1
Forth stage
Obstetric
Lec-6
د . براء
1/1/2014
Operative vaginal delivery
Definition:
Delivery of a baby vaginally using an instrument for assistance.
Introduction
Incidence of Operative Vaginal Delivery (OVD) – 10-15%
The incidence of instrumental intervention varies widely both within and between
countries and may be performed as infrequently as 1.5% or as often as 26%. These
difference are often related to labour ward management.
Percentage of forceps declining compared with vacuum extraction
Indications for OVD
No indication is absolute
Prolonged 2
nd
stage
Nulliparous: lack of continuous progress
>3hrs with regional anesthesia
>2hrs without regional anesthesia
Multiparous: lack of continuous progress
>2hrs with regional anesthesia
>1hr without regional anesthesia
Fetal compromise
Maternal benefit to shortened 2
nd
stage specially those with medically significant
conditions, such as aortic valve disease with significant outflow obstruction or
myesthenia graves.
Prerequisites for OVD :
Vertex presentation with identification of the position.
Engaged head.
2
Fully dilated cervix
Membranes ruptured
Adequate maternal pelvis
Adequate analgesia/ anesthesia
Maternal empty bladder
A knowledgable and experienced operator with adequate preparation to proceed with
an alternative approach if necessary.
Informed consent
Safe practice: prerequisites for instrumental delivery :
Fully dilated cervix
One-fifth or nil palpable abdominally
Ruptured membranes
Contractions present
Empty bladder
Presentation and position known
Satisfactory analgesia
Contraindication – OVD :
Unengaged vertex
Incompletely dilated cervix (possible exceptions occurs with the vaccum delivery of a
second twin where the cervix has contracted or with a prolapsed cord at 9 cm if rapid
delivery is anticipated).
Clinical evidence of CPD
Fetal conditions (e.g. thrombocytopenia)
< 35 weeks gestation (vacuum)
face or breech presentation (vacuum)
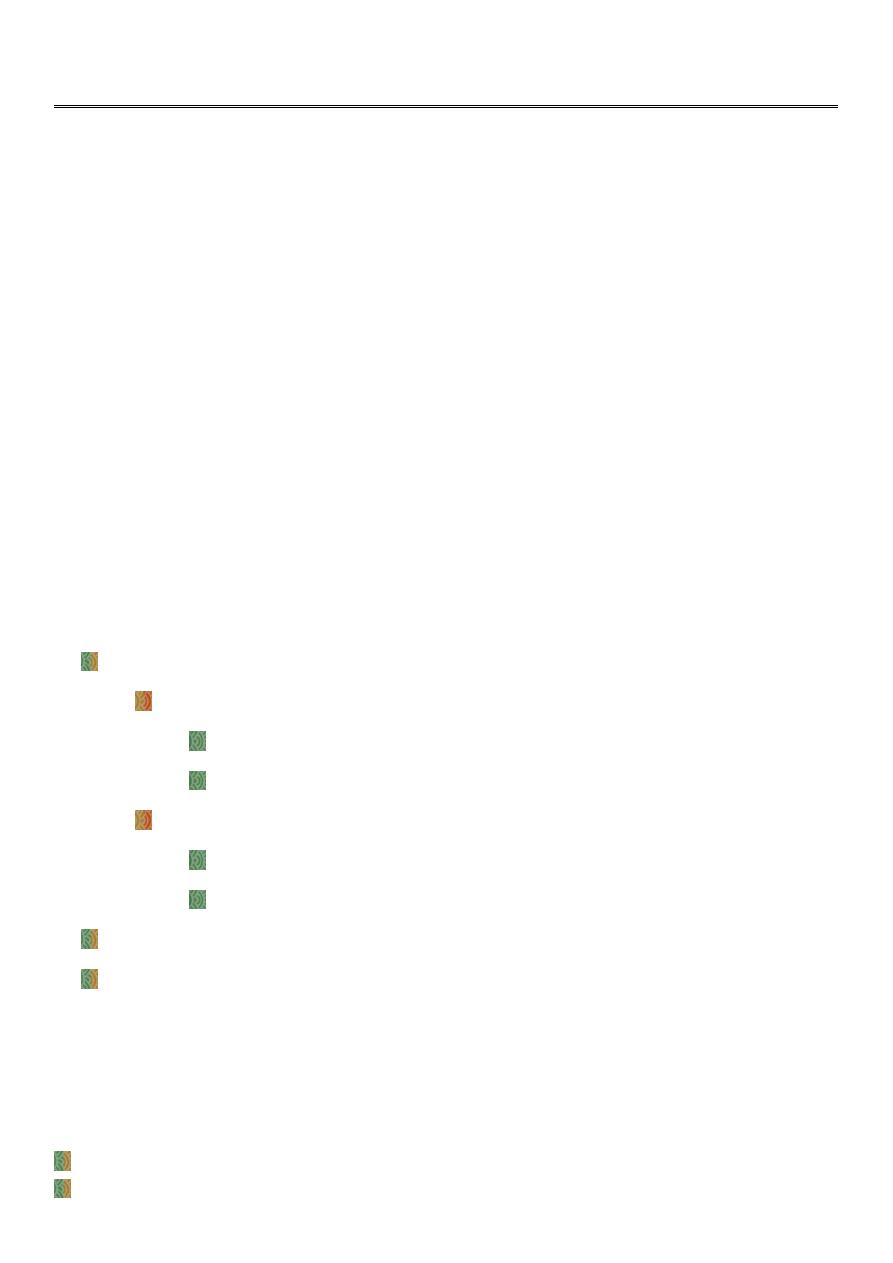
Evaluation:
The size of the baby should be estimated per abdomen and the head should be fully
engaged (none of the head should be palpable above the pubic symphysis).
