
1
Forth stage
Medicine
Lec-1
د.ضياء الحمداني
1/1/2014
Renal vascular disease
Definition: diseases that involved the renal vascular system and affecting renal blood
supply which may lead to renal ischaemia,with subsequent acute or chronic kidney disease
and or secondary hypertension
Renal ischemia
Acute renal dis.
Chronic renal dis.
Hypertension.
Renovascular disease.
Large vessels disease.
Small vessels disease
Dis of intra-renal vessels
HU syndrome .
TTP
DIC
Malignant hypertension
Small-vessel vasculitis
Systemic sclerosis .
('cholesterol' emboli).
Large-vessel disease
renal artery stenosis.
Which could be due to:
2
i.
Atherosclerosis:
ii.
Fibromuscular hyperplasia.
iii.
Large or medium vessels vasculitis
.
Renal artery stenosis:
It could be chronic, gradual dis .
Sudden occlusion.
The Aetiology Renal artery stenosis (chronic):
> 70%. reduction of renal blood flow is clinically significant.
Fibro muscular hyperplasia.
Atherosclerosis.
vasculitis, (Takayasu's arteritis ,polyarteritis nodosa).
Atherosclerosis
It’s the common cause, in older patients.
Site (it is an ostial stenosis ).
associated with atherosclerosis within the aorta ,and other vessels .
many patients die from coronary, cerebral or other vascular disease rather than
renal failure.
may cause renal failure (ischemic nephropathy).
3
fibromuscular dysplasia
it is uncommon congenital disorder of unknown cause affecting the media ('medial
fibroplasia') causing narrowing of the artery but rarely leads to total occlusion .
