
Diseases of retroperitoneal spaces
Retroperitoneal fibrosis
Retroperitoneal cysts
Retroperitoneal tumors
Retroperitoneal lymphomas
Retroperitoneal vascular diseases, e.g. aneurysms
Retroperitoneal trauma and haematoma
Retroperitoneal infection, e.g. psoas abscess, pyogenic abscess
Diseases of the specific retroperitoneal organs, e.g. adrenals, kidney.
PSOAS ABSCESS
Abscess in the psoas region in the iliac fossa, is commonly due to tuberculosis of spine
(T 10) and lymph nodes, retroperitoneal structures, lower intercostal region.
It can also be a pyogenic abscess.
Clinical Features
1- Back pain, fever, spinal tenderness, paraspinal spasm and restricted spine
movement.
2- Swelling in iliac fossa which is smooth, nontender, nonmobile, not moving with
respiration.
3- When it extends across the groin and below the inguinal ligament, it is cross
fluctuant across the inguinal ligament.
4- Patient has typical psoas muscle spasm in which patient is able to flex his hip but finds
it difficult to extend.
Differential Diagnosis
a
.
A.Iliac artery aneurysm.
b
.
B. Ovarian cyst in females.
C. Soft tissue tumours and cysts in the iliac region.
D. Hernia.
Investigations
X-ray spine and chest
CT scan.
Mantoux test, ESR, peripheral smear --- U/S abdomen.
Treatment
1- Antituberculous: INH, ethambutol, rifampicin, pyrazinamide.
2- surgery: Under G/A through lateral loin incision, the psoas region is reached
extraperitoneally. The pus is drained and collected for culture and sensitivity, AFB,
culture. The wound is closed.
RETROPERITONEAL SWELLINGS
Types ;
Benign—20%
Retroperitoneal lipoma
Retroperitoneal neurofibroma, neurilemmoma
Retroperitoneal leiomyoma
Extra-adrenal chromaffinomas
Paraganglioma
Mucinous cystadenoma
Haemangiopericytoma
Malignant—80%
Retroperitoneal liposarcoma, leiomyosarcoma—50%
Retroperitoneal lymphoma (commonly NHL)
Malignant tumours from specific organs
Germ cell tumours, chordomas.
RPLN secondaries with hard nodules
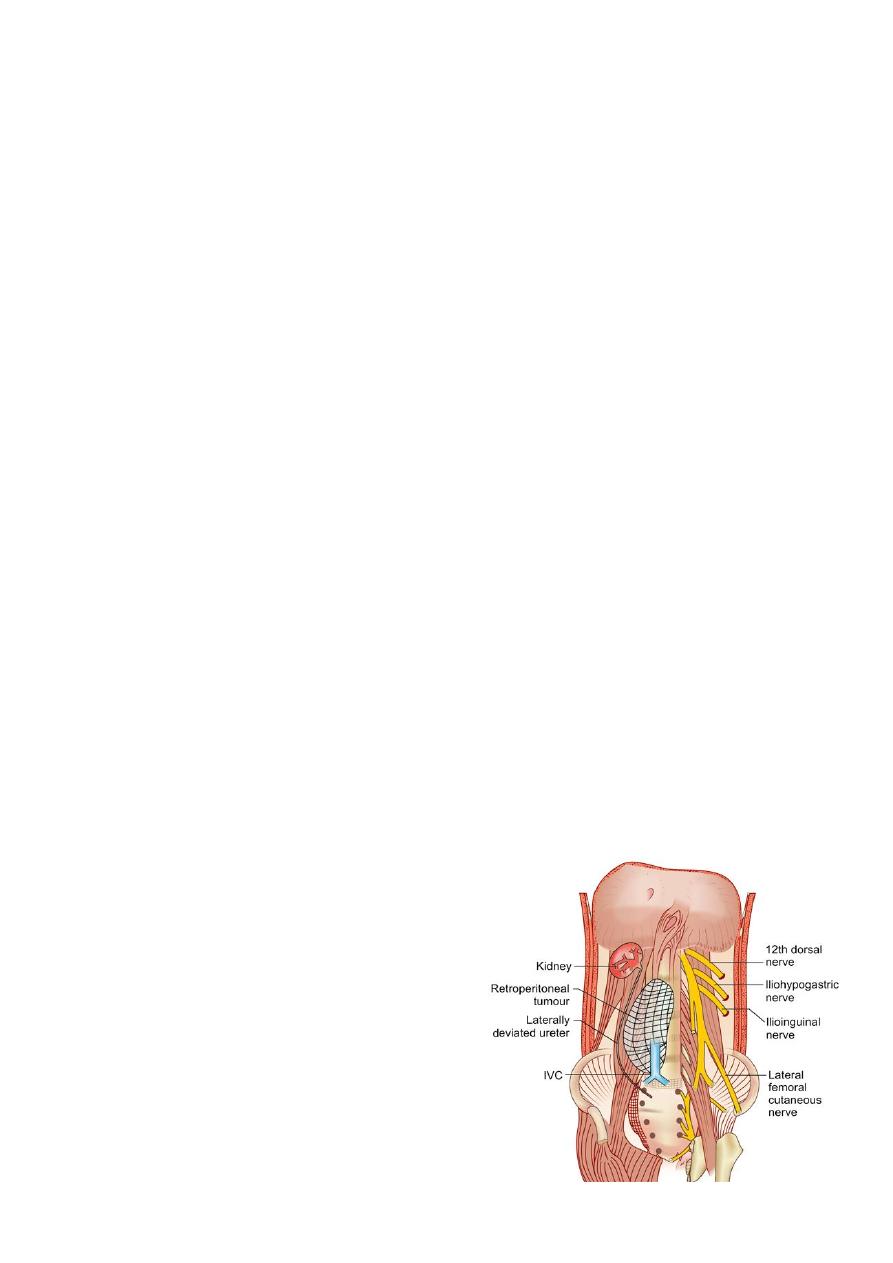
Retroperitoneal tumour can attain very large size
It causes deviation of ureter laterally often may
invade the ureter
(In retroperitoneal fibrosis ureter is deviated
medially).
It may invade or encase the IVC also causing
IVC obstruction with features of bilateral oedema
