1
4th stage
جراحة بولية
Lec-7
.د
نعمان
11/10/2015
بسم هللا الرحمن الرحيم
Renal Stone Disease
Epidemiology
Urinary calculi are the third most common affliction of the urinary
tract, exceeded only by urinary tract infections and pathologic
conditions of the prostate
Gender :
Men are affected 2 - 3 times more frequently than women
Age : No age is exempted but stone occurrence is relatively
uncommon before 20 year of age, the peak incidence in the fourth to
sixth decades of life
( 50% of patients present between 30-50 years of age)
Stone recurrence rates can be as high as 50% within 5 years
Etiology
1-Dietetic..deficiency of vitamin A causes desquamation
2-Altered urinary solutes & colloids ..Dehydration leads to an increased
concentration of urinary solutes &cause them to precipitate.
3-Decreased urinary citrate.. Normally 300-900 mg/24hr.
4-Renal infection.
5-Inadequate urinary drainage & urinary stasis, functional & anatomical
abnormalities of the urinary tract.
6-prolonged immobilization.
7-Hyperparathyroidism
.

2
Risk Factors
Crystalluria
Socioeconomic Factors: Renal stones are more common in affluent,
industrialized countries
Diet : Diet changes, with an increase in saturated and unsaturated fatty
acids, an increase in animal protein and sugar, and a decrease in dietary
fiber, vegetable protein, and unrefined carbohydrates.
Fluid intake and urine output may have an effect on urinary stone disease
.
Occupation: Individuals with sedentary occupations such as those in
