Maternal physiological Changes with Pregnancy
Pregnancy is a period of adaptation for:
• 1-The needs of the fetus
• 2-Meeting the stress of pregnancy and labour
• THE GENITAL CHANGES
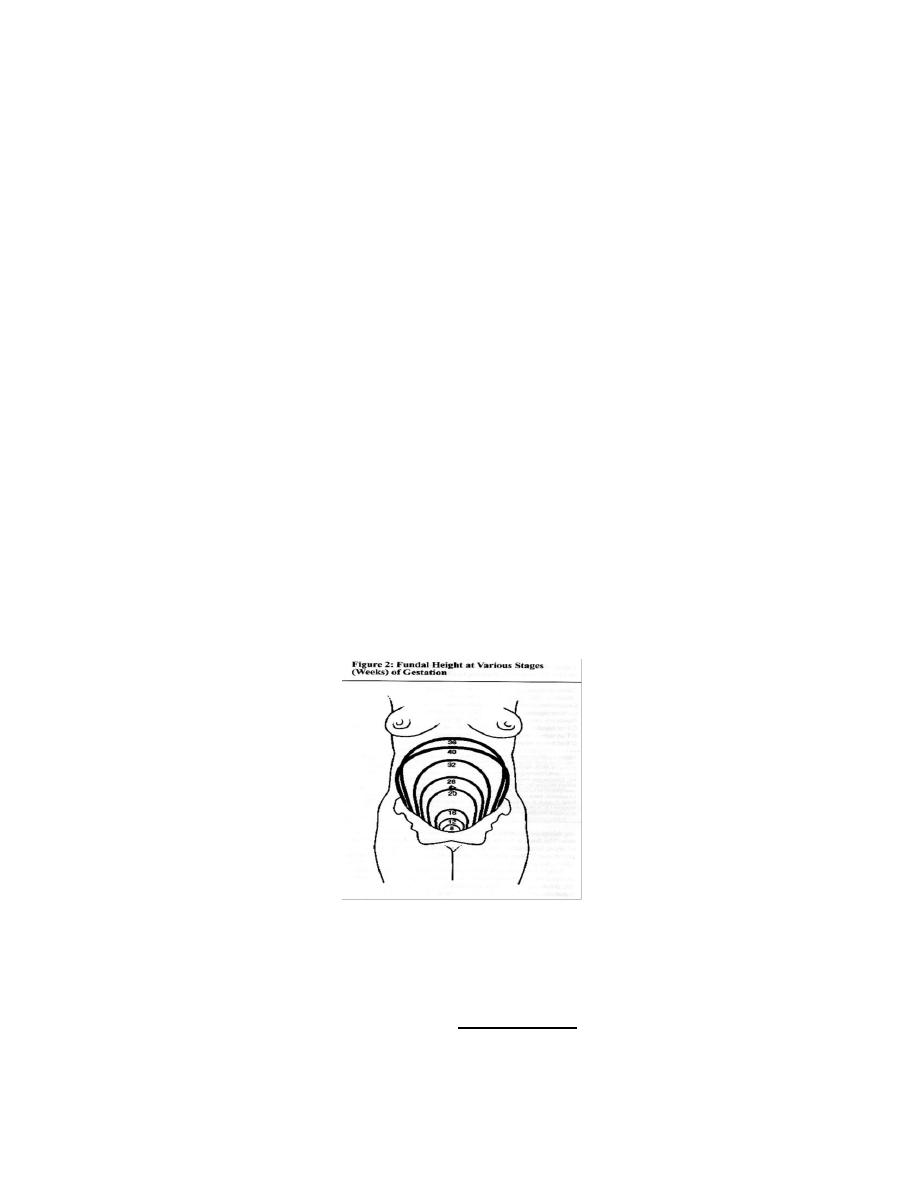
The uterus
Size:
increase from 7.5 x 5 x 2.5 cm in nonpregnant states to 35 x 25 x 20 cm
at term
Weight:
increases from 50 gm in nonpregnant state to 1000 gm at term
Consistency:
becomes progressively softer due to increased vascularity &
presence of amniotic fluid with ascent from the pelvis , the uterus rotate
with tilting to Rt (dextrorotation) due to the presence of the recto segmoid
colon on the left
Myometrial changes
• High level of maternal estrogen& progesterone induce hypertrophy &
hyperplasia of the myometrium till 14th week, then the fetus exerts a
direct stretch increasing muscle fiber length up to 15 fold.
• Intercellular gap junctions also develops facilitating myomrtrial
contraction ,these allow the pacemaker activity of uterine funds to
promote the coordinated contractions of labour .
