Empyema
Empyema:This is a collection of pus in the pleural space, which may be as thin as serous fluid or so thick that it is impossible to aspirate, even through a wide-bore needle.
Microscopically, neutrophil leucocytes are present in large numbers. An empyema may involve the whole pleural space or only part of it (‘loculated’ or ‘encysted’ empyema) and is usually unilateral. It is always secondary to infection in a neighbouring structure, usually the lung, most commonly due to the bacterial pneumonias and tuberculosis. Over 40% of patients with community acquired pneumonia develop an associated pleural effusion (‘para-pneumonic’ effusion) and about 15% of
these become secondarily infected.
Other causes are infection of a haemothorax following trauma or surgery, oesophageal rupture, and rupture of a subphrenic abscess through the diaphragm.
The pus in the pleural space is often under considerable pressure, and if the condition is not adequately treated, pus may rupture into a bronchus, causing a bronchopleural fistula and pyopneumothorax, or track through the chest wall with the formation of a subcutaneous abscess or sinus, so-called empyema necessitans.
Clinical assessment:
An empyema should be suspected in patients with pulmonary infection if there is severe pleuritic chest pain or persisting or recurrent pyrexia, despite appropriate antibiotic treatment. In other cases, the primary infection may be so mild that it passes unrecognised and the first definite clinical features are due to the empyema itself. Once an empyema has developed, systemic features are Prominent.
Investigations:
Chest X-ray appearances may be indistinguishable from those of pleural effusion, although pleural adhesions may confine the empyema to form a ‘D’-shaped shadow against the inside of the chest wall .When air is present as well as pus (pyopneumothorax), a horizontal ‘fluid level’ marks the air/liquid interface.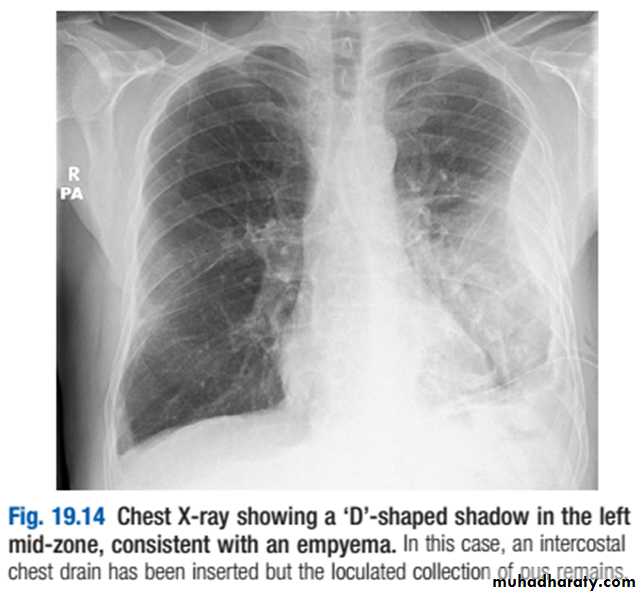
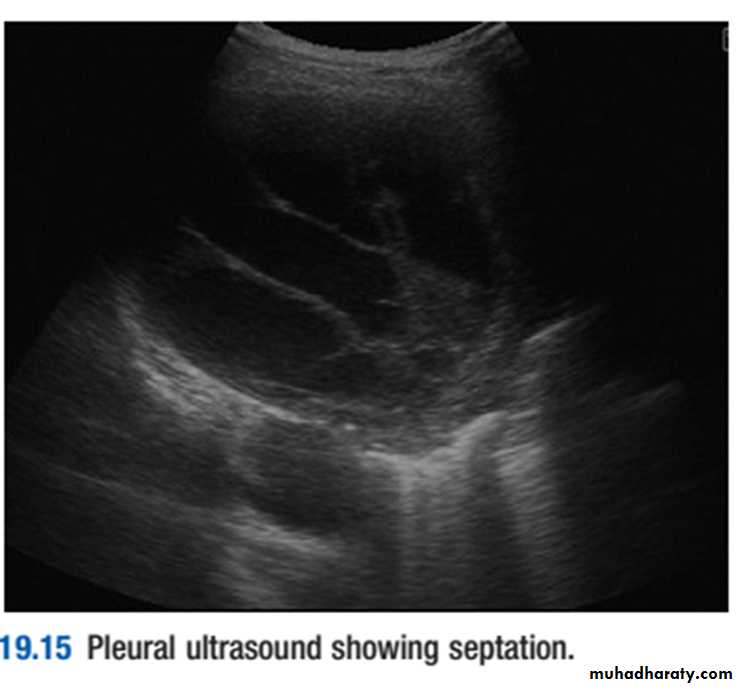
Ultrasound shows the position of the fluid, the extent of pleural thickening and whether fluid is in a single collection or multiloculated, containing fibrin and debris .
CT provides information on the pleura, underlying lung parenchyma and patency of the major bronchi.
Ultrasound or CT is used to identify the optimal site
for aspiration, which is best performed using a widebore needle. If the fluid is thick and turbid pus, empyema is confirmed. Other features suggesting empyema are a fluid glucose of less than 3.3 mmol/L (60 mg/dL), lactate dehydrogenase (LDH) of more than 1000 U/L, or a fluid pH of less than 7.0 .However, pH measurement should be avoided if pus is
thick, as it damages blood gas machines. The pus is
frequently sterile on culture if antibiotics have already
been given. The distinction between tuberculous and
non-tuberculous disease can be difficult and often
requires pleural biopsy, histology and culture.
Management:
An empyema will only heal if infection is eradicatedand the empyema space is obliterated, allowing apposition of the visceral and parietal pleural layers. This can only occur if re-expansion of the compressed lung is secured at an early stage by removal of all the pus from the pleural space. When the pus is sufficiently thin, this is most easily achieved by the insertion of a wide-bore intercostal tube into the most dependent part of the empyema space. If the initial aspirate reveals fluid or frank pus, or if loculations are seen on ultrasound, the tube should be put on suction (−5 to -10 cm H2O) and flushed regularly with 20 mL normal . If the organism causing the empyema can be identified, the appropriate antibiotic should be given 2–4 weeks. Empirical antibiotic treatment (e.g. intravenous co-amoxiclav or cefuroxime with metronidazole)
should be used if the organism is unknown. Intrapleural
fibrinolytic therapy is of no benefit.
An empyema can often be aborted if these measures are started early, but if the intercostal tube is not providing adequate drainage – for example, when the pus is thick or loculated, surgical intervention is required to clear the empyema cavity of pus and break down any adhesions. Surgical ‘decortication’ of the lung may also be required if gross thickening of the visceral pleura is preventing re-expansion of the lung. Surgery is also necessary if a bronchopleural fistula develops.