1
Medicine Dr.Sabah
1- ACUTE RHEUMATIC FEVER
Incidence:
o children (most commonly between 5 and 15 years) or young adults.
o Very rare in Western Europe and North America,
o Endemic in parts of Asia, Africa and S. America,
o Annual incidence in some countries > 100 per 100 000
o Most common cause of acquired heart disease in childhood and adolescence.
Pathogenesis
Immune-mediated –delayed response to infection with specific strains of group A streptococci that
possess antigens which may cross-react with cardiac myosin and sarcolemmal membrane protein.
Antibodies against the streptococcal antigens mediate inflammation in the endocardium,
myocardium and pericardium as well as joints and skin.
Histologically:
1- fibrinoid degeneration = collagen of connective tissues.
2- Aschoff nodules =pathognomonic and occur only in the heart. They are composed of
multinucleated giant cells surrounded by macrophages and T lymphocytes, and not seen until
subacute or chronic phases of rheumatic carditis
2
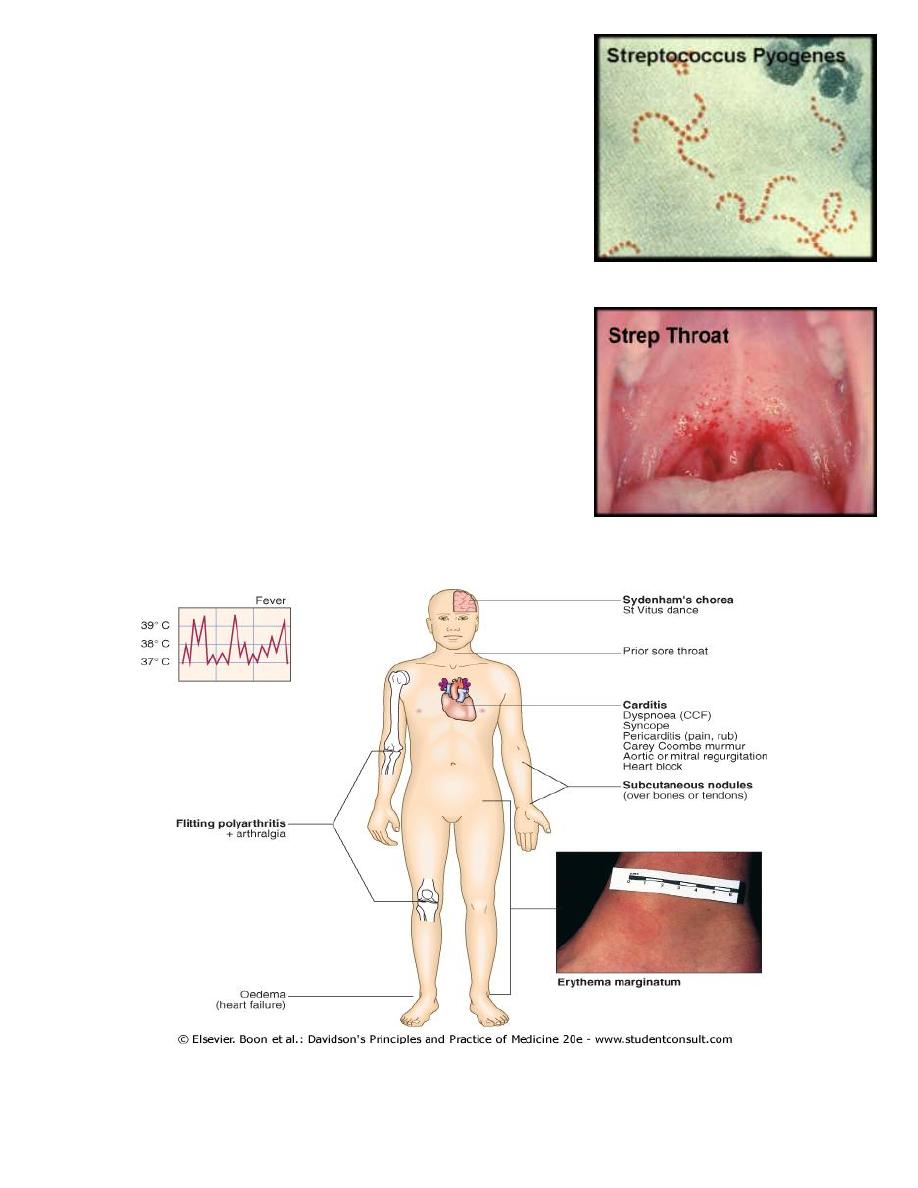
Streptoccoci
Beta-hemolytic- group A st.pyogenous(pharyn
group B st.agalactiae(neonate
group C st.equi(cellulitis)
Alpha-hemolytic- viridence
Gamma-hemolytic group D enterococci &non-enter
Anerobic st. -pneumonia
Clinical features
Multisystem disorder typically follows an episode of
streptococcal pharyngitis presents with Fever/
anorexia/lethargy / joint pains.
