Dr.Emad Colostomy & appendicular mass
Sunday, August 14, 2016
1
-Mesentric ischemia (CVS+abd. Pain) --------clinically in early hours he presented with soft
abd.(out of proportion of clinical Ex.)- severe pain but abdomen is soft
و بذلك يختلف عن ال
peritonitis
Types of adhesion
–
1. Post op. fibrinous adhesion (easy) bet. 3-6 post op unlikely cause complete obst.
Disappear completely after months
2. Post op. fibrous adhesion (difficult) it’s a strong band occur in area deficient of blood
supply & become adherent to omentum or parietal peritoneum to gain blood supply cause
obst. At any time
3. Adhesion of loop of bowel to an inflamed intra peritoneal structure →TB mesenteric LN
4. Follow chemical irritation → talk
-obstructed H. is unlikely to last >12 day
-Causes of absolute
constipation?
1_ colon cancer
2_ volvuluses
CNS causes of constipation
-
1. autonomic neuropathy
2.paraplegia
3.stroke
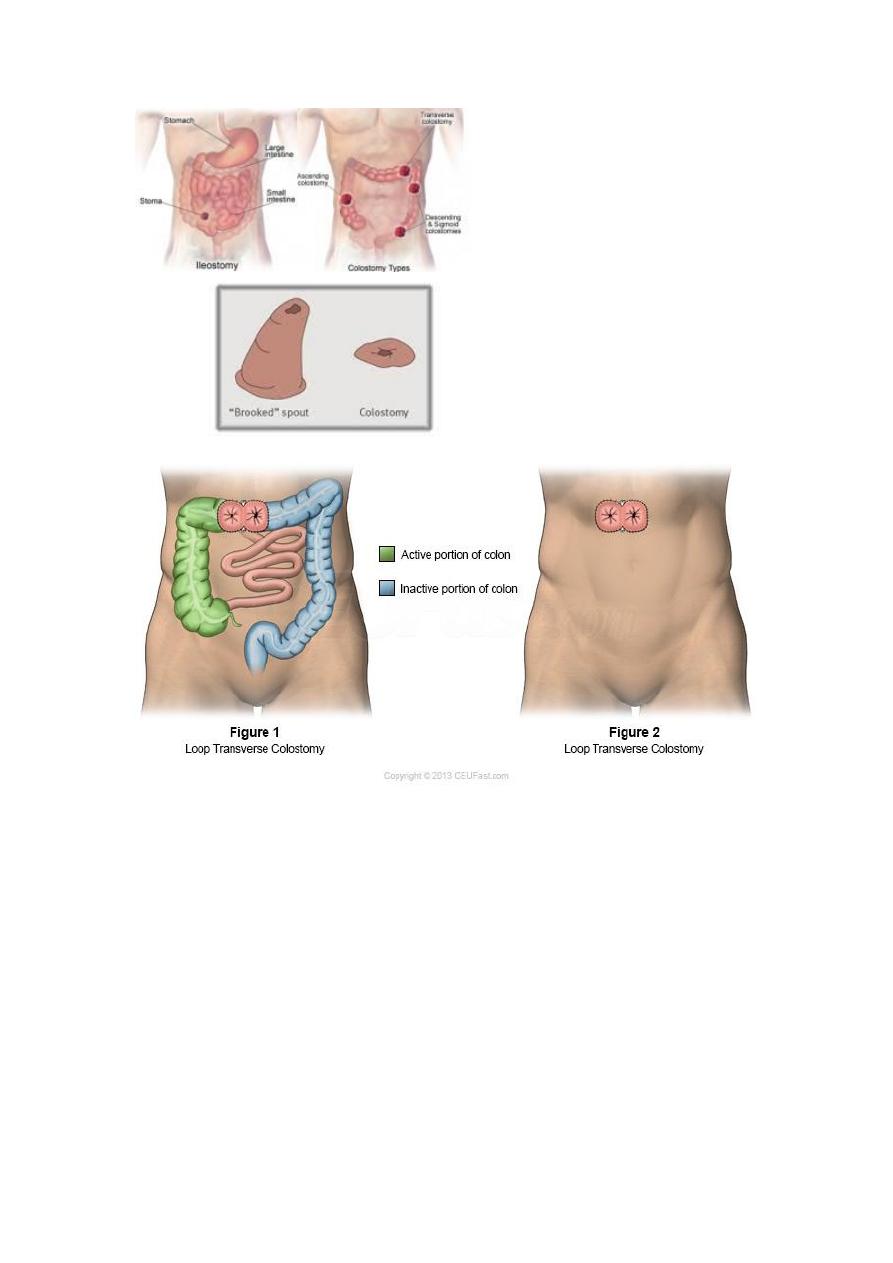
Colostomy (Stoma )-----In remix Page 5--- Go to
https://www.muhadharaty.com/lecture/
- ileostomy ---done in Rt side
-Types of ileostomy---loop(Temporary)
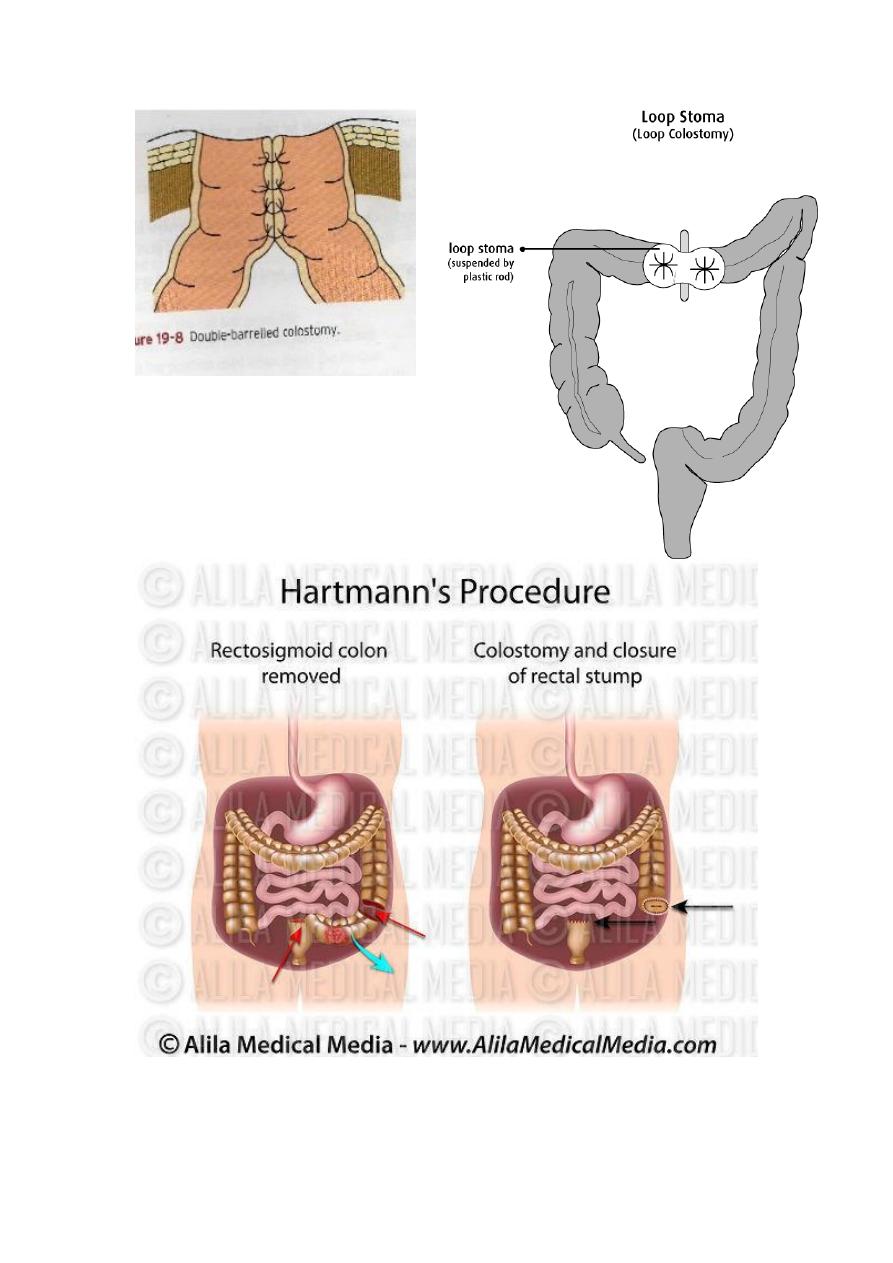
-----End (permanent) ---Hartman procedure
