
1
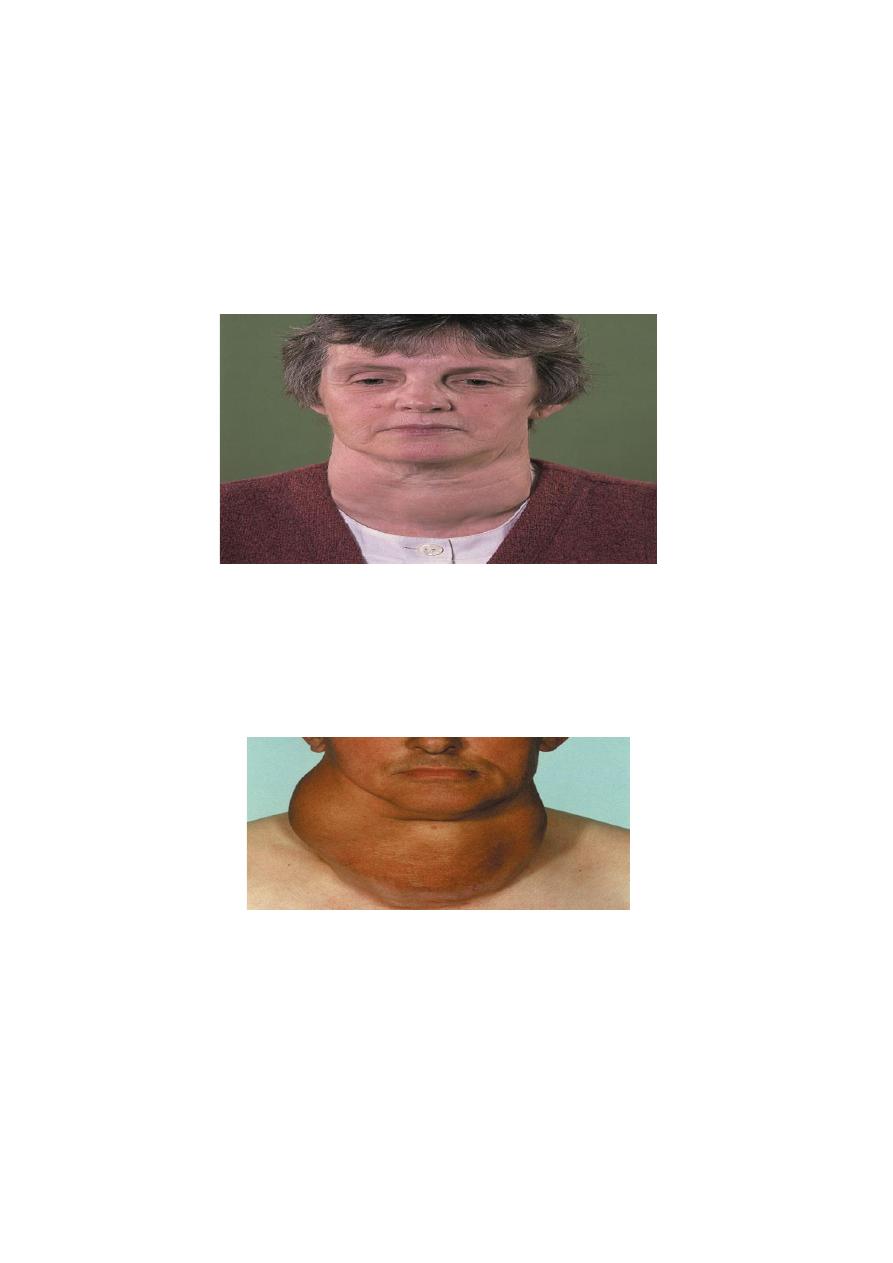
GOITRE
is enlargement of the thyroid gland. A discrete swelling (nodule) in one lobe with no palpable
abnormality elsewhere is termed an isolated (or solitary) swelling. Discrete swellings with evidence of
abnormality elsewhere in the gland are termed dominant.
