Episiotomy & perineal tear
●
Is an intentional surgical incision through the perineum made to enlarge
the diameter of vulval outlet & assist child birth.
●
blood loss is not uncommon with episiotomy and is avoided by
performing the episiotomy when the head crowns. Early incision increases
blood loss and immediate repair after delivery will help to minimize blood
loss.
Indications for episiotomy :
1. When anterior tears with bleeding or multiple perineal tears appear.
2. Fetal distress, it is carried out to expedite delivery.
3.To facilitates instrumental vaginal deliveries although the need for an
episiotomy is less with ventouse deliveries.
4. If the delivery process is delayed and it is thought to be due to a rigid
perineum & threatened to tear extensively.
5. Vaginal manipulations in assisted breech deliveries.
6. In cases of shoulder dystocia.
7. In women who had a previous pelvic floor or perineal surgery
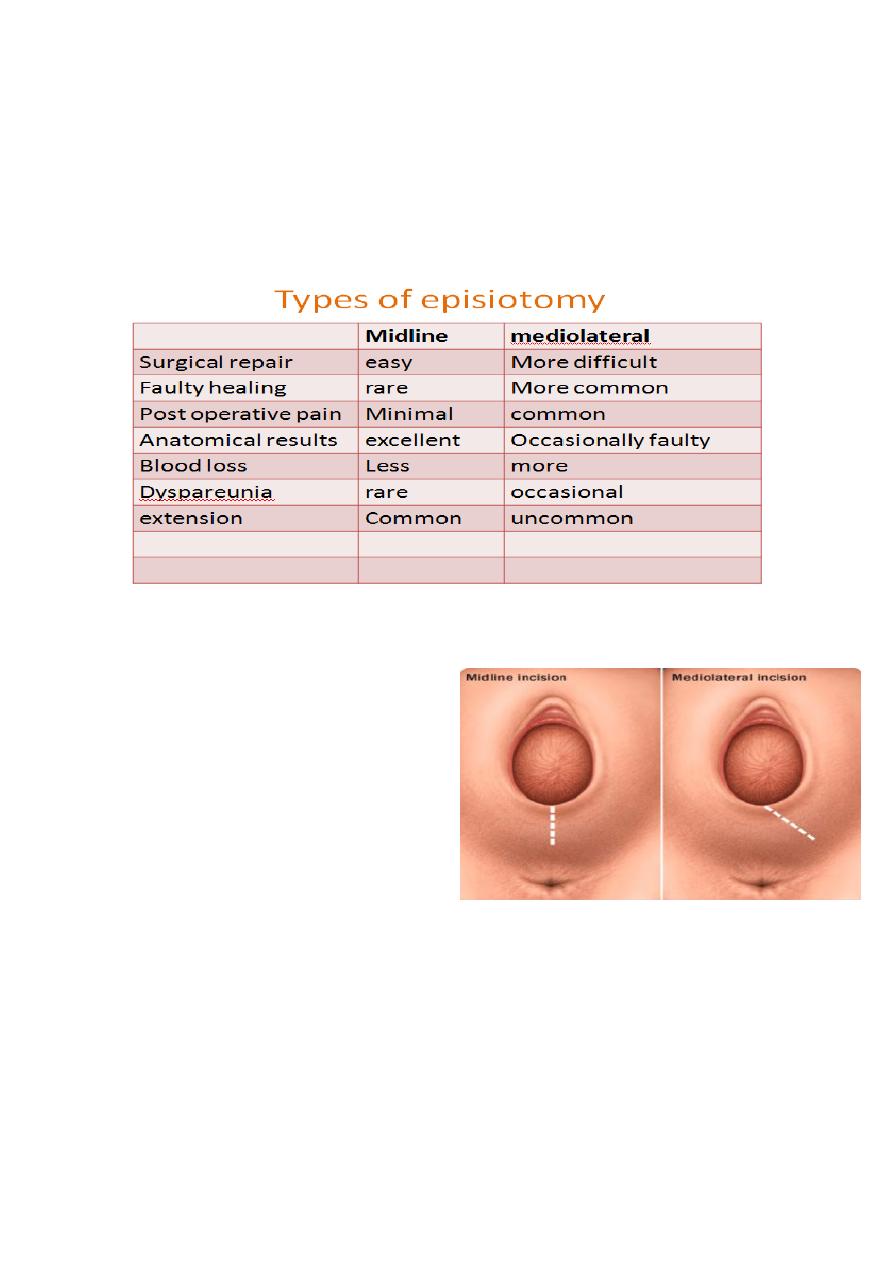
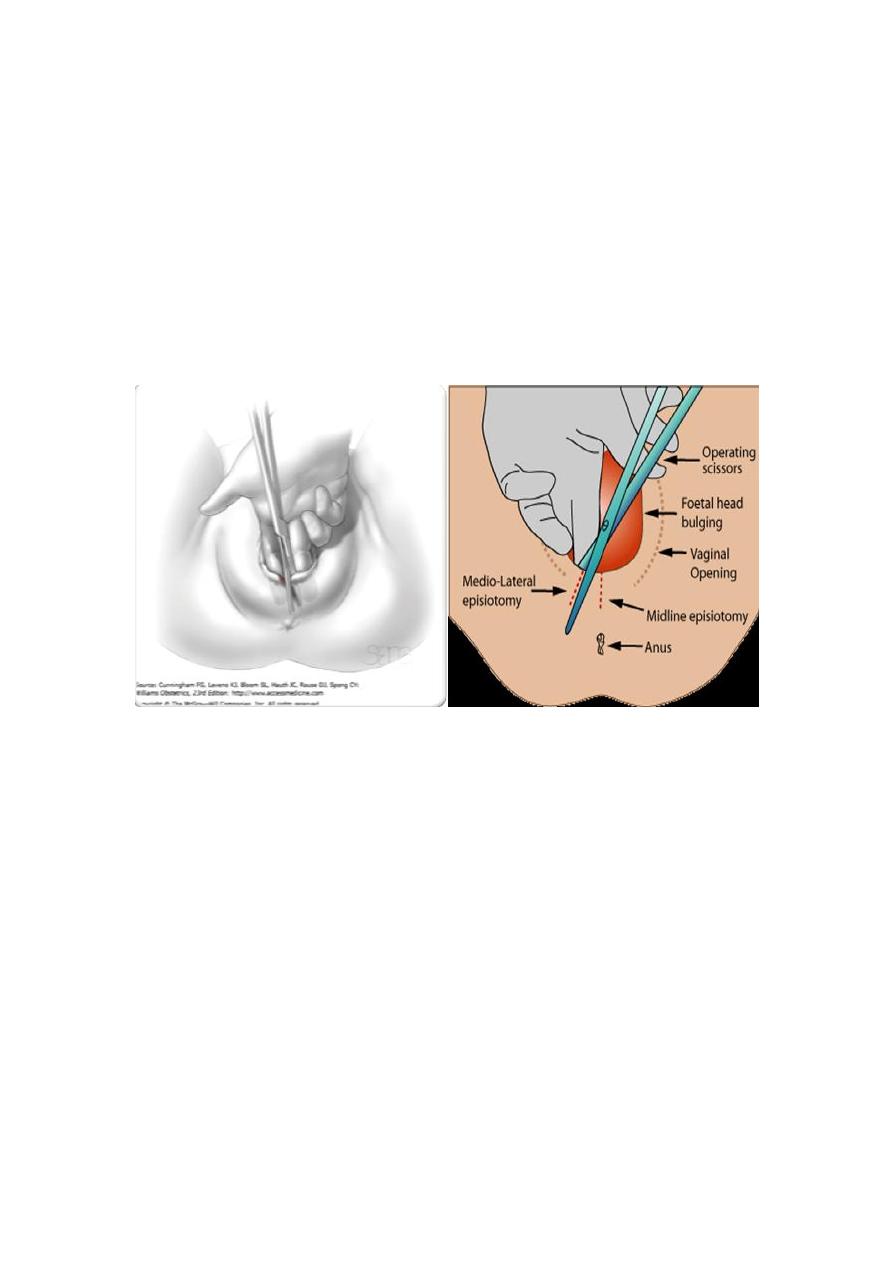
Types of episiotomy:
●
In the USA, a midline episiotomy starting from the fourchette for a few
centimetres towards the anus is popular.