feet, dilated lateral abdominal wall vein with
upward direction flow of blood

RETROPERITONEAL TUMOURS
*can be benign or malignant.
*Solid tumours=Commonly malignant
*cystic tumours are usually benign.
Malignant= may be mesodermal ,neuroectodermal or embryonic remnant in origin.
Rarely it can be urologic or metastatic also.
Sarcoma is the most common malignancy
in adult
—liposarcoma is the most common retroperitoneal sarcoma ,leiomyosarcomais
malignant nerve sheath tumour, fibrosarcoma malignant fibrous histiocytoma can also
occur.
In children
rhabdomyosarcoma is the most common one.
Aetiology:
it may be associated with radiation and exposures to chemicals like vinyl
chloride/thorium dioxide, familial Gardner’s syndrome, familial retinoblastoma or
familial neurofibromatosis, Li Fraumeni syndrome, germline mutations of p53 in
chromosome 17.
Features
Tumor arises from fat, areolar tissue, vessels, nerves, skeletal and smooth muscle,
fascia, lymph .Sarcomas can be commonly solid, cystic or mixed. Usually tumour
develops a pseudocapsule.
Liposarcoma
Liposarcoma often originates from perinephric fat. It can be well-differentiated or
undifferentiated (dedifferentiated). It spreads along the fascial planes enveloping the
organs. Infiltration of organs occurs only at late stage. Spread of retroperitoneal
sarcoma mainly occurs through blood to lungs and often to liver.Nodal spread occurs
rarely .
Presentations
1- Most patients have initial asymptomatic course with eventual presentation as mass
abdomen .
2- Pelvic mass ,vague abdominal pain and discomfort , anorexia,fatigue, vomiting,
weight loss, fullness in
abdomen, back pain due to compression over lumbar and pelvic nerves, leg pain,
recurrent episodes of fever.
3-GI bleeding; intestinal/urinary obstruction ; neurological manifestations by
compression or invasion of neurological systems by tumor; iliac vein or IVC
compression can cause lower limb varicosities, varicocele, and
dilated abdominal veins with venous flow from below upwards, and oedema.

Investigations
*CT abdomen, pelvis and CT chest (to see metastases) are essential investigations./ CT
guided core biopsy; laparoscopic biopsy are needed.( FNAC has got limited role).
*MRI is better than CT with near 100% accuracy.
*Retroperitoneoscopy may be ideal to take biopsy.
