“Description of a skin lesion &
Clinical dermatological signs”
Alkindy college of medicine
Fifth stage
2015
Mostafa Hatim
List of contents
Slide number
Description of a skin lesion
3 - 78
Lesion type (Primary & secondary skin
lesions)
4
Changes encountered in skin
44
Lesion Configuration
49
Texture
59
Area involving the lesion & Lesion shape
65
Location and Distribution
70
Color
75
Clinical dermatological signs
79 - 84

“Description of a skin lesion”

(1)
Lesion type (Primary &
secondary skin lesions)
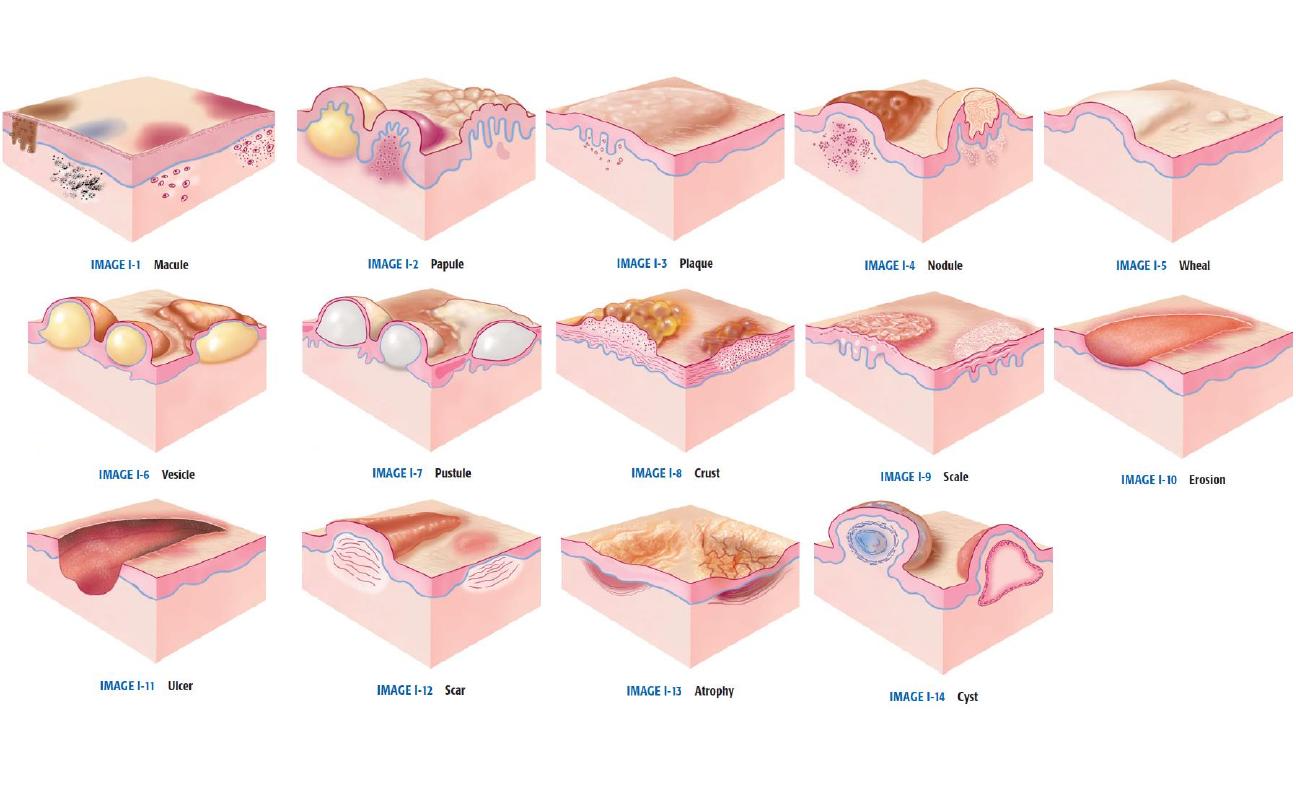
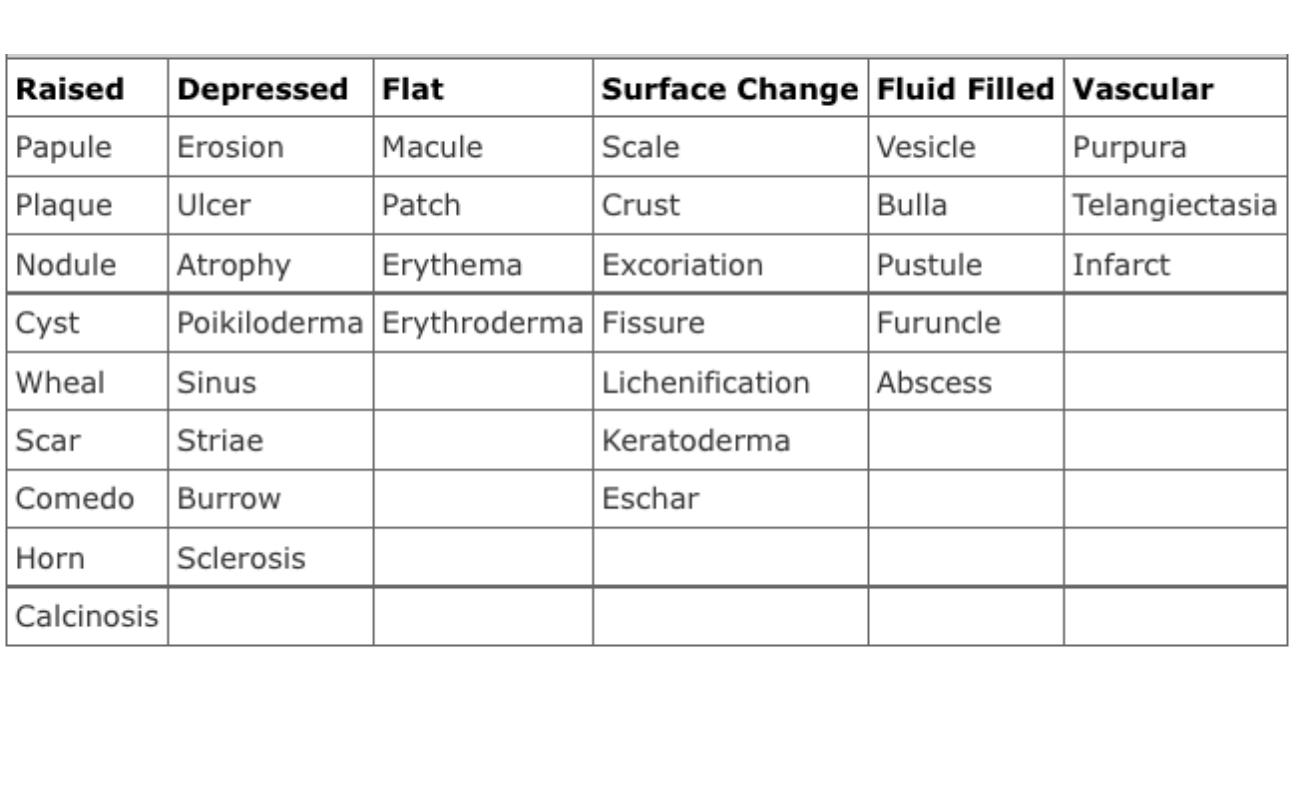

Primary skin
lesions

Erythema
: Redness caused by vascular dilatation

Macule:
Small flat area of altered color or texture

Patch:
Large macule > 0.5 cm in diameter
Papule:
Elevated solid lesion up to 0.5 cm
Papule

