prostatic cancer
1
CARCINOMA OF THE PROSTATE
Prostate cancer is the most common cancer detected in American men.prostate cancer is the second leading cause of cancer death for men.
mortality rates have been declining since the mid-1990s.
prostatic cancer
2
unlike most cancers, which have a peak age of incidence, the incidence of CaP continues to increase with advancing age.
The probability of CaP developing in a man under the age of 40 is 1 in 10,000; for men 40–59 it is 1 in 100, and for men 60–79 it is 1 in 8.
many prostate cancers are indolent , while others are virulent, and if detected too late or left untreated, they result in a patient’s death.
prostatic cancer
3
Risk Factors For Prostate Cancer
Age.Black race.
Chemicals.
Diet.
Family history .

prostatic cancer
4



Pathology
Over 95% of the cancers of the prostate are adenocarcinomas.Of the other 5%, 90% are transitional cell carcinomas, and the remaining cancers are neuroendocrine (“small cell”) carcinomas or sarcomas.
Approximately, 60–70% of cases of CaP originate in the peripheral zone, while 10–20% originate in the transition zone, and 5–10% in the central zone.
prostatic cancer
5Grading
The Gleason grading system is the most commonly employed grading system.pathologists assign a primary grade to the pattern of cancer that is most commonly observed and a secondary grade to the second most commonly observed pattern in the specimen.
Grades range from 1 to 5 and the score range from 2 - 10.
prostatic cancer
6
Staging
prostatic cancer7

prostatic cancer
8

Clinical Findings A. SYMPTOMS
Most patients with early-stage CaP are asymptomatic.The presence of symptoms often suggests locally advanced or metastatic disease.
Obstructive or irritative voiding complaints.
Metastatic disease to the vertebral column with impingement on the spinal cord may be associated with symptoms of cord compression.
Bone pain due to metastasis to bone( osteoblastic lesions).
prostatic cancer
9
SIGNS

• General Examination .
• Abdominal Examination ( palpable kidney or mass due to metastasis to liver or adrenals).• DRE.
• Specific signs of cord compression relate to the level of the compression.
• Lymphedema of the lower extremities.
10
C. LABORATORY FINDINGS
Azotemia can result from bilateral ureteral obstruction Either from direct extension into the trigone or from retroperitoneal Adenopathy.Anemia may be present in metastatic Disease.
Alkaline phosphatase may be elevated in the Presence of bone metastases.
Serum acid phosphatase may Be elevated with disease outside the confines of the prostate.
prostatic cancer
11
TUMOR MARKERSPROSTATE-SPECIFIC ANTIGEN PSA
PSA is a serine protease produced by benign and malignant prostate tissues.It circulates in the serum as uncomplexed (free) or complexed (bound) forms.
Normal PSA values are those ≤4 ng/mL.
Unfortunately, PSA is not specific for CaP, as other factors such as BPH, urethral instrumentation, and infection can cause elevations of serum PSA.
prostatic cancer
PSA12

Attempts at refining PSA have included:
• PSA velocity (change of PSA overtime).• PSA density (standardizing levels in relation to the size of the prostate).
• age-adjusted PSA reference ranges
• PSA forms (free versus total of PSA).
prostatic cancer
13
Differential Diagnosis
Not all patients with an elevated PSA concentration have CaP.(BPH, urethral instrumentation, infection, prostatic infarction, or vigorous prostate massage)Not all patients with an Induration of the prostate have CaP.(chronic granulomatous prostatitis, previous TURP or needle biopsy, or prostatic calculi).
Not all patients with sclerotic bony lesion and elevated alk. phosphatase have CaP.(Paget disease)
prostatic cancer
14IMAGING
prostatic cancer15
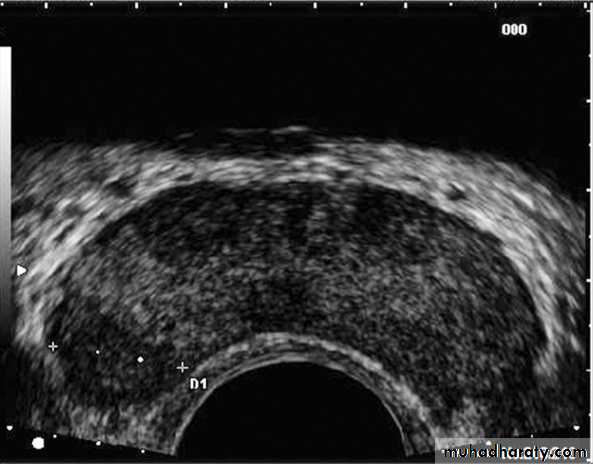
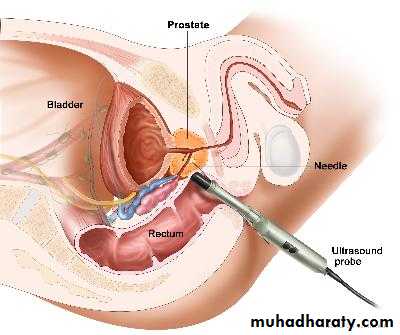
1. TRUS (transrectal ultrasound):
is useful in performing prostatic biopsies and in providing local staging information if cancer is detected.
Almost all prostate needle biopsies are performed under TRUS guidance. This makes lesion-directed biopsies possible.
If visible, CaP tends to appear as a hypoechoic lesion in the peripheral zone.
prostatic cancer
16
2. Endorectal (MRI).
3. Axial imaging (CT, MRI).4. Bone scan.
prostatic cancer17


Screening for CaP
Any male ≥ 50 years of age should underwent annual DRE and PSA test .
Screening to date has resulted in considerable stage migration (more lower stage cancers being detected) and morality rates are falling.

prostatic cancer
18
Treatment
A. LOCALIZED DISEASE (T1 and T2)Currently, treatment decisions are based on the grade and stage of the tumor, the life expectancy of the patient, the ability of each therapy to ensure disease-free survival, its associated morbidity, and patient and physician preferences.
1- Active Monitoring or Watchful Waiting
prostatic cancer19
2. Radical prostatectomy
prostatic cancer
20


prostatic cancer
21

3. Radiation therapy
external beam therapybrachytherapy
prostatic cancer
22


4- Cryosurgery
5-high-intensity focused ultrasound(HIFU)
prostatic cancer
23

b. Locally invasive ca.( T3 )
Neoadjuvant hormonal therapy followed by radiotherapy.prostatic cancer
24

c. METASTATIC DISEASE
Hormonal therapyAndrogen blockade therapy
prostatic cancer
25
prostatic cancer
26There are four general forms of ADT:
• ablation of androgen sources.
• inhibition of androgen synthesis.
• antiandrogens.
• inhibition of LHRH.

prostatic cancer
27
prostatic cancer
28

Hormone-Refractory Prostate Cancer
Although androgen deprivation therapy (ADT), is extremely effective initially, virtually most of the patients eventually develop clinical evidence of resistance to treatment(poor prognosis).Management:
• Add or Stop antiandrogens.
• 2nd . Line hormonal therapy.
• Chemotherapy ( as docetaxel or paclitaxel + estramustine+ prednisolone).
prostatic cancer
29
prostatic cancer
30