Classification of thyroid swellings
Simple goitre (euthyroid)
Diffuse hyperplastic
Physiological
Pubertal
Pregnancy
Multinodular goitre
Toxic
Diffuse
Graves’ disease
Multinodular
Toxic adenoma
Neoplastic
Benign
Malignant
Inflammatory
Autoimmune
Chronic lymphocytic thyroiditis
Hashimoto’s disease
Granulomatous
De Quervain’s thyroiditis
Fibrosing
Riedel’s thyroiditis
Infective
Acute (bacterial thyroiditis, viral thyroiditis, ‘subacute thyroiditis’)
Chronic (tuberculous, syphilitic)
Other
Amyloid

2
Simple goitre
Aetiology
Simple goitre may develop as a result of stimulation of the thyroid gland by TSH, either as a result of
inappropriate secretion from a microadenoma in the anterior pituitary (which is rare) or in response
to a chronically low level of circulating thyroid hormones.
The most important factor in endemic goitre is dietary deficiency of iodine, but defective hormone
synthesis probably accounts for many sporadic goitres .
Goitrogens
Well-known goitrogens are the vegetables of the brassica family (cabbage, kale and rape), which
contain thiocyanate, drugs such as para-aminosalicylic acid (PAS) and, the anti-thyroid drugs.
Thiocyanates and perchlorates interfere with iodide trapping whereas carbimazole and thiouracil
compounds interfere with the oxidation of iodide and the binding of iodine to tyrosine.
Iodides in large quantities are goitrogenic because they inhibit the organic binding of iodine and
produce an iodide goitre. Excessive iodine intake may be associated with an increased incidence of
autoimmune thyroid disease.
The natural history of simple goitre
The stages in goitre formation are as follows:
• Persistent growth stimulation causes diffuse hyperplasia; all lobules are composed of active follicles
and iodine uptake is uniform. This is a diffuse hyperplastic goitre, which may persist for a long time
but is reversible if stimulation ceases.
• Later, as a result of fluctuating stimulation, a mixed pattern develops with areas of active lobules
and areas of inactive lobules.
• Active lobules become more vascular and hyperplastic until haemorrhage occurs, causing central
necrosis and leaving only a surrounding rind of active follicles.
• Necrotic lobules coalesce to form nodules filled with either iodine-free colloid or a mass of new but
inactive follicles.
• Continual repetition of this process results in a nodular goitre.
Most nodules are inactive, and active follicles are present only in the internodular tissue.
3
Diffuse hyperplastic goitre
Diffuse hyperplasia corresponds to the first stages of the natural history. The goitre appears in
childhood in endemic areas but, in sporadic cases, it usually occurs at puberty when metabolic
demands are high. If TSH stimulation ceases the goitre may regress; however, it tends to recur later
at times of stress such as pregnancy. The goitre is soft, diffuse and may become large enough to
cause discomfort. A colloid goitre is a late stage of diffuse hyperplasia when TSH stimulation has
fallen off and when many follicles are inactive and full of colloid
Nodular goitre
Nodules are usually multiple, forming a multinodular goitre. Nodules may be colloid or cellular, and
cystic degeneration and haemorrhage are common, as is subsequent calcification. All types of simple
goitre are more common infemales than males because of the presence of oestrogen receptors in
thyroid tissue.
Diagnosis
Diagnosis is usually straightforward. The patient is euthyroid, the nodules are palpable and often
visible (smooth, usually firm and not hard) and the goitre is painless and moves freely on swallowing.
Hardness and irregularity, due to calcification, may simulate carcinoma. A painful nodule or the
sudden appearance or rapid enlargement of a nodule raises suspicion of carcinoma; however, such
cases are usually due to haemorrhage into a simple nodule. Differential diagnosis from autoimmune
thyroiditis may be difficult and the two conditions frequently coexist.
