1
Forth stage
Surgery
Lec-1
د.فراس
1/1/2014
Umbilical granuloma
Chronic infection of the umbilicus that continues for weeks cause
granulation tissue to pout at the umbilicus.
Treated by application of silver nitrate
Pilonidal sinus: a sinus containing a sheath of hair.
Treatment: surgery
Burst abdomen and Incisional hernia
Etiology
Technique of wound closure: (poor closure technique).
- Choice of suture material
- Method of closure
- Drainage
Factors relating to incisions (vertical or transverse incisions).
Reasons for initial operation (pancreatic and obstruction operations, or
peritonitis). Deep wound infection.
Coughing, vomiting and distension: any violent coughing by removal
of endotracheal tube, or suction of laryngopharynx, and in
postoperative ileus.
Metabolic state of the patient: obesity, jaundice, malignant diseases,
hypoprotinemia and anemia. are factors conductive to disruption of
wounds.
Clinical features:
A serosanguinous discharge from the wound is the first sign of disruption in
50% of cases. It is pathognomonic sign of impending wound disruption and
signifies that intraperitoneal contents are lying
extraperitoneally. It occur
between the sixth and eighth day after operation.
If the skin sutures have been removed, omentum and coils of intestine may
be forced through the wound.
Pain and shock are absent. May be there are symptoms and signs of
intestinal obstruction.
2
Treatment
An emergency operation is required to replace the bowel, relieve any
obstruction and resuture the wound.
While awaiting the operation:
Reassure the patient and cover the wound with a
sterile towel.
