Browse’s Introduction to
The Symptoms and Signs
of Surgical Disease
Fourth edition
NORMAN L. BROWSE
Kt, MD, FRCS, FRCP
Professor of Surgery, Emeritus, University of London, UK
Honorary Consulting Surgeon, St Thomas’ Hospital, London, UK
Formerly, Chairman, London University
MBBS
and
MS
Examiners
Formerly, Member of Court of Examiners, Royal College of Surgeons of England, UK
Formerly, Member of Council and Chairman of Examinations Committee and
Academic Board, Royal College of Surgeons of England, UK
Past President, Royal College of Surgeons of England, UK
JOHN BLACK
MD, FRCS
Consultant Surgeon, Worcestershire Royal Hospital, UK
Member of Council, Royal College of Surgeons of England, UK
Examiner, Intercollegiate Board in General Surgery, UK
KEVIN G. BURNAND
MS, FRCS, MBBS
Professor of Vascular Surgery and Chairman of the Academic Department of Surgery
and Anaesthesia in the Cardiovascular Divison of King’s College at the St Thomas’ Campus,
University of London, UK
Honorary Consultant Surgeon to Guy’s and St Thomas’ Foundation Trust, London, UK
WILLIAM E.G. THOMAS
MS, FRCS
Consultant Surgeon and Clinical Director, Sheffield Teaching Hospitals Trust
Member of Council, Royal College of Surgeons of England, UK
Formerly, Member of Court of Examiners, Royal College of Surgeons of England and
Panel of Examiners for the Intercollegiate Board in General Surgery, UK
Sponsored by AstraZeneca PLC
with Hodder Arnold
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page i

CRC Press
Taylor & Francis Group
6000 Broken Sound Parkway NW, Suite 300
Boca Raton, FL 33487-2742
© 2005 by Taylor & Francis Group, LLC
CRC Press is an imprint of Taylor & Francis Group, an Informa business
No claim to original U.S. Government works
Printed on acid-free paper
Version Date: 20140805
International Standard Book Number-13: 978-0-340-81571-7 (Pack - Book and Ebook) 978-0-340-81579-3 (Paperback)
This book contains information obtained from authentic and highly regarded sources. While all reasonable efforts have been made to
publish reliable data and information, neither the author[s] nor the publisher can accept any legal responsibility or liability for any errors
or omissions that may be made. The publishers wish to make clear that any views or opinions expressed in this book by individual editors,
authors or contributors are personal to them and do not necessarily reflect the views/opinions of the publishers. The information or guid-
ance contained in this book is intended for use by medical, scientific or health-care professionals and is provided strictly as a supplement
to the medical or other professional’s own judgement, their knowledge of the patient’s medical history, relevant manufacturer’s instruc-
tions and the appropriate best practice guidelines. Because of the rapid advances in medical science, any information or advice on dosages,
procedures or diagnoses should be independently verified. The reader is strongly urged to consult the relevant national drug formulary and
the drug companies’ printed instructions, and their websites, before administering any of the drugs recommended in this book. This book
does not indicate whether a particular treatment is appropriate or suitable for a particular individual. Ultimately it is the sole responsibility
of the medical professional to make his or her own professional judgements, so as to advise and treat patients appropriately. The authors
and publishers have also attempted to trace the copyright holders of all material reproduced in this publication and apologize to copyright
holders if permission to publish in this form has not been obtained. If any copyright material has not been acknowledged please write and
let us know so we may rectify in any future reprint.
Except as permitted under U.S. Copyright Law, no part of this book may be reprinted, reproduced, transmitted, or utilized in any form by
any electronic, mechanical, or other means, now known or hereafter invented, including photocopying, microfilming, and recording, or in
any information storage or retrieval system, without written permission from the publishers.
For permission to photocopy or use material electronically from this work, please access www.copyright.com (http://www.copyright.
com/) or contact the Copyright Clearance Center, Inc. (CCC), 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400. CCC is a not-for-
profit organization that provides licenses and registration for a variety of users. For organizations that have been granted a photocopy
license by the CCC, a separate system of payment has been arranged.
Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification and
explanation without intent to infringe.
Visit the Taylor & Francis Web site at
http://www.taylorandfrancis.com
and the CRC Press Web site at
http://www.crcpress.com
BookPower (formerly ELST) is a registered charity which makes available low-priced,
unabridged editions of British publishers’ textbooks to students in developing countries.
BookPower is grateful to the many individuals, trusts and organisations which have
provided funding to cover the costs of its operation. These include:
The Arimathea Charitable Trust
The PJK Charitable Trust
The Peter Courtauld Charitable Trust
The Rolfe Charitable Trust
The Ros Pilcher Charitable Trust
The Tanner Trust
Below is a list of some other medical books published under the BookPower imprint:
Crook
Clinical Chemistry and Metabolic Medicine
Hodder Arnold
Holt and Kumar
ABC of Diabetes
Wiley Blackwell
Houghton and Gray
Chamberlain’s Symptoms and Signs in Clinical Medicine
Hodder Arnold
Leppard
An Atlas of African Dermatology
Radcliffe Medical Press
McMinn
The Concise Handbook of Human Anatomy
Manson
Pallister and Watson
Haematology
Scion Publishing
Rogstad
ABC of Sexually Transmitted Infections
Wiley Blackwell
Strobel et al
The Great Ormond Street Colour Handbook of Paediatrics and Child Health
Manson Publishing
Truswell
ABC of Nutrition
BMJ Books
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page iii
We dedicate this book to all those who have supported
us thoughout our clinical careers:
Our wives,
families,
consultant colleagues,
registrars and house officers,
nurses in the wards, outpatients and operating rooms,
secretaries and laboratory staff,
but, above all,
our patients.
Without the support of everyone mentioned above, it would have been
impossible to write this book.
Acknowledgements
The advice and contributions of many surgical
colleagues throughout the UK to previous editions
have already been acknowledged but they are
still part of the substance of this edition. Added to
this group must be Dr Jane Terris, Consultant in
A&E Medicine, Dr Elizabeth Graham, Consultant in
Medical Ophthalmology and Mr Kieran Healey,
Consultant Plastic Surgeon, all of St Thomas’ Hospi-
tal, who gave valuable advice on Chapters 2 and 3,
and Mr David Douglas, Consultant Orthopaedic
Surgeon, Sheffield Teaching Hospitals NHS Founda-
tion Trust, who advised on Chapter 4.
In these days of word processors and computers,
much of the secretarial work has been done by the
four editors themselves, at home, but we are most
grateful for the secretarial assistance of Elizabeth
Webb and Patricia Webb of the Academic Depart-
ment of Surgery at St Thomas’ Hospital.
Over the past 2 years we have received and
are most grateful for the constant support given by
all the editorial team of Hodder Arnold led by
Georgina Bentliff.
Last, but by no means least, we thank our wives
and families for accepting the disruptions to family
life that the preparation of this fourth edition has
imposed upon them.
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page iv
Contents
History taking and clinical
examination
How to take the history
2
History of pain
7
The clinical examination
11
History and examination of a lump
29
History and examination of an ulcer
32
The symptoms, signs and emergency
management of major injuries
The primary survey and management
at the site of the event: first-aid
36
The primary survey in the accident and
emergency department
38
The secondary survey
41
The skin and subcutaneous tissues
The diagnosis of skin conditions
47
Congenital skin disorders
50
Genetic skin disorders
50
Non-genetic skin disorders
51
Haemangiomata/lymphangiomata 53
Acquired dermatological conditions
57
Conditions of the skin caused by trauma
57
Infections of the skin
66
Benign tumours and benign skin lumps
71
Pigmented naevi
75
Benign subcutaneous swellings
78
Tumours of the skin appendages
86
Pre-malignant skin lesions
87
Malignant diseases of the skin
89
Other common skin conditions
often seen in surgical patients
99
Subcutaneous infections
100
Muscles, tendons, bones and joints
A general plan for examining the
muscles, bones and joints of a limb
104
Soft tissues
106
Muscles and muscle disease
106
Fibrous tissue
110
Tendons and tendon sheaths
112
Bones and bone irregularities
114
Examination of bones
114
Fractures 117
Bone diseases and deformities
118
Benign tumours of bone
122
Malignant tumours of bone
123
Joints
127
Examination of a joint
127
Examination of the spine
134
Diseases of joints
136
Conditions peculiar to the hands
A plan for the examination of the hand
143
Recording data about the hand
148
Abnormalities and lesions of the hand
149
The nails
160
Infections in the hand
162
Conditions peculiar to the feet
Congenital and acquired deformities
of the foot and ankle
165
The toe nails
170
The arteries, veins and lymphatics
The arteries
175
Clinical assessment of the arterial
circulation of the lower limb
175
Symptoms produced by arterial
insufficiency 179
Haemorrhage 190
Transient and permanent weakness,
paralysis and blindness
190
Cold, blue digits, hands and feet
192
Hypertension 196
Intestinal ischaemia
196
The veins
196
Clinical assessment of the venous
circulation of the lower limb
196
The lymphatics
209
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page v
Contents
vi
Colour 214
General appearance
217
Diseases affecting facial appearance
224
The eyes
226
The nose
230
Shape of the skull
230
The ears
232
Meningocele 234
The chest wall
234
The submandibular salivary gland
239
The parotid gland
242
Autoimmune disease
248
Congenital abnormalities of the lips
and palate
250
The lips, buccal mucosa and tongue
251
Other conditions of the tongue
261
The palate
261
The tonsils
263
The floor of the mouth
263
The gums
266
Swellings of the jaw
267
The jaw
268
The history and examination of
swellings in the neck
270
Cervical lymphadenopathy and other
neck swellings
271
The thyroid gland
288
Symptoms of thyroid disease
288
Examination of the thyroid gland
290
Different forms of goitre
295
Thyrotoxicosis and myxoedema
299
Carcinoma of the thyroid gland
303
Thyroiditis 307
History and examination of
breast disease
312
Presentation of breast disease
318
Carcinoma of the female breast
318
Benign breast tumours
322
Benign breast disease
323
The nipple
326
Breast abscess
328
Pregnancy 329
The male breast
329
Carcinoma of the male breast
330
Examination of the male genitalia
331
The penis
334
The scrotal skin
342
The testes
343
The female external genitalia
357
14 The abdominal wall, herniae and the
Abdominal herniae
360
Inguinal hernia
361
Femoral hernia
373
Umbilical hernia
375
Epigastric hernia
378
Incisional hernia
378
Divarication of the recti
379
Rare abdominal herniae
381
The umbilicus
381
The examination of the abdomen
386
Abdominal pain
391
Upper abdominal pain – acute and/or
chronic – caused by inflammatory and
malignant conditions
393
Central abdominal pain – acute
and/or chronic
401
General abdominal pain – acute
and/or chronic
403
Lower abdominal pain – acute and/or
chronic – caused by inflammatory
and/or malignant conditions
405
Symptoms and signs resulting from
the perforation of a viscus
411
Symptoms and signs caused by an
obstructed viscus
412
Infarction of a viscus causing
abdominal pain
414
Abdominal pain caused by intra-
abdominal or retroperitoneal
haemorrhage 415
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page vi
Contents
vii
INSTRUCTIONS FOR COMPANION WEBSITE
This book has a companion website available at:
http://www.hodderplus.com/browsesintroductions
To access the image library included on the website, please register using the following access details:
Serial number: jxpz475ak9wr
Once you have registered, you will not need the serial number but can log in using the username and
password that you will create during registration.
Extra-abdominal and medical conditions
causing acute abdominal pain
418
Alimentary conditions presenting
with dysphagia or vomiting
419
Conditions presenting with diarrhoea
420
The abdominal mass: causes and signs
421
Causes of a mass in the right iliac fossa
427
Causes of a mass in the left iliac fossa
430
Causes of a lump in the groin
430
Abdominal distension
431
16 The kidneys, urinary tract and
Symptoms of renal and urinary tract
disease 435
Diseases of the urinary tract
437
Retention of urine
441
The prostate gland
443
The urethra
445
Symptoms of ano-rectal disease
447
Technique for ano-rectal examination
448
Sigmoidoscopy and proctoscopy
451
Conditions presenting with rectal
bleeding 454
Conditions presenting with anal pain
459
Conditions presenting as an anal lump
with or without pain
465
Index
471
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page vii
I believe that the main object of basic medical edu-
cation is to train the student to talk to and to exam-
ine a patient in such a way that he can discover the
full history of the patient’s illness, elicit the abnor-
mal physical signs, make a differential diagnosis and
suggest likely methods of treatment. The object of
further medical training is to amplify these capabil-
ities in range and depth through practical experi-
ence and specialist training.
It is surprising, but a fact, that some students
present themselves for their qualifying examination
unable to take a history or to conduct a physical
examination in a way that is likely to detect all the
abnormal symptoms and signs. Even more are
unable to interpret and integrate the facts they do
elicit. I think there are two reasons for these defi-
ciencies. First, and most important, students do not
spend enough time seeing patients and practising
the art of history taking and clinical examination. It
is essential for them to realize at the beginning of
their training that the major part of medical educa-
tion is an apprenticeship, an old but well-proven
system whereby the apprentice watches and listens
to someone more experienced than himself and
then tries it himself under supervision. The second
reason is the lack of books which describe how to
examine a patient and explain how the presence or
absence of particular symptoms and signs lead the
clinician to the correct diagnosis.
In this book I have attempted to describe, in detail,
the relevant features of the history and physical signs
of the common surgical diseases in a way which
emphasizes the importance of the routine application
of the techniques of history taking and examining.
The details of these techniques are fully described,
and headings such as age, sex, symptoms, position,
site, shape and surface are constantly repeated in
an unobtrusive way. I hope that when you have fin-
ished reading the book you will have these headings
so deeply imprinted in your mind that you will
never forget them. If so, I will consider that the book
has succeeded, for you will always take a proper history
and perform a correct and complete examination.
Because the main object of the book is to empha-
size the proper techniques of history taking and
clinical examination, I have described only the com-
mon conditions that you are likely to see in a surgi-
cal clinic. Indeed the whole book is presented in a
manner similar to that used by most teachers when
they are in the presence of the patient. Special inves-
tigations and treatment are completely excluded
because neither can be applied sensibly if you get
the history and physical signs wrong.
To make the book useful for revision, I have put
a number of the lists and classifications in special
Revision Panels. The photographs are close to the
relevant text but their legends contain enough
information to make the picture-plus-legend a use-
ful revision piece.
I hope this book will be more of a teach-book
than a text-book, which will be read many times
during your basic and higher medical training.
There is a well-known saying ‘A bad workman
always blames his tools’. The doctor cannot make
this excuse because his basic tools are his five senses.
If he has not trained his senses properly in the man-
ner described in this book and kept them finely
honed by constant practice, he will practise bad
medicine but he will have only himself to blame.
Norman Browse
1978
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page viii
The diseases and abnormalities described in this
book have not changed for many thousands of
years, nor have their symptoms and signs. Why then
produce a third edition? The main reason is to
improve and modernize the presentation of the
information within the book in the belief that better
presentation facilitates and improves learning.
Whereas the symptoms and signs of surgical dis-
ease have not changed in the past 20 years, methods
of printing and publishing have. Computer graphics
and colour printing now enable publishers to produce
books of superb design, with infinite varieties of
colour, at acceptable costs. The main changes in this
new edition are therefore the introduction of colour
into the general presentation and design, and the con-
version of all ‘blackboard-style’ line drawings into
coloured illustrations – still simple – but giving them
the added impact on the memory provided by colour.
At the same time I have tried to illustrate all
the clinical conditions with colour photographs –
except for the few rare conditions, worthy of pre-
sentation, for which modern colour photographs are
difficult to obtain. Unfortunately, the current trend
is for patients to be unwilling to be photographed
for illustrations to be used in books for teaching,
thus making the compilation of a comprehensive
library of clinical photographs far more difficult
than it used to be.
I have also added a considerable number of new
Revision panels, now on a blue background, as stu-
dents find them particularly helpful.
To remind students of their importance, the
illustrations of methods of clinical examination
(mostly black-and-white photographs) are outlined
in Revision Panel blue.
I hope this revised presentation will give the
book a new modern appearance and that it will con-
tinue to be attractive to new readers in the same way
that it has been to the gratifyingly large number of
students who have acquired it for their libraries over
the past 20 years.
Sir Norman Browse
1997
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page ix
The first edition of this book was written, 25 years
ago, to help medical students develop their bed-
side clinical skills, namely, their ability to take a
full clinical history and to conduct a complete clin-
ical examination – the prime purpose of medical
education.
Although the symptoms and signs of the com-
mon ‘surgical’ diseases have not changed for cen-
turies, the style in which they are presented in
textbooks and our understanding of the underlying
pathological processes and, in some instances, their
classification have. These changes have prompted
the production of this fourth edition.
The past 25 years have also seen changes in the
style and methods of medical education, especially
in the UK, with the term ‘problem-orientated med-
icine’ purporting to describe the current popular
approach. This is not a new approach. Students
beginning their medical training have always been
taught to begin the taking of a history by asking
the patient ‘What are you complaining of?’. To me,
this is and always has been a problem-orientated
approach.
Having asked all the questions about the patient’s
main complaint, together with those concerning all
the other bodily systems, the student’s growing
knowledge of the symptoms and signs of individual
diseases inevitably begins to guide them to those
further questions which are likely to illuminate the
cause of the main complaint. This is why it is helpful
to learn the symptoms and signs of the common dis-
eases from a book at the same time as acquiring that
knowledge through growing clinical experience.
This book seeks to expedite that learning.
I firmly believe that what some criticize as dog-
matic teaching – following a strict ritual when taking
a history and performing an examination – must
remain a vital part of clinical education because it
accelerates diagnosis and helps avoid errors and
omissions.
Medical students know and appreciate this. The
continuing success of this book indicates that it helps
to fill the deficit that exists in those new courses of
medical education that have mistakenly reduced the
apprenticeship aspects of learning medicine.
Having retired from clinical practice, I felt it was
important to ask three surgical colleagues with an
approach to clinical teaching similar to my own, but
who are still clinically active, to join me as editors.
They have combined Chapters 2 and 3 and Chapters
13 and 15 of the third edition into single chapters
(now Chapters 3 and 14) and added a new chapter
on the symptoms and signs of trauma (Chapter 2).
In this edition, John Black has revised Chapters 8,
12, 13, 14, 16 and 17; Kevin Burnand has revised
Chapters 1, 3, 7 and 15 and written the new Chapter
2; and William Thomas has revised Chapters 4, 5, 6,
9, 10 and 11. I have collated and edited their revi-
sions to ensure that the book’s original systematic
approach and style of presentation were maintained.
I am most grateful for their hard work and willing
co-operation. When the fifth edition is needed, in
5–8 years’ time, I know it will be in excellent hands.
I hope this edition retains its style as a ward-round
‘teach-book’ aimed directly at the individual student
rather than a library-shelf textbook. Whenever possi-
ble, the illustrations have been kept on the same page
as the relevant text, as have many of the revision pan-
els. All are there to help you reinforce those vital
items of knowledge which must be in your mind
when sitting in front of a patient – not hidden some-
where in the memory of a computer.
Note. Throughout the book, whenever a particu-
lar complaint is more common in one sex, the
patient has been referred to as ‘he’ or ‘she’ accord-
ingly. If there is no sexual predominance, ‘they’ has
been used in the singular sense.
Sir Norman Browse
2005
Browse-Power-Prelims.qxd 12/17/10 5:49 PM Page x
You must be constantly alert from the moment you
first see the patient, and employ your eyes, ears, nose
and hands in a systematic fashion to collect infor-
mation from which you can deduce the diagnosis.
The ability to appreciate an unusual comment or
minor abnormality, which can lead you to the cor-
rect diagnosis, only develops from the diligent and
frequent practice of the routines outlined in this
chapter. Always give the patient your whole atten-
tion and never take short cuts.
In the outpatient clinic try to see patients walk into
the room, rather than finding them lying, undressed,
on a couch, in a cubicle. General malaise and debility,
breathlessness, cyanosis, and difficulty with particular
movements are much more obvious during exercise.
It may also be helpful to see and speak to anyone
who is accompanying the patient. A parent, spouse
or friend can often provide valuable information
about changes in health and behaviour not noticed
by the patient. Remember, however, that many
patients are inhibited from discussing their problems
in front of a third person. It can also be difficult if the
relative or friend, with the best of intentions, con-
stantly replies on behalf of the patient. When the time
comes to examine the patient, the friend or relative
can be asked to leave; further questions can then be
asked in private. It is helpful if a nurse is present.
Patients like to know to whom they are talking.
They are probably expecting to see a specific con-
sultant. You should tell patients your name and
explain why you are seeing them. It is particularly
important for medical students to do this.
Talk with patients or, better still, let them talk to
you. At first, guide the conversation but do not dic-
tate it. Treat patients as the rational, intelligent
human beings they are. They know more about
their complaints than you do, but they are usually
unable to interpret their significance. At all stages
explain what you are doing, and why you are doing it.
The patient may not be fluent in your own lan-
guage and require an interpreter. When conducting
an interview through an interpreter, keep your ques-
tions short and simple, and have them translated
and answered one at a time. You will have to use lay
terms if you are to be easily understood.
You should not use leading questions to which
there is only one answer. All questions should leave
the patient with a free choice of answers. You should
avoid saying, ‘The pain moves to the right-hand
side, doesn’t it?’. This is a ‘leading question’ because
it implies that it should have moved in that direction,
and an obliging patient will answer ‘Yes’ to please you.
The patient should be asked if the pain ever moves?
If the answer is ‘Yes’, you must then ask the supple-
mentary question, ‘Where does it go?’. Sometimes,
however, patients fail to understand your question
and you may have to suggest a number of possible
answers, which can be confirmed or rejected.
When a patient is having difficulty communicat-
ing with you, remember that a question that you do
not think is a leading one may be interpreted incor-
rectly by the patient if they do not realize that there
is more than one answer. For example, ‘Has the pain
changed?’ can be a bad question. There are a variety of
ways in which the pain can change – severity, nature,
site, etc. – but patients may be so disturbed by the
intensity of the pain that they think only of its sever-
ity and forget the other features that have changed. In
such situations, it often helps to include the possible
answers in the question; for example, ‘Has the pain
moved to the top, bottom, or side of your abdomen
or anywhere else?’, ‘Has the pain got worse, better or
stayed the same?’, or ‘Can you walk as far, less far, or
the same distance as you could a year ago?’.
Chap-01.qxd 4/19/05 13:40PM Page 1
History taking and clinical examination
The patient should provide the correct answer
providing you ask the question correctly. Do not be
over-concerned about the questions – worry about
the answers, and accept that it will sometimes take a
long time and a great deal of patience and persever-
ance to get a good history.
HOW TO TAKE THE HISTORY
The history should be taken in the order described
below and in Revision panel 1.1. Do not write and talk
to the patient at the same time; however, it is impor-
tant to document dates and times and the full drug
history with accuracy, which you may not remem-
ber when you have finished the examination and left
the room. Brief notes are therefore essential.
Make sure you know, and always record, the
patient’s name, age, sex, ethnic group, marital status,
occupation and address; and always record the date
of the examination.
The present complaint
It is customary to ask the patient ‘What are you com-
plaining of?’ and to record the answer in the patient’s
own words.
It is currently fashionable to talk about ‘problems’
rather than ‘complaints’. There is no difference,
but problem-orientated management sounds more
sympathetic.
If you ask ‘What is the matter?’ the patient will
probably tell you their diagnosis. It is better not to
know the diagnoses made by the patient, or other
doctors, because none may be correct. It is better to
try to seek out the patient’s complaints. These should
be listed in order of severity, with a record of pre-
cisely when and how they started. Whenever possible,
it should be noted why the patient is more con-
cerned with one complaint than another.
The history of the present complaint
The full history of the main complaint or complaints
must be recorded in detail, with precise dates. It is
important to get right back to the beginning of the
problem. For example, a patient may complain of a
recent sudden attack of indigestion. If further ques-
tioning reveals that similar symptoms occurred some
years previously, their description should be included
in this section.
Remaining questions about the
affected system
When a patient complains of indigestion it is sensi-
ble, after recording the history of the indigestion, to
ask other questions about the alimentary system
because many of the replies may aid in diagnosing
the main complaint.
Systematic direct questions
These are direct questions that every patient should
be asked, because the answers may amplify your
knowledge about the main complaint and will often
reveal the presence of other disorders of which the
patient was unaware, or thought irrelevant. Negative
answers are just as important as positive answers.
The standard set of direct questions is described
in detail below because they are so important. It is
essential to know them by heart because it is very
easy to forget to ask some of them. When you have to
go back to the patient to ask a forgotten question,
you invariably find the answer to be very impor-
tant. The only way to memorize this list is by taking
as many histories as possible and writing them out
in full. All the answers to every question, whether
they be positive or negative, must be recorded.
The alimentary system
Appetite
Has the appetite increased, decreased, or
remained unchanged? If it has decreased, is this
caused by a lack of desire to eat, or is it because of
apprehension as eating always causes pain?
Diet
What type of food does the patient eat? Are
they vegetarian? When do they eat their meals?
Weight
Has the patient’s weight changed? By how
much? Over how long a time? Many patients never
weigh themselves, but they usually notice if their
clothes have got tighter or looser and friends may
have told them of a change in physical appearance.
Teeth and taste
Can they chew their food? Do they
have their own teeth? Do they get odd tastes and sen-
sations in their mouth? Are there any symptoms of
water brash or acid brash? (This is sudden filling of
2
Chap-01.qxd 4/19/05 13:40PM Page 2
How to take the history
3
Revision panel 1.1
Synopsis of a history
Names; age and date of birth; sex; marital status; occupation; ethnic group; hospital or practice
record number
Present complaints or problems (PC, CO) Preferably in the patient’s own words.
History of present complaint (HPC) Include the answers to the direct questions concerning the
system of the presenting complaint.
Systematic direct questions
(a) Alimentary system and abdomen (AS)
Appetite. Diet. Weight. Nausea. Dysphagia. Regurgitation. Flatulence. Heartburn. Vomiting.
Haematemesis. Indigestion pain. Abdominal pain. Abdominal distension. Bowel habit. Nature of
stool. Rectal bleeding. Mucus. Slime. Prolapse. Incontinence. Tenesmus. Jaundice.
(b) Respiratory system (RS)
Cough. Sputum. Haemoptysis. Dyspnoea. Hoarseness. Wheezing. Chest pain. Exercise tolerance.
(c) Cardiovascular system (CVS)
Dyspnoea. Paroxysmal nocturnal dyspnoea. Orthopnoea. Chest pain. Palpitations. Dizziness. Ankle
swelling. Limb pain. Walking distance. Colour changes in hands and feet.
(d) Urogenital system (UGS)
Loin pain. Frequency of micturition including nocturnal frequency. Poor stream. Dribbling.
Hesitancy. Dysuria. Urgency. Precipitancy. Painful micturition. Polyuria. Thirst. Haematuria.
Iincontinence.
In men Problems with sexual intercourse and impotence.
In women Date of menarche or menopause. Frequency. Quantity and duration of menstruation.
Vaginal discharge. Dysmenorrhoea. Dyspareunia. Previous pregnancies and their complications.
Prolapse. Urinary incontinence. Breast pain. Nipple discharge. Lumps. Skin changes.
(e) Nervous system (NS, CNS)
Changes of behaviour or psyche Depression. Memory loss. Delusions. Anxiety. Tremor. Syncopal
attacks. Loss of consciousness. Fits. Muscle weakness. Paralysis. Sensory disturbances.
Paraesthesiae. Dizziness. Changes of smell, vision or hearing. Tinnitus. Headaches.
(f) Musculoskeletal system (MSkS)
Aches or pains in muscles, bones or joints. Swelling joints. Limitation of joint movements. Locking.
Weakness. Disturbances of gait.
Previous history (PH) Previous illnesses. Operations or accidents. Diabetes. Rheumatic fever.
Diphtheria. Bleeding tendencies. Asthma. Hay fever. Allergies. Tuberculosis. Syphilis. Gonorrhoea.
Tropical diseases.
Drug history Insulin. Steroids. Anti-depressants and the contraceptive pill. Drug abuse.
Immunizations BCG. Diphtheria. Tetanus. Typhoid. Whooping cough. Measles.
Family history (FH) Causes of death of close relatives. Familial illnesses in siblings and offspring.
Social history (SH) Marital status. Sexual habits. Living accommodation. Occupation. Exposure to
industrial hazards. Travel abroad. Leisure activities.
Habits Smoking. Drinking. Number of cigarettes smoked per day. Units of alcohol drunk per week.
Chap-01.qxd 4/19/05 13:40PM Page 3
History taking and clinical examination
the mouth with watery or acid-tasting fluid – saliva
and gastric acid respectively.)
Swallowing
If they complain of difficulty in swal-
lowing (dysphagia), ask about the type of food that
causes difficulty, the level at which the food sticks, and
the duration and progression of these symptoms. Is
swallowing painful?
Regurgitation
This is the effortless return of food
into the mouth. It is quite different from vomiting,
which is associated with a powerful involuntary con-
traction of the abdominal wall. Do they regurgitate?
What comes up? If food, is it digested or recognizable
and undigested? How often does it occur and does
anything, such as stooping or straining, precipitate it?
Flatulence
Does the patient belch frequently? Does
this relate to any other symptoms?
Heartburn
Patients may not realize that this symptom
comes from the alimentary tract and they may have
to be asked about it directly. It is a burning sensation
behind the sternum caused by the reflux of acid into
the oesophagus. How often does it occur and what
makes it happen, e.g. lying flat or bending over?
Vomiting
How often do they vomit? Is the vomiting
preceded by nausea? What is the nature and volume
of the vomitus? Is it recognizable food from previ-
ous meals, digested food, clear acidic fluid or bile-
stained fluid? Is the vomiting preceded by another
symptom such as indigestion pain, headache or gid-
diness? Does it follow eating?
Haematemesis
Always ask if they have ever vomited
blood because it is such an important symptom.
Old, altered blood looks like ‘coffee grounds’. Some
patients have difficulty in differentiating between
vomited or regurgitated blood and coughed-up blood
(haemoptysis). The latter is usually pale pink and
frothy. When patients have had a haematemesis,
always ask if they have had a recent nose bleed. (They
may be vomiting up swallowed blood.)
Indigestion or abdominal pain
Some people call all
abdominal pains indigestion; the difference between
a discomfort after eating and a pain after eating may
be very small. Concentrate on the features of the
pain, its site, time of onset, severity, nature, progres-
sion, duration, radiation, course, precipitating, exac-
erbating and relieving factors (see pages 7–10).
Abdominal distension
Have they noticed any abdom-
inal distension? What brought this to their atten-
tion? When did it begin and how has it progressed?
Is it constant or variable? What factors are associ-
ated with any variations? Is it painful? Does it affect
their breathing? Is it relieved by belching, vomiting
or defaecation?
Defaecation
How often does the patient defaecate?
What are the physical characteristics of the stool?
■
Colour: brown, black, pale, white or silver?
■
Consistence: hard, soft or watery?
■
Size: bulky, pellets, string or tape like?
■
Specific gravity: does it float or sink?
■
Smell?
Beware of the terms ‘diarrhoea’ and ‘constipation’.
They are lay words and mean different things to dif-
ferent people. These words should not be written in
the notes without also recording the frequency of
bowel action and the consistence of the faeces.
Rectal bleeding
Has the patient ever passed any
blood in the stool? Was it bright or dark? How much?
Was it mixed in with or on the surface of the stool, or
did it only appear after the stool had been passed?
Flatus, mucus, slime
Is the patient passing more gas
than usual? Has the patient ever passed mucus or
pus? Is defaecation painful? When does the pain
begin – before, during, after, or at times unrelated to
defaecation?
Prolapse and incontinence
Does anything come out
of the anus on straining? Does it return spontane-
ously or have to be pushed back? Is the patient con-
tinent of faeces and flatus? Have they had any injuries
or anal operations in the past?
Tenesmus
Do they experience any urgent, painful
but unproductive desire to pass stool? This is called
tenesmus.
Change of skin colour
Have the patient’s skin or eyes
ever turned yellow (jaundiced)? When? How long
did it last? Were there any other accompanying symp-
toms such as abdominal pain or loss of appetite?
Did the skin itch?
The respiratory system
Cough
How often does the patient cough? Does the
coughing come in bouts? Does anything, such as a
4
Chap-01.qxd 4/19/05 13:40PM Page 4
How to take the history
change of posture, precipitate or relieve the cough-
ing? Is it a dry or a productive cough?
Sputum
What is the quantity (teaspoon, dessert-
spoon, etc.) and colour (white, clear or yellow) of the
sputum? Some patients only produce sputum in the
morning or when they are in a particular position.
Haemoptysis
Has the patient ever coughed up blood?
Was it frothy and pink? Were there red streaks in the
mucus, or clots of blood? What quantity was pro-
duced? How often does the haemoptysis occur?
Dyspnoea
Does the patient wheeze? Does he get
breathless? How many stairs can he climb? How far
can he walk on a level surface before the dyspnoea
interferes with the exercise? Can he walk and talk
at the same time? Is the dyspnoea present at rest?
Is it present when sitting or made worse by lying
down? (Dyspnoea on lying flat is called orthop-
noea.) How many pillows does the patient need
at night? Does the breathlessness wake them up at
night – paroxysmal nocturnal dyspnoea – or get
worse if they slip off their pillows? There are classi-
fications that grade dyspnoea numerically, but it is
better to describe the causative conditions rather
than write down a number.
Is the dyspnoea induced or exacerbated by exter-
nal factors such as allergy to animals, pollen or dust?
Does the difficulty with breathing occur with both
phases of respiration or on expiration?
Pain in the chest
Ascertain the site, severity and
nature of the pain. Chest pains can be continuous,
pleuritic (made worse by inspiration), constricting
or stabbing.
The cardiovascular system
Cardiac symptoms
Breathlessness
Ask the same questions as those
described above under ‘Respiratory system’.
Orthopnoea and paroxysmal nocturnal dyspnoea
Orthopnoea and paroxysmal nocturnal dyspnoea
are the forms of dyspnoea especially associated with
heart disease.
Pain
Cardiac pain begins in the mid-line and is
usually retrosternal but may be epigastric. It is often
described as constricting or band-like. It is usually
brought on by exercise or excitement. The patient
should be asked if the pain radiates to the neck or to
the left arm and whether it is relieved by rest.
Palpitations
These are episodes of tachycardia which
the patient notices as a sudden fluttering or thump-
ing of the heart in the chest.
Ankle swelling
Do the ankles or legs swell? When do
they swell? What is the effect on the swelling of bed-
rest and/or elevation of the leg?
Dizziness, headache and blurred vision
These are
some of the symptoms associated with hyperten-
sion and postural hypotension.
Peripheral vascular symptoms
Does the patient get pain in the leg muscles on exer-
cise (intermittent claudication)? Which muscles are
involved? How far can the patient walk before the
pain begins? Is the pain so bad that he has to stop
walking? How long does the pain take to wear off?
Can the same distance be walked again? Is there any
pain in the limb at rest? Which part of the limb is
painful? Does the pain interfere with sleep? What
positions relieve the pain? What analgesic drugs give
relief? Are the extremities of the limbs cold? Are
there colour changes in the skin, particularly in
response to a cold environment? Does the patient
experience any paraesthesiae in the limb, such as
tingling or numbness?
The urogenital system
Urinary tract symptoms
Pain
Has there been any pain in the loin, groin or
suprapubic region? What is its nature and severity?
Does it radiate to the groin or scrotum?
Oedema
Do any parts of the body other than the
ankles swell?
Thirst
Is the patient thirsty? Do they drink excessive
volumes of water?
Micturition
How often does the patient pass urine?
Express this as a day/night ratio. How much urine
is passed? Is the volume and frequency excessive
(polyuria)? Is micturition painful? What is the
nature and site of the pain? Is there any difficulty
with micturition, such as a need to strain or to wait?
Is the stream good? Can it be stopped at will? Is
there any dribbling at the end of micturition? Does
5
Chap-01.qxd 4/19/05 13:40PM Page 5
History taking and clinical examination
the bladder feel empty at the end of micturition or
do they have to pass urine a second time?
Urine
Has the patient ever passed blood in the
urine? When and how often? Have they ever passed
gas bubbles with the urine (pneumaturia)?
Symptoms of uraemia
These include headache,
drowsiness, visual disturbance, fits and vomiting.
Genital tract symptoms
MALE
Scrotum, penis and urethra
Has the patient any
pain in the penis or urethra during micturition or
intercourse? Is there any difficulty with retraction of
the prepuce or any urethral discharge? Has the patient
noticed any swelling of the scrotum? Can he achieve
an erection and ejaculation?
FEMALE
Menstruation
When did menstruation begin (menar-
che)? When did it end (menopause)? What is the
duration and quantity of the menses? Is menstrua-
tion associated with pain (dysmenorrhoea)? What is
the nature and severity of the pain? Is there any
abdominal pain mid-way between the periods (mit-
telschmerz)? Has the patient had any vaginal dis-
charge? What is its character and amount? Has she
noticed any prolapse of the vaginal wall or cervix or
any urinary incontinence, especially when straining
or coughing (stress incontinence)?
Pregnancies
Record details of the patient’s preg-
nancies – number, dates and complications.
Dyspareunia
Is intercourse painful?
Breasts
Do the breasts change during the men-
strual cycle? Are they ever painful or tender? Has the
patient noticed any swellings or lumps in the breasts?
Did she breast-feed her children? Has there been
any nipple discharge or bleeding? Has she noticed
any skin changes over the breasts?
Secondary sex characteristics
When did these
appear?
The nervous system
Mental state
Is the patient placid or nervous? Has
the patient noticed any changes in their behaviour
or reactions to others? Patients will often not appre-
ciate such changes themselves and these questions
may have to be asked of close relatives. Does the
patient get depressed and withdrawn, or are they
excitable and extroverted?
Brain and cranial nerves
Does the patient ever
become unconscious or have fits? What happens
during a fit? It is often necessary to ask a relative or
a bystander to describe the fit. Did the patient lie
still or jerk about, bite their tongue, pass urine? Was
the patient sleepy after the fit? Was there any warning
(an aura) that the fit was about to develop? Has there
been any subsequent change in the senses of smell,
vision and hearing?
Is there a history of headache? Where is it experi-
enced? When does it occur? Are the headaches asso-
ciated with any visual symptoms?
Has the face ever become weak or paralysed? Have
any of the limbs been paralysed or had pins and
needles? Has there ever been any buzzing in the ears,
dizziness or loss of speech? Can the patient speak
clearly and use words properly?
Peripheral nerves
Are any limbs or part of a limb
weak or paralysed? Is there ever any loss of cutaneous
sensation (anaesthesia)? Does the patient experience
any paraesthesiae (tingling, ‘pins and needles’) in
the limbs?
Musculoskeletal system
Ask if the patient suffers from pain, swelling or lim-
itation of the movement of any joint. What precipi-
tates or relieves these symptoms? What time of day
do they occur? Are any limbs or groups of muscles
weak or painful? Can he walk normally? Has he any
congenital musculoskeletal deformities?
Previous history of other illnesses,
accidents or operations
Record the history of those conditions which are not
directly related to the present complaint. Ask specif-
ically about tuberculosis, diabetes, rheumatic fever,
allergies, asthma, tropical diseases, bleeding tenden-
cies, diphtheria, gonorrhoea, syphilis, and the likeli-
hood of intimate contact with carriers of the human
immunodeficiency virus (HIV).
Drug history
Ask if the patient is taking any drugs. Specifically,
enquire about steroids, anti-depressants, insulin,
6
Chap-01.qxd 4/19/05 13:40PM Page 6
History of pain
diuretics, anti-hypertensives, hormone replacement
therapy and the contraceptive pill. Patients usually
remember about drugs prescribed by a doctor but
often forget about self-prescribed drugs they have
bought at a pharmacy. Is the patient sensitive to any
drugs or any topical applications such as adhesive
plaster? If they are, write it in large letters on the
front of the notes.
Immunizations
Most children are immunized against diphtheria,
tetanus, whooping cough, measles, mumps, rubella
and poliomyelitis. Ask about these, and smallpox,
typhoid and tuberculosis vaccination.
Family history
Enquire about the health and age, or cause of death,
of the patient’s parents, grandparents, brothers and
sisters, and ask about any children who have died.
Draw a family tree if there is obvious familial dis-
order (e.g. lymphoedema). If the patient is a child,
you will need information about the mother’s preg-
nancy. Did she take any drugs during pregnancy?
What was the patient’s birth weight? Were there any
difficulties during delivery? What was the rate of
physical and mental development in early life?
Social history
Record the marital status and the type and place of
dwelling. Ask about the patient’s sexual life, the sex
and sexual behaviour of their sexual partners and
the nature of their physical relationships. Ask about
the patient’s occupation, paying special regard to
contact with hazards such as dusts and chemicals.
What are the patient’s leisure activities? Has the
patient travelled abroad? List the countries visited
and the dates of the visits if these appear to be
relevant.
Habits
Does the patient smoke? If so what – cigarettes, cigar
or pipe? Record the frequency, quantity and duration
of their smoking habit. Does the patient drink alco-
hol? Record the type and quantity consumed and
the duration of the habit. Does the patient have any
unusual eating habits?
HISTORY OF PAIN
We have all experienced pain. It is one of nature’s
ways of warning us that something is going wrong
in our body. It is an unpleasant sensation of varying
intensity. Pain can come from any of the body’s sys-
tems but there are certain features common to all
pains that should always be recorded.
Be careful in your use of the word tenderness.
Tenderness is pain which occurs in response to a
stimulus, such as pressure from the doctor’s hand,
or forced movement. It is possible for a patient to
be lying still without pain and yet have an area of
tenderness. The patient feels pain – the doctor elicits
tenderness. But although patients usually complain
of pain, they may also have observed and complain
of tenderness if they happen to have pressed their
fingers on a painful area or discovered a tender spot
by accident. Thus tenderness can be both a symp-
tom and a physical sign.
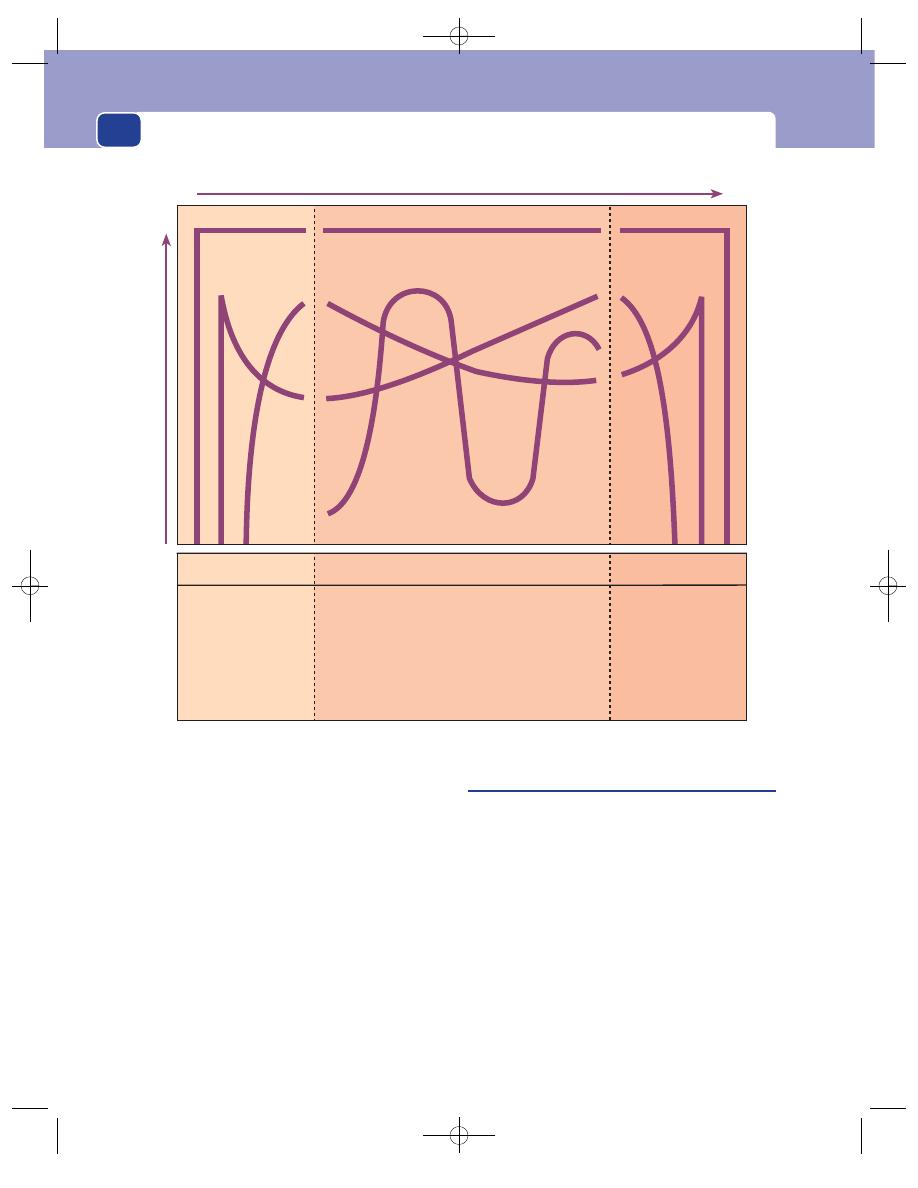
The history of a pain frequently betrays the diag-
nosis, so you must question the patient closely about
each of the following features, some of which are
depicted graphically in Figure 1.1.
Site
Many factors may indicate the source of the pain
but the most valuable indicator is its site.
It is of no value to describe a pain as ‘abdominal
pain’; you must be more specific. Although patients
do not describe the site of their pain in anatomical
terms, they can always point to the site of max-
imum intensity, which you can convert into an exact
description. When the pain is indistinct in nature and
spread diffusely over a large area, you must describe
the area in which the pain is felt and the point (indi-
cated by the patient) of maximum discomfort. It is
also worthwhile asking about the depth of the pain.
Patients can often tell you whether the pain is near
to the skin or deep inside.
Time and mode of onset
It may be possible to pinpoint the onset of the pain
to the minute, but if this cannot be done, the part of
7
Chap-01.qxd 4/19/05 13:40PM Page 7
Progression
(a) Steady
(b) Gradual decline
(c) Gradual worsening
(d) Fluctuating
Duration
Severity
Onset
(a) Sudden onset at
maximum
severity
(b) Sudden onset and
subsequent
decline
(c) Gradual onset
End
(a) Sudden cessation
(b) Gradual end
(c) Crescendo and
then sudden end
(a)
(b)
(c)
(d)
(a)
(a)
(b)
(b)
(c)
(c)
History taking and clinical examination
the day or night when the pain began should be
recorded. You should record the calendar dates on
which events occurred, but it is also very useful to
add in brackets the time interval between each event
and the current examination, because it is these
intervals, not the actual dates, which are more rele-
vant to the problems of diagnosis. For example,
‘Sudden onset of severe epigastric pain on 16th
September, 1973, at 11.00 a.m. (3 days ago)’: but
remember that such comments are useless if you
forget to record the date of the examination.
Whenever you write a note about a patient, whether
it be a short progress note or a full history, make
certain that you start your notes by writing down
the date.
Ask if the pain began insidiously or suddenly.
Severity
Individuals react differently to pain. What is a severe
pain to one person might be described as a dull ache
by another. Consequently you must be wary of the
adjectives used by a patient to describe the severity
of their pain. A far better indication of severity is the
effect of the pain on the patient’s life. Did it stop the
patient going to work? Did it make the patient go to
bed? Did they try proprietary analgesics? Did they
have to call their doctor? Did it wake the patient up
at night, or stop them going to sleep? Was the pain
better lying still or did it make the patient roll around?
The answers to these questions provide a better indi-
cation of the severity of a pain than words such as
mild, severe, agonizing or terrible. Your assessment
8
FIG 1.1
The ways in which a pain can change. (Always record dates and calculate time intervals.)
Chap-01.qxd 4/19/05 13:40PM Page 8
History of pain
of the way the patient responds to their pain, formed
while you are taking the history, may profoundly
affect your treatment.
Nature or character of the pain
Patients find it very difficult to describe the nature
of their pain, but some of the adjectives which
are commonly used, such as aching, stabbing, burn-
ing, throbbing, constricting, distending, gripping
or colic, have a similar meaning to the majority of
people.
Burning and throbbing sensations are within
everyone’s experience. We have all experienced a
burning sensation from our skin following contact
with intense heat, so when a patient spontaneously
states that their pain is ‘burning’ in nature, it is likely
to be so. We have all experienced a throbbing sensa-
tion at some time in our life, so this description is
also usually accurate.
A stabbing pain is sudden, severe, sharp, and
short-lived.
The adjective constricting suggests a pain that
encircles the relevant part (chest, abdomen, head or
limb) and compresses it from all directions. A pain
that feels like an iron band tightening around the
chest is typical of angina pectoris and almost diag-
nostic, but when patients speak of a tightness in
their chest or limb do not immediately assume that
they have a constricting pain. They may be describ-
ing a tightness caused by distension, which may
occur in any structure that has an encircling and
restricting wall, such as the bowel, bladder, an encap-
sulated tumour or a fascial compartment. Tension
in the containing wall may cause a pain which the
patient may describe as distension, tightness or a
bursting feeling.
A colicky pain has two features. First, it comes
and goes in a sinusoidal way. Second, it feels like a
migrating constriction in the wall of a hollow tube
which is attempting to force the contents of the tube
forwards. It is not a word which many patients use
and it is dangerous to ask them if their pain is col-
icky without giving an example. This is not difficult,
because most of us have experienced colic during an
episode of diarrhoea, and many women have suffered
the colicky pains of labour. A recurring, intermittent
pain is not necessarily a colic; it must also have a
gripping nature.
‘Just a pain, doctor’. Most pains have none of the
features mentioned above and are described by many
patients as ‘a pain’. This may vary in severity from a
mild discomfort or ache, to an agonizing pain that
makes them think they are about to die. When a
patient cannot describe the nature of their pain, do
not press the point. You will only make them try to
fit their pain to your suggestions and ultimately this
may be misleading.
9
Revision panel 1.2
The features of a pain that must be elicited and
recorded
Site
Time and mode of onset
Record the time and date of onset and the way
the pain began – suddenly or gradually.
Duration
Record the duration of the pain.
Severity
Assess severity by its effect on the patient.
Nature/character
Aching, burning, stabbing, constricting,
throbbing, distending, colic.
Radiation
Record the time and direction of any radiation of
the pain; remember to ask if the nature of the
pain changed at the time it moved.
Referral
Was the pain experienced anywhere else?
Progression
Describe the progression of the pain. Did it
change or alter?
The end of the pain
Describe how the pain ended. Was the end
spontaneous or brought about by some action
by the patient or doctor?
Relieving and exacerbating factors
Cause
Note the patient’s opinion of the cause of the
pain.
Chap-01.qxd 4/19/05 13:40PM Page 9
History taking and clinical examination
Progression of the pain
Once it has started, a pain may progress in a variety
of ways.
■
It may begin at its maximum intensity and
remain at this level until it disappears.
■
It may increase steadily until it reaches a peak or
a plateau, or conversely begin at its peak and
decline slowly.
■
The severity may fluctuate (see Fig. 1.1). The
intensity of the pain at the peaks and troughs of
the fluctuations, and the rate of development
and regression of each peak, may vary. The pain
may go completely between each exacerbation.
The time between the peaks of an abdominal
colic may indicate the likely site of a bowel
obstruction (e.g. in upper small bowel
obstruction, the frequency of the colic is every
1–2 minutes, in the ileum every 20 minutes). It is
essential to find out how the pain has progressed
and ascertain the timing of any fluctuations
before its nature can be determined; for
example, colic has two features – its gripping
nature and its intermittent progression.
The end of the pain
A pain may end spontaneously, or as a result of some
action by the patient or doctor. The end of a pain is
either sudden or gradual. The way a pain ends may
give a clue to the diagnosis, or indicate the develop-
ment of a new problem.
Patients always think that the disappearance of
their pain means that they are getting better. They
are usually right, but sometimes their condition may
have got worse.
Duration of the pain
The duration of a pain will be apparent from the time
of its onset and end, but nevertheless it is worth-
while stating the duration of the pain in your notes.
The length of any periods of exacerbation or remis-
sion should also be recorded.
Factors which relieve the pain
Patients will know if there is anything, such as posi-
tion, movement, a hot-water bottle, aspirins, food,
antacids, etc., which relieves the pain. The natural
response to a pain is to search for a way to relieve it.
Sometimes patients try the most bizarre remedies and
many convince themselves that some minor change
in habit or a personal remedy has been helpful, so
accept their replies to this question with caution.
Factors which exacerbate the pain
Anything that makes the pain worse is also likely to
be known to the patient.
The type of stimulus that exacerbates a pain will
depend on the organ from which it emanates and its
cause. For example, alimentary tract pains may be
made worse by eating particular types of food; mus-
culoskeletal pains are affected by joint movements,
muscle exercise and posture. It is perfectly reasonable
to ask direct questions about those stimuli which
you think might affect a pain if the initial description
has indicated its source.
Radiation and referral
Radiation
Radiation is the extension of the pain to
another site whilst the initial pain persists. For exam-
ple, patients with a posterior penetrating duodenal
ulcer usually have a persistent pain in the epigas-
trium, but sometimes the pain spreads through the
abdomen to the back. The extended pain usually has
the same character as the initial pain.
A pain may occur in one site, disappear, and then
reappear in another. This is not radiation: it is a new
pain in another place.
Referred pain
This is a pain which is felt at a dis-
tance from its source. For example, inflammation of
the diaphragm will cause a pain which is felt at the
tip of the shoulder. A referred pain is caused by the
inability of the central nervous system to distinguish
between visceral and somatic sensory impulses. From
the patient’s viewpoint, the pain is where they feel it –
the fact that the source is some distant organ does
not concern them.
Cause
It is worthwhile asking patients what they think is
the cause of their pain. Even if they are hopelessly
wrong, you will get some insight into their worries.
10
Chap-01.qxd 4/19/05 13:41PM Page 10
The clinical examination
Sometimes a patient will be obsessed with the cause
of his condition and careful questioning may reveal
that he will gain or lose compensation or insurance
money as the result of your opinion. Nevertheless,
always listen to the patient’s views with care and
tolerance.
THE CLINICAL EXAMINATION
Each chapter of this book deals with a specific region
of the body and its surgical diseases. Those methods
of examination peculiar to each region are described
in detail in the relevant chapter. The emphasis in
this introductory chapter is on the importance of
taking an exact and full history, but it would not be
complete without a description of the basic plan of
a physical examination, with particular reference to
those regions not discussed in later chapters, such as
the heart, the lungs and the nervous system. As this
is a thumb-nail sketch of clinical examination, your
knowledge will need to be enlarged by additional
reading, but your understanding and ability to solve
the practical problems of clinical examination can
only be clarified by frequent bedside practice.
Examine as many patients as you can. Nothing can
be learnt without frequent practice. Repetition is
the secret of learning. This axiom applies as much to
the doctor as it does to the sportsman or the concert
pianist. You will become confident of your interpre-
tation of your visual, tactile and aural appreciation
of the patient’s body only by repeatedly exercising
these senses.
Experienced clinicians rarely begin the routine
physical examination without some suspicions about
the diagnosis suggested by the history. Conse-
quently, they often modify the impartial system-
atized examination described in textbooks such as
this by specifically looking for signs which confirm
or refute their tentative diagnoses, but when a sign is
elicited that denies their suspicions they return to
the textbook routine. Students must not do this.
Although it is a practical and time-saving method in
a busy clinic, and acceptable from someone with
years of clinical experience who can pick out those
patients to whom it can be applied, it is fundamen-
tally wrong. Bad habits grow fast enough without
encouragement. Unless students discipline them-
selves to use the standard textbook routine for every
physical examination, many mistakes will inevitably
be made and, as time passes, some parts of the
examination will be completely forgotten, with seri-
ous consequences.
The easiest way to ensure that you perform a
complete examination is to learn the routine by heart
and repeat it to yourself during the examination.
Whilst looking at a lump, say to yourself, ‘position,
shape, size’, etc. If you do not do this, you will find
when you sit down to write your notes that you have
forgotten to elicit some of the lump’s physical fea-
tures and will have to go back to re-examine the
patient. Always keep to the basic pattern of looking,
feeling, tapping and listening (inspection, palpation,
percussion, auscultation), whatever you are exam-
ining. Whilst keeping to the routine it is, however,
often best to examine first the part of body that is
the source of the patient’s complaint.
General assessment
The first part of the physical examination is per-
formed when taking the history. While you are talk-
ing to the patient you can observe and later record
their general demeanour, their intellectual ability
and intelligence, and their attitudes to their disease,
to you, to their treatment, and to society in general.
These observations affect the manner in which you
conduct the examination. Your instructions will
need to be extremely simple if the patient is unintel-
ligent, or coaxing and gentle if the patient is shy or
embarrassed.
The patient’s general mental state, his memory
and use of words should be noted. There is a whole
vocabulary used by the neurologists to describe var-
ious speech and communication disorders. Some of
the common ones are:
■
dysarthria: impaired speech caused by muscle
weakness;
■
dysphasia or aphasia: impaired or absent
ability to speak caused by a neurological
abnormality;
■
dysgraphia or agraphia: impaired or absent
ability to write;
■
dyspraxia or apraxia: impaired or absent ability
to perform purposeful movements in the
absence of paralysis.
When a patient has been admitted as an emergency,
especially if they have been injured, it is important
11
Chap-01.qxd 4/19/05 13:41PM Page 11
History taking and clinical examination
to record their level of consciousness using the
Glasgow Coma Scale.
You can also observe a number of physical char-
acteristics when taking the history, such as posture,
mobility, weight, colour of skin, facial appearance
and general body build.
Hold the patient’s hand and examine it
Make physical contact with the patient early in the
examination by holding their hand and counting the
pulse. It is very important for the patient to feel that
you are willing to get physically as well as mentally
close to them. The physical contact that is essential for
the examination forges an intimate bond between you
and the patient. It is an extraordinary privilege granted
to you by the patient and must never be abused.
The features that can be observed by examining
the hands are as follows.
Pulse
See details on page 22.
Nails
Look at the colour and shape of the nails.
Spoon-shaped nails (koilonychia) are associated with
anaemia; clubbing of the nails occurs in pulmonary
and cardiopulmonary disease (see Fig. 5.24, page 160);
and splinter haemorrhages under the nails are caused
by small arterial emboli. Pits and furrows are associ-
ated with skin diseases such as psoriasis. Bitten nails
may indicate nervousness and anxiety.
Temperature
Observe the temperature of the hands –
but remember that it will be affected by room tem-
perature and the duration of exposure.
Moisture
Are the patient’s palms sweating excessively?
Colour
Pallor of the skin of the hands, especially
in the skin creases of the palm and in the nail beds,
suggests anaemia. Reddish-blue hands occur in
polycythaemia and cor pulmonale. The fingers may
be stained with nicotine.
Callosities
The position of any callosities may reflect
the patient’s occupation.
Examine the head and neck
Eyes
Look for any asymmetry of the position, size or
colour of the eyes and especially any abnormality in
the width of the palpebral fissures. This can be caused
by ptosis (droopy eyelids) or proptosis (exophthal-
mos) when the eyeball is pushed forwards, pushing
the lids apart (see Chapter 11, pages 292–4). The size
and equality of the two pupils should be recorded
(dilated, constricted or unequal).
12
Revision panel 1.3
The Glasgow Coma Scale
Score
Eyes
Open spontaneously
4
Open to command
3
Open to pain
2
Do not open
1
Speech
Sensible/orientated
5
Confused
4
Inappropriate words
3
Incomprehensible sounds
2
None
1
Motor
Obeys commands
6
responses
Localizes stimuli
5
Withdraws from stimuli
4
Flexion responses
3
Extension responses
2
None
1
Total
Revision panel 1.4
Some common causes of weight loss
In the young
Malnutrition
Diabetes
Malabsorption
Anorexia nervosa
Tuberculosis
From middle age onwards Diabetes
Thyrotoxicosis
Chronic hypoxia
Chronic heart failure
Malignant disease
Senile cachexia
Neglect
Chap-01.qxd 4/19/05 13:41PM Page 12
The clinical examination
The reaction of the pupil to light is checked by
shining a bright light off and on the pupil. The pupil’s
reaction to accommodation is assessed by asking the
patient to look into the distance and then to refocus
on a finger held close to their eye.
The eye movements are examined by fixing the
patient’s head with one hand while asking them to
watch your finger as it travels upwards and down-
wards and inwards and outwards to the full extremes
of movement. Patients should be asked if they expe-
rience any double vision (diplopia) in any particular
position. While the eye movements are being tested,
the presence of any strabismus (squint) can usually
be easily seen, which may be concomitant (divergent
or convergent) or paralytic.
Look for the presence of nystagmus (oscillations
of the eye characterized by a slow drift and a rapid
jerk back) at the inward and outward extremes of
movement.
Inspect the lids, conjunctiva, cornea and lens.
Styes, Meibomian cysts, and blepharitis may inflame
the lids or cause a swelling. The edges of the eyelids
may be everted or inverted (ectropion or entropion)
and the eye may water if the tearduct or lacrimal sac
is blocked.
A painful red eye may be caused by acute con-
junctivitis (when there is usually an associated dis-
charge), acute iritis (when the anterior chamber of
the eye is inflamed), acute glaucoma (which is asso-
ciated with severe pain and a misty cornea), acute
keratitis (from a corneal ulcer, seen as a cloudy opac-
ity) or episcleritis.
When an elderly patient has a gradual loss of eye-
sight they are likely to have a cataract (which can be
confirmed by finding a loss of part or the whole of
the ‘red-reflex’ when a powerful light is shone on the
pupil). Other possible causes of gradual loss of vision,
such as optic nerve or retinal damage, can only be
detected by inspecting the retina through an oph-
thalmoscope. This requires practice, and you should
take every opportunity to use the ophthalmoscope by
inspecting the retinae of all the patients you examine.
Ophthalmoscopy is best carried out in a darkened
room to ensure that the pupils are dilated. The oph-
thalmoscope is an illuminated lens system which can
be focused on the retina. Patients are asked to stare
fixedly at a point on the wall behind the examiner.
The instrument is switched on and held by its handle
in the right hand. The examiner then places his right
eye against the lens opening and his left hand on the
patient’s forehead above their right eye. He then looks
through the aperture of the ophthalmoscope, brings
the instrument very close to the patient’s right pupil
by placing his forehead against his left hand on the
patient’s forehead. The light can be watched illumi-
nating the fundus, through the pupil, as the instru-
ment and the patient’s eye are brought close together.
The approach should be slightly from the temporal
side, at an angle of 10–15° to the direct line, to avoid
noses colliding! When the pupils are level, this
approach usually ensures that the optic nerve disc is
the first part of the fundus to come into view. If the
disc is not seen, a retinal artery should be followed
back until the edge of the pale yellow disc is seen.
The optic disc is cupped by chronic glaucoma and
swollen by papilloedema (see Fig. 2.3, page 46). Other
abnormalities that can be detected by careful fun-
doscopy of the rest of the retina include haemor-
rhages and exudates (in diabetes and hypertension),
retinal emboli and infarcts, and occasionally retinal
detachment. At the end of the examination, the
patient should be asked to look directly at the light of
the ophthalmoscope in order to inspect the macula.
Ears and nose
Do not forget to look into the ears to inspect the
external auditory canal and the ear-drum. Look up
the nose. The ears and nose are often forgotten dur-
ing routine examination but they are important,
particularly if there is any possibility of disease in
the head and neck.
Clinical examination of the ear requires an auro-
scope. This instrument directs a beam of light down
a conical metal speculum which is viewed through a
lens. The speculum is gently inserted into the exter-
nal auditory meatus, while the ear is pulled gently
upwards and backwards to straighten the external
auditory canal. Wax may be present and must
be removed before the tympanic membrane can
be seen.
The whole of the tympanic membrane can only be
seen if the angle of the speculum is altered. Normal
tympanic membranes vary in colour, translucence
and shape – so you should look at as many normal
tympanic membranes as possible. The external audi-
tory canal may contain wax or foreign bodies. You
may see otitis externa (dermatitis), blood or pus. The
tympanic membrane may be normal, torn (injury),
13
Chap-01.qxd 4/19/05 13:41PM Page 13
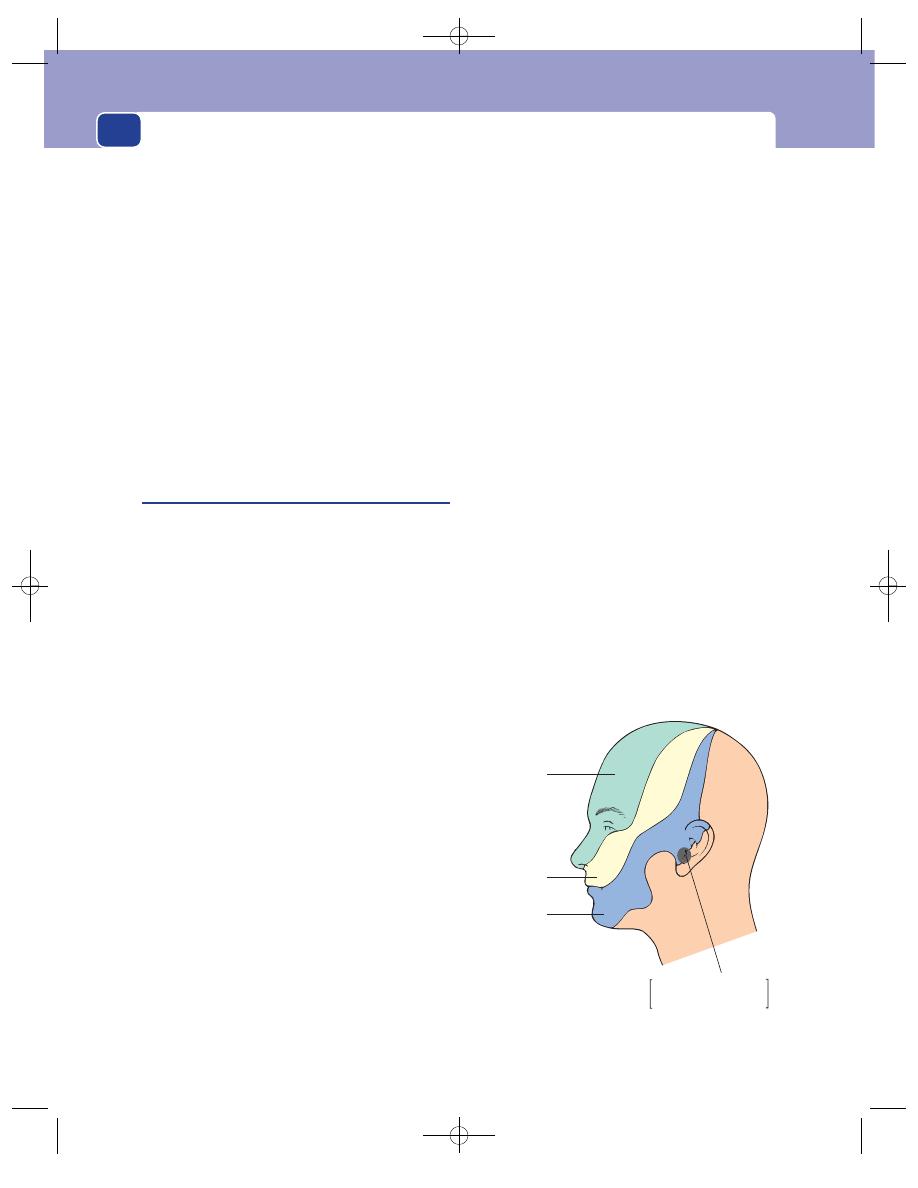
History taking and clinical examination
bulging and inflamed (acute otitis media), or perfo-
rated (chronic otitis media).
Mouth
Note the colour and state of the lips. Ask to see the
patient’s tongue; observe its movement, symmetry
and surface.
Look at the teeth and gums. Use a spatula to
inspect the soft palate, tonsils and posterior wall of
the oropharynx.
Neck
The important features to examine in the neck are
the jugular veins, the trachea, the thyroid gland and
the lymph glands.
Examine the cranial nerves
‘On Old Olympus Towering Tops A Finn And German
Picked Some Hops’ is the most-used mnemonic for the
names of the cranial nerves.
I Olfactory nerve
Ask the patient about their sense of smell. If thought
to be abnormal, it can be specifically tested with bot-
tles containing cloves, peppermint etc.
II Optic nerve
Visual acuity
Visual acuity is tested with a Snellen’s
chart at a distance of 6 metres. Vision is expressed as
a fraction of the normal: the smallest letter visible
with comfort is 6/6; if letters twice that size are all
that can be read, the vision is 6/12. The larger letter is
visible to the normally sighted at 60 metre. Below this
level of vision, ‘counting fingers’, ‘hand-movements’
and ‘perception of light’ are used to grade degrees of
blindness. Near-vision is tested by a card covered
with varying sizes of print.
Test the visual fields
Sit directly in front of the
patient, ask them to close one eye and look straight
at you with the other eye. Keeping your hand mid-
way between you and the patient, extend your arm
so that your hand is beyond your own peripheral
vision. Then gradually move it towards the mid-line
until it appears in your visual field. If you and the
patient have normal visual fields, you will both see
your finger at the same time.
III Oculomotor nerve
This nerve supplies all but two of the extrinsic eye
muscles, as well as the levator palpebrae superioris
and the muscle of accommodation. When it fails to
function, the eye turns downwards and outwards, the
upper lid droops (ptosis) and the pupil becomes fixed
(not responding to accommodation). Sometimes
individual muscles supplied by the third nerve can
be paralysed. To test the superior rectus muscle, ask
the patient to ‘look up’; the inferior rectus – ‘look
down’; the medial rectus – ‘converge’; and the inferior
oblique – ‘look up and out’.
IV Trochlear nerve
This nerve supplies the superior oblique muscle,
which turns the eye downwards and outwards. The
patient cannot perform this movement if the nerve is
damaged. The eye will look inwards and the patient
will experience diplopia below the horizontal plane.
V Trigeminal nerve
This nerve has sensory and motor functions. It is
sensory to the whole of the side of the face. The
cutaneous distribution of its three sensory divisions –
ophthalmic, maxillary and mandibular – is shown in
Figure 1.2.
The trigeminal nerve is also the sensory nerve of
the conjunctiva and the inside of the mouth. The
conjunctival reflex (ophthalmic division) is lost if
14
Ophthalmic
division
Maxillary
division
Mandibular
division
Auricular branch of
the vagus nerve
FIG 1.2
The distribution of the three sensory divisions of the
trigeminal nerve.
Chap-01.qxd 4/19/05 13:41PM Page 14
The clinical examination
the nerve is damaged. This is tested by touching the
conjunctiva with a ‘wick’ of cotton or tissue paper to
elicit a ‘blink’. Sensation in the nose, pharynx, roof
of mouth, soft palate and tonsil should also be tested.
The palatal reflex (maxillary division) is elicited by
placing a speculum against the palate to induce a
gag reflex. The sensitivity of the tongue, lower teeth
and mucous membrane over the mandible (mandi-
bular division) is tested by touching each area with
a spatula.
The taste fibres of the anterior two-thirds of the
tongue travel with the lingual nerve (one of the
branches of the mandibular division of the trigemi-
nal nerve) after leaving the geniculate ganglion as
the chorda tympani. Taste can be specifically tested
with sweet, sour, salt and bitter substances – such as
sugar, acid, salt and quinine – if this is felt to be
important.
The motor fibres of the trigeminal nerve run in
its mandibular division to the muscles of mastica-
tion – masseter, temporalis and the pterygoid mus-
cles. Ask the patient to clench their teeth and feel if
the masseter contracts.
VI Abducens nerve
This nerve supplies the lateral rectus muscle, which
turns the eye outwards. The eye will not move when
the patient attempts to look sideways and they will
experience diplopia.
VII Facial nerve
This is the motor nerve to the muscles of facial
expression. When a facial nerve fails to function, the
affected side of the face is flabby, the eyelids cannot
be closed properly, and the mouth becomes asym-
metrical when the patient tries to bare their teeth.
Whistling is impossible. The nucleus of the seventh
nerve is in the pons varolii. Any damage to the tract
or the nerve distal to the nucleus causes paralysis of
the whole of one side of the face; but a lesion above
the nucleus misses those fibres coming from the
opposite hemisphere to the upper part of the face, so
that the function of the forehead and eyelid muscles
is preserved. To test the facial nerve, ask the patient
to look up (the forehead should wrinkle), to close
their eyes tightly (test the strength of the orbicularis
oculi by trying to part the eyelids) and to show you
their teeth (lips should part symmetrically).
VIII Auditory nerve
This nerve innervates the hearing mechanism in the
cochlea and the position sense organs in the semi-
circular canals. Hearing can be tested very easily by
speaking softly and asking the patient to repeat your
words, or by asking them if they can hear your
thumb and finger rubbing lightly together close to
their ear. The deafness is called conductive when it
is the result of an obstruction in the external meatus,
tympanic membrane, middle ear cavity or ossicles
of the middle ear interfering with the normal pas-
sage of airborne sounds. This is tested by striking a
tuning fork and holding it next to the external audi-
tory meatus until the patient signals that sound can
no longer be heard. The base of the tuning fork is
then immediately placed firmly on the mastoid
process. If sound is still heard by bone conduction
(a negative Rinne’s test), the patient has a conductive
deafness. If the tuning fork is placed on the centre of
the forehead, an ear with a conduction deafness will
appreciate a louder sound. This is Weber’s test.
When there is nerve perception deafness, any
sound that can be heard will be loudest in the better
ear, and louder when the tuning fork is placed by
the ear than when it is placed on the bone, i.e. good
bone conduction
⫽ a normal cochlea and auditory
nerve, whereas poor bone conduction
⫽ a defective
cochlea and auditory nerve.
The sensitivity of the vestibular apparatus is tested
by assessing the response to syringing the external
meatus with warm and cold water. This is called the
caloric test. These tests should only be done under
careful supervision in the ENT department.
IX Glossopharyngeal nerve
This nerve is the sensory nerve of the posterior third
of the tongue. It supplies the taste receptors and the
sensory endings of the mucous membrane of the
pharynx.
It is also motor to the middle constrictor muscle
of the pharynx.
The sensory integrity of this nerve can be tested
by stroking the back of the oropharynx to evoke a
pharyngeal gag reflex.
X Vagus nerve
This is the motor nerve of the soft palate, pharynx
and larynx, and the sensory nerve of the heart, lungs
15
Chap-01.qxd 4/19/05 13:41PM Page 15
History taking and clinical examination
and gastrointestinal tract. When patients are asked
to open their mouths wide and say ‘Aarrh’, the soft
palate should arch upwards symmetrically. If one
side of the palate is paralysed, it will not move and
the uvula will be pulled over towards the function-
ing side. Loss of function of the recurrent laryngeal
nerves (branches of the vagus) should be suspected
if there is a change in the patient’s voice or an inabil-
ity to cough. The vocal cords must be examined
with a laryngeal mirror to confirm the diagnosis.
XI Spinal accessory nerve
This nerve supplies the trapezius and sterno-mastoid
muscles. The function of these muscles is tested by
asking the patient to shrug their shoulders and to
press the point of their chin downwards against your
hand.
XII Hypoglossal nerve
This is the motor nerve of the tongue. When one
hypoglossal nerve is paralysed, the tongue will deviate
to that side when the patient tries to push it for-
wards. The weak side will also be wasted (see Fig.
10.14, page 261).
Examine the chest wall and lungs
Inspection
The colour and respiratory rate of the patient indi-
cate the adequacy of ventilation. Cyanosis caused by
cardiopulmonary disease is most easily appreciated
by inspecting the inner aspect of the lips. Cyanosis
of the nail beds and the tip of the nose and ears may
be caused by a peripheral or central abnormality.
Patients may be polycythaemic rather than cyanotic
if the peripheral tissues are a deep reddish-purple
colour and their face is red and plethoric. Cyanosis
is difficult to detect in anaemic patients.
Count the rate of respiration and notice the
rhythm. A fluctuating respiratory rate and volume,
with periods of apnoea interspersed between episodes
of tachypnoea, is called Cheyne–Stokes or periodic
respiration. It is caused by variations in the sensitivity
of the respiratory centre to normal stimuli, and
occurs commonly in patients with heart failure and
following severe cerebrovascular accidents.
Notice if respiration seems to require voluntary
effort and compare the durations of inspiration and
expiration. Watch the chest during inspiration to
see if there is any inward movement of the inter-
costal spaces (paradoxical movement). This is usu-
ally caused by obstruction to the inflow of air into
the lungs, but in an injured patient may indicate
instability of a segment of the chest wall (e.g. two
sets of fractures).
Record any abnormality in the shape of the chest.
The two common deformities are funnel chest (pec-
tus excavatum) and pigeon chest (pectus carinatum)
(see Fig. 8.29, page 235).
Palpation
Trachea
Check the position of the trachea at the
suprasternal notch.
Chest expansion
Spread your hands around the
chest so that your thumbs just meet in the mid-line.
Ask the patient to take a deep breath. Your thumbs
should be dragged apart to a distance roughly
equivalent to half the chest expansion. When the
expansion is asymmetrical it will be felt and seen.
16
Revision panel 1.5
Common causes of pleuritic pain
Pleurisy
Pneumonia
Pulmonary infarction (thromboembolic)
Neoplasia (primary and secondary)
Fractured ribs
Muscle strains/prolapsed intervertebral disc
Herpes zoster
Bornholm disease (Coxsackie virus)
Don’t forget pathology below the diaphragm,
e.g. ruptured spleen, Curtis–Fitz–Hugh
syndrome (see Chapter 15)
Revision panel 1.6
Common causes of haemoptysis
Pneumonia
Carcinoma of the bronchus
Chronic bronchitis
Pulmonary tuberculosis
Pulmonary infarction (thromboembolic)
Bronchiectasis
Chap-01.qxd 4/19/05 13:41PM Page 16
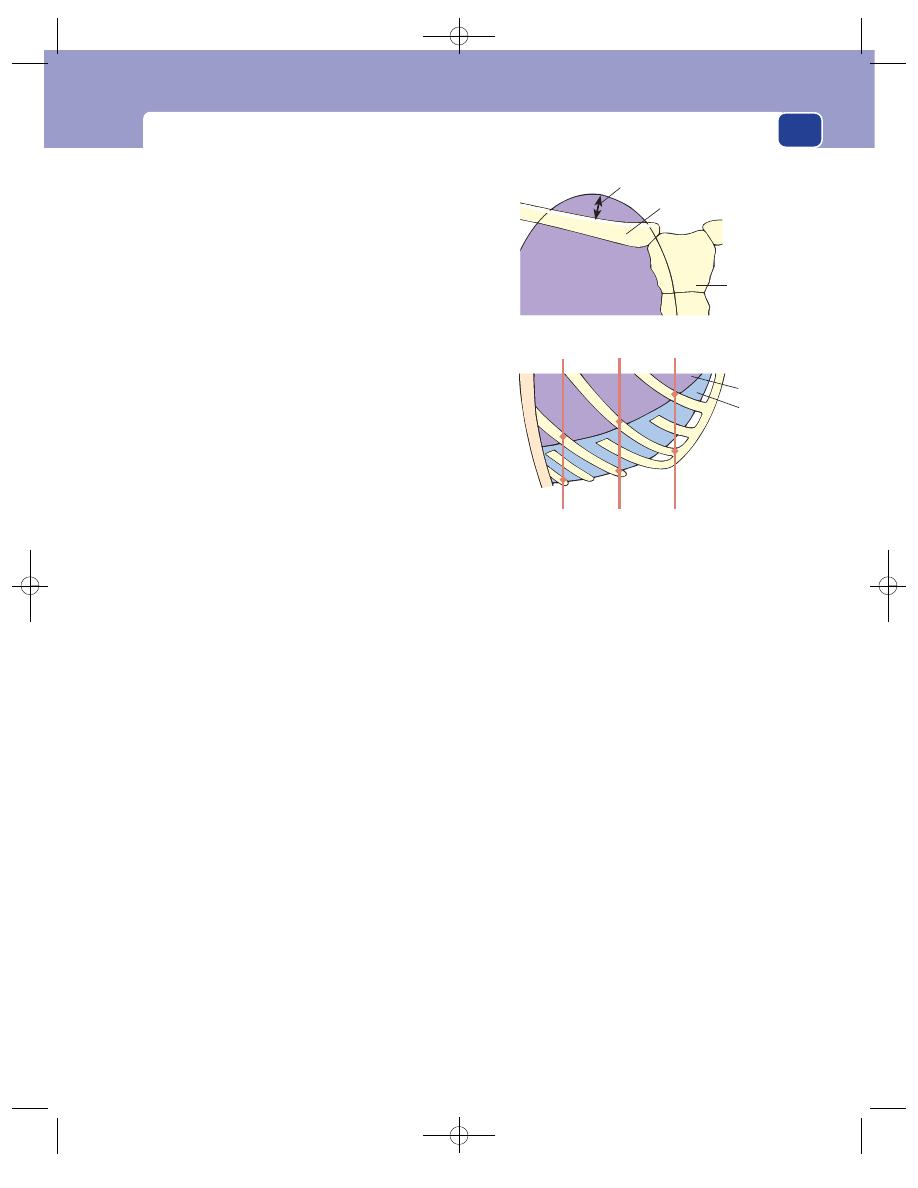
The clinical examination
Chest expansion is the difference between the
circumference of the chest at full inspiration and
full expiration, measured at the level of the
nipples.
Apex beat
The apex beat is the lowest and most lat-
eral point at which you can feel the cardiac impulse.
It will move laterally if the heart enlarges but may
also move medially or laterally if the mediastinum
shifts. The mediastinum (and the trachea) will move
to one side if it is pulled over by a collapsed, con-
tracting lung or pushed over by air or fluid in the
opposite pleural cavity.
Tactile vocal fremitus (Fig. 1.4, page 18)
Place your
whole hand firmly on the chest and ask the patient
to say ‘99’. The vibrations that you can feel with your
hand are called the vocal fremitus. Compare the
strength of these vibrations on either side of the
chest, front and back, and over the apical, middle
and basal zones of the lung. To feel vocal fremitus
the sound waves must be conducted through the air
in the bronchi, bronchioles and alveoli to the chest
wall. A blocked bronchus or a layer of fluid or air
between the visceral and parietal layers of the pleura
(a pleural effusion) will suppress the conduction of
the sound waves and reduces the intensity of the
palpable fremitus. A stiffening of the lung tissue
with patent air passages, which occurs in very early
pneumonia, increases conduction through the lung,
and tactile vocal fremitus is increased.
Palpate both axillae.
Percussion
The whole of the surface of both lungs must be per-
cussed. The surface markings of the lungs are shown
in Figure 1.3. Place one hand flat on the chest wall,
keeping the finger you intend to strike straight and
firmly applied to the underlying skin. Tap the centre
of the middle phalanx of this finger with the tip of
the middle finger of the other hand. Listen carefully
to the sound and compare it with the sound pro-
duced by percussing the same area on the other side
of the chest.
The two areas most often forgotten when per-
cussing the chest are the lateral zones high in the
axillae and the anterior aspect of the apices behind
the clavicles. Percuss the latter area by striking the
clavicle directly with the percussing finger.
The normal chest gives a resonant sound when
percussed; a sound which is, to some extent, felt
by the percussing finger as well as being heard.
Anything solid in the pleural space or in the sub-
stance of the lungs decreases the resonance and
makes the sound dull. Any extra air, whether in the
pleural space (a pneumothorax) or in the lung sub-
stance (an emphysematous bulla or multiple bullae),
makes the sound more resonant (hyper-resonance)
(page 19).
In the presence of a large pneumothorax, a ring-
ing resonance can be heard with a stethoscope when
the percussion is performed by tapping a coin held
against the chest wall with a second coin.
Auscultation
The normal sounds of breathing can be heard all
over the chest except over the heart and spine (page
20). They consist of an inspiratory sound followed
immediately by a shorter, softer, expiratory sound.
There is no gap between the two phases. This pattern
17
Apex
Base
2.5 cm
Sternum
Clavicle
Lung
Pleura
6
8
8
10
10
12
Edge of
erector
spinae
Mid-
axillary
line
Mid-
clavicular
line
Lung
6
8
8
10
Pleura
10
12
FIG 1.3
The surface markings of the lung and pleura.
Chap-01.qxd 4/19/05 13:41PM Page 17
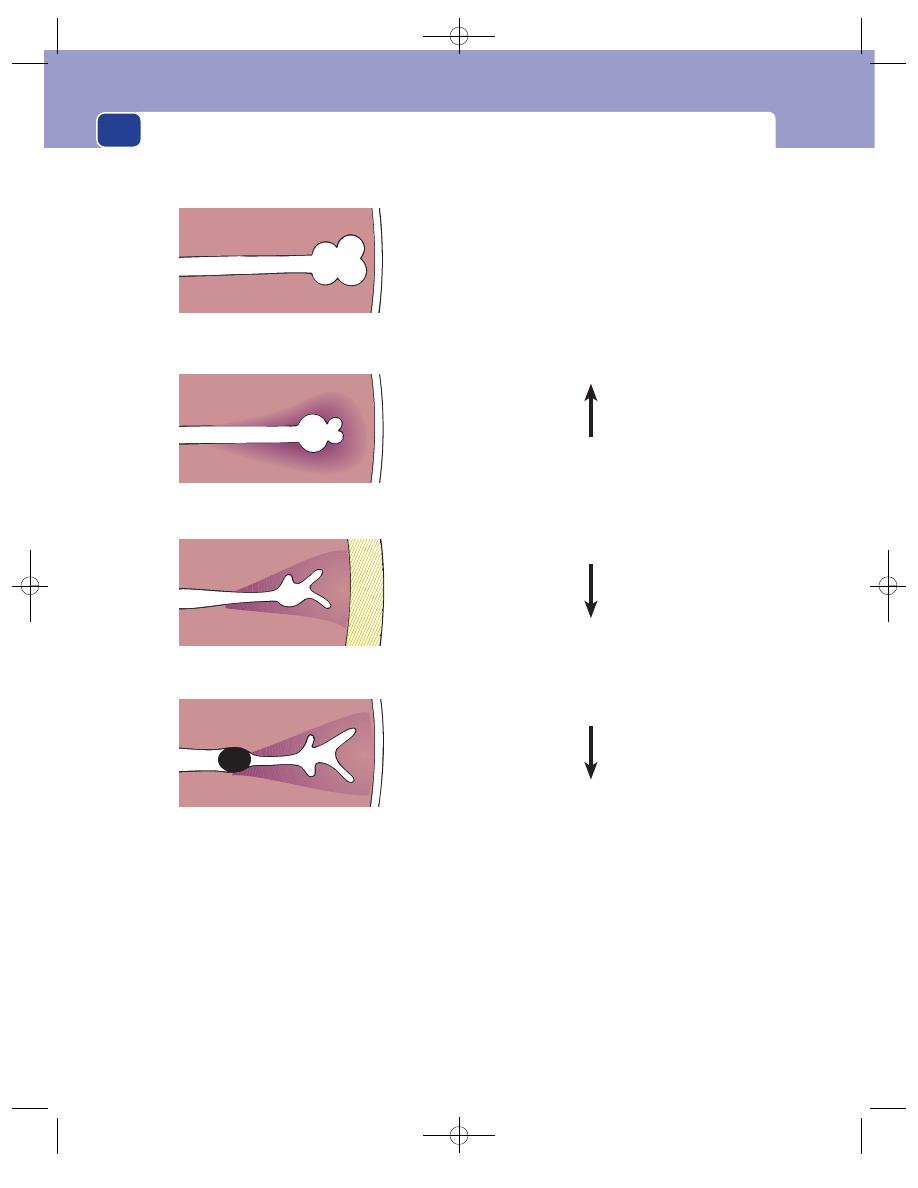
History taking and clinical examination
is known as vesicular breathing and is caused by
the movement of air in and out of the smaller bron-
chioles and alveoli – a rustling noise similar to that
of gas being blown down plastic tubing.
The sound of air moving in the larger bronchi-
oles and main bronchi is heard when the periphery
of the lung has been solidified by pneumonia or
collapse (atelectasis). This sound is harsher and
louder than the low rustle of vesicular breathing.
The inspiratory and expiratory phases are of equal
length and separated by a short, silent gap. This is
called bronchial breathing. The quality of the sound
and the presence of the gap are the two distinguish-
ing features.
The pitch of bronchial breathing may be high or
low. The high-pitched variety is sometimes called
tubular bronchial breathing. The low-pitched vari-
ety, which sounds like the noise produced by blow-
ing across the mouth of a jar, is called amphoric
bronchial breathing. Amphoric sounds are heard
when air is passing in and out of a cavity in the lung
such as a tuberculous cavity.
18
Collapse
Air passages blocked
Vibrations diminished or absent
Say
'99'
Pleural effusion or
Pneumothorax
Air passages pushed
away from chest wall
Vibrations diminished or absent
Say
'99'
Consolidation
Air passages patent
Lung substance denser
Vibrations increased
Say
'99'
Normal
Vibrations palpable
Say
'99'
TACTILE VOCAL FREMITIS
FIG 1.4
Tactile vocal fremitus can only be felt if there are patent air passages right out to the chest wall.
Chap-01.qxd 4/19/05 13:41PM Page 18
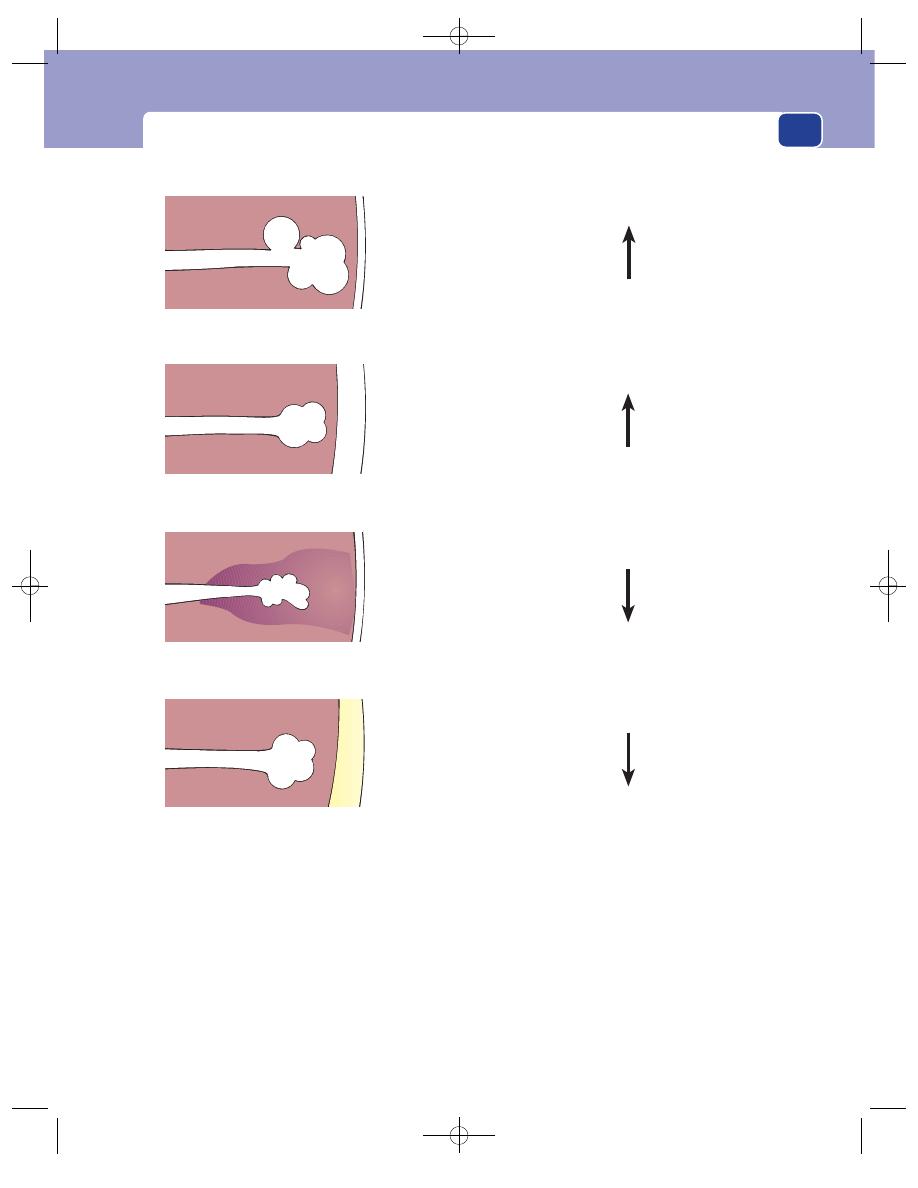
The clinical examination
There is a type of breath sound mid-way
between vesicular and bronchial breathing, known
as bronchovesicular breathing. In this variety the
inspiratory and expiratory sounds are of equal
length and slightly harsher than those of vesicular
breathing, but there is no gap between the two
phases. Bronchovesicular breathing is often heard
in normal people over the anterior aspect of the
upper lobes, where there are large bronchi near the
surface of the lung, and must not be mistaken for
bronchial breathing.
Absent sounds
Breath sounds are abolished or diminished by any
process which reduces the normal conduction of
sound through the lung substance and chest wall.
The two common causes are bronchial obstruction
(producing collapse of the distal part of the lung)
and pleural effusion or pneumothorax.
When the lung alveoli are full of fluid, exudate
or pus (consolidation) but the air passages remain
patent, the thickened lung transmits the sound
19
Increased air in the lungs
(Emphysema)
Increased resonance
Air in the pleural cavity
(Pneumothorax)
Increased resonance
Less air in the lungs
(Consolidation, Collapse)
Diminished resonance
Fluid in the pleural cavity
(Pleural effusion, Haemothorax,
Empyema)
Diminished resonance
('Stony dull')
PERCUSSION
FIG 1.5
The causes of changes in lung resonance.
Chap-01.qxd 4/19/05 13:41PM Page 19
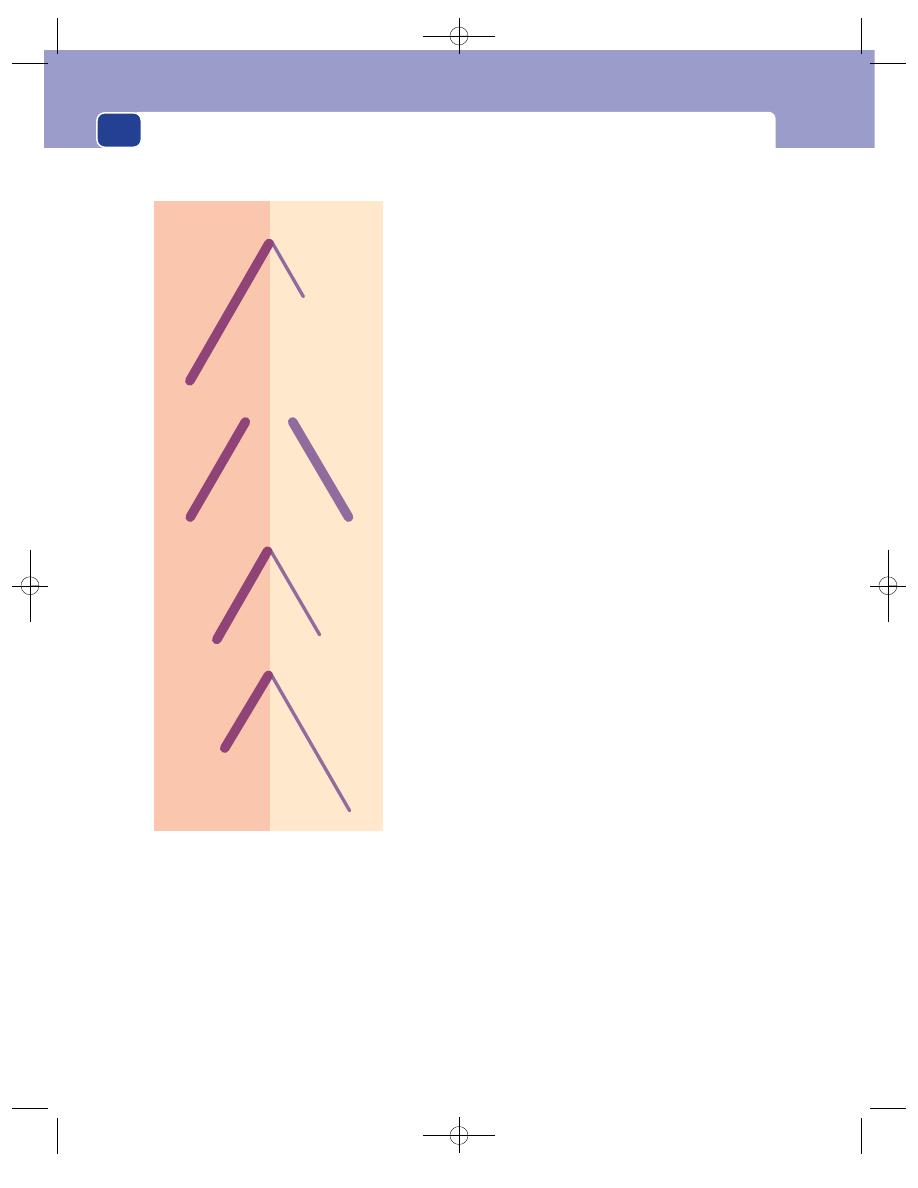
History taking and clinical examination
from the larger bronchi. Thus bronchial breathing
is heard over an area of consolidated lung. There
are, however, no breath sounds over an area of col-
lapsed lung.
Added sounds
There are three varieties of added sounds: rhonchi,
râles and crepitations. These are often referred to as
wheezes, coarse crackles and fine crackles by the
younger generation of pulmonary physicians.
Rhonchi/wheezes
These are the whistling noises
made by air passing through narrowed air passages.
They are commonly heard in patients with asthma or
chronic bronchitis. Their pitch depends upon the
velocity of airflow and the diameter of the bronchioles
from which they originate. They are unmistakable.
20
Vesicular
Bronchial
Bronchovesicular
Asthmatic
Expiration much shorter and softer
than inspiration
No gap between each phase
Inspiration and expiration of equal
length and quality (harsh and loud)
Gap between the two phases
Inspiration and expiration of equal
length but expiration is softer and
smoother
No gap between each phase
Prolonged expiration, usually assoc-
iated with inspiratory and expiratory
rhonchi
Inspiration
Expiration
BREATH SOUNDS
FIG 1.6
The four types of breath sound.
Chap-01.qxd 4/19/05 13:41PM Page 20
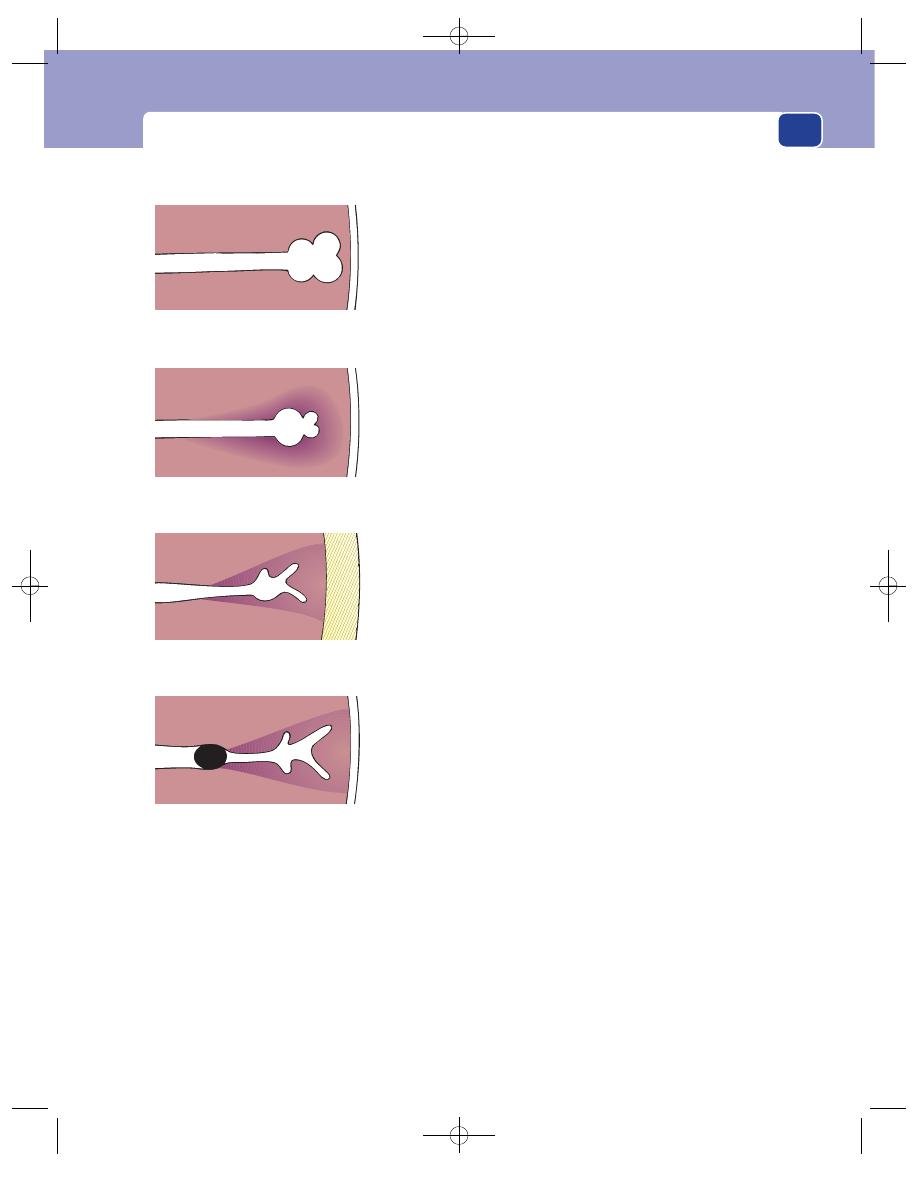
The clinical examination
Râles/coarse crackles
These are the coarse bubbling
noises caused by air passing through bronchioles con-
taining water, mucus or pus. The sound is identical to
that made by air bubbling through water. Moving the
fluid may abolish the noise, so ask the patient to take
a deep breath and cough, and then listen again. If the
bubbling sounds disappear, they must have been râles
because crepitations cannot be abolished in this way.
Crepitations/fine crackles
These are fine crackling
sounds similar to the noise heard when you hold a
few hairs close to your ear and roll them between
your thumb and index finger. They are thought to
be produced as the alveoli and their ducts pop open
to allow air to enter when there is interstitial oedema.
Crepitations are heard over areas of consolidation,
such as pneumonia, and often provide important
evidence of left ventricular failure. They are not
abolished by coughing.
Some authorities do not distinguish râles from
crepitations and use the all-embracing term moist
sounds for either variety.
21
Normal
Vesicular sounds audible
Consolidation
Bronchial sounds audible,
caused by increased sound
conduction from large bronchi
Pleural effusion or
Pneumothorax
No sounds audible as layer
of fluid or air prevents conduction
of sound to the surface
Collapse
No sounds audible as obstruction
of bronchus stops sound conduction
EFFECT OF LUNG DISEASE ON THE BREATH SOUNDS
FIG 1.7
The causes of abnormal breath sounds.
Chap-01.qxd 4/19/05 13:41PM Page 21
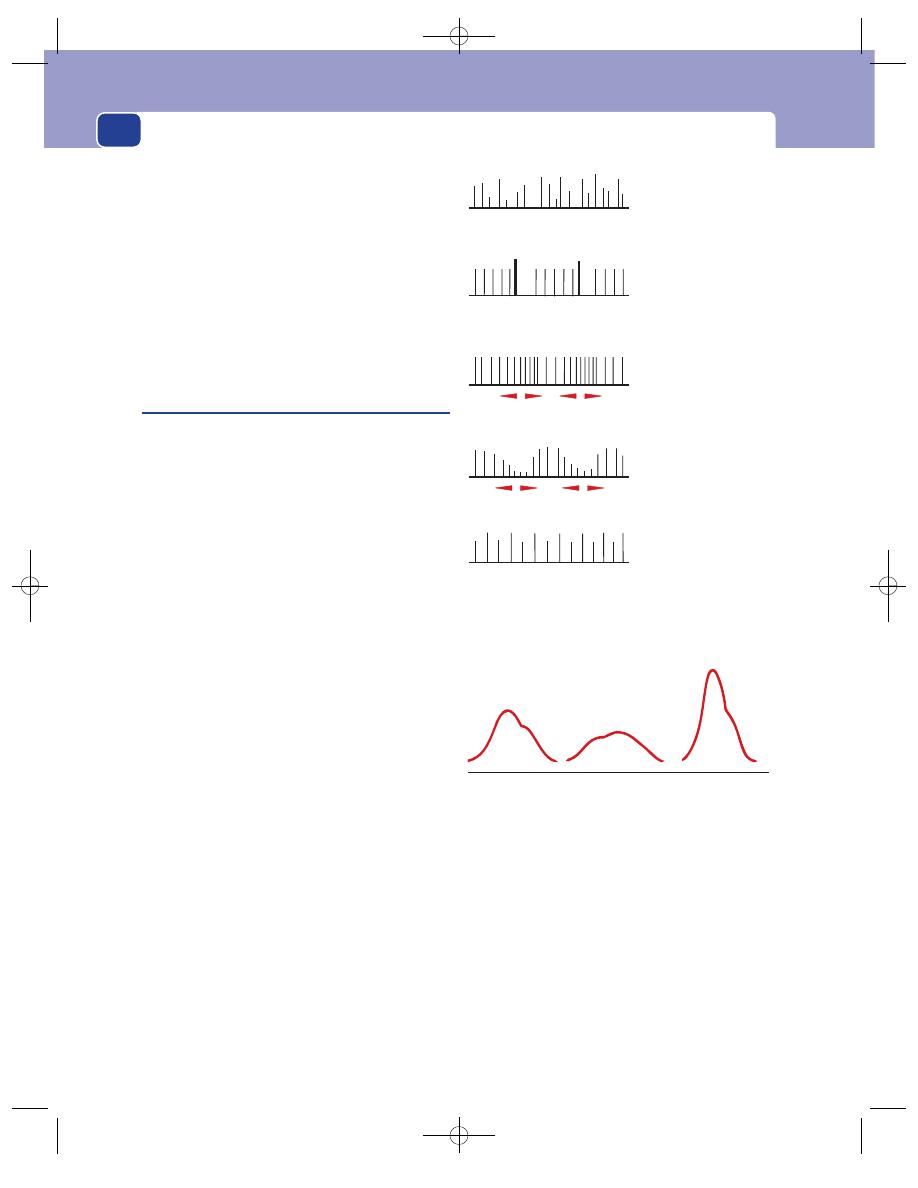
History taking and clinical examination
Pleural rub
The visceral and parietal layers of the
pleura normally slide easily over one another but,
if the pleura is inflamed, the roughened pleural sur-
faces rubbing together produce a noise which is
similar to the sound heard when a finger is pressed
hard onto a pane of glass and then slid across it. It is
a mixture of grating and squeaking sounds. A pleural
rub can only be heard when the chest is moving,
i.e. during inspiration or expiration. The patient
usually complains of pleuritic pain over an area
where there is an audible rub.
Examine the heart and circulation
Much will have been learnt about the circulation from
your initial observations of the patient’s colour and
breathing. It is common practice to feel the pulse when
you take the patient’s hand at the beginning of the
examination. Any abnormalities detected at this stage
require reassessment by further careful palpation.
The pulse
The following features should be observed and
recorded.
The rate
Express the rate in beats/minute. Do not
count the pulse for 5 seconds and multiply by 12;
always count for 15 seconds or longer if the beat
feels irregular.
The rhythm
The pulse beat may be regular or irreg-
ular. When the pulse is irregular it may have a regular
recurring pattern or be totally irregular. The latter is
sometimes called an irregularly irregular pulse and
indicates atrial fibrillation. Some common varieties
of irregular pulse are shown in Figure 1.8.
The volume
The examining fingers can appreciate
the expansion of the artery with each beat and con-
sequently get an impression of the amount of blood
passing through the artery. Patients with a high car-
diac output have a strong pulse. Patients in haemor-
rhagic (hypovolaemic) shock have a weak, thin,
‘thready’ pulse.
The nature of the pressure wave
Every pressure
wave has definable characteristics such as the rate of
increase and decrease of pressure and the height of
the pressure (see Fig. 1.9).
A steep rise followed by a rapid fall, with a large
pulse pressure (high peak), is called a collapsing
or water-hammer pulse and is typical of aortic
regurgitation. Conversely, a tight aortic stenosis
causes a slow rise and fall.
The shape of the pulse wave can be appreciated
more easily over the carotid than the radial artery.
22
Atrial fibrillation
Rhythm and volume
irregularly irregular
Extrasystoles
Premature strong
beat followed by
a pause
Sinus arrhythmia
Faster during inspiration
Pulsus paradoxus
Weaker during
inspiration
Pulsus alternans
Alternating strong
and weak beats
(i = inspiration)
i
i
i
i
FIG 1.8
Common variations of the rhythm and volume of
the pulse.
Normal
The dicrotic
notch is not
normally
palpable
Flattened
Slow rise and
fall, called
anacrotic,
caused by
aortic stenosis
Accentuated
Rapid rise and fall,
called a water-
hammer pulse,
caused by aortic
incompetence
and patent ductus
arteriosus
FIG 1.9
Variations of the pulse wave.
Chap-01.qxd 4/19/05 13:41PM Page 22
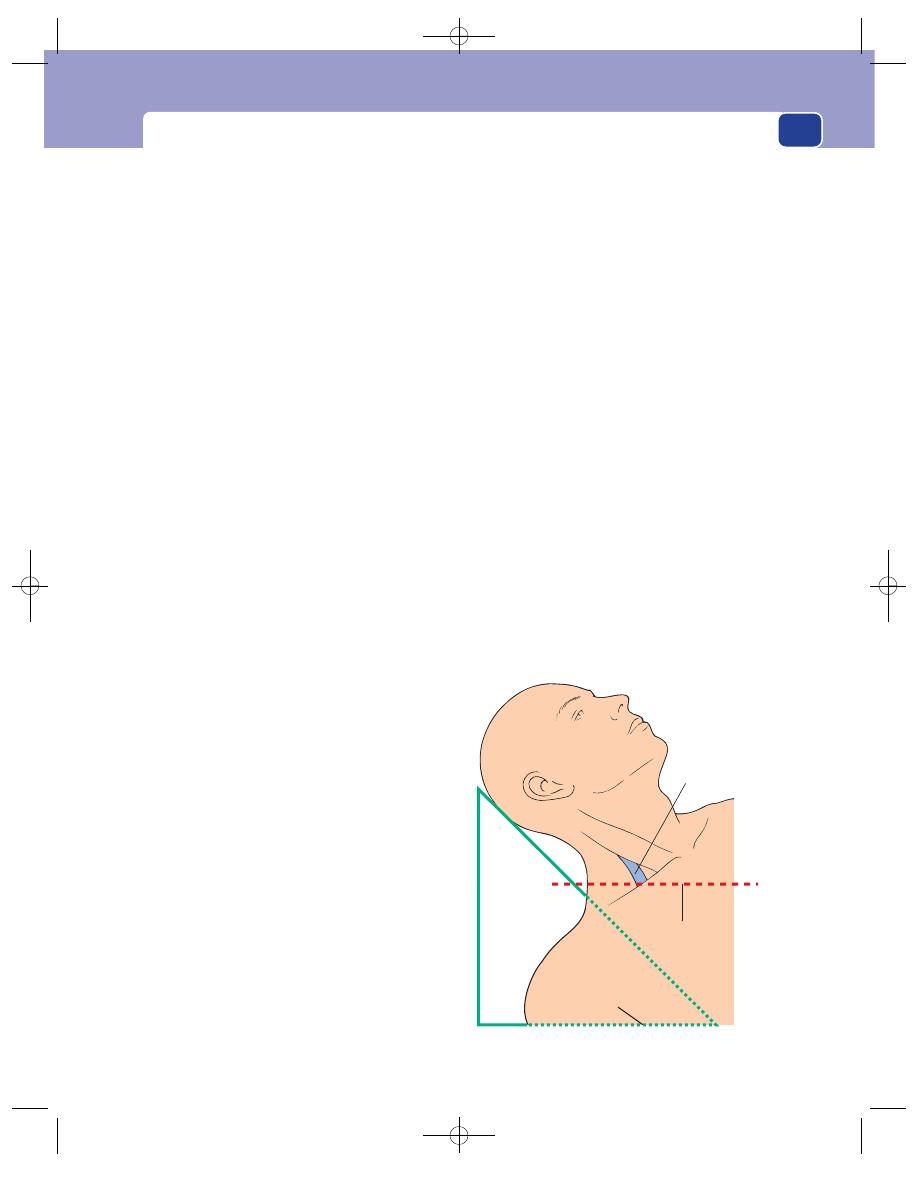
The clinical examination
The nature of the artery
It is relatively easy to esti-
mate the diameter of the radial artery and guess the
thickness of its wall, but the presence or absence of
thickening of the radial artery gives no indication
of the thickness of other vessels in the body.
Measure the blood pressure
The blood pressure is usually measured in the
brachial artery with a sphygmomanometer. The cuff,
which must fit snugly and be at least 10 cm wide
(a narrow cuff gives false readings), should be firmly
wrapped around the middle of the upper arm and
inflated above the systolic pressure (250 mmHg). It
should then be slowly deflated until the commence-
ment of blood flow below the cuff is detected by
listening over the brachial artery at the elbow with a
stethoscope or palpating the pulse at the wrist. The
pressure at this point is the systolic blood pressure.
(The sounds which indicate the commencement
of flow in the brachial artery below the cuff are caused
by turbulent blood flow. They were first described
by Korotkoff and are known as Korotkoff sounds.)
The cuff pressure is further reduced until the
Korotkoff sounds suddenly diminish or, more often,
disappear. This is the diastolic pressure.
It is worth repeating both measurements on sev-
eral occasions with the patient sitting and lying down
and again at the end of the examination when the
patient is less worried.
Whenever there is the possibility of disease of the
aorta and its branches, the blood pressure should be
measured in both arms.
Remember that the readings from a very fat arm
will be falsely high by as much as 10 mmHg.
Inspect the head and neck again
You will already have looked at the patient’s skin, face
and general demeanour. Look again for the signs
particularly indicative of cardiovascular disease –
cyanosis, plethora and dyspnoea.
Xanthomata
These are grey-yellow plaques of lipid
in the skin. They often occur in the skin of the upper
eyelid (see Fig 3.47, page 103). Their presence may
indicate an abnormal lipid metabolism such as hyper-
lipidaemia, but they may occur in patients with nor-
mal blood lipids.
Arcus senilis
This is a white ring at the junction of
the iris and sclera (see Fig. 8.14, page 227). It is said
to be more common in people with advanced arte-
riosclerosis, but in practice is not a reliable indicator
of the presence of vascular disease (see Chapter 8,
page 226). It may indicate the presence of a hyper-
lipoproteinaemia if present in a patient under the
age of 40 years.
The jugular venous pressure
The pressure in the
great veins is slightly greater than the pressure in the
right atrium. The pressure in the right atrium is one
of the most important influences of cardiac activity.
An increase in the right atrial pressure increases car-
diac output by stimulating an increase of cardiac
contractility and rate. The right atrial pressure there-
fore ‘drives’ the heart. The pressure in the right atrium
can be estimated clinically from the pressure in the
internal jugular veins. In a normal person, reclining at
45°, the great veins in the neck are collapsed. There
should be no visible venous pulsations above the
level of the manubrio-sternal joint, which, when
the patient is reclining at 45°, is at the same level as
the mid-point of the clavicles (see Fig. 1.10).
The right atrial pressure is raised if there are vis-
ible pulsations in the internal jugular veins when
the patient is reclining at 45°. The vertical distance
between the upper limit of the venous distension
and the level of the clavicle should be estimated by
eye and expressed and recorded in centimetres.
23
Internal jugular
vein
45
°
Level of
manubriosternal
joint
FIG 1.10
Measurement of the jugular venous pressure.
Chap-01.qxd 4/19/05 13:41PM Page 23
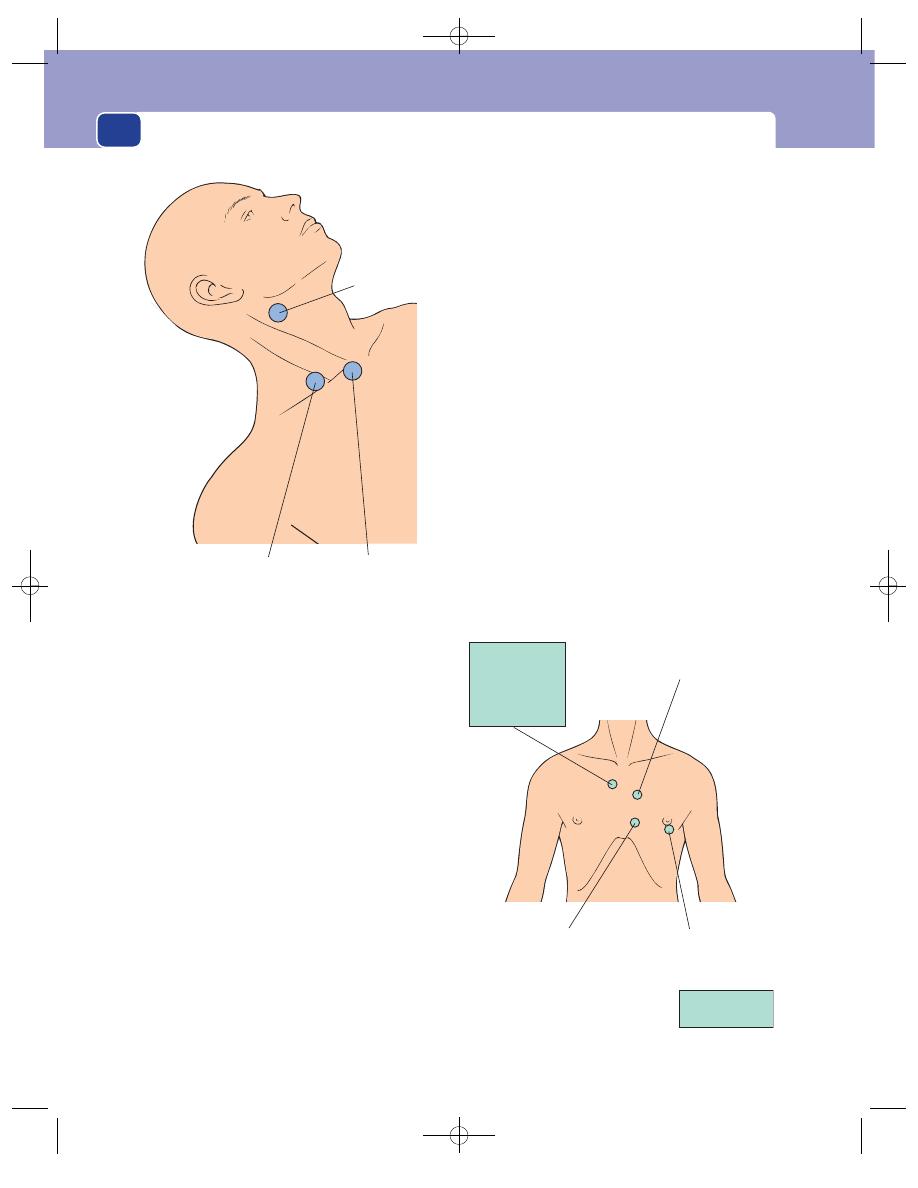
History taking and clinical examination
Obstruction of the great veins in the superior
mediastinum will also cause distension of the neck
veins, but there will not be a visible venous pulse wave.
Neck arteries
Feel the pulses in the neck and listen
along their whole length, especially over the sterno-
clavicular joints, in the supraclavicular fossae, and
at the level of the hyoid bone just below the angle of
the jaw. These sites correspond to the origins of the
subclavian, vertebral and internal carotid arteries,
respectively (see Fig. 1.11).
Examine the heart
Inspection
The heart may be seen to be beating rap-
idly or to be heaving up the chest wall with each beat.
Palpation
Place your whole hand firmly on the
chest wall, just below the left nipple, and ascertain
the strength of the cardiac impulse. It may be weak,
normal or heaving in nature. The apex beat is the
lowest and most lateral point at which the cardiac
impulse can be felt. It should be in the fifth inter-
costal space, near the mid-clavicular line (an imagi-
nary vertical line which passes through the middle
of the clavicle). The apex beat moves laterally and
may be felt as far out as the mid-axillary line if the
heart is enlarged. It may also be possible to feel vibra-
tions, called thrills, which correspond to audible
heart murmurs. Thrills may be felt during systole,
diastole or throughout the whole cardiac cycle.
Remember to palpate the back of the chest. Thrills
from abnormalities of the aorta, such as a patent
ductus arteriosus or a coarctation of the aorta, are
conducted posteriorly as well as anteriorly.
It is advisable to feel the femoral pulses at this stage.
Percussion
The area of cardiac dullness should be
delineated by percussion.
Auscultation
The whole of the anterior aspect of
the heart must be examined with the stethoscope,
but the areas where the sounds from the four valves
are best heard are shown in Figure 1.12.
24
Pulmonary area
Left second interspace
Tricuspid area
Left fourth interspace
Aortic area
Right second
costochondral
junction
Lean the patient
forwards and
also listen along
the left side of
the sternum
Mitral area
Fifth space, mid-
clavicular line
Turn the patient
towards the left
FIG 1.12
Areas of cardiac auscultation.
Listen over:
The sterno-
clavicular joints
Origin of the innominate
artery (right) and common
carotid artery (left)
The carotid
bifurcations
Origin of the
internal carotid
artery
The supra-
clavicular fossae
Origin of the
vertebral arteries
FIG 1.11
The sites of auscultation for vascular bruits on the neck.
Chap-01.qxd 4/19/05 13:41PM Page 24
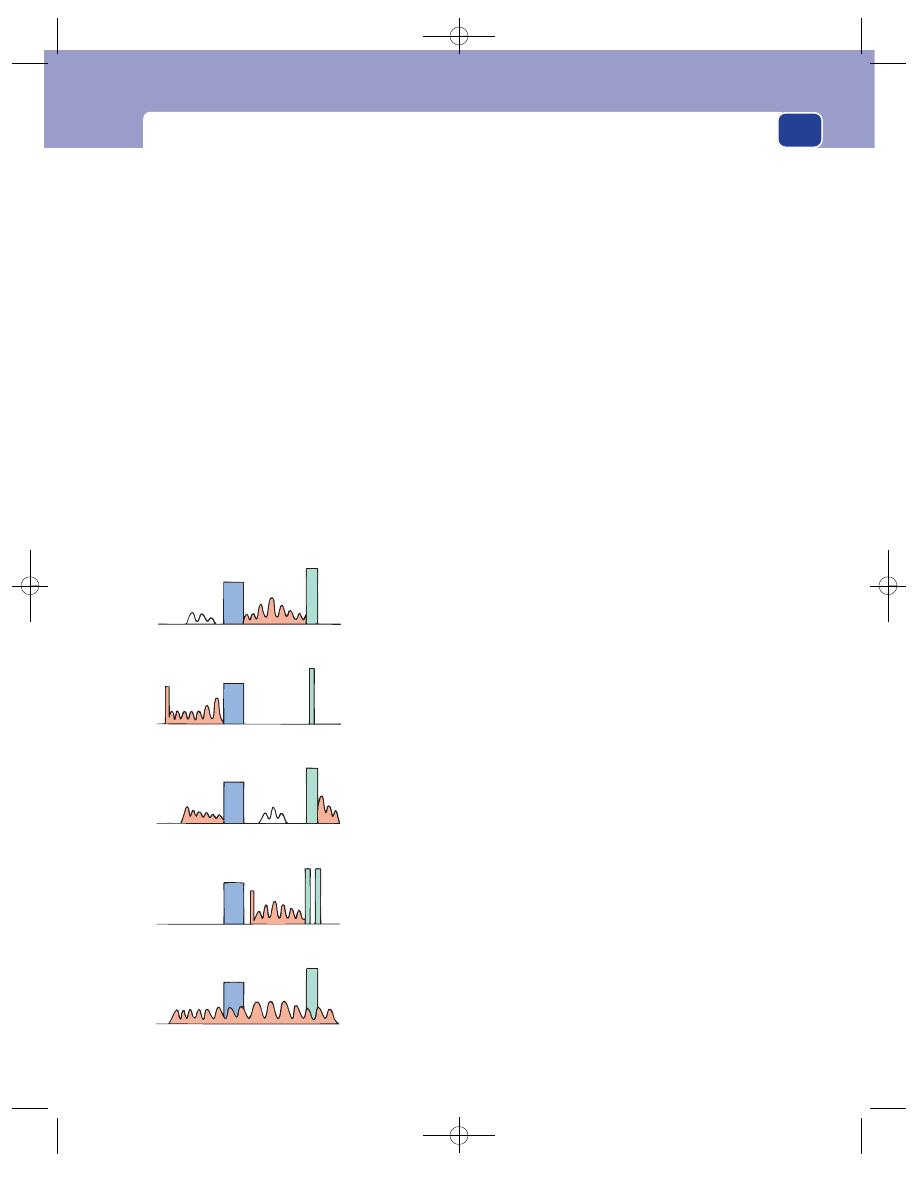
The clinical examination
Begin by listening at the apex of the heart – the
mitral area. Identify the first and second heart sounds.
