د. ليث نايف
Treatment of acute intestinal obstruction:Principles of treatment of I.O. are;
-Gastro intestinal drainage
-Fluid& electrolyte replacement
-Relief of obstruction
Supportive treatment
-NG decompression by NGT to decompress bowel proximal to the obstruction& to reduce risk of aspiration during anesthesia-Fluid replacement best by hartmans solution or NS
-Antibiotic is not mandatory to all patients but it is so for all patients undergoing small or large bowel resection
Surgical treatment
The classic clinical advice ((the sun should not both rise &set on a case of unrelieved I.O.)) should be followed unless there are reasons for delay, such a case may include I.O. secondary to adhesions where there is no pain or tenderness under these circumstances, conservative management may be continued for up to 72 hours in the hope of spontaneous resolutionThe indications of early operation are;
-obstructed or strangulated external hernia-internal intestinal strangulation
-acute obstruction
Operative assessment is directed to;
-Site of obstruction
-Nature of obstruction
-Viability of the gut
In the operation firstly identify &asses the caecum, if it is collapsed, the lesion in the small bowel while a dilated caecum indicates large bowel obstruction.
The type of surgical procedure required will depend upon the nature of the cases, it may be:
-division of adhesions (enterolysis)
-Excision
-Bypass
-Proximal decompression
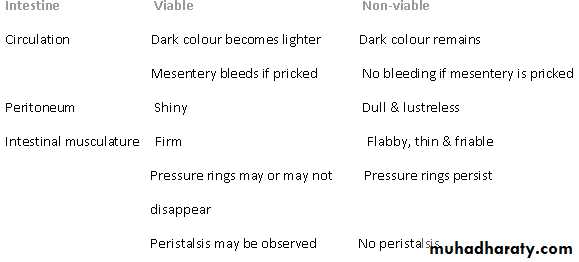
The viability of the involved bowel should be carefully assessed. If in doubt, the bowel should be wrapped in hot packs for 10 minutes with increased oxygenation & reassessed.
Differentiation between viable and non-viable intestine
Large bowel obstruction
Usually due to underlying carcinoma or diverticular disease, it is either acute or chronic. The condition of pseudo-obstruction should always be considered& excluded by limited contrast study or CT scanAfter full resuscitation laparotomy should be done.
Distension of the caecum will confirm the diagnosis of large bowel obstruction identification of distal collapsed segment will lead to identification of the cause.
-If removable lesion in the caecum, ascending colon hepatic flexure or proximal transverse colon, then right hemicolectomy should be performed.
-If the lesion is irremovable; proximal stoma or ileotransverse bypass.
-If the lesion at the splenic flexure, it should be treated by extended Rt. hemicolectomy with ileo-desending colonic anastomosis.
-If the lesion in the left colon or recto-sigmoid junction; immediate resection should be done except when:
-Inexperienced surgeon -Moribund patient
-Advanced disease
The proximal end of the colon will be brought to the surface as a colostomy
In the majority the distal end of the bowel will be closed & returned to the abdomen (hartmann's procedure). A second stage colorectal anastomosis can be planned when the patient is fit.
If an anastomosis is to be considered in the presence of obstruction, the colon must be decompressed and cleaned by an on-table colonic lavage.
Nevertheless the subsequent anastomosis should still be protected with a covering stoma.
Obstruction by adhesions & bands Adhesions
Adhesions & bands are the most common cause of intestinal obstruction following abdominal operationsAny source of peritoneal irritation results in local fibrin production which produces adhesion between opposed surfaces. Early fibrinous adhesion may disappear when the cause is removed or they may become vascularised & replaced by mature fibrous tissue.
The common causes of intra-abdominal adhesions are:
Ischaemic area: site of anastomosis, trauma, vascular occlusion
Foreign materials; talc, gauze, silk
Infection; peritonitis, TB
Inflammatory conditions; crohns
Radiation enteritis
Drugs; practolol
Prevention of adhesion formation:
-Good surgical technique
-Washing of peritoneal cavity with saline to remove clot etc.
-Minimising contact with gauze
-Covering anastomosis &raw peritoneal surfaces
Bands
-congenital; ex: obliterated vitello-intestinal duct
-a string band following previous bacterial peritonitis
-a portion of greater omentum usually adherent to the parietes
Treatment
Initial treatment is by I.V. rehydration& NG decompression, some time it is curative. Conservative treatment should not be more than 72 hours, otherwise laparotomy is required. There will be multiple adhesions but only one may be causative, these should be divided &the remaining left in situ because their division will only cause further adhesion formation. Following release of band obstruction, the constriction sites should be carefully assessed & if they show residual colour changes, invaginated.
Post operative I.O
-Early postoperative obstruction (day 1-5) is usually due to non-strangulating causes such as fibrinous adhesions& oedema. Obstruction is usually incomplete& majority improved with conservative management.-Late postoperative obstruction (more than 7 days) is usually more significant in nature& timely surgical intervention is usually required.
