Teeth extractionprinciples and technique


Methods of tooth extraction
Closed (intra-alveolar) extractionOpen ( trans-alveolar ) extraction
Principles & Techniques:
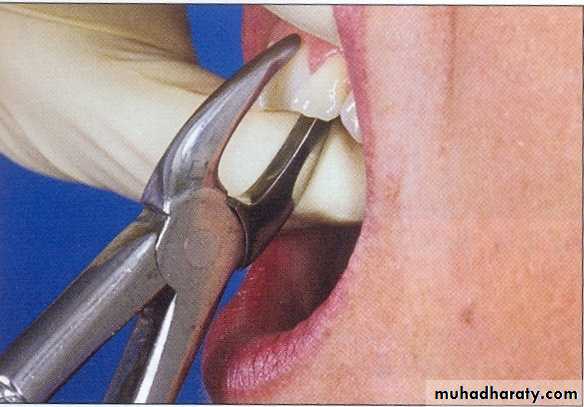
It is important that the principles & techniques of removing teeth are understood by all those in the dental profession who would pick up a pair of extraction forceps.Mechanical principles of tooth extraction
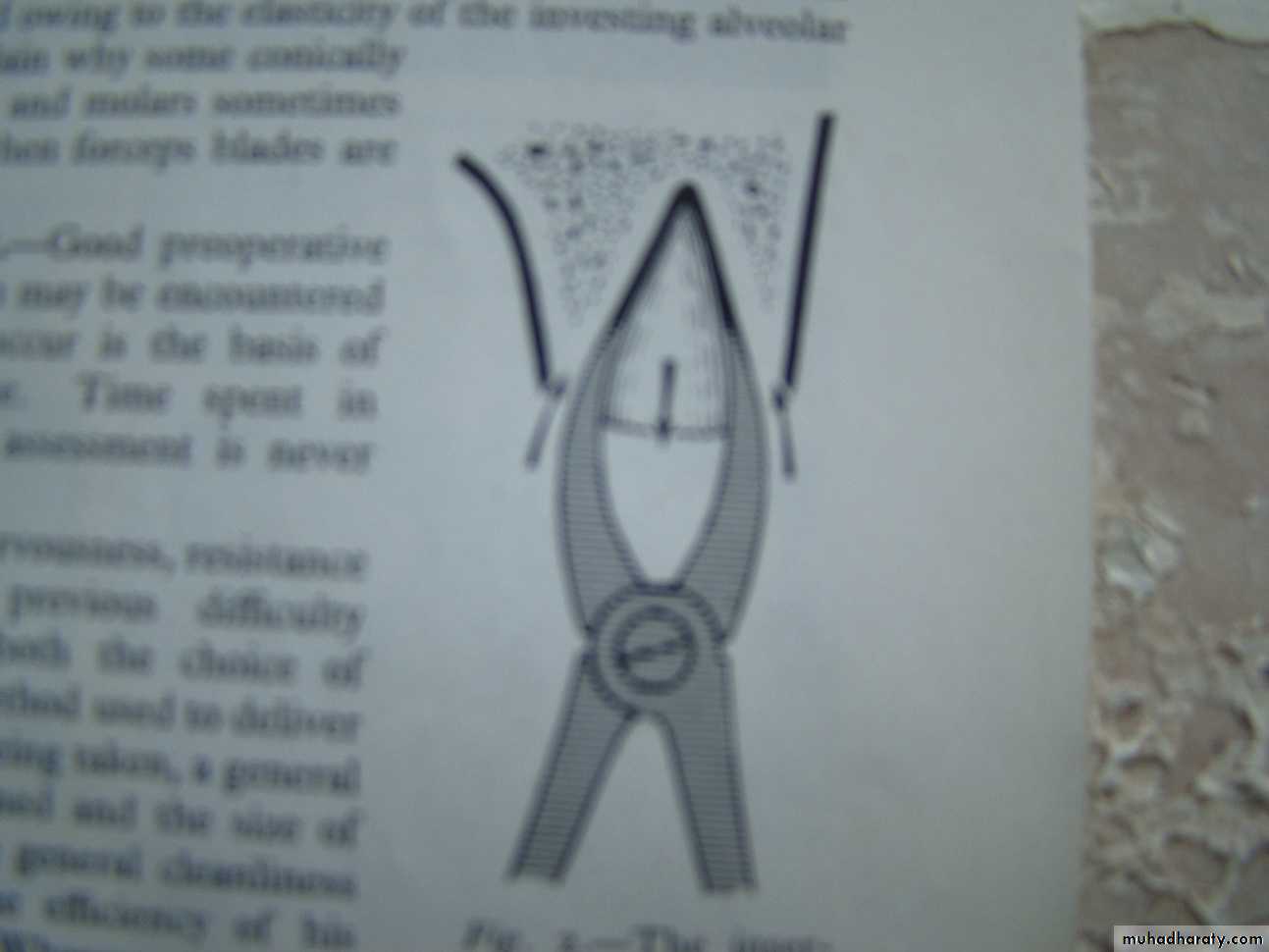
Applying displacing force: direct and indirect (forceps and elevator)Expansion of the tooth socket by lateral displacing movement (forceps )
Use of lever and fulcrum (elevator)
Insertion of a wedge or wedges between the root and the bony socket (elevator or forceps)
Bone removal using bur or chisel
Tooth sectioning .

