Forth stage
HYPERTHYROIDISMLec-1
د.فاخر
1/1/2014
Iodine MetabolismIodine is the raw material for thyroid hormone synthesis.
Ingested iodine is converted to iodide and then absorbed
The principal organs that take up the iodide are the thyroid which uses it to make thyroid hormones and the kidneys which excrete it in the urine.
Thyroid Hormone synthesis
The follicular epithelial cells synthesise thyroid hormones by incorporating iodine into the amino acid tyrosine on the surface of thyroglobulin (Tg), a protein secreted into the colloid of the follicleIn the thyroid, iodide is oxidized to iodine and bound within secs to tyrosine attached to thyroglobulin.
The enzyme responsible for oxidation and binding of of iodide is Thyroid Peroxidase.
Monoiodotyrosine (MIT) is next iodinated to Diiodotyrosine(DIT)
2 DIT molecules underao oxidative condensation to form Thyroxine(T4)
T3 is probably formed by condensation of MIT and DIT.
T3 and T4 circulate in plasma almost entirely (> 99%) bound to transport proteins, mainly thyroxine-binding globulin (TBG). It is the unbound or free hormones which diffuse into tissues and exert diverse metabolic actions. While it is possible to measure the concentration of total or free T3 and T4 in plasma.
Physiology
The functions of thyroid hormone are1- Faceletate growth and development.
2- Interfere with carbohydrate protein and fat metabolism.
3- Increase oxygen consumption by the tissue, basal metabolic rate, and heat production.
4- Increase oxygen release from HB.
5- Augmentation of adrenalin and noradrenalin function.
Thyrotoxicosis (Hyperthyroidism)
“Hyperthyroidism” refers to overactivity of the thyroid gland leading to excessive synthesis of thyroid hormones and accelerated metabolism in the peripheral tissues. The secretion of thyroid hormone is no longer under the regulatory control of the hypothalamic-pituitary center.Hormone excess causes:
1- Graves' disease2- Multinodular goiter
3- Toxic adenoma
Epidemiology
Prevalence of hyperthyroidism in the general population is 1.2%Graves’ Disease – most common etiology 0.4%
Graves’ Disease is more common in females (7:1 ratio)
Graves' Disease
The Classic Triad of Graves’ Disease
1-Hyperthyroidism (90%) With or without a diffuse goitre2-Ophthalmopathy (20-40%) proptosis, ophthalmoplegia, conjunctival irritation
3-Dermopathy (0.5-4.3%) localized myxedema, usually pretibial especially common with severe ophthalmopathy
These features usually occur in thyrotoxic patients,. Graves' disease can occur at any age but is unusual before puberty and most commonly affects women aged 30-50 years
The thyrotoxicosis results from the production of IgG antibodies directed against the TSH receptor on the thyroid follicular cell, which stimulate thyroid hormone production and, in the majority, goitre formation. These antibodies are termed thyroid-stimulating immunoglobulins or TSH receptor antibodies (TRAb)
Graves’ Ophthalmopathy
Antibodies to the TSH receptor also target retroorbital tissues > T-cell inflammatory infiltrate -> fibroblast exophthalmus
Severe: keratopathy, diplopia, ,com-pressive optic neuropathy
Eyes

1) Lid lag slowly moving point from above eye level to below and see if eyelid smoothly follows movement of eye
2) Lid retraction: Lid retraction due to exophalmos (protrusion)
Pretibial myxedema: fibroblasts produces hyaluronic acid and chondroitin sulfate
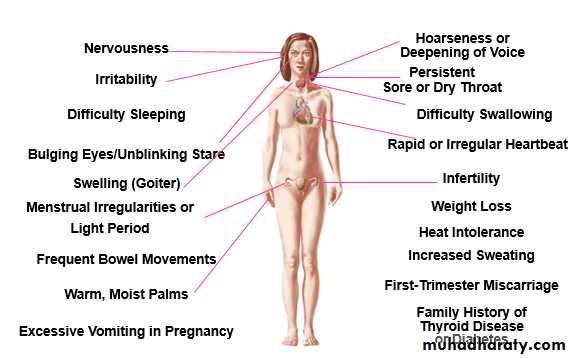
Features of Hyperthyroidism
Weight loss, heat intolerance
Thinning of hair, softening of nails
Stare and eyelid lag
Palpitations, symptoms of heart failure
Dyspnea, decreased exercise tolerance
Diarrhea
Frequency, nocturia
Psychosis, agitation, depression
Cardiac manifestations: Palpitations, Dyspnoea on exertion, Angina, Ankle swelling
Sinus tachycardia, Atrial fibrillation, Systolic hypertension/ increased pulse pressure,Cardiac failureGastroenterology: Diarrhoea, steatorrhoea, hyperdefecation, Vomiting
Neuromuscular: Anxiety, irritability, emotional lability, psyachosis, Tremor, Muscle weakness, Periodic paralysis, Hyper-reflexia, sustained clonus, Proximal myopathyBulbar myopathy
Dermatological: Sweating, Pruritis, Alopecia
Reproductive: Amenorrhoea, Infertility, abortion, Loss of libido, impotence,
Investigations:
Thyroid function tests
1-Total T3 = 1.2 to 2.8 nmol\L
2-Total T4 = 150 nmol\L
3-TSH 0.5 to 5 mU\L.
