1
Forth stage
surgery
Lec-7
د. سمير الصفار
27/10/2015
Abdominal Wall Hernia
Definition
A protrusion of a viscus or part of a viscus through an abnormal opening in the walls
of its containing cavity
Introduction:
Hernias by themselves usually are harmless, but nearly all have a potential risk of
Obstruction if their content is part of bowel.
Cut off blood supply of their content ( becoming strangulated).
Aetiology
Acquired:
Any condition that increase intra-abdominal pressure;
Strong muscular effort
Chronic coughing
Straining
Obesity
Chronic smoking
Congenital:
Patent processus vaginalis

2
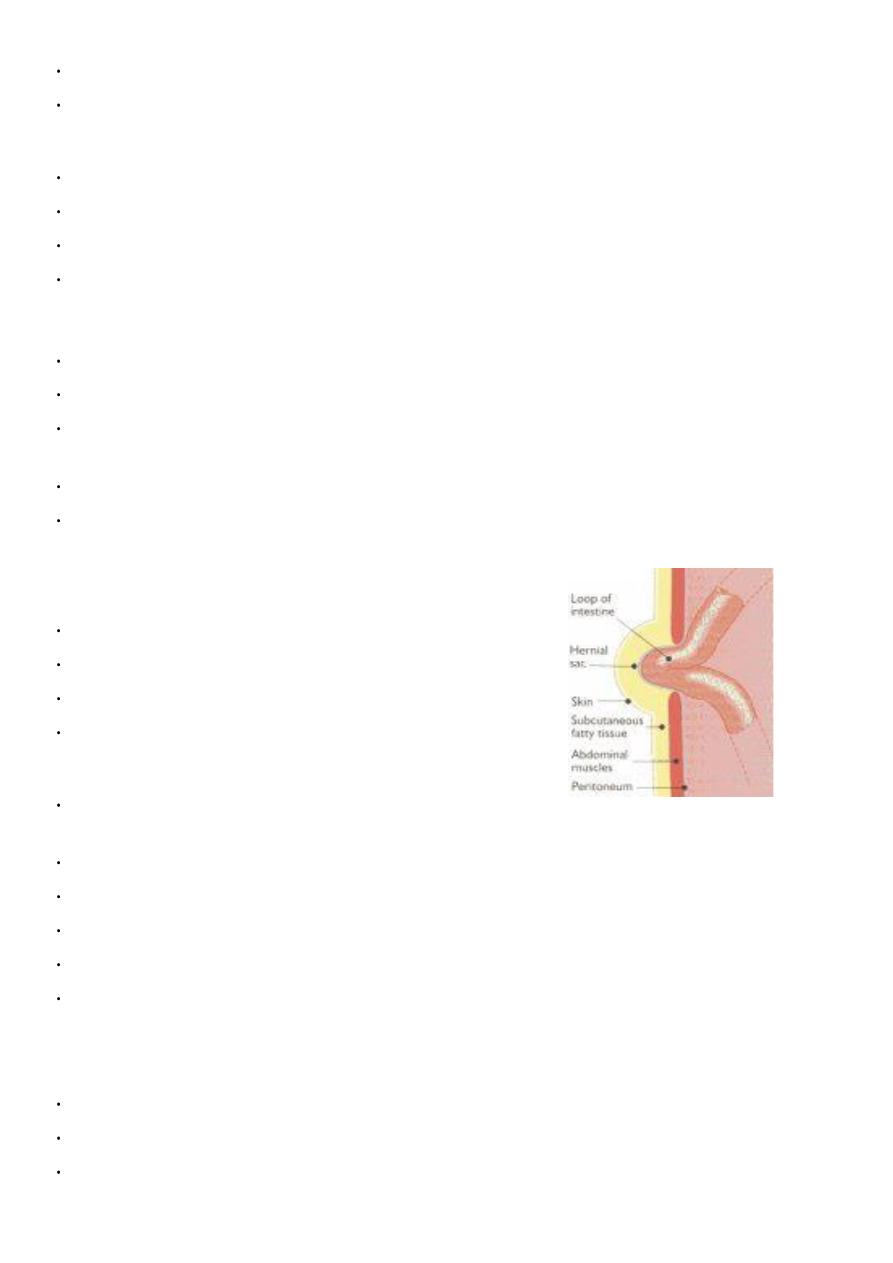
Composition of hernia
Each Hernia consist of
Defect or weak point
Peritoneal sac
Mouth
Neck
Body
Fundus
Covering of the sac
Contents of the sac
Contents of the sac
Omentum
Intestine
Portion of circumference of intestine “Richter “
Portion of bladder
Ovary with or without Fallopian tube
Meckel’s diverticulum “Littre “
Fluid
Anatomical types:
External
Interparietal
Internal
Sliding
Pathological Types :
Reducible
Irreducible
Obstructed ( Incarcerated )
Strangulated
Inflamed
3
Reducible
The hernia either reduces itself when the patient lies down, or can be reduced by the
patient or the surgeon
.
Irreducible
Here the contents cannot be returned to the abdomen, but there is no evidence of
other complications
.
Obstructed
This is an irreducible hernia containing an intestine which is obstructed but there is
no interference of blood supply to the bowel.
Strangulated
A hernia becomes strangulated when the blood supply of its contents seriously
impaired rendering the contents ischaemic.
