Thyroid gland
Professor Nashwan Q MahgoobDepartment of Surgery/Medical College/University of Mosul

Embryology
The thyroid gland developed at the fourth week of gestation.A diverticulum from the floor of the primitive pharynx, (thyroglossal duct ) passes from foramen caecum at junction of anterior 2/3 and posterior 1/3 of the tongue and descend anterior to neck structures toward the root of the neck forming two lobes linked by isthmus.
During the fifth week of gestation, the thyroglossal duct lumen starts to obliterate, and disappears at eighth week of gestation.
The fourth pharyngeal pouch give rise to Para follicular cells ( C cell) which amalgamate with the lobes of the gland.

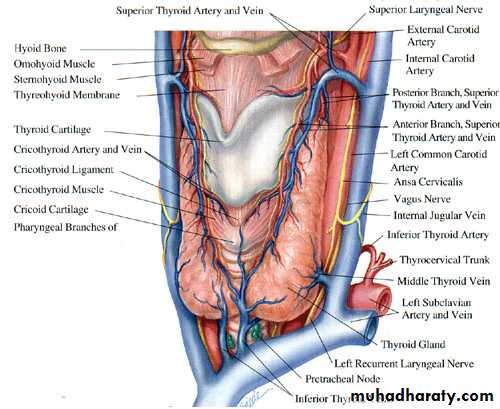
Anatomy
• It composed of 2 lobes linked• by isthmus, it lies over the second, third and fourth tracheal rings. WT about 20 to 25 gm, its heavier in female, its just visible in normal person(not palpable normaly).
• A pyramidal lobe is a long, narrow projection of thyroid tissue extending upward from the isthmus. It represents a vestige of the embryonic thyroglossal duct. It present in 50% of individuals.
The functioning unit is the lobule, which composed of follicles lined by cubical epethelium which synthesize thyroglobulin that released into the colloid and secreted to the circulation.

Anatomy
Arterial supply1-superior thyroid arteries, which arise from the external carotid arteries.
2- inferior thyroid arteries, which arises from the thyrocervical trunk
of the subclavian artery.
venous drainage
1- Superior thyroid vein at the upper pole.2- Middle thyroid vein at the middle part of the lobe, enter the internal jugular vein.
3- inferior thyroid veins from each lower pole are which drain into the innominate vein
• Lymphatic drainage is to level II, III. IV. VI and VII

physiology
Steps of thyroid H formation1- Trapping of iodide from blood.
2-Oxidation of iodide by the effect of peroxidase Enz.
3-Binding to tyrosene to form monoiodotyrosene.
4-Coupling of monoiodotyrosene to form diodotyrosene.
5- Formation of tri and tetra iodo tyrosene (T3, T4)
6- Storage of H in form of thymoglobulin
7- Release of H in response by effect of dehalogenase Enz
8-Binding of most of the released H to binding protein, small amount remain free in the circulation

The chief stimulator of thyroid hormone synthesis and secretion is thyroid
stimulating hormone (TSH) from the anterior pituitary.TSH is under control of Thyroid-releasing hormone (TRH) from
the hypothalamus
Both under negative feed back of T3.
Physiology
: The function of thyroid gland are1- Secrete thyroid hormones.
2- Secrete calcetonen hormone.
The functions of thyroid H are
1- Facilitate growth and development.
2- Facilitate carbohydrate protein and fat metabolism.
3- Increase oxygen consumption by the tissue, basal metabolic rate, and heat production.
4- Increase oxygen release from HB.
5- Increase oxidative phosphorelation.
6- Augmentation of adrenalin and noradrenalin function.
7- Positive inotropic and chronotropic effects on the heart.
• Daily requirement of iodide is 0.1 to 1.5mg .
• The free form of T3 and T4 are the active form.
• T3 is four times more powerful than T4
• T3 less adherent to the binding protein.(98% in comparison with 99.9% for T4)
• Half life of T3 is 1 to 3 days (8 to14 days for T4).
• All T4 change to T3 at the cellular level.
• The normal thyroid gland produces about 80% T4
Thyroid function tests
A- Hormone measurement1-Total T3 = 1.2 to 2.8 nmol\L
2-Total T4 = 150 nmol\L
3-TSH test: IV dose of TSH causing elevation of T3 and T4 normally but not in hypothyroidism.
4-TRH stimulation test: injection of TRH causes secretion of TSH from pituitary gland normally but not in case of Thyrotoxicosis (suppression) niether in pituitary failure.
These tests become obsolete by now and replaced by measuring of:
1-freeT4=10-30nmol\L2-freeT3=0.3-3.3nmol\L
3-TSH = 0.5 to 5 mU\L which is the most sensitive and specific test for the diagnosis of hyper or hypothyroidism and for optimizing T4 therapy.
4-Autoantibody assessment: include TPO (thyroid peroxidase) normally less than 25nmol\l, and anti thyroglobulin anti body.
They do not determine thyroid function, but indicate the underlying disorder, usually an autoimmune thyroiditis.