The heart sounds are traditionally described as sound-
ing like the words lub-dub; that is to say, the first sound
is slightly longer and softer than the second sound. As
this is not always the case, it is wise to confirm that the
sound you believe to be the first sound corresponds to
the beginning of the cardiac impulse or coincides with
the subclavian or carotid pulse. Having decided which
sound is which, listen carefully to the second sound.
It may be sharper and shorter than usual – almost a
click – or it may be split. A double, or split, second
sound occurs when the aortic and pulmonary valves
close asynchronously. A double sound can be heard
when the sounds are 0.2 or more seconds apart and
indicates pulmonary hypertension.
Next, listen carefully to the intervals between the
two main sounds, and between diastole and systole,
for any additional heart sounds or murmurs.
Murmurs are caused by turbulent flow and the
vibration of parts of the heart. They may vary in
nature from a low-pitched rumble to a high-toned
swish. Try to decide whether the murmur occupies
the whole or part of diastole or systole and whether
its intensity changes.
Think of the way you are going to record your
findings (see Fig. 1.13), two blocks for the main
heart sounds (M1 and A2) and a zig-zag line for the
murmur. Imagine your drawing as you listen to the
sound and you will find it easier to define the timing
of the murmur. A detailed description of the many
heart sounds and their interpretation is beyond the
scope of this book. The student must read a text-
book of cardiology, but Figure 1.13 illustrates the
common types of murmur and their likely causes.
The exercise just described must be repeated
over the other three areas where the aortic, pul-
monary and tricuspid valve sounds are best heard.
25
Mitral incompetence
Mitral stenosis
Aortic incompetence
Aortic stenosis
Patent ductus arteriosus
Pansystolic murmur
Soft first sound
May be a short mid-diastolic
murmur preceded by a third
sound
Diastolic murmur with a
presystolic crescendo preceded
by an opening snap (o.s.)
Loud first sound
Early diastolic murmur
May be a soft mid-diastolic
murmur
Systolic murmur preceded
by an ejection click (e)
Split second sound
‘
Machinery’ murmur
Continuous throughout
systole and diastole
M
A
A
M
A
M
M
A
M
A
o.s.
e
FIG 1.13
The sounds of some common cardiac abnormalities (M
⫽ 1st heart sound, A ⫽ 2nd heart sound).
Chap-01.qxd 4/19/05 13:41PM Page 25
History taking and clinical examination
Some murmurs will be audible in more than one
area. The site of maximum intensity of a murmur
usually indicates its site of origin. Find this by ‘inch-
ing’ the stethoscope over the chest wall between the
areas. The same technique should be used to assess
whether murmurs in the aortic area are conducted
into or coming from the neck.
The sounds at the apex, from the mitral valve,
can be made louder by asking the patient to turn
over onto their left side; the aortic valve sounds can
be amplified by asking the patient to lean forwards.
Always listen to the heart sounds at the back of the
chest. The murmur of a patent ductus or coarctation
can often be heard over the aorta, posteriorly, just to
the left of the mid-line.
Test for oedema
Oedema commonly appears first in the feet and
ankles, but may be more apparent in the sacral and
buttock regions if the patient has been bedridden
for some time. Cardiac oedema is very soft, ‘pits’ eas-
ily and often gives the skin a pale, waxy, transparent
appearance.
Examine the abdomen
Examination of the abdomen is described in detail
in Chapter 16. It has been put there in the hope that
you will read it whenever you refer to other parts of
the chapter. A large amount of the surgical disease
presenting to a surgical clinic is intra-abdominal
and so a good technique for abdominal examina-
tion is essential.
Examination of the abdomen follows the standard
pattern.
■
Inspection for asymmetry, distension, masses,
visible peristalsis and skin discolouration.
■
Palpation for superficial and deep tenderness,
the normal viscera (liver, spleen and kidneys)
and any abnormal masses.
■
Percussion of the liver and splenic areas and
any other masses.
■
Auscultation for bowel sounds and vascular
bruits.
■
Rectal examination and vaginal examination.
There are four things that are easy to forget, so do
them before you start general palpation.
1. Palpate the supraclavicular lymph glands.
2. Palpate the hernial orifices.
3. Feel the femoral pulses.
4. Examine the genitalia.
Two further things which often get forgotten are
auscultation and the rectal examination, but you
must leave these to the end.
Examine the limbs
There are four main tissues to be examined in a
limb: the bones and joints, the muscles and soft
tissues, the arteries and veins, and the nerves. The
first three are often involved in surgical disease and
their examination is described in Chapters 4 and 7.
Only the examination of the peripheral nerves is
described here.
Examine the peripheral nerves
The nerves in the limbs serve three functions: motor,
sensory and reflex. Examine each of these functions
in turn.
26
Revision panel 1.7
Common causes of ankle swelling
Dependency/immobility
Pregnancy
Heart failure
Low plasma proteins
Chronic venous insufficiency
Deep vein thrombosis
Lymphatic insufficiency
Chronic renal failure (nephrotic syndrome)
Revision panel 1.8
Classification of muscle strength
5
Normal
4
Weak but can overcome gentle resistance
3
Cannot overcome gentle resistance but can
overcome gravity
2
Cannot overcome gravity but muscle
contracts
1
Barely perceptible muscle contractions
0
No contractions
Chap-01.qxd 4/19/05 13:41PM Page 26
The clinical examination
Motor nerve function
Voluntary movement
Ask the patient to move each
joint in all directions, as far as possible. This will
demonstrate any loss of voluntary muscle function
and the presence of any musculoskeletal abnormal-
ities, such as arthritis or muscle contractures, which
limit movement.
Strength of the muscles
Check in a systematic way
the strength of the muscles which move each joint.
Strength is assessed by asking the patient to move the
joint against a resistance, or by asking them to keep
the joint fixed while you try to move it. The latter is
the simplest method because the patient only needs
to be instructed to keep the limb still.
It is customary to grade muscle strength as
follows:
5: normal
4: moderate, but not full strength
3: can work against gravity but not against a
greater resistance
2: cannot work against gravity but the muscles
contract
1: barely perceptible contractions
0: complete paralysis.
It is, however, better to describe the strength of
the muscles than use a numerical code.
The segments of the spinal cord and the nerves
which control each joint are listed in Revision
panel 1.9.
Sensory nerve function
The peripheral nerves transmit the sensations of
light touch, deep touch and pressure, pain, temper-
ature, vibration sense, position sense, and muscular
coordination.
The appreciation of light touch
This is tested with a
wisp of cotton wool.
27
Revision panel 1.9
The nerves and spinal segments which innervate the major muscle groups
Muscle groups
Spinal segments
Nerves
Shoulder
Flexion
C5, 6
Nerve to pectoralis major, circumflex nerve
Extension
C5, 6
Abduction
C5, 6
Subscapular nerve
Circumflex nerve
Elbow
Flexion
C5, 6
Musculocutaneous nerve
Extension
C6, 7, 8
Radial nerve
Wrist
Flexion
C6, 7, 8
Median nerve and ulnar nerve
Extension
C6, 7, 8
Radial nerve
Intrinsic hand muscles
C8, T1
Median nerve and ulnar nerve
Hip
Flexion
L2, 3, 4
Lumbar and femoral nerves
Extension
L5, S1, 2
Inferior gluteal nerve
Abduction
L4, 5, S1
Superior gluteal nerve
Adduction
L2, 3, 4
Obturator nerve
Rotation
L5, S1, 2
Knee
Flexion
L4, 5, S1, 2
Sciatic nerve
Extension
L2, 3, 4
Femoral nerve
Ankle
Flexion
L5, S1, 2
Medial popliteal
⫹ posterior tibial nerves
Extension
L4, 5, S1
Anterior tibial nerve
Foot
Inversion
L4, 5
Anterior
⫹ posterior tibial nerves
Eversion
L5, S1
Musculocutaneous nerve
Chap-01.qxd 4/19/05 13:41PM Page 27
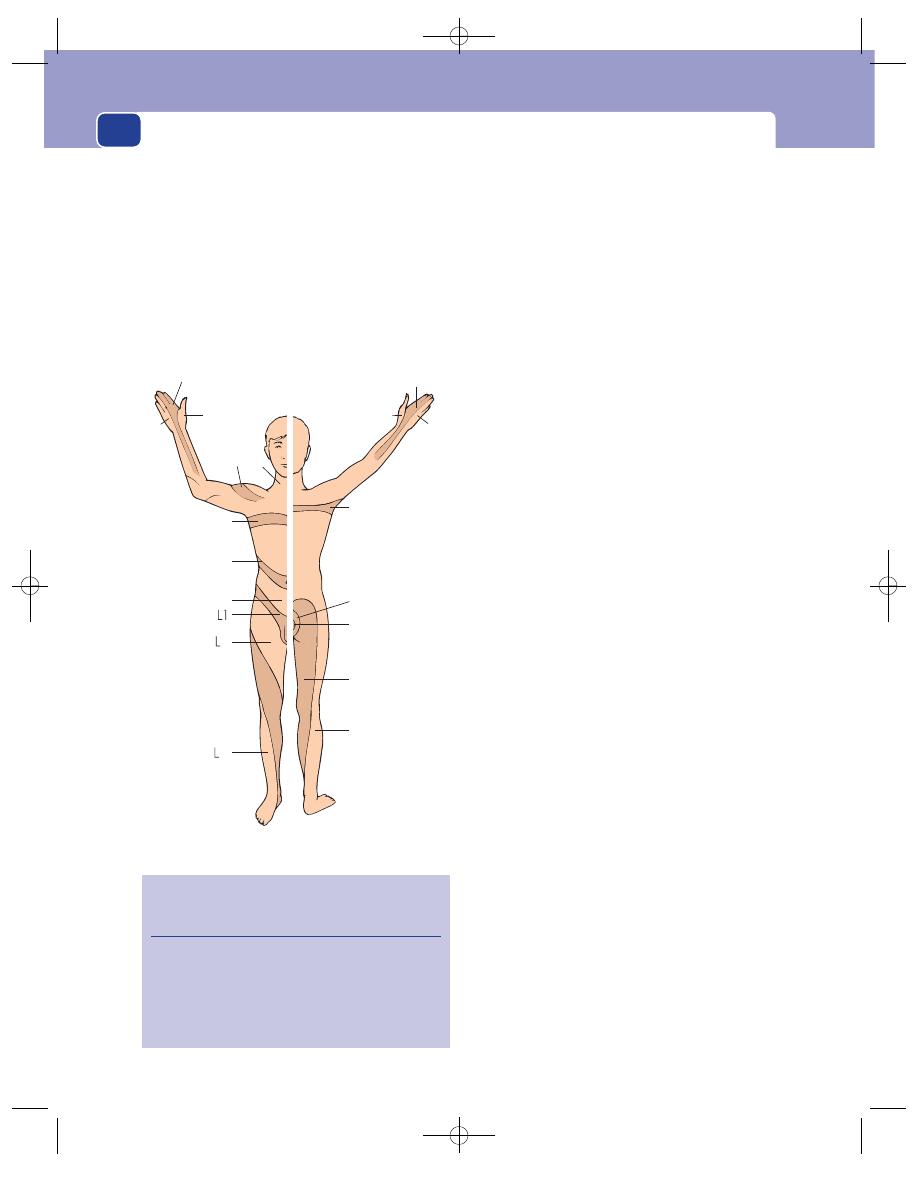
History taking and clinical examination
Make sure that the patient cannot see you when
you touch them, and touch the limb in a random
manner. Move from the normal to the abnormal
when mapping out an area of hypo-aesthesia. The
important dermatomes are shown in Figure 1.14.
Deep touch and pressure sensation
This is tested by
pressing firmly on the skin with a blunt object. It is
unlikely to be abnormal if the response to light touch
is normal.
Pain
The best test of pain sensibility is the response
to a pinprick. A new sterile needle must be used for
each patient to avoid transmitting infection such as
hepatitis. The patient must be asked whether the
needle feels ‘sharp’ or ‘blunt’.
Temperature
Ask the patient to differentiate between
a hot and a cold object. The simplest method is to
use two test tubes, one filled with hot and the other
with cold water.
Vibration sense
Strike a tuning fork firmly. Place its
base on a bony protuberance, such as the malleolus
at the ankle, and ask the patient to describe the sen-
sation they can feel. A description of a ‘buzzing’ or
‘vibrating’ sensation indicates normal vibration sense.
Do not put these words into the patient’s mind by
using them in a leading question.
Position sense
The proprioceptive nerve endings in
a joint tell the brain about the joint’s spatial orienta-
tion. Test this ability by moving the great toe or
thumb into different positions of flexion or exten-
sion and ask the patient to identify them. It is easier
to ask patients to state the direction in which the
digit is pointing (e.g. up or down) than to use unfa-
miliar anatomical terms. The patient must keep
their eyes shut.
Muscle coordination
Test the coordination of the
upper limbs by asking the patient to touch your
upheld finger with their index finger and then to
touch the tip of their nose. You will also be testing
joint position sense if you ask them to do this a sec-
ond time with their eyes shut. Coordination in the
lower limbs is tested by asking the patient to slide
the heel of one foot up and down the shin of the
other leg. This should also be done with the eyes
open and then shut.
Reflex function
The limb reflexes are all stretch reflexes and test the
integrity of the spinal segments, and the motor and
sensory nerves which innervate the muscles being
stretched.
28
Anterior
Posterior
C7
C6
C8
C5 C3
T5
T10
T12
T2
S3
S4&S5
S2
S1
C8
C6
C7
THE IMPORTANT DERMATOMES
(the others can be estimated if
you remember these)
3
5
FIG 1.14
The important dermatomes.
Revision panel 1.10
The segments involved in the common stretch
reflexes
Biceps jerk
C5, 6
Triceps jerk
C6, 7
Finger jerk
C8
Knee jerk
L2, 3, 4
Ankle jerk
S1, 2
Chap-01.qxd 4/19/05 13:41PM Page 28
History and examination of a lump
To stimulate a good stretch reflex you must stretch
the muscle’s tendon suddenly by striking it with a
rubber hammer. A weak reflex can be reinforced by
asking patients to clench their teeth or to interlock
their fingers and try to pull them apart.
Clonus
The increase in muscle tone that occurs with
an upper motor neurone lesion increases the sus-
ceptibility of the tendons to the stretch reflex. Sudden
and persistent stretching can cause repeated con-
tractions known as clonus.
The plantar reflex
Scraping the lateral aspect of the
sole of the foot causes a withdrawal reflex and flex-
ion of the great toe. If the toe extends, there is an
upper motor neurone lesion. This reflex involves the
L5, S1 and S2 spinal segments.
Abdominal reflexes
Stroking the upper and lower
abdomen causes the rectus abdominis muscle to
contract. This tests the T8, 9 and 10, and T11 and 12
segments, respectively.
Cremasteric reflex
Stroking the inner side of the
thigh makes the cremaster contract, testing the L1
segment.
Test the urine, faeces and sputum
It is important to note the colour and smell of the
urine before using the modern simple dipstick
methods for testing it for sugar, blood, acetone and
protein. Do not forget to measure the specific grav-
ity of the urine and to inspect any precipitate under
the microscope.
Look at the faeces if the patient complains that
they are abnormal.
Look at the sputum.
HISTORY AND EXAMINATION OF
A LUMP
History
Most patients with a lump feel it frequently and
should be able to tell you about the history of its
clinical features. Therefore you should seek answers
to the following questions.
1. When was the lump first noticed?
It is important to be precise with dates and
terminology. Do not write ‘the lump first
appeared 6 months ago’, when you mean ‘the
lump was first noticed 6 months ago’. Many
lumps may exist for months, even years, before
the patient notices them.
2. What made the patient notice the lump?
There are three common answers to this
question:
‘I felt or saw it when washing’.
‘I had a pain and found the lump when I
felt the painful area’.
‘Someone else noticed it and told me about it’.
The presence or absence of pain is important,
particularly if it is the presenting feature. In very
general terms, pain is usually associated with
inflammation, not neoplastic change. Most
29
Revision panel 1.11
The examination of a lump or ulcer
Local examination
Site
Size
Shape
Surface
Depth
Colour
Temperature
Tenderness
Edge
Composition:
■
consistence
■
fluctuation
■
fluid thrill
}
Solid, fluid or gas
■
translucence
■
resonance
■
pulsatility
■
compressibility
}
Vascular
■
bruit
Reducibility
Relations to surrounding structures –
mobility/fixity
Regional lymph glands
State of local tissues:
■
arteries
■
nerves
■
bones and joints
General examination
Chap-01.qxd 4/19/05 13:41PM Page 29
History taking and clinical examination
patients expect cancer to be painful – and do
themselves irreparable harm by ignoring a lump
just because it does not hurt them.
3. What are the symptoms of the lump?
The lump may be painful and if it is, you must
take a careful history of the pain, as described
earlier in this chapter. The characteristic feature
of pain associated with acute infection is its
throbbing nature.
A lump may be disfiguring or interfere with
movement, respiration or swallowing. Describe
the history of each symptom carefully.
4. Has the lump changed since it was first noticed?
This is where you use the patient’s own
knowledge of their physical signs. The feature
that they notice is the size of the lump. They
should be able to tell you if it has got bigger,
smaller, or has fluctuated in size and when they
noticed a change in size. They may also have
appreciated other changes in the nature of the
lump that they can tell you about. They may
also have noticed tenderness, which may have
altered in any of the ways that a pain may change.
5. Does the lump ever disappear?
A lump may disappear on lying down, or during
exercise, and yet be irreducible at the time of
your examination. The patient should always be
asked if the lump ever goes away, because this
physical characteristic is peculiar to only a few
types of lump.
6. Has the patient ever had any other lumps?
You must ask this question because it might not
have occurred to the patient that there could be
any connection between their present lump and
a previous lump, or even a coexisting one.
7. What does the patient think caused the lump?
Lumps occasionally follow injuries or systemic
illnesses known only to the patient.
Examination
Site/position
The location of a lump must be
described in exact anatomical terms, using distances
measured from bony points. Do not guess distances;
use a tape measure.
Colour and texture of overlying skin
The skin over a
lump may be discoloured and become smooth and
shiny or thick and rough.
Shape
Remember that lumps have three dimensions.
You cannot have a circular lump because a circle is a
plane figure. Many lumps are not regular spheres, or
hemispheres, but have an asymmetrical outline. In
these circumstances, it is permissible to use descrip-
tive terms such as pear shaped or kidney shaped.
Size
Once the shape is established, it is possible to
measure its various dimensions. Again, remember
that all solid objects have at least three dimensions:
width, length and height or depth. Asymmetrical
lumps will need more measurements to describe
them accurately; sometimes a diagram will clarify
your written description.
Surface
The first feature of the lump that you will
notice when you feel it will be its surface. It may be
smooth or irregular. An irregular surface may be
covered with smooth bumps, rather like cobble-
stones, which can be called bosselated; or be irregu-
lar or rough.
There may be a mixture of surfaces if the lump is
large.
Temperature
Is the lump hot or of normal tempera-
ture? Assess the skin temperature with the dorsal
surfaces of your fingers, because they are usually dry
(free of sweat) and cool.
30
Revision panel 1.12
The history of a lump or an ulcer
Duration
When was it first noticed?
First symptom
What brought it to the patient’s notice?
Other symptoms
What symptoms does it cause?
Progression
How has it changed since it was first noticed?
Persistence
Has it ever disappeared or healed?
Multiplicity
Has (or had) the patient any other lumps or
ulcers?
Cause
What does the patient think caused it?
Chap-01.qxd 4/19/05 13:41PM Page 30
History and examination of a lump
31
Tenderness
Is the lump tender? Which parts are ten-
der? Always try to feel the non-tender part before
feeling the tender area, and watch the patient’s face
for signs of discomfort as you palpate.
Edge
The edge of a lump may be clearly defined or
indistinct. It may have a definite pattern.
Composition
Any lump must be composed of one or
more of the following:
■
calcified tissues such as bone, which make it
hard;
■
tightly packed cells, which make it solid;
■
extravascular fluid, such as urine, serum,
cerebrospinal fluid (CSF), synovial fluid or
extravascular blood, which make the lump
cystic;
■
gas;
■
intravascular blood.
The physical signs which help you decide the
composition of a lump are: consistence, fluctuation,
fluid thrill, translucence, resonance, pulsatility, com-
pressibility and bruits.
Consistence
The consistence of a lump may vary
from very soft to very hard. As it is difficult to
describe hardness, it is common practice to compare
the consistence of a lump to well-known objects.
A simple scale for consistence is as follows:
■
Stony hard: not indentable – usually bone or
calcification.
■
Firm: hard but not as hard as bone.
■
Rubbery: but slightly squashable, similar to a
rubber ball.
■
Spongy: soft and very squashable, but still with
some resilience.
■
Soft: squashable and no resilience.
The consistence of a lump depends not only
upon its structure but also on the tension within it.
Some fluid-filled lumps are hard, some solid lumps
are soft; therefore, the final decision about composi-
tion of a lump (i.e. whether it is fluid or solid) rarely
depends solely upon an assessment of the consis-
tence. Other features such as those peculiar to fluid
may be more important.
Fluctuation
Pressure on one side of a fluid-filled cav-
ity makes all the other surfaces protrude. This is
because an increase of pressure within a cavity is
transmitted equally and at right-angles to all parts of
its wall. When you press on one aspect of a solid lump,
it may or may not bulge out in another direction,
but it will not bulge outwards in every other direction.
Fluctuation can only be elicited by feeling at least
two other areas of the lump whilst pressing on a
third. The lump fluctuates and contains fluid if two
areas on opposite aspects of the lump bulge out
when a third area is pressed in. This examination is
best carried out in two places, the second at right-
angles to the first.
Fluid thrill
A percussion wave is easily conducted
across a large fluid collection (cyst) but not across a
solid mass. The presence of a fluid thrill is detected
by tapping one side of the lump and feeling the
transmitted vibration when it reaches the other
side. A percussion wave can be transmitted along its
wall if a swelling is large. This is prevented by plac-
ing the edge of the patient’s or an assistant’s hand on
the lump mid-way between the percussing and pal-
pating hands.
Percussion waves cannot be felt across small lumps
because the wave moves so quickly that the time gap
cannot be appreciated or distinguished from the
mechanical shaking of the tissue caused by the per-
cussion. The presence of a fluid thrill is a diagnostic
and extremely valuable physical sign.
Translucence (transillumination)
Light will pass easily
through clear fluid but not through solid tissues.
A lump that transilluminates must contain water,
serum, lymph or plasma, or highly refractile fat.
Blood and other opaque fluids do not transmit
light. Transillumination requires a bright pinpoint
light source and a darkened room. The light should
be placed on one side of the lump, not directly on
top of it. Transillumination is present when the light
can be seen in an area distant from the site in con-
tact with the light source.
Attempts at transillumination with a poor-quality
flashlight in a bright room are bound to fail and
mislead.
Resonance
Solid and fluid-filled lumps sound dull
when percussed. A gas-filled lump sounds hollow
and resonant.
Pulsatility
Lumps may pulsate because they are near
to an artery and are moved by its pulsations. Always
let your hand rest still for a few seconds on every lump
Chap-01.qxd 4/19/05 13:41PM Page 31
History taking and clinical examination
to discover if it is pulsating. When a lump pulsates you
must find out whether the pulsations are being trans-
mitted to the lump from elsewhere or are caused by
the expansion of the lump. Place a finger (or fingers
if large) of each hand on opposite sides of the lump
and feel if they are pushed outwards and upwards.
When they are, the lump has an expansile pulsation.
When they are pushed in the same direction (usu-
ally upwards), the lump has a transmitted pulsation.
The two common causes of expansile pulsation
are aneurysms and very vascular tumours.
Compressibility
Some fluid-filled lumps can be com-
pressed until they disappear. When the compressing
hand is removed the lump re-forms. This finding is a
common feature of vascular malformations and fluid
collections which can be pushed back into a cavity or
cistern. Compressibility should not be confused with
reducibility (see below). A lump which is reducible –
such as a hernia – can be pushed away into another
place but will often not reappear spontaneously with-
out the stimulus of coughing or gravity.
Bruits
Always listen to a lump. Vascular lumps that
contain an arteriovenous fistula may have a systolic
bruit. Hernaie containing bowel may have audible
bowel sounds.
Reducibility
You should always see if a lump is
reducible (disappears) by gently compressing it.
A reducible lump will be felt to get smaller and then
to move into another place as it is compressed. It may
disappear quite suddenly after appropriate pressure
has been applied. If you ask the patient to cough, the
lump may return, expanding as it does so. This is
called a cough impulse and is a feature of herniae
and some vascular lumps. The reduction can be
maintained by pressing over the point at which
the lump finally disappeared. In many ways the dif-
ferences between compressibility (see above) and
reducibility are semantic.
Relations to surrounding structures
By careful palpa-
tion, it is usually possible to decide which structure
contains the lump, and what its relation is to over-
lying and deeper structures. The attachment of skin
and other superficial structures to a lump can easily
be determined because both are accessible to the
examiner and any limitation of their movement
easily felt. The lump should be gently moved while
the skin is inspected for movement or puckering.
Attachment to deeper structures is more difficult
to determine. Underlying muscles must be tensed to
see if this reduces the mobility of an overlying lump
or makes it easier or less easy to feel. The former
indicates that the lump is attached to the fascia cov-
ering the superficial surface of the muscle or to the
muscle itself; the latter that the lump is within or
deep to the muscles. Lumps that are attached to
bone move very little. Lumps that are attached to or
arising from vessels or nerves may be moved from
side to side across the length of the vessel or nerve,
but not up and down along their length. Lumps in
the abdomen that are freely mobile usually arise
from the intestine, its mesentery or the omentum.
State of the regional lymph glands
Never forget to palpate
the lymph glands that would normally receive
lymph from the region occupied by the lump. The
skin, muscles and bones of the limbs and trunk drain
to the axillary and inguinal glands; the head and neck
to the cervical glands; and the intra-abdominal struc-
tures to the pre-aortic and para-aortic glands.
State of the local tissues
It is important to examine
the overlying and nearby skin, subcutaneous tissues,
muscles and bones, and the local circulation and
nerve supply of adjacent tissues. This is more relevant
when examining an ulcer; but some lumps are asso-
ciated with a local vascular or neurological abnor-
mality, or cause an abnormality of these systems, so
this part of the examination must not be forgotten.
General examination
It is often tempting to examine
only the lump about which the patient is complaining.
This will cause you to make innumerable misdiag-
noses. You must always examine the whole patient.
HISTORY AND EXAMINATION OF
AN ULCER
An ulcer is a solution (break) of the continuity of an
epithelium (i.e. an epithelial deficit, not a wound).
Unless it is painless and in an inaccessible part of the
body, patients notice ulcers from the moment they
begin, and will know a great deal about their clinical
features.
History
The questions to be asked concerning an ulcer fol-
low a pattern similar to those for a lump.
32
Chap-01.qxd 4/19/05 13:41PM Page 32
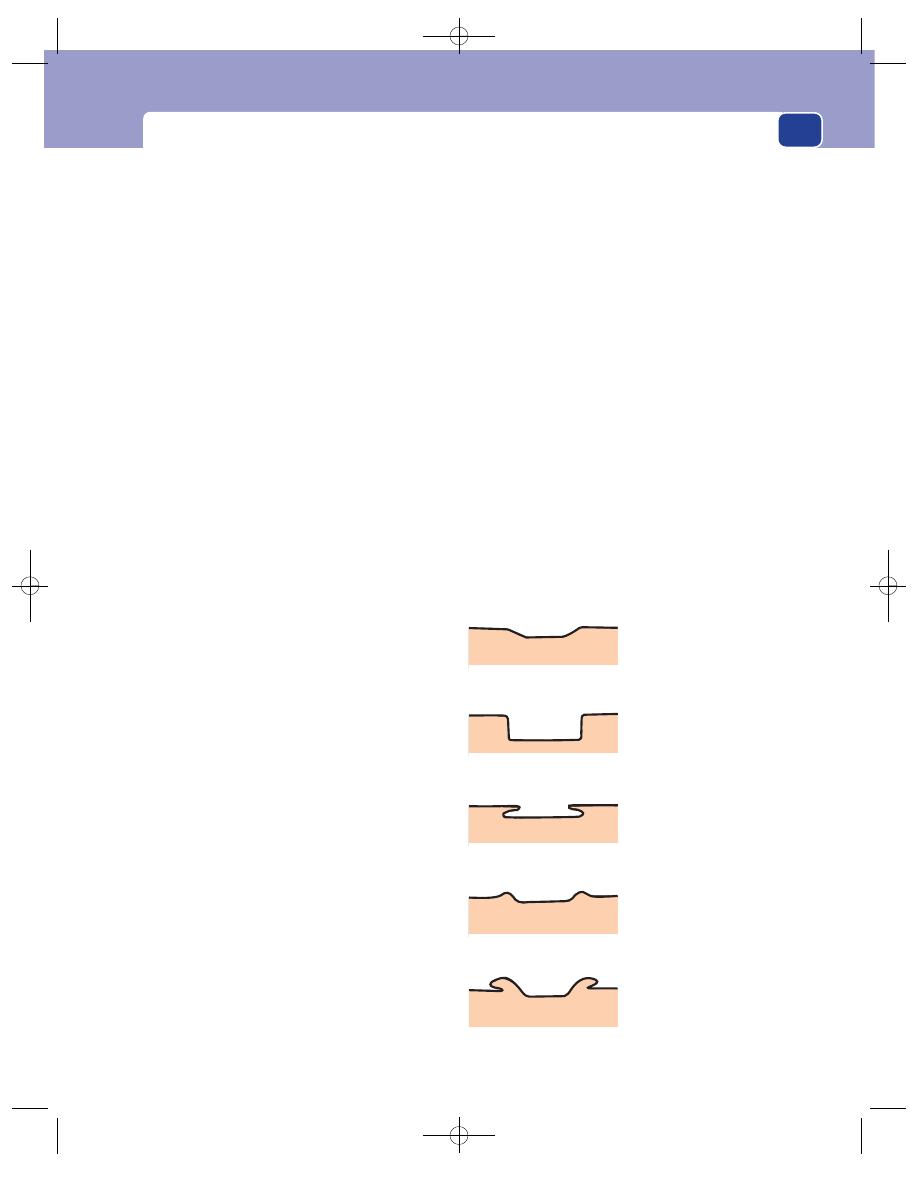
History and examination of an ulcer
33
1. When was the ulcer first noticed?
Ask the patient when the ulcer began and
whether it could have been present for some
time before it was noticed. The latter often
occurs with neurotrophic ulcers on the sole of
the foot.
2. What drew the patient’s attention to the ulcer?
The commonest reason is pain. Occasionally,
the presenting feature is bleeding, or a purulent
discharge, which may be foul smelling.
3. What are the symptoms of the ulcer?
The ulcer may be painful. It may interfere with
daily activities such as walking, eating or
defaecation. Record the history of each symptom.
4. How has the ulcer changed since it first
appeared?
The patient’s observations about changes in
size, shape, discharge and pain are likely to be
detailed and accurate. If the ulcer has healed
and broken down, record the features of each
episode.
5. Has the patient ever had a similar ulcer on the
same site, or elsewhere?
Obtain a complete history of any previous ulcer.
6. What does the patient think caused the ulcer?
Most patients believe they know the cause of
their ulcer, and are often right. In many cases it
is trauma. When possible, the severity and type
of injury should be assessed. A large ulcer
following a minor injury suggests that the skin
was abnormal before the injury.
Examination
The examination of an ulcer follows the same pattern
as the examination of a lump. When an ulcer has an
irregular shape that is difficult to describe, draw it on
your notes and add the dimensions. When an exact
record of size and shape is needed, place a thin sheet
of sterile transparent plastic sheet over the ulcer and
trace around its edge with a felt-tipped pen.
After recording the site, size and shape of the ulcer,
you must examine the base (surface), edge, depth,
discharge and surrounding tissues, the state of the
local lymph glands and local tissues, and complete
the general examination.
Base
The base, or floor, of an ulcer usually consists of
slough or granulation tissue (capillaries, collagen,
fibroblasts, bacteria and inflammatory cells), but
recognizable structures such as tendon or bone may
be visible. The nature of the floor occasionally gives
some indication of the cause of the ulcer.
■
Solid brown or grey dead tissue indicates full-
thickness skin death.
■
Syphilitic ulcers have a slough that looks like a
yellow-grey wash-leather.
■
Tuberculous ulcers have a base of bluish
unhealthy granulation tissue.
■
Ischaemic ulcers often contain poor granulation
tissue, and tendons and other structures may lie
bare in their base.
The redness of the granulation tissue reflects the
underlying vascularity and indicates the ability of
the ulcer to heal. Healing epidermis is seen as a pale
layer extending in over the granulation tissue from
the edge of the ulcer.
Edge
There are five types of edge (see Fig. 1.15).
A flat, gently sloping edge
This indicates that the
ulcer is shallow and this type of ulcer is usually
Sloping
(a healing ulcer)
Punched-out
(syphilis, trophic)
Undermined
(tuberculosis)
Rolled
(basal cell carcinoma)
Everted
(squamous cell carcinoma)
FIG 1.15
The varieties of ulcer edge.
Chap-01.qxd 4/19/05 13:41PM Page 33
History taking and clinical examination
superficial, often only half-way through the skin.
Venous ulcers usually have this type of edge, but so
do many other types of ulcer. The new skin growing
in around the edge of a healing ulcer is pale pink
and almost transparent.
A square-cut or punched-out edge
This follows the
rapid death and loss of the whole thickness of the
skin without much attempt at repair of the defect.
This form of ulcer is most often seen in the foot
where pressure has occurred on an insensitive piece of
skin, i.e. a trophic ulcer secondary to a neurological
defect. The classic textbook example of a punched-
out ulcer is the ulcer of tertiary syphilis, but these
lesions are rare today in Europe. Most of the
punched-out ulcers that are now seen are caused by
the neuropathy of diabetes and peripheral arterial
ischaemia or, outside Europe and North America,
leprosy.
An undermined edge
When an infection in an ulcer
affects the subcutaneous tissues more than the skin,
the edge becomes undermined. This type of ulcer is
commonly seen in the buttock as a result of pressure
necrosis, because the subcutaneous fat is more sus-
ceptible to pressure than the skin; but the classic
textbook example is the tuberculous ulcer – which
is now uncommon in Europe and North America.
A rolled edge
This develops when there is slow
growth of tissue in the edge of the ulcer. The edge
looks like the heaped-up mound around an ancient
Roman earthwork. A rolled edge is typical, and almost
diagnostic, of a basal cell carcinoma (rodent ulcer).
The edge is usually pale pink or white, with clumps
and clusters of cells visible through the paper-thin
superficial covering of squamous cells. Telangiectases
are commonly seen in the pearly edge.
An everted edge
This develops when the tissue in
the edge of the ulcer is growing so rapidly that it
spills out of the ulcer to overlap the normal skin. An
everted edge is typical of a carcinoma and is seen in
all those organs where carcinomata occur – the skin,
in the bowel, in the bladder and in the respiratory
tract.
Depth
Record the depth of the ulcer in millimetres, and
anatomically by describing the structures it has pen-
etrated or reached.
34
Revision panel 1.13
Remember the four basic techniques
Inspection
Palpation
Percussion
Auscultation
Revision panel 1.14
A classification of the aetiology of disease
Congenital
Genetic
Sporadic
Acquired
Traumatic
Inflammatory:
Physical
Chemical
Infection
Viral
Bacterial
Rickettsial
Spirochaetal
Protozoal
Fungal
Helminthic
Mycoplasma
Prions
Neoplastic
Benign
Malignant
Primary
Carcinoma
Sarcoma
Others
Secondary
Degenerative
Autoimmune
Proliferative
Metabolic
Hormonal
Mechanical
Vascular
Self-induced
Psychosomatic
Iatrogenic
Chap-01.qxd 4/19/05 13:41PM Page 34
History and examination of an ulcer
Discharge
The discharge from an ulcer may be serous, san-
guinous, serosanguinous or purulent. There may be
a considerable quantity of discharge which is easily
visible, or it may only be apparent from inspection of
the patient’s dressings, and you may not be able to
see the features of the ulcer at all if it is covered with
coagulated discharge (a scab). This may have to be
removed to examine the ulcer properly. Students
should not do this without the permission of the
doctor in charge of the patient.
Relations
Describe the relations of the ulcer to its surrounding
tissues, particularly those deep to it. It is important
to know if the ulcer is adherent or invading deep
structures such as tendons, periosteum and bone –
which may indicate the presence of osteomyelitis.
The local lymph glands must be carefully exam-
ined. They may be enlarged because of secondary
infection or secondary tumour deposits and they
may be tender.
State of the local tissues
Pay particular attention to the local blood supply
and innervation of the adjacent skin. Many ulcers in
the lower limbs are secondary to vascular and neu-
rological disease. There may also be evidence of pre-
vious ulcers that have healed.
General examination
This is very important because many systemic dis-
eases as well as many skin diseases present with skin
lesions and ulcers. Examine the whole patient with
care, looking especially at their hands and facies,
which can supply important clues to the diagnosis.
35
Chap-01.qxd 4/19/05 13:41PM Page 35
emergency management of
major injuries
This is the only chapter in this book that contains
advice about management. To describe the relatively
small number of symptoms and signs that accom-
pany the failure of the body’s life-supporting systems
without describing how, in emergency circum-
stances, these system failures should be treated from
the moment the signs of failure are observed would
be pointless. Furthermore, medical students, even
in their early years of learning the basic clinical
symptoms and signs of disease, are expected by the
general public to know how to administer emer-
gency first-aid measures to an injured patient.
The physical signs produced by injury are usually
more evident and immediately significant than
their history, especially if the patient is unconscious.
Obtaining the history of the type of injury and the
possible forces involved, including information on
the injured person’s habits, such as drug or alcohol
addictions, from the patient, family members, friends,
onlookers or first-aiders who witnessed the event is
always helpful but must not interfere with the initial
rapid clinical assessment and resuscitation.
Worldwide adoption of the principles enunciated
in the Advanced Trauma Life Support course (ATLS)
has established the value of a standardized approach
to trauma assessment and management, especially in
patients who have sustained injuries to more than
one of their systems. This chapter follows the ATLS
approach.
Some injured patients are brought directly to the
accident and emergency department by ambulance,
some severely injured patients may be brought in by
private vehicles, or even walk into hospital, others
may be given treatment at the site of the event. Even
when an initial assessment has been made at the site
of the event, it must be repeated in the hospital.
When ambulance staff are involved, they may radio
ahead and warn of their casualty’s likely injuries, a
measure that allows the trauma team to be alerted
and immediately available. Patients presumed to
have sustained major injuries should be taken
straight to the resuscitation area for their primary
hospital survey.
Even patients thought to have minor injuries
should be carefully assessed by an experienced
nurse or doctor as soon as possible, as apparently
stable patients may have sustained serious injuries,
which may have passed undetected during the ini-
tial assessment, especially when an influx of many
injured patients overwhelms local resources.
THE PRIMARY SURVEY AND
MANAGEMENT AT THE SITE OF
THE EVENT: FIRST-AID
This is carried out under the three easily remem-
bered headings of A, B, C, i.e.:
■
Airway
■
Breathing
■
Circulation.
This approach is particularly important when
assessing patients with multiple injuries.
Airway
The signs of an obstructed airway are cyanosis
(blue), apnoea (not breathing) and stridor (a rasp-
ing noise on respiration).
Chap-02.qxd 4/19/05 13:41PM Page 36
The primary survey and management at the site of the event: first-aid
37
It is essential to protect and secure an adequate
airway. The lungs cannot oxygenate the blood if the
airway is obstructed by the jaw and tongue falling
back, swollen soft tissues, direct damage to the upper
airway, false teeth, vomitus or blood.
The airway of unconscious patients lying on their
back often becomes obstructed by their own intra-
oral soft tissues, but before they are rolled into the
supine or semi-prone position, or the neck extended,
always consider, and if possible exclude, an associ-
ated cervical spinal injury
All patients found to be unconscious after an
injury must be assumed to have an associated injury
of their cervical spine because abrupt or careless turn-
ing may further dislocate or sublux a cervical vertebra
and injure the spinal cord when no injury existed,
or turn partial cord damage into a complete tran-
section. The neck should therefore be immobilized in
all unconscious injured patients by longitudinal,
manual support, the application of a hard collar and
the use of stabilizing sand bags and tape before
turning the patient onto their side, until clinical
examination and radiographs have excluded unsta-
ble fractures of the cervical spine.
Compromises are inevitable if an immobilizing
collar is not available at the site of injury. The presence
of two first-aiders may allow one to support the neck
while the other assesses and manually clears the air-
way, feels the neck and jaws, and assesses the respira-
tory effort by palpating the chest during respiration.
Airway obstruction is often relieved by lifting the
jaw upwards, but may only be relieved by inserting a
finger in the mouth and pulling the jaw or palate
forward, especially when the obstruction is associ-
ated with a fractured maxilla or mandible.
An oropharyngeal or nasopharyngeal airway
should be inserted as soon as possible, and then,
in an unconscious patient, replaced by an endotra-
cheal tube, inserted by an experience anaesthetist,
because the absence of a gag reflex in an uncon-
scious patient makes aspiration of saliva, vomitus or
blood into the lungs a major hazard.
Breathing
If the patient remains cyanosed or apnoeic after the
airway has been cleared, mouth-to-mouth resusci-
tation should be started immediately. This is easier
and safer (from risks of cross-infections) if a Brook’s
airway, a facemask, an Ambu bag and oxygen are
available. Mouth-to-mouth ventilation combined
with external cardiac massage may, however, be life
saving in patients who have undergone a short period
of respiratory arrest.
There are few indications for heroic attempts at
inserting home-made ‘tracheostomy’ devices at the
scene of the accident. The patients are probably better
served by a rapid transfer to hospital by experienced
ambulance staff who have been trained in resuscita-
tion techniques.
Circulation
It is absurd to concentrate on the detailed drills of
assessment of the airway and breathing if the patient
obviously has a normal airway and no neck injuries
but is losing vast amounts of blood – even to the point
of literally bleeding to death. Severe external bleeding
at the scene of the accident requires manual compres-
sion directly over the wound or pressure proximal to
the point of bleeding, where the feeding artery can
be compressed against an underlying bony point.
Tourniquets should only be used to stop distal
limb bleeding. They rarely work efficiently and often
exacerbate bleeding by obstructing the venous out-
flow, while failing to occlude the arterial inflow.
An effective tourniquet makes the whole limb
ischaemic and will cause permanent muscle and
nerve damage if it is kept in place for more than 1.5
to 2 hours. Tourniquets can also theoretically cause
re-perfusion problems when released – metabolic
acidosis, myoglobulinuria and hypercalcaemia. Never-
theless a tourniquet can sometimes be life saving if it
is applied at the correct pressure to a mangled bleed-
ing limb for a short period. The time of application
must be carefully recorded and passed on to ambu-
lance and medical staff.
Direct manual pressure, provided it is achieving its
desired effect (i.e. stopping or reducing the blood
loss), is usually preferable to a tourniquet. This can be
very tiring because it must be maintained until the
patient reaches the hospital’s accident and emergency
department.
General first-aid advice
First-aiders should ensure that there is no immediate
danger to themselves before approaching a casualty.
Chap-02.qxd 4/19/05 13:41PM Page 37
The symptoms, signs and emergency management of major injuries
38
Many injured patients are best served by leaving them
where they are until experienced help arrives, pro-
vided the environment is not continuing to damage
or threaten them. Provided the injured patient has
a strong pulse, is breathing normally and is not
overtly bleeding, this is invariably the correct course
of action. Patients should only be moved if there is a
risk of further injury from leaving them where they
are, e.g. inside a burning car.
It is, of course, important to obtain help as soon
as possible so that there is always someone available
to stay with the patient to monitor their pulse and
breathing and provide moral support. The wide-
spread availability of mobile phones has improved
the first-aider’s ability to summon help.
Under no circumstances should an injured patient
be given anything to eat or drink.
THE PRIMARY SURVEY IN THE
ACCIDENT AND EMERGENCY
DEPARTMENT
All patients who are unconscious or suspected of
having multiple or serious injuries should be admit-
ted directly to the resuscitation area of the accident
and emergency department. While medical students
are rarely required to have an active role in the man-
agement of acute trauma, the opportunity to wit-
ness assessment and resuscitation in this setting is
extremely valuable, as the principles of the process
are relevant to many other areas of medical practice.
The clinical assessment (history and examination)
and resuscitation must occur simultaneously if lives
are to be saved, hence the inclusion of treatment in
this chapter.
The routine A, B, C assessment must be repeated
whatever happened before the hospital admission.
Airway
The neck must be protected by a collar and immobi-
lized fully using sand bags and tape. An anaesthetist
should assess the need for better control of the airway.
Look for the signs of inadequate oxygenation
Respiratory distress, apnoea, cyanosis, loss of con-
sciousness and the presence of major facial, neck
or chest injuries that might obstruct the airway
may all indicate the need for endotracheal or naso-
gastric intubation once the neck has been stabilized.
Look for the signs of inadequate ventilation
The chest should be uncovered and palpated to
assess respiratory movements. Confirm the pres-
ence of air entry into the lungs with a stethoscope.
The neck and jaws should be palpated to check for
deformity. Insert a finger into the mouth to extract
any foreign bodies and to check for jaw fractures.
Occasionally severe damage to the upper airways or
trachea makes intubation impossible. An emergency
tracheostomy is indicated if the patient is deeply
cyanosed or apnoeic and an endotracheal tube can-
not be inserted safely.
Breathing
Assess the condition and function of
the thoracic cage
Once you are certain that the airway is patent, assess
the adequacy of ventilation by inspecting, palpating,
percussing and listening to the chest for symmetry,
movement, dullness and breath sounds. Patients
with multiple injuries or chest problems causing
hypoxia should be given high-flow oxygen through
a closed circuit oxygen mask from the moment of
their arrival in the accident and emergency depart-
ment. An oxygen saturation monitor placed on an
extremity is a valuable means of assessing the effec-
tiveness of the patient’s ventilation.
Inspection and palpation
The presence of open wounds or flail segments in
the chest indicates the need for a chest drain and
positive-pressure ventilation. A flail segment occurs
when several ribs are fractured in two places. The flail
segments sink inwards during inspiration. Bruising
over the chest indicates that rib fractures are likely,
and the presence of surgical emphysema suggests that
the pleura has been breached. Surgical emphysema
presents as a crackling sensation in the subcutaneous
tissues. A ‘sucking’ chest wound may be present.
Percussion
A tension pneumothorax must be suspected if
breathing is difficult, the trachea is deviated to the
contralateral side and if there is decreased air entry
over the affected lung. Although the clinical diagnosis
Chap-02.qxd 4/19/05 13:41PM Page 38
The primary survey in the accident and emergency department
39
will have to be confirmed with a chest radiograph, a
chest drain should be inserted on the evidence of
the clinical signs if the patient is unstable. Bilateral
tension pneumothoraces are very rare, but cause
severe cardiac and respiratory compromise, mani-
fest as cyanosis, severe air hunger, a weak pulse and
hypotension.
Remember that, with bilateral pneumothoraces,
the trachea remains central but air entry is poor into
both lungs. The rapid insertion of chest drains
which are connected to under-water seal drainage
bottles relieves the situation.
A large haemothorax also causes respiratory and
circulatory problems, manifest as reduced breath
sounds and a dull percussion note combined with
reduced vocal fremitus and vocal resonance. The
diagnosis should be confirmed with an erect or
decubitus chest radiograph, but a chest drain may
occasionally have to be inserted as an emergency
measure on the basis of the clinical signs.
A large amount of blood draining from a chest
may destabilize the patient and need urgent replace-
ment into the circulation (see below), so intravenous
lines should be inserted into both antecubital fossae
before a haemothorax is drained. The chest drain may
occasionally need to be clamped to prevent massive
continuing blood loss. Lost blood should be replaced
with a crystalloid solution at first, but subsequently
with blood as soon as this is available (see below).
The blood pressure must be carefully and contin-
uously monitored to confirm the adequacy of any
blood volume replacement.
Flail segments rarely cause major problems ini-
tially but are indicative of a severe underlying lung
injury. Both these problems are treated by endotra-
cheal incubation and positive-pressure ventilation,
but it must be remembered that this can cause a
tension pneumothorax and may also make an exist-
ing tension pneumothorax worse. This complica-
tion should be suspected if the anaesthetist notices
an increasing resistance to ventilation, a decreasing
oxygen saturation and signs of circulatory embar-
rassment. Decreasing air entry and breath sounds
indicate the need for chest drainage.
Circulation
Restoration of the circulation may take precedence
over the airway and ventilation if the patient is
breathing satisfactorily. It can be assessed simultane-
ously with the airway and breathing if an experienced
anaesthetist is available to manage ventilation.
There are two major causes of circulatory embar-
rassment – cardiac damage/tamponade and haemor-
rhage. The former is rare but life threatening and
easily missed. It must therefore be briefly considered
in all patients with major injuries, especially in those
with penetrating injuries of the chest.
Cardiac tamponade
Cardiac tamponade occurs when large quantities of
blood collect within the pericardial cavity, around the
heart, and embarrass its action. This reduces the car-
diac output, producing a weak pulse and hypoten-
sion. The condition should be suspected if the jugular
venous pressure is markedly elevated and rises
rather than falls with inspiration (Kussmaul’s sign);
however, jugular venous distention may not occur
in a patient who has lost a large quantity of blood.
Pulsus paradoxus, when the pulse volume
decreases on inspiration rather than increasing, may
be present. The heart sounds are usually muffled and
poorly heard.
Chest radiographs may show an enlarged car-
diac shadow. An echocardiogram will confirm the
diagnosis.
The patient’s condition may be stabilized by
aspirating the blood from the pericardial sac using
echocardiography and electrocardiography to ensure
correct placement of the needle and catheter before
definitive surgery is undertaken.
Revealed haemorrhage
Visible arterial bleeding presents as a pulsating
stream of bright red blood coming from an open
wound, whereas venous bleeding is dark and con-
tinuous. Arterial haemorrhage from an open wound
can usually be controlled by direct digital pressure
or proximal arterial compression. Sterile vascular
clamps can be applied directly to bleeding arteries for
temporary control before definitive surgery if these
simple measures fail.
Venous bleeding always responds to simple
pressure and may be made worse by the application
of a tourniquet.
Revealed bleeding should always be assessed and
controlled as soon as possible. There is no point in
pouring fluid and blood into the circulation through
Chap-02.qxd 4/19/05 13:41PM Page 39
The symptoms, signs and emergency management of major injuries
40
intravenous catheters when an equal amount is rap-
idly escaping.
Concealed (internal) haemorrhage
Concealed haemorrhage is much harder to diagnose
and therefore must be suspected in all patients with
multiple or serious injuries. It always accompanies
major fractures of long bones and fractures of the
pelvis. It must, if possible, be rapidly diagnosed and
treated, as it is an important, potentially irreversible,
cause of death in an injured patient.
Clinical signs of haemorrhage
The diagnosis is based on finding the signs of hypo-
volaemic shock – a pale, anxious, sweaty patient with
cold extremities, a rapid, thready pulse, tachyp-
noea and hypotension. These signs occur when the
body redistributes the circulation in an attempt to
maintain the blood flow to the vital organs (heart
and brain). Other organs, such as the skin, intestine
and kidneys, become inadequately perfused and
poorly oxygenated. This homeostatic response is
brought about by the sympathetic nervous system
causing a tachycardia and vasoconstriction in the
extremities. The skin becomes cool and clammy.
The systolic blood pressure is usually maintained at
first, but the pulse pressure (the pressure difference
between systolic and diastolic pressures) may be
reduced by a rise in the diastolic pressure. The rate of
respiration increases to try to improve oxygenation.
Patients who arrive in the accident and emer-
gency department without overt haemorrhage but
who exhibit these signs have almost certainly lost
1–2 litres of blood. It is important to remember that
young, fit patients can often tolerate considerable
blood loss before they develop, often very suddenly,
any signs of hypovolaemic shock, whereas elderly
patients, especially those on beta-blockers or digi-
talis, tolerate quite small amounts of blood loss
less well.
All seriously injured patients must have their
pulse rate, blood pressure, respiratory rate, level
of consciousness and tissue oxygenation moni-
tored continuously. Patients with an associated head
injury must be monitored using the Glasgow Coma
Scale (see Revision panel 1.3, page 12). A urinary
catheter and the measurement of central venous
pressure provide additional valuable information for
monitoring resuscitation when there are signs of
hypovolaemia. An intra-arterial pressure line is also
very useful for continuously monitoring the blood
pressure, and allows easy sampling of arterial blood
for blood gas and acid/base measurement.
Once blood loss is suspected, the patient must
be given immediate fluid replacement through two
wide-bore cannulae inserted into the veins of the
cubital fossae. Fluid can be given faster through a
central venous catheter if this has been inserted for
monitoring purposes and is not contra-indicated by
the presence of neck and chest injuries. One to two
litres of crystalloid (normal saline) or colloid should
be given after sending a sample of the patient’s blood
for grouping and cross-matching. For patients
with clear signs of shock, request at least 4 units of
blood.
Patients who fail to respond to the rapid restora-
tion of their blood volume in the absence of cardiac
or major respiratory problems, e.g. tamponade or
tension pneumothorax, probably have severe con-
tinuing blood loss. In these circumstances the blood
transfusion should be started while making a rapid
assessment of the potential sites of concealed blood
loss. The most common are the pleural or abdomi-
nal cavities. Fractures of the pelvis can also cause
catastrophic blood loss.
The retroperitoneum can contain litres of blood
with few external physical signs.
A rapid clinical examination looking for chest
dullness, abdominal distension and abdominal ten-
derness (if the patient is conscious) should be followed
by chest radiography, insertion of chest drains and
computerized tomography (CT) scanning of the
torso or peritoneal lavage where indicated. Properly
warmed Group O Rh-negative blood or, as a last
resort, uncross-matched blood can be given if the
situation is dire. The patient should be transferred
to an operating suite once the site of blood loss has
been established.
Echocardiographs and electrocardiographs
(ECGs) can be helpful if cardiac injury or coinci-
dental cardiac disease is suspected. The ECG leads
should be kept connected to a monitor for the
detection of any dysrhythmias. A cardiac contu-
sional injury should be suspected if there is wide-
spread ST segment elevation or depression. Very
occasionally, an emergency thoracotomy in the acci-
dent and emergency department may be required to
Chap-02.qxd 4/19/05 13:41PM Page 40
The secondary survey
41
relieve a tamponade, to suture a penetrating wound
of the heart or to clamp the hilum of the lung or the
descending aorta to prevent massive blood loss.
These heroic attempts are seldom successful.
Rapid transfer to an operating theatre with trained
staff, proper instruments and adequate lighting
increases the chances of success.
THE SECONDARY SURVEY
Many injured patients do not deteriorate catastro-
phically. The majority stabilize rapidly after being
resuscitated with intravenous fluids. This favourable
response provides time to carry out a full secondary
survey to assess other systems and body parts which
may have been injured and to assess the general fit-
ness of the patient. It is important to continue mon-
itoring the patient while the secondary survey is
being carried out to detect any further or new bleed-
ing or chest problems.
The whole patient must be examined from the top
of the head to the toes. Other blood tests, investiga-
tions and diagnostic procedures should be under-
taken as necessary after the secondary survey is
complete. Adequate analgesia may be needed before
beginning the secondary survey, especially in fully
conscious patients in whom the primary survey and
resuscitation have been quickly completed.
History
A detailed history should be taken from a stable,
conscious patient at this stage. It is helpful to ask the
patient what they remember of the accident and
useful if they can describe what happened. The
mechanism of the injury and the possible physical
forces involved often give a useful indication of the
site and severity of the damage. Knowledge about
the height of a fall, the speed of a car, the use of guns
or knives, the presence of an explosion or fire and
the use of protection devices such as seat belts or
airbags is often helpful. If the patient is uncon-
scious, obtain the observations and views of family,
friends, bystanders or paramedics.
Pain, dysfunction and malfunction
The conscious patient should be asked if they have
any localized areas of pain or malfunction, which may
indicate particular areas or systems that require more
detailed examination.
Conscious patients must also be asked if they had
experienced any loss of consciousness during or after
the injurious event. Their cognitive function should
be quickly tested by asking a few questions about
who they are, where they live and their occupation.
The history from a third party of a lucid interval is
also helpful if the patient is unconscious.
General and previous history
Take a full history of previous illnesses, operations,
drugs and allergies (see Chapter 1). The patient’s
general fitness, occupation, tobacco and alcohol
usage should be recorded following a full systematic
enquiry.
Record the time that the patient last ate or
drank. This is very important if the patient is to
have a general anaesthetic.
General examination of a conscious
patient
The head
Scalp
The scalp must be inspected and palpated for
lacerations, swellings, bony depression and distortion.
Orbits
Palpate the margins of the orbits for depres-
sions or irregularities.
Eyes
Examine the eyes for pupil size, reaction and
red-reflex. Test the eye movements and visual acuity
(see Chapter 1).
Occasionally a corneal injury may lead to loss of
the anterior chamber and prolapse of the iris, with
an obvious collection of blood behind the cornea.
The presence of a large subconjunctival hae-
morrhage (see Fig. 8.17, page 229) that spreads to the
full extent of the conjunctival attachment suggests
that there is a fracture of the base of the skull. Panda
eyes (black circumorbital haematomata around one
or both eyes) (see Figs 2.1 and 8.17, pages 42 and 229)
also suggest the presence of a skull base fracture or a
fracture of the upper jaw. Diplopia, especially on
looking up, is indicative of a blow-out fracture of the
floor of the orbit, which often allows the eyeball to
sink inwards, giving the upper face an asymmetrical
appearance.
Signs of intracranial haemorrhage
A fixed dilated pupil which fails to respond to light
indicates third nerve compression, by a contralateral
Chap-02.qxd 4/19/05 13:41PM Page 41
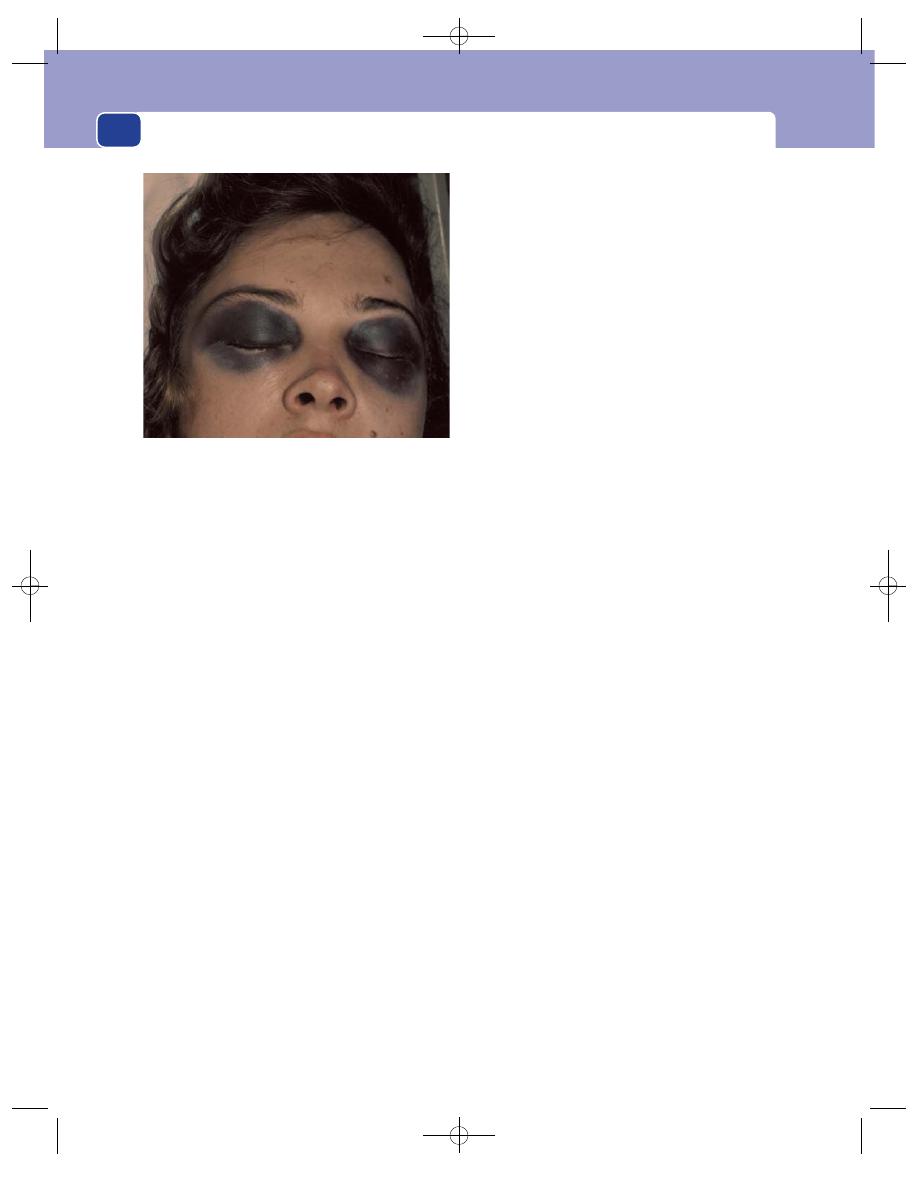
The symptoms, signs and emergency management of major injuries
42
extradural haemorrhage or a direct injury to the optic
nerve. Deterioration of the patient’s score on the
Glasgow Coma Scale – which quantifies eye opening,
verbal response and motor response – and/or agita-
tion indicate increasing cerebral compression. The
patient is in ‘coma’ if their Glasgow Coma Score is
less than 8.
Loss of upwards gaze, other cranial nerve pare-
ses or developing contralateral hemiplegia are indi-
cative of a cerebral haemorrhage.
Observations should also be made on the patient’s
mental state, including whether they are agitated
or confused. A rising blood pressure, a falling pulse
and slowing of respiration suggest coning, a con-
dition in which the swollen brain is forced down
through the medullary foramen, with subsequent
loss of all vital functions. An urgent CT scan should
be obtained.
The face
Major facial injuries often cause consider-
able orbital oedema, but it is very important to
retract the lids carefully, using two people if neces-
sary, to look for any of the features described above.
The cheek bones should also be palpated for a ‘step’
and any asymmetry noted. Fractures of the zygoma
and blow-out fractures of the orbit have to be con-
firmed by radiographs, but loss of sensation over
the cheek from damage to the infra-orbital nerve
strongly suggests a fracture of the cheek bones.
Instability of the maxillary zygomatic process (a
LeFort-type fracture) is tested by inserting a gloved
finger or thumb into the mouth and attempting
to pull the upper jaw complex forward from the
base of the skull. A fracture is present if rocking
occurs. This needs to be done with care, as forceful
rocking may cause a massive pharyngeal bleed,
which can only be controlled by pushing the whole
bony facial complex backwards to compress the
bleeding vessels.
The lower jaw and its stability on the tempero-
mandibular joints must also be assessed. Malocclusion
and an open-bite deformity suggest a fractured jaw,
as does numbness of the lower lip.
Carefully palpate and inspect the mouth, teeth and
gums and record the number of missing or damaged
teeth. Missing teeth indicate the need for a chest
X-ray, if this has not already been performed, to
exclude the possibility that they have been inhaled
and are lodged in the lung.
The nose, face and ears
The nose should be pal-
pated to exclude a fracture and detect the presence
of any bloody or clear fluid discharge of cere-
brospinal fluid which would suggest the presence of
a fracture in the anterior cranial fossa (often associ-
ated with panda eyes and an extensive subconjunc-
tival haemorrhage).
The facial muscles (VIIth cranial nerve) and
auditory acuity should be tested.
Blood or fluid coming from the ear suggests the
presence of a posterior fossa fracture. The tympanic
membrane must be examined with an auroscope.
Bruising behind the ear (Battle’s sign) (see Fig. 2.2)
suggests a fracture in the posterior cranial fossa.
Skull radiographs, specific facial views and CT scans
are usually required to assess these injuries.
The neck
The importance of not causing or exacer-
bating any spinal cord damage, especially during
airway assessment, endotracheal incubation or mov-
ing the patient, is now well recognized. A full radio-
logical assessment of the cervical spine should be
carried out as soon as the patient is relatively stable
if there are any concerns that the spine may have
been damaged.
Pain and local tenderness are suggestive of a
cervical fracture, but there may be few, if any, phys-
ical signs, and further assessment may have to be
delayed until the condition of the cervical spine has
been established. If the spine is normal, the neck can
be carefully palpated for bruising and deformity
FIG 2.1
‘Panda eyes’. Extensive peri-orbital extravasation of
blood from a fracture of the base of the skull.
Chap-02.qxd 4/19/05 13:41PM Page 42
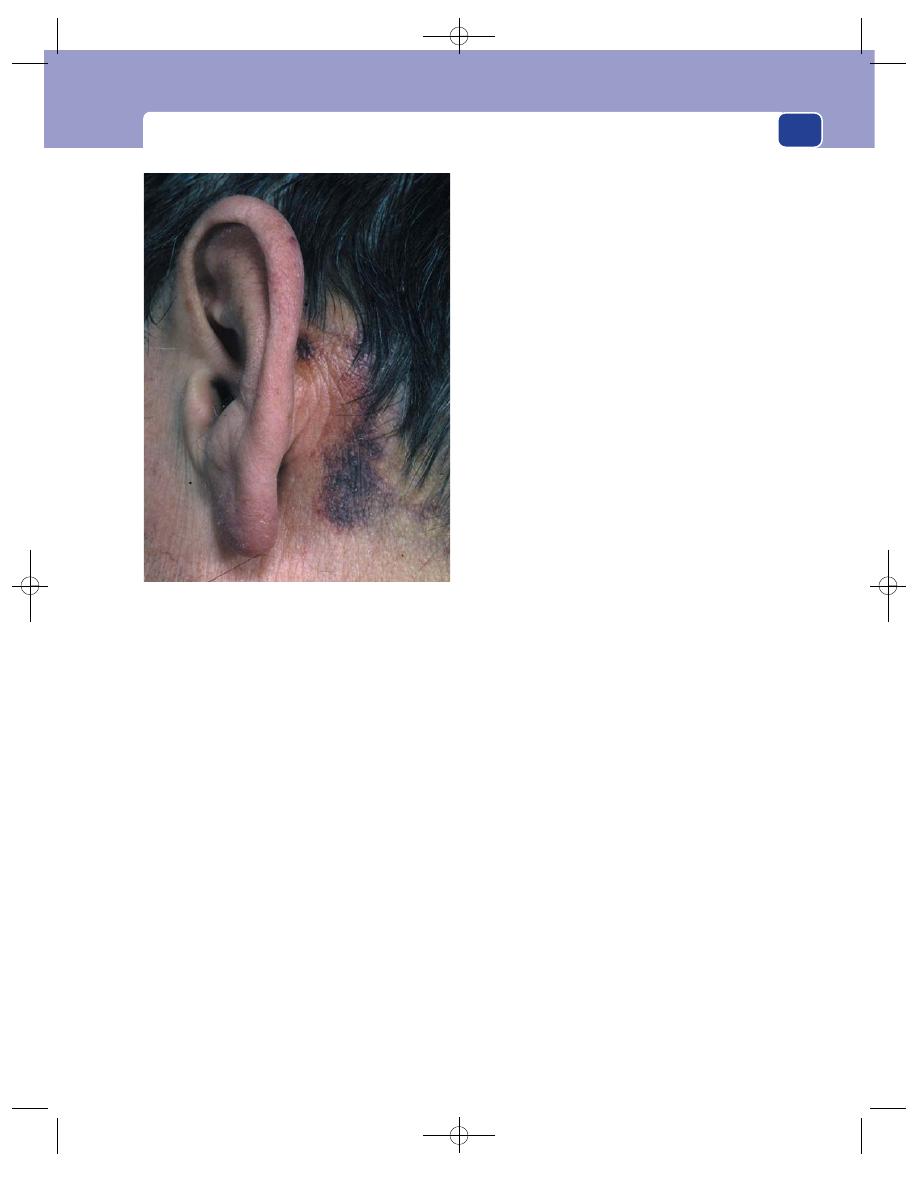
The secondary survey
43
and inspected for any penetrating wounds. The posi-
tion of the trachea in relation to the manubrioster-
nal notch should be assessed to see if it is central.
Gentle palpation should detect the presence of
any subcutaneous surgical emphysema in the neck
or supraclavicular fossae.
Penetrating descending wounds of the root of
the neck can be very dangerous, as they may cause
damage to the supra-aortic blood vessels – the
carotid, vertebral and subclavian arteries – as well as
to the trachea, larynx, pharynx and oesophagus.
Major structures within the upper chest can also be
damaged. The presence of neurological signs or
ischaemia of the upper limb suggests a major arte-
rial injury, as does a rapidly expanding haematoma
or a machinery murmur. Neck wounds should be
explored in the operating theatre.
The clavicle should be palpated along its course.
Severe compound clavicular injuries are often
associated with injuries to the subclavian or axillary
vessels, the brachial plexus and the apex of the lung.
Examine the vascular supply and peripheral nerves
of both upper limbs to exclude these possibilities.
The chest
Although the chest was quickly assessed as
part of the primary survey, it should now be carefully
re-examined by inspection, palpation, percussion
and auscultation to detect any minor signs that may
have been missed at the time of the initial examina-
tion and treatment when speedy resuscitation was
essential. New signs may have developed and subtle
signs may have been missed.
Test again for rib fractures. A careful inspection
may detect a small flail segment. The chest should be
‘sprung’ by compressing it with both hands, antero-
posteriorly and from side to side, and then quickly
releasing. Pain on compression or release indicates the
likelihood of rib fractures or costal cartilage separa-
tion from the ribs or sternum. Both can then be more
accurately localized by detailed palpation. It should be
remembered that rib fractures are often associated
with injuries to the great vessels, lungs, spleen or liver.
The sternum must also be inspected and pal-
pated. Sternal fractures are often associated with
cardiac injuries.
Check again for the presence of a haemothorax,
pneumothorax and cardiac tamponade, taking
particular care to look for small pneumothoraces
and an increase in the width of the mediastinum,
which may be the only indication of an aortic dis-
section. A chest radiograph should always be
obtained if there is any question of a chest injury.
CT chest scans are even more accurate in detecting
minor abnormalities and rib fractures.
The abdomen
The primary survey of the abdomen
usually detects the signs of major intra-abdominal
haemorrhage, but a secondary survey is essential to
pick up continuing severe haemorrhage or further
bleeding following the restoration of a normal blood
pressure.
Increasing abdominal distension, tenderness
and guarding are all significant signs, especially
when associated with a rising pulse and other signs
of hypovolaemia.
The bowel sounds may or may not be abolished
by free blood or bowel contents in the peritoneal
cavity.
Skin bruising over the abdomen, penetrating
wounds and associated rib fractures all indicate the
possibility of abdominal organ damage. When doubt
FIG 2.2
Battle’s sign. Bruising behind the ear suggests a
fracture in the posterior cranial fossa.
Chap-02.qxd 4/19/05 13:41PM Page 43
The symptoms, signs and emergency management of major injuries
44
persists, ultrasound, CT scanning or peritoneal
lavage may be indicated. A CT scan is very useful if
there is an associated pelvic fracture.
Blood coming from the external urethral meatus
or frank haematuria suggests kidney, bladder or
urethral damage. Rectal and vaginal examination
can confirm a high-riding and boggy prostate or
associated vaginal injuries. The presence of these
injuries must always be excluded before allowing
catheterization by inexperienced junior staff or
nurses. It may be preferable to insert a suprapubic
catheter if palpation or percussion detects a large
bladder, especially if the prostate feels abnormal or
blood has been seen coming from the urethra.
Pelvic fractures are commonly associated with
severe shock and with tenderness on springing the
pelvis by pressing back on both iliac crests and
releasing.
The upper and lower limbs
All surfaces of the limbs
must be fully inspected and the presence of bruis-
ing, lacerations, instability and deformity carefully
noted. All the major bones should be carefully pal-
pated along their full length to detect any bony
deformity and swelling that were not appreciated by
the inspection. The only indication of an undiag-
nosed, undisplaced fracture may be the detection of
a localized point of tenderness. Major fractures are
almost always associated with some deformity
together with swelling from the associated bleeding.
The circulation
Signs of hypovolaemic shock are
common. The radial and pedal pulses should be felt
and compared. The presence of equal symmetrical
pulses indicates that a major vascular injury in the
limbs is unlikely (see Chapter 7). Unfortunately, the
peripheral pulses are often difficult to feel in a
shocked, cold patient with severe limb bruising and
concomitant fractures. When the pulses cannot be
felt in an adequately resuscitated patient, it is helpful
to measure the arterial pressure with a Doppler flow
detector (see Chapter 7). Persisting pallor, especially if
it only affects one limb, is a sign of severe ischaemia.
The presence of a compartment syndrome must
always be considered when there are combined bony
and vascular injuries. This condition may also fol-
low the successful surgical re-vascularization of an
injured limb. Compartment syndromes begin with
pain, tenderness and swelling over the anterior shin
or calf muscles. The swelling can exacerbate the
ischaemia, obliterate the pulses and lead to muscle
and nerve death if left untreated.
The nerves
The peripheral nerves must be fully
examined in both the upper and lower limbs if the
patient is conscious. Test power, tone, coordination,
sensation and the reflexes. Test the movement of
joints controlled by the major muscle groups. Test
sensation by the response to light touch and pinprick.
Always test and document the peripheral nerves
beyond any laceration. A more detailed neurological
examination should be carried out if abnormal neu-
rological signs are detected, or if the patient is
unconscious (see below).
The back (thoraco-lumbar spine)
The discovery of
paralysis or weakness of several muscles may be the
first indication of a spinal cord injury. The patient
must then be carefully immobilized and ‘log rolled’
by a team of staff to allow examination of the spine.
Log rolling allows turning of the patient in a coordi-
nated manner that keeps the spine immobilized at
all times. Detailed radiographs and even CT scans
may be required if a spinal fracture or spinal cord
injury is suspected. Palpation down the back over
the spinous processes may detect a boggy swelling,
deformity or a ‘step’ in the regularity of the spinous
processes. While the patient is on their side, take the
opportunity to inspect and palpate the back of the
head, neck, torso and limbs to exclude any major
injuries to this surface of the body which may have
passed unnoticed at the initial survey. A rectal
examination should be performed at this stage and
peri-anal sensation, motor function and sphincter
tone and the bulbo-cavernosus reflex tested.
The secondary survey in the
unconscious patient
The secondary survey in an unconscious patient
should begin with a reappraisal of the Glasgow Coma
Scale to discover if the level of consciousness has
changed from the initial assessment. This is impor-
tant, as the whole purpose of resuscitation and assess-
ment is to rectify factors such as hypotension or
hypoxia that could cause neurological deterioration
while trying to detect the presence of an intracranial
haemorrhage, which can usually be treated effectively.
Any suggestion of a ‘lucid interval’ – a period of con-
sciousness after the injury before the patient became
Chap-02.qxd 4/19/05 13:41PM Page 44
The secondary survey
45
unconscious – is an important sign of a developing
intracranial haematoma. Monitoring of the Glasgow
Coma Scale must be carried out at frequent intervals
in comatosed patients with a score of 8 or less.
Patients must be frequently asked to open their eyes
and move their limbs. If they do not respond, apply
a painful stimulus by pressing hard on the bone of
the upper orbit or the manubrium sterni. An ability
to localize pain is accepted if the patient moves one
or other hand to try to push away the painful stim-
ulus, whereas flexion or, worse still, extension of the
upper limbs indicates a severe brain injury.
Verbal responses are impossible to assess in
patients who are anaesthetized, intubated or have suf-
fered severe facial injuries. It must also be remem-
bered that some head-injured patients may be
mentally defective, some may have taken an over-
dose of drugs or alcohol, and some be unable to
understand your language.
A detailed neurological examination should be
carried out to discover if there are any focal neurolog-
ical signs indicative of brain injury or an expanding
intracranial haematoma. This should start with the
examination of the size, symmetry and reaction to
light of the pupils. If the brain is shifted to one side
by an expanding haematoma, the ipsilateral third
nerve becomes compressed against the rigid free edge
of the tentorium cerebelli. At first this causes slight
constriction of the pupil, but then, later, dilatation
and eventually a failure to respond to a bright light
being shone directly into it.
If left untreated, the haematoma will continue to
expand and force the brain down through the tentor-
ium and into the foramen magnum. The contralat-
eral pupil then becomes dilated and unreactive.
Eventually compression of the medulla causes
bradycardia, a rising blood pressure and depressed
respiration.
Do not forget that optic nerve injuries, previous
eye disorders and drugs can also cause the pupil to
be unresponsive.
Neurological examination of the limb should con-
centrate on detecting any evidence of hemiplegia.
Unilateral paralysis, increased muscle tone, brisk
reflexes and upgoing plantar reflexes on the contralat-
eral side of the injury all indicate that a haematoma
is present.
Intracranial haematomata outside of the sub-
stance of the brain develop in two sites.
■
Extradural haematomata are usually the result
of haemorrhage from the middle meningeal
artery. This is often caused by a linear temporo-
parietal fracture of the skull. Patients are often
briefly knocked unconscious or dazed by the
initial injury, but then regain consciousness
(the lucid interval) before becoming drowsy
and eventually losing consciousness. As the
intracranial pressure rises, patients may
complain of a headache, blurred vision and
vomiting. At this time, the localizing signs
described above begin to develop.
It must be remembered that some patients
develop an extradural haematoma without a
lucid interval and without the classic
progression of neurological signs. The certain
indicator of deterioration is a progressive
reduction of their Glasgow Coma Scale score.
A CT scan will confirm the diagnosis.
■
Subdural haematomata can be classified as
either acute or chronic.
Acute subdural haematomata are invariable asso-
ciated with major brain injury when torn vessels on
the surface of the brain continue to bleed into the
subdural space. Patients are usually deeply uncon-
scious and develop neurological localizing signs. It
is very difficult to differentiate an acute subdural
haematoma from an intracerebral haemorrhage, cere-
bral oedema or diffuse axonic injury. A CT scan of the
head is essential.
Chronic subdural haematomata usually occur in
elderly patients after a minor injury which tears a vein
on the surface of the brain that bleeds slowly but per-
sistently for days or weeks. They are also common in
alcoholics and patients on anti-coagulants. Patients
often present with fluctuating levels of consciousness,
worsening over several days or weeks. The raised
intracranial pressure may cause headache, vomiting,
blurred vision (papilloedema) (Fig. 2.3), personal-
ity change and drowsiness. Pupil changes and some
neurological localizing signs are usually present. The
diagnosis is confirmed by a CT scan of the brain.
Brain death
A number of patients with severe head injuries
develop brain death or a persistent vegetative state.
In brain death the brain stem is irreversibly damaged.
Chap-02.qxd 4/19/05 13:41PM Page 45
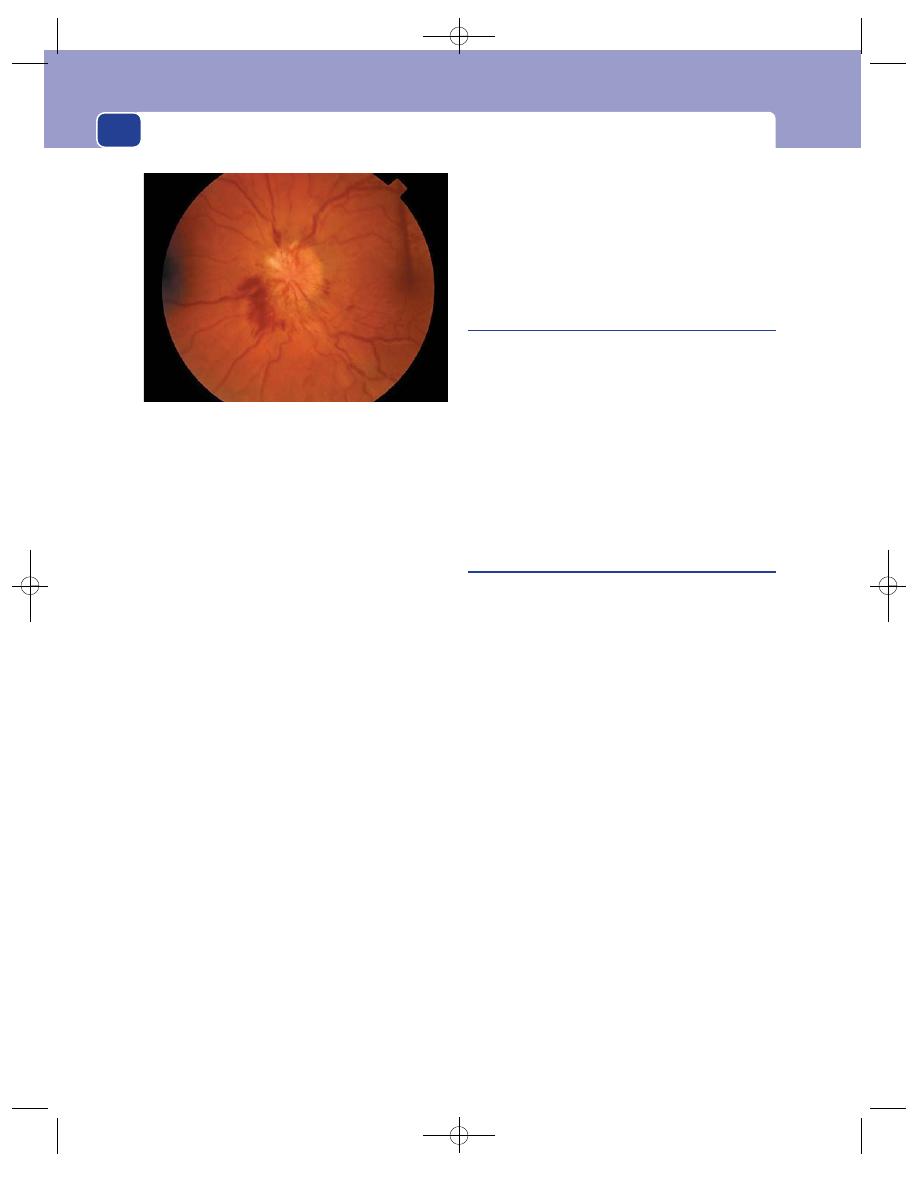
The symptoms, signs and emergency management of major injuries
46
In a vegetative state the brain survives but there is
severe cortical damage. Patients with a persistent veg-
etative state can survive on or off a ventilator for
many years. Recovery can occur after several months,
but becomes increasingly unlikely as the months
pass, especially if there are localizing or generalized
signs of brain injury.
A number of criteria must be fulfilled to confirm
brain death. Patients must be normothermic and off
all drugs. Brain-dead patients are apnoeic and deeply
comatosed. They have no pupillary response to light
and the corneal reflexes are absent. They have no
response to pain or to movement of the endotracheal
tube when off all sedation. The final test is to look for
the presence of a caloric vestibulo-ocular response.
The external auditory meatus is syringed with ice-
cold water, which normally causes nystagmus. When
this does not occur, brain death is confirmed and
relatives must be appropriately counselled. Brain-
dead patients are the main source of organs for trans-
plantation.
Assessment of multiple casualties
All hospitals should have a major accident plan in
which the roles of accident and emergency doctors,
other medical staff, nurses, theatres, telephone staff,
managers and press liaison officers are all clearly
defined. These plans should be tested from time to
time to assess their effectiveness and encourage famil-
iarity. Each patient must be carefully assessed by the
techniques described above into dead, immediate
life-threatening injuries, those with major injuries
and those who can be called the ‘walking wounded’.
Scoring systems
There are a number of scoring systems which have
been developed to try to improve management and
outcome of patients who have been injured. These
allow the results of individual centres to be com-
pared against one and other. The Revised Trauma
Score is probably the best measure. It allows an audit
of outcome against expected recovery or likely death.
Any variation from the expected outcome should be
critically examined to discover if earlier diagnosis or
more efficient resuscitation or treatment would
have achieved a better result.
FIG 2.3
Papilloedema, a diagnostic sign of a chronically raised
intracranial pressure most often caused by a space-occupying
intracranial tumour or a chronic subdural haematoma.
(Courtesy of Dr E Graham.)
Chap-02.qxd 4/19/05 13:41PM Page 46
The skin and subcutaneous tissues
The skin is the organ that controls body temperature
and fluid balance as a consequence of its barrier func-
tion (impeding water loss) and sweat glands, which
are capable of increasing or decreasing the loss of
water and electrolytes and body heat.
The skin consists of two layers: the epidermis,
derived from ectoderm, and the dermis, derived from
the mesoderm.
The epidermis
The epidermis is a stratified squamous epithelium
composed of four layers:
■
basal cells
■
prickle cells
■
granular cells
■
keratin (horny layer).
Keratin, which consists of dead epidermal cells,
acts as a protective coat. Increased mitoses occur in
the basal layer if the keratin layer is lost, so greater
amounts of keratin are produced in response to fric-
tion or pressure.
Melanoblasts, derived from the neural ectoderm
of the anterior horn cells, migrate into the basal lay-
ers of the epidermis. They produce the pigment
melanin in response to a number of stimuli and
transfer this to the nearby keratinocytes through
their dendritic processes.
Langerhans cells are also present in the epider-
mis and are part of the monocyte macrophage sys-
tem, which processes antigen.
Merkel cells are mechano-receptors present in
the epidermis.
Hair and nails are derived from modified keratin
by invagination of the epidermis.
The dermis
The dermis is made up of collagen bundles and
various proteoglycans which form a supporting
framework for blood vessels, lymphatics, nerves, seba-
ceous glands, sweat glands and hair follicles. The
dermis also contains histiocytes and mast cells,
which can act as antigen-presenting cells and are
part of the reticulo-endothelial system.
The dermis is subdivided into the capillary der-
mis and the deeper reticular dermis which sits on
the deep fascia.
THE DIAGNOSIS OF SKIN CONDITIONS
There are many skin problems that require surgical
treatment and form an important part of general
surgical practice. This chapter concentrates on the
common skin problems that are likely to be seen in
a surgical clinic.
It is difficult to draw up a set of simple diagnos-
tic pathways suitable for all skin lesions because
they have such varied features. For example, a basal
cell carcinoma can be a raised nodule, a flat plaque
or an ulcer, and can be skin coloured, pearly white,
brown or pink. It is therefore better to learn the
physical features of each skin lesion, and the best
way to do this is by examining as many as you can.
The diagnosis of skin lesions relies heavily on care-
ful inspection and pattern recognition. Tactile and
auditory skills are less important.
When you are familiar with the physical features
of the common skin lesions, do not use your knowl-
edge to indulge in the game of ‘spot diagnosis’ –
instant diagnosis after one brief glance. This is dan-
gerous and likely to lead to mistakes. Always examine
every skin blemish fully before making a diagnosis,
however familiar the lesion.
Lesions in the skin have two basic distinguishing
features: their colour and their relationship to, and
effect on, the overlying epidermis. The overlying
epidermis is likely to be raised and look abnormal if
the abnormal tissue is in the superficial part of the
Chap-03.qxd 4/19/05 13:42PM Page 47
The skin and subcutaneous tissues
48
dermis. An ulcer will develop if a localized area of the
epidermis is destroyed. Alternatively, the overlying
epidermis may be stretched but otherwise normal if
there is an abnormality deep in the dermis.
It is possible, therefore, to subdivide all skin lesions
into three categories:
■
those with an intact but abnormal epidermis,
■
those in which an area of the overlying
epidermis is destroyed (ulcers),
■
those covered with a normal epidermis.
Revision panel 3.1
The features of the history and examination of a
lump or skin lesion that must be elicited
History
Age
Sex, ethnic group, occupation
First local symptom
Other symptoms
Duration of symptoms
Development of symptoms
Persistence of symptoms
Multiple or single lesions
Systemic symptoms (direct questions)
Possible cause
Family history
Social history
Local examination
Site
Shape
Size
Colour
Temperature
Tenderness
Surface
Edge
Ulcer (edge: base, depth, discharge,
surrounding tissues)
Composition/contents:
Consistence
Fluctuation
Resonance
Fluid thrill
Transluscence
Pulsatility
Compressibility
Bruit
Reducibility
Relations to surrounding structures
Lymph drainage
State of local tissues (arteries, nerves,
bones and joints)
General examination
Revision panel 3.2
The terms used to describe skin pathology
Macule
A localized change in colour
of the skin which is not elevated
(or palpable) or freckled
Papule
A small solid elevation, flat
topped, conical, round,
polyhedral, follicular (hairs),
smooth or scaly
Vesicle
A small collection of fluid
between the dermis and
epidermis (a blister)
Bulla
A collection of fluid larger than
a vesicle, under the epidermis
Wheal
A transient elevation of the skin
caused by oedema
Cyst
A tumour that contains fluid
Naevus
A lesion present from birth,
composed of mature structures
normally found in the skin but
present in excess or in an
abnormal disposition. The term
‘naevus’ is also used to describe
lesions composed of naevus
cells, as in melanocytic or
pigmented naevi
Papilloma
A benign overgrowth of epithelial
tissue
Tumour
Literally, a swelling; commonly
but inaccurately used to mean a
malignant swelling
Hamartoma
An overgrowth of one or more
cell types that are normal
constituents of the organ in
which they arise; the commonest
examples are haemangiomata,
lymphangiomata and
neurofibromata
Ulcer
An area of solution of an
epithelial surface
Chap-03.qxd 4/19/05 13:42PM Page 48
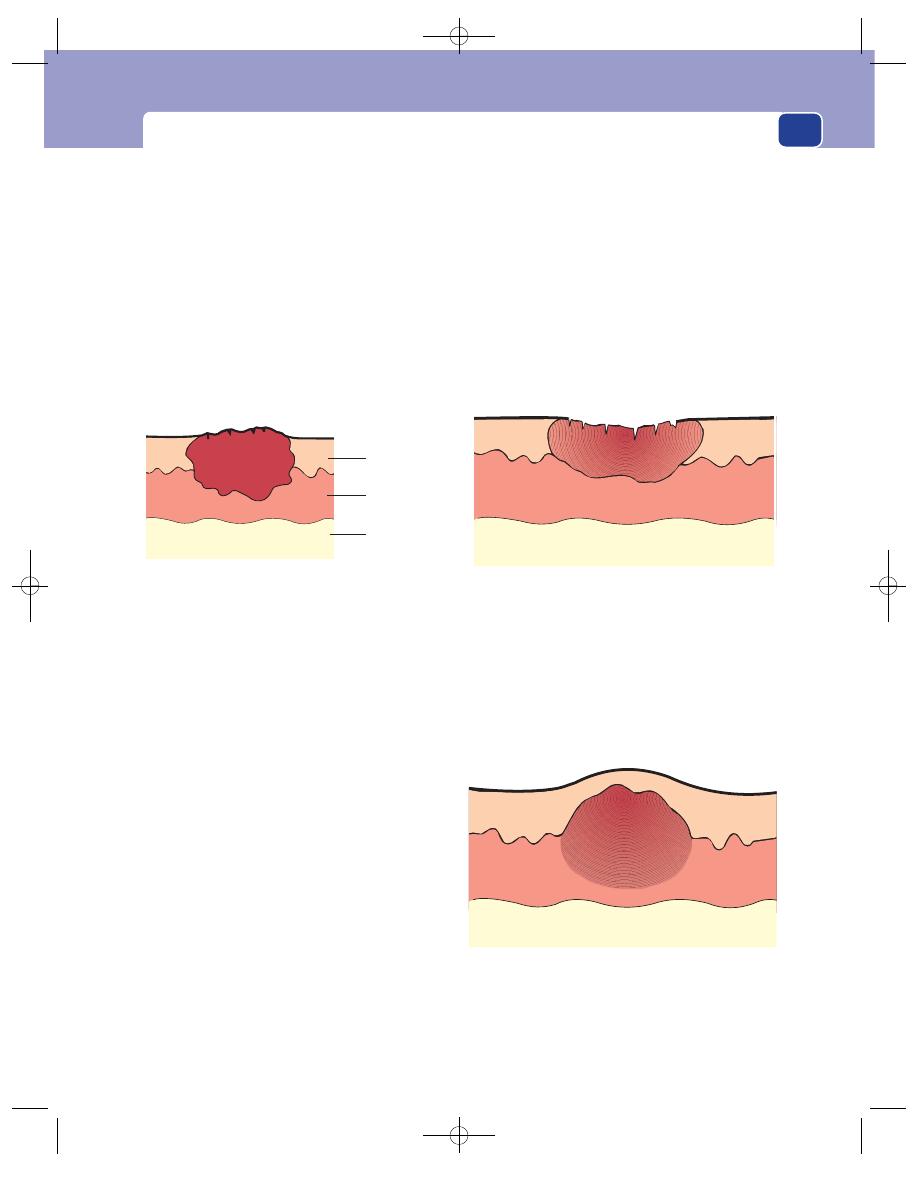
The diagnosis of skin conditions
49
In the last of these, the bulk of the pathology is
likely to be in the subcutaneous tissues, and even
though it may be derived from a skin structure (e.g.
a sebaceous gland), it is usually classified as a sub-
cutaneous lesion.
The colour of skin lesions may be helpful in mak-
ing a diagnosis. Skin lesions may be black, brown,
yellow, red, or normal skin colour.
The following classification, based on the condi-
tion of the overlying epidermis and its colour, gives
some idea of the multitude of lesions that you must
learn to recognize.
Epidermis intact but abnormal
■
Black
Gangrenous skin
Early pyoderma gangrenosum
Early anthrax pustule
■
Brown
Freckles
Seborrhoeic keratosis
Moles of all varieties
Malignant melanoma
Pigmented basal or squamous cell carcinoma
Café au lait patch
Pigmentation following a bruise,
thrombophlebitis, or venous hypertension (the
epidermis may be normal in these conditions)
■
Greyish-brown
Wart
Seborrhoeic keratosis
Keratoacanthoma
■
Yellow-white
Xanthoma
Lymphangioma
Pustules of furunculosis and hidradenitis,
subcutaneous calcinosis
■
Red-blue
Strawberry naevus
Port-wine stain
Spider naevus
Campbell de Morgan spot
Telangiectases
Pyogenic granuloma
■
Skin colour
Papilloma
Early basal and squamous cell carcinoma
Keloid scar
Keratoacanthoma
Destruction of the overlying epidermis:
ulceration
■
Sloping edge A venous, ischaemic, trophic,
neuropathic ulcer.
■
Punched-out edge Ischaemic, trophic, or
syphilitic ulcer.
■
Undermined edge Chronic infection
(tuberculosis, carbuncle), pressure sore.
■
Rolled or everted edge Malignant ulceration.
Overlying epidermis normal
Although these lesions may have arisen from a skin
structure, their mass is beneath the skin and does
not affect its structure. They are usually classified as
subcutaneous conditions.
FIG 3.2
Destruction of the overlying epidermis – ulceration.
FIG 3.3
Overlying epidermis normal.
Epidermis
Dermis
Subcutaneous
tissue
FIG 3.1
Epidermis intact but abnormal.
Chap-03.qxd 4/19/05 13:42PM Page 49
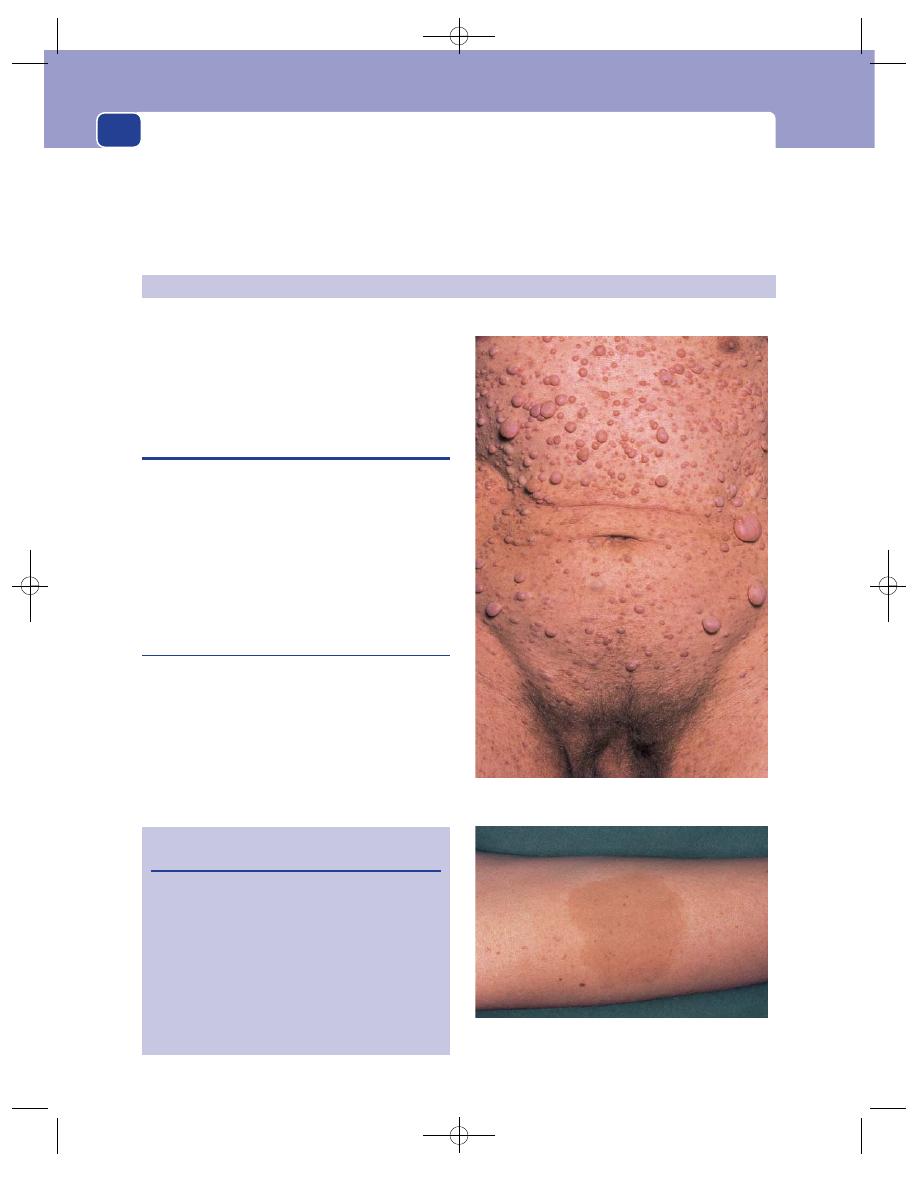
The skin and subcutaneous tissues
50
A café au lait patch on the forearm.
FIG 3.4
VON RECKLINHAUSEN’S DISEASE.
Throughout this book each disease is described
using the standard plan of history taking and
examination presented in Chapter 1. These headings
appear regularly because repetition is the secret of
learning. Revise the plan of history taking and clin-
ical examination set out in Revision panel 3.1.
These may be genetic or non-genetic. The latter are
more common and mostly hamartomata, i.e. tumour-
like malformations in which there is an overgrowth
of normal tissues arranged in an irregular fashion.
GENETIC SKIN DISORDERS
Rare genetic skin disorders such as ichthyosis (a dis-
order of keratin formation which looks like lizard
scales) or epidermolysis bullosa (in which the skin
develops massive blisters after friction or minor
trauma) are only likely to be encountered in a spe-
cialist dermatology clinic, whereas inherited neuro-
fibromatosis is not rare.
Von Recklinhausen’s disease
(Multiple neurofibromatosis)
This is an autosomal dominant condition in which
multiple neurofibromata are present at birth and
increase in number. Patients may have just a few
tumours or multiple tumours over the whole body
surface. The tumours are benign and contain a mix-
ture of neural (ectodermal) and fibrous (mesodermal)
tissue. The condition is associated with a number of
Revision panel 3.3
Congenital skin disorders
Genetic
Alopecia
Ichthyosis vulgaris
Epidermolysis bullosa
Neurofibromatosis
Plantar keratosis
Non-genetic
Hamartomata (e.g. capillary
haemangiomata, lymphan-
giomata, venous angiomata)
Dermoid cysts
CONGENITAL SKIN DISORDERS
Multiple neurofibromatosis. The patient did not have a
café au lait patch within the area of this photograph.
Chap-03.qxd 4/19/05 13:42PM Page 50
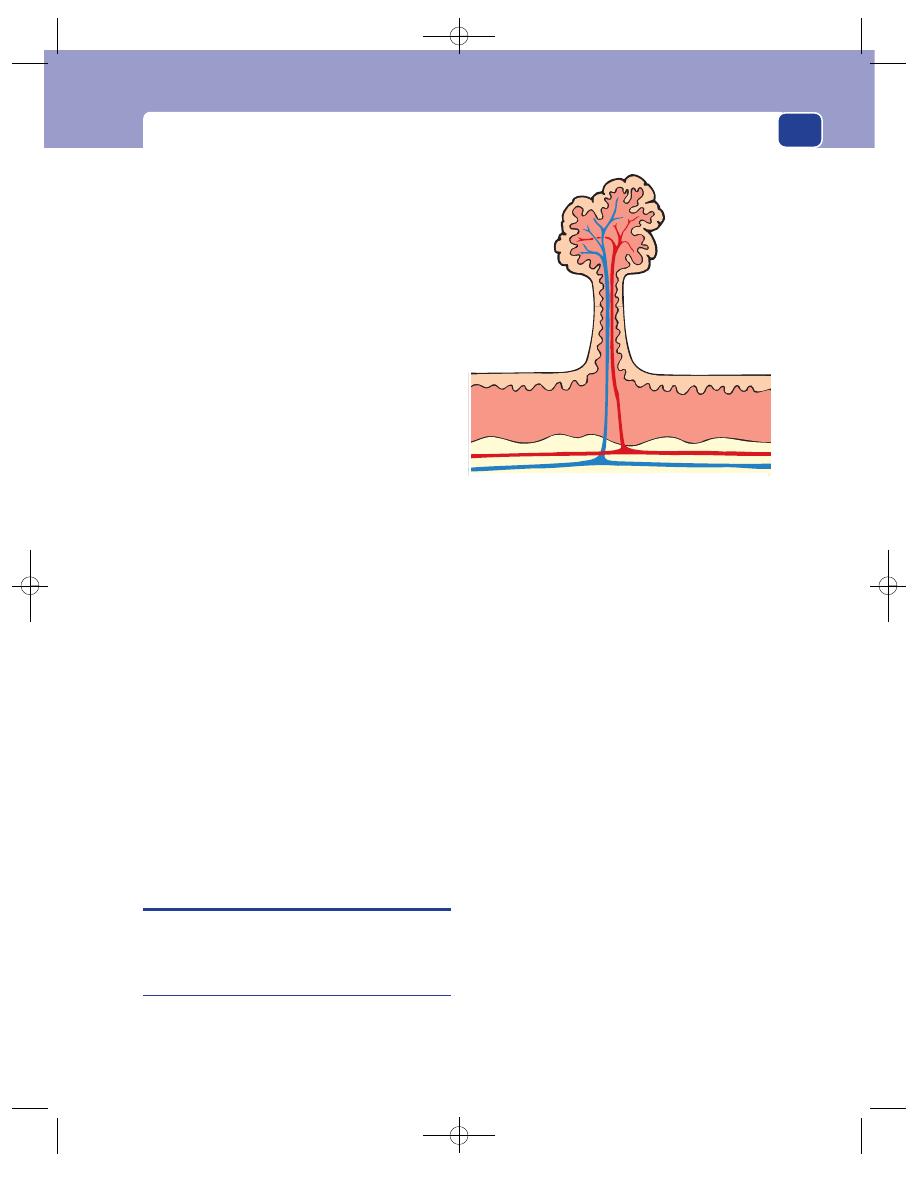
Non-genetic skin disorders
51
related abnormalities, such as:
■
fibro-epithelial skin tags,
■
patches of light-brown discolouration of the
skin (café au lait patches),
■
neuromata on major nerves, especially the acoustic
nerve (acoustic neuroma) and the sensory roots
of the spinal nerves (dumb-bell neuroma),
■
5 per cent of neuromata undergo malignant
change to a neurofibrosarcoma,
■
phaeochromocytoma of the adrenal gland
commonly coexist.
History
Most of the neurofibromata are present at birth but
they increase in size and number during life. One of
the patient’s parents and half of their brothers and
sisters are affected, as the disease is inherited through
a dominant gene.
Examination
The patient is covered with nodules of all sizes, from
minute lumps a few millimetres across to large sub-
cutaneous nodules. Some are in the skin, some are
tethered to it and some become pedunculated. The
nodules vary in consistence from soft to firm, but
each is distinct. They are often slightly pink. Careful
examination of the skin nearly always reveals irreg-
ular patches of pale-brown pigmentation. The pig-
ment is melanin and the patches are known as café
au lait patches. They are a diagnostic feature of von
Recklinhausen’s disease.
The blood pressure should be measured as a coex-
isting phaeochromocytoma may cause hypertension.
Neurological abnormalities are also common. It is
important to test hearing and to examine the spinal
nerves to exclude the presence of major nerve mal-
function caused by neuromata on the acoustic and
spinal nerves.
NON-GENETIC SKIN DISORDERS
Almost all of the following conditions are hamar-
tomata.
Benign papilloma
A benign papilloma of the skin is a simple over-
growth of all layers of the skin. The word papilloma
suggests that this lesion is a benign neoplasm, but this
is not the case; it is a hamartoma, and is better called
a skin tag.
History
Age
Papillomata can appear at any age. A few are
congenital.
Symptoms
The commonest complaint is that the
pedunculated swelling catches on clothes or rubs
against another part of the body. It can become red
and swollen and ulcerate, or even infarct if it is
injured. The skin that forms a papilloma contains
sweat glands, hair follicles and sebaceous glands. All
of these structures can become infected and make the
papilloma swollen and tender. The swelling can look
like a carcinoma if the granulation tissue that forms
in response to the infection becomes exuberant.
Examination
Site
Papillomata occur anywhere on the skin.
Shape and size
Their shape can vary from a smooth,
raised plaque to a papilliferous, pedunculated polyp.
Their size is equally variable.
Colour
They are the colour of normal skin.
Composition
Papillomata are soft, solid and not
compressible.
Lymph glands
The regional lymph glands should not
be enlarged.
FIG 3.5
A papilloma is an overgrowth of all layers of the
skin with a central vascular core.
Chap-03.qxd 4/19/05 13:42PM Page 51
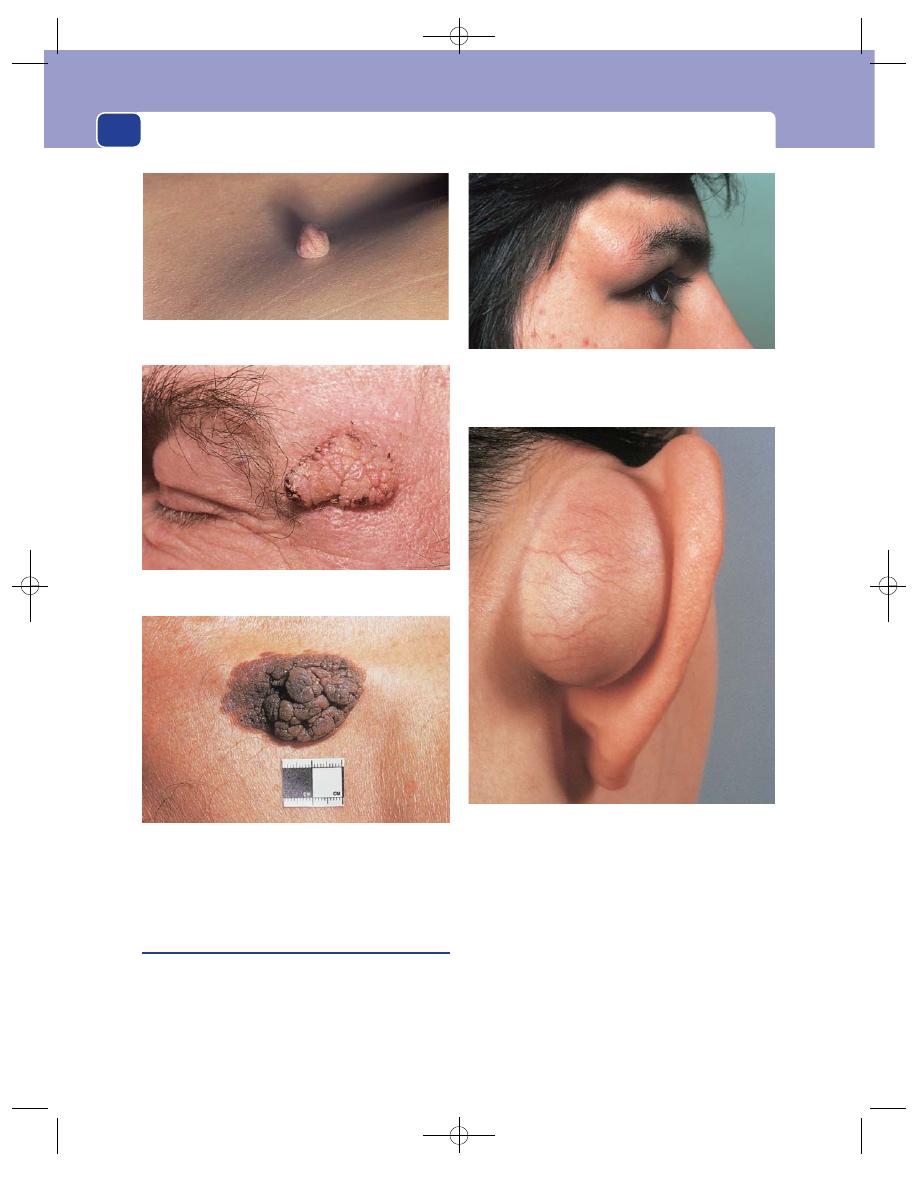
The skin and subcutaneous tissues
52
Local tissues
The adjacent local tissues should be
normal.
Congenital dermoid cysts
A dermoid cyst is a cyst that is deep to the skin and
lined by skin. There are two ways in which a piece of
skin can become trapped deep to the normal skin:
as an accident during antenatal development, and
following an injury, which implants some skin into
the subcutaneous tissue. Dermoid cysts are there-
fore congenital or acquired.
History
Duration
The cyst may have been noticed at birth but
it usually becomes obvious a few years later when it
begins to distend.
Symptoms
The principal ‘symptom’ is parental dis-
tress at the cosmetic disfigurement because most
A deeply pigmented papilloma.
FIG 3.6
PAPILLOMATA.
A smooth papilloma with a narrow pedicle, almost a
fibrolipomatous polyp.
A sessile polyp with excess epithelium covering the clefts and
corrugations.
A dermoid cyst behind the ear. A congenital postauricular
dermoid cyst.
FIG 3.7
DERMOID CYSTS.
A right external angular dermoid cyst, so called because it
lies beneath the outer end of the eyebrow over the external
angular protuberance of the skull. This is a congenital
dermoid cyst.
Chap-03.qxd 4/19/05 13:42PM Page 52
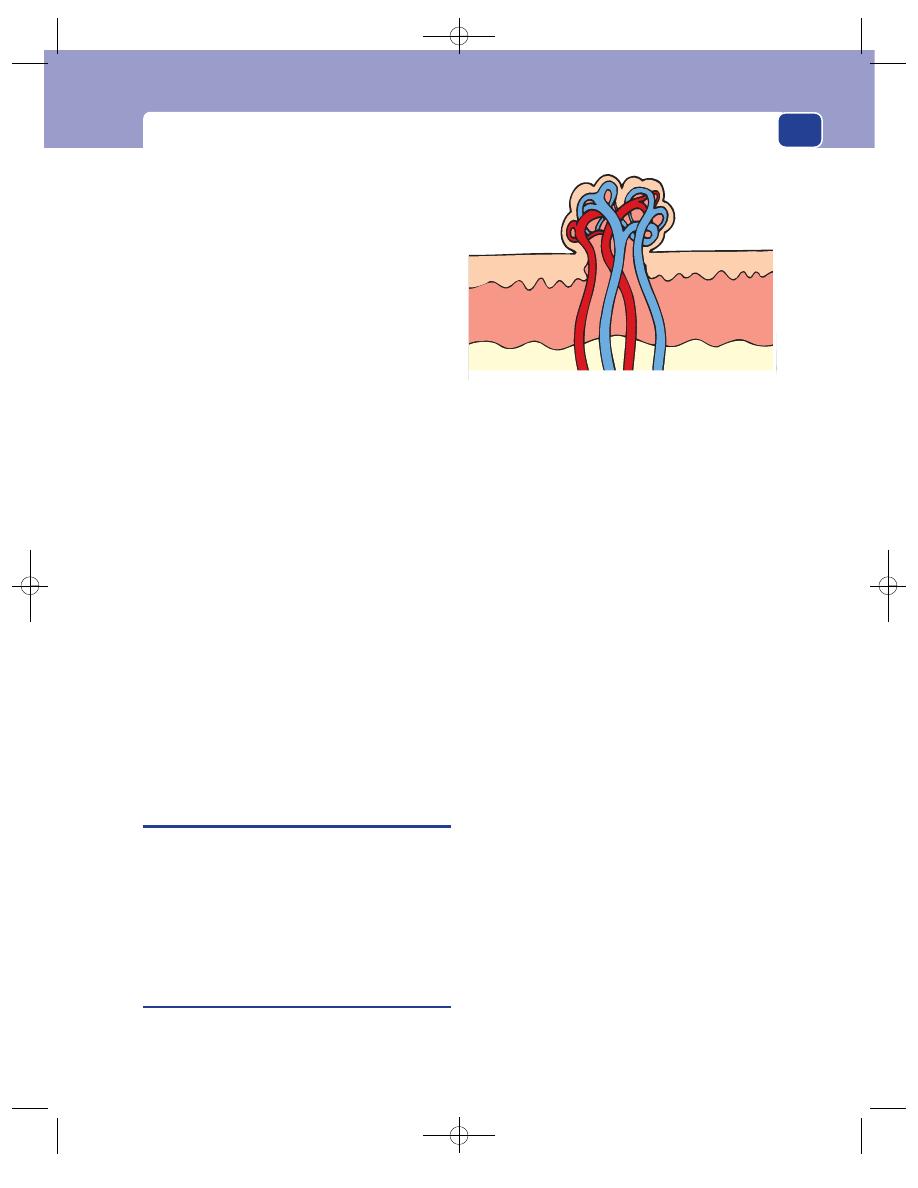
Haemangiomata/lymphangiomata
53
congenital dermoid cysts occur in the head and
neck. Parents may also be concerned about the diag-
nosis. Dermoid cysts rarely become large enough to
cause any serious mechanical disability and rarely
become infected.
Multiplicity
Congenital dermoid cysts are not usually
multiple.
Examination
Site
Congenital dermoid cysts are formed in intra-
uterine life when the skin dermatomes fuse. They
therefore occur at any point in the mid-line of the
trunk, but are particularly common in the neck and
face, along the lines of fusion of the ophthalmic and
maxillary facial processes, and at the inner and outer
ends of the upper eyebrow.
Shape and size
They are usually ovoid or spherical
and 1–2 cm in diameter.
Surface
Their surface is smooth.
Composition
Cysts on the face often feel soft, not tense
and hard. They fluctuate, but will only transillumi-
nate if they happen to contain clear fluid, instead of
the usual thick, opaque mixture of sebum, sweat and
desquamated epithelial cells. Large cysts conduct a
fluid thrill and are dull to percussion. They are not
pulsatile, compressible or reducible.
Relations
Dermoid cysts lie deep to the skin, in the
subcutaneous tissue. Unlike sebaceous cysts, they
are not attached to the skin – or to the underlying
structures.
HAEMANGIOMATA/LYMPHANGIOMATA
(See also Chapter 7)
There are many forms of cutaneous haemangioma,
such as strawberry naevus, port-wine stain, spider
naevus, vin rosé patch, and Campbell de Morgan
spot. All are various shades of pink or red but each
one has distinctive features. Once you have seen
these lesions, you will always be able to recognize
them. Many blanch on pressure.
Strawberry naevus
The name is an accurate description because this
bright-red ‘tumour’, which sticks out from the surface
of the skin, looks just like a strawberry. The term
‘naevus’ is correctly used because strawberry naevi
are present at birth. They are congenital intradermal
haemangiomata.
History
Age
Strawberry naevi are present at birth.
Sex
They are equally distributed.
Duration
They often regress spontaneously, a few
months or years after birth.
Symptoms
The child is almost always brought to the
clinic by its parent because the red lump is disfigur-
ing or a nuisance. Naevi that are rubbed or knocked
may ulcerate and bleed. When they are on the but-
tocks they get wet and infected. More than one straw-
berry naevus may be present.
Examination
Site
Strawberry naevi can occur on any part of the
body but are most common on the head and neck.
Shape and size
They protrude from the skin surface.
Small naevi are sessile hemispheres, but as they grow
they can become pedunculated.
Strawberry naevi are usually 1–2 cm in diameter,
but they can become quite large (5–10 cm).
Surface
Their surface is irregular, but covered with a
smooth, pitted epithelium. There may be small areas
of ulceration covered with scabs.
Colour
They are either bright or dark red.
Consistence
The strawberry naevus is soft and
compressible but not pulsatile. Gentle sustained
FIG 3.8
A strawberry naevus is an intradermal and subdermal
collection of dilated blood vessels.
Chap-03.qxd 4/19/05 13:42PM Page 53
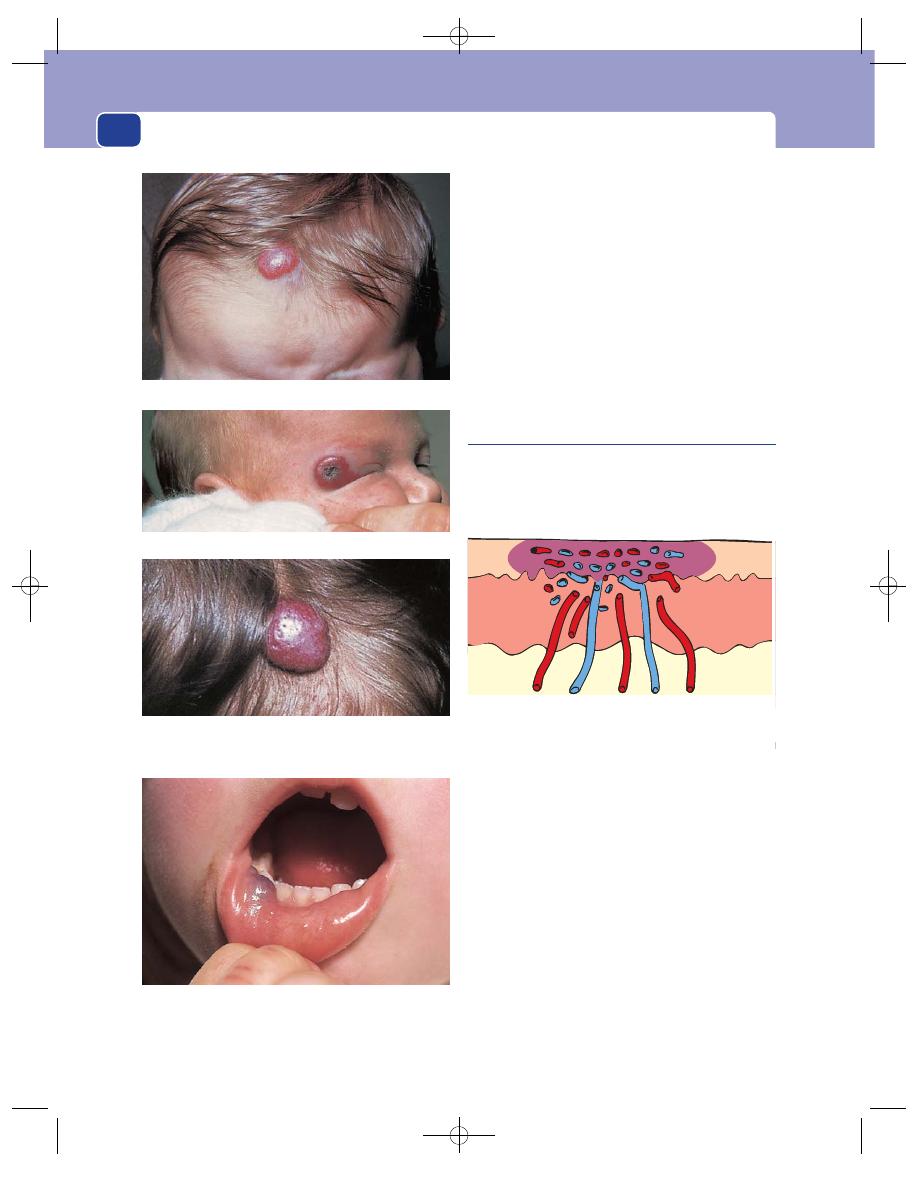
The skin and subcutaneous tissues
54
pressure squeezes most of the blood out of the
‘tumour’, leaving it collapsed, crinkled and colour-
less. The rate of refilling depends upon the number
of feeding arteries.
Relations
They are confined to the skin and are freely
mobile over the deep tissues.
Lymph drainage
The regional lymph glands should not
be enlarged.
Surrounding tissues
The blood supply of the sur-
rounding skin is absolutely normal. This congenital
condition is not associated with any other congeni-
tal vascular abnormality.
Port-wine stain
This is an extensive intradermal haemangioma,
which is mostly made up of small venules and cap-
illaries. It discolours the skin, giving it a deep purple-
red colour; hence its name.
History
Age
Port-wine stains are present at birth and there-
after do not change in size relative to the size of the
rest of the body, but their colour may alter.
Symptoms
The distress these stains cause the patient’s
parents and the subsequent disfigurement noticed
by the patient are entirely related to their colour and
position. As they are often on the face, they are very
noticeable. Occasionally, small vessels within the
stain become prominent and bleed.
The port-wine stain may be part of a more exten-
sive vascular deformity.
Examination
Site
Port-wine stains are common on the face and
at the junctions between the limbs and the trunk,
A haemangioma on the inside of the lower lip. These lesions
are similar to strawberry naevi of the skin but are smooth
and usually dark purple in colour.
FIG 3.9
HAEMANGIOMATA.
FIG 3.10
A port-wine stain is a collection of dilated venules
and capillaries just below the epidermis.
A large sessile strawberry naevus on the forehead.
A regressing cavernous haemangioma.
A close-up view of a strawberry naevus on the forehead
showing the smooth epithelial covering and little pits which,
with the red colour, make the lesion look like a strawberry.
Chap-03.qxd 4/19/05 13:42PM Page 54
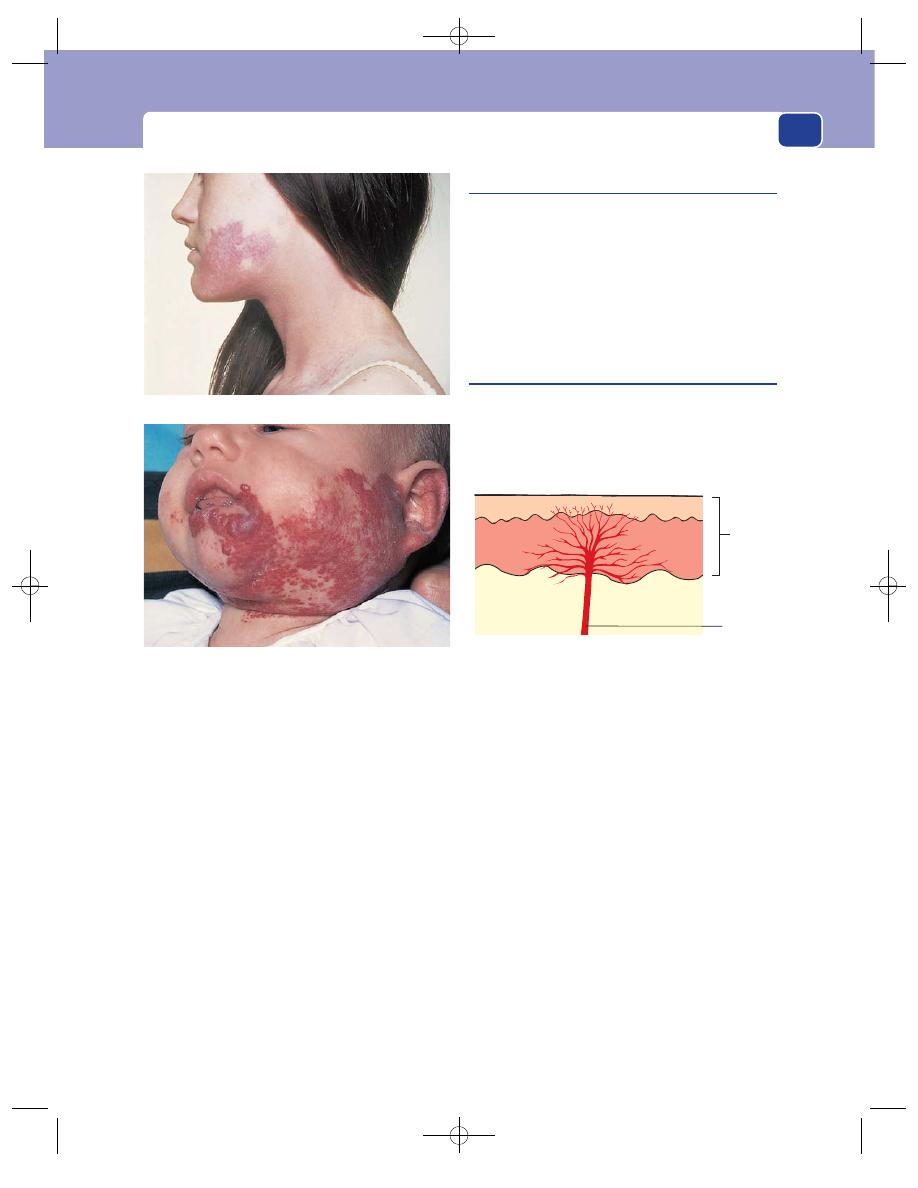
Haemangiomata/lymphangiomata
55
i.e. the shoulders, neck and buttocks. Sometimes
they seem to be confined to a single dermatome,
especially when they are part of a generalized vascu-
lar deformity, but there are never any associated
neurological abnormalities.
