
1
Forth stage
Obstetric
Lec-7
د . براء
1/1/2014
Cesarean Section
Definition
• Cesarean Section is the delivery of a fetus from the uterus by abdominal and uterine
incisions, after 28 weeks of pregnancy.
• It is called hysterotomy, if it is done before 28 weeks of pregnancy.
• The cesarean rates during the past decade, both in the United States and worldwide,
have increased dramatically.
• The percentage of women in the United States delivering by cesarean increased from
<5.0% in 1965 to 30.2% in 2005 and has increased 40% since 1996.
• Although perinatal outcome in the United States improved during the time when the
cesarean rate increased, it also improved in other countries where cesarean rates
remained low. Notably, the incidence of cerebral palsy has not declined during the
past 20 years, primarily because perinatal morbidity and mortality more often are a
function of antepartum events, abnormal fetal growth, congenital anomalies, and
premature birth.
Significance:
Cesarean section is safe, but it’s not as safe as a planned vaginal delivery.
• In the U.S. there is a fourfold risk of death compared to vaginal birth.
• In England, emergency cesarean birth has a ninefold risk of death when compared to
vaginal and elective cesareans have a threefold risk.
• Women are twice as likely to be rehospitalized within 60 days of birth when
compared with women who have a vaginal birth.

2
Avoiding First C-Section Should Be Priority
• Avoiding primary cesarean sections unless there is a medical necessity
• Doctors, midwives, and childbirth educators must give full and honest advice based on
the available information; they may persuade but never coerce. Active participation by
patients should be encouraged to arrive at a safe and logical informed decision about
method of delivery, with carers recommending what they perceive to be the best course
of action in keeping with the available evidence
Complications
• Cesarean delivery is not an innocuous procedure. A variety of postpartum complications,
including unexplained fever, endometritis, wound infection, hemorrhage, aspiration,
atelectasis, urinary tract infection, thrombophlebitis, and pulmonary embolism, can
occur in up to 25% of patients.
• The frequency of maternal death related to cesarean delivery varies with the institution
and with the condition necessitating the procedure. Maternal mortality rates are now <1
in 1,000 operations, and many deaths are related to the underlying maternal illness or
anesthetic complications.
• Late maternal complications of cesarean delivery include:
intestinal obstruction from adhesions
dehiscence of the uterine incision in subsequent pregnancies. Both of these
complications are more common with the classic incision than with a lower uterine
segment incision.
The incidence of placenta previa and abnormal myometrial invasion by the placenta
(accreta/increta/percreta) also is increased with each successive cesarean and can cause
severe and intractable hemorrhage.
Impact on Neonates
Breastfeeding, bonding & attachment issues
Respiratory effects
Fetal injuries

3
Timing Of CS
• Cesarean section may be performed as an elective procedure (planned in advance) or as
a non-elective one (the urgency of the procedure being performed determined by the
nature of the indication).
• Elective cesarean delivery
• elective caesarean section may be justified, but decisions must take into account the risk
to the infant associated with delivery before 39 weeks' gestation.
• It is now clear that respiratory distress syndrome is indeed seen in "term" infants and is
a considerable source of morbidity and mortality in this group.
Indication:
• Cesarean delivery is necessary when labor is unsafe for either the mother or fetus.
• The four primary indications for cesarean delivery include:
dystocia,
elective repeat cesarean delivery,
fetal distress,
and abnormal fetal presentation.
INDICATIONS FOR ELECTIVE CS
1. Known CPD
2. Malpresentation (Breech, Transverse lie)
3. Multiple pregnancy (when first fetus is not in cephalic presentation)
4. Fetal macrosomia (over 5000g, GDM – 4500g)
5. Placenta previa
6. Repeat CS
7. Uterine surgery eg. Hysterotomy, myomectomy
8. Ca of the Cervix/ tumour obstructing the birth canal
9. vesicovaginal fistula repair
10. HIV
11. Active herpes

4
INDICATIONS FOR EMERGRENCY CS :
1. Severe PET/ eclampsia (especially with unfavourable cervix)
2. Abruptio placntae
3. Fetal distress
4. Compromised fetus 2ry to DM, HT, isoimmunization
5. Cord prolapse
6. Failed induction
7. Failure to progress in labour
8. Obstructed labour
9. Malpresentation in labour brow, mentopost. shoulder presentations, breech
10. APH
Preoperative testing and preparation for CS :
• Pregnant women should be offered a haemoglobin assessment before CS to identify
those who have anaemia. Although blood loss of more than 1000ml is infrequent after
CS (it occurs in 4 to 8% of CS), it is a potentially serious complication.