3
A careful pelvic examination is essential to determine whether there are any
‘architectural’ contraindication to performing an instrumental vaginal delivery (the
shape of the subpubic arch, the curve of the sacral hollow, the presence of flat or
prominent ischial spine, all contribute to the decision as to whether vaginal delivery may
be safely performed).
In ventouse delivery, the position of the vertex and the amount of caput should be
determined by vaginal examination and no attempt should be made to deliver the baby
vaginally if the presenting part is above the ischial spine.
Station :
At the 0 station, the fetal head is at the bony ischial spines and fills the maternal sacrum.
Positions above the ischial spines are referred to as -1 through -5
As the head descends past the ischial spines, the stations are referred to as +1 through
+5 (head visible at the introitus).
Analgesia:
Analgesic requirements are greater for forceps than ventouse delivery.
Rotational forceps----- regional anasthesia is preferred.
Rigid cup ventouse------pudendal block with perineal infiltration.
Soft cup-----analgesic requirement may be minimal.
A requirement for haste should not preclude the use of analgesia.
4
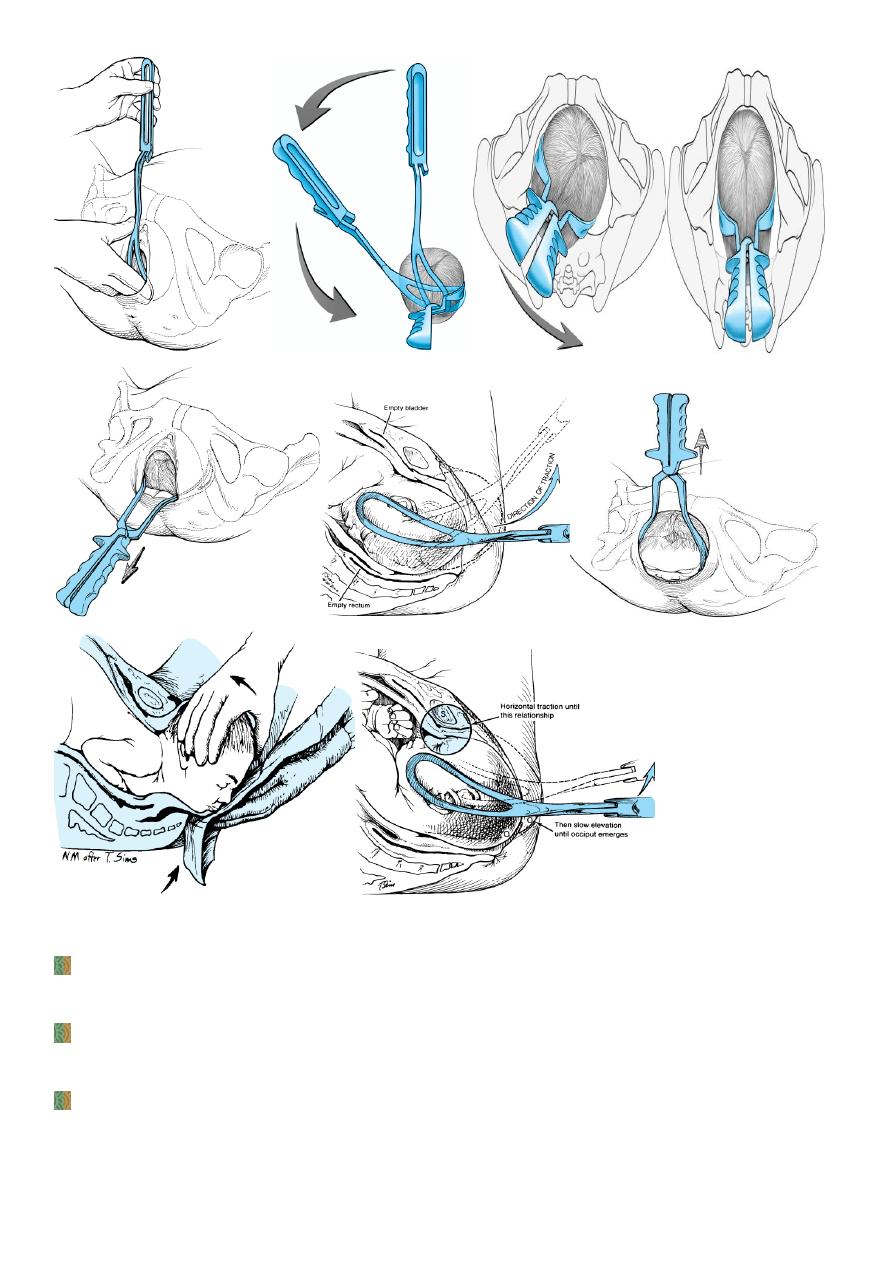
Forceps delivery:
For forceps, all the prerequisties above apply, but in addition it is essential that the
operator check the pair for forceps to ensure that a matching pair has been provided
and that the blade lock with ease.
