1
4th stage
Medicine
Lec-4
Dr.Jasim
9/11/2015
VALVULAR HEART DISEASE
Goals and Objectives :
• Discuss the common etiologies of valvular stenosis and regurgitation.
• Recognize the signs and symptoms of severe valvular stenosis and regurgitation.
• Be able to quickly identify and treat acute mitral and aortic regurgitation.
• Identify patients who should be referred for surgical replacement of their valves.
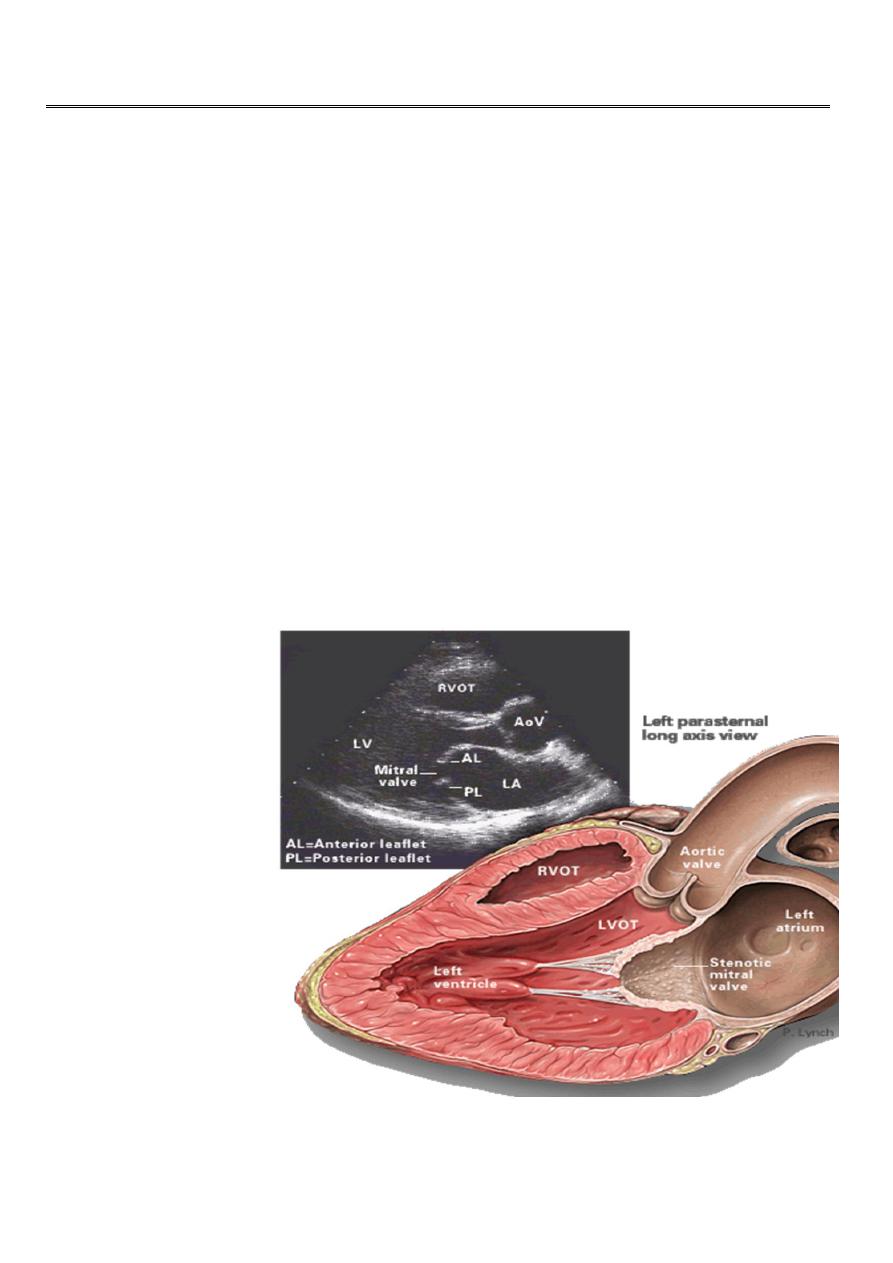
Mitral Stenosis :
Etiology:
• Rheumatic heart disease: 77-99% of all cases
• Infective endocarditis: 3.3%
• Mitral annular calcification: 2.7%
• Congenital: rare.
