
11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 1/15
Aortic valve disease
Aortic stenosis
Aetiology and pathophysiology
The likely aetiology depends on the age of the patient (
Box 18.105
). In congenital aortic stenosis, obstruction is present from
birth or becomes apparent in infancy. With bicuspid aortic valves, obstruction may take years to develop as the valve becomes
fibrotic and calcified. The aortic valve is the second most frequently affected by rheumatic fever and, commonly, both the aortic
and mitral valves are involved. In older people, a structurally normal tricuspid aortic valve may be affected by fibrosis and
calcification, in a process that is histologically similar to that of atherosclerosis affecting the arterial wall. Haemodynamically
significant stenosis develops slowly, typically occurring at 30–60 years in those with rheumatic disease, 50–60 in those with
bicuspid aortic valves and 70–90 in those with degenerative calcific disease.
18.105 Causes of aortic stenosis
Infants, children, adolescents
•
Congenital aortic stenosis
•
Congenital subvalvular aortic stenosis
•
Congenital supravalvular aortic stenosis
Young adults to middle-aged
•
Calcification and fibrosis of congenitally bicuspid aortic valve
•
Rheumatic aortic stenosis
Middle-aged to elderly

11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 2/15
•
Senile degenerative aortic stenosis
•
Calcification of bicuspid valve
•
Rheumatic aortic stenosis
Cardiac output is initially maintained at the cost of a steadily increasing pressure gradient across the aortic valve. The LV
becomes increasingly hypertrophied and coronary blood flow may then be inadequate; patients may therefore develop angina,
even in the absence of concomitant coronary disease. The fixed outflow obstruction limits the increase in cardiac output
required on exercise. Eventually, the LV can no longer overcome the outflow tract obstruction and pulmonary oedema
supervenes. In contrast to patients with mitral stenosis, which tends to progress very slowly, those with aortic stenosis typically
remain asymptomatic for many years but deteriorate rapidly when symptoms develop, and death usually ensues within 3–5
years of these.