Inflamed
•
Inflammation of its contents
Appendix
Fallopian tube
• Inflammation of overlying wall
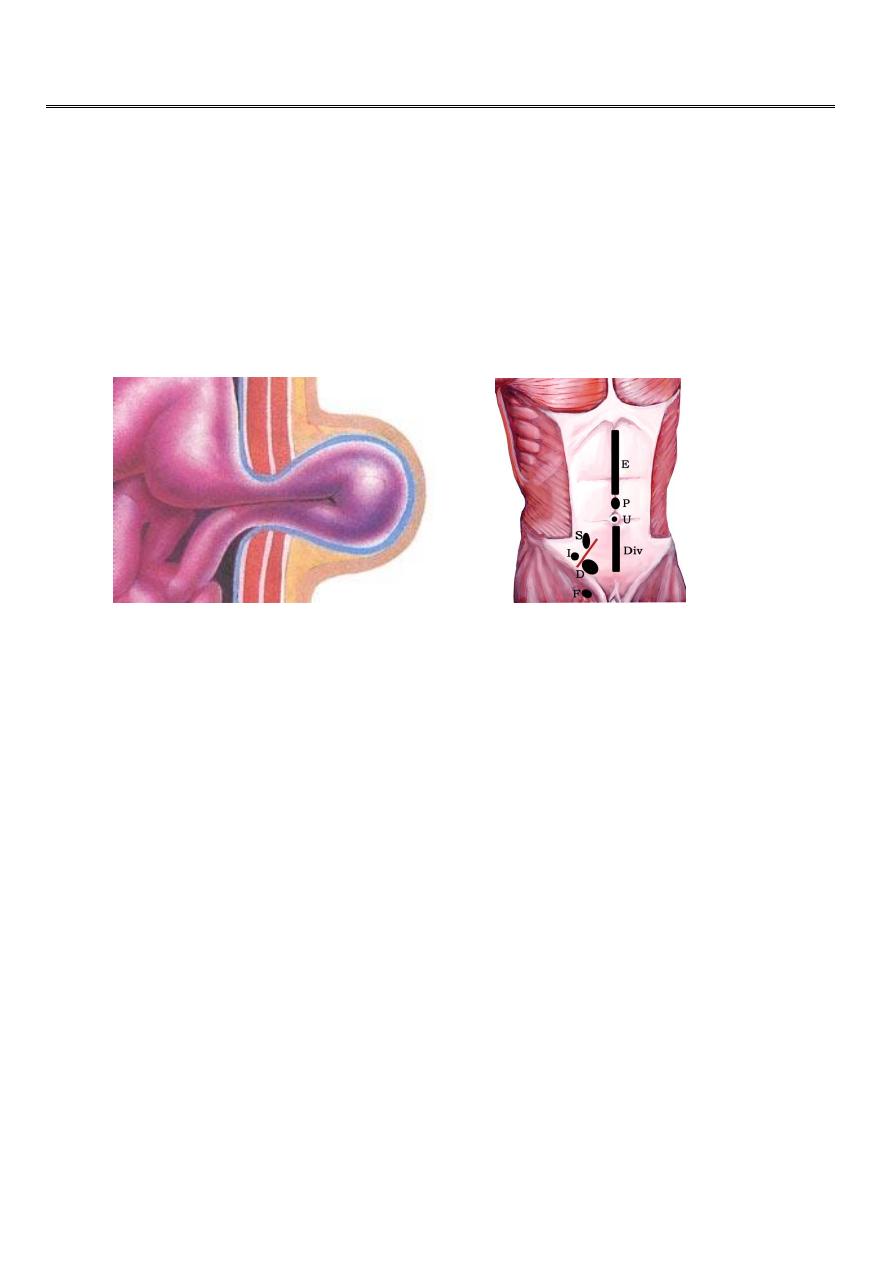
Locational Types:
• Groin
• Umbilicus
• Epigastric (Linea alba )
• Surgical incisions
• Spigelian (Semi-lunar line)
• Diaphragm
• Lumbar triangles
• Pelvis (Obturator)
4
Groin hernia
• Inguinal
• Femoral
Inguinal Hernia
Inguinal hernia : Makes up 75% of all abdominal wall hernias and occurring up to 25 times
more often in men than women.
• Indirect
• Direct
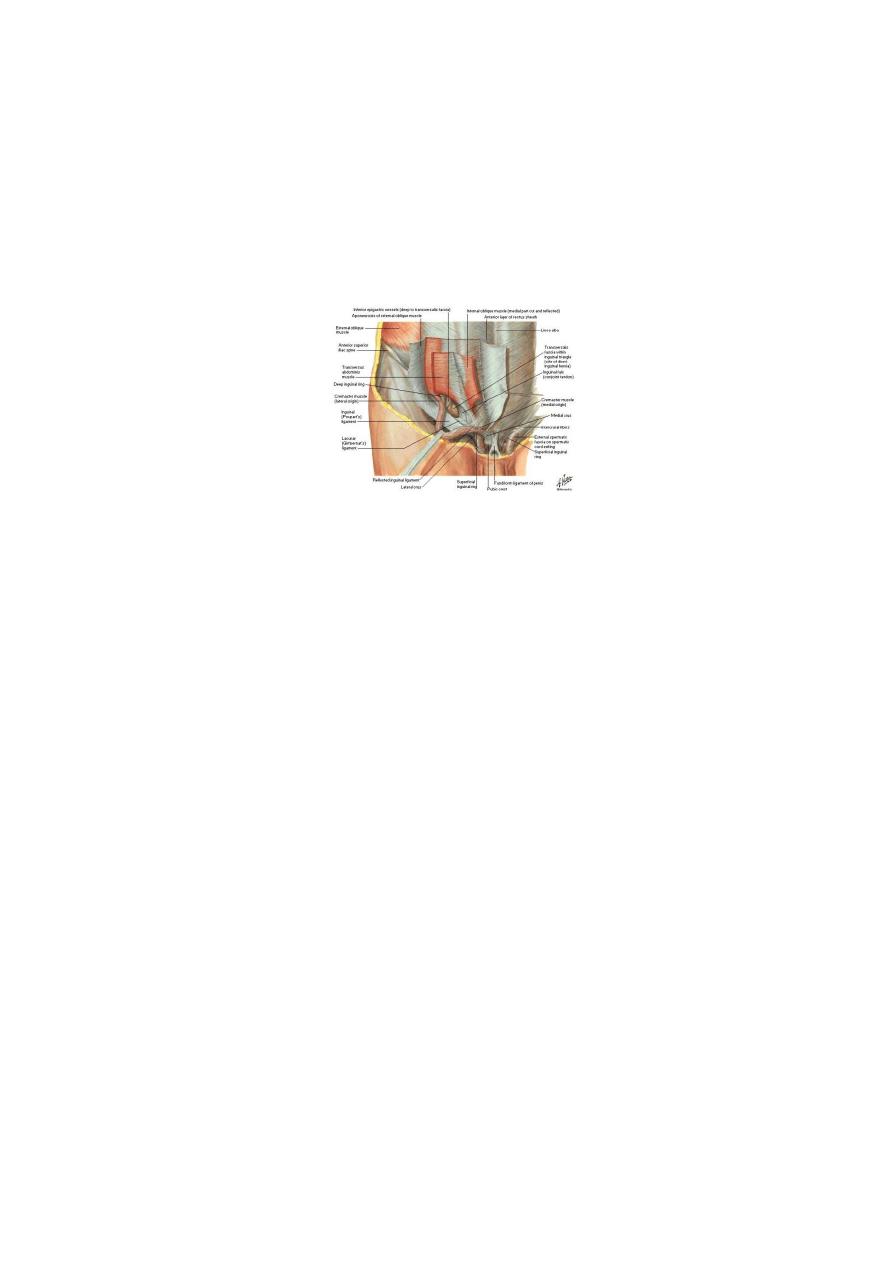
Anatomy of Inguinal Canal
• 3.75cm in length
• 1.25 cm cephalad and parallel to inguinal ligament
• Extends from deep to superficial inguinal rings
• In infants; the canal is almost not present as the DIR and SIR superimposed
Boundaries of Inguinal Canal
• Anterior EOA, CT
• Posterior C, TF
• Upper (roof) CT
• Lower (floor) IL
Anatomy of Groin
5
Contents of Canal
• Spermatic cord in male and round ligament in female
• Ileo-inguinal nerve