• Prescribe antibiotics (one dose of first-generation cephalosporin or ampicillin)
• Assess risk for thromboembolic disease (offer graduated stockings, hydration, early
mobilisation and low molecular weight heparin)
• To reduce the risk of aspiration pneumonitis: Empty stomach, Pre-medication with an
antacid (sodium citrate 0.3% 30 mL or magnesium trisilicate 300 mg) + Cimetidine IV 1
hr before CS
• Women having CS with regional anesthesia require an indwelling urinary catheter to
prevent over-distension of the bladder, because the anaesthetic block interferes with
normal bladder function
Maternal Position During CS
• All obstetric patients undergoing CS should be positioned with left lateral tilt to avoid
aorto-caval compression
• By tilting the operating table to the left or place a pillow or folded linen under her right
lower back
5
Anaesthesia
• 1 General anaesthetic.
• 2 Regional anaesthesia ( Epidural block. - Spinal block ).
• Regional anaesthesia is regarded as considerably safer than general anaesthesia with
respect to maternal mortality
Procedure overview:
• The pelvis and uterus are entered.
• The head of the infant is delivered & the infant’s airway is cleared.
• The infant’s body is delivered.
• The placenta is removed.
• The uterus is closed.
• The abdominal wall layers are closed.
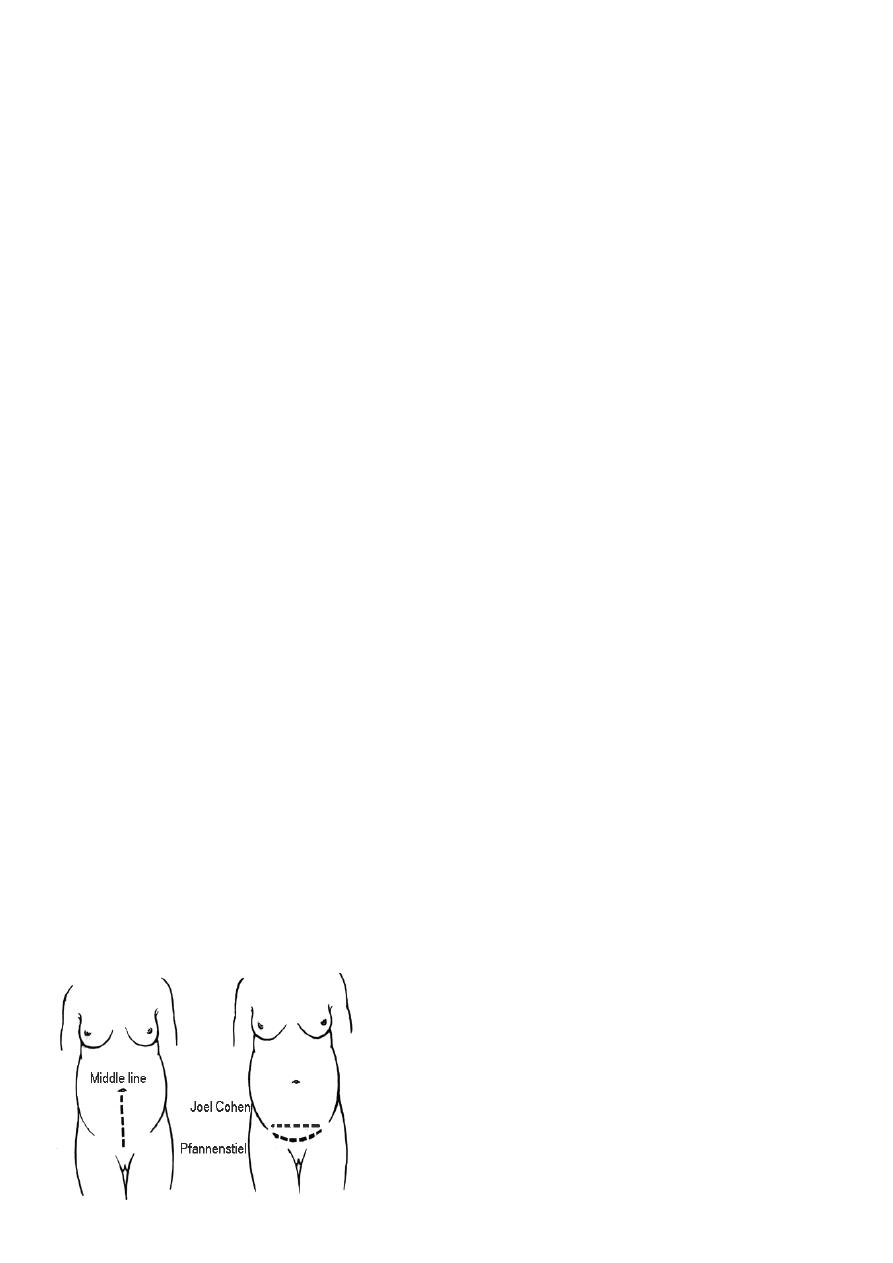
Types of abdominal wall incision:
Suprapubic transverse
Midline vertical
Transverse incision:
• Advantage:
• Stronger with less likelihood of dehiscence or hernia.
• Cosmetic advantage is apparent.
• Disadvatage
– Exposure in some women is not as optimal

6
TYPES OF CS:
Classified according to the site of uterine incisions:
• Lower segment CS Classical CS
• Lower segment C.S.
Transverse incision in the lower uterine segment .
Advantage : reduced chance of rupture .
reduced risk of bleeding, peritonitis , paralytic ileus and bowel adhesion.
• Upper segment (Classical C.S) :