Papule

Plaque:
Elevated area of skin > 0.5 cm, often formed by confluence of
papules
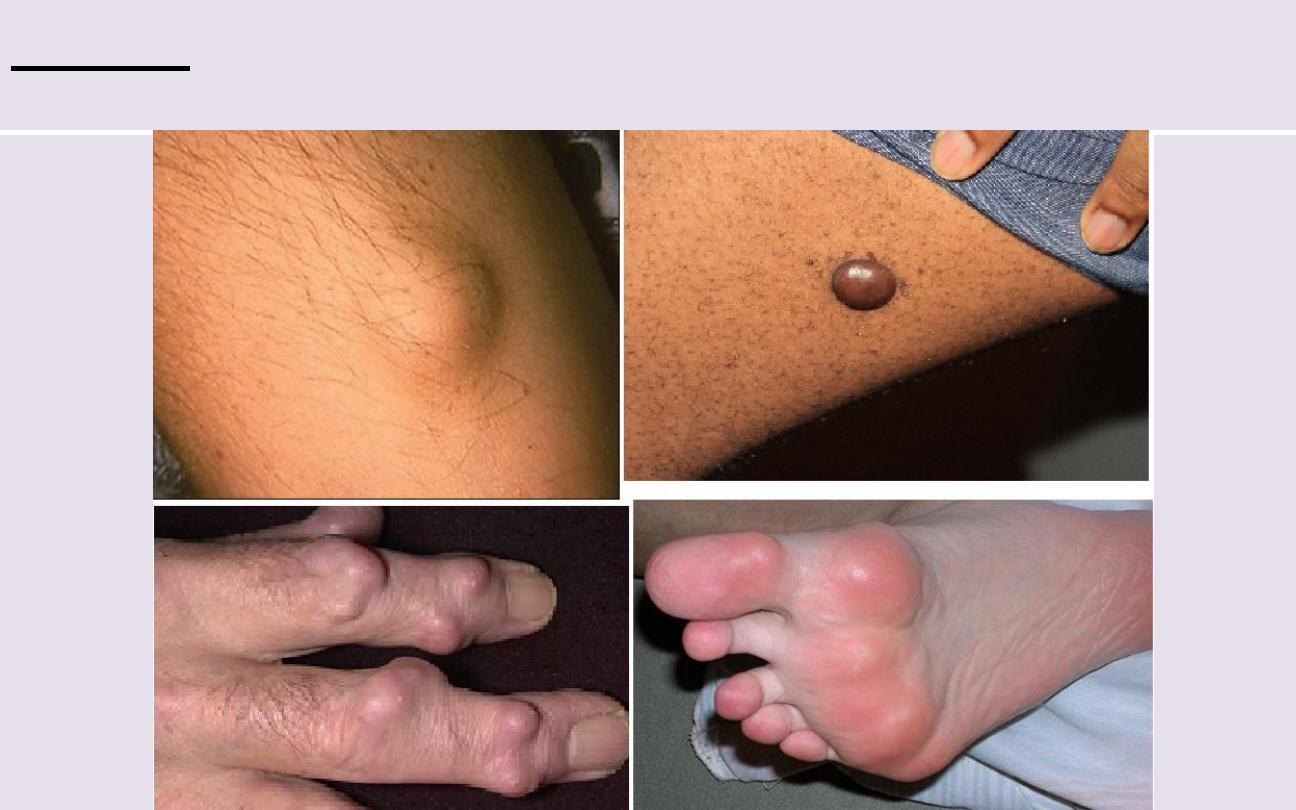
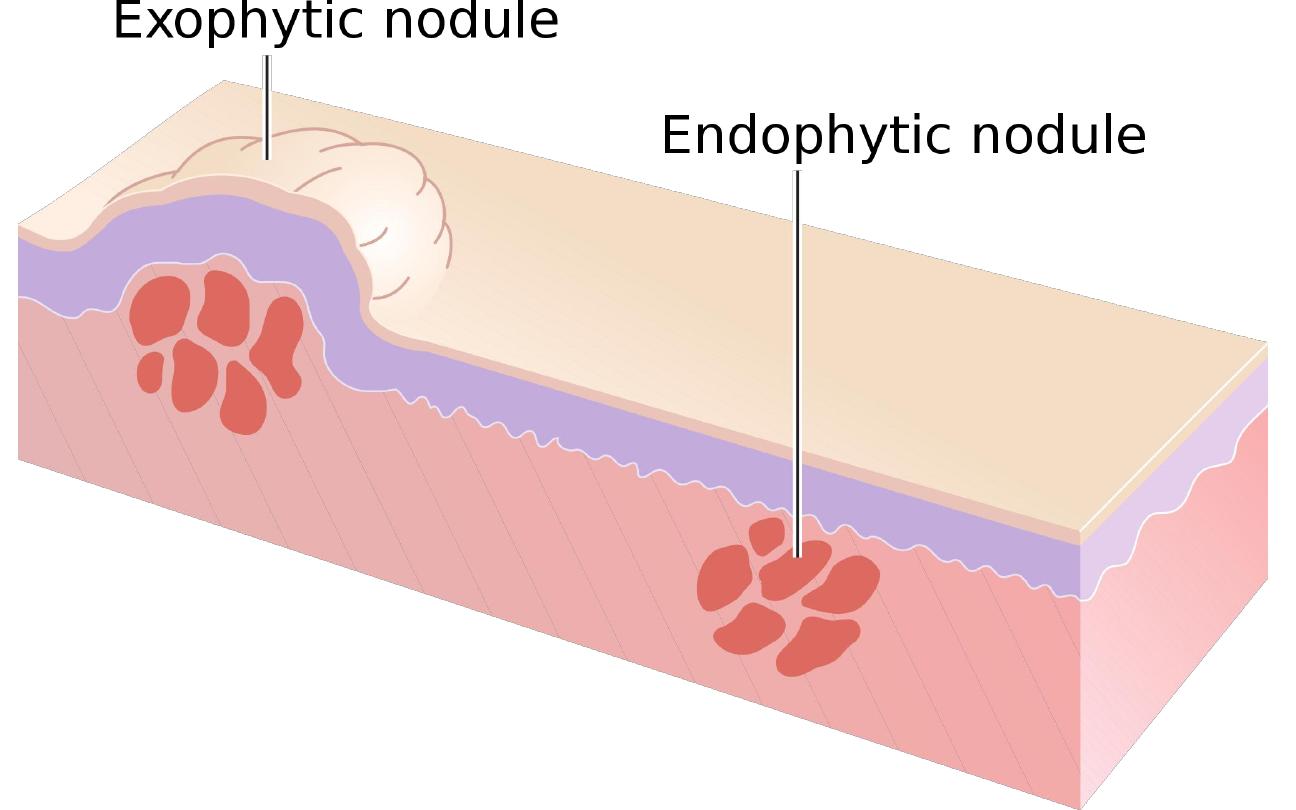
Nodule:
Circumscribed, elevated, solid lesion, usually > o.5 cm in
diameter in both width & depth.
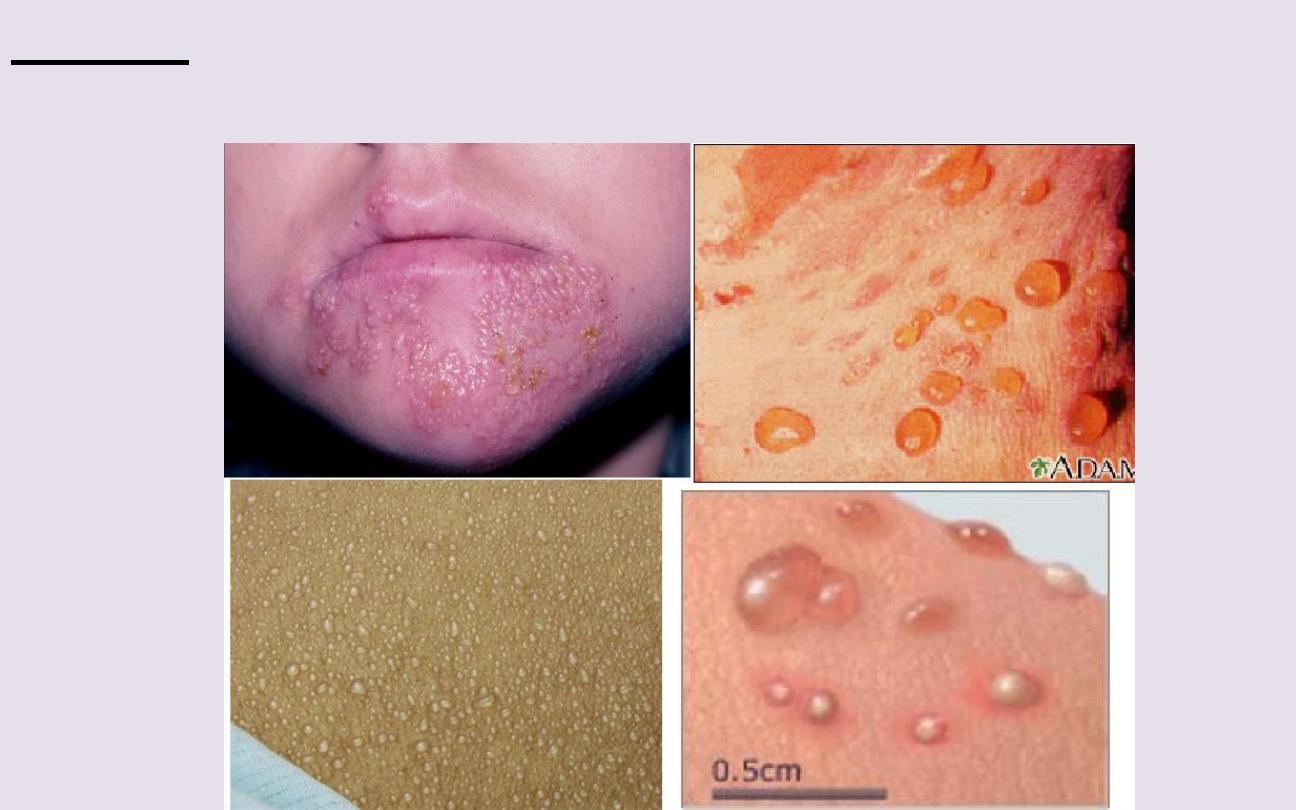
Vesicle:
Circumscribed, elevation of skin, < o.5 cm in diameter &
containing fluid.

Pustule:
A visible accumulation of pus in the skin.

Abscess:
Localized collection pf pus in cavity > 1cm in diameter

Wheal:
Elevated, white, compressible evanscent area produced by
dermal odema
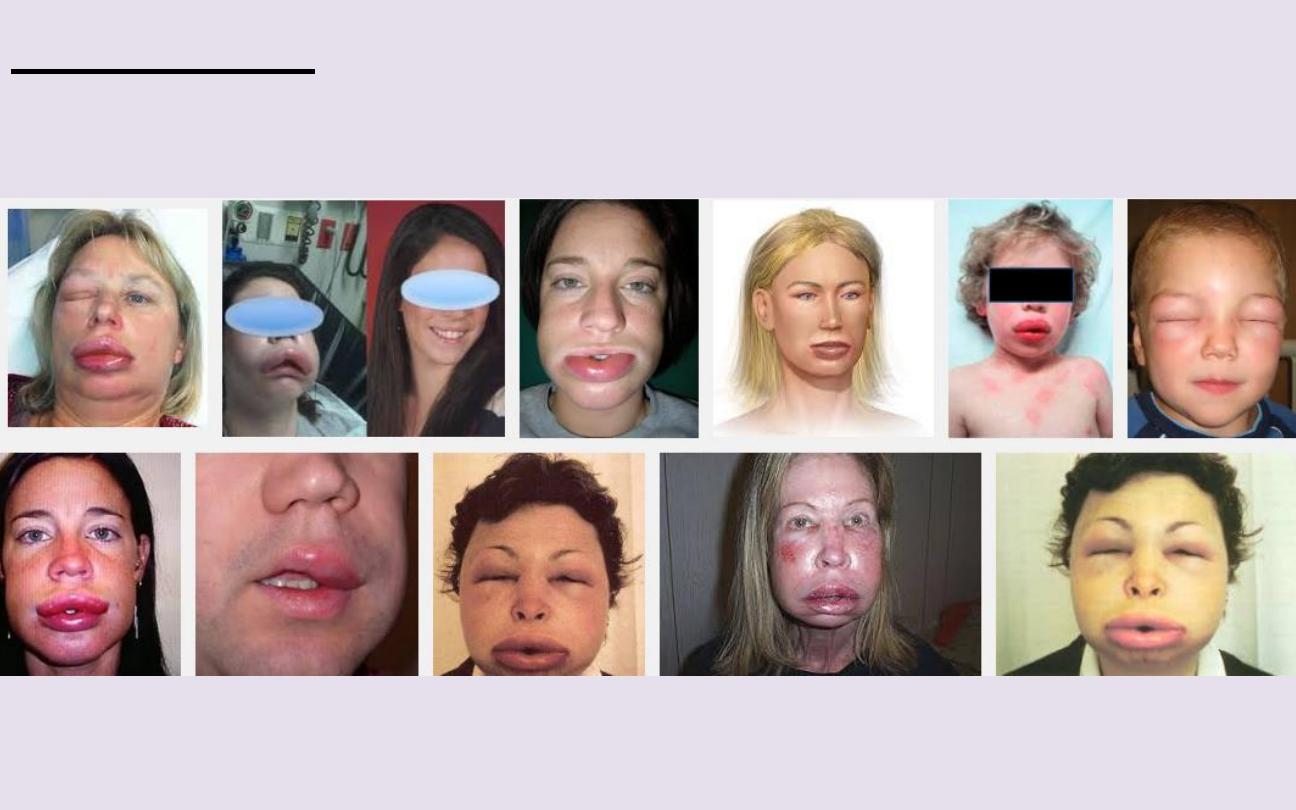
Angioedema:
Diffuse swelling caused by odema extending to the
subcutaneous tissue.

Cyst:
Closed cavity or sac with an epithelial lining & containing fluid or
semisolid material.

Petechia:
Pin-head sized macules of blood in the skin

Ecchymosis:
Macular area of haemorrhage > 2 cm.

Purpura:
Extravasation of blood into the skin up to 2 mm in diameter.

Haematoma:
Swelling from gross bleeding

Burrow:
Small tunnel in the skin that houses a parasite.

Open comedon (Black heads):
Plug of keratin & sebum in a
dilated piloseba-ceous orifice with dilated follicular orifice.

Closed comedon (White heads):
Plug of keratin & sebum in a
dilated piloseba-ceous orifice with narrow follicular orifice.