managerial or professional positions, Physicians and other white-collar
workers have an increased incidence of stones compared with manual
laborers.
Heat exposure and dehydration constitute occupational risk factors for stone
disease as well.
Climates A higher prevalence of stone disease is found in hot,
arid, or dry climates such as the mountains, desert, or tropical
areas
.
Family History A family history of urinary stones is associated with an
increased incidence of renal calculi.
Types of Renal Calculus
Calcium Calculi (( like calcium oxalate)): 80-85% of all urinary stones
are calcareous , irregular in shape with projections.
Phosphate calculus: Usually calcium phosphate ,sometimes magnesium
ammonium phosphate “Struvite “,They frequently present as renal
staghorn calculi
”, Struvite stones are infection stones associated with
urea-splitting organisms.
Uric acid & Urate calculi: are hard smooth &often multiple. pure uric acid
stones are radiolucent.
Cystine calculi: uncommon ,occur with congenital error of metabolism..
multiple, very hard, pink or yellow when first removed.
Xanthine calculi: very rare ,smooth & round.
Indinavir: Protease inhibitors are a popular and effective treatment in
patients with acquired immunodeficiency syndrome (AIDS).
Rare: Silicate stones , Triamterene stones, matrix stones.
3
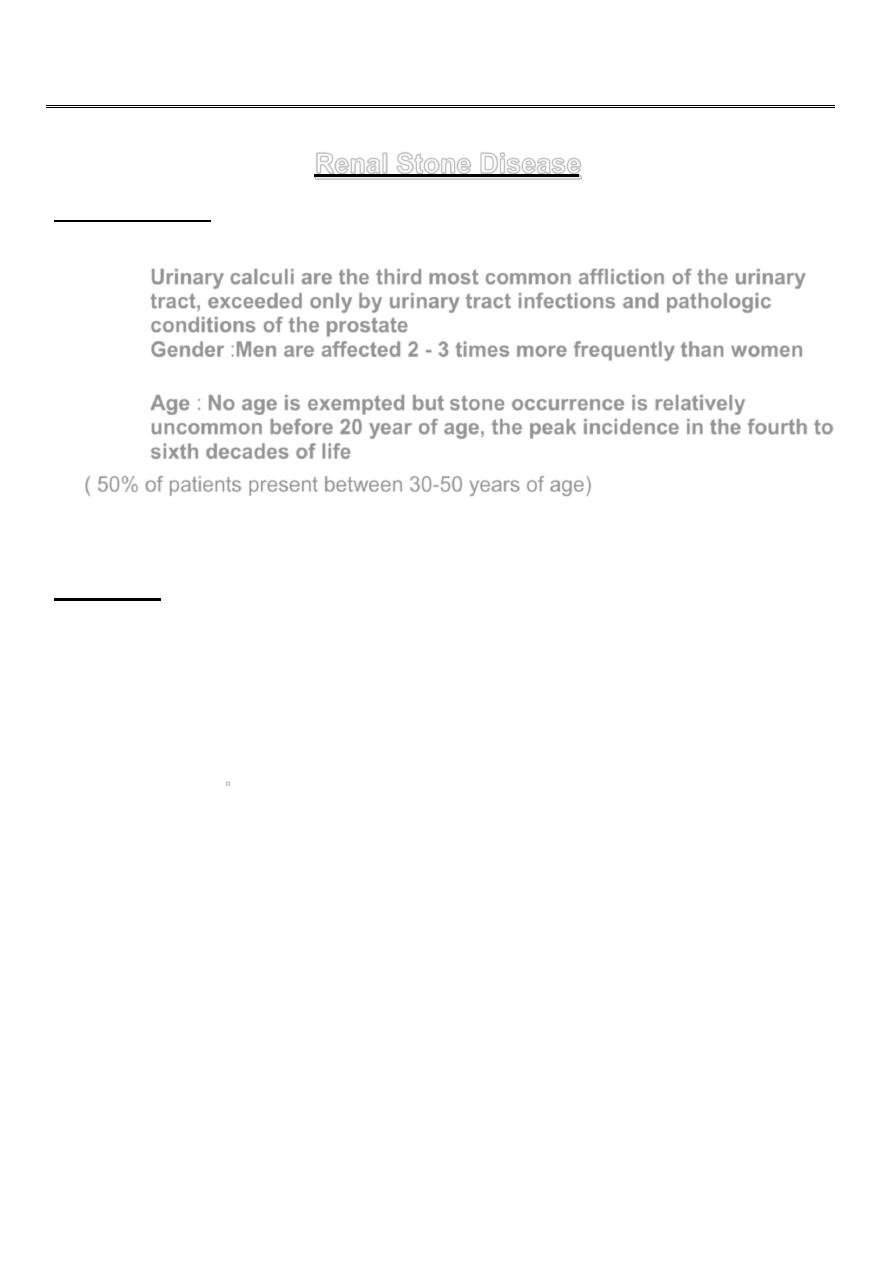
linical Features
C
Symptoms are variable
Silent calculus: Even large staghorn calculi may cause NO symptoms for
long period. If they are bilateral
uremia
