Surgery Dr. Nadim
Esophagus
Congenital anomalies
⦿ Congenital esophageal atrasia and tracheo-esophageal fistula
⦿ Congenital esophageal stenosis
⦿ Duplication cyst
⦿ Congenital achalesia
⦿ Congenital short esophagus
Congenital esophageal atrasia and tracheo-esophageal fistula
1

Surgery Dr. Nadim
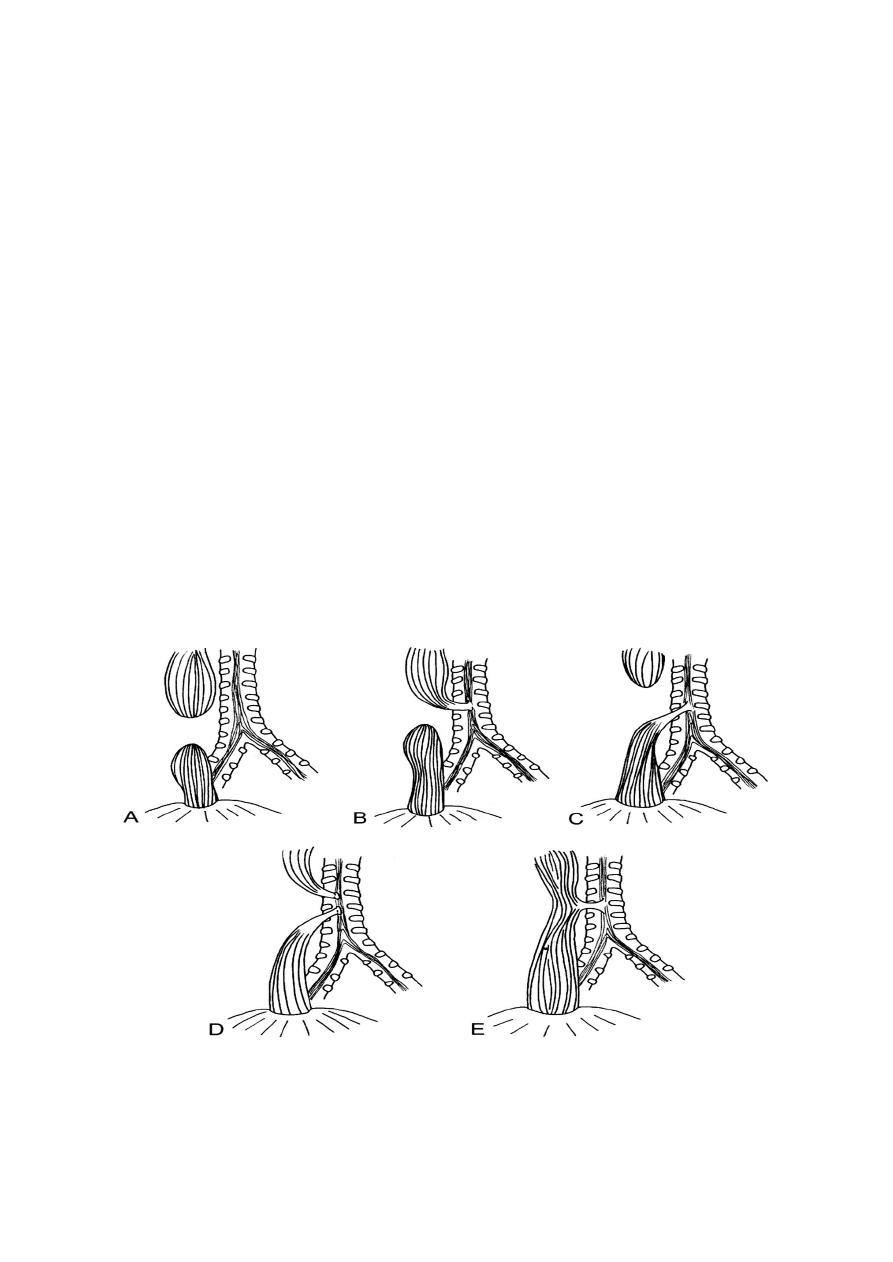
Could be divided into five groups:
Group A:
(8 %) esophageal atrasia without TE fistula, the upper esophagus
ending blindly and the lower esophagus beginning blindly with a
considerable gab between the two segments.
Group B:
(1 %) esophageal atrasia with a fistula between the upper pouch and
the trachea, but the lower esophagus not communicating with the
respiratory tract.
Group C:
(87 %) this is the most common variety, esophageal atrasia, the upper
pouch being blind and the lower esophageal segment communicating
with the trachea.
Group D:
(1 %) esophageal atrasia with both segments communicating with the
trachea by separate fistulae.
Group E:
(4 %) TE fistula but without atrasia (so-called H fistula).
The clinical features of group C (the most common type) is inability of the
infant to swallow saliva. A characteristic fine frothy mucus is continuously
produced in the mouth, while there may be episodes of chocking and cyanosis,
particularly if the diagnosis has not been suspected and a feed is given with
“spell-over” into the larynx. An important clue is the presence of
maternal hydramnios in the antenatal history. Contamination of the
lung is possible not only from inhalation of infected saliva but also
from regurgitation of gastric juice through the distal fistula into the
bronchial tree.
Congenital obstruction of the esophagus is demonstrated by
passage of a 10 Fr plastic radiopaque catheter through the mouth and then into
the esophagus. It will usually be held up, a radiography will demonstrate the
level of the obstruction together with the presence of gas in the stomach and
the intestine.
2
Surgery Dr. Nadim
Preoperatively, the infant should be nursed in a humidified oxygen-enriched
atmosphere in an incubator, the temperature which is usually low on admission
should be restored to normal. The head of the infant should be tilt down 10
degrees, and his position changed from side to side every 30 minutes. The
pharynx must be aspirated repeatedly. Antibiotic therapy is commenced and
vitamin K1 is given by intramuscular injection.
Urgent operation is required, it is usually performed through right
thoracotomy, with separation of the lower esophageal pouch from the trachea,
suturing of the trachea, then primary anastomoses between the upper and the
lower esophageal pouches.
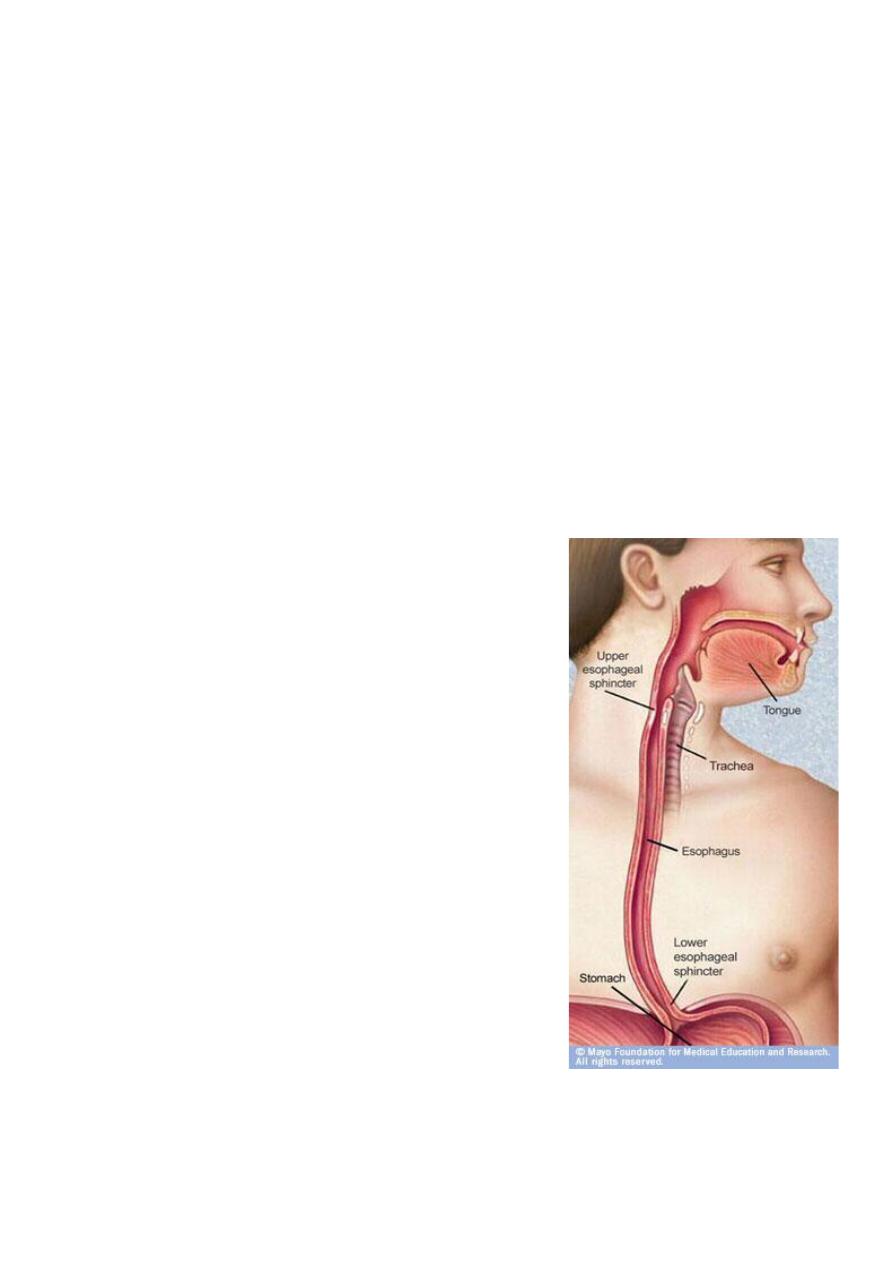
Surgical anatomy of the esophagus
The esophagus is a muscular tube, approximately
25 cm long, extending from the upper esophageal
sphincter in the neck to the junction with the
cardia of the stomach. The musculature of the
upper esophagus is striated, this is followed by
transitional zone.
In the lower half of the esophagus, there is only
smooth muscles. The parasympathetic nerve
supply is mediated by the vagus nerve through the
myenteric (Auerbach’s) plexus.
The upper sphincter consist of powerful striated
muscles. The lower phincter is more subtle, and is
created by asymmetrical arrangement of muscle
fibers in the distal esophageal wall just above the
esophag-ogastric junction. when you perform
endoscopy it is helpful to Remember:
15 cm is the level of upper esophageal sphincter
25 cm is the level of aortic and bronchial
constriction
3

