1
Lec.1
Pediatrics
6
th
stage
Wednesday 17-8-2016
Session notes
د.رنا
How you approach to examine a pt with neurologic problem?
Start from the head , 1-hair texture :-shiny brittle hair easily broken in
FTT, sparse with coarse facies in hypothyroidism.
2-fontanelles:-examine the pt in semi-sitting position (45 degrees) ,avoid
supine position as this will depress the fontanelle
While sitting position will buldge the fontanelle so also avoid it.
DDx of delayed closure of fontanelle?
1)ricket
2)hydrocphalus
3)osteogenesis imperfect
4)metabolic disease
5)hypothyroidism.
*******************************
3-eye :-nystagmus,squint,upright slanting (as in Down syndrome).
Eyelashes & eyebrows if thick as in CP
4-nose :-shape of nose ,saddle nose in syphilis/ Hypertelorism.
5-mouth:-dental caries , state of hydration, tongue size .
**protruded tongue but not microglossic tongue in down syndrome.
6-Neck swelling in midline for goiter.
7-Hand:-fingers & hand creases.
2
8-foot ,legs for peripheral edema ,sandle gap in down syndrome.
9-peripheral pulses
10-LAP
11-vital signs
12-growth parameters.
-
Growth parameters :
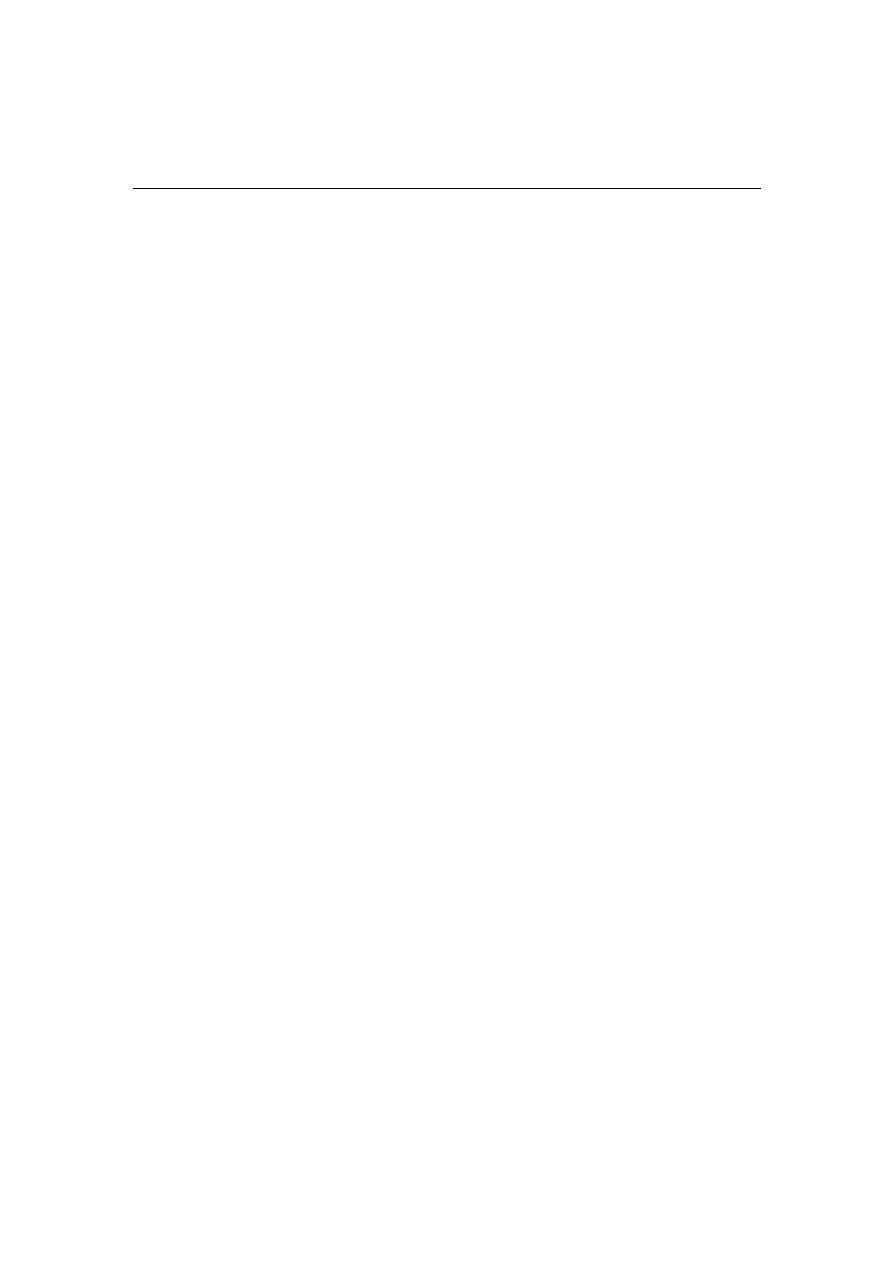
Head circumference :-
3times attempts & take the highest.