measuring of:
1- freeT4=10-30nmol\L
2- freeT3=0.3-3.3nmol\L
3- TSH = 0.5 to 5 mU\L which is the most sensitive and specific test for the diagnosis of hyper- and hypothyroidism
4- Autoantibody: TPH (thyroid peroxidase), and anti thyroglobulin anti body.
Diagnostic Imaging
Radioactive Iodine Uptake
Shows distribution of uptake
Technetium-99 Pertechnetate Uptake
Distinguishes high-uptake from low-uptake
Thyroid ultrasonography: Identifies nodules
Doppler can distinguish high from low-uptake
Thyroid scanning: iodine 123 (123I) and iodine 131 (131I) Technetium Tc 99m
pertechnetate (99mTc).The images obtained by these studies provide the size and shape of the gland and the distribution of functional activity.Management
The choice of therapy depends on:
1-Age of the patient
2-Size of the thyroid
3-Type of thyroxicosis
Guide in thyrotoxicosis treatment
1-Graves below 45 year: anti thyroid drug2-No response or large goiter or recurrence: surgery
3-Graves above 45 year: RAI
4-Toxic multinoduler: surgery
5-Toxic nodule: surgery. if not fit: RAI
6-Recurrent after surgery above 45 year: RAI
7-Pregnancy: surgery in the first and second trimester
Antithyroid (propylthiuracil) in the third trimester in low doses.
Antithyroid drugs
carbimazole 40-60 mg dailyprophylthiouracil 400-600 mg daily. There is subjective improvement within 10-14 days and the patient is usually clinically and biochemically euthyroid at 3-4 weeks, when the dose can be reduced. The maintenance dose is determined by measurement of T4 and TSH, attempting to keep both hormones within their respective reference ranges...
Adverse effects: Rash, Arthralgias, Urticaria, GI symptoms, Agranulocytosis
β-adrenoceptor antagonist (β-blocker), such as propranolol (160 mg daily) or nadolol (40-80 mg daily), will alleviate but not abolish symptoms within 24-48 hours. Beta-blockers cannot be recommended for long-term treatment, but they are extremely useful in the short term, e.g. for patients awaiting hospital consultation or following 131I therapy.
Radioactive iodine
131I is administered orally as a single dose and is trapped and organified in the thyroid .Although it will decay within the thyroid in a few weeks, the effects of its radiation are long-lasting, with cumulative effects on follicular cell survival and replication.Subtotal thyroidectomy
Patients must be rendered euthyroid with antithyroid drugs before operation. Potassium iodide, 60 mg 8-hourly orally, is often added for 2 weeks before surgery to inhibit thyroid hormone release and reduce the size and vascularity of the gland, making surgery technically easier. Complications of surgery are rare.Treatment of Ophthalmopathy
-Mild Symptoms:Eye shades, artificial tears
-Progressive symptoms (injection, pain):
Oral steroids – typical dosage from 30-40mg/day for 4 weeks
Impending corneal ulceration, loss of vision
Oral versus IV steroids
Orbital Decompression surgery