●
In UK a mediolateral episiotomy starting from the fourchette going
laterally to 45◦ is carried out.
Technique:
●
An episiotomy is performed in the 2
nd
stage, when the perineum is stretched.
●
If there is no epidural, the perineum
should be infiltrated with local
anaesthesia.
●
The incision can be midline starting
from the fourchette for a few centimetres towards the anus, while a
mediolateral episiotomy starting from the fourchette going laterally to
45◦.
●
A sharp scissors is used to make a single incision about 3–6 cm
depending on the size of the perineum. The depth involves the superficial
perineal muscles like a second degree tear.
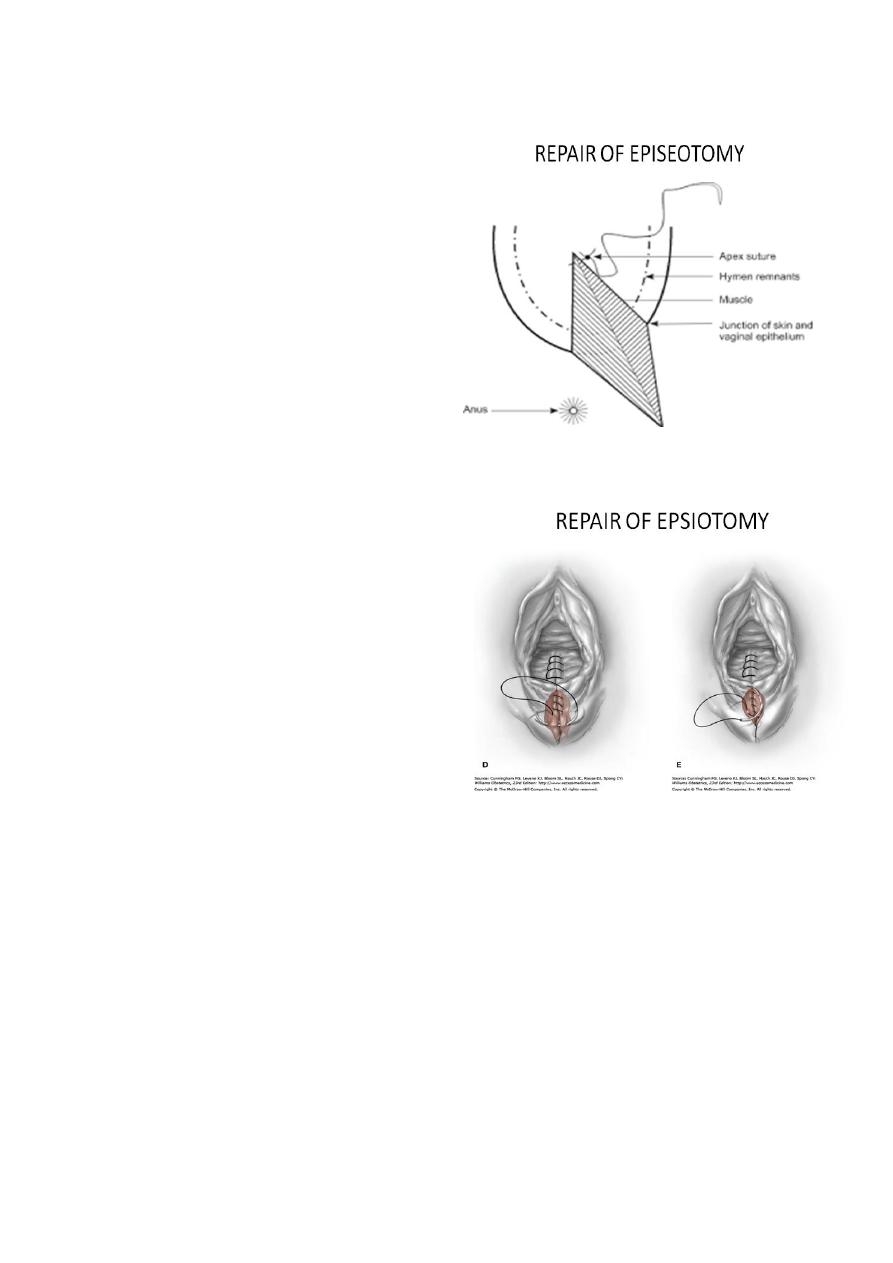
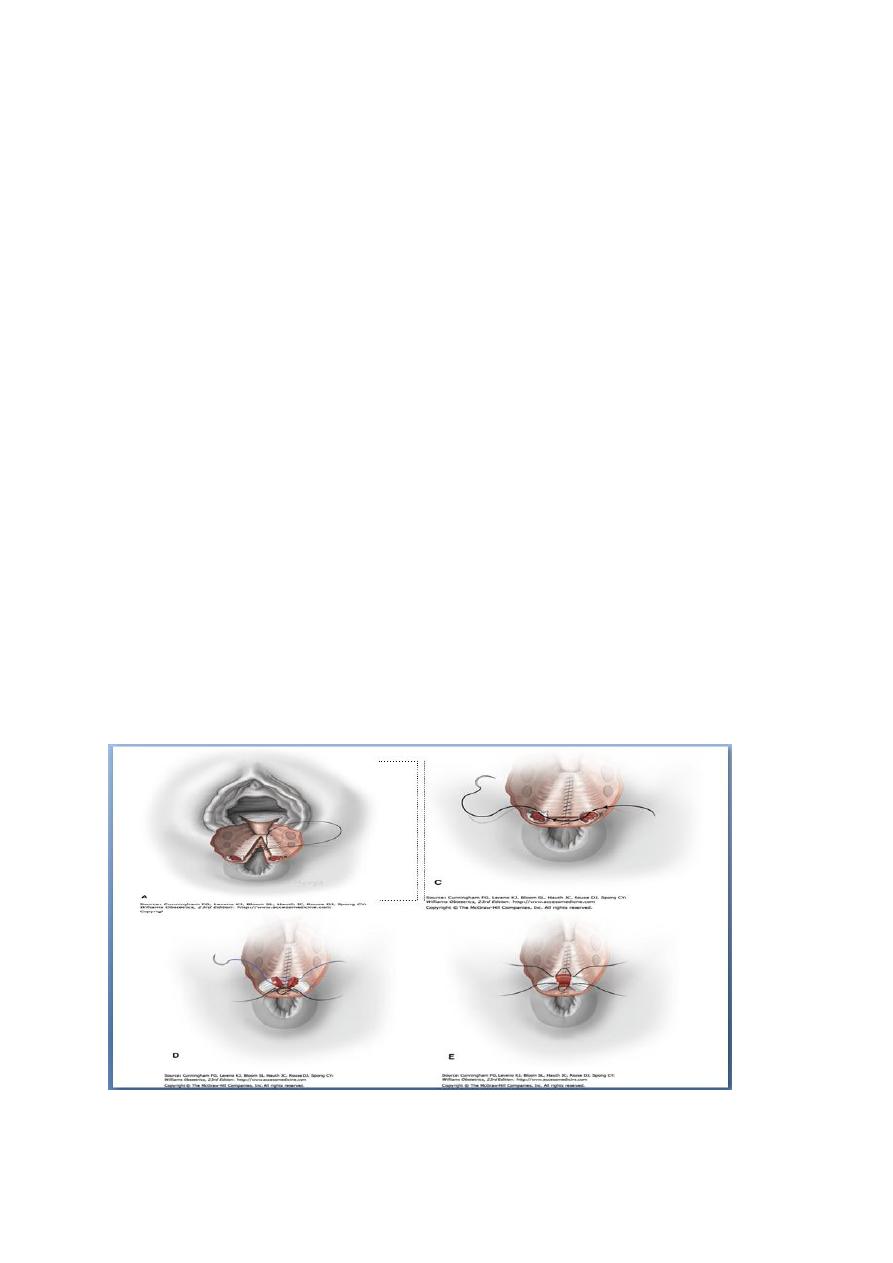
Repair of episiotomy:
●
The adequacy of pain relief should be
rechecked prior to starting the repair
which is made easy with good light and
optimal exposure.
