R
CARDIOVASCULA
((
دكتور جاسم دائما يقول انا باالمتحان اجيب الناحية الكلنكل من المحاضرة
)
)
e
y artery diseas
Lec : coronar
محاضرة جدا مهم
ة
disease impact
-
غير مهم
ة
risk factors
-
التعداد مالها مه
م
ولكن الشرح المطول الي على كل رسك فاكتر غير مطلو
ب
>
---
> drugs
---
> management
--
chronic stable angina
-
ضيف
is normal
lipid drug like atrovastatin even if lipid profile
-
anti
p
, usually taken before slee
present
-
more than 2 mm in chest leads 3
-
more than 1 mm in limb leads 2
-
pathological st elevation should include: 1
-
s
in two or more adjacent lead
)
s( cardiac enzymes+cbc+rbs+rft
> basic investigation
---
> management
---
acute coronary syndrome
-
s
during first 12 hours from onset of symptom
-
STEMI 2
-
indication of thrombolysis : 1
-
rupture of papillary muscle lead to sever mitral regurg lead to
-
>mechanical complications : 1
---
complications of MI
-
k
and shoc
acute pulm edema
m
rupture of interventricular septu
-
2
e
> cardiac tamponad
---
rupture of ventricle
-
3
note : in case of pericarditis , nsaids and steroids increase risk of aneurysm and rupture of myocardium so should be
-
d
avoide
note : aspirin and clopidogrel and b blocker and ace inhibitor are "secondary preventive
>
----
maintanace therapy
-
"
measures
MI syndrome ( Dressler syndrome ) : characterized by persistent fever , pericarditis and pleurisy ,, probably due to
-
post
-
weeks after infarction ,, if symtoms are prolonged or sever, high dose of aspirin or nsaids
immunity ,, typically occur few
d
or corticosteroid may be neede
e
Lec : peripheral arterial diseas
g
> aspirin or clopidogrel 75m
---
antiplatelet
-
r
> antiplatelet with vasodilato
--
cilostazol
-
k
Lec : shoc
c
MAP = 1/3 systolic + 2/3 diastoli
-
neurogenic shock
-
غير مهم
ة
failure
Lec : heart
%
75
-
normal EF = 55
-
F
> decreased E
---
systolic dysfunction
-
F
> preserved E
---
diastolic dysfunction
-
)
kick" which is parially responsible for pumping blood to ventricles ( about 30%
note : in atrial fib there is loss of "atrial
-
)
gallop rythm : tachycardia + extra sound (s3 or s4
-
a
acute left sided HF = acute pulm edem
-
s
nd diuretic
hypokalemia due to renin angiotensin aldosterone system a
-
complication : 1
-
s
Hyperkalemia due to potassium sparing diuretic
c
BNP : increase in HF , sensitive but non specifi
-
management of acute HF
-
جدا جدا مهم
ة
s
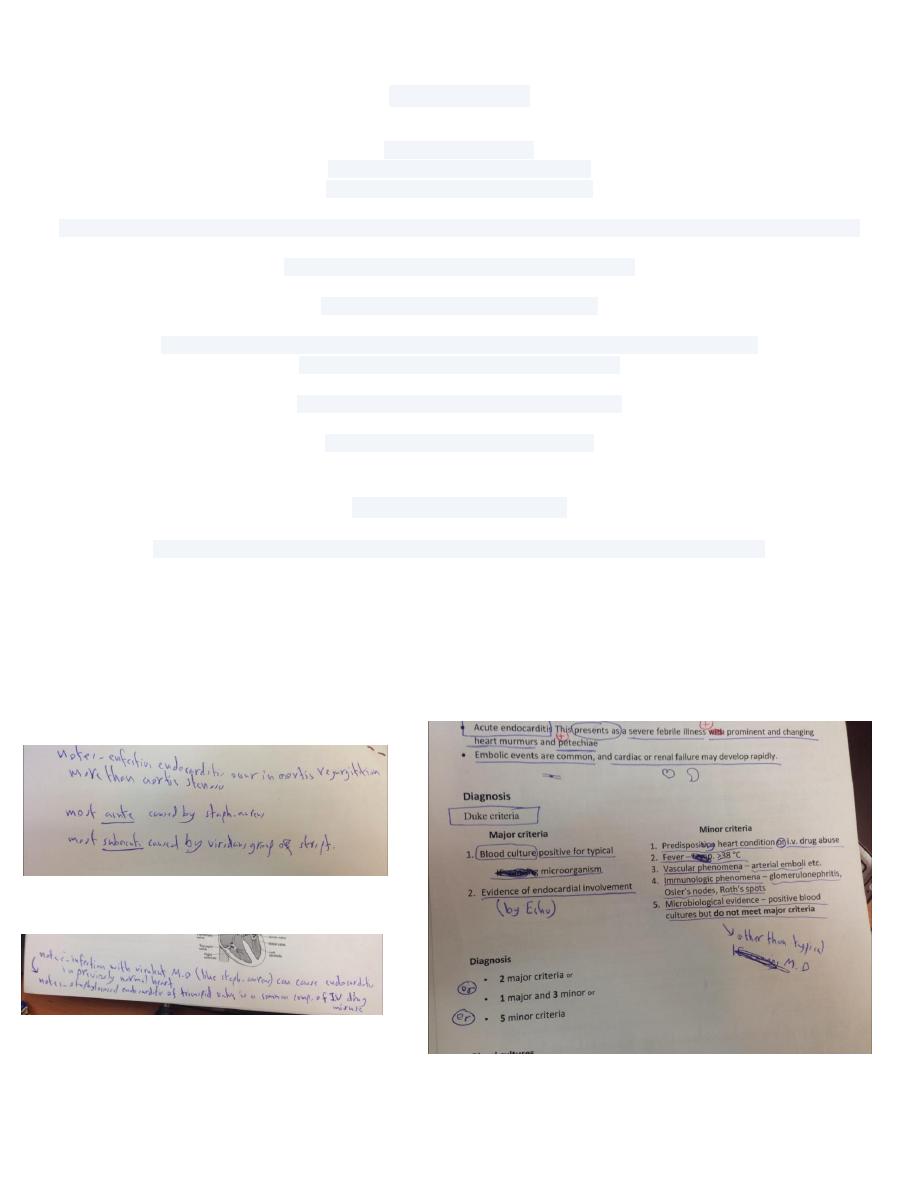
Lec : Infective endocarditi
)
ication+ prophylaxis
important subjects ( clinical features + diagnosis+ treatment + compl
-
:
characteristics of antibiotics given
-
l
bactericida
-
1
l
parentera
-
2
s
in large dose
-
3
e
for long tim
-
4
y
Lec : myocarditis and cardiomyopath
-
المهمين
p
: dilated CMP and hypertrophic CM
-
غير المهمين
p
: restrictive CMP and arrythmogenic CM
)
in dilated CMp , echo is diagnostic ( ecg not diagnostic
-
c
diastoli
–
pulsr pressure = systolic
-
s
Lec : pericarditi
d
retrosternal pain relevied by sitting and leaning forwar
-
?
