1
Forth stage
Obstetric
Lec-1
.د
ا
منة
1/1/2016
Coagulation Disorders in Pregnancy
Hematological changes during pregnancy
1-expansion of plasma volume & relative hemodilution.
2-HB level increases, but there is physiological anaemia.
3-increase erythrocyte production but the RBC counts decreases.
4-S.iron decreases, iron binding capacity increases.
5-increase iron absorption from the gut.
6-increase coagulation factors, so there is hyper coagulable state, except factors XI, XIII &
anti-thrombin III.
7-decreases in fibrinolytic activity.
8-decreases platelet count.
The normal function of the coagulation & fibrinolytic system is to maintain an intact but patent
vascular tree.
Normal hemostasis requires 3 main factors;
*Vascular constriction.
*Platelet aggregation &formation of platelet plug.
*Fibrin formation through coagulation system.
When these factors stop bleeding, the fibrinolytic system starts to remove the thrombus &
restore the vascular patency.
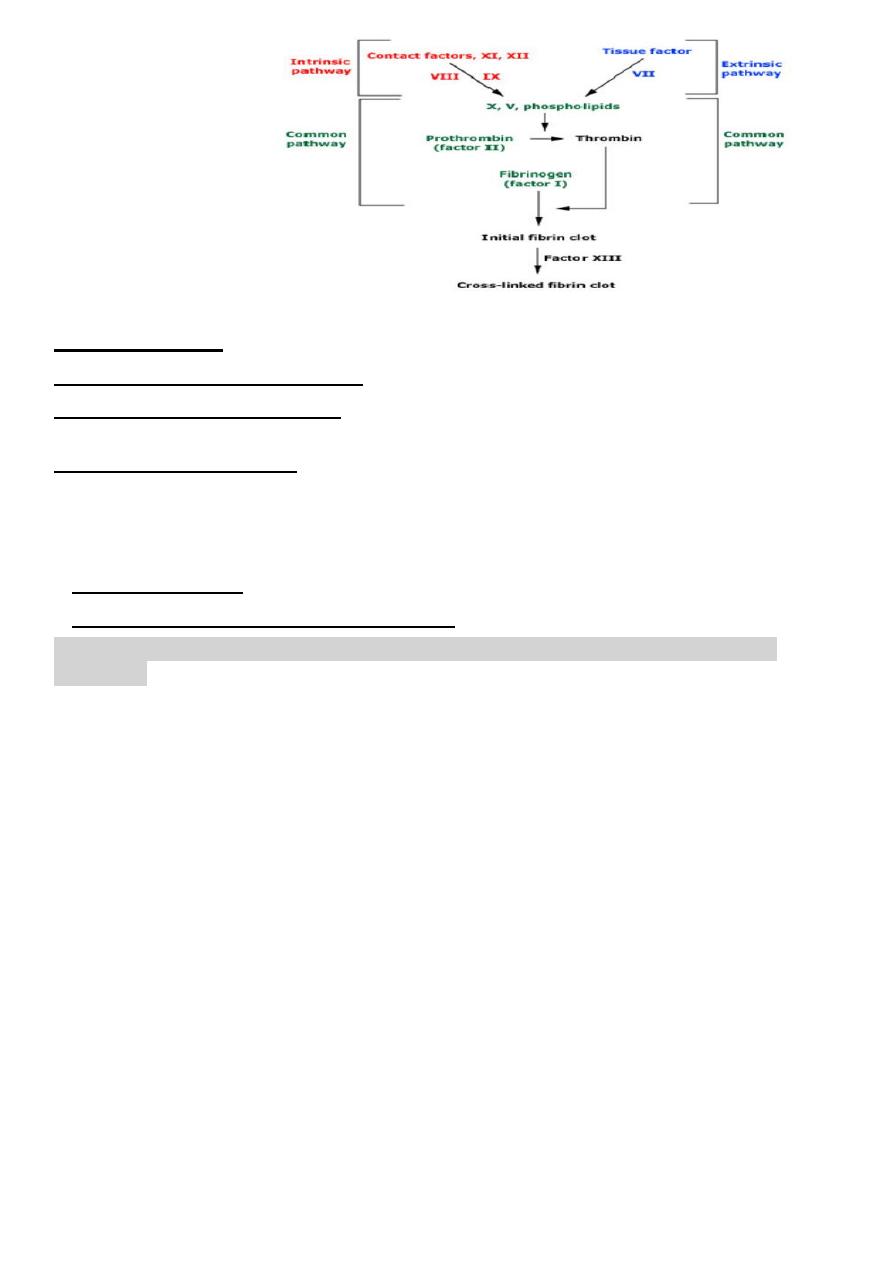
Fibrin formation:
Fig.1
1. Activation of the extrinsic pathway, thro tissue damage~
activation of VII~
activation
of factor~ X
change prothrombin to thrombin~
change fibrinogin to fibrin.
