Dr.aseel
obstetrics
Cephalopelvic disproportion
Cephalopelvic Disproportion:
Is disproportion between the size of the fetal head and that of the
maternal pelvis. It can be due to a large head, small pelvis or a combination of both which cause
difficult labour and danger to the mother and fetus.
In every case of disproportion the
efficiency of the uterine contractions play a major part in determining whether or not vaginal
delivery will occur , equally important is the attitude and position of fetal head.
The diagnosis of disproportion before labour
1-
past orthopedic history
of metabolic disease or fracture of the spine, hip or pelvis Obstetric
history whether the patient is primigravida or multigravida, In multigravida CPD is usually
because she has a fetus larger than any she has previously born, so ask about duration of
labour, size of fetus and outcome of delivery.Fetal anomaly like hydrocephalus may contribute,
& fetal thyroid &neck tumours may cause extension leading to relative disproportion
2-
General examination
:
short stature (Height less than 150 cm), abnormalities of skeleton&
abnormal gate.
3
- Abdominal examination
:
Engagement of head 36-38 week in primigravida. Test for
engagement to exclude inlet disproportion, this is done by moderate pressure on the head in
the backwards and downwards direction.
4-
pelvic examination(Clinical pelvimetry
):
Size of pelvis is of primary importance while the
shape is of secondary importance.
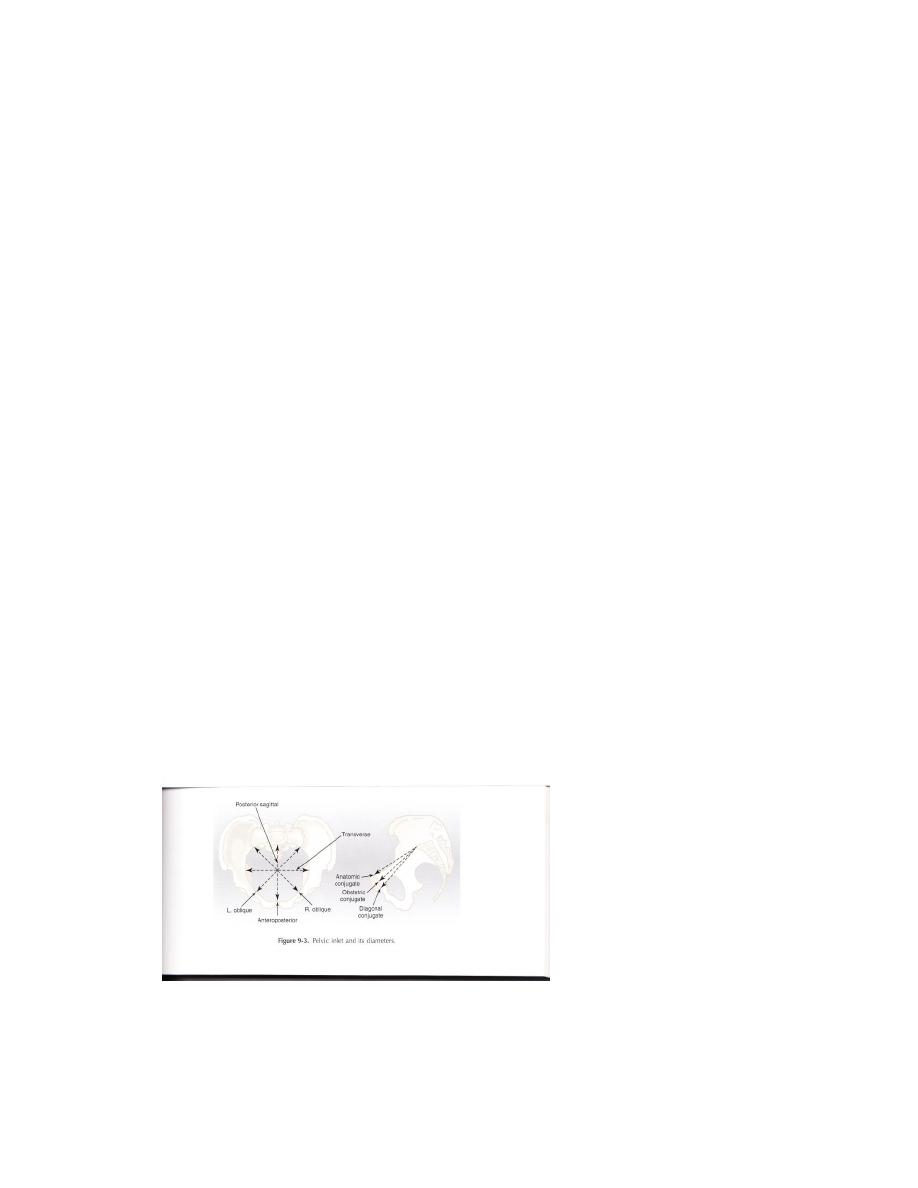
1) Pelvic inlet: Antero-posterior diameter (diagonal conjugate) is measured clinically by
attempting to touch the sacral promontory with the vaginal examining finger while
simultaneously noting where the inferior border of the symphysis touches the
examining finger. A measurement >11.5 cm suggests adequacy.
2) Mid pelvis: (cavity):
An inter-spinous diameter <9.5 cm suggests midpelvis contraction
,but it is difficult to estimated clinically. The ischial spines should not be promenent.
Dr.aseel
obstetrics
concavity or straightness of sacrum should be noted.
convergence of the sidewalls of
the pelvic cavity(should be parallel).
