1
Forth stage
Obstetric
Lec-5
.د
أحمد جاسم
25/11/2015
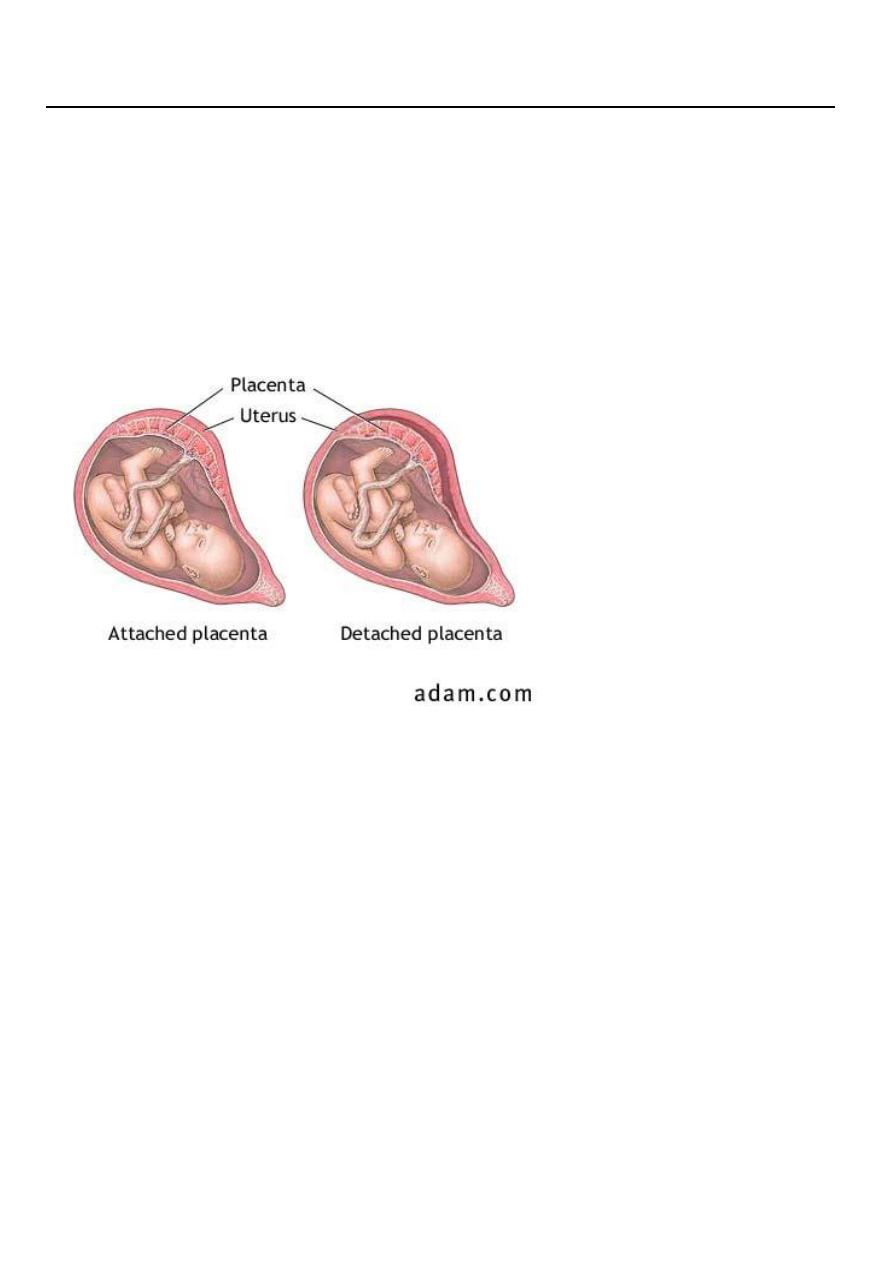
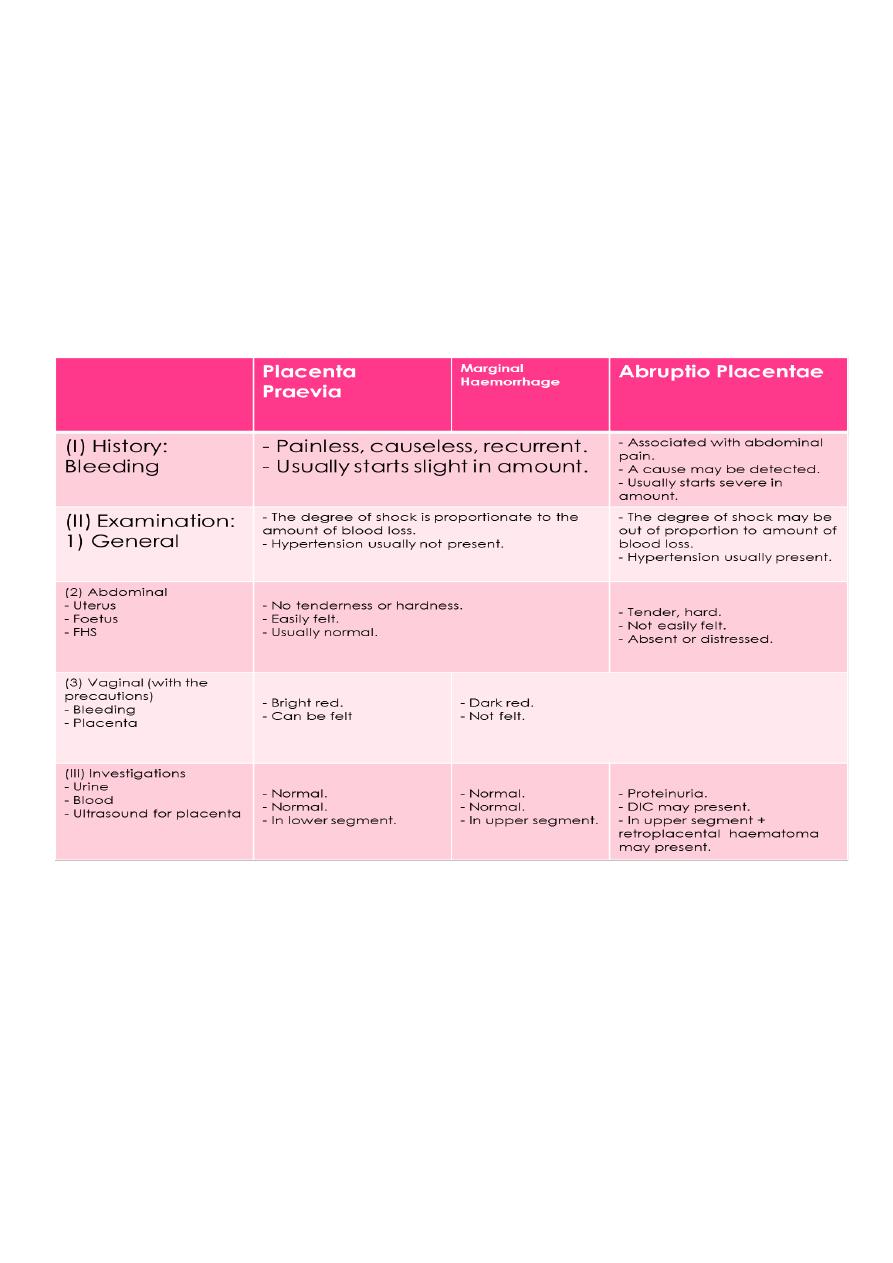
Abruptio Placentae (Accidental Haemorrhage)
Definition :
Premature separation of a normally situated placenta after the 24th week of
pregnancy and before delivery of the foetus.
Incidence :-
0.5-1%.
Aetiology :-
Unknown, but the following factors may be associated with:
1-Hypertensive disorders of pregnancy (30%) due to spasm and degenerative
changes in the decidual arterioles.
2-Trauma as during external version.
3-Sudden drop of intrauterine pressure as rupture of membranes in
polyhydramnios.
4-Folate deficiency and may be vitamin C,K, or E deficiency.
5-Passive congestion of the uterus due to pressure of the gravid uterus on the
inferior vena cava.
6-Torsion of the uterus.
7-Smoking.