NG tube, IVF, antibiotics and sedation.
The edges approximated by through and through
monofilament nylon and by tension sutures.
Contrary to what is expected peritonitis rarely
supervenes and healing is satisfactory.
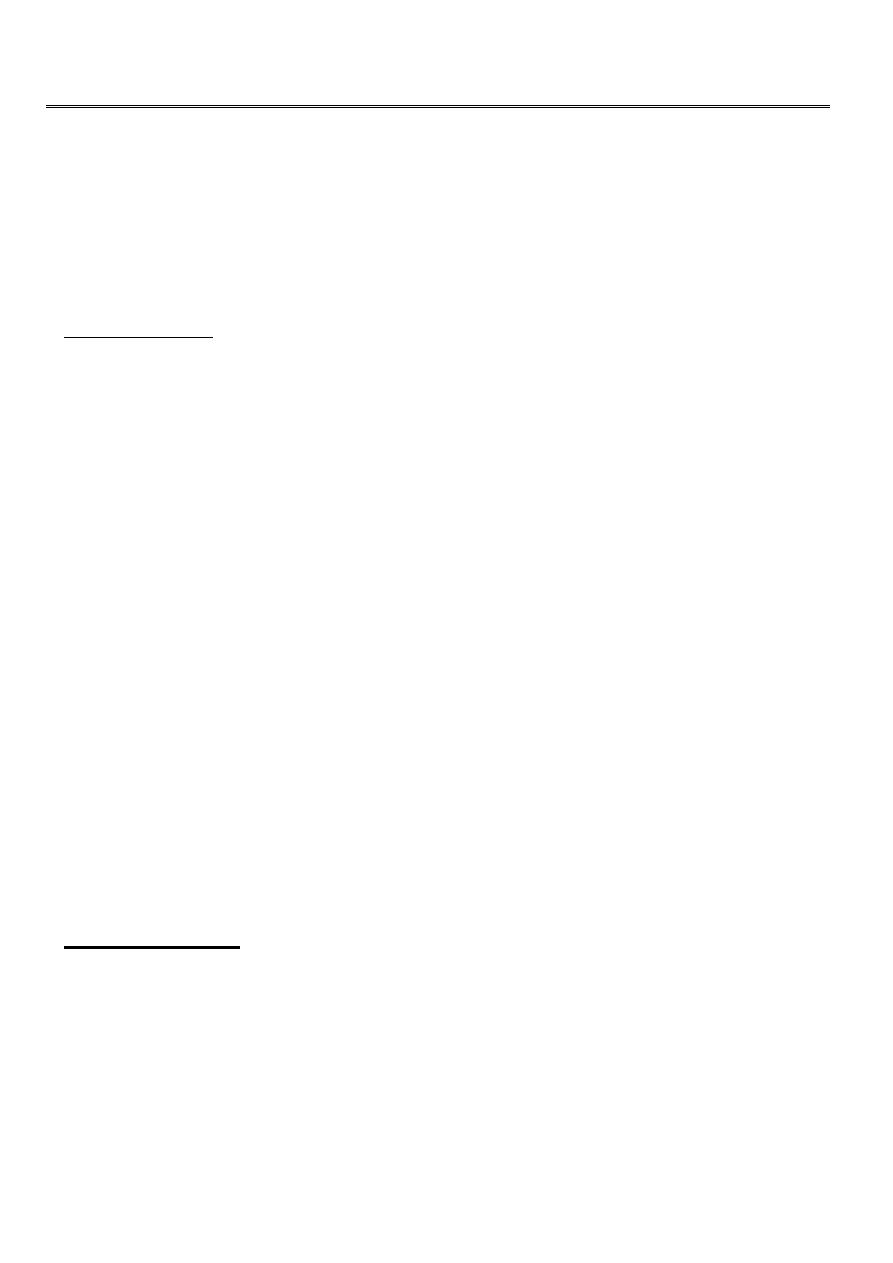
Incisional hernia
Clinical features
Starts as symptomless partial disruption of the deeper layers of laparotomy
wound during the early postoperative period. It is passed unnoticed if the
skin wound remains intact after the skin sutures have been removed.
Bulging of part or all the scar
Increases steadily in size
The skin overlying it becomes thin and atrophied
Attacks of intestinal obstruction and strangulation
Most cases are asymptomatic and broad necked
•
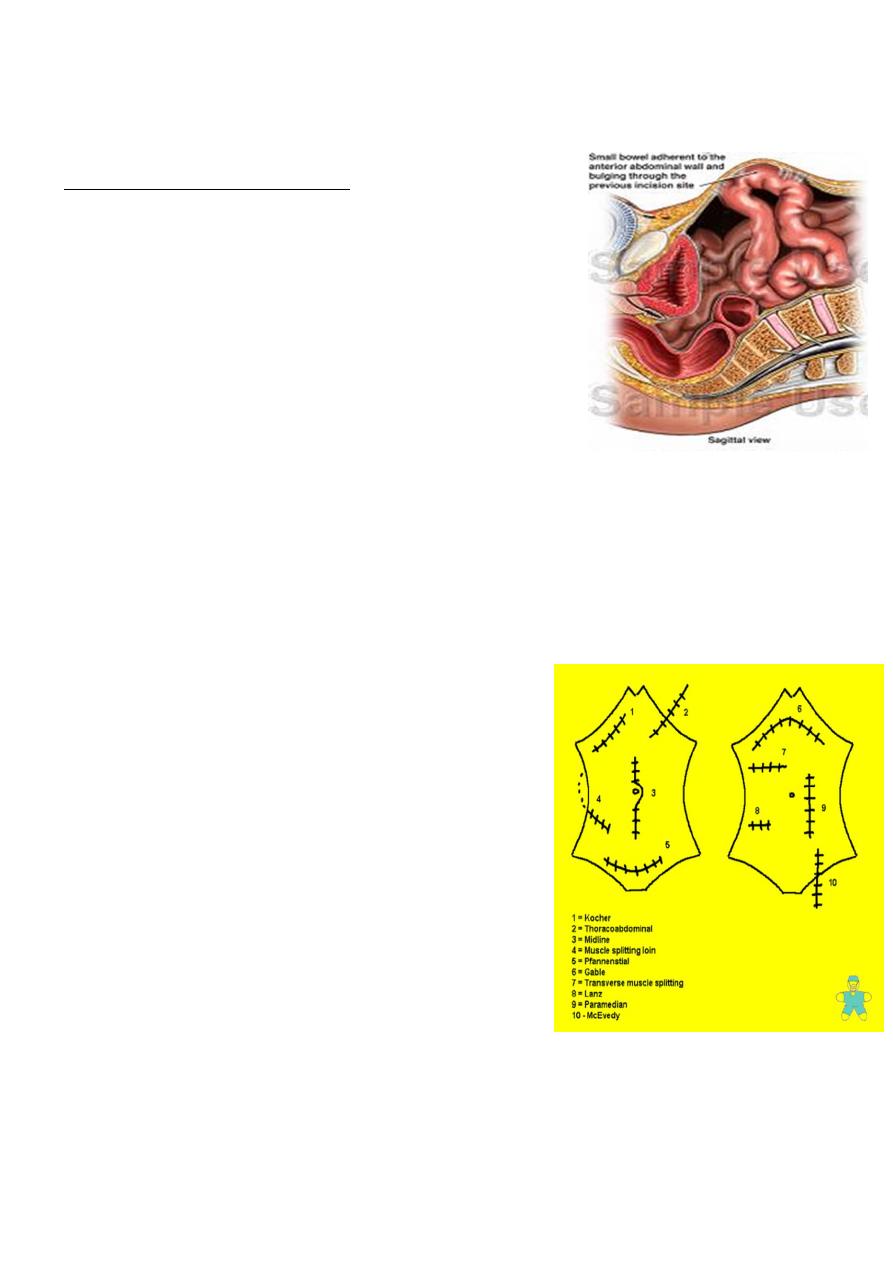
Kocher or Right Subcostal Incision: oblique
abdominal incision paralleling the thoracic
cage on the right of the abdomen for
cholecystectomy.
•
Pfannenstial Incision: A transverse incision
through the external sheath of the rectus
muscles, about an inch above the pubes.
•
Lanz incision: muscle splitting transverse
abdominal incision employed in
appendectomy.
Treatment
Palliative: An abdominal belt. Weight reduction.
Simple apposition: The layers are repaired with non absorbable sutures, the
muscles and remaining facial layers are approximated.

3
Plastic fiber mesh closure: These are now the method of choice for all but the
small hernias < 4cm. If the defect is more than 4 cm mesh is indicated.
Laparoscopic surgery can be used to close incisional hernia.
Careful hemostasis and meticulous asepsis are essential during these operations.