• Genital br of genito-femoral nerve
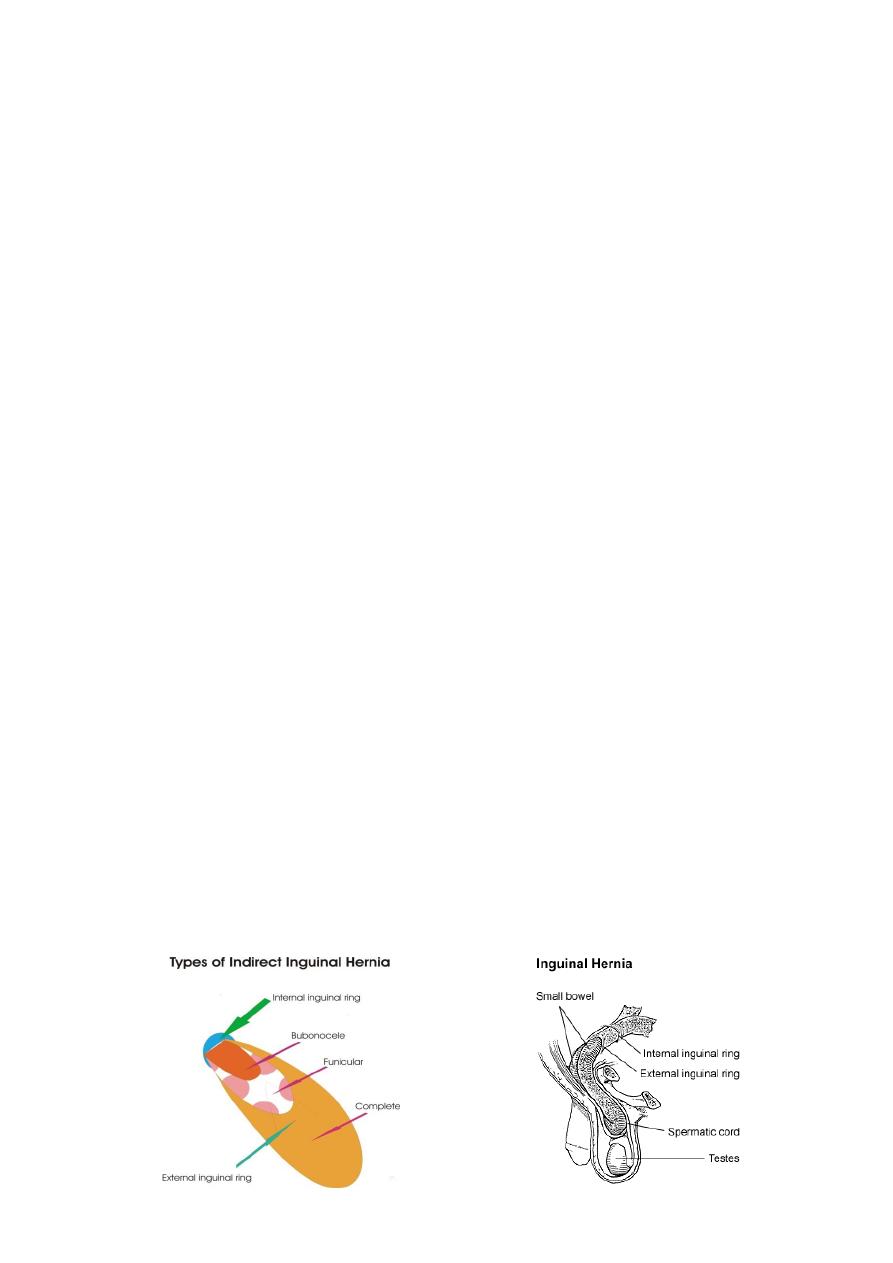
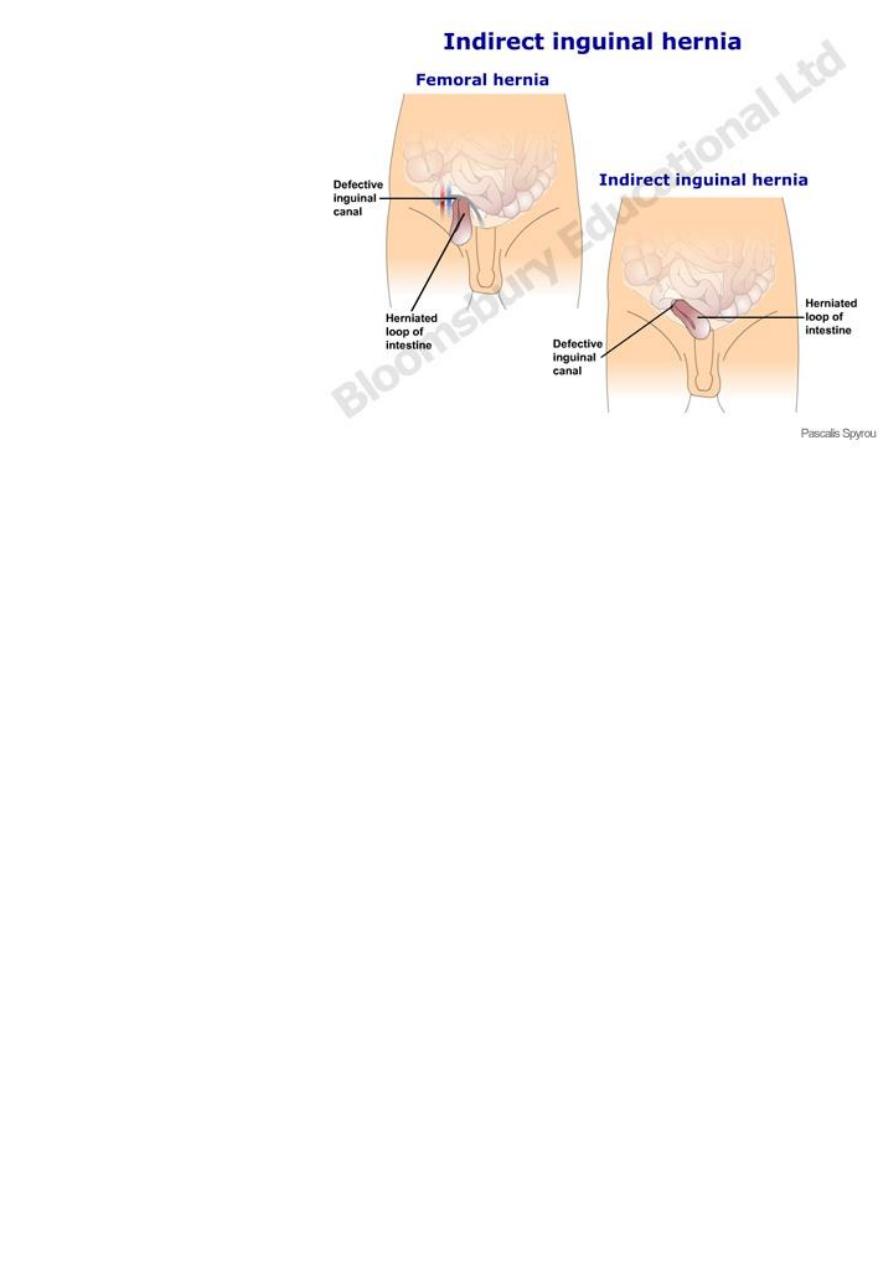
Indirect Inguinal Hernia
• Is the most common of all forms of hernia
• Most common in young
• Men > women
• Right > left
• 10% of premature babies
• 5% of adult population
In adults:
• 65% of all inguinal hernia is indirect
• 55% right
• 12 % bilateral
Incomplete
• Bubonocele
• Funicular
Complete
• Inguinoscrotal

6
Pathogenesis of Indirect Hernia
Indirect hernia
• Congenital
• Acquired
Congenital:
• Persistent processus vaginalis
• Within spermatic cord
• Follows indirect course
• Complete vs. incomplete sac
Acquired
Precipitating factors
• Increased intra-abdominal pressure
• Defects in collagen synthesis
• Smoking
Clinical Features
• Any age
• Right < Left
• Male < Female (20 times)

7
Presenting symptoms
• Swelling appear on standing or coughing
• Pain in the groin
• Swelling in the groin
• Swelling in the groin descended to scrotum