It is generally advised that catheterization and an episiotomy is required for forceps
delivery.
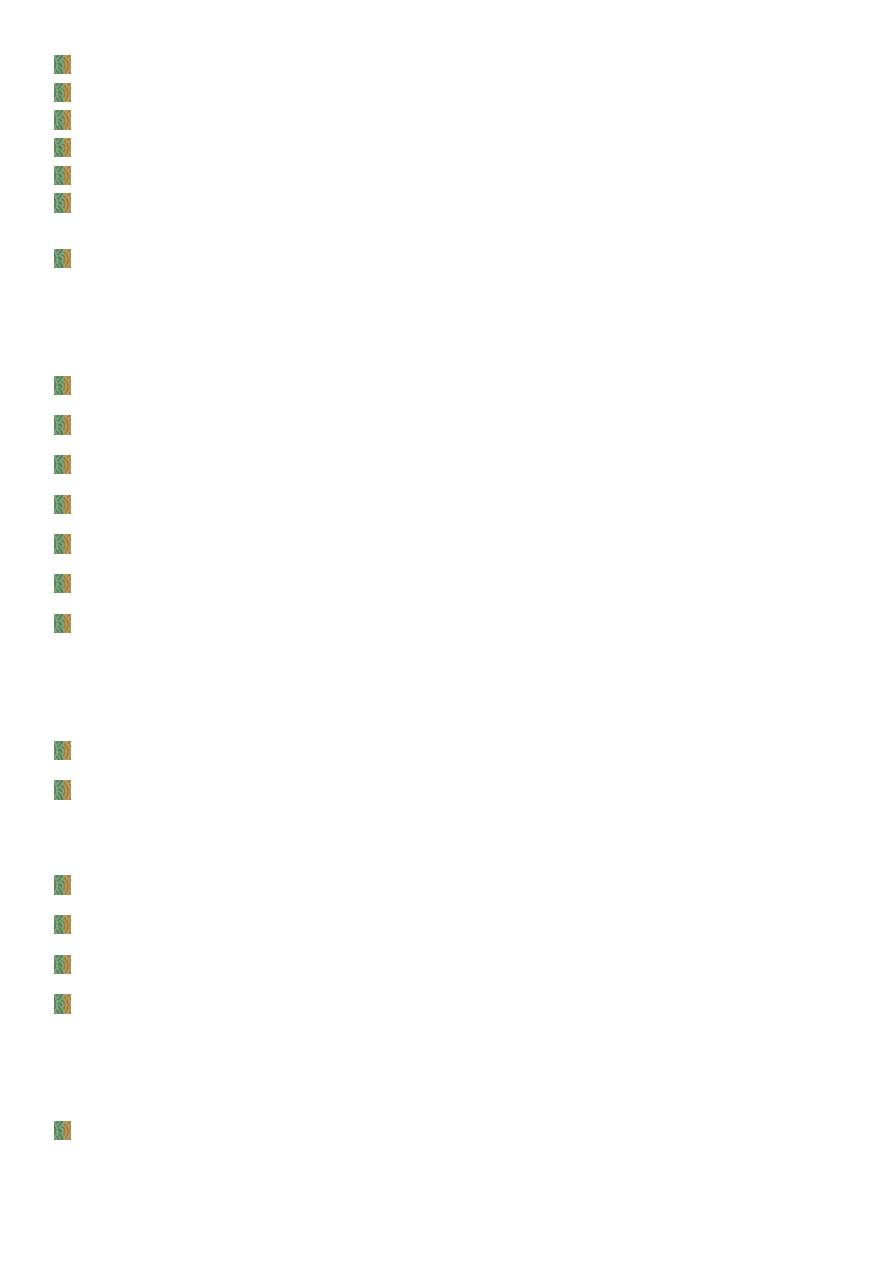
Types of forceps:
There are three main types of forceps:
• Low-cavity outlet forceps (e.g. Wrigley's), which are short and light
• Mid-cavity forceps (e.g. Simpson's) for when the sagittal suture is in the
anteroposterior plane (usually occipitoanterior).