Forces for tooth extraction
Force should be firm, smooth and controlledto separate gingival attachment, cutting periodontal ligament and expanding bone
Closing force
parallel apical force
Lateral force ( Bucco-lingual)
Rotational force ( 1ry & 2ry )
Parallel occlusal force
Closing and apical forces are maintained through out the course of the extraction until delivery is begun.
The primary force of expansion is the lateral force (buccal and lingual) with the buccal forces usually dominating .
The most effective force are those that are applied gradually and maintained briefly at the limit of achieved displacement .
Forces delivered with rapid ,short arcs are ineffective .
Rotational forces are essentially limited to either single or fused rooted teeth . These forces are particularly effective in rupturing the periodontal ligament ,while achieving only little alveolar expansion .
Upper central incisors has single conical root and yield to Primary rotational movement.
Upper lateral incisors: the tooth have slender roots which are often flattened on the mesial and distal surfaces. Fine bladed forceps, labio-palatal movement.Upper canine: Long strong root with a nearly triangular cross section. Great force needed. Fracture of the labial cortical plate may occur. Movement is labio-palatal.
Extraction Specifics
Maxillary 4 : Birooted, remove in the direction of least resistance. It is better for this tooth to be pulled out but in practice slight lateral movement is often required to deliver the tooth. Rotational forces for this tooth are contraindicated.
Maxillary 5 : Buccal bone thinner, this tooth yields to lateral movement buccally and then secondary rotational movement is made followed by pulling tooth occlusally in the buccal direction.
Maxillary 6 : The palatal root is usually straight; the mesio-buccal root apex has a severe distal curvature, By careful rocking of the tooth buccally, the palatal root may become loose and by a complete bucco-lingual movement will complete luxation. This tooth is removed without secondary rotational movements.
Maxillary 7 : Buccal alveolar plate offers least resistance, roots are straight and close together and may be fused, If this tooth is fractured, difficult to be removed.
Maxillary 8 : Crown placed more posterior than its roots, difficult application of forceps ,if mouth opened widely, coronoid process interferes with access and increase difficulty. Partial closure of the mouth with the mandible deviated towards the extraction site will aid in achieving access. Root is tilted backwards distally.
For all upper extractions it is necessary to push firmly in the long axis of the tooth during extraction.
Access for extraction of teeth far back in the mouth can be difficult so A further variation involves a step in the beaks of the forceps which enables us to put the beak on the upper 3rd molar whilst avoiding the lower lip
29-Mar-14
Mandibular incisors: Fine mesial and distal surfaces of the roots, apex curved distally, narrow bladed forceps are used to grasp them without trauma to the neighboring teeth, luxated labially.
Mandibular canine: Long and bulky, firmly embedded and in cross section it is nearly triangular in shape, it can be luxated by bucco lingual movement..
Mandibular 1st premolars: Tooth yields to buccal pressure with slight mesiodistal rotation.
Mandibular 2nd premolars: Straight and conical root , initial rotary movement can luxate the tooth changed to lateral bucco-lingual movement
Lower 1st molars: it may be Fracture during tooth extraction. The roots are wide and flat in the mesial and distal surfaces, great resistance ; loosened by buccolingual pressure and are best delivered by a figure eight secondary rotational movement.
Lower 2nd molars: More easier than lower 1st molars. As it is smaller , straight tapering and less divergent roots ;may be fused; use bucco-lingual pressure; removal is made in a buccal and upward direction
• Lower 3rd molars: Careful radiograph indicated . The roots of this tooth may be short, long , fused , multiple , diverged , curved or straight . The alveolar bone is extremely thick especially in the buccal side of the tooth where the external oblique ridge may project and so a lingual movement of forceps is dominated and in most cases an elevator is required.
Deciduous teeth extraction
Mouth is smallForming premolars are enclosed within the roots of their deciduous predecessors
Deciduous roots which can not be grasped by forceps should be displaced with Warwick James elevator using the bony socket as fulcrum.
Resorption occur in uneven manner
It is better to leave a small root fragment of a deciduous tooth to undergo resorption
Post-extraction procedures
Removal of tooth fragments or calculus
Granuloma or cyst removed by currate only when necessary
Gauze placement
Instruction
Analgesic