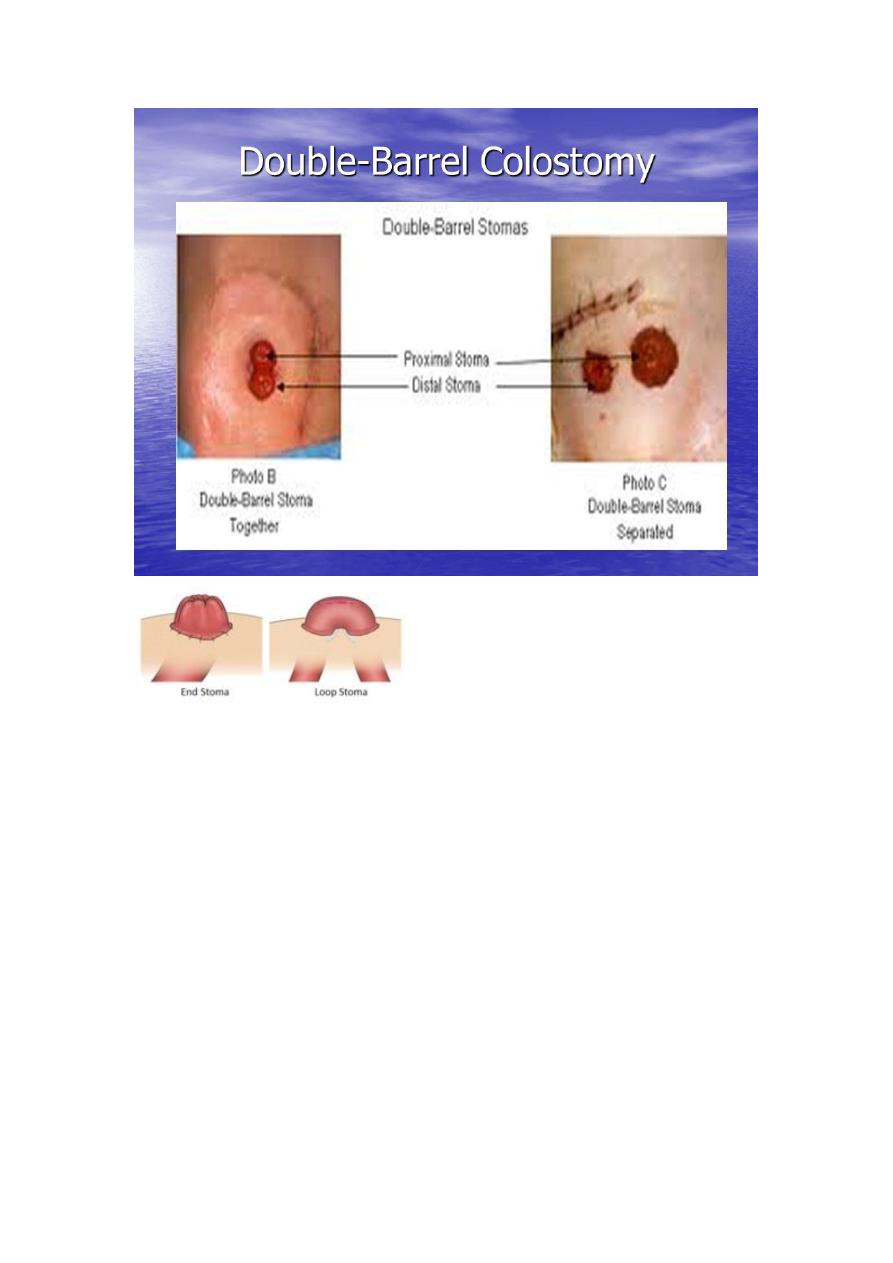
-Types of colostomy ----Loop &End & Double barrel(to make the closure easier )
-How to differentiate the colostomy &ileostomy in the Ex.
-How to differentiate loop & double
1-site: Left side : mostly colostomy.
2-content &color
#after opening –incision
causes of constipation
1.past surgical Hx
Adhesions
Recurrence of CA colon
Recurrence of volvolus
2.Drug Hx
Anticholinergics
TCA
Narcotic.… .morphine
Long Hx of laxative use
Dr.Emad Colostomy & appendicular mass
Sunday, August 14, 2016
2
--Diameter: ; small is mostly ileostomy.