2
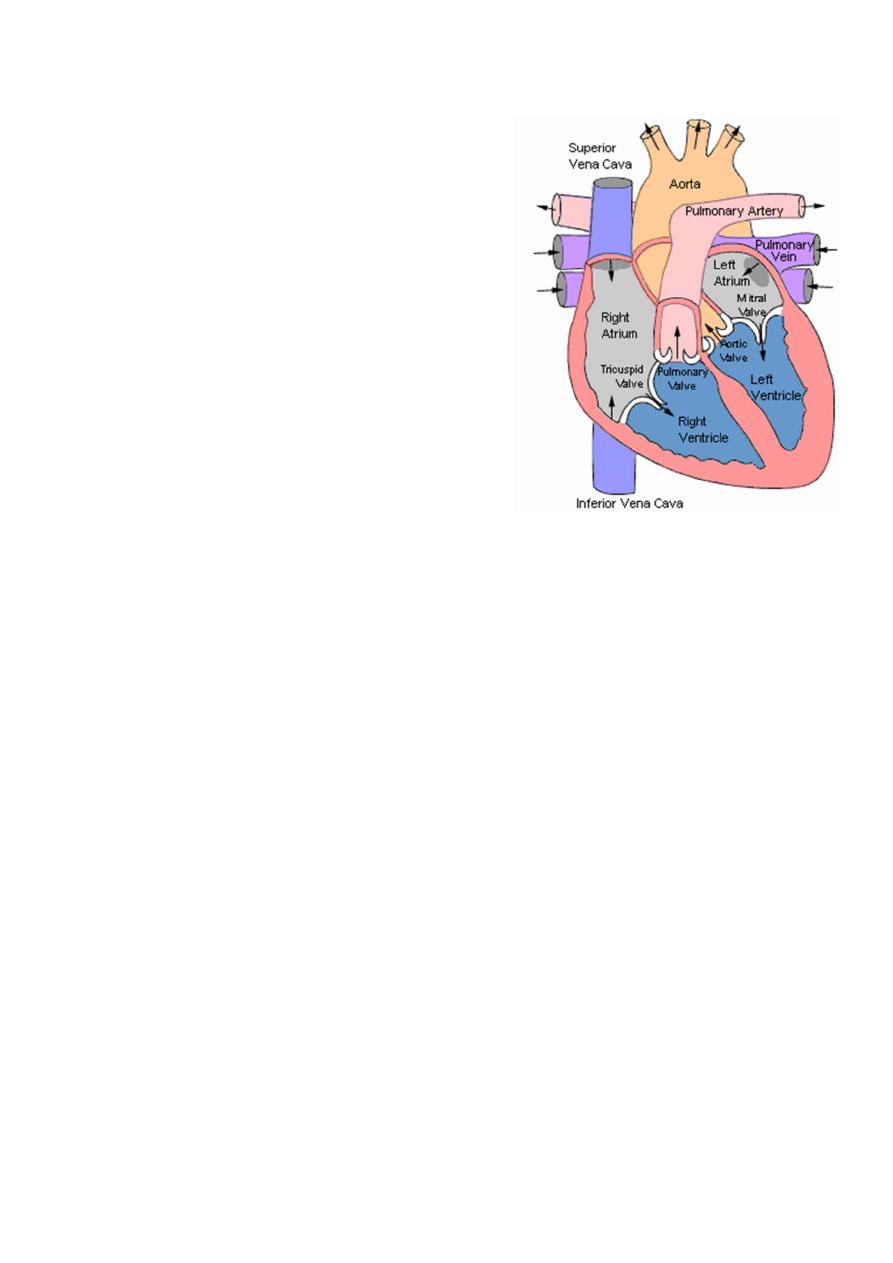
Mitral Stenosis Overview:
• Definition: Obstruction of LV inflow that prevents proper filling during diastole
• Normal MV Area: 4-6 cm
2
• Transmitral gradients and symptoms begin at areas less than 2 cm
2
.
• Rheumatic carditis is the predominant cause.
• Prevalence and incidence: decreasing due to a reduction of rheumatic heart
disease.