may be the first indication of their
presence , although 2ry infection usually gives symptoms first.
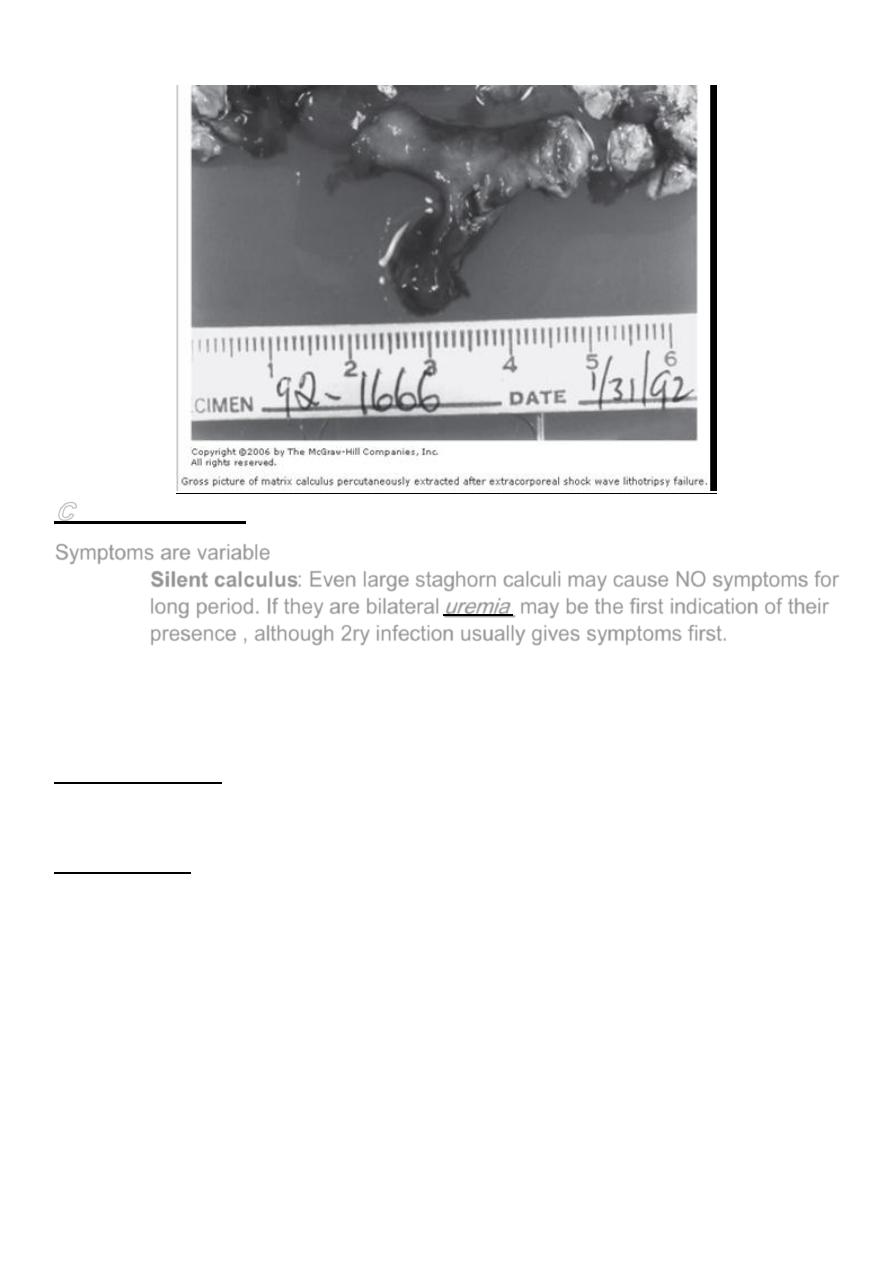
Pain: Occurs in 75% of patients
Renal colic and noncolicky renal pain are the 2 types of pain originating from the
kidney.
Fixed Renal Pain Is located posteriorly in the renal angle, anteriorly in the
hypochondrium or in both.
Ureteric Colic sudden severe agonising pain passing from the loin to the groin. It
starts suddenly causing patient to move around trying to find comfort .
Attack of colic rarely lasts more than 8 hours, not associated with pyrexia by itself
although pulse rate usually rises.
Ureteric colic is often caused by stone entering the ureter or occur when a stone is
being lodged in the PUJ.
4
. Hematuria: Intermittent gross hematuria or occasional tea-colored urine (old
blood).
Most patients will have at least microscopic hematuria.
Complete ureteral obstruction presents without hematuria
. Infection
:Magnesium ammonium phosphate (struvite) stones are
synonymous with infection stones. They are commonly associated with
Proteus, Pseudomonas, Providencia, Klebsiella, and Staphylococcus
infections.
Calcium phosphate stones (brushite stones ) is another infection stone.
Fever: The association of urinary stones with fever is a relative medical
emergency.
Nausea and Vomiting
Clinical examination
Abdominal Exam.: Rigidity of lateral abdominal muscles.
Renal Angle Tenderness +ve.
Palpable swelling in the loin in case of hydronephrosis or pyonephrosis.