• Kielland's forceps for rotational delivery (the reduced pelvic curve allows rotation
about the axis of the handle).
Forceps: from left to right, Kielland's,mid-cavity, Wrigley's. ( left photo )
( b) Wrigley's forceps, (c) Simpson's midcavity obstetric forceps (d) Kielland's forceps (
right photo )
5
Vacuum (Ventouse) Delivery:
The advantage of the vacuum extractor over forceps include the avoidance of insertion
of space-occupying steel blades within the vagina.
A metal cap designed so that the suction creates an artificial caput, or chignon, within
the cup that holds firmly and allows adequate traction.
In the United States, the metal cup generally has been replaced by newer soft cup
vacuum extractors
6
Vacuum Cups:
Soft vs. Rigid
Soft cups were more likely to fail to achieve vaginal delivery
Soft cups were associated with less scalp injury.
There appear to be no difference in terms of maternal injury.
The soft cups are appropriate for straightforward deliveries with an
occipitoanterior position; metal cups appear to be more suitable for
occipitoposterior, occipit transverse and difficult occipitoanterior position
deliveries where the infant is larger or there is a marked caput.
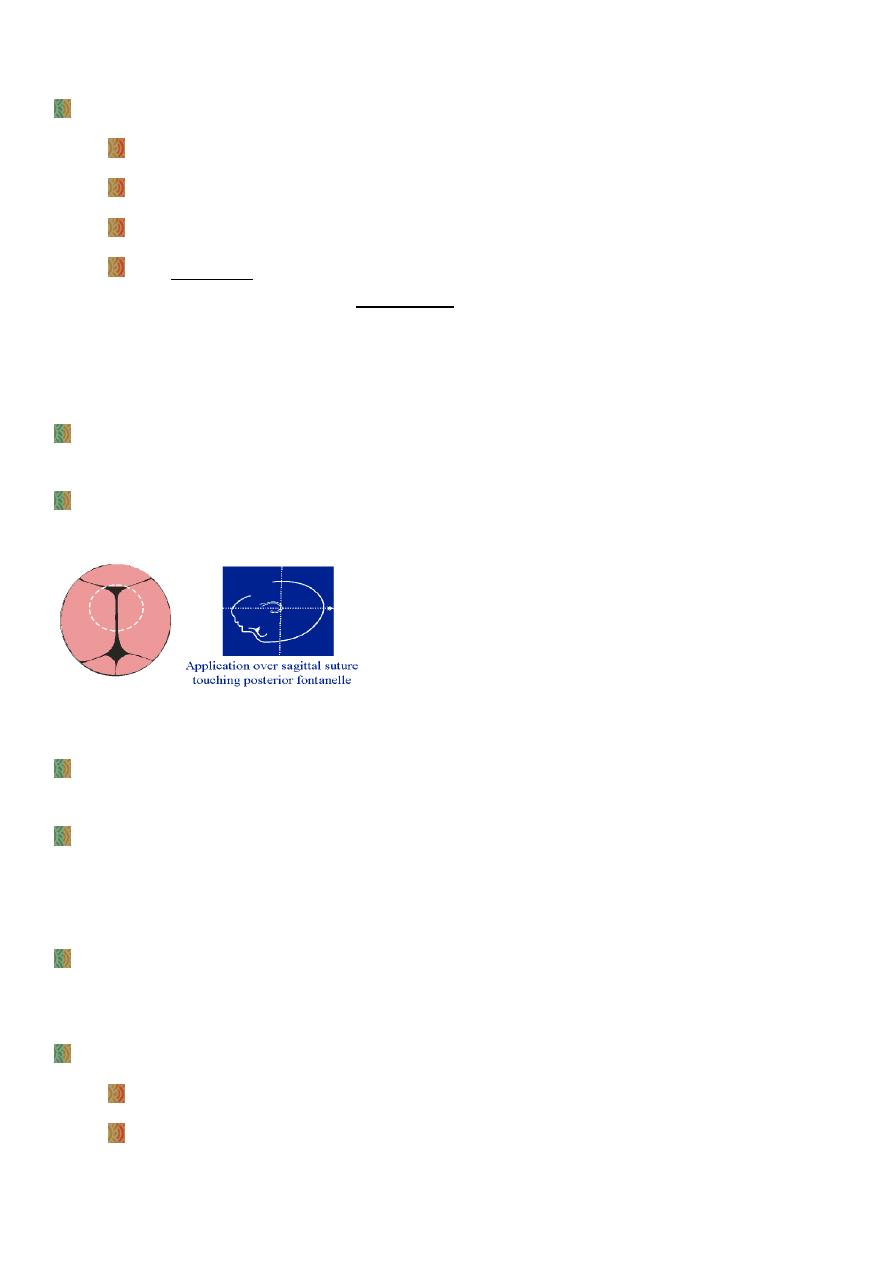
Vacuum Placement :
Proper cup placement is the most important determinant of success in vacuum
extraction.