MS Pathophysiology:
Progressive fibrosis ,thicking ,calcifications of of valve leaflets and fusion of
commisures leads to gradual narrowing of mitral valve orifice,symptoms begin at
areas less than 2 cm
2
.
3
restricted blood flow from LA to LV and LA pressure rises -Leads to left atrial
enlargement and atrial fibrillation(very common)….. pulmonary congestion(reduced
lung compliance) pulmonary venous hypertension –Progressive and gradual rise in
pulm.venous HTN leads to increase pulm.vascular resistance and pulm.arterial HTN
leading to RVH-later RV dilatation and RT heart Failure .
SYMPTOMS :-
1. Fatigue (low cardiac output).
2. Palpitation (atrial fibrillation).
3. Haemoptysis (pulmonary congestion, pulmonary embolism).
4. Cough (pulmonary congestion).
5. Chest pain (pulmonary hypertension).
6. Oedema, ascites (right heart failure).
7. Thromboembolic complications (e.g. stroke, ischaemic limb).
SIGNS :-
• Dyspneaic,Mitral facies -malar flush(pinkish-purple patches on the cheeks).
• JVP normal or raised.
• Pluse usually irregular due to Atrial fibrillation.
LOCAL:
• Palpation : Apex tapping(loud S1), RV heave, loud P2 (pulmonary
hypertension)-diastolic thrill.
• Auscultation Loud first heart sound, opening snap ,Mid-diastolic murmur .
• Crepitations, pulmonary oedema, effusions.
• Signs of right-sided heart failure: in advanced disease.
Heart Sounds in MS :
• Diastolic murmur:
– Low-pitched diastolic rumble most prominent at the apex.
– Heard best with the patient lying on the left side in held expiration.
– Intensity of the diastolic murmur does not correlate with the
severity of the stenosis.
• Loud S1-Opening snap: heard at the apex when leaflets are still mobile
– Due to the abrupt halt in leaflet motion in early diastole, after rapid