Telangiectasia:
Visible dilatation of small cut blood vessel.
Secondary
skin lesions
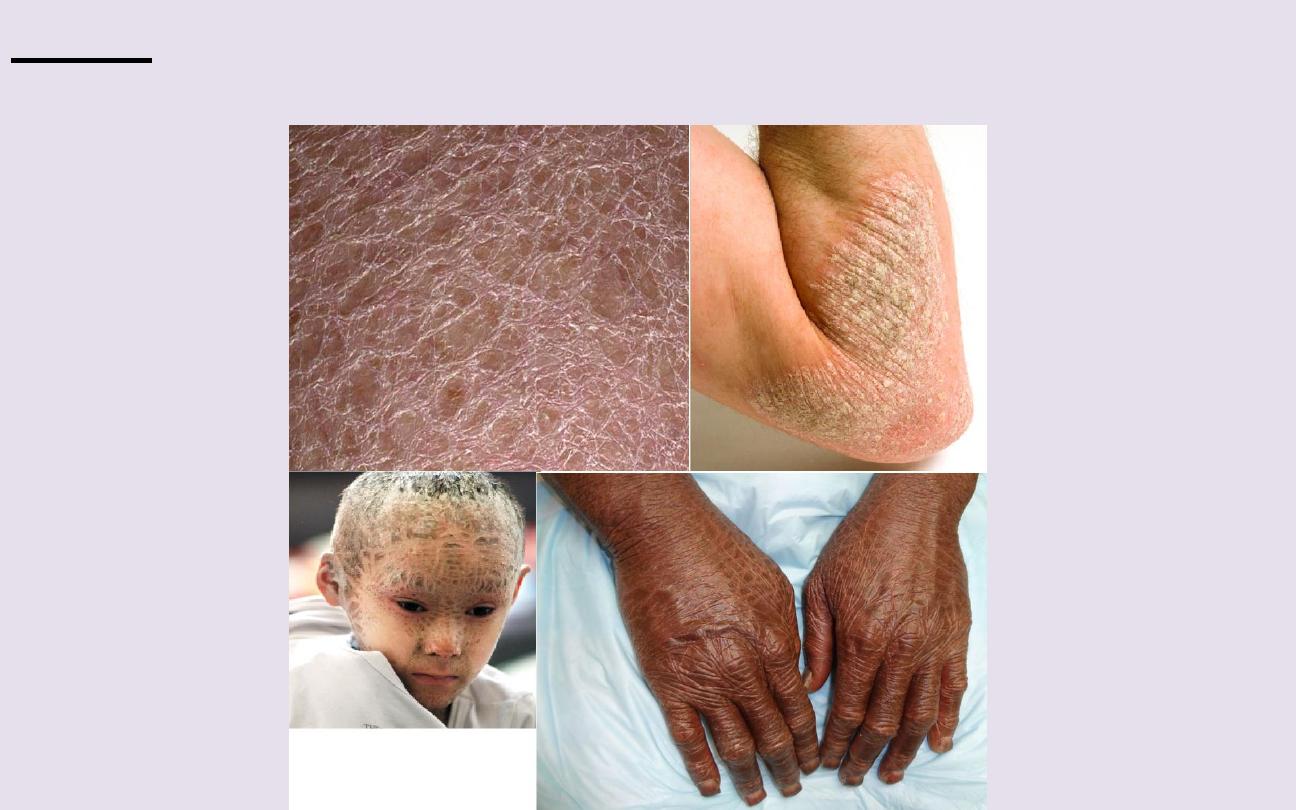
Scale:
Flat plate or flake of stratum corneum

Crust:
Dried serum & other exudates.
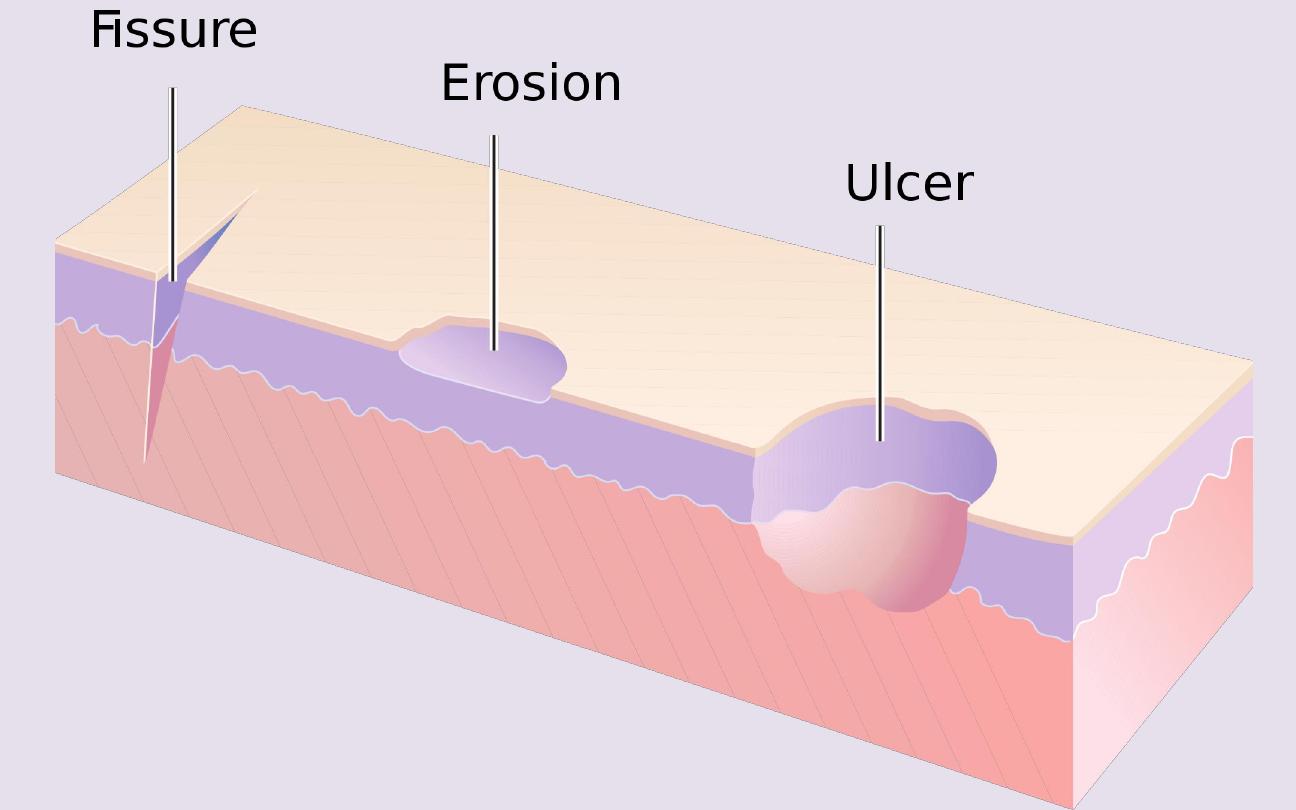

Erosion:
Focal loss of epidermis, not penetrate below DEJ, heal without
scarring.

Ulcer:
Focal loss of epidermis, dermis, subcutaneous tissue, heal with
scaring.

Fissure:
Linear gap or a slit in the skin surface.