●
The exposure and difficulty with
seeing the edges of the vaginal skin due
to bleeding from above can be
overcome by placing a vaginal swab
with a tail that comes outside the
introitus.
●
The apex of the tear or episiotomy
should be secured by a suture above the
apex to stop any bleeding.
●
The suture is then threaded down at
half to 1 cm intervals taking each vaginal
wall in turn with a continuous locking
suture using a synthetic suture material
like ‘vicryl rapide’. This helps in
haemostasis and prevents vaginal
shortening
●
The distance between sutures in the medial side may be longer
compared with the lateral vaginal wall to bring about good approximation
so that at the fourchette, the hymenal membrane and the junction of the
pink vaginal skin to pigmented outer skin margin at the introitus meet as it
was before the tear or the episiotomy.
●
The perineal muscles can be approximated by continuous or interrupted
sutures.
●
The perineal skin is approximated by subcuticular suture as it is
associated with less pain and heals well.

●
A vaginal examination should confirm good approximation of the cut
edges and good haemostasis.
●
A rectal examination to exclude accidental suture involvement of the
rectum.
●
Before cleaning and placing a pad against the vagina an instrument,
needle and swabs count should be carried out. Care should be exercised to
remove swab after completion of the repair.
●
blood loss and post repair care should include sufficient instructions for
pain relief including appropriate analgesics.
Complications :
Haemorrhage or hematoma
●
Pain
●