Surgery Dr. Nadim
40 cm is the level of diaphragmatic and sphincter constriction.
Physiology of the esophagus
The main function of the esophagus is to transfer food from the mouth to the
stomach in a coordinated fashion.
➢ The initial movement from the mouth is voluntary.
➢ The pharyngeal phase of swallowing involve sequential contraction of the
oropharyngeal musculature, closure of the nasal and respiratory passages, cessation
of breathing and opening of upper esophageal sphincter.
➢ The body of the esophagus propel the bolus through a relaxed lower esophageal
sphincter (LES) into the stomach, taking air with it. This coordinated esophageal wave
is called primary peristalsis. It is under vagal control (involuntary).
➢ The LES is a zone of relatively high pressure that prevents gastric contents from
refluxing into the lower esophagus. in addition to opening in response to primary
peristaltic wave, the sphincter also relaxes to allow air to escape from the stomach
and at the time of vomiting. The normal LES is 3-4 cm long and has pressure of 10-25
mm Hg
➢ Secondary peristalsis is normal reflux response to a stubborn food bolus or refluxed
materials, designed to clear the esophagus by contraction that is not proceeded by
conscious swallowing.
➢ Tertiary contractions are non-peristaltic waves that are infrequent (<10 %).
Symptoms
Dysphagia
:
Difficulty with swallowing, described as food or fluid sticking, it may occur in
acute or chronic fashion, malignancy must be ruled out.
Odynophagia:
Pain on swallowing, patient with reflux esophagitis often feel retrosternal
discomfort within few seconds of swallowing hot beverages or alcohol.
Regurgitation and reflux (heartburn)
4