Atrophy:
Depression of skin result from thinning of epidermis, dermis
or subcutaneous tissue.
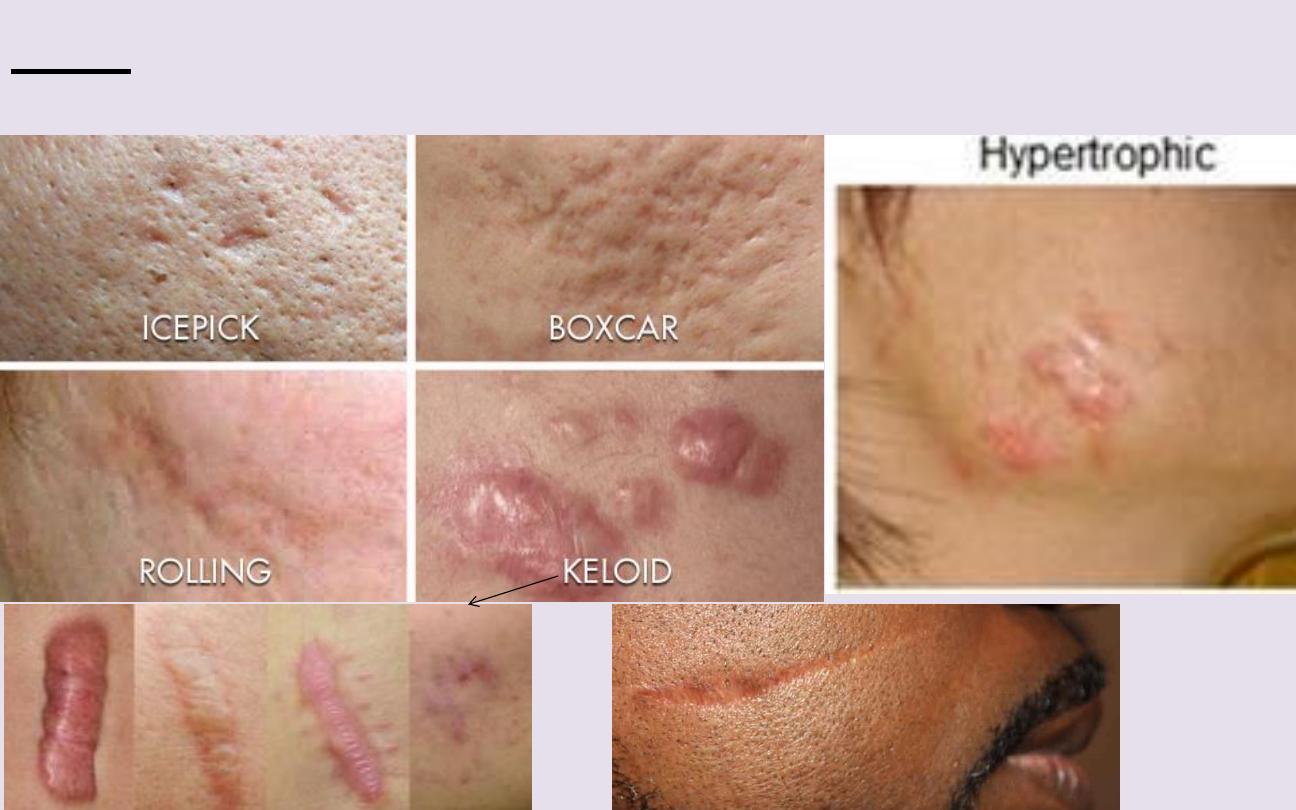
Scar:
Is a result of healing where normal structure are permanently
replaced by fibrous tissue.
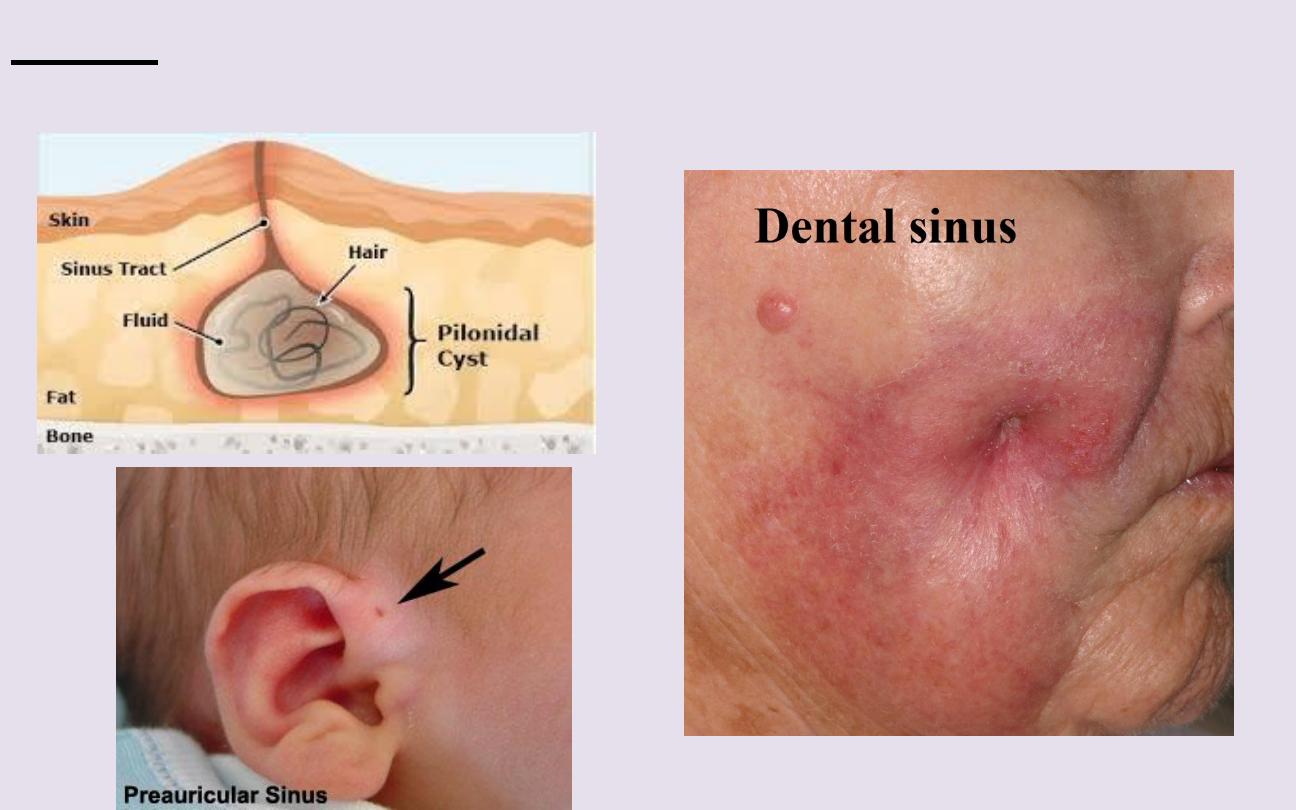
Sinus:
Channel that permits the escape of fluid or pus.
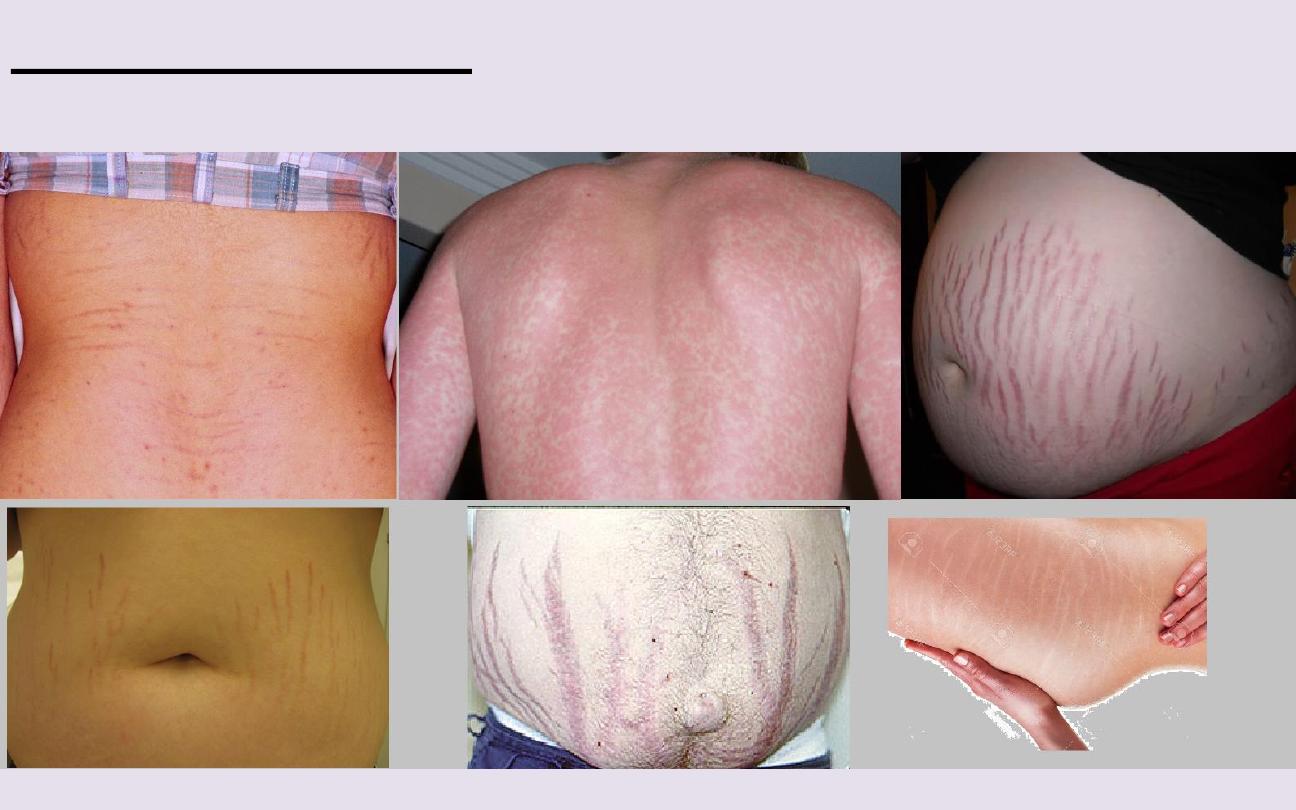
Stria (Stretch mark):
Is a streak-like linear atrophic pink, purple or
white lesion of the skin caused by changes in connective tissue.

Excoriation:
Loss of skin substance caused by scratching.
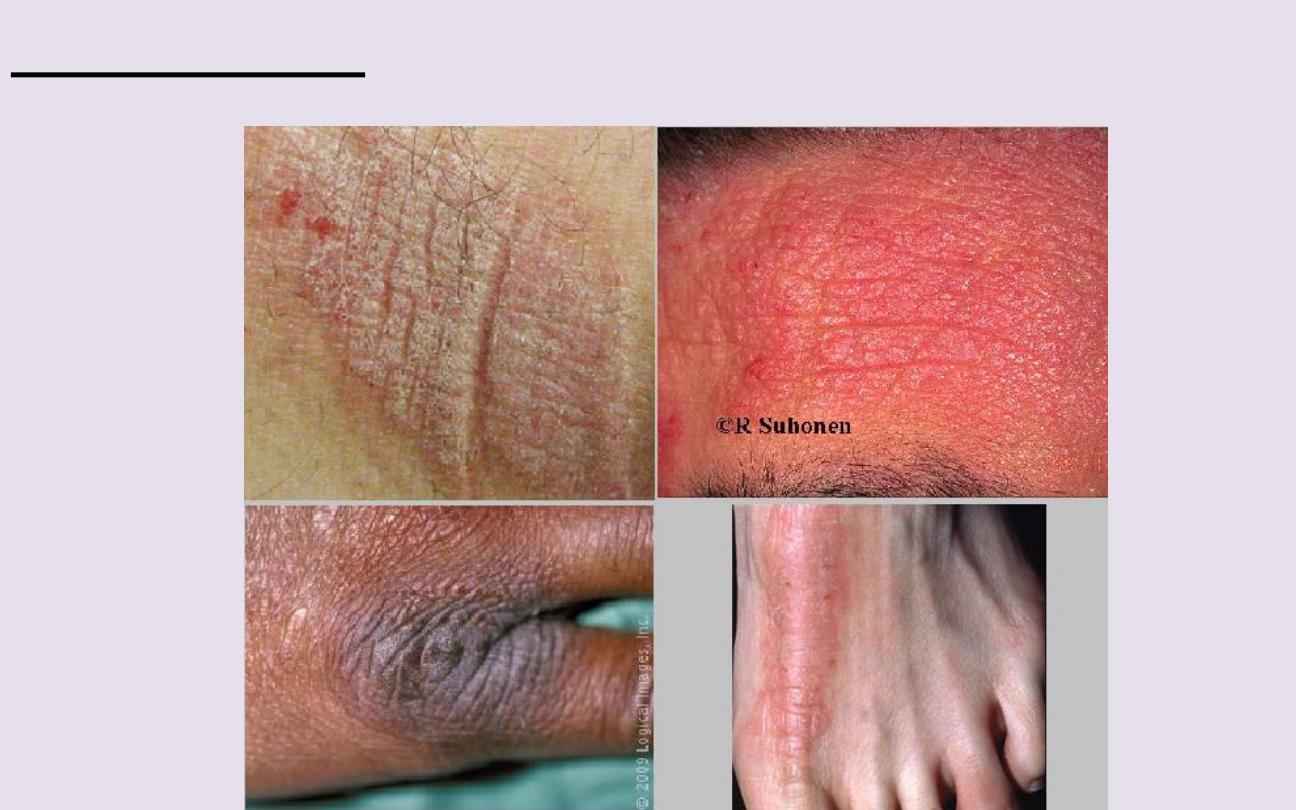
Lichenification:
Thickened skin with exaggeration of normal skin line

