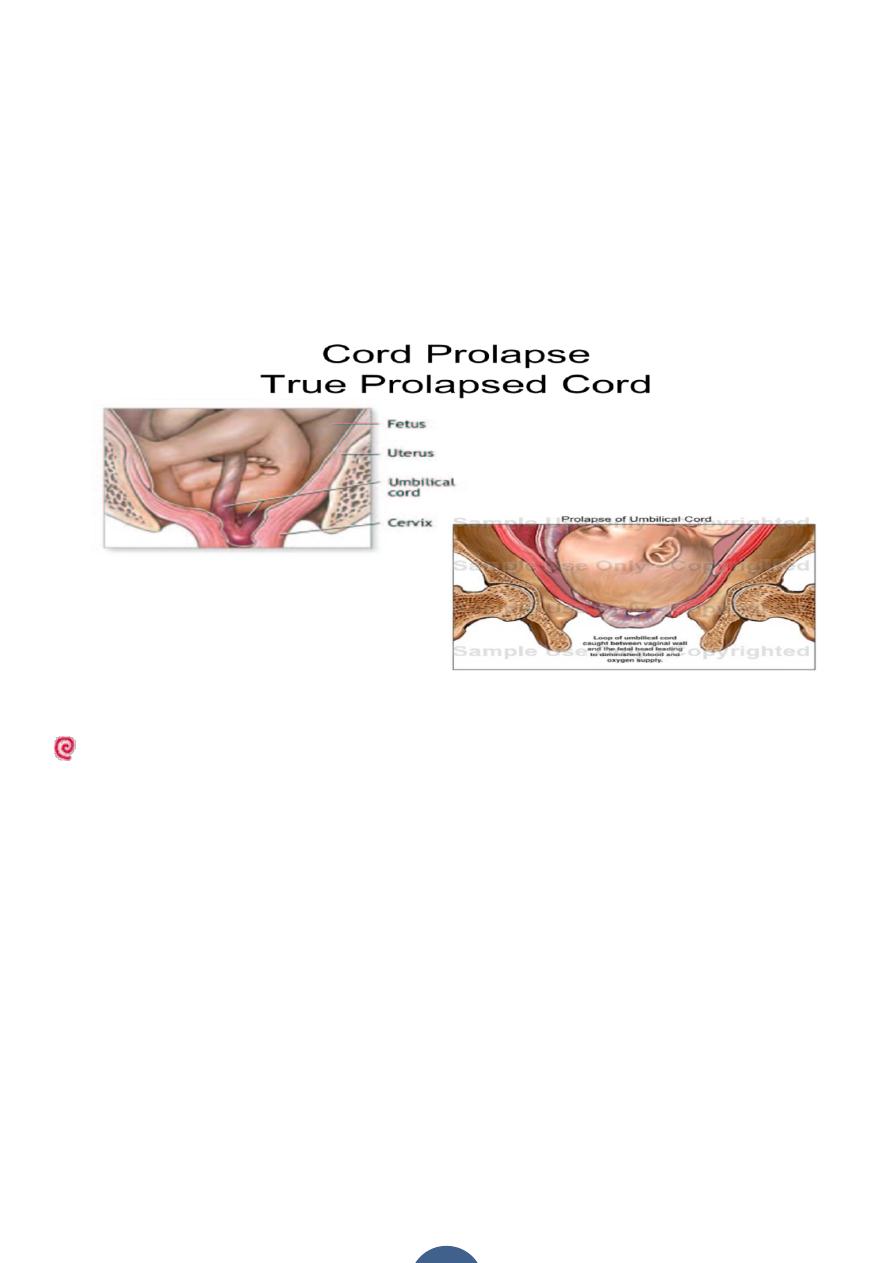
1.Cord presentation – cord is slipped down below the presenting part when the
membrane is intact.
2.Cord prolapse – cord is slipped below the presenting part inside the vagina or
even outside the vulva following rupture of membranes.
Incidence:
The overall incidence of cord prolapse is1:500 deliveries&occurs when the fetal
presenting part dose not fit well into the maternal pelvis, giving space for the
cord to prolapse when the membranes rupture.
What are the risk factors for cord prolapse?
Maternal causes: -Pelvic tumours(fibroid)
Narrow pelvis
Fetal causes: -Malpresentation(breech , transverse)
Multiple pregnancy
Polyhydramnios
Placenta previa
Large baby.
CORD PROLAPSE/PRESENTATION
Diagnosis:
Cord presentation – by feeling the pulsation of cord through an intact
membrane.
Cord prolapse -:
1.by seeing cord at the introitus or can be felt during vaginal examination &it will
be pulsating if the fetus is alive.