2. Intrinsic pathway: Endothelial damage causes activation of factor XII~
activation of
factor XI~
activation of factor VIII~
activation of factor X which change prothrombin to
thrombin and this change fibrinogin to fibrin
Coagulation system during pregnancy: Pregnancy represent a hypercoagulable state. This
include the following:
1-Plasma fibrinogen concentration rises during pregnancy by about 50%.
2-Increase in factors V, VII, VIII, IX, X, XII.
2
Fig. 1 fibrin formation
Basic definitions
Venous thromboembolism (VTE ),
any thrombo embolic event in the venous system.
Deep venous thrombosis (DVT),
radiologically confirmed occlusion of deep venous system of the leg
sufficient to produce symptoms of pain or swelling.
Pulmonary embolism (PE),
radiologically confirmed occlusion of pulmonary arteries sufficient to
cause symptoms of breathlessness, chest pain or both.
Hemostatic problems associated with pregnancy:
1-Thromboembolism.
2-Hemorrhage with or without coagulopathy
Venous thromboembolism (VTE) is the most common cause of maternal death during
pregnancy.
The incidence of thromboembolic complications, pulmonary thromboembolism and deep vein
thrombosis presented during pregnancy is around 1 in 1000 with a further 2 per 1000 women
presenting in the puerperium. The most dangerous period for fatal pulmonary
thromboembolism (PE) is the 1st week postpartum, then the 2nd week. Most cases occur after
CS. Most maternal deaths after CS are due to PE. 90% of death occurs in the 1st 24 h after
delivery. Pregnancy increases the risk of TE by 6 folds.
Risk factors:
1-Hypercoagulable state of pregnancy.
2-Decrease activity of naturally occurring anticoagulant.
3- Decrease fibrinolytic activity.
4- Increase tendency to venous stasis during pregnancy.
5-Other factors pregnancy related:
...Operative delivery 20 times more than NVD.
...Age and parity, could be due to atherosclerosis
3
...Obesity over 76 kg
...Restricted activity: HT, DM, multiple pregnancy, heart disease (bed rest).
...Estrogen for suppression of lactation.
...Endothelial injury
6-Other factors not pregnancy related:
...Previous TE.
...Lupus anticoagulants, anticardiolipin antibodies, and antiphospholipid syndrome. The thrombosis could be
venous or arterial and could occur at any site.
...Inherited thrombophilia like antithrombin III deficiency, protein C deficiency, and protein S deficiency.
...Smoking.
Clinical Features of Venous TE:
1-Superficial thrombophlebitis: This means inflammation of a superficial vein which if
extended to a deep vein it carries a risk of PE. Active mobilization of the affected limb is
encouraged to prevent DVT.
2-DVT: The classical signs of DVT are leg edema, calf tenderness,and positive Homans
signwhich is calf pain on dorsiflexion of the foot, it could be asymptomatic.
3-PE . a. Massive PE: cyanosis, shortness of breath, chest pain, hemoptysis.
b. Small PE: transient dyspnea, tinge of cyanosis, some pleuritic chest pain,
unproductive cough, unexplained pyrexia, tachycardia, leukocytosis.
Diagnosis of DVT
1-Clinical features usually affects left femoral vein.