Investigations
Laboratory Investigations:
- GUE (general urine examination)
- C&S (urine culture &sensitivity)
- KFT (kidney function test)
- CBC
(complete blood count)
5
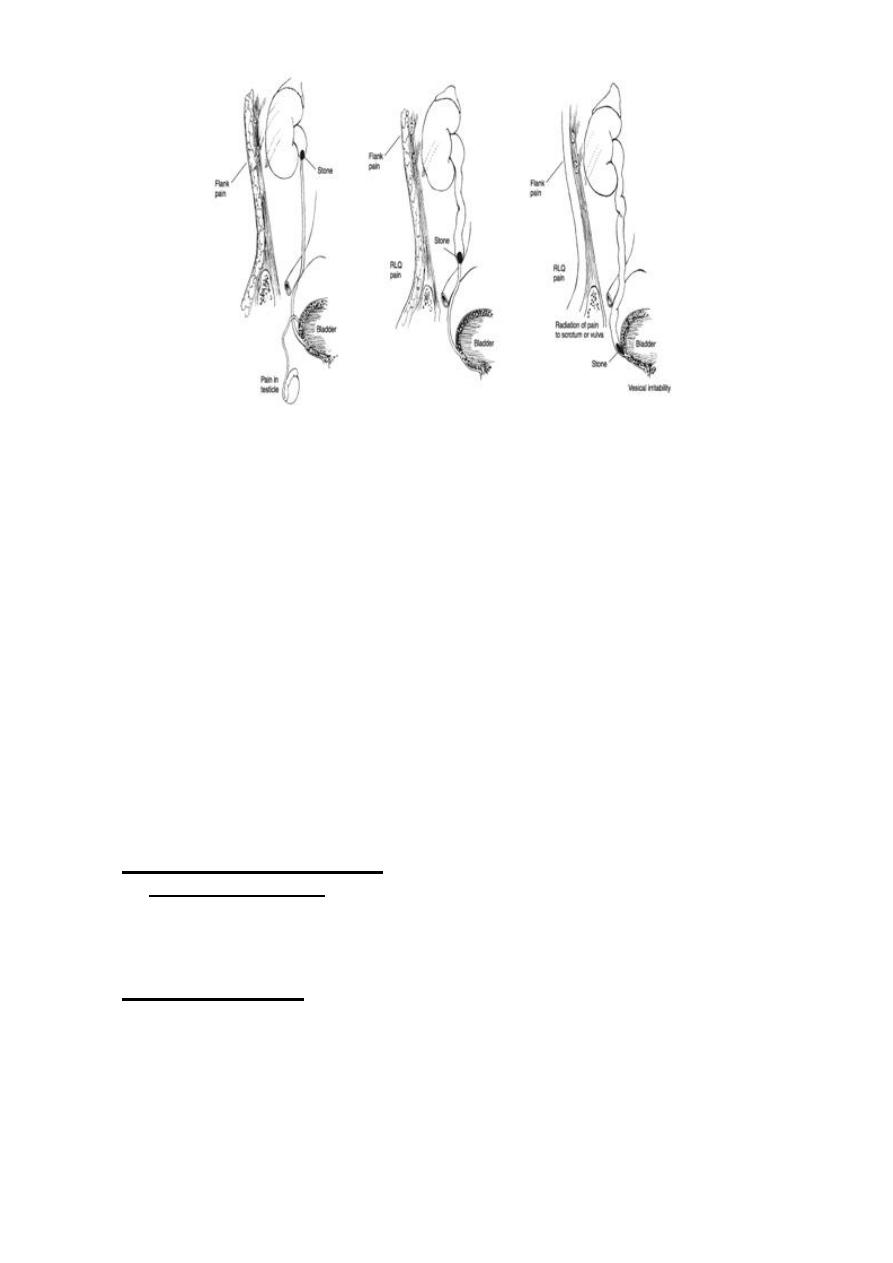
nvestigations(cont.)
I
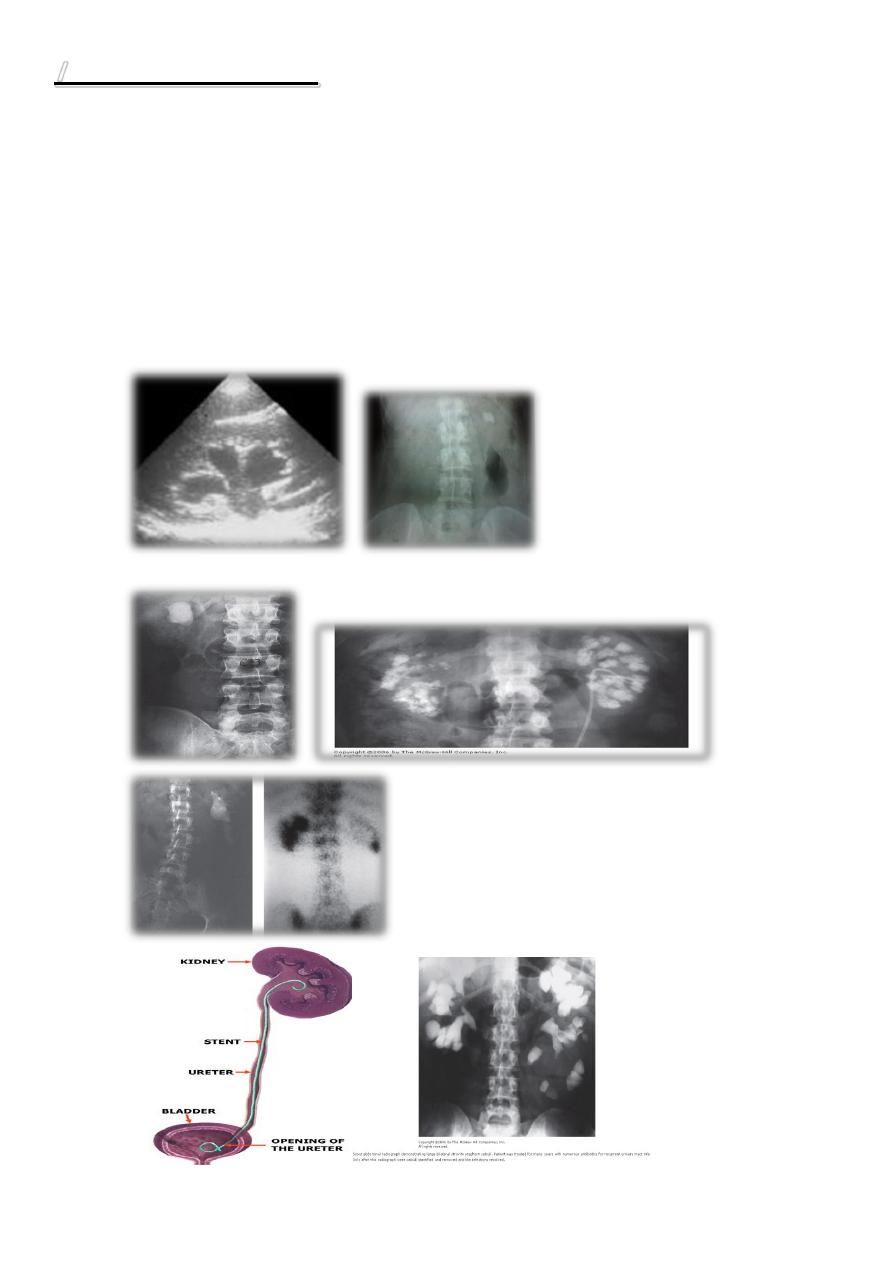
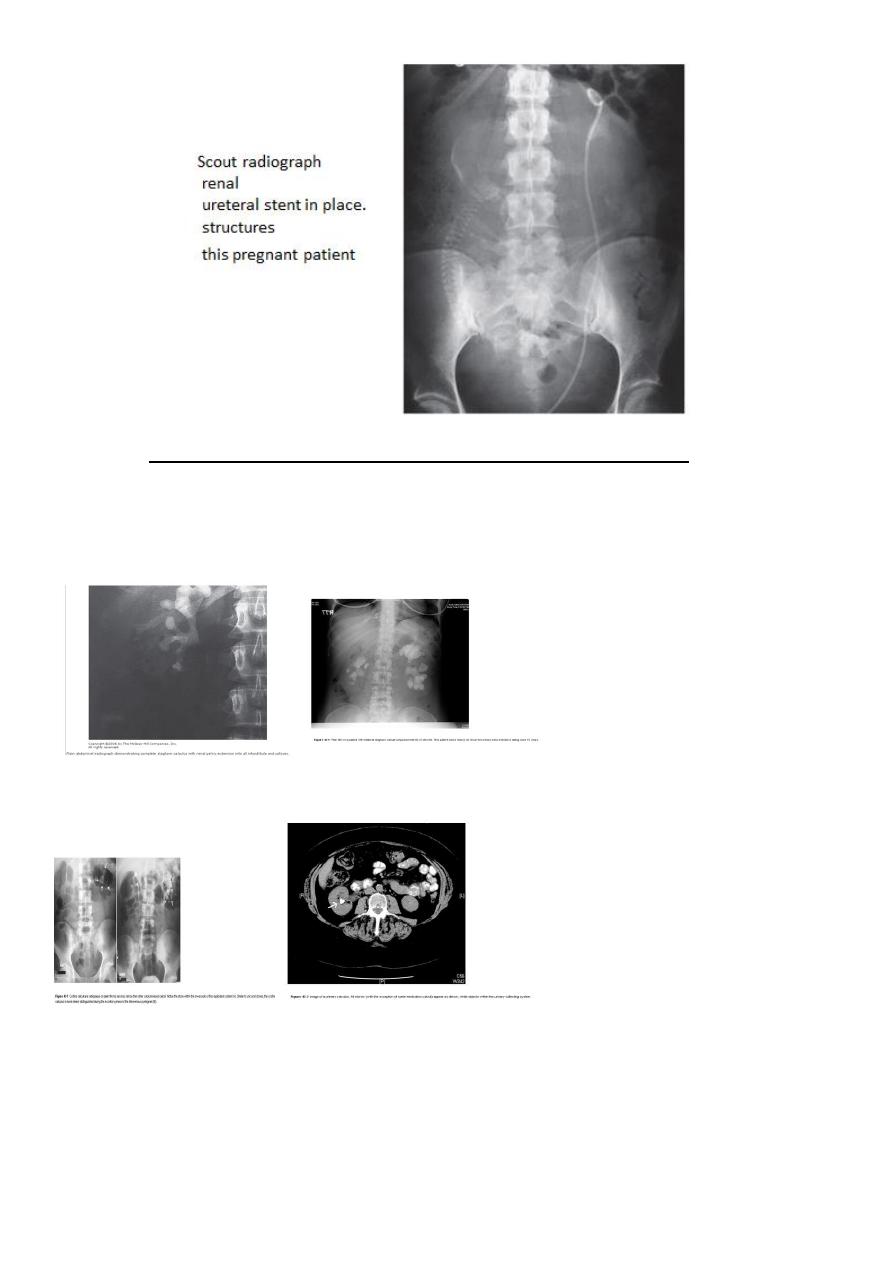
Radiological investigations (imaging studies):
U/S (Ultrasound Scanning).
KUB (kidney, ureter, &bladder): 90% of urinary stones are
radioopaque.
Excretory Urography (intravenous Urography IVU, intravenous
pyelograpgy IVP).
Retrograde Pyelography.
Computed Tomography (CT scan).
Magnetic Resonance Imaging (MRI).
