
Community Dr. Zahraa A. Hassan
Influenza
Influenza is an acute infectious respiratory disease caused by RNA viruses of the family
orthomyxoviridae (the influenza viruses). The influenza virus, known to cause recurrent
epidemics and global pandemics.
CLINICAL FEATURES
:
1. Infection with influenza may be asymptomatic but usually gives rise to fever and typical
prostrating disease, characteristic in epidemics.
2. Usual symptoms are flushed face, congested conjunctivae, cough, sore throat, fever for two
to three days, headache, myalgia, back pains and marked weakness.
3. Pneumonia due to secondary bacterial infection is the most common complication.
4. Laboratory confirmation is made by recovery of virus from throat washings or by
demonstration of significant rise of influenza antibodies in the serum in acute and
convalescent stages of the disease or by direct identification of the virus in nasopharyngeal
cells.
EPIDEMIOLOGY
A large number of cases are either missed or are unreported because of their mildness.
Morbidity rate varies from 15 to 25 percent of the population exposed to risk in case of large
communities. The rate may be as high as 40 percent in case of closed populations.
Once an epidemic starts, its peak is reached in three to four weeks before declining.
CAUSATIVE AGENT
Influenza viruses are RNA viruses of orthomyxoviridae family. The virus has three distinct
genera (types A, B or C) based on antigenic differences of their nucleo and matrix proteins.
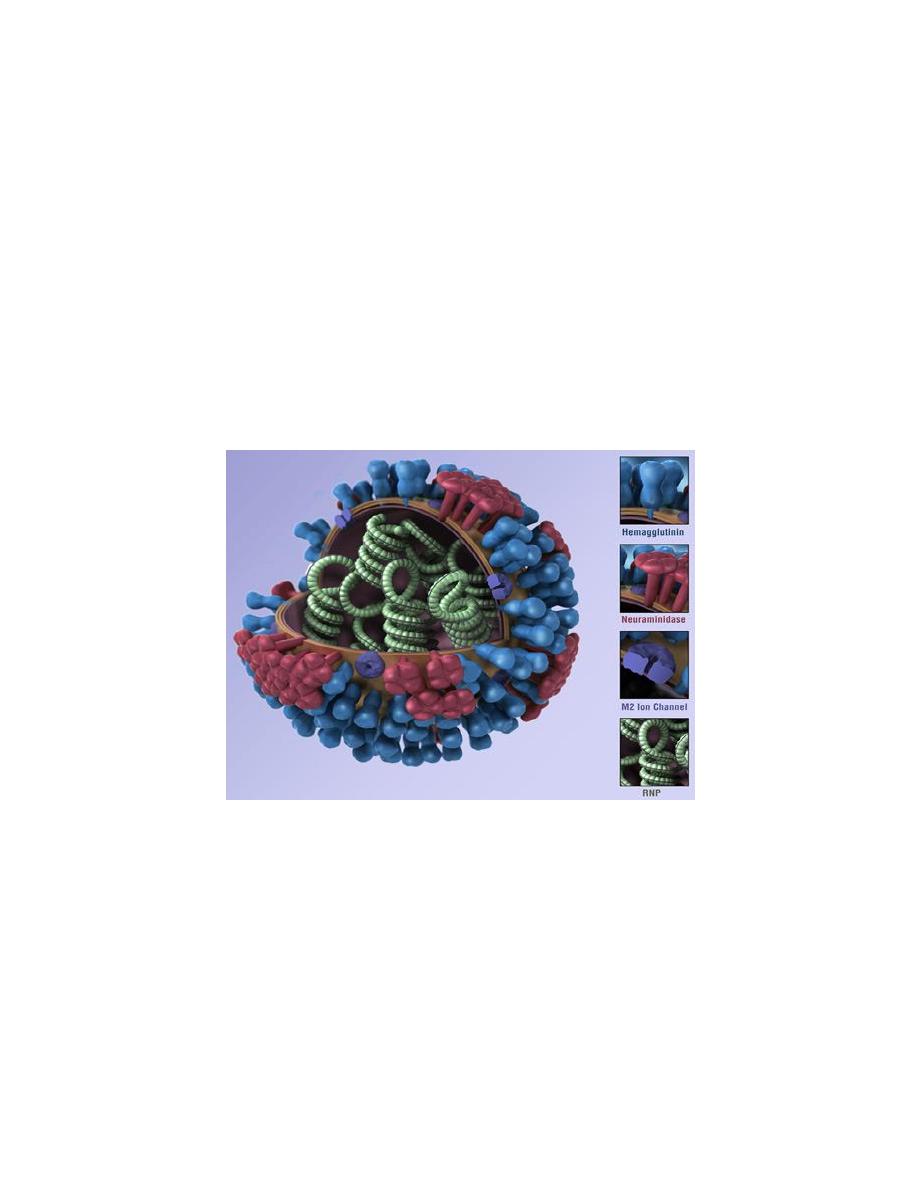
Influenza A viruses are divided into subtypes based on two proteins on the surface of the
virus: the hemagglutinin (H) and the neuraminidase (N). For example, an “H7N2 virus”
designates an influenza A subtype that has an HA 7 protein and an NA 2 protein. Similarly
an “H5N1” virus has an HA 5 protein and an NA 1 protein. There are 16 known HA subtypes
and 9 known NA subtypes. Many different combinations of HA and NA proteins are
possible. Only some influenza A subtypes (H1N1, H1N2, and H3N2) are currently in general
circulation among people.
Influenza type A viruses can infect people, birds, pigs, horses, and other animals, but wild
birds are the natural hosts for these viruses

Influenza B viruses: are not categorized into subtypes. Influenza B viruses can cause morbidity
and mortality among humans, but in general are associated with less severe epidemics than
influenza A viruses(they have not caused pandemics.)
Currently among many subtypes of viruses, influenza A (H1N1) viruses, influenza A (H3N2)
viruses, and influenza B viruses are circulating worldwide in human.
Influenza Type C: Influenza type C viruses cause mild illness in humans and do not cause
epidemics or pandemics. These viruses are not classified according to subtype.