3) Outlet:
This transverse diameter of the outlet can be estimated by placing a clenched
fist between the two ischial tuberosities. A measurement of 8 cm or more suggests an
adequate diameter.Sub pubic arch should be >90
5- Radiological examination:
A) x-Ray: lateral view – A.P diameter of inlet - curve of sacrum - sacrosciatic notch-
engagement of fetal head- A.P view: transverse diameter of inlet and outlet
B) MRI
The diagnosis of disproportion during labour.
1- failure to progress or slow progress (failure of head to descend and the cervix to dilate
during labour) despite efficient uterine contraction.
2-the fetal head is not engaged.
3-vaginal examinatin shows excessive molding or caput.
4-the head is poorly applied to the cervix.
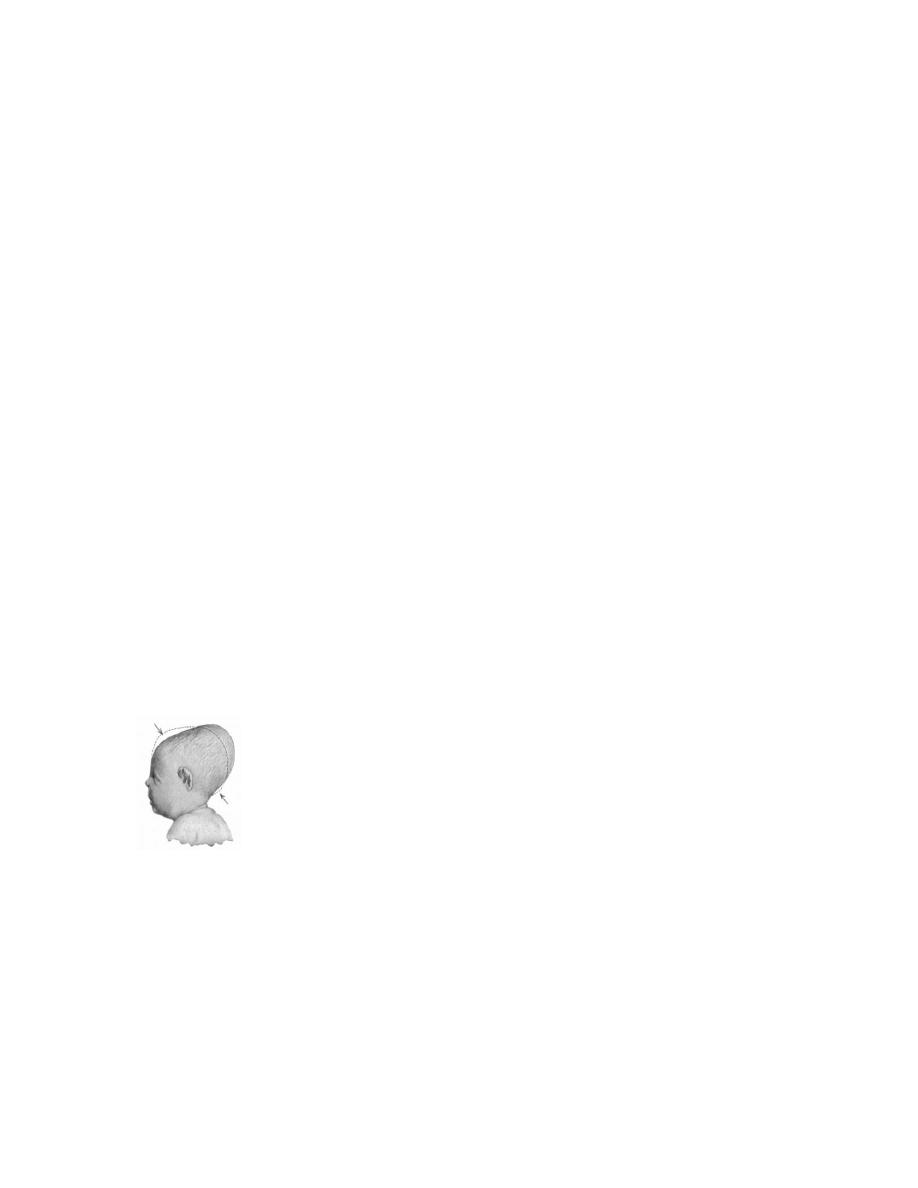
Caput succedaneum
:
is a localized scalp oedema affecting the most dependent part of the
fetal head due to pressure effect of dilated cervical ring and vaginal introitus on descending
head . the caput disappears within one or two days after delivery. The presence of big caput
indicate that Labour was prolonged and difficult
.
management of disproportion
1-indications of elective caesarean section
a- severe disproportion
b- less degree of disproportion + complicating factors such as breech, previous
caesarean section or previous vaginal delivery causing perinatal mortality and women with
medical complications such as diabetes and hypertension.
c- fetal /or maternal distress.
Dr.aseel
obstetrics
2- Trial of labour
Women with mild disproportion should be allowed a trial of labour with careful
monitoring of progress of labour and of the fetal & maternal condition , if there is failure to
progress after a period of 4 hours of good uterine contraction or whenever there is fetal or
maternal distress emergency caesarean section is indicated.
3-Oxytocin can be given for augmentation of labour to provide good uterine contraction
carefully to a primigravida with milde CPD as long as the CTG is reactive ,it must never be
used in a multiparous woman if CPD is suspected because of risk of over stimulation.
By:TWANA NAWZAD