Examination
• Apparent on standing
• Expensile cough impulse
• Controlled on pressing over the DIR
8
Indirect Inguinal hernia
Diagnosis:
• Groin swelling that disappear with supine position
• Examine erect and supine
• Does not transilluminate
• Expensile cough impulse
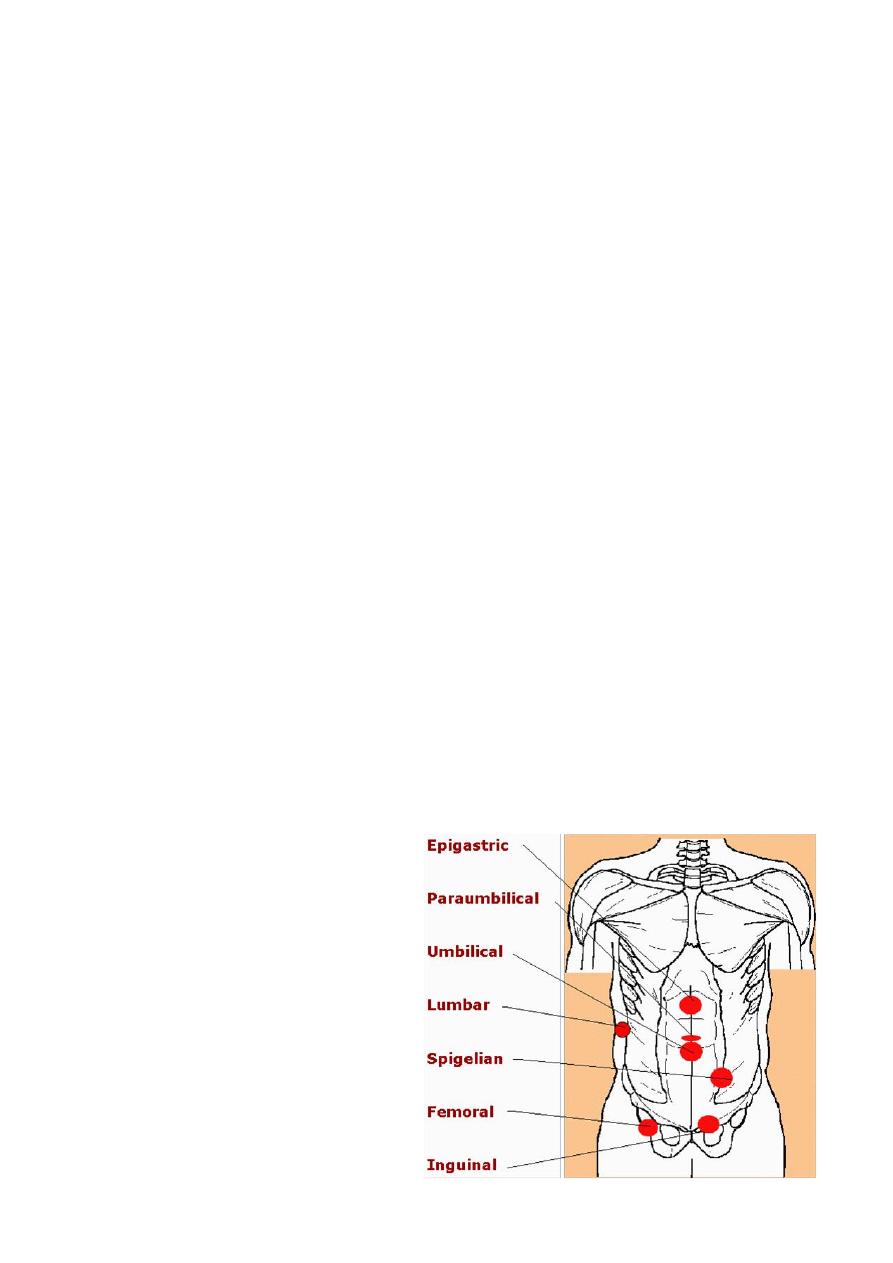
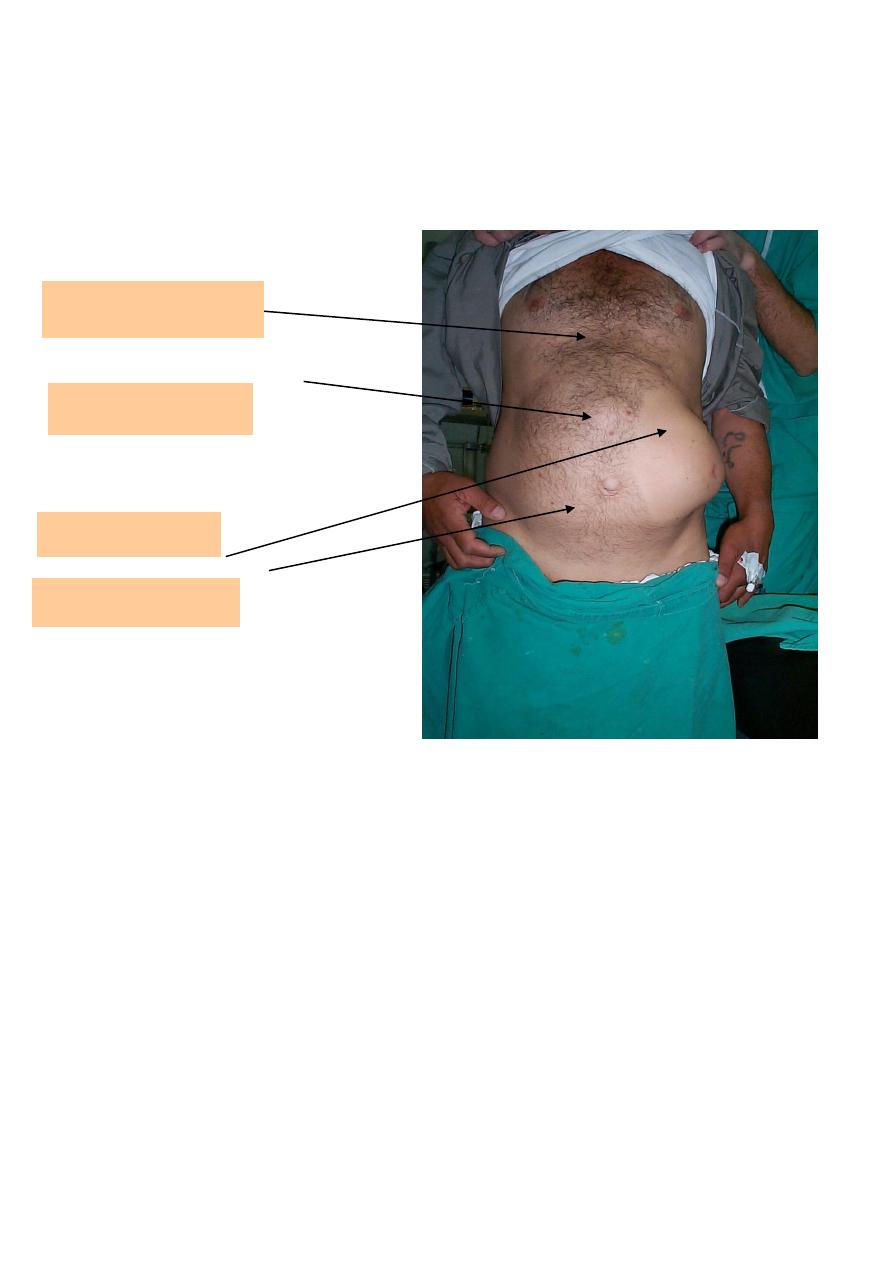
Epigastric hernia
Umbilical hernia
Spigelian Hernia
Inguinal hernia

9
How to differentiate IIH from DIH
When the swelling localized to groin
The differential diagnosis:
• Femoral hernia
• Lipoma of cord
• Inguinal lymphadenopathy
• Incompletely descended testis
• Ectopic testis
• Femoral artery aneurysm
Differential Diagnosis
When the swelling is inguino-scrotal
Vaginal hydrocele
Encysted hydrocele of cord
Spermatocele
Varicocele
Epididymoorchitis
Torsion of testis
Testicular tumor
11
In female
Femoral hernia
Hydrocele of canal of
Nuck
Inguinal
lymphadenopathy
Treatment:
• Operation is treatment of choice:
• Open surgery