Surgery Dr. Nadim
Regurgitation refer to return of esophageal contents from above a functional or
mechanical obstruction. Reflux is the passive return of gastroduodenal contents to
the mouth as part of the symptomatology of gastroesopageal reflux disease (GERD).
Chest pain
Chest pain similar in character to angina pectoris may arise from an
esophageal cause, especially gastroesophageal reflux and motility disorders.
Investigations
Radiography:
1- plain radiography:
will show some foreign bodies.
2- contrast radiography:
useful investigation for demonstrating narrowing,
space-occupying lesion, anatomical distortion or abnormal motility. Video
recording is useful to allow subsequent replay and detailed analysis. Barium
radiography is, however, inaccurate in the diagnosis of GERD.
3- computerised tomography ( CT scan):
is an essential investigation in the
assessment of neoplasms of the esophagus.
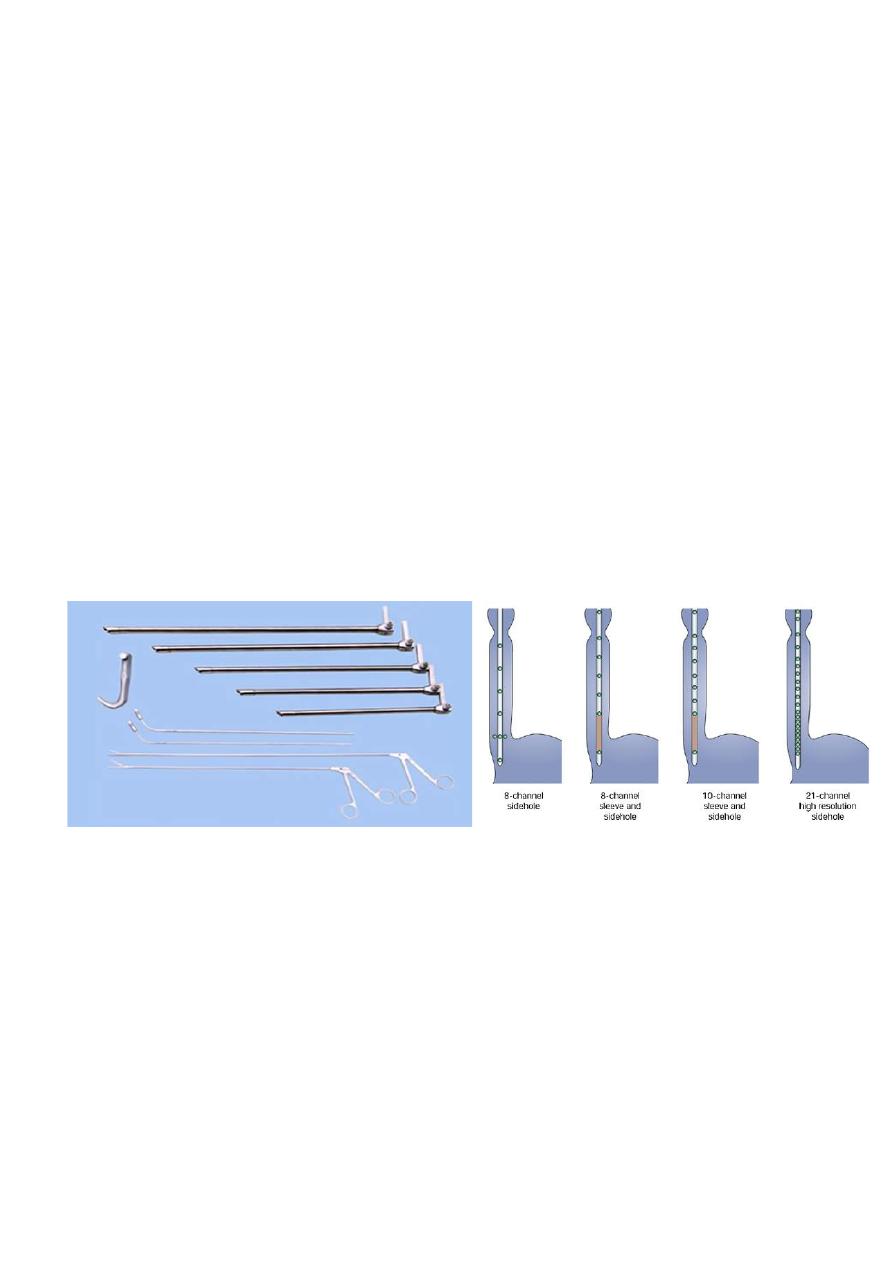
Endoscopy:
Endoscopy is necessary for the investigation of most esophageal conditions. It
is required to view the inside of esophagus and the esophagogastric junction, to
obtain a biopsy or cytology specimen, for removal of foreign bodies and to
dilate strictures. There are two types of instruments available, the rigid
esophagoscope and the flexible video endoscope.
Endosonography:
Endoscopic ultrasonography provide high detailed images of the layers of the
esophageal wall and mediastinal structures close to the esophagus.
Esophageal manometry:
Manometry is now widely used to diagnose esophageal motility disorders.
Recording are usually made by passing a multilumen catheter with three to
eight recording orifices at different levels down the esophagus and into the
stomach. Electronic microtransducers that are not influenced by change in
5
Surgery Dr. Nadim
Patient position during the test is used. The catheter is withdrawn progressively
up the esophagus,
and recording are taken at intervals of 0.5 – 1 cm to measure the length and the
pressure of LES and assess motility in the body of the esophagus during
swallowing.
24 –hours pH recording
Prolong measurement of pH is now accepted as the most accurate method
for the diagnosis of gastro-esophageal reflux. A small pH probe is passed into
the distal esophagus and positioned 5 cm above the upper margin of the LES.
The probe is connected to miniature digital recorder that is worn on a belt and
allow most normal activities. a 24 hour recording period is usual, and the pH
record is analysed by an automatic computer program.
Foreign body in the esophagus
Different type of materials may become arrested in the esophagus. The most
common impacted material is food. Denture materials also commonly seen,
button batteries is a troublesome problem in children.
plain radiographs are often useful investigation, a contrast examinations is
not usually required.
6

Surgery Dr. Nadim
Foreign bodies that have become stuck in the esophagus could be removed
either with the use of flexible endoscopy using suitable grasping forceps, a snare
or a basket, or with the use of rigid esophagoscope. During endoscopy care
should be taken that foreign body may stuck above a significant pathological
lesion, especially, if the foreign body is food materials.
Perforation of the esophagus
Etiology
1- Barotraumas ( spontaneous perforation, Boerhaave syndrome)
This occur usually when a person vomits against a closed glottis. The pressure
in the esophagus increases rapidly, and the esophagus burst at its weakest point
in the lower third, sending stream of material into the mediastinum and often
the pleural cavity as well.
2- Pathological perforation
Free perforation of ulcers or tumors of the esophagus into the pleural space
is rare. Erosion into adjacent structures with fistula formation is more common.
Fistula into the bronchus is most common and usually encountered in primary
malignant disease of the esophagus or bronchus.
3- Penetrating injury
Penetration by knives and bullets is uncommon, even in wars, as the
esophagus is relatively small target surrounded by other vital organs.
4- Foreign bodies
An object that have been left in the esophagus for several days will erode
through the wall, Perforation during removal of foreign body is more common.
5- Instrumental perforation
7

Surgery Dr. Nadim
Instrumentation is by far the most common cause of perforation, it may
follow biopsy of a malignant tumor. Patients undergoing therapeutic endoscopy
( e.g., graduated dilatation) have a perforation risk that is at least 10 times
greater than those undergoing diagnostic endoscopy.
Symptoms
1- suspicion, in the presence of technical difficulties or interventional
procedures.
2- cervical perforation may result in pain localized to neck, hoarseness, painful
neck movement and subcutaneous emphysema.
3- intrathoracic and intraabdominal perforation, are more common, giving rise
to immediate symptom and signs either during or at the end of the procedure,
including chest pain, haemodynamic instability , oxygen desaturation.
4- within the first 24 hours, there may be evidence of subcutaneous
emphysema, pneumothorax or hydropneumothorax.
5- delayed diagnosis beyond 24 hours, the patient will present as unexplained
pyrexia, systemic sepsis or the development of clinical fistula.
Investigations
1- careful endoscopic assessment at the end of the procedure.
2- chest x-ray.
3- contrast swallow, water soluble contrast or a dilute barium swallow.
4- CT scan can be used to replace contrast swallow or as adjunct with it.
Treatment
8