-
Fetus may be alive even in the absence of cord pulsation, therefore USG should
be done to determine cardiac movement.
2.An abnormal fetal heart rate pattern may suggest it because compression of the
umbilical vein between the presenting part& the pelvis, reduces or stops the
flow of oxygenated blood to the fetus causing deep variable
deceleration ,thenbradycardia if the situation not relieved.
Management :Rapid Response to Prolapse
-
Assess fetal status (FHTs, ultrasound)&call for help
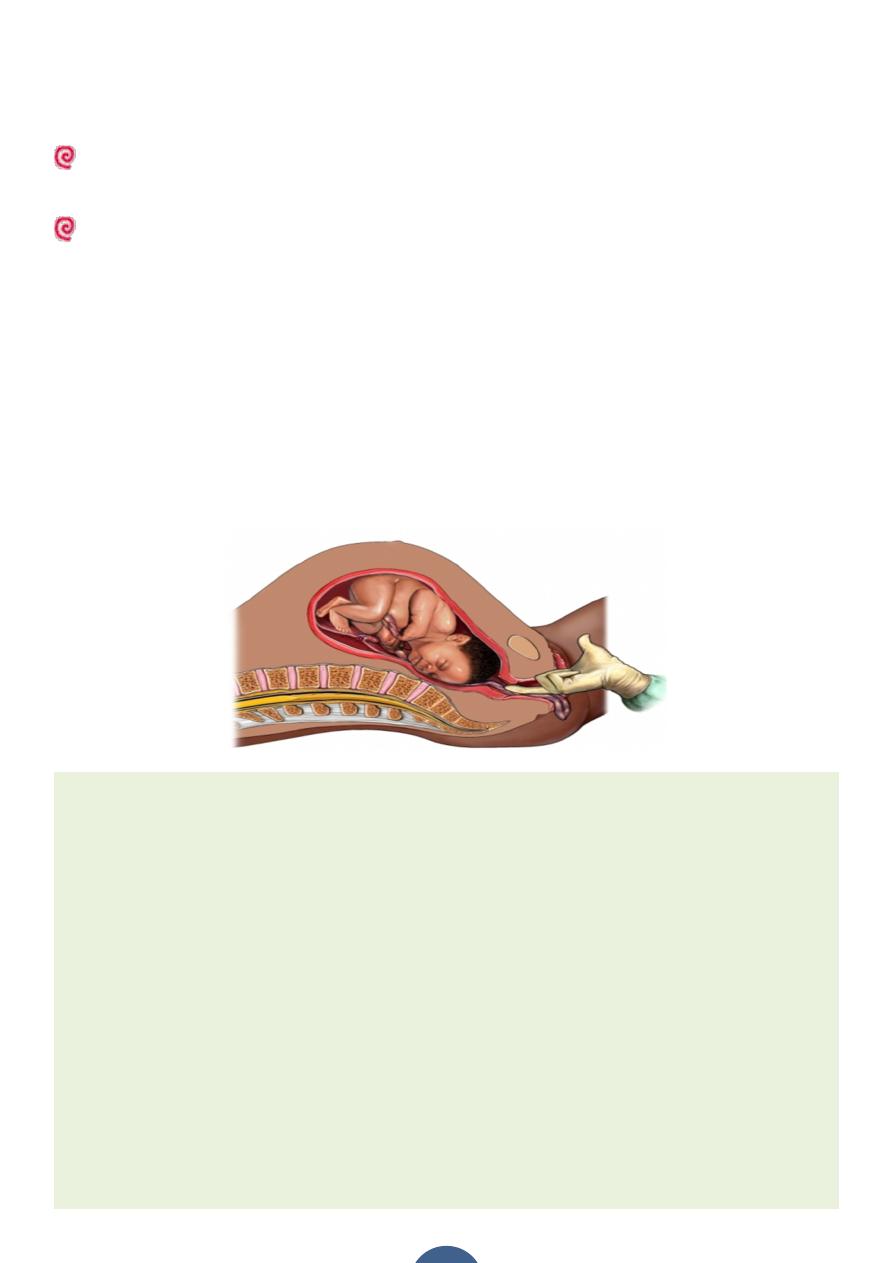
- If the cord is beyond the introitus it should be replaced into the vagina to keep
it warm but there should be minimal handling of the cord as this causes spasm &
worsen blood flow ,or cover it by warm wet towel.
-
Immedite management aims to minimize the pressure of the presenting part on
cord while plans are made to deliver the baby &this is achieved by:-
1)Applying pressure vaginally to push the presenting part out of the pelvis.
