1
Intestinal obstruction
Dr.Husen 18.11.2014 tue>
Intestinal obstruction may be classified into two types:
• Dynamic, in which peristalsis is working against a mechanical obstruction. It
may occur in an acute or a chronic form.
• Adynamic, in which there is no mechanical obstruction; peristalsis is absent or
inadequate (e.g. paralytic ileus or
pseudo-obstruction).
Causes of intestinal obstruction
Dynamic
Intraluminal
Faecal impaction
Foreign bodies
Bezoars
Gallstones
Adynamic
Paralytic ileus
Pseudo-obstruction
PATHOPHYSIOLOGY
Irrespective of aetiology or acuteness of onset, in dynamic
(mechanical) obstruction the bowel proximal to the obstruction dilates and the
bowel below the obstruction exhibits normal peristalsis and absorption until it
becomes empty and collapses. Initially, proximal peristalsis is increased in an
attempt
to overcome the obstruction. If the obstruction is not relieved, the bowel continues
to dilate, ultimately there is a reduction in peristaltic strength, resulting in flaccidity
and paralysis.
The distension proximal to an obstruction is caused by two factors:
•
Gas
: there is a significant overgrowth of both aerobic and anaerobic organisms,
resulting in considerable gas production.
Following the reabsorption of oxygen and carbon dioxide, the majority is made up
of nitrogen (90 per cent) and hydrogen sulphide.
•
Fluid:
this is made up of the various digestive juices (saliva 500 mL, bile 500 mL,
pancreatic secretions 500 mL, gastric secretions 1 litre – all per 24 hours). This
accumulates in the gut lumen as absorption by the obstucted gut is retarded.
Dehydration and electrolyte loss are therefore due to:
1. reduced oral intake;
Intramural
Stricture
Malignancy
Intussusception
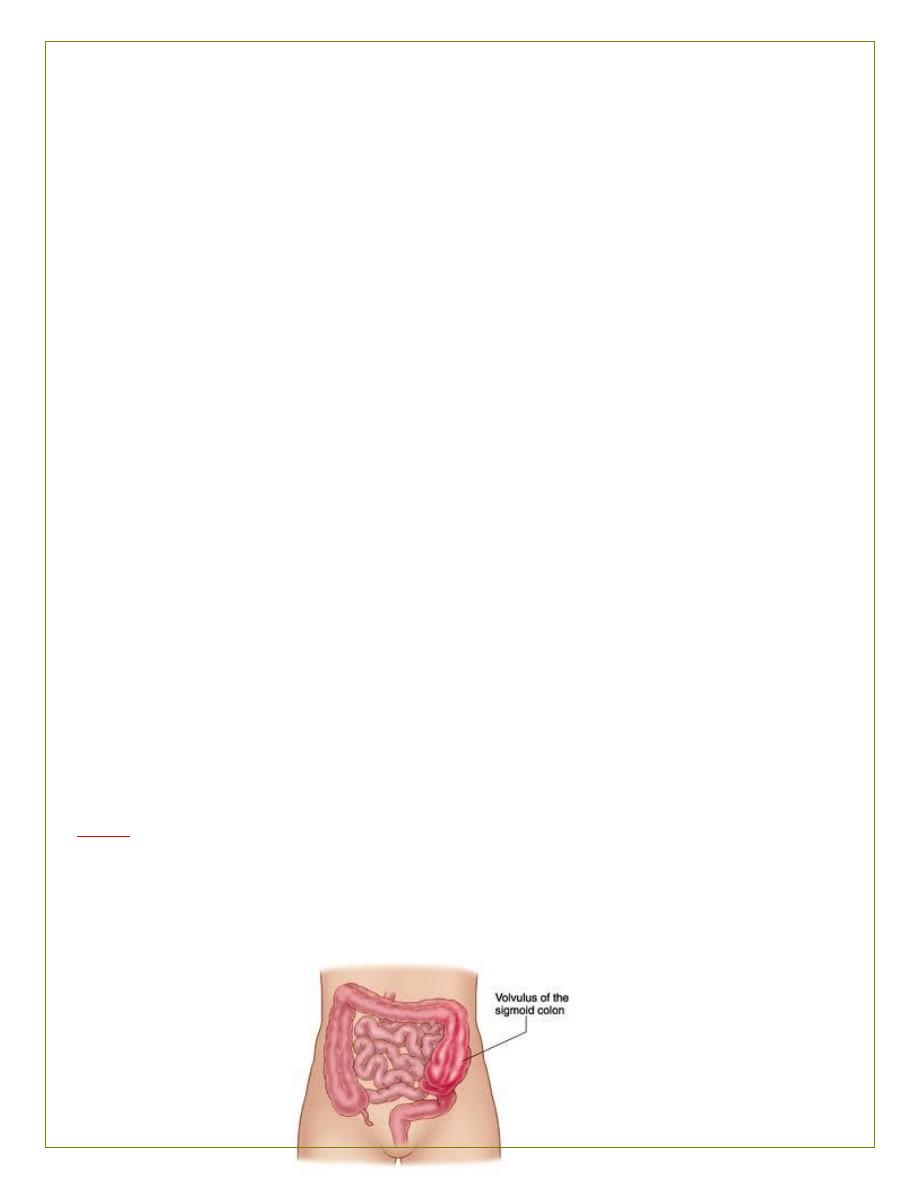
Volvulus
Extramural
Bands/adhesions
Hernia
2
2. defective intestinal absorption;
3. losses as a result of vomiting;
4. sequestration in the bowel lumen;
5. transudation of fluid into the peritoneal cavity.