4
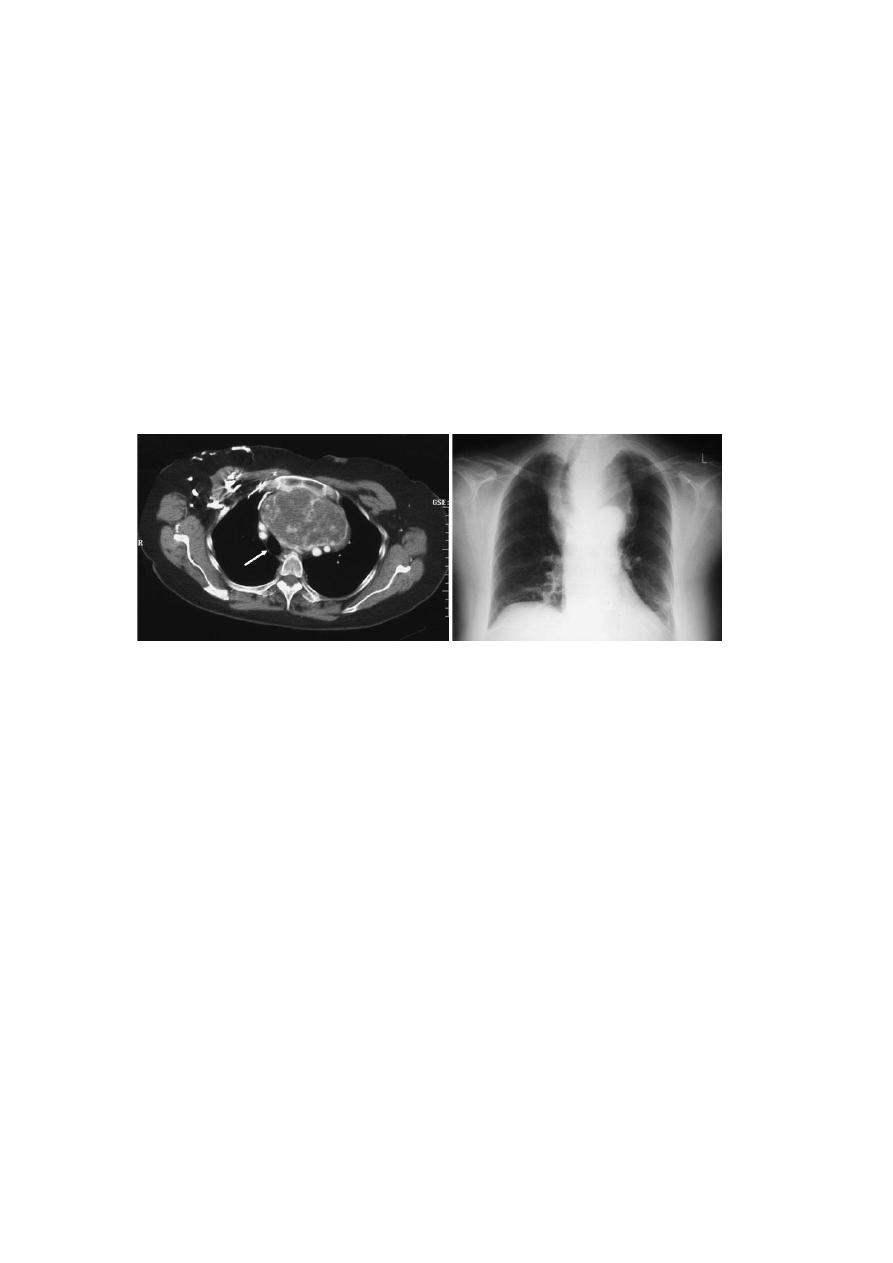
Investigations
Thyroid function should be assessed to exclude mild hyperthyroidism, and the presence of
circulating thyroid antibodies tested to differentiate from autoimmune thyroiditis. Plain radiographs
of the chest and thoracic inlet will rapidly demonstrate clinically significant tracheal deviation or
compression. Ultrasound and CT give more detailed images but rarely influence clinical
management. FNAC is only required for a dominant swelling in a generalised goitre.
Complications
Tracheal obstruction retrosternal extension of the goitre .
Acute respiratory obstruction may follow haemorrhage into a nodule impacted in the thoracic inlet.
Prevention and treatment of simple goitre
In endemic areas, the incidence of goitre has been strikingly reduced by the introduction of iodised
salt.
In the early stages a hyperplastic goitre may regress if thyroxine is given at a dose of 0.15–0.2 mg
daily for a few months.