Clinical features
Aortic stenosis is commonly picked up in asymptomatic patients at routine clinical examination but the three cardinal symptoms
are angina, breathlessness and syncope (
Box 18.106
). Angina arises because of the increased demands of the hypertrophied
LV working against the high-pressure outflow tract obstruction, leading to a mismatch between oxygen demand and supply, but
may also be due to coexisting coronary artery disease, especially in old age, when it affects over 50% of patients. Exertional
breathlessness suggests cardiac decompensation as a consequence of the excessive pressure overload placed on the LV. Syncope
usually occurs on exertion when cardiac output fails to rise to meet demand, leading to a fall in BP.
18.106 Clinical features of aortic stenosis
Symptoms
•
Mild or moderate stenosis:
usually asymptomatic
•
Exertional dyspnoea
•
Exertional syncope
•
Sudden death
•
Episodes of acute pulmonary oedema
11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 3/15
•
Angina
Signs
•
Ejection systolic murmur
•
Slow-rising carotid pulse
•
Thrusting apex beat (LV pressure
overload)
•
Narrow pulse pressure
•
Signs of pulmonary venous congestion
(e.g. crepitations)
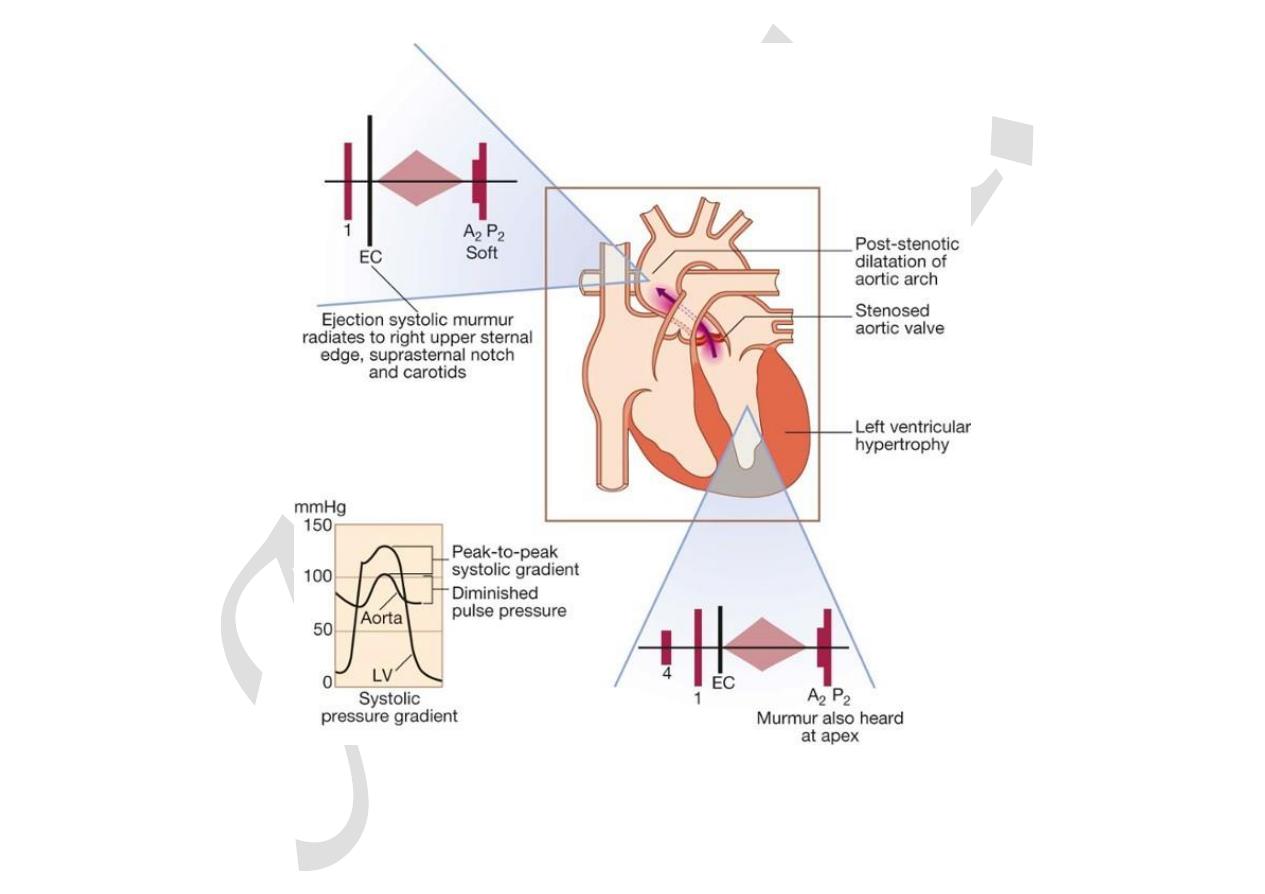
The characteristic clinical signs of severe aortic stenosis are shown in
Box 18.106
. A harsh ejection systolic murmur radiates
to the neck, with a soft second heart sound, particularly in those with calcific valves. The murmur is often likened to a saw
cutting wood and may (especially in older patients) have a musical quality like the ‘mew’ of a seagull (
Fig. 18.89
). The
severity of aortic stenosis may be difficult to gauge clinically, as older patients with a non-compliant ‘stiff’ arterial system may
have an apparently normal carotid upstroke in the presence of severe aortic stenosis. Milder degrees of stenosis may be difficult
to distinguish from aortic sclerosis, in which the valve is thickened or calcified but not obstructed. A careful examination should
be made for other valve lesions, particularly in rheumatic heart disease, when there is frequently concomitant mitral valve
disease.
11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 4/15
F I G.