Formation of lower uterine segment:
After 12 weeks, the isthmus starts to
expand gradually to form the lower uterine segment which measures 10 cm
in length at term
Upper Segment:
3 layers; outer longitudinal, middle oblique and inner
circular .It is active, contracts, retracts and becomes thicker during labour
Lower Segment:
2 layers; outer longitudinal and inner circular . Passive,
dilates, stretches and becomes thinner during labour
Uterine blood flow
increases 40-fold progressively reaching 500 ml/min at
term
1 - Uterine artery lumen:
is doubled and its blood flow
5 times
2 - Myometrial and decidual arteries (spiral arteries
) undergo fibrinoid
degeneration due to 2 waves of trophoblastic migration , so they become
dilated to be the uteroplacental arteries
Changes in the cervix :
1 - It becomes hypertrophied , soft and bluish in colour due increased vascularity
2 – the mucous glands become distended &screating a thick secretion obstructs
the cervical canal forming a mucous plug
3 - The endocervical columnar epithelium proliferates and everted forming
ectropion

Changes in the vagina :
The vaginal epithelium becomes more vascular with increased desquamation
resulting in increased vaginal discharge which has more acidic pH & may
protect against ascending infection
II - Haematological Changes
(A)
Blood volume
:
The total blood volume increases steadily from early
pregnancy to reach 35-45 % above the non-pregnant level at 32 w.The
most marked expansion occurs in the plasma.The discrepancy between the
in plasma volume (50%)& the
in red blood cell mass (25%) results in
haemodilution (physiologic anemia.
(B)
Blood indices
:
1 - Decreased Hb concentration :
Hb conc. falls from 13g/dl in non
pregnant to 11g/dl at 36
th
w of pregnancy.There is increased demand for
iron &if supplementary iron not takened there will be reduction in bone
marrow iron as well as in mean red cell vol.& serum ferritin level.Renal
clearance of folic acid is increased & plasma folat conc. fall
2 - Reticulocytes : mild
3 - E.S.R :
from 12 to 50 mm / hour:
4-White cell count from
(from 7.000 / mm3 to 10.500 / mm3 during
pregnancy and up to 16.000 / mm3 during labour
Coagulation system
Pergnancy is a hypercoagulable state which return to normal 4ws after
delivery .Fibrinogen
from 300 mg / dl to 450 mg / dl. All procoagulant
factors are
including. Factor VII, VIII, IX, X & XII .Antithrombin III
unchanged whereas protein S activity
with
activated protein C
resistance( Fibrinolytic activity
)
Ill - Cardiovascular system changes
Changes in the heart:
As the diaphragm is elevated progressively during pregnancy the apex is
displaced upwards and to the left .
• The first heart sound become louder and may split .The third heart sound
may be audible .
• An ejection systolic murmur can be heard in90% of NR pregnant women.
Pulse & blood pressure:
- The PR
progressively from early pregnancy till term to about 10-15
beat/min -B.P. is decreased in 2
nd
trimester to increase again in 3rd
trimester due to Decreased Peripheral resistance The decrease in
diastolic BP is more marked than in systolic. Thus, pregnancy is
associated with a relative increase in pulse pressure.
Cardiac output:
increases mainly by increased stroke volume (10%)reaching a maximum level
at 20 weeks to be maintained till term.
During labour C.O.P.
more during the second stage due to uterine contractions