The center of the cup should be over the sagittal suture and about 3 cm in front of the
posterior fontanelle and thus 6 cm posterior to the anterior fontanelle – flexion point.
Vacuum Procedure :
The entire 360º circumference of the cup must then be digitally inspected to insure that
no vaginal or vulvar tissues are trapped between the cup and the fetal surface.
The operating vaccum pressure for nearly all ventouse is between 0.6 and 0.8 kg/cm
2
. It
is prudent to increase the suction to 0.2 kg/cm
2
first and then to recheck that no
maternal tissue is caught under the cup edge. When this is confirmed the suction can
then be increased.
The fingertips of the dominant hand pull the device's crossbar, while the nondominant
hand monitors the progress of descent and prevents cup detachment by placing counter
pressure with the thumb
Apply traction along the axis of the pelvic curve.
Initially, the angle of traction is downward (toward the floor).
The axis of traction is then extended upwards to a 45 degree angle to the floor as
the head emerges from the pelvis and crowns.
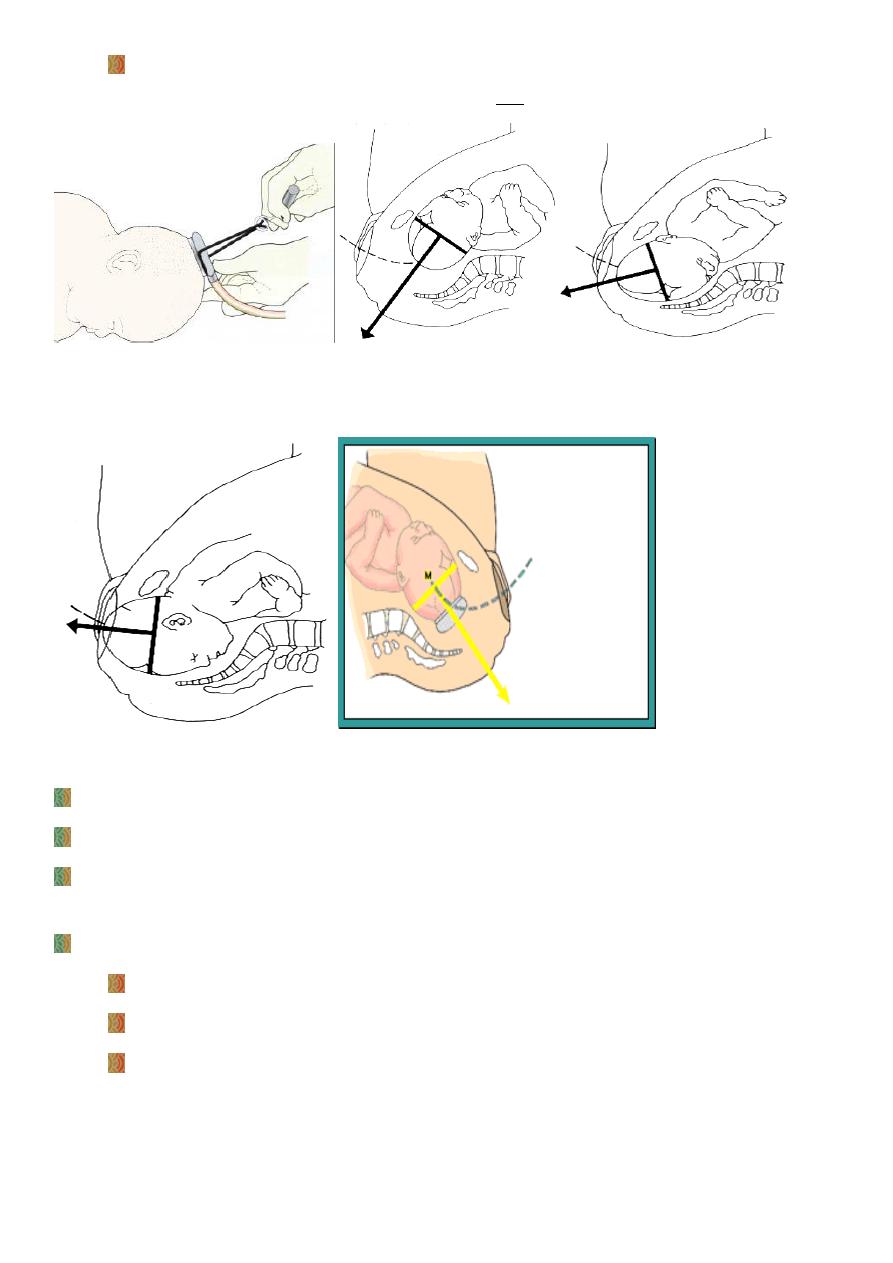
7
The handle of the device is allowed to passively turn as the head auto-rotates
through its descent. This will usually be at 90° to the cup.
((( Ventouse - method of traction. ( Mid Pelvis) ( Pelvic Floor)
Note the finger-thumb position. )))
( Outlet ) Axis Animation
Traction is applied in concert with uterine contractions and voluntary expulsive effort.