1 8 . 8 9
Aortic stenosis. Pressure traces show the systolic gradient between LV and aorta. The ‘diam…
Investigations
11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 5/15
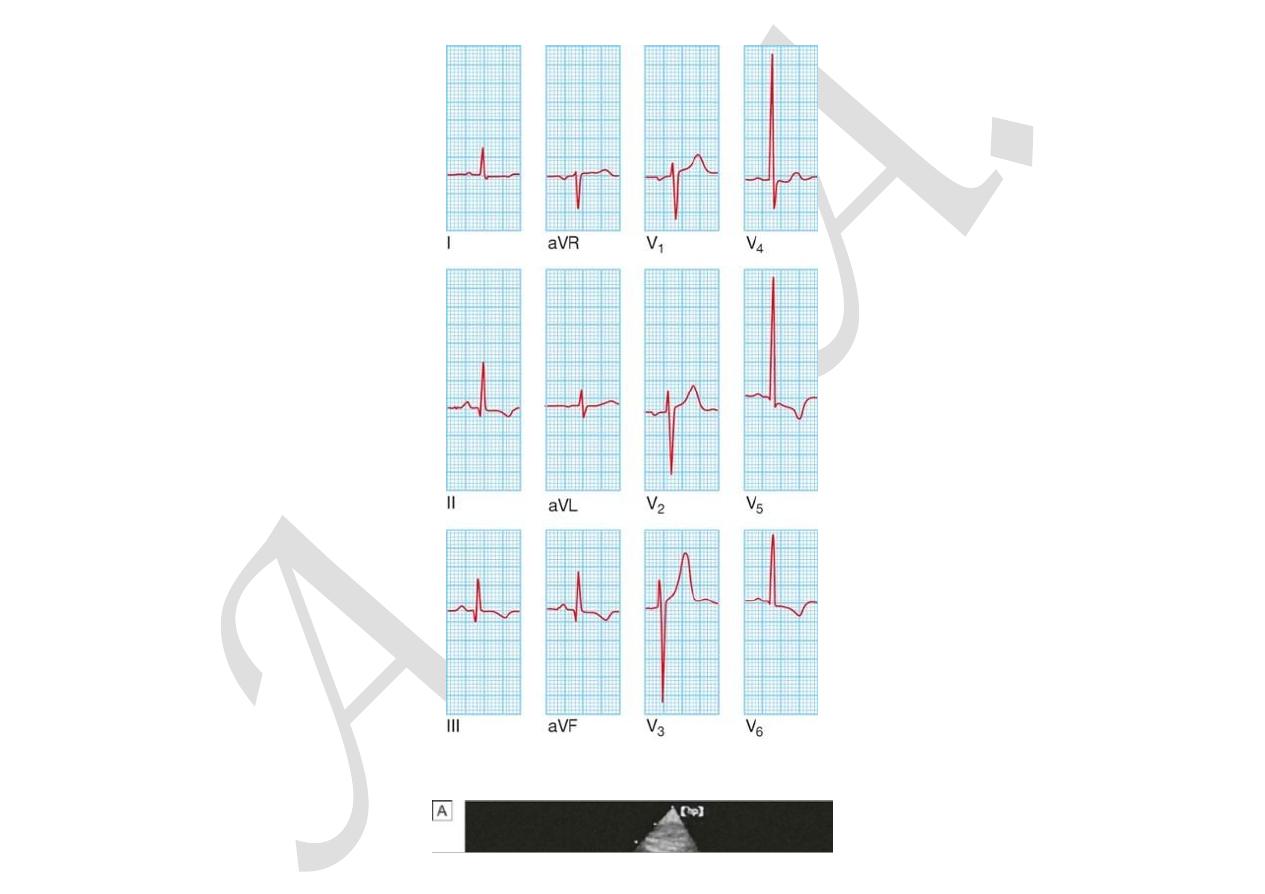
In advanced cases, ECG features of hypertrophy (
Box 18.107
) are often gross (
Fig. 18.90
), and down-sloping ST segments
and T inversion (‘strain pattern’) are seen in leads reflecting the LV. Nevertheless, especially in old age, the ECG can be normal,