Symptoms characteristically occur 2-3 weeks after the initial
attack of pharyngitis no history of sore throat.
Arthritis 75%
Other feature rashes, carditis neurological changes .
Other systemic manifestations = rare= pleurisy, pleural effusion
and pneumonia

3
1- Carditis مهم
Pericardium=
exudative pericarditisfibrosis and obliteration
rarely constrictive
Myocardium=
lymph.infiltration,necrosis, Aschoff nodules
Endocardium=
valvulitis,cellular infiltrate and fibrin.new insufficiency murmers
.
AS and MS donot
occur for many years(progression of fibre
Pancarditis
= endocardium, myocardium and pericardium
incidence declines with increasing age- 90% at 3 years to 30% in adolescence.
Manifestations
breathlessness (heart failure or pericardial effusion),
palpitations or chest pain (pericarditis or pancarditis).
tachycardia
cardiac enlargement
new or changed cardiac murmurs.
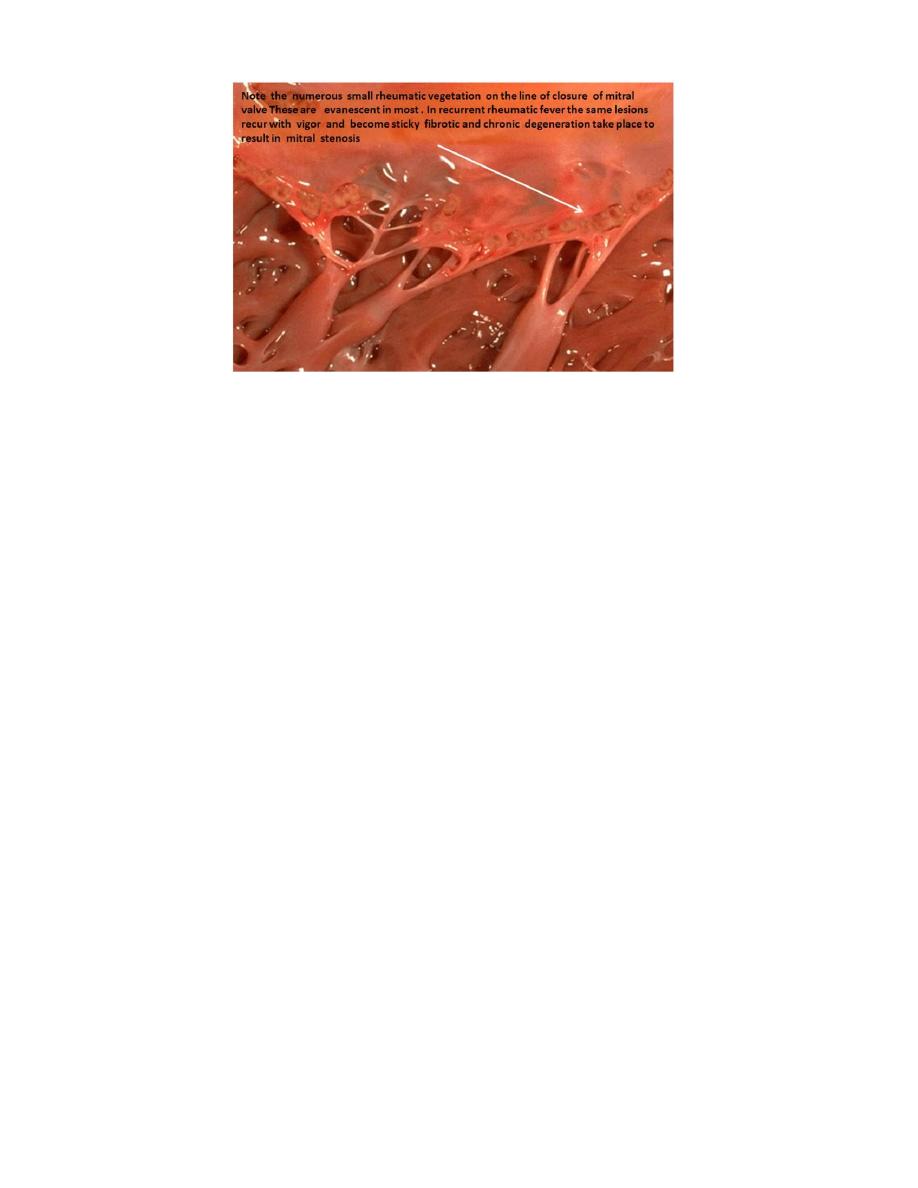
1- soft systolic murmur due to mitral regurgitation very common.