Normal ranges:-
At 1
st
(3)moincreased by 2cm
At 2
nd
(3)moincreased by 1cm.
At (6)mo &later on1/2cm
After 1yr 1cm/yr.
3
The increment stops when we stop growth.
LENGTH
Till 2yrs we use the term (length).
Then after use the term(height).
BP
Start to be measured at(3)yrs &later but with indications.
i
Cvs
ii
Renal problem
iii
Umbilical problem
**Use Who chart for BP
In child with convulsion
CNS exam :-
1)general look for
1-nutrition,well or sick?conscious ?alert?oriented?
2-gait
3-posture
4-any deformity
5-any abnormal movement
6-tremor
7-any scar over legs

4
8-wasting ,hypertrophy
9-irritability
2)Tone exam
3) Power exam
4) reflexes
5)coordination(Heel shin test,finger nose test).
**speech(dysarthria),nystagmus,dysdiadichokinesia.
In ER , how do you treat pt with convulsion?
ABC-put pt in recovery position(lateral position) /airway in mouth
for avoiding tongue biting/suctioning of mouth.
Diazepam IV/rectally very slowly with O2.
--(ampoule contain 10mg/2cc),we give (1) mg for each (3)kg or (4)kg.
--Every( 1)cc =(5)mg.
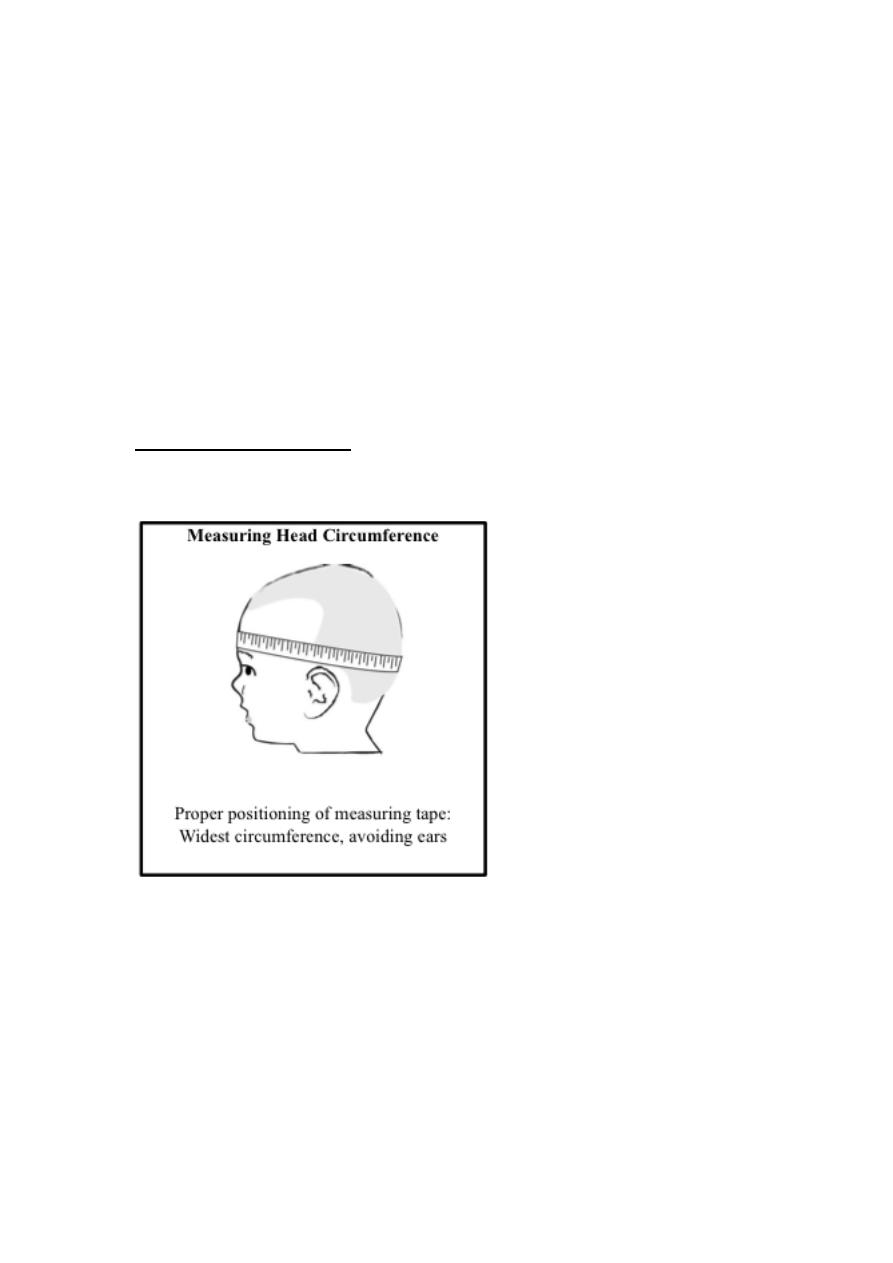
--We use insulin syringe
--It is graduated into (100) ,, divide 100 by (5) =(20)units in insulin
syringe =(1)mg.
Fill the syringe fully with D.W.
تخفيف
--