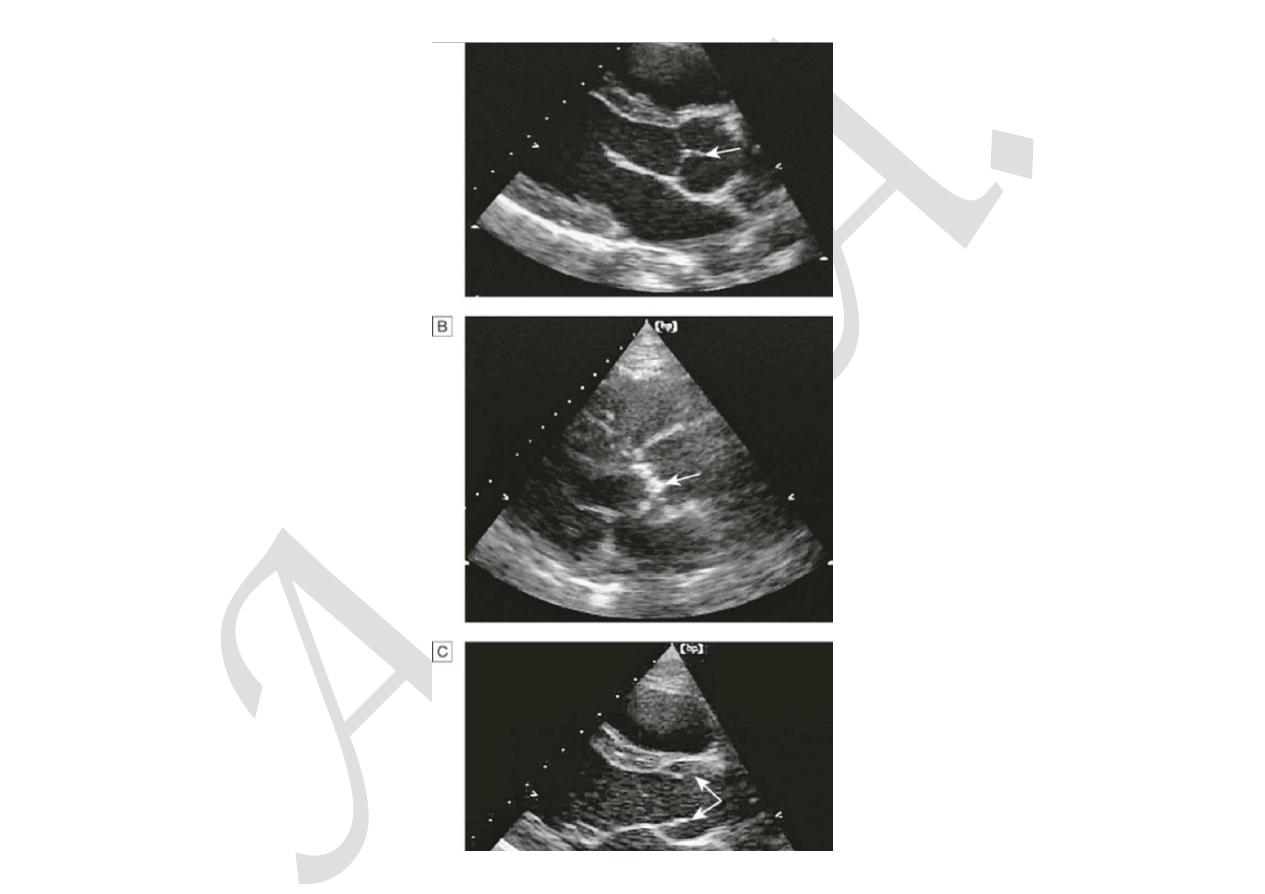
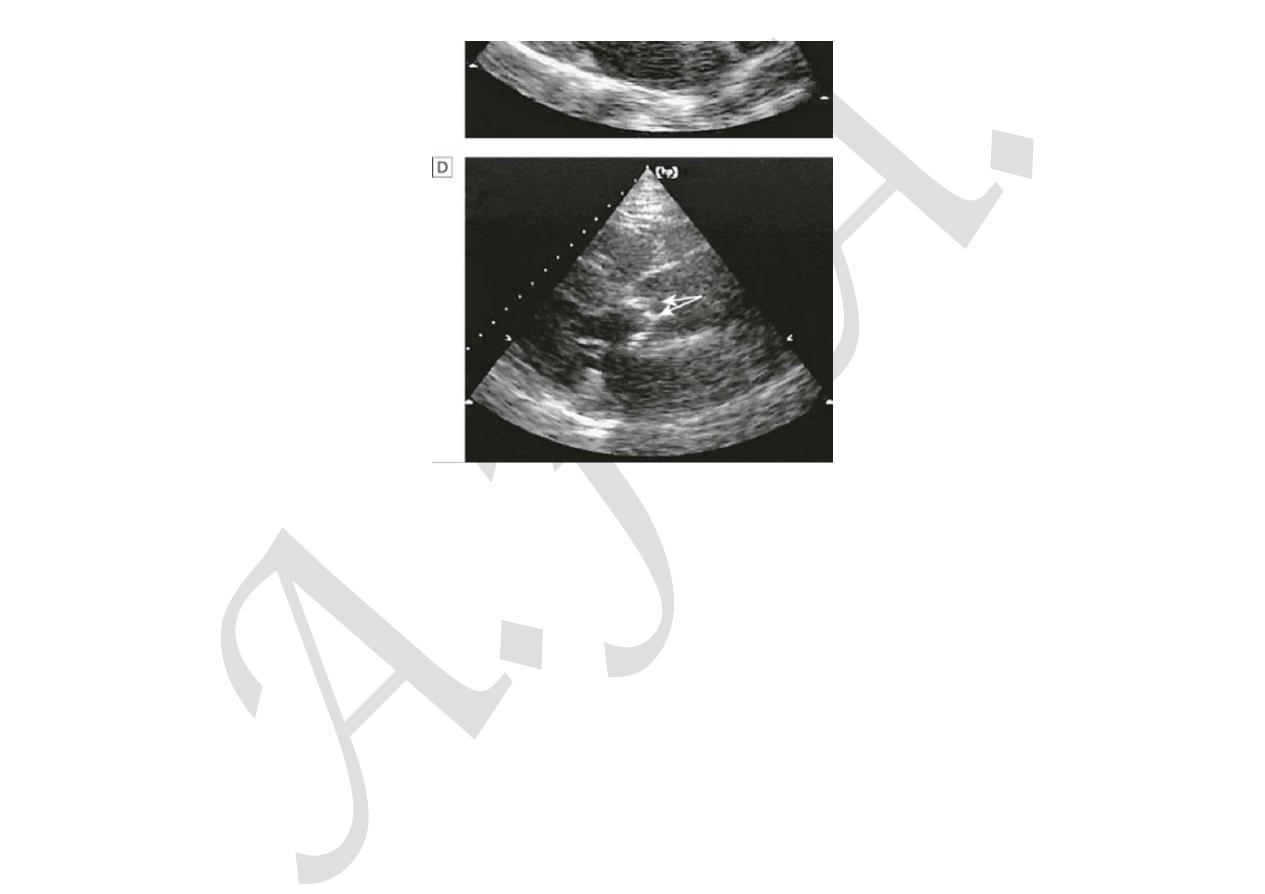
despite severe stenosis. Echocardiography demonstrates restricted valve opening (
Fig. 18.91
) and Doppler assessment permits
calculation of the systolic gradient across the aortic valve, from which the severity of stenosis can be assessed (see
Fig.
18.11
,
p. 536
). In patients with an impaired LV, velocities across the aortic valve may be diminished because of a reduced
stroke volume, while when aortic regurgitation is present, velocities are increased because of an increased stroke volume. In
these circumstances, aortic valve area calculated from Doppler measurements is a more accurate assessment of severity. CT and
MRI are useful in assessing the degree of valve calcification and stenosis, respectively, but are rarely necessary.