Shape and size
Both are very variable.
Surface
This is usually smooth, but vessels can be
prominent and many bleed.
Colour
Their distinctive feature is their deep purple-
red colour. There may be paler areas at the edge of
the patch. The colour can be diminished by local
pressure, but pressure rarely returns the skin to its
normal colour because all the blood vessels within
the patch are abnormal.
Surrounding tissues
There may be some dilated sub-
cutaneous veins beneath and around the lesion. The
sensory innervation of the stain is normal.
Venous angiomata
Venous angiomata are usually situated in the deeper
levels of the subcutaneous tissues and can extend
into muscles or joints (see Chapter 7), but there are
usually some distended veins in the skin over the
surface of the subcutaneous soft mass. These veins
are usually irregularly aranged but empty with pres-
sure. It is always wise to listen for a bruit, see below.
Spider naevi
A spider naevus consists of a solitary dilated skin arte-
riole feeding a number of small branches which leave
it in a radial manner. It is an acquired condition and
may be associated with a generalized disease.
History
Spider naevi are not noticed by the patient except
when they are in a prominent position on the face.
They cause no symptoms. They are multiple and
tend to increase in number over the years. It is impor-
tant to enquire about the patient’s consumption of
alcohol because they may be associated with chronic
liver disease.
Examination
Site
Spider naevi appear on the upper half of the
trunk, the face and the arms. It has been observed that
this is the area of drainage of the superior vena cava,
but it is doubtful if this is a significant observation.
Shape and size
It looks like a little red spider. The cen-
tral arteriole is 0.5–1.0 mm in diameter. The radiat-
ing vessels spread for a varying distance, usually
1–2 mm.
Skin
Arteriole
FIG 3.12
A spider naevus is a solitary dilated arteriole with
visible radiating branches.
An extensive port-wine stain of the lower face and neck.
A mixture of strawberry and port-wine-stain naevi of the face,
which is beginning to regress.
FIG 3.11
HAEMANGIOMATA.
Chap-03.qxd 4/19/05 13:42PM Page 55
The skin and subcutaneous tissues
56
Colour
The central arteriole is bright red and the
vessels radiating from it are of a similar colour but
not so red or so noticeable.
Temperature
Spider naevi do not cause a change of
skin temperature and are not tender.
Compressibility
Spider naevi fade completely when
compressed with the finger or, preferably, a glass
slide, and refill as soon as the pressure is released.
Compression of the central arteriole with the head
of a pin makes the radiating ‘legs’ fade.
Local tissues
There should be no other abnormalities
of the local circulation.
General examination
The general examination is
important because spider naevi may be associated
with serious diseases such as hepatic cirrhosis,
tumours destroying the liver, and oestrogen-
producing tumours.
Vin rosé patch
This is a congenital intradermal vascular abnormal-
ity in which mild dilatation of the vessels in the sub-
papillary dermal plexus gives the skin a pale-pink
colour. It is often associated with other vascular
abnormalities such as extensive haemangiomata,
giant limbs caused by arteriovenous fistulae (see
Chapter 7) and lymphoedema.
A vin rosé patch can occur anywhere and causes
no symptoms. It is not dark enough to be disfigur-
ing and the patient has commonly accepted its pres-
ence as a minor birthmark and forgotten about it.
Campbell de Morgan spot
This lesion is a bright-red, clearly defined spot caused
by a collection of dilated capillaries fed by a single
or small cluster of arterioles. The cause of these spots
is unknown and they are not associated with any
other disease.
History
Age
Campbell de Morgan spots increase in number
with age. They are uncommon in people under the
age of 45 years.
Duration
They appear suddenly, usually one at a time,
but sometimes a cluster of spots will appear in one
area of the skin.
Symptoms
They are not painful or tender, and not
disfiguring unless they are multiple and extensive.
Examination
Site
Campbell de Morgan spots appear on both
aspects of the trunk, more on the upper half than
the lower half. They occasionally appear on the
limbs and rarely on the face.
Shape and size
They are circular and have a sharp
edge, which is sometimes slightly raised. They vary
from 1 to 3 mm in diameter.
Colour
They have a uniform deep-red or purple
colour which makes them look like drops of dark-red
paint or sealing wax just under the epidermis. This
is their diagnostic feature.
Compressibility
Although they are a collection of
dilated capillaries, they do not always empty when
compressed, but always fade slightly.
Lymphangioma circumscriptum
This is a circumscribed cluster of many small dilated
lymph sacs in the skin and subcutaneous tissues
which do not connect into the normal lymph sys-
tem. The aetiology of these blind sacs is unex-
plained but, as they are congenital, it is likely that
they are clusters of lymph sacs that failed to join
into the lymph system during its development.
Large, translucent lymph cysts confined to the sub-
cutaneous tissues are called cystic hygromata (see
page 281).
History
Sex
Lymphangiomata are present at birth but may not
be noticed until the skin vesicles appear a few years
later. They are equally common in boys and girls.
Symptoms
They are usually noticed by the child’s
parents, who consult the doctor because they are
concerned about the ‘lump’ and the disfigurement it
causes. Occasionally, the skin vesicles contain clot-
ted blood, which turns them brown. Sometimes the
vesicles leak clear fluid. When very prominent, the
vesicles can be rubbed by clothes and may get
infected and painful.
Development
As the years pass, the subcutaneous
cysts enlarge and become prominent and the num-
ber and extent of the skin vesicles increases.
Chap-03.qxd 4/19/05 13:42PM Page 56
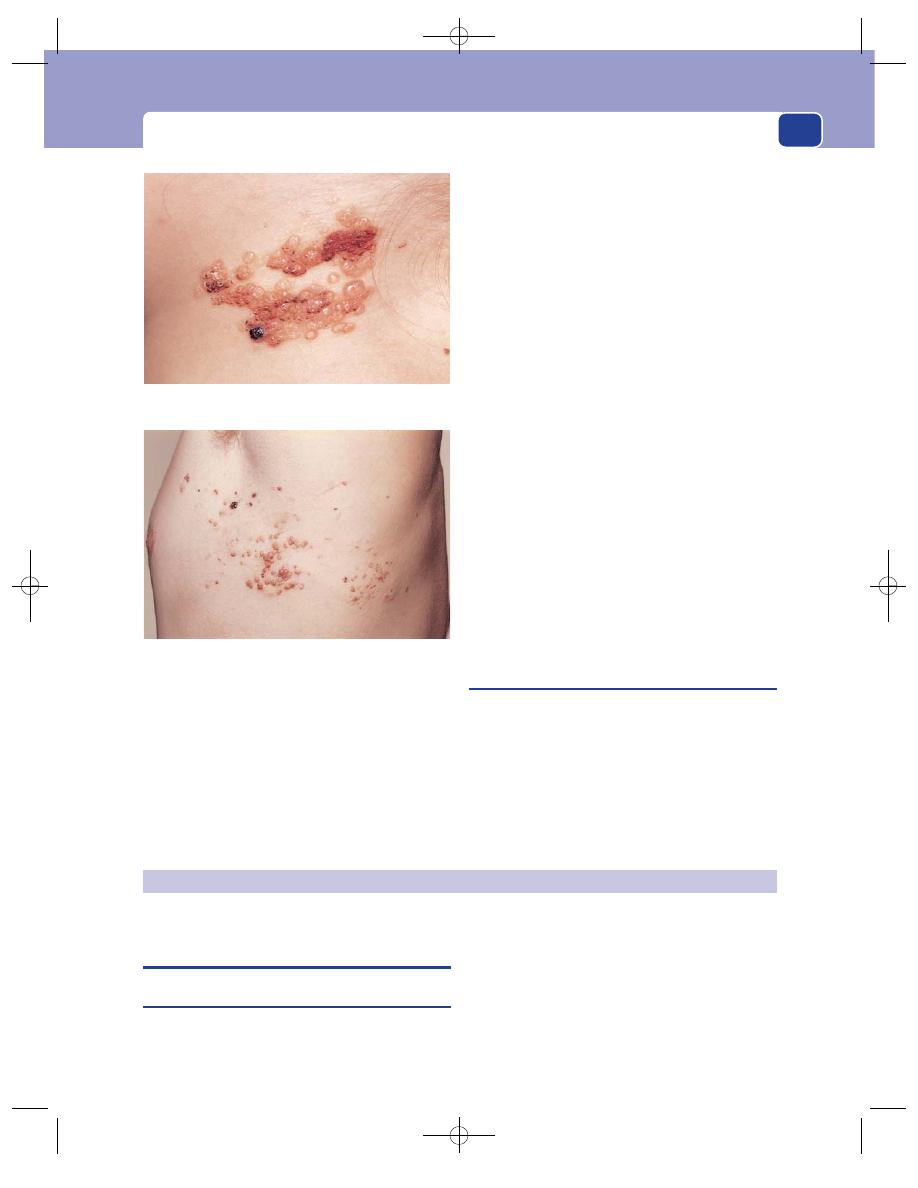
Conditions of the skin caused by trauma
57
Examination
Site
Lymphangiomata circumscriptum are found at
the junction of the limbs and the neck with the trunk,
i.e. around the shoulder, axilla, buttock and groin.
Shape and size
They may present as a single or mul-
tiple lumps.
A large area of skin may be involved – the whole
of the buttock or shoulder may be abnormal – but
most lymphangiomata are 5–20 cm across when
they present for treatment.
Surface
Their surface is smooth but their edge is
often ill-defined and indistinct.
Colour
The skin vesicles contain clear fluid which
looks watery or yellow. Blood in the vesicles turns
them red-brown or even black.
Overlying skin
The subcutaneous cysts make the abnor-
mal area bulge slightly, but the edges of this swelling
are indistinct. The skin contains vesicles of varying
sizes and colour, ranging from 0.5 to 3 or 4 mm in
diameter.
Composition
The whole lesion is soft and spongy. If the
swelling is composed of multiple cysts, it will not
fluctuate. If the swelling contains one or two large
cysts, fluctuation, a fluid thrill and translucence will
all be present.
The mass is not compressible. The dark-red or
brown vesicles do not fade with pressure.
Lymph drainage
The local lymph glands are usually
normal unless the cysts have been infected.
Arteriovenous fistulae
These may cause a swelling in the skin or subcutaneous
tissues, which may have a vascular appearance (see
Chapter 7). The veins are also often distended but care-
ful inspection may reveal pulsation, which is confined
by palpation. Arteriovenous fistulae are not compress-
ible but should have a loud machinery murmur situ-
ated over them providing that they have a high flow.
CONDITIONS OF THE SKIN CAUSED
BY TRAUMA
Keloid and hypertrophic scars
An incised wound heals in three stages. First, the
gap in the tissue is filled by blood and fibrin. This is
then replaced by collagen and fibrous tissue which
knit the tissues together. Finally, the fibrous tissue is
organized to give the wound its maximum strength.
This process, which is called healing by primary
intention, is remarkably well controlled. Most surgi-
cal scars in the skin are thin lines containing the min-
imum amount of scar tissue. Sometimes, however,
ACQUIRED DERMATOLOGICAL CONDITIONS
In this small, localized lesion, many of the vesicles are red,
black or brown because they contain old blood.
This extensive lesion spreads across the whole of the side of
the chest just below the axilla. The swelling deep to the
posterior part of the lesion is caused by the subcutaneous cysts.
FIG 3.13
LYMPHANGIOMATA CIRCUMSCRIPTUM.
Chap-03.qxd 4/19/05 13:42PM Page 57
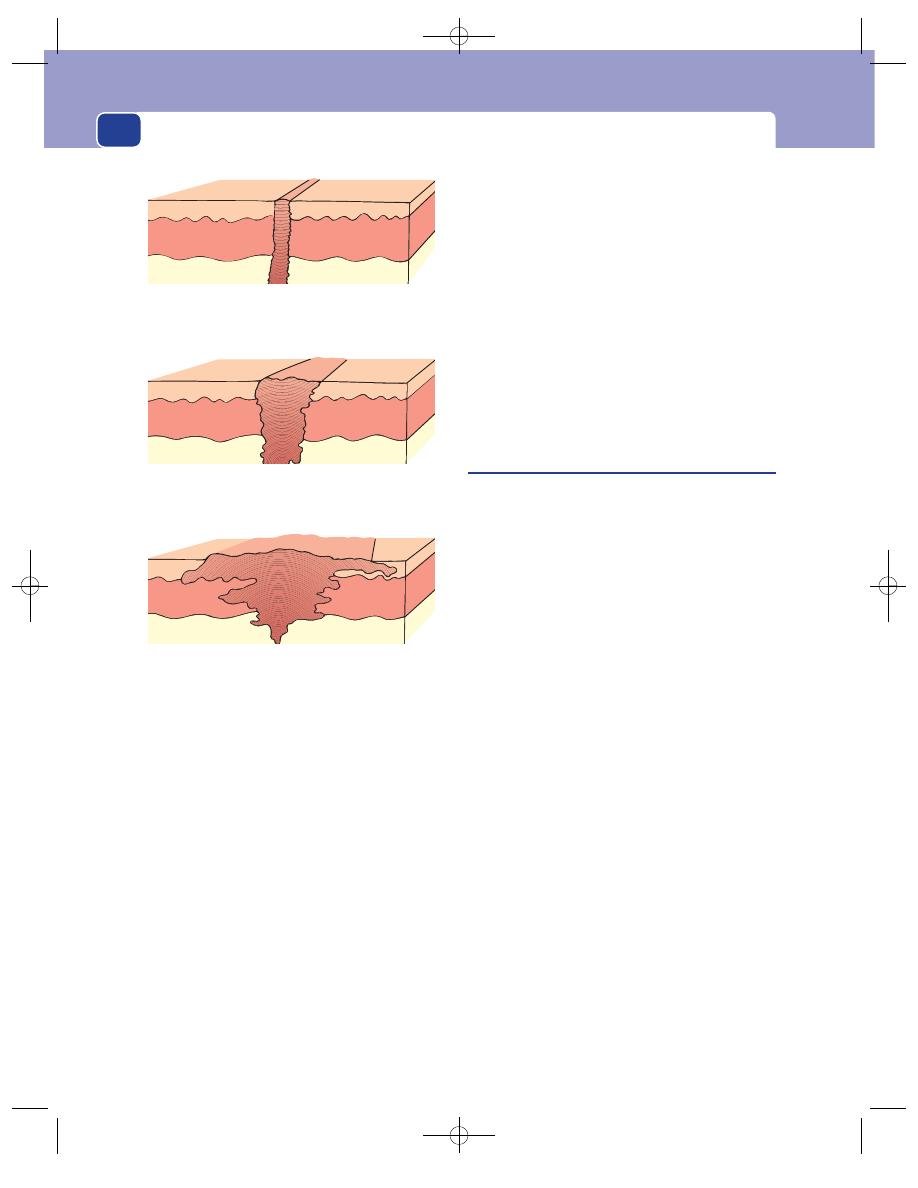
The skin and subcutaneous tissues
58
the fibrous tissue response is excessive and the result
is a hypertrophic or keloid scar.
In a hypertrophic scar there is an excessive
amount of fibrous tissue but it is confined to the
scar; i.e. it is between the skin edges. Hypertrophic
scars are quite common, particularly if there has
been some extra stimulus to fibrous tissue forma-
tion during healing, such as infection or excessive
tension, both of which are common complications
of scars crossing skin creases. Hypertrophic scars
only enlarge for 2–3 months.
In a keloid scar the hypertrophy and overgrowth
of the fibrous tissue extend beyond the original
wound into normal tissues. This means that the scar
has some of the characteristics of a locally malig-
nant neoplasm. The tendency to produce keloid
scars is a congenital trait, common in Negroes.
Some tribes exploit the trait for the production of
decorative scars on the face and trunk. Keloid scars
continue to enlarge for 6–12 months after the initial
injury. This is almost certainly the result of a local
release of fibroblast growth factors, which are
unsuppressed.
As a keloid scar grows, it can become exceedingly
unsightly, is often tender to the touch and may itch.
Although the cosmetic disfigurement of a hyper-
trophic scar may be as great as that of a keloid scar,
it is important to try to distinguish the two abnor-
malities because hypertrophic scars do not recur
after they have been excised if the causative factors
are eliminated, whereas keloid scars will recur unless
special measures are taken.
Callosities and corns
These conditions are known to everyone. They are
areas of skin thickening and hyperkeratosis second-
ary to pressure and repeated minor trauma (see also
Chapter 6). If the thickened skin is pushed inwards
by constant pressure, e.g. on the sole of the foot or
on the dorsum of the toes, it becomes painful and is
known as a corn. Corns and callosities often occur
over bunions and deformed toes.
History
Age
Corns and callosities are more common in the
elderly, not because their skin growth changes but
because changes of the skeleton cause redistribution
and maldistribution of weight bearing.
Symptoms
Callosities may get rubbed and sore but
are not usually painful. Corns are painful when
pressed, because they are narrow and deep and may
impinge upon deep structures.
Examination
A callosity is a raised, thickened patch of greyish-
brown hyperkeratotic skin over an area of excessive
wear and tear. Callosities are therefore common on
the hands and feet, and their site varies with the
patient’s occupation and skeletal structure.
As they exercise a protective function, they are
best left alone; but the diagnosis can be confirmed
by carefully paring away the top layer of roughened
skin to expose homogeneous, shiny, translucent lay-
ers of dead skin beneath.
A corn is a similar but smaller lesion that is
pushed into the skin, thus forming a palpable nodule
Normal scar
Hypertrophic scar
Keloid scar
FIG 3.14
Normal, hypertrophic and keloid scars.
Chap-03.qxd 4/19/05 13:42PM Page 58
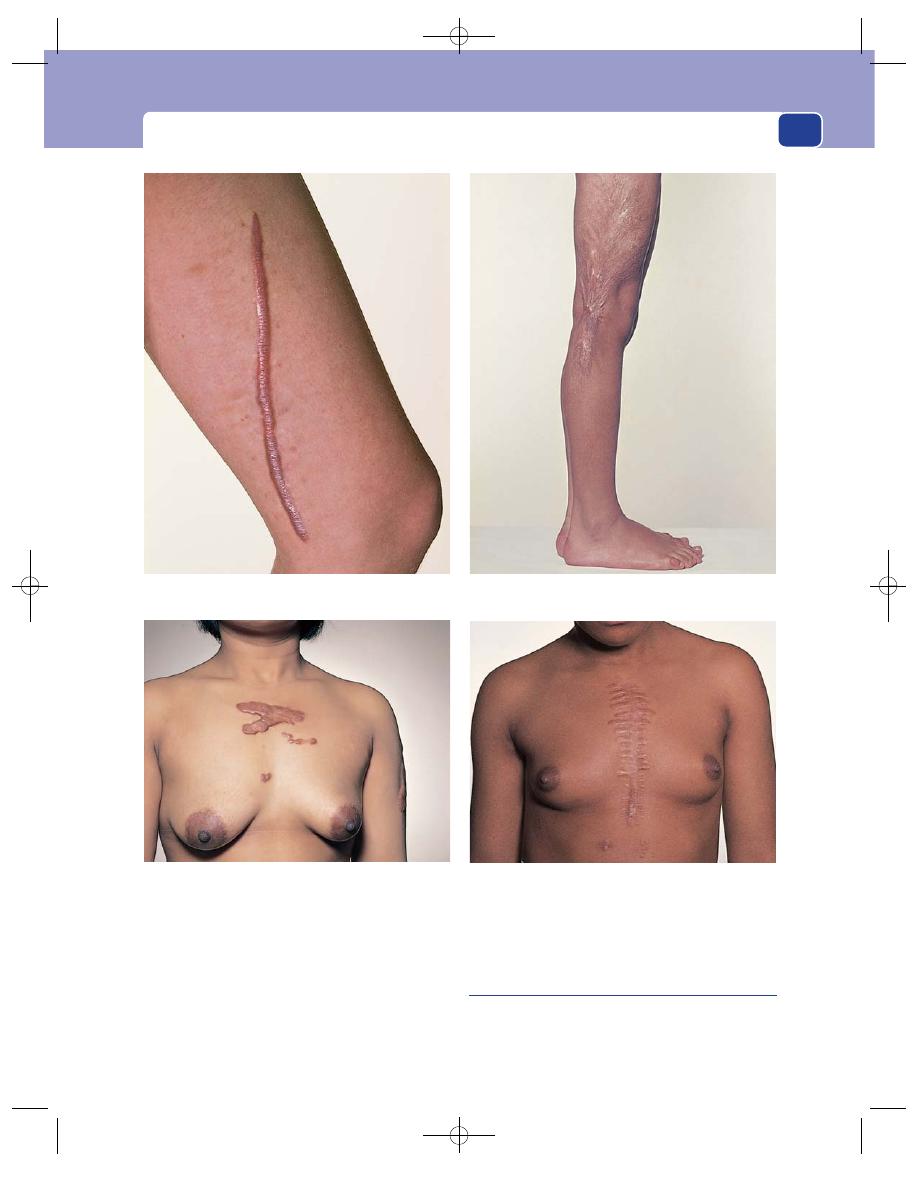
Conditions of the skin caused by trauma
59
with a central yellow-white core of dead cornified
epidermal cells. Corns are found on the soles of the
feet, the tips of the toes and over the dorsal surface of
the interphalangeal joints.
The main differential diagnosis is the plantar
wart (verruca). These two lesions can be distin-
guished by paring away the top layers of skin with a
knife to expose either the corn’s core of dead
translucent tissue, or the verruca’s soft filiform
processes.
Acquired implantation dermoid cysts
History
These cysts develop when a piece of skin survives
after being forcibly implanted into the subcutaneous
A hypertrophic scar on the medial side of the thigh following
the excision of a large lipoma.
Hypertrophic scars after a burn.
Keloid scars after tribal marking.
Keloid scars after a median sternotomy.
FIG 3.15
HYPERTROPHIC AND KELOID SCARS.
Chap-03.qxd 4/19/05 13:43PM Page 59
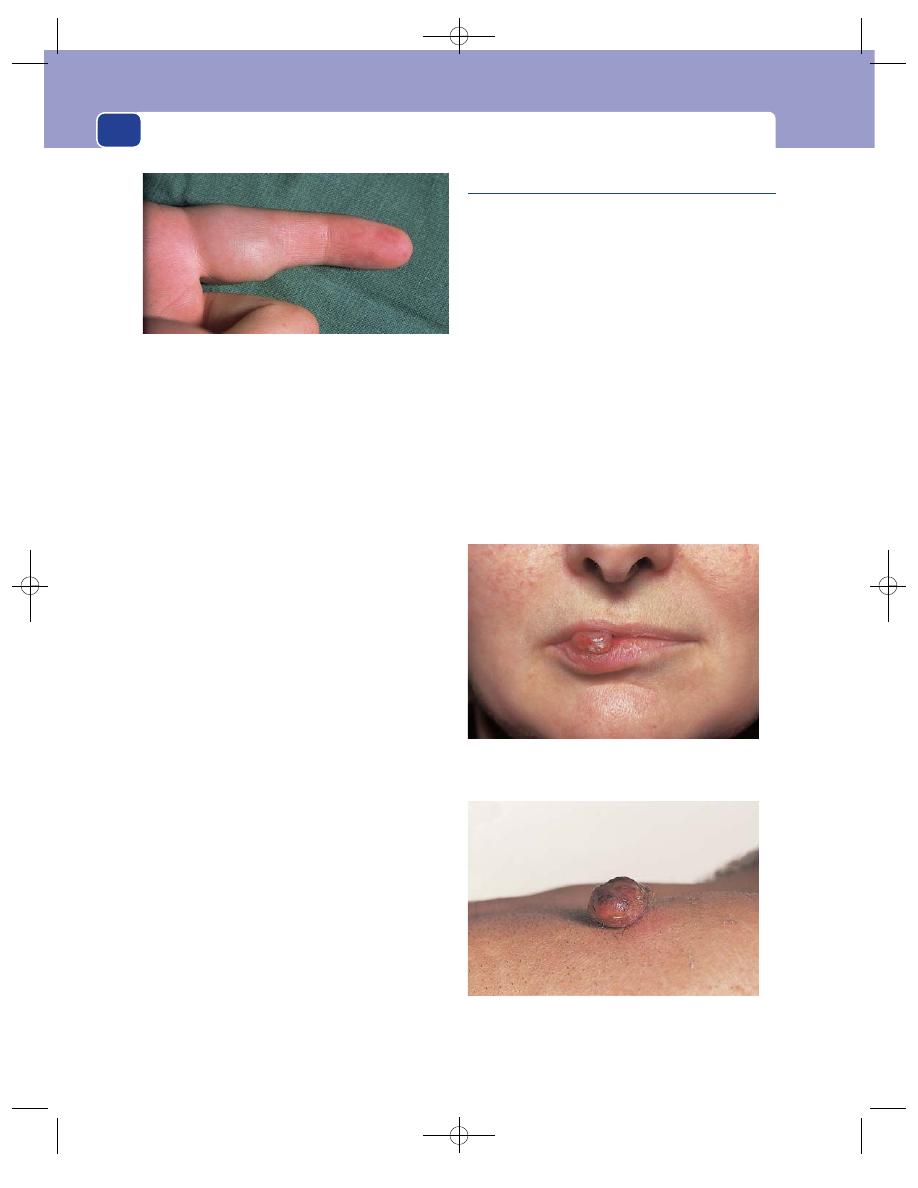
The skin and subcutaneous tissues
60
tissues by an injury – often a small, deep cut or stab.
The patient may not remember the initial injury.
Symptoms
Implantation dermoid cysts are usually
small and tense. They may be painful and tender
because they usually occur in areas subject to
repeated trauma. Cysts on the fingers may interfere
with the grip and touch.
Examination
Site
Implantation dermoid cysts are commonly
found beneath skin liable to be injured, such as that
of the fingers. Surprisingly, surgical incisions rarely
cause these cysts.
Shape and size
The cysts are spherical, smooth and
small, about 0.5–1.0 cm in diameter.
Composition
Implantation dermoid cysts feel hard and
tense, sometimes stony hard. Their small size makes
detection of their cystic nature – fluctuation and
fluid thrill – almost impossible. The deduction that
they are cystic usually depends solely on their shape.
Relations
The overlying skin is often scarred. The
cyst may be tethered to the deep aspect of the scar or
even be within it. The deeper structures should be
normal and the cyst freely mobile over them unless
they were involved in the initial injury.
Lymph drainage
The regional lymph glands should be
normal.
Complications
Implantation dermoid cysts rarely
become infected.
Differential diagnosis
The sebaceous cyst is commonly
confused with the implantation dermoid cyst. The
history of an old injury and the presence of a scar
closely related to the cyst are the most significant
diagnostic features.
Pyogenic granuloma
Small capillary loops develop in a healing wound to
knit it together and provide sustenance and support
for the covering epithelium. In the base of a healing
ulcer these capillary loops form a layer of bright-red
tissue known as granulation tissue. When the capil-
lary loops grow too vigorously, they may form a pro-
truding mass of tissue which becomes covered with
epithelium. It is called a pyogenic granuloma because
its surface is often ulcerated and infected, but it is
probably neither pyogenic nor granulomatous. The
infection is a secondary event and probably not the
initiating stimulus. They are simply rapidly growing,
sessile or pedunculated clusters of capillaries that
become covered with epithelium.
History
Age
Pyogenic granulomata are uncommon in
children.
FIG 3.16
An implantation dermoid cyst that appeared 2 years
after a small stab wound at the base of the finger.
A pyogenic granuloma on the lip. This lump grew in 6 days
following a minor injury to the lip. By the time this photograph
was taken, the lump was covered with epithelium.
A pyogenic granuloma on the skin of the chest that
appeared 4 days after a deep scratch.
FIG 3.17
PYOGENIC GRANULOMATA.
Chap-03.qxd 4/19/05 13:43PM Page 60
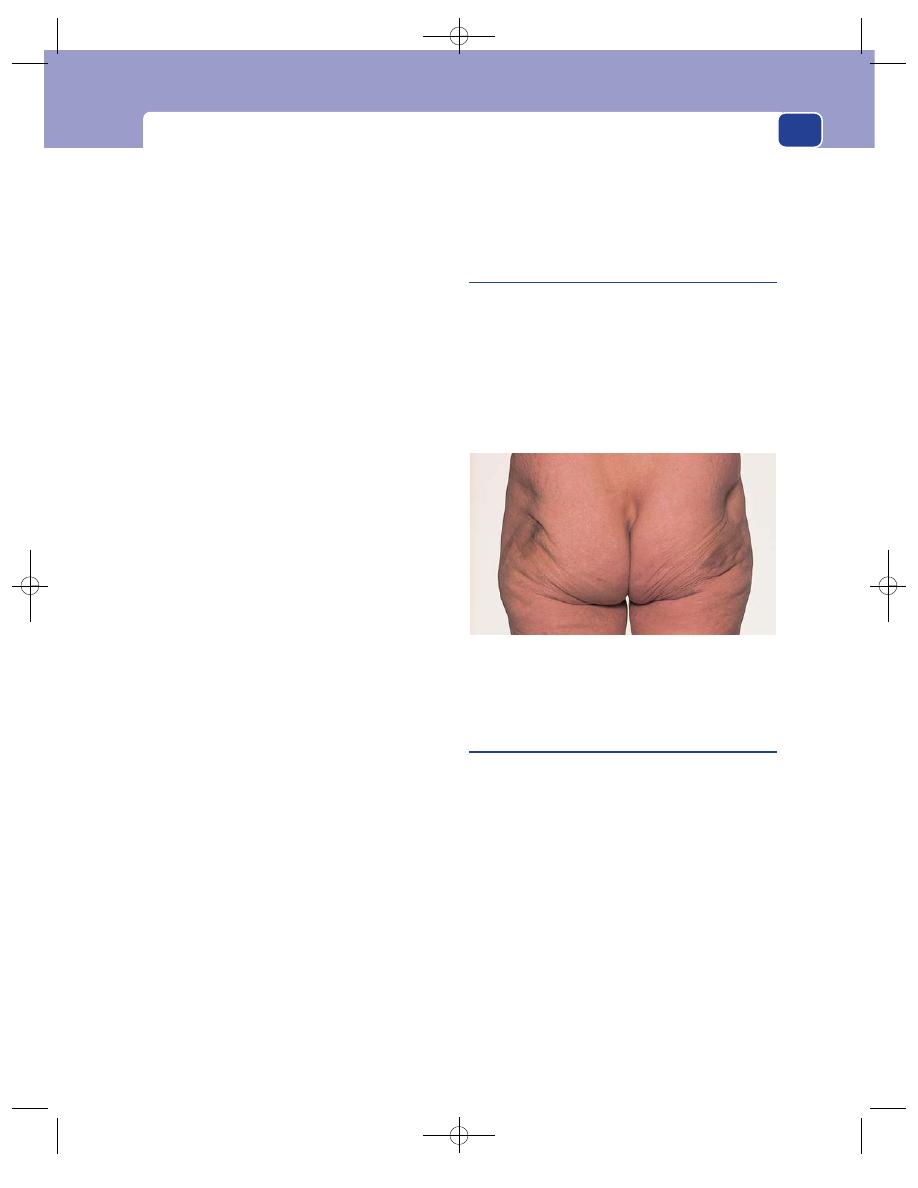
Conditions of the skin caused by trauma
61
Symptoms
There may be a history of a minor injury,
usually a cut or scratch, but the patient cannot always
remember the initial injury. Pyogenic granulomata
sometimes occur in response to a chronic infection
such as occurs in a paronychia.
The patient complains of a rapidly growing lump
on the skin, which bleeds easily and discharges a
serous or purulent fluid. So rapid is the growth of
the lump (it may double in size in a few days) that
most patients think it is a tumour. When it is com-
pletely covered with epithelium, the bleeding, weep-
ing and pain stop.
Examination
Site
Pyogenic granulomata are most common on
those parts of the body likely to be injured, such as
the hands and face.
Shape and size
They begin as a hemispherical nodule
which grows upwards and outwards. The lump is
rarely more than 1 cm across because beyond this size
the blood supply becomes inadequate. Growth from
a few millimetres to full size can occur in a few days.
Surface
Before the surface is epithelialized, it has a
covering of dried blood or plasma. It may bleed
when rubbed.
Colour
At first they have the bright-red colour of
healthy granulation tissue, but as they get bigger
and less vascular they fade to a pale pink. When they
become covered with epithelium, they turn pink or
white.
Tenderness
Although they are not painful, they are
sometimes slightly tender.
Composition
Pyogenic granulomata are soft.
Relations
They are usually confined to the skin.
Complications
They bleed easily when knocked. Very
rough handling may break a pyogenic granuloma
off at its base. The base rarely bleeds very much. The
granuloma may reform in the next few days, or the
bare area epithelialize normally.
Natural history
Once the granulations have become
completely covered with epithelium, the nodule
begins to shrink, but it rarely goes completely.
Differential diagnosis
The important conditions to
exclude are squamous carcinoma, non-pigmented
melanoma and, in some parts of the world, Kaposi’s
sarcoma. A history of trauma and the very rapid
growth are the peculiar features of a pyogenic gran-
uloma, but an excisional biopsy is often needed to
confirm the diagnosis.
Fat necrosis
Necrotic fat becomes hard and fibrous. If the necrotic
mass of fat is close to the skin, the skin becomes
tethered or fixed to it and in-drawn.
In the breast, which is an organ that is frequently
knocked and bruised, fat necrosis may be mistaken
for a carcinoma. The buttock is also a common site
of fat necrosis, particularly in patients who have fre-
quent subcutaneous injections, such as diabetics.
Ulcers
An ulcer is a solution of the continuity of an epithelial
surface. Ulcers follow traumatic removal, or death
and desquamation by disease, of the whole or part
of an epithelium, and most occur in the lower limb.
Ulcers are discussed in this section on trauma
because trauma is often the final cause of the skin
breakdown, although there are many underlying
causes that make the skin susceptible to injury and
impede subsequent healing.
The features of an ulcer that must be examined
and recorded are as follows.
The edge
The edge of an ulcer is the most important feature
because it is the junction between healthy and
diseased tissue and takes a characteristic form
FIG 3.18
Fat necrosis of the buttock fat caused by repeated
injections of insulin. Note the tethering, indrawing and
pigmentation of the skin. Beneath these areas were hard,
indistinct lumps of necrotic fat.
Chap-03.qxd 4/19/05 13:43PM Page 61
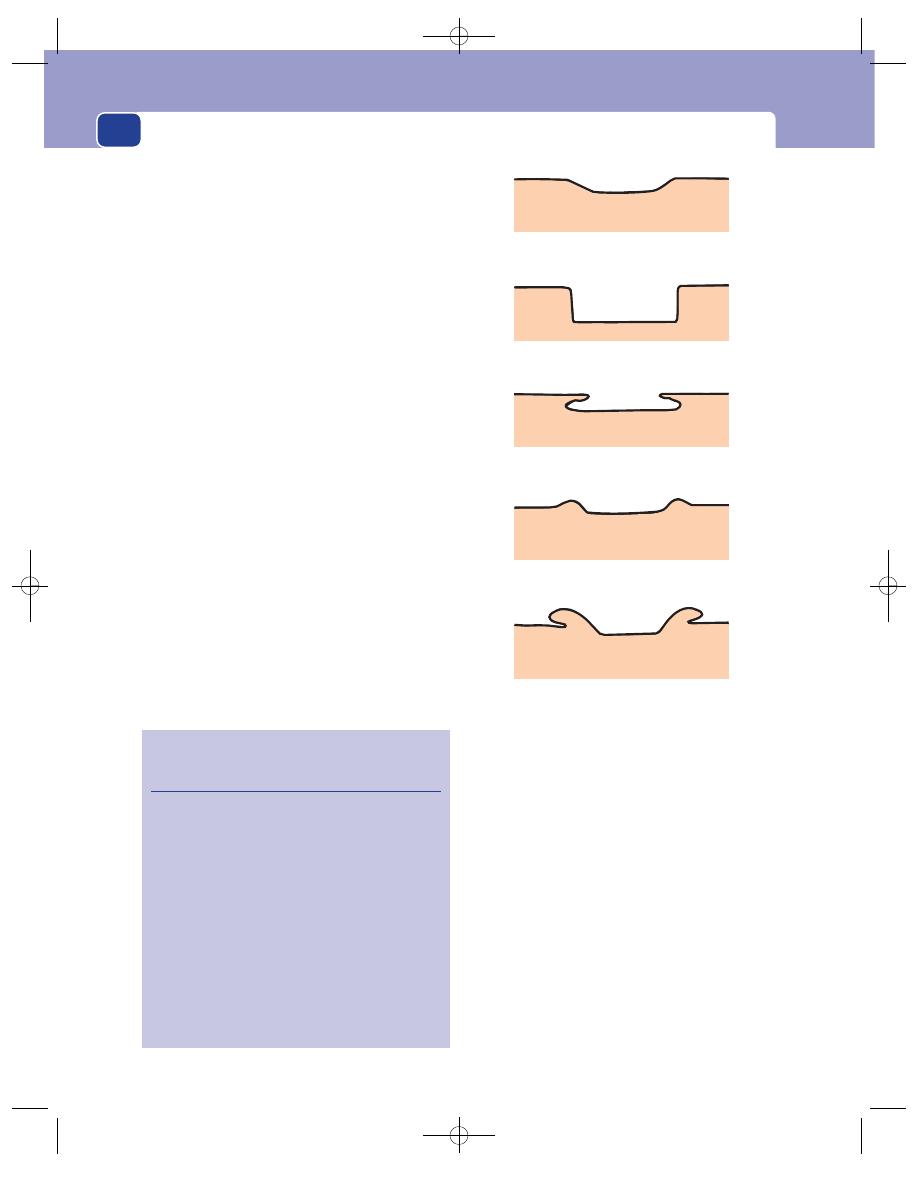
The skin and subcutaneous tissues
62
according to the underlying disease. There are five
common types of ulcer edge (Fig. 3.19).
Sloping edge
The edge slopes gently from the nor-
mal skin to the base of the ulcer. It is pale pink and
consists of new, healthy epithelium growing in over
the base of the ulcer. Healing ulcers have a sloping
edge. The best examples are healing, traumatic and
ischaemic venous ulcers.
Punched-out edge
This edge drops down at right-
angles to the skin surface to make the ulcer look as if
it has been cut out of the skin with a punch. It indi-
cates a localized, usually full-thickness, area of skin
loss surrounded by healthy tissue. The best exam-
ples of this type of ulcer are the deep trophic ulcer
and the ulcer left after a patch of gangrenous skin
has sloughed. The condition causing the ulcer is lim-
ited to the ulcer and much less severe in the sur-
rounding tissues, but sufficient to prevent healing.
Ischaemic and syphilitic ulcers have this type of edge.
Undermined edge
The disease causing this type of
ulcer spreads in and destroys the subcutaneous
tissues faster than it destroys the overlying skin. The
overhanging skin is usually reddish-blue, friable
and unhealthy. Tuberculous ulcers are usually
undermined.
Rolled edge
A rolled ulcer edge develops when an
invasive cellular disease becomes necrotic at its cen-
tre but grows quite quickly at its periphery, so that it
rises above the surface of the skin. A rolled-edge
ulcer is typical of a basal cell carcinoma. ‘Rolled’ is a
poor description, but it is the best we have. The edge
of this type of ulcer looks like the circular mound of
earth found around an ancient fortification.
Everted edge
When an ulcer is caused by a fast-
growing infiltrating cellular disease, the growing
portion at the edge of the ulcer heaps up and, in its
malignant exuberance, spills over the normal skin to
produce an everted edge. This appearance is typical
of the squamous cell carcinoma and the ulcerated
adenocarcinoma.
The base
The base of the ulcer should be examined carefully.
It may be necessary to remove the slough before this
can be done.
Sloping edge
Punched-out edge
Undermined edge
Rolled edge
Everted edge
FIG 3.19
The five types of ulcer edge.
Revision panel 3.4
Causes of ulceration of the skin of the
lower limb
Venous
60% (half varicose and
half post-thrombotic)
Ischaemia
20% (one-quarter have
an associated venous
cause)
Collagen disease
5% (rheumatoid and
systemic lupus
erythematosus)
Neuropathic 2%
Traumatic 1%
Neoplastic
1%
Many rare causes
5%
Unknown
10%
Chap-03.qxd 4/19/05 13:43PM Page 62
Conditions of the skin caused by trauma
63
The base is likely to consist of three types of tissue.
Granulation tissue
This is a red sheet of delicate cap-
illary loops and fibroblasts covered by a thin layer of
fibrin or plasma. It is the first stage of the healing
process.
Dead tissue
This is called a slough. When a slough
separates, it may expose healthy tissues, which then
become covered with granulation tissue or tissue
becoming involved in the ischaemic process.
Tumour
The base of a squamous cell carcinoma is the
malignant tissue itself. It may be slightly vascular or
necrotic but does not develop healthy granulation
tissue.
Discharge
The discharge from an ulcer may be serous or sero-
sanguinous, purulent, offensive, copious, or so slight
that it dries into a scab. It should be cultured to ascer-
tain the nature of any infecting organisms.
Venous ulcers
Venous ulcers are found in the lower medial third of
the lower limb. Their site is a diagnostic feature. They
are described in detail in Chapter 7.
Ischaemic ulcers
Arterial insufficiency is usually manifest at the
ends of the limbs. It is rare to see ulcers caused by
arterial disease at the base of the limbs or on the
trunk. Ischaemic ulcers are described in detail in
Chapter 7.
Trophic ulcers
A trophic ulcer is an ulcer which has developed as
the result of the patient’s insensitivity to repeated
trauma. These ulcers are commonly associated with
those forms of neurological disease which cause loss
of the appreciation of pain and light touch in weight-
bearing areas (see Chapter 7).
Neoplastic ulcers
The ulcers caused by basal and squamous cell carci-
nomata are described in detail later in this chapter.
When metastases from distant or underlying
cancers appear in the skin, they may ulcerate and
have features similar to those of a primary carcino-
matous ulcer – an everted edge and a proliferating
base.
Burns
The skin can be burnt by heat, irradiation, electrical
or chemical noxious stimuli. A ‘heat’ burn is usually
caused by direct flames, an explosion, contact with a
hot object, steam or hot fluid. Burns caused by
steam or hot water are called scalds. Most burns are
the result of accidental household injuries, but pre-
viously rare causes such as self-immolation and tor-
ture are becoming more common.
Prophylaxis
The fitting of household fire alarms
and the use of non-flammable fabrics and fittings
and sprinkler systems are all designed to try to
reduce the incidence of household and place of
work burns. Poor electrical wiring and gas leaks are
potentially avoidable but continue to be a common
cause of major burn injuries. Children and the eld-
erly are particularly at risk: the young fail to recog-
nize the hazard and the elderly are often unable to
avoid it as a consequence of immobility and frailty.
Education and safeguards are the best form of
defence in these age groups.
First-aid
Wherever possible, burnt parts should be
immersed in cold water. This is easy after a scald of
the hand but impractical if the whole body has been
burnt. Chemicals should be washed off, and hot and
damaged clothing removed.
Assessment and resuscitation
As in a major injury,
these two must proceed simultaneously. Intravenous
access and fluid replacement are essential in any
patient who has a sizeable burn, and cannulae
should be placed in large veins in an area of unburnt
skin. The size and depth of the burn must be care-
fully assessed. The burn size is measured as a per-
centage of total body area using the ‘Rule of nines’
(see Fig. 3.20). For a child, this must be modified –
the head and neck being scored as 18 per cent and
the lower limbs downgraded from 18 per cent to
12 per cent.
The depth of a burn used to be subdivided into
six degrees, but nowadays the depth is usually cate-
gorized as being partial or full thickness.
Partial-thickness burns are further subdivided
into superficial and deep dermal burns. The former
are often blistered and very painful, while the latter
are often pale with decreased sensation.
Full-thickness burns usually have subcutaneous
fat visible in their base and are insensate.
Chap-03.qxd 4/19/05 13:43PM Page 63
The skin and subcutaneous tissues
64
A number of formulae exist for the calculation of
the patient’s early fluid requirement based on the
extent and depth of the burn and the patient’s age.
These are beyond the scope of this book but it must
be stressed that early and adequate fluid replace-
ment is the most important initial treatment.
Clinical features
Pain
The main problem is pain, especially in
patients with superficial burns.
Skin sensation
Sensation must be carefully tested
whenever a full-thickness burn is suspected, and
re-tested 24 hours later, when it may be easier to
determine.
The airway
It is important to assess the face, mouth
and airways, as inhalation injury of their lining
commonly accompanies extensive burns. Burns
around the mouth, nose and lips should provide a
high index of suspicion. The buccal mucous mem-
brane and tongue must be inspected for mucosal
burns.
Breathing
Special attention must be paid to any cir-
cumferential burns of the neck or chest, as these
may constrict breathing. The occurrence of stridor
or a difficulty with breathing is an indication for
intra-tracheal intubation and ventilation, especially
if the patient is unconscious.
Circulation
In addition to monitoring the airways,
the state of the circulation must be repeatedly
assessed, as burns are associated with massive losses
of electrolytes and protein from their surface, and
red cell damage or destruction.
The pulse, blood pressure, central venous pres-
sure, urine output and haematocrit must be carefully
18%
18%
4.5%
Anterior surface
Posterior surface
1%
9%
9%
9%
9%
4.5%
4.5%
4.5%
4.5%
4.5%
FIG 3.20
The ‘Rule of nines’ method for calculating the proportion of the body surface that has been burnt, viz. 9% for the
head, 9% for each arm, 18% for each leg, 18% for the front and 18% for the back of the trunk.
Chap-03.qxd 4/19/05 13:43PM Page 64
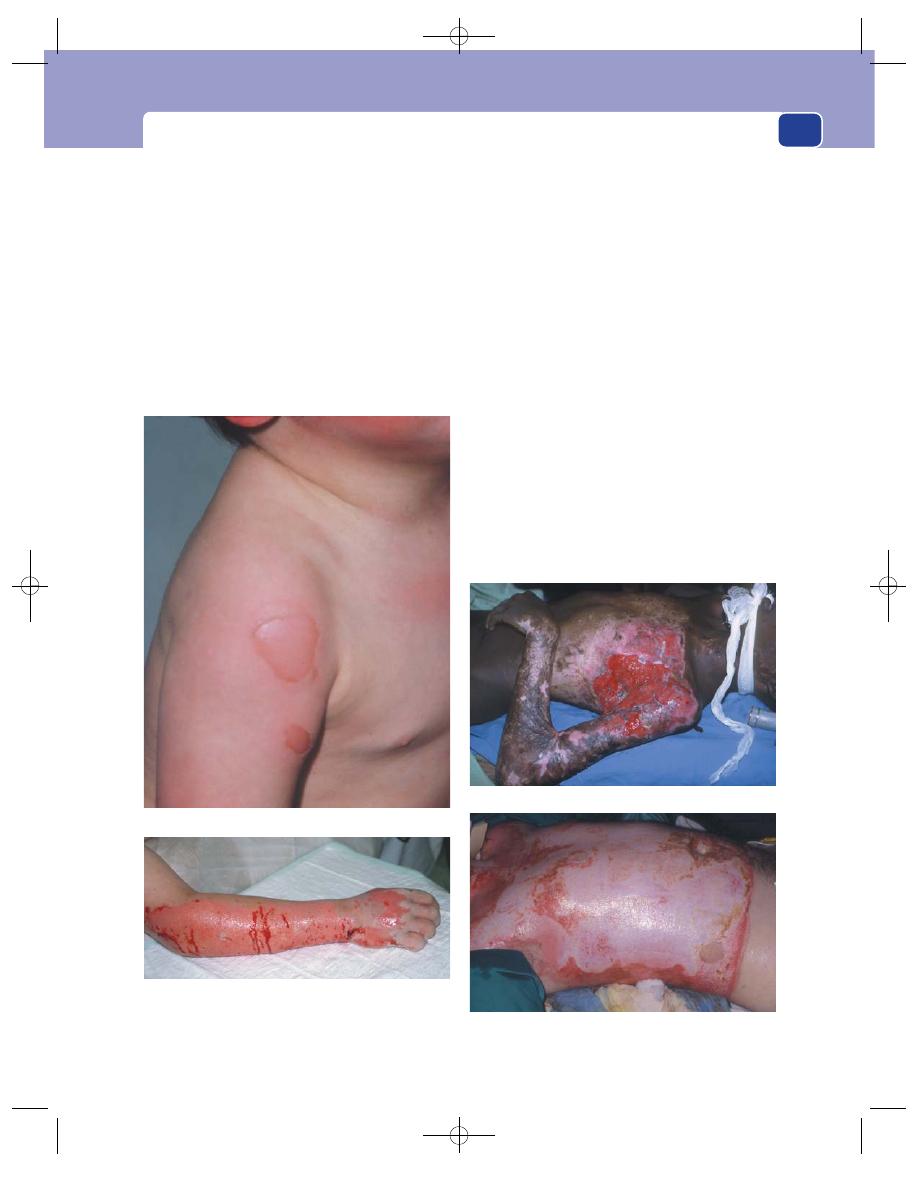
Conditions of the skin caused by trauma
65
monitored in all patients with major burns. Failure
to maintain an adequate circulation may be fol-
lowed by renal failure and eventually multi-organ
failure. The latter is the complication that often fol-
lows septicaemia from secondary infection in and
around the burns.
Circumferential burns of the limbs or digits may
cause peripheral ischaemia.
Depigmentation
This is a rare problem that can
occur in black races after extensive scarring and
burns.
Electrical burns
Most electrical burns come from faulty home
appliances or the careless touching of electrodes.
High-voltage burns, such as lightening strikes, with
subsequent survival are uncommon because the
depolarization usually causes severe cardiac arrhyth-
mias and cardiac arrest.
A severe local burn develops at the point of
entry, and adjacent nerves and muscles are often
damaged. Deep tissue damage can lead to metabolic
derangements, compartment syndromes, arterial
and venous thrombosis and even visceral damage if
the entry point is over the torso.
Radiation injury
The initial skin injury caused by radiation often
resembles a standard thermal burn. The clinical evi-
dence of the commonly associated lung and bowel
damage and bone marrow depression appears later.
Many patients exposed to high doses of radiation die
from pulmonary complications or aplastic anaemia,
FIG 3.21
BURNS.
A superficial burn: hyperaemia, blistering and pain.
A partial-thickness burn: loss of epithelium, some superficial
capillary bleeding and a few pale patches which may turn out
to be deeper areas of destruction.
A mixture of partial-thickness and full-thickness burns.
An extensive scald, probably mostly a partial-thickness burn.
Chap-03.qxd 4/19/05 13:43PM Page 65
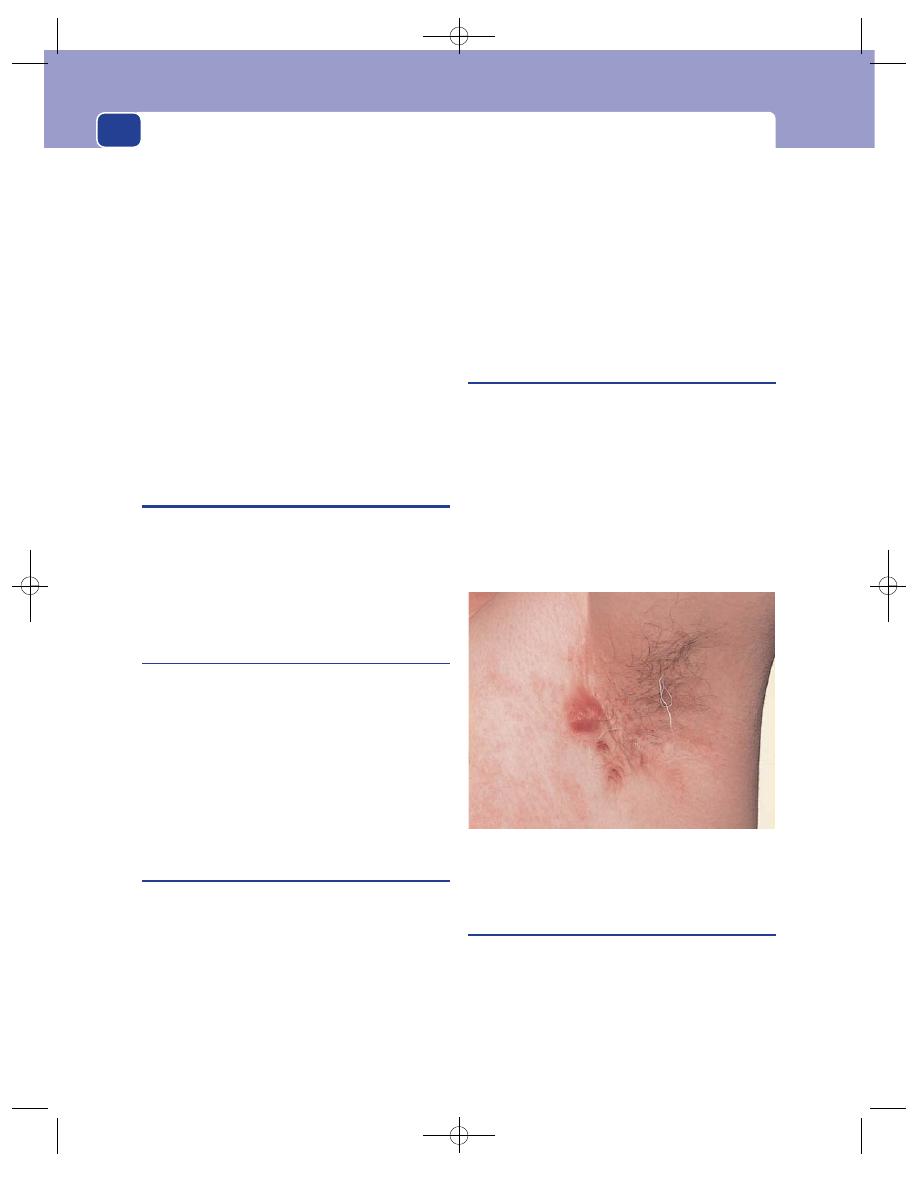
The skin and subcutaneous tissues
66
and those who survive the early systemic effects may
die later from radiation-induced malignant change
in organs such as the thyroid gland.
Chemical burns
Most chemical burns are caused by contact with
acids or alkalis; a few are caused by phosphorus and
phenols. Chemical burns of the skin can be avoided
by wearing protective clothing and washing off the
contaminant as quickly as possible. They produce
the same clinical appearance as full-thickness and
partial-thickness thermal burns.
The oral ingestion of corrosive chemicals may
destroy the lining of the oesophagus and cause life-
threatening complications and serious long-term
morbidity.
INFECTIONS OF THE SKIN
Skin and subcutaneous infections are common, espe-
cially when the skin is breached. The cardinal signs
of rubor, calor, dolor, tumor are usually present in all
infections and patients are invariably pyrexial.
BACTERIAL INFECTIONS
Impetigo
This is now a relatively rare condition. It is a staphy-
lococcal infection that causes blistering of the hands
and face. Vesicles form and rupture and are covered
with a honey-coloured crust. They may form circi-
nate or gyriform patterns. Fresh blisters form daily
and may develop inflammatory halos. A microbio-
logical swab should be sent for culture. Patients are
usually referred to dermatology clinics.
Furunculosis
(boils)
Furuncles and boils are caused by infection entering
a hair follicle. The infection first produces pus and
then a central core of necrotic tissue.
When the lesion contains only pus it is called
a furuncle; when it contains a solid core it is called
a boil.
Boils are often multiple and associated with gen-
eral debility, or an underlying disease such as dia-
betes. They can occur on any part of the body but are
common in the skin of the head and neck, axillae and
groins. They begin as a hard, red, tender area, which
gradually enlarges and causes a throbbing pain.
Eventually the tissue in the centre of the infected area
dies and forms a thick yellow slough that will not sep-
arate from the adjacent tissue until it is surrounded
by pus. When this happens the lump becomes fluc-
tuant, the centre of the covering skin sloughs and
the pus and necrotic core are discharged.
Hidradenitis suppurativa
Whereas boils are infections in the hair follicles,
hidradenitis is an infection of the apocrine sweat
glands. It is most often seen in the axillae and groins
of Caucasians living in tropical countries.
The patient presents with multiple tender swel-
lings in the axillae or groins, which enlarge and then
discharge pus. The condition is made worse if there
is an underlying systemic disease, such as diabetes.
The site and the chronic recurring nature of this con-
dition make it unpleasant and disabling.
Erysipelas and cellulitis
Erysipelas is an infection in the skin and subcuta-
neous tissues by a pathogenic Streptococcus. Whereas
the Staphylococcus commonly causes a localized infec-
tion and pus formation, the Streptococcus spreads
easily through the skin and produces a diffuse celluli-
tis. The erythrotoxins produced by the Streptococcus
FIG 3.22
Hidradenitis suppurativa. One set of infected apocrine
glands has already been excised from this man’s left axilla, but
another cluster has become red, swollen and tender.
Chap-03.qxd 4/19/05 13:43PM Page 66
Infections of the skin
67
make the infected area red, hot, tender and oedema-
tous. Oedema of the reddened skin gives the involved
area a raised border – a diagnostic clinical appear-
ance. The patient has a high temperature, tachycardia
and general debility. Streptococcal infections rarely
form thick pus.
Careful examination may reveal a source of entry
for the organism, such as a small cut or a scratch.
Erysipelas is especially common when there is pre-
existing oedema caused by venous or lymphatic
insufficiency.
Infection of the skin and subcutaneous tissues
caused by other organisms, without the bright-red
discolouration of the skin and the raised border, is
called cellulitis. A patch of cellulitis may necrose and
suppurate.
Erysipeloid
This is a Gram-positive coccal infection that is pres-
ent in shellfish, meat and poultry. It commonly affects
fishermen, fishmongers and butchers. It occurs in the
hands, usually as a purple/red papule with a well-
defined edge, and may spread to other fingers.
Anthrax
This is a spore-forming, highly resistant bacterium
which is found in animal carriers and is present in
wood, hide and bones. It causes a black, malignant-
looking sore on the skin and patients may die rap-
idly from pulmonary complications.
Tuberculosis
Tuberculosis of the skin is a rarity. Primary tuber-
culosis of the skin produces a persistent ulcer with
undermined edges. This is more commonly seen now
in an unhealed BCG vaccination site. The associated
lymph glands are enlarged and may suppurate.
Lupus vulgaris
This is the well-recognized cutaneous form of tuber-
culosis which often affects the head and neck of chil-
dren. The skin is red, telangiectatic and scaly. When
it is compressed with a glass slide it appears to be
composed of pale yellow-brownish nodules (apple
jelly). It is a slowly progressive lesion which causes
massive scarring.
Syphilis
Syphilis is rare in the United Kingdom, although its
incidence has slightly increased in recent years.
The primary sore, or chancre, is acquired by sex-
ual intercourse, biting or kissing and develops
between 3 and 6 weeks after inoculation. The com-
mon sites for chancres are the penis and the vulva,
but they can occur on the cervix, lips, fingers, nipple
or anus. A chancre is usually a 1 cm or less solid
papular ulcer with an indurated base which can be
lifted up like a button in the skin. Approximately 1
week after its appearance, one or more of the regional
lymph glands become enlarged. Affected glands are
not painful and feel rubbery. They are called bubos.
The secondary stage develops 5–6 weeks later if
the primary condition is not treated. This is the result
of organisms disseminating through the blood-
stream. A widespread polymorphic rash develops
which is not itchy and consists of macules, papules
and scaly lesions. Patients often complain of malaise,
headaches and limb pains when the rash begins. At
first the macules are pink or copper-coloured and
oval in shape with an ill-defined edge. They are widely
distributed on the trunk, limbs, palms of the hands
and soles of the feet. The papules have similar char-
acteristics. The picture becomes more varied if the
condition progresses untreated. The papules become
florid and scaly and appear in groups, often with an
annular pattern, which makes them look almost like
psoriasis. This is associated with a generalized lym-
phadenopathy. Enlargement of the epitrochlear
lymph glands is said to be characteristic.
Superficial erosions develop in the buccal
mucosa. These may appear as tender, red patches.
When they are covered by adherent mucus, they are
likened to snail tracks. It is, therefore, always impor-
tant to look in the mouth and fold back the lips.
Flat, moist plaques which are purple in colour
may appear in the peri-anal and vulval skin, at the
angle of the mouth and in any of the skin flexures
(e.g. armpits and groins). These are called condylo-
mata lata.
A patchy loss of hair often occurs in the late stages
of syphilis, which gives patients a ‘moth-eaten’
appearance.
Tertiary syphilis begins 2–10 years after the ini-
tial infection. Serpiginous or arculate nodules may
develop which are either scaly or ulcerated. These
Chap-03.qxd 4/19/05 13:43PM Page 67
The skin and subcutaneous tissues
68
leave central scars which may be mistaken for lupus
vulgaris (see above), though the latter is usually much
more chronic in its development.
Gummata can also develop at this stage. They
start as a small nodule in the subcutis but then
enlarge and become red before ulcerating. The ulcer
associated with gumma is discreet, punched out
(see above) and characteristically has a wash-leather
slough in its base.
Palmar hyperkeratosis is a rare association.
Leukoplakia of the mouth and tongue is another
manifestation of the tertiary stage of syphilis. The
epithelium appears thickened and white. This condi-
tion is potentially pre-malignant. Aortic aneurysms
and tabes dorsalis are other important complications
of the tertiary stage.
General paralysis of the insane eventually devel-
ops and is the quaternary (final stage) of syphilis.
Congenital syphilis is almost extinct in the
home-born population of the UK because of routine
serological screening in pregnancy. Affected chil-
dren develop a bullous eruption on their palms and
soles a few days after birth. The liver enlarges and
they develop ‘snuffles’ from severe nasal discharge
which obstructs the breathing. The bridge of the
nose eventually ‘caves in’. The long bones develop
osteochondritis and periostitis, causing deformity.
Diagnosis
The diagnosis of primary syphilis is usu-
ally made by scarifying the chancre, transferring
the resultant discharge onto a microscope slide and
examining it with dark-ground illumination for the
presence of spirochaetes. There are a number of sero-
logical tests that are useful for detecting the present
or prior infection.
Leprosy
(Hansen’s disease)
This is increasingly appearing in all parts of the
world because of the ease of air travel and shifts of
large populations to seek asylum. It must always be
considered in a patient from a tropical country pre-
senting with an unusual rash. It is spread by pro-
longed contact.
The ‘tuberculoid’ form is most commonly seen
in the UK. The skin usually contains sharply defined
asymmetrical areas of hypo-pigmentation with dry,
scaly surfaces. Alternatively, there may be infiltrated,
raised, hyperpigmented plaques with sharply
demarcated erythematous edges. These may resem-
ble viteligo, but differ in that some pigment remains.
These plaques or patches are insensate.
The ulnar, peroneal and greater auricular nerves
are commonly thickened and easily palpable. Foot
drop and ulnar palsy are common. Eventually, the
insensate fingers are damaged by repeated trauma
and disappear.
Patients with lepromatous leprosy have no
resistance to the spread of organisms. The early skin
lesions are small, ill-defined, erythematous macules
which have a smooth and shiny surface. These
become infiltrated to form plaques and nodules,
especially in the face and pinnae. The polyneuritis
described above is a late manifestation of this form
of disease.
Diagnosis
The diagnosis is made by biopsy and nasal
scrapings, when the microbacteria may be seen
within the granulomata consisting of epithelioid
cells surrounding histiocytes and lymphocytes.
VIRAL INFECTIONS
Viral warts
Warts are papilliferous patches of overgrown hyper-
keratotic skin whose growth has been stimulated by
the human papilloma virus.
History
Age
Warts occur at any age but are most common
in children, adolescents and young adults.
Duration
They grow to their full size in a few weeks,
but may be present for months or years before a
patient complains about them. Patients have usually
made their own diagnosis and decided that there was
no cause for concern.
Symptoms
Warts are disfiguring. Multiple warts on the
fingers can interfere with fine movements. They are
only painful if they are rubbed or become infected.
Progression
Once present, they may persist unchanged
for many years or regress and disappear sponta-
neously. ‘Kiss lesions’ may appear on adjacent areas
of skin that make frequent contact. Warts occur in
crops and may come and go spontaneously.
Family history
Other members of the family may have
warts.
Chap-03.qxd 4/19/05 13:43PM Page 68
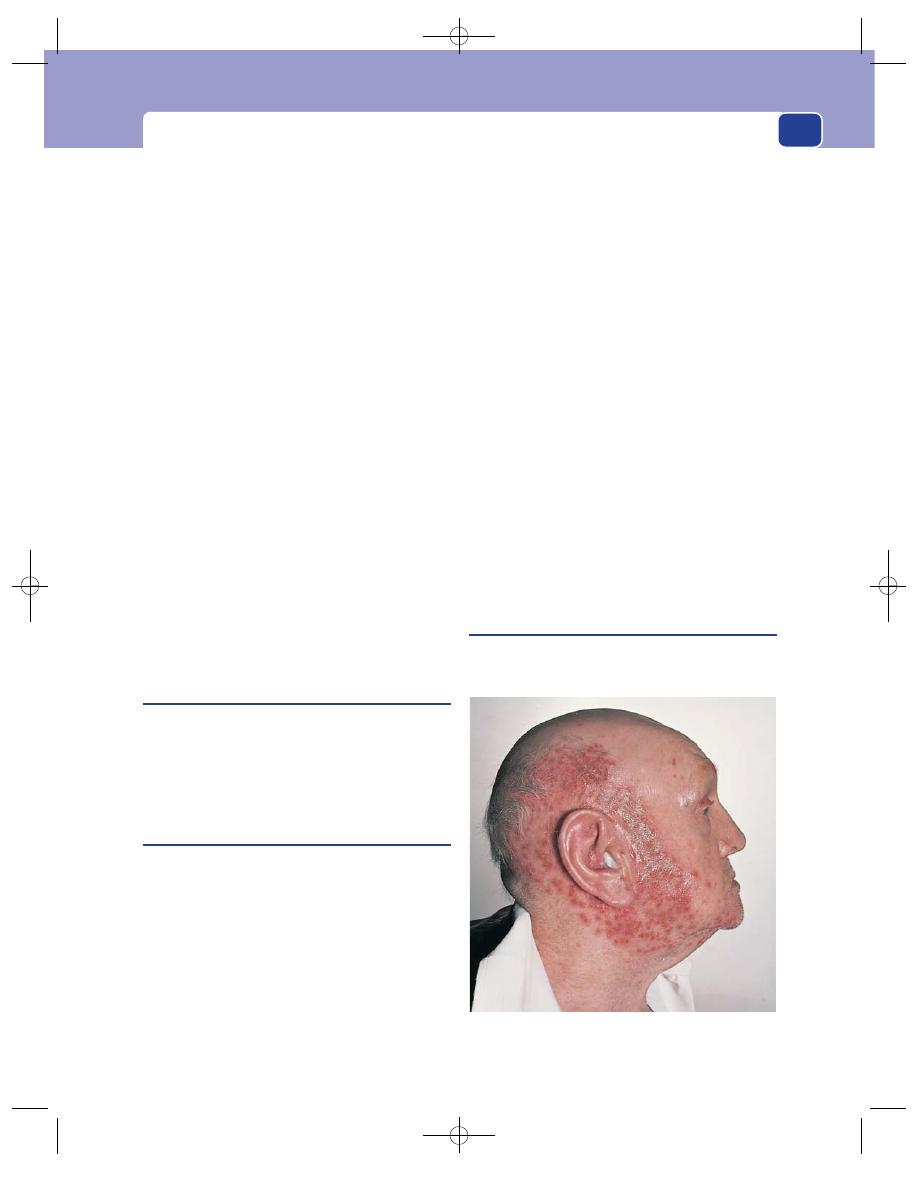
Infections of the skin
69
Examination
Site
Warts are commonly found on the hands, but
they may appear on other exposed areas that are fre-
quently touched by the hands, such as the face, arms
and knees.
Shape and size
They arise as flat-topped, angular,
smooth or hemispherical macules which are less
than 1 cm in diameter.
Surface
Their surface is rough and hyperkeratotic,
and often covered with fine filiform excrescences.
Colour
Warts are greyish-brown.
Composition
Warts are firm and not compressible.
Lymph drainage
The regional lymph glands should
not be enlarged.
Differential diagnosis
Squamous papilloma, mollus-
cum contagiosum and condylomata lata are other
conditions that may be considered in the differen-
tial diagnosis.
Plantar warts
Warts on the soles of the feet are fundamentally the
same as any other wart, but they have a different
appearance because they are pushed into the skin.
They must be differentiated from callosities and
corns (see description in Chapter 6, page 169).
Molluscum contagiosum
Discrete, pearly, rounded nodules with umbilicated
centres are indicative of this infection. They are usu-
ally grouped in one area of the trunk. They release a
white exudate when squeezed, which contains the
virus.
Herpes simplex
This is the commonest skin virus. More than 60 per
cent of the population are infected and remain car-
riers throughout their lives. The primary infection
often passes unnoticed, but it may cause a severe gin-
givo-stomatitis with fever and local lymphadenopa-
thy. The mouth often contains a crop of ‘aphthous’
ulcers. Vesicles may be present over the face, neck
and even the eyes. The attack subsides in 10–14 days,
but the virus remains latent in the epithelial cells of
the buccal and nasal mucosa. The micro-organisms
may proliferate again in response to a noxious
stimulus such as a fever, sunlight, pneumonia or
immune suppression.
History
Patients usually complain of a painful localized sore
on their lip which develops blisters that discharge
and then crust over.
Examination
Site
Most lesions occur at the mucocutaneous junc-
tions, particularly on the lips and angle of the
mouth, but they may appear on the nail clefts,
trunk, genitalia, cheeks and natal cleft.
Shape and size
A burning, uncomfortable papule dev-
elops which is usually oval or elliptical. It is slightly
raised and very tender.
Surface
The papular surface is smooth at first but
becomes covered in a crop of small vesicles which
break to leave a crust. This heals in 7–10 days and
the skin returns to normal.
Lymph drainage
The draining lymph glands are rarely
enlarged.
Herpes zoster
This skin rash is thought to be caused by reactiva-
tion of the chickenpox virus, which can lie dormant
FIG 3.23
Shingles (herpes zoster) in the distribution of the
mandibular nerve.
Chap-03.qxd 4/19/05 13:43PM Page 69
The skin and subcutaneous tissues
70
for many years in the anterior horn cells of the
spinal cord.
History
Age
It usually occurs after the age of 45 years.
Onset
It can develop within a week of re-exposure
to the varicella virus. Reactivation can be the result
of tuberculosis or tumour.
Symptoms
Pain occurs over the distribution of the
nerve roots involved before the rash develops.
Examination
Site
The rash can occur in any cutaneous dermatome
or dermatomes. It appears in a continuous line or as
patches throughout these segments. The trigeminal
nerve may be involved, and if the virus enters the
ophthalmic branch, the eye will be affected.
Rash
Initially, there is a raised patch of erythema
which rapidly becomes covered with a cluster of
umbilicated vesicles. These quickly become infected
and haemorrhagic before necrotic crusts form. There
may be severe photophobia, with a red, watering eye
if the ophthalmic division of the trigeminal nerve is
involved.
Resolution
The pain improves as the rash clears. The
rash starts to disappear after about 10 days but, in
some patients, severe cutaneous necrosis can leave
disfiguring scars and there may be persisting pain.
Do not forget that herpes zoster may be the
cause of severe abdominal pain before the rash
develops and the diagnosis is clear.
FUNGAL INFECTIONS
Candida
(moniliasis)
This is a normal component of the body’s flora and
is present in the skin, mouth, vagina and gut of us
all. Clinical problems only develop when there is a
reduction in the normal defence mechanism which
leads to infection.
Moniliasis may present in a number of different
ways.
The buccal mucosa and tongue of infants or adults
on prolonged courses of antibiotics may become cov-
ered in white spots or plaques.
Flexural intertrigo
Scattered soft macules may appear in the skin flex-
ures, especially in the submammary areas and axil-
lae of obese women. Patients with these problems
should be checked for coexisting diabetes.
Balanitis
Monilial balanitis can be a problem in uncircum-
cized men.
Chronic paronychia
Housewives, nurses and barmaids who frequently
immerse their hands for prolonged periods have an
increased risk of developing this problem. The pro-
longed immersion causes the quick to separate from
the nail plate, which allows the fungus to gain access
from its reservoir in the gastrointestinal tract or
vagina. Established infection causes a painful red
swelling at the base of the nail. If the nail is damaged
or invaded by the fungus, it becomes thickened,
opaque and soft.
The differential diagnosis of a chronic parony-
chia includes herpetic paronychia, bacterial parony-
chia, collagen diseases and Buerger’s disease.
Tinea pedis
(athlete’s foot)
This is a common skin infection caused by one of
three fungi which may be found in many surgical
patients. Damage to the protective barrier function
of the skin caused by athlete’s foot may predispose
to the entry of bacteria which can cause cellulitis,
especially in patients with chronic lymphoedema.
History
Age and sex
Tinea pedis has a high incidence in fit,
young male athletes and swimmers who pick it up
in showers and communal baths.
Symptoms
Patients usually complain of itching, mac-
eration and fissure formation in the inter-digital
spaces of the toes, most often in the space between
the fourth and fifth toes. One foot is usually more
affected than the other. It often improves in winter
and worsens in summer. The sole of the foot may
also develop vesicles and itching and the palms may
also develop the rash. Lymphangitis and cellulitis
may develop (see above).
Chap-03.qxd 4/19/05 13:43PM Page 70
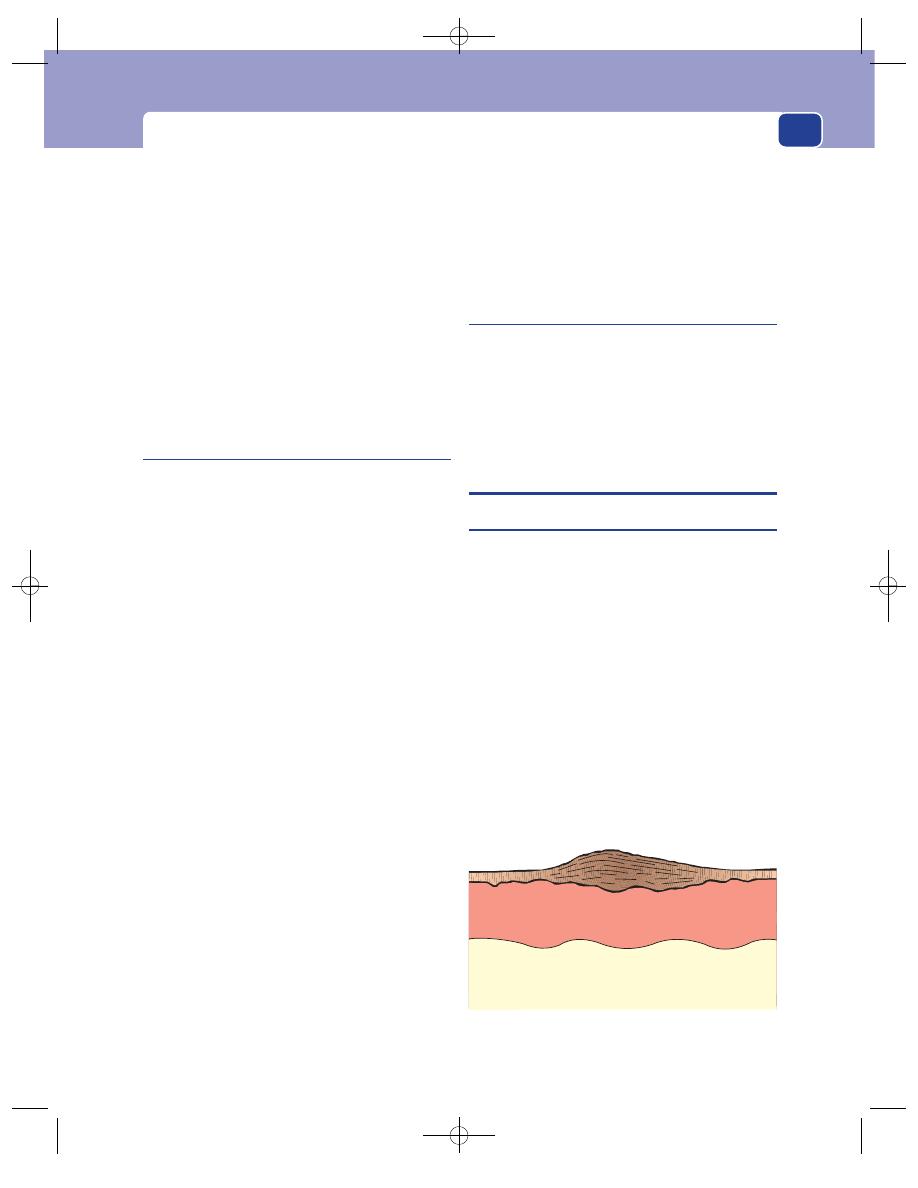
Benign tumours and benign skin lumps
71
Examination
Site
Always inspect between the toes.
Rash
Maceration, odour and fissure formation with
desquamation may be present. These may spread
onto the dorsum of the foot. Asymmetry is charac-
teristic. A vesicular eruption with bullae may be
present on the soles of the feet and the palms of the
hands. The nails may become distorted, white and
soft. The fungus may spread to the limbs and trunk,
especially the groins, where annular or ring lesions
may develop.
INFESTATIONS
Scabies
This is the result of invasion of the epidermis by the
Acarus scabies mite. The adult female is about
0.5 mm in length and is only just visible to the naked
eye. The male is half this size. The fertilized female
moves over the warm body until it finds a place to
burrow through the horny layer of the skin. The
female remains here for the rest of her life, laying two
or three eggs per day for several weeks. These hatch
in 3–4 days and the larvae leave the burrow and enter
the hair follicles to mature. The adult mites then
escape onto the skin, where mating occurs. This cycle
then begins again, roughly every fortnight. Sixty
per cent of burrows are on the hands and wrists, the
remainder being on the soles of the feet, the genitalia,
the axillae, the elbows and the buttocks.
History
In a patient who has never had scabies, an erythe-
matous rash develops around the burrows 1 month
after infestation, followed by a generalized urticarial
reaction. The skin then begins to itch, especially at
night. Other family members are often affected.
Examination
An urticarial rash is usually present, which in adults
consists of wheals developing mostly on the trunk and
limbs. Vesiculation may be present on the hands and
limbs, which may become eczematous or infected.
Confirmation of diagnosis
The diagnosis is confirmed
by finding burrows. A magnifying lens, a good light
and a sterile needle are required. The mite is visible
at the anterior end of the burrow as a white oval
with a black dot at its front. The needle is inserted
into the burrow, which is opened up, and the mite
adheres to the tip of the needle. The mite is then put
on a microscope slide and inked around, and the
diagnosis is confirmed. The differential diagnosis
includes other causes of generalized itching.
Pediculosis capitis
Infestation with head lice is common in school chil-
dren. Severe infestation causes intolerable itching
and there is often secondary infection and enlarged
cervical lymph glands.
Nits are present on the shafts of the hairs.
BENIGN TUMOURS AND BENIGN SKIN
LUMPS
Seborrhoeic keratosis
This lesion is also called a senile wart, seborrhoeic
wart, verruca senilis or basal cell papilloma. It is a
benign overgrowth of the basal layer of the epidermis
containing excess small, dark-staining basal cells,
which raise it above the level of the normal epidermis
and give it a semi-transparent, oily appearance.
History
Age
Senile warts occur in both sexes but, as the name
implies, they become more common with advanc-
ing years. Most people over the age of 70 years have
got one or two of these lesions.
Duration
They are slow growing, beginning as a
minute patch which gradually increases in area.
Patients do not notice the early changes in the skin
FIG 3.24
A seborrhoeic keratosis. The plaque consists of an
excess number of basal cells and will peel off.
Chap-03.qxd 4/19/05 13:43PM Page 71
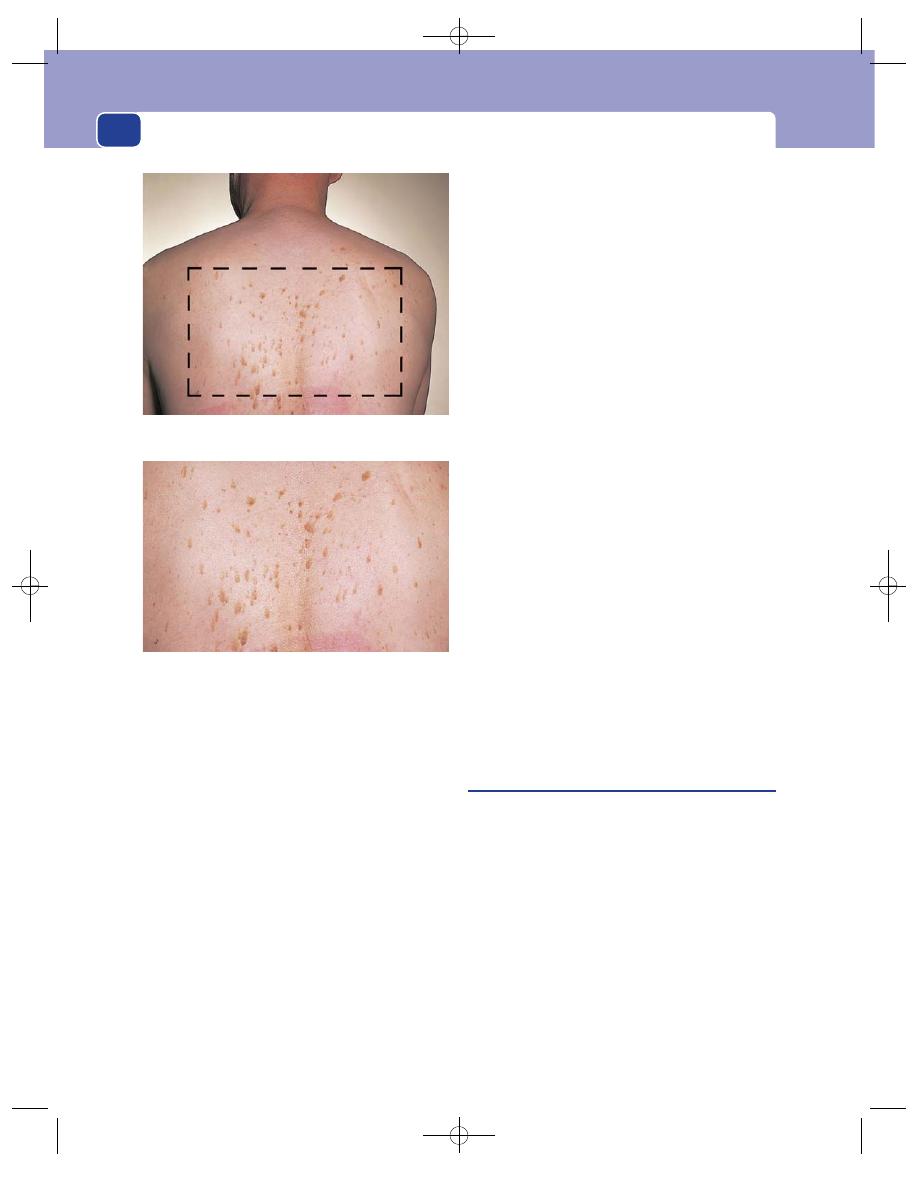
The skin and subcutaneous tissues
72
and have invariably had the lesion for months or
years before complaining about it.
Symptoms
As the lesion gets bigger, it becomes dis-
figuring and may start to catch on clothes. It seldom
bleeds but may get infected. Sometimes there is suf-
ficient melanin in the lesion to make the patient
think it is a mole.
Progression
Senile warts gradually increase in area, but
not in thickness. They can suddenly fall off, uncov-
ering a pale-pink patch of skin.
Examination
Site
Seborrhoeic keratoses occur on any part of the
skin except those areas subjected to regular abrasion,
such as the palms of the hands and the soles of the
feet. The majority are found on the back of the trunk.
Shape and size
They form a raised plateau of hyper-
trophic, slightly greasy skin, with a square-cut and
distinct edge. They vary in size from a few millime-
tres to 2–3 cm in diameter.
Surface
They have a rough, sometimes papilliferous,
surface.
Colour
Their colour varies from normal skin colour
through pale yellow to dark brown, depending on
the thickness of the epithelium and the quantity of
melanin in the underlying skin.
Bleeding into a senile keratosis caused by trauma
makes the lesion swell and turn brown – changes
that may be confused with malignant change in a
melanoma.
An infected keratosis also becomes swollen and
tender and can be confused with a pyogenic granu-
loma or squamous cell carcinoma.
Consistence
Senile warts are a little harder and stiffer
than normal skin. The surrounding tissues are
healthy, but there may be other seborrhoeic warts
nearby. They have a greasy, soapy feel.
Special diagnostic feature
Because seborrhoeic kera-
toses are patches of thick squamous epithelium,
they can be picked off. They feel ‘stuck on’. If you are
sure of the diagnosis, you may try to pick off the
edge of the plaque with blunt forceps.
When a seborrhoeic wart peels off, it leaves a
patch of pale-pink skin and one or two fine surface
capillaries that bleed slightly. No other skin lesion
behaves like this.
Never pick hard at the edge of any lesion for
fear of damaging it. Interfering in this way with a
malignant tumour may hasten its local spread.
Sebaceous cysts
The skin is kept soft and oily by the sebum secreted
by the sebaceous glands. The mouths of these glands
open into the hair follicles. If the mouth of the gland
becomes blocked, it distends with its own secretion
and ultimately becomes a sebaceous cyst. Sebaceous
cysts in the scalp are more correctly called pilar or
trichilemmal cysts, as they arise from infundibular
parts of hair follicles and have no function.
History
Age
Sebaceous cysts occur in all age groups, but as
they are slow growing they rarely present before
adolescence. Sometimes they appear suddenly dur-
ing adolescence because the skin gland secretions
A patient whose back was covered with seborrhoeic
keratoses.
The area outlined in the upper panel is enlarged here.
FIG 3.25
Chap-03.qxd 4/19/05 13:43PM Page 72
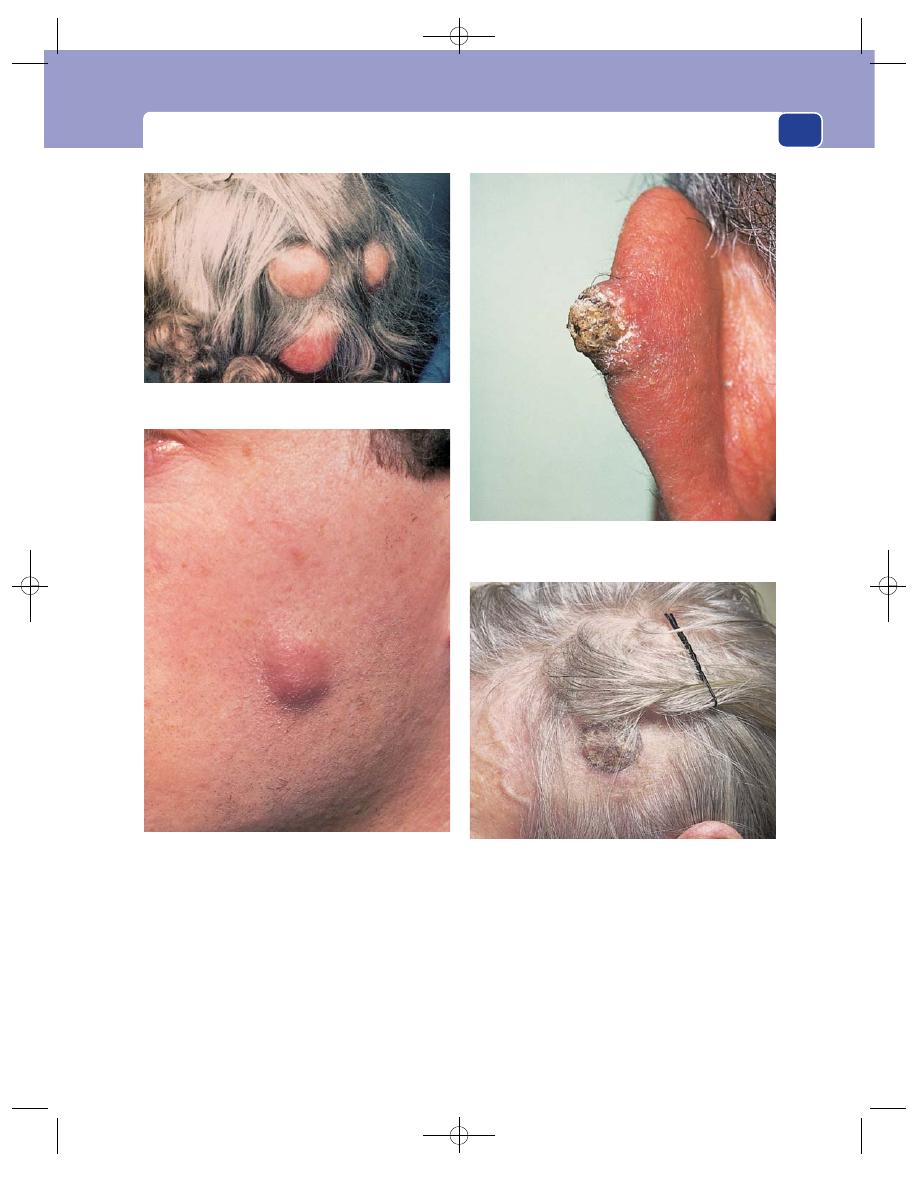
Benign tumours and benign skin lumps
73
change at puberty, but most sebaceous cysts present
in early adulthood and middle age.
Duration
Sebaceous cysts are slow growing and have
usually been present for some years before the patient
asks a surgeon to remove them.
Symptoms
Sebaceous cysts are most frequently found
on the scalp, and the commonest complaint is of a
lump that gets scratched when the patient is combing
their hair. Such scratches may get infected. When
infection develops in a cyst, it enlarges rapidly and
becomes acutely painful.
FIG 3.26
SEBACEOUS CYSTS.
A small sebaceous cyst on the skin. The slight erythema is the
residue of a recent infection in the cyst.
A sebaceous horn on the ear. The ‘horn’ is simply the hardened
sebaceous material (epithelial cells and sebum) extruding from
the cyst.
Cock’s peculiar tumour. This is a mass of granulation tissue
protruding from the base of a previously infected and
ruptured sebaceous cyst.
Three sebaceous cysts on the scalp. Note that you cannot see
a punctum, a common finding.
Chap-03.qxd 4/19/05 13:43PM Page 73
The skin and subcutaneous tissues
74
A slow discharge of sebum from a wide punctum
sometimes hardens to form a sebaceous horn.
Infection of the cyst wall and the surrounding
tissues produces a boggy, painful, discharging swelling
known as Cock’s peculiar tumour. This only hap-
pens if an infected cyst is neglected.
Development
Sebaceous cysts usually enlarge with
time, but the increase in size is accelerated if the cyst
becomes infected. Sometimes a cyst will discharge
its contents through its punctum and then regress
or even disappear.
Multiplicity
Sebaceous cysts are often multiple.
Examination
Site
Most sebaceous cysts are found in the hairy
parts of the body. The scalp, scrotum, neck, shoul-
ders and back are the common sites, but they can
occur wherever there are sebaceous glands. There
are no sebaceous glands on the palms of the hands
and soles of the feet.
Shape and size
Most sebaceous cysts are tense and
spherical. Even on the scalp, where there is the
unyielding skull beneath them, they remain spheri-
cal by bulging outwards and stretching the over-
lying skin.
They can vary from a few millimetres to 4–5 cm
in diameter, but most patients seek advice before
they become very large.
Surface
The surface of a sebaceous cyst is smooth.
Edge
The edge is well defined and easy to feel, as it is
usually lying in subcutaneous fat.
Colour
The skin over the cysts is usually normal.
Tenderness
Uncomplicated sebaceous cysts are not
tender. Pain and tenderness indicate infection.
Temperature
The temperature of the skin over a cyst
is normal except when the cyst is inflamed.
Composition
Most sebaceous cysts feel hard and solid.
Occasionally they are so tense that it is not possible
to elicit fluctuation, especially if there is no firm
underlying tissue to press them against. On the scalp
the resistance of the underlying skull aids detection
of fluctuation. They do not transilluminate because
they are full of sebum.
Relations
They arise from a skin structure but lie in
the subcutaneous tissues, although they are attached
to skin. Their point of discharge is usually along a
hair follicle and, as the cyst grows, this point of fixa-
tion is often pulled inwards to become a small punc-
tum. Only one-half of the cysts that you will see will
have a visible punctum, but when it is present it is a
useful diagnostic sign. Even if there is no punctum,
all sebaceous cysts are attached to the skin. The area
of attachment may be quite small but it prevents the
cyst moving independently of the skin. Sebaceous
cysts are not attached deeply.
Lymph drainage
The local lymph glands should not
be enlarged.
Cock’s peculiar tumour
This eponym is still used by surgeons for sentimen-
tal and aesthetic reasons – it is a nice name. Cock’s
peculiar tumour is an infected, open, granulating,
oedematous sebaceous cyst. It looks angry, sore and
malignant and is often mistaken for a squamous cell
carcinoma of the scalp. Granulation tissue arising
from the lining of the cyst heaps up and bursts
through onto the skin, giving the lesion an everted
edge. The infection in the cyst wall and surrounding
tissues makes the whole area oedematous, red and
tender. The regional lymph glands may be enlarged.
The history usually betrays the diagnosis. The
patient will tell of a long-standing lump which
became painful and discharged pus spontaneously
or was treated by an inadequate incision.
Sebaceous horn
A sebaceous horn arises from a sebaceous cyst.
The sebum in a sebaceous cyst may slowly exude
from a large central punctum and dry and harden
into a conical spike. This is a sebaceous horn.
Normally the friction from clothes, and soap and
water, removes the secretions of the gland as soon as
they appear. A horn can only grow if the patient fails
to wash the skin over the cyst. The tendency to form a
horn is greater if there is a wide opening into the cyst.
Sebaceous horns can be broken off or pulled out
of the cyst, because they have no intrinsic living
structure.
Chap-03.qxd 4/19/05 13:43PM Page 74
Pigmented naevi
75
PIGMENTED NAEVI
(Moles)
The word mole is a lay term used to describe a
brown spot or blemish on the skin. The brown pig-
ment is melanin. There are three ways in which an
excess of melanin may be produced to colour the
skin brown.
1. There may be a normal number of melanocytes,
in their normal position, each producing an
excess quantity of melanin. The lesion produced
by this abnormality is called a freckle or
ephelis. It is not called a mole because it
does not contain an increased number of
melanocytes.
2. There may be an increased number of
melanocytes, in their normal position, each
producing normal quantities of melanin. The
lesion produced by this abnormality is called a
lentigo.
3. There may be an increased number of
melanocytes, in abnormal clusters at the dermo-
epidermal junction, producing normal or excess
quantities of melanin. The lesion produced by
this abnormality is called a mole or pigmented
naevus.
A mole becomes a malignant melanoma if the
melanocytes invade adjacent tissues or show signs
of abnormal and excessive multiplication. It is
called a dysplastic naevus if there is no invasion but
some nuclear abnormalities.
Because the three benign pathological entities
described above often have similar macroscopic fea-
tures, it is safest to be non-committal and call all
benign melanin-producing lesions moles or pig-
mented naevi and malignant melanin-producing
lesions malignant melanoma.
Pathology
Whereas the clinical appearance of pigmented naevi
is infinitely variable and almost unclassifiable, moles
can be defined according to their microscopic appear-
ance (see Fig. 3.27). Melanocytes are normally found
in small numbers among the cells of the basal layer
of the epidermis. If they proliferate, they first cluster
in this layer and then migrate into the dermis. The
mature adult mole consists of clusters of melanocytes
in the dermis and is therefore called an intradermal
naevus. An intradermal naevus can be flat or raised,
smooth or warty, and hairy or non-hairy. Most of
the moles on the arms, face and trunk are of this
variety. They hardly ever turn malignant.
If the growth and movement of the melanocytes
stop before they have all migrated into the dermis,
there will be clusters of cells at various stages of matu-
rity in the epidermis and the dermis. This lesion is
called a compound cellular naevus.
If the melanocytes remain close to the junction
between the epidermis and dermis, the naevus is
called a junctional naevus. Junctional naevi are
immature and unstable and can turn malignant.
The majority of malignant melanomata begin in
junctional moles. Many of the moles on the palms
of the hands, the soles of the feet and the external
genitalia are of the junctional variety.
Melanocytes which have never reached the epi-
dermis and therefore lie in the deep dermis or sub-
cutaneous tissues may still proliferate and produce
excess melanin. The resulting lesion has a blue
appearance and is called a blue naevus.
The only practical clinical approach is to excise
any mole that is suspected of undergoing malignant
change.
History
Age
Except for albinos, everyone has a few moles at
birth, but the number increases during life. It has been
estimated that most Caucasians have 15–20 moles.
During childhood and adolescence, these may
become more pigmented or completely regress.
When enlarging and getting darker, a mole on a
child may be clinically and histologically difficult to
distinguish from a malignant melanoma, but true
malignant change is uncommon before puberty.
Ethnic group
Moles are more common in Caucasians
living in hot countries, such as Australia, because
the skin is exposed to more ultraviolet light. Moles
occur in Negroes, particularly in the less pigmented
areas such as the soles of feet and palms of the
hands, but are rare.
Symptoms
Moles rarely cause any serious symptoms.
They may be disfiguring, protrude above the skin
surface and catch on clothes. Itching or bleeding
suggests the possibility that malignant change has
occurred (see below).
Chap-03.qxd 4/19/05 13:43PM Page 75
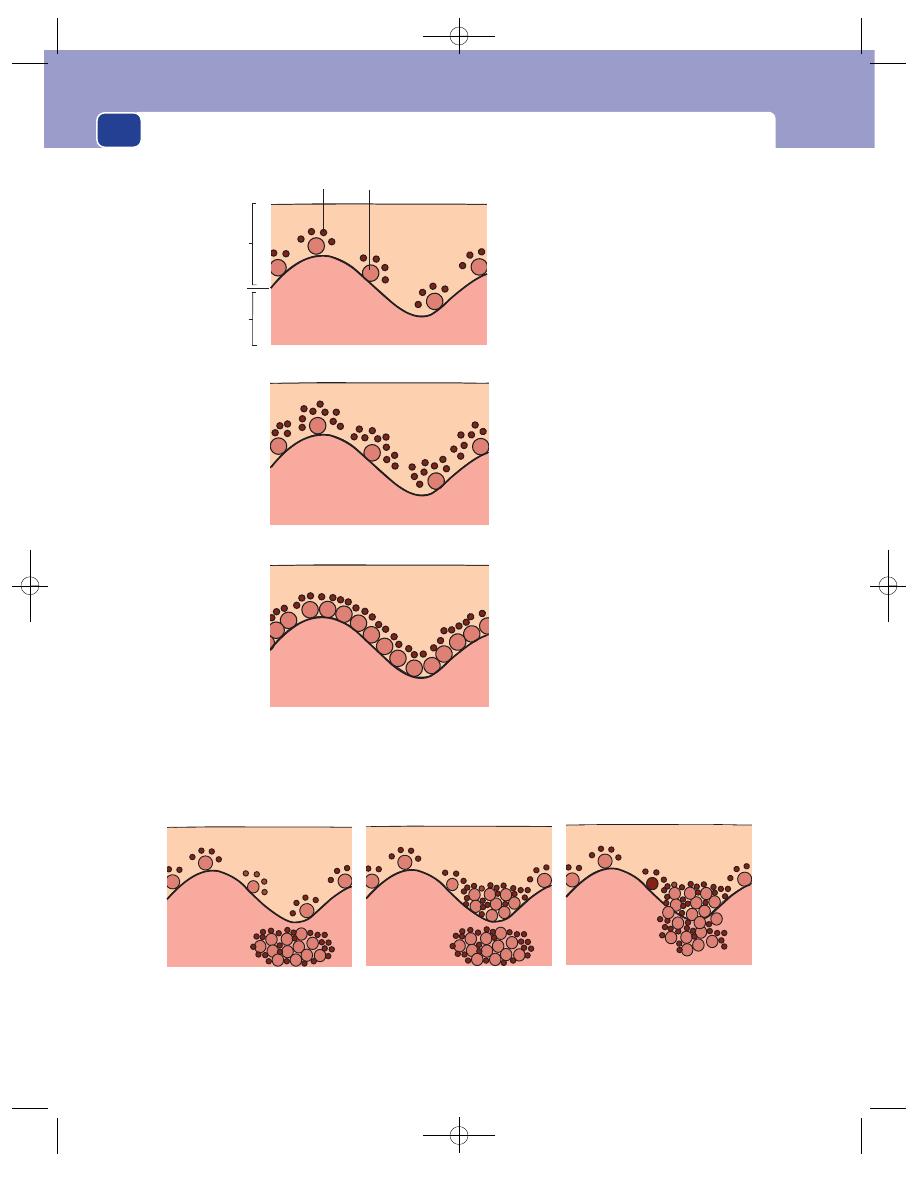
The skin and subcutaneous tissues
76
Pigmented naevus/mole
Intradermal naevus
Compound naevus
Junctional naevus
Excess melanocytes, in clusters, variable but usually excess
melanin production
Normal skin
Freckle (ephelis)
Normal number of melanocytes,
in normal position, producing
excess melanin
Lentigo
Excess melanocytes, in normal
position, producing normal
amount of melanin
Epidermis
Basal layer
Dermis
Melanin
Melanocyte
FIG 3.27
The histological varieties of pigmented spots and blemishes.
Chap-03.qxd 4/19/05 13:43PM Page 76
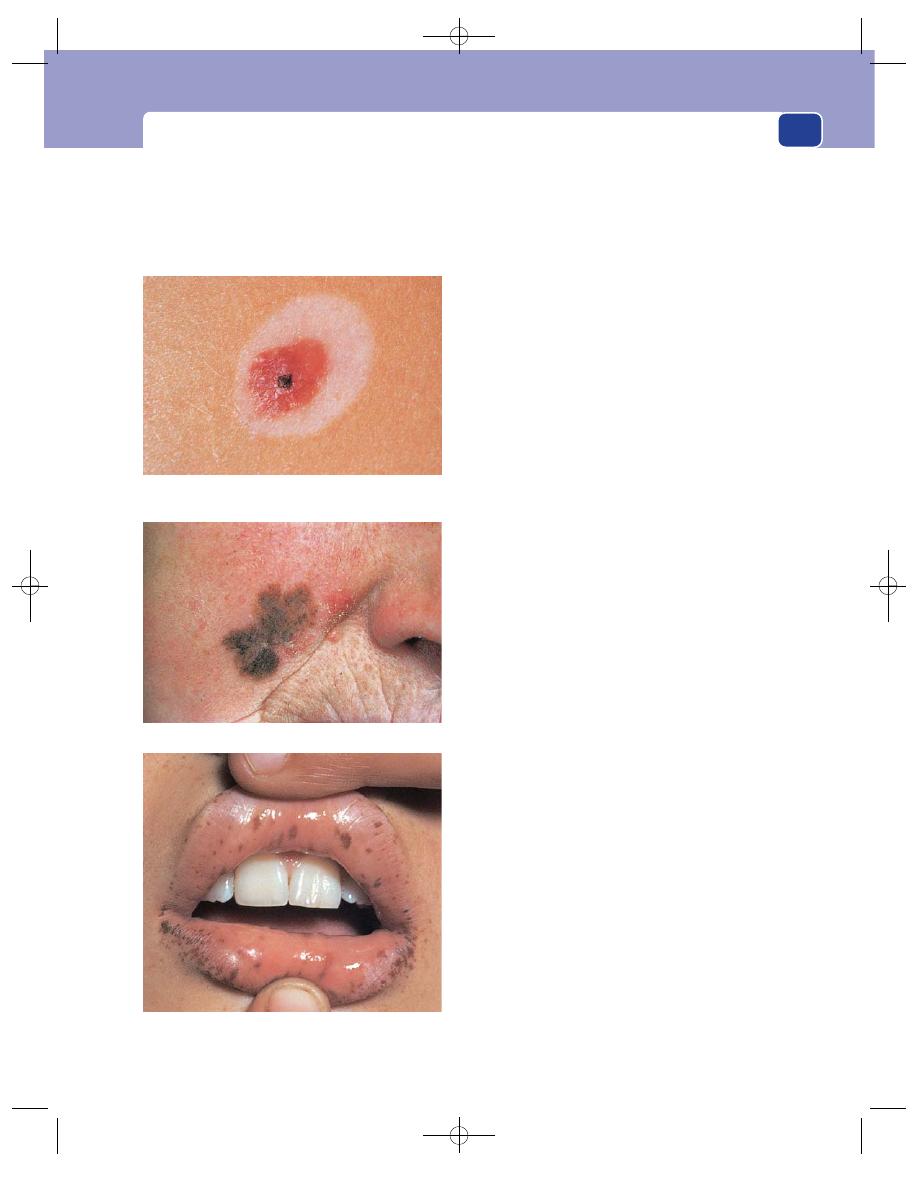
Pigmented naevi
77
Examination
Site
Moles can occur on any part of the skin, but are
most common on the limbs, face, neck and trunk.
Size
Most moles are 1–3 mm in diameter.
Colour
Their colour varies from light brown to black.
Amelanotic naevi do occur, but without their pig-
ment they are unlikely to be recognized. The colour
does not fade with pressure.
Pigmented naevi may regress. A mole sur-
rounded by a white halo of regression is known as a
halo naevus.
Composition
Moles usually have a soft consistence
and are indistinguishable, by palpation, from the
surrounding tissues.
Lymph glands
The local lymph glands should not be
enlarged.
Shape and surface
There are four clinical varieties of
mole.
■
Hairy mole is a common variety. It is flat, or
very slightly raised above the level of the
surrounding skin, with a smooth or slightly
warty epidermal covering, and has hairs growing
from its surface. The presence of hairs means
that the mole also contains sebaceous glands that
can become infected and cause changes such as
swelling and tenderness, which may be
indistinguishable from malignant change. Hairy
moles are always intradermal naevi.
■
Non-hairy or smooth mole is also a common
variety. The epithelium is smooth and not
elevated. The brown pigment looks as if it is
deep in the skin – deeper than that of the hairy
mole – but this is just an optical illusion. There
is no hair growing from its surface. Non-hairy
moles may be intradermal, junctional or
compound naevi.
■
Blue naevus is a mole deep in the dermis. The
thick overlying layers of dermis and epidermis
mask the brown colour of the melanin and
make it look blue. The overlying skin is often
smooth and shiny. This is an uncommon type of
mole, more often seen in children. It usually
occurs on the face, the dorsum of the hands and
feet, and the buttock.
■
Lentigo is an area of pigmentation that appears
in late adult life and is prone to undergo
malignant change (see page 88).
There are two other varieties of melanotic skin
pigmentation – the café au lait patch, and the circu-
moral moles of the Peutz–Jeghers syndrome.
The circumoral pigmented naevi of Peutz–Jeghers syndrome.
FIG 3.28
VARIOUS PIGMENTED NAEVI.
A ‘halo’ mole. This mole is regressing. It has faded and the
skin around it has become de-pigmented.
Hutchinson’s lentigo on the face.
Chap-03.qxd 4/19/05 13:43PM Page 77
The skin and subcutaneous tissues
78
The café au lait patch is an area of pale-brown
pigmentation, present at birth and often associated
with neurofibromatosis and sometimes with phaeo-
chromocytoma. The pale-brown, milk-coffee colour
is a reflection of the small amount of melanin in
the lesion. Histologically these patches can be freck-
les or lentigo. They do not undergo malignant
change.
The Peutz–Jeghers syndrome (primarily multi-
ple polyposis of the mucosa of the stomach and
small intestine) is associated with multiple small
moles on the skin of the face, particularly around
the mouth, on the lips and in the buccal mucous
membrane. Histologically these are patches of lentigo.
They do not turn malignant.
BENIGN SUBCUTANEOUS SWELLINGS
Lipoma
A lipoma is a cluster of fat cells which have become
over-active and so distended with fat that they have
become palpable lumps. They are never malignant.
Liposarcomata, which often develop in the retroperi-
toneal tissues (see page 424), arise de novo.
History
Age
Lipomata occur at all ages but are not common
in children.
Duration
They have usually been present, growing
slowly, for months or years before being noticed.
They rarely regress.
Symptoms
Most patients present because they have
noticed a lump and want to know what it is. The
lump may be unsightly or interfere with movement,
especially if it becomes pedunculated.
Multiplicity
Patients often have many lipomata, or
have had others excised in the past. Multiple con-
tiguous lipomata cause enlargement and distortion
of the subcutaneous tissues. This condition is called
lipomatosis. It usually occurs in the buttocks and
sometimes in the neck.
Multiple lipomatosis (Dercum’s disease) is a con-
dition in which the limbs and sometimes the trunk
are covered with lipomata of all shapes and sizes.
These can be painful and may contain angiomatous
elements and therefore be angiolipomata.
Examination
Site
Lipomata are most common in the subcuta-
neous tissues of the upper limbs, chest, neck and
shoulders, but they can occur anywhere.
Colour
The skin that overlies the lump is normal and
the veins crossing the lipoma may be visible as faint
blue streaks.
Tenderness
Lipomata are not usually tender, but
angiolipomata are.
Temperature
The temperature of the overlying skin is
normal.
Shape and size
Lipomata are usually spherical, but
subcutaneous lipomata which develop between the
skin and the deep fascia are usually discoid or hemi-
spherical. Most lipomata are lobulated, as fat in
the body is in the form of lobules. The lobules can
be seen and felt on the surface and at the edge of
the lump.
Lipomata come in all sizes.
Surface
The surface feels smooth, but firm pressure
reveals the depressions between the lobules. The
lobules become more prominent with firm palpa-
tion or gentle squeezing because the increased pres-
sure within the lipoma makes each lobule bulge out
between the fine strands of fibrous tissue that sur-
round it.
Edge
The edge is not circular but a series of irregu-
lar curves corresponding to each lobule. Because the
edge is soft, compressible and sometimes quite thin,
it slips away from the examining finger. This has
been described as the ‘slip sign’. It is not a very useful
or a diagnostic feature. Evidence of lobulation on
the surface and at the edge is the most significant
physical sign.
Composition
Most lipomata contain a soft but solid
jelly-like fat if they are cut open immediately after
removal. Small lipomata feel soft but do not fluctu-
ate. Because lipomata are soft, they give the impres-
sion of fluctuating, but careful examination reveals
that they are just yielding to pressure and spreading
out in all directions. They do not become more tense
and prominent in the plane at right-angles to the
palpating finger. The larger the lipoma, the more it
will appear to fluctuate, but fat at body temperature
is solid, not liquid.
Lipomata do not transilluminate in that they do
not transmit light from a torch shone beside them,
Chap-03.qxd 4/19/05 13:43PM Page 78
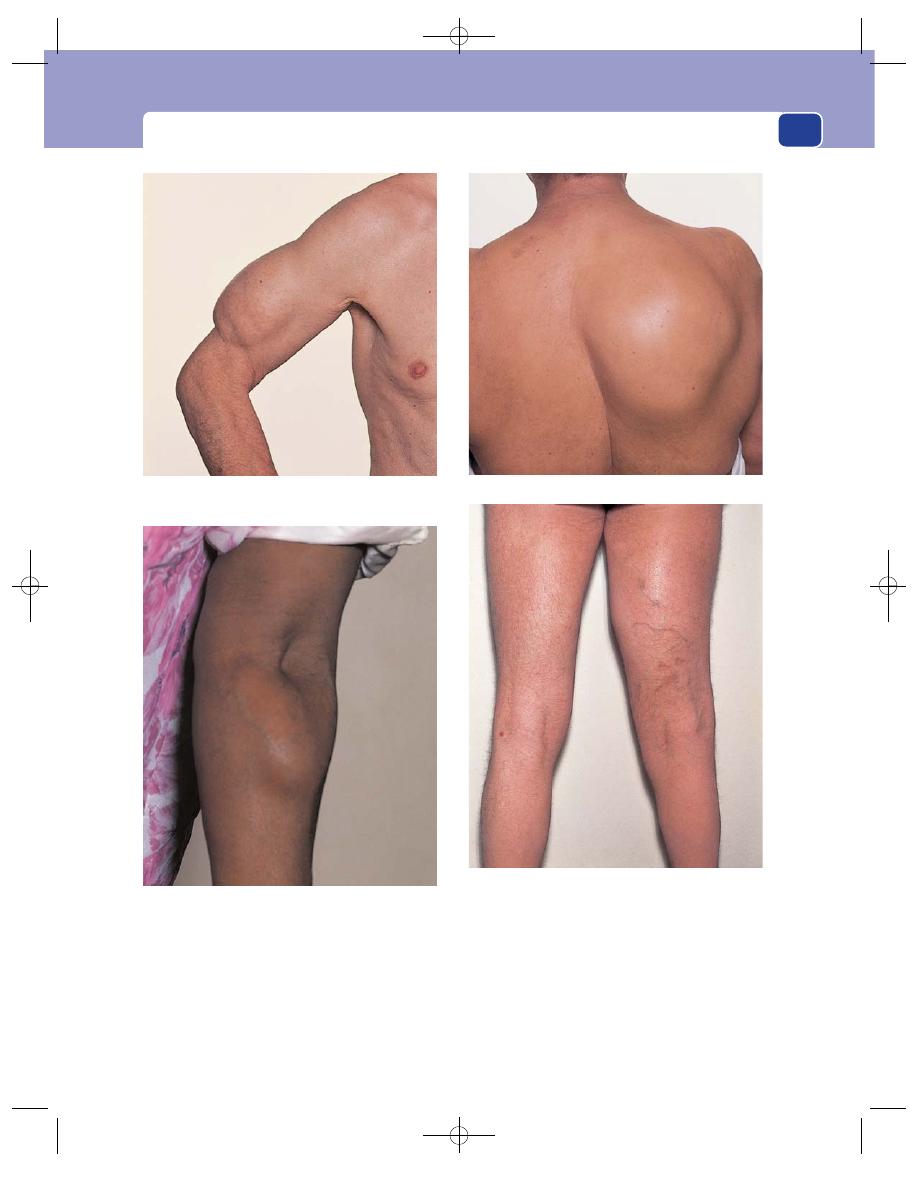
Benign subcutaneous swellings
79
but they may light up if torchlight is shone directly
across them. They do not have a fluid thrill and they
do not reduce or pulsate.
The physical signs of pseudo-fluctuation and
transillumination make them appear cystic, a false
impression which emphasizes the diagnostic impor-
tance of finding lobulation.
Relations
Lipomata may arise within deep structures,
such as muscles. These lipomata are fixed deeply
FIG 3.29
LIPOMATA.
A lipoma in the subcutaneous tissues of the upper arm.
Note the lobulation.
A large lipoma overlying the scapula.
A lipoma in the forearm. This swelling became more
prominent and fixed when the forearm muscles were
contracted, showing that it was superficial to the muscle
but attached to its fascia.
A large lipoma in the inner aspect of the upper right thigh
which became less distinct when the hamstring muscles
were contracted, showing that it was deep to the muscles.
Note the distended veins caused by compression of the
superficial femoral vein by the mass.
Chap-03.qxd 4/19/05 13:43PM Page 79
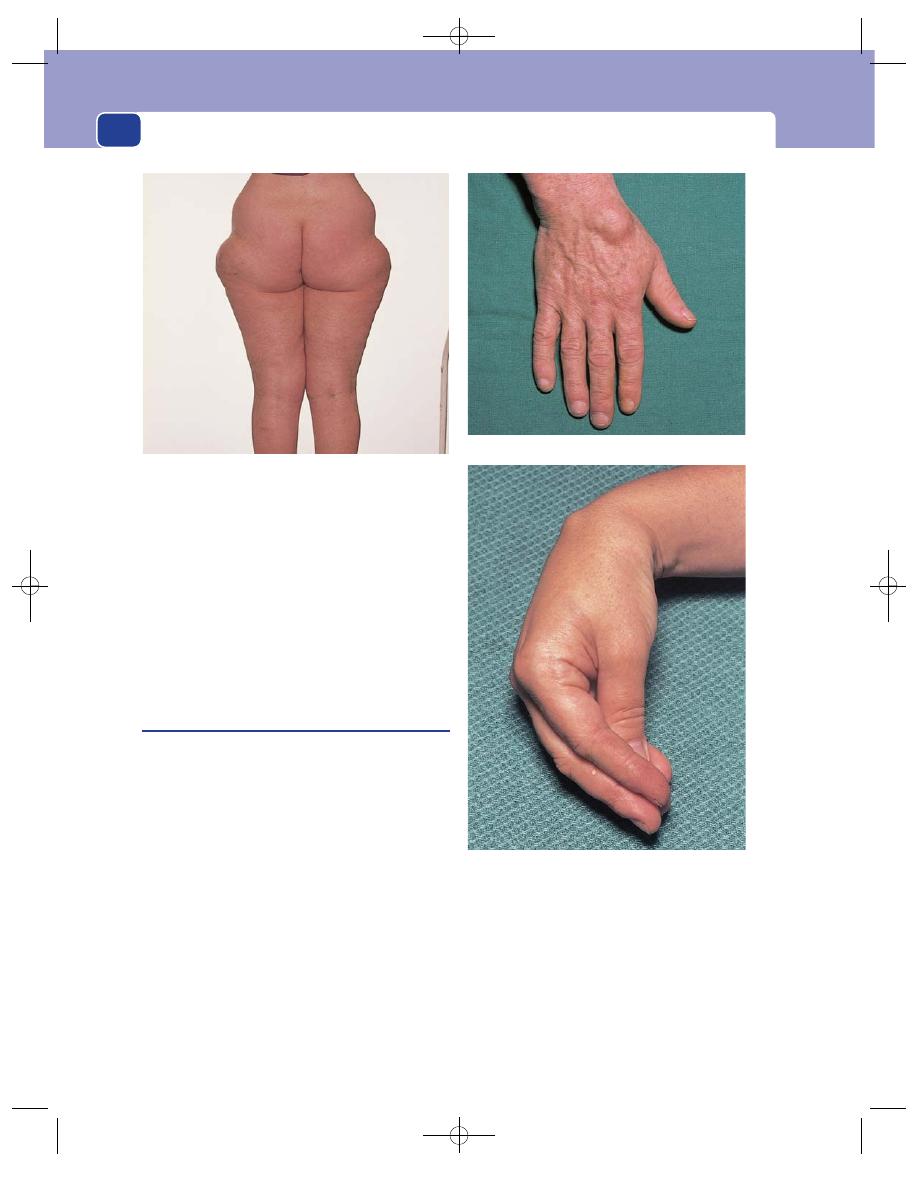
The skin and subcutaneous tissues
80
and may become more prominent if they are pushed
out of the muscle, or disappear if they are drawn
into the muscle when it contracts.
Subcutaneous lipomata are not attached superfi-
cially or deeply and can be moved in all directions.
Lymph drainage
The regional lymph glands should
not be enlarged.
Local tissues
The surrounding tissues should be nor-
mal, but there may be other lipomata nearby.
Ganglion
A ganglion is a cystic, myxomatous degeneration of
fibrous tissue. Ganglia can occur anywhere in the
body, but they are common where there is a lot of
fibrous tissue, i.e. around the joints. Ganglia are not
pockets of synovium protruding from joints.
History
Age
The majority present between the ages of 20
and 60 years and they are rare in children.
Duration
They grow slowly over months or years.
Symptoms
A ganglion is not painful. Most patients
seek advice because they wish to know the diagnosis
or because the lump is disfiguring. Some ganglia
slip away between neighbouring bones, so giving
the false impression that they are reducing into the
joint, but a true ganglion should not connect with
or empty into a joint. Ganglia may be injured
and rupture into the subcutaneous tissues and not
reappear.
Examination
Site
Most ganglia are found near joint capsules
and tendon sheaths, but they can occur anywhere.
FIG 3.30
Diffuse lipomatosis over both hips.
A soft multilocular ganglion on the back of the wrist.
A small, tense ganglion on the back of the wrist which was
only clearly visible and palpable when the wrist was flexed.
FIG 3.31
GANGLIA.
Chap-03.qxd 4/19/05 13:43PM Page 80
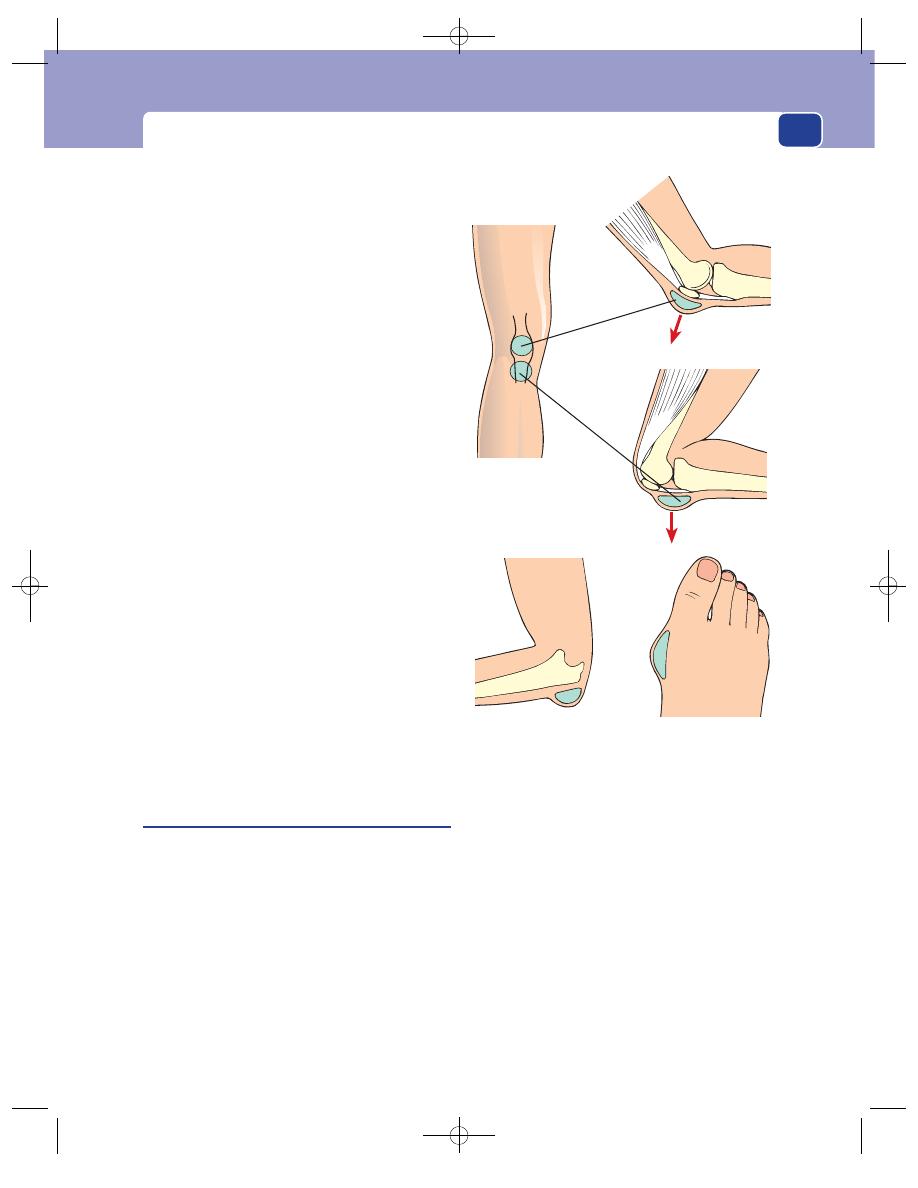
Benign subcutaneous swellings
81
Ninety per cent arise on the dorsal and ventral sur-
faces of the wrist joint and hand.