(2)
Changes
encountered in
skin
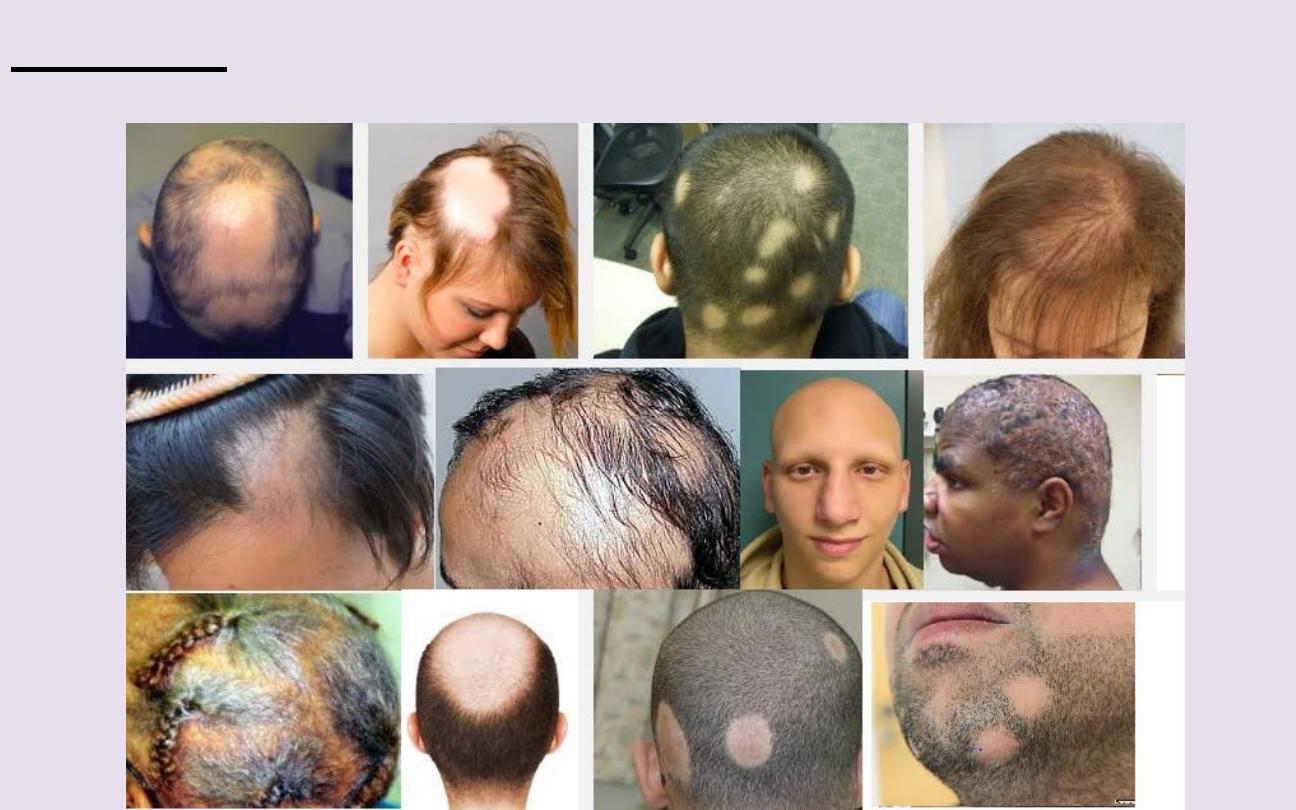
Alopecia:
Hair loss from any part of the body.
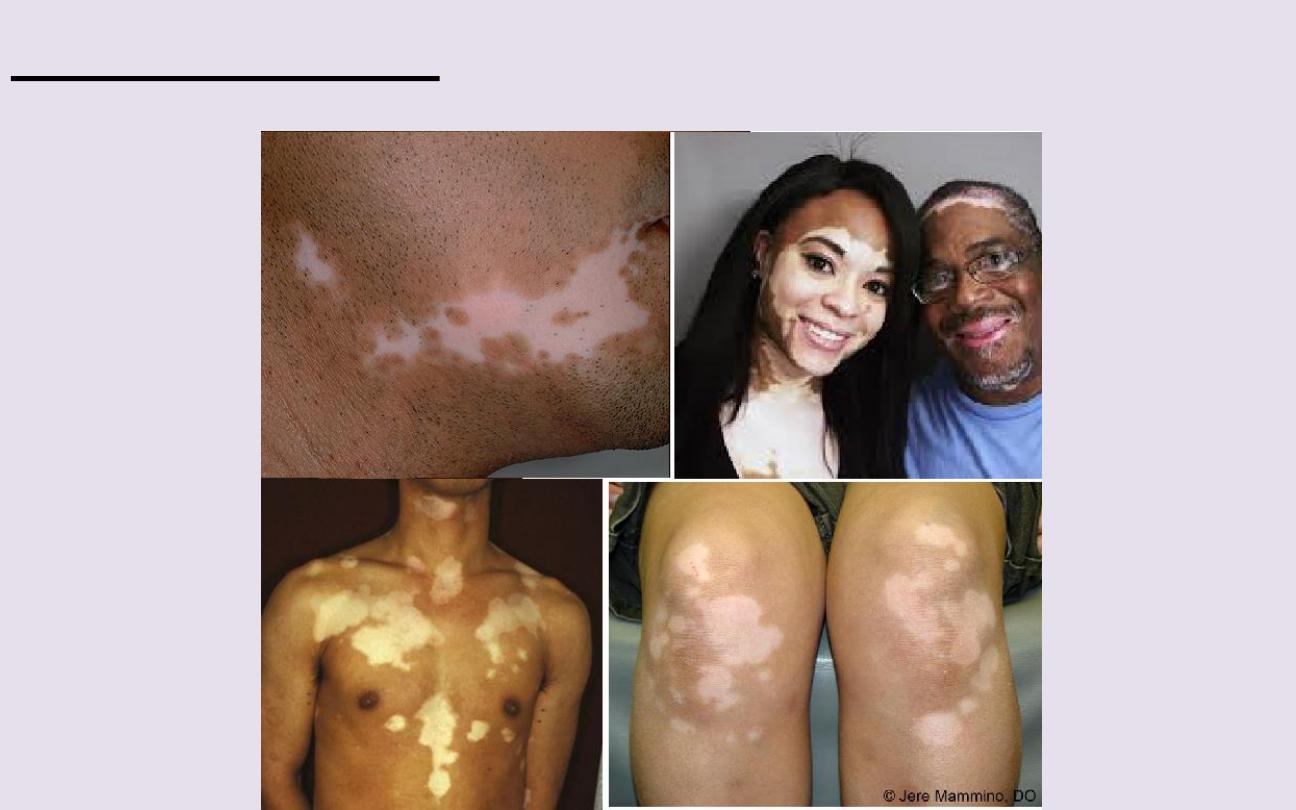
Depigmented skin:
Complete loss of pigment of the skin.

Hypopigmented skin:
Lightening of the skin due to decreased
melanin activity.

Hyperpigmented skin (melanosis):
Darkening of the skin due
to increased melanin activity.

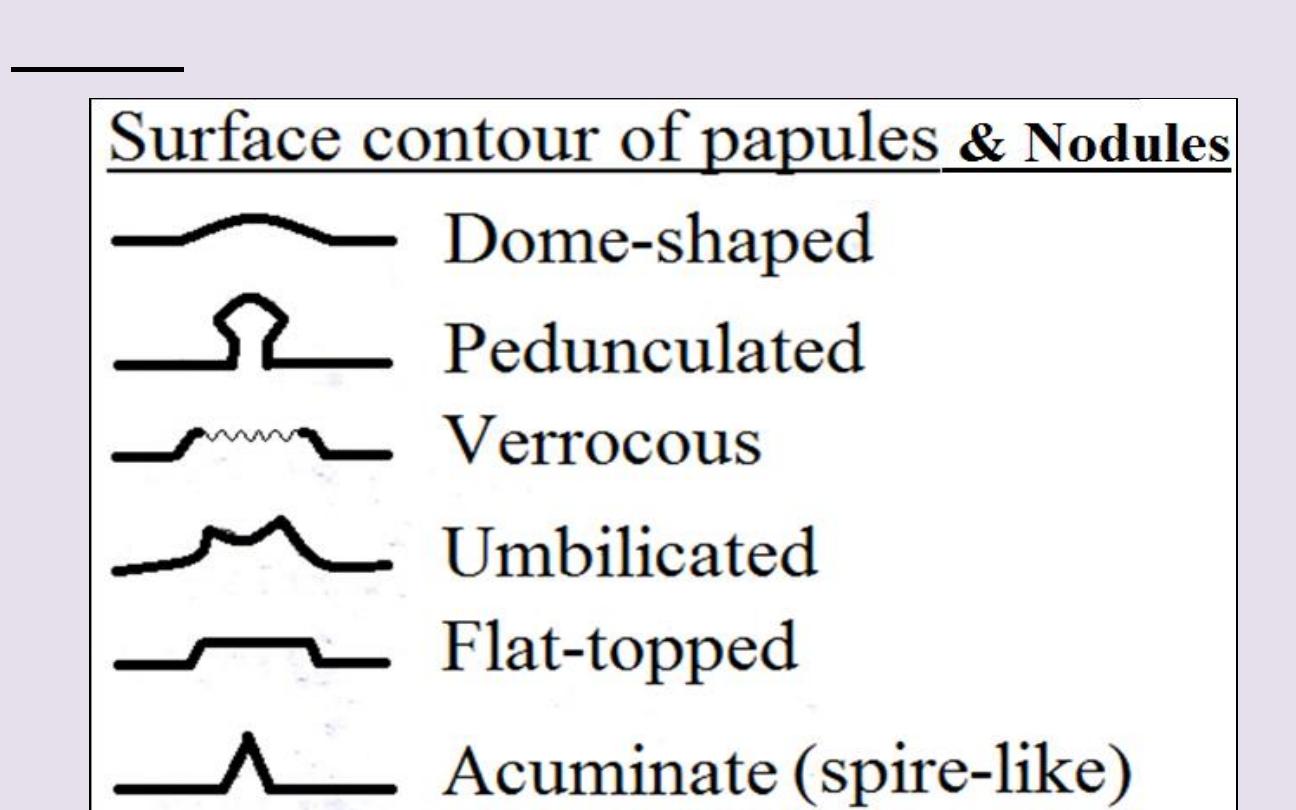
(3)
Lesion
Configuration
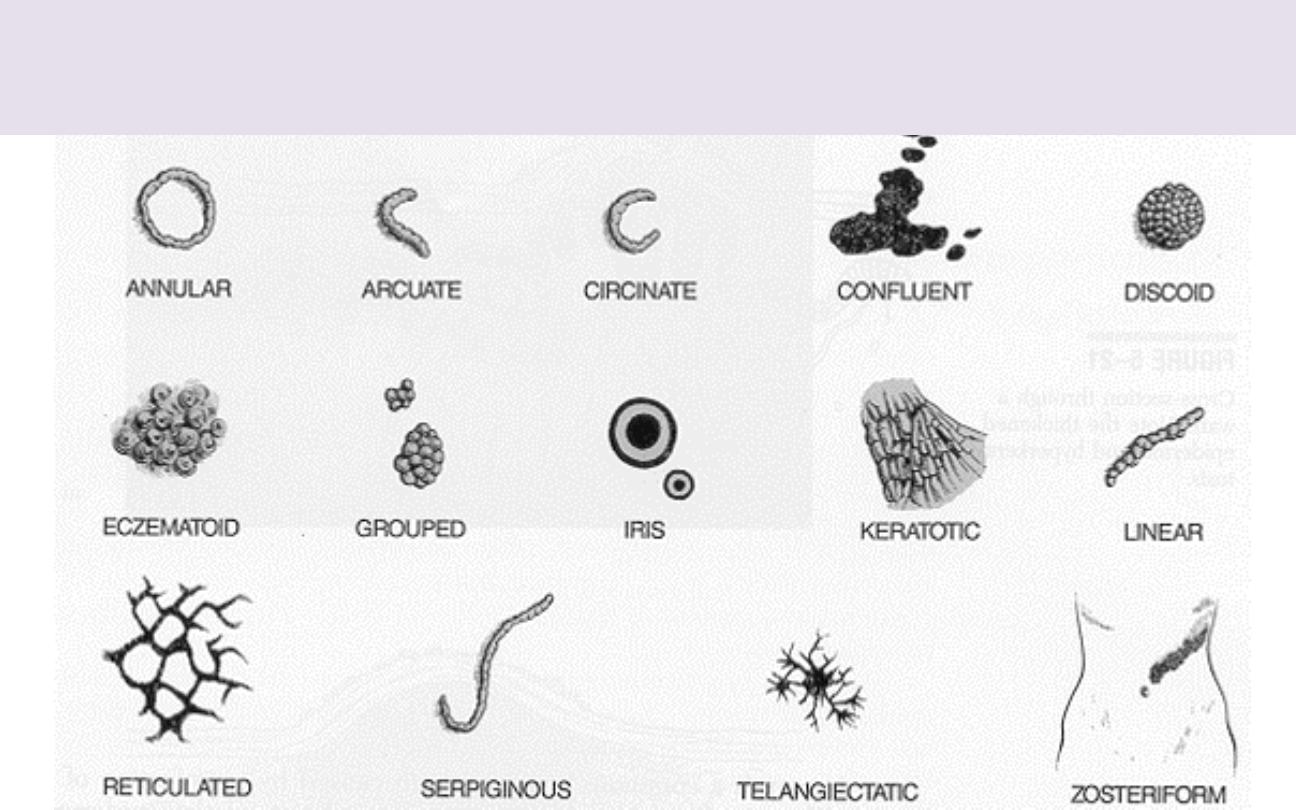
Configuration is the shape of single lesions
and the arrangement of clusters of lesions.