2- soft mid-diastolic murmur (the Carey Coombs murmur)=due to valvulitis, with nodules
forming on the mitral valve leaflets.
3- Aortic regurgitation = 50% of cases but tricuspid and pulmonary valves are rarely involved
acute process.
Pericarditis = chest pain, P. friction rub and precordial tenderness.
Cardiac failure = myocardial dysfunction and/or mitral or aortic regurgitation.
ECG changes =commonly include ST and T wave changes; conduction defects sometime occure
and may cause syncope.
2- Arthritis
most common major manifestation and tend early feature / tends to occur when str. AB titres are
high.
Acute, painful, asymmetric and migratory inflammation of the large joints (typically the knees,
ankles, elbows and wrists).
joints : involved in quick succession usually red, swollen and tender for a day and up to 4 weeks.
The pain characteristically responds to aspirin; if it does not, the diagnosis is in doubt.
4
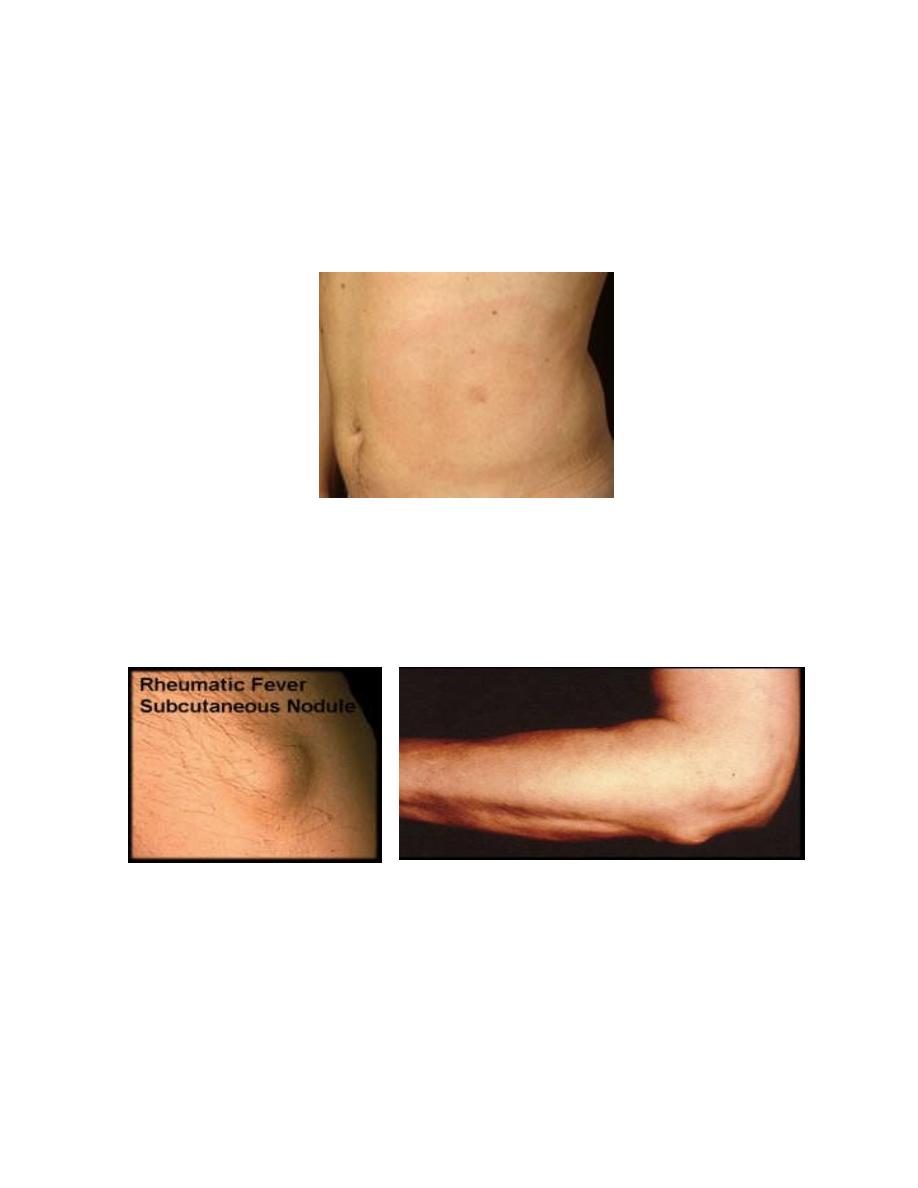
Skin lesions= 3-Erythema marginatum 4-Subcutaneous nodules
3- Erythema marginatum
occurs in < 5% of patients.