, and expulsive efforts
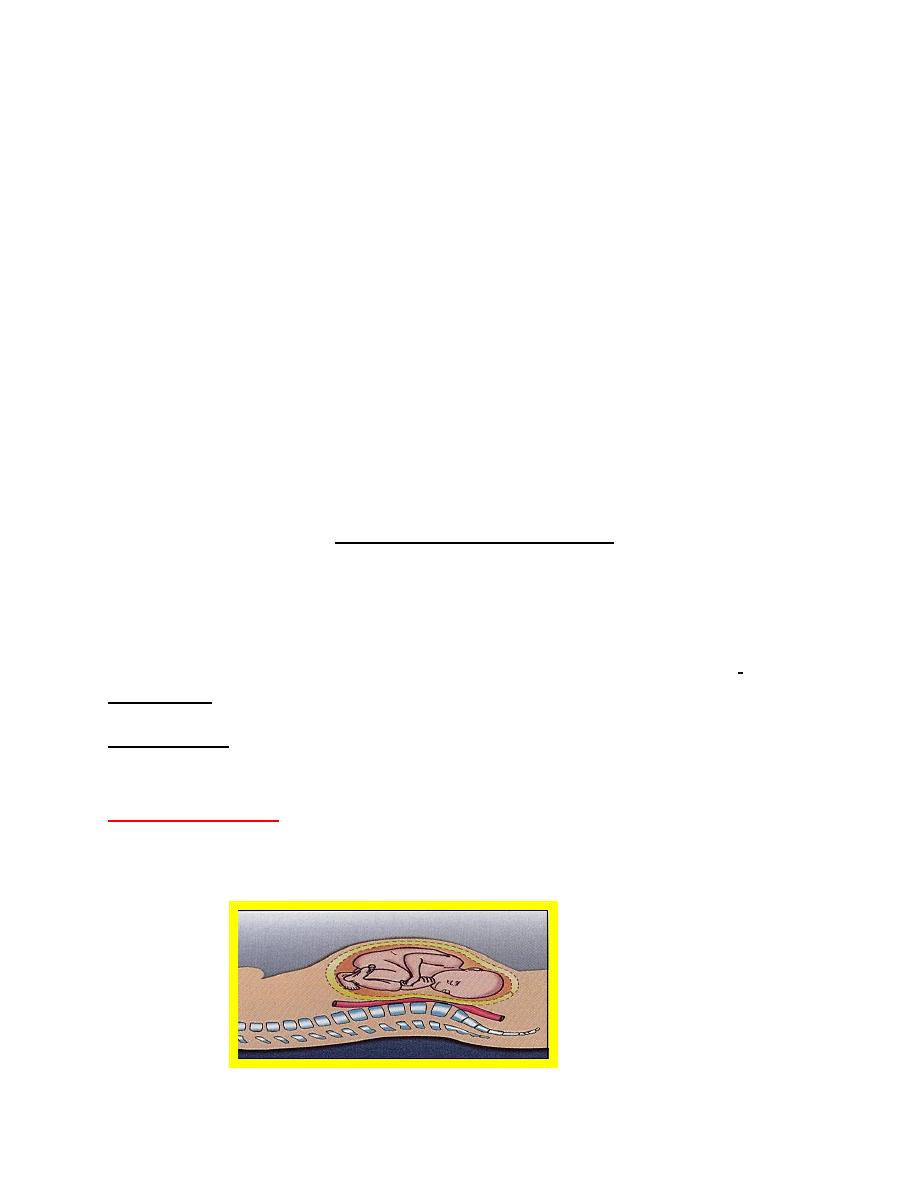
Supine hypotension :
may develop in some women in late pregnancy while lying
supine due to compression on the I.V.C. by the large pregnant uterus , resulting
in decreased venous return
C.O.P.
IV - Respiratory system:
Respiratory functions:
Due to the displacement of diaphragm up to
4cm,
O2cosumption &
respirotary center sensitivity to CO2 Minute
ventilation (tvxRR) increased as RR : un changed. tidal volume is
This
in MV is perceived by the pregnant woman as shortness of breath.
Functonal residual capacity is decreased
V - Urinary system :
(A) Kidney and kidney function tests:
• Renal blood flow and glomerular filtration rate increases by 50 % .
This leads to increased excretion
1. There is
serum creatinine (due to
creatinine cleareance) ,
uric acid.
2.
blood urea .
3.
kidney excretion of glucose due to
filtration load leading to glucosuria
(B) Ureters & Bladder:
Dilatation of the ureters and renal pelvis due to :
i - Relaxation of the ureters by the effect of progesterone .
ii - Pressure against the pelvic brim by the uterus particularly on the right side
due to dextrorotation of the uterus
Pressure on the bladder causes frequent micturation.
VI - Gastrointestinal tract:
Indigestion ,conistipation and flatulence:
This is probably due to :
i - Decreased gastric & intestinal motility (progesterone effect).
ii - Pressure on the pelvic colon by the pregnant uterus.
Heart burn Due to reflux of acidic gastric contents to the oesophagus due to
reduced lower oesophageal sphincter tone.
VII - Metabolic changes:
(A) Weight gain:
The average weight gain in pregnancy is 10 - 12 kg .Out of the 11 kg weight gain
6 kg is composed of maternal tissues (breast, fat, blood and uterine tissues), and
5 kg of fetal tissue , placenta and amniotic fluid.
)
B) metabolism:
-Water: there is tendency to water retention secondary to sodium retention
-Protein: There is tendency for nitrogen retention (+ ve nitrogen balance) for
fetal and maternal tissue formation
Carbohydrate Pregnancy is potentially diabetogenic (
insuline resistance)
Fat: There is
of plasma lipids
VIII - Musculoskeletal changes:
(a) Increased mobility of pelvic joints due to softening of the joints and
ligaments caused by progesterone and relaxin

(b) ) Progressive lordosis leading to lordotic gait & backache
IX - Endocrine system:
The pituitary:
The ant.pituitary increase in size more than increase in
vascularity .This renders it liable for ischaemia
-
Prolactin level
to ensure lactation
-
The post.pituitary Does not
hypertrophy , but
its oxytocin secretion near term
Thyroid gland:
There is diffuse slight enlargement of the gland
TSH
in early pregnancy
thyroid binding globulin (TBG)
Total T3 &T4 with
fT4 in late pregnancy
Suprarenal gland:
Hypertrophy particularly the cortex resulting in increased
glucocorticoids (cortisone) and increased mineralocorticoids (aldosterone)
Breast signs:
i - increased size & vascularity due to hormonal responses
number of
mammary ducts (by estrogen)and
number of gland alveoli (by progesteron)
ii- Third trimester :
secretion of colostrum (thick yellowish fluid) which can be expressed from the
nipple
iii-Prolactin stimulates milk secretion after delivery following the removal of
estrogen inhibition &initiation of suckling
by:Twana nawzad