* IVU shows laterally deviated ureter.
*Plain X-ray may show soft tissue shadow, obliterated psoas shadow, and often
calcification.
* AFP, HCG and other tumour markers are done often.
*LFT, blood urea and serum creatinine is done.
* Histochemistry is essential in many suspicious types.
Treatment
1- Surgery is the main modality of therapy with wide excision is the ideal.
2- Limited resection; debulking (controversial) are other options.
**
Complications are
—injury to major structures, bleeding, sepsis, and leak.
* Postoperative chemotherapy and radiotherapy is used as adjuvant method.
Features of the Retroperitoneal Mass
*It is usually large.
*Not moving with respiration.
*Nonmobile.
*Does not fall forward (confirmed by knee-elbow position).
*Deeply placed.
*Resonant on percussion (because of the bowel in front). In retroperitoneal cyst and
sarcoma the
*swelling is smooth.In lymphoma it is smooth and firm. In aneurysm it is pulsatile
(expansile pulsation) which will persist even in knee-elbow position.
Confirmation
is by U/S, CT scan, MRI.
Most common retroperitoneal benign tumour is lipoma.
Sarcoma (commonest is liposarcoma 40%) which attains a very large size, goes for
myxomatous degeneration very early and is aggressive.

RETROPERITONEAL FIBROSIS
Causes
1- Idiopathic type (70%) is called as Ormond’s disease which is associated other fibrosis.
It is nonspecific inflammation of fibro-fatty tissue in the retroperitoneum.
2-Methysergide and beta blocker , Ergot’s alkaloids, dopamine agonists
3- Urine leak and collection in the space
4-6-Retroperitoneal surgeries, haemorrhage , Haematoma, blood collection
5- Advanced malignancy, radiation.
7-Trauma, infection.
Clinical features ;-
Disease is progressive one.
1-Patient presents with severe and persistent back pain.
2- Diffuse fibrosis in retroperitoneum can compress both ureters leading to bilateral
hydronephrosis and renal failure.* In 30% cases it is bilateral.
3-Hypertension, lower limb oedema (lymphatic or venous block), feeble lower limb
arterial pulses are common.
* It is like woody fibrous tissue which narrows ureters, vessels and nerves.
*Venous and lymphatic oedema of limbs can occur.
* It may be localised or generalised
. Generalised type may extend into duodenum, CBD
and pancreas. It is not encapsulated but margin is well-demarcated.
Investigation;-
U/S- CT scan. -IVU—diagnostic.
Blood urea and serum creatinine, raised ESR and CRP.
Triad;-
Deviation of middle 1/3rd of ureter medially / Hydroureteronephrosis/
Extrinsic ureteral compression
Treatment;-
1- Drug therapy: Methylprednisolone, azathioprine, penicillamine, tamoxifen.
2- Cystoscopic stenting of the ureters to prevent renal failure.
3- Symptomatic treatment:
*If stenting fails, bilateral nephrostomy is done.
* Ureterolysis./ Lateral repositioning of ureters./ Omental wrap after ureterolysis.
* Vascular bypass graft for vascular encasement.

Retroperitoneal sarcoma (RPS)
Clinical presentations
1-nontender palpable RP mass, weight loss, pain and discomfort
2-neurologic ;urinary ; bowel obstruction;
3-paraneoplastic syndrome (hypoglycaemia)
4- metastases
Features of retroperitoneal sarcomas
*Mass per abdomen
*Pain in the back and compressive features
*GIT obstruction especially by leiomyosarcoma
*Compression over the ureter causing hydro nephrosis
*Compression over the major veins causing varicose veins
*Arterial compression features are not common
*Liver and lung secondaries can occur
*CT guided biopsy is ideal method of investigations
Treatment of retroperitoneal tumours
Wide local excision often requires removal of adjacent structures like colon, kidney, and
spleen.
Debulking operation as a palliative/ Enucleation through pseudocapsule.
Radiotherapy / Chemotherapy
Liposarcoma
is the most common RP sarcoma;
it can be well-differentiated, dedifferentiated, myxoid, round cell, Pleomorphic .
*CT guided core biopsy through posterior approach, MRI are the investigations needed.
*Surgery is the choice of therapy—monobloc complete surgical resection .
Adjuvant RT to retroperitoneum is used to prevent local recurrence.