initial rapid opening, due to fusion at the leaflet tips.
– A shorter S2 to opening snap interval indicates more severe
disease.
4
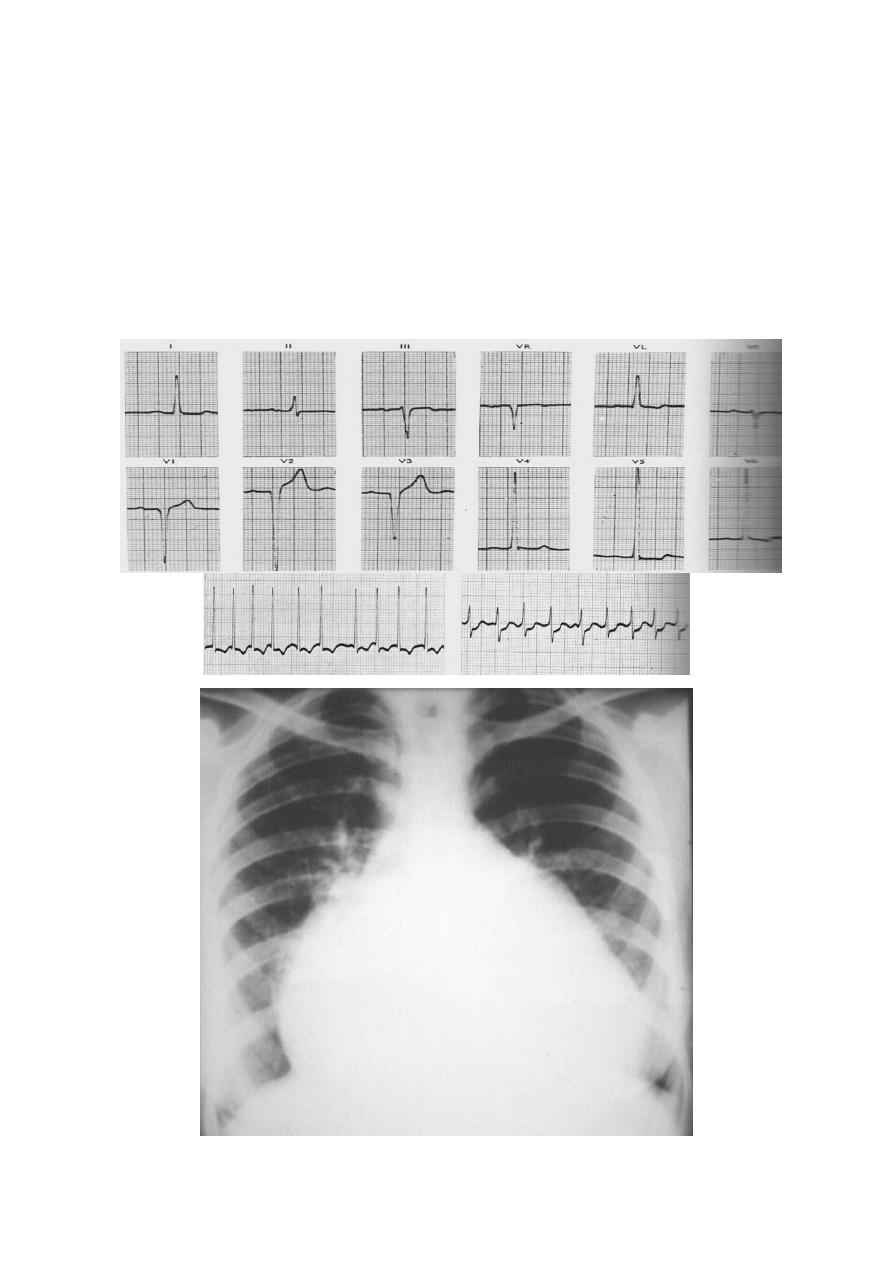
Investigations:
• ECG: may show atrial fibrillation and LA enlargement.
• CXR: LA enlargement and pulmonary congestion. Occasionally calcified MV
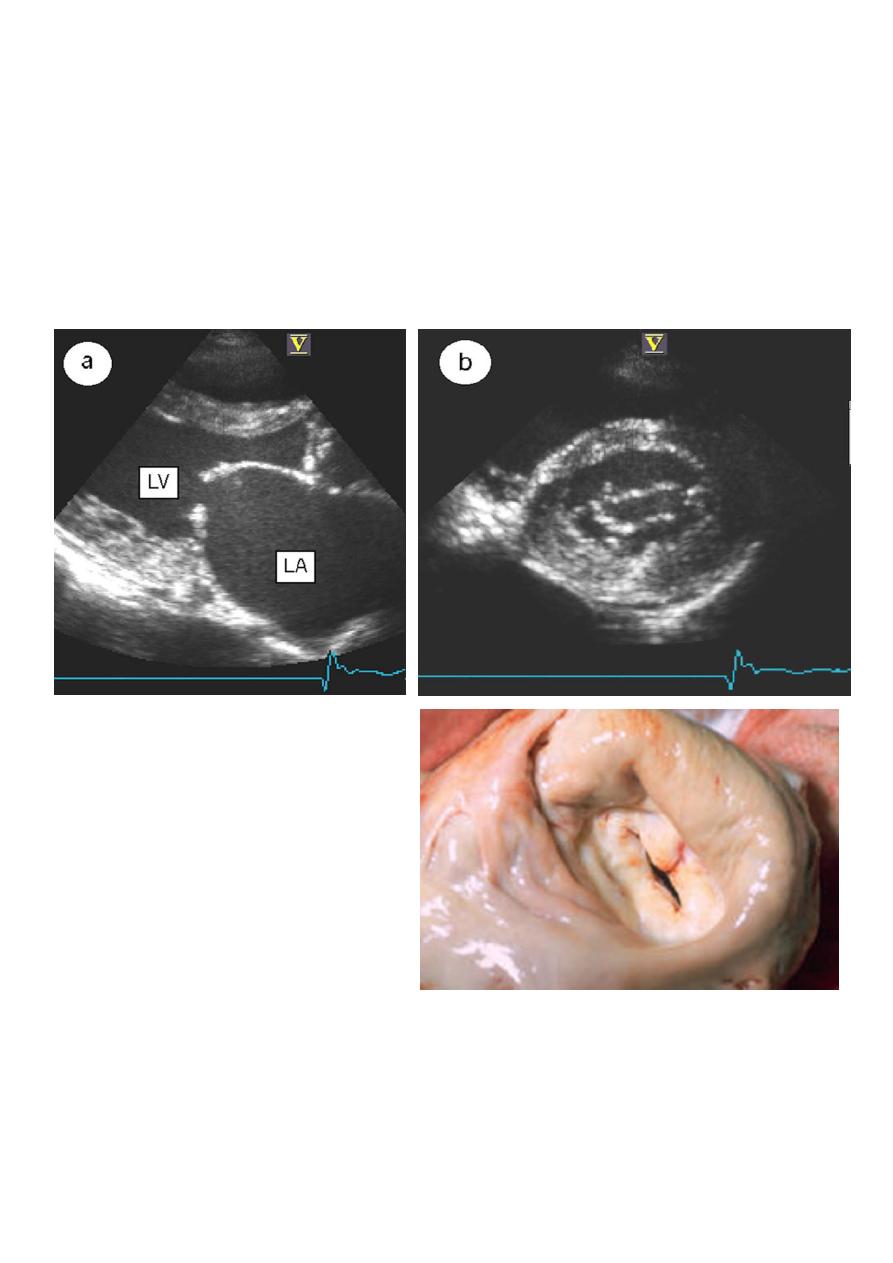
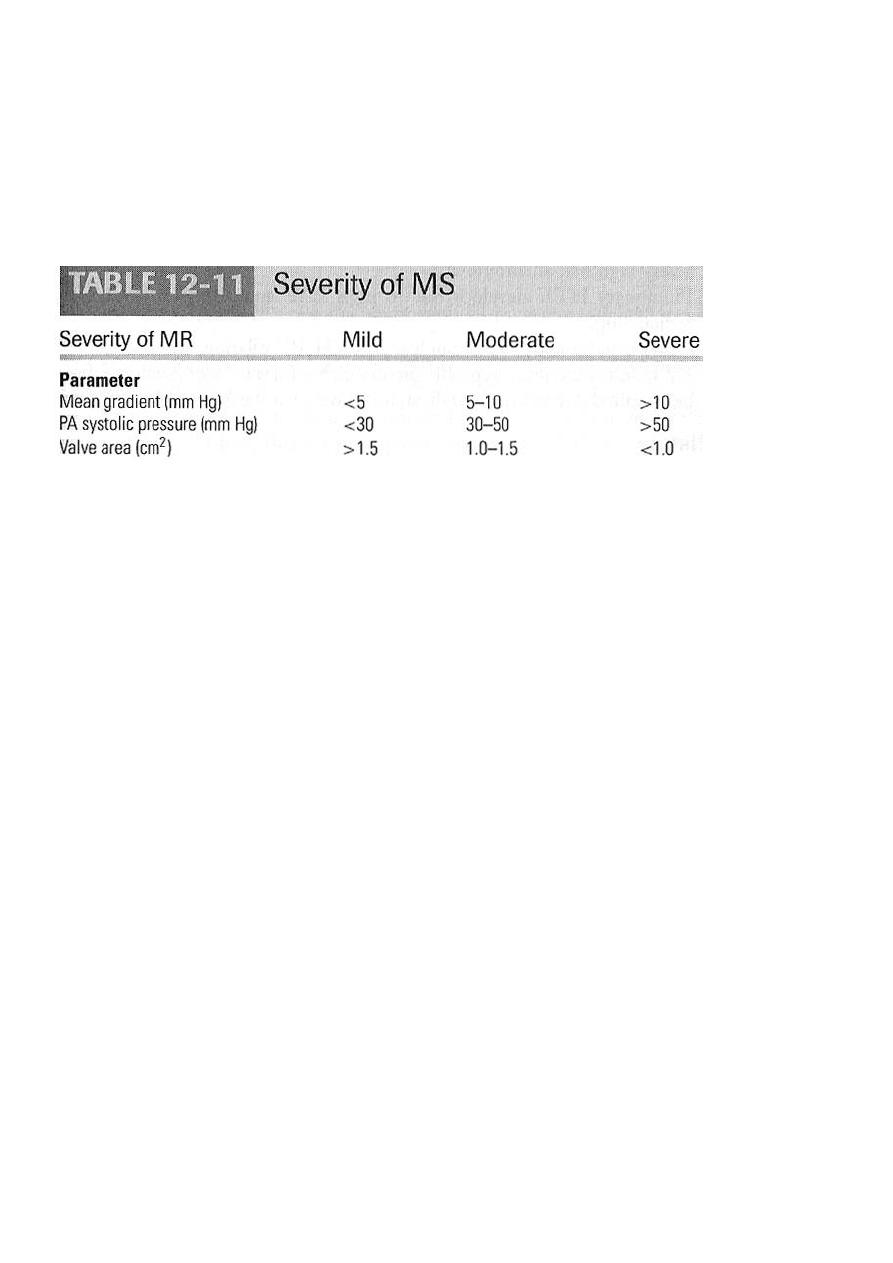
• ECHO: The GOLD STANDARD for diagnosis. Asses mitral valve mobility, gradient
and mitral valve area,other lesions
• Cardiac catheterization
Management of MS :
Serial echocardiography:
– Mild: 3-5 years
– Moderate:1-2 years
– Severe: yearly
Medications: MS is a mechanical problem and medical therapy does not
prevent progression
–
-blockers, CCBs, Digoxin which control heart rate in atrial fibrillation
– Anticoagulant to prevent thromboembolization in atrial fib.