STRANGULATION
When strangulation occurs, the blood supply is compromised and the bowel
becomes ischaemic.
Causes of strangulation
1.
Direct pressure on the bowel wall
2.
Hernial orifices
3.
Adhesions/bands
4.
Interrupted mesenteric blood flow
5.
Volvulus
6.
Intussusception
7.
Increased intraluminal pressure
8.
Closed-loop obstruction
Distention of the obstructed segment of bowel results in high pressure within the
bowel wall. This can happen when only
part of the bowel wall is obstructed as seen in Richter’s hernias.
Venous return is compromised before the arterial supply. The resultant increase in
capillary pressure leads to impaired local
perfusion and once the arterial supply is impaired, haemorrhagic infarction occurs.
As the viability of the bowel is compromised, translocation and systemic exposure
to anaerobic organisms and
endotoxin occurs.
The morbidity and mortality associated with strangulation are largely dependent
on the duration of the ichaemia and its
extent. Elderly patients and those with comorbidities are more vulnerable to its
effects. Although in strangulated external hernias the segment involved is often
short, any length of ischaemic bowel can cause significant systemic effects
secondary to
sepsis and obstruction proximal to the obstruction can result in significant
dehydration. When bowel involvement is extensive circulatory failure is common.
Closed-loop obstruction
3
This occurs when the bowel is obstructed at both the proximal
and distal points. A classic form of closed-loop obstruction is seen in the presence
of a malignant stricture of the colon with a competent
ileocaecal valve (present in up to one-third of individuals). This
can occur with lesions as far distally as the rectum. The inability
of the distended colon to decompress itself into the small bowel results in an
increase in luminal pressure, which is greatest at the caecum, with subsequent
impairment of blood flow in the wall. Unrelieved, this results in necrosis and
perforation
SPECIAL TYPES OF MECHANICAL
INTESTINAL OBSTRUCTION
Internal hernia
Internal herniation occurs when a portion of the small intestine
becomes entrapped in one of the retroperitoneal fossae or in a
congenital mesenteric defect.
The following are potential sites of internal herniation (all
are rare):
• the foramen of Winslow;
• a defect in the mesentery;
• a defect in the transverse mesocolon;
• defects in the broad ligament;
• congenital or acquired diaphragmatic hernia;
• duodenal retroperitoneal fossae – left paraduodenal and right
duodenojejunal;
• caecal/appendiceal retroperitoneal fossae – superior, inferior
and retrocaecal;
• intersigmoid fossa.
Obstruction from enteric strictures
Small bowel strictures usually occur secondary to tuberculosis or
Crohn’s disease. Malignant strictures associated with lymphoma
are uncommon, whereas carcinoma and sarcoma are rare.
Presentation is usually subacute or chronic. Standard surgical
management consists of resection and anastomosis. Resection
is important to establish a histological diagnosis as this can be
uncertain clinically. In Crohn’s disease, strictureplasty may be
considered in the presence of short multiple strictures without
active sepsis.
Bolus obstruction
4
Bolus obstruction in the small bowel may be caused by gallstones,
food, trichobezoar, phytobezoar, stercoliths and worms.
Gallstones
This type of obstruction tends to occur in the elderly secondary
to erosion of a large gallstone directly through the gall
bladder into the duodenum. Classically, there is impaction
about 60 cm proximal to the ileocaecal valve. The patient
may have recurrent attacks as the obstruction is frequently
incomplete or relapsing as a result of a ball-valve effect. The
characteristic radiological sign of gallstone ileus is Rigler’s
triad, comprising: small bowel obstruction, pneumobilia and
an atypical mineral shadow on radiographs of the abdomen.
The presence of two of these radiological signs has been considered
pathognomic of gallstone ileus and is encountered in
40–50 per cent of the cases
Food
Bolus obstruction may occur after partial or total gastrectomy
when unchewed articles can pass directly into the small bowel.
Fruit and vegetables are particularly liable to cause obstruction.
Trychobezoars and phytobezoars
These are firm masses of undigested hair ball and fruit/vegetable
fibre, respectively. The former is due to persistent hair chewing
or sucking, and may be associated with an underlying psychiatric
abnormality. Predisposition to phytobezoars results from a
high fibre intake, inadequate chewing, previous gastric surgery,
hypochlorhydria and loss of the gastric pump mechanism.
Stercoliths
These are usually found in the small bowel in association with a
jejunal diverticulum or ileal stricture. Presentation and management
are identical to that of gallstones.
Worms
Ascaris lumbricoides may cause low small bowel obstruction,
particularly in children .An attack may follow the initiation
of antihelminthic therapy., If worms are not
seen in the stool or vomitus, the diagnosis may be indicated by
eosinophilia or the sight of worms within gas-filled small bowel
loops on a plain
radiograph
Done by: Diaa Abdulfatah M