


Infectious mononucleosis (IM) and Epstein-Barr virus (EBV)
• For Third- Year Medical Students• Dr: Hussein Mohammed Jumaah
• CABM
• Mosul Medical College
• 31/3/2014
EBV is a gamma herpes virus.
In developing countries, subclinical infection in childhood is virtually universal.In developed countries, primary infection may be delayed until early adult life.
The virus is acquired from asymptomatic excreters via saliva, by droplet infection, or by kissing.
EBV is not highly contagious ,isolation is unnecessary.
Infectious mononucleosis (IM) and Epstein-Barr virus (EBV)
Infectious mononucleosis (IM) and Epstein-Barr virus (EBV)
IM is an acute viral illness characterised by fever , pharyngitis, cervical lymphadenopathy, and lymphocytosis.
Whereas ~90% of cases of IM are due to EBV,
5–10% of cases are due to Cytomegalovirus (CMV).
CMV is the most common cause of heterophile-negative mononucleosis.
Less common causes rubella ,Toxoplasma, HIV, herpesvirus 6, hepatitis viruses and drug reactions.
Clinical features
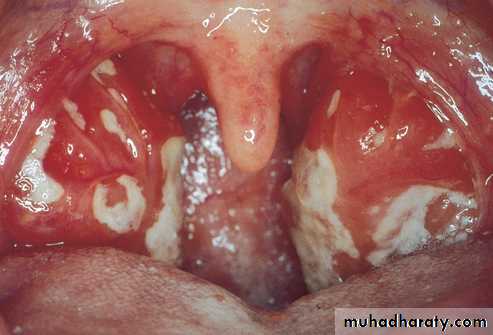
IM has a prolonged and undetermined incubation period, followed by a prodrome of fever, headache and malaise, succeeded by IMwith severe pharyngitis, which may include tonsillar exudates, and non-tender cervical lymphadenopathy.
Palatal petechiae, periorbital oedema, splenomegaly, macular, petechial or erythema multiforme rashes may occur.
In most cases fever resolves over 2 weeks, and other abnormalities settle over a further few weeks.
EBV may present with jaundice, PUO* or with a complication.
Death is rare but can occur due to
1. Respiratory obstruction.
2. Haemorrhage (splenic rupture or thrombocytopenia).
3. Encephalitis.
*pyrexia of unknown origin
Clinical features
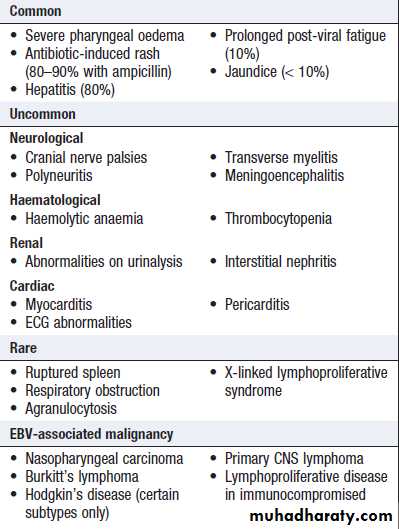
Complications of Epstein–Barr virusn infection
In children under 10 years the illness ismild and short-lived, but in adults over
30 years of age it can be severe and
prolonged.
Investigations
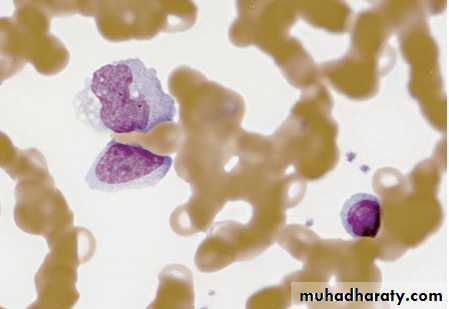
• Atypical lymphocytes are common in
• EBVinfection but also occur in other
• causes of IM, HIV infection, viral
• hepatitis, mumps and rubella. The most
• commonly used diagnostic criteria is
• the presence of 50% lymphocytes.
• (at least 10% atypical) .
• Atypical lymphocytes.
enlarged lymphocytes that have abundant cytoplasm, vacuoles, and indentations of the cell membrane .
• Diagnosis
A 'heterophile' antibody is present during the acute illness and convalescence, agglutinates erythrocytes of other species, e.g. sheep and horse.
detected by the classical
Paul-Bunnell titration or
a more convenient slide test such as the
'Monospot'.
• Investigations
Specific EBV serology (immunofluorescence) can be used to confirm the diagnosis if necessary.Acute infection is characterised by IgM antibodies against the viral capsid, antibodies to EBV early antigen and the initial absence of antibodies to EBV nuclear antigen (anti-EBNA).
Seroconversion of anti-EBNA at approximately1 month after the initial illness may confirm the diagnosis in retrospect.
CNS infections may be diagnosed by detection of viral DNA in cerebrospinal fluid.
• Investigations
Management
largely symptomatic. If a throat culture yieldsaβ-haemolytic streptococcus, a course of penicillin should be prescribed. ampicillin or amoxicillin in this condition commonly causes an itchy macular rash, and should be avoided.
When pharyngeal oedema is severe, a short course of corticosteroids, e.g. prednisolone 30 mg daily for 5 days, may help.
Antivirals are not sufficiently active against EBV.
Return to work or school is governed by the patient's physical fitness. contact sports should be avoided until splenomegaly has completely resolved because of the danger of splenic rupture.
10% of patients with IM suffer a chronic relapsing syndrome.