2-Investigations
...Impedance plethysmography (IPG), little value in 3
rd
trimester.
...Doppler US, same as IPG.
...Duplex US, used in pregnancy.
...Contrast venography, gold standard.
...Iodine 125 fibrinogen scan
...D-dimer level
Radiological studies are contraindicated in pregnancy
4
Investigations of PE:
CXR, ECG, perfusion / ventilation lung scan, arterial blood gas analysis, pulmonary
angiography& CT scan.
Management of venous TE during pregnancy:
1-Acute phase treatment.
2-Chronic phase treatment.
Acute phase treatment:
1-Thrombolytic therapy: by streptokinase, and tissue plasminogen activaters.It cannot be
recommended during pregnancy except as a lifesaving procedure as in case of: Shocked
patient with massive PE.& Iliofemoral venous thrombosis
Streptokinase does not cross the placenta and not affect the fetus but it causes fibrinolysis on
the placental bed and severe PPH if given in the postpartum period.
2-Anticoagulants: unfractionated heparin 40,000 IU daily continuous intravenous
infusion...S.E. Bleeding, hypotension by the effect of the preservative.It should be given
intravenously to prevent intramuscular hematoma. Monitoring of the drug by APTT which
should be 1.5 times the normal.If you want to stop the effect of heparin you should stop the
drug and give protamin sulfate 1 mg for every 100 IU. Heparin is given for 3-7 days. Low
molecular weight heparin has replaced unfractionated heparin.
3-Surgery.
Chronic phase treatment:
Warfarin which crosses the placenta. If this drug is given during pregnancy it should be
stopped at 36 weeks. The action of warfarin is monitored by prothrombin time. S.E. during
pregnancy is teratogenicity and bleeding tendency in the fetus, bleeding in the mother.
Reversal of the effect is by stopping the drug, it will take three days to reserve the action, so
we can give FFP and vitamin K.
We should change the dose constantly during pregnancy. There are many drugs interact with
warfarin and affect its action.The teratogenic effect of warfarin include embryopathy, CNS
abnormalities, increased risk of abortion and premature labor, chondroplasia punctata, nasal
hypoplasia, hypertelorism and stippled epiphysis.
DIC (Disseminated intravascular coagulation)
:
Trigger mechanism of DIC during pregnancy:
1-Endothelial injury:
...preeclampsia.
5
...Hypovolemia.
...Septicemia
2-Release of thromboplastin as in:
...Abruptio placentae.
...Amniotic fluid embolism.
...Retained dead fetus.
...Intrauterine sepsis
...Hydatidiform mole
...Placenta accreta
3-Release of phospholipid as in
...Intravascular hemolysis
...Incompatible blood transfusion
...Large feto maternal bleed
...Septicemia
Clinical manifestation of DIC:
1-Asymptomatic:compensated state. There is lab evidence of increased production and
breakdown of coagulation factors, as in PET and in retained dead fetus.
2-Variable degrees of thrombocytopenia as in small abruptio placentae.
3-Massive uncontrollable hemorrhage as abruptio placentae, amniotic fluid embolism and
eclampsia.
Diagnostic tests:
1. Thrombin time: estimation of fibrin clottable fibriongen in activated sample of plasma,
normally 10-15 sec and the fibrin clot formed should firm and stable. There is prolongation
thrombin time with formation of friable clot which dissolve on standing due to fibrinolytic
substances present in the plasma in DIC.Thrombin time is increased when there is defect in
extrinsic or intrinsic systems or due to increase in FDP.
2. Increase in APTT.
3. Increase in PT.
4. Decrease in fibrinogen level.
5. Decrease in platelet count.
6
Management:
1-Fluid replacement to avoid renal shut down usually by simple crystalloid eg. Hartmanns
solution 2-3 times the estimated volume blood loss.
2-FFP which contains all coagulation factors.
3-Fresh blood transfusion.
Thrombophilia and adverse pregnancy outcome
*Sever PET
*Recurrent early pregnancy loss
*IUGR
*Late fetal loss
*Venous TE during pregnancy