Thyroid function tests
B-Thyroid scanning: iodine 123 (123I) and iodine 131 (131I) and Technetium Tc 99mThe images Provides size and shape of the gland and functional activity.
Its principal value is in the toxic patient with a nodule or nodularity for localization of over activity in the gland


C- Biopsy1- FNA.2-Core biopsy3- Incisional biopsy.4-Excisional biopsy.

D-Imaging study1-plan X ray of the neck: to evaluate the trachea, retrosternal extension and cervical spine . 2-Ultrasound: distinguishing solid from cystic masses, information about size and multicentricity, assess cervical lymph nodes and guides for FNAC.




3-CT scan and MRI: assessment of known malignancy, extent of retrosternal and occasionally recurrent
Goitres.
Congenital anomalies
1-Ectopic location: due to arrest of descend of the thyroglossal duct. It my be Lingual, supra or infrahyoed or mediastinal.
Lingual thyroid
Thyroid tissue arrested at the posterior third of the tongue. Its more common in female.It may be the only thyroid tissue.
Clinically: The mass causes dysphagea, dysphonea and dyspnoea.
Degeneration or bleeding may result in sudden increase in size and suffocation.

Diagnosis: by RAIU (radio active isotope uptake)or by CT.
Treatment : thyroid ablation using I131 with life long replacement therapy.Surgery (intra-oral excision of the mass) is indicated in very large mass or in case of suffocation or suspicious of malignant changes.
Thyroglossal cyst

Persistent of part of thyroglossal
duct causing cyst, sinus, or fistulae.40% present < 10 years of age.
75% present as midline swellings.
The most common site is sub-hyoid.
Can occur at the base of the tongue, supra or infra hyoid, or at thyroid cartilage.
Male : female ratio is equal, Often present as an infected cyst due lymphoid tissue in the cyst wall.
Most fistulae are acquired following rupture or incision of infected cyst
The cyst move upward on protrusion of the tongue as well as on swallowing.


Complication:1-Infection, and abscess formation2-Fistula which is either due to incision of an abscess or inadequate surgical removal 3-Malignant changes


Treatment(Sistrunk Operation) excision of the cyst middle 1/3 of hyoid bone up to the base of tongue.

Goiter
simpletoxic
inflammatory
tumour
miscellaneous
defuse
multinoduler
Solitary nodule
Graves
Toxic nodule
Toxic Multinoduler
Riedel
Hashemotodequervian
Benign
malignantBacterial
Amyloidoses
hydatid
Simple defuse goiter
Due to excessive TSH secretion in response to low circulating T3 andT4, result in uniform increase in the size of the thyroid gland. its more common in female owing to the presence of oestrogen receptors in thyroid tissue.Causes:
1- Iodine deficiency: due to low intake (endemic goiter).2- Increase demand to hormone : in pregnancy, lactation and teenage (physiological goiter).
3- Goiterogenic food: Brasseca family like cabbage, kale, rape, and yellow turnips.
4- Drug: antithyroid, PAS, high dose of iodine.
5- Dyshormogeneses: deficiency in Enz responsible for hormone production (sporadic goiter).
6- Failure of intestinal absorption may produce iodine deficiency.
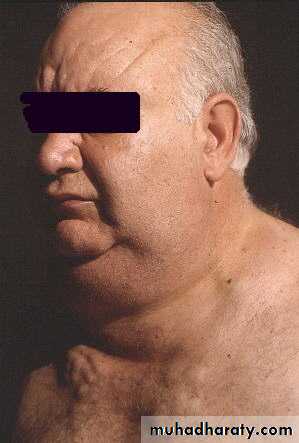
Simple defuse goiter - clinical picture-