--Give it over(7)min to (10) min (very slowly).
--Wait for (20) min for response
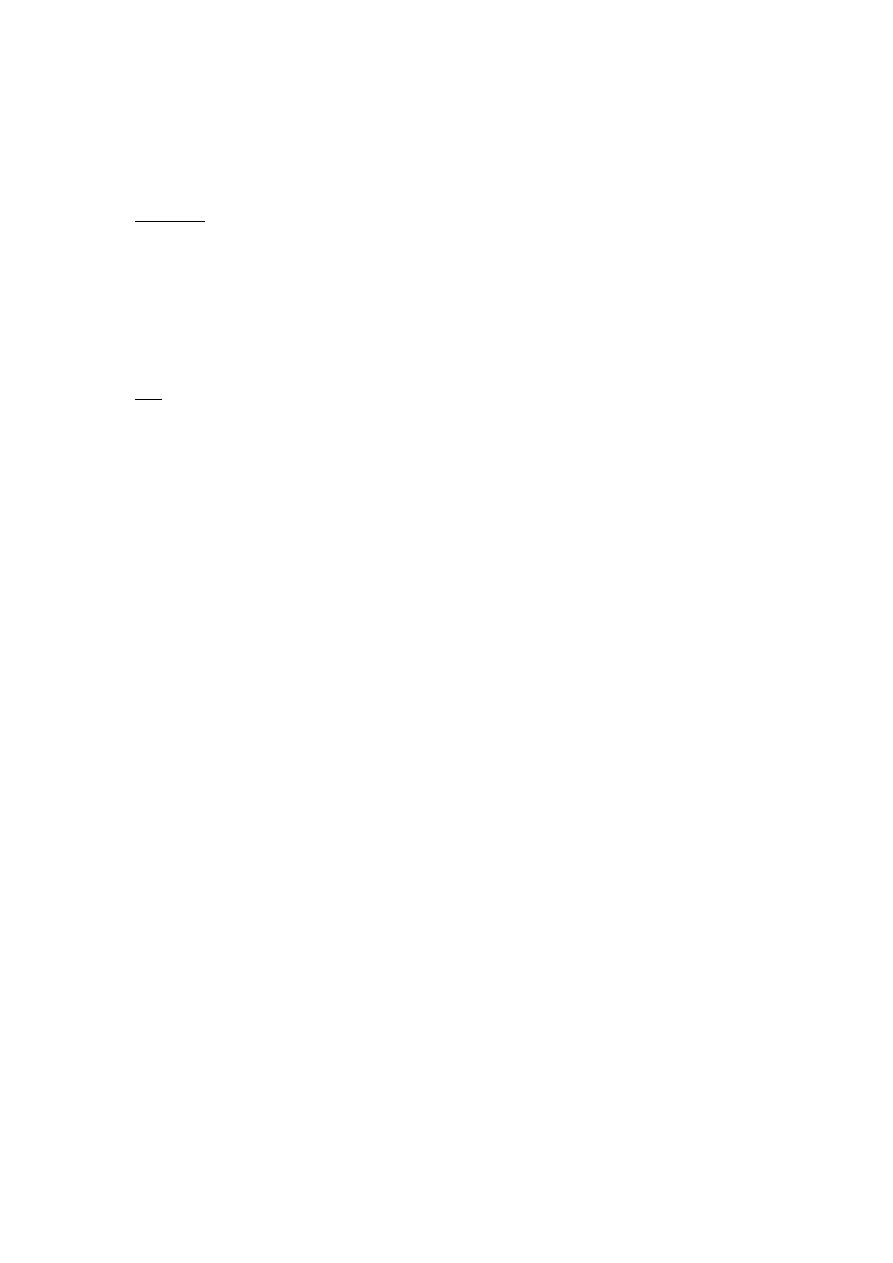
--the microdrip is used for dilution & to control the speed of infusion)in
pediatric age group to avoid overload.
--In microdrip ,each(1)ml gives(15)drops.
5
If NO RESPONSE
Give 20mg/kg luminal (luminal in ampoul is "200"mg/kg) then wait
( 20)min, NO RESPONSE increase the dose by 5 ,then 10 min
afterincrease by 5 ,till you reach to 40 no response give
both diazepam + Phenobarbital.
If you prescribe AED allow pt to take them for 2yrs if no
response then change.
Case of Epilepsy
C.C
:-abnormal involuntary body movement for 10 days duration.
H.P.I:-
(9mo) old baby ,known case of epilepsy on treatment, his condition
started as continuous fever , for (2)days duration not associated with
sweating or rigor ,then suddenly abnormal involuntary body movement
for (10)min duration occured with generalized ,spastic posturing
It was Associated with salivation & bluish discoloration of mouth ,not
passed motion or urine,aggravated by fever with no Hx of trauma ,the pt
immediately was brought to hospital after admission &receiving Rx ,he
had developed vomiting & FBM ,(6)times/day,watery in nature ,no blood
