Pediatrics
CVS
Dr.Newal
1
H
H
e
e
a
a
r
r
t
t
f
f
a
a
i
i
l
l
u
u
r
r
e
e
the heart cannot deliver adequate cardiac output to meet the metabolic needs of the body.
In the early stages of heart failure, various compensatory mechanisms are evoked to maintain
normal metabolic function.
When these mechanisms become ineffective, severe clinical manifestations result .
PATHOPHYSIOLOGY.
Frank-Starling law As stated by Frank, when the preload increases, the left ventricle distends,
the left ventricular pressure rises to a higher peak pressure, and the stroke volume augments.
there is a point at which further increases in EDV are not met with an increased force of
contraction, but rather stroke volume starts to decrease.
volume overload.
Etiology of Heart Failure
FULL-TERM NEONATE
Asphyxial cardiomyopathy
Arteriovenous malformation (vein of Galen))
Left-sided obstructive lesions (coarctation of aorta, hypoplastic left heart syndrome)
Large mixing cardiac defects (single ventricle, truncus arteriosus)
Myocarditis
Genetic cardiomyopathy
INFANT-TODDLER
Left-to-right cardiac shunts (ventricular septal defect
Hemangioma (arteriovenous malformation
Anomalous left coronary artery
Genetic or metabolic cardiomyopathy
Acute hypertension (hemolytic-uremic syndrome
Supraventricular tachycardia
Kawasaki disease
Myocarditis
CHILD-ADOLESCENT
Rheumatic fever
Acute hypertension (glomerulonephritis
Pediatrics
CVS
Dr.Newal
2
Myocarditis
Thyrotoxicosis
Hemochromatosis-hemosiderosis
Cancer therapy (radiation, doxorubicin
Sickle cell anemia
Endocarditis
Cor pulmonale (cystic fibrosis
Genetic or metabolic cardiomyopathy
CLINICAL MANIFESTATIONS
- depend on the degree of the child's cardiac reserve.
symptomatic at rest : cardiac output is not sufficient to meet the basal metabolic needs.
Symptomatic with mild activity:-
incapable of increasing cardiac output .
Symptomatic with vigorous exercise : less severe heart disease
In children:-
fatigue, effort intolerance, anorexia, abdominal pain, dyspnea, Orthopnea and cough.
The elevation in systemic venous pressure (JVP, liver enlargement).
basilar rales ; edema is usually in dependent portions or anasarca .
Cardiomegaly A gallop rhythm is common; holosystolic murmur may be heard
infants
tachypnea, feeding difficulties, poor weight gain,
excessive perspiration, irritability, weak cry noisy, labored respirations
with intercostal and,subcostal retractions, flaring of the alae nasi.
wheezing is prominent.
Pneumonitis, atelectasis is common.
Hepatomegaly .
cardiomegaly is invariably present. tachycardia, a gallop rhythm .
auscultatory signs of the underlying cardiac lesion.
Edema generalized and usually involves the eyelids , sacrum and less
often the legs and feet.
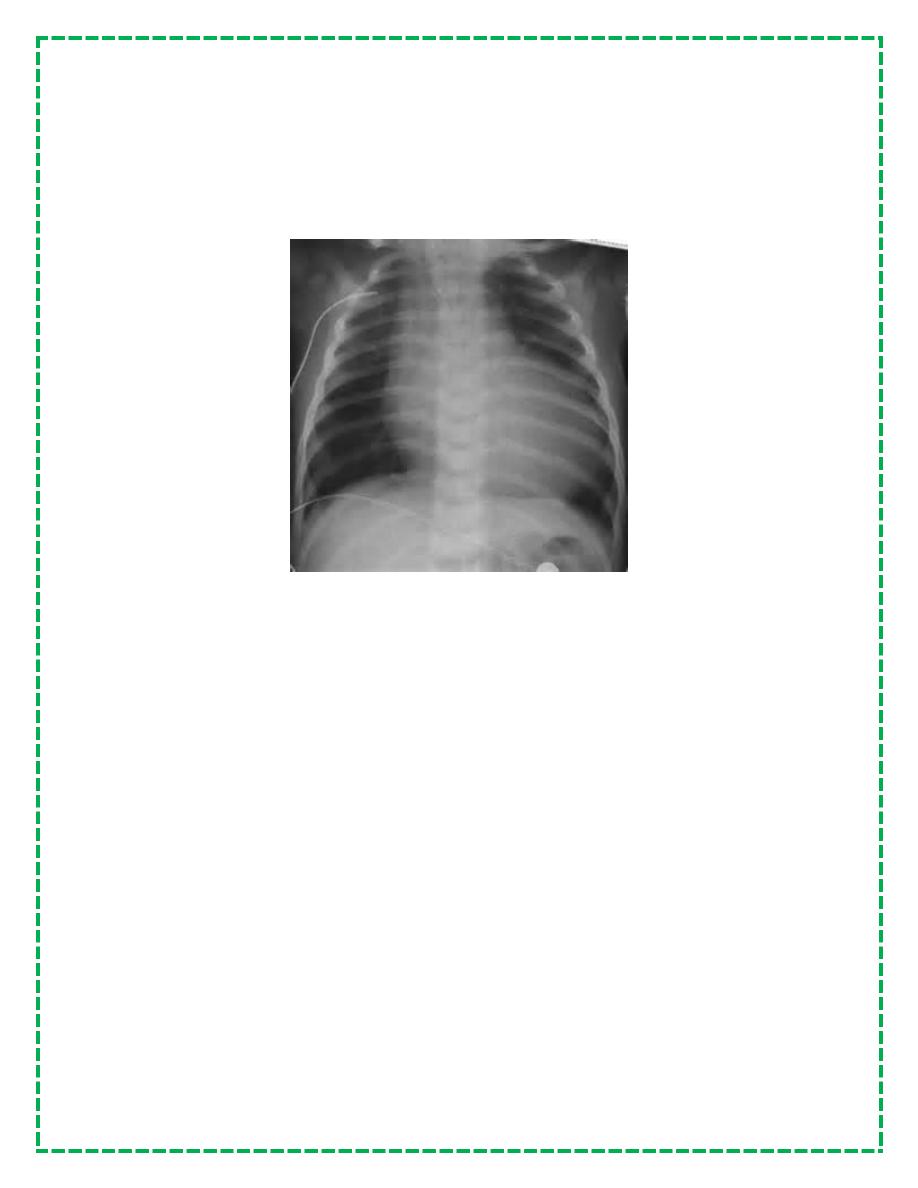
DIAGNOSIS
.CXR cardiac enlargement.