Descent should occur with each application of traction.
When the head is delivered, the suction is released, the cup is removed, and the
remainder of the delivery proceeds as usual.
During the procedure:
A maximum of two cup detachments should be allowed.
3 sets of pulls
Total vacuum application time should be ideally less than 15 minutes
8
Complications:
Assisted deliveries with both vacuum and forceps can be associated with significant
maternal and fetal complications, however, with good technique and adherence to
guidelines, the risk of complications to mother or baby is small.
Trauma to the genital tract is the commonest maternal comlicpation.
Postpartum haemorrhage.
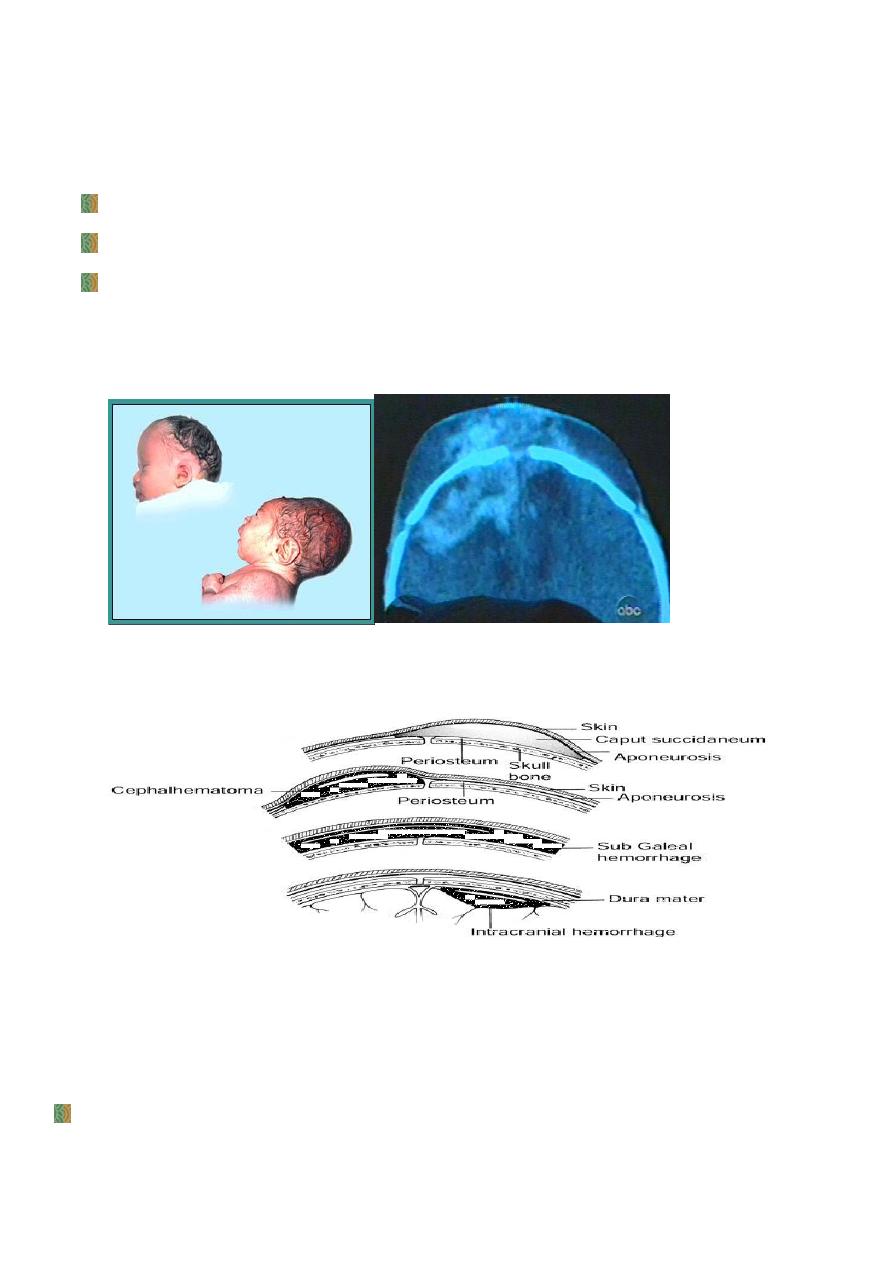
Fetal complication: most babies will have a chignon (oedematous skin bump) at the
site of the cup application. Some will also have a cephalhaematoma (subperiosteal
bleed). Rare serious intracranial injuries will be more likely to occur if multiple
attempts at delivery are made (especially if a variety of instruments is used).
CT of Subgaleal
Swellings and Bleeds Associated With Normal and Operative Vaginal Delivery
With any difficult instrumental delivery, the risk of shoulder dystocia occurring after
successful delivery of the fetal head should always be remembered.