2
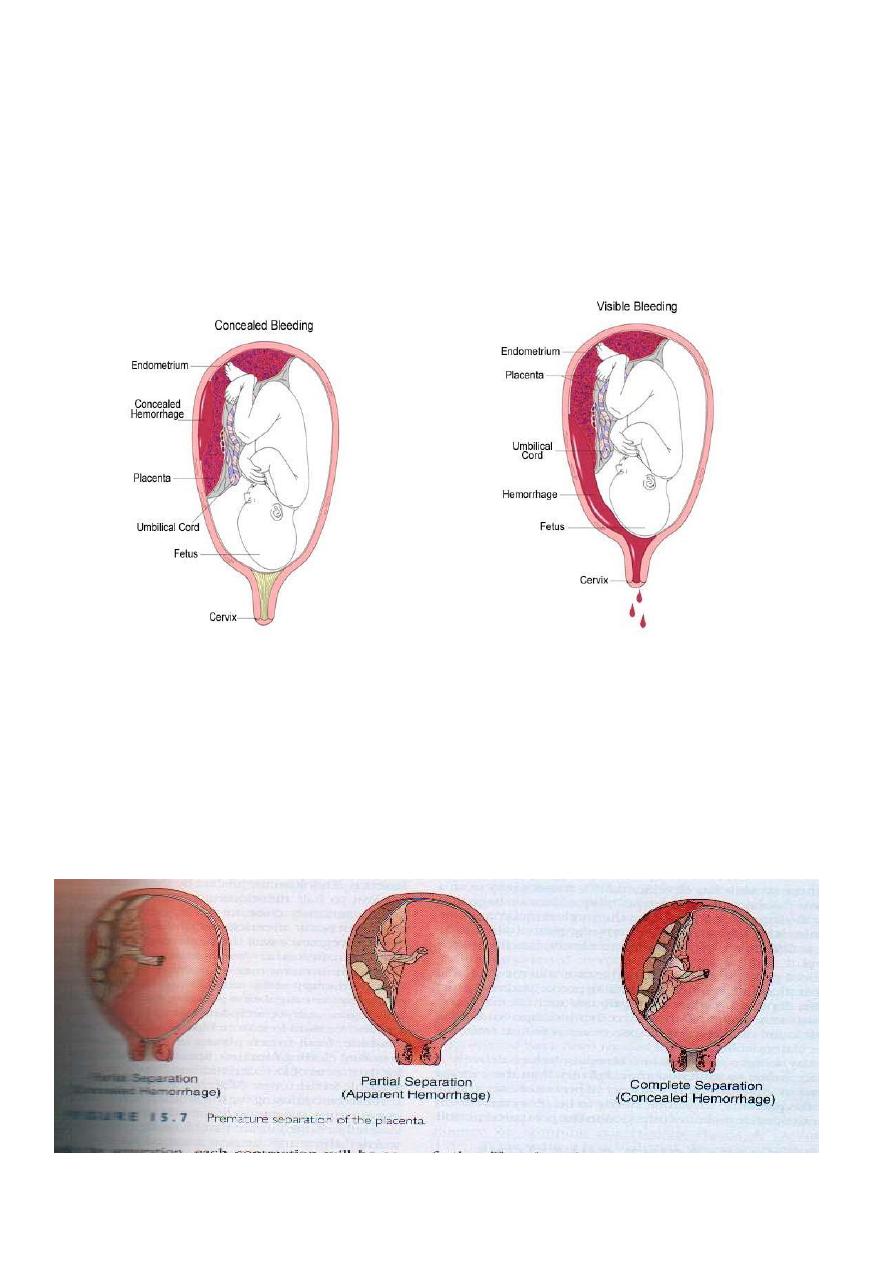
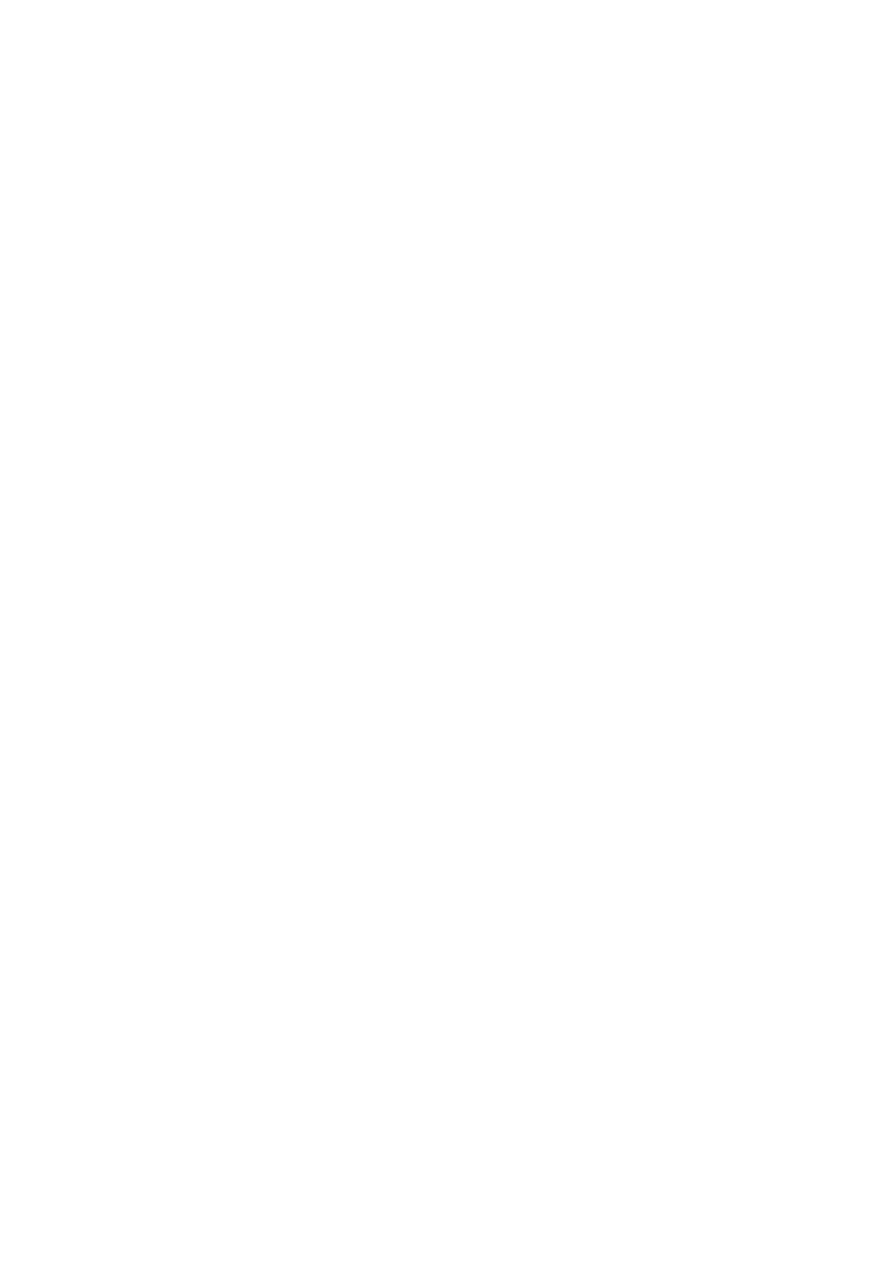
Pathogenesis :-
Separation of the placenta results in formation of a retroplacental haematoma
and its extension leads to more separation of the adjacent placental tissue
(concealed haemorrhage).
Ultimately the blood reaches the placental margin and tracks between the
membranes and uterine wall to escape from the cervix (revealed haemorrhage).
The presence of concealed and revealed haemorrhage together called mixed
variety. Thus the three varieties are actually different presentations to one
process.
If separation of the membranes does not occur, there is progressive disruption of
the placental tissue and intravasation of blood through the myometrium even up
to the peritoneal coat resulting in Couvelaire’s uterus.

3
-Thromboplastin-like substances are released from the damaged placental site
and passed to the maternal circulation initiating the process of disseminated
intravascular coagulopathy (DIC).
-Acute renal failure may result from renal ischaemia caused by:
1-hypovolaemia,
2-reflex spasm of the renal vessels due to sudden distension of the uterus,
3-occlusion of the glomerular capillaries by microthrombi from DIC,
4-and /or kidney pathology caused by hypertensive states of pregnancy.
-Early stage of renal ischaemia causes renal tubular necrosis which is
reversible. Later on, irreversible cortical necrosis occurs.
-Postpartum haemorrhage is common as the result of:
1-uterine damage,
2-uterine atony,
3-coagulation failure (DIC),
4-anaemia,
5-inhibition of myometrial activity by fibrinogen degradation products (FDP)
present in DIC, and
-Sheehan’s syndrome: severe antepartum and / or postpartum haemorrhage
leads to necrosis of the anterior pituitary.
Diagnosis :-
Symptoms :
1-Acute constant severe abdominal pain which may be localised or diffuse.
2-Dark vaginal bleeding results from escape of blood from the retroplacental
haematoma.
3-Cessation of foetal movement is common.

4
Signs :
A.General examination:
-Shock is usually present and may be marked and not proportionate to the
amount of visible bleeding due to:
1-concealed and/ or revealed haemorrhage,
2-overdistension of the uterus and damage of the myometrium causing
neurogenic shock.
