


Lec.3
Pediatrics
6
th
stage
2016/8/23
Session notes
د.ربيع الدبوني
General notes :
Palpitation : never mention in the history " palpitation " because it
is subjective ( it is feeling by the patient him/herself )
Feeding Hx :
Ask about any new introduction of unmodified cow's milk ?
Convlusion is pyrmidal tract in origin
While occulogyric crisis is extra-pyramidal origin
When Examine patient pericordium and listen to the heart sound
And check for arrythmia , but there is no any abnormal finding , we can
send him for ECHO to search if there is cardiomegaly
Periodic breathing
:
occurs when the breath pause for up to 10 seconds at time, there may
be several such pauses close together, followed by series of rapid
shallow breaths, then breathing returns to normal.
This is common condition in premature babies in first few weeks of life.
Even healthy full term babies sometimes spells periodic breathing,
usually after sleeping deeply.
Home care: supine position, avoid soft pillows and smoking, never snake
your baby to breath brain injury

CVS notes
On exam :
Apical pulse:
o Apex beat outermost, lowermost visible or palpable to the right or
left
o If you don’t find the pulsation ; look at the axilla (left side), if you still
don’t find the pulsation ; see the right side (dextrocardia)
o Causes of absent apex beat: obesity, thick chest wall, pericardial
effusion, dextro
regions in auscultation:
o Mitral (Apex) area : 4th left ICS in mid-clavicular line or 5th ICS in older
child
o Aortic area : 2nd ICS right to the sternum
o Pulmonary area : 2nd ICS left to the sternum
o Tricuspid area : left sternal border in 4th ICS or 5th ICS in older child
Coarctation of aorta is characterised by the following features
Usually seen in male patient and they presents with headache,
claudication, palpitation, anginal pain or cold extremities.
The upper extremity and thorax may be more developed
compared to lower extremities.
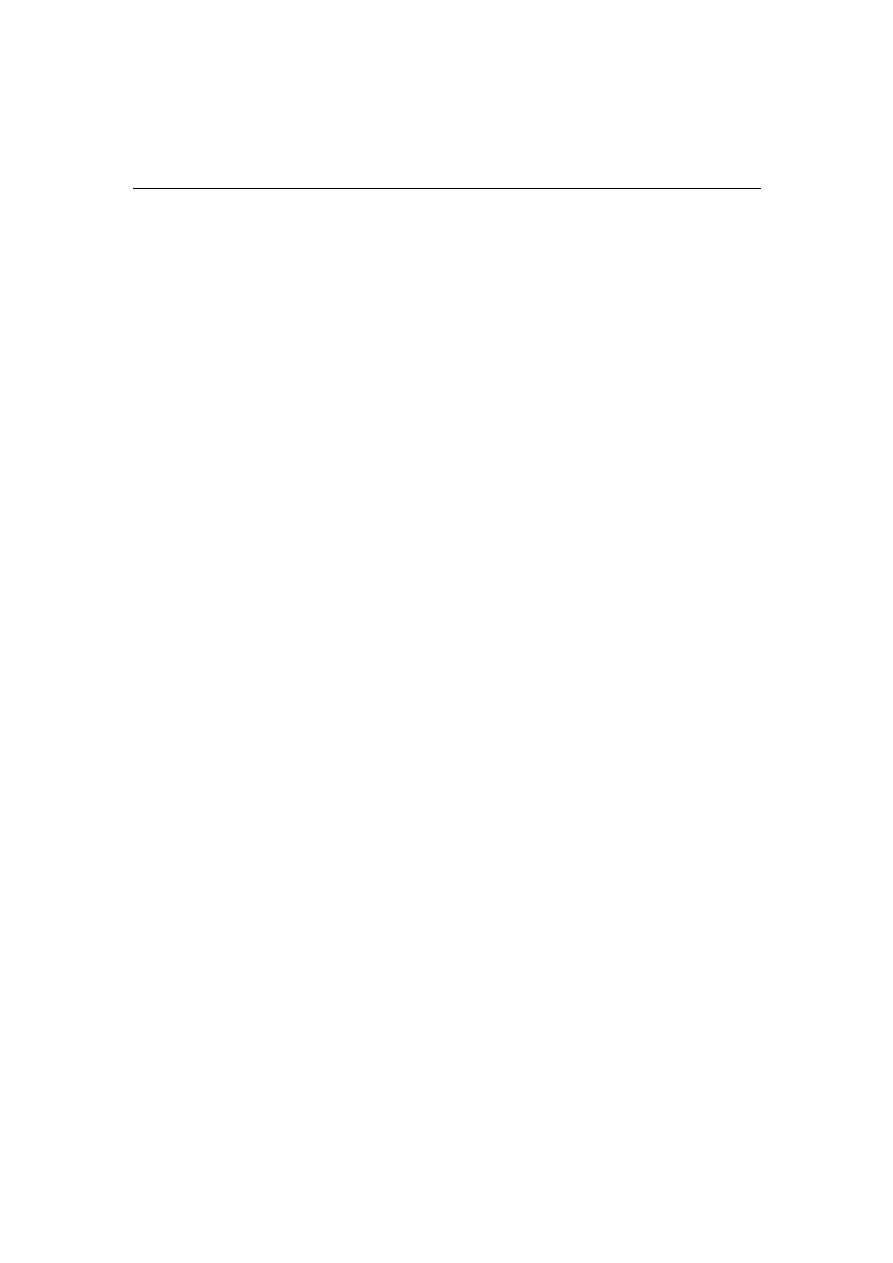
Radiofemoral delay is present .
All the peripheral pulses shoud be examined carefully
Prominent suprasternal and carotid pulsations are present

Collateral pulsation may be seen and felt over the axilla .trunk and
infrascapular areas.This is clled as Suzmans sign and is best
elicited with patient bending forwad with arms hanging by the
side of the body
Systemic hypertension.
Bruit over the collaterals.
Left ventricular type of cardiac enlargement and heaving apex is
seen.
A systolic murmur may be heard over the anterior chest and