Shape and size
Ganglia are spherical. Some are mul-
tilocular and feel like a collection of cysts.
They come in all sizes. Small ganglia (0.5–1.0 cm)
tend to be tense and spherical. Large ones, which
can be up to 5–6 cm across, are flattened and soft.
Surface
They have a smooth surface.
Composition
Ganglia feel solid but their consistence
can vary from soft to hard. The gelatinous material
within them is very viscous, but most ganglia fluc-
tuate, provided they are not very small or very tense.
They usually transilluminate brilliantly.
Reducibility
A ganglion may slip away between deeper
structures when pressed, giving the false impression
that its contents have reduced into the joint.
Relations
Ganglia are usually attached to the fibrous
tissue from which they originate. They are not
attached to the overlying skin, which should be freely
mobile over them. The mobility of a ganglion
depends on the extent and nature of its deep attach-
ment. When the tissue of origin is part of a joint cap-
sule, tendon sheath or intramuscular septum, the
ganglion becomes less mobile when these structures
are made tense. Therefore remember to palpate gan-
glia in all positions of the underlying joint and with
the surrounding muscles relaxed and tense.
Differential diagnosis
The three common swellings
found close to joints are bursae, cystic protrusions
of the synovial cavity of arthritic joints, and ganglia.
The first two are usually soft; the ganglion is tense.
With the first and third, the joint is normal.
Subcutaneous bursae
Bursae are fluid-filled cavities, lined with a flattened
endothelium similar to synovium, that develop
between tendons, bones and skin to allow easier
movement between them. There are a considerable
number of bursae that are always present and
described in anatomical textbooks, but others may
develop wherever there is friction between two lay-
ers of tissue. These are called adventitious bursae.
History
Age
Bursae are uncommon in the young unless they
have a skeletal deformity. They usually appear in
middle and later life as a result of prolonged friction
between skin and bone, associated with the patient’s
occupation or with a deformity produced by injury
or arthritis.
Symptoms
Pain and an enlarging swelling at the site
of repeated trauma are the common presenting
symptoms. A severe throbbing pain and a rapid
increase in size indicate the presence of infection.
When the bursa is an occupational hazard –
such as housemaid’s knee – it may stop the patient
working.
Development
The growth of the swelling is usually
rapid, even though the bursa has probably been
Olecranon bursa
(student’s elbow)
Housemaid‘s
knee
Bunion
Clergyman‘s
knee
FIG 3.32
The common adventitious bursae.
Chap-03.qxd 4/19/05 13:43PM Page 81
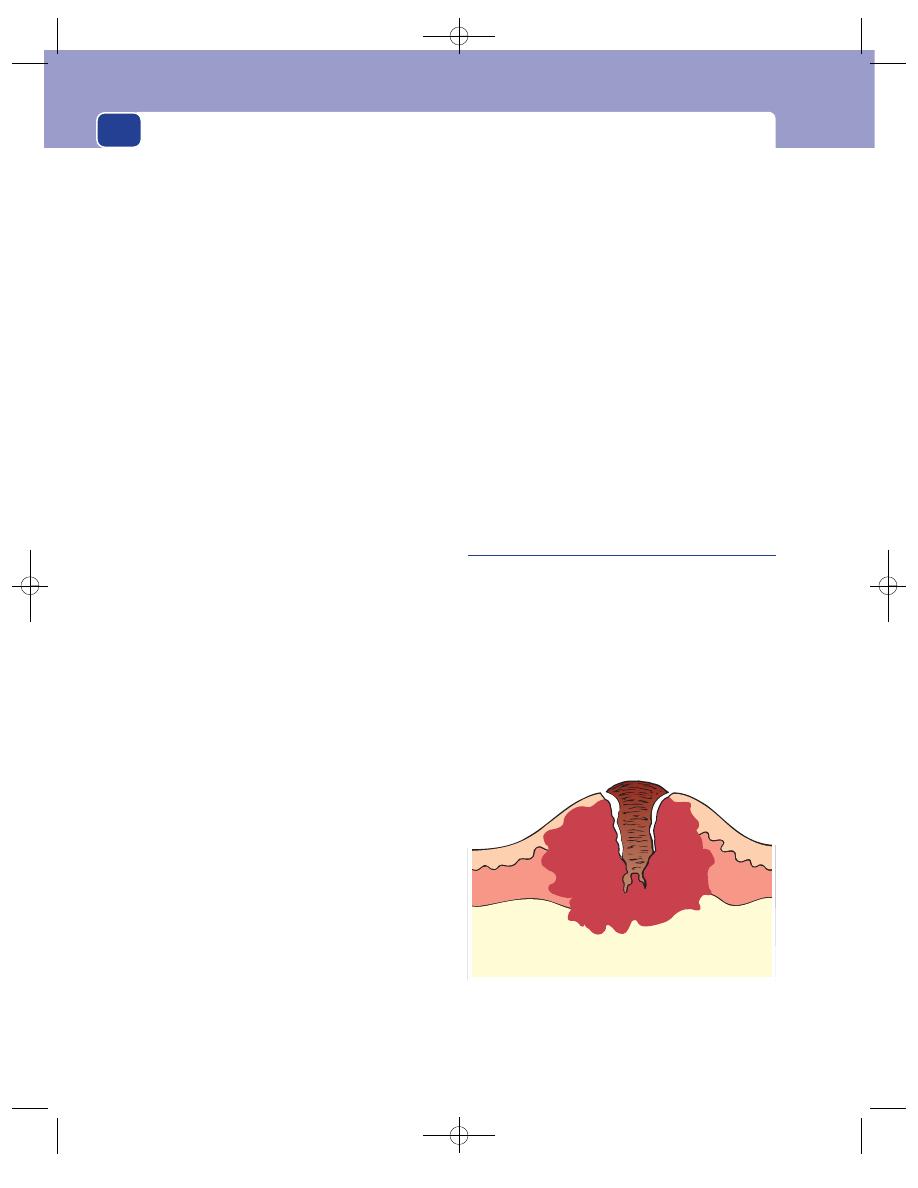
The skin and subcutaneous tissues
82
present in its normal, almost empty, state for many
years. A sudden increase in the quantity of fluid in
the bursa that makes it enlarge is usually secondary
to minor infection or trauma.
Multiplicity
Bursae are often symmetrical, e.g. on
both knees or elbows.
Cause
The patient often knows the cause of the
swelling (prolonged friction or a skeletal deformity)
and may have had a similar complaint before.
Examination
Site
Subcutaneous bursae occur where there is fric-
tion between skin and bone. The common sites are:
■
between skin and olecranon – student’s elbow,
■
between skin and patella – housemaid’s knee,
■
between skin and patellar ligament –
clergyman’s knee,
■
between skin and head of first metatarsal –
bunion.
Shape and size
Bursae are usually circular in outline
with an indistinct edge, but their depth, or thick-
ness, can vary from a few millimetres to 3–4 cm.
Surface
The texture of the surface of a bursa is diffi-
cult to assess because it is intimately attached to the
overlying skin. When the skin is not attached to the
bursa, the surface feels smooth.
Colour
They are covered with skin that has been
repeatedly rubbed and worn, so it is always thick-
ened, shiny, white and cracked.
Tenderness
Bursae are only tender if they are very
tense or inflamed. When they become inflamed, the
overlying skin turns red and hot.
Composition
Bursae contain a clear viscous fluid,
similar to synovial fluid, that gives them a soft or
spongy consistence. They fluctuate, transilluminate
and may have a fluid thrill. These signs may be diffi-
cult to elicit if the wall of the bursa is thick or the
quantity of fluid small.
Relations
As a subcutaneous bursa develops between
two moving tissue planes to reduce the amount of
friction between them, the deep and superficial sur-
faces of a bursa are usually firmly attached to the two
tissues it separates, so that the friction occurs between
the lubricated inside surfaces of the bursa. This makes
the bursa immobile and the walls impalpable.
State of local tissues
The bones and joints beneath
the bursa must be carefully examined because a bursa
may have developed to ease the movement of the
skin over a skeletal abnormality such as an exostosis
or deformed joint. The overlying skin is often horny
and cracked.
Complications
Bursae can become inflamed by repeated
trauma and by conditions which cause inflammation
of synovial surfaces, such as rheumatoid arthritis
and gout. They also get infected from organisms cir-
culating in the bloodstream.
General examination
Even though the patient com-
plains of one lump, examine the same spot on the
other limb because it is quite likely that they have
symmetrical lesions. Also look for other skeletal
abnormalities and joint diseases.
Keratoacanthoma
(Adenoma sebaceum, molluscum
pseudo-carcinomatosum)
This is a self-limiting overgrowth and subsequent
spontaneous regression of hair follicle cells. Because
it grows rapidly, it is often mistaken for a squamous
cell carcinoma.
History
Keratoacanthomata occur in adults, who complain
of a rapidly growing lump in the skin. They are not
painful, but can be very unsightly. The lump takes
2–4 weeks to grow and 2–3 months to regress. The
FIG 3.33
A keratoacanthoma is an overgrowth of hair follicle
cells which produce a central plug of keratin. When the plug
separates, the lesion usually undergoes spontaneous
regression.
Chap-03.qxd 4/19/05 13:43PM Page 82
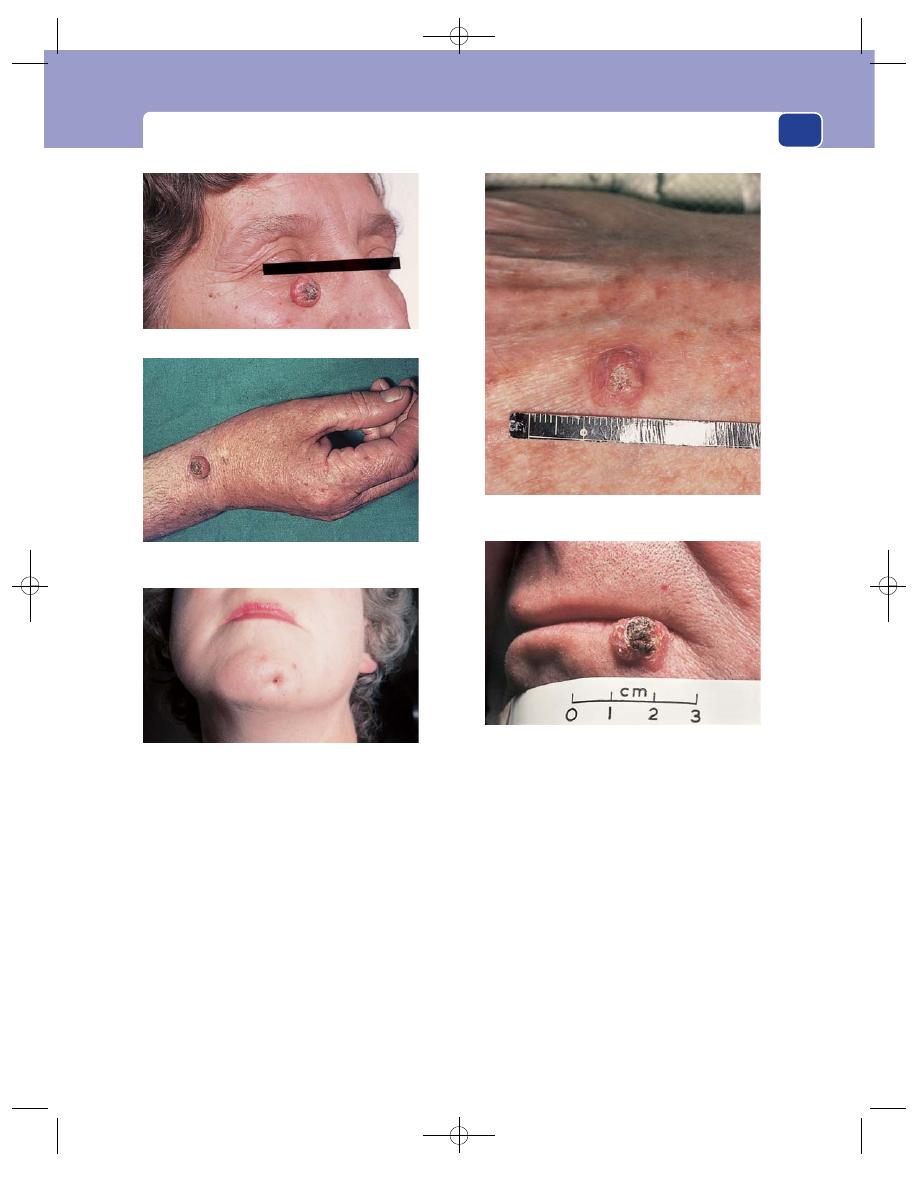
Benign subcutaneous swellings
83
cause is unknown. It may be a self-limiting benign
neoplasm or an unusual response to a viral infection.
Examination
Site
Keratoacanthomata are often found on the face
but they can occur anywhere where there are seba-
ceous glands. They are usually solitary.
Shape and size
The lump is hemispherical or conical
and looks like a volcano when the central slough
appears and the surrounding skin retracts.
The nodule is usually 1–2 cm in diameter by the
time the centre of the lump begins to necrose.
Consistence
The bulk of the lesion is firm and rub-
bery, but the central core is hard.
Colour
The lump has a normal skin colour, but the
necrotic centre is brown or black.
Relations
The lump is confined to the skin and is
freely mobile over the subcutaneous tissues.
Lymph drainage
The local lymph glands should not
be enlarged.
Natural history
The central core eventually separates
and the lump collapses, leaving a deep indrawn
scar. In spite of this self-limiting natural history,
FIG 3.34
KERATOACANTHOMATA.
A large keratoacanthoma on the face.
A keratoacanthoma on the wrist. The slough is just
beginning to separate.
A keratoacanthoma that is beginning to collapse, the
slough having separated.
The end result if the lesion is not excised – a deep,
puckered scar.
A close-up view of the slough.
Chap-03.qxd 4/19/05 13:43PM Page 83
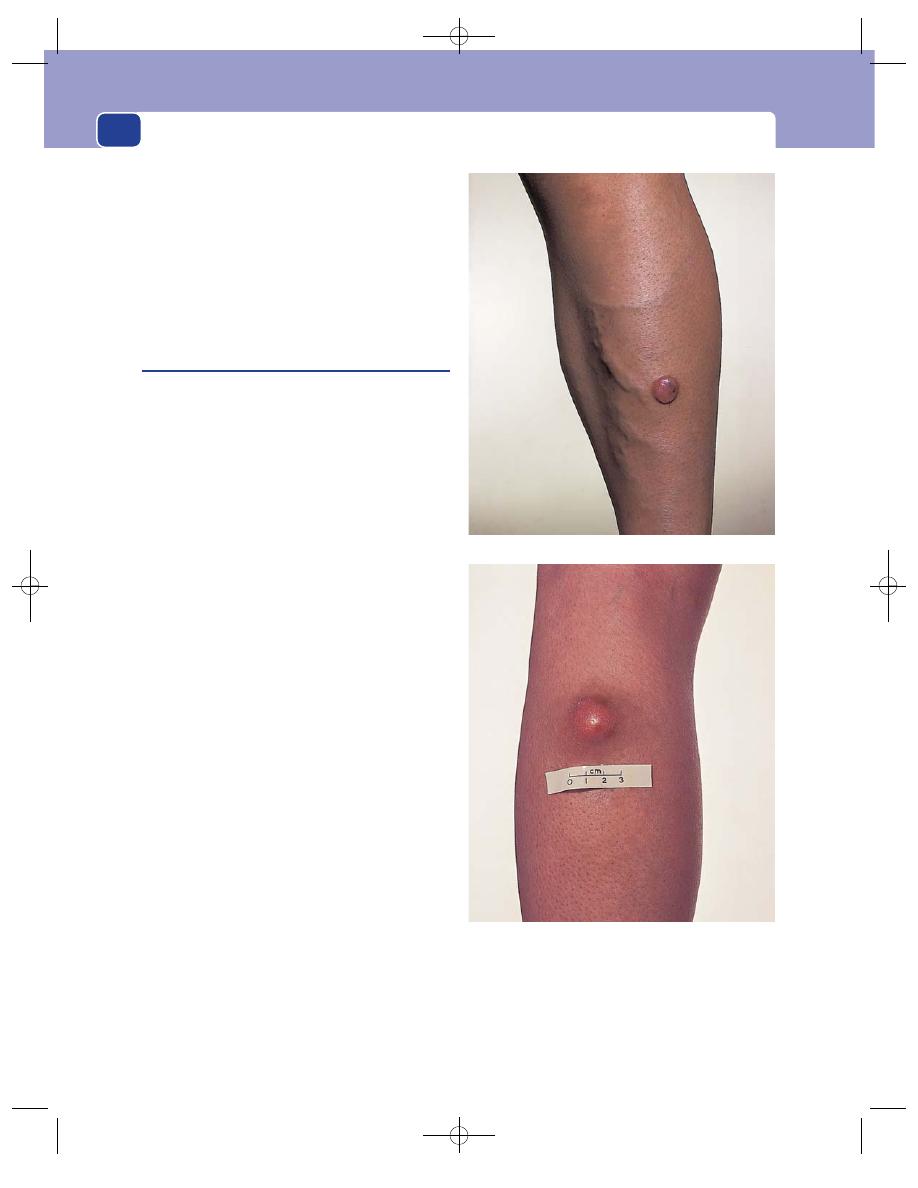
The skin and subcutaneous tissues
84
keratoacanthomata are usually excised to confirm
the diagnosis.
Differential diagnosis
A keratoacanthoma must be
differentiated from a squamous cell carcinoma. The
latter grows more slowly and eventually becomes an
ulcer. The diagnosis is confirmed by a pathologist
after an excisional biopsy.
Hystiocytoma
(Dermatofibroma, sclerosing angioma)
This is a benign neoplasm of the fibroblasts of the
dermis. Its name is derived from the many histio-
cytes that are present between the fibroblasts. The
overlying epidermis is normal. It has also been sug-
gested that this may be an haemangioma with a
marked desmoplastic response.
History
Age
Histiocytomata appear on the skin of young and
middle-aged adults.
Sex
Both sexes are equally affected.
Symptoms
The patient complains of a slow-growing
lump on the skin. The rate of growth is so slow that
the lump may take years to reach a size sufficient to
excite the patient’s curiosity or get in the way of
clothing.
There are no associated general symptoms.
Examination
Site
Histiocytomata can occur anywhere, but are
slightly more common on the skin of the limbs.
Shape
As they grow, they form a hemispherical lump
which then flattens into a thick disc. The edges of the
disc may overhang its base.
Size
Most patients complain of these tumours when
they are 1–2 cm across, but they can grow to a con-
siderable size if they are neglected.
Surface
The skin covering the lump is often loose
and slightly crinkled, even though it is inseparable
from the lump.
Colour
They are covered by normal-coloured epi-
dermis, which may contain sufficient haemosiderin
to give them a brown colour and therefore the appear-
ance of a mole.
Tenderness
They are not tender.
Composition
These tumours usually have a rubbery
or spongy consistence. They do not fluctuate or
transilluminate.
A histiocytoma of the skin of the lower leg.
A large histiocytoma on the calf.
FIG 3.35
HISTIOCYTOMATA.
Chap-03.qxd 4/19/05 13:44PM Page 84
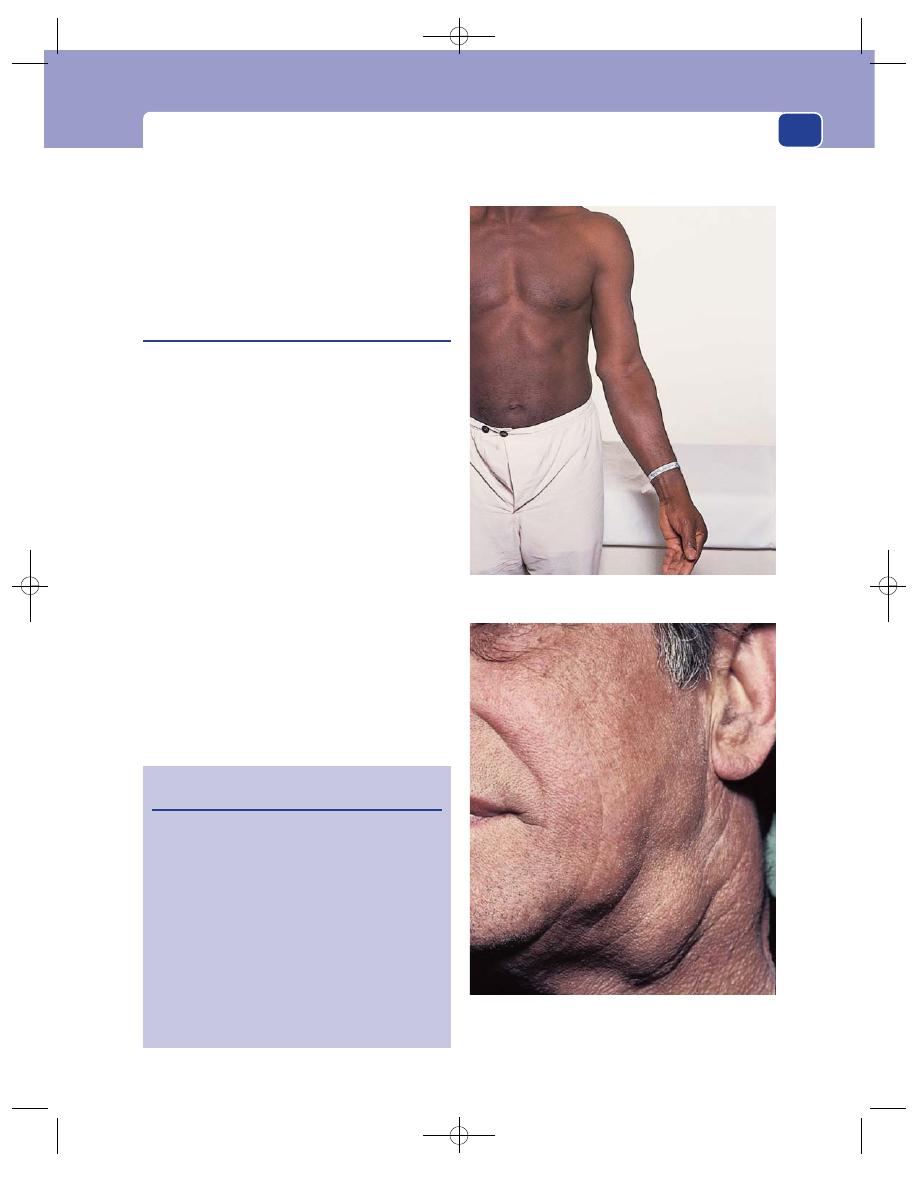
Benign subcutaneous swellings
85
Relations
They are in the skin, separate from and
freely mobile over the deep tissues.
Lymph drainage
The local lymph glands should not
be enlarged.
State of local tissues
The surrounding tissues are
normal.
The lymph glands
The lymph glands which receive lymph from the
skin and the limbs lie in the subcutaneous tissues of
the groins and axillae. The epitrochlear lymph gland
in the arm and the popliteal lymph gland in the leg
are present in most adults and may enlarge before
the axillary or groin glands when there is disease in
the hand or foot.
Lymph glands are enlarged and made tender by
inflammatory conditions, and enlarged by infiltra-
tion with metastatic and primary tumours.
The diagnosis of axillary and inguinal lym-
phadenopathy depends as much on the site of the
swellings as on the presence of multiple firm lumps
in the subcutaneous tissues.
It is difficult to misdiagnose axillary or inguinal
lymphadenopathy, but enlargement of the cervical
lymph glands can be difficult to diagnose and is dis-
cussed in Chapter 11.
When examining the lymph glands, it is impor-
tant to examine all sites containing lymph glands
which might be palpable, i.e. the neck, both axillae,
both groins and the abdomen.
Revision panel 3.5
The causes of enlargement of lymph glands
Infection
Non-specific
Glandular fever
Tuberculosis
Syphilis
Lymphogranuloma
Metastatic tumour
Primary reticuloses
Lymphoma
Lymphosarcoma
Reticulosarcoma
Sarcoidosis
An enlarged epitrochlear lymph gland. The patient had a
non-Hodgkin’s lymphoma.
Multiple enlarged upper cervical lymph glands. The patient
had a carcinoma of the nasopharynx.
FIG 3.36
LYMPH GLANDS.
Chap-03.qxd 4/19/05 13:44PM Page 85
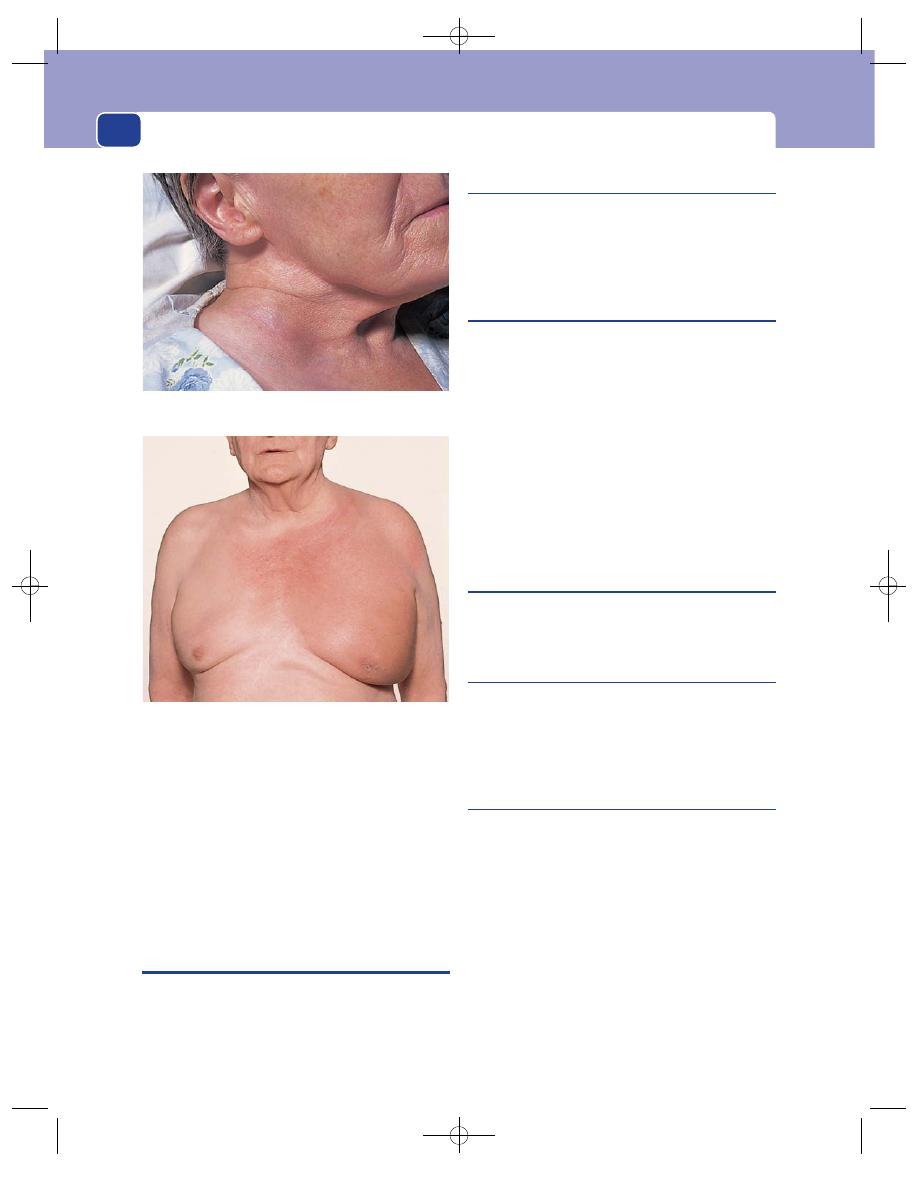
The skin and subcutaneous tissues
86
The size and shape of the glands should be
recorded. Enlarged glands may be solitary or multiple;
clearly defined, indistinct or ‘matted’ together; hard,
rubbery or soft; tender or painless.
Whenever a lymph gland is found to be enlarged,
the area of tissue it drains should be carefully
examined.
TUMOURS OF THE SKIN APPENDAGES
These arise from the sebaceous glands, sweat glands,
apocrine glands and hair gland cells. Most are
benign and have exotic names. Five to ten per cent
are malignant.
Sebaceous gland tumours
These include the naevus sebaceous of Jadassohn,
sebaceous adenoma and sebaceous carcinoma,
which is rare. They are all solitary subcutaneous
tumours that are either soft and warty, or firm.
Sweat gland tumours
These include the eccrine poroma, the spiradenoma
and the acrospiroma. These all present as solitary
subcutaneous lumps, which can be reddish-pink,
red-blue or stain coloured.
Syringomata also arise from the sweat glands and
present as multiple flesh-coloured or yellow papules on
the faces of women. Cylindromata (turban tumours)
are rare tumours that arise from the sweat glands of
the head and scalp. They present as solitary or multi-
ple, pink, spherical or slightly flattened nodules, which
may coalesce to look like a turban, hence the com-
mon name. They are soft with an ill-defined edge.
The apocrine gland tumours
These include the apocrine hydrocystoma and the
syringocystadenoma papilliferum.
The hair gland tumours
These include the trichofolliculoma, the trichoep-
ithelioma, the trichilemmoma and the piloma-
trixoma. All arise as subcutaneous pink, brown or
red/white nodules at different parts of the body.
Sporadic neurofibroma
Multiple familial neurofibromatosis (Von Recklin-
hausen’s disease) is discussed on page 50.
Sporadic neurofibromata are benign tumours
which contain a mixture of neural (ectodermal) and
fibrous (mesodermal) elements. They are often
multiple.
The tumours that are derived from nerve sheaths
(the neurilemmoma, also known as schwannoma),
are very rare.
History
Age
Neurofibromata can appear at any age but usu-
ally present in adult life.
An enlarged right supraclavicular lymph gland. The patient
had a carcinoma of the right breast.
Enlarged left supraclavicular and axillary lymph glands
causing oedema of the arm and chest wall. The patient had a
lymphosarcoma.
FIG 3.36
continued
Chap-03.qxd 4/19/05 13:44PM Page 86
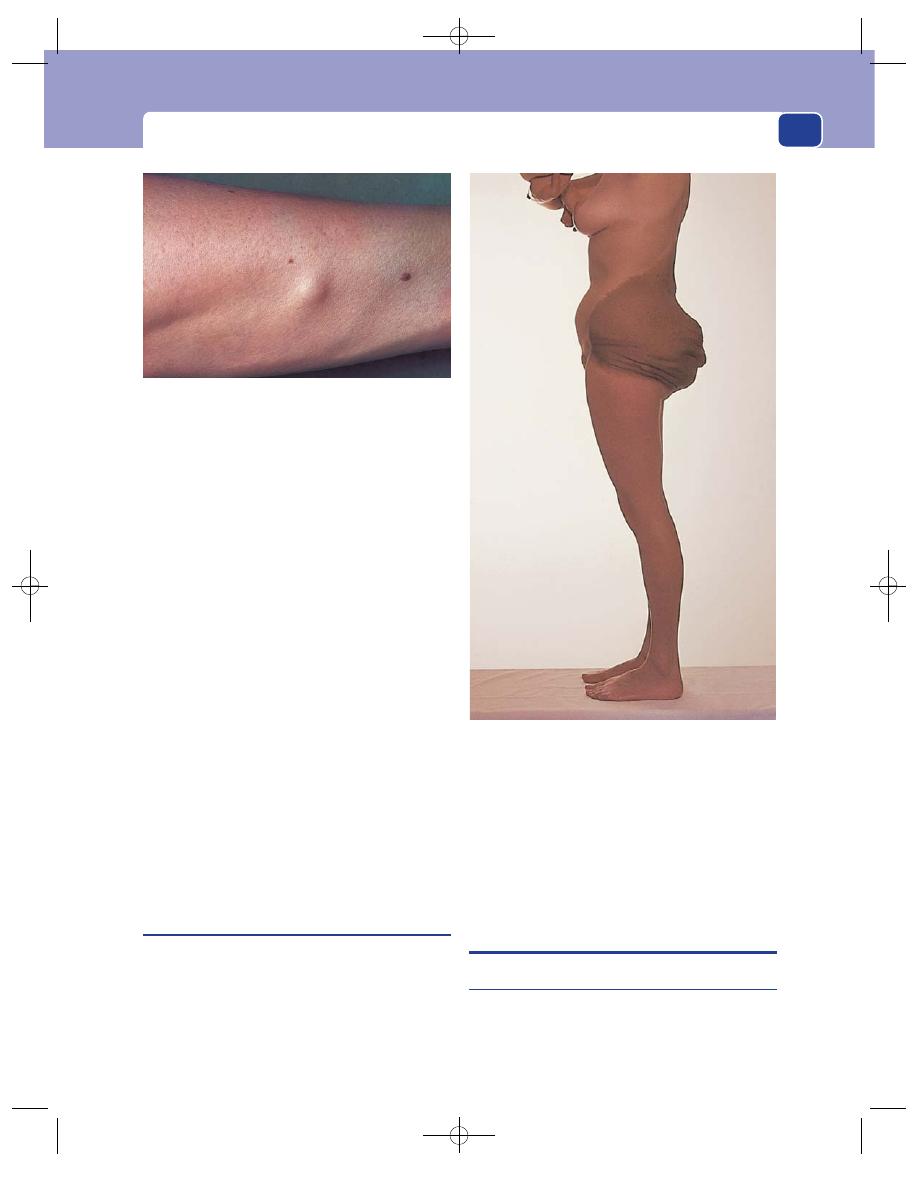
Pre-malignant skin lesions
87
Symptoms
Most neurofibromata cause no discom-
fort and are rarely big enough to be disfiguring. If
they are related to a nerve trunk, they may be tender
and the patient may get tingling sensations in the
distribution of the affected nerve.
Multiplicity
Neurofibromata are often multiple.
Examination
Site
They can occur anywhere in the skin and sub-
cutaneous tissues. The forearms seem to be most
often affected, perhaps because they are the part of
the body most frequently palpated by the patient.
Shape and size
Neurofibromata are usually fusiform,
with their long axes lying along the length of the
limb. They are rarely more than a few centimetres in
length.
Composition
They have the consistence of firm rub-
ber and are dull to percussion.
Relations
The surrounding structures are normal.
Subcutaneous neurofibromata are mobile within
the subcutaneous tissues but move most freely in a
direction at right-angles to the course of the nerve
to which they are connected.
Plexiform neurofibroma
Although this is a very rare condition, it is men-
tioned because it is one of those conditions that
cause considerable diagnostic confusion if the doc-
tor has never heard of it.
It is an excessive overgrowth of neural tissue in the
subcutaneous layers which gives the tissues a swollen
and oedematous appearance. It is sometimes called
elephantiasis neurofibromatosis. It is often misdi-
agnosed as lymphoedema, but the lymphatics are
normal. Remember it when presented with a child
with an apparent overgrowth of the soft tissues of
the hand or foot. The diagnosis can only be made by
the pathologist.
PRE-MALIGNANT SKIN LESIONS
Solar keratosis
Prolonged exposure of the skin to sunlight can cause
areas of hyperkeratosis of the skin, which may
undergo malignant change.
FIG 3.37
A neurofibroma on the leg of a patient with five
other similar lesions.
FIG 3.38
A very dark brown area of pigmentation over an
extensive mixed plexiform neurofibroma and haemangioma.
Chap-03.qxd 4/19/05 13:44PM Page 87
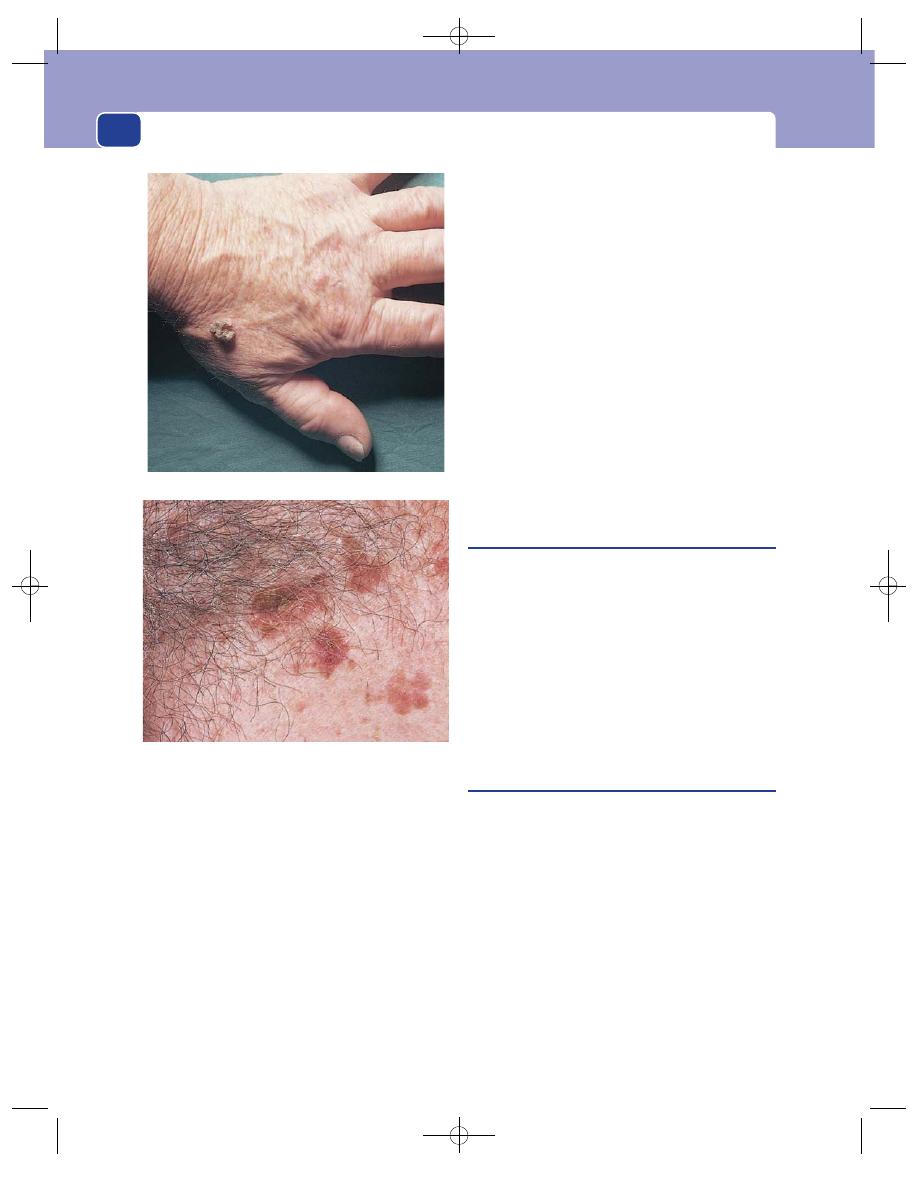
The skin and subcutaneous tissues
88
History
The patient notices the gradual appearance of
thickened patches of skin, which are not painful but
can become unsightly.
Natural history
Solar keratoses grow slowly and the
patients, usually elderly men who have worked out
of doors for many years, ignore them. These lesions
must be watched carefully for any change in size or
appearance.
Examination
Site
Solar keratoses are commonly found on the
backs of the fingers and hands, on the face and on
the rim of the ears.
Shape and size
Beneath their horny surface layer
there is a raised plaque of skin which may vary in
diameter from a few millimetres to 1 cm and pro-
trude above the skin surface. The whole of the strip
of skin along the rim of the pinna may be affected.
Colour
The thickened patches of skin have a yellow-
grey or red-brown colour.
Composition
The keratinous layer is very hard and
clearly part of the underlying skin.
Relations
Solar keratoses are confined to the skin. If
a nodule or patch is tethered to the underlying
structures, it has turned into a squamous carcinoma
and is infiltrating deeply.
Lymph drainage
The local lymph glands should not
be enlarged. If they are, one of the keratoses has
probably become a squamous cell carcinoma.
Bowen’s disease
This also is a pre-cancerous lesion. It presents as a
cluster of flat, pink, papular patches which are
covered with crusts. The patches and the adjacent
skin have a pale-brown, thickened appearance.
Patients usually believe they have a patch of eczema.
When the crusts are removed, the papules can be
seen to have a wet, oozy, slightly bloody, papillifer-
ous surface.
When in any doubt about a chronic skin lesion, it
is wise to carry out a biopsy.
Hutchinson’s lentigo
This eponym is used to describe a large area of pig-
mentation which commonly appears and slowly
enlarges on the face and neck in late (after the age of
60) adult life. The surface is smooth but there may be
raised, rough nodules, which correspond to areas of
junctional activity and become the sites of malignant
change, alongside pale areas of regression. Because
the background pigmentation is so dark, areas of
malignant change causing an increase in pigmenta-
tion but no thickening may pass unnoticed.
It is worth using the eponym to remind you that
this mole is different from other moles because of
two special features: its late development and its
high incidence of malignant change. Some patholo-
gists believe that this variety is pre-malignant or
A solar keratosis on the back of the hand.
Bowen’s disease on the skin of the chest.
FIG 3.39
PRE-CANCEROUS CONDITIONS OF THE SKIN.
Chap-03.qxd 4/19/05 13:44PM Page 88
Malignant diseases of the skin
89
actually malignant from the start, an example of
malignant change ‘in situ’.
MALIGNANT DISEASES OF THE SKIN
Basal cell carcinoma
(Rodent ulcer)
This is a locally invasive carcinoma of the basal layer
of the epidermis. It does not metastasize, but can infil-
trate adjacent tissues. It is common in exposed skin,
especially in countries where there is a high incidence
of ultraviolet irradiation, i.e. bright sunlight.
History
Age
The incidence of basal cell carcinoma increases
with age because it is related to the duration of
exposure of the skin to ultraviolet light.
Geography
It is more common in countries that have
much bright sunlight.
Ethnic group
Basal cell carcinomata are rare in dark-
skinned races.
Sex
Males are affected more often than females.
Duration
Basal cell carcinomata grow very slowly
and have usually been present for months or years
before the patient seeks advice.
Symptoms
The principal complaint is of a persistent
nodule or an ulcer with a central scab that repeatedly
falls off and then re-forms. The lesion grows slowly
but eventually becomes disfiguring and annoying.
It may itch. It may cause pain and, if it is neglected,
becomes a deep infected ulcer. A large, neglected
ulcer destroying one side of the face is now rare.
Development
The lesion grows very slowly and may
have been present for months or years before the
patient complains about it. This long history gives
the patient a false impression that the lesion is
benign and unimportant.
Persistence
Some basal cell carcinomata spread radi-
ally through the skin, leaving a central scar.
Multiplicity
Basal cell carcinomata are often multiple.
Predisposing factors
Skin that has been treated with
arsenic, once a common ingredient of skin oint-
ments, is liable to develop basal cell carcinomata.
Examination
Site
Basal cell carcinomata are commonly found on
the face above a line drawn from the angle of the
mouth to the lobe of the ear. This does not mean
that they do not occur in other sites; all skin is sus-
ceptible, particularly the skin of the scalp, neck,
arms and hands.
Size
Most patients complain of the nodule or ulcer
when it is quite small, but basal cell carcinomata can
grow to a considerable size if they are neglected. A few
grow outwards from the skin to become a fungating
mass on the skin surface, but the majority erode
deeply, destroying the underlying tissues and form-
ing a deep cavity – hence the name ‘rodent’.
Shape
Some of the many macroscopic appearances
of basal cell carcinomata are shown in Figure 3.41.
Only two are true ulcers, so it is better to use the
term ‘basal cell carcinoma’, not ‘rodent ulcer’. The
Revision panel 3.6
The clinical appearances of basal cell
carcinomata
Nodule
‘Cystic’ (a large, seemingly transparent nodule)
Ulcer
Deeply eroding ulcer: the ‘rodent’ ulcer
Pigmented nodule
Geographical (advancing edge, healing centre)
FIG 3.40
Basal cell carcinomata commonly appear in the
shaded area.
Chap-03.qxd 4/19/05 13:44PM Page 89
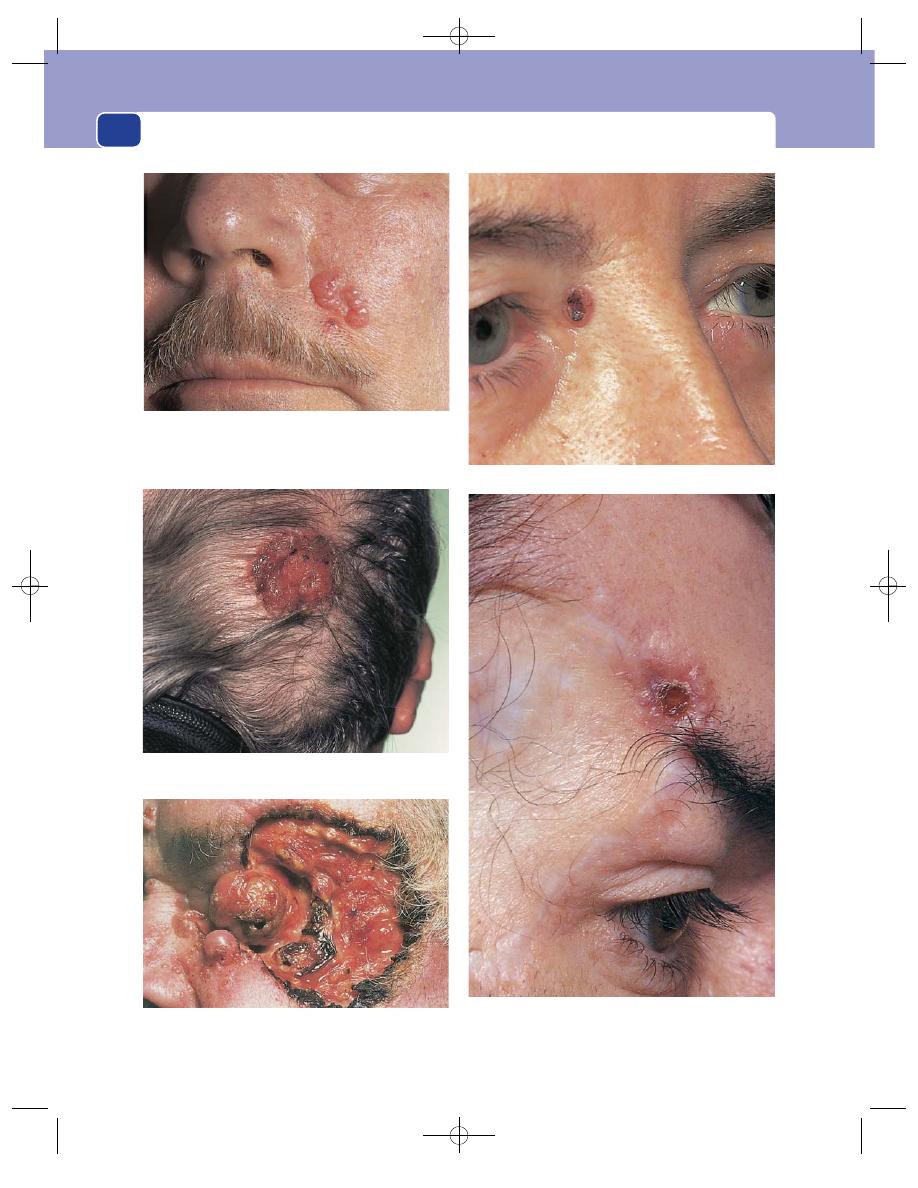
The skin and subcutaneous tissues
90
FIG 3.41
BASAL CELL CARCINOMATA.
A slow-growing lesion on the cheek. This type of lesion is
difficult to see and often ignored by the patient, who notices
only a small scab (which periodically appears and then falls
off) at the centre of a slightly thickened area of the skin.
A raised, wet, weeping basal cell carcinoma that was thought
by the patient to be a patch of eczema.
A true ‘rodent ulcer’. The basal cell carcinoma has destroyed
the orbit and the eye.
A pigmented basal cell carcinoma.
A recurrent basal cell carcinoma at the edge of a skin graft
placed to cover the skin defect of a previous excision 7 years
earlier.
Chap-03.qxd 4/19/05 13:44PM Page 90
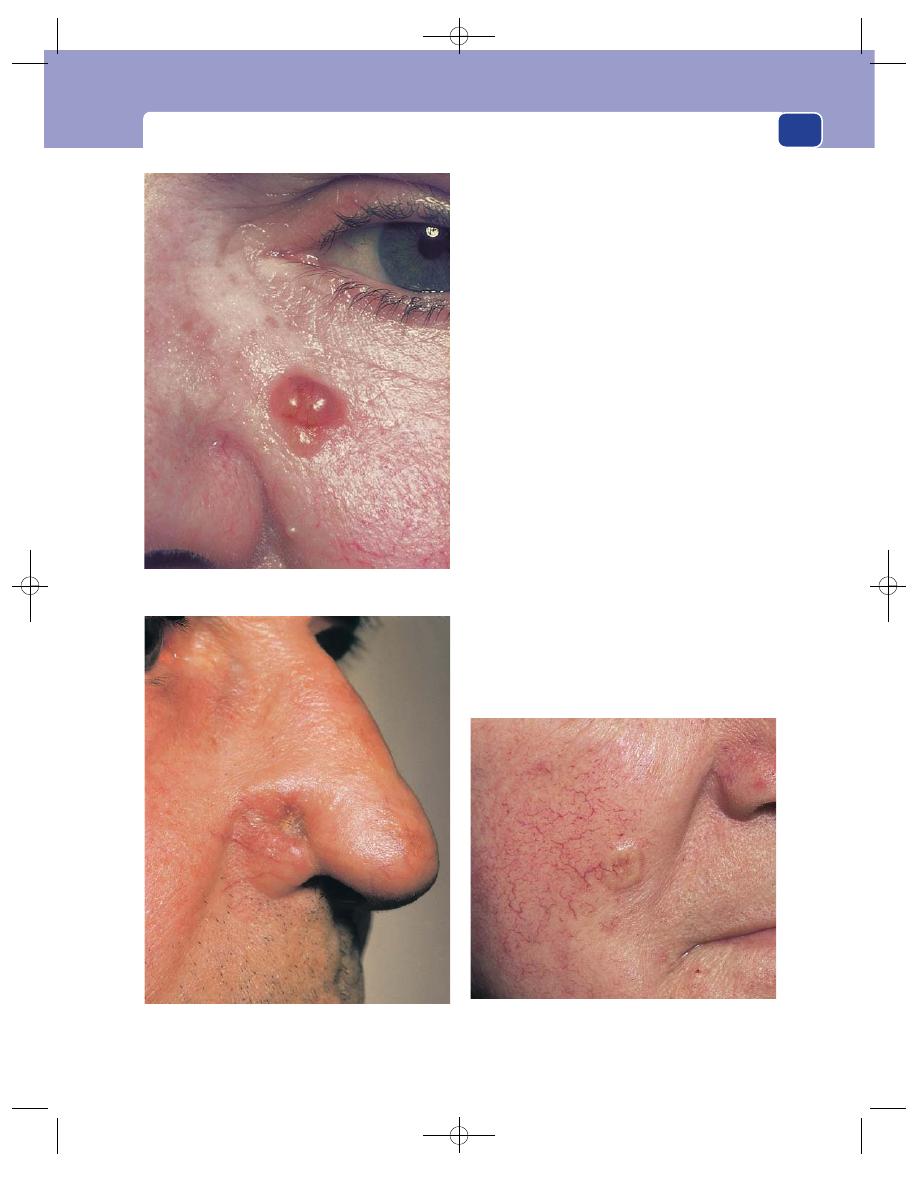
Malignant diseases of the skin
91
tumour always starts as a nodule. When the central
epithelium dies, the resulting ulcer develops a rolled
edge. This means that the edge is raised up and
rounded but not everted. If the centre of the tumour
does not necrose and ulcerate, the nodule can
become quite large and look like a cyst. It is not cys-
tic, however, because it is solid and non-fluctuant,
but the term ‘cystic rodent ulcer’ is unfortunately
sometimes used to describe this appearance.
Colour
The raised portion of the lesion – that is to
say, its edge if it is annular, or its centre if it is a nod-
ule – is smooth, glistening and slightly transparent.
This gives the impression that there are pearl-white
nodules of tissue just below the epidermis. These
nodules also give the ulcerating variety its typical
‘rolled edge’.
The whole lesion may be coloured brown by
excess melanin.
Surface
The surface of the nodular variety is covered
by fine, distinct blood vessels, which may give it a
pink hue.
Edge
When the nodule first ulcerates, the rolled
edge is circular, but as the malignant cells spread,
the shape of the ulcer becomes irregular. The raised
edge may be the only clue to the diagnosis if the
ulcer heals. An irregular raised edge around a flat
white scar is sometimes called a ‘geographical’ or
FIG 3.41
continued
An early nodule just below the eye. These nodules are
sometimes mistakenly thought to be cystic.
A lesion with a deep, scarred centre without a noticeably
raised edge.
A nodular lesion spreading outwards and leaving a collapsed,
scarred centre.
Chap-03.qxd 4/19/05 13:44PM Page 91
The skin and subcutaneous tissues
92
‘forest fire’ basal cell carcinoma. When the ulcer
erodes into deeper structures, the edge becomes
more prominent and florid but not everted.
Base
The base of a small rodent ulcer is covered
with a coat of dried serum and epithelial cells and
will bleed slightly if this layer is picked off.
The base of deeply eroding ulcers consists of fat,
bone, muscle, or even the eye, all covered with poor-
quality granulation tissue.
Depth
Long-standing ulcers may erode deep into
the face, destroying skin and bone and exposing the
nasal cavity, air sinuses and even the eye, hence the
name ‘rodent’ because the tissues look as if they have
been gnawed by a rat.
Such extensive lesions are uncommon. Most basal
cell carcinomata are superficial and confined to the
skin.
Lymph drainage
The local lymph glands should not
be enlarged.
Relations
A small tumour is confined to the skin and
is freely movable over the deep structures. Fixation
of the ulcer indicates that it has invaded deeply.
Important differential diagnoses
A rodent ulcer can
resemble a squamous cell carcinoma. The long
history and the rolled edge are the clinical features
that indicate its basal cell origin. A keratoacan-
thoma (see page 82) just beginning to slough at its
centre can also look like an early rodent ulcer but
the short history and the deep slough should sug-
gest the correct diagnosis.
In every instance, the final diagnosis must be made
by the pathologist. Sweat gland tumours and malig-
nant melanomata are other differentiated diagnoses
that should be considered.
Squamous cell carcinoma
(Epithelioma)
This is a carcinoma of the cells of the epidermis that
normally migrate out towards the surface to form the
superficial keratinous squamous layer. The tumour
cells infiltrate the epidermis, the dermis and adjacent
tissues. Microscopic examination reveals tongues of
tumour cells spreading in all directions, and clusters
of cells with concentric rings of flattened squamous
cells at their centre. These onion-like clumps of cells
are often called ‘epithelial pearls’, but are only seen
under the microscope.
History
Age
The incidence of squamous carcinoma of the
skin increases with age.
Causes
Prolonged exposure to sunlight, solar kera-
toses, Bowen’s disease, certain chemicals and irradi-
ation and the presence of old scarring, particularly
following burns, or chronic ulcers are associated with
an increased incidence of squamous carcinomata.
Cancer of the scrotal skin was once common in
chimney sweeps, and still occurs in engineers whose
clothes become soaked in oil.
Duration
The ulcerating tumour has usually been
growing steadily for 1 or 2 months before the patient
complains of it. If it is in an inaccessible part, such
as in the middle of the back, it may grow quite large
before being noticed.
Symptoms
The patient complains of a lump, or of
bleeding and discharge from an ulcer. Bleeding is
more common with squamous cell than basal cell
carcinomata. The tumour may become painful if it
invades deep structures.
Occasionally patients notice enlarged lymph
glands and are unaware of the primary tumour.
There are no systemic effects while the tumour is
confined to the skin. Dissemination of tumour cells
throughout the body is a late event.
Development
The ulcer or nodule enlarges steadily
and inexorably. The edges of a squamous cell carci-
nomatous ulcer become more prominent and florid.
Multiplicity
There may be multiple tumours in skin
affected by exposure to ultraviolet light, such as the
scalp, or chemicals, such as the hands and arms.
Examination
Site
Squamous cell carcinomata can occur on any
part of the skin, but are more common on the
exposed skin of the head and neck, hands, forearms
and upper trunk. They also develop in skin subjected
to repeated chemical or mechanical irritation.
Colour
The everted edge of a carcinomatous ulcer is
usually a dark red-brown colour because it is very
vascular. The whole ulcer may be covered with old
coagulated blood or serum.
Chap-03.qxd 4/19/05 13:44PM Page 92

Malignant diseases of the skin
93
Tenderness
The ulcer is not usually tender.
Shape and size
Squamous carcinomata begin as
small nodules on the skin. As they enlarge, the cen-
tre becomes necrotic, sloughs, and the nodule turns
into an ulcer, which is initially circular with promi-
nent everted edges, but can become any shape as it
enlarges.
Edge
Squamous cell carcinomata have an everted
edge because the excessive tissue growth raises it
above and over the normal skin surface.
Base
The base of the ulcer consists of necrotic
tumour covered with serum and blood. There is
usually some granulation tissue, but this tends to be
pale and unhealthy. Deep tissues may be exposed.
Depth
The depth of the ulcer is affected by the nature
of the underlying tissues and the virulence of the
tumour. Soft tissues are easily invaded and when
they slough they leave a deep ulcer.
Discharge
The discharge can be copious, bloody,
purulent and foul smelling. This is often the patient’s
most depressing and debilitating symptom.
Relations
The relations to nearby tissues will vary
according to the extent of the malignant infiltra-
tion. If the ulcer is immobile, the tumour has spread
beyond the skin and subcutaneous tissues into
deeper structures – tendon, bone and muscle.
Local lymph glands
The local lymph glands are often
enlarged, but this does not always mean that they
contain tumour. In about one-third of patients with
palpable lymph glands, the lymphadenopathy is
caused by infection, which subsides after excision of
the ulcer. Nevertheless it should be assumed that
palpable lymph glands contain metastases.
Local tissues
The surrounding tissues may be oede-
matous and thickened, and subcutaneous spread may
involve nearby nerves. Invasion of local blood vessels
An extensive squamous cell carcinoma of the skin of the
groin and scrotum.
FIG 3.42
SQUAMOUS CELL CARCINOMATA.
An ulcer, on the face, with an everted edge and a necrotic
base.
An ulcer, on the hand, whose edge is not yet everted but is
raised and almost everted on the proximal side.
Chap-03.qxd 4/19/05 13:44PM Page 93
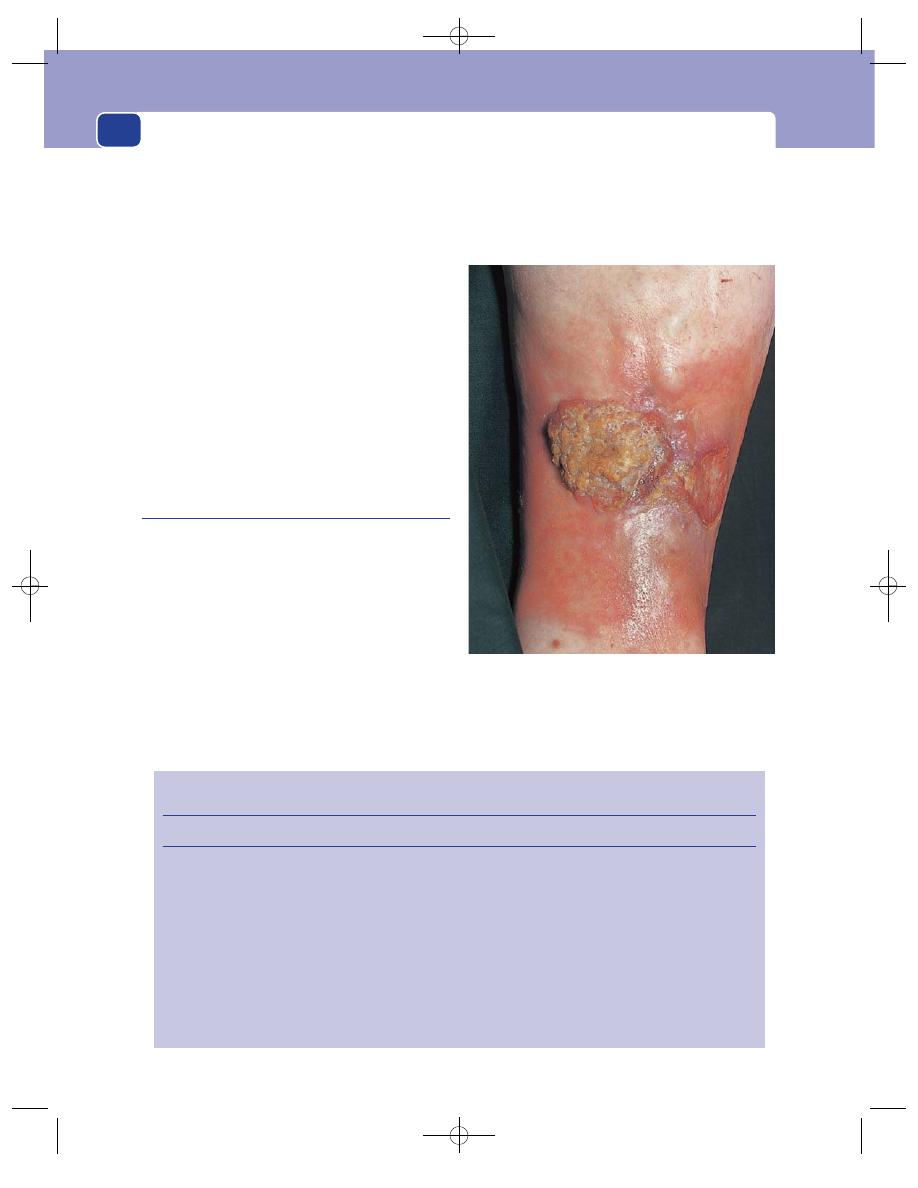
The skin and subcutaneous tissues
94
can cause thrombosis and tissue ischaemia. These
events are features of the late stages of the disease.
Complications
Infection and bleeding are the com-
mon complications. If the ulcer erodes into a large
blood vessel, the bleeding can be massive and fatal.
General examination
All the lymph glands between
the primary lesion and the great veins in the neck
should be examined. Distant metastases are uncom-
mon, but a pleural effusion and hepatomegaly are
indicative of systemic spread.
Differential diagnosis
This includes tumours of the
skin appendages, cutaneous secondary deposits,
basal cell carcinoma, keratoacanthoma, malignant
melanoma, solar keratosis, pyogenic granuloma and
an infected seborrhoeic wart.
Marjolin’s ulcer
(Squamous cell carcinoma)
Marjolin’s ulcer is an eponym reserved for a squa-
mous carcinoma that arises in a long-standing benign
ulcer or scar. The commonest ulcer to become malig-
nant is a long-standing venous ulcer. The scar that is
most often associated with malignant change is the
scar of an old burn.
These carcinomata are very similar to an idio-
pathic squamous carcinoma, except that they may
not be so florid. Their edge is not always raised and
everted, and other features may be masked by the
pre-existing chronic ulceration or scarring.
Unusual nodules or changes in a chronic ulcer or
a scar should be viewed with suspicion, especially
if they increase in size and develop a very smelly
discharge.
FIG 3.43
A Marjolin’s ulcer. The pigmentation and scarring
caused by long-standing venous hypertension and ulceration
can be seen around the patch of hyperplastic neoplastic
tissue.
Revision panel 3.7
The diagnostic features of the four common surgical skin lesions
Duration of growth
Physical features
Squamous cell carcinoma
Few months
Occasional bleeding
Nodule or ulcer with everted edge
Basal cell carcinoma
Many months or years
Nodule or ulcer with rolled edge and
permanent scab
Keratoacanthoma
Few weeks
Nodule with central hard necrotic core
No bleeding
Spontaneous regression
Pyogenic granuloma
Few days
Soft red nodule that becomes covered
with epithelium
Bleeds easily
Chap-03.qxd 4/19/05 13:44PM Page 94
Malignant diseases of the skin
95
Malignant melanoma
Because of the confusion which has arisen from using
the word ‘melanoma’ to describe a benign lesion
and ‘malignant melanoma’ to describe a malignant
one, use the terms mole or pigmented naevus for
benign lesions and malignant melanoma for malig-
nant lesions.
As the melanocyte originates from the neural crest
and so is neuro-ectodermal in origin, it could be
argued that malignant change in melanocytes should
be called a carcinoma. Terms such as ‘melanocarci-
noma’ or even ‘melanosarcoma’ only add to the con-
fusion. It is therefore best to use the well-established
descriptive term ‘malignant melanoma’.
Cardinal symptoms of malignant change
in a mole
■
Change in surface. One of the earliest signs
associated with malignant change is loss of the
normal skin markings (creases) over the mole.
The skin may also become rough and scaly.
■
Itching. This is an early and significant
symptom, often associated with a pale-pink
halo around the mole.
■
Increase in size, shape or thickness. The patient
usually complains that a long-standing mole,
or a recently developed brown spot, has grown
steadily over a period of a few weeks or months.
The mole or part of the mole may become
wider and thicker, often changing from a flat
plaque to a nodule. Alternatively the mole may
simply change in outline.
■
Change in colour. Malignant melanocytes usually
produce more melanin, so the mole gets darker.
The colour change is often patchy, with some
areas becoming almost black, others turning
blue-purple with the increased vascularity,
and some areas not changing at all. Very
occasionally the malignant melanocytes do not
produce melanin, so that the new growth is
colourless.
■
Bleeding. As the tumour cells multiply, the
overlying epithelium becomes anoxic and either
ulcerates spontaneously or breaks down after
a very minor injury. Bleeding is slight and a
late sign.
■
Evidence of local or distant spread. The
pigment produced by the malignant
melanocytes may spread diffusely into the
surrounding skin to produce a brown halo
around the primary lesion. The malignant cells
may also spread through the skin in the
intradermal lymphatics. When they stop
migrating and multiply, they become small
intradermal nodules. Small nodules around the
primary lesion are called satellite nodules.
Occasionally patients notice enlarged lymph
glands in the groin or axilla.
Not all malignant melanomata arise in pre-
existing pigmented naevi. All the changes listed above
can develop in a lesion that appeared quite quickly a
few weeks or months previously.
History
Age
Malignant melanoma is very rare before puberty,
although it has been reported in children. Most cases
occur in patients aged 20–30 years or more.
Sex
Malignant melanoma occurs equally in both
sexes, but is found more often in the lower limbs in
women and on the trunk in men.
Ethnic group
Malignant melanoma is common in
Caucasians and rare in Negroes. People with fair
complexions, red hair and a tendency to freckle are
more susceptible.
Cause
Melanocytes are stimulated by ultraviolet light.
White-skinned people living in those parts of the
world that enjoy abundant sunlight, such as Australia
and the west coast of America, have a high incidence
Revision panel 3.8
The changes which suggest that a mole has
turned malignant
Loss of normal surface markings
(e.g. skin creases)
Change in size, shape or thickness
Change in colour
Itching
Bleeding/ulceration
Halo
Pink (inflammatory reaction) – early
Brown (pigment) – late
Satellite nodules
Chap-03.qxd 4/19/05 13:44PM Page 95
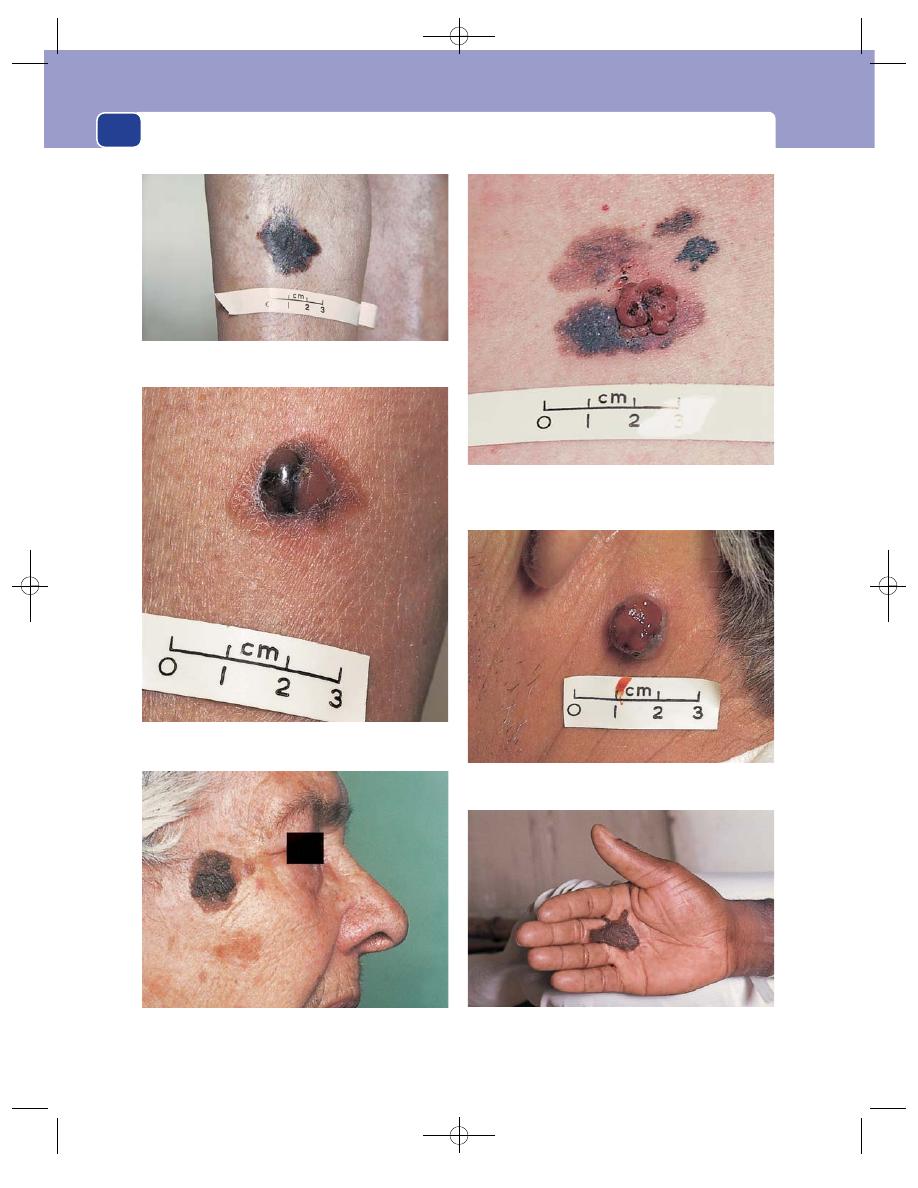
The skin and subcutaneous tissues
96
FIG 3.44
MALIGNANT MELANOMATA.
A superficial spreading melanoma. The lesion is thin, with an
irregular edge and varying degrees of pigmentation.
A superficial spreading melanoma with an amelanotic
nodular area. The nodule had appeared within the previous
month and had itched and bled.
A nodular melanoma arising in a long-standing benign mole
(pigmented naevus).
A large nodular melanoma which arose in previously normal
skin.
Nodules of malignant melanoma arising in a patch of
Hutchinson’s lentigo which had been present for many years.
A malignant melanoma in the palm of the hand of a black-
skinned manual worker.
Chap-03.qxd 4/19/05 13:44PM Page 96
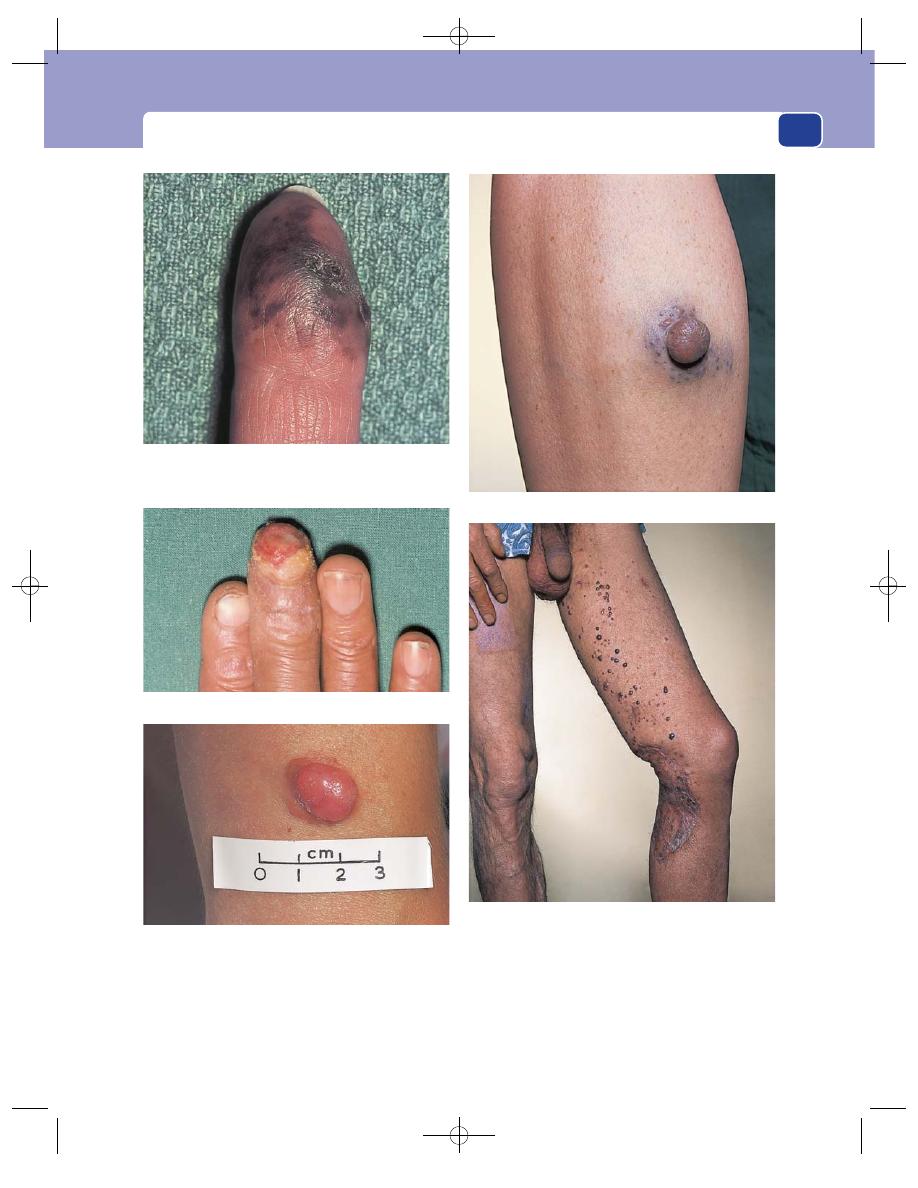
Malignant diseases of the skin
97
of malignant melanoma. Those who work out of
doors in these regions, especially those with a history
of repeated episodes of sunburn, are particularly
susceptible.
Symptoms
The cardinal features have already been
described. The common reasons for seeking medical
advice are a change of size or colour, bleeding, and the
appearance of a brown halo or satellite nodules. It is
An ulcerated melanoma on the tip of the middle finger. The
ulceration and lack of pigmentation caused the referring
physician to think it was a chronic pulp space infection.
An acral lentiginous melanoma of the tip of the index finger.
Multiple metastatic nodules of melanoma that appeared
4 years after the primary lesion (which was behind the knee)
had been excised.
Satellite nodules of tumour cells around a nodular melanoma.
A nodular amelanotic melanoma. This arose in normal skin
and was at first thought to be a histiocytoma.
FIG 3.44
continued
Chap-03.qxd 4/19/05 13:45PM Page 97
The skin and subcutaneous tissues
98
usually the cosmetic disfigurement caused by an
enlarging mole that brings the patient to the doctor,
but more than 25 per cent arise de novo, i.e. in normal
skin rather than in a pre-existing lesion. Malignant
melanomata often itch but are not painful.
Sometimes the patient has observed the changes
described above, but if the mole is on the sole of the
foot or the back of the trunk where it cannot be seen,
the patient may present with lymph gland enlarge-
ment or symptoms caused by distant metastases, such
as weight loss, dyspnoea or jaundice.
Multiplicity
Multiple malignant melanomata are very
rare, but there are often multiple secondary nodules
around a primary lesion Two concurrent primary
lesions are very uncommon.
Examination
Site
The majority of malignant melanomata are
found on the limbs, head, neck and trunk. They are
uncommon on the palms of the hands and the soles
of the feet (except in African Negroes). They may
arise in the subungual tissues, at the mucocutaneous
junction and in the mouth and the anal margin.
Shape and size
When first noticed, the area of malig-
nant change is usually quite small (0.5–2 cm in diam-
eter), but the mole in which the change has begun
may be of any size. When a malignant melanoma is
neglected it becomes a large, florid tumour, protrud-
ing from and overlapping the surrounding skin.
Surface
When the tumour is small it is covered by
smooth epithelium. When the epithelium dies, from
ischaemic necrosis, the resulting ulcer is covered with
a crust of blood and serum. Bleeding and subacute
infection may make the surface of the tumour wet,
soft and boggy.
Colour
Malignant melanomata may be any colour
from a pale pinkish-brown to black. If they have a rich
blood supply, they develop a purple hue. Variations
in the colour are common, some areas being very
black and others pale.
Temperature and tenderness
A malignant melanoma is
no warmer than the surrounding skin, in spite of its
vascularity and cellular activity, and is not tender.
Composition
The primary tumour has a firm consis-
tence. Small satellite nodules feel hard.
Relations
The malignant tissue is within the skin and
moves with it.
Lymph drainage
The local lymph glands may be
enlarged.
Surrounding tissues
There may be a halo of brown
pigment in the skin around the tumour and satellite
nodules in the skin and subcutaneous tissue between
the primary tumour and the nearest lymph glands.
It is important to feel all the subcutaneous tissues
along the course of the lymphatics that drain the
lesion, as nodules of melanoma may be palpable.
Clinical types
Although the above description indicates that a
malignant melanoma may have many forms, there
are four common clinical types.
■
Superficial spreading melanoma is the most
common variety. It may occur on any part of
the body, is usually palpable but thin, with an
irregular edge and a variegated colour.
■
Nodular melanoma is thick and protrudes
above the skin. It has a smooth surface and a
regular outline, and may arise de novo. It may
become ulcerated and then often bleeds.
■
Lentigo maligna melanoma is a malignant
melanoma arising in a patch of Hutchinson’s
lentigo. The malignant areas are thicker than the
surrounding pigmented skin, usually darker in
colour, but seldom ulcerate.
■
Acral lentiginous melanoma is a rare type of
malignant melanoma but important to
remember because it is often misdiagnosed as a
chronic paronychia or a subungual haematoma.
It presents as an irregular, expanding area of
brown or black pigmentation on the palm, the
sole or beneath a nail.
General examination
Malignant melanoma spreads
via the lymphatics to the regional lymph glands. It
may then spread in the bloodstream to the lungs,
liver and brain. Pleural effusions, hepatomegaly,
jaundice and neurological abnormalities are indica-
tions of distant metastases. Blood-borne secondary
deposits in the skin and subcutaneous tissues are
not uncommon.
Mycosis fungoides
This is a rare skin lymphoma but it occasionally
presents in a surgical clinic. It begins as a patch of
Chap-03.qxd 4/19/05 13:45PM Page 98
Other common skin conditions often seen in surgical patients
99
thickening and reddening of the skin which enlarges
into a plaque above the surrounding skin and then
ulcerates. The lesions may be multiple. It is often
associated with a generalized lymphoma.
Kaposi’s sarcoma
Kaposi’s sarcoma is a cutaneous sarcoma which,
before the appearance of human immunodeficiency
virus (HIV) infection, was a rare sporadic condition
in Europe, but not uncommon and endemic in sub-
Saharan Africa, particularly Zaire and Western
Uganda.
The variety not associated with HIV infection
runs a slow, indolent course and is only very rarely
associated with spread to the intestine or general-
ized malignant lymphoma.
The variety associated with HIV infection and
acquired immunodeficiency syndrome (AIDS) runs
an aggressive course and is usually associated with
systemic tumour infiltration of lymph glands, intes-
tine, mucous membranes, lungs and other organs.
History
The patients complain of the presence of painless
nodules or plaques in and beneath the skin, which
often appear first in the legs. There are likely to be a
multitude of systemic symptoms if the patient has
AIDS.
Examination
The nodules are red, hemispherical and painless.
They lie in the subcutaneous tissues, but the overly-
ing skin is often red, adherent to and involved in the
disease process. The overlying skin may break down
into an ulcer.
OTHER COMMON SKIN CONDITIONS
OFTEN SEEN IN SURGICAL PATIENTS
Hyperhidrosis
All skin contains sweat glands. If these glands secrete
an excessive quantity of sweat (hyperhidrosis), the
skin becomes soggy, white and moist.
Hyperhidrosis of the hands is a distressing con-
dition. The sweat may drip off the fingers, and every-
thing the patient touches gets wet.
Axillary hyperhidrosis is also embarrassing
because the adjacent clothes become saturated with
sweat and offensive.
Eczema/dermatitis
This is a red, weepy, vesicular rash which usually has
an immune cause. There are constitutional ‘endoge-
nous’ factors in all patients with eczema, but ‘exoge-
nous’ sensitizing factors are also very important.
The condition may be inherited, when it is often
associated with hay fever and asthma. It can also be
initiated by an allergy, drugs or infection, or physi-
cal problems such as an injury, scratching or vari-
cose veins.
Drug eruptions
A whole variety of different types of rash can occur
in response to drugs, including maculopapular
rashes, eczema, purpura, urticaria and generalized
desquamation. Occasionally patients develop severe
malaise, pyrexia and generalized lymphadenopathy.
A drug eruption must be considered in any patient
who develops a rash (see Revision panel 3.9).
Urticaria
This used to be called hives and is the development
of allergic wheals in the skin in response to a noxious
stimulus. The condition is caused by degranulation
of mast cells, which release histamine. In some patients
the cause proves impossible to identify and these cases
are called idiopathic. Nettle stings, jelly-fish stings and
insect bites are recognized causes, as are morphine
and atropine.
The term angioneurotic oedema is used to des-
cribe swelling of the tongue, eyelids, lips and larynx,
Revision panel 3.9
Common causes of drug eruption
Antibiotics
Barbiturates
Non-steroidal anti-inflammatory drugs
Diuretics
Chlorpromazine
Chap-03.qxd 4/19/05 13:45PM Page 99
The skin and subcutaneous tissues
100
which comes on intermittently and for which there
is no known cause. Occasionally a family history is
present indicating a genetic factor.
Acne and sycosis barbae
These are conditions in which the ducts of the seba-
ceous glands become blocked by over-activity. They
may then become inflamed and secondarily infected.
The condition causes comedos (blackheads) and
blind cysts, which may turn into sebaceous cysts.
Severe scarring may result. The condition declines
after the age of 20.
Psoriasis
This condition occurs in 1–2 per cent of the Cau-
casian population, usually beginning between the
ages of 5 and 25. About a third of those affected have
a family history of the condition. It tends to improve
in summer and during pregnancy. It presents as
sharply demarcated, red, raised, oval plaques mainly
situated over the elbows, knees and scalp. The plaques
have a silver, scaly surface and the pattern of distri-
bution varies widely. Psoriasis is often associated with
an arthritis of the hands, which has to be distin-
guished from rheumatoid arthritis. A quarter of those
affected develop pits in the nails, which are often
thick, opaque, discoloured and break easily. It may
occur in the flexures of the groin and axillae, where
moist conditions prevent scaling.
Pityriasis rosacea
This is the commonest cause of a slightly itchy skin
rash in a young person. It usually starts with a single
red, oval, scaly macule, which often arises over the
lower abdomen or shoulder. Three or four days later,
a characteristic rash appears over the trunk, consist-
ing of both macules and papules. The rash does not
involve the skin below the upper thighs and arms
and has a ‘vest and pants’ distribution. The long axes
of the macules are arranged along the line of skin
cleavage (Langer’s lines). They typically have a fawn
centre with a pink surround. Scaling is often present
at the junction with normal skin. The rash usually
clears completely in 6–12 weeks. The differential
diagnosis includes drug sensitivity, tinea pedis, gut-
tate psoriasis and secondary syphilis.
Lichen planus
This develops on the wrists as an itchy rash before
spreading to the trunk and legs. Papules are present
on the wrist, forearms, trunk and shins. The rash may
be widespread or may remain localized to the wrist
and shins. The papules are usually highly character-
istic. They are flat topped, shiny, purple and often
polygonal in shape. They are often umbilicated and
appear in scratch marks (the Koebner phenonomen).
They may become warty and form larger plaques,
which can coalesce. Delicate, white striae, annular
lesions or white dots may be present on the buccal
mucosa, tongue or inside of the lips. Oral ulceration
may develop but this is not painful. The condition
invariably affects adults, and the face and scalp are
almost never involved. Its course is very variable but
it usually lasts 3–6 months.
SUBCUTANEOUS INFECTIONS
Subcutaneous abscess
Abscesses in the subcutaneous tissue are common
and usually follow implantation of bacteria by a
penetrating injury, or infection in a haematoma.
The common infecting organism is Staphylococcus
aureus, but almost any organism can cause an abscess
if the local conditions are favourable to its growth. An
abscess is a pocket of pus (dead cells, exudate and
bacteria) surrounded by granulation tissue.
History
Age
Subcutaneous abscesses occur in all ages and
both sexes.
Hygiene
Poor social conditions and bodily hygiene
will increase the chances of an infection following a
minor injury such as a pinprick.
Symptoms
The principal complaint is of a throbbing
pain which gets steadily worse and keeps the patient
awake at night.
The patient notices an area of thickening and
tenderness at the site of the pain, which slowly turns
into a hard mass.
The mass may discharge spontaneously, with
relief of the symptoms, before the patient comes to
the doctor.
Chap-03.qxd 4/19/05 13:45PM Page 100
Subcutaneous infections
101
Previous history
Patients who are debilitated, diabetic
or drug addicts may have had previous abscesses
because of the debility caused by their underlying
disease and frequent injections.
Habits
Enquire about the drug-taking habits of the
patient if you have cause to think that the abscess
has followed a self-administered injection.
Examination
The four classical signs of an abscess (the signs of
Celsus) are tumour, rubor, calor and dolor (swelling,
redness, heat and pain).
Site
Areas subjected to trauma are more suscepti-
ble. The hands are common sites for subcutaneous
infection (see page 162).
Injections are usually given into the buttock or
thigh, so these are also common sites for abscesses.
Self-administered injections by drug addicts are
usually given into the veins in the cubital fossa and
groin.
Shape and size
The initial change is the development
of a patch of induration. As the pus forms, this patch
turns into a definite mass which is basically spherical.
The mass may become large and lose its spherical
shape if the pus begins to spread through the subcu-
taneous tissues.
Surface
The inner surface of an abscess is a layer of
granulation tissue which is inseparable from the
indurated inflamed tissues around it. Thus an
abscess does not have a definable outer surface, even
though its contents may be easy to feel.
Colour
The overlying skin is red.
Temperature
The skin over an abscess is hot.
Tenderness
Abscesses become increasingly tender as
the tension in the pocket of pus increases.
Edge
The edge is not palpable, as the induration and
oedema gradually merge into the normal tissues.
Composition
In the early stages an abscess feels hard
and solid. As the pus forms, the centre of the area
becomes soft and, if it is not too tender to press,
fluctuant. It is dull to percussion and not reducible.
Relations
The skin over a subcutaneous abscess is
invariably involved in the inflammatory process, so it
is red, oedematous and fixed to the underlying mass.
If the pus points towards the skin, the skin
becomes white and then black as it dies and sloughs
away. When the dead skin separates, the pus can
escape from the abscess. Deep fixation depends
upon the size and direction of spread of the abscess.
Local lymph glands
The lymph glands which receive
lymph from the infected area are likely to be
enlarged and tender. They may even become abscesses
themselves.
Local tissues
The local tissues should be normal,
apart from those close to the abscess which are
involved in the inflammation. There may be scars
from previous abscesses.
General examination
A large abscess can cause consid-
erable systemic disturbance. The patient looks pale
and ill but may be sweating and having rigors and
episodes of flushing. The temperature and pulse are
elevated.
Carbuncle
A carbuncle is a spreading necrotizing infection in
the subcutaneous tissues, with pus and slough for-
mation, similar to the changes that occur in a boil,
but with many points of discharge through holes
in the skin that appear when patches of necrotic
skin slough. The subcutaneous tissue necrosis is
much more extensive than the reddened area of
overlying skin.
Sinuses and fistulae
Sinus
A sinus is a tract lined by granulation tissue which
connects a cavity (usually an old abscess) with an
epithelial surface. A sinus produces a serous or
purulent discharge and fails to close if:
■
the cavity is inadequately drained,
■
it is caused by a specific chronic infection
(e.g. actinomycosis, tuberculosis, syphilis),
■
a foreign body (e.g. stitch material) is present at
the bottom of the sinus,
■
the cavity has epithelialized,
■
the cavity has undergone malignant change,
■
the surrounding tissues have poor vascularity or
have been irradiated.
Sinuses commonly follow surgical wound infec-
tions and necrosis of tumours.
Chap-03.qxd 4/19/05 13:45PM Page 101
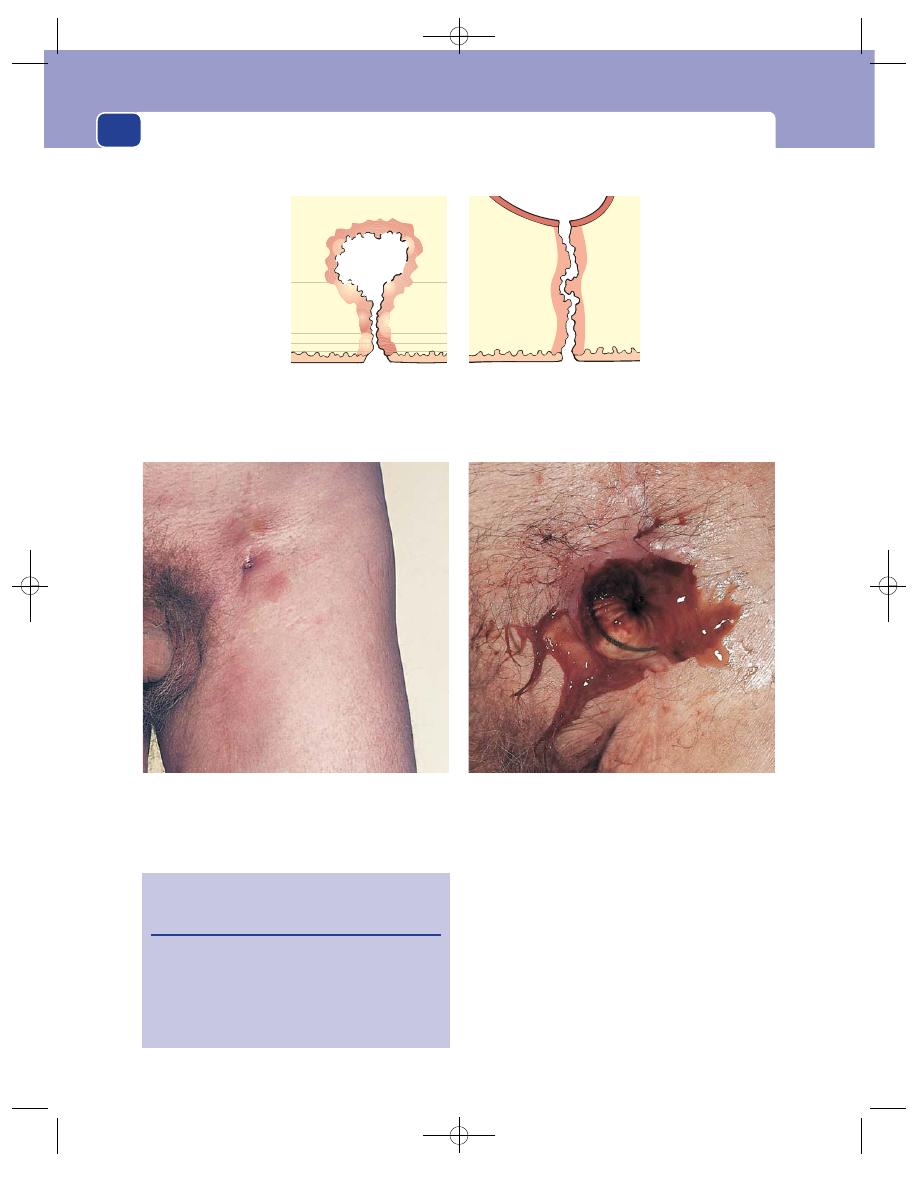
The skin and subcutaneous tissues
102
Fistula
Sinus
FIG 3.45
THE DIFFERENCE BETWEEN A SINUS AND A FISTULA.
Fistula
A fistula is a pathological connection between two
epithelial surfaces. For example, it is possible to have
a fistula between the bowel and the skin, the bowel
and another loop of bowel, or the bowel and the
bladder.
Fistulae are usually lined with granulation tissue
but they can become epithelialized. They form
when a chronic abscess bursts in two directions con-
necting two epithelial surfaces. They persist if they
The same wound 3 weeks later. The sinus has opened widely
to reveal its cause – an infected Dacron arterial graft.
FIG 3.46
A SINUS AND ITS CAUSE.
Revision panel 3.10
The causes of a chronic abscess or
persistent sinus
Inadequate drainage
Specific chronic infection, e.g. tuberculosis
Foreign body, e.g. a stitch
Epithelialization of the cavity
Malignant change in the wall of the cavity
A discharging sinus from the centre of a groin wound.
A sinus is a connection between a cavity lined
with granulation tissue and an epithelial surface.
A fistula is a connection between two epithelial-
lined surfaces.
Chap-03.qxd 4/19/05 13:45PM Page 102
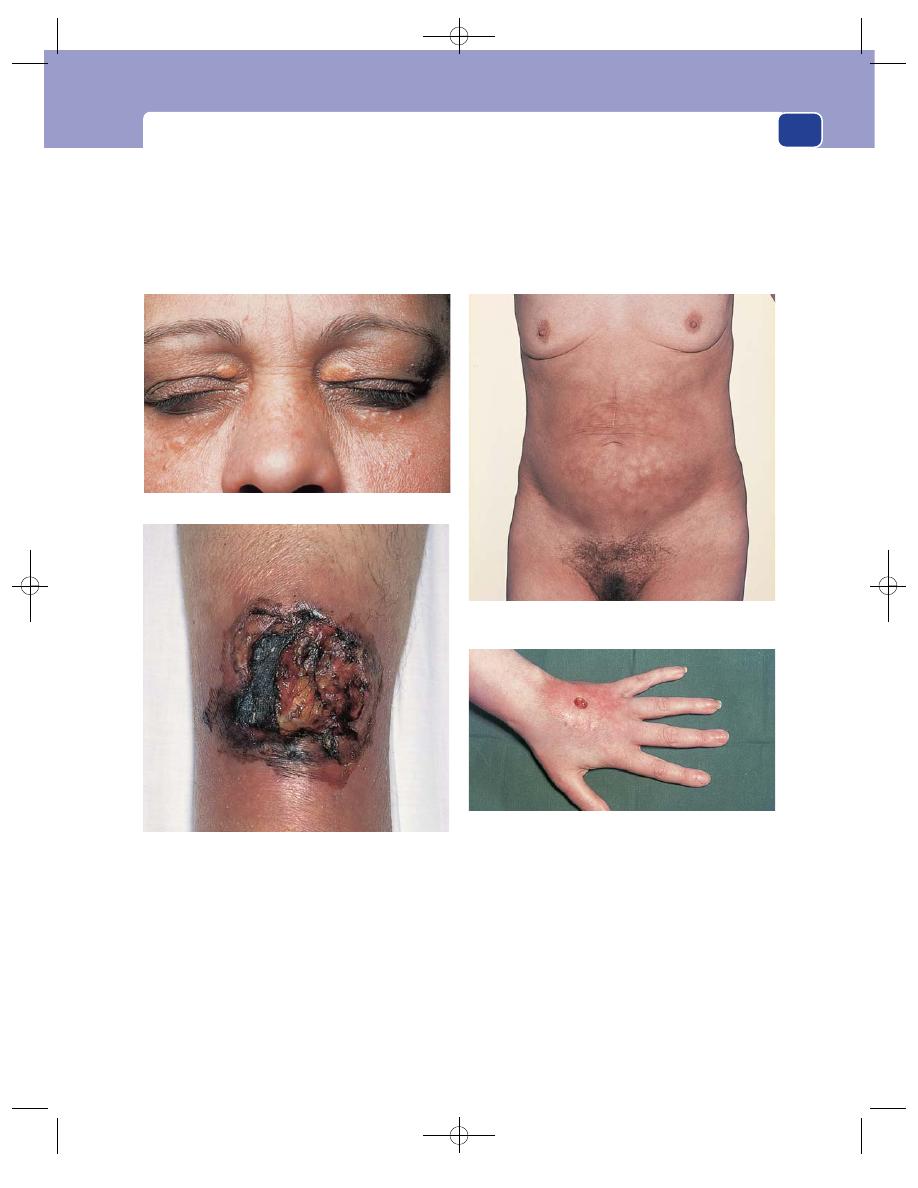
Subcutaneous infections
103
have to transmit the contents of one of the epithelial-
lined cavities to the other if the former’s normal
outflow is obstructed.
They do not resolve until the cause of the abscess
is eradicated (see above for the factors which delay
abscess closure) or the obstruction to the emptying
of the viscus is removed.
The common fistulae seen in surgical practice
are between the anal canal and the peri-anal skin
and the bowel.
An injection ulcer on the back of the hand.
Erythema ab igne caused by the repeated application of a
hot-water bottle to relieve abdominal pain.
Xanthoma of the upper eyelid.
Infected necrosis (gangrene) of the skin following local
trauma in a patient taking steroids.
FIG 3.47
SOME MORE SKIN LESIONS.
Chap-03.qxd 4/19/05 13:45PM Page 103
It is essential that all doctors have a sound basic
knowledge of orthopaedic disease, because so many
of the patients who come to the general surgical and
medical clinics have abnormalities of their muscu-
loskeletal system. As the primary concern in ortho-
paedic conditions is often function, you must be able
to examine the muscles, bones and joints properly,
assessing function as well as any structural abnor-
mality. This chapter describes the examination of each
of these structures and some of the common abnor-
malities and diseases that affect them.
A GENERAL PLAN FOR EXAMINING
THE MUSCLES, BONES AND JOINTS OF
A LIMB
The basic approach can be broken down into five
components:
■
inspection
■
palpation
■
movement
■
percussion and/or auscultation when indicated
■
special tests as appropriate.
Although moving the limb would normally be
part of inspection and palpation, it is such an impor-
tant part of the examination that it is presented as a
separate exercise and, as percussion, auscultation and
special tests are not relevant to all joints or bones, the
basic plan becomes inspection, palpation and move-
ment, or in simple English:
■
look
■
feel
■
move.
Always begin by looking at both limbs, front and
back, and examining the good limb first.
Always ask the patient to perform active move-
ment before you perform passive movements.
Inspection and movement should be performed
with the patient supine and standing.
Inspection
Skin
Is the skin discoloured, erythematous or oede-
matous? Is there any bruising that may suggest
trauma? Look for scars and sinuses. Are there any
abnormal or asymmetrical skin creases? Is there any
localized bony tenderness suggestive of the presence
of a fracture?
Shape
Is there any swelling and, if so, is it diffuse or
localized? Is there any deformity or postural alter-
ation in shape and, if so, is it confined to a joint (Fig.
4.1) or is it more generalized? (Fig. 4.2) Is there any
muscle wasting?
Length
Compare the length of each part of the limb
with the other side, at this stage by eye.
Palpation
Skin
Feel the temperature of the skin. Is there any
oedema – local or dependent? Feel any scars or areas
of thickening and find their relation to the bones
and joints. Is any part of the limb tender, and if so, is
it diffuse or localized?
Shape
Try to define the cause of any swelling, e.g.
swelling confined to a joint may be an effusion,
haemarthrosis, pyarthrosis, thickening of the syn-
ovium or localized masses related to the muscle
or bone. Note the relation of any swelling to under-
lying or neighbouring anatomical structures and
elicit all its physical characteristics, described on
pages 29–32.
Record on a diagram any abnormality or degrees
of deformity of alignment.
Length
Measure the real length of each limb and of
each bone and the apparent length of the limb (see
page 114).
Chap-04.qxd 4/19/05 13:49PM Page 104
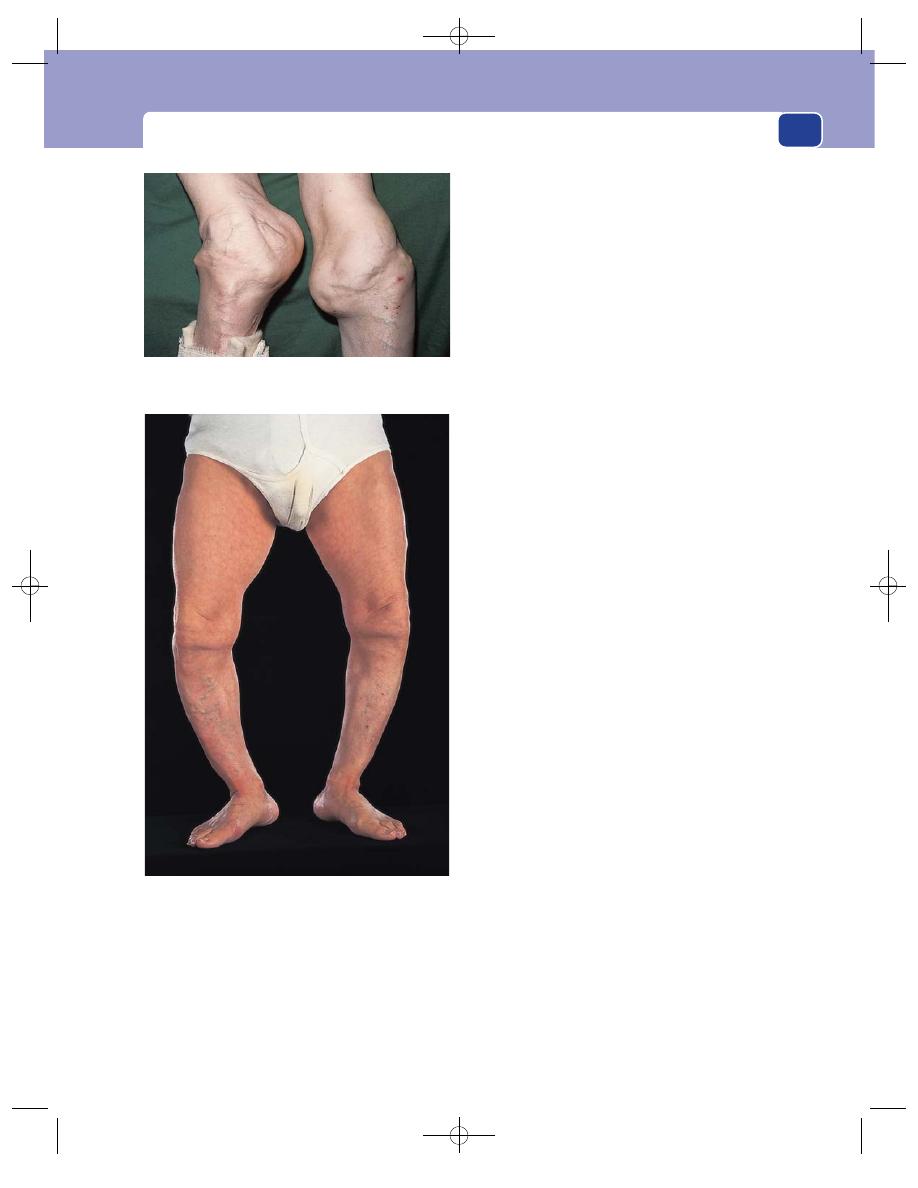
A general plan for examining the muscles, bones and joints of a limb
105
Movement
Active
Ask the patient to move each joint through
its full range of movements and show you any trick
or abnormal movements. Watch the limb working:
standing, walking, lifting, etc.
Passive
Move all the joints of the limb through
their full range. Complete loss of all movement of a
joint implies either surgical arthrodesis or fibrous
or bony ankylosis as a result of some pathological
process such as infection. Note any restriction to
movement or fixed deformity which may result
from contraction of the joint capsule, muscles or
tendons. Locking or limitation may also occur as a
result of interposition of soft tissues, bone or loose
bodies. Record as accurately as possible the range of
movements in degrees (e.g. 45° of flexion or 120° of
extension).
Test the strength of each movement against
resistance (see ‘Muscle strength’, page 107). Look for
any clicks or crepitations in the joint on movement.
Test for abnormal movements by testing the integrity
of the ligaments of each joint.
Other tests
It is essential to examine the structures that keep the
limb alive and make it work – the arteries and nerves.
Arteries
Palpate all the pulses. Note the tempera-
ture and colour of the limb (see page 175).
Nerves
Test the motor, sensory and reflex innerva-
tion of the limb.
Motor
You will already have obtained some infor-
mation on the ability of the muscles to contract
during your examination of movement and strength.
If there is any weakness, work out which muscles are
affected and their nerve root innervation.
Sensory
Check the appreciation of light touch, pin-
prick, temperature changes, deep pain, vibration
sense and position sense. When applicable, record
the Medical Research Council (MRC) grading of
loss of sensation and its subsequent recovery or
deterioration:
■
S0: absent sensation in the area supplied by the
affected nerve,
■
S1: return of deep cutaneous pain,
■
S2: return of some superficial pain and tactile
sensibility,
■
S3: return of superficial pain and tactile
sensibility without over-reaction,
■
S3
ⴙ: return of two-point discrimination,
■
S4: normal sensation.
Reflexes
Test all the limb’s reflexes, and if diminished
or altered in any way, seek to identify the nerve root
innervation.
FIG 4.2
Marked deformity of the lower limbs associated with
rickets.
FIG 4.1
The grossly deformed knees that are the results of
neuropathic joints.
Chap-04.qxd 4/19/05 13:49PM Page 105
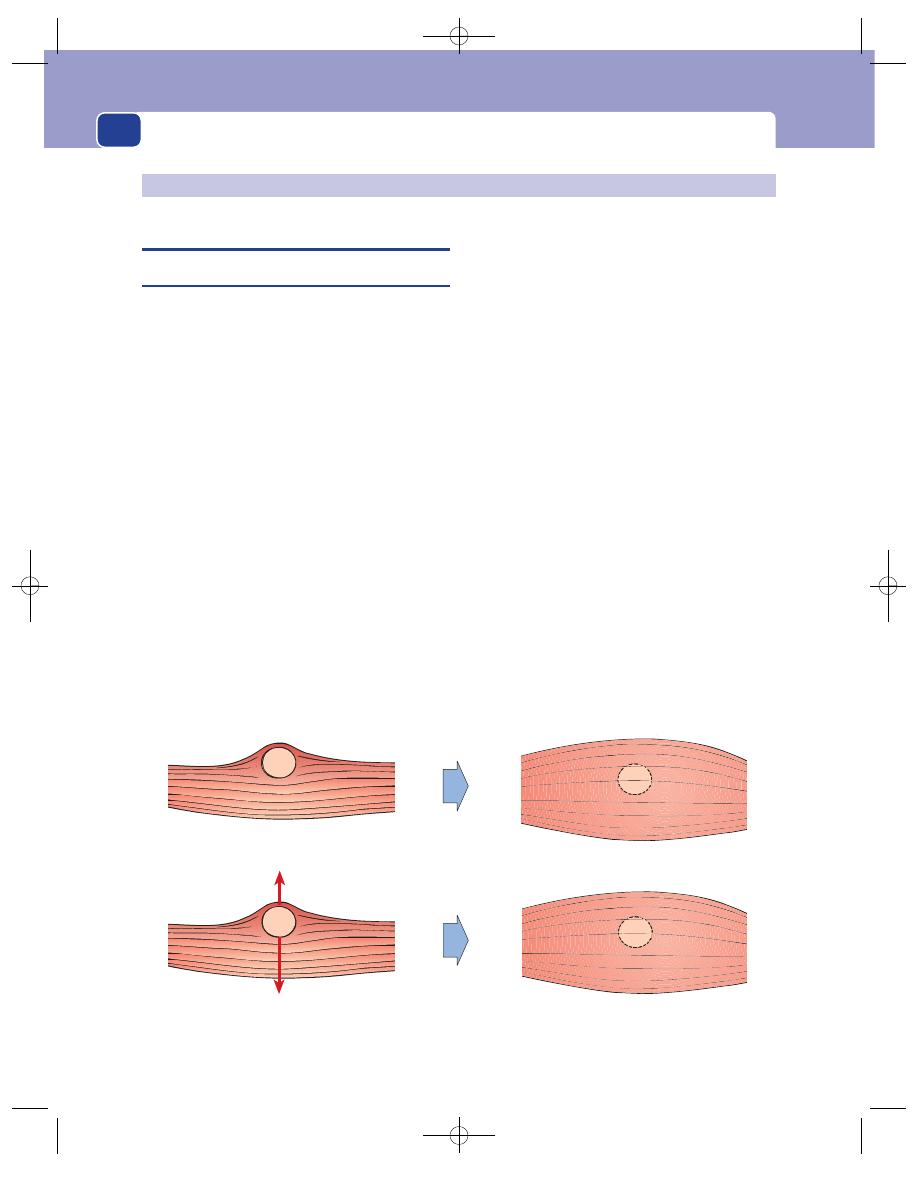
Muscles, tendons, bones and joints
106
MUSCLES AND MUSCLE DISEASE
Examination of a muscle
If a muscle appears to contain a definite lump, begin
by examining the lump to ascertain its physical
characteristics, as described in Chapter 1. If there is
doubt about the relationship of a lump to the whole
muscle, it is better to examine the muscle first and
the lump second.
Inspection
Observe the shape of the muscle at rest. Note any
wasting, hypertrophy or irregularity of shape caused
by a lump, or displacement of the muscle. Always
compare the abnormal muscle with the normal mus-
cle of the other limb.
Observe the shape of the muscle when it is con-
tracting. Alterations in shape that appear when the
muscle is contracting are caused either by a lump
being concealed or made more obvious by the con-
tracting muscle, or by knotting-up or parting of
ruptured muscle fibres.
Look at the neighbouring bones and joints.
Palpation
Feel the muscle at rest. Place the limb in a comfort-
able position so that the muscle is relaxed. Assess the
texture of the muscle.
Try to decide whether any abnormality is caused
by a localized swelling or an abnormal muscle. Elicit
all the features of any lump that you find.
Feel the muscle when it is contracting. See if any
of the features of the lump you felt when the muscle
was relaxed change when it contracts. A lump inside
the muscle becomes fixed and more difficult to feel
when the muscle contracts. A lump beneath the mus-
cle may become more difficult to palpate when the
muscle is contracted. A lump superficial to the mus-
cle, or breaking through its fibrous sheath, becomes
more prominent.
A gap or hollow that appears in the muscle when
it contracts usually means that the fibres are rup-
tured (see below).
A lump that appears only when the muscle con-
tracts is probably a bunch of ruptured fibres knot-
ting up.
SOFT TISSUES
Muscle relaxed
Lump easy to feel
Lump moves at right-angles
to length of muscle
Muscle contracted
Lump difficult to feel
Lump immobile
FIG 4.3
Principal features of an intramuscular lump.
Chap-04.qxd 4/19/05 13:49PM Page 106
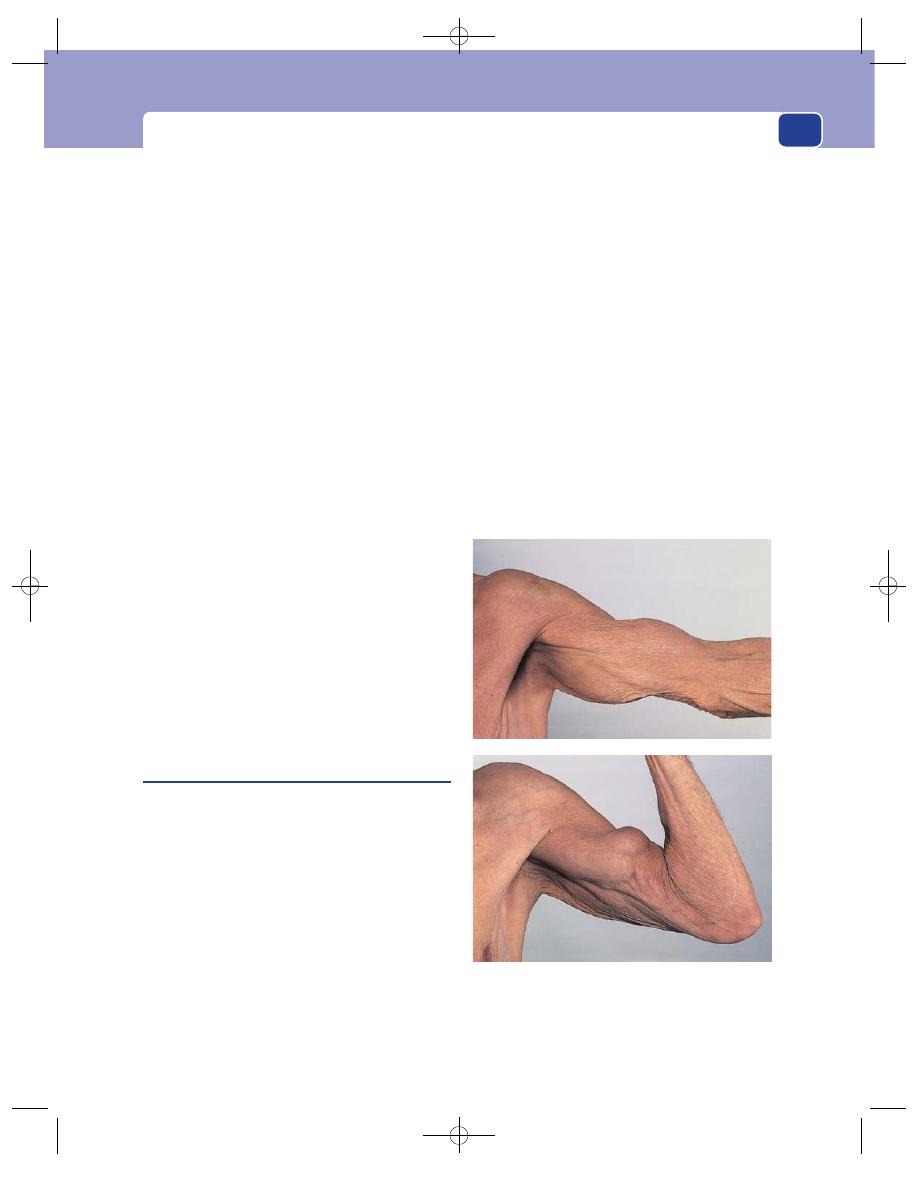
Muscles and muscle disease
107
Strength
Muscle power can be classified according to the MRC
scale. However, it is often better not to use numbers
but to describe the strength:
■
M0: no active contraction at all,
■
M1: barely perceptible flicker of contraction but
insufficient to cause any movement,
■
M2: weak contraction producing some
movement but insufficient to lift the limb
against the pull of gravity,
■
M3: weak contraction but can move the limb
against the pull of gravity only,
■
M4: fairly strong contraction but not full
strength; can produce movement against gravity
and some added resistance,
■
M5: full strength.
Remember that muscle strength can be impaired
by pain, wasting, denervation or other disease
processes.
Innervation and blood supply
You will know if a muscle is innervated after testing
its motor function, but you must also examine the
integrity of the whole nerve and the spinal segment
supplying the muscle by testing all of its other motor,
sensory and reflex functions. This means that you
must know which nerves and which spinal segments
innervate the main muscle blocks in the body (see
Revision panel 1.9, page 27).
Examine the pulses in the limb.
Ruptured muscle fibres
Muscle fibres usually rupture during an excessively
strong or unusually sudden contraction of the mus-
cle. Pathological rupture can follow a normal contrac-
tion if the muscle is weakened by some degenerative
process. The rupture usually occurs at the musculo-
tendinous junction.
History
Age
Muscle rupture can occur at all ages but is most
common in athletic young men at play, and elderly
men performing excessive or unaccustomed physi-
cal exercise.
Symptoms
Sometimes there is pain, swelling and
bruising at the time of the rupture, but in the elderly
patient the original incident is often not noticed
and the patient presents with weakness, a limp or a
swelling of the muscle.
Site
The muscles commonly affected are the biceps
brachii and the quadriceps femoris – two muscles
which often have to withstand sudden severe strains.
Examination
The diagnostic feature of a bundle of ruptured mus-
cle fibres is the appearance of a lump in the muscle
on one or both sides of a depression when the mus-
cle contracts. The lumps are the bunched-up free
ends of the contracted ruptured fibres.
The lumps cannot be felt when the muscle is
relaxed because they have the same consistence as
the adjacent muscle, but the hollow between the
broken fibres may be palpable and visible.
The lump (or lumps) which appears when the
muscle contracts is firm in consistence, has indistinct
FIG 4.4
A rupture of the long head of the biceps. In the upper
photograph the muscle is relaxed and its contours are normal.
In the lower photograph the muscle is contracting and the
ruptured fibres are bunched up into a firm mass in the middle
of the arm.
Chap-04.qxd 4/19/05 13:49PM Page 107
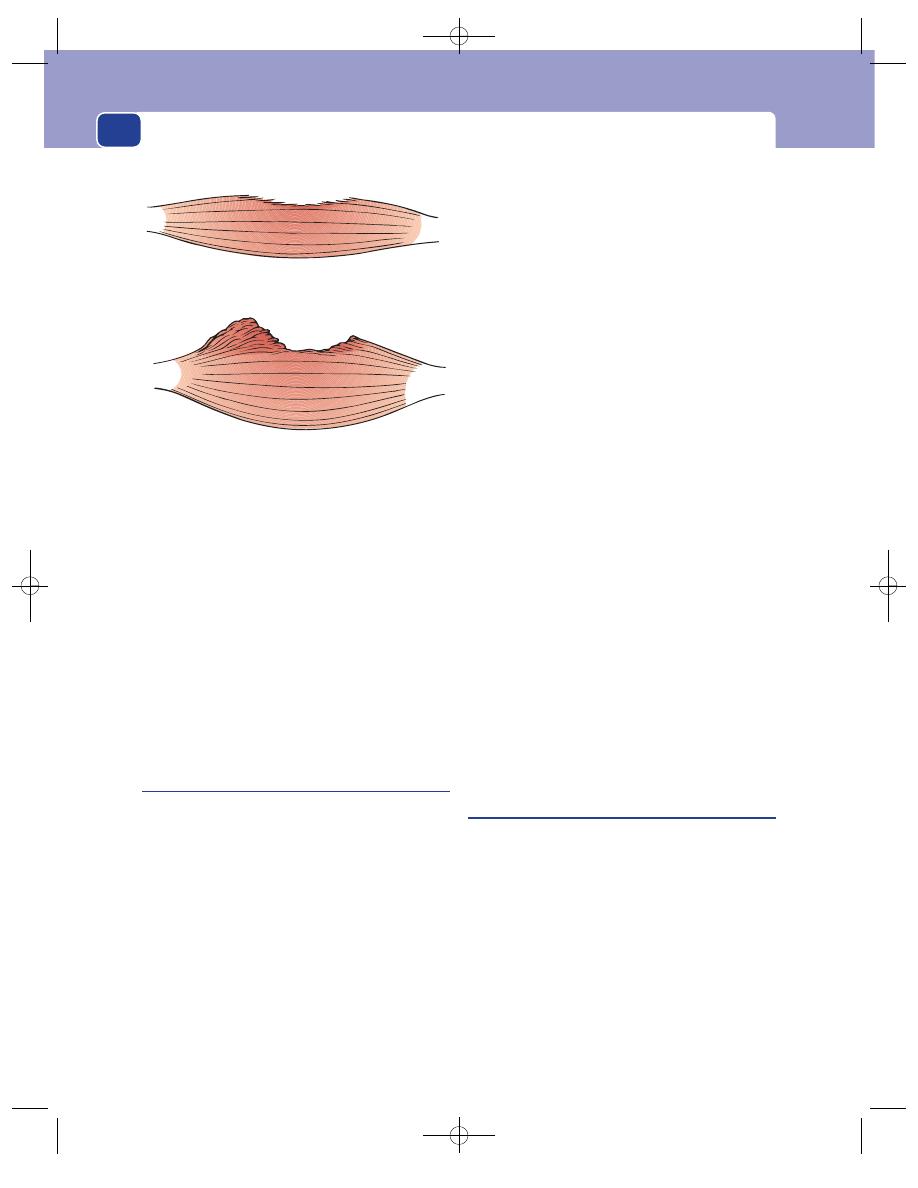
Muscles, tendons, bones and joints
108
edges and cannot be moved independently of the
muscle.
The local arteries, nerves, bones and joints are
normal unless the rupture is caused by attrition or a
chronic musculoskeletal disease such as rheumatoid
arthritis.
Do not forget to examine the neighbouring
bones and joints.
If a significant number of fibres are ruptured, the
strength of the muscle will be reduced. If all the
fibres are ruptured, the movement normally pro-
duced by the muscle will be absent.
Intramuscular haematoma
This condition usually follows a direct injury or tear
of the muscle fibres and the intramuscular blood ves-
sels. It can follow a severe cramp or a violent, sudden
muscle contraction. Although some of the muscle
fibres are ruptured, not enough are divided to pro-
duce the physical signs of a ruptured muscle.
History
Symptoms
The two main symptoms are pain and
swelling in the muscle. The pain is present at rest
but is exacerbated by any movement of the muscle,
passive or active. The patient may also have noticed
a diffuse swelling of the limb or a tender lump in
the muscle.
Cause
The patient can often recall the initial injury.
Trivial injuries only cause intramuscular bleeding if
there is a haematological or vascular abnormality.
Ask the patient if he or she is taking anti-
coagulants and, if male, whether he has haemophilia.
Examination
Site
The muscles of the lower limbs, especially the
gastrocnemius, are most often affected.
Tenderness
The lump is tender for a few days, and all
movements of the muscle are very painful. Although
the tenderness subsides quite quickly, the pain caused
by contraction of the muscle may persist for weeks.
Shape and size
Haematomata are usually ovoid, with
their long axis parallel to the muscle fibres.
The size of the lump depends upon the amount
of bleeding. This is not always easy to assess, because
the edge of the lump is usually indistinct.
Composition
The composition of a haematoma
depends upon the state of the blood within it. The
blood in most haematomata is coagulated, so the
lump feels hard. Sometimes the central portion stays
fluid, making the lump soft and fluctuant.
Local tissues
The surrounding tissues, including the
adjacent muscle, should feel normal, but contraction
of the muscle causes pain and makes the lump more
difficult to feel.
Lymph glands
The lymph glands at the root of the
limb should not be enlarged.
Muscle hernia
When a muscle contracts, it becomes shorter
and thicker. If it is contained by a fibrous sheath, the
tension within the sheath rises. If there is a defect in
the fibrous sheath, the muscle will bulge through it,
especially when it contracts. This is called a muscle
hernia.
History
Symptoms
The patient may notice the lump when
looking at or feeling the muscle, or experience a slight
ache in the muscle and find a lump when trying to
pinpoint the source of the discomfort.
Relaxed
Contracted
May be a small depression
A lump appears on one or both
sides of a sharp depression
FIG 4.5
The clinical features of ruptured muscle fibres.
Chap-04.qxd 4/19/05 13:49PM Page 108
Muscles and muscle disease
109
Examination
Site
Although all muscles are surrounded by a fibrous
sheath, only those with a thick covering are likely to
cause symptomatic muscle herniae. The common-
est muscle hernia is through the thick fascia which
covers the anterior compartment of the lower leg.
Shape and size
Muscle herniae can be of any size.
Their characteristic feature is that they change in
size according to the tension in the muscle. When
the muscle contracts, it bulges through the fascial
defect. When the muscle is relaxed, there is no lump –
just a hole.
Occasionally these signs are reversed. The muscle
may bulge through the defect when relaxed but be
pulled back into its compartment when it retracts.
Do not be confused by this variation. Provided the
lump comes and goes as the muscle tension changes
and there is a palpable defect in its covering fascia, it
is a muscle hernia.
Intramuscular and intermuscular
lipomata
There is not much fat inside a muscle, but there are
often small collections of fat around the nutrient
blood vessels and in the loose areolar tissue which
separates the different sections of a group of mus-
cles. Lipomata can develop in this fat. Histologically
they are no different from any other lipomata, but
the site gives them some distinctive physical signs.
History
Symptoms
An intramuscular or intermuscular lipoma
may interfere with the function of the muscle and
cause pain when the muscle is being used, but it rarely
makes the muscle weak.
The patient may have felt, or seen, a lump appear
during exercise. If an intramuscular lipoma suddenly
bursts out of a muscle during exercise, the patient
experiences a sharp pain and notices the sudden
appearance of the lump. They will then believe that
the exercise caused the lump. The lump may change
in size and shape as the muscle contracts.