Vacuum versus Forceps :
The obstetricians should be competent and confident in the use of both forceps and
ventouse.
9
“Selection of the appropriate instrument and decisions about the maternal and fetal
consequences should be based on clinical findings at the time of delivery.
The ventouse,when compared to the forceps:
is significantly more likely to:
Fail to achieve a vaginal delivery.
Be associated with cephalhaematoma (subperiosteal bleed).
Be associated with retinal haemorrhage (but this dosen’t seem to be of any clinical
significance).
Be associated with maternal worries about the baby.
And is significantly less likely to be associated with:
Use of maternal regional/ general anasthesia.
Significant maternal perineal and vaginal trauma
Severe perineal pain at 24 hours
And is equally likely to be associated with:
Delivery by cesarean section
Low 5 minutes Apgar score
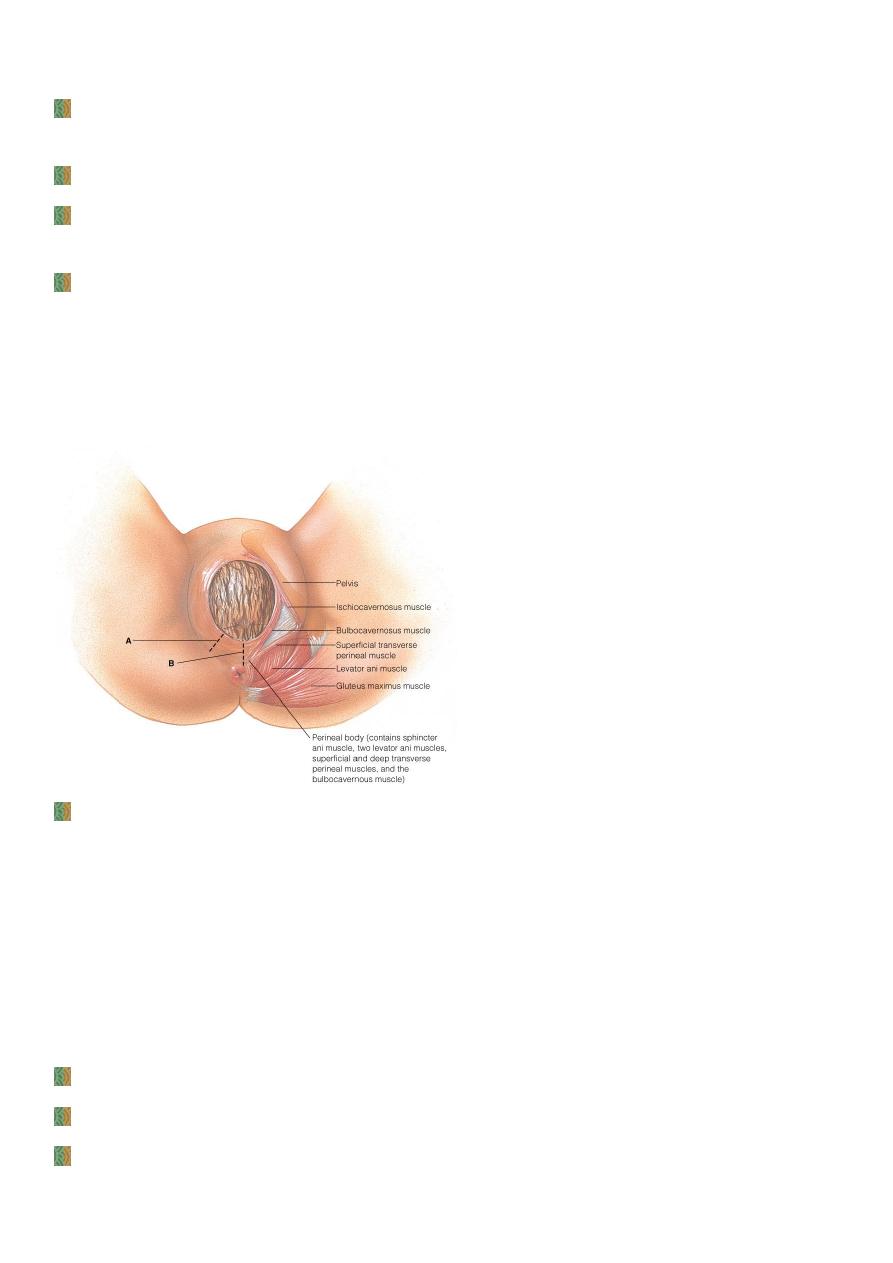
Episiotomy:
Intentional incision at perineum made to enlarge vulval outlet to ease birth process or to
protect mother from uncontrolled perineal lacerations.