Nuclear Scintigraphy.
6
7
Differential Diagnosis
A full differential diagnosis of the acute abdomen should be made, including:
- Acute appendicitis
- Ectopic pregnancies - Ovarian pathologic conditions
- Diverticular disease of the colon - Bowel obstruction
- Biliary stones with and without obstruction - Peptic ulcer disease
- Acute renal artery embolism - Abdominal aortic aneurysm
• Treatment of Renal Calculi
• Conservative Observation.
• Methods of Stone Removal:
1-ESWL(Extracorporeal Shock Wave Lithotripsy).
2- Endoscopic Intervention (ureteroscopy & nephroscopy).
3-PCNL (Percutaneous Nephrolithotomy).
4- Laparoscopic Surgery.
5- Open Surgery.
Conservative Observation
• Spontaneous passage depends on stone size, shape, location, and associated
ureteral edema.
• Ureteral calculi 4-5 mm in size have a 40 - 50% chance of spontaneous
passage.
• The vast majority of stones that pass do so within a 6-week period after the
onset of symptoms.
Dissolution Agents
• Oral alkalinizing agents include sodium or potassium bicarbonate and potassium
citrate, especially effective with pH-sensitive calculi as in uric acid and cystine
lithiasis. Orange juice alkalinizes urine
• Struvite stone dissolution requires acidification of urine.