Muscle lipomata are rarely multiple.
Examination
Site
Any muscle can be affected. There is more fat
between the flat muscles of the trunk than between
the muscles of the limbs, so deep lipomata are more
common on the back of the trunk.
Shape and size
If there is only a thin layer of muscle
or fascia covering the lipoma, its typical multilobu-
lar shape will be palpable.
These lipomata are often quite large (5–10 cm in
diameter) because they grow unnoticed within or
between the muscles for many years. They may
become larger, smaller or disappear when the muscle
contracts, according to their relation to the main bulk
of the muscle.
Edge
Their edge is difficult to feel. When a lipoma
has herniated through the thick layer of fibrous tissue
surrounding the muscle, you may feel a sharp edge,
corresponding to the defect in the fascia, but there is
usually a lot more of the lipoma deep to this edge
that you cannot feel.
Composition
The consistence varies with the tension in
the muscle. When the muscle is relaxed, the lipoma
has its typical soft consistence and may seem to fluc-
tuate. When the muscle contracts, the lipoma, if it is
still palpable, becomes hard and tense.
Relations
Intermuscular and intramuscular lipomata
are tethered to their site of origin and usually become
fixed when the muscle contracts. An intermuscular
lipoma may become impalpable when the muscle
overlying it contracts.
Myositis ossificans
This is calcification, and sometimes ossification, in
part of a muscle. It is an uncommon condition that
may follow an injury that has caused extensive intra-
muscular haemorrhage, sometimes associated with a
fracture of the adjacent bone. The muscles most often
affected are the brachialis, after a supracondylar frac-
ture of the humerus, and the quadriceps femoris, after
a fracture of the femur or a direct blow such as a kick.
History
Previous injury
The patient will know about their pre-
vious fracture or, when not associated with a fracture,
remember a previous major soft tissue injury.
Symptoms
The principal symptoms are caused by
an inability of the muscle to relax. The nearby joint
becomes stiff because there is a reduction of all
the movements normally permitted by relaxation of
Chap-04.qxd 4/19/05 13:49PM Page 109
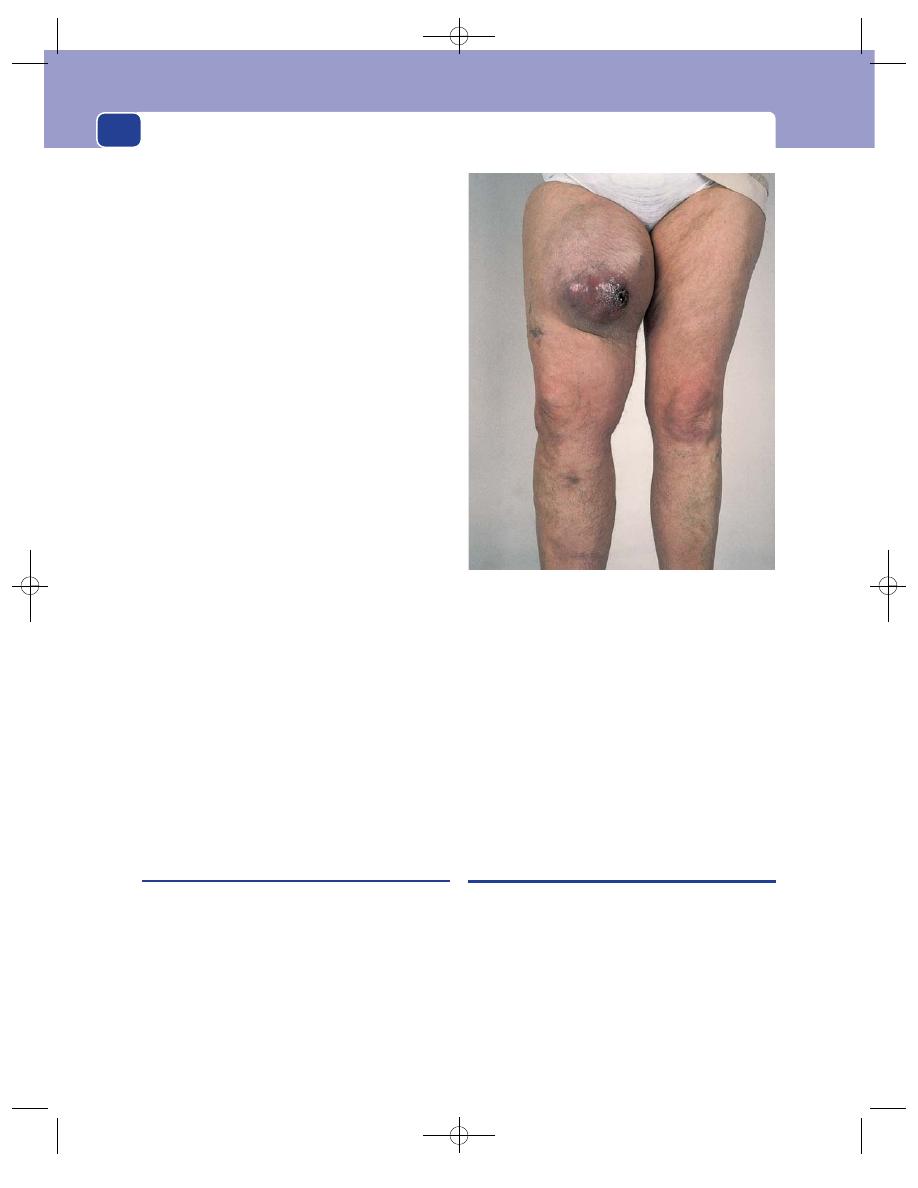
Muscles, tendons, bones and joints
110
the affected muscle (e.g. myositis of the quadriceps
femoris restricts knee flexion but there is full exten-
sion). All forced movements are painful. If the intra-
muscular ossification is extensive, the joint may
become completely fixed.
Examination
Site
The common sites for myositis ossificans are
the lower part of the brachialis muscle and the lower
part of the quadriceps femoris muscle.
Tenderness
The mass of ossified muscle is not nor-
mally tender, but forced passive movements may
cause pain.
Temperature
The mass has a normal temperature.
Shape
The ossification takes the shape of the muscle
in which it is occurring. It is usually an elongated
mound filling the muscle and fixed to the underly-
ing bone.
Surface
The surface is smooth but irregular.
Composition
The mass is bony hard and dull to per-
cussion.
Relations
In most cases the ossification in the mus-
cle is continuous with the callus that developed
around the fracture. Thus the mass is often mis-
taken for a bony swelling.
Normally the muscles over the callus of a healing
fracture will work normally, whereas ossifying mus-
cles cannot work properly and cannot be moved
over the callus. The muscle fibres can be felt run-
ning into the mass.
Local tissues
There may be other evidence of the pre-
vious trauma – bone and joint deformities, or nerve
and artery damage – so it is important to examine
the whole limb very carefully.
Myosarcoma
True tumours of muscle are rare. Those that arise
from smooth muscle are called leiomyosarcomata.
Those that arise from striated muscle are called
rhabdomyosarcomata.
Almost all of the soft tissue sarcomata occurring in
the limbs will actually be fibrosarcomata arising from
the intermuscular and intramuscular fibrous septae
or the fibrous tissue at the origin or inser-tion of the
muscles. These tumours are described below. True
rhabdomyosarcomata are uncommon and clinically
cannot often be differentiated from fibrosarcomata.
The diagnostic features of a tumour arising in or
from a muscle are:
■
it moves freely when the muscle is relaxed,
especially in a direction at right-angles to the
length of the muscle;
■
it becomes immobile when the muscle contracts
and its physical features may change; it may
become more or less prominent, harder or
softer, and change shape.
FIBROUS TISSUE
The fibrous tissue that covers muscles and links them
to bone in the form of tendons, fibrous insertions,
aponeuroses, tendon sheaths etc. is tough, durable
and stable. It causes little trouble during life but is
sometimes the site of malignant change.
Three tumours can arise from this tissue. The
pure benign fibroma is very rare and can be forgot-
ten, but the fibrosarcoma is one of the commonest
mesodermal soft tissue malignant tumours. The third
FIG 4.6
A large rhabdomyosarcoma of the thigh arising in the
quadriceps muscles.
Chap-04.qxd 4/19/05 13:49PM Page 110
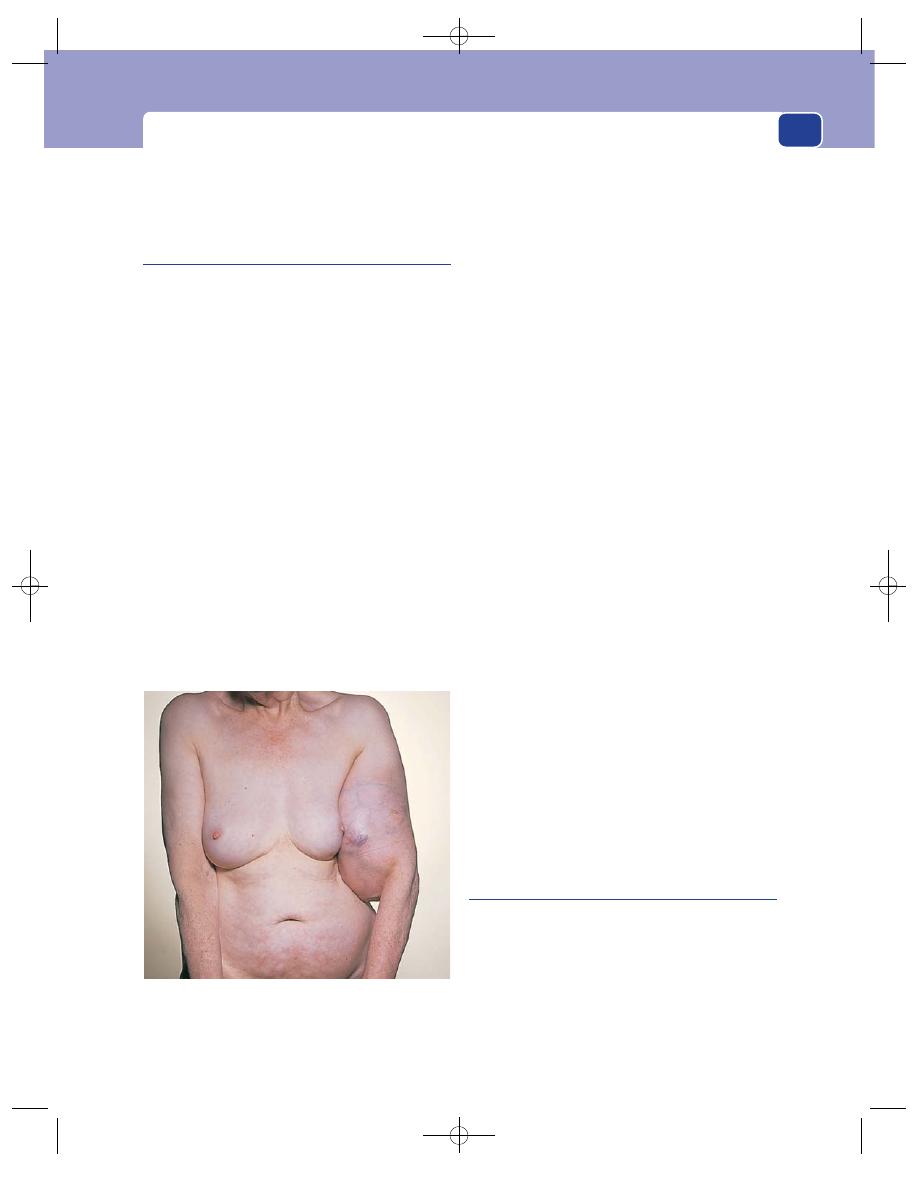
Fibrous tissue
111
variety is a less common, locally invasive and recur-
rent tumour known by various names, but most
often as Paget’s recurrent desmoid tumour.
Fibrosarcoma
This is a malignant tumour of fibrous tissue. It is
locally invasive and also spreads via the blood-
stream to the lungs and liver. Spread to the lymph
glands is an uncommon, but not unheard of, event.
Distant spread is a late event and the primary will
often grow locally for years before metastasizing.
History
Age
Fibrosarcomata are more common in elderly
patients but they can occur at any age.
Duration
The patient has often known of the exis-
tence of a lump for months – sometimes years –
before he comes to the doctor to complain of it.
Symptoms
The reasons for complaint include:
■
growth of the lump, causing disfigurement or
interference with muscle movements,
■
pain in the lump itself or from invasion of
nearby structures,
■
muscle weakness caused by infiltration of
nearby muscles,
■
general debility, from multiple metastases.
Examination
Site
Fibrosarcomata can occur anywhere in the
body but more occur in the limbs than elsewhere.
Colour
If a large vascular tumour is near the skin, it
may make the skin shiny and pink.
Temperature
Sarcomata, even slow-growing ones such
as fibrosarcomata, have an abnormal blood supply
and usually feel warmer than the surrounding tissue.
Shape
Their shape depends upon their site of ori-
gin. If a tumour grows in the middle of a soft tissue,
it will be roughly spherical. If it arises close to a
bone, it will be hemispherical, with its deep surface
fixed to the bone.
Surface
The surface is usually smooth but may be
bosselated.
Edge
The edge of slow-growing tumours is well
defined. Fast-growing and invasive tumours have an
indistinct edge.
Composition
The consistence of fibrosarcomata is
firm or hard. They are rarely stony hard because they
do not ossify and their marked vascularity tends to
keep them soft. They may be so vascular that they can
pulsate, have an audible bruit and a palpable thrill.
Relations
The relations of the tumour to the sur-
rounding tissues depend entirely on its site of origin,
size and invasiveness. Fibrosarcomata are usually
firmly fixed to nearby structures and often invade
neighbouring bones, nerves and arteries.
Lymph drainage
On rare occasions the local lymph
glands may be enlarged by secondary deposits.
State of local tissues
Take particular care to test the
integrity of any nerves running close to the mass of
the tumour. A nerve deficit is more likely to indicate
infiltration than stretching of the nerve, and is
almost diagnostic of a locally malignant lesion.
Paget’s recurrent desmoid tumour
This very rare condition is mentioned because it is an
interesting variety of sarcoma. It occurs most often
in middle-aged women, usually in the fascia covering
the abdominal muscles, i.e. the rectus sheath and
the external oblique aponeurosis. However, it can
occur in other sites such as the plantar fascia of the
foot or the palmar fascia of the hand. The malignant
change affects a wide area because after an extensive
FIG 4.7
A slow-growing fibrosarcoma of the arm. The
overlying skin is stretched and many distended subcutaneous
veins are visible. There was no ischaemia or paralysis in the
arm or forearm.
Chap-04.qxd 4/19/05 13:49PM Page 111
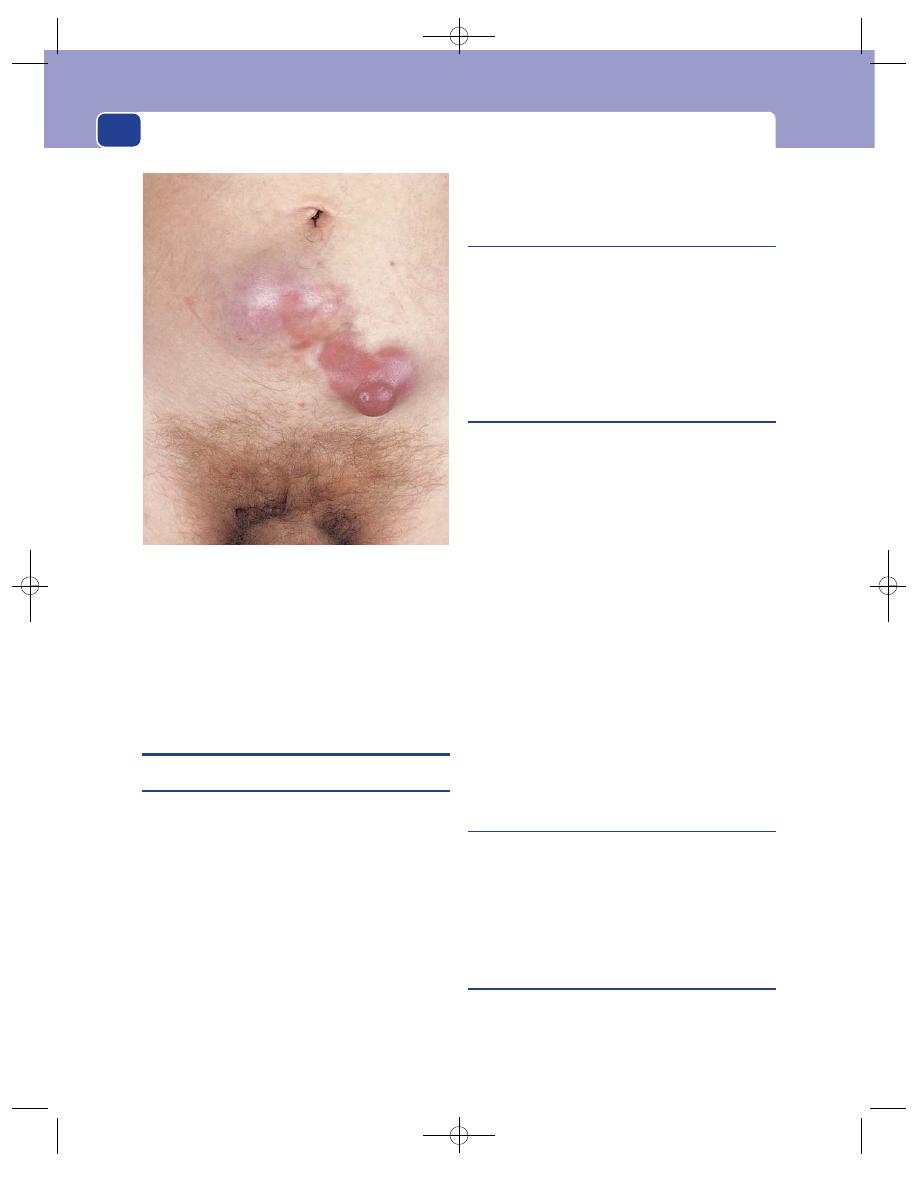
Muscles, tendons, bones and joints
112
and apparently adequate excision of the presenting
lump, new lesions may appear years later, in fascia
that was apparently healthy at the time of operation.
The lump has the same features as a fibrosarcoma,
but is less vascular and very slow growing.
TENDONS AND TENDON SHEATHS
Ruptured tendons
When the tendon of a muscle is divided the muscle
becomes ineffective. To assess the integrity of a tendon
you must know its site of insertion and the move-
ment that contraction of its parent muscle would
normally produce.
Tendons can be ruptured by direct violence, espe-
cially if they have been weakened by rubbing over
a fracture callus or the osteophytes and new bone
produced by arthritis – a process called attrition.
However, in most cases tendons rupture at a site that
has been weakened by avascularity and degeneration
(e.g. the Achilles tendon and long head of the biceps)
or ischaemic pressure necrosis, such as that caused
by a haematoma in the fibro-osseous sheath of the
extensor pollicis longus. The tendon of the biceps
brachii, the Achilles tendon and various tendons in
the hands are the tendons most often ruptured.
Ruptured biceps tendon
If the long, thin tendon of the long head of the
biceps muscle ruptures, the muscle belly retracts
into the middle of the arm, where it can be seen as
a lump and be made more prominent by asking the
patient to flex their elbow against a resistance. This
condition is common in the elderly. It does not
cause any significant weakness of the shoulder joint.
Ruptured Achilles tendon
Rupture of the Achilles tendon follows a sudden con-
traction of the gastrocnemius muscle during exercise.
The patient feels a sudden severe pain, as if shot in the
leg, and cannot walk properly. If the rupture happens
during walking or running, the patient may fall down.
Examination reveals pain on attempting to plantar
flex the foot and to stand on the toes of the affected
leg, but some degree of plantar flexion is still possi-
ble using the long flexor and peroneal muscles. The
gap in the tendon is easy to feel, even though there is
often a considerable amount of oedema around the
tendon and the ankle joint.
The rupture may be bilateral or the patient may
have ruptured the other side in the past.
Rupture of the Achilles tendon is easy to miss but
easy to detect with Simmond’s test. Lie the patient
prone with the feet beyond the edge of the couch,
fully relaxed. Squeeze the calf. The foot will plantar
flex if the Achilles tendon is intact but will not move
if it is ruptured.
Ruptured quadriceps tendon
This is an avulsion of the tendinous insertion of the
quadriceps femoris from the upper border of the
patella. It usually occurs in elderly people and is
uncommon. There is a loss or reduction of knee
extension and a visible and palpable gap between the
quadriceps muscle and the upper border of the patella.
Ruptured patellar ligament
This rare event is caused by an excessively strong
contraction of the quadriceps femoris muscle in
athletic young men. The obvious abnormality is an
inability to extend the knee joint. The patella lies
FIG 4.8
A large Paget’s recurrent desmoid tumour arising
from the anterior sheath of the rectus abdominis muscle.
Chap-04.qxd 4/19/05 13:49PM Page 112
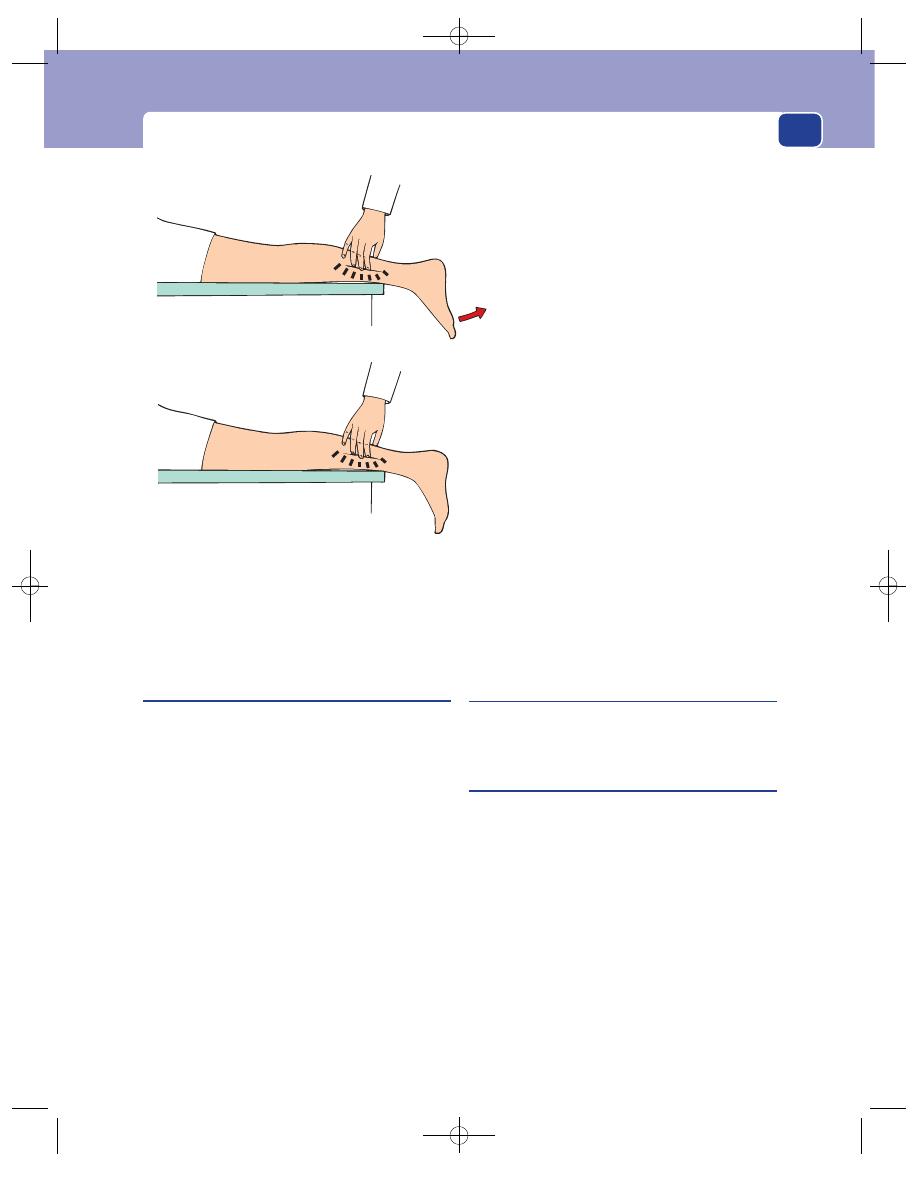
Tendons and tendon sheaths
113
high in the supracondylar groove of the femur, with
a visible and palpable gap below it, in the area nor-
mally occupied by the hard, tense patellar ligament.
Ruptured extensor pollicis longus
Any of the finger tendons can be cut by penetrating
injuries, but these present as an acute emergency
with the appropriate history of trauma. In these
cases it is important to check which finger move-
ments are lost and confirm that this is due to the
tendon injury and not to muscle paralysis caused by
an associated nerve injury.
Some tendons, especially the tendon of the exten-
sor pollicis longus, lie in a position which makes
them liable to constant friction if arthritic changes
(rheumatoid arthritis or osteoarthritis) occur in
the underlying joint, or increasing pressure if their
surrounding fibro-osseous sheath becomes tight or
inflamed. When the tendon ruptures there is no
pain, just a sudden loss of movement. In the case of
the extensor pollicis longus, the patient cannot
extend the distal phalanx of the thumb. Palpation
will reveal the absence of tension in the tendon dur-
ing extension of the thumb and the loss of the ulnar
border of the anatomical ‘snuff box’ at the base of
the thumb. This is often seen complicating Colles’
fracture and rupture of the extensor tendons of the
fingers complicating rheumatoid arthritis.
Mallet finger
This is a rupture of the extensor tendon of a finger just
proximal to its insertion. It is described on page 154.
Trigger finger
The movement of a tendon through its sheath can
be impeded in two ways:
■
by thickening of the tendon,
■
by thickening of the tendon’s sheath.
A trigger finger is a finger which gets fixed in flex-
ion and can only be extended by excessive voluntary
effort or sometimes physical assistance from the
other hand. When extension actually occurs it does
so with a jerk, just as the trigger of a gun moves
when the resistance of its spring is overcome. The
cause of this abnormality is a thickening of the ten-
don or the tendon sheath just where the tendon
enters the sheath, which stops the tendon sliding
freely into the sheath during extension.
Tendon intact
Squeeze lower third
of calf muscle
Foot plantar
flexes
Squeeze
Tendon ruptured
No movement
of foot
Squeeze the calf muscles. If the Achilles
tendon is intact, the foot will plantar flex.
FIG 4.9
Simmond’s test for a ruptured achilles tendon.
Place the patient prone with the feet hanging
freely over the end of the couch.
Chap-04.qxd 4/19/05 13:49PM Page 113
Muscles, tendons, bones and joints
114
Stenosing tenovaginitis
(of de Quervain)
This is an example of the restriction of tendon
movement caused by thickening of the tendon
sheath and/or the paratenon (i.e. a tenovaginitis or a
tenosynovitis). The tendons involved are the extensor
pollicis brevis and the abductor pollicis longus where
they lie in their fibrous sheath on the lateral side of
the wrist, just above the styloid process of the radius.
The cause of the inflammation is usually repeated
excessive movement of the tendons, e.g. typing.
All movements of the proximal phalanx of the
thumb, especially abduction, become painful, and
crepitus may be felt as the tendons move through
their sheath.
Palpation reveals a tender, sausage-shaped swel-
ling just above the styloid process of the radius.
BONES AND BONE IRREGULARITIES
EXAMINATION OF BONES
The basic plan follows a format similar to that
described at the beginning of the chapter and
includes inspection, palpation (including measure-
ment), movement and percussion.
Inspection
The overlying skin may give an indication of the
underlying pathology. An old tethered scar or a
discharging sinus may indicate old or active
osteomyelitis.
Redness and oedema of the skin may be caused
by underlying infection or malignant growth.
If there is a bony deformity, record its site and
angle.
Palpation
If there is a localized swelling, you must elicit all the
physical signs pertaining to a swelling (described on
pages 29–32).
Feel the whole length of the bone to assess its
shape and compare it to the normal side.
Note the temperature of the skin. Conditions
which increase bone blood flow, such as infection,
tumours and Paget’s disease, may raise the tempera-
ture of the surrounding tissues.
Measurement
Measure the length of the bone and the length of the
limb. There are three measurements you can obtain:
1. the true length of individual bones,
2. the apparent length of the whole limb,
3. the real length of the whole limb.
The methods and principles of measurement are
best described with respect to the lower limb, but
they apply equally to the upper limb.
Bone length
This is a simple measurement because you are not
measuring across any joints. Choose recognizable
anatomical points at either end of the bone and meas-
ure between them. Do the same on the other side.
Bony points have to be felt through the overlying
skin and muscle and it is difficult to get the end of
the tape measure on identical points on both sides.
The easiest method is to hold the measure between
thumb and index finger and then press the back of
the index finger firmly up against the bony point or
edge that you are using as a landmark.
Apparent length of the limb
When a patient lies flat and ‘straight’ on a couch the
limbs may appear to be of different length. This may
be caused by a bone or joint abnormality. It is cus-
tomary to record the apparent length, because when
it is compared with the true length it gives some
indication of the degree to which the skeleton has
adapted its position to keep both legs parallel and
both feet flat on the ground when the patient stands
up, or alternatively an indication of the effect of a
joint deformity on the length of the limb.
Method
Ask the patient to lie straight on the bed.
(Ask a child to lie like a soldier standing to attention.)
Choose a point in the mid-line of the trunk – the
umbilicus or xiphisternum – and measure from this
central point to the tips of both medial malleoli. These
lengths will be the apparent lengths of the limbs.
Chap-04.qxd 4/19/05 13:49PM Page 114
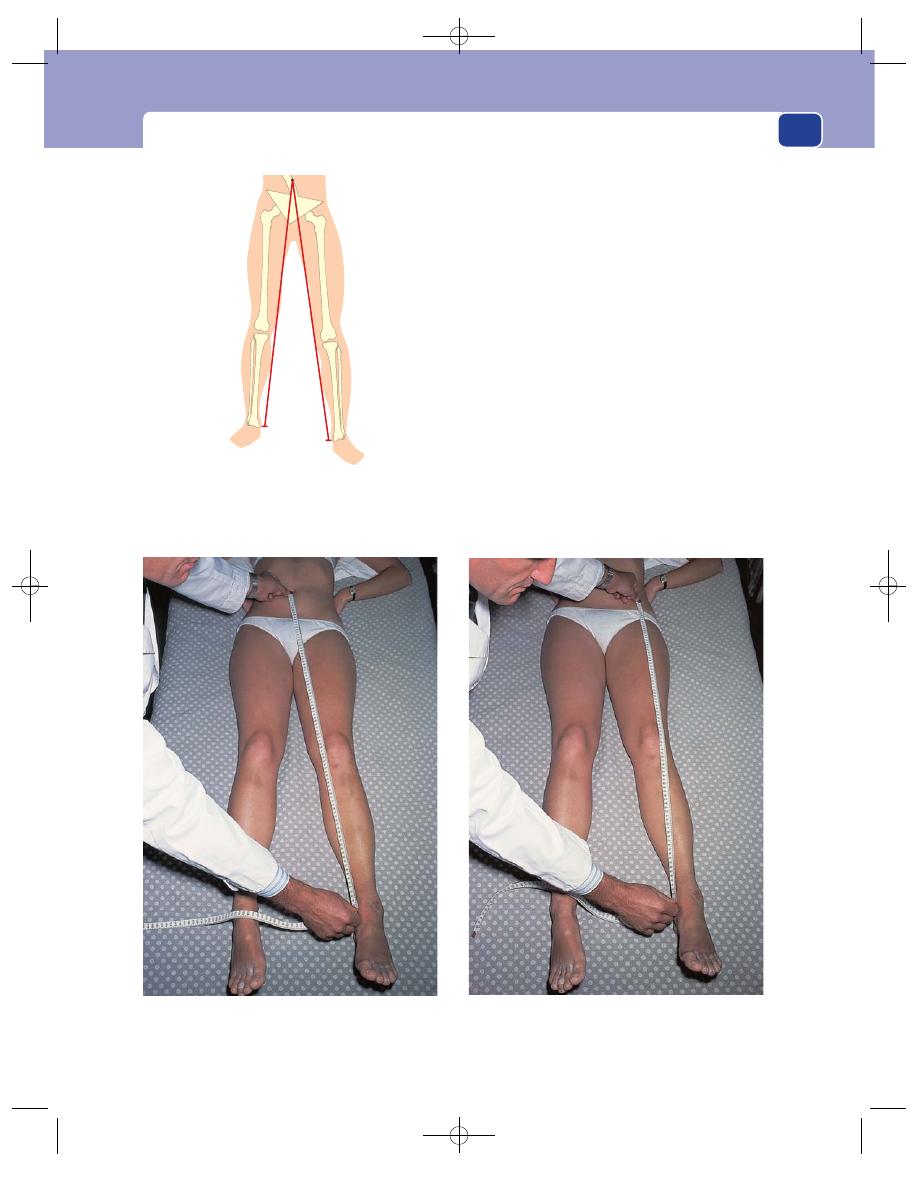
Examination of bones
115
Real length of the limb
To find out the real length of the limb (i.e. the com-
bined length of the limb bones and joints, unaffected
by the position of the spine, pelvis or hip joints) you
must measure between bony points at each end
of the limb with the joints in identical positions.
The customary points to use in the leg are the
anterior superior iliac spine and the tip of the
medial malleolus.
The position of the joints profoundly affects this
measurement. Figure 4.12a shows the measurements
between the iliac spine and the medial malleolus in
a patient, lying straight in bed, with disease of the
left hip which has caused some fixed abduction.
In order to lie straight in the bed the patient has
tilted his pelvis and adducted the other hip. If you
measure between the iliac spine and malleolus in
this position, you are bound to get different meas-
urements, because one hip is abducted and the other
adducted.
FIG 4.11
MEASURING LIMB LENGTH.
FIG 4.10
The apparent length of the limbs is measured from a
central point with the patient lying comfortably straight. It is not
possible with this measurement to tell whether any difference
in limb length is caused by a bone or a joint abnormality.
Measuring apparent limb length using the umbilicus as the
measuring point.
Measuring real limb length using the anterior superior iliac
spine as the measuring point.
Chap-04.qxd 4/19/05 13:50PM Page 115
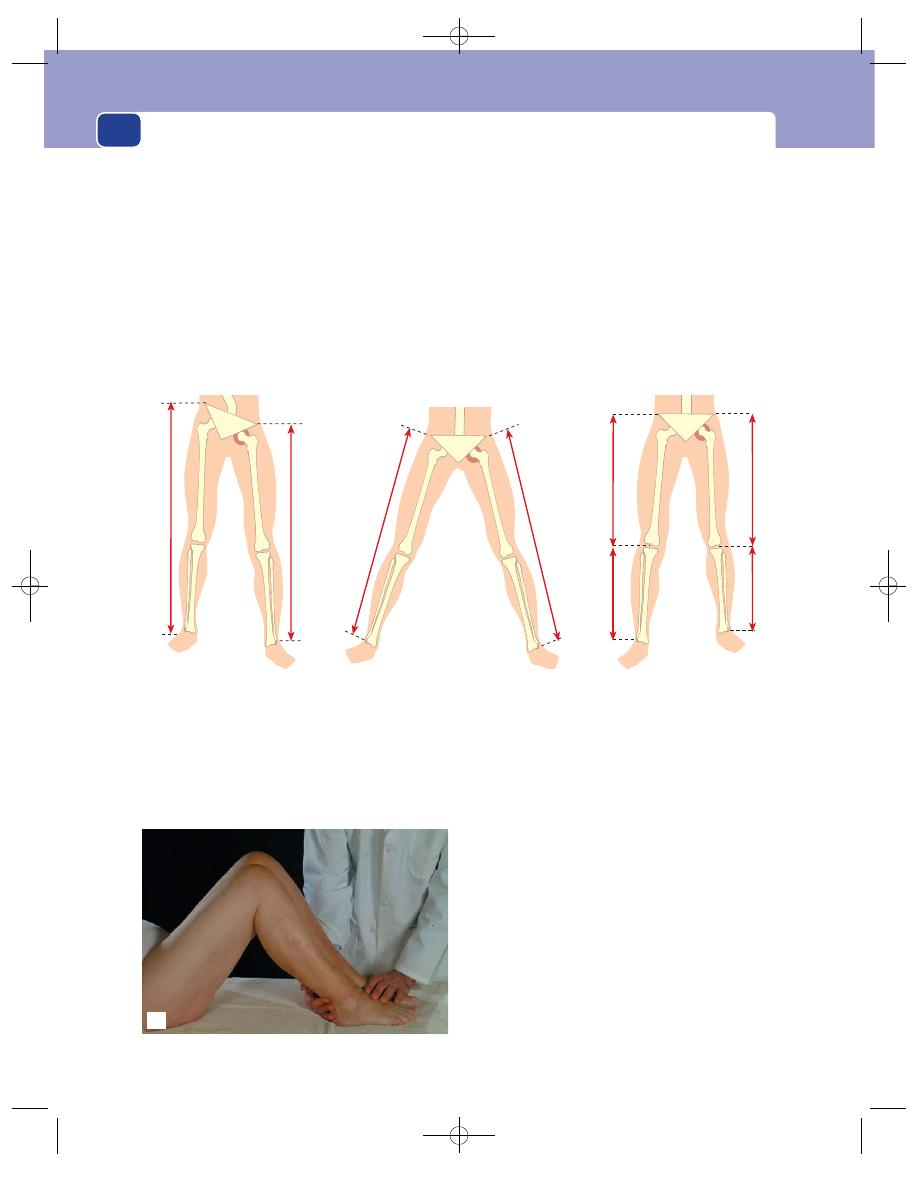
Muscles, tendons, bones and joints
116
Before measuring real limb length, place the
joints of both limbs in identical positions (see Figs
4.12b and c).
Begin by getting the pelvis square to the sagittal
plane by checking that both iliac spines are in the
same plane at a right-angle to the line of the spine.
After doing this you may find the femur on the dis-
eased side abducted or adducted. Place the good leg
in the same position. Check that the positions of the
knee joints are identical – if one has some fixed flex-
ion, flex the good side to the same degree.
Now you can measure on both sides, from ante-
rior superior iliac spine to medial malleolus, and get
a true comparison of real leg lengths.
Joint deformities
Record the deformity of a joint in terms of the
angle by which the distal bone is deviated from the
No
You cannot detect the real
length of the limbs like this
because the joints are in
different positions
Yes
To measure the true lengths of the limbs
you must put the joints in identical positions.
This patient has a fixed abduction of the
left hip so the right hip was abducted to the
same degree before measuring
To detect the site of bone
shortening you must
measure the length of
each bone
(a)
(b)
(c)
(d)
A quick method of detecting difference in bone length is to
put the heels together, with the knees flexed, and look from
the side and the end of the bed. This patient has shortening of
the right tibia and femur.
FIG 4.12
MEASURING LIMB LENGTH.
Chap-04.qxd 4/19/05 13:50PM Page 116
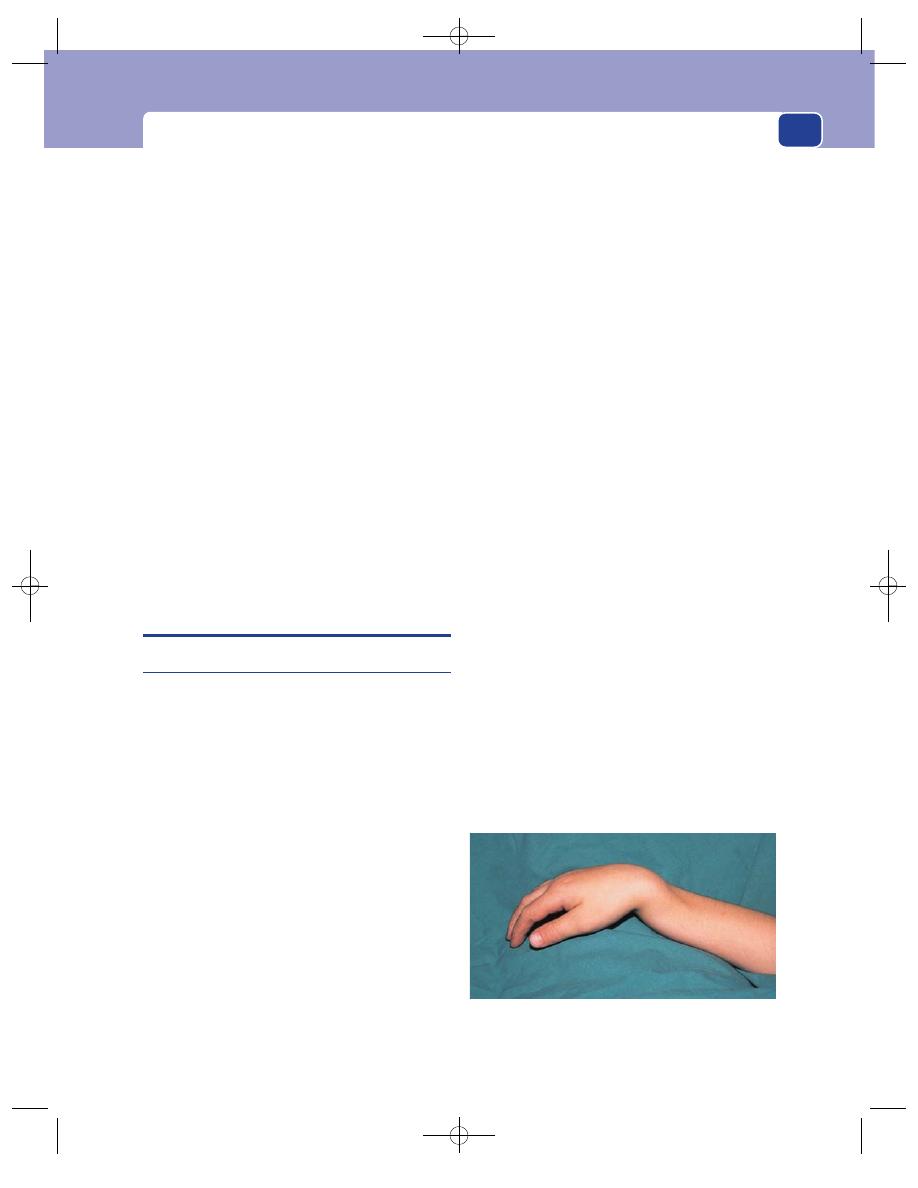
Fractures
117
sagittal plane (i.e. the angle of varus or valgus – see
page 128). Bones may also be rotated on their long
axis. Assess the angle of rotation from the displace-
ment of the bony protuberances.
Movement
Examine the joints at both ends of the bone. Also
make certain that each bone moves as one piece.
A fracture of a long bone may be obvious by pain-
ful abnormal movement within the bone itself.
Furthermore a false joint that has developed in the
shaft of a long bone as a result of non-union of a
fracture may also produce abnormal movements,
which if longstanding may actually be pain free.
Percussion
The bone may not be tender when touched but
painful if percussed. This indicates an abnormality
deep inside the bone. Many of the long bones can be
percussed using the heel of your hand. Other bones,
such as the pelvis and vertebral column, have to be
firmly struck with the side of a clenched fist to elicit
deep tenderness. Percussion is seldom indicated and
need not be part of a routine examination.
FRACTURES
The clinical signs of a fracture
Inspection
Look for the following signs.
■
Deformity Measure and record any:
angulation
rotation
displacement
shortening.
These may be better assessed on X-rays
(see next column).
■
Swelling
■
Any compound wounds (i.e. any wounds that
reach to the site of the fracture) These should be
assessed accurately and measured and recorded
using the Gustillo classification:
– Grade 1: wounds less than 1 cm
– Grade 2: wounds measuring 1–10 cm
– Grade 3: wounds greater than 10 cm plus:
A: no periosteal stripping
B: periosteal stripping
C: neurovascular damage.
Palpation
■
Bony tenderness
■
Crepitus
■
Soft tissue damage This is often graded as follows:
Grade 0: little or no soft tissue injury;
Grade 1: superficial abrasion with moderate
swelling and bruising;
Grade 2: deep abrasion, tense swelling with
bruising and blistering;
Grade 3: extensive contusion, tense swelling,
compartment syndrome and/or vascular damage.
Movement
■
Abnormal/painful movement Do not cause
the patient extra discomfort just to confirm
abnormal movement. Furthermore, such
abnormal movement may cause further soft
tissue damage and further periosteal stripping.
X-rays
In the case of bone fractures, X-rays are almost a
continuity of the clinical examination. When con-
sidering ordering the appropriate views, follow the
‘Rule of twos’.
■
Two views: usually an anterior/posterior view
(AP) and a lateral view.
■
Two joints: include the joint above and the joint
below the bone under consideration.
■
Two sides: useful for comparison, particularly
in children, because it allows comparison of the
epiphyseal lines in immature bones and
distinguishes them from the fracture line.
All X-rays should be centred on the area of maxi-
mal tenderness.
FIG 4.13
The classical dinner-fork deformity of a Colles’
fracture, in this case in a child with a Colles’ type fracture
through the distal epiphysis of the radius and ulna.
Chap-04.qxd 4/19/05 13:50PM Page 117
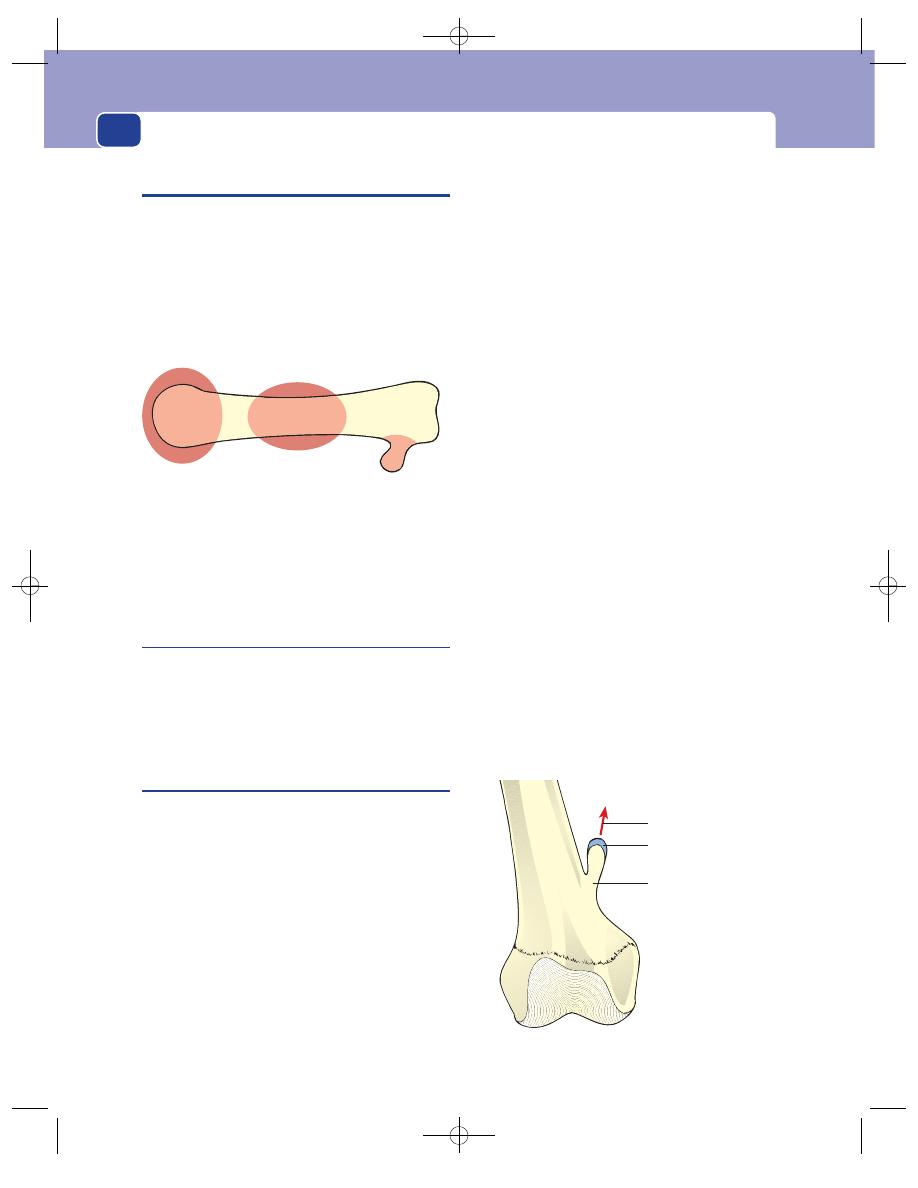
Muscles, tendons, bones and joints
118
BONE DISEASES AND DEFORMITIES
It is vital to make an accurate diagnosis of any bony
lump, as bony swellings can be entirely benign or
highly malignant lesions. The clinical presentation
may provide some useful hints as to the underlying
nature of the lesion, although radiological assis-
tance is usually required. The actual site of a lesion
in a long bone may give some clue as to the under-
lying pathology, as is demonstrated in Figure 4.14.
Exostosis
As the word implies, an exostosis is a lump which
sticks out from the bone. The lump is mainly can-
cellous bone with a covering of cortical bone and a
cartilaginous cap. Exostoses are usually single but
may be congenital and multiple.
Solitary (diaphyseal) exostosis
Exostoses are derived from small pieces of metaphy-
seal cartilage which were not remodelled during the
growth of the bone and have become separated from
the main cartilaginous epiphyseal plate. Although
isolated and left on the side of the shaft (diaphysis)
of the bone, they continue to grow and ossify and so
produce a bony knob just above the epiphyseal line.
They sometimes have an adventitious bursa over
their cap. They are not neoplasms.
History
Age
Exostoses present when they are large enough
to cause symptoms – usually in teenage and early
adult life.
Symptoms
The patient may have felt the lump or
it may have become noticeable and cosmetically
disfiguring. Because exostoses are near joints, they
sometimes interfere with the movement of the joint
and its tendons. Patients may find the movements of
the joint limited or associated with ‘clicks’ or ‘jumps’
as the tendons slip over the lump.
The overlying bursa, if present, may become
enlarged and inflamed.
Examination
Position
Exostoses are usually found adjacent to the
epiphyseal line of the bone, just on the diaphyseal
side. The majority occur at the lower end of the
femur and upper end of the tibia.
Shape and size
Initial palpation gives the impression
of a sessile, smooth, hemispherical protuberance,
but with careful palpation it is often possible to feel
that the base is quite narrow and that the exostosis
leans away from the joint.
Exostoses are usually 1–2 cm in diameter when
they are first noticed, but if they are not removed
they may enlarge until all their cartilaginous cap is
ossified, and become so large (4–5 cm across) that
they interfere with joint movement.
Surface
Their surface is smooth.
Composition
Exostoses are bony hard but their con-
sistence may be masked by a soft, fluctuant bursa
overlying their cap.
Relations
They are fixed to the underlying bone. It is
important to palpate the lump while the adjacent
On surface,
at end
Exostosis
Ecchondroma
Expanding
one end
Osteoclastoma
Osteosarcoma
Centre
Callus
Secondary tumour
Enchondroma
FIG 4.14
Relationship between the site of a bony lump and
its cause.
Cartilaginous cap
Points away from
the joint
Narrow pedicle
FIG 4.15
The features of a solitary exostosis.
Chap-04.qxd 4/19/05 13:50PM Page 118
Bone diseases and deformities
119
joint is moving to feel which muscles and tendons
lie close to the lump and to measure the range of
joint movement.
Local tissues
The rest of the bone and the nearby
joint should be normal.
Multiple exostoses
(diaphyseal aclasis)
This is a hereditary condition. It is carried in an auto-
somal dominant manner, so half the patient’s chil-
dren can be expected to have the abnormality. Boys
are more susceptible than girls. All the bones that
ossify in cartilage can be affected, with the exception
of the spine and skull. Because this condition is
caused by a widespread generalized abnormality of
bone remodelling at the epiphyseal line, as opposed to
the sporadic event that produces a solitary exostosis,
the long bones may be a little shorter than normal.
The clinical features of each exostosis are similar
to those described for the solitary variety. They are
multiple and especially common on the limb bones.
They can grow to a considerable size up to 5–10 cm
in diameter.
Callus
Perhaps the commonest cause of thickening of a bone
is callus. Callus is the buttress of new bone formed
around a fracture site to unite and strengthen it
while the cortical bone is being slowly repaired.
History
In the majority of cases the patient knows of the injury
and the subsequent discomfort associated with the
fracture that caused the callus, but this is not always
the case. Some fractures are caused by minor stress, or
stress that the patient does not connect with the
breaking of bones, such as coughing causing a fracture
of the ribs. Furthermore, not all fractures cause severe
pain, so the absence of a history of trauma or pain
does not necessarily exclude the possibility that the
lump might be callus, but makes it unlikely.
Examination
Position
The thickening of a bone by callus should
be greatest at the site of the fracture, but it may be
asymmetrical if the stresses on the bone do not run
directly down the centre of the shaft.
Tenderness
Mature callus is not tender. Once a frac-
ture has united, there is no local tenderness, and if
an area of thickening in a bone is tender, it is
unlikely to be callus around a united fracture. It may
be callus around non-union, but other signs of non-
union will be present.
Shape
Callus usually causes a fusiform enlargement
of the whole bone – thickest at the site of the fracture.
Surface
Newly formed callus has an irregular sur-
face but it becomes smooth as time passes. In young
people callus is eventually completely resorbed.
Local tissues
Callus may surround a deformed bone –
angulated or rotated – if the fracture was not set
properly.
Paget’s disease of bone
(Osteitis deformans)
This condition occurs in later life. Normally, bone is
continually repaired and replaced throughout life.
This process follows the same pattern as the original
ossification. The ossified cartilage that is reorgan-
ized into mature bone is called osteoid bone. In
Paget’s disease the repair process stops at the osteoid
bone stage so that the healthy, mature bone is grad-
ually replaced by thick, bulky, very vascular osteoid
bone. If the repair process stops a stage earlier, the
old bone, which has been absorbed by the osteo-
clasts, is replaced by fibrous tissue. This makes the
bone very weak.
Paget’s disease of bone usually affects many bones
but can affect just one bone in the whole skeleton
(monostotic Paget’s disease). Osteogenic sarcoma
complicates 1 per cent of cases.
History
Age
The patient is rarely under 50 years of age,
often much older.
Symptoms
Pain is the commonest symptom. As the
bones enlarge and become more vascular, the patient
feels a deep-seated aching, gnawing pain in the
bone. They can usually tell that it is deep-seated but
may have difficulty in appreciating its skeletal ori-
gin. The back is the commonest source of pain.
Make a careful note of any change in the nature
and severity of the pain. This may indicate malig-
nant change.
Chap-04.qxd 4/19/05 13:50PM Page 119
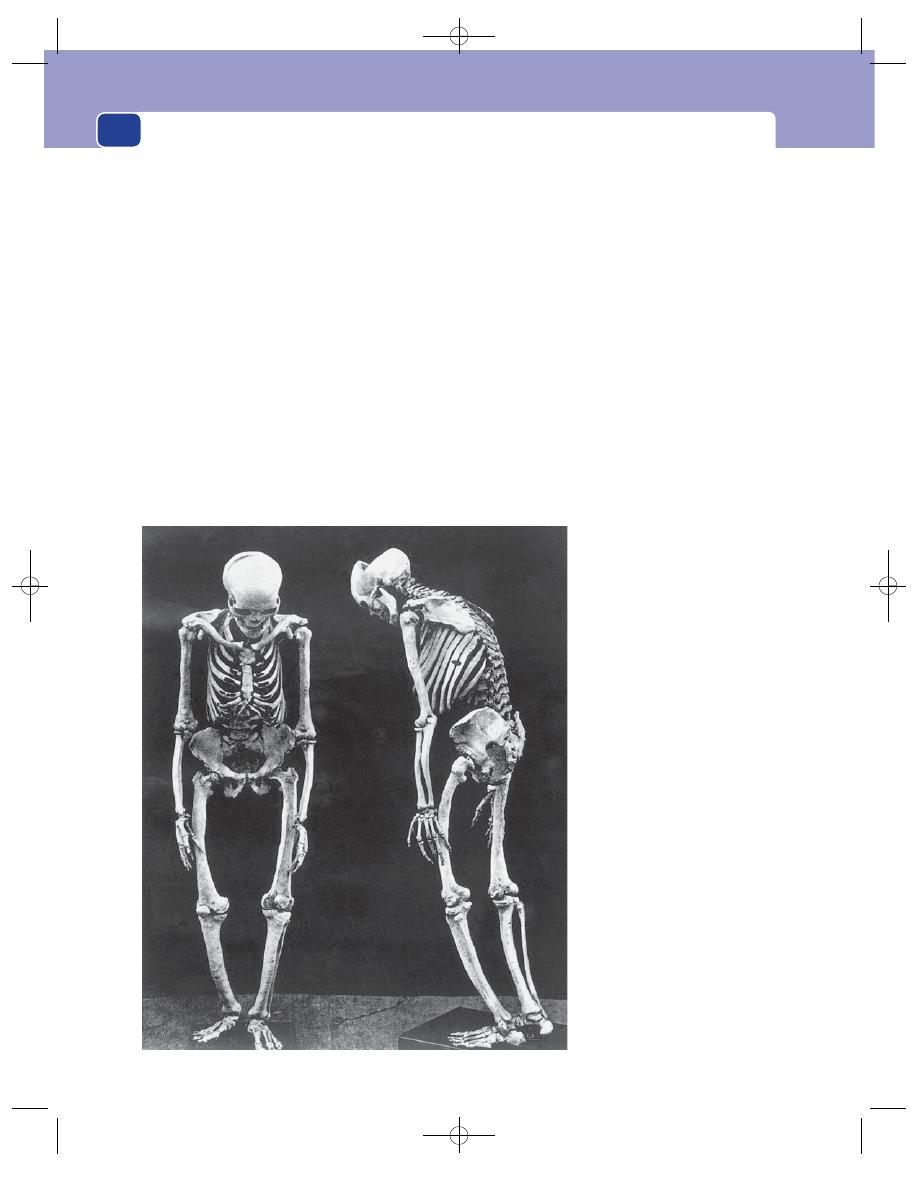
Muscles, tendons, bones and joints
120
Deformity
The bone grows bigger and bends. The
typical complaints are:
■
enlargement of the skull so that the patient’s hat
no longer fits and the frontal bones become
prominent;
■
curvature of the spine, causing a kyphosis and
increasing difficulty with fitting clothes; patients
occasionally complain that they are getting
shorter;
■
bowing of the legs.
Headache
This pain is caused by the changes in the
vascularity of the skull bones but is mentioned as a
separate symptom because the patient rarely associ-
ates the headache with the skull changes.
Deafness
Paget’s disease in the temporal bones may
affect the middle ear and cause otosclerosis and
deafness. The patient may also develop vertigo.
Examination
General appearance
The patient with generalized dis-
ease has a large head, a bent back, arms that seem
too long (because of the kyphosis) and bow legs.
Cardiovascular system
Examine the cardiovascular
system with care. The increased bone blood flow
causes an increased cardiac output. The heart may
be enlarged, there may be an aortic ejection mur-
mur and the blood pressure may be elevated. It is
claimed that Paget’s disease can cause a high-output
heart failure, but this is a very uncommon occur-
rence. What is common is the exacerbation of any
myocardial ischaemia, secondary to coronary vessel
disease, by the extra demands placed upon the heart
of an old person.
Respiratory system
The patient may have râles and
rhonchi at both lung bases if the kyphosis is severe
FIG 4.16
The skeleton of a man who
had extensive Paget’s disease. All the
bones are thick. The kyphosis makes
the arms seem long. The left femur is
split in the coronal plane, revealing
the thickening of the cortical bone.
(Reproduced by kind permission of
the Curator of the Pathology Museum
of the Royal College of Surgeons, and
the Medical Illustration Unit.)
Chap-04.qxd 4/19/05 13:50PM Page 120
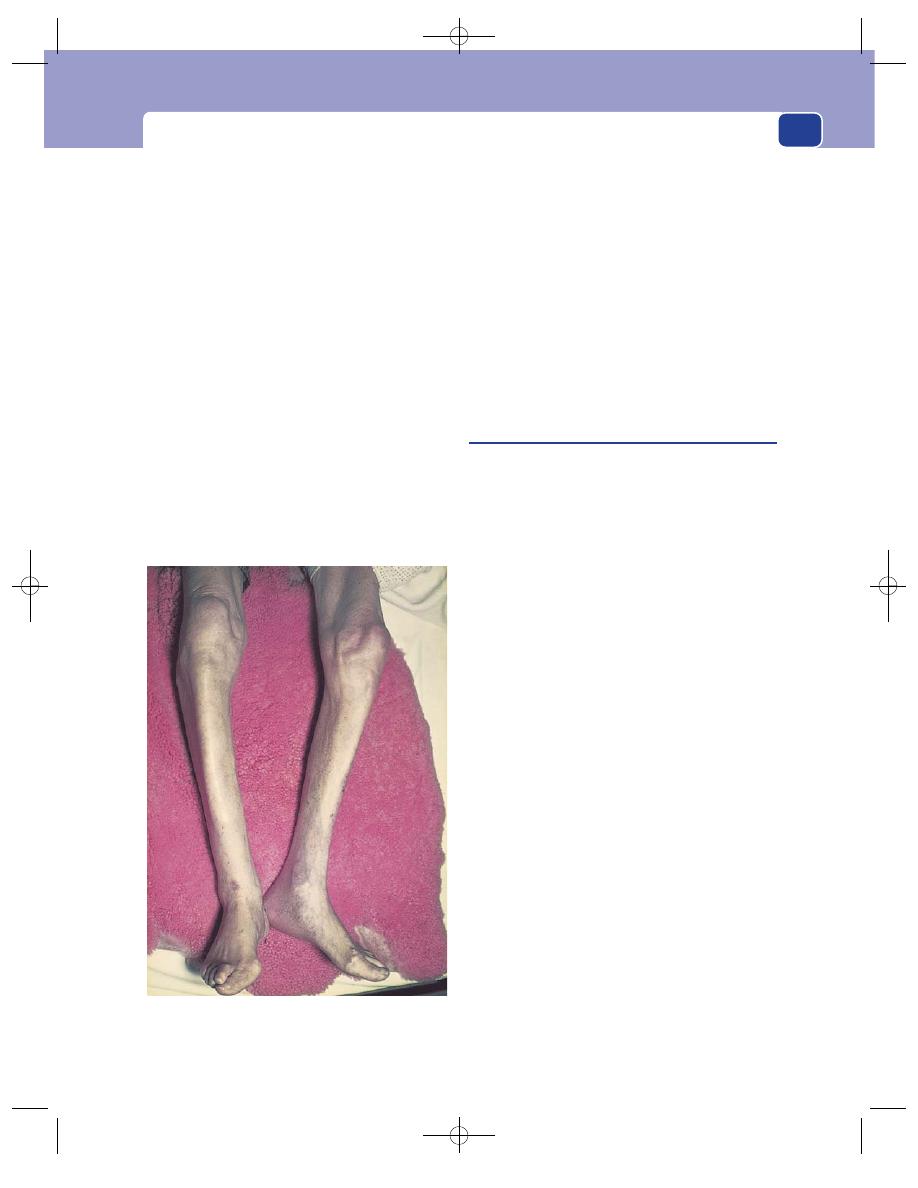
Bone diseases and deformities
121
enough to interfere with the movements of the
chest wall.
Skeleton
■
Skull the enlargement occurs in the vault. The
dome looks swollen and the enlarged frontal
bones make the forehead bulge forwards.
Deafness is common.
■
Spine The disease usually affects the whole
skeleton, so producing an even kyphosis. The
shoulders are rounded and the head and neck
protrude anteriorly.
■
Legs The femur and the tibia may bow in both
anterior/posterior and lateral directions. The
sharp anterior edge of the tibia becomes so
prominent that the description ‘sabre tibia’ is
apt, although this expression is usually reserved
for bowing caused by syphilis and yaws.
When examining the skeleton, look for any local-
ized bony enlargement, especially in the areas where
the pain is severe or has changed. A swelling of
the bone that is painful, a little tender and warm
to the touch suggests the presence of sarcomatous
change.
Central nervous system
The patient may have a con-
duction deafness and difficulty when standing, caused
by middle ear and vestibular apparatus damage. The
function of other cranial nerves can be affected if
the thickening of the bones reduces the size of the
foramina in the base of the skull. Blindness can
occur if the optic nerves are compressed.
Spinal nerves may also be damaged by collapse of
the vertebrae.
Acute osteomyelitis
Bone can become infected by organisms which reach
it through the bloodstream or directly through a
wound. Blood-borne organisms are probably trapped
in thrombi or haematomata caused by minor trauma,
usually in the capillary loops in the part of the
shaft adjacent to the epiphyseal line known as the
metaphysis.
The common infecting organisms are strepto-
cocci and staphylococci.
History
Age
Patients with acute osteomyelitis are usually
between 1 and 12 years old.
Symptoms
The site of infection is painful, though in
the early stages this is only a deep-seated ache. When
pus forms and the intramedullary tension increases,
the pain becomes intense and throbbing.
There is usually some swelling around the pain-
ful area, but this is not marked as it is caused by
diffuse oedema of the overlying tissues, not swelling
of the bone.
The patient may notice that the adjacent joint is
swollen and stiff.
The infection causes a loss of appetite and gen-
eral debility. Most patients feel hot and sweaty and
may suffer from rigors.
Examination
Site
The bones commonly infected are the tibia,
femur, humerus, radius and ulna.
Colour
The skin over the painful area may be red or
reddish-brown.
FIG 4.17
‘Sabre tibiae’. The anterior edge of the tibia is
normally straight and sharp. In this patient, Paget’s disease
has made these edges thick and curved.
Chap-04.qxd 4/19/05 13:50PM Page 121
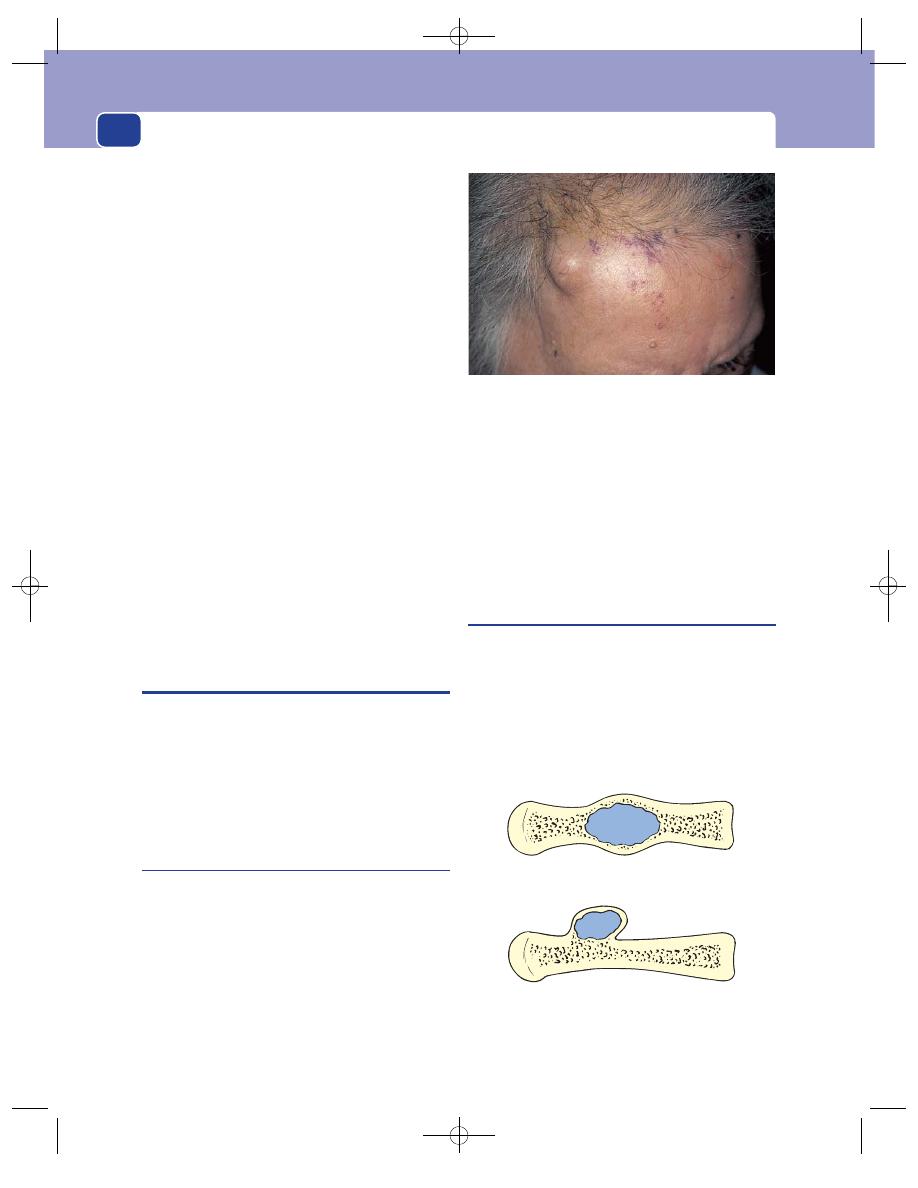
Muscles, tendons, bones and joints
122
Temperature
The skin does not become palpably hot
until the infection has spread through the bone into
the subperiosteal layer.
Tenderness
The swollen area is tender and the whole
bone is sensitive. Percussion on the end of the bone
is painful.
Consistence
Any swelling is soft and indistinct
because it is caused by oedema of the overlying
structures. If there is pus near the surface, there may
be an area which fluctuates.
Lymph glands
The local lymph glands will only be
enlarged if the infection has spread outside the bone.
Surrounding structures
The overlying skin may be oede-
matous. The neighbouring joint may be swollen by
an effusion and its movements limited and slightly
painful. If the joint movements are very restricted
and painful, the infection has probably spread into
the joint and caused a septic arthritis.
The subcutaneous veins of the limb are often
dilated.
General examination
The patient looks ill and fever-
ish. Their face may be flushed and their temperature
raised. If the patient has a septicaemia, they may be
hypotensive, sweating, possibly shaking and have a
dry tongue and oliguria.
BENIGN TUMOURS OF BONE
Benign tumours of bone fall into two categories:
those arising from cortical bone (the so-called
‘ivory’ osteoma) and those which are primarily car-
tilage tumours but arise within or on the surface of
long bones (enchondroma and ecchondroma). An
exostosis (described earlier in this chapter) is not a
benign neoplasm.
Osteoma
History
The patient complains of a lump which they have
either felt or had drawn to their attention. These
lumps are not painful and rarely occur in a site that
interferes with joint or tendon movements.
Examination
Site
Osteomata are common on the surface of the
vault of the skull, frequently the forehead.
Shape and size
They are sessile, flattened mounds
with a smooth surface.
Consistence
Osteomata are bony hard – hence the
name ‘ivory’ osteoma.
Relations
Nearby muscles and fascia move freely
over the lump, which is obviously fixed to and an
integral part of the underlying bone.
Chondroma
A chondroma can grow inside a long bone only
if a piece of the cartilage from which the bone
developed fails to become converted to bone.
An enchondroma is a chondroma growing in the
centre of the bone; an ecchondroma is a chondroma
growing on the surface of the bone. There is no
pathological difference between these two varieties
of chondromata.
FIG 4.18
An osteoma of cortical bone – an ‘ivory’ osteoma –
on the forehead, which has been present for 40 years.
ENchondroma
ECchondroma
FIG 4.19
The two varieties of chondromata that are found in
long bones.
Chap-04.qxd 4/19/05 13:50PM Page 122
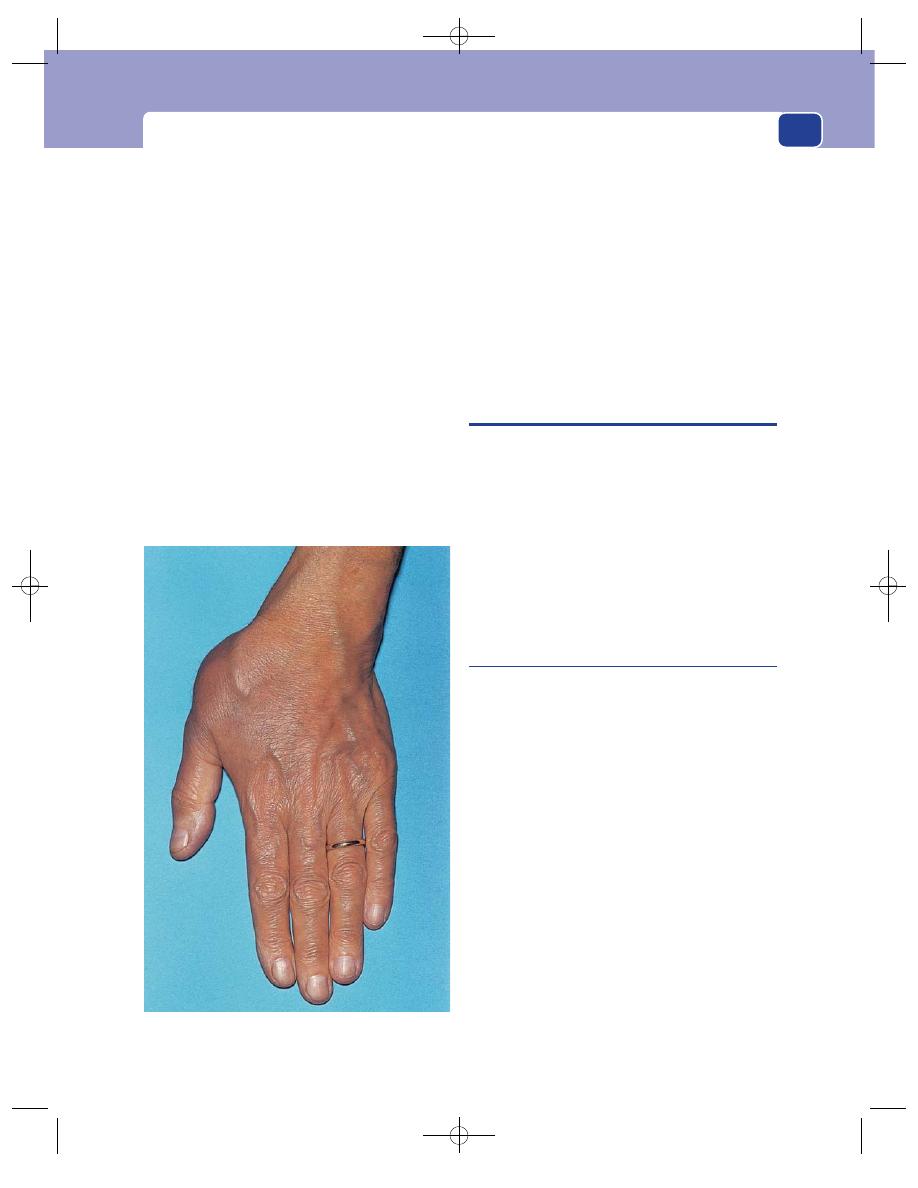
Malignant tumours of bone
123
When the chondromata are multiple and con-
genital (but not familial), the condition is called
dyschondroplasia or Ollier’s disease.
History
Age
Chondromata usually present in teenage or
early adult life.
Symptoms
The patient notices either that a bone is
gradually expanding or that a lump is appearing on
the side of a bone.
Neither type of chondroma is painful, but an
ecchondroma may interfere with joint and tendon
movement.
Examination
Site
Chondromata are common in the bones of the
hands and feet but may occur anywhere. Large, long
bones are rarely affected, except when the patient
has congenital and multiple chondromata (Ollier’s
disease).
Temperature
The overlying skin has a normal tem-
perature.
Shape
Enchondromata cause a fusiform enlarge-
ment of the shaft of the bone. Ecchondromata form
a sessile lump on the surface of the bone.
Surface
The surface of both varieties is smooth.
Consistence
As chondromata are usually covered by
a thin layer of cortical bone, they feel hard.
MALIGNANT TUMOURS OF BONE
Malignant tumours in bone are either primary or
secondary. The secondary deposit is by far the most
common and is usually a metastasis from one of the
carcinomata listed below.
There are four primary tumours of bone:
■
osteosarcoma
■
reticulum cell sarcoma (Ewing’s tumour)
■
giant cell tumour (osteoclastoma)
■
multiple myeloma.
These are all relatively rare tumours.
Secondary (metastatic) tumour
The primary cancers that commonly metastasize to
bone are to be found in the lung, breast, kidney,
thyroid and prostate. The first four tend to produce
lytic-type lesions as seen on radiographs, while pro-
static secondaries tend to appear sclerotic.
These are the five to keep uppermost in your mind,
but also remember that any tumour can metastasize
to bone.
The bones most often afflicted by secondary
deposits are the vertebral bodies, pelvic bones, ribs
and the upper ends of the femur and the humerus,
because these bones contain red bone marrow and
so have a good blood supply.
History
General features
Patients often give a history of a pre-
vious disease and its treatment (e.g. a mastectomy
for a lump in the breast). If not, they are likely to be
complaining of symptoms related to the primary
growth, such as a cough with haemoptysis, or diffi-
culty with micturition.
FIG 4.20
A large ecchondroma of the metacarpal bone of
the thumb.
Chap-04.qxd 4/19/05 13:50PM Page 123

Muscles, tendons, bones and joints
124
Some patients develop bony secondary deposits
with no signs or symptoms to indicate the site of the
primary lesion.
Symptoms
The commonest symptom is pain. Low
back pain or pain in the pelvis and hip is often the first
indication of the existence of secondary deposits.
Acute pain will occur if there is a pathological
fracture, such as the collapse of a vertebral body or a
fracture of the femur. The patient rarely notices any
swelling at the site of a metastasis unless it is in a
superficial bone such as the vault of the skull, the
clavicle or a rib.
Examination
If the metastases are deep-seated, they may present
no physical signs except pain on movement and ten-
derness on percussion.
When superficial, they may cause a swelling of
the bone which appears rapidly and grows steadily.
The consistence of a secondary deposit in a bone
may vary from hard and bone-like to soft, com-
pressible and even pulsatile.
Carcinoma of the kidney is a source of very vas-
cular secondary deposits, so vascular that in certain
more advanced cases they may pulsate dramatically
and even be misdiagnosed as aneurysms.
Osteosarcoma
This is a malignant sarcoma of bone. It is seen in
two groups of patients:
■
the young
■
the elderly with Paget’s disease.
Sarcoma complicating Paget’s disease has already
been described (see page 119).
Osteosarcoma spreads early and rapidly by the
bloodstream.
History
Age
Primary osteosarcoma occurs in childhood and
the teenage years.
Symptoms
Pain is the predominant symptom. It usu-
ally begins before the patient notices a lump and is a
persistent ache or throb.
Swelling of the bone may be noticed and in some
instances this increases rapidly.
The development of general malaise, cachexia
and loss of weight may precede or coincide with the
appearance of local symptoms.
Pulmonary metastases may cause a cough and
haemoptysis.
Abdominal discomfort and jaundice may follow
the enlargement and destruction of the liver by
metastases.
Patients will often relate the onset of their symp-
toms to an injury, but there is no evidence that
Breast
Thyroid
Lung
Prostate
Kidney
FIG 4.21
Common sources of bone metastases.
Upper end
of humerus
Ribs
Vertebrae
Pelvis
Upper end
of femur
FIG 4.22
Common sites for skeletal metastases.
Chap-04.qxd 4/19/05 13:50PM Page 124
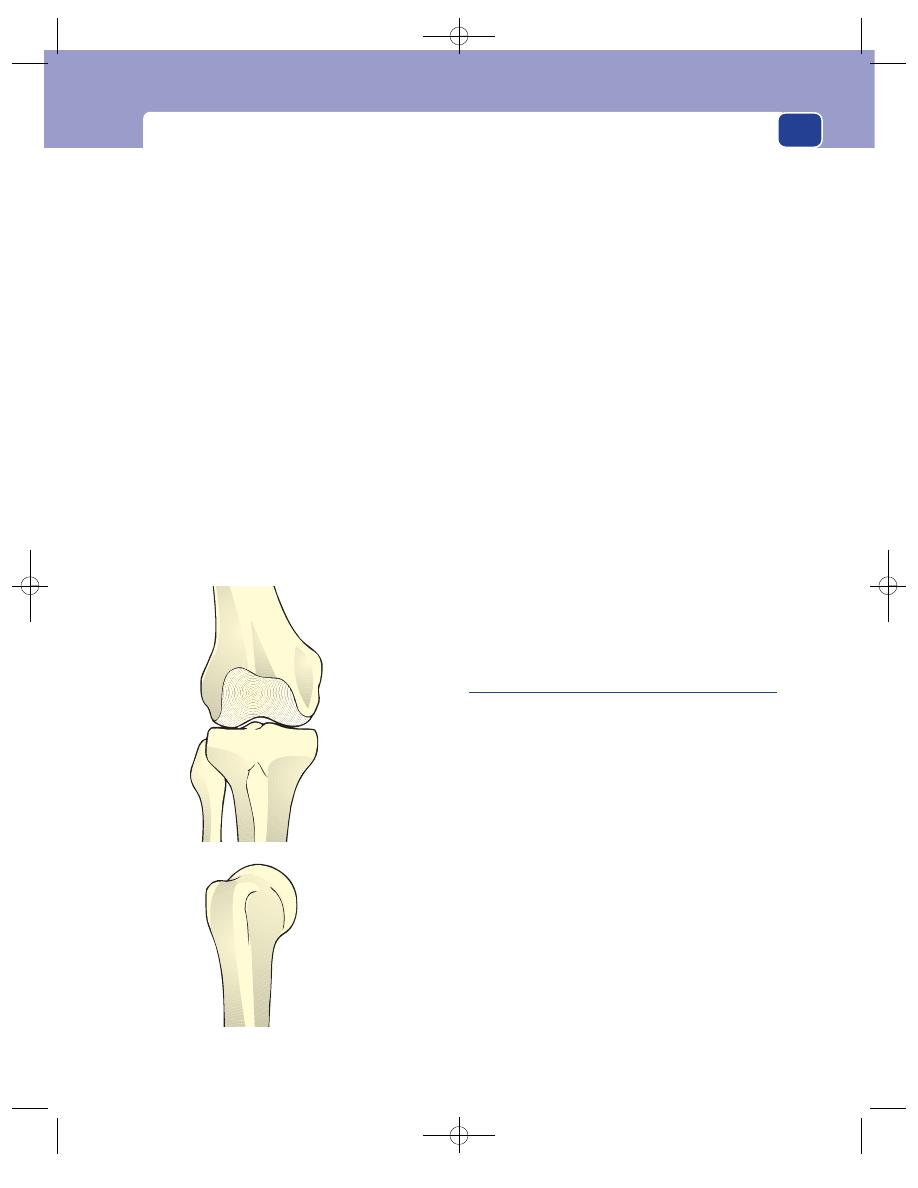
Malignant tumours of bone
125
trauma causes sarcoma. The injury simply focuses
patients’ attention on symptoms which they had
previously dismissed as trivial and insignificant.
Examination
Site
The commonest place to find an osteosarcoma
is the lower end of the femur. The upper end of the
tibia is the second most common site, followed by
the upper end of the humerus.
Colour
The overlying skin may be reddened and the
subcutaneous veins visibly distended.
Tenderness
The swelling may be slightly tender
but not exquisitely so like osteomyelitis. Any red,
warm, non-tender bony swelling should, in the first
instance, be considered to be a tumour and not an
infection.
Temperature
The skin over the swelling is usually
warm, sometimes quite hot.
Shape
The swelling tends to appear on one side of
the lower end of the bone, making it asymmetrical.
Surface
Its surface is smooth unless it has spread into
the surrounding tissues, when it becomes irregular.
Consistence
Bony sarcomata feel firm but not bony
hard. It is a clinical aphorism that benign tumours
of bone feel hard whereas malignant tumours of
bone feel soft. A very vascular tumour may pulsate.
Relations
The structures overlying a small osteosar-
coma are mobile but become fixed to it if the
tumour spreads locally beyond the bone.
Lymph drainage
The draining lymph glands will not
be enlarged in the early stages of the disease, which
may be another indication that the red, warm
swelling is not an infection. However, when the
tumour invades the surrounding soft tissues, it may
then spread to local lymph glands.
Local tissues
The nearby joint often becomes stiff
and develops an effusion. The adjacent artery and
nerves are only involved in advanced local disease.
General examination
Take particular care to examine
the chest and the abdomen because the lungs and
the liver are common sites for metastases. There
may be generalized wasting, and wasting of the
muscles of the affected limb.
Reticulum cell sarcoma
(Ewing’s tumour)
This is a tumour which appears most often, but not
exclusively, in the centre of long bones – a feature
that helps distinguish it from osteosarcoma and
osteomyelitis. The cells of this tumour have a dis-
tinct reticulate staining. In many instances the
tumour represents a secondary deposit from an
adrenal neuroblastoma, but there is a primary vari-
ety whose cell of origin is not known.
History
Age
Ewing’s tumour occurs in childhood and the
teenage years.
Symptoms
The commonest symptom is a persistent
ache or pain made worse by movement.
As the femur is the bone most often affected,
many children present with a limp.
These tumours can sometimes present as a
pyrexia of unknown origin (PUO) and cause rigors
and night sweats.
Lower end
of femur
Upper end
of tibia
Upper end
of humerus
FIG 4.23
The common sites to find osteosarcomata.
Chap-04.qxd 4/19/05 13:50PM Page 125
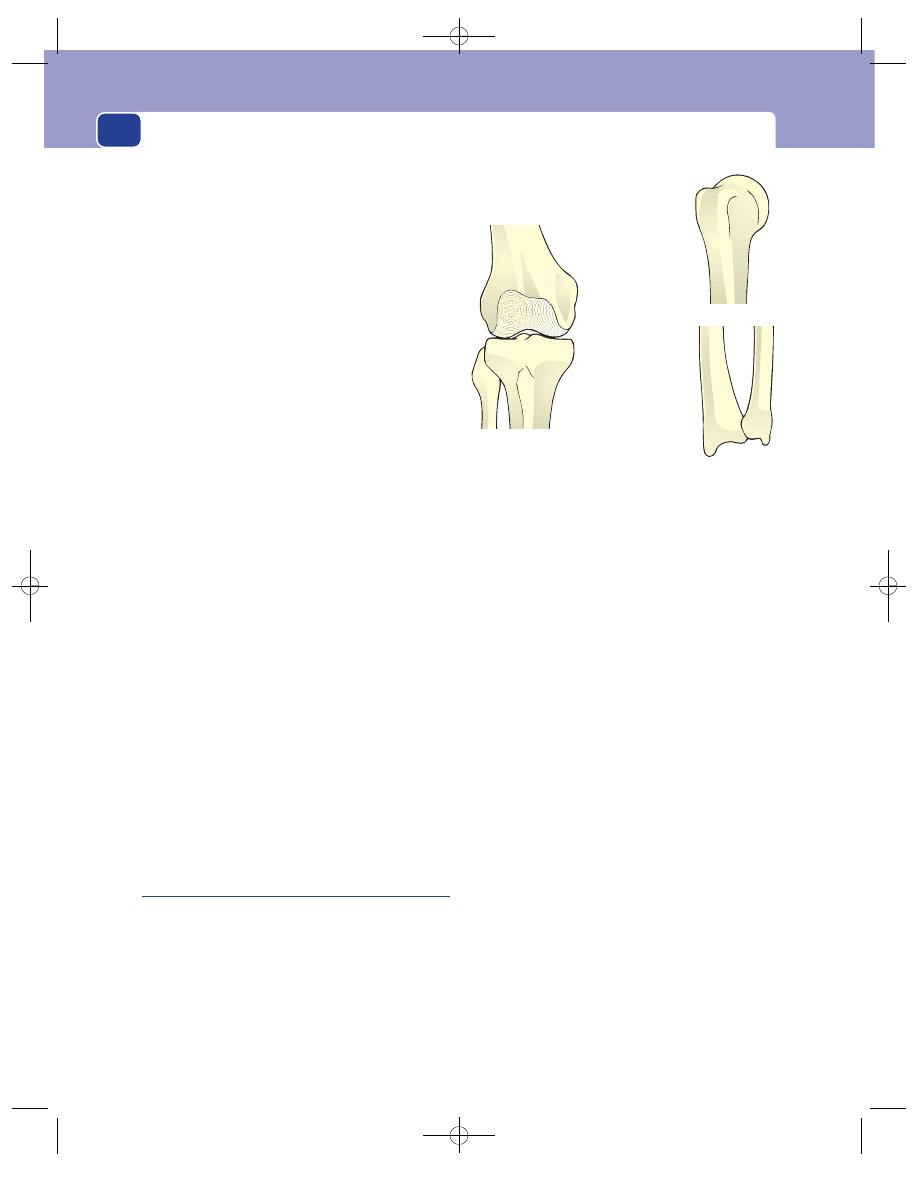
Muscles, tendons, bones and joints
126
There may be weight loss and malaise, especially
if the lesion is a metastasis from a neuroblastoma.
Examination
Site
The mid-shaft of the femur is the commonest
site to find these tumours, but the tibia and the
humerus can be affected.
Colour
The overlying skin may be reddened.
Tenderness
The swelling is usually a little tender.
Temperature
The increased vascularity makes the
whole area feel warm.
Shape
The tumour causes a symmetrical fusiform
enlargement of the shaft of the bone, the upper and
lower limits of which are indistinct.
Surface
The surface of the swelling is smooth.
Consistence
When the bone is so expanded that the
tumour mass is palpable, it feels firm and rubbery,
not bony hard.
Relations
The overlying structures can be moved
over the mass because, although they are displaced,
they are not usually infiltrated.
Lymph drainage
The lymph glands should not be
palpable.
Local tissues
The arteries and nerves of the limb are
rarely involved.
General examination
There may be pyrexia and
generalized wasting. The lungs and liver may reveal
evidence of secondary deposits and, very rarely,
a primary neuroblastoma may be palpable in the
abdomen as a lobulated mass in the upper part of
the abdomen, which may cross the mid-line.
Giant cell tumour
(Osteoclastoma)
These tumours are sometimes classified as having a
variable malignant potential because approximately
one-third are entirely benign, one-third invade
nearby tissues and only one-third metastasize.
History
Age
The patient is usually between 20 and 40
years old.
Symptoms
The usual presenting symptom is pain.
The pain is a dull ache, but may become acute if
there is a pathological fracture.
The patient may also notice swelling of the lower
end of the femur or the upper end of the tibia.
The nearby joint may get stiff if the swelling dis-
turbs the tendons around it, or if the tumour
invades the bone just beneath the articular cartilage.
Examination
Site
The common sites to find giant cell tumours
are the lower end of the femur and the upper end of
the tibia (i.e. either side of the knee), and the upper
end of the humerus and the lower end of the radius
(i.e. away from the elbow).
Colour
The colour of the skin is normal.
Tenderness
The swelling may be tender.
Temperature
These tumours are not usually vascular
and the temperature of the overlying skin should be
normal.
Shape
Giant cell tumours usually cause a diffuse
expansion of the end of a bone but it may be asym-
metrical and noticeable on one side only.
Surface
Their surface is smooth.
Consistence
If the outer layer of bone is reasonably
thick, the lump feels bony hard. If it is thin, it may
feel firm and slightly pliable. When it is very thin it
crackles and bends when touched, and feels like a
broken egg shell.
Lower end
of femur
Upper end
of tibia
Upper end
of humerus
Lower end
of forearm
FIG 4.24
The common sites for giant cell tumours of bone.
Chap-04.qxd 4/19/05 13:50PM Page 126
Examination of a joint
127
It does not pulsate unless very thin walled and
malignant.
Relations
The surrounding structures are usually
freely mobile over the swelling.
Lymph drainage
The local lymph glands should not
be enlarged.
Multiple myeloma
(Plasmacytoma)
This is a disease of the blood and bone marrow
in which multiple deposits of myeloma cells
(plasmacytes) are found throughout the bones
containing red bone marrow – the vertebral bodies,
ribs, pelvis, skull and proximal ends of the femur
and the humerus.
The patient presents complaining of general
malaise, loss of weight and intractable pain in the
skeleton – mostly the back and chest wall.
There may be signs of involvement of other parts
of the blood-forming tissues – enlarged lymph
glands, hepatomegaly and splenomegaly.
Occasionally a deposit in a subcutaneous bone
causes a palpable lump and is the presenting
symptom.
The urine may contain Bence–Jones protein.
JOINTS
EXAMINATION OF A JOINT
Use the same basic approach to examine a joint as
for other aspects of the musculoskeletal system –
inspection, palpation and movement: look at it, feel
it and move it.
Inspection
Overlying skin
What is the colour of the overlying
skin and are there any associated sinuses or scars?
Shape
What is the shape of the joint? Is there
any general or localized swelling? Are there any
deformities?
Malalignment of a joint in the coronal plane, the
plane of abduction and adduction, is known as a val-
gus or a varus deformity. Figure 4.25 illustrates these
terms. When the part of the limb below the joint is
angled away from the mid-line (abducted), there is
a valgus deformity; when the part of the limb below
the joint is angled towards the mid-line (adducted),
there is a varus deformity. Students often get these
deformities confused. The easiest way to remember
them is to remember one deformity and work out the
rules. For example: knock-knees
⫽ genu valgum (the
tibia is angled away from the mid-line).
Do the muscles that move the joint look normal
or wasted? What do the other joints in the limb look
like? In what position does the patient hold the
joint?
Palpation
Skin
Feel the temperature and texture of the skin
over the joint.
Subcutaneous tissues
Are the subcutaneous tissues
normal or thickened?
Muscles
Feel the texture of the local muscles for
wasting and tone. The muscles may be in spasm if
joint movement is painful.
Joint capsule
Is the capsule thickened? Is the thick-
ening diffuse or localized?
Synovium
Is the synovial membrane thickened
and palpable? Is there excess synovial fluid (i.e. an
effusion)?
Bones
Define the contours of the bones that form
the joint. Check that they are in their correct anatom-
ical positions.
Movement
Active movement
Ask the patient to move the joint
through its full range of movements. Record the
degree of any limitation of movement and any asso-
ciated discomfort.
Strength of movements
Make the patient move the
joint against resistance so that you can assess the
strength of the muscles producing each movement.
Chap-04.qxd 4/19/05 13:50PM Page 127
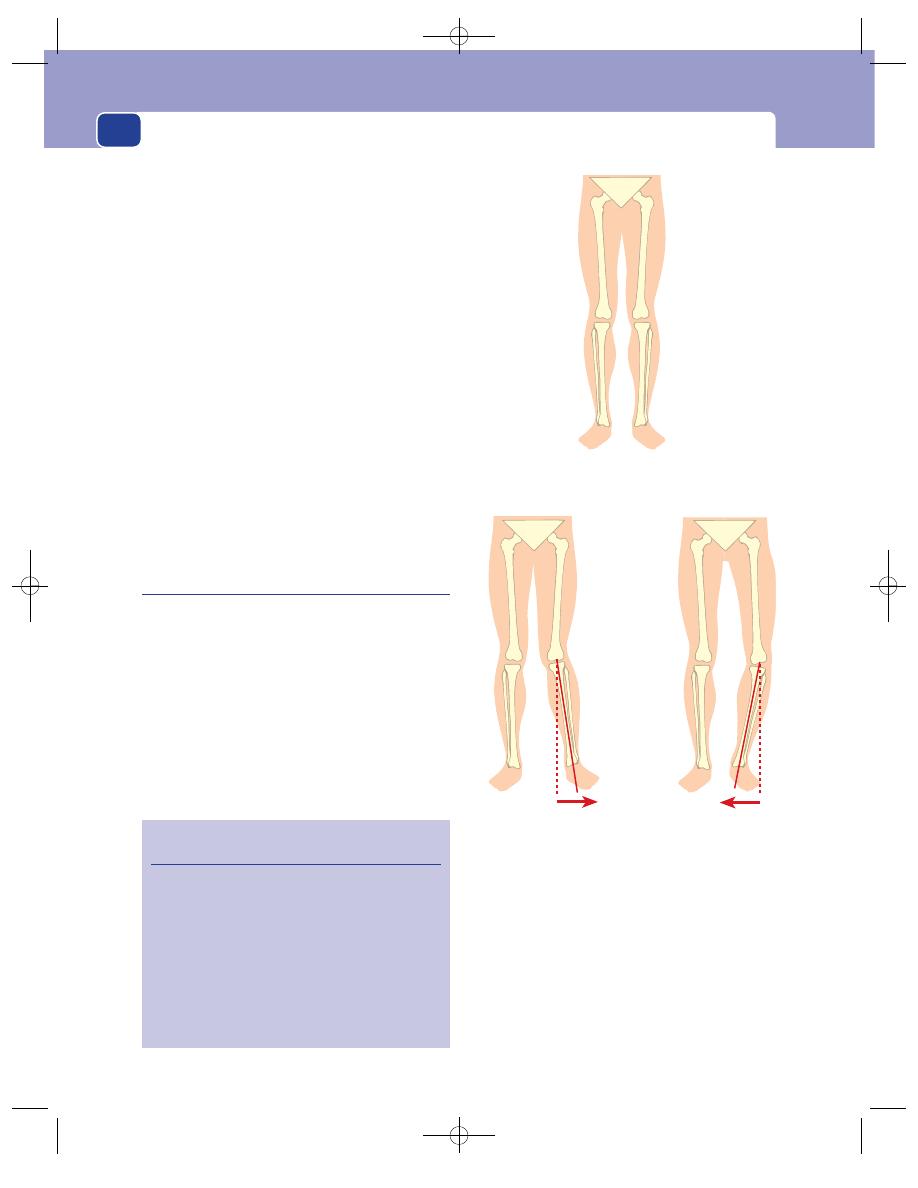
Muscles, tendons, bones and joints
128
Record the power of such movements as described
on page 107.
Passive movements
Move the joint through its full
range of movement with the patient’s muscles
relaxed. Note any crepitus (grating sensations) felt
during this passive movement and any pain or
discomfort.
Ligaments
Check the integrity of each ligament
associated with the joint by stretching it. This will
also reveal any abnormal movements.
General examination of the limb
Examine the arteries, nerves, lymph glands and the
other joints of the limb.
The majority of joints have simple movements
(e.g. extension and flexion) and their examination
presents no problem. The examination of the two
complex joints of the lower limb, the hip and the
knee, which are frequently diseased or deranged,
deserves a detailed description.
Examination of the hip joint
Position
First examine the patient standing up if possible.
This gives you the opportunity of inspecting the
patient from the front, the side and then from the
back. You may either assess their gait at this stage or
after the rest of the examination has been com-
pleted (see below). Then ask the patient to lie flat
and straight on the couch, and check that the pelvis
is square to the mid-line by feeling the positions of
the anterior superior iliac spines.
Inspection
Skin
Remember that sinuses and scars from the hip
joint are often on the buttock and posterior aspect
of the upper thigh, so look at the skin over the back
of the joint as well as the front.
Normal
Valgus
Varus
FIG 4.25
The definition of a varus and a valgus deformity.
In valgus deformity the distal bone forming the joint is
abnormally abducted. In a varus deformity it is abnormally
adducted. Remember, knock-knees
⫽ genu valgum.
Revision panel 4.1
The causes of joint deformities
Skin
Contractures
Fascia
Contractures
Muscle
Paralysis, fibrosis, spasm
Tendon
Division, adhesion
Ligament
Rupture, stretching
Capsule
Rupture, fibrosis
Synovium
Inflammation
Bone
Changes in shape,
trauma, pressure atrophy
Chap-04.qxd 4/19/05 13:50PM Page 128
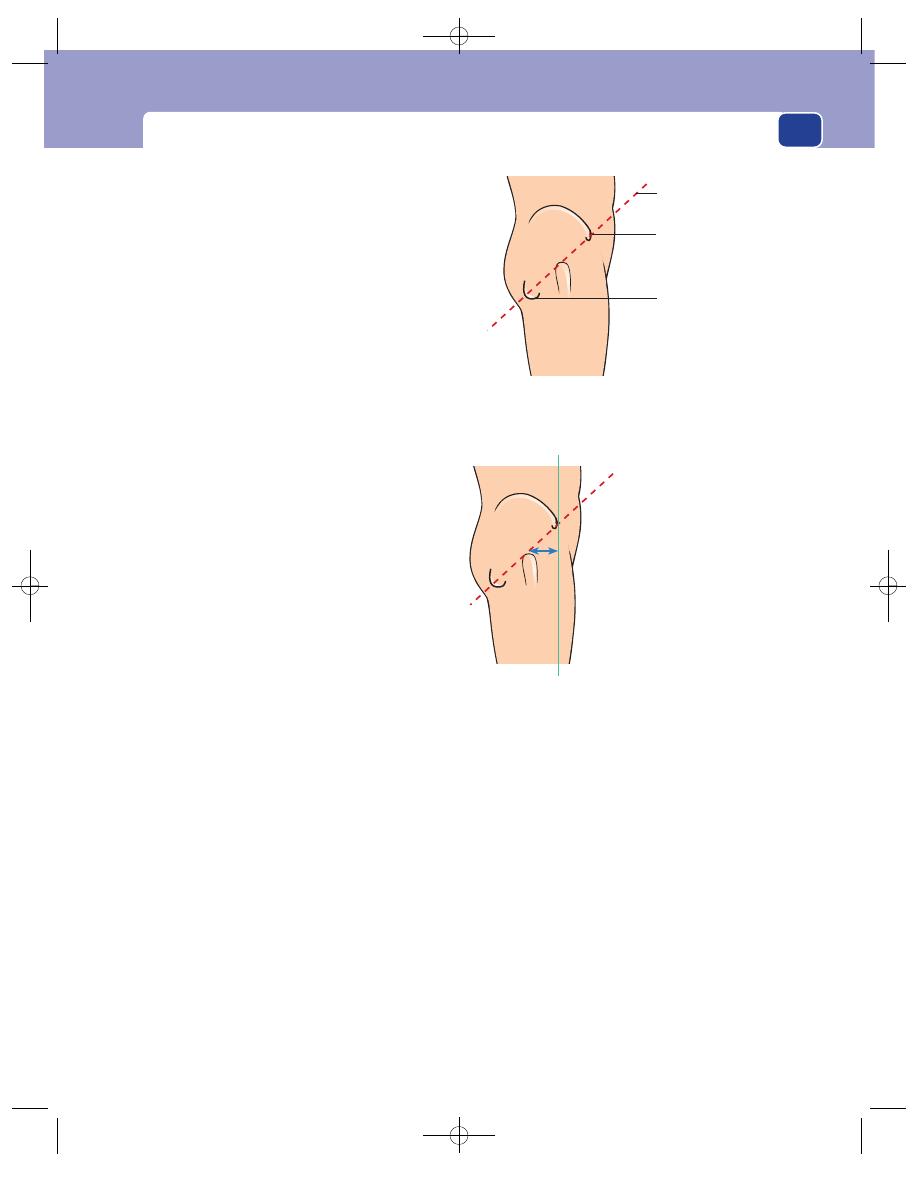
Examination of a joint
129
Shape
Check the contours of the thigh and buttock.
Asymmetrical skin creases indicate joint displace-
ment. Note any muscle wasting or rotational defor-
mity. Also note any increased lumbar lordosis or
scoliosis.
Position
When the hip joint is painful or distended by
an effusion it is held slightly flexed and abducted. This
flexion deformity may also be fixed. In cases of true
shortening, once the anterior superior iliac spines are
level, the degree of shortening may be apparent by
noting that the heels are not level. This should stimu-
late an accurate assessment of shortening and limb
length measurement (see pages 114–16).
Palpation
The capsule and synovium of the hip joint cannot
be felt but the muscles and the bony contours can be
examined. Place the fingers of one hand over the
head of the femur, i.e. just below the inguinal liga-
ment and lateral to the femoral pulsation. Note
any tenderness and then rotate the leg to allow the
detection of any crepitations arising in the joint.
Relationship between pelvis and femur
In cases of shortening, the position of the greater
trochanter with respect to the pelvis (i.e. acetabulum)
can be checked in three ways.
1. Bilateral palpation. To compare the two sides,
put your thumbs on the anterior superior iliac
spines and your fingers on the tops of the
greater trochanters. You will appreciate any
difference in the distance between these points
through the position of your fingers.
2. Nélaton’s line. Turn the patient on their side.
Imagine a line drawn from the anterior superior
iliac spine to the ischial tuberosity. The top of the
greater trochanter should just touch this line. If
it lies above the line, there is shortening of the
neck of the femur or a dislocation of the hip.
3. Bryant’s triangle. This gives a measurement of
the distance between the top of the greater
trochanter and the coronal plane of the iliac
spine. Lie the patient supine. Imagine a horizontal
line passing through the anterior superior iliac
spine. Measure the vertical distance between this
line and the top of the greater trochanter.
Nélaton’s line and Bryant’s triangle are now very
rarely used clinically (radiographs are much more
accurate), but they are useful ways of remembering
the normal relationships of the bony landmarks.
Movement
Test for fixed flexion
Other fixed deformities (e.g.
abduction or adduction) will be clearly visible from
the position of the thigh when you set the pelvis
square with the spine, but fixed flexion can be
masked by a lumbar lordosis.
Place your left hand underneath the hollow of
the lumbar spine. Grasp one leg and flex the hip and
knee until the lumbar spine straightens and presses
against your left hand. If the other hip joint is nor-
mal, the thigh on that side will remain flat on the
couch. If the other hip lifts off the couch, this will
indicate a loss of extension in that hip, which is
Nélaton's line
Anterior superior
iliac spine
Ischial tuberosity
FIG 4.26
Nélaton’s line is a line drawn through the anterior
superior iliac spine and the ischial tuberosity. It should just
touch the top of the greater trochanter.
Bryant's triangle
The horizontal distance between
the coronal planes of the anterior
superior iliac spine and the
greater trochanter and the vertica
distance between these two bony
points will be abnormal if the hip
joint is dislocated
FIG 4.27
Bryant’s triangle measures the vertical distance
from the anterior superior iliac spine to the greater
trochanter, and the horizontal distance between the coronal
planes of the iliac spine and trochanter.
Chap-04.qxd 4/19/05 13:50PM Page 129
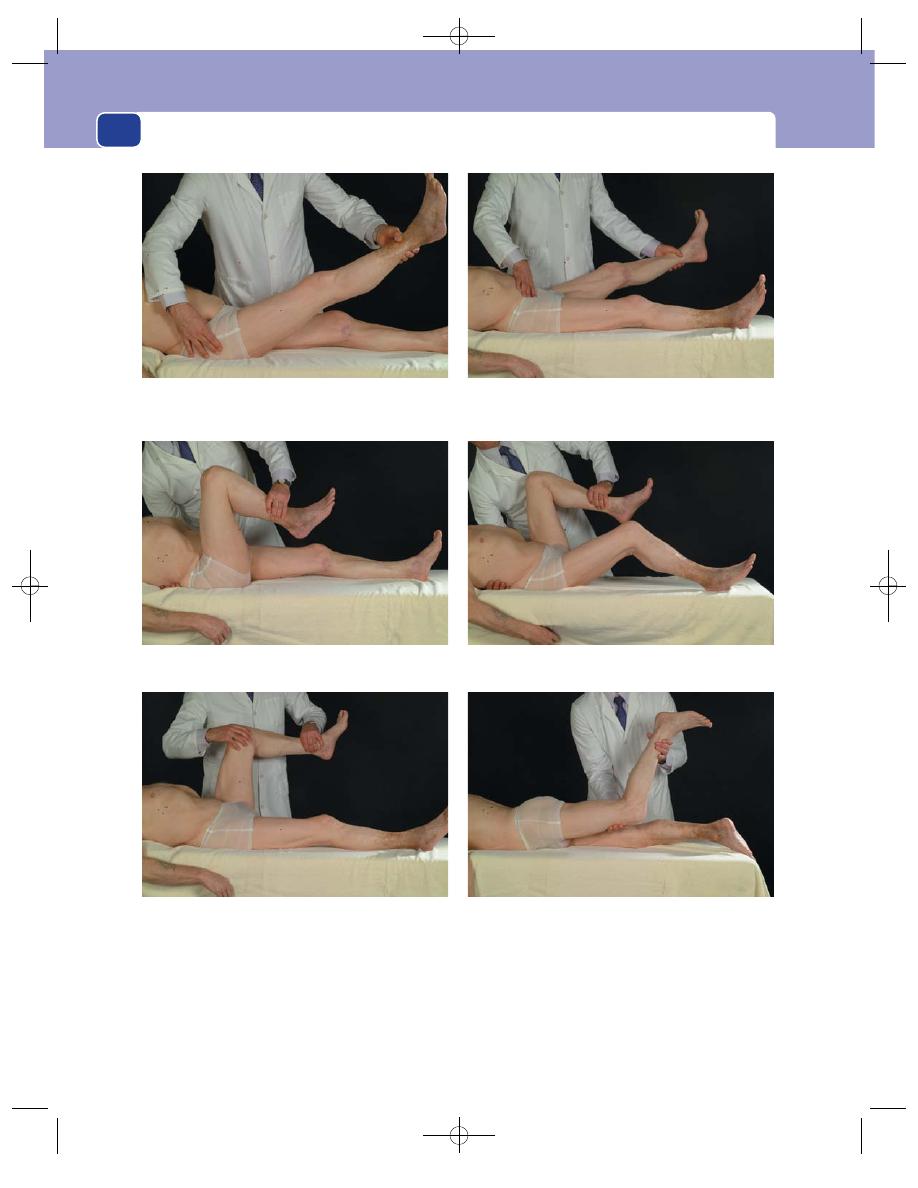
Muscles, tendons, bones and joints
130
referred to as a fixed flexion deformity, and the angle
of elevation, or fixed flexion, should be recorded.
This is called Thomas’ test for fixed flexion. Now flex
the other leg to check the opposite joint.
Passive movements
You can only test the movements
of a joint by keeping one of the bones that forms the
joint still, and moving the other bone. A false impres-
sion of hip movement may be obtained if the pelvis
FIG 4.28
SOME IMPORTANT ASPECTS OF THE EXAMINATION OF THE HIP JOINT.
When testing movements such as flexion, place your fingers
on the great trochanter and your thumb on the iliac spine so
that you detect any tilting of the pelvis.
Keep your fingers and thumb stretched across the iliac
spines when testing abduction and adduction to detect any
movement of the pelvis.
Measure the degree of fixed flexion by flexing the good hip until the lumbar spine straightens and presses on your other hand
placed beneath the lumbar spine. No fixed flexion in the left hip. 25° fixed flexion in the right hip. This is Thomas’ test.
Rotation is measured by flexing the hip and the knee to 90°
and rotating the femur by moving the foot back and forth
across the line of the limb.
With the patient lying on their front, lift each thigh and assess
hip extension.
Chap-04.qxd 4/19/05 13:50PM Page 130
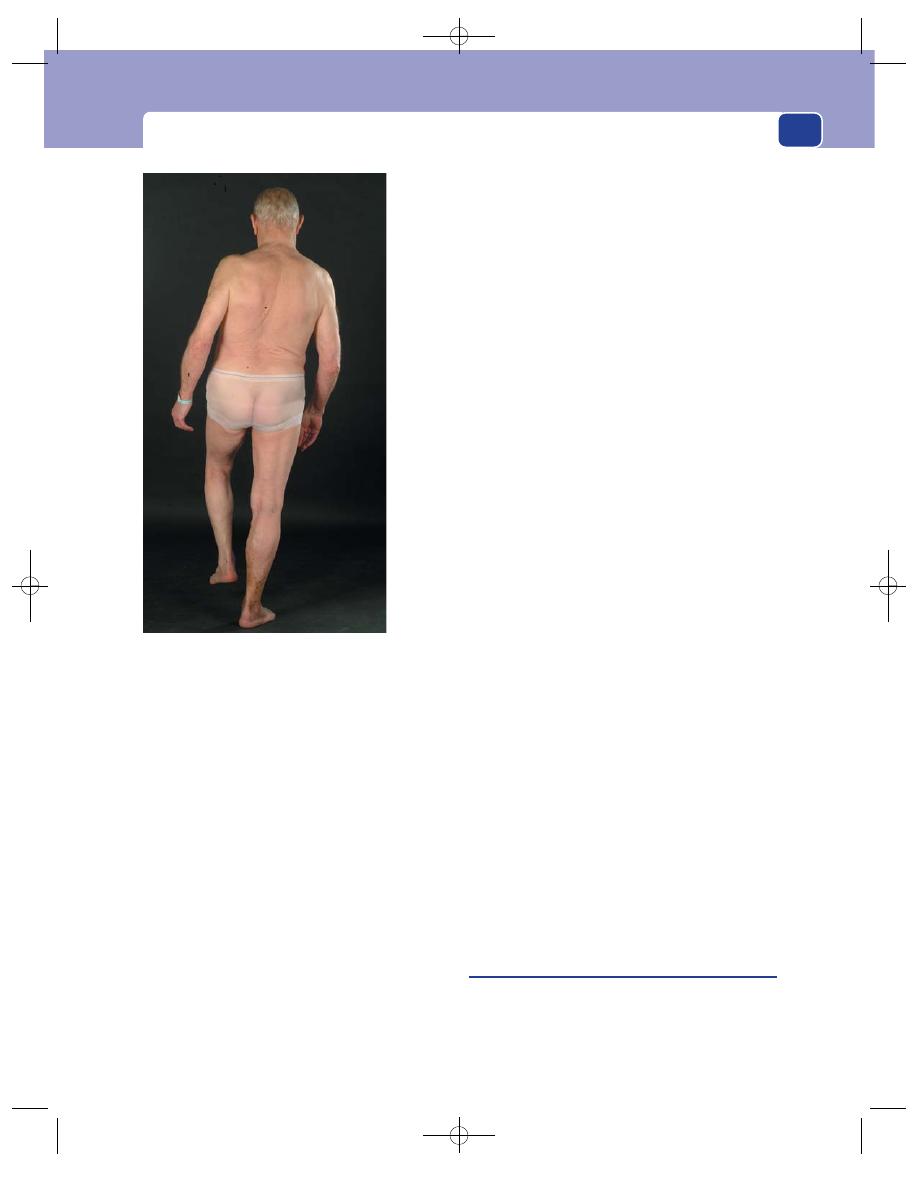
Examination of a joint
131
moves during the examination. Therefore during all
passive movements of the hip you must continually
check that the pelvis is not moving by keeping the
thumb and little finger of one hand resting upon the
two anterior superior iliac spines.
Flexion
Flex the good hip and knee until the thigh
presses against the abdomen and get the patient to
hold the leg in this position. Then flex the hip under
consideration, using your other hand to check that
no further pelvic movement takes place. Record the
degree of flexion and any fixed flexion deformity.
Abduction and adduction
Keeping the left hand firmly on
the pelvis, abduct or adduct each leg until the pelvis
begins to move, and record the range of movement.
Rotation
Both internal and external rotation can be
assessed by rolling the whole limb, but the best way
is to flex the hip and knee to 90°. The foot can then
be moved laterally to assess internal rotation and
medially to assess external rotation. The range of
movement can then be measured by comparing the
position of the leg to the mid-line.
Abnormal movements
The only abnormal movement
you are likely to meet, except those caused by acute
trauma, is ‘telescoping’ of the joint, caused by a dis-
located head of the femur sliding up and down the
outer aspect of the ilium. This abnormal movement
is detected by pushing and pulling the femur along
its long axis while steadying the pelvis and feeling
the top of the greater trochanter. It is sometimes
easier to do this by flexing the hip to 90° and pulling
the thigh upwards.
Extension
Do this last, as you need to turn the
patient on their face. Put your hand under the knee
and lift up the thigh, again steadying the pelvis with
your other hand. A normal hip extends only 5–2°.
With the patient standing
Look for deformities and
abnormal skin creases if this has not already been
done.
Trendelenburg test
Ask the patient to stand on one
leg. The opposite side of the pelvis should rise to help
balance the trunk on the leg by bringing the centre of
gravity over the weight-bearing foot. This involves
the use of the hip abductors – gluteus medius and
minimus. If the opposite side of the pelvis falls and
the patient has difficulty standing, the test is positive.
A positive test means one of the following:
■
paralysis of the abductor muscles,
■
an unstable joint (e.g. congenital dislocation of
the hip or a fracture of the neck of the femur),
■
approximation of the insertion and origin of the
abductor muscles preventing their proper function
by a severe coxa vara or a dislocation of the hip.
Assessing the gait
Make the patient walk. Observe
their gait from the front, the rear and the side.
Any instability of a joint becomes more notice-
able during the stresses of walking.
Examine the nerves and arteries of the limb
Joint dis-
ease is often secondary to neurological abnormalities.
Examination of the knee joint
Inspection
Skin
Look at the skin all round the joint – front and
back – for discolouration, scars and sinuses. Erythema
Ask the patient to stand on one leg. They should raise the
pelvis on the opposite side. This is Trendelenburg’s test.
FIG 4.28
continued
Chap-04.qxd 4/19/05 13:50PM Page 131
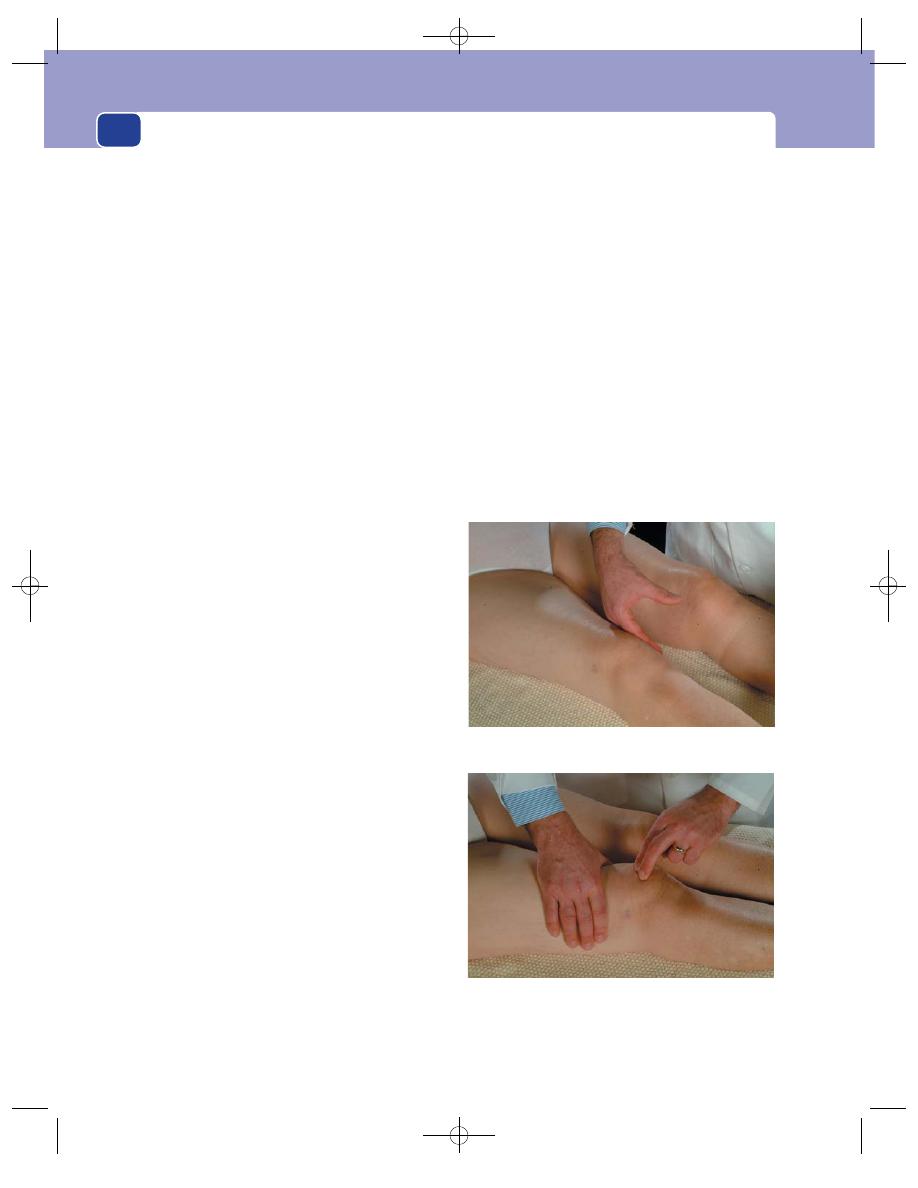
Muscles, tendons, bones and joints
132
may suggest inflammation, whereas bruising may
indicate trauma. Note any skin conditions that are
often associated with joint problems, such as psori-
asis and arthritis.
Shape
The contours of the knee joint are easy to see
and any bony or joint swelling distorts them at an
early stage. The size of the whole joint should be
compared with the other side, but the areas in which
minor degrees of swelling caused by a small effusion
are first apparent are the hollows either side of, and
above, the patella. Assess any swelling in terms of
whether it is confined to the limits of the synovial cav-
ity or extends beyond the joint boundaries, which
would suggest infection, tumour or injury. Note any
localized swellings that may represent bursitis,
meniscal cyst or lesions such as exostoses. Look for
any evidence of muscle wasting, particularly of the
quadriceps muscle.
Position
A knee joint that is swollen and painful is
most comfortable when slightly flexed. Also look for
any degree of genu valgus or varus.
Palpation
Skin
Note any increase in temperature that may
indicate active arthritis or infection.
Synovium
The synovium of the knee joint can be felt
on either side of the patella, and in the suprapatellar
pouch. In some diseases it becomes thickened and
rubbery, or ‘boggy’. A thickened synovium is usually
hyperaemic and makes the overlying skin warm.
Bony contour
Check the position of the patella. It
should be in the patellar groove of the femur, but it
may be displaced laterally or superiorly if there is
lengthening or rupture of the patellar ligament.
Check the position of the knee joint. When stu-
dents are asked to put their index finger on the line
of the knee joint, they invariably point to a spot 2.5
to 5 cm above it. Remember that the main bulge of
the knee is formed by the lower end of the femur.
The easiest way to find the joint line is to flex the
knee until you can feel the anterior curved edge of
the femoral condyles and can slide your finger
downwards over this edge until you reach the tibial
plateau.
It is important to relate areas of tenderness to the
joint line and the points of attachment of the collat-
eral ligaments.
Effusions
Effusions of the knee joint are common
and easy to detect because the excess synovial fluid
collects in the front of the joint where it can be seen
and felt. There are three tests for detecting an effu-
sion in the knee joint.
1. Visible fluctuation. A small quantity of fluid
present does not make the whole joint look
swollen, but if you press gently on one side of
the joint, the other side may bulge outwards.
Get the leg in a good oblique light so the
hollows on either side of the patella are visible.
Stroke the joint just to one side of the patella
and watch the hollow on the other side of the
patella to see if it gradually fills out as the
effusion is pushed into it. This is the most
sensitive way of detecting a small effusion. It
cannot be used if the joint is full and tense.
The patellar tap test: squeeze any fluid out of the supra-
patellar pouch using the right hand and then press down on
the patella. A tap or click will indicate an effusion.
FIG 4.29
TESTING FOR A KNEE EFFUSION.
The fluid displacement test: compress one side of the knee
and note the joint distending on the opposite side.