CHANGING NATURE OF VIRUS
New influenza virus strain may evolve due to point mutation or by genetic reassortment.
Two type of antigenic change may occur in the virus namely antigenic drift and shift
Minor changes in the hemagglutinin and/or neuraminidase antigens on the surface of the
virus which results from point mutation during viral replication is called antigenic drift.
Antigenic drift occurs in both Influenza A and B viruses. Influenza B viruses undergo
antigenic drift less rapidly than influenza A viruses.
Antigenic drift refers to small, gradual changes that occur through point mutations in the
two genes that contain the genetic material to produce the main surface proteins,
hemagglutinin, and neuraminidase.
These point mutations occur unpredictably and result in minor changes to these surface
proteins. Antigenic drift produces new virus strains that may not be recognized by
antibodies to earlier influenza strains.
This process works as follows: a person infected with a particular influenza virus strain
develops antibody against that strain. As newer virus strains appear, the antibodies against
the older strains might not recognize the "newer" virus, and infection with a new strain can
occur.
Antigenic drift explains why a person can be infected by Influenza A viruses several times
and also why Influenza vaccine need to be updated every year.
Antigenic shift refers to an abrupt, major change to produce a novel influenza A virus
subtype in humans that was not currently circulating among people Antigenic shift can
occur either through direct animal to human transmission or through mixing of human
influenza A and animal influenza A virus genes to create a new human influenza.
A subtype virus through a process called genetic reassortment. Antigenic shift results in a
new human influenza A subtype.
Antigenic shift is noted only with type A influenza virus.
CHARACTERISTICS OF INFLUENZA PANDEMICS
1. Occurrence outside the usual season.
2. Extremely rapid transmission with concurrent
outbreaks throughout the globe.
3. High attack rates in all age groups with high mortality rates even in young adults.

Epidemics are primarily caused by type A viruses and occasionally by type B in human being.
Type C influenza virus has been associated with sporadic cases and minor localized outbreaks.
Avian influenza viruses (AIV) belong to type A influenza virus.
HOST FACTORS
Age and sex: the influenza virus maximally attacks those in the age group 5 to 15 years but no
age group or sex is spared. Rates of infection are highest among children, but death and
serious illness are common amongst persons aged 65 years, children below two years and
persons of any age with associated medical conditions that place them at increased risk for
complications from influenza.