Postoperative collection of serum can be removed by drainage.
Complications of Incisional Hernia Repair
Enterotomy
Superficial wound Infection
Mesh Infection
Seroma
Prolonged Pain
Ileus
Bleeding/Hematoma
Recurrence
Respiratory Distress
Abdominal Compartment syndrome or IVC compression
Postoperative care
Gastric decompression
IV fluid
Nothing by mouth
Early ambulation
Gentle physical exercise
Tearing of the inferior epigastric artery
Occurs in three types of patients
Elderly women, thin and feeble
Athletic muscular men
Pregnant woman late in pregnancy
The site of the hematoma at the level of the arcuate line
Clinical features: Following a bout of coughing, or a sudden blow to the
abdominal wall, a tender lump appears in relation to the rectus abdominis.
The diagnosis may be difficult if there is no ecchymosis of the skin

4
Differential diagnosis
Twisted ovarian cyst
Appendicular mass
Strangulated spigelian hernia
Treatment: a small hematoma may resolve,
It is safer to operate and evacuate the clot and ligate the artery.
Neoplasm of the abdominal wall
Desmoid tumor: it is a hard tumor arising in the musculoaponeorotic structures
of the abdominal wall, specially below the level of the
umbilicus. it is an
unencapsulated fibroma .
Etiology: 80% in women, occur in scars of old operation wounds. Trauma,
stretching of muscle fibers during pregnancy, or hematoma of the abdominal
wall are aetiological factors. It can occur in cases of familial adenomatous
polyposis.
Pathology: no metastasis or sarcomatous changes.
Treatment: The tumor should be excised widely with a margin of 2.5 cm of
healthy tissue
Fibrosarcoma
adenocarcinoma