Surgery Dr. Nadim
Perforation of the esophagus usually lead to mediastinitis. The aim of the
treatment is to limit mediastinal contamination and to prevent or deal with the
infection.
Non-operative treatment aim to limit the effect of mediastinitis and provide
an environment in which healing can take place. Indications for non-operative
treatment include:
1- small instrumental perforation of clean esophagus without obstruction.
2- instrumental perforation in the cervical esophagus, which are usually small.
3- thoracoabdominal perforations that are detected early before oral
alimentation.
4-patients who have remained clinically stable despite delay diagnosis.
The principles of non-operative treatment include:
1- hyperalemintations preferably by an enteral rout.
2- nasogastric suction.
3- broad-spectrum intravenous antibiotic.
Surgical management is indicated whenever patients:
1- unstable with sepsis and shock.
2- have evidence of heavily contaminated mediastinum, pleural space or
peritoneum.
3- have widespread intrapleural or intraperitoneal extravasations of contrast
media.
Interventions include:
1- placement of self-expanding stent, in frail patient unfit for major surgery with
on-going luminal obstruction (mostly due to malignancy).
9
Surgery Dr. Nadim
2- direct repair if the perforation is recognized early (within 4-6 hours), and the
extent of mediastinal and pleural contamination is small.
3- T-tube into the esophagus along with appropriately located drain and feeding
jejunostomy in the presence of wide spread mediastinitis and pleural
contamination.
10

Surgery Dr. Nadim
Corrosive injury of the esophagus
Accidental ingestion occur in children and when corrosives are stored in bottles
labeled as beverages. Corrosives either alkalis or acids, all can cause damage to
the mouth, pharynx, larynx, esophagus and stomach. The type of the agent, its
concentration and the volume ingested largely determined the extent of
damage.
Alkali cause liquefaction, saponification of fat, dehydration and thrombosis of
blood vessels that usually leads to fibrous scaring. Acids cause coagulative
necrosis with eschar formation, and this coagulant may limit penetration to
deeper layers of the esophageal wall. Acids also cause more gastric damage
than alkalis because of the induction of intense pylorospasm with pooling in the
antrum.
Symptoms and signs are unreliable in predicting the severity of the injury, the
widespread use of broad-spectrum antibiotics and steroids is not supported by
evidence . The key of the management is early endoscopy to inspect the whole
of the esophagus and stomach. Minor injuries with only oedema of mucosa
resolve rapidly with no late sequelae, these patients can safely be fed.
With more sever injuries, a feeding jejunostomy maybe appropriate until the
patient can swallow saliva satisfactory. Regular endoscopic examination are the
best way to assess stricture development.
significant stricture formation occur in about 50 % of the patients with extensive
mucosal damage.
Dilatation may be appropriate for short strictures. Esophageal resection should
be differed for at least 3 months until the fibrotic phase is established.
Esophageal replacement is usually required for very long or multiple strictures.
Because of associated gastric damage, colon may be used as the replacement
conduit.
11
Surgery Dr. Nadim
Gastro-esophageal reflux diseases
Aetiology
Normal competence of gastro-esophageal junction is maintained by LES.
Failure of the LES is caused by inadequate pressure, inadequate overall length,
or abnormal position, i.e., the portion exposed to positive-pressure
environment of the abdomen. In normal circumstances, the LES relaxes
transiently as a coordinated part of swallowing, as a means of allowing vomiting
to occur, and in response to stretching of the gastric fundus, particularly after
meal to allow swallowing air to be vented. Most episodes of physiological reflux
occur during postprandial transient lower esophageal relaxations (TLESRs).
In early stages of GERD, most pathological reflux occur as a result of an
increase number of TLESRs rather than a persistent fall in overall sphincter
pressure. In more sever GERD, LES pressure tends to be generally low, and this
loss of sphincter function seems to be made worse if there is loss of an
adequate length of intra-abdominal esophagus.
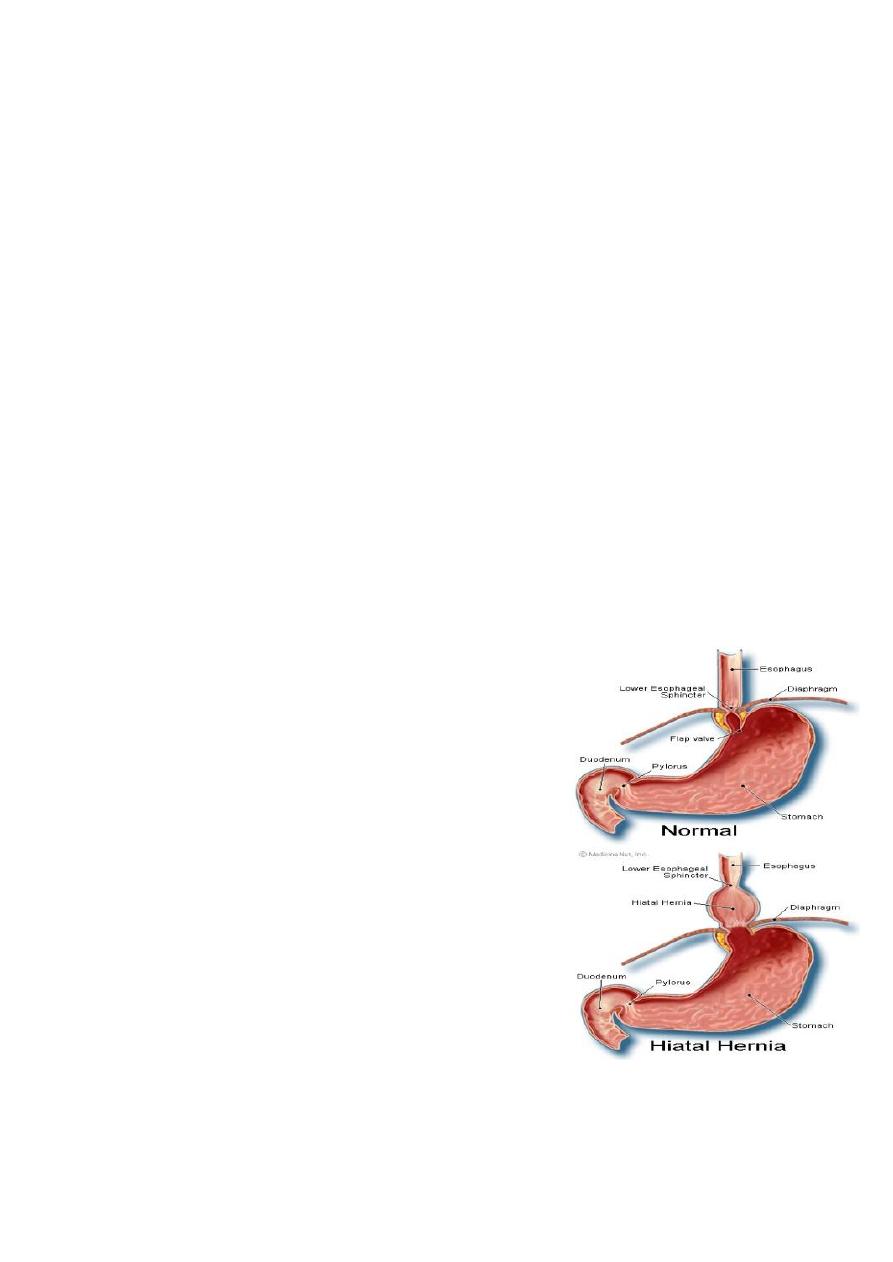
The absence of an intra-abdominal length of the
esophagus result in sliding hiatus hernia. The
normal condensation of peritoneal fasia over the
lower esophagus ( the phreno-esophageal ligament
) is weak, and the crural opening widens allowing
the upper stomach to slide up through the hiatus.
Sliding hiatus hernia is associated With GERD and
make it worse but, as long as the LES remain
competent pathological GERD does not occur.
Many GERD sufferers does not have
hernia, and many of those with hernia do not have
GERD. Reflux esophagitis is a complication of GERD
and occur in a minority of sufferers overall.
12