back.Continuous murmur is heard over the collaterals
Clinical association of coarctation are :
Bicuspid aortic valve
Turners syndrome
Berry aneurysm
Polycystic kidney
Radio radial delay :
To detect the radioradial delay you should simultaneously palpate both
the radial arteries by both your hands, using your left hand for patients
right radial artery and vice versa
Normal situation radial and femoral pulsations are felt equally and
synchronously.The inequality between two radial pulses is known
as Radio radial delay.The delay between the radial pulse and femoral
pulse is called as Radiofemoral delay.
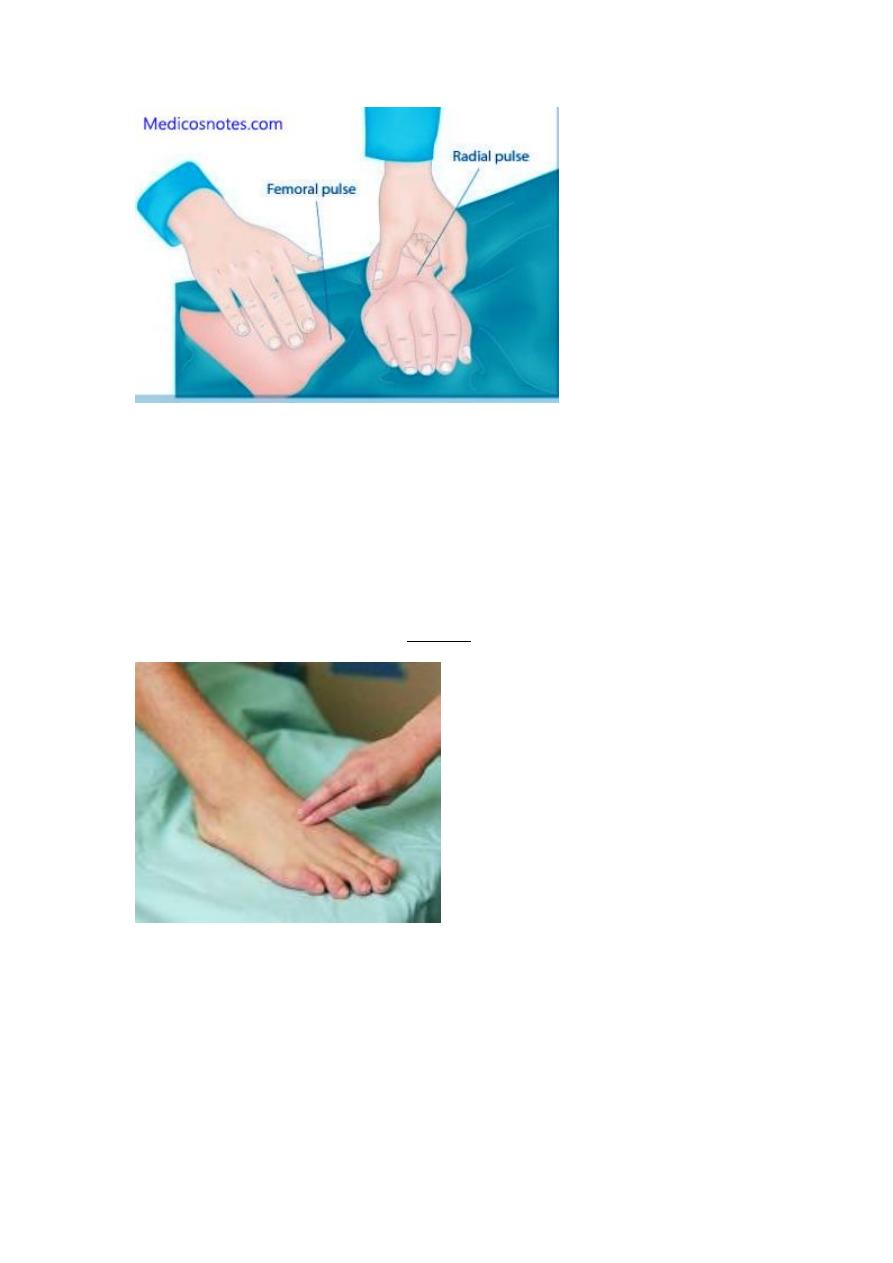
Dorsalis pedis exam :
the pulse of the dorsalis pedis artery, palpable at the prominent arch of t
he top of the foot between the first and secondmetatarsal bones. It can
be felt in approximately 90% of people.
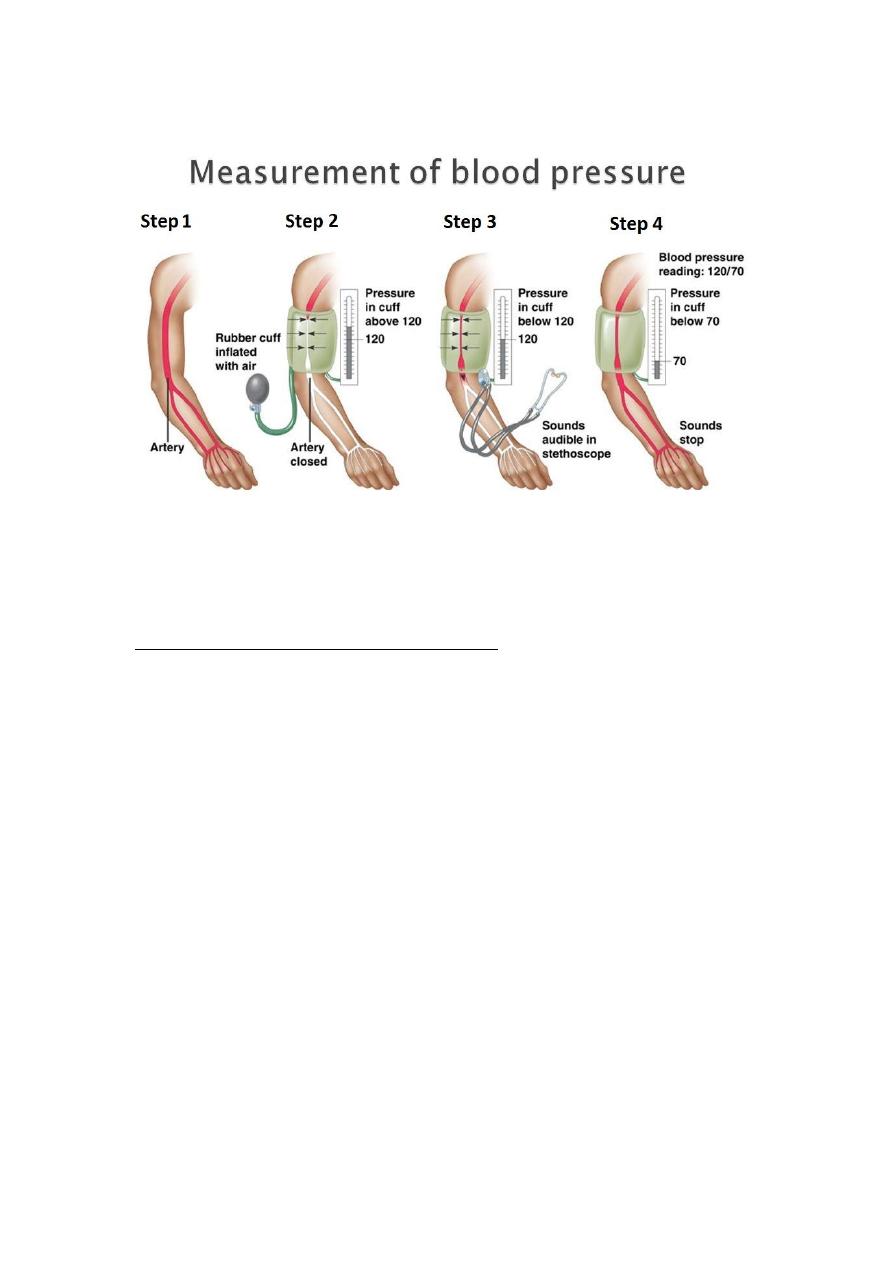
Blood pressure measurement :
Flush method :
Flush technique for obtaining pediatric BP:
Used in infants or very young children where lack of cooperation
precludes use of auscultation and palpation to determine BP
The flush technique allows for a value lying between the systolic
and diastolic to be determined
with the cuff in place, an elastic bandage is wrapped around the