18.107 Investigations in aortic stenosis
ECG
•
Left ventricular hypertrophy (usually)
•
Left bundle branch block
Chest X-ray
•
May be normal; sometimes enlarged LV and dilated ascending aorta on PA view, calcified valve on lateral
view
Echo
•
Calcified valve with restricted opening, hypertrophied LV (see
Fig. 18.91
)
Doppler
•
Measurement of severity of stenosis
•
Detection of associated aortic regurgitation

11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 6/15
Cardiac catheterisation
•
Mainly to identify associated coronary artery disease
•
May be used to measure gradient between LV and aorta
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fb
f
t l
r i
.
.
20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 7/15
b4e6 85%22%20s y e%3D%22ma g n%3A%201 3em%200px%200 5em%3B%
F I G.
1 8 . 9 0
Left ventricular hypertrophy. QRS complexes in limb leads have increased amplitude with …
11/18/2015
i
f t
rt l
|
i
’ ri i l
r ti
f
…
D seases o he hea va ves Dav dson s P nc p es and P ac ce o
b4e6 85%22%20s y e%3D%22ma g n%3A%201 3em%200px%200 5em%3B%
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fb f t l r i . . 20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 8/15
11/18/2015
i
f t
rt l
|
i
’ ri i l
r ti
f
…
D seases o he hea va ves Dav dson s P nc p es and P ac ce o
F I G.
1 8 . 9 1
Two-dimensional echocardiogram comparing a normal subject with a patient with ca…
Management
Irrespective of the severity of valve stenosis, patients with asymptomatic aortic stenosis have a good immediate prognosis and
conservative management is appropriate. Such patients should be kept under review, as the development of angina, syncope,
symptoms of low cardiac output or heart failure has a poor prognosis and is an indication for prompt surgery. In practice,
patients with moderate or severe stenosis are evaluated every 1–2 years with Doppler echocardiography to detect progression in
severity; this is more rapid in older patients with heavily calcified valves.
Patients with symptomatic severe aortic stenosis should have prompt aortic valve replacement. Old age is not a contraindication
to valve replacement and results are very good in experienced centres, even for those in their eighties (
Box 18.108
). Delay
exposes the patient to the risk of sudden death or irreversible deterioration in ventricular function. Some patients with severe
aortic stenosis deny symptoms, and if this could be due to a sedentary lifestyle, a careful exercise test may reveal symptoms on
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-famil
… 9/15

11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-fam
…
1010/15
modest exertion. Aortic balloon valvuloplasty is useful in congenital aortic stenosis but is of no value in older patients with
calcific aortic stenosis.
18.108 Aortic stenosis in old age
•
Incidence: the most common form of valve disease affecting the very old.
•
Symptoms: a common cause of syncope, angina and heart failure in the very old.
•
Signs: because of increasing stiffening in the central arteries, low pulse pressure and a slow rising pulse
may not be present.
•
Surgery: can be successful in those aged 80 yrs or more in the absence of comorbidity, but with a
higher operative mortality. The prognosis without surgery is poor once symptoms have developed.
•
Valve replacement type: a biological valve is often preferable to a mechanical one because this
obviates the need for anticoagulation, and the durability of biological valves usually exceeds the patient’s
anticipated life expectancy.
Anticoagulants are only required in patients who have atrial fibrillation or those who have had a valve replacement with a
mechanical prosthesis.
Aortic regurgitation
Aetiology and pathophysiology
This condition is due to disease of the aortic valve cusps or dilatation of the aortic root (
Box 18.109
). The LV dilates and
hypertrophies to compensate for the regurgitation. The stroke volume of the LV may eventually be doubled or trebled, and the
major arteries are then conspicuously pulsatile. As the disease progresses, left ventricular diastolic pressure rises and
breathlessness develops.