Chap-04.qxd 4/19/05 13:50PM Page 132
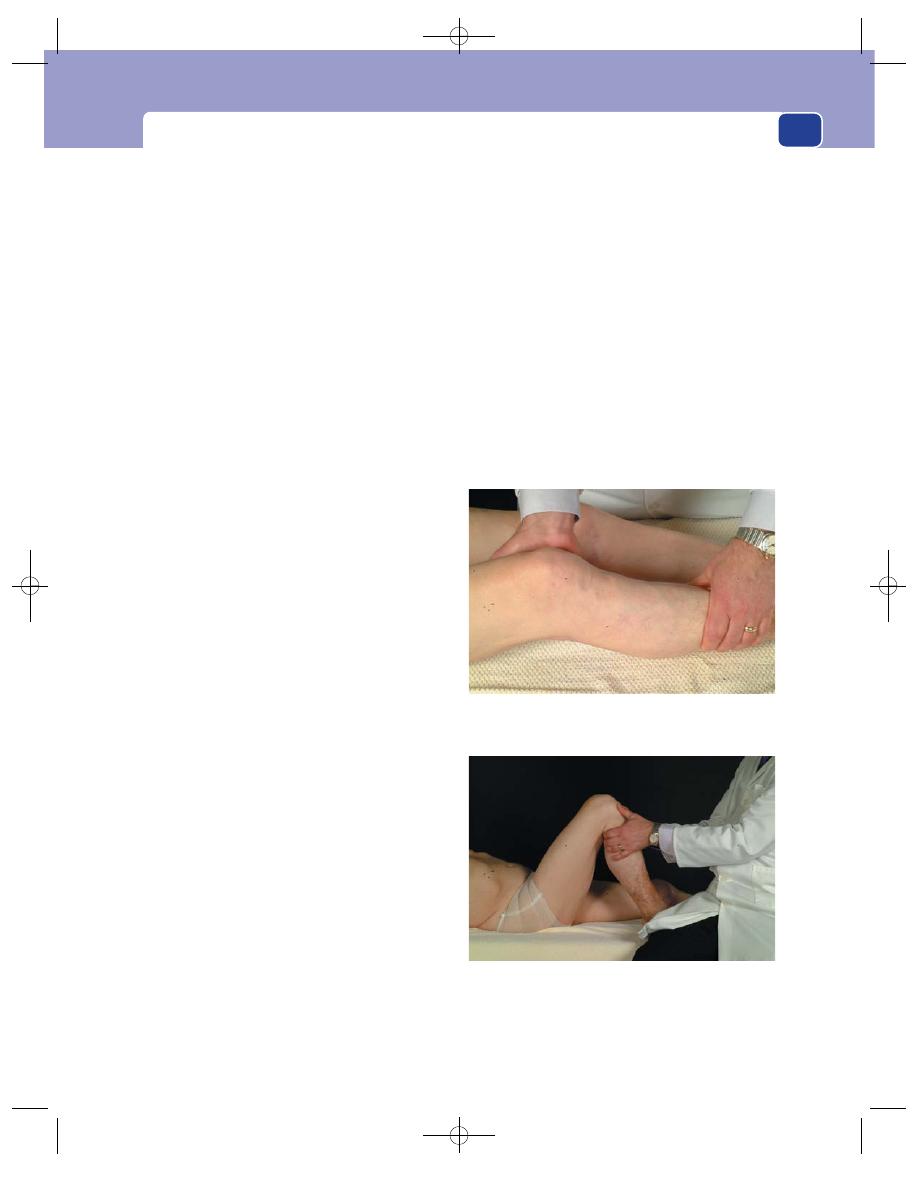
Examination of a joint
133
2. Palpable fluctuation. When the knee joint is full
of fluid it is possible to press on one side and feel
the increase in pressure transmitted over to the
other side. Place the palm of the left hand above
the patella, and the thumb and index finger
either side of it. Press posteriorly and distally to
squeeze any fluid in the suprapatellar pouch
down into the joint behind and either side of the
patella. Place the thumb and index finger of the
right hand either side of the patella and see if
you can feel fluctuation or fluid displacement
between your thumb and finger.
3. Patellar tap. When the joint is full of fluid the
patella is lifted off the femur. If it is pressed or
tapped, it can be felt to move backwards and
hit the femur. This test is also helped by
emptying the suprapatellar pouch into the space
behind the patella with the left hand.
Surrounding tissues
Pay particular attention to the bulk
and strength of the quadriceps muscle, but remember
the quadriceps of the patient’s dominant leg will
always be slightly bulkier. Any substantial wasting can
be measured by comparing the circumference of the
thighs at the same distance above the joint line.
Movements
Ask the patient to move the joint themself before
checking passive movement. Record the extent of the
active knee movements in degrees. Remember that
when the leg is straight the angle between the femur
and tibia is 0°. At full flexion the angle is usually
135–150° and full extension 0° to minus 10°.
Flexion
Bend the knee as much as possible. When
there is hip joint disease you may have to turn the
patient on to their side to see the full extent of knee
flexion. Record the degrees of flexion from the zero
position of normal extension.
Extension
Lift the leg off the bed by the heel and ask
the patient to relax. Record any limitation to exten-
sion as well as any excess extension. In women the
knee joint often extends 5° or 10° past the 0° mark.
Rotation
There are small degrees of rotation of the
tibia on the femur, but these are not easy to detect
unless the knee is slightly flexed.
Abnormal movements
The knee joint is a hinge joint
which depends entirely on muscles and ligaments
for its stability. If the ligaments are ruptured or
stretched, abnormal movement can occur. Thus by
testing for abnormal movements such as abduction
and adduction, and antero-posterior glide or sliding
of the tibia on the femur, you are really checking the
stability of the knee and the integrity of its ligaments.
1. Lateral ligaments. Let the leg rest extended on
the couch. If standing on the patient’s left side,
place the fingers of your right hand under the
right knee joint and the butt of your hand
firmly against the medial aspect of the joint.
Keep this hand firm and use it as a fulcrum to
try to adduct the knee joint by pulling the ankle
towards you with your left hand. There should
be only the slightest movement in the joint. If it
moves easily, the lateral collateral ligament is
Assess the cruciate ligaments by flexing the knee to about
70°, fixing the foot, and then pulling the tibia towards you or
pushing it away. Any significant movement or glide will
indicate cruciate damage.
FIG 4.30
TESTING THE LIGAMENTS OF THE KNEE JOINT.
Assess the collateral ligaments of the knee by using the heel
of your hand as a fulcrum and then stressing the collateral
ligaments by pulling laterally and medially.
Chap-04.qxd 4/19/05 13:50PM Page 133
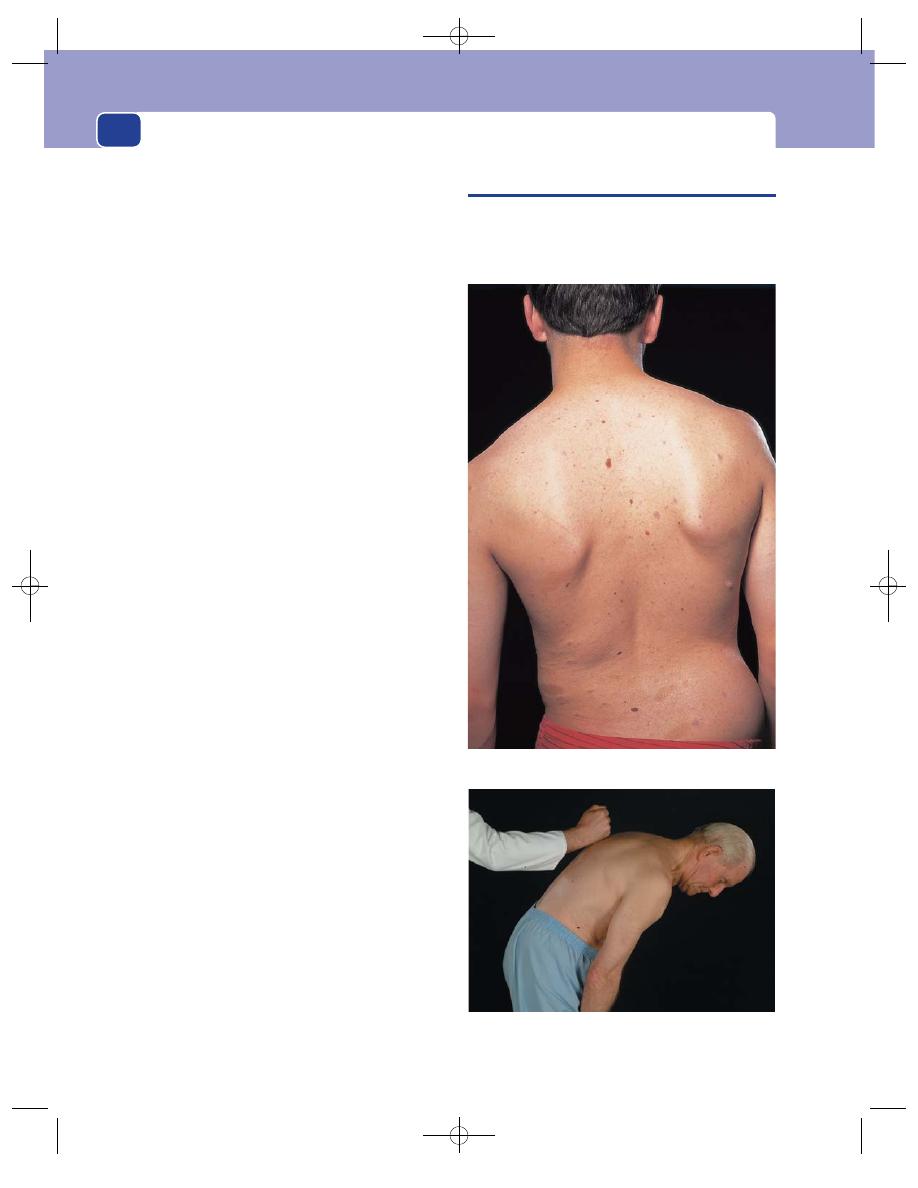
Muscles, tendons, bones and joints
134
ruptured. If you stay on the same side of the
patient, the same action on the other leg will
abduct the joint and test the medial collateral
ligament.
To test the ligaments on the other side of the
joint, change your hands around so that your
right hand lies on top of the joint with the
fingers resting on the side of the joint. Pull this
hand towards you and push the ankle away
from you with the other hand.
An alternative method is to tuck the patient’s
leg under your arm and then, with your hands
on each side of the knee joint to detect movement,
move the tibia from side to side with your body.
2. Cruciate ligaments. Remember the anterior
cruciate ligament stops the tibia sliding
anteriorly. The posterior ligament stops the tibia
sliding posteriorly.
Flex the knee to about 70°. Grasp the upper
end of the tibia with both hands and pull it
towards you. This is the anterior draw test, and
any significant movement suggests a torn
anterior cruciate ligament, possibly associated
with damage to the lateral ligaments as well.
Now repeat the test but this time pushing the
tibia backwards – the posterior draw test. Any
significant displacement indicates rupture of the
posterior cruciate ligament. Always compare the
degree of movement between both sides.
In normal knees there should be little or no
movement.
Note. It is not necessary to sit on the patient’s
foot and crush their toes to death to perform this
procedure, but it does help if the foot is fixed by the
pressure of your buttock as you sit beside the leg,
facing the patient’s head, so that both of your arms
are in front of you and in line with the leg.
Clicks
There are some special tests which make the
joint click if there is a torn cartilage. Do not try these
tests. They are difficult to perform and to interpret.
Normal joints sometimes click. If the patient is
complaining of clicking, find out exactly when it
occurs, if it is painful, and ask the patient to repro-
duce it for you, but do not indulge in excessive
manipulation just to hear it.
Gait
Ask the patient to stand up and walk about.
Observe the gait carefully.
EXAMINATION OF THE SPINE
Many pains that are felt in the front of the trunk and
down the limbs are caused by disease of the spine.
The general surgeon must always bear this in mind
FIG 4.31
Scoliosis of the spine secondary to neurofibromatosis.
FIG 4.32
Percussion over the spine will reveal tenderness that
may indicate infection or metastatic disease.
Chap-04.qxd 4/19/05 13:50PM Page 134
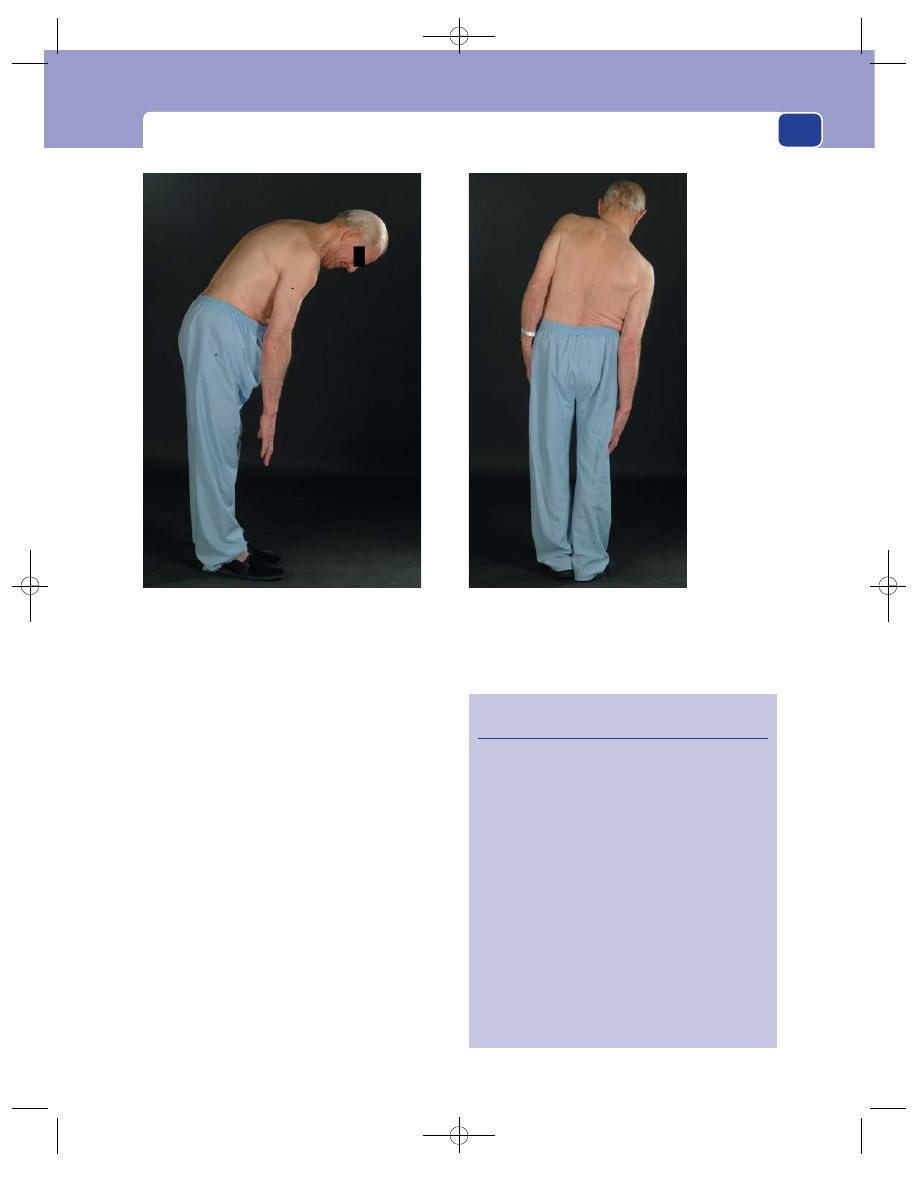
Examination of the spine
135
and make the examination of the spine part of their
routine examination. The routine is the same as that
for examining any other joint.
Inspection
Skin colour
This is usually normal, but note any
erythema.
Scars and sinuses
Note any scars from previous
surgery or trauma, any sinuses that might indicate
previous sepsis or tuberculosis, and any fat pad or
hairy patch that might suggest spina bifida.
Shape of the back
Assess the patient’s posture and
note any kyphosis, scoliosis or lumbar lordosis.
Record any bony deformity or abnormality relating
to the muscles of the back.
Palpation
Temperature
Note any change in skin temperature.
FIG 4.33
EXAMINING THE SPINE.
Revision panel 4.2
Some causes of scoliosis and kyphosis
Scoliosis
Congenital
Idiopathic
Neuromuscular
Cerebral palsy
Spina bifida
Muscle dystrophies
Poliomyelitis
Trauma
Postural
Kyphosis
Congenital
Tuberculosis
Ankylosing spondylitis
Osteoporosis
Secondary carcinoma
Flexion: ask the patient to attempt to touch their toes
and record the degree of flexion.
Assess lateral flexion by asking the patient to slide
their hand down their side as far as possible.
Chap-04.qxd 4/19/05 13:50PM Page 135
Muscles, tendons, bones and joints
136
The bony landmarks
Check the bony landmarks,
such as the lumbar vertebral spines, for any tender-
ness. In a similar way, check the sacroiliac joints and
also look for any step at the lumbo-sacral junction
that may indicate spondylolisthesis. Percuss over the
spine lightly, as marked pain may indicate tubercu-
losis or other infections, or metastatic disease.
Movement
These movements should be performed by the
patient while standing upright, apart from rotation.
It is not practicable to perform passive movements
of the spine.
Flexion
Ask the patient to bend forwards and seek
to touch their toes. Flexion may be recorded in
terms of how far towards the toes the patient can
actually reach.
Extension
Ask the patient to arch their back. This
movement is very limited and is seldom more than
about 30°.
Lateral flexion
Ask the patient to slide their hand
down their side as far as possible. Record the dis-
tance reached on both sides.
Rotation
This part of the examination should be
performed with the patient sitting to fix the pelvis. Ask
the patient to twist from side to side and assess the
angle between the plane of the shoulder blades and
pelvis.
Nerves
A full neurological examination is essential in all
patients with any spinal abnormality.
Test for irritation of the roots of the sciatic nerve
with the straight-leg raising test.
It is advisable to palpate the abdomen and do a
rectal examination to exclude intra-abdominal and
pelvic lesions which might be affecting the spine or
the spinal nerves.
DISEASES OF JOINTS
The main object of this chapter is to ensure that you
can examine the muscles and the skeleton properly.
The two commonest joint abnormalities that you
will find are swelling and deformity.
Swelling of a joint must be caused by one or
more of:
■
bony enlargement
■
synovial thickening
■
an effusion.
Deformity of a joint is invariably be caused by
one or more of:
■
skin contractures (e.g. scar following burns)
■
fascial contracture (e.g. Dupuytren’s
contracture)
■
muscle spasm or weakness
■
tendon division or fixation
■
capsule fibrosis
■
bone deformity.
Detailed descriptions of the diseases affecting
joints are to be found in orthopaedic textbooks. The
following section describes the signs and symptoms
of the four common diseases of joints.
Osteoarthritis
This condition can affect any joint. It is believed to
be caused by prolonged wear and tear, and exacer-
bated by injury and any disturbance of the normal
stresses and strains associated with the transference
of weight across the joint. The common causative
factors are therefore:
■
age
■
previous fractures involving the articular
surface and cartilage
■
previous joint diseases
■
malalignment of the skeleton following trauma
or bone disease.
The articular cartilage becomes thin and ulti-
mately wears through. The bone at the edges of the
cartilage hypertrophies, but the bone beneath the
cartilage degenerates.
History
Age
Most patients with osteoarthritis are over 50
years old, but secondary osteoarthritis following
trauma or disease may begin in early adult life.
Symptoms
The principal symptom is pain, which
comes on gradually, but steadily increases until all
movements of the joint are very painful. This is a very
Chap-04.qxd 4/19/05 13:50PM Page 136
Diseases of joints
137
slow process. Associated with the pain is an increasing
stiffness. If the arthritis is secondary to an old injury,
the stiffness may precede the onset of the pain.
Weakness
The stiffness and pain lead to disuse atro-
phy, so the muscles controlling the joint become weak.
Deformity
As the stiffness increases, the joint often
develops a degree of fixed flexion and the limb may lie
with a degree of abnormal abduction or adduction.
Limping
Pain, stiffness, weakness and deformity of
the joints in the lower limb interfere with walking.
Swelling
The whole joint is often swollen by bony
osteophytes and an effusion. The synovium is not
usually thickened.
Examination
Inspection
Colour
The skin should not be reddened or dis-
coloured.
Contour
The joint is usually swollen.
Deformity
The joint may be fixed in an abnormal
position.
Relations
Other joints in the same limb, and the
same joint in the other limb, may be similarly dis-
eased. Nearby muscles are wasted.
Palpation
Skin
The skin temperature is normal, not hot.
Tenderness
Pressure on the joint, especially if it is
swollen, may cause pain, but local tenderness is
uncommon except during an acute exacerbation
when there is an effusion.
Synovium
The synovium is not usually palpable.
Muscle bulk
The bulk of the muscles that control
the joint is reduced.
Bony contours
The bone at the edge of the articular
cartilage may feel irregular and protuberant.
Movement
All movements of the joint are painful at their
extremes and some movements are reduced.
(Make sure that you assess the limitation of move-
ment accurately by asking the patient to do active
movements before you perform passive movements.)
Not all movements of the joint will be equally
affected. For example, early osteoarthritis of the hip
may cause limitation of abduction and medial rota-
tion long before it affects flexion, extension, adduc-
tion and lateral rotation.
Crepitus
The joint often crackles and clicks during movement.
Although the patient can feel a grating sensation
associated with the crepitus, it is not usually painful.
Abnormal movements
There should be no abnormal movements because
all the ligaments should be intact.
Arteries and nerves in the limb
These structures should all be normal.
Other joints
Osteoarthritis is sometimes bilateral and symmetri-
cal. The joints most often affected are the hip, knee,
spine and fingers.
General examination
Osteoarthritis is not associated with any other gen-
eralized disease, so the rest of the examination
should be normal. As many of the patients with
osteoarthritis are old and overweight, they fre-
quently have unrelated diseases such as coronary,
cerebral and peripheral artery disease.
The detection of these diseases is important
because their existence may alter the management
of the patient.
Rheumatoid arthritis
Rheumatoid arthritis is a generalized inflammatory
joint disease. Its cause is unknown. The synovial
membrane becomes thickened by hyperaemia and
lymphocyte infiltration. There may be an effusion. As
the disease progresses, the cartilage becomes damaged
and eroded and eventually the joint is destroyed.
Near the joints there may be nodules consisting
of necrotic collagen surrounded by fibroblasts.
History
Age
Rheumatoid arthritis may appear in patients of
all ages, but the common time of onset is between
the ages of 30 and 40 years.
Chap-04.qxd 4/19/05 13:50PM Page 137
Muscles, tendons, bones and joints
138
Sex
Women are affected three times more often
than men.
Symptoms
The main symptoms are pain and swelling,
which usually begin together. The commonest first
complaint is of swollen, stiff fingers.
Wasting
As the disease progresses, the joint move-
ments are restricted and the muscles which control
the joint waste away and become weak. As the joints
of the upper limbs are often the first to become
affected, the patient complains that she keeps drop-
ping things, and cannot carry a shopping basket.
General malaise
The patient may feel ill, listless and lose
weight. The muscles ache, especially after exercise, and
tender, painful nodules appear around the joints.
Skin rashes
The patient may complain of skin irri-
tation and rashes, especially if the joint changes are
part of another generalized disease such as Reiter’s
syndrome or systemic lupus erythematosus.
Examination
Inspection
The disease usually starts in the small joints at the
end of the limbs – fingers, wrists, toes and ankles –
before it moves to the larger joints of the limb and
ultimately to the joints of the trunk. The manifesta-
tions of the disease in the hands are described on
page 158.
Contour
The joints are evenly enlarged. The finger
joints become fusiform.
Colour
The skin overlying the joint may be red and,
if there is much swelling, shiny and taut.
Deformity
As the disease advances, it affects the lig-
aments and tendons around the joint as well as the
articular surfaces, so causing a variety of joint
deformities. For example there is usually ulnar devi-
ation at the wrist joint and hyperextension of the
proximal interphalangeal joints.
Wasting
The muscles which control the affected
joints will be wasted.
Other joints
Many joints are affected and the condi-
tion is frequently symmetrical.
Palpation
Temperature
The skin over the joint is warm.
Tenderness
In the acute stage of the disease the
joint is tender to light palpation. As the disease
becomes chronic, the tenderness subsides but the
pain during movement persists.
Synovium
Soft tissue thickening can often be felt
around the joint. It is only possible to be certain that
this is thickened synovium in those joints where it
has a clearly palpable edge beyond the joint line.
There may also be an effusion in the joint.
Muscle bulk
The muscles which control the joint
feel thin and atrophic.
Bony contours
Until the joint surfaces are destroyed
and pathological dislocations occur, the general
bony contour of the joint remains normal, but it is
often obscured by the synovial thickening.
Arteries and nerves in the limb
The other structures
in the limb should be normal. Patients with long-
standing rheumatoid arthritis sometimes get a
peripheral arteritis, which causes gangrene of the tips
of the toes and fingers, and ulceration of the skin of
the lower third of the leg. Swelling of the joints
around the wrist may cause a carpal tunnel syndrome.
Movement
Active movements are limited by pain and reduced
in power. Passive movements are limited by pain
and fibrous contractures. Abnormal movements
appear when the disease has weakened the liga-
ments, or tendons have ruptured.
General examination
Apart from other joint involvement, there may be
generalized wasting and anaemia. There are three
systemic diseases associated with rheumatoid joint
disease:
1. Still’s disease: a disease in which children get
arthritis, splenomegaly and lymphadenopathy;
2. Reiter’s syndrome: urethritis, conjunctivitis,
skin rashes and arthritis;
3. Systemic lupus erythematosus: a collagen
disease in which there is a scaly, red rash on the
face, debility and manifestations in all tissues of
a small vessel arteritis.
Psoriasis and rheumatoid arthritis often coexist.
The connection between these two apparently very
different diseases is not understood.
Chap-04.qxd 4/19/05 13:50PM Page 138
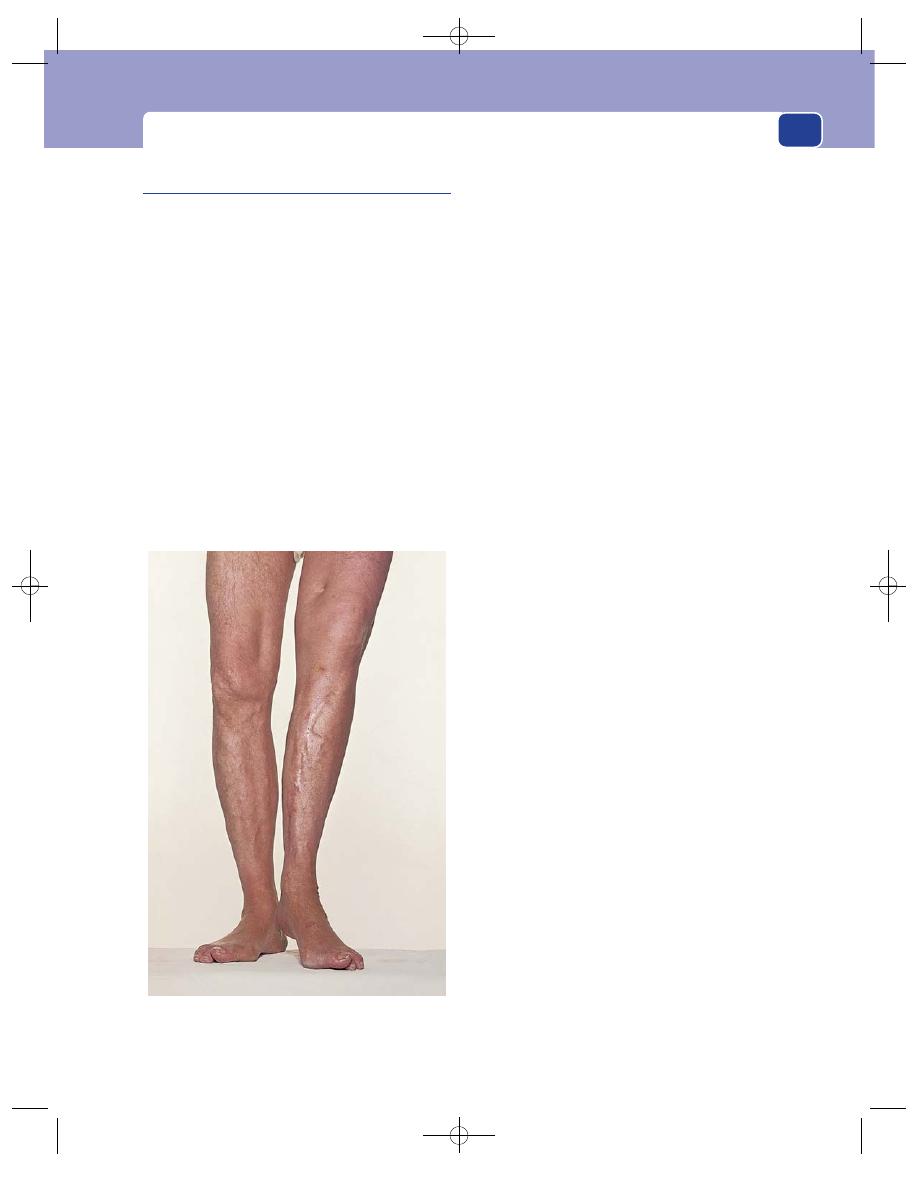
Diseases of joints
139
Tuberculous arthritis
Any joint can become infected with the human or
bovine tubercle bacillus. The joints of the vertebral
column are most often affected. The infection
reaches the joint via the bloodstream and produces
typical pathological changes in the synovium –
giant cells, lymphocytes, infiltration and caseation.
As the disease progresses, the effusion in the joint
becomes purulent and the articular cartilage and
the bone are destroyed.
History
Age
Tuberculous arthritis tends to occur in young
adults and children. Mild symptoms may be present
for many years before the patient complains or seeks
advice.
Symptoms
The common joint symptoms of pain
and swelling usually begin simultaneously, but in
the hip or the spine where the swelling is not so
apparent, pain is the presenting feature.
The pain limits movement of the joint and this
usually interferes with walking, bending and stoop-
ing. If an abscess forms in the joint, it may point
onto the skin and then discharge. The resulting
chronic sinus, with a seropurulent discharge, per-
sists until the disease is cured or dies out.
General malaise and loss of weight are common
symptoms.
Social history
It is important to enquire about social
conditions, such as diet, housing and international
travel, as well as the existence of any family history
of tuberculosis.
Local examination
Inspection
Contour
The joint (especially the knee) is diffusely
swollen.
Colour
The colour of the skin over the joint is normal.
Sinuses
There may be a discharging sinus near the
joint, or the scars of healed sinuses.
Muscle wasting
There is usually marked muscle
wasting, especially of the quadriceps femoris mus-
cles when the knee joint is diseased.
Palpation
Skin
The skin over the joint is not hot but the
inflammatory hyperaemia in the underlying syn-
ovium may make it slightly warmer than normal.
Tenderness
The joint is tender for a short period in
the early acute phase of the disease, but once the infec-
tion is established, the joint is not usually painful.
Synovium
The swelling around the joint feels soft
and pliable – something like unbaked dough. There
is always an effusion in the joint.
Bony contour
The bones are only deformed or des-
troyed in long-standing severe disease.
Movement
Movements are only limited if they are painful. In
these circumstances there is usually a pronounced
protective muscle spasm. There should be no
abnormal movements.
When the disease is advanced and has destroyed
the joint, it becomes fixed by a fibrous ankylosis.
FIG 4.34
The end-result of severe tuberculosis of the left
knee joint: a fibrous ankylosis, shortening and wasting of
the limb and healed sinuses.
Chap-04.qxd 4/19/05 13:50PM Page 139
Muscles, tendons, bones and joints
140
General examination
There may be evidence of tuberculosis elsewhere,
such as in the lungs or the kidneys, so the general
examination should be complete and thorough.
Neuropathic joints
(Charcot’s joint)
The brain is unable to protect a joint which has lost
its pain and position sense from harmful stresses
and strains. The resulting frequent minor injuries
ultimately destroy the bones and the ligaments of
the joint. A neuropathic joint is therefore a painless,
disorganized joint. The possible causes of loss of
joint sensation are:
■
diabetic neuropathy
■
tabes dorsalis
■
syringomyelia
■
leprosy
■
cauda equina lesions such as myelomeningocele.
Tabes dorsalis used to be the commonest cause of
a Charcot’s joint in Great Britain, but now that
untreated tertiary syphilis is rare, the commonest
cause is diabetes.
History
Age
Neuropathic joints occur in middle and old
age. However, in cases of syringomyelia, the condi-
tion often dates from an earlier age and there is
often dissociation of sensory loss, with loss of pain
and temperature sense but not of touch.
Symptoms
The patient notices that the joint is becom-
ing swollen and deformed and gives way frequently
but is not painful, except in the early stages of the
disease when there may be a few pain fibres but no
proprioceptive fibres functioning.
The mechanical weakness of the joint together
with the sensory defects of the neuropathy make the
patient’s gait unstable.
Previous illness
The patient will probably know if
they have had diabetes for many years, but may not
know if they have had syphilis. Other neurological
conditions are usually obvious.
Local examination
Inspection
Colour
The colour of the skin over the joint is normal.
Contour
The joint is usually swollen and obviously
deformed. There is no common pattern of deformity
for any particular joint.
Palpation
Tenderness
The joint is not tender and movements
in any direction do not usually cause pain.
Synovium
The synovium is not thickened, but there
is always an effusion.
Bony contours
Displacement of the bony land-
marks reveals that the bones are displaced or
deformed. The normal shape of the bones forming
the joint may completely disappear as a result of the
combination of bone destruction in some areas and
new bone formation and hypertrophy in others.
The joint fluid is often greatly increased.
The joint may be subluxed or dislocated and
there is gross bone erosion with irregular calcified
masses in the capsule.
Movement
The patient may be unable to perform normal move-
ments because of the destruction of the joints and
ligaments. Some passive movements may be limited
by the bony deformities, while grossly abnormal
movements may be possible in other directions. It
may be possible to dislocate the joint and then reduce
it, and move it in a variety of abnormal ways without
the patient feeling any pain or discomfort.
The knee and elbow joints may become so disor-
ganized that the limb becomes flail-like, with grossly
abnormal but painless movements.
Nerves of the limb
Examine the nerves of the limb
with great care. Vibration sense, position sense and
deep pain sensitivity are usually all reduced or
absent. The motor innervation should be normal.
Revision panel 4.3
The causes of a disorganized, painless
(Charcot) joint
Diabetic neuropathy
Tabes dorsalis
Syringomyelia
Leprosy
Cauda equina lesions (e.g. myelomeningocele)
Chap-04.qxd 4/19/05 13:50PM Page 140
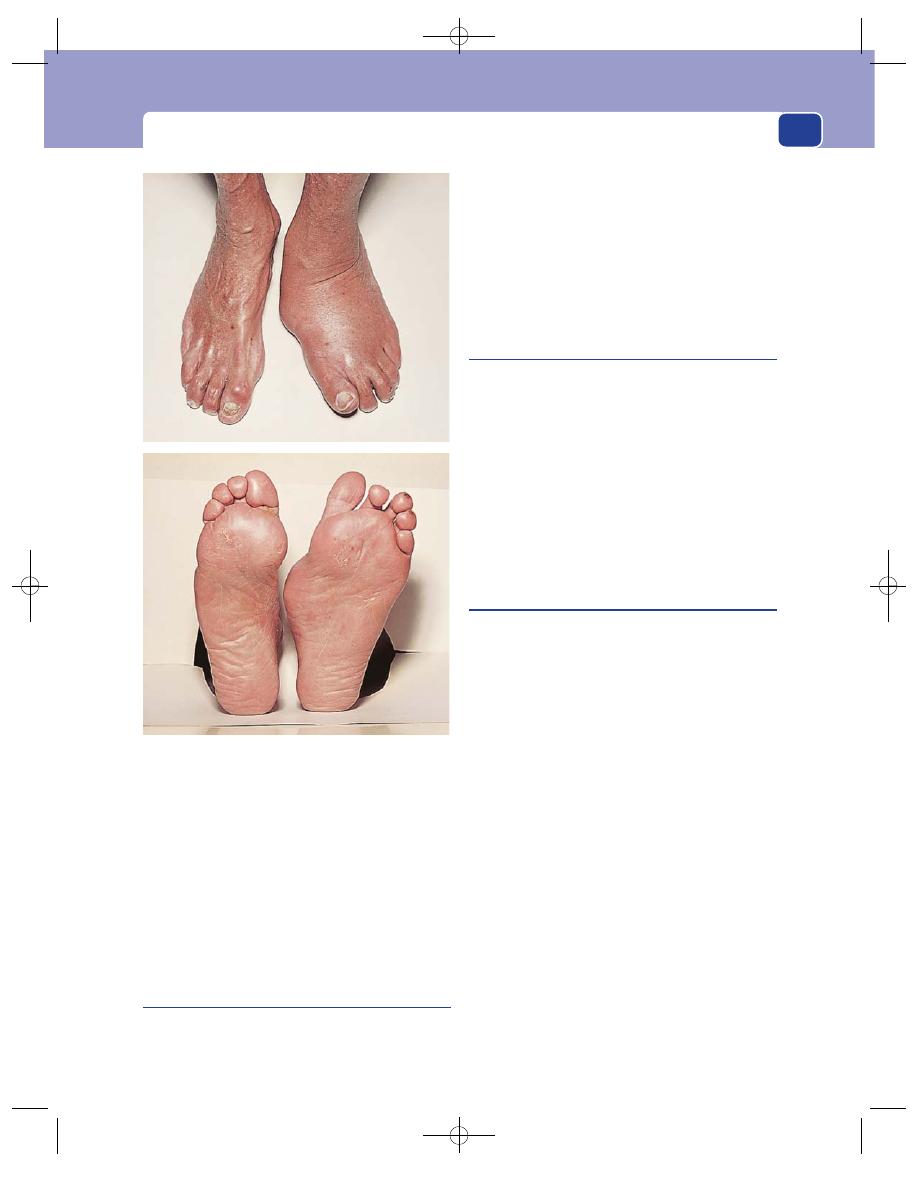
Diseases of joints
141
General examination
Look for the signs of diabetes and syphilis. Take par-
ticular care to examine the whole of the nervous sys-
tem for evidence of any other neurological disease
process, such as syringomyelia, and test the urine for
sugar.
Ankylosis
An ankylosed joint is a fixed joint. If the bones
that form the joint are fixed together by bone, this
is referred to as a bony ankylosis. If the bones are
fixed by dense fibrous tissue, this is a fibrous ankylo-
sis.
A bony ankylosis is absolutely fixed and pain-
less, even when stressed.
A fibrous ankylosis moves a little, and forced
movement causes pain.
Semimembranosus bursa and
Baker’s cyst
The common forms of subcutaneous bursae are
described in Chapter 3.
The normal anatomically constant bursae around
joints, usually between the joint and those tendons
which cross it, do not enlarge very often. The one
which gives most trouble is the bursa between the
semimembranosus tendon and the posteromedial
aspect of the femoral condyle.
This presents as a swelling behind the knee and is
often confused with the other common swelling in
this site, a Baker’s cyst.
Semimembranosus bursa
History
The common complaint is of a swelling behind the
knee joint that interferes with knee movements,
particularly flexion.
The swelling tends to grow slowly and does not
usually cause pain.
Examination
Age
The patient is usually a young or middle-aged
adult.
Colour
The skin over the swelling is of normal
colour and temperature.
Position
The swelling lies in the popliteal fossa and is
covered only by skin. It lies above the level of the
joint line, slightly to the medial side of the fossa.
Consistence
It is firm in consistence but clearly cystic
because it fluctuates and often transilluminates. It
may have a fluid thrill.
Variability
Semimembranosus bursae often appear
to empty into the knee joint with firm pressure, or
during flexion of the knee joint, but this does not
actually occur because the bursa does not connect
FIG 4.35
TWO VIEWS OF A CHARCOT JOINT.
A totally disorganized, but painless, left ankle and foot. This
Charcot ankle and foot was caused by diabetic peripheral
neuropathy.
Chap-04.qxd 4/19/05 13:50PM Page 141
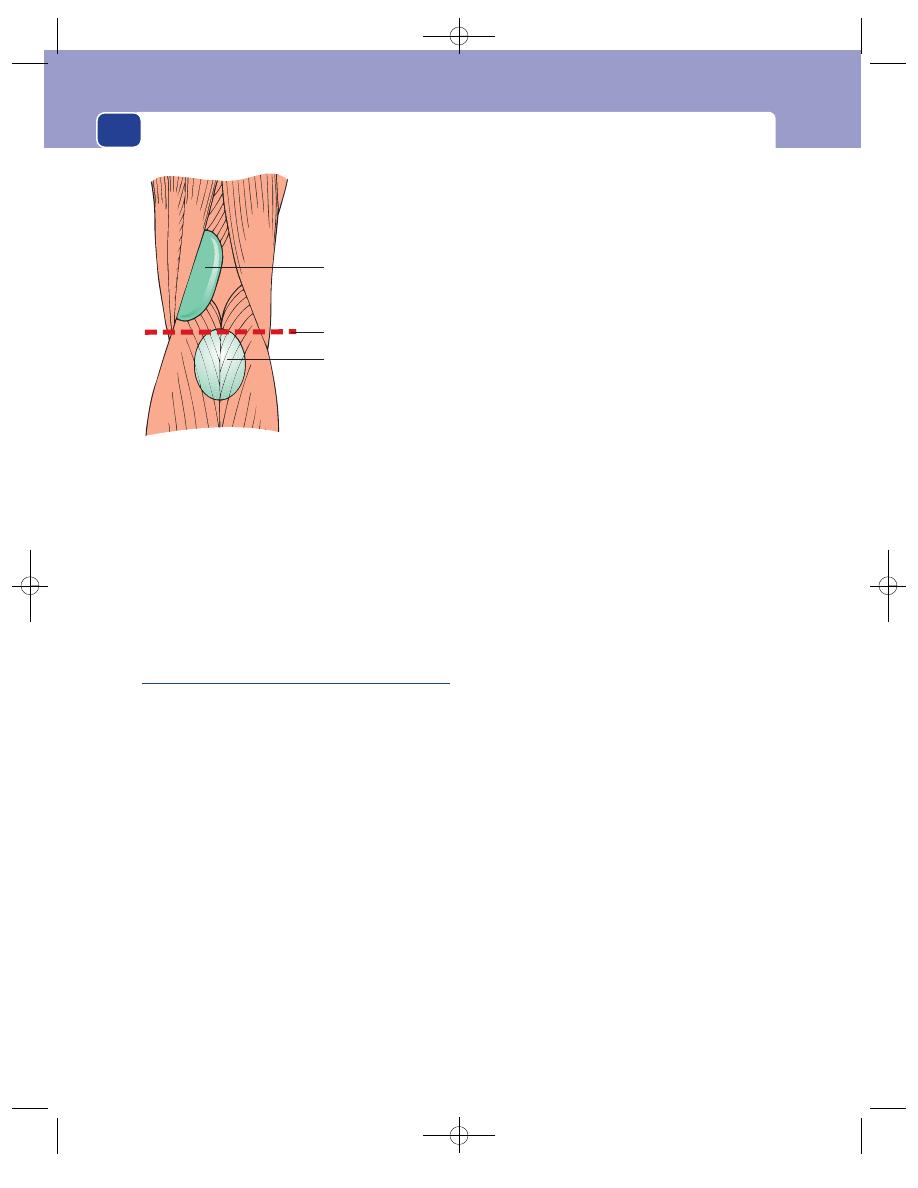
Muscles, tendons, bones and joints
142
with the joint. The fluid is just moving into the
deeper recesses of the bursa between the tendons.
Lymph glands
The local lymph glands should not
be enlarged.
Adjacent tissues
The knee joint and other nearby tis-
sues are normal.
Baker’s cyst
A Baker’s cyst is a pulsion diverticulum of the knee
joint, caused by chronic disease in the joint.
History
Previous illness
The patient will usually give a history
of chronic aches, pains and swelling of the knee
joint, often known to be caused by osteoarthritis or
rheumatoid arthritis.
The use of the knee is already limited when the
patient notices a swelling behind it which further
interferes with knee flexion. The swelling itself is
not painful. It often fluctuates in size. The patient
may have arthritis in other joints.
Examination
Age
Baker’s cyst appears in elderly patients with
long-standing osteoarthritis or in younger patients
with rheumatoid arthritis.
Colour
The skin over the cyst is usually a normal
colour, but may be a little red and warm if the
arthritis in the knee joint is active.
Position
The lump is below the level of the knee joint
and deep to the gastrocnemius muscle. This is
because the diverticulum, which becomes the cyst,
is a blow-out through the posterior aspect of the
capsule of the knee joint, which is covered by the
two heads of the gastrocnemius muscle as they
descend from their origin on the back of the femur.
Some of the cyst may bulge out between the
heads of the gastrocnemius.
Consistence
The swelling is soft and fluctuant but will
not usually transilluminate because of the density of
the muscles which cover it. It is dull to percussion
and the fluid content can often be reduced into the
joint. Cyst fluid that has moved into the joint can
sometimes be seen as a swelling, which appears at
each side of the patella as the cyst is compressed.
The knee joint usually shows evidence of arthri-
tis, with limited movements, crepitus and often an
effusion.
Adjacent tissues
Sometimes these cysts rupture and
cause pain and swelling in the calf; this is usually
misdiagnosed as a deep vein thrombosis.
Differential diagnosis
It is usually easy to differentiate
between a Baker’s cyst and a semimembranosus
bursa (see Fig. 4.36).
Remember the other common cause of a swelling
behind the knee joint – a popliteal aneurysm. This is
easy to diagnose if it has an expansile pulsation, but
easy to confuse with one of the above swellings if
it is thrombosed. Remember to feel the pulses at
the ankle and to palpate the other leg – popliteal
aneurysms are often bilateral.
Semimembranosus
bursa
Above the joint line
Joint line
Baker's cyst
Below the joint line
and deep to
gastrocnemius
FIG 4.36
A semimembranosus bursa appears above the joint
line. A Baker’s cyst appears below the joint line, deep to the
gastrocnemius muscle.
Chap-04.qxd 4/19/05 13:50PM Page 142
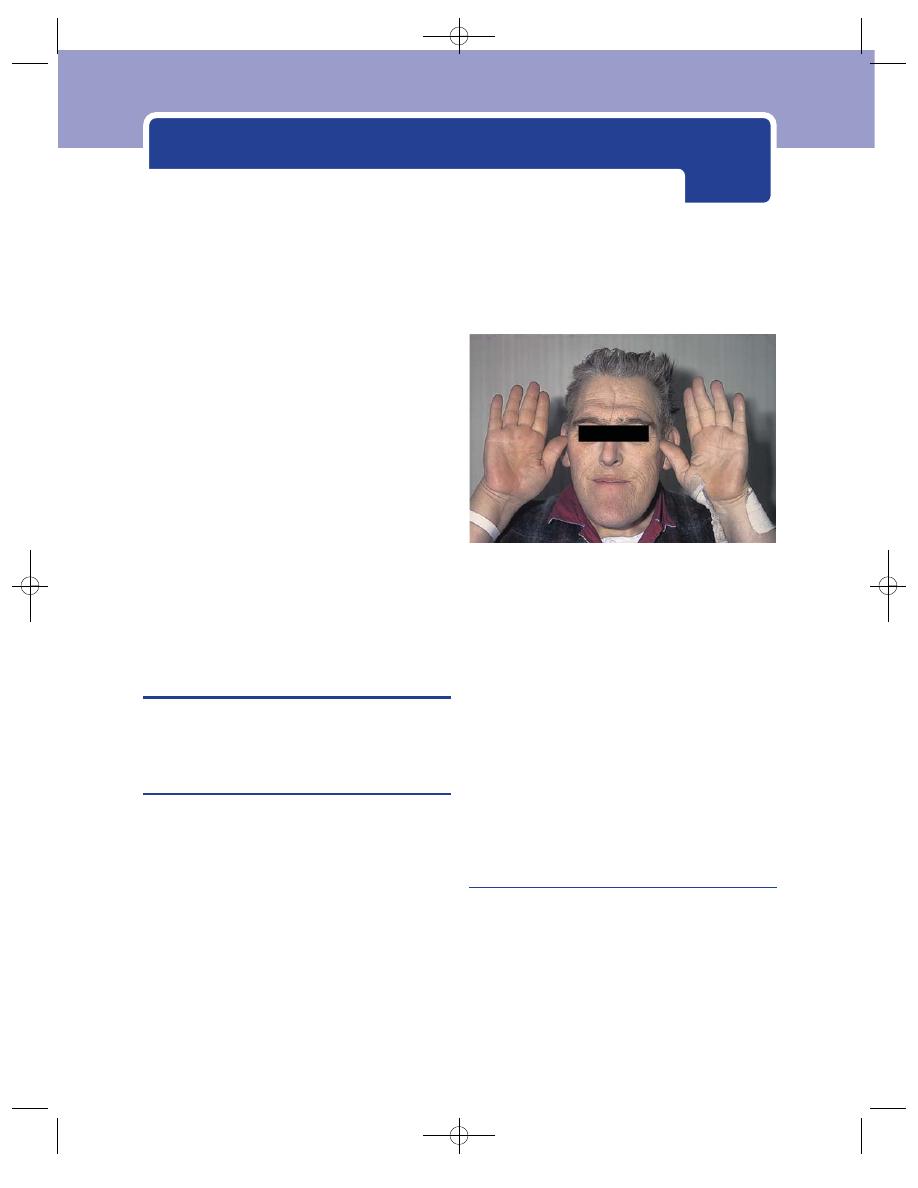
Conditions peculiar to the hands
The hand is mankind’s greatest physical asset and,
anatomically, one of his most distinctive features.
It has enabled humans to use the tools that their
brains have invented, and is indispensable to their
well-being. Everything that the doctor does to the
hand should be aimed at restoring or maintaining
its function.
When you examine the hand there are four sys-
tems to assess: the muscles, bones and joints; the cir-
culation; the nerves; and the skin and connective
tissues. The general examination of these systems is
described in other chapters, but the important
points relating to the hand are repeated here and
assembled into a system of examination designed
to ensure that you do not miss any important
abnormalities.
A PLAN FOR THE EXAMINATION OF
THE HAND
Examine each system in turn.
The musculoskeletal system (bones,
joints, muscles and tendons)
Inspection
Look for any abnormality of the shape, size and
contour of the hand. Look for local discolouration,
scars and sinuses. Look for muscle wasting by
assessing the size of the thenar and hypothenar emi-
nences and the bulk of the muscles between the
metacarpal bones (the interossei). Look at the wrist
joint.
Palpation
Feel the bony contours, the tender areas, and any
localized swellings. Feel the finger joints to assess
the cause of any swelling of these joints.
Movement
Check the range and ease of movement of all the
joints:
■
the carpometacarpal joint of the thumb
(flexion, extension, abduction, adduction and
opposition),
■
the metacarpophalangeal joints of the fingers
(flexion, extension, abduction and adduction),
■
the interphalangeal joints (flexion and
extension).
Inability to move these joints may be caused by
joint disease, soft-tissue thickening, divided tendons
or paralysed muscles.
The circulation
Inspection
Pallor of the fingers indicates arterial insufficiency
or anaemia. During an episode of vasospasm the
fingers may be white or blue. Observe the degree of
filling of the veins on the back of the hands. Ischaemic
atrophy of the pulps of the fingers makes the fingers
thin and pointed. Ischaemic ulcers, small abscesses
and even frank gangrene may be visible.
FIG 5.1
The large spade-like fingers and hands of acromegaly.
Chap-05.qxd 4/19/05 13:55PM Page 143
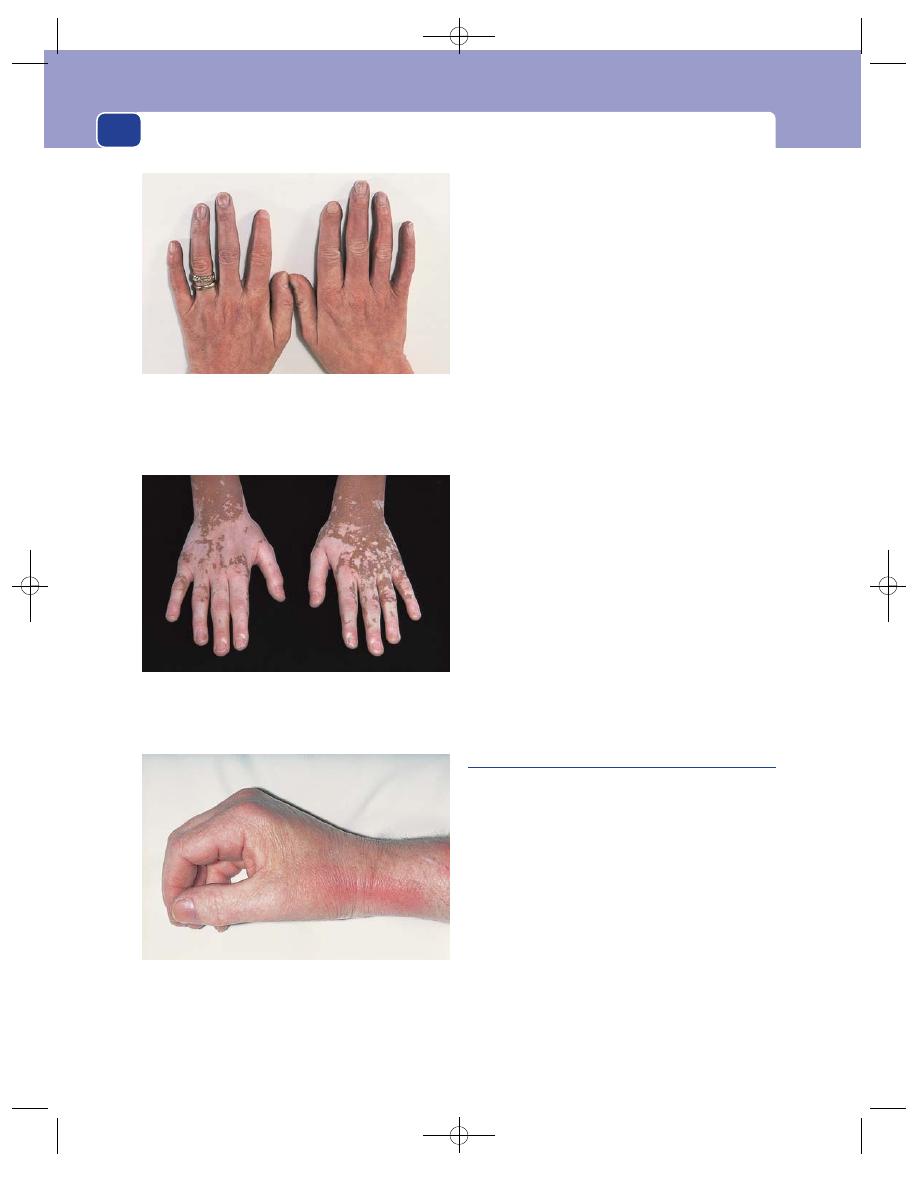
Conditions peculiar to the hands
144
Palpation
Feel the temperature of the skin of each finger.
Feel both pulses (radial and ulnar) at the wrist.
Sometimes the digital arteries can be felt on either
side of the base of the fingers.
Capillary return
A crude indication of the arterial
inflow to the fingers can be obtained from watching
the rate of filling of the vessels beneath the nail
after emptying them by pressing down on the tip of
the nail.
Allen’s test
Ask the patient to clench one fist tightly
and then compress the ulnar and radial arteries at
the wrist with your thumbs. After 10 seconds, ask the
patient to open the hand. The palm will be white.
Release the compression on the radial artery and
watch the blood flow into the hand.
Slow flow into one finger caused by a digital artery
occlusion will be apparent from the rate at which
that finger turns pink.
Repeat the procedure, but release the pressure on
the ulnar artery first.
Auscultation
Listen with the bell of your stethoscope over any
abnormal areas. Vascular tumours and arteriovenous
fistulae may produce a bruit, sometimes a palpable
thrill.
Measure the blood pressure in both arms.
The nerves
Sensory nerves
When there is loss of sensation you must find out
which type of sensation is lost (e.g. light touch,
pain, position sense, vibration sense), as described
in Chapter 1, and the distribution of the sensory
loss. Does it correspond to the innervation of one
nerve or to a dermatome? The following gives
details of the areas of skin innervated by the three
nerves of the hand.
Median nerve
The median nerve innervates the pal-
mar aspect of the thumb, index and middle fingers,
the dorsal aspect of the distal phalanx and half of the
middle phalanx of the same fingers, and a variable
amount of the radial side of the palm of the hand.
FIG 5.2
Acrocyanosis. A persistent blue discolouration of the
skin of the hands caused by mild vasospasm, usually induced
by a drop in ambient temperature.
FIG 5.3
Vitiligo (loss of pigmentation) in a dark-skinned
patient.
FIG 5.4
Inflammatory changes at the wrist. Such findings
often occur from superficial thrombophlebitis when an
intravenous infusion site becomes inflamed. In this patient
this was flitting thrombophlebitis migrans secondary to
carcinoma of the pancreas.
Chap-05.qxd 4/19/05 13:55PM Page 144
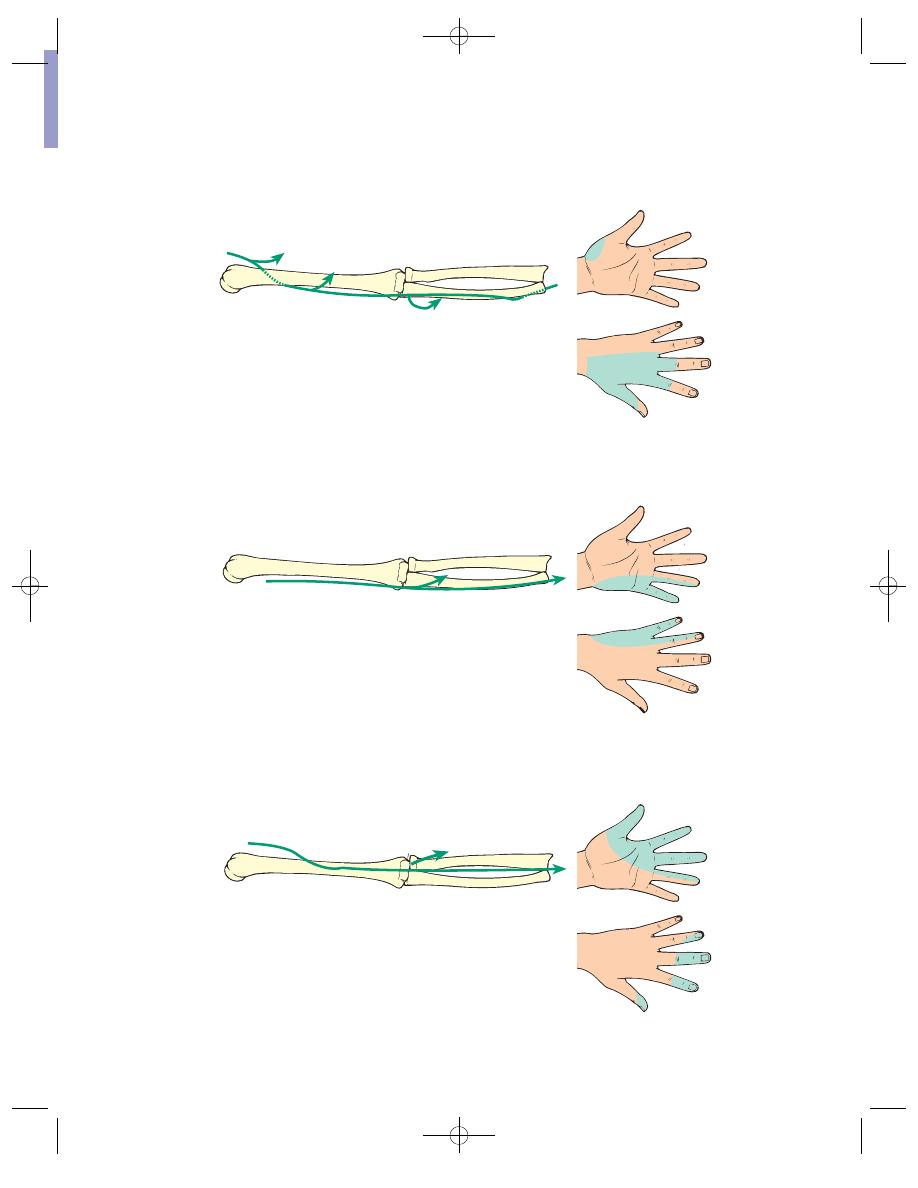
Median ner
ve
Flexor digitorum sublimis
Lateral half of flexor
digitorum profundus
(Flex the index finger)
Opponens and abductor
pollicis
(Lift the thumb
away from the palm)
Ulnar ner
ve
Flexor carpi ulnaris
Medial half of flexor
profundus
(Adduct
the wrist)
Muscles of hypothenar
eminence
Interossei
Adductor pollicis
(Abduct the little finger)
Radial ner
ve
Extensor digitorum
(Extend the wrist)
Triceps
(Extend the
elbow)
Brachioradialis
Posterior
Anterior
Posterior
Anterior
Posterior
Anterior
FIG
5.5
DISTRIBUTION OF THE NERVES OF THE UPPER LIMB
Chap-05.qxd 4/19/05 13:55PM Page 145
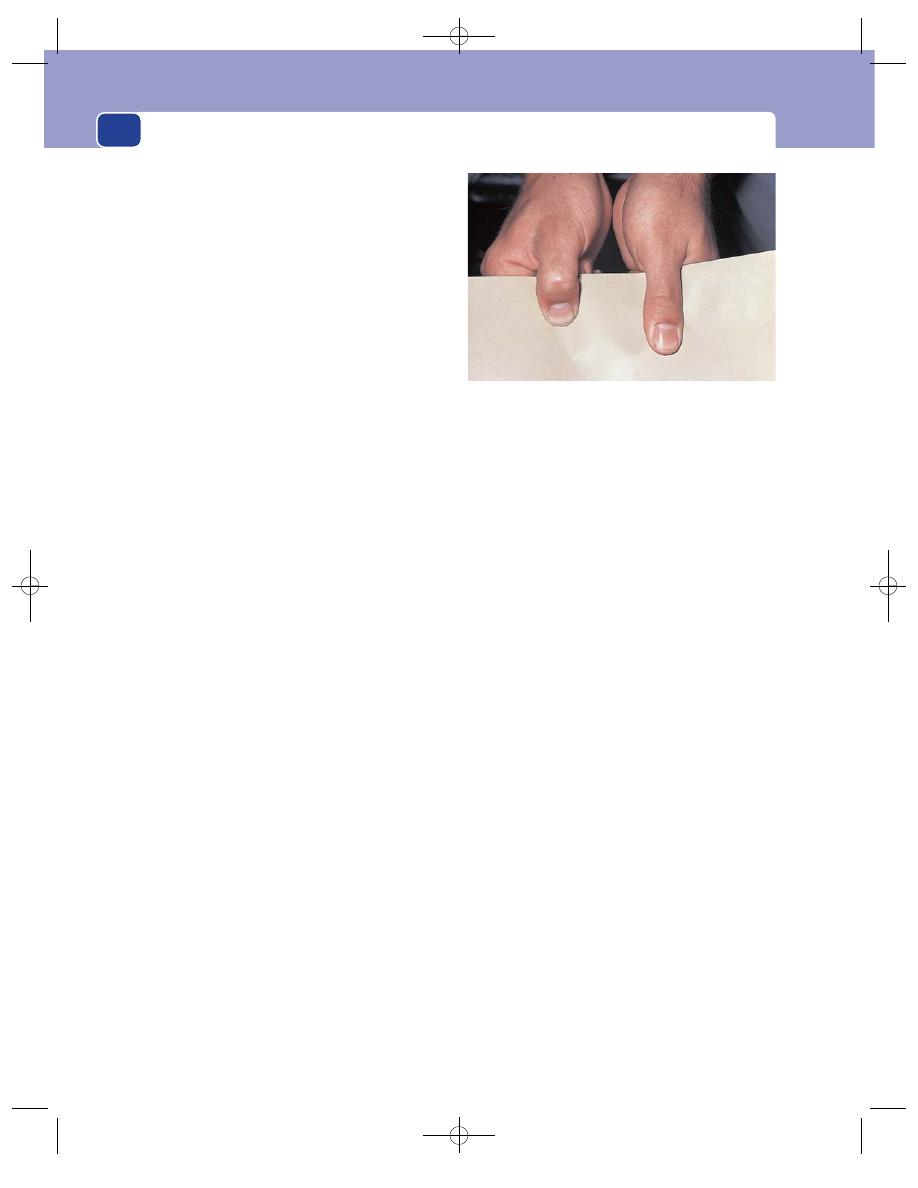
Conditions peculiar to the hands
146
Ulnar nerve
The ulnar nerve innervates the skin on
the anterior and posterior surfaces of the little fin-
ger and the ulnar side of the ring finger, the skin
over the hypothenar eminence, and a similar strip of
skin posteriorly. The ulnar nerve sometimes inner-
vates all of the skin of the ring finger and the ulnar
side of the middle finger.
Radial nerve
This innervates a small area of skin
over the lateral aspect of the first metacarpal and the
back of the first web space.
The dermatomes of the hand are:
■
C6 – thumb
■
C7 – middle finger
■
C8 – little finger.
Motor nerves
The muscles that control the movements of the
hand lie within the hand and in the forearm (i.e.
they are intrinsic and extrinsic). All the long flexors
and extensors of the fingers lie in the forearm, and
the nerves that innervate them leave their parent
nerves at or above the elbow.
The nerves that innervate the intrinsic muscles
have a long course in the forearm before they reach
the hand. Thus it is necessary to examine all the
motor functions of the three principal nerves in the
upper limb (median, ulnar and radial) if you wish
to find the level at which a nerve is damaged. A rapid
assessment of the motor function of these three
nerves in the hand can be obtained by looking for
the following physical signs.
A median nerve palsy, which may follow pene-
trating injuries, lacerations at the wrist, dislocation
of the carpal tunnel and carpal tunnel compression,
may present as follows.
If the injury is at wrist level:
■
wasting of the thenar eminence
■
absent abduction of the thumb
■
absent opposition of the thumb.
If the injury is at or above the cubital fossa:
■
wasting of the forearm and thenar eminence
■
loss of flexion of the thumb and index finger
■
hand held in the benediction position, with
ulnar fingers flexed and index finger straight.
An ulnar nerve palsy, which may follow damage
or compression at the elbow, penetrating injuries,
fractures of the medial epicondyle, lacerations at the
wrist and long-standing marked cubitus valgus, may
present as follows.
If the injury is at wrist level:
■
wasting of the hypothenar eminence and
hollows between the metacarpals
■
absence of flexion of the little and ring
fingers
■
claw hand, with ring and little finger
hyperextended at the metacarpophalangeal
joint and flexed at the interphalangeal
joints
■
absence of adduction and abduction of the
fingers with a positive Froment’s test.
If the injury is at the level of the elbow:
■
wasting of intrinsic muscles
■
claw hand, but with terminal interphalangeal
joints not flexed as half of flexor digitorum
profundus now paralysed
■
positive Froment’s test.
If the injury is high above the elbow:
■
all the above
■
the flexor carpi ulnaris also paralysed.
A radial nerve palsy, which may follow fractures
of the shaft of the humerus, penetrating injuries and
pressure in the axilla from prolonged resting with
the arm suspended over a chair or over a crutch,
may present in the following ways.
FIG 5.6
A positive Froment’s test on the right hand (i.e. on the
left of the picture) indicating an ulnar nerve palsy and
inability to adduct the thumb due to paralysis of adductor
pollicis. This means that the thumb flexes to grip paper due
to contraction of the flexor pollicis longus.
Chap-05.qxd 4/19/05 13:55PM Page 146
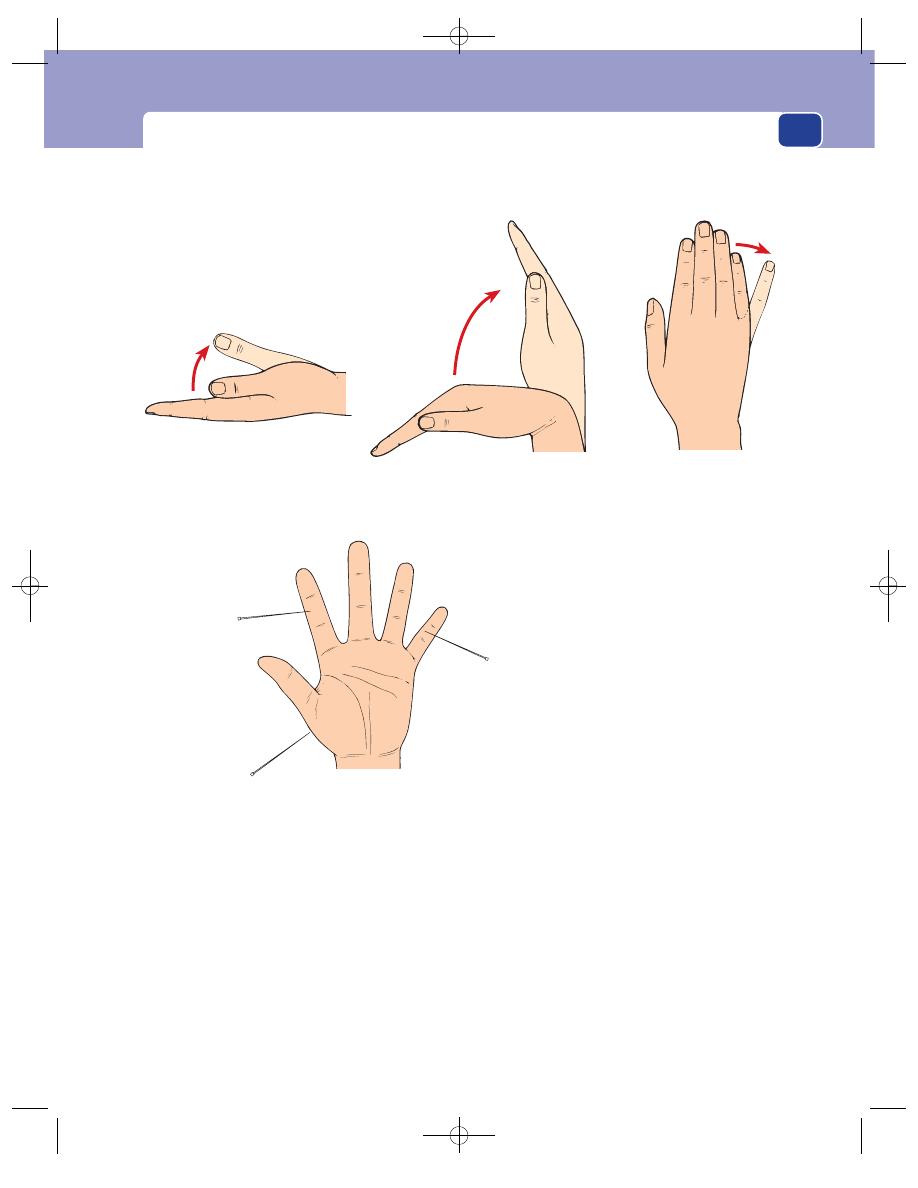
A plan for the examination of the hand
147
If there is an injury in the axilla:
■
absence of extension of the wrist (wrist drop)
■
loss of triceps action.
If the injury is at the level of the middle third of
humerus:
■
wrist drop
■
sparing of the brachioradialis (when paralysed,
this weakens elbow flexion).
If the injury is to the posterior interosseous:
■
hand held in radial deviation when attempting
extension
■
no wrist drop
■
an inability to maintain finger extension against
forcible flexion.
If the injury is to a superfical branch of the nerve:
■
no motor loss.
Motor innervation
Sensory innervation
Test sensation in these three areas
Abduct the thumb
Abduct the fingers
Ulnar nerve
Radial nerve
Median nerve
Index finger
Lateral aspect of
base of thumb
Little finger
Median nerve
Radial nerve
Ulnar nerve
Extend the wrist
FIG 5.7
FOUR QUICK TESTS OF THE MOTOR AND SENSORY INNERVATION OF THE HAND
Chap-05.qxd 4/19/05 13:55PM Page 147

Conditions peculiar to the hands
148
The examination of the motor function of these
three nerves can be simplified by using three screen-
ing tests:
1. median nerve: abduction of the thumb;
2. ulnar nerve: abduction of the little finger;
3. radial nerve: extension of the wrist.
As you perform each of these tests, feel the mus-
cle you are testing to check whether or not it is
contracting.
The skin and connective tissues
Much will have been learnt about the skin after
studying its circulation and innervation. Be careful
to note any colour changes and any inflammatory
processes. It is also important to palpate the palmar
fascia, as thickening and contraction of this struc-
ture are a common cause of contraction deformities
(Dupuytren’s contracture). Also note any change in
the shape or configuration of the hand and digits
and any abnormal skin creases. Hyperextensibility
of the joints may indicate a connective tissue dis-
order such as Ehlers–Danlos syndrome.
The wrist, elbow, shoulder, thoracic
outlet, neck
Examine the wrist, elbow, shoulder, thoracic outlet
and neck because abnormalities at these sites can
cause symptoms in the hand.
RECORDING DATA ABOUT THE HAND
Almost every issue of the Medical Insurance Societies’
publications contains references to errors that have
arisen because of inadequate or misleading records
of lesions in the hand.
Never forget to state which hand you are describ-
ing. Write the words in full: RIGHT or LEFT. A bad
R can easily be confused with an L.
Name the digits
Some people prefer to number rather than name the
digits, the first digit being the thumb, the second
digit the index finger and so on. But unless you
remember to write the word ‘digit’ every time, you
will eventually make a mistake because the first fin-
ger, which is the index finger, is the second digit. Do
not use this system; always use names: thumb,
index, middle, ring and little finger.
FIG 5.8
Arachnodactyly – long spindly fingers associated with
Marfan’s syndrome (see page 220).
FIG 5.9
The abnormal palmar creases associated with
Down’s syndrome.
FIG 5.10
The hyperextensibility of the thumb and
metacarpophalangeal joints of Ehlers–Danlos syndrome.
Chap-05.qxd 4/19/05 13:55PM Page 148
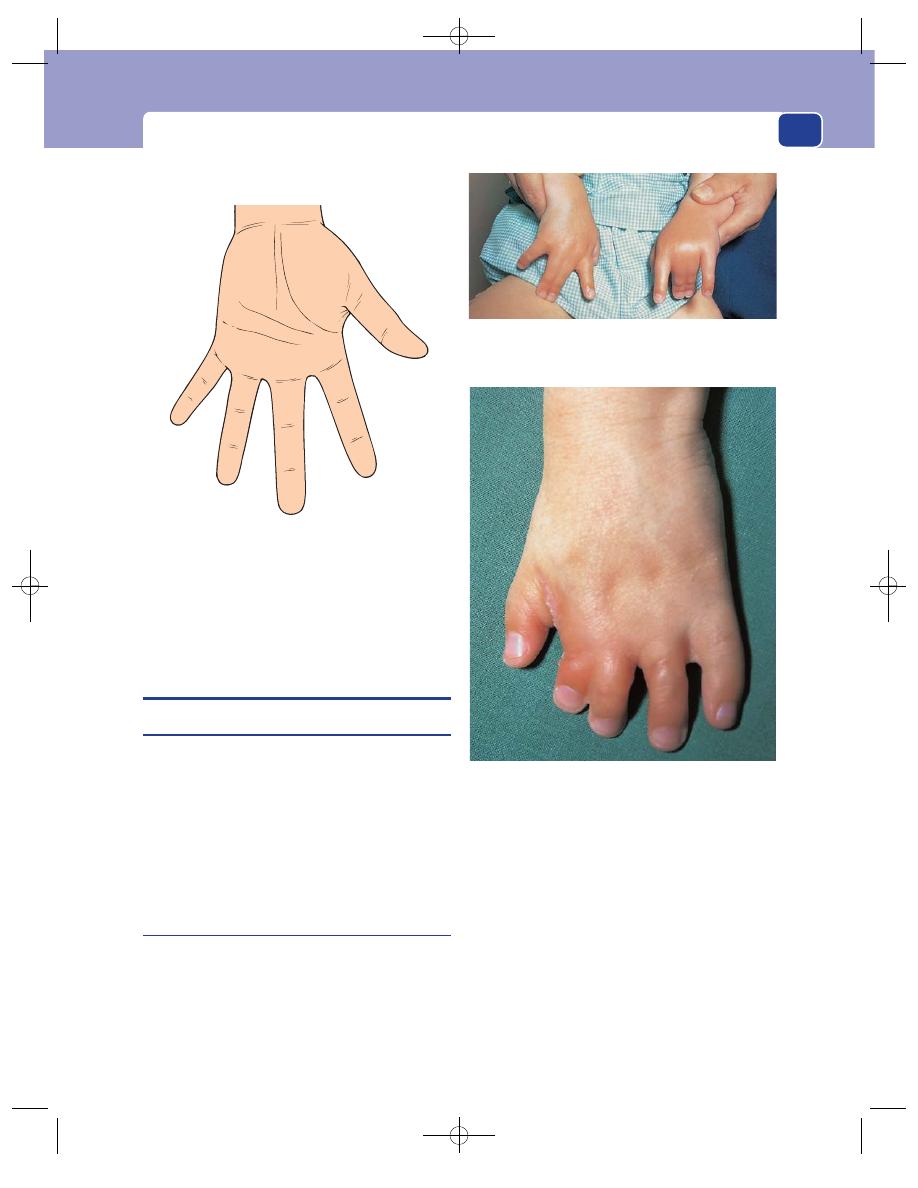
Abnormalities and lesions of the hand
149
It is acceptable to number the toes, as the first toe
is the great toe.
ABNORMALITIES AND LESIONS OF
THE HAND
Congenital abnormalities
There are three common skeletal abnormalities in
the hand:
1. part of the hand (usually a digit) may be absent
2. there may be an extra digit
3. the digits may be fused (syndactyly).
All these abnormalities are rare, but immediately
recognizable.
Dupuytren’s contracture
This is a thickening and shortening of the palmar
fascia and the adjacent connective tissues that lie deep
to the subcutaneous tissue of the hand and superfi-
cial to the flexor tendons. The cause of this change in
the fascia is not known. As the thickening increases,
it becomes attached to the skin of the palm.
It is known to occur in response to repeated local
trauma and in association with cirrhosis of the liver,
but in most cases there is no obvious predisposing
cause.
History
Age
Dupuytren’s contracture usually begins in mid-
dle age but progresses so slowly that many patients
do not present until old age.
Sex
Men are affected ten times more often than
women.
Little
Ring
Middle
Index
Thumb
Left hand
FIG 5.11
The names of the digits of the hand.
FIG 5.12
Syndactyly. Fusion of the middle and ring fingers of
each hand.
FIG 5.13
Syndactyly. Fusion of the middle and index fingers,
in this case associated with a marked failure of finger growth
and other bony abnormalities.
Chap-05.qxd 4/19/05 13:55PM Page 149
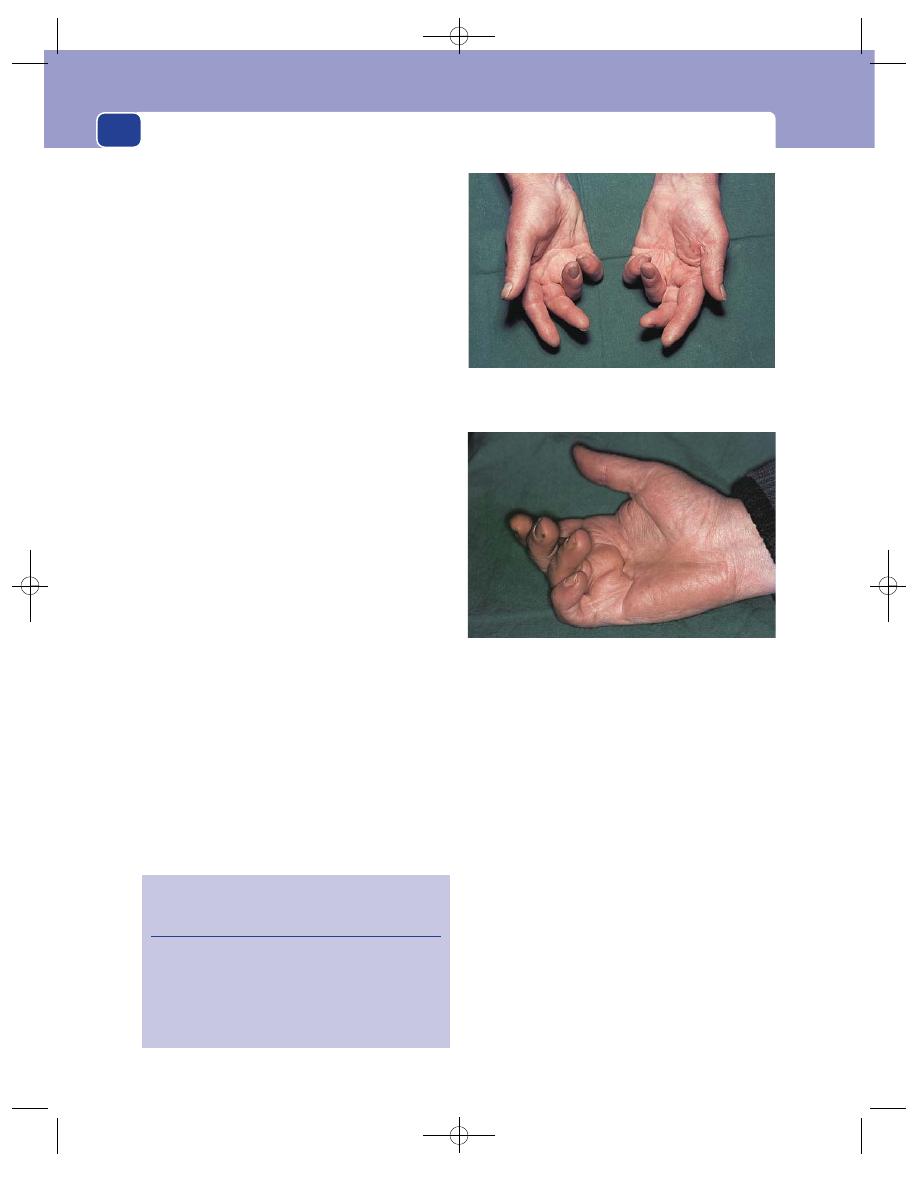
Conditions peculiar to the hands
150
Symptoms
A nodule in the palm. The patient may
notice a thickening in the tissues in the palm of the
hand, near the base of the ring finger, many years
before the contractures develop.
Contraction deformities. The patient notices an
inability fully to extend the metacarpophalangeal
joint of the ring finger, and later the little finger. If
the contraction of the palmar fascia becomes severe,
the finger can be pulled so far down into the palm of
the hand that it becomes useless.
There is no pain associated with this condition.
Very rarely, the nodule in the palm may be slightly
tender.
Development
The nodule gradually enlarges and the
strands of contracting fascia become prominent.
Deep creases form where the skin becomes tethered
to the fascial thickening, and the skin in these creases
may get soggy and excoriated. The deformity of the
fingers slowly worsens.
Multiplicity
Dupuytren’s contracture is commonly
bilateral and can also occur in the feet.
Cause
Dupuytren’s contracture may follow repeated
trauma to the palm of the hand, which is probably
why it used to be found in shoe repairers and other
manual workers, but nowadays it is uncommon to
find a convincing cause.
Systemic disease
There may be symptoms of epilepsy
or cirrhosis of the liver. There is a higher incidence
of the condition in patients suffering from these
diseases. The reasons for these associations are
unexplained.
Family history
Dupuytren’s contracture can be famil-
ial. If so, it is inherited in an autosomal dominant
manner.
Examination
The palm of the hand
Palpation of the palm of the
hand reveals a firm, irregular-shaped nodule with
indistinct edges, 1–2 cm proximal to the base of the
ring finger. Taut strands can be felt running from
the nodule to the sides of the base of the ring and
little fingers, and proximally towards the centre of
the flexor retinaculum. These bands get tighter if
you try to extend the fingers.
The skin is puckered and creased, and tethered to
the underlying nodule.
The deformity
The metacarpophalangeal joint and the
proximal interphalangeal joint are flexed because
the palmar fascia is attached to both sides of the
proximal and middle phalanges. The distal inter-
phalangeal joint tends to extend. The ring finger is
most affected and may be pulled down so far that its
nail digs into the palm of the hand.
FIG 5.14
DUPUYTREN’S CONTRACTURE.
Revision panel 5.1
Factors associated with Dupuytren’s
contracture
Alcoholism
Epilepsy
Diabetes
Repeated trauma
Family history
The anterior view shows the typical deformity: flexion of the
metacarpophalangeal and proximal interphalangeal joints and
extension of the distal interphalangeal joints.
This view shows the puckering of the skin of the palm and
the taut strands of palmar aponeurosis.
Chap-05.qxd 4/19/05 13:56PM Page 150
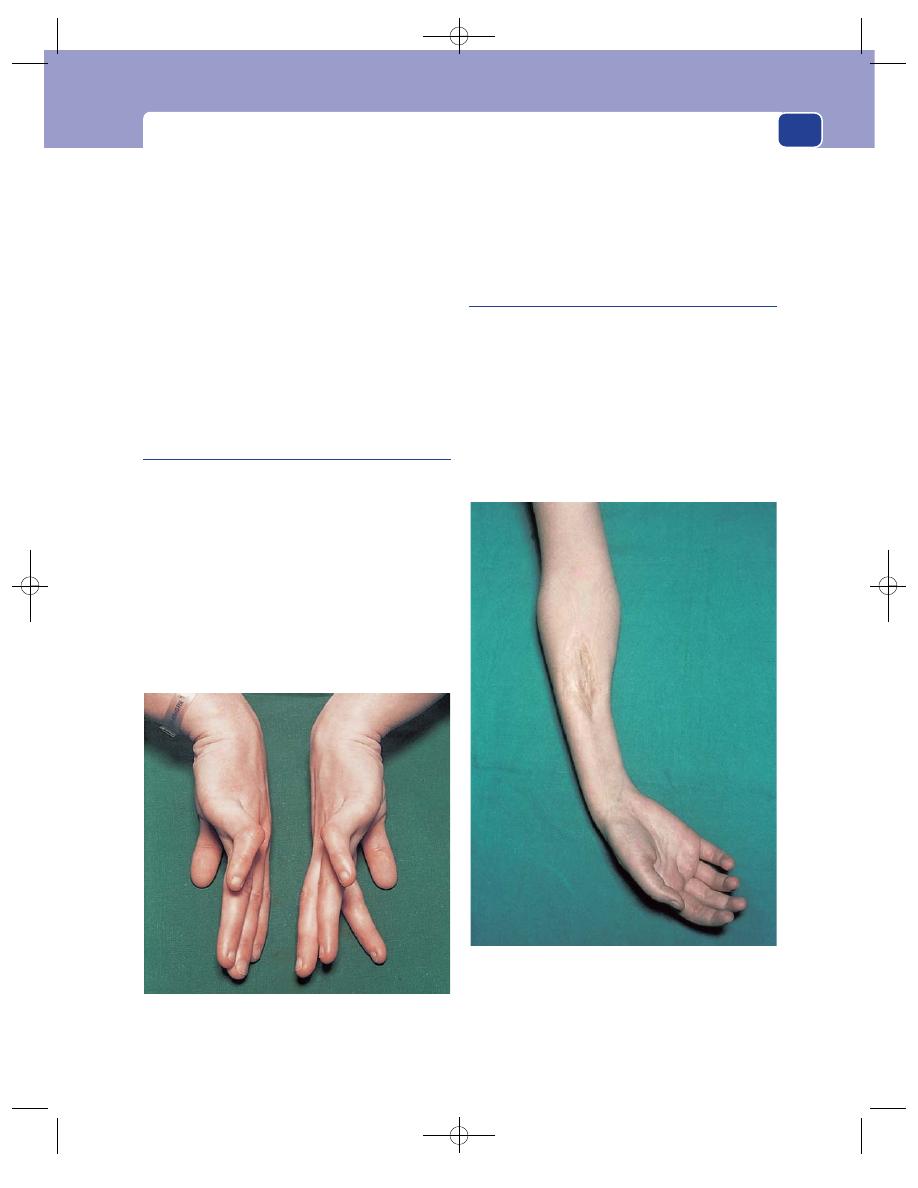
Abnormalities and lesions of the hand
151
The flexion deformity is not lessened by flexing
the wrist joint.
Local tissues
The rest of the hand is normal. There
may be some thickening of the subcutaneous tissue
on the back of the proximal phalanges of the
affected fingers, sometimes called Garrod’s pads.
General examination
Dupuytren’s contracture is some-
times associated with epilepsy and cirrhosis of the
liver. There may be systemic evidence of these dis-
eases. These are rare associations.
The condition may be present in the feet.
Congenital contracture of the little
finger
This is a congenital deformity of the little finger.
The patient is rarely aware of the fact that they have
a deformity, accepting it as the normal shape of their
little finger.
It is mentioned here because, although it is the
opposite deformity to a Dupuytren’s contracture,
the student who is unaware of its existence may
misdiagnose it.
Pick up a tea cup with your thumb and index fin-
ger and hook your little finger in the manner of the
affected snob at a tea party. You will find that you
have extended your metacarpophalangeal joint and
flexed both of the interphalangeal joints. Someone
with a congenital contracture of the little finger has
this deformity all the time and cannot straighten the
finger.
Volkmann’s ischaemic contracture
Volkmann’s ischaemic contracture is a shortening
of the long flexor muscles of the forearm, caused
by fibrosis of the muscles, secondary to ischaemia.
The common causes of the ischaemia are direct
arterial damage at the time of a fracture near the
elbow (most often a supracondylar fracture), a tight
plaster which restricts blood flow, and arterial
embolism.
FIG 5.15
Congenital contracture of the little finger. Extension
of the metacarpophalangeal joint and flexion of the proximal
interphalangeal joint.
FIG 5.16
Volkmann’s ischaemic contracture. Wasting,
fibrosis and contraction of the muscles of the forearm
following ischaemic damage, causing flexion and ulnar
deviation of the wrist joint and flexion of all the finger
joints. Further contraction will turn this into a permanently
clawed hand.
Chap-05.qxd 4/19/05 13:56PM Page 151
Conditions peculiar to the hands
152
History
Age
Supracondylar fractures are common in chil-
dren and young adults, so Volkmann’s contracture
most often begins between the ages of 5 and 25.
Cause
The patient usually knows the cause of the
deformity because they can clearly relate the loss of
finger extension to their injury. Indeed, the loss of
finger movements frequently begins while the arm
is immobilized for the treatment of the fracture.
Symptoms
When muscles become ischaemic, they
are usually painful. If a patient complains of pain
under their plaster at a point distant from the site of
the fracture, remove the plaster and examine the
muscles carefully.
Movements of the fingers, especially extension,
become painful and then limited. This is more
noticeable if there is no restriction of movement
caused by a coexisting fracture. If the forearm is not
in a plaster cast, the patient soon discovers that they
can extend their fingers if they flex their wrist.
If the blood supply of the hand is also dimin-
ished, the skin of the hand will be cold and pale.
Ischaemia of the nerves in the anterior compart-
ment (the median and anterior interosseous nerves)
often causes ‘pins and needles’ (paraesthesia) in the
distribution of the median nerve, and sometimes
the severe burning pain of ischaemic neuritis.
Development
As the acute phase passes, the pain
slowly fades away, but the restriction of finger exten-
sion increases and the hand becomes claw-like. The
patient may present with a fully developed deformity.
Examination
Inspection
The skin of the hand is usually pale and
the hand looks wasted. All the finger joints are
flexed and the anterior aspect of the forearm is thin
and wasted. The deformity is called a ‘claw hand’.
Palpation
In the acute phase the forearm is swollen
and tense, but once this has passed the forearm feels
thin, the hand is cool and the pulses at the wrist may
be absent. In the later stages the fibrosis and short-
ening make the forearm muscles hard and taut.
Movement
Extension of the fingers is limited but
improves as the wrist is flexed. This is an impor-
tant sign, as it differentiates Volkmann’s ischaemic
contracture from Dupuytren’s contracture. Further
flexion of the fingers (beyond the deformity) is
present but the grip is weak. All other hand move-
ments are present but may be difficult to perform
with the fingers fixed in an acutely flexed position.
Passive forced extension of the fingers is painful
in the acute stage and uncomfortable in the estab-
lished condition. An important diagnostic feature
of ischaemic contracture is that all the muscles, even
the damaged ones, have some function, whereas
when a claw hand is caused by a nerve lesion, some
of the muscles will be completely paralysed.
State of local tissues
The abnormalities in the arteries
and nerves of the forearm and hand have already
been described. If the contracture follows a fracture,
the vessels and nerves above the level of the fracture
should be normal.
The heart, great vessels, subclavian and axillary
arteries must be examined carefully in case they are
the source of an arterial embolus.
Palpate the supraclavicular fossa for a cervical rib
or subclavian artery aneurysm.
Carpal tunnel syndrome
This is a condition in which the median nerve is
compressed as it passes through the carpal tunnel –
the space between the carpal bones and the flexor
retinaculum. The compression can be caused by
skeletal abnormalities, swelling of other tissues within
the tunnel, or thickening of the retinaculum. It is
often associated with pregnancy, rheumatoid arthri-
tis, diabetes, myxoedema, previous trauma and
osteoarthritis.
History
Age and sex
Carpal tunnel syndrome is common in
middle-aged women – especially at the menopause.
Local symptoms
Pins and needles in the fingers,
principally the index and middle fingers, is the com-
mon presenting symptom. Sometimes the thumb is
involved.
Theoretically the little finger should never be
affected, as it is innervated by the ulnar nerve, but
occasionally patients complain that the whole of
their hand tingles.
Pain in the forearm. For some (so far unex-
plained) reason, patients often complain of a pain
which radiates from the wrist, up along the medial
Chap-05.qxd 4/19/05 13:56PM Page 152
Abnormalities and lesions of the hand
153
side of the forearm. This is usually an aching pain,
not pins and needles.
Loss of function. As the compression increases,
the axons in the nerve are killed and objective signs
of nerve damage appear. Because the sensitivity of
the skin supplied by the median nerve is reduced,
the patient notices that she drops small articles and
cannot do delicate movements. Note that this is not
caused by a loss of muscle power, but by the loss of
fine discriminatory sensation. Ultimately, if the
nerve damage is severe, there may be a loss of motor
function, which presents as weakness and paralysis
of the muscles of the thenar eminence and the
first two lumbricals (see median nerve palsy on
page 146).
Exacerbations at night. Patients are often woken
in the middle of the night by their symptoms. This
feature is difficult to explain but is so characteristic
that it is considered to be pathognomonic of the
condition.
General symptoms
An increase of weight commonly
exacerbates carpal tunnel syndrome symptoms.
A change in weight may be secondary to another
disease such as myxoedema, diabetes or steroid
therapy, or to physiological water retention, as in
pregnancy.
If the condition is secondary to rheumatoid arthri-
tis or osteoarthritis, the patient may have symptoms
of arthritis in the wrist and other joints.
Examination
Inspection
The hand usually looks quite normal,
except in the advanced case where there may be visible
wasting of the muscles forming the thenar eminence.
Palpation
Pressure on the flexor retinaculum does
not produce the symptoms in the hand, but holding
the wrist fully flexed for 1 or 2 minutes may induce
symptoms. Light-touch sensitivity and two-point
discrimination may be reduced in the skin inner-
vated by the median nerve (palm, thumb, index and
middle finger). The loss of muscle bulk in the thenar
eminence may be easier to feel when these muscles
are contracting.
The wrist pulses and the colour and temperature
of the skin should be normal.
Movement
All movements of the joints of the hand,
active and passive, should be present.
Abduction, adduction and opposition of the
thumb may be weak, but the muscles that cause
these movements are rarely completely paralysed.
General examination
There are two important aspects
of the general examination.
First, you must exclude other causes of paraes-
thesia in the hand, such as cervical spondylosis, cer-
vical rib, peripheral neuritis, and rare neurological
disease. This requires a detailed examination of the
head, neck and arm.
Second, you must look for evidence of the cause
of the carpal tunnel syndrome, such as pregnancy,
rheumatoid arthritis, osteoarthritis and myxoedema.
Claw hand
Claw hand is a deformity in which all the fingers
are permanently flexed. Although an ulnar nerve
paralysis makes the hand claw-like, because it causes
flexion of the ring and little fingers, it does not cause
a true claw hand, because only part of the hand is
involved.
The causes of claw hand are neurological and
musculoskeletal.
Neurological causes
Remember these causes by thinking of the course of
the nerve fibres from the spinal cord through the
brachial plexus into the peripheral nerves. Although
the deformity is caused by a loss of motor function,
there is often an associated sensory loss.
Spinal cord
Poliomyelitis, syringomyelia, amy-
otrophic lateral sclerosis.
Brachial plexus
Trauma to medial roots and cord –
especially birth injuries to the lower cord as in
Klumpke’s paralysis; infiltration of the brachial
plexus by malignant disease.
Peripheral nerves
Traumatic division of the median
and ulnar nerves; peripheral neuritis.
Musculoskeletal causes
Volkmann’s ischaemic contracture
This only causes
a claw hand at rest, as the deformity can be reduced
or abolished by flexion of the wrist.
Joint disease
Asymmetrical muscle tension, bone
and joint deformities and subluxation of the finger
Chap-05.qxd 4/19/05 13:56PM Page 153
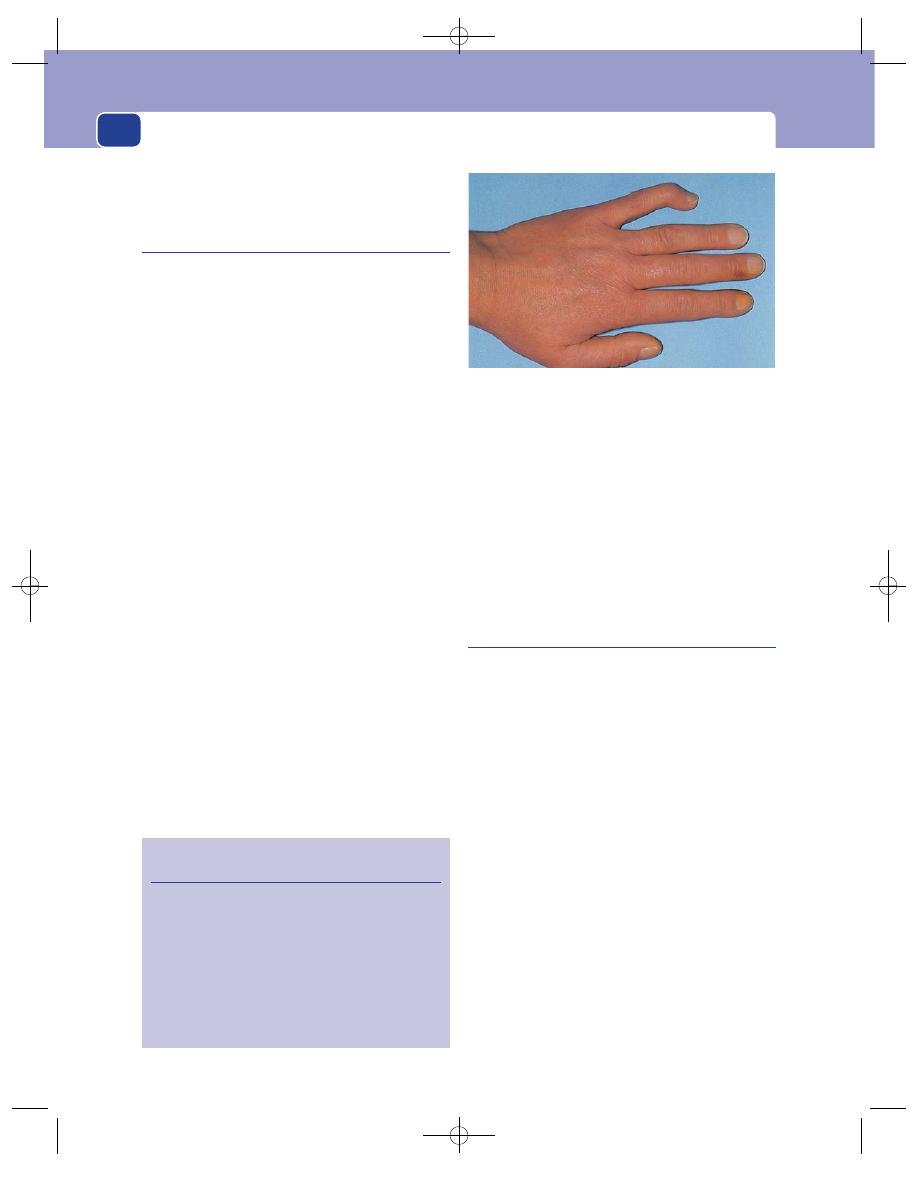
Conditions peculiar to the hands
154
joints caused by rheumatoid arthritis may produce
a claw-like hand.
Trigger finger
This is a condition in which a finger gets locked in full
flexion and will only extend after excessive voluntary
effort, or with help from the other hand. When exten-
sion begins, it does so suddenly and with a click –
hence the name trigger finger. The condition is caused
by a thickening of the flexor tendon, paratenon, or a
narrowing of the flexor sheath, preventing movement
of the tendon within the flexor sheath.
History
Age and sex
There are two groups of patients affected
by this condition – middle-aged women and very
young children. The thumb can be affected in
neonates and infants, but this is a rare condition.
Symptoms
The patient complains that the finger
clicks and jumps as it moves, or gets stuck in a flexed
position.
A trigger finger is not usually a painful condi-
tion, even when force is required to extend it.
The disability gradually gets more severe, but a
fixed, immovable flexed finger is uncommon.
Cause
Occasionally the patient can recall an injury
to the palm of the hand which may have caused the
tendon or tendon sheath to thicken, but in most
cases there is no indication of the cause.
Examination
Inspection
The patient will show you how the finger
gets stuck and how it snaps out into extension. The
finger looks quite normal.
Palpation and movement
The thickening of the tendon
or tendon sheath can be felt at the level of the head
of the metacarpal bone. During movement, the
thickening can be felt snapping in and out of the
tendon sheath.
General examination
Trigger finger is not associated
with any systemic musculoskeletal disease.
Mallet finger
This is a fixed flexion deformity of the distal inter-
phalangeal joint of a finger, caused by an interruption
of the extensor mechanism: either a rupture of the
extensor tendon or an avulsion fracture of its inser-
tion. It is also known as ‘baseball’ finger because the
commonest cause of the injury is a blow on the tip
of the finger by a ball or hard object which forcibly
flexes it against the pull of the extensor tendon,
which then ruptures or pulls off the bone.
History
The patient usually remembers the original injury
but, if it is not painful, may not complain about it
until the deformity is established and a nuisance.
Symptoms
The inability to extend the tip of a finger
is not a great disability, but to a person with an
occupation that requires fine finger movements,
including full extension of the distal interpha-
langeal joints, the deformity can be a serious handi-
cap. Some patients complain that the deformity is
disfiguring.
FIG 5.17
A mallet finger. The patient’s inability to extend the
terminal phalanx of the little finger is only noticeable when he
holds his fingers out straight.
Revision panel 5.2
The causes of claw hand (main en griffe)
Combined ulnar and median nerve palsy
Volkmann’s ischaemic contracture
Advanced rheumatoid arthritis
Brachial plexus lesion (medial cord)
Spinal cord lesions
Syringomyelia
Poliomyelitis
Amyotrophic lateral sclerosis
Chap-05.qxd 4/19/05 13:56PM Page 154
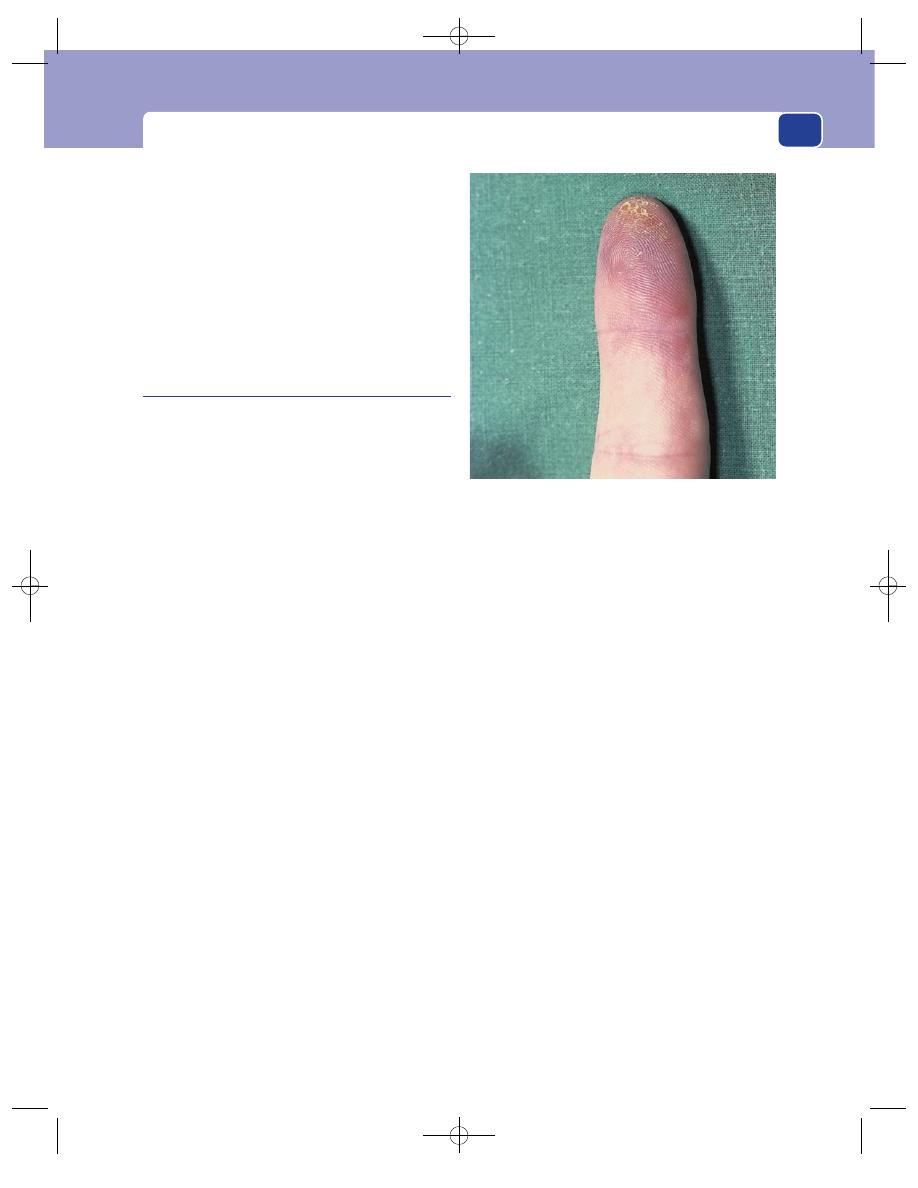
Abnormalities and lesions of the hand
155
Examination
When the patient holds out their hand, with the fin-
gers extended, the distal phalanx of the affected fin-
ger remains 15–20° flexed. If you flex the distal
interphalangeal joint to 90°, the patient can extend
it back to the 20° position but cannot get it straight.
An X-ray is required to decide whether the ten-
don is ruptured or avulsed.
Chilblains
(Erythema pernio)
A chilblain is an area of oedema in the skin and sub-
cutaneous tissues that follows a local change in cap-
illary permeability induced by cold. Chilblains are
by far the most common of the group of conditions
known as cold sensitivity states. In addition to the
oedema, there is vasospasm and interstitial infiltra-
tion with lymphocytes.
History
Age
Chilblains first appear in childhood or early
adult life.
Sex
Woman are affected more often than men.
Occupation
An outdoor occupation increases the
chances of a susceptible subject getting chilblains.
Symptoms
The patient complains of a swelling on the
side or back of a finger (or toe) that has developed
within a few minutes or hours of exposure to cold.
The swelling is painful, especially in a warm envi-
ronment, and often itches. The overlying skin may
ulcerate and weep serous fluid. As chilblains usually
follow exposure to the cold, they are more common
in winter.
Chilblains are often multiple and occur on the
toes, heels and lower leg, as well as the hands.
Development
Chilblains first appear in childhood
and adolescence and then appear regularly every
winter until the patient reaches middle age. After
the susceptibility to chilblains subsides, most patients
continue to have some cold sensitivity problems in
the hands, such as Raynaud’s phenomenon (see
next page).
Family history
The tendency to get chilblains is often
familial.
Examination
Position
Chilblains usually occur on the backs and
sides of the fingers.
Colour
At first the skin over the swelling is pale, but
it quickly turns a reddish-blue colour.
Temperature
The temperature of the skin over the
swelling is normal or slightly cooler than normal.
Shape and size
The lumps on the fingers are flat-
tened, elongated mounds, with indistinct edges that
fade away into the normal finger. They vary in size.
On the fingers they are usually 0.5–2 cm wide, but on
the legs they can be 4–5 cm across.
Surface
The oedema involves the skin and subcuta-
neous tissues and often collects in an intradermal
blister, which can burst and leave a superficial ulcer.
If the acute superficial ulcer fails to heal, it may
become deeper, destroying the full thickness of the
skin and leaving a permanent scar.
Composition
Although the lump is mainly oedema
fluid, there is often sufficient cellular infiltration to
make it feel firm and sometimes hard.
Lymph glands
The axillary or inguinal lymph glands
will not be enlarged unless the chilblain is infected –
a rare event.
FIG 5.18
Patchy areas of discolouration and coldness, which
are sometimes painful, sometimes hypoaesthetic, caused by
digital artery embolism.
Chap-05.qxd 4/19/05 13:56PM Page 155
Conditions peculiar to the hands
156
Local tissues
There may be evidence of long-standing
arterial insufficiency – absent wrist pulses, loss of the
finger pulps, recurrent paronychia and scars from
previous chilblains. The changes should be distin-
guished from the painful hypoaesthetic patchy areas
of discolouration and coldness that can result from
arterial emboli. The nerves of the hands should be
normal.
General examination
The other extremities may be
cold and show Raynaud’s phenomenon or acro-
cyanosis.
Raynaud’s phenomenon
The symptoms and signs which are commonly
called Raynaud’s phenomenon are a series of colour
changes in the hands following exposure to cold.
To remember the order of the colour changes,
remember the initials WBC (the same as ‘white
blood count’): white, blue and crimson (red).
White. The skin of one, or a number, of the fin-
gers turns white.
Blue. After a variable time, the skin turns a purple-
bluish colour but is still cold and numb.
Red. When the vasospasm relaxes, the skin turns
red and hot and feels flushed, tingling and often
painful.
One or two of these phases may be absent. The
fingers may go white and then turn red, or return to
normal after the blue phase, or just turn blue.
The orthodox explanation of these changes is as
follows.
The white phase is caused by severe arteriolar
spasm, making the tissues bloodless.
The blue phase is produced by a very slow trickle
of deoxygenated blood through dilated capillaries.
Venous congestion may also be caused by persistent
venous spasm.
The red phase is the period of high blood flow
(reactive hyperaemia) that follows relaxation of the
arteriolar spasm. The increased blood flow through
the dilated vessels makes the skin red, hot and
painful.
There are many causes of Raynaud’s phenomenon.
These are described in Chapter 7 because Raynaud’s
phenomenon is not a condition peculiar to the hands
alone, although they are invariably affected. It can also
occur in the feet, ears, nose and lips.
In between attacks the tissues look quite
normal. Ultimately the arteries suffer permanent
structural damage, which causes permanent tissue
damage.
Scleroderma
Scleroderma is an uncommon disease in which the
skin and subcutaneous tissues become thickened and
stiff. Although it is a systemic disease affecting the
bowel, especially the oesophagus and colon, as well as
the skin, it often appears in the hands many years
before it develops in other sites. Structural changes in
the hands may be preceded for many years by
Raynaud’s phenomenon. The aetiology of the disease
is unknown. The principal abnormality is found in
the collagen fibrils, which are thick and stiff.
History
Age
Scleroderma commonly begins in the late 30s,
but may not become severe for many years.
Sex
Females are more often affected than males.
Symptoms
There is thickening of the fingers. The
patient notices that the skin of her fingers is slowly
becoming pale and thick, and the movements of the
interphalangeal joints are reduced.
Many patients present with the colour changes of
Raynaud’s phenomenon years before the skin
changes begin.
Painful splits and ulcers appear in the skin of
the fingertips.
Some patients get multiple, recurrent small
abscesses around the nails; these abscesses throb
and ache and finally discharge a small bead of pus.
Development
Although the symptoms may begin in
one hand or even one finger, they gradually spread
to involve all the digits of both hands.
Systemic effects
If the disease affects the oesophagus,
the patient will complain of dysphagia. Involvement
of the colon causes constipation and colicky
abdominal pain.
Local examination
Colour
The skin of the hands has a white, waxy
appearance caused by the combination of ischaemia
and skin thickening.
Chap-05.qxd 4/19/05 13:56PM Page 156

Abnormalities and lesions of the hand
157
Temperature
The hands are cool, especially at the
fingertips.
Shape and size
The hands and fingers look swollen
and the skin thickened but the pulps of the finger-
tips may be wasted. There are often small scars on
either side of the finger nails, and on the pulps, where
previous abscesses have pointed and discharged.
Nodules
There may be small, hard subcutaneous
nodules in the finger pulps and on the dorsal aspect
of the hands and fingers. These are patches of calci-
fied fat. This abnormality is called calcinosis.
Pulses
The pulses at the wrist are usually palpable,
but Allen’s test often reveals occlusions of the digital
arteries.
Nerves
The nerve supply of the hand is normal.
Joints
The thick skin reduces the range of all move-
ments of the finger joints. The interphalangeal joints
are particularly affected, and the most noticeable
abnormality is an inability to straighten the fingers.
General examination
Other signs of scleroderma may be visible.
Face. The skin of the face looks tight and shiny
and the mouth is small – microstomia. There are
often multiple telangiectases all over the face (and
sometimes on the hands).
Wasting. There may be generalized wasting if the
dysphagia is causing malnutrition.
Abdominal distension. Scleroderma in the large
bowel inhibits peristalsis and causes chronic consti-
pation and abdominal distension.
The combination of Calcinosis, Raynaud’s
phenomenon, Esophageal problems (dysphagia),
Scleroderma and Telangiectases is known as the
CREST syndrome.
Flexor sheath ganglion
A ganglion is an encapsulated myxomatous degen-
eration of fibrous tissue. When a ganglion occurs on
the anterior aspect of a flexor sheath it can interfere
with the grip and cause pain and disability out of
proportion to its size.
History
Age and sex
Flexor sheath ganglia are most common
in middle-aged men.
FIG 5.19
THE EFFECT ON THE HANDS OF SCLERODERMA.
Thick, stiff fingers with pale, waxy, thick skin.
An ischaemic ulcer on the fingertip. These slowly destroy the
pulp of the finger and make it pointed.
Calcinosis in the pulps of the fingers of a patient with CREST
syndrome.
Chap-05.qxd 4/19/05 13:56PM Page 157
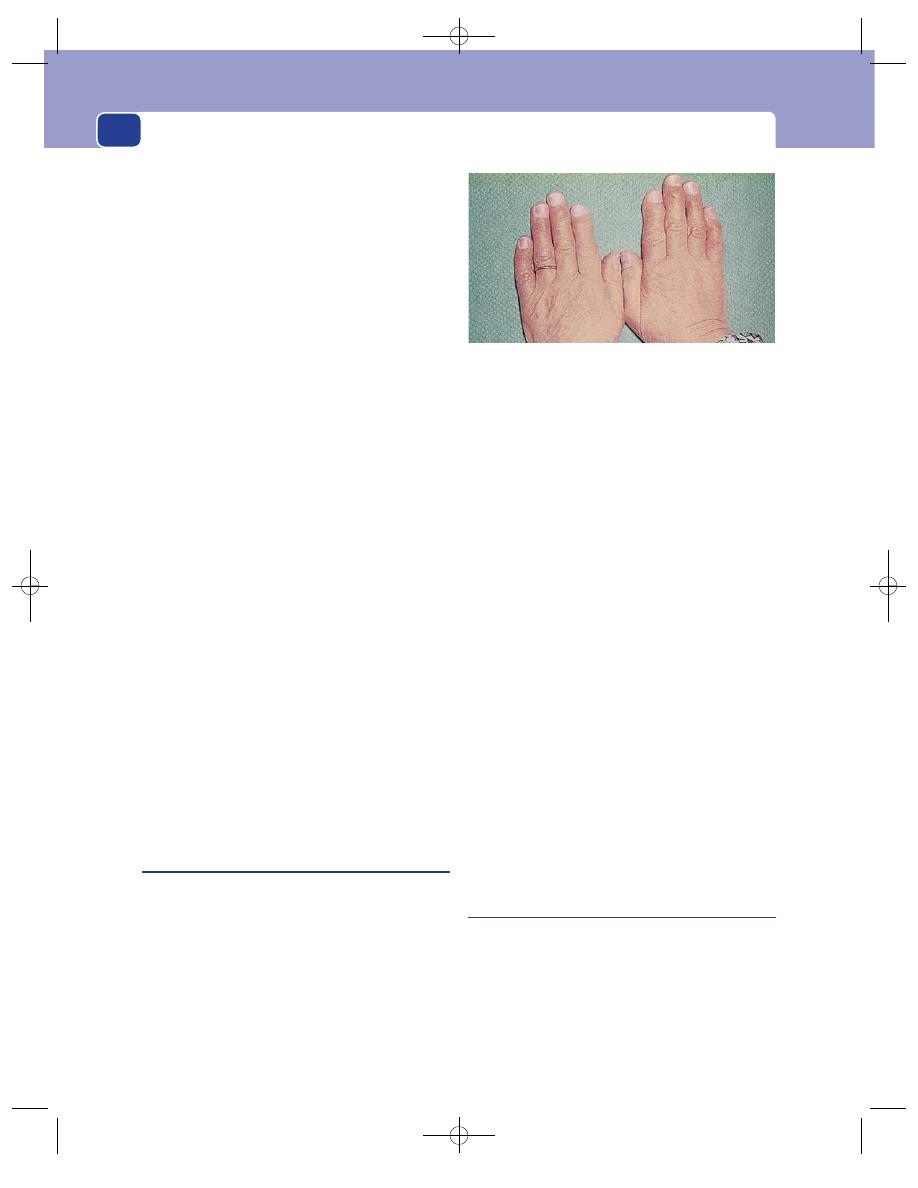
Conditions peculiar to the hands
158
Symptoms
The patient complains of a sharp pain at
the base of one finger whenever they grip some-
thing tightly.
They may also complain of a lump at the site of
the pain.
Examination
Colour and temperature
These are normal.
Site
A small tender nodule can be felt on the palmar
surface of the base of a finger, superficial to the
flexor sheath.
Tenderness
Direct pressure on the lump is usually
very painful.
Shape
The nodule is spherical or hemispherical.
Size
Flexor sheath ganglia are usually quite small;
some cause symptoms when they are only 2–3 mm
in diameter.
Surface and edge
The surface of the nodule is smooth
and the edge sharply defined.
Composition
The nodule feels solid and hard. It is
usually too small to permit the assessment of any
other features such as fluctuation or translucence.
Lymph glands
The local lymph glands should not be
enlarged.
Local tissues
The rest of the hand is normal.
Comment
Benign giant cell tumours of the flexor sheath pres-
ent in an identical manner and are indistinguishable
from flexor sheath ganglia.
Heberden’s nodes
Heberden’s nodes are bony swellings close to the dis-
tal finger joints. They are non-specific and do not
indicate any particular disease.
History
The patient complains of swelling and deformity of
their knuckles. There may be a history of an old injury
to the finger or aching pains in both the lumps and
the joints.
Examination
Heberden’s nodes are commonly found on the dor-
sal surface of the fingers just distal to the distal
interphalangeal joint. They are not mobile and can
be easily recognized as part of the underlying bone.
The joint movements may be slightly restricted
by osteoarthritis, and there may be radial deviation
of the distal phalanx. The index finger is the finger
most often affected. Small adventitious bursae may
develop between the skin and the nodes. Similar
nodes may appear near the proximal interpha-
langeal joint.
Comment
Heberden’s nodes do not indicate any specific
underlying bone or joint disease and have no clini-
cal significance. They should not be confused with
rheumatoid nodules, which are areas of necrosis
surrounded by fibroblasts and chronic inflamma-
tory cells and are found in all types of connective
tissue. Patients with rheumatoid nodules invariably
have other evidence of rheumatoid arthritis.
Rheumatoid arthritis in the hand
The symptoms and signs of rheumatoid arthritis
are described in Chapter 4, but, as this disease
affects the hand so often, its manifestations in the
hand are described here. All the deformities of
rheumatoid arthritis result from the combination of
uneven pull by the tendons and destruction of the
joint surfaces.
FIG 5.20
Heberden’s nodes. This patient had full, painless
movements of all her finger joints but large Herberden’s
nodes on the base of the distal phalanges of both index and
middle fingers.
Chap-05.qxd 4/19/05 13:56PM Page 158
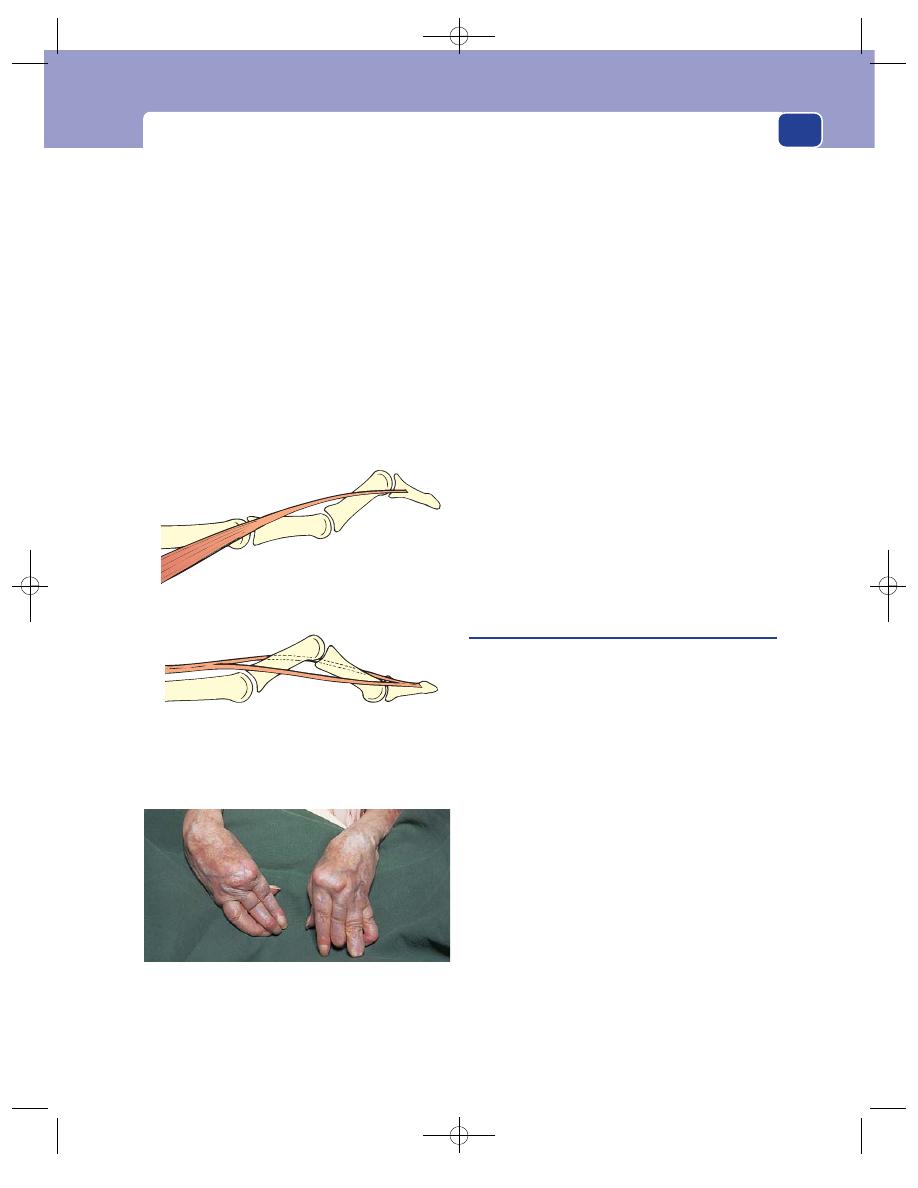
Abnormalities and lesions of the hand
159
Thickening of the joints
The joints most affected are the metacarpopha-
langeal and the proximal interphalangeal joints.
Swelling of these joints gives the finger a fusiform,
spindle shape.
Ulnar deviation of the fingers
The fingers are pulled towards the ulnar side of the
hand, causing a varus deformity at the metacar-
pophalangeal joints. In advanced disease the varus
deformity can be as much as 45–60°.
Flexion of the wrist
The wrist joint develops a fixed flexion deformity
and usually some ulnar deviation.
‘Swan neck’ deformity of the fingers
This deformity is hyperextension of the proximal
interphalangeal joint and flexion of the distal inter-
phalangeal joint. It is caused by fibrotic contraction
of the interosseous and lumbrical muscles.
Boutonnière deformity
The joint deformities of this abnormality are the
opposite of those of the ‘swan neck’ deformity: flexion
of the proximal interphalangeal joint and hyperex-
tension of the distal interphalangeal joint.
It is caused by the projection and trapping of
the flexed proximal interphalangeal joint through a
rupture of the central portion of the extensor ten-
don expansion.
Tendon ruptures
In severe rheumatoid arthritis, any tendon may
undergo attrition (damage from friction) and rup-
ture. This causes a variety of deformities. The com-
monest tendons to rupture are the long extensor
tendons of the fingers and thumb.
Compound palmar ‘ganglion’
This is a term that is applied to an effusion in the
synovial sheath that surrounds the flexor tendons. It
is not a ganglion. In the UK it is now invariably sec-
ondary to rheumatoid arthritis, but in many other
parts of the world it is almost always caused by a
tuberculous synovitis.
History
The commonest presenting symptom is swelling on
the anterior aspect of the wrist and sometimes in
the palm of the hand. Pain is uncommon.
The patient may notice crepitus during move-
ments of the fingers.
Paraesthesia may occur in the distribution of
the median nerve.
Examination
Distension of the flexor tendon synovial sheath pro-
duces a soft, fluctuant swelling which can be felt on
the anterior aspect of the wrist and lower forearm,
and in the palm of the hand. Because the swelling
passes beneath the flexor retinaculum, compression
FIG 5.22
Rheumatoid arthritis in the hands. These hands are
grossly deformed. The joints are swollen, the wrists flexed
and the fingers deviated. In the right hand the index finger
has a ‘swan neck’ deformity, whereas the ring finger has a
boutonnière deformity.