– Duiretics for fluid overload and pulm .congestion.
Rheumatic fever prophylaxis
IE prophylaxis: Patients with prosthetic valves or a Hx of IE for dental
procedures.
Nonmedical management :
1. Mitral balloon valvuloplasty and valve replacement(MVR).
2. Symptomatic mod/sever MS +favorable anatomy.
3. Asymptomatic mod/sever MS +pulm.HTN +favorable anatomy(Isolated mitral
stenosis • No mitral regurgitation, Mobile, non calcifiedvalve/subvalve
apparatus on echo • LA free of thrombus ).
4. Valve replacement(MVR).
5
Mitral Regurgitation :
Chronic Mitral Regurgitation Overview :
Definition: Backflow of blood from the LV to
the LA during systole
Mild (physiological) MR is seen in 80% of
normal individuals.
Acute MR :
Endocarditis
Acute MI
Malfunction or disruption of prosthetic valve.
Etiologies of Chronic Mitral Regurgitation :
1. Mitral valve prolapse .
2. Dilatation of the LV and mitral valve ring (e.g. coronary artery disease,
cardiomyopathy).
3. Rheumatic fever.
4. Ischaemia or infarction of the papillary muscle.
5. Myocardial infarction.
Mitral valve prolapse :
1. Occurs in 5% of adults
2. Floppy MV, caused by congenital anomalies or degenerative myxomatous changes,
Marfans syndrome.
3. Asymptomatic,atypical chest pain ,benign arrythmia ,small risk of embolic stroke
4. Mid systolic click and late systolic murmur
5. Prognosis is good.
Pathophysiology of MR :
Pure Volume Overload
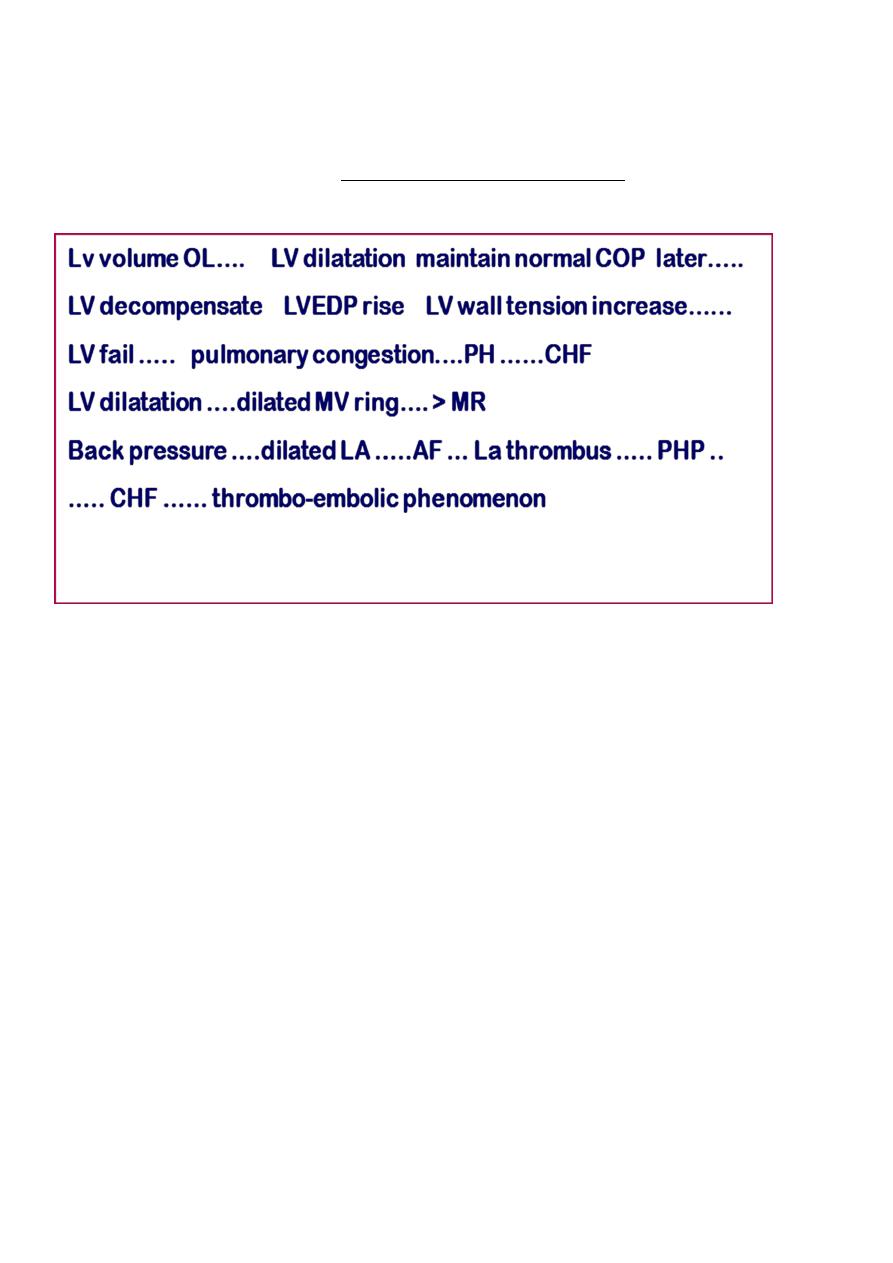
6
Compensatory Mechanisms: Left atrial enlargement, LVH and increased
contractility,LV dilatation.
– Progressive left atrial dilation and right ventricular dysfunction due to pulmonary
hypertension.