The gland is soft, smooth, move with swallowing, not tender with universal enlargement, no picture of toxicity.
There may be pressure manifestation
inform of:
1- Dyspnoea due to pressure on the trachea.
2- Dysphagea due to pressure on the esophagus.
3- Dilatation of veins at
Supra-sternal area due
occlusion of SVC in case
of mediastinal extension.

Investigation :normal H level and RAU, no antibody .The condition is preventable by: increase iodine intake and can be treated by thyroxin for long time.Surgery indicated in presence of pressure symptoms or for cosmetic reason.
Due to fluctuation in the TSH secretion after prolonged defuse simple goiter, result in activation of part of the gland and inactivation of other.
The active portions underwent hemorrhage, necrosis or degeneration result in multiple cystic and solid lesions of various size and shape.
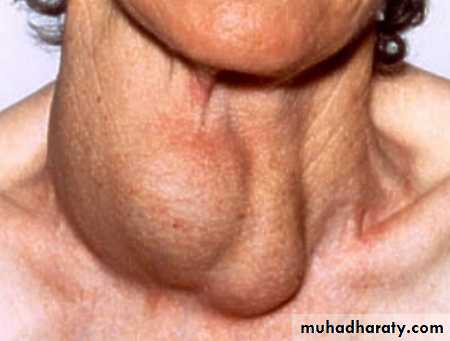
Simple multinoduler goiter
Simple multinoduler goiterClinically: The patient is euthyroid with painless cystic and solid (not hard neither fixed) masses of variable size and shape and may show pressure manefistations.
Investigation: Revealed normal H level and RAU. No antibody. ULS revealed multinodularity of the gland.
Surgery Is always indicated because:
1- Possibility of changing to toxicity (3o%) after 10 to 20 years.
2-Posibility of malignant changes (5 to 8%) after 10 to 20 years.
3- No response to thyroxin medication.
4- Presence of pressure symptoms.



Solitary thyroid nodule
The gland show one visible or palpable mass. within a normal gland with euothyroid state.Thyroid nodule present in 4 % of individuals.
15 per cent of isolated swellings prove to be malignant, and 30–40 per cent are follicular adenomas.
The remainder are non-neoplastic, largely consisting of areas of colloid degeneration, thyroiditis or cysts.
The problem, is to differentiate benign from malignant mass, this can be achieved by
:

1-clinical picture (chriteria of malignancy):
1-Age less than 20 or age greaterthan 70.
2- Male gender.
3- Rapid increase in size.
4- Resent onset of swallowing difficulties.
5- Resent onset of hoarseness.
6- History of external neck irradiation during
childhood.
7- Hard, irregular and fixed nodule.
8- Presence of cervical lymphadenopathy.
9-Previous history of thyroid cancer.
10-Nodule that is "cold" on scan.
11-Solid or complex on ULS.
12- Positive FNA cytology for malignancy.
2- investigation:
1- RAIS :show cold (80%) warm (10%) or hot (10%) nodule. 15% of cold, 5% of warm and 1% of hot nodule are malignant.
2- ULS: ultrasonic features in a thyroid swelling associated with thyroid neoplasia, including micro calcification and increased vascularity, but only macroscopic capsular breach and nodal involvement are diagnostic of malignancy.
3- FNA:It is the investigation of choice but there is a false negative (1%) and false positive (3%) results and it cannot differentiate between follicular adenoma and follicular carcinoma. 4- CT and MRI describe the anatomy rather than the pathology.


• Indications for operation in salotery thyroid swellings.
• 1- Neoplasia proved by FNAC positive• 2- Clinical suspicion
• Age
• Male sex
• Hard texture
• Fixity
• Recurrent laryngeal
• nerve palsy
• Lymphadenopathy
• Recurrent cyst
• Toxic adenoma
• Pressure symptoms
• Cosmesis
• Patient’s wishes