The swan neck deformity is caused by fibrotic
contracture of the interosseus and lumbrical muscles.
The boutonnière deformity develops when the proximal
interphalangeal joint pokes through the centre of the
extensor expansion following rupture of its central portion.
FIG 5.21
The finger deformities of rheumatoid arthritis.
Chap-05.qxd 4/19/05 13:56PM Page 159
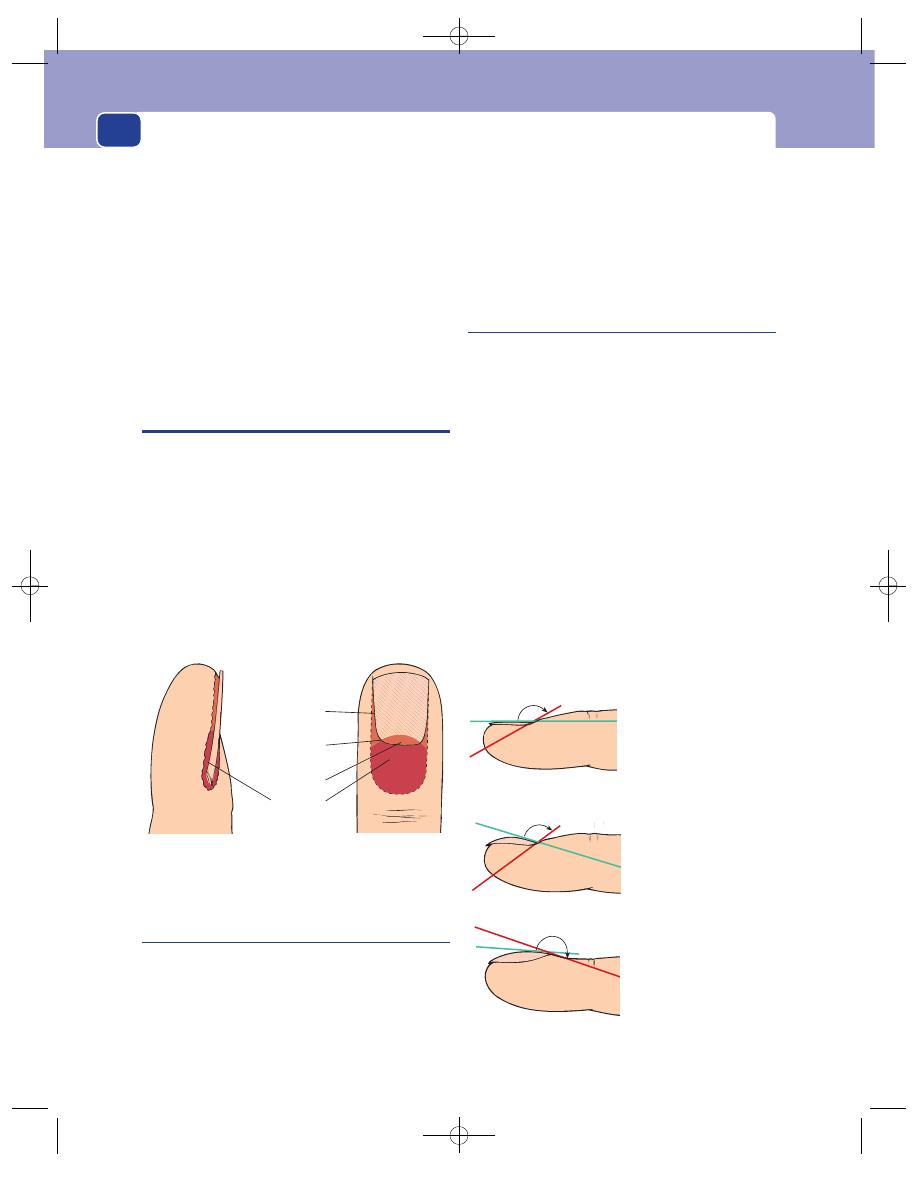
Conditions peculiar to the hands
160
of the lump on one side of the retinaculum makes it
distend on the other side.
Crepitus may be felt during palpation and when
the patient moves their fingers. This is caused by the
presence of fibrin bodies within the synovial sheath –
commonly called ‘melon seed bodies’.
There are no local signs of inflammation.
General examination
All the joints should be exam-
ined to exclude rheumatoid arthritis, and the chest
should be examined (and X-rayed) to exclude
tuberculosis.
THE NAILS
Inspection of the nails often yields useful informa-
tion about the patient’s general health.
The nails are usually pale pink. The commonest
cause of loss of this colour is anaemia.
Another sign of anaemia in the hands of white-
skinned races is loss of skin crease colour. When the
hand is relaxed, the palmar skin creases are slightly
darker than the rest of the skin, but if the skin of
the palm is stretched, the creases turn a deep red.
This deep red colour is not visible if the patient is
anaemic.
Splinter haemorrhages
Splinter haemorrhages are small extravasations of
blood from the vessels of the nail bed caused by
minute arterial emboli. They are long, thin, red-
brown streaks, their long axis running towards the
end of the finger. Their colour and shape make them
look like splinters of wood beneath the nail.
The presence of splinter haemorrhages is an
important physical sign because they are usually
caused by emboli from a bacterial endocarditis or a
fulminating septicaemia. They may also occur in
rheumatoid arthritis, mitral stenosis and severe
hypertension.
Clubbing
Clubbing of the nails is a term used to describe the
loss of the normal angle between the surface of the
nail and the skin covering the nail bed.
If you look at your finger from the side, you will
see that the plane of the nail and the plane of the
skin covering the base of the nail bed form an angle
of 130–170°.
In clubbed nails there is hypertrophy of the tis-
sue beneath the nail bed, which makes the base of
the nail bulge upwards and distorts nail growth so
that the nail becomes curved. The planes of the nail
and the skin covering the nail bed then meet at an
angle greater than 180°.
It is possible to have a very curved nail but still have
a normal nail/nail-fold angle, so do not look only at
the shape of the nail when assessing clubbing: look
at the whole finger.
The terminal phalanx may enlarge to make the
end of the finger bulbous.
Nail bed
Lunule
Cuticle
(eponychium)
Lateral nail
fold
FIG 5.23
The anatomy of the nail.
Normal nail/nail-
fold angle
Acute angle caused by a
curved nail, not clubbing
Nail/nail-fold angle
greater than 180
°=
clubbing
Normal and abnormal nail/nail-fold angles.
FIG 5.24
CLUBBING.
Chap-05.qxd 4/19/05 13:56PM Page 160
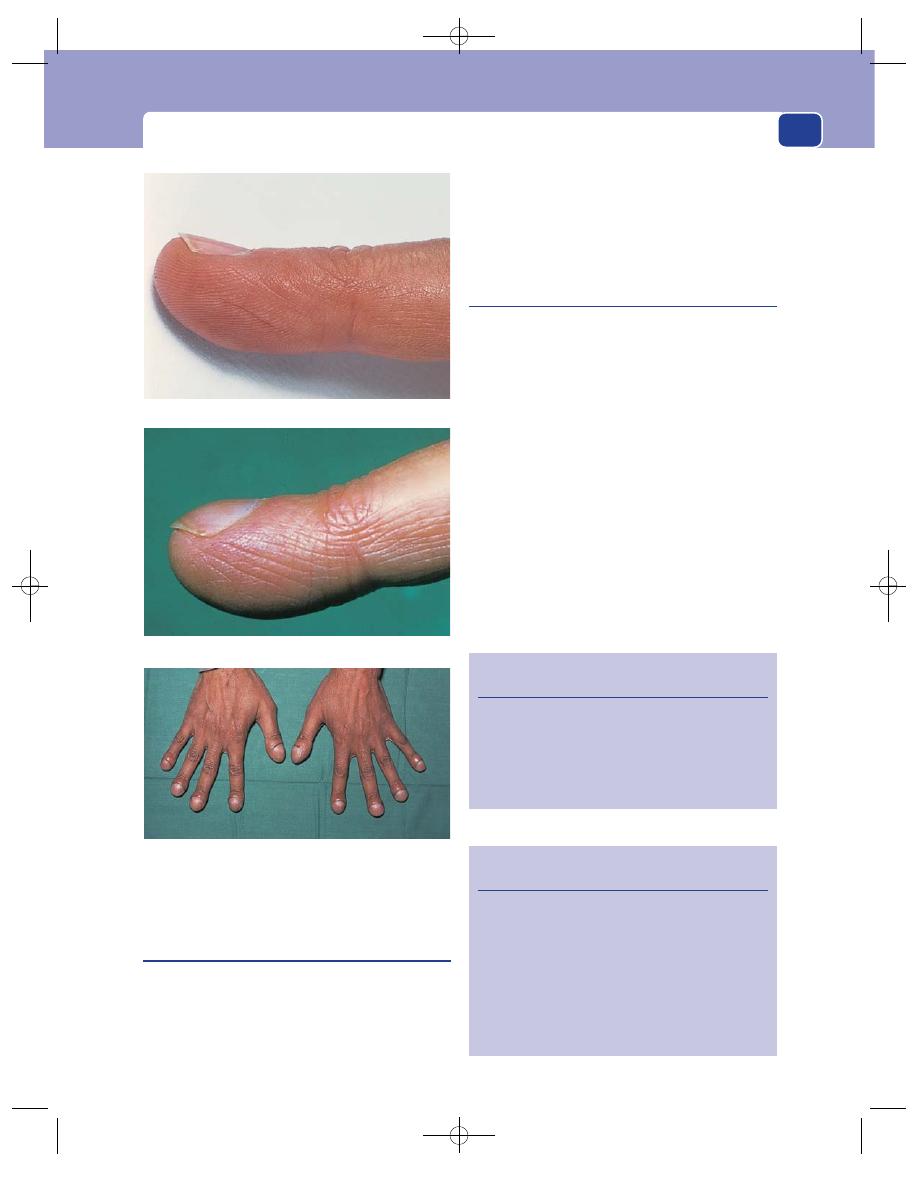
The nails
161
Spoon-shaped nails
(koilonychia)
A normal nail is convex transversely and longi-
tudinally, the degree of curvature varying consider-
ably from person to person. Loss of both these
curves produces a hollowed-out spoon-shaped nail
(koilonychia).
When a patient complains that their nails have
changed from a normal to a spoon shape, it is very
likely that they have developed anaemia following
chronic loss of blood, usually from menorrhagia or
haemorrhoids.
Subungual haematoma and melanoma
A blow on a nail can cause bleeding beneath it.
A collection of blood beneath the nail is called a sub-
ungual haematoma. If it appears at the time of the
injury, the patient usually makes their own diagno-
sis and only comes for treatment if it is painful.
Sometimes the patient does not notice the injury
and comes complaining of a brown spot beneath the
nail. The clinical problem in this case is to decide
whether the brown spot is haemosiderin or melanin –
a haematoma or a mole.
The features of the spot sometimes help. A
haematoma is usually reddish-brown, with sharp
edges. A melanoma is brown with a greyish tinge,
and has indistinct edges.
Inspection with a small hand-lens may solve the
problem by revealing small blood vessels in the
lesion, which means it is cellular.
FIG 5.24
continued
Revision panel 5.3
The signs of clubbing
Increased nail/nail-fold angle
Increased longitudinal and transverse nail
curvature
Bulbous terminal phalanges
Spongy nail bed
Revision panel 5.4
Some causes of clubbing
Congenital
Carcinoma of the bronchus
Chronic lung disease
Alveolitis
Bronchiectasis
Cystic fibrosis
Congenital cyanotic heart disease
Ulcerative colitis/Crohn’s disease
A normal finger.
A nail/nail-fold angle greater than 180°
⫽ clubbing.
Clubbing of all the fingers. Note the swelling of the terminal
phalanges.
Chap-05.qxd 4/19/05 13:56PM Page 161
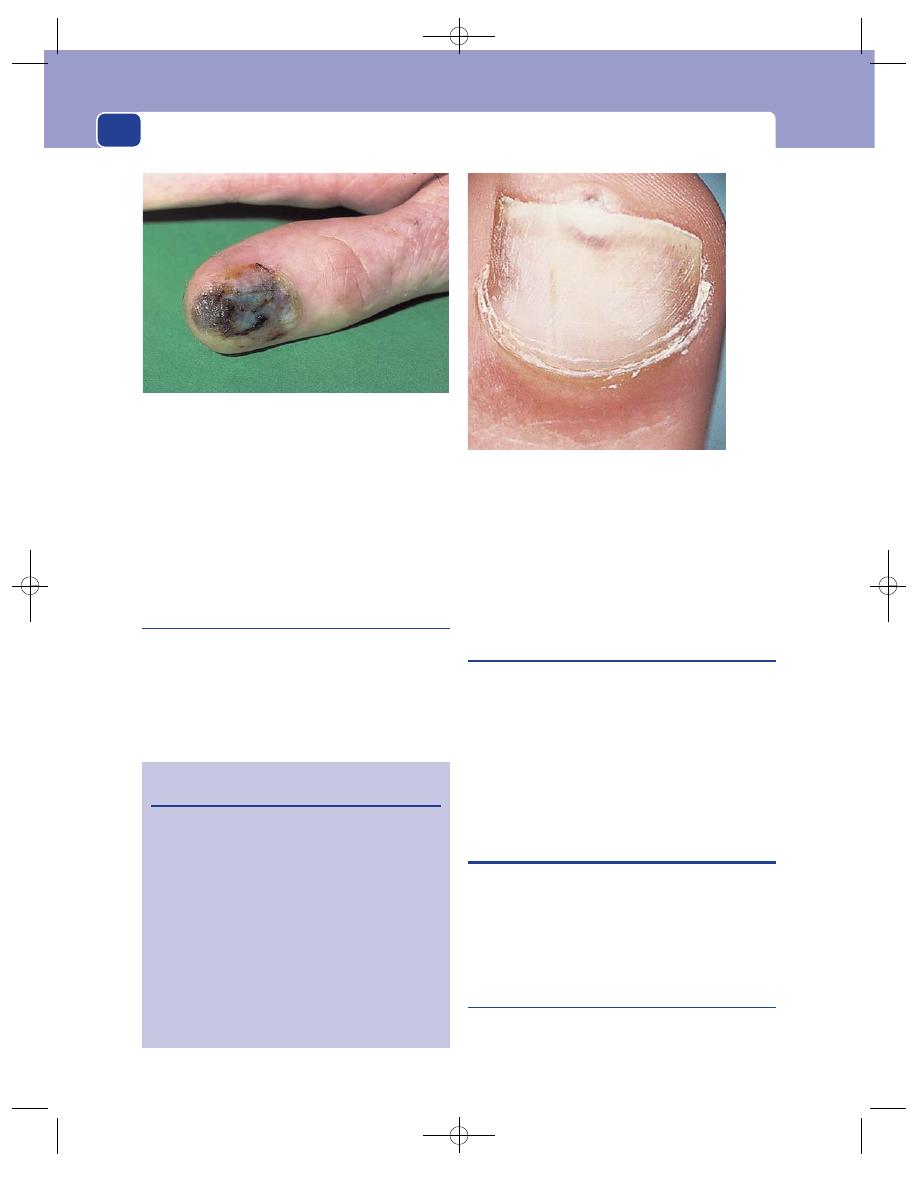
Conditions peculiar to the hands
162
If the patient has watched the lesion for a few
weeks, they will be able to tell you if it has moved
down the nail with nail growth, or stayed still.
Haematomata move down the nail; melanomata do
not move.
If it is not possible to make a definite clinical
diagnosis, the patient should be managed as if they
had a melanoma until you prove otherwise.
Glomus tumour
This is a very rare tumour but is mentioned because
it can cause a great deal of pain, and often occurs
beneath the nail. It is an angioneuromyoma.
The patient complains of severe pain every time
they touch the nail. Examination usually reveals a
small, purple-red spot beneath the nail. The colour
is due to the angiomatous nature of the tumour; the
pain comes from its abnormally rich nerve supply.
Glomus tumours can occur in any part of the skin
but are most often found in the hands.
Changes in the nails associated with
generalized diseases
■
Psoriasis: pitting, ridges, poor growth.
■
Myxoedema: brittle nails.
■
Cirrhosis of the liver: white nails.
■
General debilitating illnesses: transverse
furrows (Bean’s lines).
■
Anaemia: koilonychia.
■
Telangiectasia: Rendu–Osler–Weber syndrome.
■
Gout (and pseudogout).
INFECTIONS IN THE HAND
Infections in the hand cause severe pain and swelling.
They are more likely to present in an emergency
department than in a routine surgical outpatient
clinic, but two varieties are so common that they
deserve a description in this chapter.
Paronychia
This is an infection beneath the skin at the side or base
of the nail, and which develops into a small abscess.
FIG 5.26
A subungual glomus tumour.
Revision panel 5.5
Common nail abnormalities
Loosening
Psoriasis
Fungal infections
Pitting
Psoriasis
Transverse ridges
Systemic illness
Local damage
(paronychia)
Longitudinal ridges
Myxoedema
Thickening and twisting
Trauma
(onychogryphosis)
Age
Clubbing
See Revision
panel 5.4
FIG 5.25
A subungual malignant melanoma of the thumb.
Chap-05.qxd 4/19/05 13:56PM Page 162
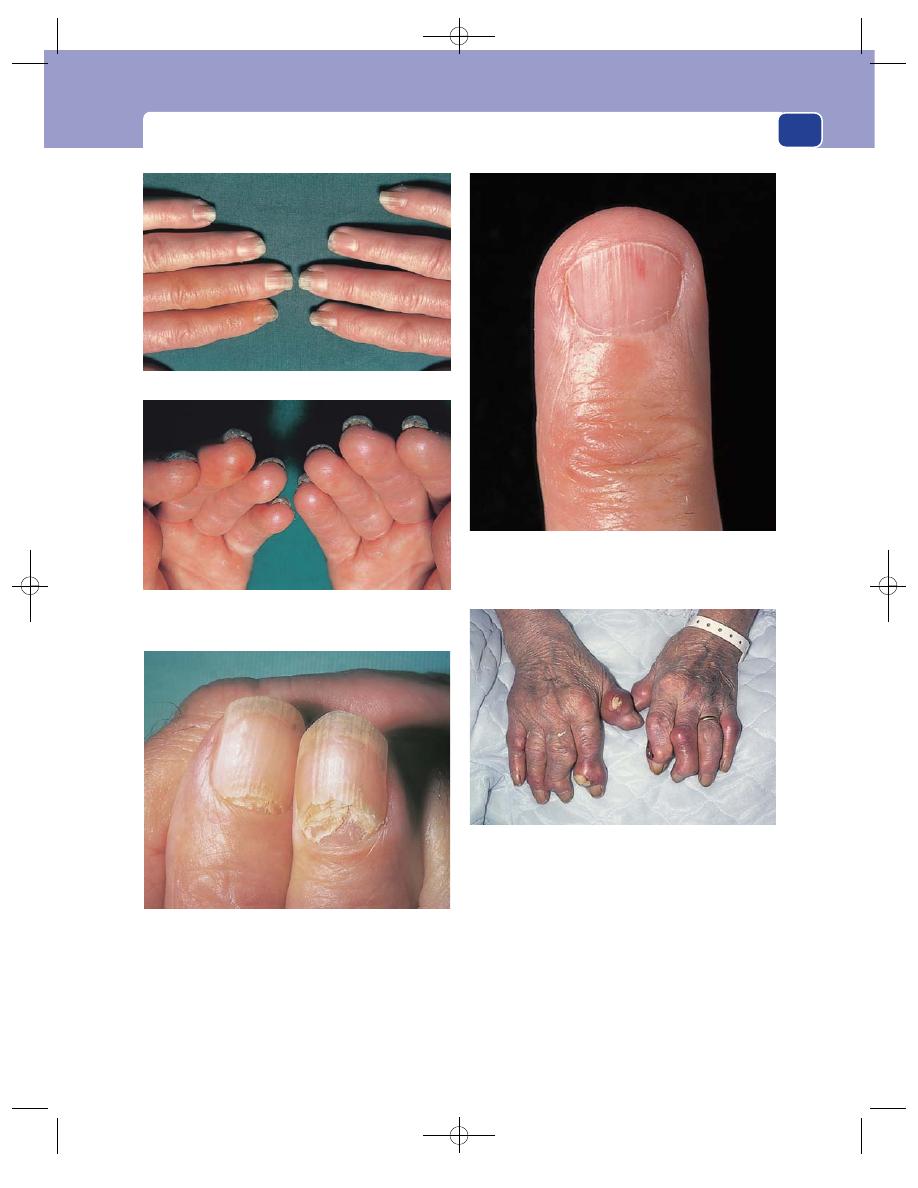
Infections in the hand
163
The patient complains of a painful, tender spot
close to the nail that may have throbbed all night
and kept them awake. They may remember picking
or cutting a piece of cuticle or split skin (hang nail)
a few days before the pain began.
The skin at the base and side of the nail is red,
shiny and bulging and the whole area is exquisitely
tender.
In the early stages the pus collects between the
nail and the overlying skin, but later it spreads deep
to the nail so that movement of the nail is painful
and pus is visible through it.
Paronychia are more common in fingers with a
poor circulation.
FIG 5.27
NAIL CHANGES IN PSORIASIS.
FIG 5.28
The brittle nails of a patient with hypothyroidism
(myxoedema).
FIG 5.29
Telangiectasia under the nail in a patient with
Rendu–Osler–Weber syndrome.
FIG 5.30
The gouty tophi of a patient with long-standing gout.
Pits and furrows in the nails in a patient with psoriasis.
Thickening of the nails in psoriasis.
Chap-05.qxd 4/19/05 13:56PM Page 163
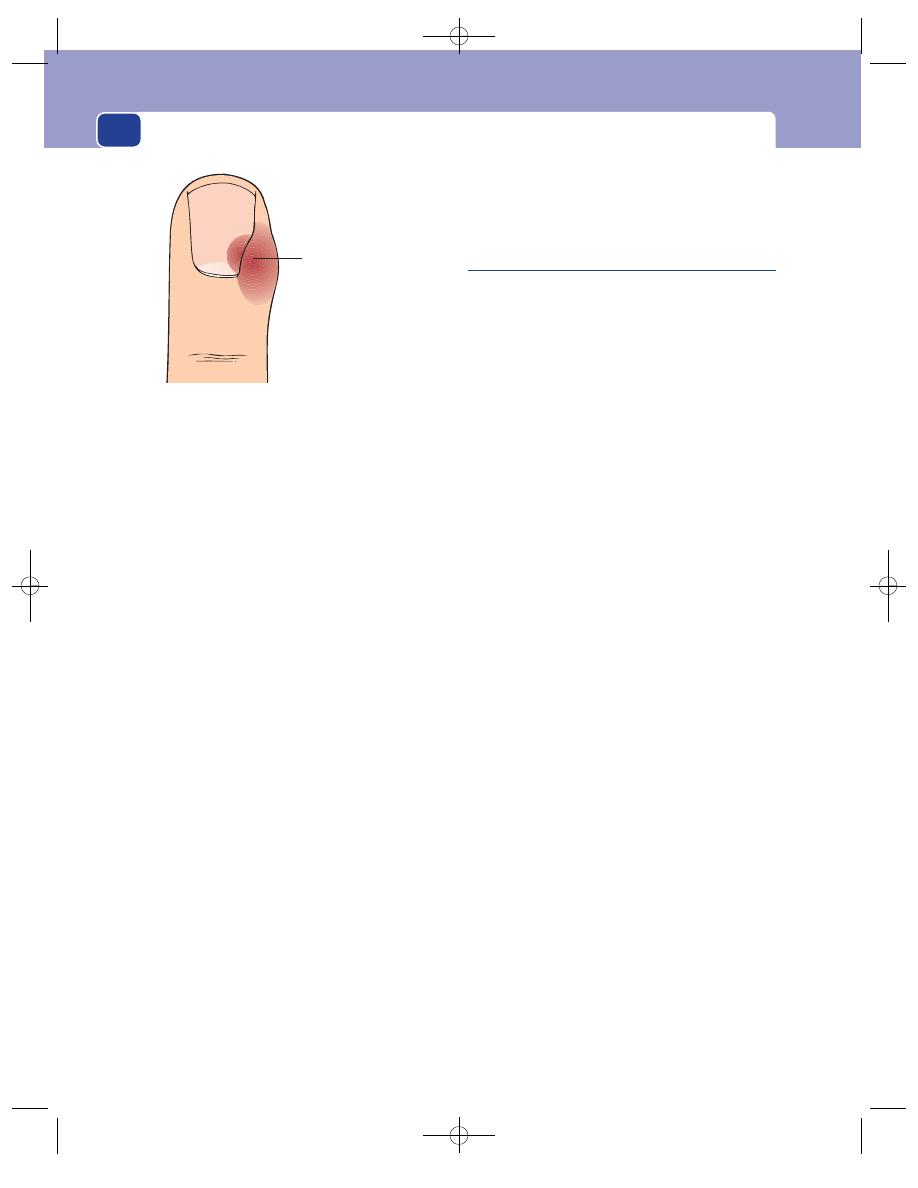
Conditions peculiar to the hands
164
Chronic paronychia
Normally a paronychia subsides after the pus has
drained out, but if there is a foreign body present or
the infecting organism is an unusual bacterium or a
fungus, the wound may fail to heal and continue to
discharge. The patient may then present with a dis-
charging sinus in a discoloured area close to the
nail, with unhealthy bluish granulation tissue pro-
truding from it. Biopsy is an essential part of the
management of such a case to exclude other condi-
tions such as malignant melanoma and squamous
cell carcinoma.
Pulp space infections
These are infections, usually followed by abscess
formation, in the subcutaneous tissue which forms
the pulp of the fingertip.
They present with throbbing pain, swelling and
redness. Sometimes there is a history of a penetrating
injury such as a prick with a needle. On examina-
tion, there is swelling and tenderness and some-
times a pus-filled blister. If the blister is opened, you
will see a hole in the skin leading to the subcuta-
neous abscess.
If neglected or poorly treated, the skin of the
pulp, and the distal phalanx, may necrose.
The only lesion likely to be mistaken for a pulp
space infection is a rapidly growing, vascular, sec-
ondary tumour deposit in the distal phalanx.
Although this will be red, hot and tender, it will
progress much more slowly than an infection and
not suppurate. There may also be clinical evidence
of the primary lesion.
A tender red swollen
pocket of pus beneath
the lateral nail fold
FIG 5.31
A paronychia.
Chap-05.qxd 4/19/05 13:56PM Page 164

Conditions peculiar to the feet
CONGENITAL AND ACQUIRED
DEFORMITIES OF THE FOOT AND
ANKLE
There are many congenital abnormalities of the
foot, such as polydactyly, but the most important
ones clinically and functionally are those related to
club foot.
Club foot
(Talipes)
These deformities of the ankle and foot develop in
utero and are usually present at birth. They are clas-
sified according to the skeletal deformity but are
collectively known as talipes or club foot. However,
these are inappropriate terms when used in such
a broad, non-specific manner. Similar deformities
can also develop in adult life after injury, paralysis
and other musculoskeletal disorders.
There are two main types of deformity.
1. The ankle may be abnormally extended so that
weight bearing is on the toes – an equinus
deformity; or abnormally dorsiflexed so that
weight bearing is on the heel – a calcaneous
deformity.
FIG 6.1
An infant demonstrating polydactyly on both feet.
Normal
Equinus
Calcaneous
Lateral view
Superior view
Normal
Varus
Valgus
FIG 6.3
The deformities of the foot.
FIG 6.2
Severe bilateral clubbed feet. The varus deformity is
so gross that the feet are pulled upwards as well as inwards,
making this a talipes calcaneovarus.
Chap-06.qxd 4/19/05 14:07PM Page 165
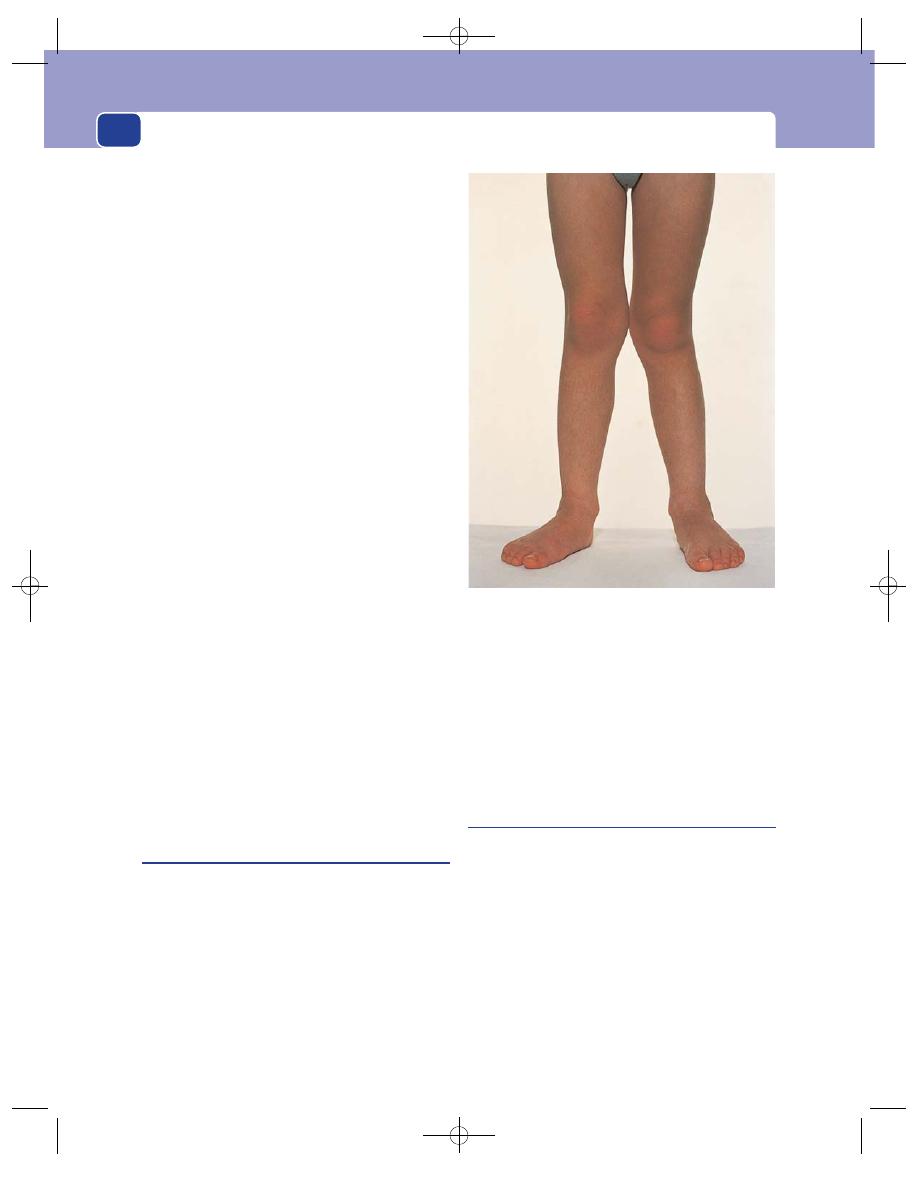
Conditions peculiar to the feet
166
2. The foot may be deviated into a varus or valgus
position, which usually means that there is
also some associated inversion and eversion,
respectively. These terms are defined below.
There are, therefore, eight types of deformity –
four simple and four mixed. Each is prefixed with the
term ‘talipes’ to indicate that the site of the abnormal-
ity is the ankle–foot (talipes):
simple:
■
talipes varus
■
talipes valgus
■
talipes equinus
■
talipes calcaneous
mixed:
■
talipes equinovarus
■
talipes equinovalgus
■
talipes calcaneovarus
■
talipes calcaneovalgus.
Of these eight variations, only two are common:
talipes equinus caused by a short Achilles tendon,
and talipes equinovarus – the true ‘club foot’.
The clinical examination of the foot should follow
the pattern described for bones and joints in Chapter
4: look, feel and move. The obvious deformities of
the true club foot will be the equinus at the ankle,
the varus of the heel with supination of the subtalar
joint, and the adduction of the forefoot. The joint
movements may be limited and the muscles that
effect the joint movements wasted.
The nerves and arteries are usually normal when
the abnormality is a congenital skeletal deformity,
but there may be neurological abnormalities if the
deformity has been acquired since birth.
Flat feet
(Pes planus)
The foot has a longitudinal and a transverse arch. If
the longitudinal arch flattens to the extent that the
medial border of the foot rests on the ground, the
patient has pes planus.
Pes planus is usually associated with a mild val-
gus deformity of the hind foot which results in
pronation of the forefoot and subsequent loss of the
medial arch.
All children are flat-footed when they start walk-
ing, but the arch develops as they grow more active.
However, the infantile pattern may persist into adult
life and the deformity may become fixed by second-
ary changes in the bones.
Contrary to popular opinion, flat feet rarely cause
trouble in adult life as the body weight is spread over
a large flat area.
Hollow or high-arch foot
(Pes cavus)
This is the opposite to flat foot; the longitudinal
arch is accentuated. Pes cavus is secondary to muscle
imbalance with relative weakness of the intrinsic
(small muscles) of the foot. Usually no specific cause
is found, but it is important to examine the peripheral
nerves thoroughly. Peripheral neuropathies, espe-
cially Charcot–Marie–Tooth disease, spina bifida and
poliomyelitis, can all present with pes cavus.
The high arch is clearly visible and easy to diag-
nose. The toes are always ‘clawed’ (hyperextension
of the metatarsophalangeal joints and flexion of
the interphalangeal joints) and the patient cannot
FIG 6.4
Flat feet (pes planus). The medial border of the
foot rests on the ground. There is also mild genu valgum
(knock-knees).
Chap-06.qxd 4/19/05 14:07PM Page 166
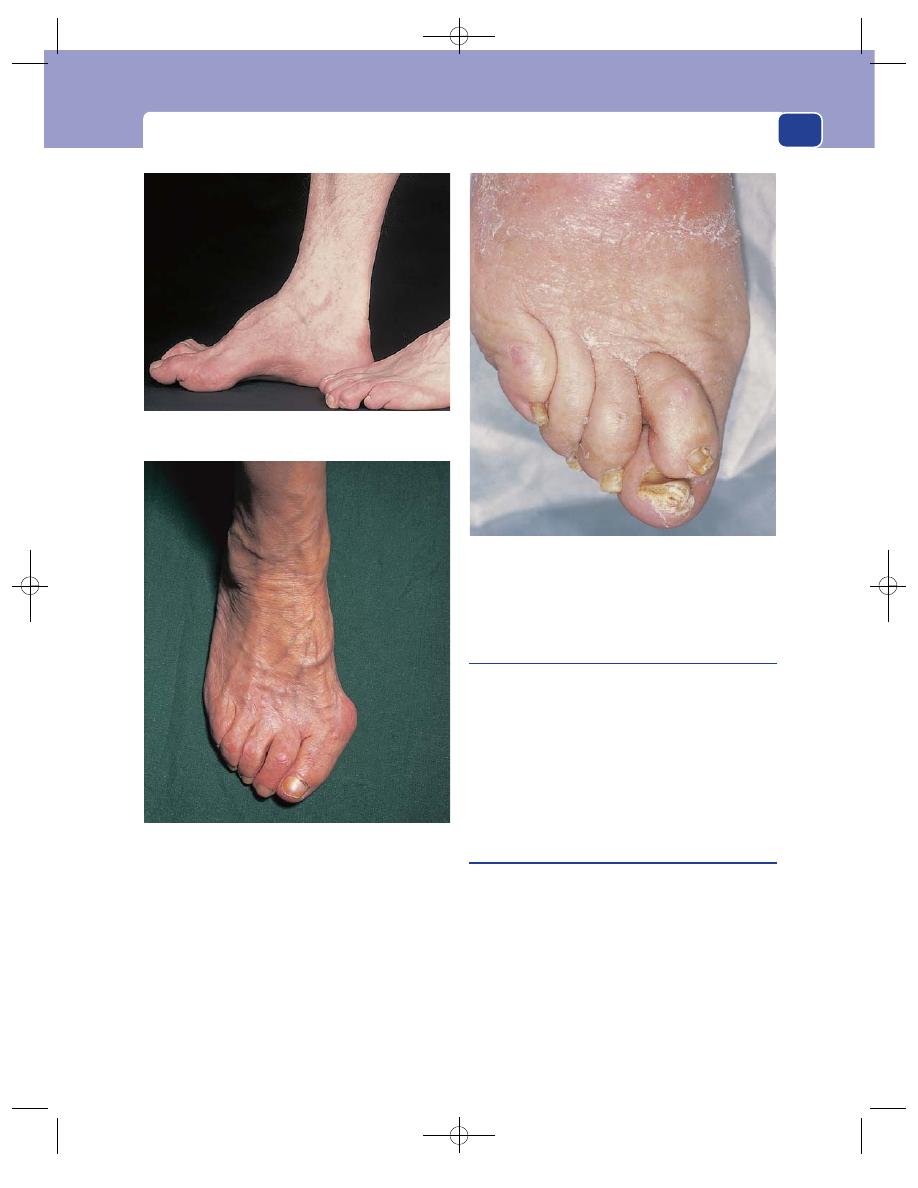
Congenital and acquired deformities of the foot and ankle
167
straighten their toes. Extension of the metatarsopha-
langeal joints and the high arch make the ball of the
foot more prominent and lift the tips of the toes off
the ground so that they do not participate in weight
bearing. Consequently callosities develop on the ball
of the foot beneath the heads of the metatarsal bones,
and on the dorsal aspect of the toes where they rub
against shoes.
Unlike the flat foot, the high-arched foot frequen-
tly causes pain and discomfort.
Hallux valgus
A valgus deformity at the metatarsophalangeal joint
of the great toe is a common abnormality. It can be
congenital or acquired. The acquired variety is more
common in women than men and is often attrib-
uted to poorly fitting footwear.
The valgus deformity is obvious to the patient and
the doctor. In itself it causes little trouble, but two sec-
ondary effects are the source of much discomfort.
Bunion
This is the name given to the bursa which forms
over the medial aspect of the prominent head of the
first metatarsal. It often swells up and sometimes
becomes infected. The patient has difficulty in find-
ing a comfortable pair of shoes because the bunion
is painful when rubbed or touched. The fluctuant
subcutaneous swelling is easy to feel and distinguish
from the underlying bony prominence.
As a result of prolonged abnormal stresses across
the deformed metatarsophalangeal joint, the joint
FIG 6.5
A high-arched foot (pes cavus).
FIG 6.6
Significant hallux valgus. There is a tendency for the
second toe to rise up over the great toe, while the remaining
toes are deviated towards the lateral side of the foot.
FIG 6.7
Marked over-riding of the second toe over the great toe.
Chap-06.qxd 4/19/05 14:08PM Page 167
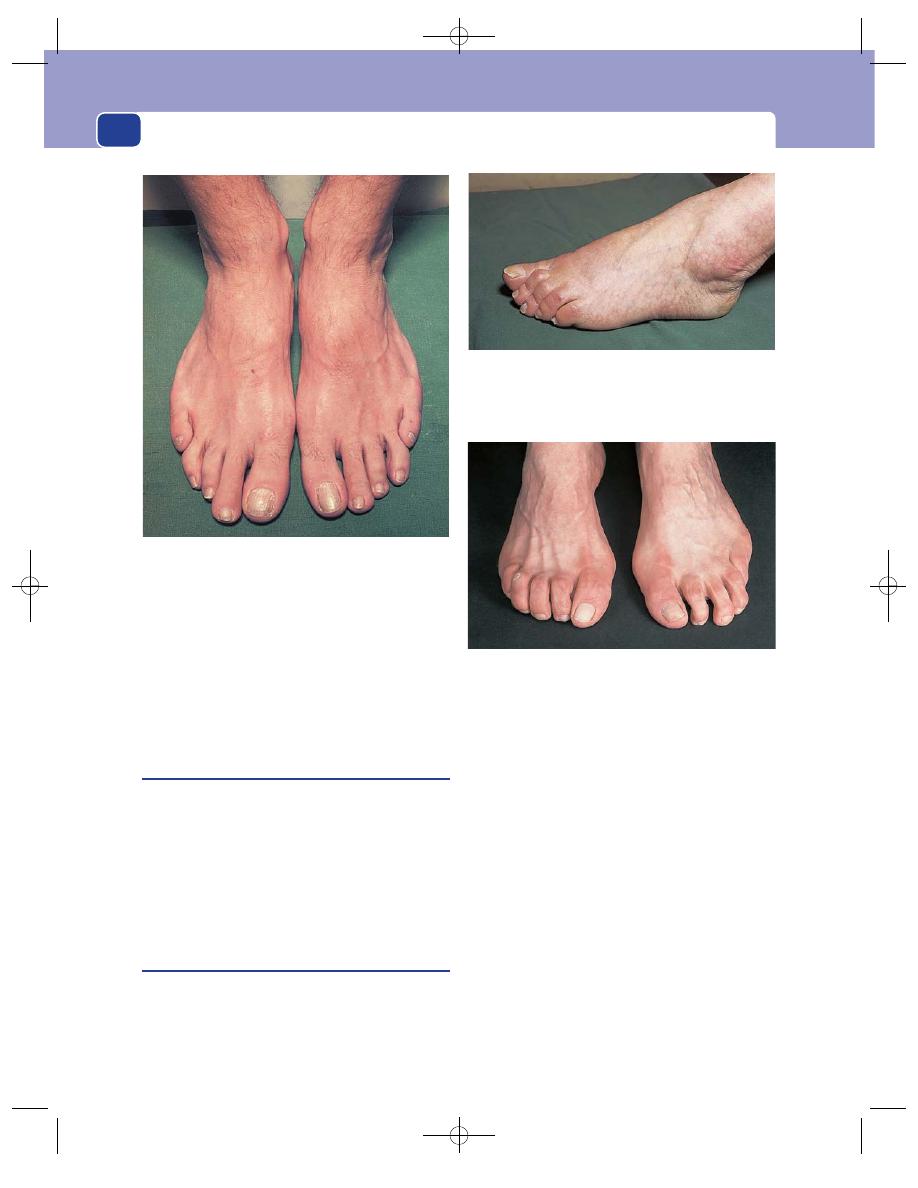
Conditions peculiar to the feet
168
surfaces degenerate and osteoarthritis develops. This
causes pain in the joint during movement and
weight bearing, and hypertrophy of the bone, which
makes the deformity more obvious.
Clinical examination reveals the deformity, the
adventitious bursa (the bunion), pain on moving the
joint, limited movements and, sometimes, crepitus.
Hallux rigidus
The first metatarsophalangeal joint is often afflicted
by osteoarthritis even when it is in normal alignment.
This causes pain and a progressive reduction of joint
movement.
A stiff, painful metatarsophalangeal joint second-
ary to osteoarthritis is known as hallux rigidus.
The pain may become less severe when the joint
becomes fixed by a fibrous ankylosis.
Hammer toe and claw toe
A hammer toe is caused by a fixed flexion of the
proximal interphalangeal joint. The middle phalanx
points downwards so much that the distal interpha-
langeal joint has to hyperextend to enable the pulp
of the toe to rest on the ground. There is also hyper-
extension of the metatarsophalangeal joint.
The cause of hammer toe is not understood,
except that it must ultimately result from an imbal-
ance of muscle tone.
A hammer toe causes pain and discomfort when
the skin over the proximal interphalangeal joint rubs
on the sole or top of the shoe, respectively.
A claw toe is caused by a contracture of its long
flexor tendon. This causes flexion of both interpha-
langeal joints and a secondary extension of the
metatarsophalangeal joint. The tip of the toe rests
upon the ground and may develop a painful callosity.
As the metatarsophalangeal joint extension develops,
the tip of the toe may be lifted off the ground and a
callosity may develop over the proximal interpha-
langeal joint.
FIG 6.8
Digiti quinti varus. This is the opposite deformity to
hallux valgus and affects the fifth toe. It is a common
congenital abnormality and rarely causes symptoms.
FIG 6.9
A row of hammer toes. The tips of some of the toes are
off the ground and there are callosities over the flexed proximal
interphalangeal joints. The distal interphalangeal joints of the
fourth and fifth toes are only slightly hyperextended.
FIG 6.10
Bilateral claw toes. Claw toes are caused by
hyperextension of the metatarsophalangeal joint and the
flexion of both interphalangeal joints. The tip of the toe points
directly downwards and may not reach the ground.
Chap-06.qxd 4/19/05 14:08PM Page 168
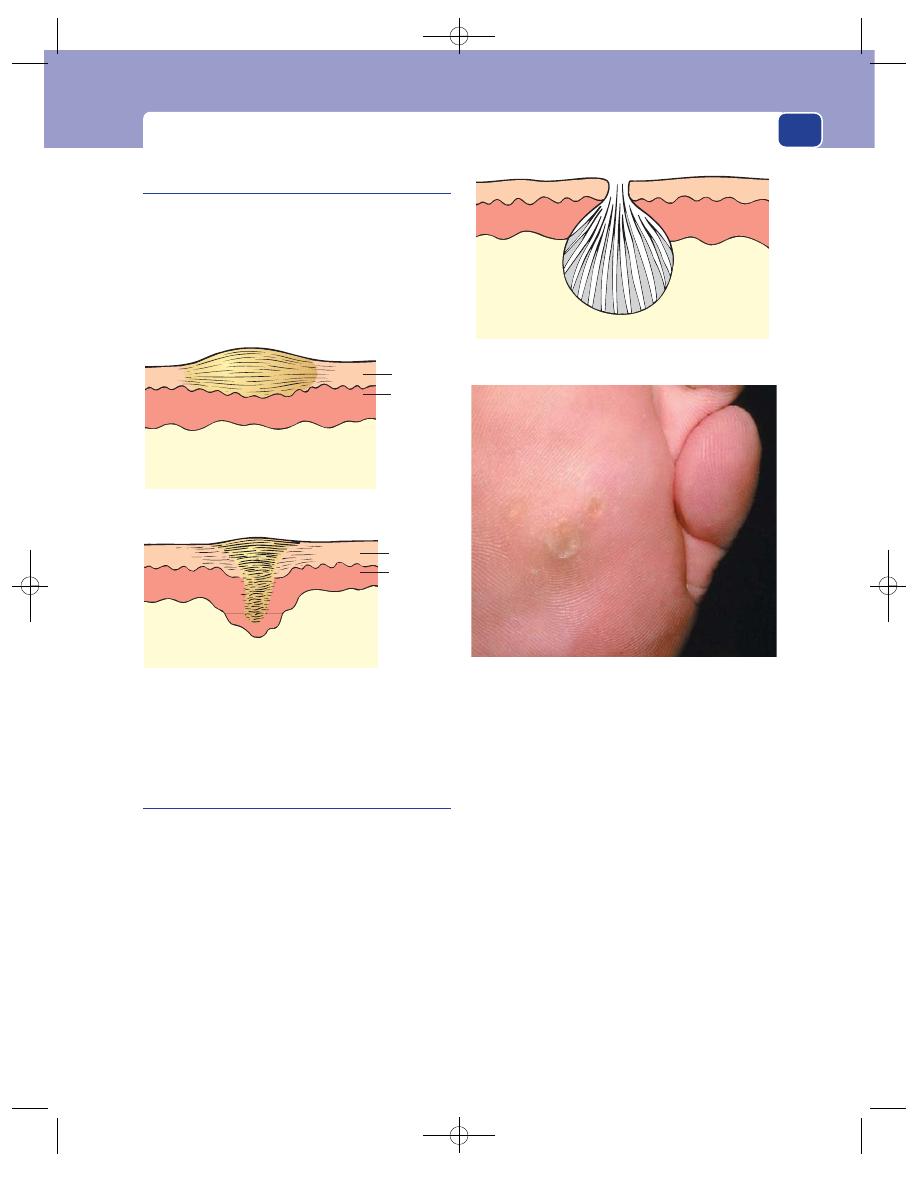
Congenital and acquired deformities of the foot and ankle
169
Plantar wart
(Verruca plantaris)
This is a wart on the sole of the foot. It is caused by
a virus similar to that which causes warts on the hands
but, because it gets pushed into the sole of the foot,
it has different physical characteristics.
History
The patient is usually a child or young adult and the
main complaint is of pain in the sole of the foot dur-
ing walking.
Examination
Site
Plantar warts are usually found on the ball and
the heel of the foot.
Colour
The painful spot is pearly white in colour, with
occasional brown flecks caused by haemorrhage.
Tenderness
Pressure on the wart is very painful, in
contrast to corns and callosities, which are not very
tender when pressed.
Size
The area of tenderness may be a few millime-
tres, or 1 cm, in diameter.
Surface
When the wart is small, it is covered by
apparently normal skin, but as it enlarges the skin
breaks down to reveal a circular pit and the ends of
the grey-white filiform strands which are the sub-
stance of the wart.
Edge
A plantar wart has clearly demarcated edges,
as it is really a pit containing a wart. This gives it a
Callosity
Corn
Epidermis
Dermis
Epidermis
Dermis
FIG 6.11
Callosities and corns are patches of thickened, hard
epidermis. A callosity protrudes above the surface of the skin;
a corn is pushed into the skin.
FIG 6.12
THE PLANTAR WART. (By kind permission of
Professor David Gawkrodger.)
The tips of the embedded fronds of the wart and the
surrounding skin become thick and hard. The patient has
the sensation of standing on hard stone.
A diagrammatic representation of a plantar wart (verruca).
The fine fronds get pushed down into the sole of the foot.
Callosities and corns
Continual pressure and friction on small areas of the
skin of the foot caused by poor-fitting shoes or skeletal
deformities stimulate thickening of the skin. A patch
of thickened hyperkeratotic skin is called a callosity.
If it is pushed into the skin so that it appears to have
a deep central core, it is often called a corn, but there
is no real difference between a corn and a callosity.
Chap-06.qxd 4/19/05 14:08PM Page 169
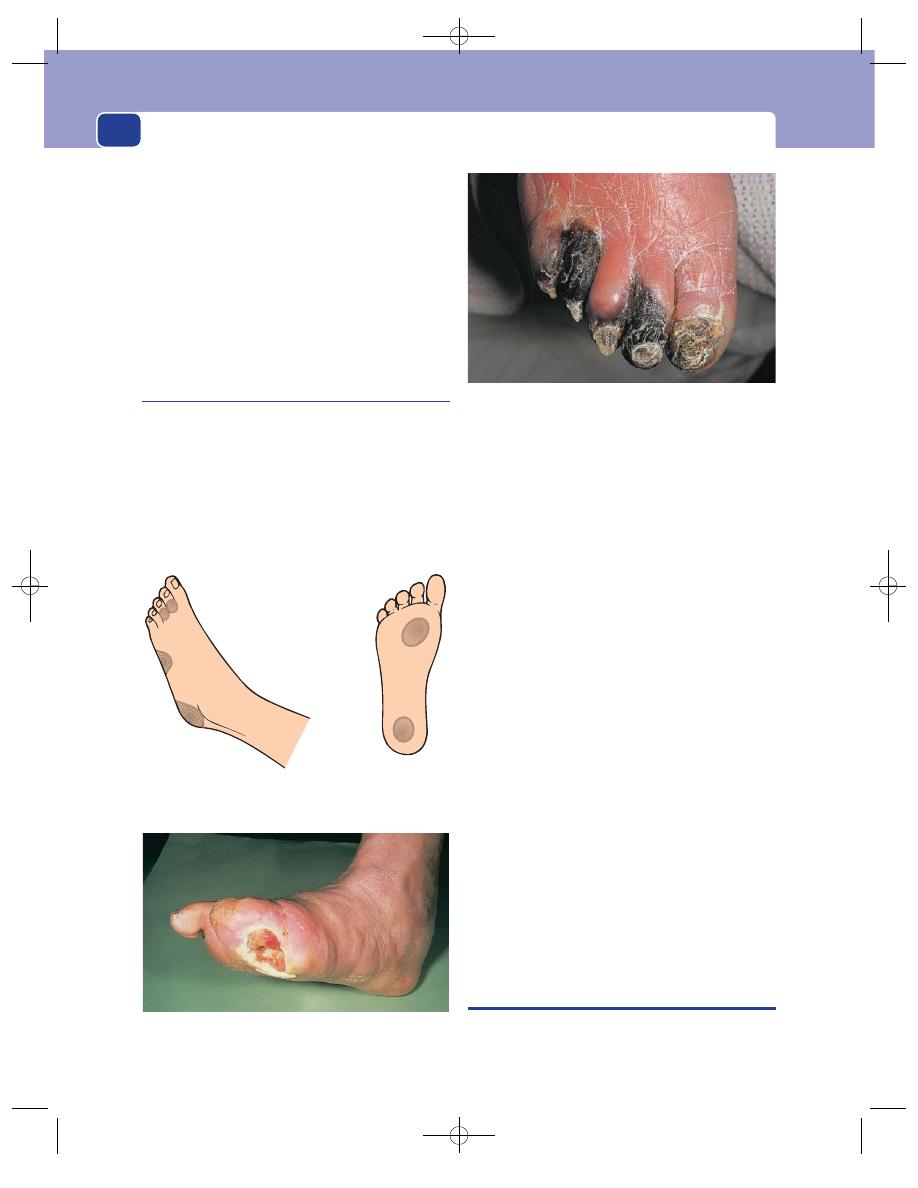
Conditions peculiar to the feet
170
‘punched-out’ appearance, in contrast to the indis-
tinct edge of a corn or callosity.
Consistence
Because the wart is pushed into the hard,
thick skin of the foot it is rarely possible to feel a well-
defined lump. The fine strands in the centre of the
wart are soft.
Multiplicity
There may be more than one plantar wart.
Local structures
The local lymph glands, arteries and
nerves should be normal.
Trophic and ischaemic ulcers
The presentation of ischaemia in the lower limb is
described in Chapter 7, but as ischaemic ulcers are
very common in the feet, they are mentioned here.
Ischaemic ulcers are caused by an inadequate cir-
culation of blood in the skin. Trophic ulcers are ulcers
secondary to an inadequate sensory nervous system.
Both occur in those parts of the feet which are sub-
jected to repeated pressure and trauma, the prime
cause of both types of ulcer.
Prolonged pressure on one part of the foot causes
ischaemic damage of the tissues, and pain. If the cir-
culation is inadequate, the tissues cannot repair them-
selves and an ischaemic ulcer develops. If the nerves
are inadequate, the patient does not feel the pain and
continues to damage the area until it is beyond repair.
These ulcers occur on the heel, the ball of the
foot, over the head of the fifth metatarsal and over
the tips and knuckles of the toes.
When a patient is ambulant, the main pressure
areas are on the sole of the foot (i.e. the heel and ball
of the foot and the tips of the toes). When a patient
is lying in bed, the main pressure areas are on the
back of the heel and lateral side of the foot.
Whenever you examine a patient with an ulcer
on their foot:
1. examine the circulation (pulses, etc.),
2. examine the sensory nerves (light and deep
touch and pain sensation),
3. test the urine for sugar.
Ischaemic ulcers are usually secondary to athero-
sclerosis of the iliac and femoral arteries and can
be accompanied by gangrene of the toes. Trophic
ulcers are usually secondary to conditions such as
diabetic peripheral neuropathy, leprosy and primary
neurological abnormalities.
THE TOE NAILS
The toe nails may show the same changes in response
to local or generalized disease that have been described
Sole of foot
In bed
Ambulant
Side of foot
Side of foot
FIG 6.13
The sites of ischaemic and trophic ulcers.
FIG 6.14
A trophic ulcer on the sole of the foot. This patient
had undergone previous toe amputations for ischaemia.
FIG 6.15
Gangrene of the toes.
Chap-06.qxd 4/19/05 14:08PM Page 170

The toe nails
171
for the finger nails (pages 162–4). Paronychia and
other forms of infection are far less common, but
fungal infection (athlete’s foot) between the toes
and near the nails is very common.
Onychogryphosis
The normal nail is a thin plate which slides along the
nail bed. When the sliding mechanism goes wrong,
the nail begins to thicken and heap up until it
appears to be growing vertically out of the nail bed.
It then curves over the end of the toe and looks like
an animal’s claw. This deformity of the nail is called
onychogryphosis. It can occur in young people after
an injury to the nail bed, but is most common in eld-
erly people, in whom it is presumed to be a failure of
the sliding mechanism caused by old age.
Ingrowing toe nail
This is a common condition in which the side of the
nail, usually the lateral side of the great toe nail,
appears to be growing or digging into the substance
of the toe.
It is a misnomer because, although the nail may
be excessively curved in its transverse plane, it is
growing normally as a thin plate sliding forwards on
the nail bed.
If you remove an ingrowing toe nail, you invari-
ably find that it has an irregular edge, which is dam-
aging the skin. The damage is exacerbated when the
skin at the side of the toe is forced upwards during
walking.
The usual cause of the irregularity of the nail is an
attempt by the patient to cut off the corner, which
has ended with the nail being torn off, leaving a jagged
spike at the edge.
History
Age and sex
Ingrowing toe nails are commonly found
in adolescent and young adult males. The excessive
use of the feet in games such as football, and less strin-
gent hygiene in young boys and men, may contribute
to the sex incidence.
Symptoms
The principal symptom is pain. The toe is
sore and painful when walking. If it gets badly
infected, it throbs at night. There may be a purulent
or serous discharge from beneath the lateral nail fold.
The toe becomes swollen and wide because the skin
at the lateral nail fold becomes prominent, oedema-
tous and soggy.
The normal nail
is slid forwards
as a thin plate
In onychogryphosis
the nail heaps up
and curls over the
end of the toe
FIG 6.16
Onychogryphosis.
A severe degree of onychogryphosis with the nail heaped up
and curling over the side of the toe.
FIG 6.17
ONYCHOGRYPHOSIS.
The nail is thick, growing upwards and beginning to curl
around the end of the toe like a claw.
Chap-06.qxd 4/19/05 14:08PM Page 171
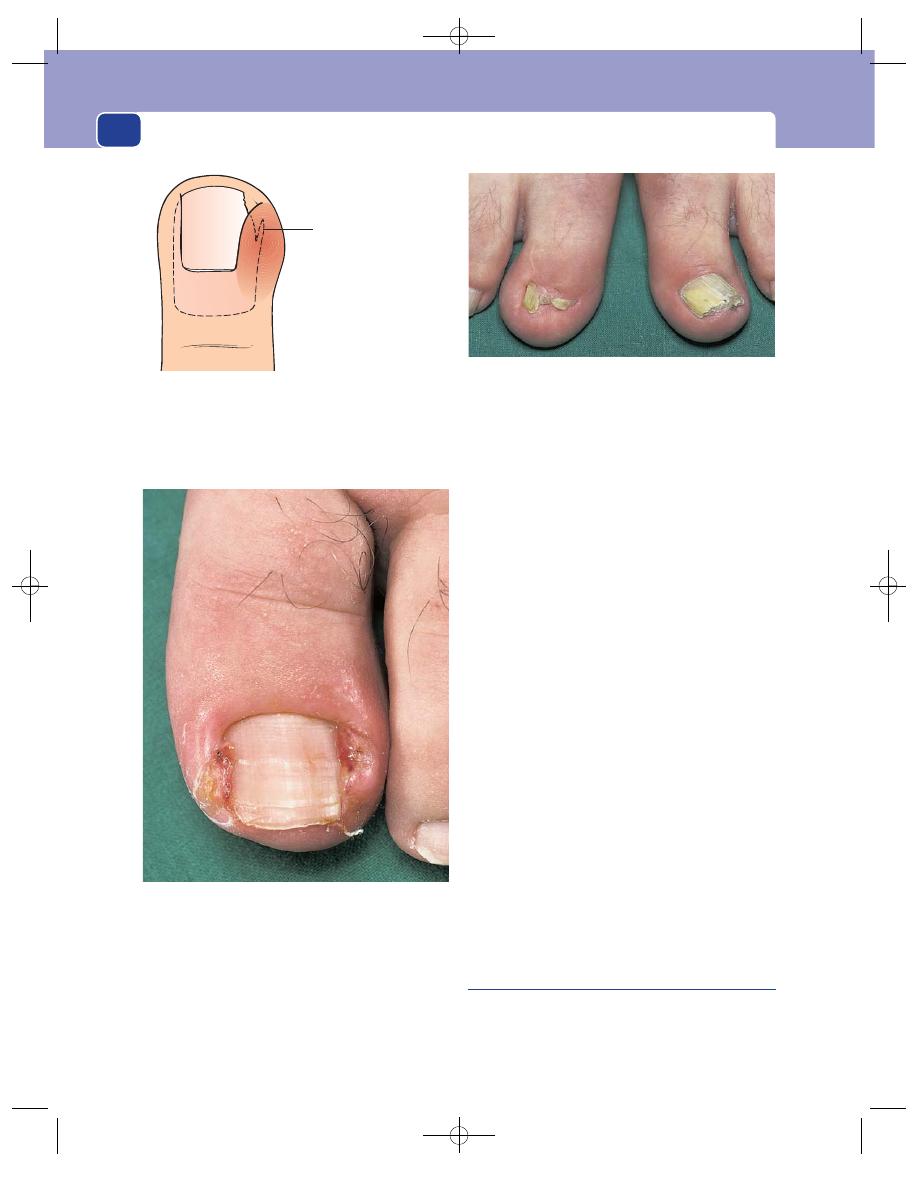
Conditions peculiar to the feet
172
Examination
Site
The symptoms of ingrowing toe nail invariably
occur in the great toe. The lateral side of the nail
(between the great and second toe) is affected more
than the medial side, but both sides and both great
toes are commonly abnormal.
Colour
The skin of the lateral nail fold is reddish-blue.
Red granulation tissue may be visible between the
skin fold and the nail.
Tenderness
The swollen skin and the nail are tender.
When there is extensive infection, the whole toe is
tender and movement of the interphalangeal joint is
painful.
Shape
The increase in the bulk of the lateral nail
fold makes the great toe wide and spatulate.
The nail itself does not look abnormal. If the nail
fold can be pulled away from the nail without caus-
ing too much pain, it may be possible to see the
extent to which the nail is digging into the tissues
and the jagged spikes on the edge of the nail.
Local lymph glands
The inguinal lymph glands may
be enlarged if there has been long-standing infec-
tion, but this is uncommon.
Complications
Inadequate excision of the nail bed
may result in the re-growth of spikes of nail from
the residual corners of the nail bed.
Subungual exostosis
When an exostosis grows on the dorsal surface of
the distal phalanx it soon impinges upon the nail
bed, causing pain and distortion of the nail.
Jagged spike on the
side of the nail digging
into the lateral nail fold
FIG 6.18
The jagged, irregular edge of the nail beneath the
lateral nail fold is the real cause of the pain and infection
known as ‘ingrowing toe nail’. The nail is damaged by
misguided efforts to cut off the corner of the nail.
FIG 6.19
An ingrowing toe nail. Both sides of the nail are
pushing into the soft tissues, which are infected and
producing exuberant granulation tissue.
FIG 6.20
This patient had the right nail bed excised 4 years
before this photograph was taken. It shows two spikes of nail
growing up the corners of the nail bed that were not excised.
The nail of the left foot (on the right in the photograph)
shows the thickening that precedes the appearance of an
onychogryphosis. A fungus infection can cause a similar
thickening.
Chap-06.qxd 4/19/05 14:08PM Page 172
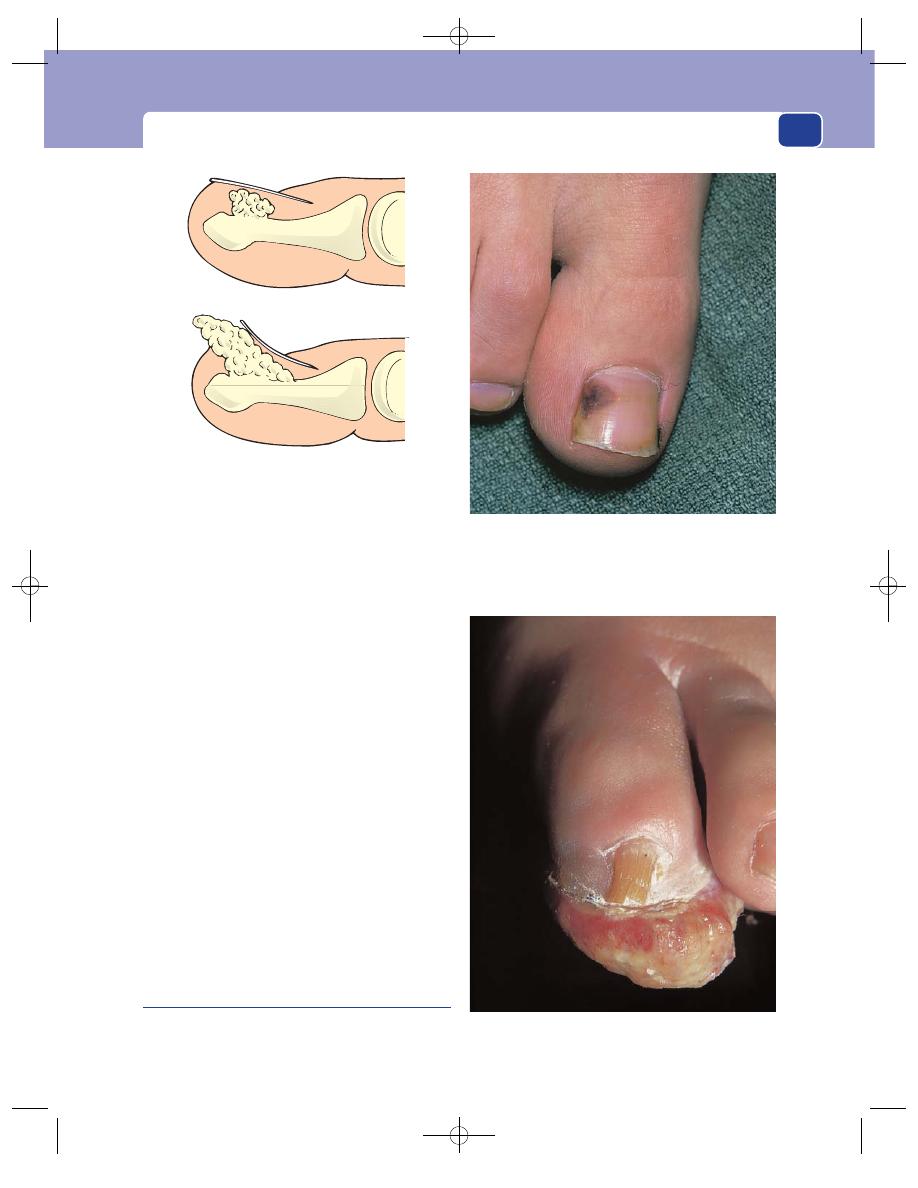
The toe nails
173
History
Age
Subungual exostoses present in all age groups,
but young and middle-aged adults are most often
affected.
Symptoms
The patient complains of pain in the toe,
especially when it is pressed. The toe may swell
slightly and the nail become pushed up and
deformed.
Examination
In the early stages the toe looks normal, but pressure
on the nail causes severe pain. At this stage, when
there are no visible changes in the nail, the diagno-
sis can only be made from a radiograph. As the
exostosis grows, the nail bulges upwards and then a
swelling appears between the toe and the end of the
nail. The skin overlying this swelling (which is the
exostosis) is hard, rough and fissured.
If the exostosis is not removed, it will continue to
grow and form a prominent mass on the dorsal sur-
face of the toe, with the nail tipped up and displaced
posteriorly.
The cracks and fissures on the skin covering the
exostosis may become infected.
Subungual melanoma
The features of malignant melanoma are described
in Chapter 2.
FIG 6.21
A diagrammatic representation of a small and a
large subungual exostosis.
FIG 6.22
A brown patch beneath the great toe nail. Subungual
melanoma or haematoma? The latter will migrate down the
toe with nail growth, but do not wait too long to detect this
sign – remove the nail and biopsy the lesion.
FIG 6.23
An advanced amelanotic malignant melanoma that
initially started subungually.
Chap-06.qxd 4/19/05 14:08PM Page 173
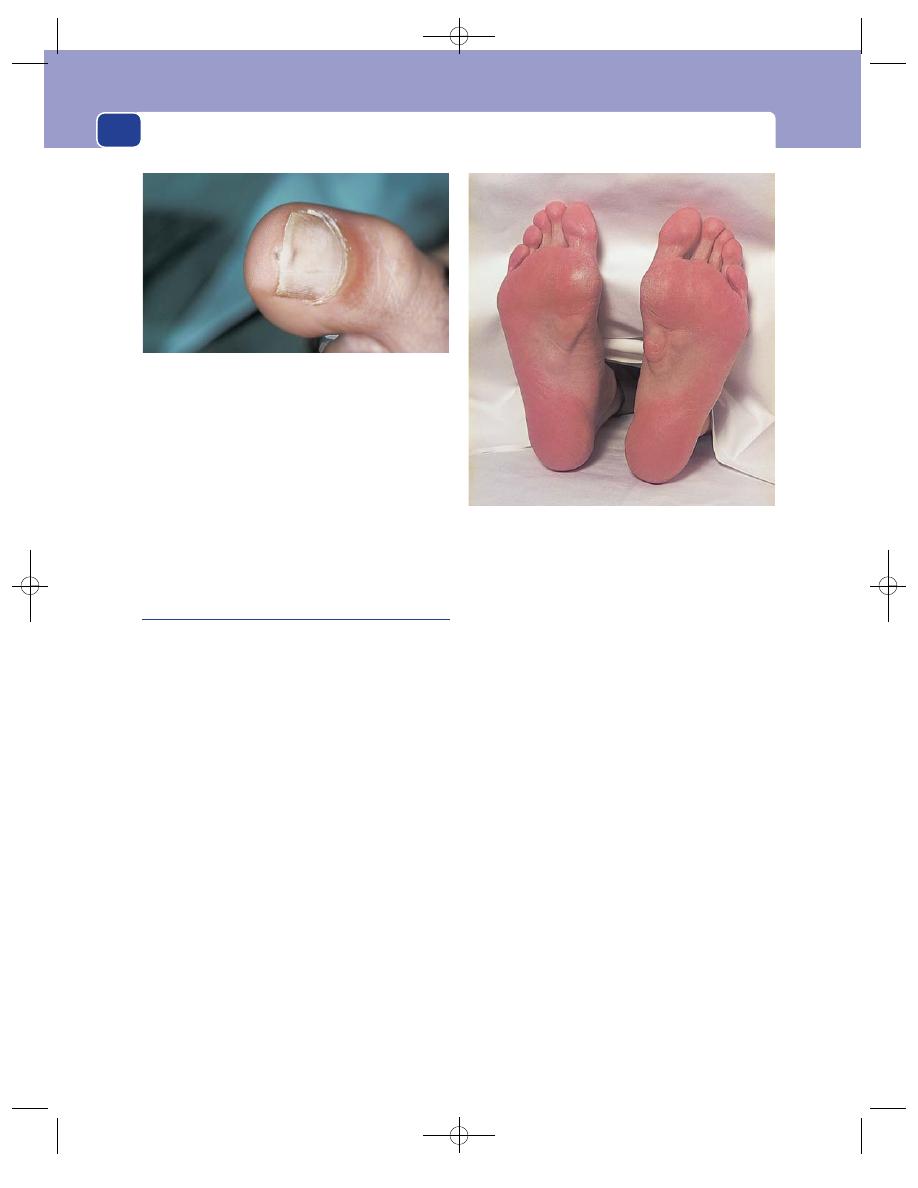
Conditions peculiar to the feet
174
Beware of the brown spot beneath the nail. It
may be a subungual haematoma or a melanoma.
Assume it is the latter unless there is a definite his-
tory of injury and clear evidence that the brown
area is moving down the nail with nail growth. Also
beware of the amelanotic malignant melanoma –
any fungating lesion like this should be treated with
great suspicion. Other more benign conditions can
also occur subungually, such as a glomus tumour.
Dupuytren’s and ischaemic
contractures
Do not forget that both these conditions may
occur in the feet. Their presentation and signs are
similar to those in the hands (see pages 149–52),
except that Dupuytren’s contracture in the foot
usually involves the whole of the plantar fascia and
all of the toes.
FIG 6.24
A subungual glomus tumour.
FIG 6.25
Dupuytren’s contracture of the feet. There are
bilateral thick nodules in the plantar fascia but no flexion
deformities of the toes.
Chap-06.qxd 4/19/05 14:08PM Page 174
The arteries, veins and lymphatics
The examination of the arteries, veins and lymphat-
ics requires special techniques, which are described
before the detailed descriptions of the history and
clinical features of individual conditions.
THE ARTERIES
CLINICAL ASSESSMENT OF THE
ARTERIAL CIRCULATION OF THE
LOWER LIMB
Always examine the patient in a warm room.
Inspection
COLOUR
The first, most notable, feature of an ischaemic limb
is its colour. The skin may be as white as marble or
show varying degrees of redness or blueness, which
become more obvious in the lower parts of the leg
and the toes. Sometimes excessive deoxygenation of
the blood in the skin capillaries gives the foot a
purple-blue cyanosed appearance, but the blue fades
to white within a few seconds when the patient lies
down. A black skin of ethnic origin masks these
subtle colour changes, making the diagnosis of mild
and moderate arterial insufficiency in black and
coloured races more difficult.
In acutely ischaemic legs, blue streaks around
white patches produce a mottled discolouration.
When the cyanotic areas become fixed, the ischaemia
is irreversible.
Gangrene turns the skin a permanent blue/black
colour which is usually first seen in the toes (see
pages 170 and 183).
THE VASCULAR ANGLE
The vascular angle, which is also called Buerger’s
angle, is the angle to which the leg has to be raised
before it becomes white. In a limb with a normal
circulation the toes stay pink, even when the limb is
raised by 90°. In an ischaemic leg, elevation to 15° or
30° for 30–60 seconds may cause pallor. A vascular
angle of less than 20° indicates severe ischaemia. This
test is useful as a comparator. When both limbs are
raised together, the ischaemic foot goes white while
the normal foot remains pink.
CAPILLARY FILLING TIME
After elevating the legs, patients should be asked to
sit up and dangle their feet over the side of the
couch. A normal leg and foot will remain a healthy
pink colour, whereas an ischaemic leg slowly turns
from white (after elevation) to pink and then takes
on a suffused purple-red colour. The latter is caused
by de-oxygenated blood filling the dilated capillaries.
The time taken for the colour of the foot to change
from white to pink is the capillary filling time, and
depends upon the degree of arterial obstruction. In
severe ischaemia it may be as long as 15–30 seconds.
A red-purple foot is indicative of severe ischaemia.
VENOUS FILLING
In a warm room the veins of a normal foot are
dilated and full of blood, even when the patient is
lying horizontally. In an ischaemic foot the veins
collapse and sink below the skin surface to look like
pale-blue gutters. This appearance is called gutter-
ing of the veins.
Chap-07.qxd 4/21/05 12:50AM Page 175
The arteries, veins and lymphatics
176
PRESSURE AREAS
Inspect all areas subjected to pressure or trauma
during walking or bed rest very carefully, because
these are the first sites to show evidence of trophic
changes, ulceration and gangrene. It is important to
look at the bottom, back and lateral surfaces of the
heel, and the ball of the foot. It is also important
to look at the skin over the malleoli. The skin over
the head of the fifth metatarsal must be carefully
inspected, as must the tips of the toes, and between
the toes where pressure of one toe nail against the
side of the adjacent toe can cause ulceration.
Pressure necrosis is manifest by thickening of the
skin, a purple or blue discolouration, blistering, ulcer-
ation or patches of black, dead, gangrenous skin.
Many textbooks state that loss of hair on the skin
of the lower leg, foot and toes is a sign of ischaemia.
This is a very unreliable sign and does not need to
be recorded.
Palpation
TEMPERATURE
The skin temperature can only be assessed reliably if
both lower limbs have been exposed to the same
ambient temperature for a full 5 minutes. Uncover the
limbs and perform some other part of the physical
examination to allow the skin temperature to adjust
to the temperature of the surrounding air. Most cli-
nicians prefer to use the backs of their fingers to
assess temperature. The cool, dry backs of the fin-
gers are ideal temperature sensors.
The whole limb should be assessed to discover
which parts are warm or cold, and the level at which
these changes occur. A blue or even red foot can be
very cold.
CAPILLARY REFILLING
Press on the tip of a nail, or the pulp of a toe or fin-
ger, for 2 seconds and then observe the time taken
for the blanched area to turn pink after you have
stopped pressing. This gives a crude indication of
the rate of blood flow in the capillaries and the pres-
sure within them.
FEEL ALL THE PULSES
Pulses are most easily felt where an artery is superficial
and crosses a bone. In the neck, shoulder and upper
limbs the carotid, subclavian, brachial and both wrist
arteries are close to the skin and easy to palpate.
The femoral pulse in the groin lies halfway
between the symphysis pubis (in the mid-line) and
the anterior superior iliac spine (the mid-inguinal
point). The artery is so superficial it can usually be
felt, even when it is pulseless.
The dorsalis pedis artery runs from a point on
the anterior surface of the ankle joint, mid-way
between the malleoli, towards the cleft between the
first and second metatarsal bones. In 10 per cent of
subjects, the anterior tibial artery is absent and
replaced by a branch of the peroneal artery.
The posterior tibial artery lies one-third of the
way along a line between the tip of the medial
malleolus and the point of the heel, but is easier to
feel 2.5 cm higher up, where it lies just behind the
medial malleolus.
It is often helpful to feel the dorsalis pedis and
posterior tibial pulses in both limbs simultaneously.
Stand at the end of the bed or couch and feel the
dorsalis pedis artery of each foot, simultaneously, by
placing the pulps of all the fingers of each hand along
the line of the artery, with your thumbs beneath the
arch of the foot. From this position, the hands can
be rotated over the foot, until the pulps of your fin-
gers lie in the groove between the Achilles tendon
and the medial malleolus. The pulps of the fingers
Revision panel 7.1
Routine for assessing the arterial
circulation
Inspection
Colour when:
horizontal
elevated (vascular angle)
dependent
Venous filling
Look at the pressure areas and
between the digits
Palpation
Skin temperature
Capillary refilling time
Palpate the pulses
Auscultation
Listen for bruits
Measure the blood pressure
Reactive hyperaemia time
Chap-07.qxd 4/21/05 12:50AM Page 176

Clinical assessment of the arterial circulation of the lower limb
177
can then be pulled up against the back of the tibia,
trapping the posterior tibial pulse against the bone.
The popliteal pulse is difficult to feel because it
does not cross a prominent bone and is not superfi-
cial. There are three ways to feel it and all three may
have to be tried before deciding that the pulse is
present or absent.
1. The most convenient technique for feeling the
popliteal pulse is to extend the patient’s knee
fully and place both hands around the top of the
calf with the thumbs placed on the tibial
tuberosity and the tips of the fingers of each
hand touching behind the knee, over the lower
part of the popliteal fossa. The pulps of all the
fingers are then pulled forwards against the
posterior part of the tibial condyle, trapping the
popliteal artery between them and the posterior
surface of the tibia. The pulsating artery can be
felt in the mid-line (provided the fingers are
held still). If in doubt, count any pulse you feel
against the rate detected by a second examiner
feeling the radial or superficial temporal pulse
to check for synchronization.
2. Flexing the knee to 135° loosens the deep fascia
and may make the lower half of the artery easier
to feel, but moves the vessel further from the
surface and may make palpation of the upper
half of the artery more difficult as it sinks into
the large fat pad between the femoral condyles.
3. It is sometimes worth turning the patient into
the prone position and feeling along the course
of the artery with the fingertips of both hands.
FIG 7.1
PALPATION OF THE PERIPHERAL PULSES.
Palpating the popliteal pulse with the knee extended.
The position of the fingers when feeling the popliteal pulse
with the knee fully extended and the patient supine – method
1 in the text. (The patient has rolled over to one side to reveal
the back of the knee.)
Simultaneous palpation of the posterior tibial pulses.
Simultaneous palpation of the dorsalis pedis pulses.
Chap-07.qxd 4/21/05 12:50AM Page 177
The arteries, veins and lymphatics
178
Remember:
■
when a popliteal pulse is very easy to feel, the
artery may be aneurysmal
■
the popliteal pulse should be palpable if the foot
pulses are easy to feel and there are no adductor
canal or femoral artery bruits.
TEST THE MUSCLES AND NERVES
Severe ischaemia causes loss of muscle and nerve
function, ultimately producing an immobile, numb
limb.
Auscultation
Use your stethoscope to listen along the course of all
the major arteries, especially if the pulses are weak.
It is an important part of the routine examination
to listen to the arteries in the neck, the abdomen, the
groin and the thigh. Always remember to listen
over the adductor canal. Bruits are caused by tur-
bulent flow beyond a stenosis or an irregularity in
the artery wall. Do not press too hard over a super-
ficial artery with the bell of your stethoscope, as
pressure can distort flow and cause a bruit. Bruits
may change in volume and character if there are
changes in blood flow.
Before finishing the physical examination of the
lower limb you should always measure the blood
pressure in both arms to exclude significant subcla-
vian or innominate artery disease.
Pressure measurement with the Doppler flow
detector
Ultrasound can be used to detect blood flow and
produce images of deep structures. The ultrasound
is generated by exciting a piezo-electric crystal to
vibrate at its resonant frequency in response to a small
electric current. In the small hand-held Doppler
ultrasound instruments used in the clinic, the sound
waves are focused into a beam and directed towards
the vessel to be examined by placing the probe over the
surface of the vessel after abolishing any air between
the probe and the skin with a coupling jelly. Moving
red cells alter the frequency of the reflected ultra-
sound according to the Doppler principle. The
chosen vessels, usually the dorsalis pedis, posterior
tibial or peroneal arteries at the ankle, are located by
insonating over their known anatomical course and
listening for regular changes in sound generated by
the pulsatile flow. A sphygmomanometer cuff, pre-
viously placed around the ankle, is then inflated
until the noise created by the flow ceases. The pres-
sure at which this occurs is the systolic blood pres-
sure. This can be measured in all three ankle vessels.
The pressure index is the ratio between the pres-
sure measured by this technique and the pressure in
Femoral
Popliteal
Dorsalis
pedis
Posterior
tibial
(
⫽ bruit)
±
+
_
+
+
_
+
+
R
L
FIG 7.3
Record the pulses and bruits on a simple diagram.
FIG 7.2
The common sites to hear bruits over the arteries of
the lower limbs.
Chap-07.qxd 4/21/05 12:50AM Page 178
Symptoms produced by arterial insufficiency
the brachial artery. It is normally unity or 1.1, i.e.
both foot and brachial artery pressures should be
almost identical. Ratios above 1.0 indicate stiff,
calcified limb vessels (often diabetic arteries), which
cannot be squashed by the external pressure applied
by the sphygmomanometer cuff. Ratios below 1 indi-
cate occlusive disease upstream to the foot vessels.
The Doppler ultrasound flow detector is a very
useful tool because it can detect pulsatile flow when
the pulse pressure is impalpable to the fingers. The
pressure index provides a rough indicator of disease
severity. A more accurate assessment of the severity
of the disease can be obtained by measuring the
pressure before and after exercise.
SYMPTOMS PRODUCED BY ARTERIAL
INSUFFICIENCY
Severe limb pain of sudden onset
This occurs when the arterial blood supply of a limb
is suddenly interrupted, with no time for collaterals
to form. The pain comes from ischaemic muscles and
nerves, which develop irreversible changes within a
few hours.
The symptoms are easy to remember, as each
begins with P:
■
Pain, usually very severe and of sudden onset
■
Paraesthesiae (‘pins and needles’) and
numbness, which develop over a few hours and
eventually progress to
■
Paralysis.
The three principal physical signs also begin with P:
■
Pallor
■
Pulselessness, and the limb feels
■
Perishingly cold to the touch.
The limb looks white and feels cold. These findings
can be compared with the appearance of the other
side if the symptoms are unilateral. The capillary
circulation is poor, with a prolonged refilling time
after digital compression. The veins are empty and
the limb may become blue and develop a blotchy,
blue-white appearance. The femoral pulse may be
present if the arterial occlusion is at the division of
the common femoral artery into the superficial and
profunda femoris arteries or is situated more dis-
tally. Similarly in the upper limb, the subclavian and
axillary pulses may be palpable, whereas the distal
pulses, e.g. brachial, wrist and ankle pulses, are not.
Muscle tenderness, a bad prognostic sign, espe-
cially in the muscles of the anterior and posterior calf
compartments, should be sought by gently pressing
the bellies of these muscles.
A full neurological examination should concen-
trate on power, sensation and reflexes.
The Doppler ultrasound probe should be used to
confirm the absence of pulsatile blood flow in the
peripheral arteries. If any pulsatile flow is detected,
it is likely to be severely diminished in height and
intensity.
If the ischaemia persists, the leg becomes mot-
tled and marbled, the muscles become hard, and the
skin begins to blister and develop gangrene, which
usually starts in the toes before spreading proxi-
mally. The causes of acute limb ischaemia are shown
in the Revision panel 7.3.
General examination
Examine the heart and general circulation with care
to ascertain the cause of the sudden arterial occlu-
sion, such as the following.
An arterial embolus is suspected if the patient is
fibrillating, has had a recent heart attack, or is known
179
Revision panel 7.2
The symptoms and signs of acute ischaemia
Pain, becoming
Painless (numb)
Pallor
Paralysis
Pulseless
Revision panel 7.3
Causes of acute arterial ischaemia
An arterial embolus
Thrombosis on an atheromatous plaque
Thrombosis of an aneurysm (usually popliteal)
Arterial dissection (usually aortic)
Traumatic disruption
External compression, e.g. cervical rib, popliteal
entrapment
Chap-07.qxd 4/21/05 12:50AM Page 179
The arteries, veins and lymphatics
180
to have heart valve disease. Patients may never have
had any symptoms of arterial ischaemia, e.g. inter-
mittent claudication, before the embolus occurs.
An acute arterial thrombosis is suspected if the
patient has already experienced symptoms of chronic
arterial ischaemia, such as intermittent claudication
or even rest pain (see below).
A thrombosed aneurysm is suspected if other
arteries, such as the popliteal artery of the opposite
limb, are found to be dilated.
An aortic dissection is suspected if the patient
presents with severe chest and/or back pain. Other
pulses such as the left subclavian artery may be absent.
A traumatic arterial disruption is suspected
if there is a clear history of injury or vascular
intervention.
Cervical rib is suspected if there is a palpable
supraclavicular swelling. Patients with cevical ribs
may have experienced neurological symptoms in
the arm and hand for many years. (Special investi-
gations are required to diagnose the other causes of
subclavian artery compression.)
Also exclude two of the major non-arterial
causes of an acute limb pain of sudden onset – acute
venous thrombosis (see page 206) and spinal cord
compression or infarction.
Intermittent claudication
Strictly speaking, intermittent claudication means
intermittent limping (Latin claudicatio
⫽ to limp,
a word derived from the disability of the Emperor
Claudius). This term is used to describe a cramp-
like pain in a muscle which appears during exercise.
It is caused by an inadequate blood flow to the mus-
cles. The pain stops the patient using the muscle
and, if the affected muscle is in the leg, causes them
to limp and then stop walking.
History
Age
The majority of patients presenting with inter-
mittent claudication are males, over the age of 50,
with smoking-related atherosclerotic disease of the
lower limb vessels. But claudication can develop in
young adults with Buerger’s disease or after an arterial
embolism or a traumatic occlusion of a major artery.
Sex
Claudication is more common in men than in
women. There may be impotence if the occlusive
disease is at the aortic bifurcation.
Pain
The pain of intermittent claudication is quite
specific and must fulfill three criteria.
1. The patient must experience the pain in a
muscle, usually the calf.
2. The pain should only develop when the muscle
is exercised.
3. The pain must disappear when the exercise stops.
Walking distance
Limitation of walking is the princi-
pal complaint. The patient finds they can only walk a
limited distance before an ache begins in the muscles
of the leg, which then becomes a cramp and then
stops them walking any further. The distance walked
by the time walking has to stop is called the claudica-
tion distance. This should be recorded. If necessary,
the patient should be observed walking to see when
the pain develops. They should also be asked how long
they have to wait until the pain goes away and whether
they can then walk the same distance again. Some
patients complain of an ache or cramp which does not
stop them walking and which fades away if they force
themselves to continue walking. Others find they can
prevent the pain developing by walking slowly.
The severity of the pain and the time taken for it
to begin and cease vary from patient to patient. Any
muscle can be affected. The calf muscles are most
often affected, but a claudication pain can arise in
the thigh, buttock or foot muscles and in the mus-
cles of the upper limb and forearm.
Patients may also describe numbness and
paraesthesiae in the skin of the foot at the time that
the muscle pain begins. This is the result of blood
being shunted from the skin to the muscle.
Pains that begin when at rest or immediately
the patient stands up, and pains that occur in tis-
sues other than muscles and that do not abate with
rest are not claudication pains.
Onset and progression
The pain of claudication usu-
ally begins insidiously. The walking distance gradu-
ally shortens over a few months before becoming
static. In a third or more of affected patients, the
walking distance then increases, with spontaneous
remission of the symptoms as the collateral circula-
tion develops.
It is always important to ask about rest pain in a
patient with claudication, as its presence signifies the
onset of critical limb ischaemia. Patients with rest pain
may have had intermittent claudication in the affected
limb for many years before the onset of rest pain.
Chap-07.qxd 4/21/05 12:50AM Page 180
Symptoms produced by arterial insufficiency
181
Examination of the legs in patients with
claudication
Inspection
The appearance of the limb on inspec-
tion is often remarkably normal, although if the
condition is severe, there may be some blanching
on elevation of the legs.
Palpation
The foot and leg may be cold. The pulse
immediately above the affected group of muscles is
likely to be weak or absent. Thus, if claudication is
experienced in the calf, the popliteal pulse is usually
impalpable but the femoral pulse is likely to be pres-
ent. The femoral pulse is likely to be absent if the
pain is felt in the thigh muscles. Thus the level of the
symptoms and signs often indicates the level of dis-
ease. It is possible to have claudication in the calf
with palpable ankle pulses, but careful examination
often reveals a bruit in the thigh, and if the pulses
are re-examined after exercise, they may no longer
be palpable.
The Doppler pressures are invariably reduced
and fall still further with exercise.
Auscultation
The common sites to find bruits in
association with intermittent claudication are over
the aortic bifurcation, the iliac and common femoral
arteries and the superficial femoral artery at the
adductor hiatus.
Examination of the motor and skeletal
systems
This should be normal.
Differential diagnosis
Other causes of a claudication-like pain include
osteoarthritis of the hip and knee, spinal stenosis,
prolapsed intervertebral disc and venous claudication.
The hip and knee should always be carefully
examined, as should the spine, especially if all the
pulses are palpable (see Chapter 4).
Venous claudication should be considered if the
limb is swollen or if there is lipodermatosclerosis of
the gaiter skin.
Rest pain
Rest pain is a term used to describe the continuous,
unremitting pain caused by severe ischaemia. In
contrast to the pain of intermittent claudication,
which only appears during exercise, this pain is
present at rest throughout the day and the night.
History
Age
Most patients with arterial disease severe
enough to cause rest pain are 60 or more years old,
but Buerger’s disease and trauma can cause rest pain
in young men.
Symptoms
Patients complain of a continuous, severe
aching pain which stops them sleeping. Rest pain is
usually experienced in the most distal part of the
limb, namely the toes and forefoot. If any gangrene
is present, the patient feels the pain at the junction
of living and dead tissues.
Rest pain is often relieved by putting the leg
below the level of the heart, so patients hang their
legs over the side of the bed or prefer to sleep sitting
in a chair. The painful part is very sensitive. Move-
ment or pressure exacerbates the pain. The patient
often sits in bed with the knee bent, holding the foot
still to try and relieve the pain. Strong analgesic
drugs are the only means of providing relief. Rest
pain is unremitting and gets steadily worse.
Systematic questions
It is important to enquire about
symptoms suggestive of pre-existing arterial disease
in the affected limb, such as claudication, and any
symptoms which indicate the presence of athero-
sclerosis elsewhere. Chest pains, a previous myocar-
dial infarction, fainting, weakness, paraesthesiae in
the upper limbs, episodes of blurred vision or stroke
are all important indications of serious vascular dis-
ease elsewhere.
Family history
Arterial disease is often familial, so it is
important to ascertain the cause of death of parents
and siblings and whether they had any symptoms of
vascular disease.
Risk factors
These include cigarette smoking, hyper-
tension, diabetes and hypercholesterolaemia.
Examination
General appearance
Patients with rest pain usually
look drawn and haggard because of continuous pain
and sleepless nights. They are often unwilling to lie
flat on a couch with the leg horizontal for more than
a short period because elevation of the leg exacer-
bates the pain.
An arcus senilis (see Fig. 8.14, page 227) is not
diagnostic of vascular disease but is worth noting.
Chap-07.qxd 4/21/05 12:50AM Page 181
The arteries, veins and lymphatics
182
Xanthelesmata and xanthomata (see Fig. 3.47,
page 103), which are cholesterol deposits around the
eye and in the subcutaneous tissues, are indicative
of hypercholesterolaemia. Pallor suggesting anaemia
or a rubicund appearance suggesting polycythaemia
(rubra vera) is worthwhile noting, as both these
conditions can predispose to claudication and rest
pain.
General examination
The whole cardiovascular system
must be examined with care. The blood pressure
must be measured in both arms and recorded, the
heart examined, the major arteries auscultated and
the abdominal aorta felt in case it is dilated and
aneurysmal (see below).
Inspection
When dependent, a painful ischaemic
foot is a deep reddish-purple colour. The tips of the
toes may be grey or white if they are completely
bloodless. There may be black patches of gangrene
on the toes or the heel.
When horizontal, the foot rapidly becomes pale
or marble white and the veins empty, becoming gut-
tered. Further elevation of the leg increases the pal-
lor. If the foot is not white when horizontal, it will
certainly become so when elevated to 20°.
It is possible to have severely ischaemic toes and
a good circulation in the rest of the foot. In these
circumstances, the description above applies to the
toes only. The pain is unlikely to be an ischaemic
pain if the whole foot is painful but stays pink above
an angle of 20°. The foot may be swollen and blue if
the patient has been sitting with the leg dependent
to ease the pain.
The pressure areas on the heel and the skin
between the toes may be gangrenous, ulcerated or
infected. Ischaemic changes often develop at the site
of the nail beds.
Palpation
The skin temperature from mid-calf
downwards is usually reduced, even when the foot is
dependent and congested. Capillary re-filling is
retarded.
In general, rest pain is caused by a combination
of large and small vessel disease, so it is common to
find that the popliteal and femoral pulses are
absent. Small vessel disease should be suspected if
these pulses are palpable. The likely cause is then
diabetes or Buerger’s disease.
AUSCULTATION
Bruits may be heard over the iliac and femoral arteries.
OTHER SIGNS
There may be muscle wasting caused by disuse, and
if the patient has been sitting holding the ischaemic
foot for many weeks, there may be a fixed flexion
deformity of the knee and hip joint.
Examination of the nervous system is important
because a severe, constant pain in the lower limb
may be caused by a neurological abnormality. The
nervous system may be abnormal in diabetics, but
these patients rarely have very severe rest pain, as
the diabetes destroys the limb’s pain sensation.
Gout may cause severe pain in the foot, with red-
ness and tenderness.
Very occasionally, an abscess or foreign body
needs to be excluded.
Pre-gangrene and gangrene
Pre-gangrene
This term is used by clinicians to describe the changes
which indicate that a tissue’s blood supply is so pre-
carious that it will soon be insufficient to keep the
tissue alive.
The principal symptom of pre-gangrene is rest
pain, which is described in detail above.
The principal signs are pallor of the tissues when
elevated, congestion when dependent, guttering of
the veins, thick and scaling skin, and wasting of the
pulps of the toes or fingers. The limb is cold and has
poor capillary refilling. Ischaemic tissue is tender.
Any further reduction in the blood supply will result
in tissue death, or gangrene (see below). These
symptoms must therefore be treated with the utmost
urgency.
Gangrene
Gangrene is the term used to describe dead tissue.
Dead tissue is brown, dark blue or black, and grad-
ually contracts into a crinkled, withered, hard mass.
These changes can happen if a patch of skin, a toe or
the whole of the lower limb becomes ischaemic. The
nerves in the dead part die and therefore gangrenous
tissues are not painful. The junction between the
living and dead tissue gradually becomes distinct,
provided there is adequate venous drainage and the
Chap-07.qxd 4/21/05 12:50AM Page 182
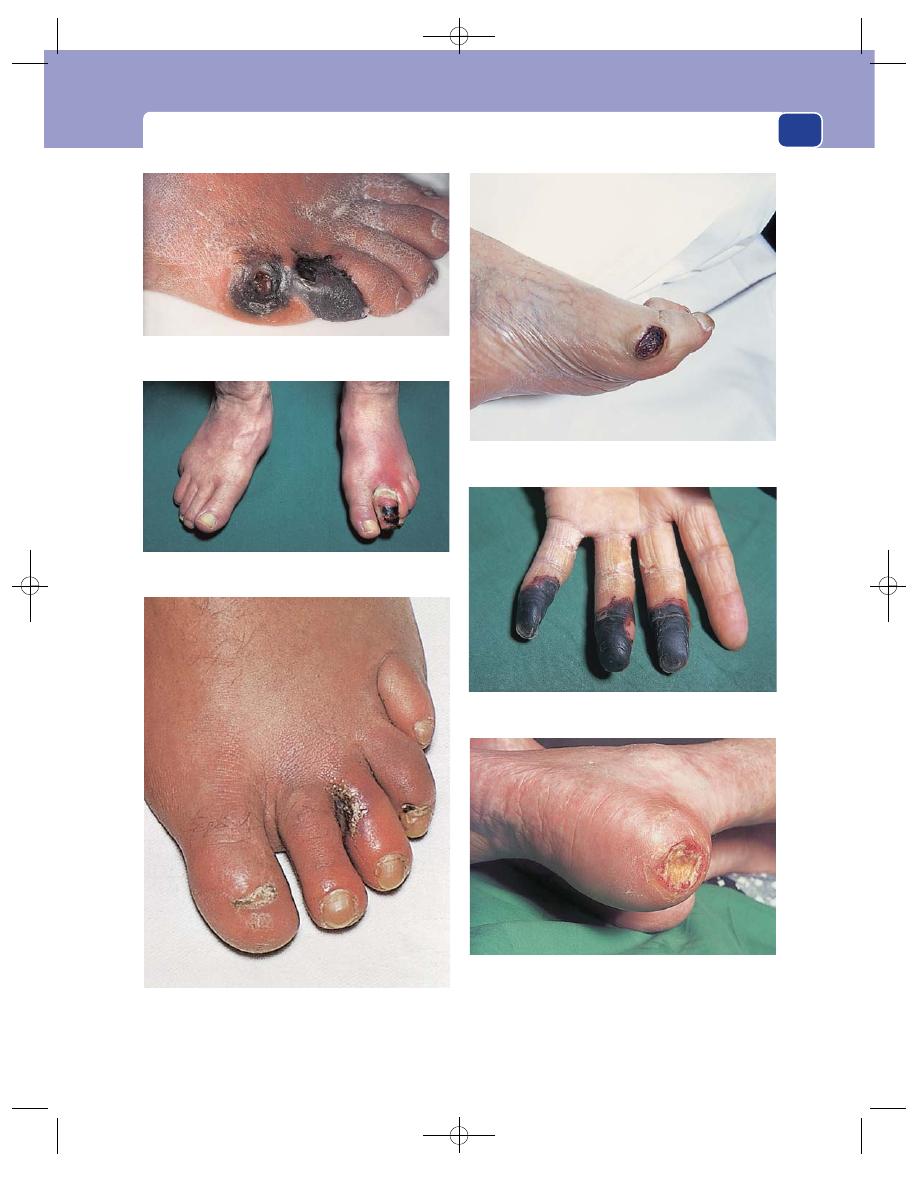
Symptoms produced by arterial insufficiency
183
FIG 7.4
THE COMMON SITES AND CAUSES OF GANGRENE.
Gangrene of the fifth toe caused by atherosclerotic
obstruction of the iliac and femoral arteries.
Pressure necrosis over a bunion caused by a tight bandage
and mild occlusive vascular disease.
Gangrene of the fingertips caused by emboli from a
subclavian aneurysm.
Infected (wet) gangrene caused by a mixture of infection and
mild ischaemia in a diabetic.
Pressure necrosis on the heel following a prolonged period of
unconsciousness (normal circulation).
Infected gangrene between the second and third left toes in a
diabetic.
Chap-07.qxd 4/21/05 12:50AM Page 183
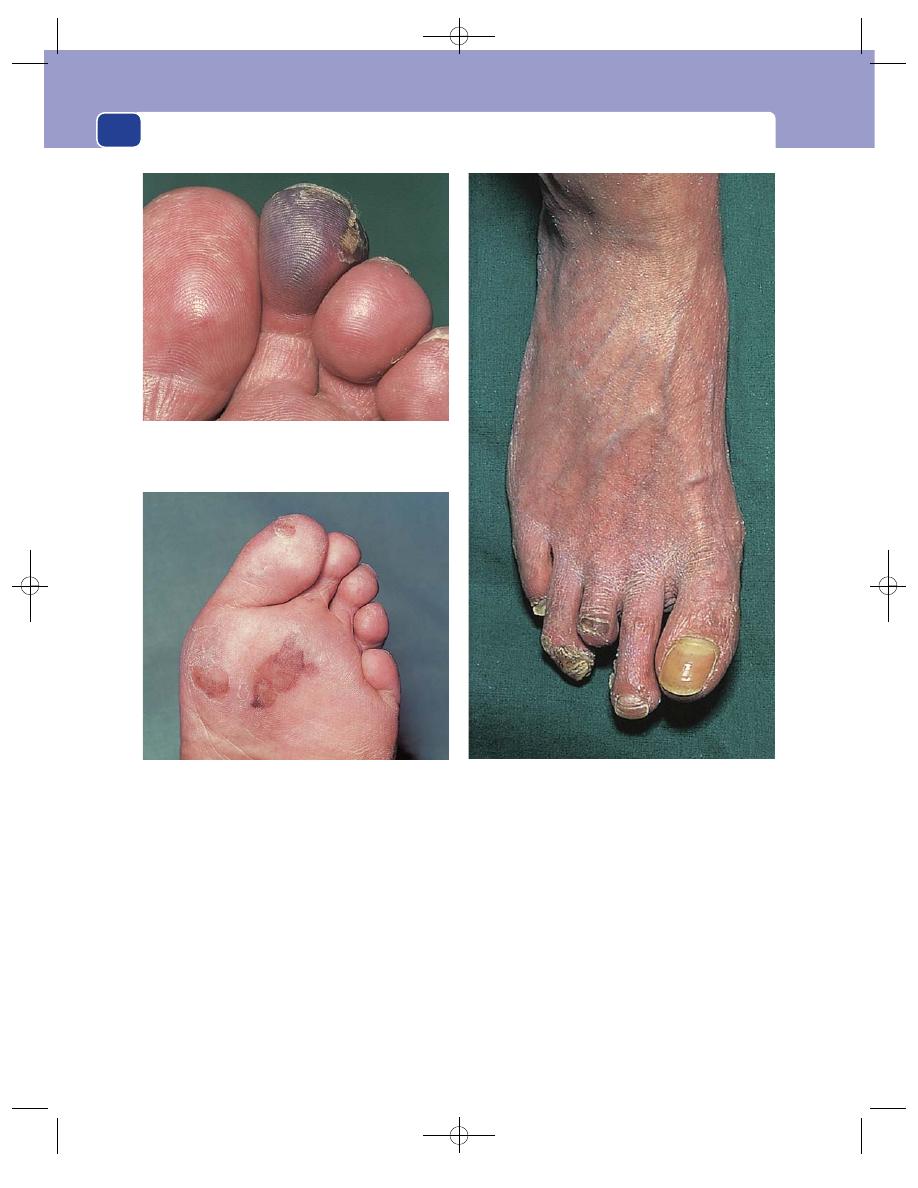
The arteries, veins and lymphatics
184
proximal blood supply remains intact. This junc-
tion is known as the line of demarcation. The dead
tissue may eventually separate and fall off. The liv-
ing tissue on the proximal side of the line of demar-
cation is usually ischaemic and so is often constantly
painful (rest pain) and tender. If the gangrene is the
result of local trauma and the surrounding tissues
are normal, they are not usually painful.
Gangrene usually develops in the extremities of
the limbs – the tips of toes and fingers, and in areas
of skin subjected to pressure. The dead tissue does not
become shrivelled if its venous drainage is impaired
or if it becomes infected. In these circumstances the
gangrene becomes soft and boggy and the line of
demarcation often becomes purulent.
A hard, shrunken, non-infected patch of gangrene
with a clear line of demarcation is called dry gan-
grene. A soft, swollen, infected patch of gangrene
without a clear margin is called wet gangrene.
However, it is better to use the terms infected and
non-infected rather than wet and dry. This differ-
ence is important because sometimes, as in diabe-
tics, the gangrene is actually secondary to the
infection not the ischaemia.
FIG 7.4
continued
A blue ischaemic toe caused by emboli from a femoral artery
stenosis.
Multiple ischaemic areas on the sole of the foot caused by
emboli from the left side of the heart.
Long-standing ischaemia of the toes with gangrene of the third
toe that has proceeded to auto-amputation.
Chap-07.qxd 4/21/05 12:50AM Page 184
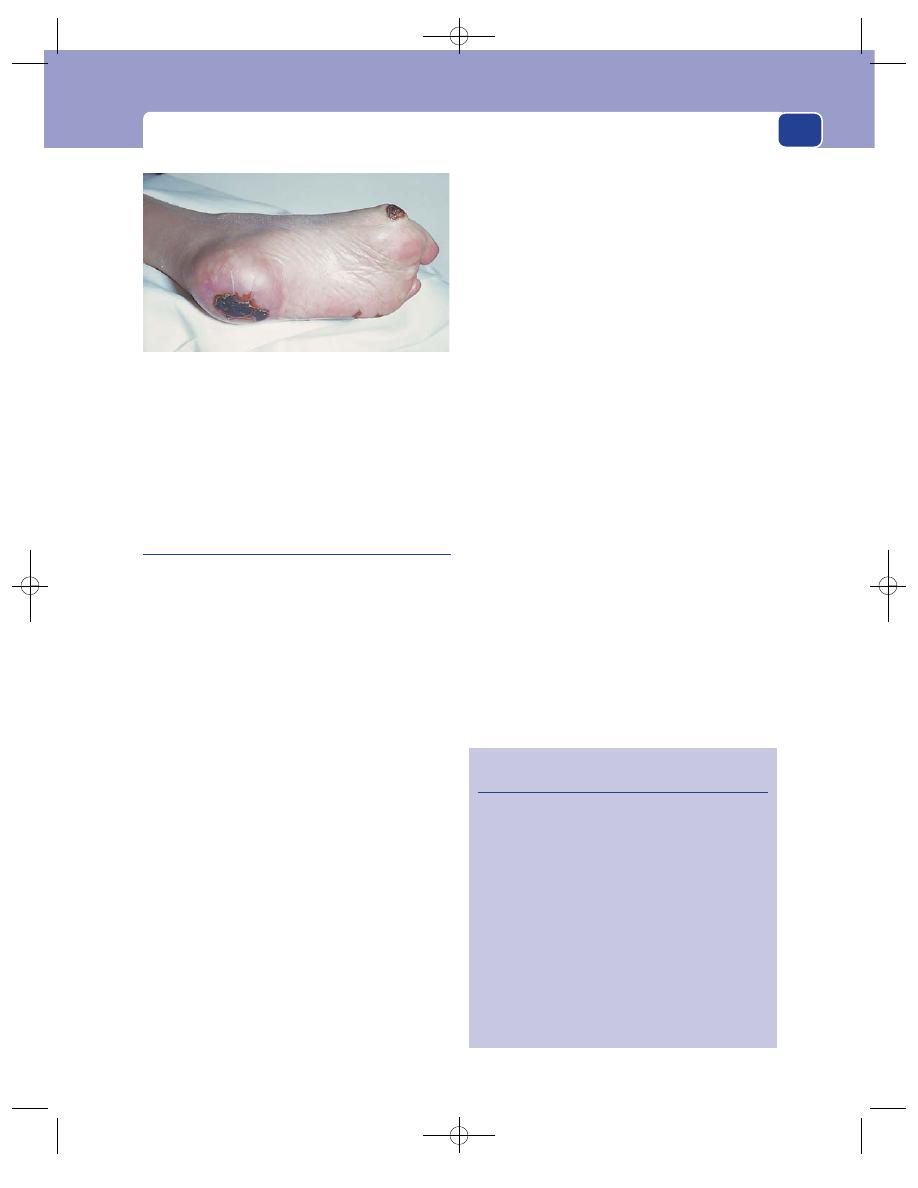
Symptoms produced by arterial insufficiency
185
Diabetic gangrene is often associated with gas in
the tissues (tissue-crepitus) and a foul smell.
Venous gangrene, which may complicate a mas-
sive deep vein thrombosis and phlegmasia caerulia
dolens, usually affects all of the toes.
Ischaemic ulceration
An ischaemic ulcer is the aftermath of gangrene. By
definition, it is caused by an inadequate blood supply.
History
Ischaemic ulcers are common in the elderly, who
often also have symptoms of coronary or cerebral
vascular disease. Patients sometimes remember a
minor precipitating injury.
Symptoms
Ischaemic ulcers, except those associated
with a neurological abnormality, are very painful.
They cause rest pain.
They do not bleed, but discharge a thin serous
exudates, which can become purulent. They are
usually indolent and often get slowly deeper and
larger. Ischaemic ulcers may occasionally penetrate
into joints, making movements very painful. The
causes of ischaemic ulcers are:
■
large artery obliteration: atherosclerosis,
embolism,
■
small artery obliteration: Buerger’s disease,
athero-embolism, diabetes, scleroderma and
physical agents such as prolonged local pressure,
radiation, trauma and electrical burns.
Systematic questions and past history
The patient may
give a history of prior claudication or symptoms of
generalized vascular disease such as chest pain.
Examination
Site
Ischaemic ulcers are found at the tips of the
toes or fingers and over the pressure points.
Size
Ischaemic ulcers vary in size from small, deep
lesions, a few millimetres across, to large, flat ulcers
10 cm or more wide on the lower leg.
Shape
The ulcers are most often elliptical.
Tenderness
The ulcer and the surrounding tissues
are often very tender. Removing a dressing can cause
exacerbation of the pain that lasts for several hours.
Temperature
The surrounding tissues are usually
cold because they are ischaemic. Warm, healthy tis-
sue suggests another cause for the ulceration.
Edge
The edge of an ischaemic ulcer is either
punched out, if there is no attempt at healing by the
surrounding tissues, or sloping, if the ulcer is begin-
ning to heal (see Chapter 1, page 33). The skin at the
edge of the ulcer is usually a blue-grey colour. There
is no lipodermatosclerosis in the surrounding skin
unless venous disease coexists (see page 204).
Base
The base of the ulcer usually contains grey-
yellow slough covering flat, pale, granulation tissue.
Depth
Ischaemic ulcers are often very deep. They
may penetrate down to and through deep fascia,
tendon, bone and even an underlying joint.
Discharge
This may be clear fluid, serum or pus.
Relations
The base may be stuck to, or be part of, any
underlying structure. It is quite common to see bare
FIG 7.5
An ischaemic foot with patches of gangrene on all the
pressure areas: the heel, the head of the first metatarsal and
the base of the fifth metatarsal.
Revision panel 7.4
The causes of ischaemic ulceration
Large-artery obliteration
Atherosclerosis
Embolism
Small-artery obliteration
Scleroderma
Buerger’s disease
Embolism
Diabetes
Physical agents
Pressure necrosis
Radiation
Trauma
Electric burns
Chap-07.qxd 4/21/05 12:50AM Page 185
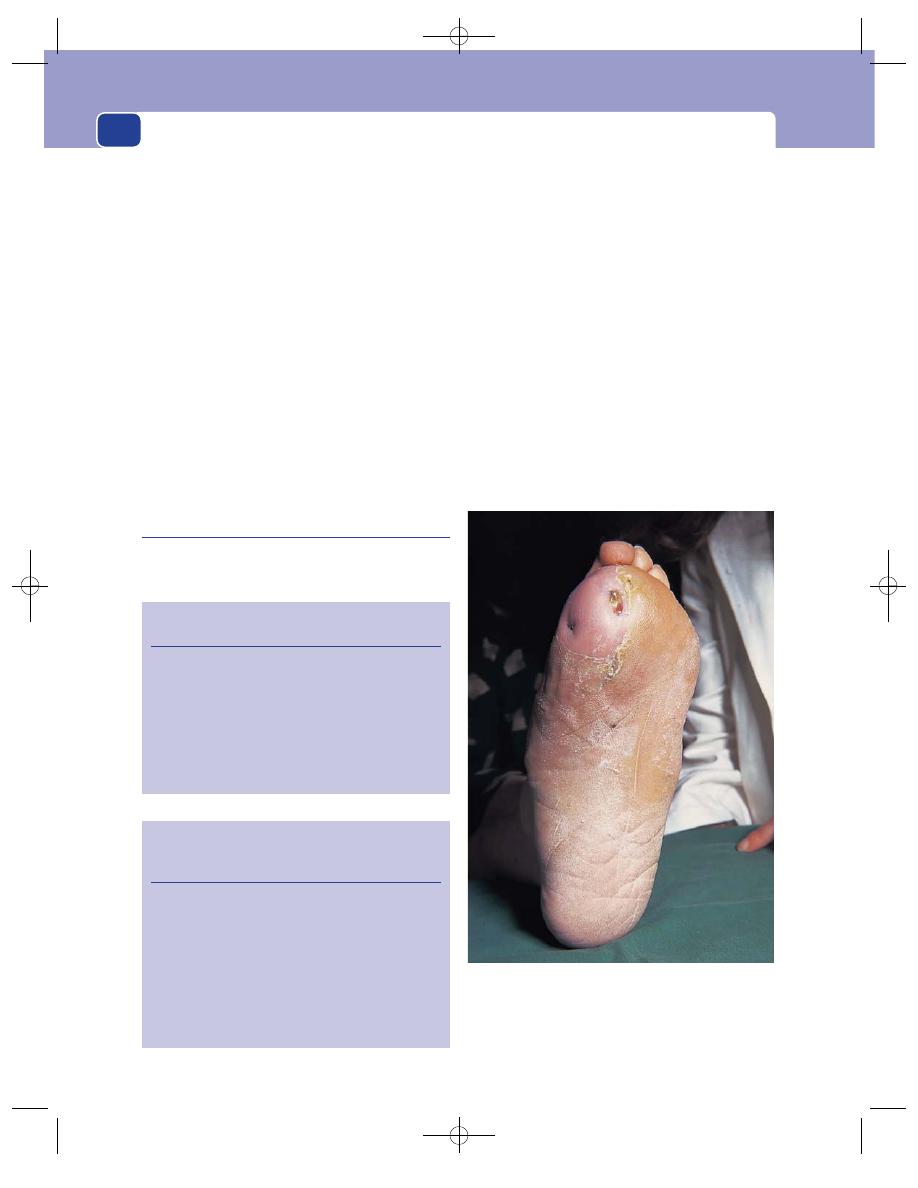
The arteries, veins and lymphatics
186
bone, ligaments and tendons exposed in the base of
an ischaemic ulcer (see above).
Lymph drainage
Infection in an ischaemic ulcer usu-
ally remains confined to the ulcer, so that the local
lymph glands are not normally enlarged.
State of the local tissues
Surrounding tissues may
show signs of ischaemia – pallor, coldness and atrophy.
Distal pulses
These are invariably absent.
Doppler pressures
The Doppler pressure index is
invariably reduced.
Neurological examination
If the ulcer is caused by a
neuropathy (see below), there may be a loss of
superficial and deep sensation, weakness of move-
ment and a loss of reflexes.
General examination
There may be evidence of vascular
disease elsewhere. The urine should be tested for sugar.
Neuropathic ulceration
Tissue ischaemia is usually painful. Pain is the
mechanism by which the body appreciates that any
part of the skin is becoming deprived of blood. The
feet and buttocks become painful after prolonged
standing or sitting, encouraging movement to remove
the pressure from the painful part. When pain sen-
sation is lost this warning is lost, and any compres-
sed tissue may become permanently damaged.
Neuropathic ulcers are therefore only indirectly
caused by local ischaemia. The main cause is lack
of sensation in the tissues, allowing unrecognized
trauma to occur.
Neuropathic ulcers are deep, penetrating ulcers
which occur over pressure points, but the surround-
ing tissues are healthy and may have a good circula-
tion. The diagnostic features are:
■
the ulcers are painless,
■
the surrounding tissues are unable to appreciate
pain,
FIG 7.6
Trophic ulcers on the sole of the foot in a patient with
diabetic peripheral neuritis. The circulation was good and all
the pulses were present, but there was a total loss of pain
sensation. The great toe had been amputated 2 years earlier
for similar ulceration.
Revision panel 7.5
The causes of chronic ulceration
Infection
Repeated trauma
Ischaemia
Oedema
Denervation
Localized destructive disease (tuberculosis,
carcinoma)
Revision panel 7.6
The causes of neuropathic ulceration (ulcers
secondary to a loss of sensation)
Peripheral nerve lesions
Diabetes
Nerve injuries
Leprosy
Spinal cord lesions
Spina bifida
Tabes dorsalis
Syringomyelia
Chap-07.qxd 4/21/05 12:50AM Page 186
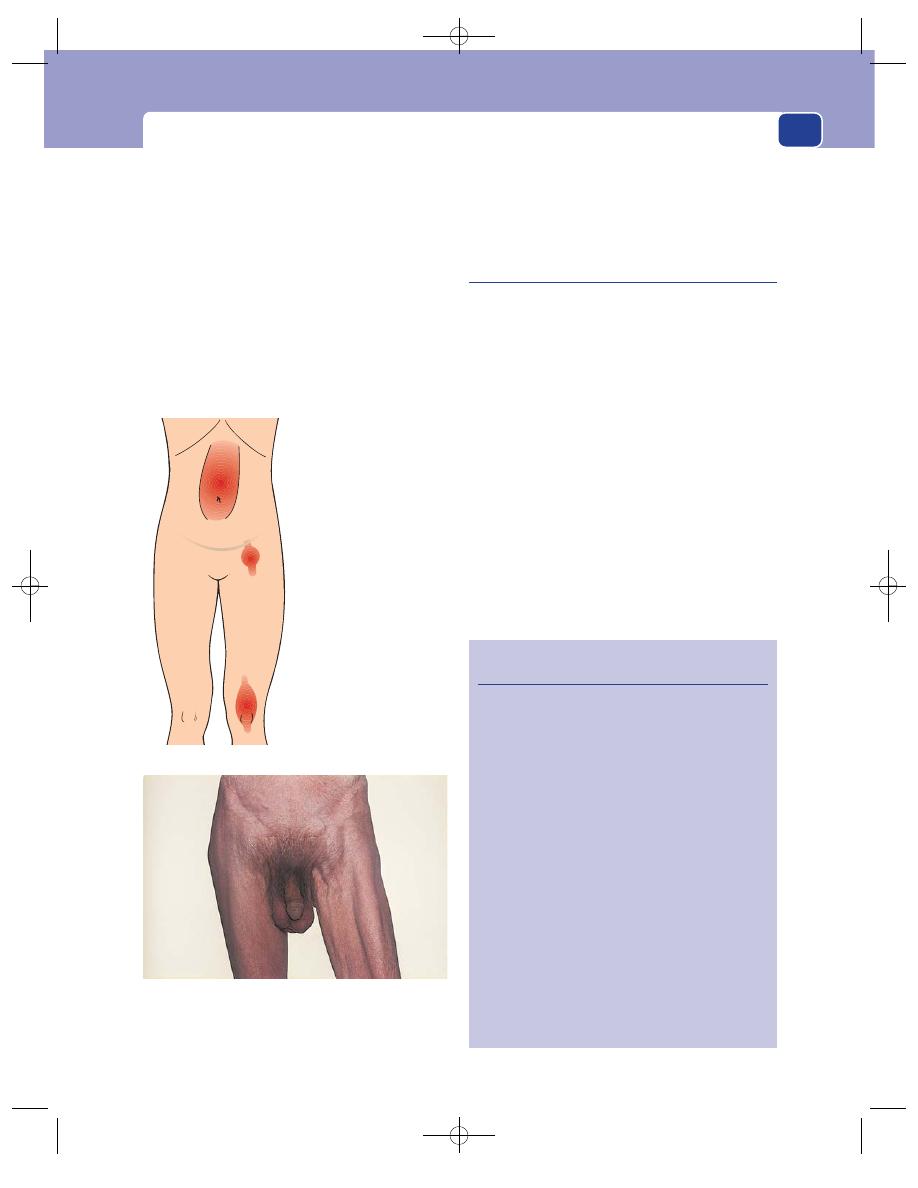
Symptoms produced by arterial insufficiency
187
■
the surrounding tissues may have a normal
blood supply.
These ulcers can easily be mistaken for ischaemic
ulcers, which is why a neurological examination is
always important. The causes of neuropathic ulcer-
ation are:
■
peripheral nerve lesions: diabetes, nerve
injuries, leprosy,
■
spinal cord lesions: spina bifida, tabes dorsalis
and syringomyelia.
However, all these conditions may occur in
patients with vascular disease and so true ischaemic
and neuropathic ulcers may occur together and the
combined effect of both diseases may be synergistic.
Careful examination of the arterial and neurolog-
ical systems is required to identify the major cause.
Pulsatile swellings (aneurysms)
An aneurysm is a localized dilatation of an artery.
The majority of aneurysms are associated with ath-
erosclerosis, but some are caused by a primary weak-
ness in the connective tissues of the arterial wall.
The causes of aneurysms are shown in the
Revision panel 7.7.
In a true aneurysm all the layers of the arterial
wall are involved (intima, media and adventitia). In
a false aneurysm the arterial wall is breached and
the wall of the aneurysm consists of blood clot and
compressed surrounding normal tissues.
Although an aneurysm can develop in any artery,
most occur in the abdominal aorta and the femoral
and popliteal arteries.
Berry aneurysms are believed to arise in a con-
genitally weak area of the circle of Willis. They are
associated with hypertension and are responsible
for many subarachnoid haemorrhages in middle
Revision panel 7.7
The causes of aneurysms
Congenital
A localized weakness
Berry aneurysm
Marfan’s syndrome
Ehlers–Danlos syndrome
Arterial dilatation associated with a
congenital arterio-venous fistula
Acquired aneurysm
Trauma
Direct injury
Infection
Bacterial arteritis (mycotic)
Syphilis
Acquired immunodeficiency syndrome
Degeneration
Atherosclerosis
False aneurysms
Trauma
Post-arterial surgery
Abdominal aorta
Common femoral artery
Popliteal artery
An aneurysm of the left common femoral artery compressing
the femoral vein and causing distension of the long
saphenous vein.
FIG 7.7
ANEURYSMS.
The common sites to find aneurysms.
Chap-07.qxd 4/21/05 12:50AM Page 187
The arteries, veins and lymphatics
188
age. It is debatable if these are truly congenital, but
the weakness responsible for their development
may indeed be inherited.
Syphilitic aneurysms of the thoracic aorta were
once common but are now extremely rare.
History
Age
Atherosclerotic aneurysms are rare before the age
of 50. Thereafter, their frequency increases with age.
Sex
Men are affected 10 to 20 times more often than
women.
Other causative factors
A family history, cigarette
smoking and hypertension are well-recognized risk
factors.
Symptoms
Many aneurysms cause no symptoms dur-
ing life and are discovered by chance during a routine
physical examination or screening programme.
The commonest presenting symptom is dull,
aching pain. With abdominal aneurysms, this is usu-
ally experienced over the swelling in the centre of the
abdomen, but the pain often radiates to the back and
may be experienced only in this site. The abdominal
pain is caused by stretching of the artery, and the
back pain by erosion of the lumbar vertebrae.
Some patients with abdominal aneurysms pres-
ent with sciatica or loin pain as a consequence of
local pressure on the nerves.
Acute pain occurs if the vessel suddenly stretches
or begins to tear. This becomes a very severe pain
if the aneurysm ruptures and a large haematoma
forms (see Chapter 15). The patient may collapse
from the accompanying hypotensive shock or sud-
denly die.
A few thin patients notice a pusatile mass. This
is a common presentation for femoral aneurysms
but is rare for abdominal aneurysms.
Occasionally patients notice their abdomen pul-
sating when they lie in the bath or in bed.
Severe ischaemia of the lower limb follows
thrombosis of an aneurysm. This is a rare event in
aortic and femoral aneurysms but is a common
presentation of popliteal aneurysms.
Less severe ischaemia may be caused by emboli
originating in the aneurysm. One of the best exam-
ples of this complication is the multiple small
emboli which may block the digital arteries of a
patient with a subclavian aneurysm.
Peripheral emboli in the lower limb may cause
intermittent claudication or rest pain.
The aorta, femoral and popliteal arteries are
closely related to the inferior vena cava, femoral and
popliteal veins, respectively. Dilatation of an artery
may block its adjacent vein by direct pressure, or
cause it to thrombose. Patients may then present
with a swollen, blue, painful limb.