– Progressive left ventricular volume overload leads to dilation and progressive heart
failure.
SYMPTOMS :
1. Asymptomatic
2. Dyspnoea (pulmonary venous congestion)
3. Fatigue (low cardiac output)
4. Palpitation (atrial fibrillation, increased stroke volume)
5. Oedema, ascites (right heart failure)
Systemic embolization { stroke , ischaemic limb etc.. }
Signs :
1. Pulse :Atrial fibrillation/flutter.
2. Cardiomegaly: displaced hyperdynamic apex beat
3. Apical pan.systolic murmur ± thrill • Soft S1, apical S3.
4. Signs of pulmonary venous congestion (crepitations, pulmonary oedema, effusions)
5. Signs of pulmonary hypertension and right heart failure.
7
Investigations in MR :
• ECG: May show, LA enlargement, atrial fibrillation and LV hypertrophy with
severe MR
• CXR: LA enlargement, central pulmonary artery enlargement.
• ECHO: Estimation of LA, LV size and function. Valve structure assessment
– TEE if transthoracic echo is inconclusive
• Cardiac catheterization.

8
Management of MR :
• Medications
• Mild –moderate MR can be treated medically
a) Vasodilator such as hydralazine,ACE inhibitors
b) Rate control for atrial fibrillation with
-blockers, CCB, digoxin in
AF
c) Anticoagulation in atrial fibrillation and flutter
d) Diuretics for fluid overload
• Serial Echocardiography:
– Mild: 2-3 years
– Moderate: 1-2 years
– Severe: 6-12 months
• IE prophylaxis: Patients with prosthetic valves or a Hx of IE for dental
procedures.
Surgical :
• Repair or MVR
• Sever even asymptomatic
• Progressive cardiomegaly or progressive deterioration of LV function by ECHO
Treatment of Acute MR :
• Balloon Pump
• Nitroprusside even if hypotensive
• Emergent Surgery