• The standard method
• Laparoscopic hernia repair
• should be reserved for bilateral or recurrent hernia
• Open surgery
• Herniotomy
• Herniorrhaphy
• Anaesthesia
• Local
• Spinal
• General
Herniotomy
• Indications:
• In infants, children and adolescents
• Steps of surgery:

11
• Dissection of sac
• Open of sac
• Reduction of contents
• Transfixation of neck
• Cut of reminder
Herniorrhaphy
• Repair of stretched DIR and transversalis fascia
• Reinforcement of posterior wall by:
• Shouldice repair
• Mesh repair
Complications:
• Bleeding
• Skin bruises, SC hematoma
• Scrotal hematoma
• Retention of urine
• Wound infection
• Injury to vas deference
• Ischemic orchitis
• Neuralgia
-Ilioinguinal
-Iliohypogastric
-Genitofemoral
-Lateral cutaneous
• Recurrence >1%
12
Direct Inguinal Hernia
• Acquired
• Adults
• 35% of inguinal hernia
• 12% bilateral
• Not occur in females
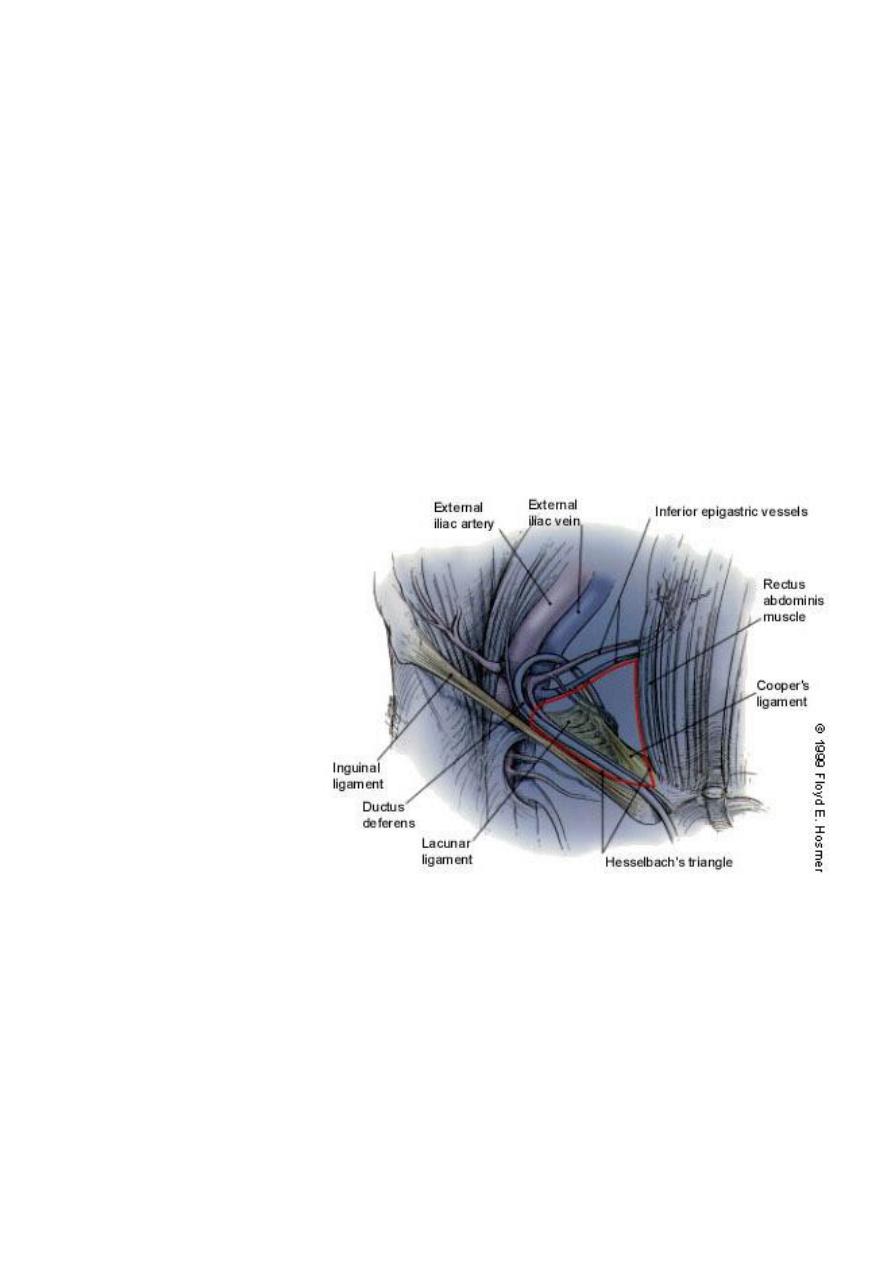
Anatomy of Direct Hernia:
• Hesselbach’s triangle
– Inguinal ligament (base), rectus (medial), inferior epigastric vessels (lateral)
Hesselbach’s triangle
• Pathogenesis:
• Through weak posterior wall of inguinal canal
• Medial to Inferior epigastric vv
• Not attain large size or descent into scrotum
• Lies behind spermatic cord
• Wide neck

13
• Varieties
• Dual ( Pantoloon,saddle bag)
• Funicular (Prevesical)
Clinical Features:
• Swelling in the groin
• On examination:
• controlled on pressing on SIR
• ECI
Treatment:
• Surgical repair
• Dissection of sac
• Inverted
• Repair of transversalis fascia
• Mesh(Lichtenstein) or Shouldice repair
Strangulated Inguinal Hernia
• Can occur at any time
• More liable to occur in patients with irreducible hernia.
• More commonly occur in IIH
• Less often in DIH
Constricting agent
• Neck of sac
• External inguinal ring
• Adhesions within the sac
Content of hernia
• Small intestine
• Omentum
• Both
14
Clinical features:
• Severe pain in the groin
• Vomiting
• General upset
• Fever ?
