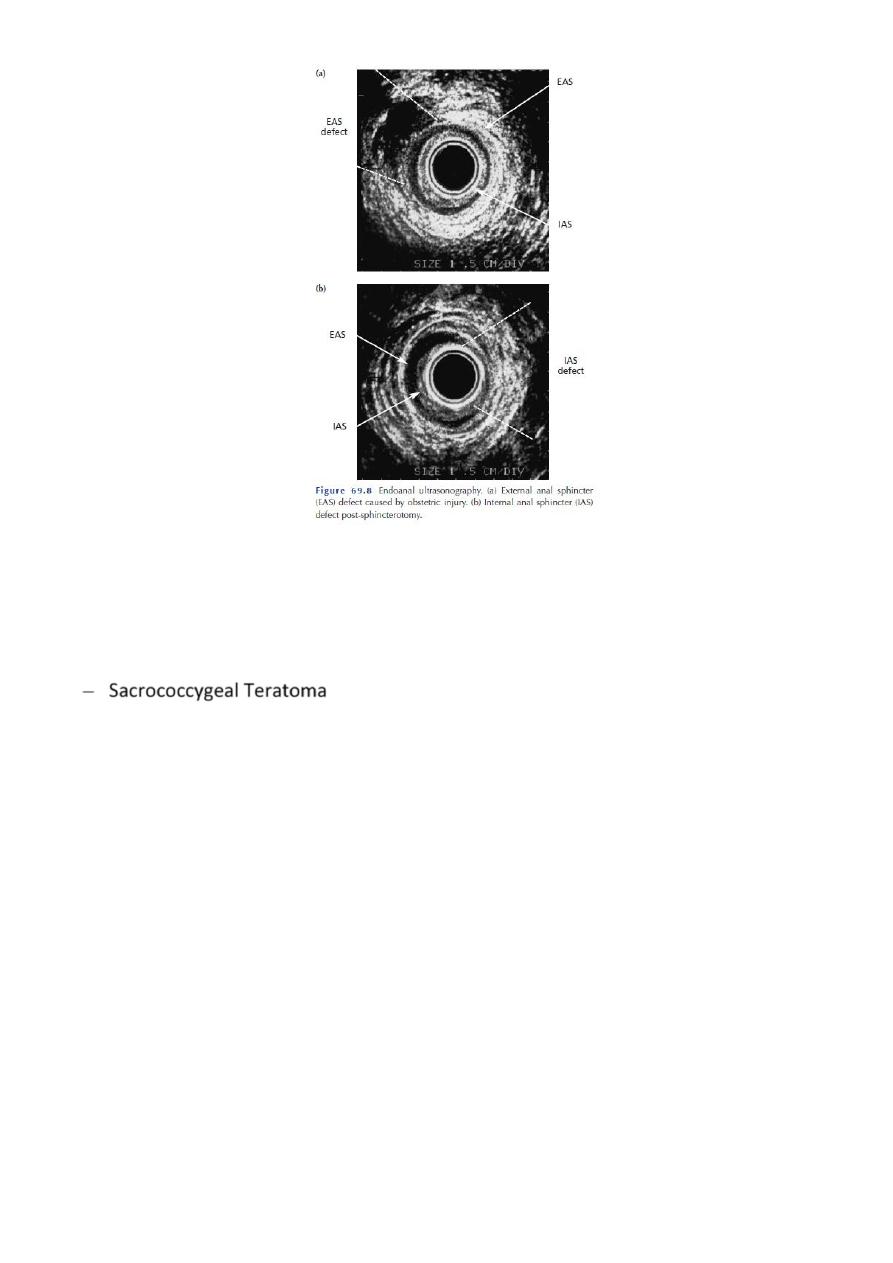
Endoluminal ultrasound
6
Congenital Abnormalities :
Imperforate anus
Sacrococcygeal Teratoma
Post anal Dermoid
Post-anal Dimple
…