lesions start as red macules (blotches) which fade in the centre but remain red at the edges and
occur mainly on the trunk and proximal extremities but not the face. The resulting red rings or
'margins' may coalesce or overlap .
4- Subcutaneous nodules
Occur in 5-7% of patients.
Small (0.5-2.0 cm), firm and painless, and are best felt over extensor surfaces of bone or tendons.
Nodules typically appear more than 3 weeks after the onset of other manifestations a feature
helps to confirm rather than make the diagnosis.
5- Sydenham's chorea (St Vitus dance)
late neurological manifestation typically appears at least 3 months after the episode of ARF
(when all the other signs may have disappeared).
Occurs in up to 1/3 of cases , more common in females.
Emotional lability may be the first feature followed by purposeless involuntary choreiform
movements of the hands, feet or face.
Speech may be explosive and halting.
Spontaneous recovery usually occurs within a few months.
Approximately one-quarter of patients =develop chronic rheumatic valve disease
5
Investigations
ESR and CRP: non-specific markers of systemic inflammation, and are useful for monitoring
progress of the disease.
throat swab: Positive cultures are obtained in only 10-25% of cases of ARF.
ASO titres: are normal in about one-fifth of adult cases of rheumatic fever and most cases of
chorea.
Echocardiography: typically shows mitral regurgitation with dilatation of the mitral annulus and
prolapse of the anterior mitral leaflet; other common findings are aortic regurgitation and
pericardial effusion.
INVESTIGATIONS IN ACUTE RHEUMATIC FEVER
Evidence of a systemic illness (non-specific): Leucocytosis, raised ESR, raised CRP
Evidence of preceding streptococcal infection (specific)
- Throat swab culture: group A β-haemolytic streptococci (also from family members and
contacts)
- Antistreptolysin 0 antibodies (ASO titres): rising titres, or levels of > 200 U (adults) or > 300 U
(children)
Evidence of carditis
- Chest X-ray: cardiomegaly; pulmonary congestion
- ECG: first- and rarely second-degree heart block; features of pericarditis; T-wave inversion;
reduction in QRS voltages
- Echocardiography: cardiac dilatation and valve abnormalities
DIAGNOSIS
According to revised Jones criteria =based upon
1) DEFINTE= two or more major manifestations, or one major and two or more minor
manifestations;
PLUS evidence of preceding streptococcal infection .
1- positive culture(25% +VE for group A streptococcus at the time of diagnosis { latent period
between infection and presentation}
2- serological evidence of recent streptococcal infection with a raised antistreptolysin O (ASO)
antibody titre
2) PRESUMPTIVE= without evidence of preceding streptococcal infection cases of isolated chorea or
pancarditis,( other causes excluded).
3) In cases of established rheumatic heart disease or prior ARF diagnosis of ARF = based only on the
presence of
a. multiple minor criteria and
b. evidence of preceding group A streptococcal pharyngitis.