• Swelling with skin discoloration in the groin
• Severely tender
• Abdominal signs
Treatment:
• Urgent surgery
• Pinciples:
-Dissection of sac
-Open the sac
-Exploration of content
-Excision of gangrenous tissues
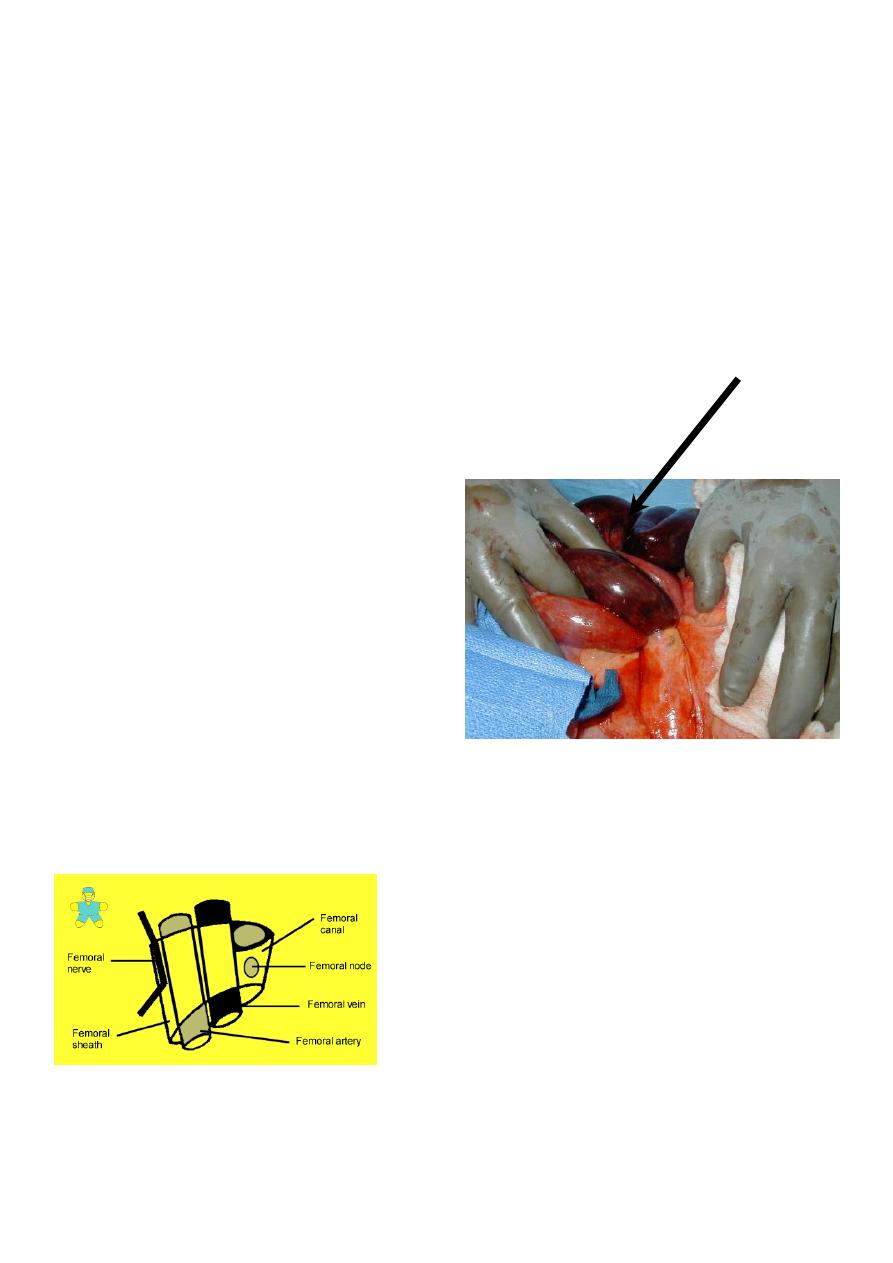
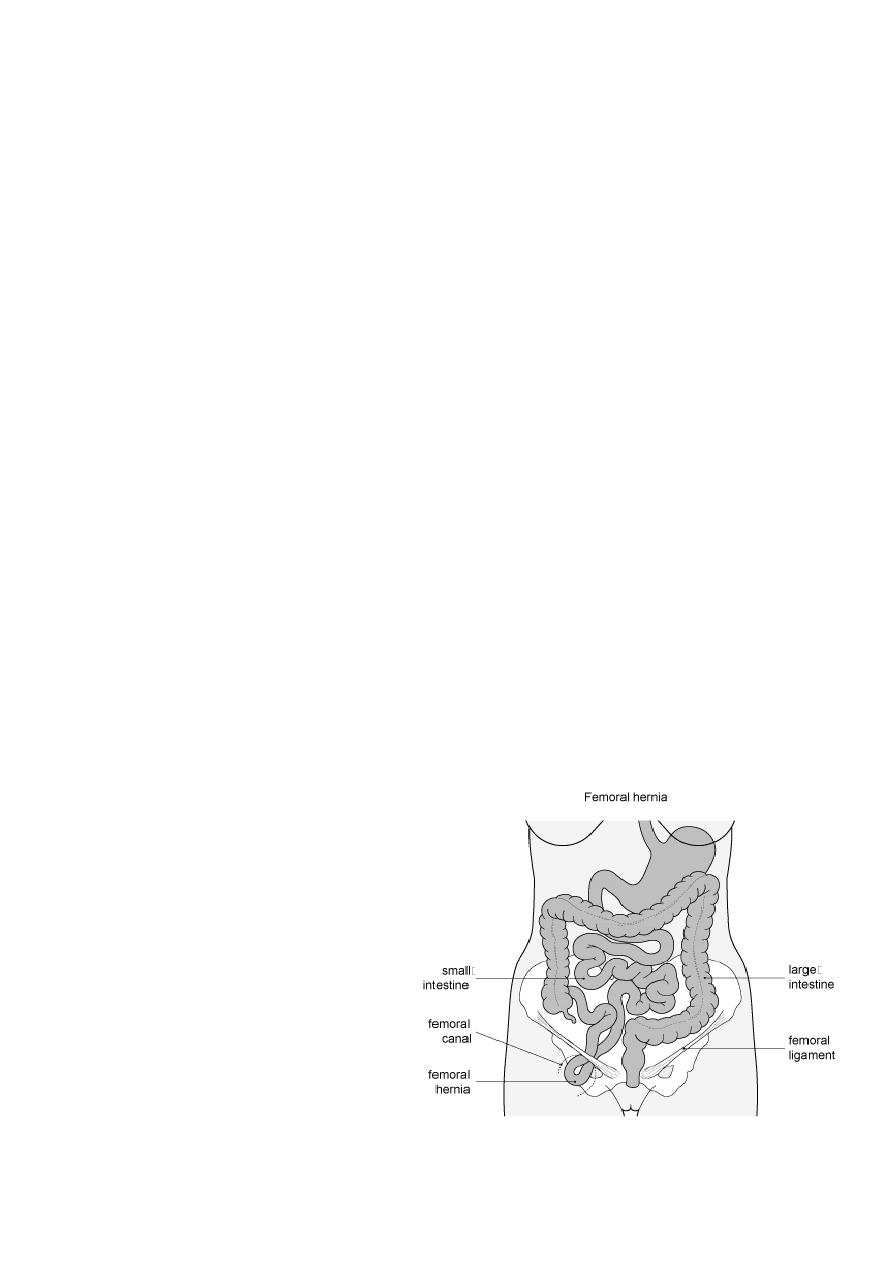
Femoral Hernia
Anatomy of the femoral canal
• Boundaries of femoral ring
• Anterior border is the inguinal ligament
• Posterior border is the pectineal ligament
Gangrenous bowel
15
• Medial border is the lacunar ligament
• Lateral border is the femoral vein
Femoral Hernia
• Women> men
• 20% of hernias in women
• More in parous
• Most liable for strangulation
Clinical features
• Rare before puberty
• May be un-noticed by the patient
• Strangulated hernia
• Sudden painful swelling in the groin
• Abdominal symptoms
Examination
• The swelling is inferior to inguinal ligament and lateral to pubic tubercule
• Mostly irreducible
Differential Diagnosis:
• Inguinal hernia
• Lymphadenopathy
• Saphena varix
• Ectopic testis
• Psoas abscess
• Distended Psoas bursa
• Lipoma
• Rupture of adductor longus
16
Treatment:
• Uncomplicated hernia:
• Operation as early as possible
• Strangulated hernia
• Urgent surgery
• Approaches for the surgery
• Low approach – Lookwood
• High approach - McEvedy
• Inguinal approach - Lotheissen
• Principle of surgery
• Dissection of sac
• Open sac
• Reduction of contents if healthy otherwise gangrenous tissue must be
excised.
• Repair of femoral ring
Richter’s hernia
Frequent complication of femoral hernia
Only part of circumference of bowel enclosed in the hernia sac which
may become gangrenous
Clinically; abdominal symptoms of IO but with no constipation
Diagnosis:
High index of suspicion
Urgent surgical interference
Almost always the diagnosis made at surgery
Umbilical hernia
In neonates
Exomphalos
1/6000 of births
Failure of all or part of midgut to return to the coelom
In infants and children
Defect in the umbilical cicatrix
17
Equal sex incidence
Black infants 8 times more
Clinical features
Symptomless
More prominent during crying
Obstruction or strangulation is rare below 3 years of age
Most of cases resolve by itself within 2 years
Diagnosis
Swelling with umbilical cicatric at fundus of swelling
Reducible
ECI +ve -----Crying
Treatment
Conservative below the age of 2 years – reassurance of parents
After 2 years needs surgical repair
Paraumbilical Hernia
Adults
Women> men
Risk factors :Obesity ,Pregnancy
Repair primarily or with mesh
Pathogenesis
Weak point in the linea alba just above or just below the
umbilical cicatrix
Round or oval in shape
May sag downwards
May become a large size
The neck of sac is often remarkably small in size