Surgery Dr. Nadim
Clinical features
The classical triad of symptoms is retrosternal burning pain (heart burn),
epigastric pain (some time radiated through to the back) and regurgitation.
Most patients do not experience all three.
Symptoms are often provoked by food, particularly those that delay gastric
emptying (e.g. fats, spicy foods). As the condition become more sever, gastric
juice may reflux to the mouth and produce an unpleasant taste often described
as “acid’ or “bitter”. A proportion of patients have odynophagia with hot
beverages. Some patients present with less typical symptoms such as
angina-like chest pain,
pulmonary or laryngeal symptoms.
Diagnosis
➢ In most cases, the diagnosis is assumed rather than proven, and treatment
is empirical.
➢ Investigation is only required when: a- the diagnosis is in doubt, b- when
the patient does not response to proton pump inhibitor (PPI), c- if
dysphagia is present.
➢ The most appropriate examination is endoscopy and biopsy. If the typical
appearance of reflux esophagitis, peptic stricture or Barrett’s esophagus is
seen, the diagnosis is clinched, but visible esophagitis is not always present
because the widespread use of PPIs, which cause rapid healing of early
mucosal lesions.
➢ In patients with atypical or persistent symptoms despite therapy,
esophageal manometry and 24-hour esophageal pH recording (gold
standard test) may be justified to establish the diagnosis and to guide
management. These tests are essential in patients being considered for
anti-reflux surgery.
13