Pulmonary vascularity is variable and depends on the cause. large left-to-right shunts have
exaggeration of the pulmonary arterial vessels to the periphery of the lung fields, Fluffy
perihilar pulmonary markings suggestive of venous congestion and acute pulmonary edema
(severe degrees of heart failure).
Pediatrics
CVS
Dr.Newal
3
ECG Chamber hypertrophy ( cause of heart failure).
Low-voltage QRS morphologic characteristics with ST-T wave abnormalities (myocardial
inflammatory disease) or pericarditis
ECG best tool for evaluating rhythm disorders as cause of heart failure.
Echocardiography assessing ventricular function
-PO2 decreased ( pulmonary edema.)
-respiratory & or metabolic acidosis, if heart failure is severe.
-hyponatremia as a result of renal water retention &
Chronic diuretic treatment.
-Serum B-type natriuretic peptide (BNP), a cardiac neurohormone released in response to
increased ventricular wall tension, as in patients with (cardiomyopathy) & ventricular septal
defect
TREATMENT
remove underlying cause or alleviated..
-General Measures
Strict bed rest in extreme cases.
sleeping in a semi-upright position, infant chair
After response to treatment, restrictions on activities can often be modified ( the patient's
ability).
Competitive and strenuous sports activities are usually contraindicated.
Ppv , O2
Pediatrics
CVS
Dr.Newal
4
Diet
fail to thrive because of increased metabolic
requirements and decreased caloric intake.
- Increasing daily calories ( 24 calories/oz)
diarrhea, solute load for compromised kidneys
-nasogastric feedings may be helpful
-gastroesophageal reflux is a major problem so use continuous drip NG feedings at night,
-A strict, extremely low sodium diet is rarely required
medications
Digitalis.
Rapid digitalization carried out intravenously. (½ initially, followed by ¼ q12h × 2
Full-term neonate :20–30 gμ/kg
Infant or child: 25–40 μg/kg,
These doses are PO;IV dose is 75% of oral dose
ECG closely monitored and rhythm strips obtained before each of the
three digitalizing doses. Digoxin should be discontinued if a new rhythm
disturbance is noted.
Serum digoxin determination is helpful when digitalis toxicity is
suspected (arryhmia, vomitt ).
Baseline serum electrolyte levels should be measured
before and after digitalization. Hypokalemia and
hypercalcemia exacerbate digitalis toxicity. ( diuretics)
Maintenance digitalis therapy
is started ≈12 hr after full digitalization, divided q12h r
The dosage is one quarter of the total digitalizing dose
.slow digitalization : initiation of a maintenance digoxin.
schedule achieves full digitalization in 7–10 days( outpatient)
Diuretics.
Effect?
Furosemide most commonly used diuretic . It inhibits the reabsorption of sodium and chloride
in the distal tubules and the loop of Henle. intravenous or intramuscular furosemide at an initial
dose of 1–2 mg/kg,
maintain 1–4 mg/kg/24 hr given between one and four times a day.
Side effect hypokalemia, alkalosis, hyponatremia.
Pediatrics
CVS
Dr.Newal
5
Spironolactone is an inhibitor of aldosterone
2–3 mg/kg/24 hr.
Chlorothiazide (less severe chronic heart failure), dose is 20–40 mg/kg/24 hr in two divided
doses.
After load-Reducing Agents and ACE Inhibitors.
ACE inhibitor captopril produces
arterial dilatation by blocking the production of angiotensin II, resulting in afterload reduction.
Venodilation
interferes with aldosterone production,
beneficial effects on cardiac structure and function.
The oral dose is 0.3–6 mg/kg/24 hr given.
Adverse reactions
Enalapril is a longer acting ACE inhibitor.
α- and β-Adrenergic Agonists
-Dopamine is a predominantly β-adrenergic receptor agonist, but it has α-adrenergic effects at
higher doses. also it results in selective renal vasodilation
At a dose of 2–10 μg/kg/min
-Dobutamine, a derivative of dopamine, is useful in treating low cardiac output. It causes direct
inotropic effects with a moderate reduction in peripheral vascular resistance.
-Epinephrine is a mixed α- and β-adrenergic receptor agonist that is usually reserved for
patients with cardiogenic shock and low arterial blood pressure..
Formatted By Mohammed Musa