elevated arm
Proceeding from the fingers to the anticubital space emptying of
the capillaries and venous network occurs
The cuff is now inflated to a pressure above the expected systolic
reading
the bandage is removed
the now pallid arm is placed at the patient’s side
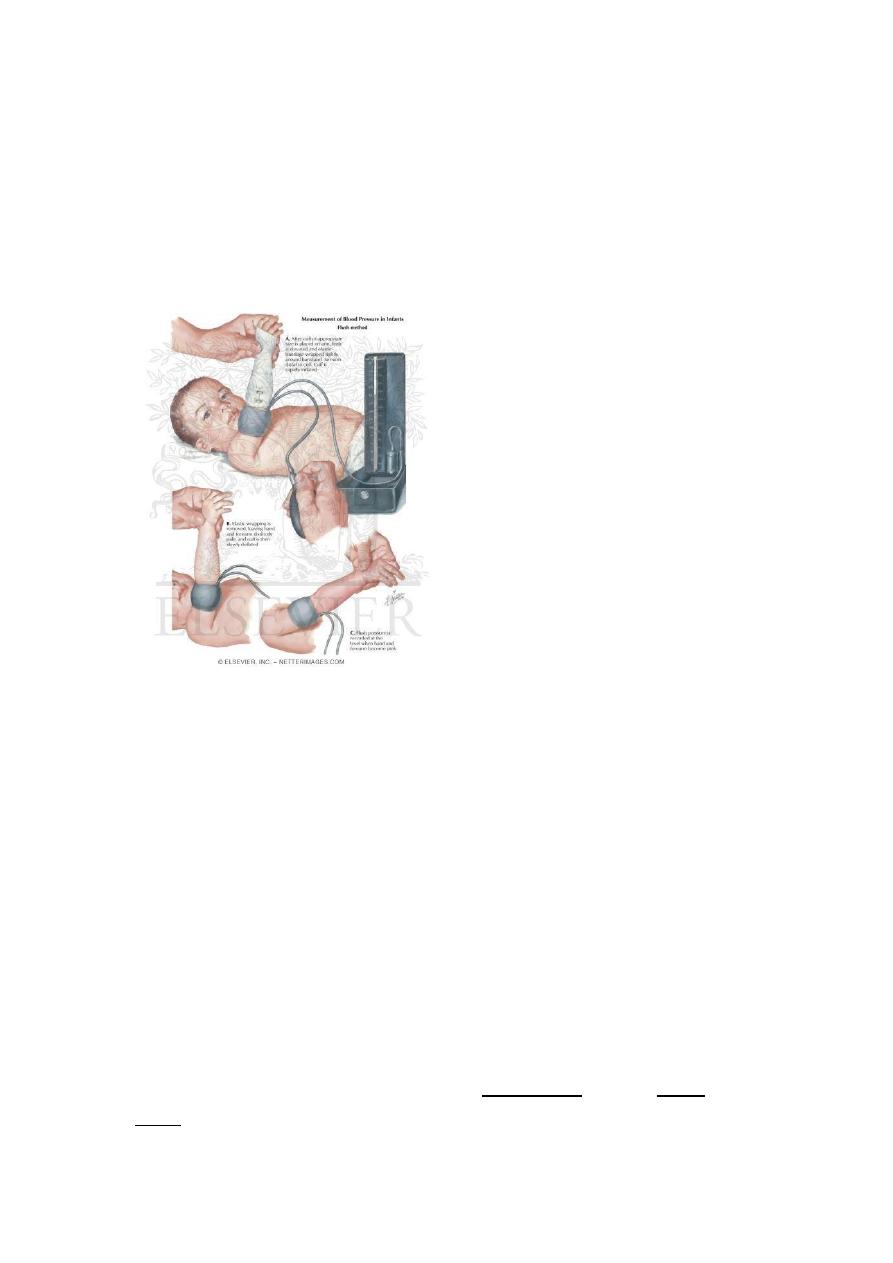
the pressure is allowed to fall slowly until the sudden flush of
normal colour returns to forearm, hand and fingers.
The endpoint is strikingly clear
This method may also be used on the thigh
First check for brachial blood pressure it is audible or not by the
stethoscope then check for the radial pulse it is palpable or not if neither
brachial or radial pulse felt now you can change to the Flush meyod
Pulsus deficit :
a condition in which a peripheral pulse rate is less than the ventricular co
ntraction rate as auscultated at the apex of theheart or seen on the elect
rocardiogram, indicating a lack of peripheral perfusion.
pulse deficit the difference between the apical pulse and the radial
pulse, obtained by having one person count theapical pulse as heard thr
ough a stethoscope over the heart and a second person count the radial
pulse at the same time.
Exam the gentalia :
Check for any ambigious gentalia , imperforated anus