• Control of UTI
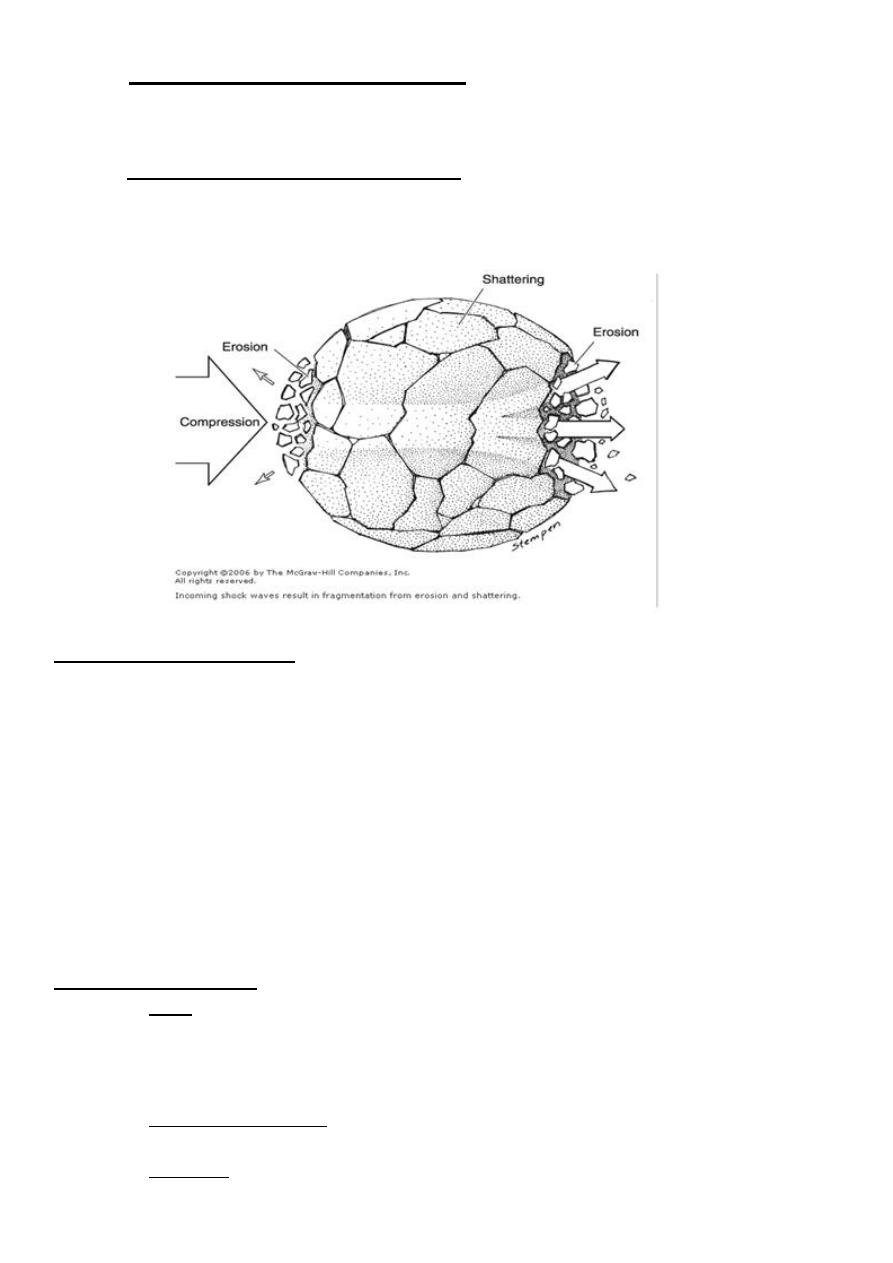
Extracorporeal Shock Wave Lithotripsy ESWL
It can be given without General Anesthesia(except in children)
Factors found to be associated with poor stone clearance rates:
- Factors related to the stones:
• Stone size: Large renal calculi (mean 20 mm)
• Stone composition: (mostly calcium oxalate monohydrate, cystine and brushite)
8
-
Factors related to the kidneys:
• Stones within dependent position (in the lower pole) or obstructed portions of
the collecting system like PUJ obstruction.
-
Factors related to the patient:
• Obesity or a body habitus that inhibits imaging, and unsatisfactory targeting of
the stone.
•
Contraindications to ESWL
:
Absolute CI:
-Pregnant women.
-Patients with large abdominal aortic aneurysms
- Uncorrectable bleeding disorders should not be treated with ESWL.
Relative CI:
-Hypertension.
-Patient with arrhythmia on pacemaker.
