Obstetrics Lec 13 Dr. Aseil
1
ECTOPIC PREGNANCY
DEFINITION
Any pregnancy where the fertilised ovum gets implanted & develops in a site
other than normal uterine cavity.
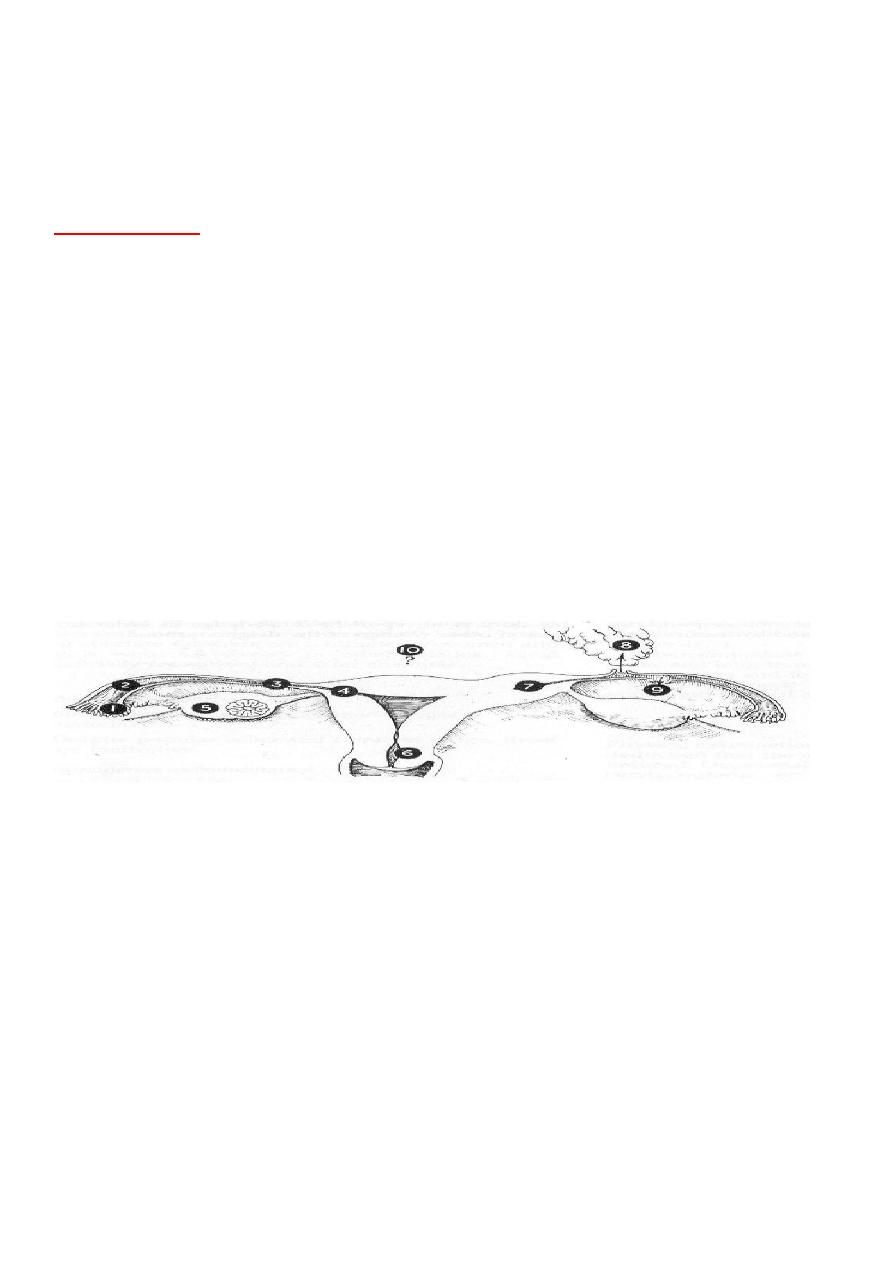
Implantation sites:
1- Outside the uterus :
Fallopian tube ( 95 % )
Abdominal cavity.
o Overy 3%
2- Abnormal position within the uterus:
Cornua of the uterus .
Cervix .
1)Fimbrial 2)Ampullary 3)Isthemic 4)Interstitial 5)Ovarian 6)Cervical 7)Cornual-
Rudimentary horn 8)Secondary abdominal 9)Broad ligament 10)Primary
abdominal
AETIOLOGY
Any factor that causes delayed transport of the fertilised ovum through the
fallopian tube favours implantation in the tubal mucosa itself thus giving rise
to a tubal ectopic pregnancy(peristaitic activity,damage to ciliated
epith.,peritebal adhesion). These factors may be Congenital or Acquired.
CONGENITAL –

