
Acute Renal Colic
The overall lifetime rate of kidney stones in the general population is approximately 12% for men
and 4% for women. Peak incidence occurs in people aged 35-45 years. When stones occur in persons in
these uncommon age groups, a metabolic workup consisting of a 24-hour urine collection and
appropriate serum laboratory testing is recommended.
Black people have a lower incidence of stones than white people
Clinical Aspects of Acute Renal Colic
§
In general, smaller stones are more likely to pass spontaneously, If the stone is 4 mm or smaller,
the stone is eventually passed 90% of the time. Stones 5-7 mm generally have a 50% chance of
passing spontaneously. Calculi larger than 7 mm are unlikely to pass unassisted.
Clinical findings
§
1-acute renal colic is the sudden onset of severe pain originating in the flank and radiating
inferiorly and anteriorly.
§
2-Approximately 85% of all patients with renal colic demonstrate at least microscopic
hematuria
§
3-pyuria, fever, leukocytosis, or bacteriuria suggests the possibility of a urinary infection
and the potential for an infected obstructed renal unit or pyonephrosis
§
4-Nausea and vomiting are often associated with acute renal colic and occur in at least
50% of patients.
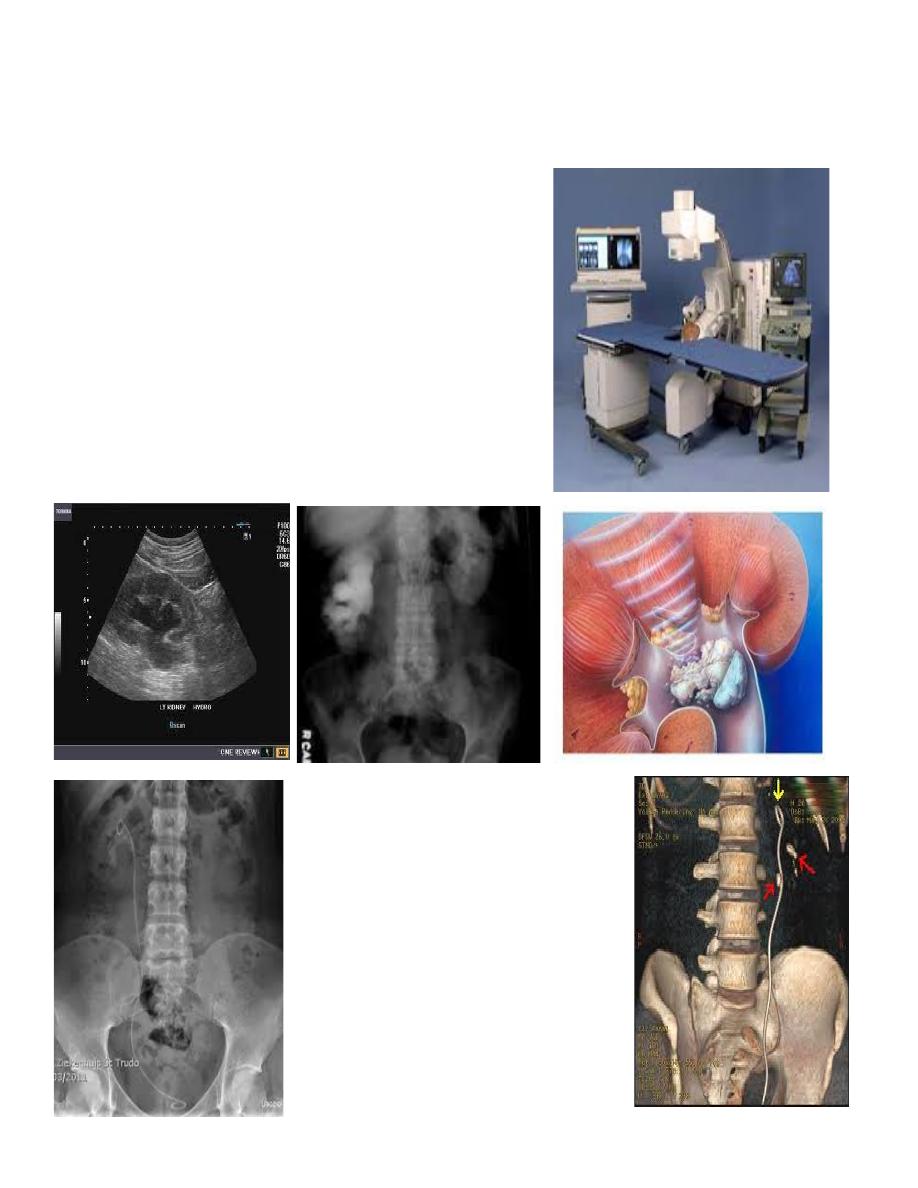
Imaging Studies
§
Plain Abdominal Film
§
Renal Ultrasound(size,operator,safe,cheap).
§
Intravenous Pyelogram(clear outline)
§
CT Scans
§
Retrograde Pyelograms
§
Magnetic Resonance Imaging?
Differential Diagnoses of Flank Pain
§
Muscle pain., Radiculitis, Pelvic inflammatory disease,acute appendicitis,biliary
colic,dysmenorrhea, Ectopic or tubal pregnancy, Herpes zoster, Ovarian cyst rupture or
torsion
§
Pregnancy
§
Pregnancy is usually associated with a physiologic hydronephrosis
Hospitalization
§
Hospital admission is clearly necessary when any of the following is present:
§
1-Oral analgesics are insufficient to manage the pain.
§
2-Ureteral obstruction from a stone occurs in a solitary or transplanted kidney.
§
3-Ureteral obstruction from a stone occurs in the presence of a UTI, fever, sepsis, or
pyonephrosis.
§
Relative indications to consider for a possible admission include comorbid conditions (eg,
diabetes), dehydration requiring prolonged intravenous fluid therapy, renal failure, or any
immunocompromised state. Larger stones (ie, >7 mm) that are unlikely to pass spontaneously
require some type of surgical procedure.
1-Medications
§
Narcotics and opioids
§
Nonsteroidal anti-inflammatory drugs
§
Antiemetics
§
Antidiuretics
§
Antibiotics
§
Aggressive Medical Therapy
2-Stents
3-Percutaneous nephrostomy (P.C.N.L.)
4-Extra corporial shockwave lithotripsy(E.S.W.L.)
5-uretroscopic stone fragmentation
6-open surgical stone removal
By:
Muhammed Shakir Yashar
M. Shakir