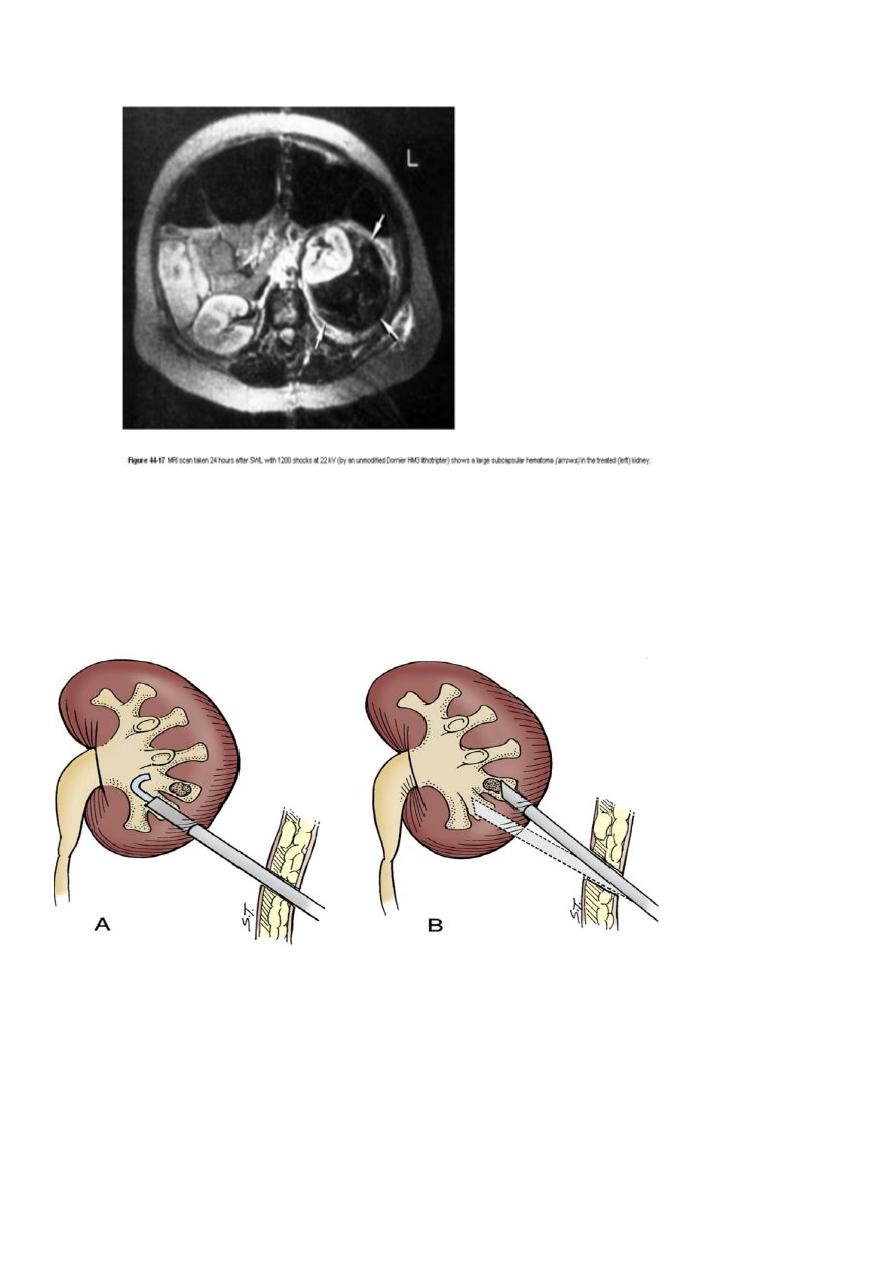
Complications of ESWL:
• Pain: NSAID as diclofenac or narcotics are given
Abdominal pain may be related to the shock waves. Severe pain unresponsive to routine
oral or intravenous medications should alert the physician for possible rare (0.66%)
perirenal hematomas in such a situation.
• Fragment impaction: in to the ureter especially in large stone fragmentation so JJ
stent is used.
• Infection; Antibiotics before ESWL.
9
• Steinstrasse (stone street) or columnation of stone gravel in a ureter can be
frustrating.
Per Cutaneous Nephro Lithotomy (PCNL)
Small stones may be grasped under vision &extracted in whole.
Large stones are fragmented & removed.
Sometimes combined with ESWL in the treatment of staghorn calculi.
Complications of PCNL
• Hemorrhage from punctured renal parenchyma.
• Perforation of pelvicalysial system & extravasation of irrigant fluid.
• Injury to the surrounding organs.
• Arteriovenous fistula formation.
11
Open & laparoscopic surgery for Renal calculi
• Pyelolithotomy
• Extended pyelolithotomy
• Nephrolithotomy
• partial nephrectomy
• Nephrectomy
•
Prevention of Recurrence
The following investigations are done in bilateral & Recurrent stone:
• Stone analysis.
• Serum Ca & Uric Acid.
• Urine a 24 hr collection for Urate, Ca++ , Phosphate & cystine.