Surgery Dr. Nadim
Management
Medical management
• Simple measures include advice about weight loss, smoking, excessive
consumption of alcohol, tea or coffee, the avoidance of large meals late at
night and a modest degree of head-up tilt of the bed.
• PPIs are the most effective drug treatment for GERD. Most patients have
rapid improvement in symptoms within few days, and more that 90 % can
expect full mucosal healing at 8 weeks time.
• If medical management is unsuccessful, these patients should be formally
investigated.
Surgery
The need for surgery should have been reduced as medications has improved
so much. Indication for surgery
➢ “volume” reflux.
➢ “hermit” lifestyle in which the least deviation from life style rules leads to
symptoms.
➢ Poor compliance, this is due to side effects of treatment.
➢ Psychological distress with intolerance of minor symptoms.
Which operation? All the operations must achieve the following:
➢ An intra-abdominal segment of esophagus.
➢ Crural repair.
➢ Some form of wrap of the upper stomach (fundoplication) around the
intra-abdominal esophagus.
Operations that fail to address all the three components have inferior success
rate.
14
Surgery Dr. Nadim
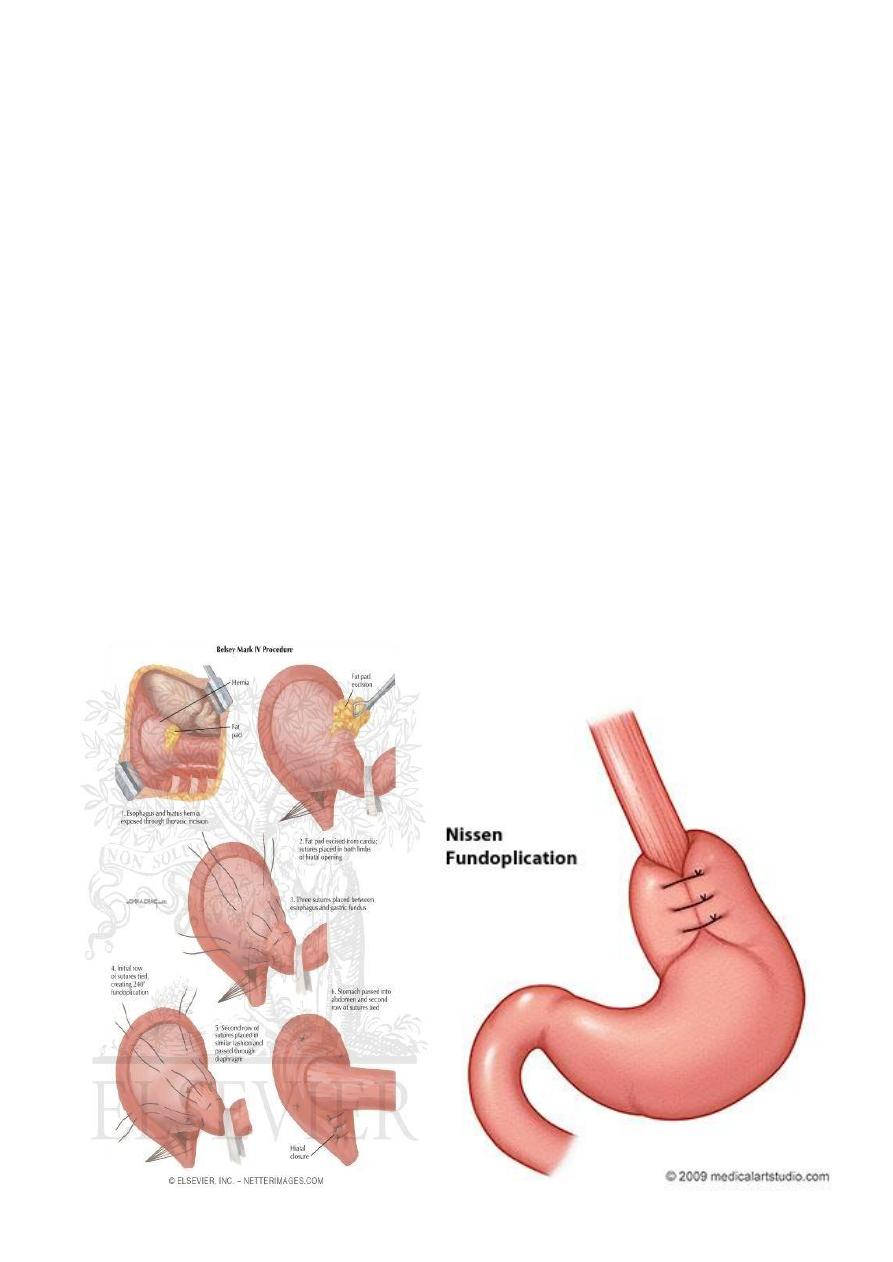
Type of operations:
➢ Total fundoplication (Nissen), through the abdomen, the funds of the
stomach is drawn behind the esophagus and then sutured to itself in front
of the esophagus. One of the disadvantage of this surgery is the creation
of overcompetent cardia, resulting in the “gas bloat” syndrome in which
belching impossible.
➢ Partial fundoplication, through the abdomen, whether performed
postreiorly (Toupet) or anteriorly (Dor, watson).
➢ Laparoscopic fundoplication, through the abdomen, by the use of
laparoscope to perform total or partial fundoplication.
➢ Belsey mark IV operation, through the chest, the fundus of the stomach is
warped around the lower esophagus, and the hiatus is narrowed, and
appropriate segment of the esophagus is created inside the abdomen.
15
Surgery Dr. Nadim
Complications of gastro-esophageal reflux diseases
Stricture
Occur mainly in late middle-aged and elderly, it is about 1-2 cm above the
esophago-gastric junction, and should be distinguished from carcinoma. Peptic
strictures generally respond well to dilatation and long term treatment with a PPI.
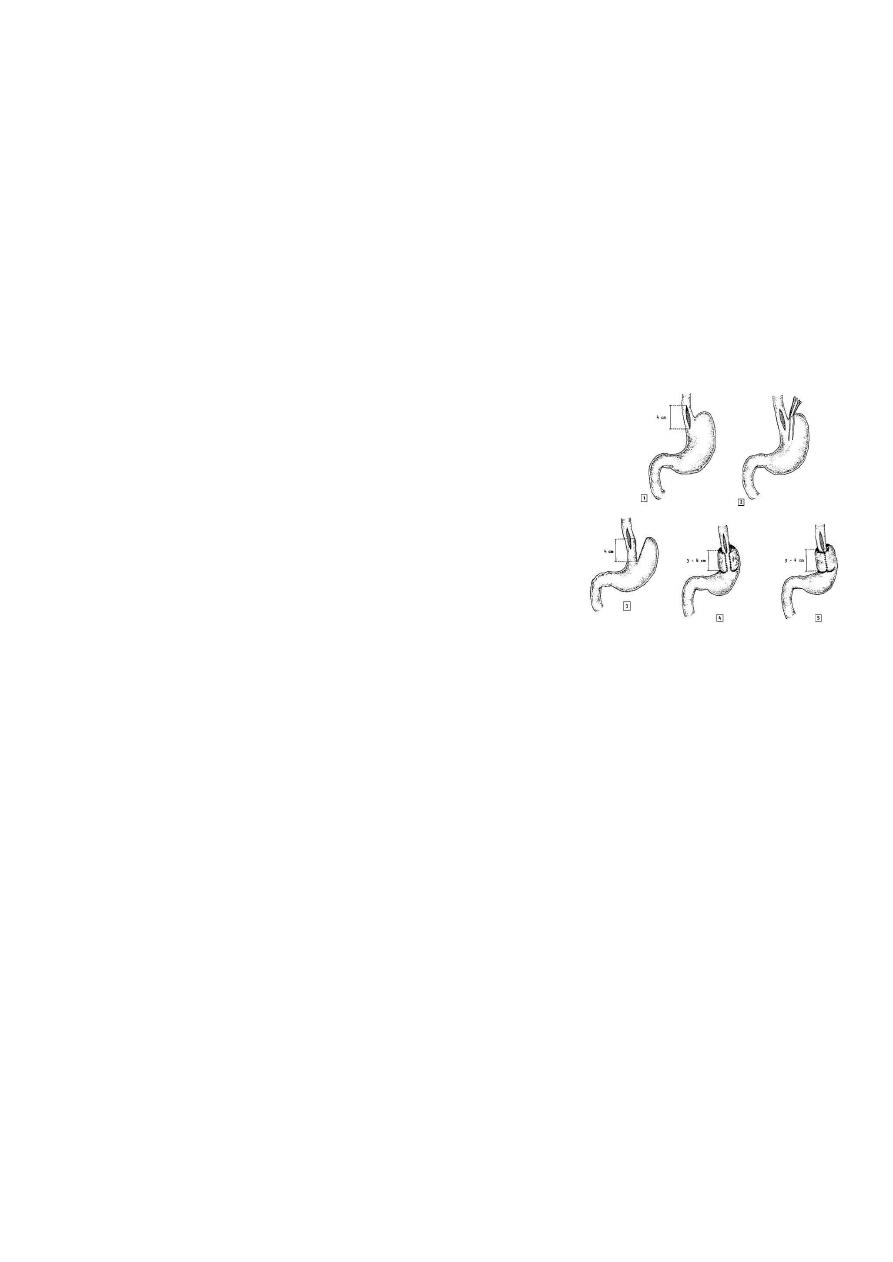
Esophageal shortening
Sever inflammation in the wall of the esophagus
causes fibrosis,and may cause shortening. In the
presence of a large sliding hiatus hernia, the
esophagus is short, but this does not necessarily
mean that, with mobilization from the mediastinum,
it cannot easily be restored to its normal length. If a
good segment of intra-abdominal esophagus cannot
be restored without tension, a Collis gastroplasty
should be performed, usually fundoplication is performed around the
neo-esophagus (Collis-Nissen operation).
Barrett’s esophagus (columnar lined lower esophagus)
Barrett’s esophagus is a metaplastic changes in the lining mucosa of the
esophagus in response to chronic gastro-esophageal reflux. Many of these
patients do not have particularly sever symptoms. The adaptive response to
GERD begins as a simple columnar epithelium that become specialized with
time. The hallmark of specialized Barrett’s epithelium is the presence of mucus
secreting goblet cells (intestinal metaplasia). In Barrett’s esophagus the junction
between sequamous esophageal mucosa and gastric mucosa moves proximally.
When intestinal metaplasia occurs, there is an risk of adenocarcinoma of the
esophagus.
Patients who are found to have Barrett’s esophagus may be submitted to
regular surveillance endoscopy with multiple biopsies in the hope of finding
16