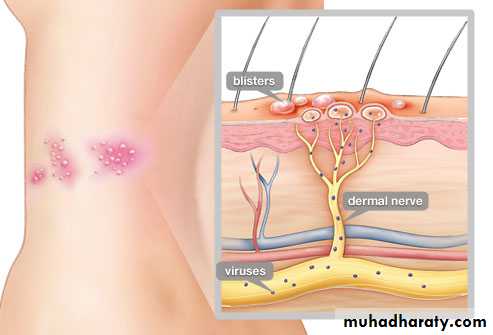
After initial infection ,Varicella zoster virus ,(VZV) persists in latent form in the dorsal root ganglion of sensory nerves and can reactivate in later life as a localised rash or with other clinical manifestations.
• Commonly seen in the elderly, shingles
• may also present in younger patients
• with immune deficiency.
• Chickenpox may be contracted from
• acase of shingles but not vice versa.
• It is not clear why this happens.
• Clinical features
Burning discomfort occurs in the affected dermatome, where discrete vesicles appear3-4 days later, associated with a brief viraemia and can produce distant satellite 'chickenpox' lesions.
Severe disease, a prolonged duration of rash, multiple dermatomal involvement or recurrence suggests underlying immune deficiency.
Clinical features
• Thoracic dermatomes are most
• Commonly involved .
• Ophthalmic division of the
• trigeminal nerve is also frequently
• affected;vesicles may appear on the
• cornea and lead to ulceration,and
• can lead to blindness.
• Bowel and bladder dysfunction
• occur with sacral nerve root
• involvement.
• The virus occasionally causes
• myelitis or encephalitis.
Clinical features



Ramsay Hunt syndrome
Involvement of the Geniculate ganglion causes facial palsy, ipsilateral loss of taste and buccal ulceration, plus a rash in the external auditory canal. This may be mistaken for Bell's palsy.Post-herpetic neuralgia
Postherpetic neuralgia arises in approximately 20% of patients .
Troublesome persistence of pain for 1-6 months or longer, following healing of the rash. It is more common with advanced age.


Clinical features
Management and preventionAciclovir has been shown to reduce both early- and late-onset pain. new drugs valaciclovir and famciclovir . demonstrate similar or superior efficacy and good safety and tolerability.
Post-herpetic neuralgia requires aggressive analgesia, along with agents such as amitriptyline or gabapentin. Capsaicin cream may be helpful. Although controversial, corticosteroids have not been demonstrated to reduce post-herpetic neuralgia to date.


Acyclovir for chickenpox/shingles
Aciclovir shortens symptoms in chickenpox by an average of 1 day. In shingles aciclovir reduces pain by 10 days and the risk of post-herpetic neuralgia by 8%. Aciclovir is therefore cost-effective in shingles but not chickenpox.'Human VZ immunoglobulin (VZIG) is used to attenuate infection in people who have had significant contact with VZV, are susceptible to infection (i.e. have no history of chickenpox or shingles and are negative for serum VZV IgG) and are at risk of severe disease (e.g. immunocompromised, steroid-treated or pregnant).
Newborn whose mother develops chickenpox no more than 5 days before delivery or 2 days after delivery.
Ideally, VZIG should be given within 7 days of exposure, but it may attenuate disease even if given up to 10 days afterwards.
Susceptible contacts who develop severe chickenpox after receiving VZIG should be treated with aciclovir.
A zoster vaccine (Zostavax) ,VZV vaccine ,.
Is a live, attenuated . Is exceedingly safe ,On March 24, 2011, the Food and Drug Administration (FDA) approved its use for the prevention of shingles in individuals 50 to 59 years of age, including persons who have already had an episode of shingles.
should not be given to individuals who have
• A weakened immune system
• Individuals with active, untreated tuberculosis.
• Pregnant women should not receive this vaccine.
UK ,its use has been restricted to non-immune healthcare workers and household contacts of immunocompromised individuals.
Children receive one dose after 1 year of age and a second dose at 4–6 years of age; seronegative adults receive two doses at least 1 month apart.
The vaccine may also be used prior to planned
iatrogenic immunosuppression, e.g. before transplant.