6
JONES CRITERIA FOR THE DIAGNOSIS OF RHEUMATIC FEVER
Major manifestations
1. Carditis
2. Polyarthritis
3. Chorea
4. Erythema marginatum
5. Subcutaneous nodules
Minor manifestations
1- Fever
2- Arthralgia
3- Previous rheumatic fever
4- Raised ESR or CRP
5- Leucocytosis
6- First-degree AV block
PLUS:
Supporting evidence of preceding streptococcal
infection: recent scarlet fever, raised antistreptolysin 0 or
other streptococcal antibody titre, positive throat culture
Treatment of the acute attack:
1- Antibiotics
2- Bed rest and supportive therapy
3- Aspirin and Steroids
ANTIBIOTICS:
single dose of benzyl penicillin 1.2 million U i.m. or oral phenoxymethylpenicillin 250 mg
6-hourly for 10 days (to eliminate any residual streptococcal infection).
If the patient is Penicillin allergic, erythromycin or a cephalosporin can be used. Treatment is then
directed toward limiting cardiac damage and relieving symptoms.
Bed rest and supportive therapy
Bed rest lessens joint pain and reduces cardiac workload.
Duration of bed rest should be guided by symptoms and markers of inflammation (e.g.
temperature, leucocyte count and ESR) and should be continued until these have settled.
Patients can then return to normal physical activity but strenuous exercise =avoided in those who
have had carditis.
Cardiac failure
- fulminant form =particularly those in early adolescence, =>severe mitral regurgitation and
sometimes concomitant aortic regurgitation.
- If HF does not respond to medical treatment =>valve replacement may be necessary often
associated with a dramatic decline in rheumatic activity.
Atrioventricular block is seldom progressive and pacemaker insertion is rarely needed.

7
Aspirin
This will usually relieve the symptoms of arthritis rapidly and prompt response (within 24 hours) help
to confirm the diagnosis. A reasonable starting dose is 60 mg/kg body weight per day divided into six
doses. In adults, 100 mg/kg per day may be needed up to the limits of tolerance or a maximum of 8 g
per day. Mild toxic effects include nausea, tinnitus and deafness; more serious = vomiting, tachypnoea
and acidosis. Aspirin should be continued until the ESR has fallen and gradually tailed off.
Corticosteroids
These produce more rapid symptomatic relief than aspirin and are indicated in cases with carditis or
severe arthritis. These is no evidence that long-term steroids are beneficial. Prednisolone, 1.0-2.0
mg/kg per day in divided doses, should be continued until the ESR is normal then tailed off
Secondary prevention
Patients susceptible to additional attacks of FR if further streptococcal infection occurs, long-term
prophylaxis with penicillin -as benzyl penicillin 1.2 million U i.m. monthly or oral
phenoxymethylpenicillin 250 mg 12-hourly.
Sulfadiazine or erythromycin used if the patient is allergic to penicillin; sulfadiaine prevent the
infection but are not effective in the eradication of group A streptococci.
Further attacks of rheumatic fever are unusual after the age of 21 at which age treatment may be
stopped. However it should be extended if an attack has occurred in the last 5 years, or the patient
lives in an area of high prevalence or has an occupation (e.g. teaching) with high exposure to
streptococcal infection.
In those with residual heart disease, prophylaxis should continue until 10 years after the last
episode or 40 years of age, whichever is longer.
Long-term antibiotic prophylaxis prevents another attack of ARF but does not protect against
infective endocarditis.
2-CHRONIC RHEUMATIC HEART DISEASE
Chronic valvular heart disease develops in at least half of those affected by rheumatic fever with
carditis.
Two-thirds of cases occur in women.
Some episodes of rheumatic fever may pass unrecognised only possible to elicit a history of
rheumatic fever or chorea in about half of all patients with chronic rheumatic heart disease.
The mitral valve is affected in more than 90% of cases;the aortic valve is the next most frequently
affected, followed by the tricuspid and then the pulmonary valve.
Isolated MS accounts for 25% of all cases of rheumatic heart disease, 40% have mixed mitral
stenosis and regurgitation.
Valve disease may be symptomatic during fulminant forms of ARF, but may remain asymptomatic
for many years
8
Pathology
ARF =destructive lytic process main pathological process in chronic rheumatic heart disease is
progressive fibrosis.
1- heart valves are predominantly affected
2- pericardium and myocardium may contribute to heart failure and conduction disorders.
Fusion of the mitral valve commissures and shortening of the chordae tendineae = mitral stenosis
with or without regurgitation.
Similar changes in the aortic and tricuspid valves produce distortion and rigidity of the cusps
leading to stenosis and/or regurgitation.
Once a valve has been damaged the altered haemodynamic stresses perpetuate and extend the
damage, even in the absence of a continuing rheumatic process.