Extension to anal sphnicter
●
Late complication:
●
Infection : prophylactic antibiotic is indicated
-
Breaking down of repair
-
Pain
-
Scaring
-
Dyspareunia
-
Granuloma : can be treated with sliver nitrate.
-
Fistula
-
Endometiosis : cyclical pain at site of episiotomy
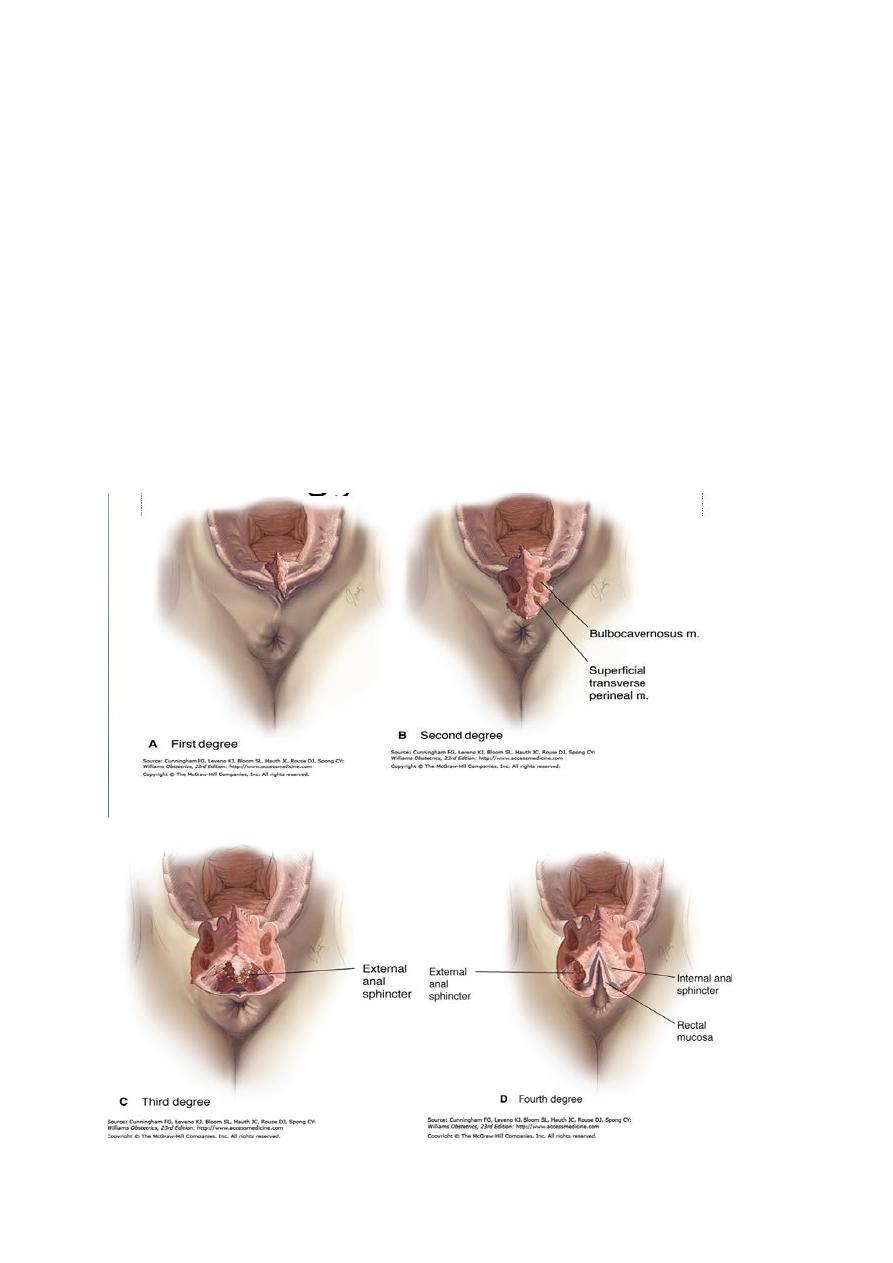
Perineal trauma :
1
st
degree:
laceration of skin or vaginal epithelia.
2
nd
degree:
involve perineal muscle , this include episiotomy
3
rd
degree:
involve anal sphnicter complex
a-less than 50% of external anal sphnicter is torn
b-more than 50% of ext. Anal sphnictor is torn.
c-tear involve internal anal sphnicter
4
th
degree:
involve injury to anal sphnicter complex extending to rectal
mucosa
Repair of perineal tear:
●
Repair of 3
rd
or 4
th
degree tear require adequate analgesia such as
regional or general anaesthesia, because local infiltration of anaesthesia
does not allow relaxation of sphnicter to allow satisfactory repair.
Good light & an assistant is usually needed.
●
●
Repair of rectal mucosa should be performed first, then repair of ext anal
sphnicter, muscle should be approximated with long acting suture to give
adequate time for healing, repair either by end-end or overlap technique
Lactulose should be given for 5-10 days
●
●
Broad spectrum antibiotic covering anaerobic contamination such as
metronidazole
Adequate analgesia
●
Follow up with involvement of colorectal surgeon
●
●
At 6-12 months , evaluation should be done for symptoms such as anal
or fecal incontinence, symptomatic women should be offered endoanal
ultrasound & manometry
Meral Cevdet