Special type of I.O.
Internal herniaOccur when portion of small intestine become entrapped in one of the retroperitoneal fossae or in a congenital mesenteric defect
-Foramen of Winslow
-A hole in the mesentry
-Defects in the transverse mesocolon
-Defects in the broad ligament
-Congenital or acquired diaphragmatic hernia
-Duodenal retroperitoneal fossae
-Caecal/appendicular retroperitoneal fossae
-Inter-sigmoid fossae
The standard treatment for a hernia is to release the constricting agent by division
Obstruction from enteric stricture
Small bowel stricture usually occurs in case of TB, crohns, lymphoma &rarely carcinoma & sarcoma. Presentation usually subacute or chronic. Standard surgical treatment is by resection & anastomosisBolus obstruction
May be caused by; food, gallstones, trichobezoar, phytobezoar, stercoliths &worms.
Gallstones; tend to occur in an elderly secondary to erosion of large gallstone through the gallbladder into the duodenum, classically it impacts about 60cm proximal to the ileocaecal valve. Diagnosis usually radiologically will show evidence of small bowel obstruction with diagnostic of air-fluid in the biliary tree. The stone may or may not be visible. Treatment by laparotomy, it may be possible to crush the stone within the bowel lumen or by opening the bowel &remove the stone.
Food; bolus obstruction may occurs after partial or total gastrectomy.
Trichobezoar& phytobezoar; these are firm masses of undigested hair bolus& fruits/vegetables fibre respectively.Treatment by laprotomy if possible the lesion may be squeezed into the caecum, otherwise open removal is required.
Stercoliths; usually found in the jejunal diverticlum or ileal stricture.
Worms; ascares lumbricoides may cause low small bowel obstruction especially in children. An attack follows initiation of anti helminthic therapy. If the worms are not seen in the stool or vomitus, the diagnosis may be indicated by oesinophilia or the sight of worms within gas-filled small bowel loop on a plain radiograph.
Treatment by laprotomy the worm squeezed into the caecum if not should be removed.
Acute intussusception
This occurs when one part of the gut become invaginated within adjacent segment, invariably it is the proximal into the distal bowel.Aetiology:
The condition most common in children in whom it occurs in an idiopathic (peak incidence at 3-9 months) and an associated illness such as gastroenteritis or UTI is found in 30%.It is believed that hyperplasia of peyer's patches in the terminal ileum may be the initiating event which may occur secondary to weaning.
Children with intussusception associated with a lead point such as Meckel's diverticulum, polyps, Henoch-Schonlein purpura or appendix are usually older than those with idiopathic disease.
In adult cases are invariably associated with a lead point which is usually polyps, submucosal lipoma or tumor.
Pathology:
It is composed of three parts;
-Entering or inner tube (intussusceptum)
-Returning or middle tube
-Sheath or outer tube (intussuscepiens)
It is an example of strangulating obstruction as the blood supply of inner layer is usually impaired. It may be ilecacal, ileocolic (77%), colocolic or retrograde.
Clinical features:
Presentation in child is classical, fit &well male child of 6 months develops sudden onset of screaming associated with drawing up of the legs. The attack lasts for few minutes& recurs every 15 minutes & become progressively sever.During attacks the child has facial pallor while between episodes he is listless and drawn.Vomiting may occur and becomes conspicuous with time. Initially the stool may be normal while later blood &mucus are evacuated (red current jelly stool).
O/E: Lump is present in 50-60%, may be associated with feeling of emptiness in the RIF. (Sign of dance).On rectal examination the blood stained mucus on finger.
Occasionally in extensive ileocolic or colocolic, the apex may be palpable or even protrude from the anus.
Unrelieved, the pain will become continuous with abdominal distension and profound vomiting lead to intestinal obstruction or peritonitis secondary to gangrene.
Radiology: Evidence of small or large bowel obstruction, absent caecal gas shadow. Barium enema may be used to diagnose ileocolic or colocolic (the claw sign).Barium enema may be used to reduce an infant intussusception, but it is contraindicated in presence of obstruction, peritonism or prlong history (more than 48 hrs), it is successful in 50%.
C.T. scan reveal the presence of small bowel mass in ileo ileal type.
Differential diagnosis:
-Acute enterocollitis (diarrhea)Henoch-schoenlein purpura (rash &abdominal pain)-
-Rectal prolapse (projecting mucosa can be felt in continuity with the perineal skin) where in intussusception the finger may pass indefinitely into the depths of a sulcas.
Operative management
This is required when hydrostatic reduction has failed or is contraindicated
After preoperative resuscitation by NG decompression & IV rehydration, laparotomy done, reduction by squeezing the most distal part of the mass in a cephalad direction