Linear lesions
take on the shape of a straight line and are suggestive of
some forms of contact dermatitis, linear epidermal nevi, and lichen striatus.

Annular lesions
are rings with central clearing. Examples include
granuloma annulare, some drug eruptions, some dermatophyte infections (eg,
ringworm),& secondary syphilis.

Nummular lesions
are circular or coin-shaped; an example is nummular
eczema.

Target (bull’s-eye or iris) lesions
appear as rings with central
duskiness and are classic for erythema multiforme.

Serpiginous lesions
have linear, branched, & curving elements.
Examples include some fungal & parasitic infections (eg, cutaneous larva
migrans).

Reticulated lesions
have a lacy or networked pattern. Examples include
cutis marmorata and livedo reticularis.

Herpetiform
describes grouped papules or vesicles arranged like those of
a herpes simplex infection.

Zosteriform
describes lesions clustered in a dermatomal distribution
similar to herpes zoster.

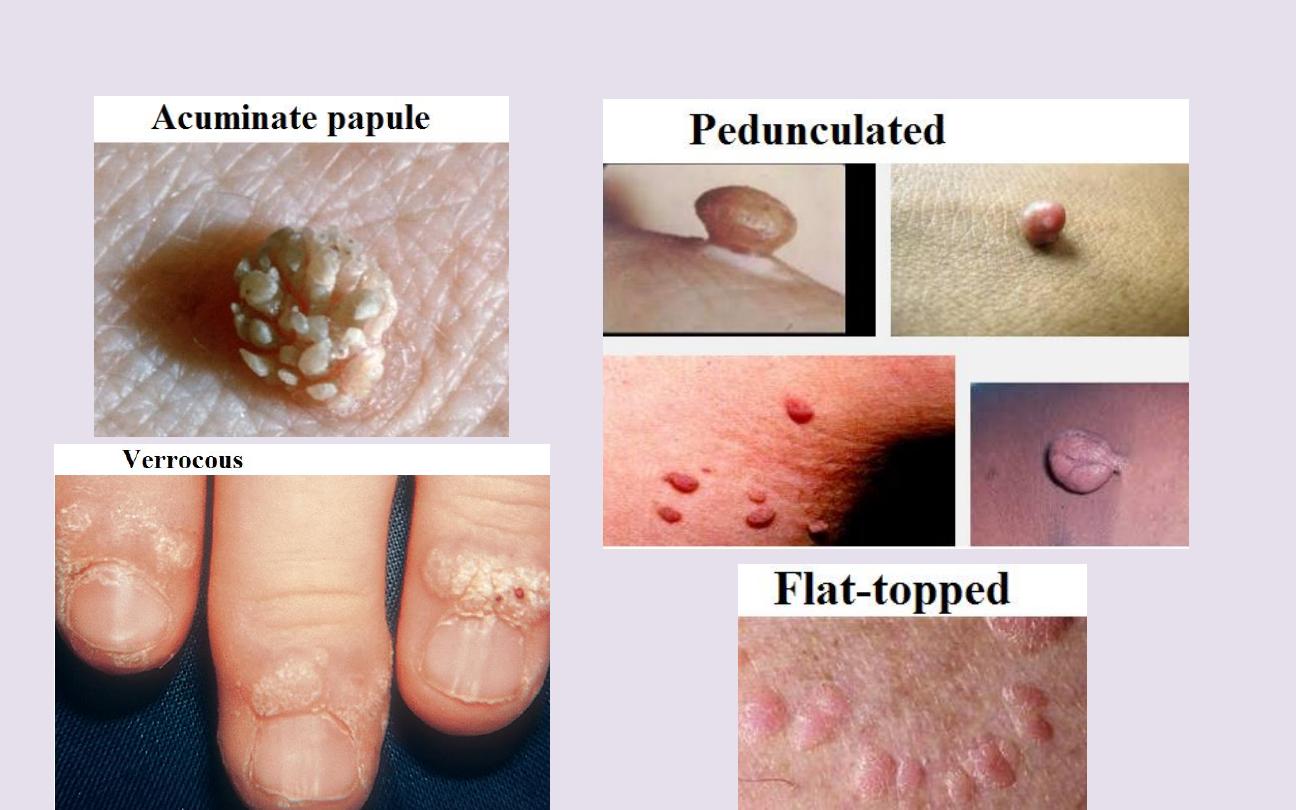
(4)
Texture
Some skin lesions have visible or palpable
texture that suggests a diagnosis.

Verrucous lesions
have an irregular, pebbly, or rough surface.
Examples include warts and seborrheic keratoses.
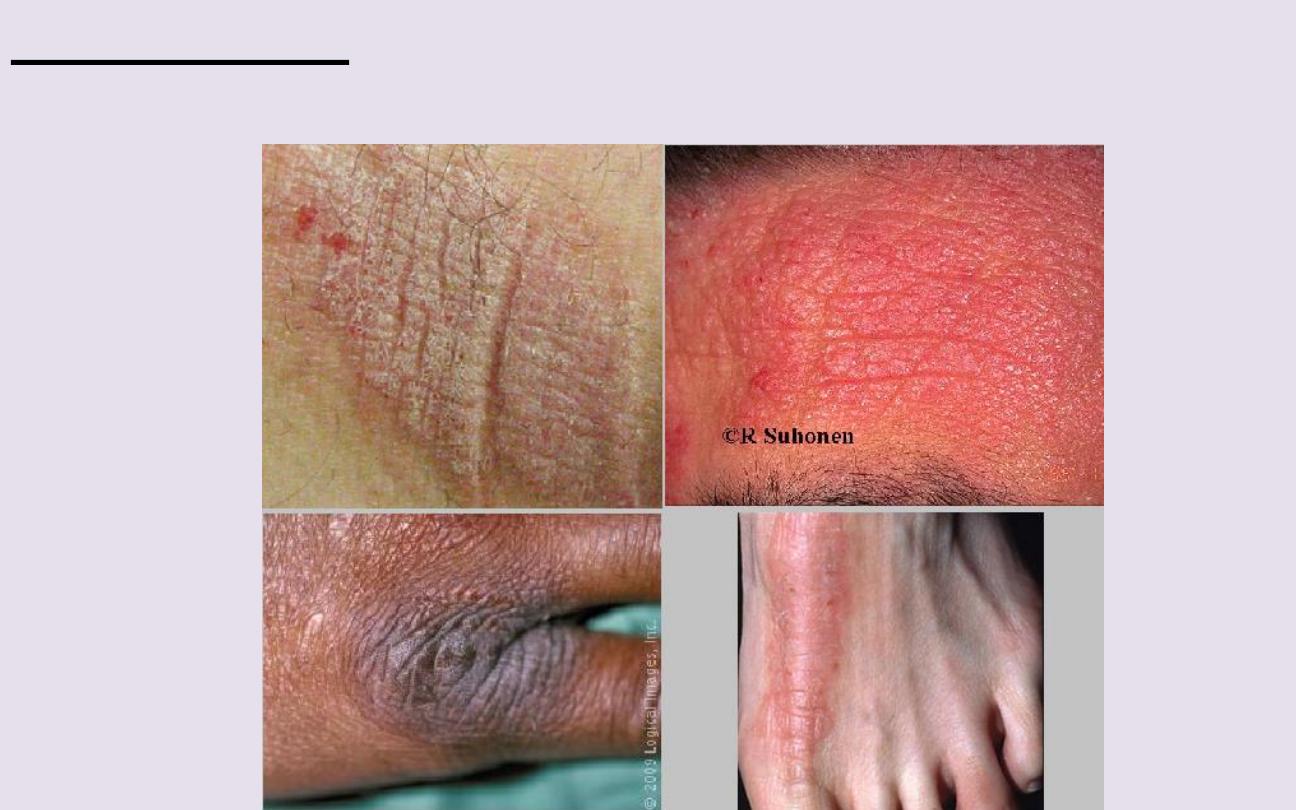
Lichenification
is thickening of the skin with accentuation of normal skin
markings; it results from repeated scratching or rubbing.

Induration
, or deep thickening of the skin, can result from edema,
inflammation, or infiltration, including by cancer. Indurated skin has a hard,
resistant feeling. Induration is characteristic of panniculitis, some skin infections,
and cutaneous metastatic cancers.

Umbilicated lesions
have a central indentation and are usually viral.
Examples include molluscum contagiosum and herpes simplex.

Xanthomas
, which are yellowish, waxy lesions, may be idiopathic or may
occur in patients who have lipid disorders.