Contents; mostly small intestine or omentum or both(Sometimes part of transverse colon)
Clinical features
Classical patient:
Adult Female (F:M ; 5:1)
Aged between 35 and 50 years
Overweight
18
multipara
Symptoms
Abdominal swelling
Dragging pain
Intestinal colics—obstruction
Epigastric pain (stomachache)
Complications
1. Irreducibility with possibility of IO
2. Ulceration of skin over fundus of sac
3. Intertrigo
Diagnosis -------> clinical :
Swelling just above or below the umbilicus
Prominent on standing
Disappear on lying
Expensile cough impulse
Treatment
Operation is advised in nearly all patients.
Indications:
1. Liable for complication
2. Cosmetic
The operation is "Herniotomy and Repair" ,Either Myo’s repair or Mesh repair.
Mesh repair is indicated for
1. Large defect > 4 cm
2. Recurrent hernia
Postoperative complications
Local and specific
1. Collection(Hematoma,Seroma )
2. Infection (Wound infection,Pus collection)
3. Recurrence
Epigastric Hernia(Fatty hernia of linea alba)
Incidence 1-5%
Men> women
Between xiphoid and umbilicus
20% multiple
Repair primarily
Pathogenesis
Extraperitoneal fat protrusion through decussating fibers at linea alba
At sites of blood vessels
19
Clinical features
Symptomless:
Accidental finding
The size of a Pea
Felt not seen
Painful ---local pain and tenderness
Referred pain----DU like symptoms
Treatment: operation
Spieghelian Hernia
Rare
Hernia through subumbilical portion of semi-lunar line
Difficult to diagnose
– Clinical suspicion (location)
– CT scan
Repair primarily or with mesh
Incisional Hernia
This occurs after 2-10% of all abdominal surgeries, although some people are more at risk.
After surgical repair, these hernias have a high rate of returning (20-45%).
Risk factors
– Technical
– Wound infection
– Smoking
– Hypoxia/ ischemia
– Tension
– Obesity
– Malnutrition
Laparoscopic vs. open repair
Lumbar Hernia
Congenital, spontaneous or traumatic
Grynfeltt’s triangle:
– 12th rib, internal oblique and sacrospinalis muscle
– Covered by latissimus dorsi
Petit’s triangle:
– Latissimus dorsi, external oblique and iliac crest
– Covered by superficial fascia
21
Pelvic Hernia
1) Obturator hernia
– Most commonly in women
– Howship-Romberg sign
2) Sciatic hernia
3) Perineal hernia
Parastomal Hernia
Variant of incisional hernia
Paracolostomy > paraileostomy
Low rate if through rectus muscle
Traditionally relocate stoma, repair defect
Concern for mesh erosion
Laparoscopic repair
Abdominal Wall Hernia
1) Richter’s hernia
2) Littre’s hernia
3) Hernia in W
4) Pantallon
Umbilical Hernia
Common in infants
Close spontaneously if <1.5 cm
Repair if > 2 cm or if persists at age 3-4 years
Repair primarily or with mesh