Vertical incision in the upper uterine segment .
This incision may be made in the lower segment (low vertical incision) but It’ll invariably
extend into the upper segment
Indications for classical incision:
• Transverse lie with SROM
• Structural abnormality that makes lower segment approach difficult
• Constriction ring with neglected labour
• Fibroids in the lower segment
• Ant. PP & abnormally vascular lower segment
• Mother dead & rapid delivery is required
• Very preterm fetus in breech presentation
Uterine Incisions
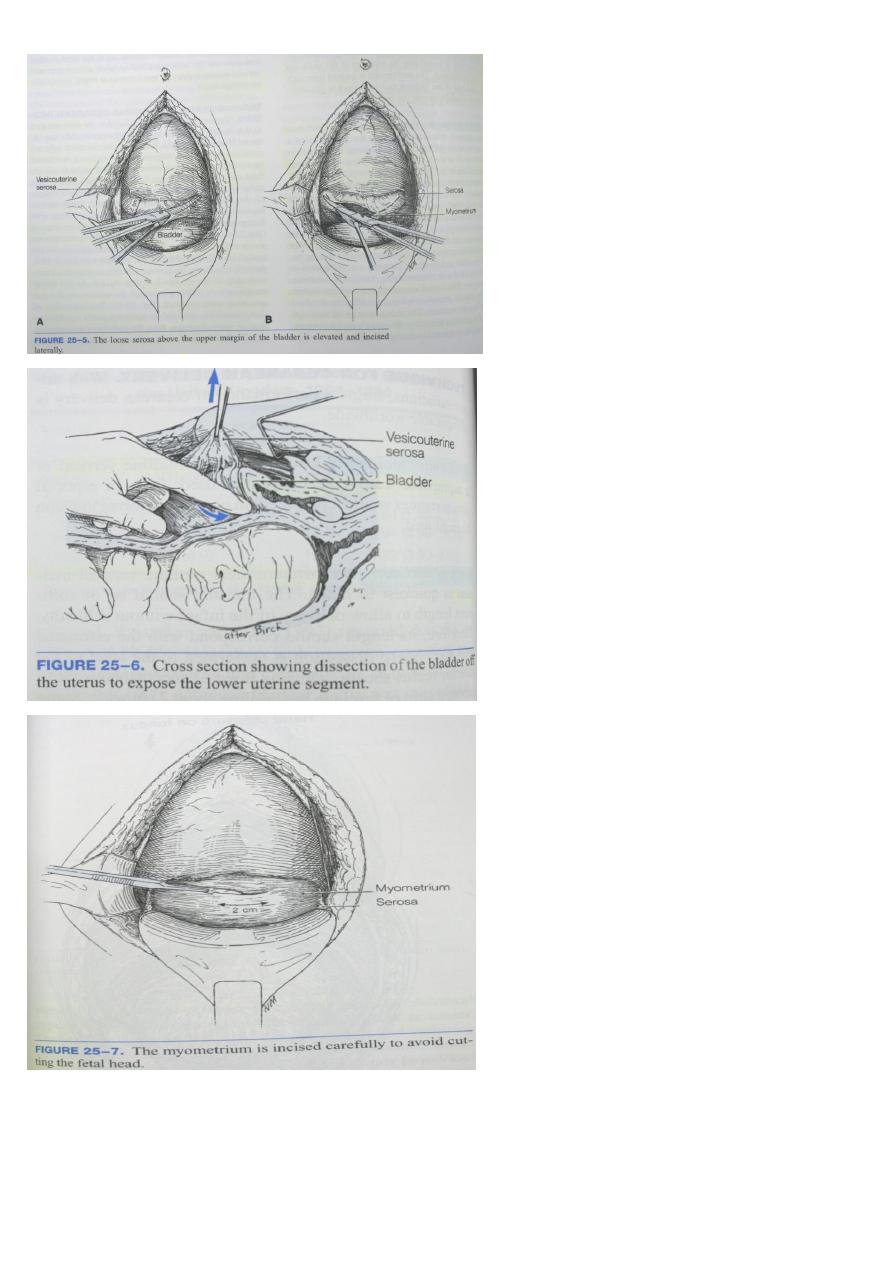
7
The uterus is opened through the lower uterine segment about 1 cm below the upper margin
of the peritoneal reflection
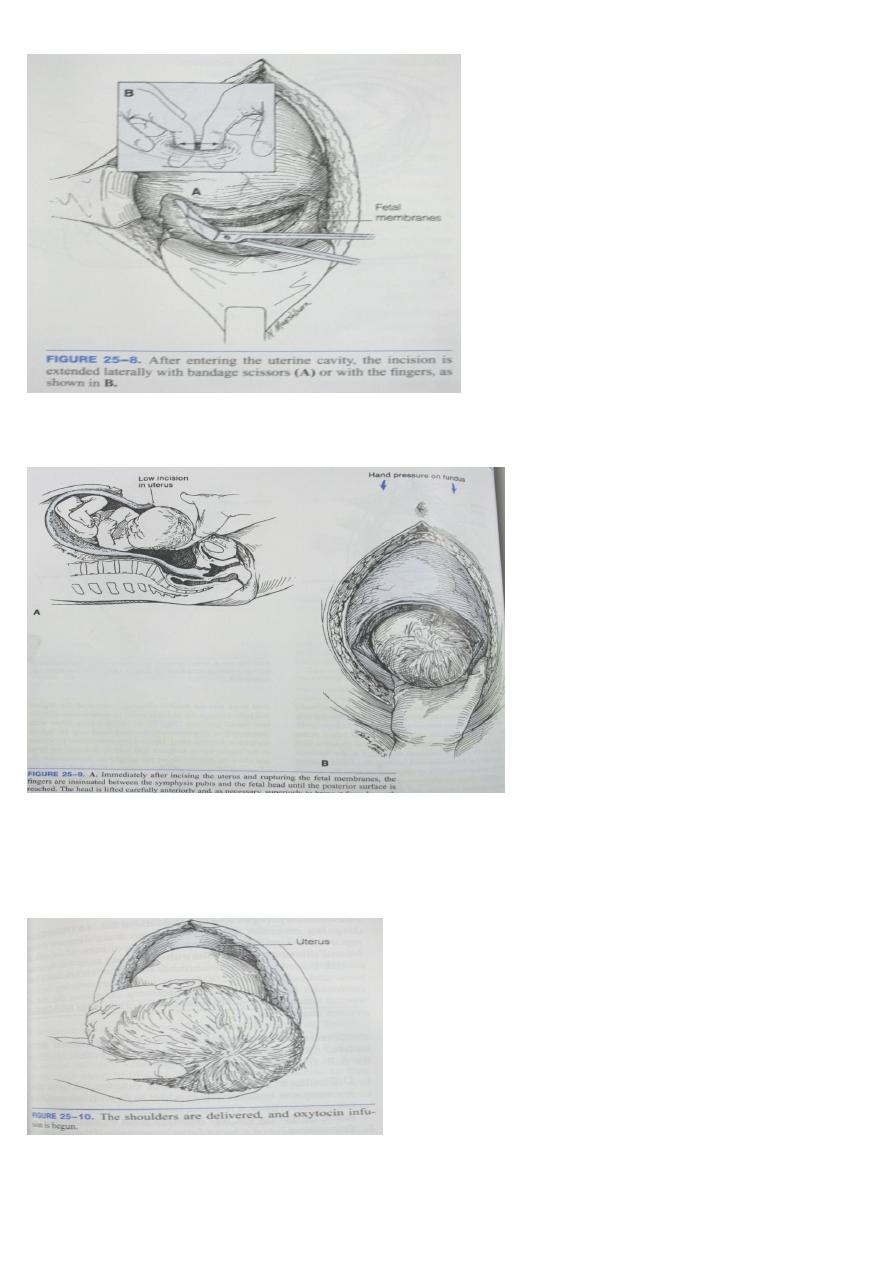
8
Uterine incision large enough to allow
delivery of the head and trunk of the fetus without either tearing into or having to cut into the
uterine arteries and veins that course through the lateral margins of the uterus