(5)
Area involving the
lesion & Lesion shape
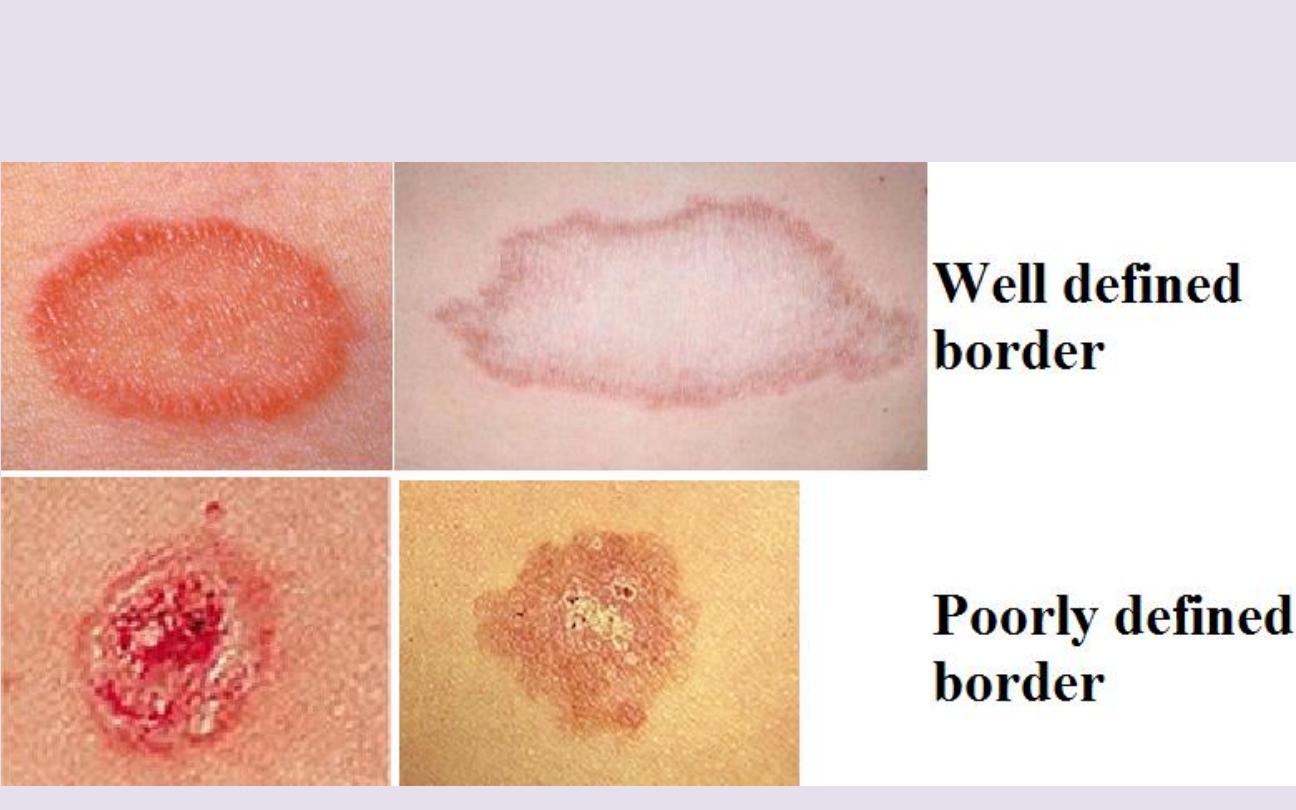
Border of skin lesion
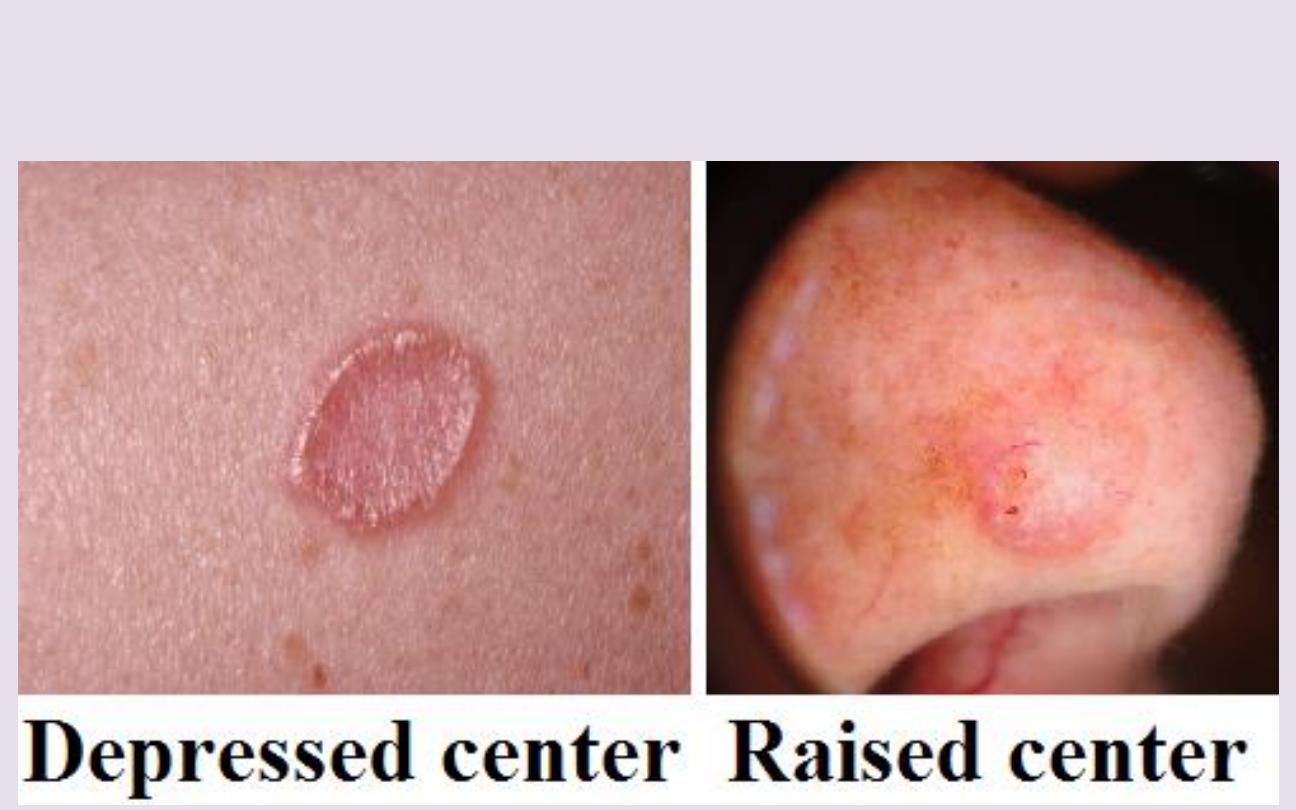
Lesion center
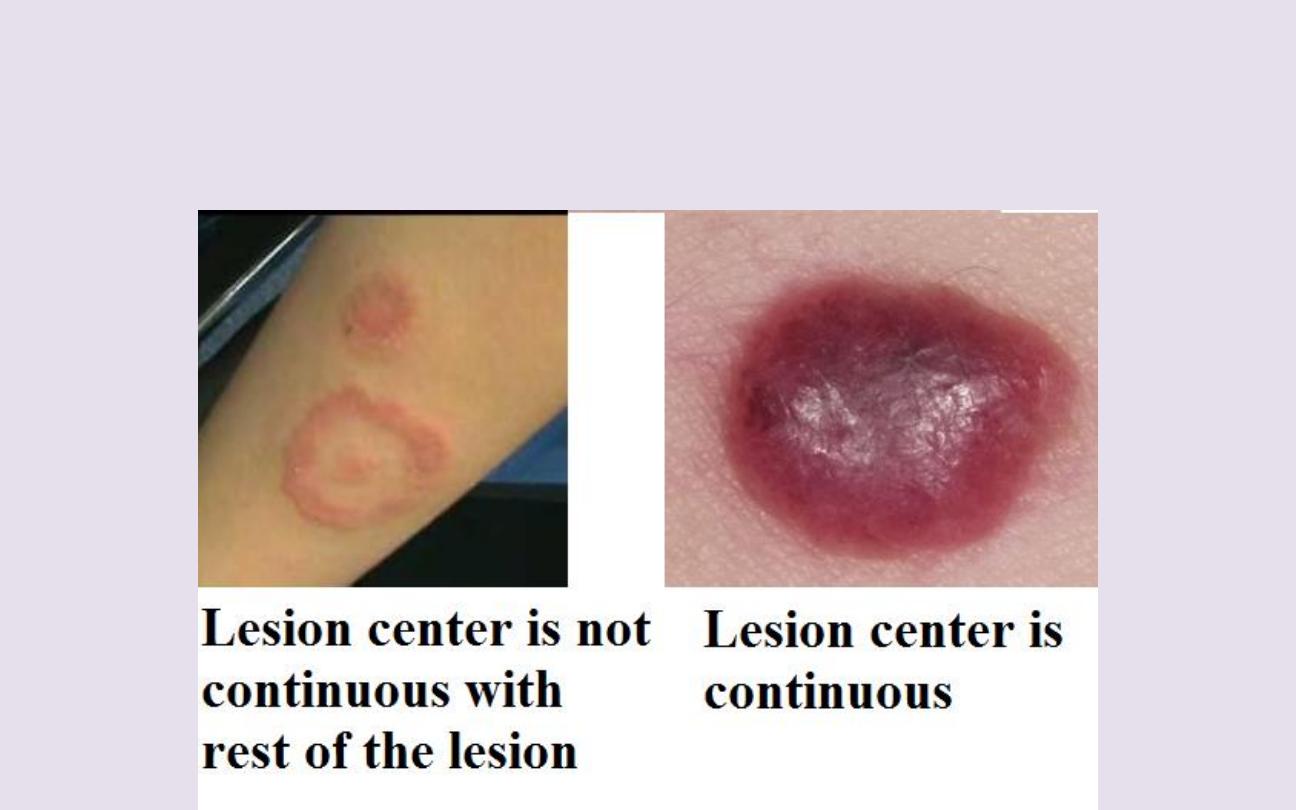
Is lesion center Continuous with rest of the
lesion?

Overall shape of skin lesion

(6)
Location and
Distribution
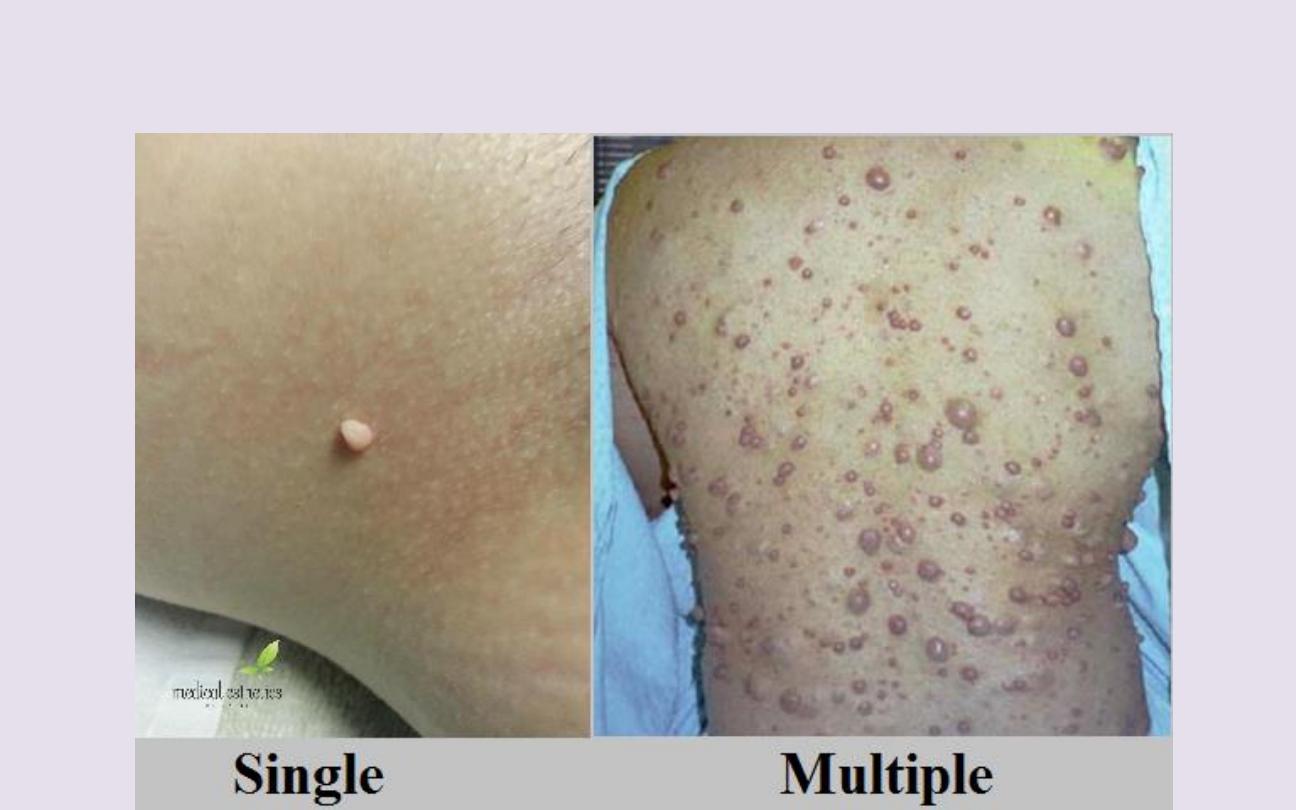
Is skin lesion single?