11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-fam
…
1111/15
18.109 Causes of aortic regurgitation
Congenital
•
Bicuspid valve or disproportionate cusps
Acquired
•
Rheumatic disease
•
Infective endocarditis
•
Trauma
•
Aortic dilatation (Marfan’s syndrome, aneurysm, dissection, syphilis, ankylosing spondylitis)
Clinical features
Until the onset of breathlessness, the only symptom may be an awareness of the heart beat (
Box 18.110
), particularly when
lying on the left side, which results from the increased stroke volume. Paroxysmal nocturnal dyspnoea is sometimes the first
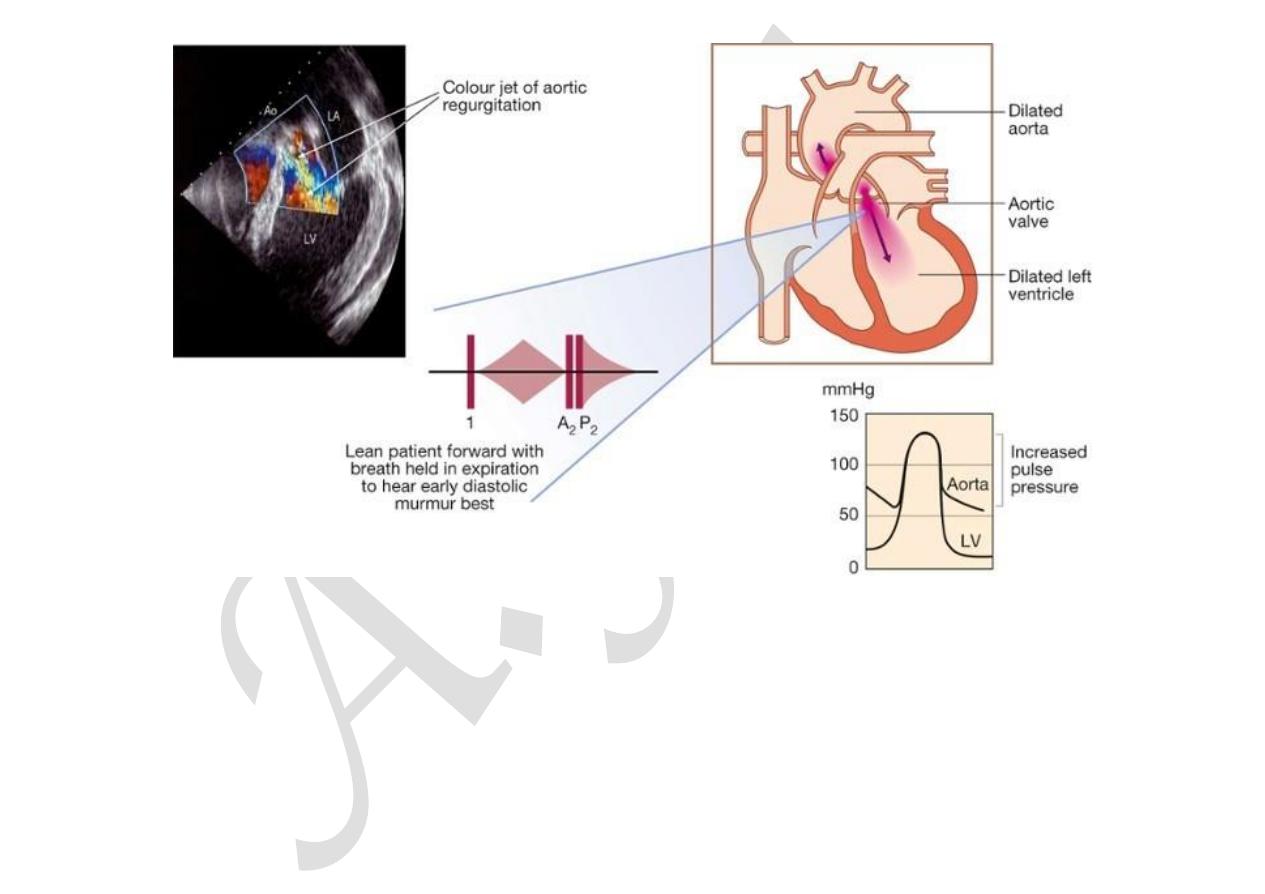
symptom, and peripheral oedema or angina may occur. The characteristic murmur is best heard to the left of the sternum
during held expiration (
Fig. 18.92
); a thrill is rare. A systolic murmur due to the increased stroke volume is common and does
not necessarily indicate stenosis. The regurgitant jet causes fluttering of the mitral valve and, if severe, causes partial closure of
the anterior mitral leaflet, leading to functional mitral stenosis and a soft mid-diastolic (Austin Flint) murmur.