Obstetrics Lec 13 Dr. Aseil
2
Tubal Hypoplasia , Tortuosity , Congenital diverticuli , Accessory ostia , Partial
stenosis
ACQUIRED -
Inflammatory: PID(T.B,chlamydia,gonococus), Septic Abortion, Puerperal Sepsis,
Surgical: Tubal reconstructive surgery pelvic surgery
Miscellaneous Causes: IUCD ,POP,inj.prog Endometriosis, ART (IVF & GIFT),
Appendisits, Previous ectopic
Incidence :
-
11 per 1000 pregnancies .
Mortality rate :
-
1 per 100000.
Clinical presentation
-
The usual presentation is at 8 weeks except when the pregnancy is
rudimentary horn at 16 -18 weeks or even with out MP when EP is in
isthmic part of the tube.
Acute presentation
Amenorrhoea(MP)
Unilateral pain
Irregular bleeding,decidual cast shedding
Rectal pain/ shoulder tip pain
Dizzy/faint
Risk factors
Examination
Tenderness, peritonism (rebound/guarding)
PV : uterine enlarged with tender mass on1side
Cervical excitation
Sub acute presentation
-
Milde abdominal pain in one iliac fossa.
-
Episodes of vaginal bleeding .
-
Or the pt. may come have no symptoms (silent presentation ).

Obstetrics Lec 13 Dr. Aseil
3
Differential diagnosis
1- Pelvic inflammatory disease( PID ).
- In ectopic p. no fever while in PID there is.
- Fowl vaginal discharge in PID .
2- Abortion.
3-Other causes of acute abdomen e.g Appendesitis,UTI
Diagnosis
1- Clinical.
2-
HCG level ;when it is around 1500mIU an intrauterine G.S of about 4.5w should be
visualized by TVS if not EP is suspected & B-HCG level should be repeated after 48 h in
EP there is either suboptimal rise,steady level or slow decline.
3- Vaginal U /S ; extrauterine sac with an embryo or adenexal mass and the
presence of fluid in the pouch of Douglas.
4- Culdocentesis .
5- Laparoscopy; Definite Dx of ectopic preg is by this way.
MANAGEMENT
Depends on the stage of the disease and the condition of the patient at
diagnosis. Options-
Surgery – Laparoscopy / Laparotomy
Medical – Administration of drugs at the site / systemically
Expectant – Observation
MANAGEMENT OF ACUTE ECTOPIC PREGNANCY
Hospitalisation
Resuscitation -
Treatment of shock
Analgesics
Blood transfusion
Surgery as early as possible
SURGICAL TREATMENT OF ECTOPIC PREGNANCY
Carried out either by Laparoscopy / Laparotomy.
Laparotomy is reserved for severely compromised patient or in lack of endo-
scopic facilities.

Obstetrics Lec 13 Dr. Aseil
4
Laparoscopy is the mainstay of management .
The procedures are: -
Salpingectomy(removal of the tube) is the Rx of choice if the tube was
ruptured.
Conservative surgery is done(in cases of Infertility & desire for pregnancy) if
the tube is unruptured:-
Salpingostomy Create an opening in the tube but keep it open to heal by
secondary intention.
Salpingotomy Create an opening then suture it .
Medical treatment for ectopic pregnancy
Sub acute cases can be treated by:-
* Systemic methotrexate. Or
*Local injections of trophotoxic substance like : methotrexate, prostaglandins,
potassium chloride into the ectopic pregnancy sac or into the affected tube by
-laparoscopy
- trans cervical
- trans vaginal
-
trans abdominal under U / S guides.
Criteria for medical treatment :
1-
The pregnancy size less than 4 cm,no viable fetus,no signs of rupture or bleeding.
2- the HCG less than 1500 I.U./L.
3- Asymptomatic or milde symptoms
* Need follow up by HCG level and vaginal U / S on days 4 and 7, 15% fall
Contraception for 3 m after Rx
S.E: Stomatitis, GI upset, conjunctivitis
EXPECTANT TREATMENT
Tubal Pregnancies are known to Abort / Resolve spontanuosaly& selected cases
can be managed expectantly, screened and identified by ultrasound scanner
and monitored by serial serum HCG assay(there should be gradual resolution of
EP by ULS & falling serum HCG level at 2 day interval)
Obstetrics Lec 13 Dr. Aseil
5
Abdominal pregnancy
It is usually a result of the secondary implantation of a primary tubal pregnancy.
Diagnosis
History.
O/E : Fetal parts readily palpable and the uterus may felt separately from
the fetus, persistent abnormal lie.
ULS:Fetus outside the uterus.
Treatment :
* Termination by laparotomy
Ovarian ectopic
It may be primary or secondary to tubal pregnancy.
It may be confused with complicated corpus luteum.
Diagnosis :ULS& laparoscopy.
Treatment : Wedge resection of that part of the ovary or oopherectomy.
Cervical pregnancy
Very rare condition, suspected if the cervix enlarged and normal size uterus.
U/S : Empty uterus with the gestational sac in the cervix.
Treatment :
Suction curettage.
Vascular ligation by cerclage.
Rarely hysterectomy.
Obstetrics Lec 13 Dr. Aseil
6
Cornual pregnancy
Very rare in the a rudimentary horn of bicornuate uterus.
Clinical features:
Abdominal pain precedes or coincident with rupture uterus in the early
second trimester.
Treatment :
Excision of the rudimentary horn.
Hetrotopic pregnancy
Combination of intrauterine and extrauterine.
It may follow I.V.F.
Diagnosis
: by U/S
Treatment :
Intratubal pregnancy injection of KCL, methotrexate or surgical removal.
About 75% of the intrauterine pregnancies reach term.
Edited by :TWANA NAWZAD