or muscus in stool ,convulsion attacks continued at hospital although Rx
is continuous
6
Electrolytes & blood sugar with GUE were performed ,MRI has been
given as appointment but has NOT been done till now,
Diazepam was given on admission,the pt was on Phenobarbital then
converted to sodium valproate before (2)mo.
Review of system:-nothing significant.
Prenatal Hx
Prenatal:-No vaccination,no smoking , mother age 39yrs,not anemic,bad
ANC.
Natal :-primigravida,no fever,No APH,No G.D,No Hypertension, no
preclampsia,NVD,No PPH,slight leaking liquor,no abortion .
Postnatal:-cyanosed,2days in NICU, wt:3.5kg,No jaundice,no crying at
birth.
Developmental Hx:-
Gross motor:-no sitting,no crawling, no rolling over,he controlled his
head at 4
th
month.
Fine motor:-palmar grasp,not able to reach the object to mouth,not able
to transfer objects from one hand to another.
Social :-smile to his mother at 2
nd
month.
Language & speech:- only prounounce some incomprehensible
sounds,not able to say mamma ,baba.
Hearing&vision:-no response to his name.
7
Immunization:- upto date.
Family Hx:- no member in the family with febrile convulsion or
epilepsy/no Hx of chronic illnesses
Social Hx:-using tap water, no travel to other areas or countries, no
animals in the house ,average outcome.