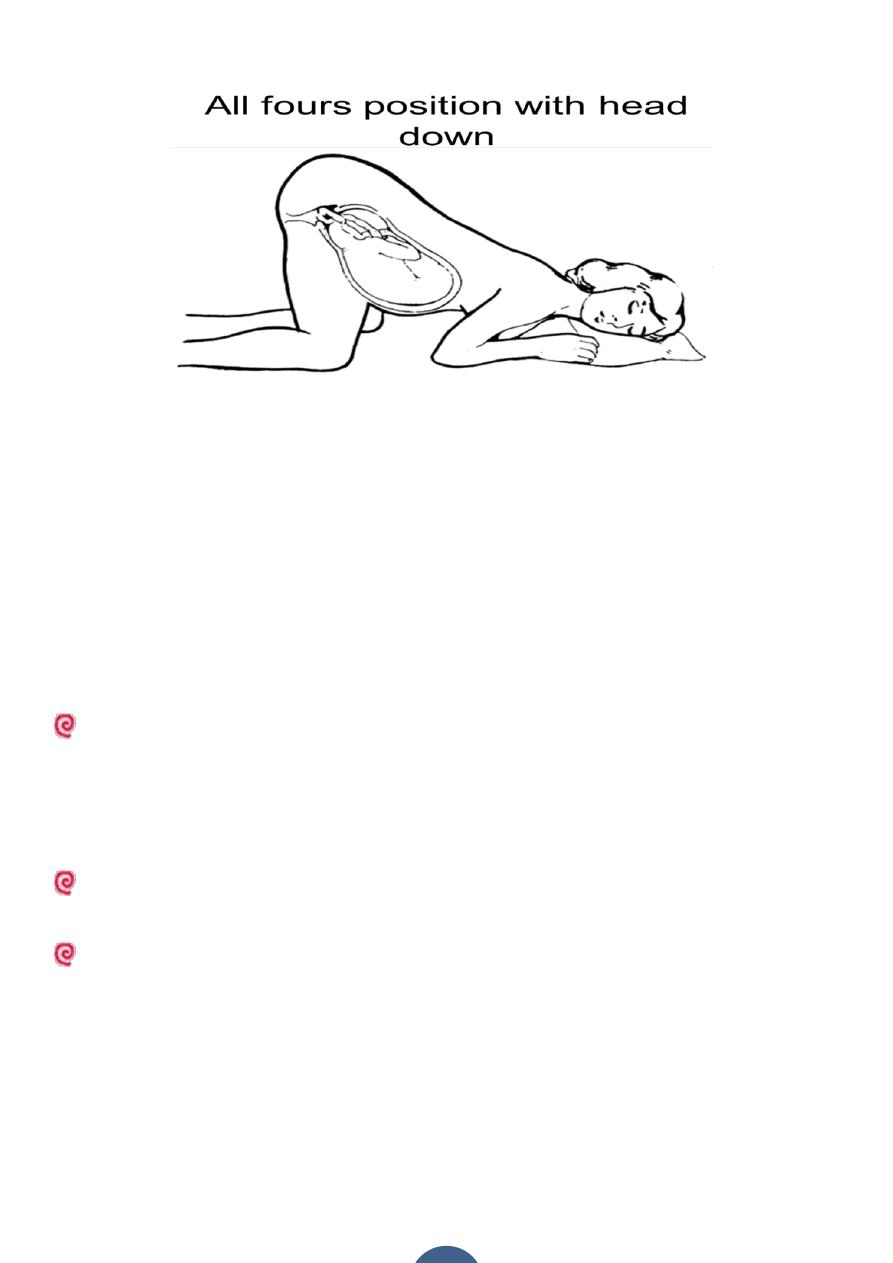
2)Position change (Trendelenburg, Knee-chest)
3)Filling the bladder with 500ml of saline with Foley catheter.
Delivery– :
1.Mode of delivery depends on-:
a)baby living or dead.
b)maturity of the baby.
c) dilatation of the cervix &station.
2.Emergency caesarean section is the best choice if the baby is alive unless the
cervix is fully dilated & an assisted vaginal delivery (forceps or vacuum) can be
safely & easily performed .
If the baby is dead labour should be allowed to continue vaginally if there is no
other contraindications to it like transverse lie , contracted pelvis,…..etc .
Prognosis:
Fetal outcome depends upon the gestation , other complicating factors, & for
how long the cord has been compressed .
Total cord compression for longer than 10 min. will cause cerebral damage & if
continued for arround 20 min. death will occur.These times will be shorter in a
fetus that is already compromised for reasons such as prematurity or fetal
growth restriction.