18.110 Clinical features of aortic regurgitation
Symptoms
Mild to moderate aortic regurgitation
•
Often asymptomatic
11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-fam
…
1212/15
•
Awareness of heart beat, ‘palpitations’
Severe aortic regurgitation
•
Breathlessness
•
Angina
Signs
Pulses
•
Large-volume or ‘collapsing’ pulse
•
Low diastolic and increased pulse pressure
•
Bounding peripheral pulses
•
Capillary pulsation in nail beds: Quincke’s sign
•
Femoral bruit (‘pistol shot’): Duroziez’s sign
•
Head nodding with pulse: de Musset’s sign
Murmurs
•
Early diastolic murmur
•
Systolic murmur (increased stroke volume)
•
Austin Flint murmur (soft mid-diastolic)
Other signs
•
Displaced, heaving apex beat (volume overload)
•
Pre-systolic impulse
•
Fourth heart sound
•
Crepitations (pulmonary venous congestion)
11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-fam
…
1313/15
F I G.
1 8 . 9 2
Aortic regurgitation. The early diastolic murmur is best heard at the left sternal edge and m…
In acute severe regurgitation (e.g. perforation of aortic cusp in endocarditis), there may be no time for compensatory left
ventricular hypertrophy and dilatation to develop and the features of heart failure may predominate. In this situation, the
classical signs of aortic regurgitation may be masked by tachycardia and an abrupt rise in left ventricular end-diastolic pressure;
thus, the pulse pressure may be near normal and the diastolic murmur may be short or even absent.
Investigations
Regurgitation is detected by Doppler echocardiography (
Box 18.111
). In severe acute aortic regurgitation, the rapid rise in left
11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-fam
…
1414/15
ventricular diastolic pressure may cause premature mitral valve closure. Cardiac catheterisation and aortography can help in
assessing the severity of regurgitation, and dilatation of the aorta and the presence of coexisting coronary artery disease. MRI is
useful in assessing the degree and extent of aortic dilatation.
18.111 Investigations in aortic regurgitation
ECG
•
Initially normal, later left ventricular hypertrophy and T-wave inversion
Chest X-ray
•
Cardiac dilatation, maybe aortic dilatation
•
Features of left heart failure
Echo
•
Dilated LV
•
Hyperdynamic LV
•
Doppler detects reflux
•
Fluttering anterior mitral leaflet
Cardiac catheterisation (may not be required)
•
Dilated LV
•
Aortic regurgitation
•
Dilated aortic root
Management
Treatment may be required for underlying conditions, such as endocarditis or syphilis. Aortic valve replacement is indicated if
aortic regurgitation causes symptoms, and this may need to be combined with aortic root replacement and coronary bypass
surgery. Those with chronic aortic regurgitation can remain asymptomatic for many years because compensatory ventricular
dilatation and hypertrophy occur, but should be advised to report the development of any symptoms of breathlessness or

11/18/2015
Diseases of the heart valves | Davidson
’s Principles and Practice of…
data:text/html;charset=utf-8,%3Ch2%20id%3D%22d10f8282bd6d4d039994f22fbb4e6f85%22%20style%3D%22margin%3A%201.3em%200px%200.5em%3B%20padding%3A%200px%3B%20border%3A%200px%3B%20font-fam
…
1515/15
angina. Asymptomatic patients should also be followed up annually with echocardiography for evidence of increasing
ventricular size. If this occurs or if the end-systolic dimension increases to 55 mm or more, then aortic valve replacement should
be undertaken. Systolic BP should be controlled with vasodilating drugs, such as nifedipine or ACE inhibitors. There is
conflicting evidence regarding the need for aortic valve replacement in asymptomatic patients with severe aortic regurgitation.
When aortic root dilatation is the cause of aortic regurgitation (e.g. Marfan’s syndrome), aortic root replacement is usually
necessary.