Is particular body parts are affected?
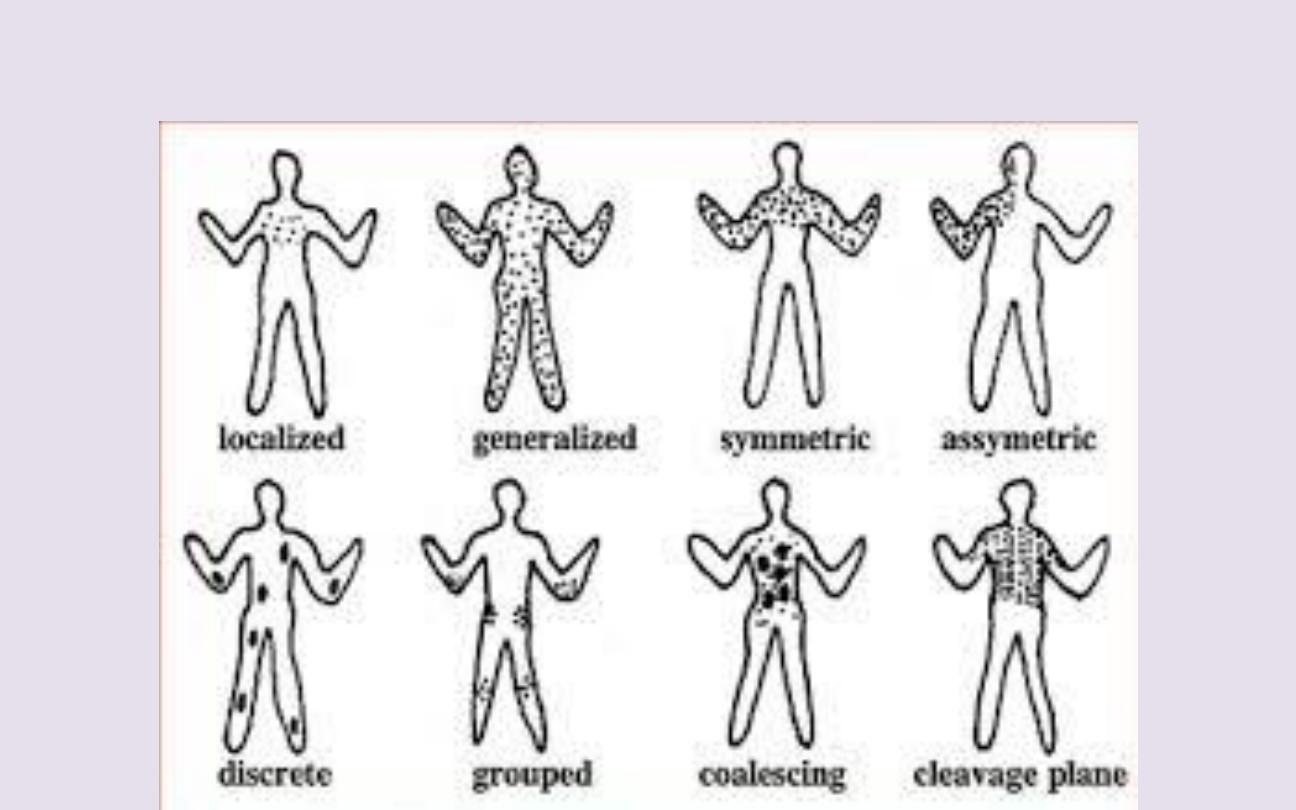
Distribution pattern
Although few patterns are pathognomonic, some are
consistent with certain diseases.
• Psoriasis frequently affects the scalp, extensor surfaces of the
elbows and knees, umbilicus, and the gluteal cleft.
• Lichen planus frequently arises on the wrists, forearms, genitals,
and lower legs.
• Vitiligo may be patchy and isolated or may group around the
distal extremities and face, particularly around the eyes & mouth.
• Chronic cutaneous lupus erythematosus has characteristic
lesions on sun-exposed skin of the face, especially the forehead,
nose, and the conchal bowl of the ear.
• Hidradenitis suppurativa involves skin containing a high density
of apocrine glands, including the axillae, groin, and under the
breasts.

(7)
Color
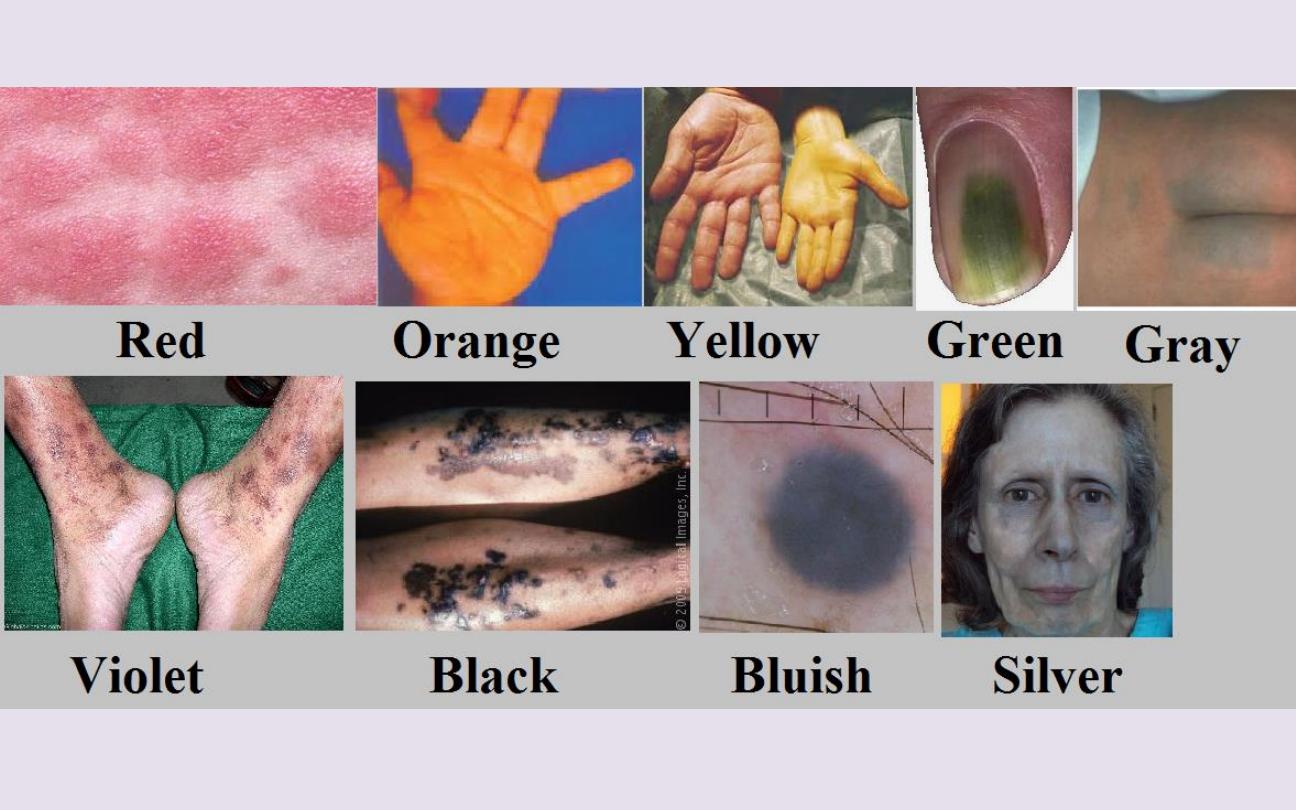
• Red skin (erythema) can result from many different inflammatory
or infectious diseases. Cutaneous tumors are often pink or red.
Superficial vascular lesions such as port-wine stains may appear
red.
• Orange skin is most often seen in hypercarotenemia, a usually
benign condition of carotene deposition after excess dietary
ingestion of
β-carotene.
• Yellow skin is typical of jaundice, xanthelasmas & xanthomas,&
pseudoxanthoma elasticum.
• Green fingernails suggest
Pseudomonas aeruginosa
infection.
• Violet skin may result from cutaneous hemorrhage or vasculitis.
Vascular lesions or tumors, such as Kaposi sarcoma and
hemangiomas, can appear purple. A lilac color of the eyelids or
heliotrope eruption is characteristic of dermatomyositis.

• Shades of blue, silver, and gray can result from deposition of
drugs or metals in the skin, includingminocycline, amiodarone,
and silver (argyria). Ischemic skin appears purple to gray in color.
Deep dermal nevi appear blue.
• Black skin lesions may be melanocytic, including nevi and
melanoma. Black eschars are collections of dead skin that can
arise from infarction, which may be caused by infection (eg,
anthrax, angioinvasive fungi
including
Rhizopus,
meningococcemia), calciphylaxis, arterial
insufficiency, or vasculitis.
“Clinical dermatological signs”

Dermatographism
is the appearance of an urticarial wheal after focal
pressure (eg, stroking or scratching the skin) in the distribution of the pressure.
Up to 5% of normal patients may exhibit this sign, which is a form of physical
urticaria.

Darier sign
refers to rapid swelling of a lesion when stroked. It occurs in
patients with urticaria pigmentosa or mastocytosis. In other term,
Darier sign
is
“positive” when a brown macular or a slightly papular lesion of urticaria
pigmentosa (mastocytosis) becomes a palpable wheal after being vigorously
rubbed with an instrument such as the blunt end of a pen. The wheal may not
appear for 5
–10 min.

Nikolsky sign
is epidermal shearing that occurs with gentle lateral
pressure on seemingly uninvolved skin in patients with toxic epidermal
necrolysis and some autoimmune bullous diseases. In other term, The
Nikolsky
phenomenon
is positive when the epidermis is dislodged from the dermis by
lateral, shearing pressure with a finger, resulting in an erosion. It is an important
diagnostic sign in acantholytic disorders such as pemphigus or the
staphylococcal scalded skin (SSS) syndrome or other blistering or
epidermonecrotic disorders, such as toxic epidermal necrolysis.

Auspitz sign
is “positive” when slight scratching or curetting of a scaly
lesion reveals punctate bleeding points within the lesion. This suggests
psoriasis, but it is not specific.

Koebner (Isomorphic) phenomenon
describes the development
of lesions within areas of trauma (eg, caused by scratching, rubbing, or injury).
It is seen in: Psoriasis, warts, lichen planus, vitiligo, acute eczema,
molloscum contagiosum.