Although the nodular stage of simple goitre is irreversible, more than half of benign nodules will
regress in size over 10 years. Most patients with multinodular goitre are asymptomatic and do not
require operation. Operation may be indicated on cosmetic grounds, for pressure symptoms or in
response to patient anxiety. Retrosternal extension with actual or incipient tracheal compression is
also an indication for operation, as is the presence of a dominant area of enlargement that may be
neoplastic. There is a choice of surgical treatment in multinodular goitre.
This includes total thyroidectomy, with immediate and lifelong replacement of thyroxine, or some
form of partial resection, to conserve sufficient functioning thyroid tissue to subserve normal
function while reducing the risk of hypoparathyroidism that accompanies total thyroidectomy.
Subtotal thyroidectomy involves partial resection of each lobe, removing the bulk of the gland and
leaving up to 8 g of relatively normal tissue in each remnant.

5
Clinically discrete swellings
Discrete thyroid swellings (thyroid nodules) are common and are three to four times more frequent
in women than men.
Diagnosis
A discrete swelling in an otherwise impalpable gland is termed isolated or solitary, whereas the
preferred term is dominant for a similar swelling in a gland with clinical evidence of generalised
abnormality in the form of a palpable contralateral lobe or generalised mild nodularity. About 70%
of discrete thyroid swellings are clinically isolated and about 30% are dominant.
The importance of discrete swellings lies in the increased risk of neoplasia compared with other
thyroid swellings. Some 15% of isolated swellings prove to be malignant, and an additional 30–40%
are follicular adenomas.
Investigation
Thyroid function
Serum TSH and thyroid hormone levels should be measured. Ifhyperthyroidism associated with a
discrete swelling is confirmed biochemically, it indicates either a ‘toxic adenoma’ or a manifestation
of toxic multinodular goitre. The combination of toxicity and nodularity is important and is an
indication for isotope scanning to localise the area(s) of hyperfunction.
Autoantibody titres
The autoantibody status may determine whether a swelling is a manifestation of chronic lymphocytic
thyroiditis. The presence of circulating antibodies may increase the risk of thyroid failure after
lobectomy.
Isotope scan
Isotope scanning used to be the mainstay of investigation of discrete thyroid swellings to determine
the functional activity relative to the surrounding gland according to isotope uptake. On scanning,
swellings are categorised as ‘hot’ (overactive), ‘warm’ (active) or ‘cold’ (underactive).
Ultrasonography
This was formerly widely used as a non-invasive supplement to clinical examination in determining
the physical characteristics of thyroid swellings.

6
Fine-needle aspiration cytology
FNAC is the investigation of choice in discrete thyroid swellings. FNAC has excellent patient
compliance, is simple and quick to perform in the out-patient department and is readily repeated.
Thyroid conditions that may be diagnosed by FNAC include colloid nodules , thyroiditis, papillary
carcinomamedullary carcinoma, anaplastic carcinoma and lymphoma. FNAC cannot distinguish
between a benign follicular adenoma and follicular carcinoma, as this distinction is dependent not
on cytology but on histological criteria, which include capsular and vascular invasion.
Radiology
Chest and thoracic inlet radiographs may confirm tracheal deviation, compression or retrosternal
extension and are required when either clinical suspicion or FNAC indicates malignancy.
Other scans
CT and MRI scans give excellent anatomical detail of thyroid swellings but have no role in the first
line of investigation. A PET scan may be useful, particularly in localising disease that does not take up
radioiodine.
Laryngoscopy
Flexible laryngosopy has rendered indirect laryngoscopy obsolete and is widely used preoperatively
to determine the mobility of the vocal cords, although usually for medico-legal rather than clinical
reasons. Nevertheless, the presence of a unilateral cord palsy coexisting with a swelling suggestive of
malignancy is usually diagnostic.
Core biopsy
Core biopsy gives a strip of tissue for histological rather than cytological assessment. It has a high
diagnostic accuracy but requires local anaesthesia and may be associated with complications such as
pain, bleeding and tracheal and recurrent laryngeal nerve damage.
Treatment
The main indication for operation is the risk of neoplasia.