Hand is slipped into the uterine cavity
between the symphysis and fetal head
Head is elevated gently with the fingers and palm through the incision .
Aided by modest transabdominal fundal pressure
The shoulders then are delivered using gentle
traction plus fundal pressure
And oxytocin infusion (10-20IU/L at 10ml/min) Until the uterus contracts satisfactorily
9
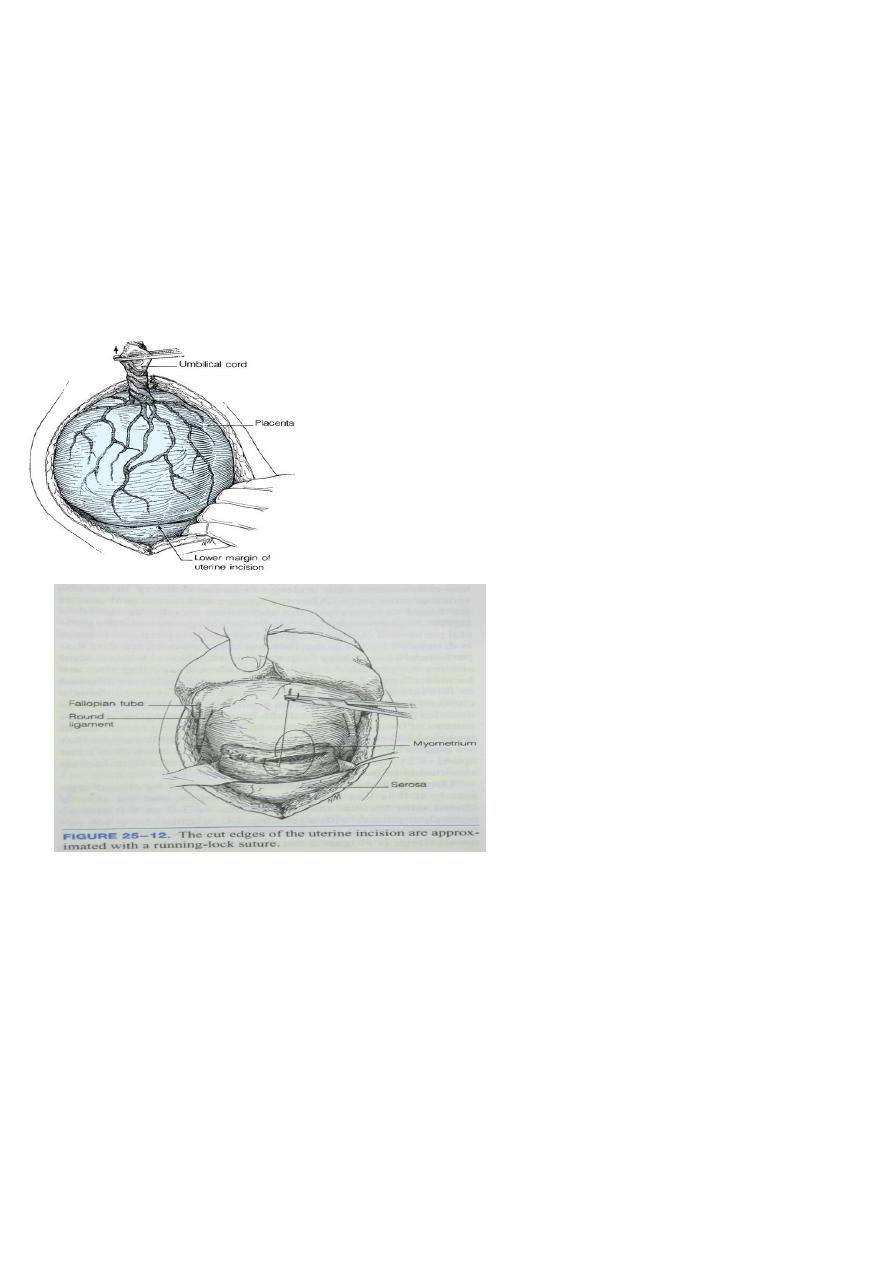
Delivery of the placenta:
• At CS, the placenta should be removed using controlled cord traction and not manual
removal as this reduces the risk of endometritis.
• Spontaneous delivery of the placenta may reduce blood loss and decrease the chance of
postoperative endometritis
• By Keeping gentle traction on the cord and massage (rub) the uterus through the
abdomen.
• Deliver the placenta and membranes
– The upper and lower cut edges and each angle of the uterine incision are examined
carefully for bleeding vessels
– The uterine incision is closed with one or two layers of continuous absorbable suture.
Immediate post-operative care :
• After surgery is completed, the woman will be monitored in a recovery area
• to ensure that the uterus remains contracted, that there is no excessive vaginal bleeding
or bleeding at the incision site, that there is adequate urine output, and to monitor
routine vital signs (pulse, blood pressure, temperature, breathing). Pain medication is
also given, initially through the IV line, and later with oral medications.
11
• When the effects of anesthesia have worn off, about four to eight hours after surgery,
the woman is transferred to a postpartum room
POSTNATAL CARE :
• Vital signs & blood loss must be monitered
• Uterine fundus palpated
• Effective parentral analgesics
• Deep breathing & coughing encouraged
• Early mobilization
• Fluid therapy &diet
• Bladder & bowel function
• Wound care
• Breast care
• Prophylaxis for thromboembolism
•
Review for consent of patient.