--Elevation :ileostomy –spouted out
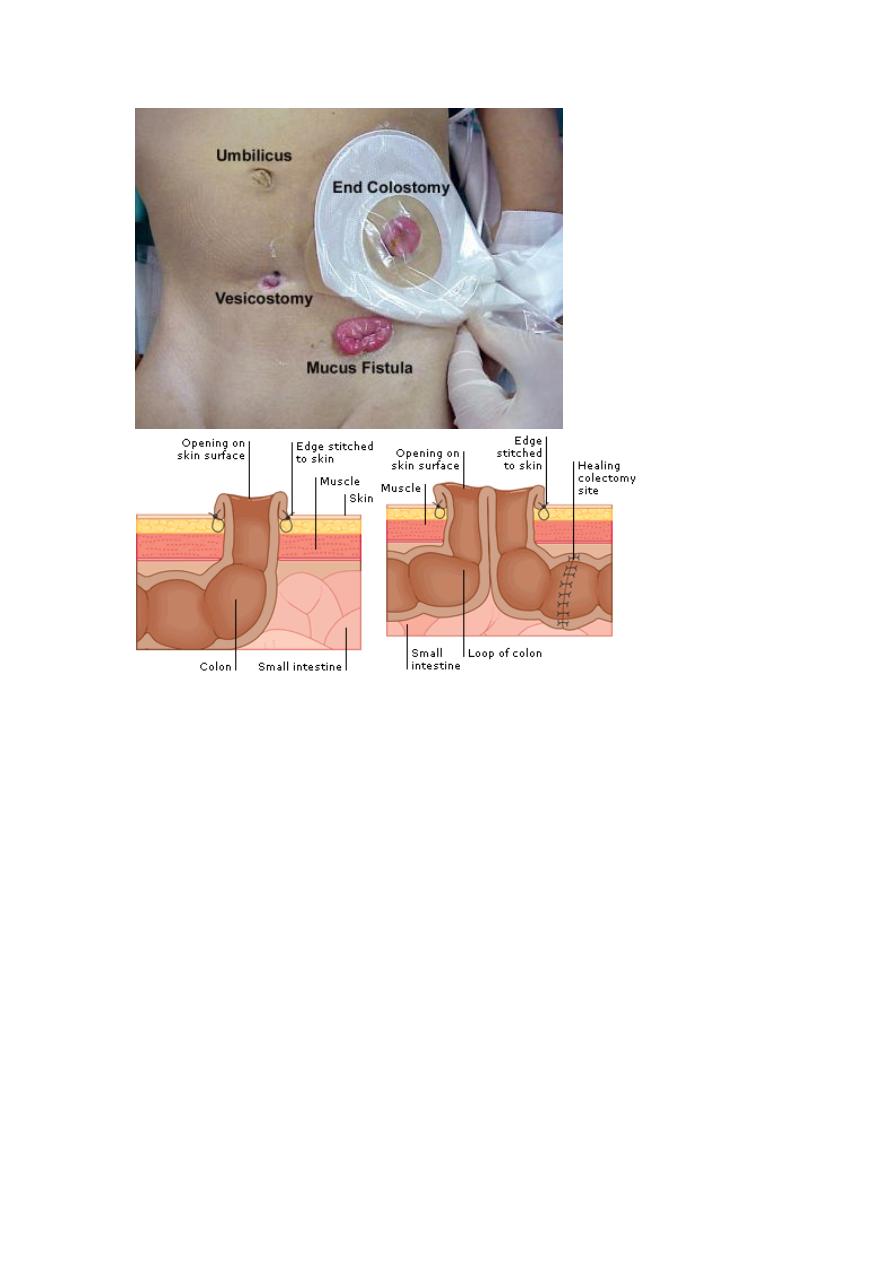
-no. of opening
#in early post.op for colostomy U can differentiate B/t loop & double
-by elastic bar that is found in early (2 days)loop colostomy
#sometimes we found two stoma
1-proximal ---end colostomy
2-Distal –mucosa fistula –to make closure easier
-complication of colostomy
1-skin excoriation –more in ileostomy
2-obstruction –technical-early
--stenosis-late
3-retraction ---how to manage it ??
4-ischemia –gangrene-bz of tension or twisting
5-parastomal H.
-Preparation for colonic surgery
1_npo
2_ laxative oral or enema
3_see the patient fit for surgery or not by observation the Distal end is patent or not and this
done by barium enema
Post operative care of colostomy closure
1. NBM
2.NGT for feeding ( 3-5 ) days
3. Antibiotic
4. Monitor of patient if he has fever and tachycardia he may has leakage from
anastomosis
Dr.Emad Colostomy & appendicular mass
Sunday, August 14, 2016
3
Appendicular mass
paediatric age male with RIF swelling
D.DX
Abscess
Ectopic pelvic kidney
Haematoma if there is injury
RIF hernia>>spegilian hernia and paraumbilical H.
TB
Crohn`s disease
Lymphoma
IF it is abscess there will be presence of constitutional symptoms like fever, tachy cardia,
anorexia
We treat abscess by two ways which are either by PercutNous drainage under U/S or CT
guide
or by retroperitoneal drainage
**Most important D.DX of appendicular mass is ectopic kidney therefore we should ask
about urinary symptoms and the duration of mass
Management of appendicular mass in remix page ( 91- 92 )
**** Mx. Of appenducular mass *Clinical features;
Pain
Anorexia
Fever
No bowel motion
* Invx. Us
CBC, (lukucytosis )
Electrolyte.
* Treatment
Admission
NPO
IV fluid
Antibiotics
Marker to mass size and follow up for 5 days , if it's size decrease then treat
conservatively until symptoms improve and no need to elective appendectomy.
Dr.Emad Colostomy & appendicular mass
Sunday, August 14, 2016
4
Dr.Emad Colostomy & appendicular mass
Sunday, August 14, 2016
5
Dr.Emad Colostomy & appendicular mass
Sunday, August 14, 2016
6
Dr.Emad Colostomy & appendicular mass
Sunday, August 14, 2016
7
Done by :group A Active