Exam the back
Exam the skin : for any neurocutaneous disease ; eg: neurofibromatosis
Tuberus sclerosis
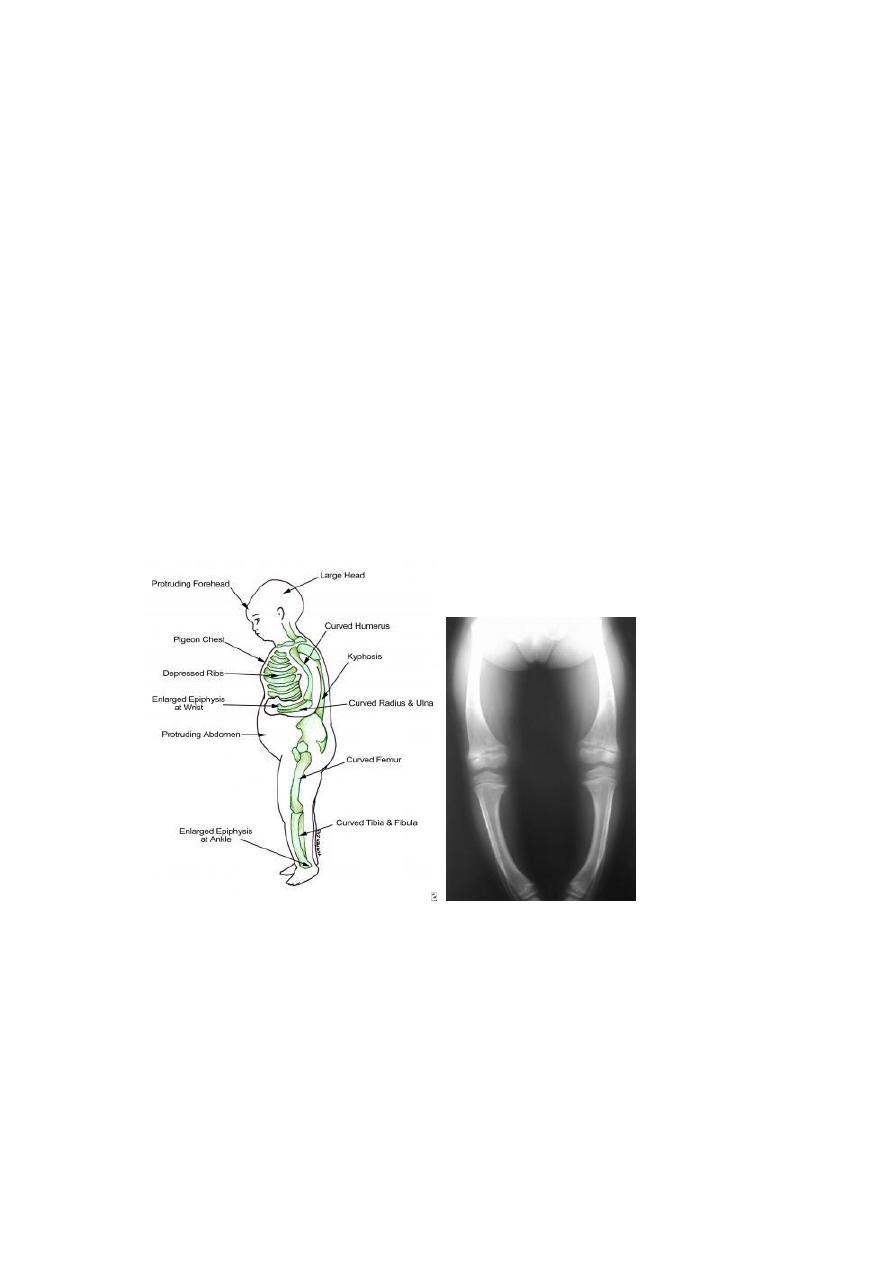
Rickets :
Serum measurements in the workup for rickets may include the
following:
Calcium
Phosphorus
Alkaline phosphatase
Parathyroid hormone
25-hydroxy vitamin D
1,25-dihydroxyvitamin D
Early on in the course of rickets, the calcium (ionized fraction) is low.
However, this level is often within the reference range at the time of
diagnosis, as a consequence of increased parathyroid hormone
secretion.
Although calcidiol (25-hydroxy vitamin D) is low and parathyroid
hormone is elevated, determining calcidiol and parathyroid hormone
levels is typically not necessary in order to establish a diagnosis.
Calcitriol levels maybe normal or elevated because of increased
parathyroid activity.
The phosphorus level is invariably low for age, unless recent partial
treatment or recent exposure to sunlight has occurred. Alkaline
phosphatase levels are uniformly elevated.
A generalized aminoaciduria occurs from the parathyroid activity.
However, aminoaciduria does not occur in familial hypophosphatemia
rickets (FHR).
Treatment
Children with nutritional vitamin D deficiency should receive vitamin D
and adequate nutritional intake of calcium and phosphorus. There are 2
strategies for administration of vitamin D. With stoss therapy, 300,000-
600,000 IU of vitamin D are administered orally or intramuscularly as 2-4
doses over 1 day. Because the doses are observed, stoss therapy is ideal
in situations where adherence to therapy is questionable. The

alternative is daily, high-dose vitamin D, with doses ranging from 2,000-
5,000 IU/day over 4-6 wk. Either strategy should be followed by daily
vitamin D intake of 400 IU/day if 1 yr, typically given as a multivitamin
Most sensitive alkaline phosphatse enzemye the first one is affeted
And the last improved if it is become normal after treatment
So rickets due to vit.d deficiency if not return to normal
Rickets may be due to :
1-vit.D resistant
2-congenital hypophosphatemia
3-renal tubular acidosis
SHORT STATURE :
Constitutional growth delay: This condition describes children who are
small for their ages but who are growing at a normal rate. They usually
have a delayed "bone age," which means that their skeletal maturation
is younger than their age in years. (Bone age is measured by taking an X-
ray of the hand and wrist and comparing it with standard X-ray findings
seen in kids the same age.)