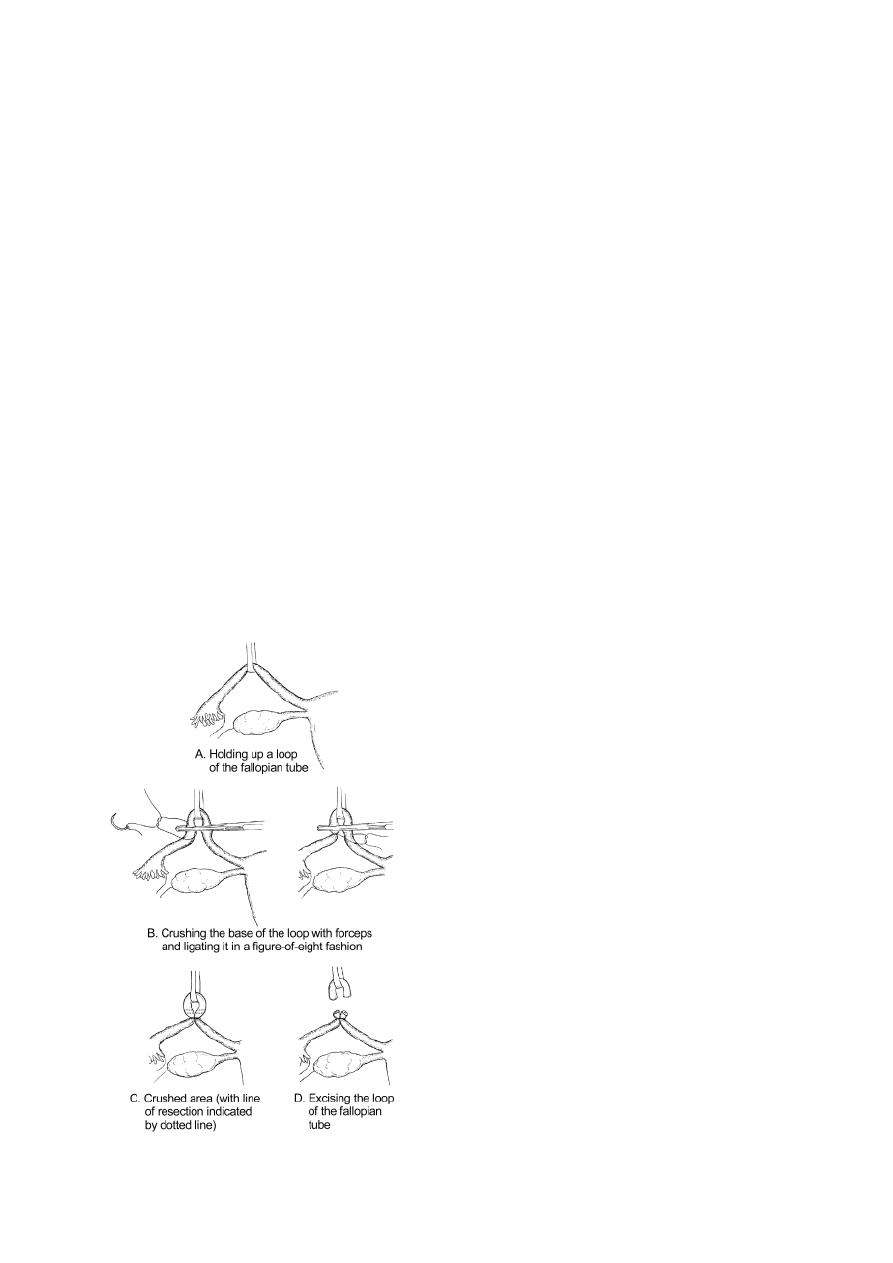
• Grasp the least vascular, middle portion of the fallopian tube with a Babcock or Allis
forceps.

11
• Hold up a loop of tube 2.5 cm in length
• Crush the base of the loop with artery forceps and ligate it with 0 plain catgut suture .
• Excise the loop (a segment 1 cm in length) through the crushed area.
• Repeat the procedure on the other side .
Cesarean Hysterectomy :
Hysterectomy is carried out after caesarean section in the same sitting for one of the
following reasons:
• Uncontrollable postpartum haemorrhage.
• Unrepairable rupture uterus.
• Operable cancer cervix.
• Couvelaire uterus.
• Placenta accreta cannot be separated.
• Severe uterine infection particularly that caused by Cl. welchii.
• Multiple uterine myomas in a woman not desiring future pregnancy although it is
preferred to do it 3 months later.