11
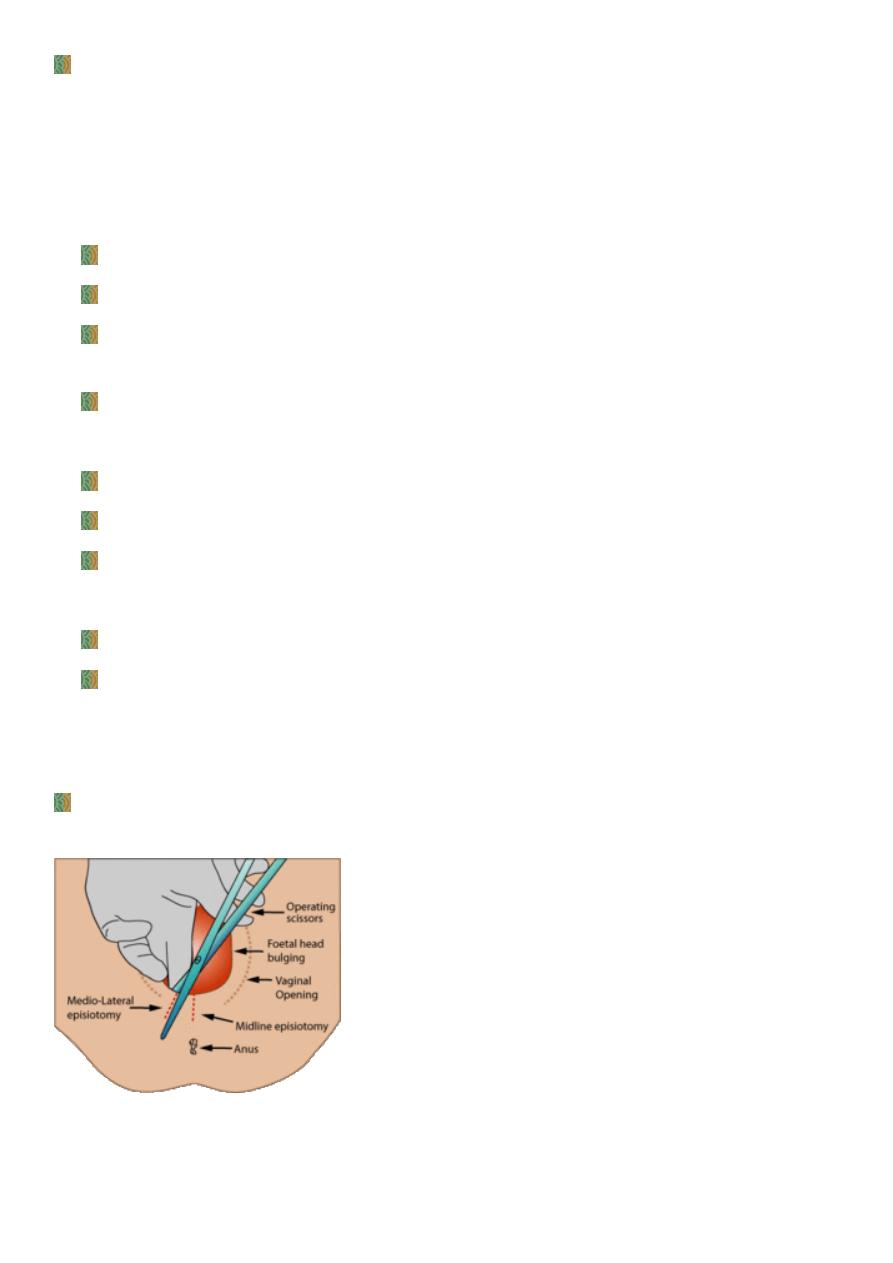
Technique:
An episiotomy is performed in the second stage, usually when the perinium is being
stretched (when the head is crowning) and it is deemed necessary.
If there is not a good epidural, the perinium should be infiltrated with local anaesthetic.
The incision can be midline or at an angle from the posterior end of the vulva (a
mediolateral episiotomy).
A mediolateral episiotomy is usually recommended; a midline episiotomy results in less
bleeding, quicker healing and less pain, however,there is an increased risk of extension
to involve the anal sphincter (third/ fourth-degree tear).
Episiotomies: Midline & Rt Mediolateral
In 2009, a Cochrane meta-analysis based on studies with over 5,000 women concluded
that: "Restrictive episiotomy policies appear to have a number of benefits compared to
policies based on routine episiotomy. There is less posterior perineal trauma, less
suturing and fewer complications, no difference for most pain measures and severe
vaginal or perineal trauma, but there was an increased risk of anterior perineal trauma
with restrictive episiotomy".
Indications:
Previous pelvic reconstructive surgery
When perineal muscles are excessively rigid
There is a serious risk to the mother of spontaneous irregular tear
11
When instrumental delivery is indicated
Prolonged late decelerations or fetal bradycardia during active pushing
shoulder dystocia (Note that the episiotomy does not directly resolve this problem, but
it is indicated to allow the operator more room to perform maneuvers to free shoulders
from the pelvis)
Fetal macrosomia
Complication:
Haemorrhage
Infection
Extension to the anal sphincter (third/ fourth-degree tears)
Dyspareunia.