Surgery Dr. Nadim
dysplasia or in situ cancer rather than allowing invasive cancer to develop and
cause symptoms. 2-year intervals are probably adequate, provided no dysplasis
has been detected. When Barrett’s esophagus is discovered, the treatment is
that of the underlying GERD.
Neoplasms of the esophagus
Benign tumors
Benign tumors of the esophagus are relatively uncommon. Leiomyomas are
the most common benign esophageal tumors (50 %). The average age at
presentation is 38 years, mostly located in the lower two-third of the
esophagus, usually solitary, vary greatly in shape and size. Typically, leiomyomas
are oval, they grow toward the lumen. Dysphagia and pain are the most
common complaints. Barium swallow is the most useful method to demonstrate
leiomyoma of the esophagus.
Leiomyomas should be removed surgically, the majority can be removed by
simple enucleation.
Other benign tumors: fibromas, myomas, fibromyomas, lipomyomas, myxoma,
firbrolipomas.
Malignant tumors
Non-epithelial primary malignancies are also rare, as in malignant melanoma.
Secondary malignancies rarely involve the esophagus with the exception of
bronchogenic carcinoma by direct invasion of the primary tumor or contagious
lymph node.
Carcinoma of the esophagus
Cancer of the esophagus is the sixth most common cancer in the world. It is a
disease of mid to late adulthood, with a poor survival rate. Only 5-10% of those
diagnosed will survive for 5 years.
Pathology and aetiology
17

Surgery Dr. Nadim
Sequamous cell carcinoma
is the most common type, generally affect the
upper two-thirds of the esophagus.
Adenocarcinoma
is increasing in incidence,
and usually affects the lower one-third. The geographical variation and the
aetiology is as the following:
➢ Sequamous cell cancer is endemic in south Africa and in the Asia “cancer
belt” that extends across the middle of Asia from north Iran to china. The
highest incidence in the world is in Linxian in Henan province in china. The
cause of the disease in the endemic areas in unknown, but it is probably
due to the combination of fungal contamination of food and nutritional
deficiencies.
➢ Tobacco and alcohol are major factors in the occurrence of sequamous cancer.
➢ Obesity and the GERD is likely to be an important factor for the increase
incidence of adenocarcinoma.
Clinical features
Most esophageal neoplasm present with mechanical symptoms, principally
dysphagia. Other symptoms include vomiting, regurgitation, odynophagia and weight
loss. Clinical findings suggestive of advance malignances and surgical cure is unlikely
include:
➢ Recurrent laryngeal nerve palsy
➢ Horner’s syndrome
➢ Chronic spinal pain.
➢ Diaphragmatic paralysis.
➢ Cutaneous tumor metastasis.
➢ Enlarged supraclavicular lymph nodes.
Both denocarcinoma and sequamous cell carcinoma tend to disseminate
early. Tumor can spread in three ways:
➢ Direct spread occur both laterally through the esophageal wall layers and
longitudinally within the esophageal wall.
➢ Lymphatic spread, either longitudinally through the submucosal lymphatic
channels, consequently, the length of the esophagus involved by the tumor is
much longer than the macroscopic length of the malignancy at the epithelial
surface. lymph node spread occur commonly, Any regional lymph nodes from
the superior mediastinum to the coeliac axis and lesser curvature of the
18

Surgery Dr. Nadim
stomach may be involved regardless of the location of the primary lesion within
the esophagus.
➢ Haematogenous spread may involve different organs including the liver,
lung, brain and bones.
Investigations
➢ Endoscopy is the first line investigation for most patients, it provides direct
view of the esophageal mucosa and any lesion allowing its site and size to
be documented. Cytology and biopsy specimens taken via the endoscopy
are crucial for accurate diagnosis.
➢ Transcutaneous ultrasound, used mainly to assess spread to the liver.
➢ Chest radiography, to assess spread to the lungs and mediastinum.
➢ Bronchoscopy, may reveal either impingement or invasion of the main
airways in over 30% of patients with cancer in the upper third of the
esophagus.
➢ Laparoscopy, this is useful technique for the diagnosis of intra-abdominal
metastasis. It has the advantage of enabling tissue samples or peritoneal
cytology to be obtained.
➢ Computerised tomography (CT scan), for assessment of the esophagus,
the size and site and the direct invasion of the tumor, lymph nodes
involvement , and haematogenous spread.
➢ Endoscopic ultrasound (EUS), it is more accurate than CT scan in determination
the depth of spread of malignant tumor through the esophageal wall, the
invasion of the adjacent organs, and metastasis to lymph nodes.
➢ Positron emission tomography (PET), reduction in PET activity following
chemotherapy might be a way of predicting responders to this approach.
19

Surgery Dr. Nadim
Treatment of malignant tumors
At the time of diagnosis, around two –third of all patients with esophageal
cancer will already have incurable disease and must be offered some form of
palliation. As dysphagia is the predominant symptom in advanced esophageal
cancer, the principle aim of palliation is to restore adequate swallowing. A varity
of methods are available, this include:
➢ Intubations like souttar tube, which made of coiled silver wire, or other
types of rigid plastic or rubber tubes, usually placed under endoscopic
and/or radiological control.
➢ expanding metal stent, more commonly used now in most centers allover
the world, also inserted under radiographic or endoscopic control.
➢ Other methods, like endoscopic laser treatment to core a channel through
the tumor or brachytherapy which include delivering intraluminal
radiation with short penetration distance to a tumor.
Surgery
alone
is best suited to patients with disease confined to the
esophagus without nodal metastasis, with a prospect of cure in between 50%
and 80%. The operative approaches are:
➢ Left thoracoabdominal approach, which opens the abdominal and the
thoracic cavity together, this approach is limited proximally by the aortic
arch and should be avoided when the primary tumor is at or above this
level.
➢ Ivor Lewis operation, the most widely practiced approach in the world,
with an initial laparotomy and construction of gastric tube, followed by
right thoracotomy to excise the tumor and create an esophageogastric
anastomoses.
➢ Transhiatal esophagectomy (without thoracotomy), the stomach is mobilized
through a midline abdominal incision, and the esophagus is mobilized through
20
Surgery Dr. Nadim
an incision in the neck. it may be useful procedure for tumor of lower
esophagus.
➢ Patients with more advanced stages of disease required multimodal
approaches (surgery plus
➢ chemotherapy or chemoradiotherapy). In patients who are unfit for
surgery, chemoradiotherapy may
➢ be a useful alternative.
Achalasia
Pathology and aetiology
Achalasia (Greek “failure to relax”) is uncommon. It is due to loss of the
ganglion cells in the myenteric (Auerbach’s) plexus, the cause of which is
unknown. The physiological abnormalities are a non-relaxing LES and absent
peristalsis in the body of the esophagus. In its earliest stages, the esophagus is
of normal caliber and still exhibit contractile (although non-peristaltic) activity.
With time, the esophagus dilates and contractions disappears, so that the
esophagus empties mainly by the hydrostatic pressure of its contents. This is
nearly always incomplete, leaving residual food and fluid.
The gas bubble in the stomach is frequently absent. The esophagus may
becomes huge, and tortuous with persistent retention esophagitis due to
fermentation of food residues “ megaesophagus”.
Clinical features
The disease is most common in middle
life, but can occur at any age. It typically
presents with dysphagia. Patients often
present late, having had relatively mild
symptoms for many years
Regurgitations is frequent, and may be
overspill into the trachea, especially at
night.
Diagnosis
➢ Barium radiography, may show
hold-up in the distal esophagus,
21