-Blood pressure is;
1-subnormal due to haemorrhage,
2-normal due to falling from previous hypertension
3-high due to slight bleeding in hypertensive patient.
-Tachycardia.
B. Abdominal examination:
-Uterus is large for date and increasing gradually in size due to retained blood.
-Uterus is very tender and hard (board-like).
-Foetal parts are difficult to be felt.
-FHS may be absent due to foetal death in severe cases or distressed in mild
cases.
C. Vaginal examination:
Done under the same precautions in placenta praevia may reveal:
-Vaginal bleeding which is dark as it is retained for some time before escape.
-If the cervix is dilated the placenta is not felt.
Differential diagnosis :
-Other causes of antepartum haemorrhage.
-Other causes of acute abdomen
5
Investigation :
-Ultrasound: detects normally sited placenta with retroplacental haematoma
that may dissect the placental margin.
-Tests for DIC.
Treatment :
There is no treatment to stop placental abruption or reattach the placenta , it
depends on:
-Severity of condition.
-Gestational age.
-maternal condition.
-Fetal condition.
-Associated complications.
The main principles of treatment in obvious cases of placental abruption are:
1. Early delivery.
2. Adequate blood transfusion.
3. Adequate analgesia.
4. Detailed monitoring of maternal condition.
5. Assessment of fetal condition.
-At home :-
The same as in placenta praevia.
-At hospital :-
As placenta praevia regarding Assessment of the patient’s condition, general
and abdominal examination and resuscitation.
Blood volume preservation.
Ultrasonography.
6
According to this principle the patient need:
1-Admission to hospital.
2-Insert 2 large bore IV canula and infusion with normal saline, ringer lactate,
blood, fresh frozen plasma.
3-Send blood for cross match of 4 units of blood, and send for Hb and coagulation
studies.
4-Urinary catheter to monitor U.O.P.(urinary out put ) hourly.
5-Input and output chart.
6-C.V.P.measurment and strict fluid balance.
7-Early delivery is vital.
Delivery :-
-Patient with abruptio placenta has to be delivered and usually there is no place
for conservative treatment.
-Amniotomy + oxytocin if:
1-bleeding is not severe,
2-vertex presentation,
3-the cervix is partially dilated.
4-adequate pelvis with no soft tissue obstruction,
Advantages of amniotomy:
1-It reduces the intrauterine tension, intravasation of blood between myometrial
muscles and its damage.
2-Reduces the pain and shock.
3-Reduces the incidence of renal failure.
4-Stimulates the onset of labour and improves uterine contractions pattern.
Caesarean section is indicated in:
1-Severe haemorrhage whether the foetus is dead or alive.
2-Living foetus and labour is expected to be longer than 6 hours e.g. closed
cervix.

7
3-Foetal distress.
4-Failure of progress after amniotomy + oxytocin.
Other indications for C.S. as contracted pelvis, malpresentations and elderly
primigravida.
Postpartum :
The patient is more liable for postpartum haemorrhage so oxytocin is continued
after delivery of the foetus, methergin is given with delivery of the shoulders if
there is no hypertension with continuous massage of the uterus.
Complications :
A.Effects on the mother
1.Hypovolemic shock.
2.DIC (Disseminated Intravasculer Coagulopathy)
which means hypofibrinogenemia, decrease platlet, increase FDP (Fibrin
Degradation Product). triggered by tissue thromboplastin.
3.Acute renal failure Which occurs due to :-
A. Hypovolemia.
B. Hypotension.
C. DIC (microthrombi in kidneys).
4.post-partum haemorrhage (ppH) Which occurs due to:
A. Coagulation failure.
B. Poorly contracting couvelair uterus.
C. Predisposing factors for antepartum haemorrhage (APH) as polyhydramnios,
multiple pregnancy.
5.Feto-maternal haemorrhage
6.It can lead to sensitization of mother especially if Rh –ve mother. So all
mother who are Rh-ve should have Kleihaure test to quantify size of transfer
and appropriate dose of anti-D immunoglobin.
7.Maternal mortality due to complication.
8.recurrence of abruptio placentae 10%
8
B. effects on fetus :-
1.increase in perinatal mortality and the increase depend on:
-Size of abruption.
-Interval to delivery.
-Gestational age at delivery.
-Other associated factors.
2.IUGR (Intra Uterine Growth Restriction) in few cases which treated
conservatively.