Immunity: Antibody against one influenza virus type or subtype confers limited or no
protection against another type or subtype of influenza.
Frequent development of antigenic variants through antigenic drift is the virologic basis for
seasonal epidemics and the reason for the usual incorporation of one or more new strains in
each year’s influenza vaccine.
Antibodies appear in about seven days after an attack and peak in the blood by two weeks.
The level drops to pre infection level by 8 to 12 months.
MODE OF TRANSMISSION
A. Influenza viruses predominantly transmitted through respiratory droplets of coughs and
sneezes from an infected person.
B. Influenza viruses may also spread through direct (skin to skin) or indirect contact with
infected material, which ultimately enters through nasopharyngeal route. Transmission of
viruses starts one day before the onset of symptoms and continue up to five to seven days
after the symptoms subsides.
C. Transmission is possible from asymptomatic carriers. Children may pass the virus for longer
than seven days. Influenza viruses can be inactivated by sunlight, disinfectants and
detergents easily. Frequent hand washing reduces the risk of infection.
CONTROL OF INFLUENZA
Influenza vaccination is the key strategy for the prevention of influenza during the inter
pandemic periods and a pillar of pandemic preparedness. Antiviral drugs can only be used as
an adjunct.
Route and dose:
Inactivated influenza vaccines are given via the intramuscular route in the deltoid muscle,
except in infants where the recommended site is the antero-lateral aspect of the thigh.
A single dose of inactivated vaccine annually is appropriate, The usual dose is 0.5 ml except in
case of children, where the dose should be half. Seroprotection is usually obtained within two
to three weeks and the post-vaccination immunity lasts for about 6 to 12 months.

WHO RECOMMENDS THE FOLLOWING PRIORITY CASES FOR VACCINATION
Elderly individuals suffering from chronic conditions such as Pulmonary or Cardiovascular
disease, metabolic illness including diabetes mellitus and renal dysfunction,
Various types of immunosuppression including persons with AIDS and transplant recipients.
Health care persons in regular and frequent contact with high risk persons.
Household contacts of high-risk persons including elderly and the disabled.
Pregnant women who will be in their second or third trimester by the start of the influenza
season.
When adequate vaccine supplies are available,vaccination of general public may be
considered.
Prevention and control strategies:
People with respiratory infection symptoms should practice the following respiratory
protection . All symptomatic people should:
1. Avoid close contact (less than 1 meter) with
other people.
2. Cover their nose and mouth when coughing or sneezing.
3. Use disposable tissues to contain respiratory secretions.
4. Immediately dispose off used tissues.
Treatment:
1) Antibiotics for bacterial complications of influenza.
2) Antiviral therapy.
3) Management of contacts may include-antiviral prophylaxis and advice about relevant
vaccination.
Avian Influenza A Virus Infections in Humans
Although avian influenza A viruses usually do not infect humans, rare cases of human
infection with avian influenza A viruses have been reported. Most human infections with
avian influenza A viruses have occurred following direct or close contact with infected
poultry. Illness in humans has ranged from mild to severe.
The spread of avian influenza A viruses from one ill person to another has been reported
very rarely. However, because avian influenza A viruses have the potential to change and
gain the ability to spread easily between people, monitoring for human infection and
person-to-person transmission is extremely important for public health.
Swine Influenza
Swine flu viruses do not normally infect humans. However, sporadic human infections with
influenza viruses that normally circulate in swine and not people have occurred. When this
happens, these viruses are called “variant viruses.
Most commonly, human infections with variant viruses occur in people with exposure to
infected pigs ( children near pigs at a fair or workers in the swine industry). There have
been documented cases of multiple people becoming sick after exposure to one or more
infected pigs and also cases of limited spread of variant influenza viruses from person-to-
person.
The vast majority of human infections with variant influenza viruses do not result in person-
to-person spread. However, each case of human infection with a swine influenza virus
should be fully investigated to be sure that such viruses are not spreading in an efficient
and ongoing way in humans and to limit further exposure of humans to infected animals if
infected animals are identified