Surgery Dr. Nadim
abnormal contractions in the esophageal body, and tapering stricture in
the distal esophagus often describe as a “bird’s beak”. The gastric bubble
usually absent.
➢ Endoscopy, by finding tight cardia and food residue in the esophagus.
➢ Esophageal manometry, give a firm diagnosis.
Treatment
Achalasia respond well to treatment. The two main methods are forceful
dilatation of the cardia and Heller’s myotomy.
Pneumatic dilatation
This involve stretching the cardia with a balloon to disturb the muscle and
render it less competent. The balloon are inserted over a guide wire. Perforation
is the major complication (less than 5%). In the well developed centers forceful
dilatation is curative in 75-85% of cases.
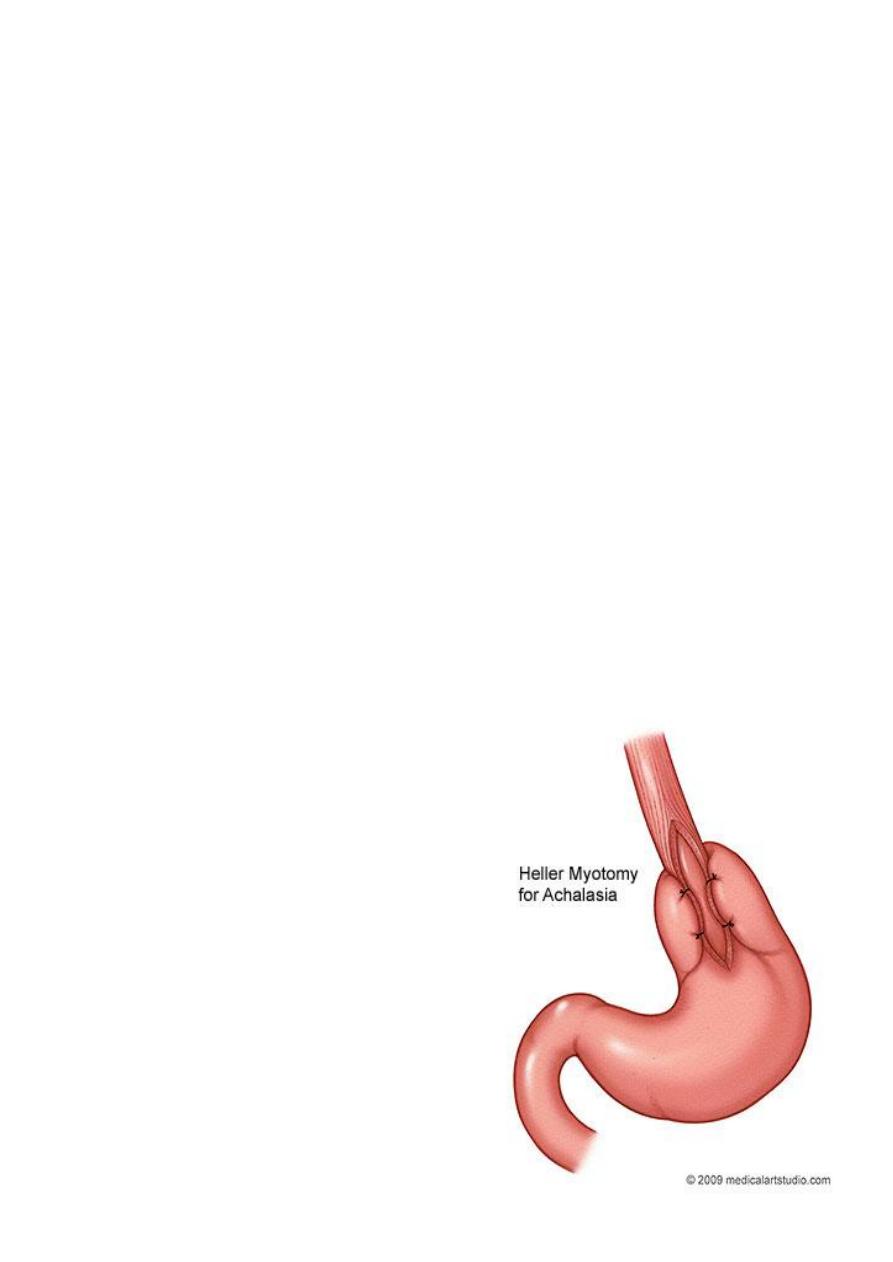
Heller’s myotomy
This involve longitudinal cutting in the muscles of the lower esophagus and
cardia. The major complication is GERD, and many surgeons, therefore, add a
partial anterior fundoplication (Heller’s-Dor’s operation). The operation is
ideally performed through the thoracic approach, but could be done through
abdominal approach, and recently, through minimal access laparoscopic
approach. It is
successful in more than 90% of cases and may be used after failed dilatation.
Botulinum toxin
This is done by endoscopic injection into the LES. It acts by interfering with
cholinergic excitatory neural activity at the LES. The effect is not permanent,
and the injection usually has to be repeated after a few months. For this reason,
its use is restricted to elderly patients with other comorbidities.
Drugs
22

Surgery Dr. Nadim
Drug such as calcium channel antagonists or sublingual nifedipine may be
useful for transient relief of symptoms.
Miscellaneous conditions
Zinker’s diverticulum (pharyngeal pouch)
It protrudes posteriorly above the cricopharyngeal sphincter through the
natural week point (the dehiscence of Killian) between the oblique and the
horizontal fibers of the inferior pharyngeal constrictors.
Epiphrenic diverticulum
Situated in the lower esophagus above the diaphragm, they may be quite
large, but causing few symptoms.
Plummer-Vinson syndrome
Also called Paterson-kelly syndrome, dysphagia occur because of the
presence of a post-cricoid web that is associated with iron deficiency anemia,
glossitis, and Koilonychia.
Schatzki’s ring
Is a circular ring in the distal esophagus, usually at the sequamocolumnar
junction, it may associated with reflux disease. Most are asymptomatic, when
associated with dysphagia, dilatation with anti-reflux drugs must be used.
23