Age (< 50 years).
It most commonly presents with hypertension in patients aged 15-30 years.
Sex (Female > Male ).
It may be associated with disease in other arteries; for example, carotid artery
dissections
Clinical presentation
a. Hypertension.
b. Renal impairment(15%).
c. Renal infarction.
When one should suspect RAS:
How patient present :
Sudden , severe, uncontrolled hypertension .
Hypertensive patient with Recurrent attack of pulmonary oedema .
Hypertension with peripheral vascular disease of lower limbs .
Both kidneys are asymmetrical in their size .
Raised urea and creatinine after usage ACE inhibitors as antihypertensive drug
Sudden occlusion(renal infarction).
Causes (atheroma,emblus).
Loin Pain.
Hematuria.
Hypertension.
Probably Renal failure ??.
Investigations
Blood urea and serum creatinine.
serum K may be low?? (high BP &low K)
4
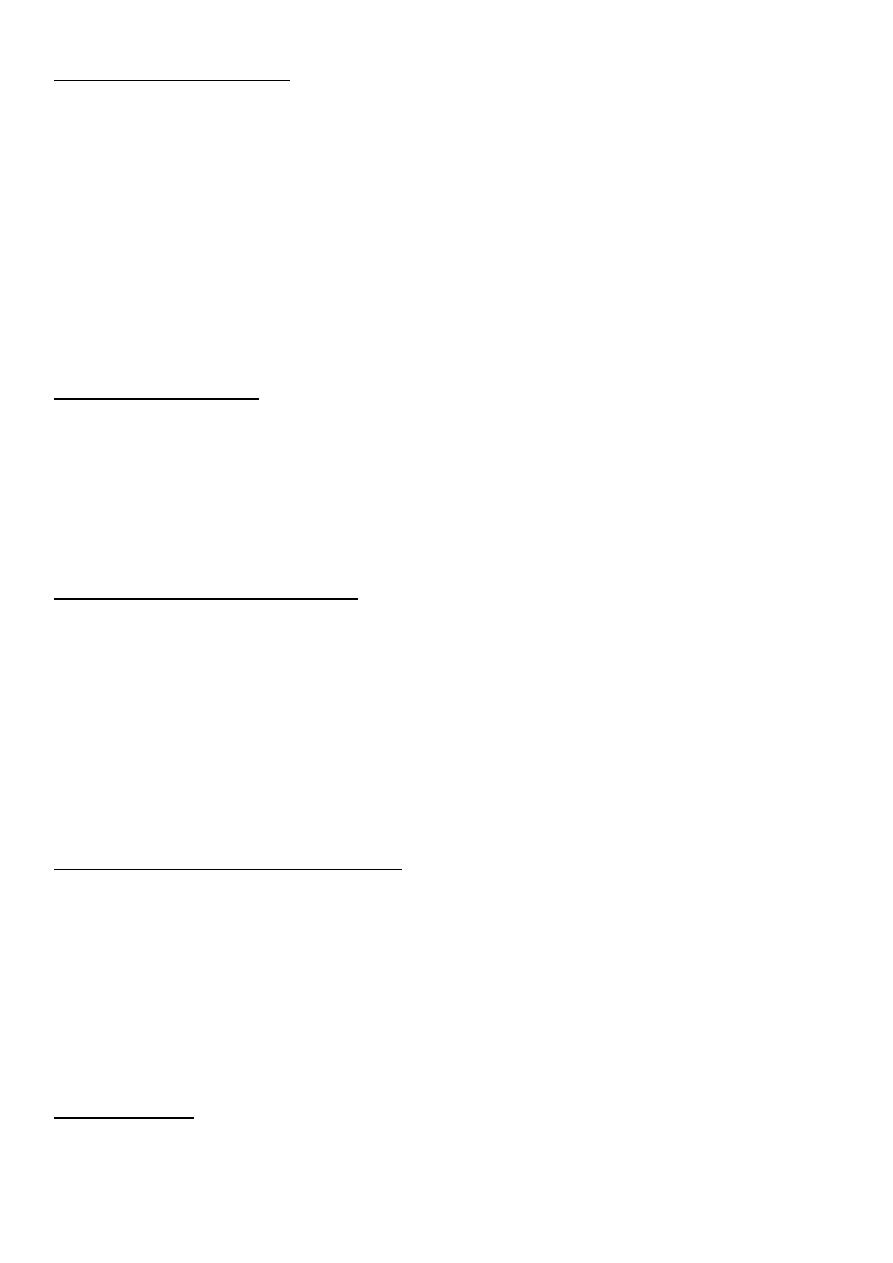
Ultrasound
may reveal a discrepancy in size between the two kidneys.(small size kidney).
Doppler study of renal artery.
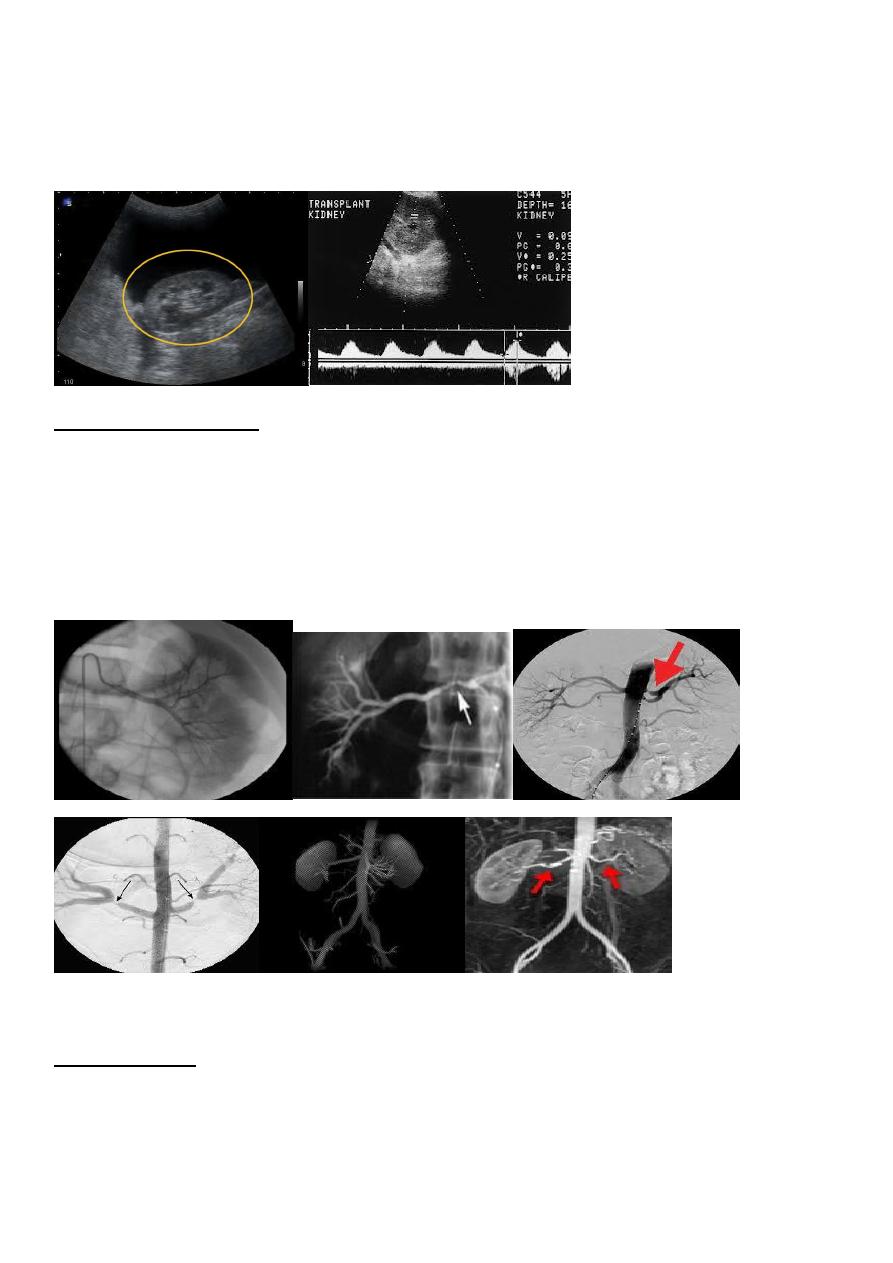
Vascular imaging is required to diagnose renovascular disease
Angiogram or MRIA
.
Indicated in:
young patients with uncontrolled hypertension. ('resistant hypertension').
those who have a history of ‘recurrent ' pulmonary oedema .
accelerated phase ('malignant') hypertension.
those in whom renal function is deteriorating
Management:
medical management
Antihypertensive drug with low-dose aspirin and lipid-lowering drugs; if no benefit:
angioplasty, with placement of stents in atherosclerotic disease areas to improve
primary patency rates and prevent rapid recurrence.

5
Angioplasty complication:
contrast nephropathy .
renal artery occlusion and renal infarction.
and atheroemboli from manipulations in a severely diseased aorta.
Small-vessel disease distal to the stenosis may preclude substantial functional
recovery.
Surgical intervention is rarely undertaken now for atherosclerotic disease, as it is
associated with high morbidity and mortality
Small vessels disease.
A number of conditions are associated with acute damage and occlusion of small
blood vessels (arterioles and capillaries) involving the kidney and other parts of the
body).
Characterized by microangiopathic haemolytic anaemia.
fragmented red cells can be seen on a blood film.
marked reduction in the platelet count.
in HUS the kidney microcirculation tends to be most affected.
In TTP the brain is commonly affected and involvement of the kidney is usually less
severe
Disseminated intravascular coagulation
consumption of clotting factors and platelets.
Precipitating conditions include:
septic shock.
obstetric complications.
disseminated cancer.
massive transfusion.
other causes .
'malignant') hypertension
Headache.
impaired vision .
Severe hypertensive retinopathy with papilloedema is almost always present.
manifestations of renal impairment.
some of the features of microangiopathy.
High blood pressure.
renal function is permanently lost in 20% of cases