etween pleural rub and pericardial rub ?
how can we diff b
-
b
> pleural ru
--
We ask patient to hold his breath , if rub disappear
b
> pericardial ru
--
If not
e
> subxiphoid approach is the best on
---
treatment of pericardial effusion
-
d
tuberculus percardial effusion is usually hemorrhagic while tuberculus pleural effusion is usually straw colore
-
e
diastolic collapsr of right atrium and ventricle is diagnostic for cardiac tamponad
-
n
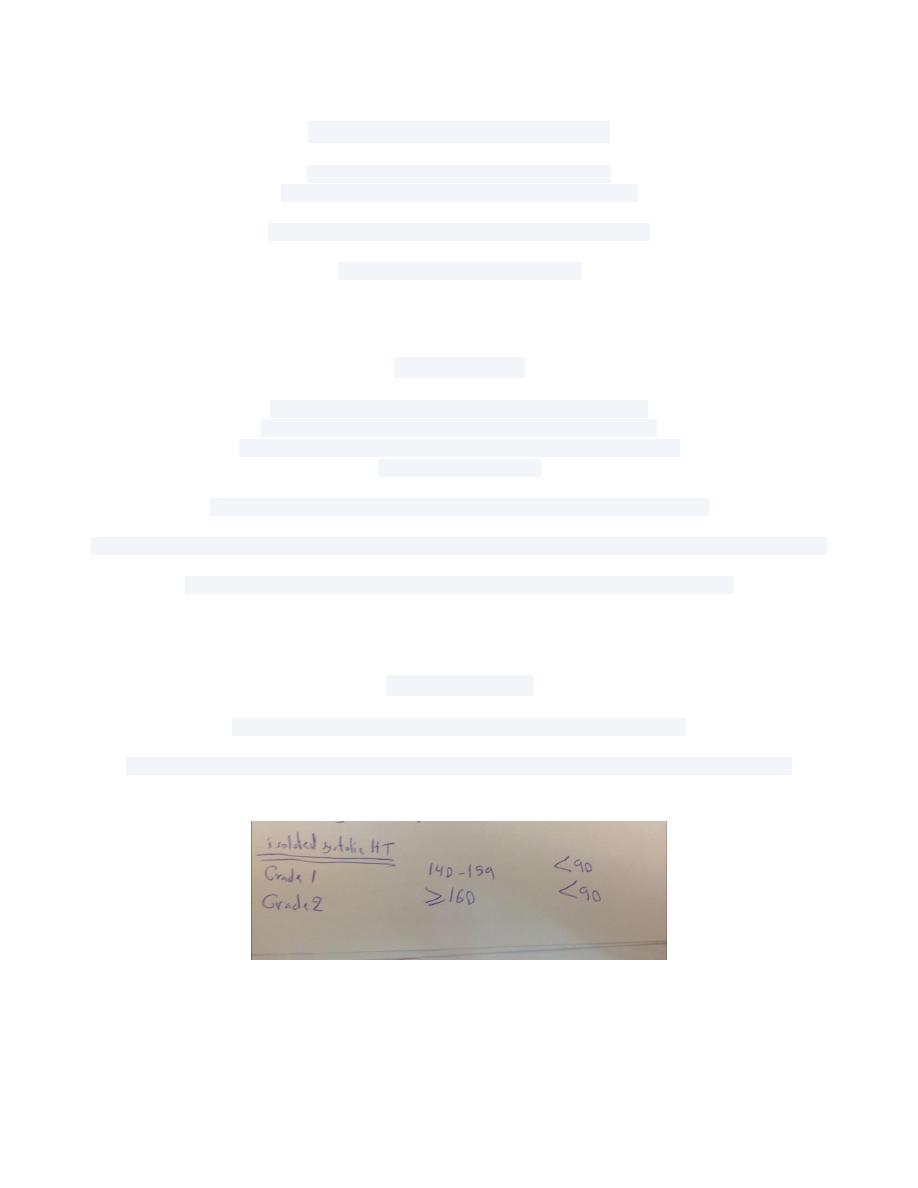
Lec : hypertensio
s
ines : start managemet with diuretic
note: according to new guidel
-
n
attacks of hypotensio
-
refractory HT 3
-
white coat HT 2
-
indications of ambulatory BP recordings 1
-