These children don't have any signs or symptoms of diseases that affect
growth. They tend to reach puberty later than their peers do, with delay
in the onset of sexual development and the pubertal growth spurt. But
because they continue to grow until an older age, they tend to catch up
to their peers when they reach adult height. One or both parents or
other close relatives often had a similar "late-bloomer" growth pattern.
Familial (or genetic) short stature: This is a condition in which shorter
parents tend to have shorter children. This term applies to short children
who don't have any symptoms of diseases that affect their growth. Kids
with familial short stature still have growth spurts and enter puberty at

normal ages, but they usually will only reach a height similar to that of
their parents.
With both constitutional growth delay and familial short stature, kids
and families need to be reassured that the child does not have a disease
or medical condition that poses a threat to health or that requires
treatment.
However, because they may be short or may not enter puberty when
their classmates do, some may need extra help coping with teasing or
reassurance that they will go through full sexual development
eventually. In a few children who are very short or very late entering
puberty, hormone treatment may be helpful.
Diseases of the kidneys, heart, gastrointestinal tract, lungs, bones, or
other body systems might affect growth. Other symptoms or physical
signs in kids with these illnesses usually give clues as to the disease
causing the growth delay. However, poor growth can be the first sign of
a problem in some.
Growth disorders include:
Failure to thrive : which isn't a specific growth disorder itself, but can be
a sign of an underlying condition causing growth problems. Although it's
common for newborns to lose a little weight in the first few days, failure
to thrive is a condition in which some infants continue to show slower-
than-expected weight gain and growth. Usually caused by inadequate
nutrition or a feeding problem, it's most common in kids younger than
age 3. It may also be a symptom of another problem, such as
an infection, a digestive problem, or child neglect or abuse.
Endocrine diseases : (diseases involving hormones, the chemical
messengers of the body) involve a deficiency or excess of hormones and
can be responsible for growth failure during childhood and adolescence.
Growth hormone deficiency is a disorder that involves the pituitary
gland (the small gland at the base of the brain that secretes several
hormones, including growth hormone). A damaged or malfunctioning
pituitary gland may not produce enough hormones for normal growth.
Hypothyroidism is a condition in which the thyroid gland fails to make
enough thyroid hormone, which is essential for normal bone growth.
Occipitofrontal circumferance of the head :
OFC ratio
Increased by (no.)
cm
Age
93
4
2 months
44
9
4 months
44
4
6 months
44
1
8 months
44
1
10 months
44
1
12 months
2.5
2 year
1/2
3-7 year
1/3
8-12 year
Hypocalcemia cauesd by SOB :
Hyperventilation syndrome often occurs under stressful conditions
which cause hypocapnia and consequently results in respiratory alkalosis
and a wide range of somatic symptoms. Respiratory alkalosis can induce
secondary hypocalcaemia that may cause cardiac arrhythmias,
conduction abnormalities and various somatic symptoms such as
paraesthesia, hyperreflexia, convulsive disorders, muscle spasm and

tetany . Acute hypocalcaemia is an emergency that requires prompt
attention and management.
Difference between modified and unmodified cow's milk ?
Unmodified cows milk:
o Contain protein 4% (human milk 1%) so it lead to exhaustion of liver
and kidney.
o Much higher sodium than breast milk hypernatremic dehydration.
o Higher phosphorus chelate calcium lead to convulsion.
Unmodified cows milk not give to baby less than one year age but
modified cow milk
suitable from birth.
Water, solids, calories, fat same level in human and cow milk.
Modified cows milk is cow milk with less protein and sodium and
phosphorus and
contain oils to prevent calories deficiency.
Modified and fortified milk is modified milk with vitamins and minerals.