Very occasionally aneurysms rupture into an adja-
cent vein. The resulting acute arterio-venous fis-
tula may cause severe cardiac embarrassment. The
tissues distal to the fistula become cyanosed, the
neck veins are elevated and there is usually a loud
machinery murmur over the aneurysm.
Systematic questions and past history
Coronary or
cerebral vascular disease can coexist.
Examination
Abdominal aneurysms
The abdominal aorta divides into the iliac arteries at
about the level of the umbilicus. Consequently most
abdominal aneurysms are felt in the upper umbili-
cal and epigastric regions.
Iliac artery aneurysms present as a pulsating
mass in the iliac fossa or hypogastrium.
Aneurysms produce an expansile pulsation.
In order to feel the expansion, both hands must be
placed on either side of the mass to confirm that the
hands are pushed apart as well as being pushed
upwards. Many lumps in the upper abdomen trans-
mit aortic pulsation and may be misdiagnosed as
aneurysms. Real difficulty may occasionally be
encountered if the aorta is encased by pathologi-
cally enlarged lymph glands.
Aneurysms feel firm and smooth, and some-
times can be moved a little from side to side. The
presence of tenderness implies that there is inflam-
matory change or that the wall of the aneurysm is
stretching and likely to rupture.
The pulses at the groins and in the legs are usu-
ally present and the vessels often slightly dilated. All
pulses must be carefully palpated and their presence
or absence documented, as in some patients aneurys-
mal and occlusive disease may coexist.
The signs and symptoms of a ruptured aneurysm
are described on page 416. When an aneurysm rup-
tures it becomes very painful and tender. The patient
Chap-07.qxd 4/21/05 12:50AM Page 188
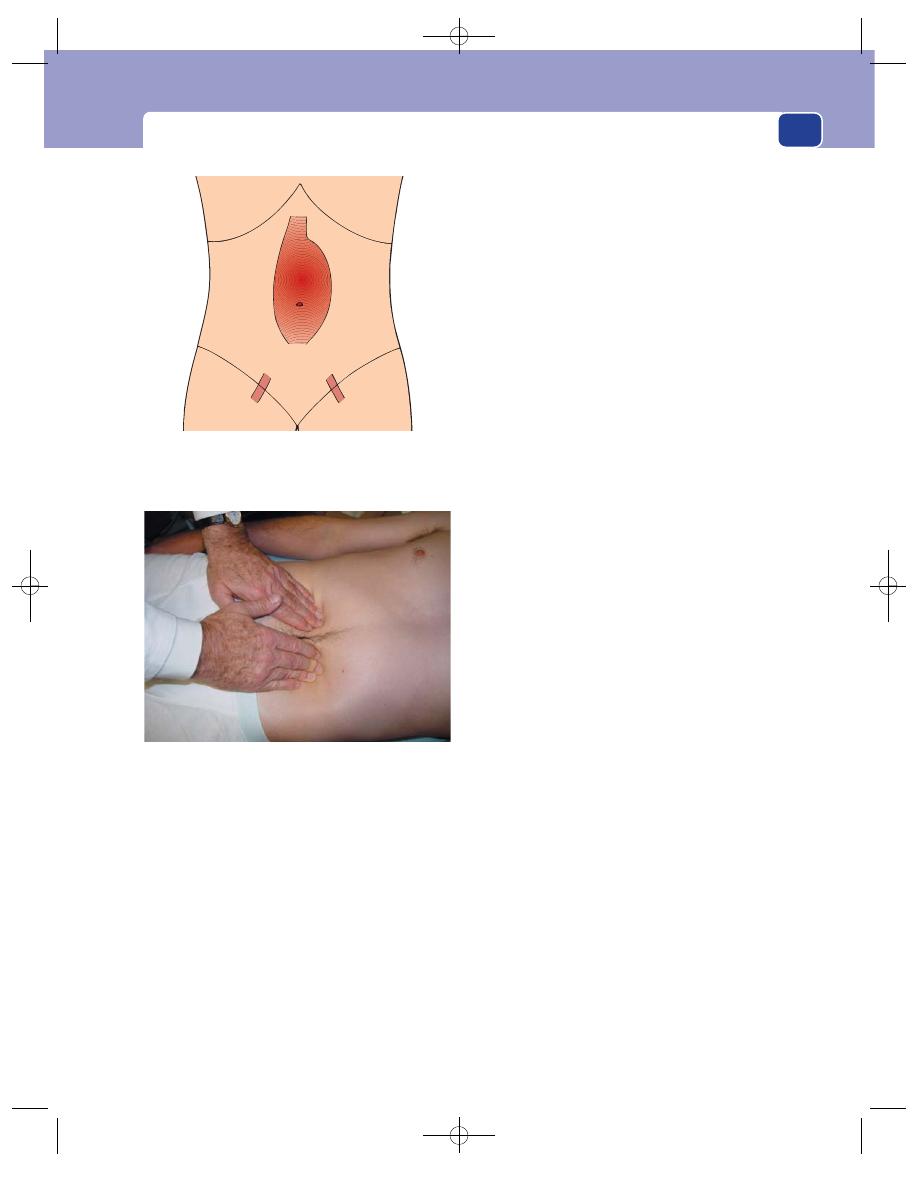
Symptoms produced by arterial insufficiency
189
may collapse with signs of hypovolaemia – pallor,
tachycardia and hypotension.
An expanding retroperitonal haematoma may be
felt as a large mass in the abdomen spreading down
into the iliac fossa or posteriorly into the loins.
Femoral aneurysms
These usually arise in the common femoral artery
and produce a bulge just below the inguinal liga-
ment. They have an expansile pulsation. A mass of
enlarged lymph glands may transmit pulsation and
can be misdiagnosed as an aneurysm (see the differ-
ential diagnosis of groin lump, page 430). The other
pulses in the leg must be documented, as there is
often an associated popliteal aneurysm. Femoral
and popliteal aneurysms are often bilateral, but do
not necessarily develop or present at the same time
(see below).
Popliteal aneurysms
Aneurysms of the popliteal artery are occasionally
noticed by patients if they bulge out of the popliteal
fossa. They may be found by chance in patients pre-
senting with claudication. Popliteal aneurysms
should always be excluded in patients presenting
with an idiopathic calf vein thrombosis.
Unfortunately,
popliteal aneurysms often
thrombose before they are noticed and present with
acute ischaemia of the lower limb (see above).
The diagnosis is confirmed by finding an expan-
sile pulsation in the popliteal fossa. The pulse is
easy to feel. The examiner’s fingers are pushed apart
and away by the pulse, which can often be felt on
both sides of the popliteal fossa. A popliteal
aneurysm should always be suspected when a
popliteal pulse is easy to feel. A bruit may be pres-
ent above or over an enlarged segment of the vessel.
A thrombosed popliteal aneurysm is smooth
and solid and does not pulsate or flucuate. It can be
moved slightly from side to side, but never moves
up and down. It may be confused with a Baker’s
cyst or semimembranosus bursa (see Chapter 4),
but its size does not change when the knee is flexed
and it occupies the whole length of the mid-line of
the popliteal fossa.
The ankle pulses will not be palpable.
The legs should be examined for signs of venous
obstruction, as this is a common complication of
popliteal aneurysms.
False aneurysms
A false aneurysm is a large haematoma whose centre
contains fluid blood which connects with the lumen
of the blood vessel. The commonest cause is a thera-
peutic or diagnostic vascular puncture or a stab
wound. Following the arterial puncture, a haematoma
forms outside the artery. At first, thrombus plugs the
defect, but pulsatile blood pressure gradually pushes
out the haemostatic plug from the defect in the
artery wall and excavates the haematoma to form a
cavity connected to the vessel.
+
+
Assess the width of the abdominal aorta by placing your
hands on either side of the pulse in the epigastrium.
FIG 7.8
ASSESSMENT OF AN ABDOMINAL AORTIC ANEURYSM.
The position of an aneurysm of the abdominal aorta. If there
is a gap between the top of the aneurysm and the costal
margin, the aneurysm probably begins below the origin of the
renal arteries. The femoral pulses are usually palpable.
Chap-07.qxd 4/21/05 12:50AM Page 189
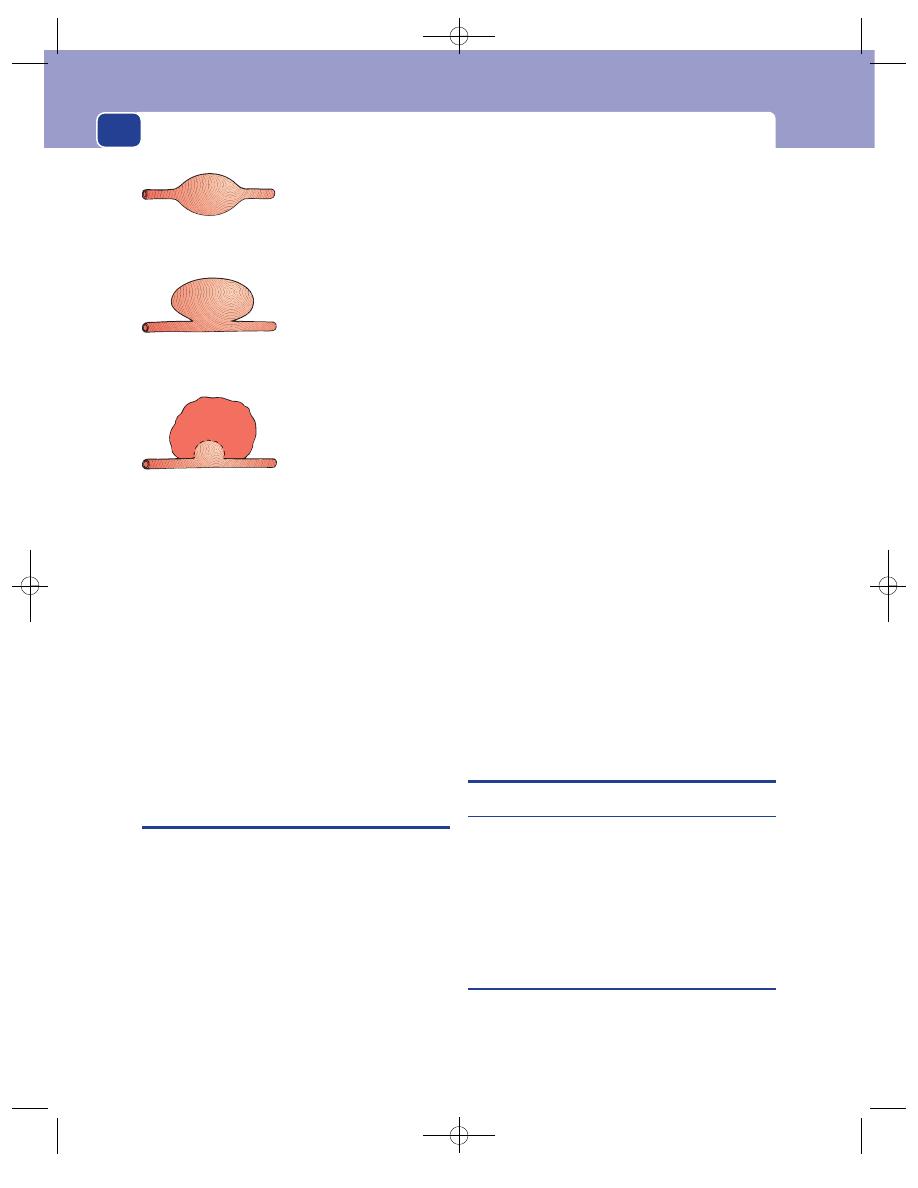
The arteries, veins and lymphatics
190
The symptoms, signs and complications of false
aneurysms are exactly the same as those of a true
aneurysm except:
■
there is a history of trauma or iatrogenic
intervention, followed by
■
the sudden appearance of a swelling;
■
false aneurysms tend to occur at unusual sites,
e.g. wrist or ankle, though iatrogenic false
aneurysms are now most common in the groin.
False aneurysms also occur when a surgical graft
separates from the native vessel. A pulsatile mass
beneath an incision in the groin at the site of a pre-
vious vascular anastomosis is most likely to be a
false aneurysm.
HAEMORRHAGE
A major vascular disruption, which may be the
result of a penetrating, blunt or hyperextension
injury is likely to result in severe hemorrhage. The
bleeding may be concealed, as when, for example, a
serrated or spiculated end of a fractured long bone
pierces an artery or a ruptured aneurysm bleeds
into the tissues or a body cavity, or may be revealed,
as when an aneurysm erupts through the skin or a
congenital vascular malformation bleeds onto the
skin surface.
Concealed haemorrhage from an arterial injury
is suspected if a large swelling rapidly develops in
association with signs of hypovolaemia, i.e. pallor,
sweating, venoconstriction, tachycardia and eventu-
ally hypotension. The pulses distal to the injury will
not be palpable if the artery has been transected,
when the limb may show signs of acute ischaemia
(the six Ps, see page 179).
In patients presenting with visible (revealed)
haemorrhage, the diagnosis is straightforward. There
is usually a jet of bright-red, high-pressure, pulsatile
blood coming out of an obvious cutaneous defect or
wound. (Venous bleeding, in contrast, is dark red
and wells up out of the wound.) The pulses distal to
the injury may be absent if the artery has been tran-
sected. Direct pressure or proximal arterial com-
pression over a bony point should arrest the bleeding
until definitive treatment can be administered.
When the bleeding is coming from the site of a
penetrating wound it is important to assess local
nerve and muscle, as other vital structures may be
damaged. This may be difficult because the arrest of
the haemorrhage must take precedence.
Artery, vein, nerve and muscle injuries com-
monly coexist.
When the haemorrhage occurs into a body cavity
or is deeply seated, there may be no signs of swelling
and the symptoms of hypovolaemia predominate.
Haemorrhage into the peritoneum or retroperi-
toneum often causes pain as well as collapse (see
page 416).
TRANSIENT AND PERMANENT
WEAKNESS, PARALYSIS AND
BLINDNESS
Transient cerebral ischaemia
A transient ischaemic attack (TIA) is an episode of
sudden paralysis, paraesthesiae or speech loss
caused by a sudden reduction in the blood flow to a
part of the brain. To be classified as transient, the
symptoms must recover completely within 24 hours.
(TIA is a poor term, as it does not indicate which
tissue in the brain is ischaemic.)
Persistant cerebral ischaemia
Persistant cerebral ischaemia causes a stroke. This is
a sudden episode of prolonged cerebral malfunction
caused by cerebral infarction or haemorrhage, both
Fusiform aneurysm
Saccular aneurysm
False aneurysm
A cavity in a haematoma
which connects with the
lumen of the artery
FIG 7.9
The types of aneurysm.
Chap-07.qxd 4/21/05 12:50AM Page 190
Transient and permanent weakness, paralysis and blindness
191
caused by vascular disease, which usually takes the
form of a prolonged weakness or paralysis of half
the body (a hemiplegia) and sometimes an associ-
ated sensory or speech defect, which may predom-
inate. The malfunction does not begin to recover for
several days and may never recover completely.
Ischaemia of the mid-brain that damages the
vital centres in this area may cause coma and car-
diovascular and respiratory instability.
It is important to remember that the right side
of the brain controls the left side of the body, and
vice versa.
The speech area (Broca’s area) is invariably in the
left temporo-parietal area in right-handed people,
although it can be in the right hemisphere in left-
handed patients.
Strokes are more commonly caused by infarc-
tion than by cerebral haemorrhage and are usually
embolic or thrombotic, though an arterial wall
dissection can occlude an artery’s lumen.
Stroke caused by cerebral haemorrhage pro-
duces identical cerebral symptoms but is more com-
mon in women and is associated with hypertension.
Both types of stroke usually cause upper motor
neurone signs, with reduced power, spastic tone and
brisk reflexes in the limbs, associated with an up-
going plantar reflex (Babinksi’s sign). A cerebral
haemorrhage can only be differentiated from an
infarct with certainty by computerized tomography
(CT) scanning, not by the history or physical signs.
Transient ischaemic attacks
Transient ischaemic attacks are caused by emboli or
hypoperfusion.
The emboli that cause TIAs come from the carotid
arteries, heart valves and the great vessels. Platelet
clumps and cholesterol crystals originally attached
to ulcerated plaques break off and are swept up into
the retinal or cerebral vessels. Retinal emboli cause
transient loss of vision, known as amaurosis fugax
(fleeting blindness), which seems to the patient like
a curtain coming across the visual field or a grey veil
blocking out all or part of the vision in one eye.
Anyone presenting with a brief episode of weak-
ness, paraesthesiae or loss of sensation in one half of
the body which lasts a few minutes or several hours
and then recovers completely must be suspected of
having a TIA.
There are usually no physical signs by the time the
patient presents, but evidence of previous ischaemic
episodes – facial weakness, expressive dysphagia,
upper motor neurone lesions and cholesterol emboli
in the retinal vessels or areas of retinal infarction –
should be sought.
The detection of a carotid bruit over the carotid
artery just below the angle of the jaw indicates the
presence of at least some stenosis in the region of
the carotid bifurcation. However, a severe internal
carotid artery stenosis can be present without any
bruit, and a loud bruit can be caused by a stenosis of
the external carotid artery.
Arrhythmias and cardiac murmurs suggest a car-
diac source for the emboli. A low pulse pressure and
an ejection systolic murmur suggest the presence of
aortic valve disease, while an irregularly irregular or
very slow pulse suggests a possible cause of Stokes–
Adams attacks.
Transient hypoperfusion
Whereas emboli are common, hypoperfusion is rare
because auto-regulation usually ensures adequate
cerebral perfusion unless there is a very severe reduc-
tion in carotid blood pressure and flow. Episodes of
hypoperfusion usually occur with much greater fre-
quency than embolic attacks – often several times a
day or week – and can be brought on by exercise
or vasodilatation. They may cause ‘global’ brain
ischaemia and present with dizziness and collapse
rather than motor cortical symptoms.
Differential diagnosis
The differential diagnosis of a TIA is shown in
Revision panel 7.8.
A history from a bystander or relative may be
very helpful in making the diagnosis. Any history of
aura, twitching, tongue biting or incontinence is
indicative of grand mal epilepsy, whereas petit mal
causes patients to lose touch temporarily with their
surroundings.
Hypoglycaemic attacks
These occur during periods
of food abstinence, especially at night. Patients often
describe hunger, malaise and vague abdominal pain,
which is accompanied by trembling, dizziness and
blurred vision. They may also notice incoordination,
slurred speech, diplopia and drowsiness. The blood
Chap-07.qxd 4/21/05 12:50AM Page 191
The arteries, veins and lymphatics
192
and urinary sugar is low during an attack, the symp-
toms of which can be instantly relieved by glucose.
Migraine
Migrainous attacks are usually associated
with severe unilateral headache, often situated over
one eye and associated with photophobia and vom-
iting and occasionally transient blindness. There are
no physical signs and the diagnosis relies entirely on
the history.
Vertebrobasilar insufficiency
Sometimes it can be
quite difficult to separate TIAs from vertebrobasilar
insufficiency, but the symptoms of the latter are
often precipitated by neck movements or looking
up. Neurological signs may indicate pathology in
the hind-brain or cerebellum. Bruits may be heard
over the origin of the vertebral artery.
Subclavian steal syndrome
Occasionally patients
present with transient motor or sensory symptoms,
even loss of consciousness, after arm exercise. The
presence of a weak brachial and radial pulse, reduced
blood pressure in the affected arm, and a bruit over
the subclavian artery should suggest the diagnosis
of subclavian steal syndrome.
This syndrome occurs when the first part of the
subclavian artery is blocked and blood flows down
the vertebral artery because, during arm exercise, it
acts as a collateral vessel to supply the arm. This
steals blood away from the hind-brain and gives rise
to hind-brain and cerebellar symptoms.
Multiple sclerosis, acute glaucoma, retinal tears
and temporal arteritis can cause transient blindness.
Multiple sclerosis can cause considerable diagnostic
confusion, but multiple lesions occurring in time
and space eventually indicate the likely diagnosis.
Other intracranial disease
Patients with a subdural
haematoma may experience fluctuations in their
level of consciousness and will almost always develop
some localizing neurological signs before eventually
developing signs of raised intracranial pressure.
This is also true of cerebral tumours and metas-
tases, which can initially cause diagnostic confusion
until the patient eventually develops signs of fixed
and expanding defects.
Completed strokes
A full neurological examination is essential in all
patients who present with a completed stroke, in
order to exclude a vascular cause as well as a neurolog-
ical dysfunction caused by space-occupying lesions,
abscesses, haematomata and multiple sclerosis. The
blood pressure and heart must be carefully assessed.
The superficial temporal arteries should be palpated.
The carotid bifurcation and lower neck should be aus-
cultated for bruits. A stethoscope placed over the
closed eye can occasionally detect intracerebral bruits
in patients with a stenosis of the carotid siphon.
COLD, BLUE DIGITS, HANDS AND FEET
Intermittent colour changes in the skin of the periph-
ery of the limbs suggest the presence of vasospasm
or recurrent minor episodes of arterial occlusion, the
many causes of which are listed in Revision panel 7.9
and must be excluded before the diagnosis of
vasospastic disease is accepted. To do this, the supra-
clavicular fossa must be inspected and palpated for a
fullness or occasionally a bony lump caused by a cer-
vical rib or a dilated subclavian artery. The subcla-
vian, axillary, brachial, radial and ulnar pulses must
all be palpated and auscultated. The blood pressure
should be measured in both arms, and Doppler pres-
sures must be measured in the radial, ulnar and
brachial pulses. Abnormalities in any of these exami-
nations may require special tests such as plain radi-
ographs, Duplex scanning and arteriography.
Patients not found to have a physical obstruction
of their blood vessels are likely to be suffering from
excessive vasospasm of the small vessels in their
hands in response to cold and emotional stimuli.
Revision panel 7.8
The differential diagnosis of a transient
ischaemic attack
Grand or petit mal epilepsy
Stokes–Adam’s attacks from a tight aortic
stenosis
Arrhythmias
Vasovagal attacks
Hypoglycaemia
Migraine
Vertebrobasilar disease
Subdural haematoma
A space-occupying lesion in the brain
Chap-07.qxd 4/21/05 12:50AM Page 192
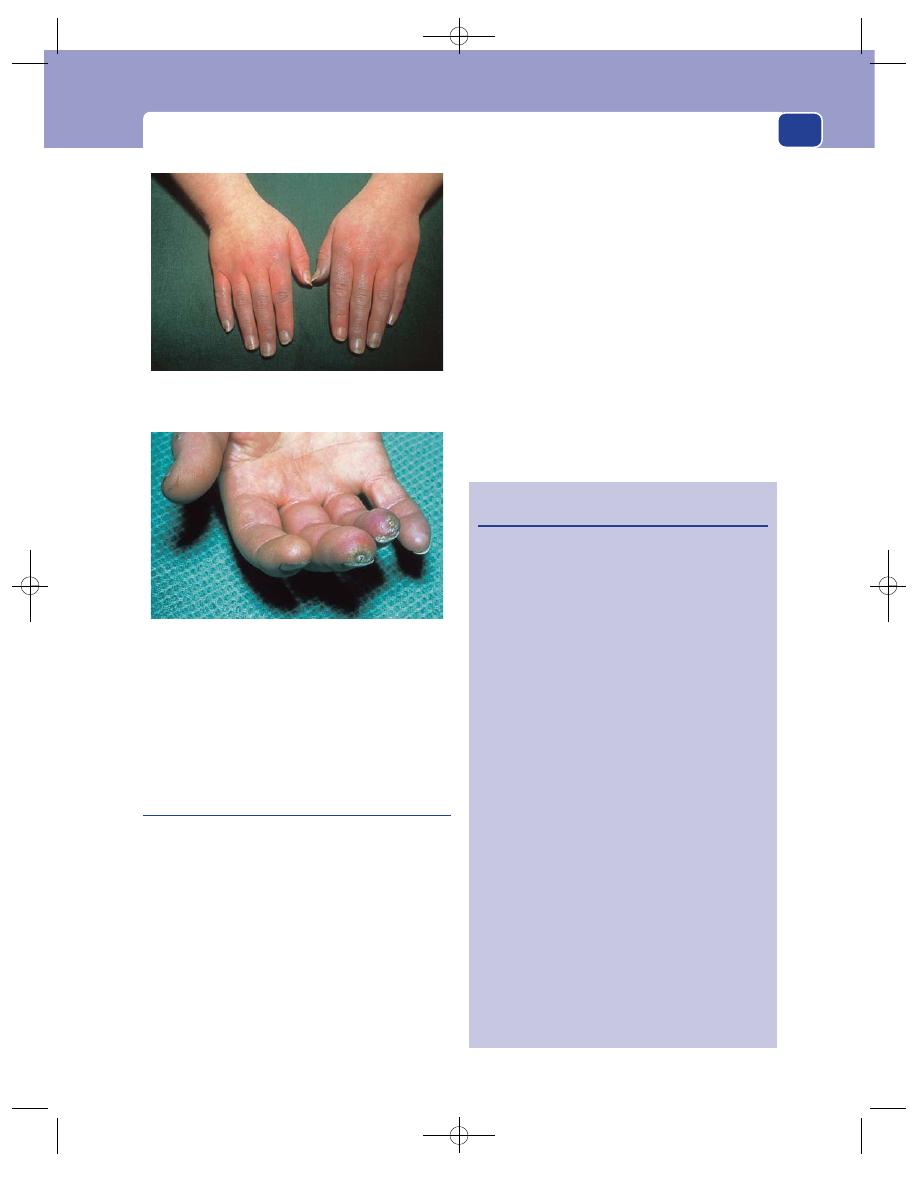
Cold, blue digits, hands and feet
193
Some conditions can be diagnosed by the physical
appearances they produce, but their aetiology is still
largely conjectural and there is a considerable over-
lap between each condition.
Raynaud’s phenomenon
This is the best known vasospastic disorder. The
term is used to describe a series of colour changes in
the skin of the hands or feet following exposure to
cold. The condition can be most distressing in cold
climates, especially in winter.
■
The skin first turns white and becomes cold and
numb.
■
It next turns blue but remains cold and numb.
■
Finally, it turns red, hot and painful.
Many attacks are brought on by cold or emotion
and many do not pass through all the classic colour
changes.
History
Sex
Ninety per cent of those affected are women,
and many are cigarette smokers. It affects 5–20 per
cent of the population.
Past history
It is worthwhile asking patients if they
have a history of frostbite, have ever worked in a
cold storage environment or have regularly used
vibrating tools.
Joint problems, rashes and swallowing difficulty
indicate the likelihood of scleroderma or another
collagen vascular disease.
Examination
Those conditions that, in addition to the colour
changes, cause permanent damage to the digital
Revision panel 7.9
The causes of Raynaud’s phenomenon
Atherosclerosis and Buerger’s disease
Platelet emboli from:
subclavian aneurysm (secondary to
cervical rib)
atherosclerotic stenosis of subclavian
artery
Collagen disease
Scleroderma
Systemic lupus erythematosus
Rheumatoid arthritis
Vibrating tools
Irritation of nerves
Cervical spondylosis
Cervical rib
Spinal cord disease
Old poliomyelitis
Repeated immersion in cold water
Working in a cold environment
Previous frostbite
Blood abnormalities
Cold agglutinins
Cryoglobulins
Polycythaemia
Drugs
Ergot
General diseases
Hypothyroidism
Diabetes
Malnutrition
Ischaemic ulceration of the fingertips. This usually
indicates permanent, rather than spastic, occlusion of the
digital vessels.
FIG 7.10
RAYNAUD’S PHENOMENON.
Hands showing the transition from the blue to the red
phase. Ten minutes earlier the fingers of both hands had
been white and numb.
Chap-07.qxd 4/21/05 12:50AM Page 193
The arteries, veins and lymphatics
194
arteries, such as scleroderma, vibration injury and
blood abnormalities, gradually cause atrophy of the
pulps of the fingers, poor nail growth and ulcera-
tion of the fingertips.
If the digital arteries become occluded, the fingers
waste, especially the pulps, and become thin, stiff
and pointed. The hand is cold and the joints may be
stiff. Sometimes there are small, painful, ischaemic
ulcers on the fingertips which are slow to heal, or
small scars at the site of the resolution of previous
patches of ischaemia. Both are very painful and ten-
der. The patient may eventually get rest pain and
gangrene of the fingertips.
Repeated infections around the nails (paronychia)
are common.
Many patients eventually develop the signs of
scleroderma, evidence that the phenomenon is a
secondary abnormality, not a primary disease.
If the cause of the colour changes is solely
vasospasm, the hands will look normal between
attacks, making the diagnosis of the underlying cause
far more difficult. As has been shown, the symptoms
are often secondary to many other conditions and
the diagnosis of idiopathic Raynaud’s disease is only
made when these have been excluded. The common
causes are the collagen vascular diseases, especially
scleroderma, the excessive use of vibrating tools, and
cold exposure. Patients with scleroderma, systemic
lupus erythematosus and rheumatoid arthritis may
show the characteristic changes in their skin and face.
Primary Raynaud’s disease
When all the other causes of Raynaud’s phenomenon
have been excluded, one is left with the diagnosis of
primary Raynaud’s disease.
This is quite common in teenage girls. It is mild,
familial and often associated with chilblains. It
often disappears in the late twenties, but a few women
have symptoms all their life and occasionally the
disease becomes very severe.
If the phenomena start in adult women, often
around the menopause, they are likely to be the first
sign of scleroderma.
It is always worthwhile measuring the Doppler
pressures at the wrist, especially if the pulses are
impalpable. The digital vessels may also be insonated
with the Doppler flow detector, and in patients with
collagen diseases, pulses in these may well be absent
near the tips of the fingers.
Some doctors use a cold exposure test – dipping
the hands in cold water and re-mapping and
re-measuring the Doppler digital pressures in the fin-
gers – to reproduce the symptoms and confirm the
existence of a cold sensitivity. This can also be carried
out at the bedside using thermographic equipment.
Acrocyanosis
This is a condition, usually affecting women, in
which the hands and feet are persistently blue and
cold. The colour of the skin does not vary with the
environmental temperature as it does in Raynaud’s
phenomenon, but the blueness may come and go.
The hands may be pink and normal between
attacks, or cold with sweaty palms. As the attack
subsides, the hands may become warm, sweaty and
painful. The fingers are susceptible to chilblains.
The diagnosis is based solely on the colour, temper-
ature and appearance of the hands.
Erythrocyanosis crurum puellarum
frigidum
This condition affects the posterior and medial aspects
of the lower legs of young (15–25 years old) girls in
response to cold. The legs are often fat and hairless.
The affected areas become red/blue (erythrocyanotic)
and swollen. Dusky reddish purple blotches appear
and may feel cold to the touch. The swollen area is
tender and may progress to chilblains and superficial
ulceration. The swelling is often more noticeable
than the discolouration, and if it spreads around the
ankle, can be mistaken for lymphoedema. When the
chilblains break down and ulcerate, they must be
differentiated from other forms of leg ulcer.
Erythromelalgia
This is a condition in which the patient complains
of burning red extremities. These symptoms may
be exacerbated by the pressure of bedclothes against
the skin. The condition is much commoner in women.
It appears to result from the release of vasodilator
neurochemicals, with 5-hydroxytryptamine accu-
mulating in the tissues. It must be differentiated
Chap-07.qxd 4/21/05 12:50AM Page 194
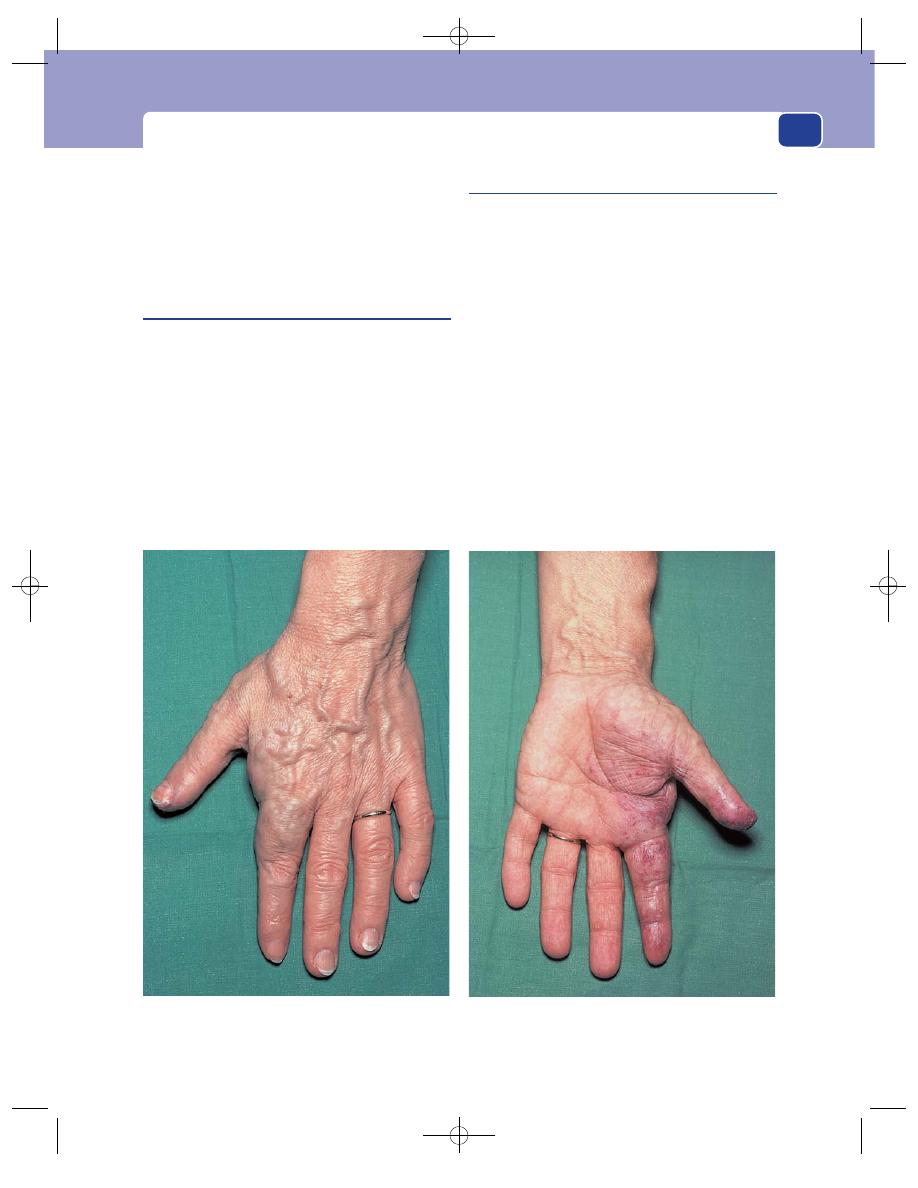
Cold, blue digits, hands and feet
195
from gout, Buerger’s disease, systemic lupus ery-
thematosus, rheumatoid arthritis and peripheral
neuritis.
Examination of the extremities confirms that
they are red and the patients complain that depend-
ency causes an increase in the pain.
Hyperhidrosis (excessive sweating)
This condition (see Chapter 3, page 99) is closely
associated with vasospastic disorders. The excessive
sweating is unrelated to heat and affects especially
the palms of the hands, the soles of the feet and the
axillae. Excessive sweating from the groins and face
may also be troublesome. It is more common in
women and is socially embarrassing, particularly
during the patient’s first clinic consultation.
Hyperhidrosis can be caused by thyrotoxicosis,
which must be excluded by careful examination and
special tests.
Large limbs
Local gigantism, multiple arterio-venous fistulae
and the Klippel–Trenauney syndrome all cause a
limb to grow larger and thicker than its fellow.
Multiple arterio-venous fistulae throughout a
single limb is known as the Parkes Weber syn-
drome. This is a congenital abnormality. The limb,
as well as being enlarged, feels hot. The subcuta-
neous veins are often dilated. There may be palpable
thrills and audible machinery murmurs over the
major sites of fistulation.
A tourniquet inflated around the root of the limb
should cause slowing of the pulse (the Branham–
Nicoladoni sign). This is a consequence of reducing
the venous return by abolishing the shunt. The dif-
ferential diagnoses are the other causes of limb
hypertrophy mentioned above. Rarely, patients with
a swollen, lymphoedematous limb are misdiag-
nosed as having a hypertrophic limb.
FIG 7.11
A congenital arterio-venous fistula of the hand, anterior and posterior views. The index finger and thenar eminence
are enlarged, the veins are distended and the thenar eminence is pulsatile. There is ischaemic ulceration on the tip of the
thumb. A bruit could be heard, on auscultation, all over the hand.
Chap-07.qxd 4/21/05 12:50AM Page 195
The arteries, veins and lymphatics
196
HYPERTENSION
Patients with high blood pressure rarely present to a
surgical outpatients, but renal artery stenosis, adre-
nal tumours and coarctation of the aorta are impor-
tant, surgically correctable causes of hypertension.
The renal function must be assessed and the abdomen
should be auscultated for bruits in all atheroscle-
rotic patients who are found to be hypertensive.
A ‘moon’ face, abdominal striae and a ‘buffalo’
hump (see Chapter 8) are indicative of Cushing’s
syndrome, while the presence of neurofibromata
suggests the possibility of a phaeochromocytoma.
Coarctation of the aorta is a rare but important
condition. Knowledge of the physical signs enables
early detection before symptoms develop. This can
lead to a surgical correction, which prolongs life.
Coarctation is a congenital narrowing of the aorta
just beyond the left subclavian artery close to the
site of the ligamentum arteriosum, which is the
remnant of the ductus arteriosus. Provided the duc-
tus closes normally, a coarctation usually remains
symptomless until adult life, but if the ductus
remains patent, patients rapidly develop symptoms
and often have other cardiac abnormalities.
The symptoms and signs include:
■
dyspnoea on exertion,
■
cerebrovascular accidents associated
with hypertension in the upper half of the
body,
■
collateral arteries visible and palpable over the
scapulae, and
■
weak or delayed femoral pulses.
There will be a strong cardiac impulse as the left
ventricle hypertrophies in an attempt to overcome
the resistance to aortic blood flow caused by the
coarctation. A systolic murmur is usually present to
the left of the vertebral column at the T4/5 level, just
over or beyond the stenosis.
Ophthalmoscopic examination may reveal reti-
nal haemorrhages, exudates and papilloedema.
INTESTINAL ISCHAEMIA
Ischaemia of the bowel may have an acute or
chronic onset.
Acute obstruction of the superior mesenteric
artery by an embolus or by thrombosis causes acute
abdominal pain, peritonitis and shock (see Chapter
15, page 414).
Chronic atherosclerotic occlusion or stenosis of
the coeliac or mesenteric vessels can cause intestinal
angina – abdominal pain that develops 30–60 minutes
after eating – causing fear of eating and weight loss.
A reduced blood flow in the arteries of the colon,
particularly the splenic flexure, can cause ischaemic
colitis with diarrhoea and sometimes rectal bleeding.
The only physical sign in the chronic syndromes
may be the presence of an abdominal bruit.
THE VEINS
CLINICAL ASSESSMENT OF
THE VENOUS CIRCULATION OF
THE LOWER LIMB
Anatomy and physiology
The veins of the lower limb are divided into super-
ficial and deep systems, separated by the deep fascia
of the leg. At certain points there are veins that pass
through the deep fascia to provide a communica-
tion between the two systems. Normally the valves
in these communicating veins only allow blood to
pass from the superficial into the deep system. The
deep veins have many valves to ensure that blood
only flows upwards against the force of gravity
towards the heart.
Blood flow in the erect position is mostly pro-
duced by the calf muscle pump. Within the soleal
muscles of the calves are large venous sinusoids – the
soleal sinusoids – which are compressed during
contraction of the calf muscles, e.g. during walking,
so that blood is forced out of the calf veins into the
popliteal veins and on towards the heart. During
calf muscle relaxation, the intramuscular veins open
Chap-07.qxd 4/21/05 12:50AM Page 196
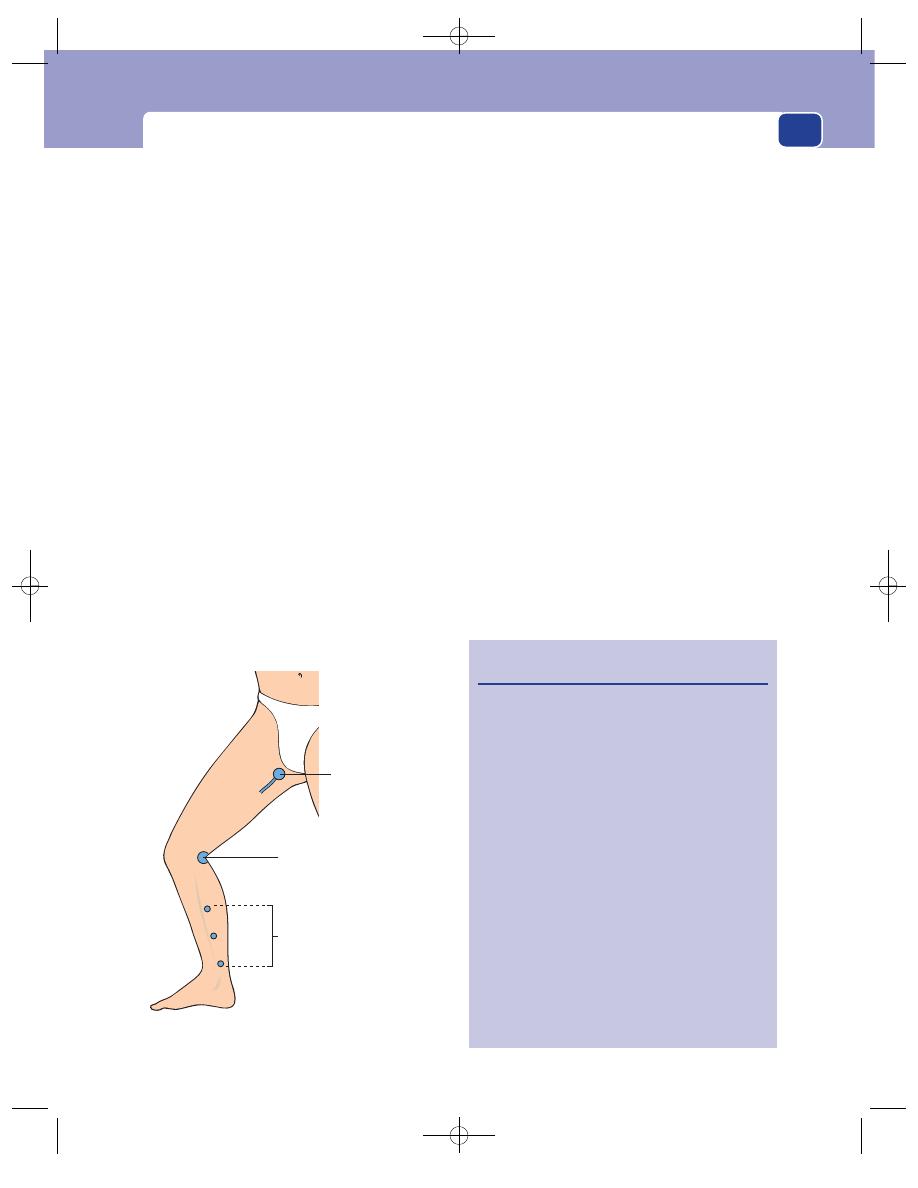
Clinical assessment of the venous circulation of the lower limb
197
but blood is prevented from refluxing back into them
from the proximal deep veins by the valves in the
popliteal veins. The negative pressure in the deep
veins then sucks blood in from the superficial system
through the communicating veins to reduce the
superficial venous pressure, incrementally, with each
calf muscle contraction.
The superficial veins all eventually join either the
great (long) or lesser (short) saphenous system.
These two major subcutaneous veins end where they
communicate with the femoral and popliteal veins,
respectively.
Both superficial systems are also joined to the
deep veins by a number of other communicating
(perforating) veins, the most important of which
are in the calf.
The main tributaries of the saphenous veins are
the veins that become varicose because they, unlike
the saphenous veins, do not contain a strong coat of
smooth muscle in their wall. They lie in a more
superficial position and are not bound down to the
deep fascia.
The deep veins accompany the arteries of the
lower leg join to form the popliteal vein, which also
receives blood from the calf muscle sinusoids.
Deep vein thrombosis usually starts in the sinu-
soids and venae commitantes. The thrombus may
then extend up into the popliteal vein, the femoral
vein, the iliac veins and even into the vena cava.
Symptoms of lower limb venous disease
Most patients with venous disorders complain of
unsightly veins in their lower limbs, pain or dis-
comfort when standing and minor ankle swelling.
They also may complain of skin changes (lipoder-
matosclerosis, eczema, pigmentation and ulcera-
tion) in the skin of the gaiter region. Superficial
veins may occasionally bleed.
Superficial vein thrombosis causes painful
lumps or cords.
Deep vein thrombosis presents with calf pain
and leg swelling or pleuritic chest pain, haemopty-
sis and dyspnoea if it is complicated by a pulmonary
embolism.
Examination of the veins of the lower limb
Inspection
The lower limbs need to be properly exposed with
the patient standing erect on a low stool in a warm,
Long saphenous –
femoral vein junction
Short saphenous –
popliteal vein junction
Lower leg communicating
veins 5, 10 and 15 cm
above the medial malleolus
FIG 7.12
The common sites where the superficial veins
connect with the deep veins.
Revision panel 7.10
Routine for assessing the venous circulation
Ask the patient to stand up
Inspection
Site and size of visible veins
Effect of elevation and dependency
Ankle oedema
Skin colour
Palpation
Palpate the trunks of long and short
saphenous veins
Palpate the sapheno-popliteal junction
Feel for fascial defects
Feel the texture of the skin and
subcutaneous tissues
Percussion
Percussion wave conduction
Auscultation
Listen for bruits over prominent varices
Tourniquet tests
Doppler ultrasound
Chap-07.qxd 4/21/05 12:50AM Page 197
The arteries, veins and lymphatics
198
well-lit examination room. Many patients with
venous disorders have visible, dilated and tortuous
subcutaneous veins, which are described as varicose
veins.
Both limbs must be examined from in front and
behind to ensure that all aspects of the legs are
examined. The site and course of all the varicosities
should be recorded on anterior and posterior out-
line drawings of the lower limb.
A blue-tinged bulge in the groin, which disap-
pears on lying down, is likely to be a saphena varix.
Some varicose veins are large and prominent,
whereas others are minute and intradermal. The lat-
ter may cause a blue patch, which can arise from a
single feeding vein. Intradermal veins are called spi-
der veins or venous stars. Slightly larger intermedi-
ate veins are often called reticular veins. Large,
prominent, distended veins on the medial side of
the lower calf are often called blow outs if they lie in
close proximity to the site of incompetent calf com-
municating veins.
The network of small dilated venules that devel-
ops beneath the lateral and/or the medial malleolus
of limbs with severe venous hypertension is called
an ankle flare or a corona phlebectactica.
Distended veins crossing the groins and extend-
ing up over the abdominal wall are collateral veins
and indicate the presence of a deep venous obstruc-
tion. Cross-pubic collateral veins may be visible if
one iliac system is obstructed.
The skin of the lower medial third of the leg, the
gaiter region, must be carefully inspected. Venous
hypertension caused by venous outflow obstruction
or severe reflux may cause an area of skin pigmen-
tation, tenderness and subcutaneous induration,
called lipodermatosclerosis, and eventually eczema
and ulceration.
Palpation
The examiner’s dominant hand should be gently
run over the course of the main veins and their tribu-
taries because dilated veins can sometimes be more
easily felt than seen, especially in fat legs. Veins in the
lower leg often lie in a gutter of indurated subcuta-
neous fat. Dilated long and short saphenous veins are
usually easy to feel. The termination of a distended
short saphenous vein is easier to feel if the patient is
asked to bend the knees slightly to relax the deep fas-
cia covering the popliteal fossa.
Carefully palpate the sapheno-femoral junction
(2.5 cm below and lateral to the pubic tubercle) and
the sapheno-popliteal junction, which has a vari-
able termination in the popliteal fossa (high or low).
The patient should be asked to cough while the
dilated veins are palpated to see if there is any
impulse or thrill (a cough impulse) indicating that
the valves at their junctions with the deep veins are
incompetent and the back flow is turbulent.
Palpate the skin of the calf to define any areas of
induration and tenderness (lipodermatosclerosis).
Palpate the medial side of the calf for deficits in the
deep fascia which may be the sites of incompetent
calf communicating (perforating) veins. (This is an
unreliable technique, as large surface varicosities
produce lacunae in the subcutaneous fat of the calf
similar to the perforating vein deficits.)
Percussion
The distended, dilated trunks of the
long and short saphenous systems will always trans-
mit a percussion wave in an orthograde direction
whether the valves are competent or not. The more
distended the vein, the better the wave is transmit-
ted. If a percussion wave is transmitted retrogradely,
i.e. downwards while the patient is standing, the
valves must be incompetent.
Percussion can also be used to help define the
terminations of the long and short saphenous veins
by placing the fingers of one hand gently over the
upper end of the dilated saphenous trunk and per-
cussing the vein below it using the middle finger of
the other hand to ‘flick’ the distended varicosities.
The process can then be repeated in reverse, with
the upper end of the vein being ‘flicked’ and the
lower hand detecting a downward percussion wave,
to check the competence of the valves.
Auscultation
Listen with your stethoscope over any large clusters
of veins, especially if they remain distended when
the patient lies down and the limb is elevated. A
machinery murmur over such veins indicates that
they are secondary to an arterio-venous fistula.
Tourniquet tests
Many clinicians have abandoned tourniquet tests as
a means of assessing varicose veins in favour of
more sophisticated investigations, but these tests
are simple to perform and, if correctly carried out,
Chap-07.qxd 4/21/05 12:50AM Page 198
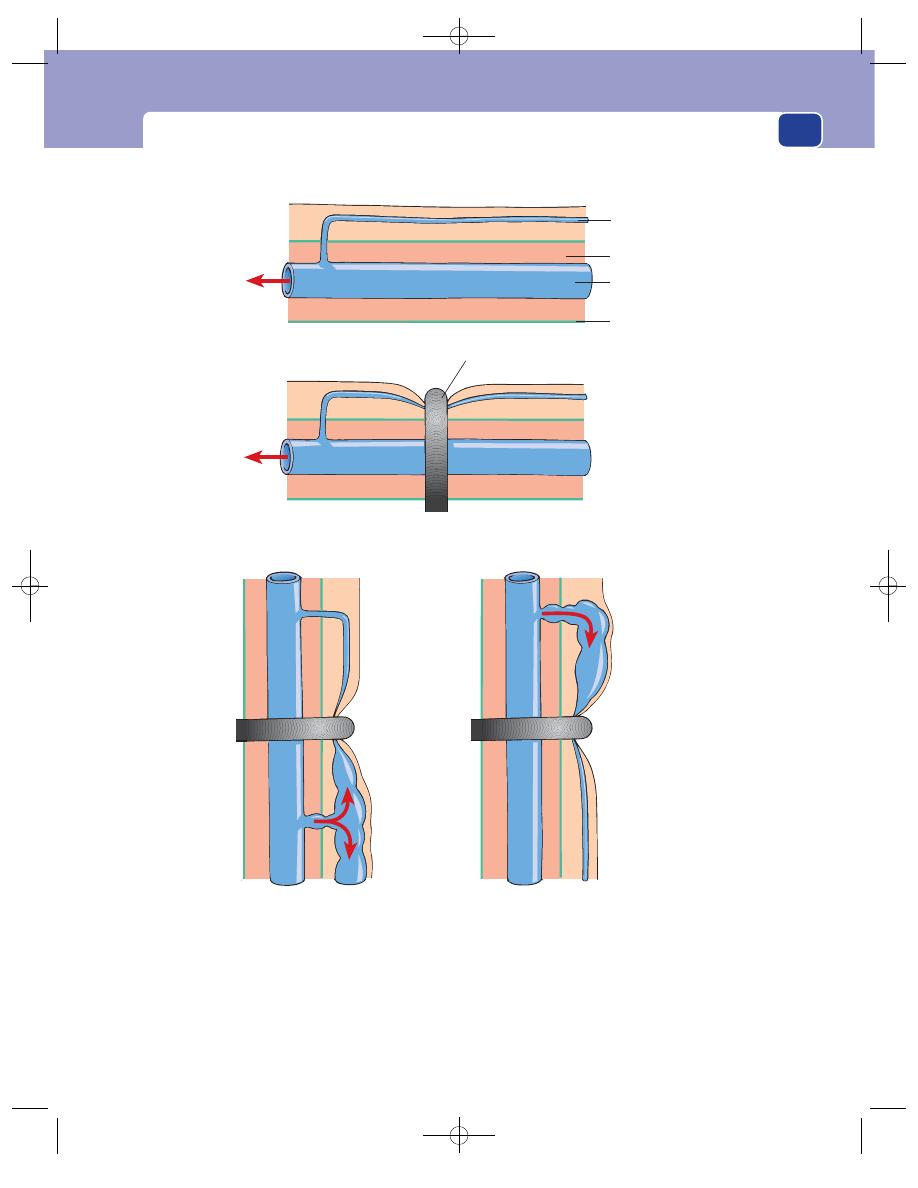
Clinical assessment of the venous circulation of the lower limb
199
By moving the tourniquet up and down the leg it is possible to determine
the level of the incompetent communicating veins
The patient stands up
An incompetent communicating
vein below the tourniquet fills
the superficial veins below the
tourniquet
An incompetent communicating
vein above the tourniquet fills
the superficial veins above the
tourniquet
Leg horizontal, superficial veins empty
Tourniquet occludes the
superficial veins
Superficial vein
Deep vein
Muscle
Fascia
FIG 7.13
The principles of the tourniquet test.
Chap-07.qxd 4/21/05 12:50AM Page 199
The arteries, veins and lymphatics
200
can provide useful information on the major sites of
communicating vein incompetence.
The patient should lie on a couch which has a
small foot stool attached to it, onto which the patient
can rapidly stand. The limb to be examined is then
elevated – often by placing it on the examiner’s
shoulder – to empty the veins, a process that can be
expedited by stroking the blood within the veins
towards the heart.
A tourniquet made from a long length of 1 cm
diameter soft rubber tubing is then pulled tight
around the upper thigh and held in place by strong
artery forceps (Spencer Wells). The rubber tubing
must press firmly into the subcutaneous tissues of
the thigh to ensure that the subcutaneous veins are
completely occluded. The Velcro tourniquets used
by many house officers for venesection do not apply
enough pressure, but the soft tubing on a stetho-
scope is an effective alternative if rubber tubing is
not available, provided it is long enough. The
patient is then asked to stand up quickly and the
legs are observed for 10–15 seconds. If the sapheno-
femoral junction is the only site of superficial to
deep valvular incompetence, the veins above the
tourniquet will rapidly fill but those below it will
remain collapsed. This can be confirmed by sud-
denly releasing the tourniquet and watching the
veins below the site of the tourniquet rapidly dis-
tend from above, as blood regurgitates down the
long saphenous vein. If the veins below the tourni-
quet fill immediately the patient stands up, there
must be other sites of superficial to deep incompe-
tence below the level of the tourniquet.
This test can be repeated with the tourniquet
moved progressively down the whole length of the
leg to try to define all the sites of superficial to deep
vein incompetence, but it is easier and simpler to
apply it once below the knee to exclude short saphe-
nous incompetence.
Tourniquet tests are often difficult to interpret in
patients with recurrent varicose veins, and the value
of applying multiple tourniquets in an effort to
locate the precise level of calf communicating veins
has never been scientifically verified.
A modification of the tourniquet test is to
empty the limb as described above and apply direct
digital pressure over the upper end of the long
saphenous vein while the patient stands up to see if
this prevents retrograde filling. This is called the
Trendelenburg test.
Venous hypertension caused by proximal vein
obstruction or the presence of an arterio-venous
fistula should be suspected if varicose veins fail
to collapse on elevation. This can be confirmed by
asking the patient to stand up after placing a tourni-
quet just below the knee, to cut off both long and
short saphenous reflux, and then to stand repeat-
edly on tiptoe and relax. In a normal limb this exer-
cise will empty the superficial veins by sucking
the blood in the surface varicosities into the deep
veins, through competent perforating veins, and
then pumping it up through the popliteal vein to
the heart. Failure to achieve superficial vein empty-
ing during this exercise indicates deep vein obstruc-
tion or reflux through incompetent valves in the
deep or communicating veins. This is called Perthés’
walking test.
Doppler flow detector studies
The simple directional Doppler ultrasound flow
probe described on page 178 can be used to assess
venous reflux. The patient is asked to stand up and
the ultrasound probe is placed over the termination
of the long and then the short saphenous veins using
coupling jelly. The direction of venous blood flow,
augmented by rapid intermittent manual compres-
sion of the calf and any prominent varicosities in the
lower limb, is then assessed. A uniphasic signal on
squeezing, with no sound on releasing the compres-
sion, indicates competent valves with forward flow.
A biphasic signal, with prolonged retrograde flow
on releasing the compression, indicates reflux and
valvular incompetence. Retrograde flow can also be
confirmed by asking the patient to perform the
Valsalva manouevre, i.e. taking a deep breath, pinch-
ing off the nose, closing the mouth and attempting a
forced expiration. This causes venous flow to reverse
if the valves are incompetent.
The Doppler ultrasound flow detector can also
be used in association with the tourniquet test to
demonstrate retrograde flow in the saphenous trunks
when the tourniquet is released.
The simple hand-held Doppler flow detector can-
not detect retrograde flow in either the deep or calf
perforating veins with any accuracy. The detection of
Chap-07.qxd 4/21/05 12:50AM Page 200
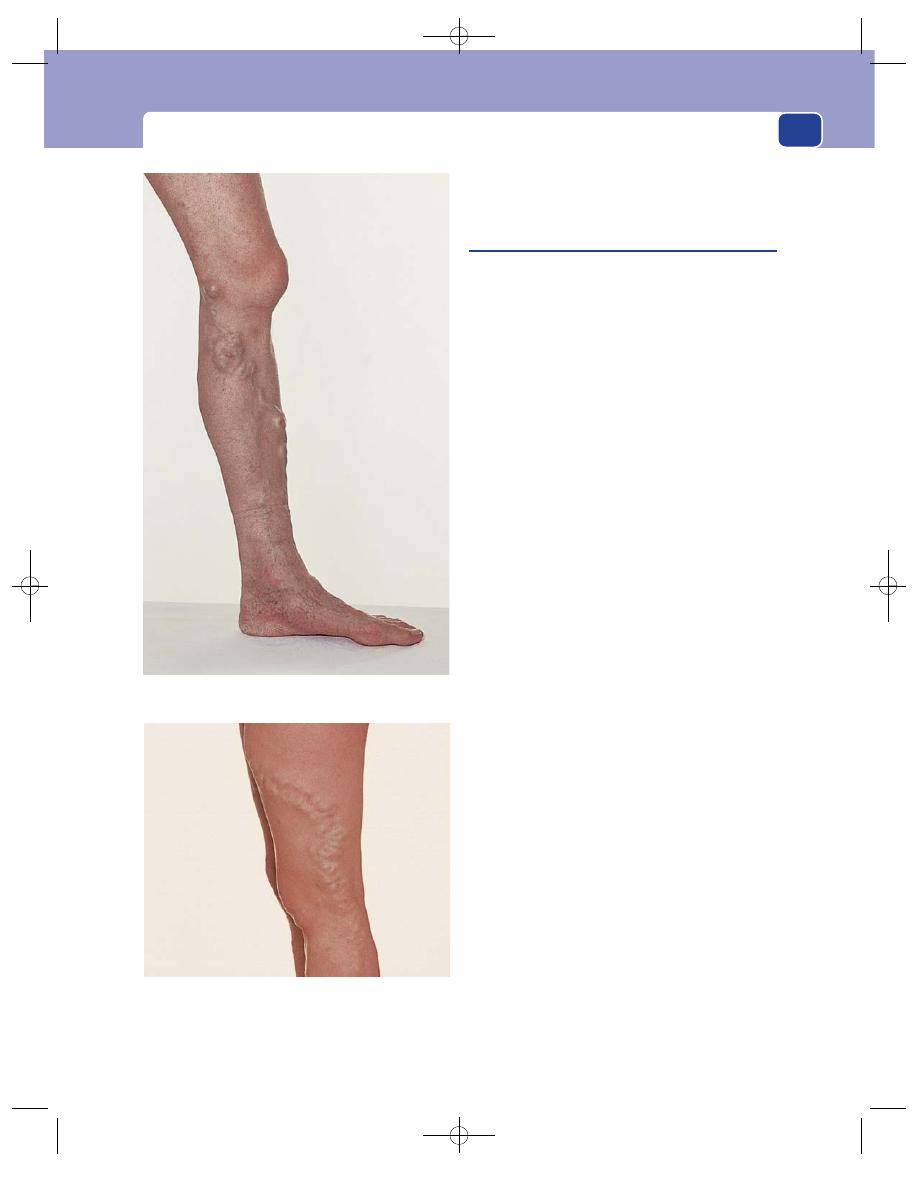
Clinical assessment of the venous circulation of the lower limb
201
deep vein flow abnormalities requires more sophisti-
cated Duplex scans.
Varicose veins
A varicose vein is a dilated, tortuous vein. The cause
of ‘primary’ varicose veins is unknown, but the erect
stance and abnormalities in the components and
structure of the vein wall may be important factors.
‘Secondary’ varicose veins may be secondary to
a proximal venous obstruction, destruction of the
valves by thrombosis or an increase in flow and
pressure caused by an arterio-venous fistula.
Varicosities do not cause symptoms, apart from
unsightliness. Symptoms are caused the physiologi-
cal malfunction that follows the valvular incompe-
tence and retrograde flow.
Consequently, many patients have massive vari-
cose veins but no symptoms, whilst others have severe
symptoms with very few visible varicose veins. To add
to the confusion, many patients with normal veins have
symptoms similar to those caused by venous disease.
History
Age
Varicose veins affect all age groups but are more
common in older people. In children they are usually
caused by a congenital vascular abnormality.
Sex
Ten times more women than men attend hospi-
tal with venous complaints, but surveys in the com-
munity have shown there is little difference in the
incidence of varicose veins between the sexes.
Ethnic groups
Varicose veins are said to be less com-
mon in Africa and the Far East than in Europe and
North America.
Occupation
Many patients with symptomatic vari-
cose veins have occupations that involve standing
for prolonged periods. It is doubtful if standing, by
itself, causes varicose veins, but it certainly exacer-
bates leg symptoms.
Symptoms
Many patients with varicose veins have
no symptoms. The disfiguring effect of the veins is
often the principal complaint.
The next commonest complaint is pain. This is
usually a dull ache felt in the calf and lower leg that
gets worse throughout the day, especially when the
FIG 7.14
Varicose veins are, by definition, dilated and
tortuous, and usually have incompetent valves. They occur
on both the medial and lateral sides of the leg.
Chap-07.qxd 4/21/05 12:50AM Page 201
The arteries, veins and lymphatics
202
patient is standing up for prolonged periods. It is
relieved by lying down for 15 or 30 minutes or by
wearing compression hosiery. The pain is often
experienced in the dilated varicosities.
Night cramps and itching are common com-
plaints.
Mild swelling of the ankle by the end of the day is
common, but marked ankle oedema is not, and other
causes of oedema should be eliminated before
accepting that it is caused by the varicose veins. Some
patients present with red, painful, tender lumps
caused by acute superficial thrombophlebitis (see
below).
Lipodermatosclerosis, eczema and ulceration
are important complications which indicate the
need for treatment. Always exclude conditions
which may obstruct the iliac veins and cause second-
ary varicose veins, such as pregnancy and abdominal
tumours.
Previous history
Most patients with varicose veins
have had them for years and many have had various
forms of treatment such as operations and injec-
tions. It is important to exclude a previous deep vein
thrombosis that may have accompanied previous
illnesses, operations, accidents or pregnancies. All
women should be asked if they had swelling of their
legs or a deep vein thrombosis during pregnancy.
Family history
It is common to find the patient’s
mother and sisters also have varicose veins. A definite
family history is obtained in one-third to one-half of
the patients who present with varicose veins.
Local examination
Inspection
Look for large visible veins. Record their
site, extent and size on large drawings of the front
and back of the limbs. The skin of the leg should be
inspected, especially the skin of the lower third of the
medial side of the calf, for signs of chronic venous
hypertension, lipodermatosclerosis, pigmentation,
induration and inflammation as well as eczema and
ulceration.
Palpation
Assess the texture of the skin and subcuta-
neous tissue of the lower leg by palpation. There
may be pitting oedema or thickening, redness and
tenderness. These changes are caused by chronic
venous hypertension and are known as lipoder-
matosclerosis, a term which indicates that there is a
progressive replacement of the skin and subcuta-
neous fat by fibrous tissue, induration and an asso-
ciated inflammation caused by the fibrin deposition
which proceeds the fibrosis.
Palpation along the course of the veins just behind
the medial border of the tibia may reveal defects in
the deep fascia where the communicating veins
pass from the superficial to the deep system.
Feel for a cough impulse and thrill in the groin
and in a dilated trunk of the short saphenous vein
behind the knee. This is easier if the fascia is relaxed
by slightly flexing the knee.
Percussion
Test whether a percussion impulse is con-
ducted up or, more significantly, down the main
superficial veins.
Auscultation
Listen over any large bunch of varicosi-
ties, especially if the veins do not collapse when the
patient lies down.
Tourniquet and Doppler flow detector tests
The Trende-
lenburg and tourniquet tests must be carried out to
detect the site of any incompetent superficial to deep
communicating veins. Confirm the presence of reflux
with the Doppler flow detector.
Revision panel 7.11
The causes of varicose veins in the lower limbs
Secondary
Obstruction to venous outflow by:
pregnancy
fibroids/ovarian cyst
abdominal lymphadenopathy
pelvic cancer (cervix, uterus, ovary, rectum)
ascites
iliac vein thrombosis
retroperitoneal fibrosis
Valve destruction
Deep vein thrombosis
High flow and pressure
Arterio-venous fistula (especially the
acquired traumatic variety)
Primary
Cause not known; often familial
Probably a weakness of the vein wall that
permits valve ring dilatation
Very rarely, congenital absence of valves
Chap-07.qxd 4/21/05 12:50AM Page 202
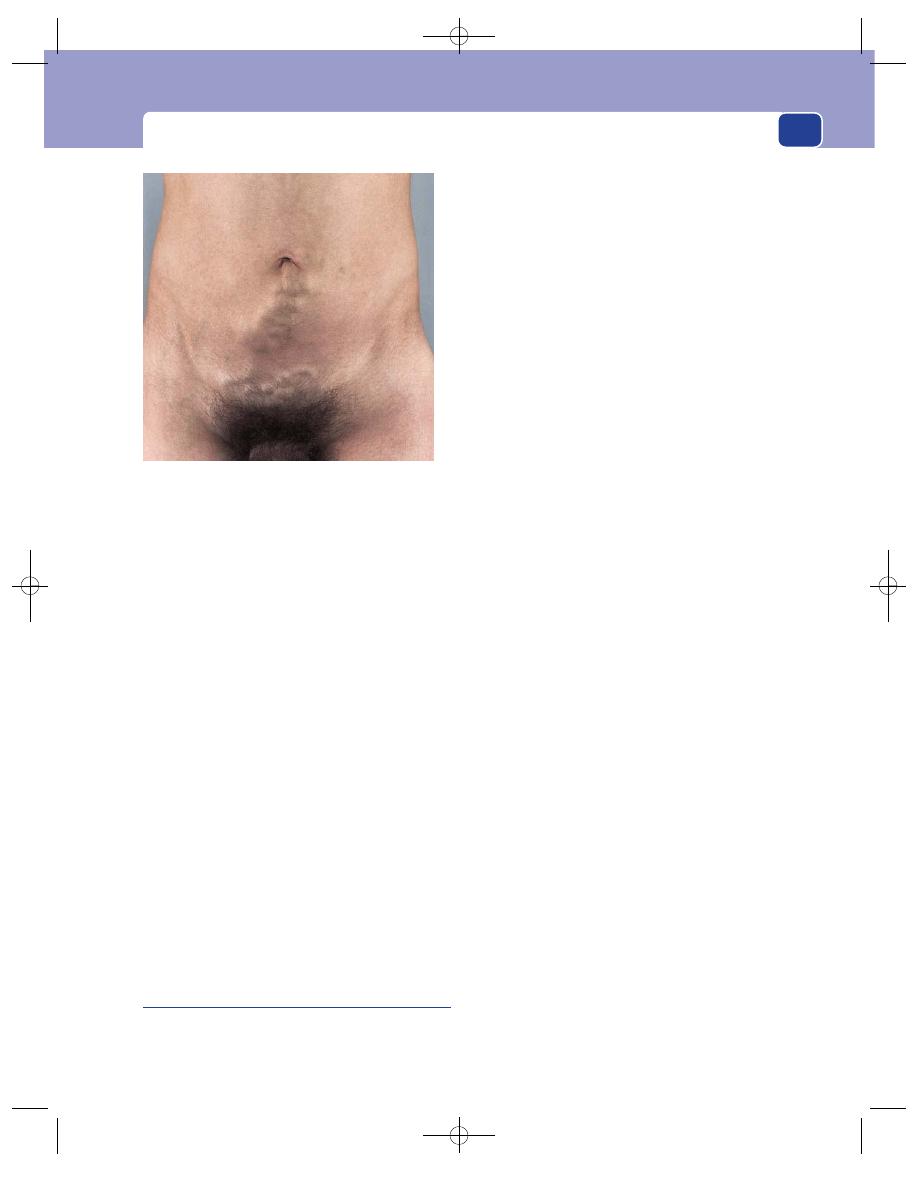
Clinical assessment of the venous circulation of the lower limb
203
General examination
Because varicose veins are so common, it is tempt-
ing to omit a full general examination. Never do
this. Always examine the abdomen and make sure
the patient is not pregnant.
Inspection of the abdomen may reveal dilated col-
lateral veins crossing to the other groin or up over the
abdomen and chest to join the tributaries of the supe-
rior vena cava. The direction of flow in these veins is
detected by placing two fingers on the veins, sliding
one finger along the vein to empty it and then releas-
ing the other finger and watching which way the
empty segment fills (Harvey’s test). This test may have
to be repeated moving the fingers in either direction
before the direction of blood flow can be confirmed.
A rectal or vaginal examination may be required
to exclude a pelvic or abdominal cause for the vari-
cose veins. In men it is important to feel the testes.
Massive enlargement of the abdominal lymph glands
by metastases from small testicular tumours can cause
inferior vena cava obstruction.
Venous ulceration
Many patients with venous ulcers do not have
visible varicose veins. Approximately 50 per cent of
all venous ulcers are associated with primary vari-
cose veins. The remainder are the result of post-
thrombotic deep vein damage (see below).
History
Age
Venous ulcers usually follow many years of
venous disease, so the majority are seen in patients
over the age of 40, many of whom have had recurrent
ulceration for some years before seeking medical
help. Post-thrombotic disease can cause ulceration in
young adults, and ulcers can occur in children and
teenagers with congenital venous malformations.
Sex
Venous ulcers are more common in women
than in men.
Symptoms
Patients have often had aching pain, dis-
comfort and tenderness of the skin (lipodermatoscle-
rosis and pigmentation) for many months or years
before an ulcer appears. Some ulcers are painful, but
many are not. The discharge may be very smelly,
leading to depression and social isolation. There is
often an episode of trauma that initiates the break-
down of the skin, but sometimes itching and
scratching may start an ulcer.
Previous history
A majority of venous ulcers are
caused by deep and communicating vein damage,
so there is often a history of venous thrombosis dur-
ing an illness or pregnancy. The patient may have
had previous episodes of ulceration.
Cause
The ulcer invariably begins after the skin of
the leg has been knocked and damaged. Sometimes
the initial incident is remembered, but often not.
Examination
Site
Venous ulcers are commonly found around the
gaiter area of the lower leg and usually begin on the
medial aspect. Ulcers situated lower down on the
foot or higher up on the fleshy part of the calf are
rarely caused by venous disease.
Shape and size
Venous ulcers can be of any shape and
any size.
Edge
The edge is gently sloping and, when healing
begins, pale pink as new epithelium migrates across
its surface.
Base
This may be covered with yellow slough but
becomes covered with pink granulation tissue when
FIG 7.15
Dilated, tortuous collateral veins crossing the
abdomen in a patient with an inferior vena cava thrombosis.
The common cause of inferior vena cava obstruction is
intra-abdominal malignant disease.
Chap-07.qxd 4/21/05 12:50AM Page 203

The arteries, veins and lymphatics
204
The ‘gaiter’ area. This photograph shows the medial aspect of
the lower third of the leg narrowed and hardened by venous
lipodermatosclerosis. This is the area in which most venous
ulcers develop.
Chronic venous insufficiency causes pigmentation of the skin
and dilated intradermal venules. The venules first appear in
a triangular area over and below the medial malleolus, with
the apex of the triangle over the first or second lower leg
communicating vein. This is known as the ankle-flare or
corona phlebectatica.
The pigmentation of chronic venous disease may cover the
whole of the lower limb.
Acute lipodermatosclerosis usually begins on the medial side
of the gaiter area and is painful, hot, red and tender. It is often
misdiagnosed as cellulitis or acute thrombophlebitis.
FIG 7.16
THE CUTANEOUS MANIFESTATIONS OF CHRONIC VENOUS INSUFFICIENCY.
Chap-07.qxd 4/21/05 12:50AM Page 204

Clinical assessment of the venous circulation of the lower limb
205
FIG 7.16
continued
Atrophie blanche is the name given to white scars in the
skin that appear without the skin ever having broken down or
ulcerated.
Subcutaneous fibrosis, following chronic lipodermatosclerosis,
and/or painful ulceration may cause a fixed flexion of the
ankle joint.
A chronic, recurrent, infected, enlarging venous ulcer. The
base contains little healthy granulation tissue and many
areas of avascular fibrous tissue.
A healing venous ulcer. The surrounding skin looks healthy,
the granulation tissue in the base of the ulcer is clean and
pink, and the edges of the ulcer are sloping and made of new
epithelium.
An acute venous ulcer. The surrounding lipodermatosclerosis
is clearly visible. In the acute stages, when tissues are dying
and sloughing, venous ulcers can be very painful.
Chap-07.qxd 4/21/05 12:50AM Page 205
The arteries, veins and lymphatics
206
the ulcer is healing. Areas of white fibrous tissue
may be seen between the granulations and there
may be more white fibrous tissue than granulation
tissue when the ulcer is very chronic and indolent.
The base is usually fixed to the deep tissues. Tendons
and the tibial periosteum may be exposed in the
base of the ulcer.
Depth
Venous ulcers are usually shallow and flat.
Discharge
The discharge is usually seropurulent but
can occasionally be blood stained.
Surrounding tissues
The surrounding tissues usually
show the signs of chronic venous hypertension –
induration, inflammation, pigmentation and tender-
ness, i.e. lipodermatosclerosis. There may be old
white scars (atrophie blanche) from previous ulcera-
tion and many dilated intradermal and subcutaneous
veins. Movements of the ankle joint may be limited
by scar tissue, which may cause an equinus deformity
of the joint. Occasionally true cellulitis occurs.
Local lymph glands
Ulcers are usually colonized rather
than infected, so the inguinal lymph glands should
not be enlarged or tender.
Remember that squamous cell carcinoma can
arise in a chronic venous ulcer, particularly in a
patient known to have a long-standing venous ulcer
which has enlarged, become painful and malodorous,
and especially if the edge of the ulcer is found to be
raised or thickened. Malignant change is also sug-
gested by finding enlarged inguinal lymph glands.
Biopsy is indicated should any of these changes appear.
Malignant change in a chronic venous ulcer is
known as a Marjolin’s ulcer (see Chapter 3, page 94).
The lower limbs
The whole of both lower limbs must be
examined for the presence of varicose veins, compe-
tent and incompetent communicating veins and skin
changes, as described above. Most patients have bilat-
eral disease and the majority of patients with venous
ulcers have incompetent communicating veins.
It is also important to assess the arterial circula-
tion and the nerves, to exclude an ischaemic or neu-
ropathic cause of the ulcer.
General examination
The abdomen should be examined to exclude an
abdominal cause of venous insufficiency, and the
other leg should be examined for signs of venous
disease.
Look for any general features of the many other
causes of skin ulceration such as ischaemia, rheuma-
toid arthritis, skin tumours, pyoderma gangreno-
sum, collagen diseases, anaemia, polycythaemia,
neuropathic ulcers and sickle cell disease.
Deep vein thrombosis
Only a quarter of deep vein thromboses cause symp-
toms and signs. Many occur spontaneously, but in
more than half there is a predisposing cause such as an
operation, bed rest, thrombophilia, or recent air travel.
History
Patients complain of pain and swelling in the calf
or the whole leg. The onset of symptoms is sudden
and they are usually severe enough to make walking
difficult. The first indication may be a pulmonary
embolism, which causes symptoms such as pleuritic
pain, breathlessness, haemoptysis and collapse.
Examination
Swelling of a leg, particularly if it is unilateral, is the
most significant physical sign. The ankle may be the
only site of swelling if the thrombosis is confined to
the calf. Swelling of both ankles needs to be differ-
entiated from other causes of oedema.
The swelling may extend up to the groin if the
iliac vein is thrombosed.
The muscles that contain the thrombosed veins
may become hard and tender. A change in texture of
the muscle is more significant than tenderness
because, although there are many conditions that
make a muscle tender, there are few that make it stiff
and hard.
Stretching the calf muscles by forced dorsiflexion
is known as Homan’s sign. This sign is a poor dis-
criminator and should be abandoned.
The superficial veins may be dilated and the leg
may feel hot. A large, swollen limb that is made pale
by severe oedema is called phlegmasia alba dolens.
When the venous thrombosis blocks almost all the
main outflow veins, the skin of the leg becomes con-
gested and blue. This is called phlegmasia caerulea
dolens.
Venous gangrene can develop when there is
very severe venous outflow obstruction. Venous
gangrene usually affects the peripheral tissues (toe
or fingers).
Chap-07.qxd 4/21/05 12:50AM Page 206
Clinical assessment of the venous circulation of the lower limb
207
Chest signs
If the patient has had a pulmonary
embolus, the neck veins may be dilated and there
may be central cyanosis and signs of right ventricu-
lar hypertrophy. A fixed-split second heart sound
may be heard and there may be a pleural rub.
The post-thrombotic limb
The symptoms and signs that follow the damage
caused by a deep vein thrombosis – obstruction and
valvular incompetence – may appear months or
years after the thrombosis. The initiating thrombo-
sis may have passed unrecognized, but more often it
produced clinical signs and required treatment. The
earliest symptoms are usually a slowly progressive
swelling of the leg that becomes painful as the day
wears on. Initially the skin of the gaiter area
becomes pigmented, but eventually it becomes a
hard inflamed, indurated, pigmented plaque (lipo-
dermatosclerosis). These changes may spread
around the whole circumference of the gaiter area.
Varicose veins become more prominent and, if
the thrombosis obstructs the venous outflow at the
base of the limb, collateral veins may develop across
the groins and the pubis, and the superficial veins
will not empty when the patient is asked to carry
out heel-raising on the spot with a mid-thigh
tourniquet in place (Perthes’ test).
A small group of patients develop true venous
claudication. This is a severe calf and sometimes
thigh pain caused by walking. It must be differenti-
ated from intermittent claudication caused by arte-
rial insufficiency. These patients usually have a
swollen, tender limb, multiple varicose veins, collat-
eral veins and lipodermatosclerosis, all indicating
the likelihood of a previous deep vein thrombosis.
The pain of venous claudication is usually accom-
panied by an increase of the swelling, and the pain
fades very slowly.
Superficial thrombophlebitis
Deep vein thrombosis begins in normal veins, the vein
wall becoming secondarily inflamed. In superficial
thrombophlebitis, the inflammation of the vein wall
is invariably the cause of the thrombosis.
The causes of superficial thrombophlebitis are
given in Revision panel 7.12.
An occult carcinoma should be suspected when
the episodes occur in the arms of patients over the
age of 45 years, especially if they are transient and
migrate. Thrombophlebitis migrans is, however, a
rare condition.
History
Patients complain of the sudden appearance of a
painful lump on their arm or leg. The pain usually
subsides in 3–7 days, leaving a tender lump or subcu-
taneous cord which takes several weeks to disperse.
There may be a preceding injury such as a venepunc-
ture or, if the vein is varicose, a direct injury.
Examination
The swelling is in the subcutaneous tissues. It has an
elongated, cord-like shape and may be several cen-
timetres long, running along the long axis of the
limb. The lump is tender. The overlying skin is at
first red and inflamed before becoming pigmented
and brown. Enlargement of the local lymph glands
is rare and other tissues in the limb are normal, unless
the condition is secondary to varicose veins.
The whole patient must be examined for an
occult carcinoma, even if they have varicose veins.
Axillary vein thrombosis
Thrombosis of the axillary/subclavian vein may fol-
low excessive use of the limb, especially above the
head, or compression of the vein by musculoskeletal
abnormalities such as a cervical rib.
Revision panel 7.12
The causes of superficial thrombophlebitis
Varicose veins
Occult carcinoma
Bronchus
Pancreas
Stomach
Lymphoma
Thromboangiitis obliterans (Buerger’s disease)
Polycythaemia
Polyarteritis
Idiopathic
Iatrogenic
Intravenous injection and injuries
Chap-07.qxd 4/21/05 12:50AM Page 207
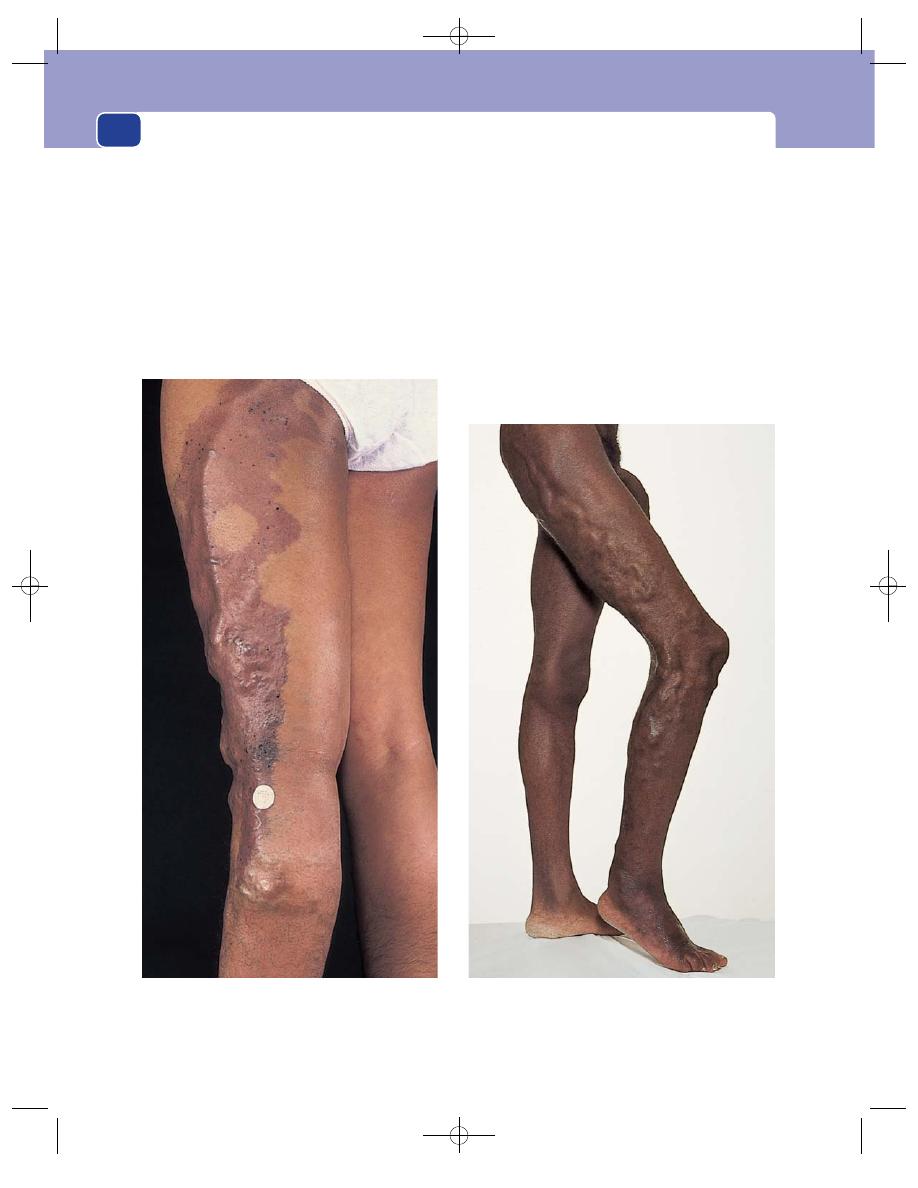
The arteries, veins and lymphatics
208
History
The patient complains of a sudden discomfort and
swelling of the arm. The arm, forearm and hand
swell up, and there is discomfort on the medial side
of the upper arm and in the axilla. The arm may feel
hot and if it becomes very swollen, movements may
become restricted. The patient may give a history of
unusual activity in the preceding 24 hours, such as
painting a ceiling.
Examination
The whole arm is swollen, congested and blue, and
the surface veins usually distended. When the hand is
raised above the level of the heart, the veins at the
back of the hand do not collapse. The axillary vein
may be palpable and tender. Distended cutaneous
veins develop across the anterior chest wall and over
the scapula to provide collateral drainage. The supra-
clavicular fossa must be carefully palpated to exclude
a causative mass such as a cervical rib, a subclavian
aneurysm, or lymph glands enlarged by secondary
malignant disease.
FIG 7.17
CONGENITAL VARICOSE VEINS.
The dilated, anatomically abnormal varicose veins of a
congenital venous deformity. There are also patches of
port-wine staining.
This patient had the abnormal dilated veins on the lateral side
of the leg typical of the Klippel–Trenaunay syndrome, with
marked overgrowth of the length and circumference of the leg.
Chap-07.qxd 4/21/05 12:51AM Page 208
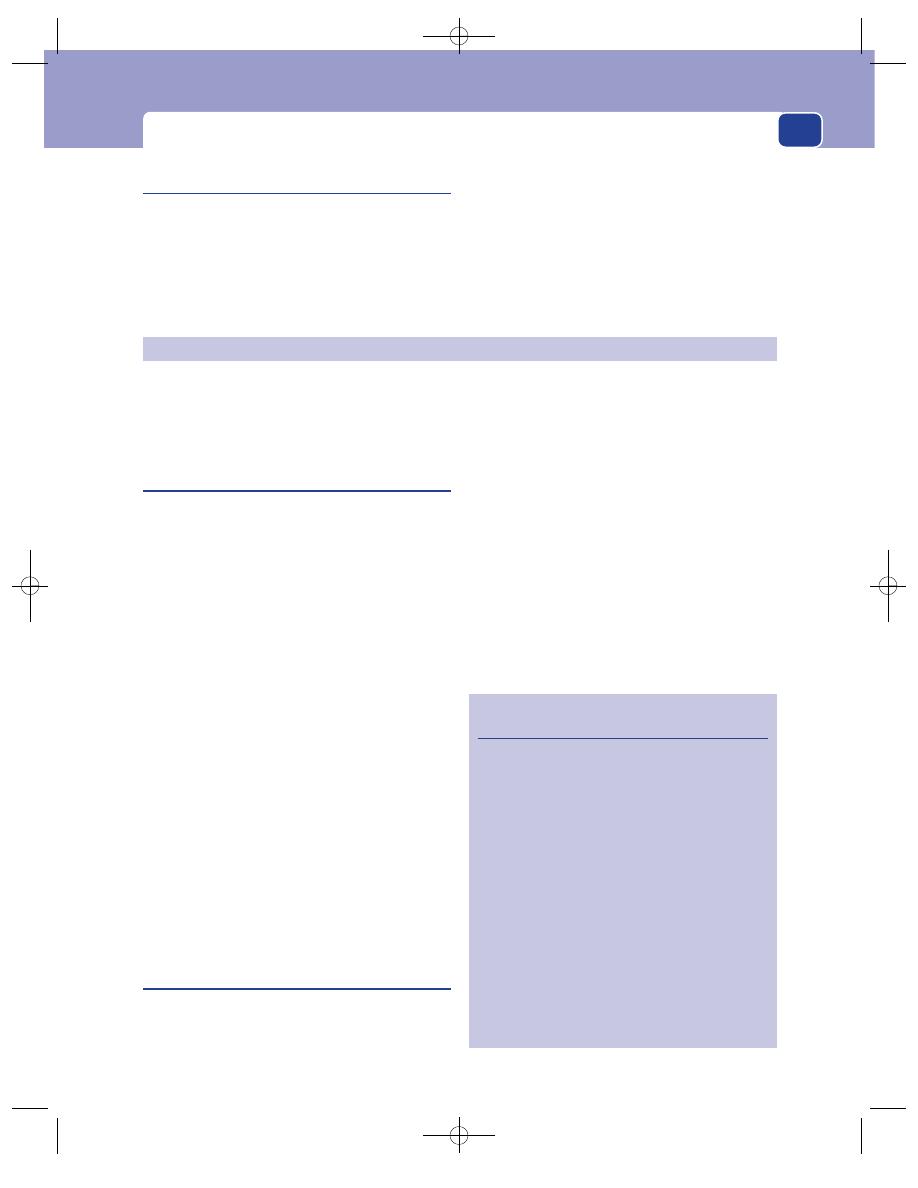
The lymphatics
209
Primary abnormalities of the lymphatic vessels are
rare. Disease in the lymph glands that interrupts the
flow of lymph is common.
Lymphangitis
When bacterial infection spreads through the tis-
sues, the bacteria get into the lymphatics and pass
along in the lymph to the draining lymph glands.
Inflamed lymphatics close to the skin are visible as
thin, tender, red streaks on the skin. Lymphangitis is
most often seen as a complication of infection start-
ing in the hands or feet.
History
The patient complains of a throbbing pain at the
site of the primary infection, tenderness along the
red streaks and tenderness in the groin or axilla.
Examination
Inspection of the limb reveals the red, tender
lymphatics. The overlying skin may be slightly
oedematous. The axillary or inguinal lymph glands
are usually swollen and tender.
The site of the primary infection is often not
obvious. It may be a small crack between the toes or
alongside a finger nail.
If a lymph gland in an oedematous limb with
poor lymphatic drainage becomes infected, the
infection quickly spreads throughout the oedema-
tous tissues – cellulitis.
Lymphoedema
Lymphoedema is the accumulation of lymph in the
interstitial spaces as a consequence of defective lym-
phatic drainage. The oedema fluid is rich in protein,
in contrast to the oedema of heart and kidney fail-
ure, which has a low protein content.
The causes of lymphoedema are given in Revision
panel 7.13.
The commonest cause of lymphoedema is sec-
ondary disease in the lymph glands. Primary lym-
phoedema is only diagnosed when all the causes of
secondary lymphoedema have been eliminated, or
there is a clear family history of the condition.
History
Age
Primary lymphoedema may present at birth, in
young adults or, much less often, in middle age.
Secondary lymphoedema presents in middle and old
age and is common after treatment for cancers.
Congenital vein abnormalities
Klippel–Trenaunay syndrome
This is a rare syndrome in which dilated veins
develop early in life, often on the outer side of the
leg, which is longer than the normal leg and covered
in cutaneous angiomata (port-wine stains).
Venous angiomata
These are localized hamartomatous overgrowths of
small to middle-sized veins. They mostly occur in the
subcutaneous tissues and skin. They have a blue dis-
colouration and become distended when dependent,
collapse on elevation and are compressible.
THE LYMPHATICS
Revision panel 7.13
The causes of lymphoedema
Primary
Congenital genetic disorders causing
dilatation, incompetence, aplasia or
obliteration of the lymphatics
Secondary
Neoplastic infiltration of lymph glands by:
secondary carcinoma
lymphomas (Hodgkin’s/non-Hodgkin’s)
Infection
Filariasis
Lymphogranuloma inguinale
Tuberculosis
Recurrent non-specific infection
Iatrogenic
Surgical excision of lymph glands
Irradiation of lymph glands
Chap-07.qxd 4/21/05 12:51AM Page 209
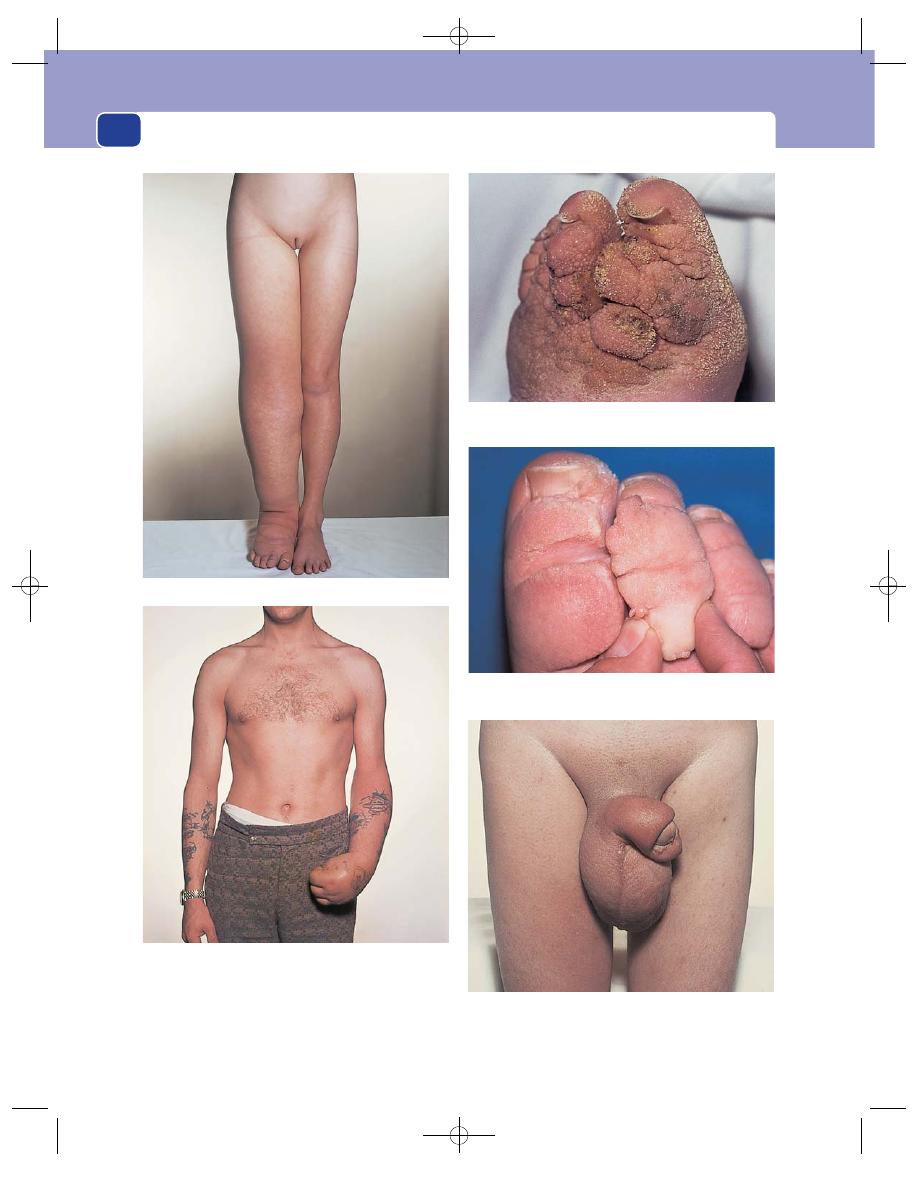
The arteries, veins and lymphatics
210
FIG 7.18
LYMPHOEDEMA.
Lymphoedema of the right leg.
Severe long-standing lymphoedema. The skin is thickened
and hyperkeratotic.
‘Hysterical’ oedema. Immobility and dependency, in this
case caused by a ‘hysterical’ paralysis, can cause severe
oedema. This is not a true lymphoedema, but a gravitational
oedema. The limb is often bluish in colour because of the
concomitant venous congestion – hence the name hysterical
oedeme blue.
Genital lymphoedema. This usually affects the penis and
scrotum but may be confined to the scrotum. In about 50 per
cent of patients there is also mild lymphoedema of the legs.
Stemmer’s sign. An inability to pinch the skin together on the
dorsum of the toes.
Chap-07.qxd 4/21/05 12:51AM Page 210
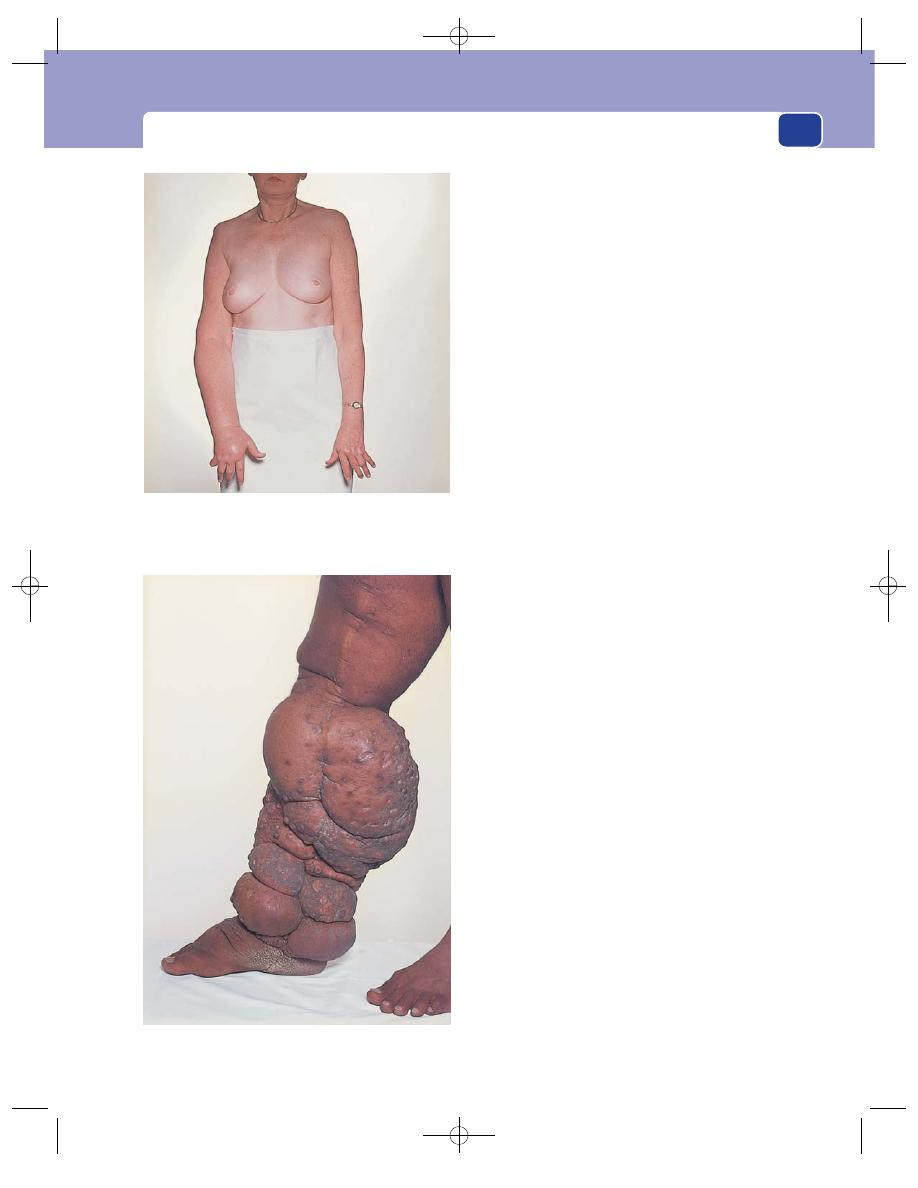
The lymphatics
211
Family history
Many forms of primary lymphoedema
are familial, and abnormal genes have now been dis-
covered in several of them.
Sex
Females are affected three times more often
than males. Even secondary lymphoedema is more
common in women, because tumours of the uterus
and ovary metastasize to the iliac lymph glands, and
carcinoma of the breast spreads to the axillary
lymph glands.
Geography
Filariasis – infestation with the parasite
Wuchereria bancrofti, which is found in tropical and
sub-tropical countries – is a common cause of lym-
phoedema (elephantiasis).
Symptoms
The patient notices a slowly progressive
swelling of
the limb or genitalia. Primary
lymphoedema most often affects the lower limb,
often beginning after a sprained ankle or another
form of trivial injury. The swelling takes many years
to develop and is often bilateral.
In contrast, the swelling of secondary lym-
phoedema may appear in a few weeks and may
progress rapidly.
The swelling is not painful
There is no discomfort in
the swollen limb apart from that caused by the
increased weight, which may produce a mechanical
disability.
Patients with lymphoedema often develop severe
episodes of acute cellulites, which may be accompan-
ied by septicaemia. Acute cellulitis is often preceded by
a prodromal period of sweating, rigors and malaise,
which is then followed by the development of pain,
tenderness, redness and swelling in the limb. The
infection often gets in through cracks between the toes
caused by athlete’s foot (Tinea pedis). Vesicles may
appear on the skin and leak a clear, colourless fluid.
Examination
The swollen limb
Lymphoedema has no special characteristics. It is
often said that lymphoedema does not pit – this is
incorrect. All oedema pits. The longer the lym-
phoedema has been present, the denser the accom-
panying fibrosis and the firmer and more ‘doughy’
the oedema; nevertheless, lymphoedema always pits
if you press hard enough and long enough.
Lymphoedema of the lower limb affects the toes
much more often than other forms of oedema. If it
Secondary lymphoedema. This patient’s right arm
lymphoedema was caused by infiltration of the axillary lymph
glands by metastases from a carcinoma in the right breast.
Some carcinomata of the breast present in this way.
Long-standing gross lymphoedema– elephantiasis.
FIG 7.18
continued
Chap-07.qxd 4/21/05 12:51AM Page 211

The arteries, veins and lymphatics
212
has been present for years, the toes are squashed
together and become square in cross-section. This
hardly ever occurs with other types of oedema.
Stemmer’s sign is an inability to pinch the skin
together on the dorsal surface of the second toe.
This indicates the presence of lymphoedema and is
a consequence of secondary thickening and hyper-
keratosis of the skin. Sometimes thick scales grow
outwards, looking like warts.
Lymphoedema is usually diagnosed when other
general causes of oedema (cardiac, renal, hypopro-
teinaemia) and other local causes (venous obstruction,
multiple arterio-venous fistulae, local gigantism
and excessive fat deposition – lipodystrophy) have
been excluded. It is therefore essential to examine
the whole patient once the presence of oedema has
been confirmed, especially the heart, the abdomen
and the veins of the limb.
The lymph glands
The lymph glands are often slightly thickened and
enlarged in patients with primary lymphoedema.
They will almost certainly be enlarged and hard
if they are infiltrated with primary or secondary
tumour.
All the areas that drain to any palpable glands
must be carefully examined.
General examination
A full examination of the patient must be carried
out to look for any possible causes for secondary
lymphoedema.
Post-mastectomy oedema
Swelling of the arm is a common complication of any
form of mastectomy or combination of lumpectomy
and radiotherapy which damages or removes the
axillary lymph glands.
Oedema which develops in the first days or
weeks after the initial treatment is likely to be an
axillary vein thrombosis.
Swelling after this time may be caused by scar tis-
sue constricting the axillary vein, especially if it pro-
gresses rapidly.
Though lymphoedema caused by obliteration of
the lymphatics can appear within months or many
years after the initial treatment, it is always possible
that late swelling may be caused by recurrent carci-
noma, especially if there is any enlargement of the
axillary lymph glands.
Lymphatic reflux
A relatively small number of patients have dilated
ecstatic incompetent lymphatics that allow lymph
and chyle (which is the milky lymph draining from
the intestine) to reflux back into the skin, or drain
into large cavities such as the peritoneum, pleura or
intestine. Patients with lymphatic reflux can develop
leaky vesicles on their skin, ascites and pleural
effusions and may even pass chyle in their urine
(chyluria).
Lymphangiomata
These are rare malformations with distinct clinical
features that are easy to recognize.
History
A patient or, in the case of a child, the parents first
notice a small soft subcutaneous swelling. Sometimes
there may be associated small vesicles on the surface
of the skin which may weep clear fluid. These abnor-
malities may be present at birth or appear later in life.
The subcutaneous swellings slowly enlarge and the
vesicles increase in number, but neither are usually
painful.
Examination
The skin over the subcutaneous cysts usually con-
tain many small vesicles. Lymphangiomata tend to
Revision panel 7.14
The causes of lymphadenopathy
Infection
Non-specific
Glandular fever
Tuberculosis
Toxoplasmosis
Syphilis
Cat-scratch fever (Rochalimaea henselae)
Filariasis
Lymphogranuloma (inguinale)
Metastatic tumour
Primary reticuloses
Sarcoidosis
Chap-07.qxd 4/21/05 12:51AM Page 212
The lymphatics
213
occur at the junction of the leg, arm or neck with
the trunk.
The subcutaneous swellings cannot be com-
pressed or emptied. They are often indistinct and
multiple. They fluctuate and transilluminate if they
are of a reasonable size, and have the same signs as a
cystic hygroma (see Chapter 11, page 281).
Lymphadenopathy is described in the chapter
on the neck (Chapter 11), but as lymphoedema is so
often secondary to lymph gland disease, you should
refresh your knowledge of the causes of lymph
gland enlargement (see Revision panel 7.14).
Chap-07.qxd 4/21/05 12:51AM Page 213
(Scalp, head, eyes, nose, ears and chest wall)
COLOUR
One of the first things that one notices about a
patient is the colour of their skin: not their racial
colour, though it is important to record their racial
origin, but changes from what you would expect to
be their normal colour. Although minor colour varia-
tions are easier to appreciate in white-skinned
people, they are also visible in dark-skinned races.
The skin may be pale or tinged blue, yellow or
brown.
Pallor
Normal skin colour varies according to the thickness
of the skin, the state of the skin circulation and the
degree and type of pigmentation. If the skin thickness
and circulation appear to be normal, pallor of the skin
usually indicates anaemia. Anaemia is best detected
by looking at the colour of the mucous membranes.
■
Look at the colour of the conjunctiva on the
inner side of the lower eyelid.
■
Look at the colour of the buccal mucous
membrane.
■
Stretch the skin of the palm and look at the
colour of the palmar creases.
Cyanosis
Cyanosis is the purple-blue colour given to the skin by
de-oxygenated blood. It is most apparent in areas with
thin skin but a rich blood supply, such as the lips,
tongue, finger nails and ear lobes. Cyanosis is difficult
to see in black skin and when the patient is anaemic.
The causes of cyanosis can be divided into two
categories: central, when the defect lies in the car-
diopulmonary circulation, and peripheral, when
there is excessive de-oxygenation in the tissues, usu-
ally because of inadequate tissue perfusion.
If the cyanosis is caused by a central abnormality,
it will be generalized and the patient’s extremities
are likely to be warm.
If the cyanosis is caused by a peripheral abnor-
mality, the extremities will be blue and cold, but
central organs such as the tongue will be pink.
Polycythaemia
An excess of circulating red blood cells gives the
patient a purple-red, florid appearance. This may
be mistaken for cyanosis. It differs from cyanosis in
that it heightens the colour of all the skin, especially
the cheeks, neck and backs of hands and feet. The
discolouration of cyanosis is usually limited to the
tips of the hands, feet and nose.
Jaundice
Jaundice is a yellow discolouration of the skin, caused
by an excess of bile pigments in the plasma.
The yellow colour is first visible against the white
background of the sclera, but as the jaundice
increases, the whole skin turns yellow.
The colour changes with the depth of the jaun-
dice. White skin first turns a pale lemon yellow. As
it deepens, it becomes yellow-orange, sometimes
almost brown, and in those rare conditions in which
severe jaundice may exist for many years, such as
biliary cirrhosis, the skin eventually turns a yellow-
grey-green colour.
It is not possible to diagnose the cause of jaun-
dice from its presence. The most useful diagnostic
features are the sequence of events preceding its
onset and the presence or absence of pain.
Jaundice can be caused by excessive haemolysis –
pre-hepatic jaundice; by liver malfunction – hepatic
jaundice; or by obstruction of the bile ducts –
post-hepatic jaundice.
Chap-08.qxd 4/19/05 14:12PM Page 214
Colour
215
The common causes of these three types of jaun-
dice are:
■
pre-hepatic jaundice – haemolytic anaemia,
■
hepatic jaundice – infectious hepatitis,
■
post-hepatic jaundice – gallstones and
carcinoma of the pancreas.
Figure 8.1 describes the principal premonitory
symptoms, pain and fluctuations of jaundice that
accompany the common diseases that cause jaundice.
Brown pigmentation
An increase in the natural brown pigmentation of
the skin can be generalized or localized.
Causes of generalized pigmentation
■
Addison’s disease is the important cause of
increased pigmentation to remember, because if
it is not diagnosed and treated, it can cause
sudden death. The brown pigmentation of
Addison’s disease is visible in the buccal mucous
membrane.
■
Arsenic and silver poisoning.
■
Haemochromatosis.
■
Gaucher’s disease.
Causes of localized pigmentation
■
Pregnancy: round the areolae and along the
mid-line of the abdomen.
■
Chronic venous hypertension: lower medial
third of the lower leg.
■
Erythema ab igne: frequently seen on parts of
the legs exposed to heat.
■
Ultraviolet and high-voltage irradiation.
■
Café au lait patch: associated with
neurofibromatosis.
■
Various forms of melanoma.
■
Pellagra: nicotinic acid deficiency.
■
Rheumatoid arthritis.
■
Acanthosis nigricans.
Vitiligo
Vitiligo is the name given to white, de-pigmented
areas of skin. It commonly occurs without a gen-
eralized cause, but it can be secondary to leprosy,
scleroderma, syphilis, and some organ-specific
autoimmune diseases such as Hashimoto’s thy-
roiditis, Addison’s disease, pernicious anaemia and
diabetes.
Excoriation/pruritus
This is itching of the skin caused by a local or gen-
eral abnormality. The presence of multiple scratches
on the skin is usually very obvious and noticed dur-
ing your initial inspection. Itching of the skin is
caused by:
■
skin diseases:
urticaria
eczema
(psoriasis does not usually cause itching)
■
local irritation:
clothing/washing powder
parasites – fleas, scabies
discharges – vaginal and rectal
■
occult disease:
subclinical jaundice with bile salt retention
Hodgkin’s disease
leukaemia
uraemia
food sensitivity
polycythaemia
thyrotoxicosis.
If a skin disease or local irritation is the initiating
stimulus, the cause of the pruritis and excoriation
is usually obvious on inspection, so the causes
to remember are the occult diseases. Any patient
presenting with an itching, but otherwise normal,
skin should be suspected of having subclinical
jaundice, Hodgkin’s disease or uraemia until you
prove otherwise.
Revision panel 8.1
Causes of a generalized increased skin
pigmentation
Sunlight
Pregnancy
Addison’s disease
Renal failure
Haemochromatosis
Drugs (e.g. busulphan)
Chap-08.qxd 4/19/05 14:12PM Page 215
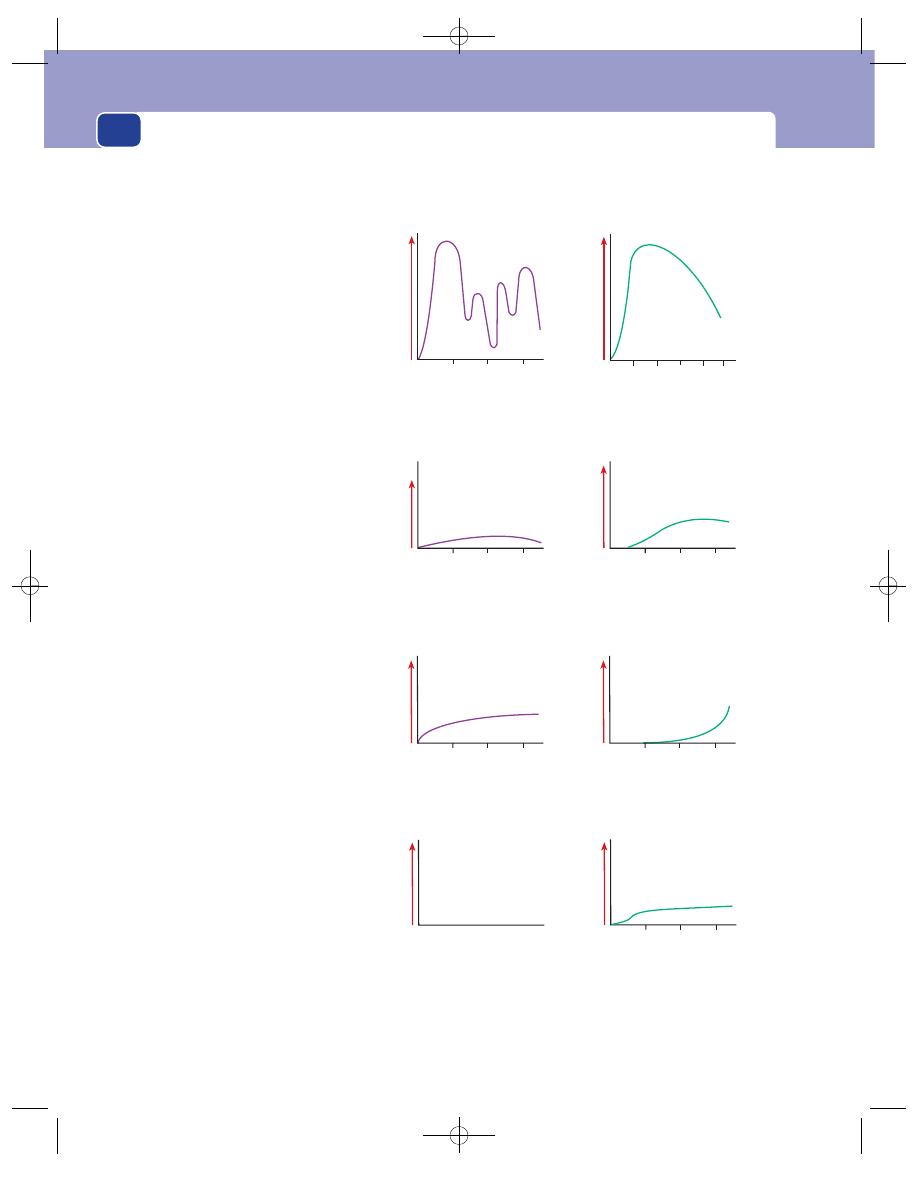
General and facial appearance
216
Disease
Premonitory
symptoms
Jaundice
Pain
Haemolytic
anaemia
General malaise
Breathlessness
Loss of weight
Slow onset and
persists
Severity
2
4
6
Years
No pain
Severity
Carcinoma
of head
of pancreas
Loss of appetite
and weight
Itching skin
Steady increase
Months
Severity
3
2
1
Backache
Severity
3
2
1
Months
Infectious
hepatitis
Loss of appetite
Malaise, nausea
Gradual onset and
disappearance
Weeks
Severity
3
2
1
Dull ache
Severity
3
2
1
Weeks
Gallstones
Episodes of indigestion
or flatulent dyspepsia
Itching skin
Sudden onset
Fades slowly in days
Days
Severity
10
8
6
4
2
Intermittent and
severe
Severity
Hours
3
2
1
FIG 8.1
THE DISTINGUISHING FEATURES OF THE FOUR COMMON DISEASES THAT CAUSE JAUNDICE
Chap-08.qxd 4/19/05 14:12PM Page 216
General appearance
217
GENERAL APPEARANCE
When you look at a patient’s size, shape and phys-
ical characteristics you will subconsciously put them
into one of four categories: their body will look
normal, wasted, overweight, or have some skeletal
or sexual characteristics that look out of proportion.
The following sections describe the principal con-
ditions that cause these three changes in body build.
Wasting
There are many causes of wasting. Almost all seri-
ous diseases cause some loss of appetite and weight,
so only the common conditions are listed in Revision
panel 8.3.
Severe wasting of the upper half of the body with
oedema of the lower half is a common physical
appearance in the elderly and is usually caused by
advanced carcinoma which has either destroyed the
liver and so caused hypoproteinaemia or formed large
intra-abdominal masses which have obstructed the
vena cava or iliac veins.
The degree of wasting is apparent from the way in
which the skeleton, particularly the shoulder girdle,
and the folds of loose skin on the arms, trunk and
buttocks become visible.
This clinical picture can also be caused by the com-
bination of two diseases: a disease which causes wast-
ing, such as carcinoma, and congestive heart failure.
Although you should always try to make one diagno-
sis, many elderly people have more than one disease.
Overweight
Patients with normal skeletal and sexual proportions
but whose bodies are bigger than they should be are
most likely to be obese from overeating, but three
serious pathological conditions cause an increase in
weight that can easily be mistaken for obesity: water
retention, myxoedema and Cushing’s syndrome.
Water retention
Nephrosis and other causes of water retention
(renal, cardiac or hepatic) cause an increase in
weight. The whole body swells but the swelling is
most noticeable in the dependent parts. These
patients have oedema of the legs, or the sacral
region if they have been confined to bed, but also in
the loose tissues of the face, especially in the skin
below the eyes. The swelling around the eyes is often
the first symptom and is present when the patient
wakes up. Cardiac oedema is also most apparent in
the dependent parts and similarly tends to disperse
to other areas (not resolve) at night in response to
the change of body position.
Revision panel 8.2
The common causes of itching
General
Cholestasis (subclinical jaundice)
Hodgkin’s disease
Lymphoma
Renal failure (uraemia)
Food sensitivities
Iron deficiency
Polycythaemia
Skin disease
Infestations (e.g. scabies)
Insect bites
Eczema
Urticaria
Prickly heat
Clothing/washing powder sensitivities
Revision panel 8.3
The common causes of wasting
In children
Severe gastroenteritis
Malabsorption syndromes
In young adults
Tuberculosis
Reticuloses
Anorexia nervosa
In middle age
Diabetes
Thyrotoxicosis
Carcinoma
In old age
Carcinoma
Senility
Gross cardiorespiratory disease
All age groups
Starvation
Chap-08.qxd 4/19/05 14:12PM Page 217

General and facial appearance
218
Myxoedema
Myxoedema, which is caused by a deficiency of thy-
roid hormone, causes a puffy face, a generalized,
non-pitting increase in the subcutaneous tissues of
the trunk and limbs, a ‘peaches and cream’ com-
plexion and a dulling of thought, speech and action
(see pages 301–3).
Cushing’s syndrome
Cushing’s syndrome is caused by an excess of adrenal
glucocorticoids. One in four patients with Cushing’s
syndrome has an adrenal adenoma; the remainder
have a pituitary abnormality, either an adenoma or
excess hypothalamic stimulation.
The patient puts on weight, particularly on the face,
neck and trunk. The arms and legs stay thin. The face
becomes ‘moon-shaped’ and the rounded, thickened
shoulders are often described as a ‘buffalo hump’.
There is excess of lanugo hair, an increase in skin
pigmentation and red (fresh) striae in the skin that
has been stretched, particularly the skin of the
abdomen. Hypertension is common.
Revision panel 8.4
The common causes of an increase in weight
Obesity
Pregnancy
Interstitial fluid retention (renal, cardiac or
hepatic failure)
Localized fluid retention (massive ovarian cysts,
ascites)
Myxoedema
Cushing’s syndrome
FIG 8.2
Gross obesity usually affects the whole body, but
may, as in this patient, be predominantly confined to the
buttocks and thighs.
FIG 8.3
This woman has myxoedema. There is some loss of
hair, especially the outer third of the eyebrows, heaviness of
the face and creamy skin, but none of these features is
diagnostic. This photograph is included to emphasize that
early myxoedema is extremely difficult to recognize (see also
Fig. 11.39, page 302).
Chap-08.qxd 4/19/05 14:12PM Page 218

General appearance
219
Skeletal or sexual disproportion
There are a variety of skeletal abnormalities and a few
rare disorders of general body development usually
associated with chromosomal abnormalities that will
be apparent from your initial general inspection.
Paget’s disease of bone
(Osteitis deformans, see page 119)
This is a disease in which normal bone is absorbed
and replaced by primitive vascular (osteoid) bone.
This makes the bones thick but soft.
The skull enlarges. The bones of the vault bulge
outwards above the eyes and ears so much that the
patient may complain that they have had to buy a
larger hat.
The spine bends into a marked kyphosis which
reduces the patient’s height and may make respiration
difficult. The bending of the spine makes the arms
look longer.
The long bones of the limbs become thicker and
curve forwards and outwards.
FIG 8.4
CUSHING’S SYNDROME.
An increase of fat on the trunk and shoulders but thin arms
and legs. Red striae on the abdomen and breasts.
A round ‘moon’ face, some early hypertrichosis and an
unusually florid acneiform rash.
Revision panel 8.5
The common causes of hair loss
Local
Male balding
Alopecia areata
Skin infections
General
Hypothyroidism
Cytotoxic drugs
Hypopituitarism
Iron deficiency
Severe illness
Chap-08.qxd 4/19/05 14:13PM Page 219
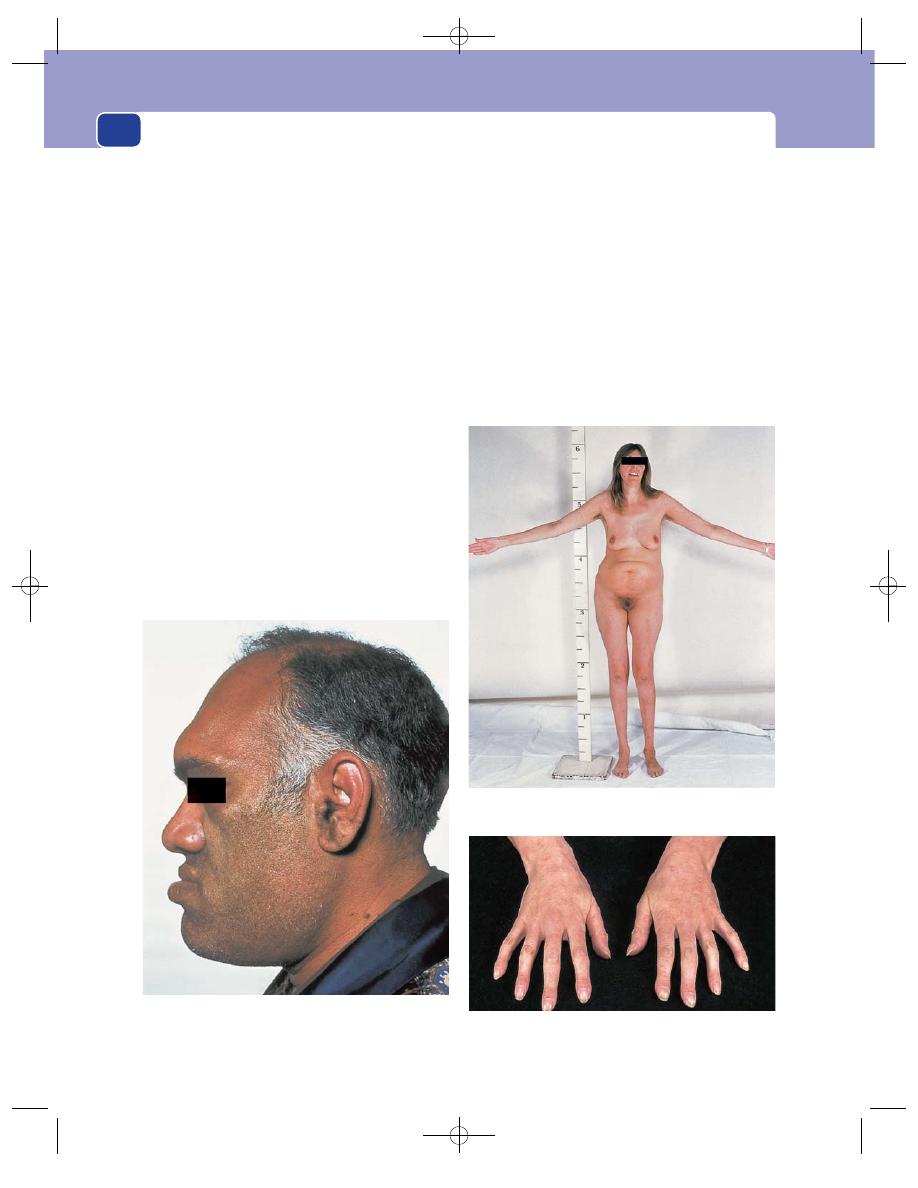
General and facial appearance
220
Acromegaly
The deformities of acromegaly are caused by the
stimulation of growth after normal growth has
ceased. The primary abnormality is a pituitary acido-
phil adenoma secreting too much growth hormone.
The patient has a large face and large hands.
There is overgrowth of the soft tissues of the face,
nose, lips and tongue and of the facial air sinuses
and jaw. The enlargement of the hands is caused by
overgrowth of the small bones of the fingers, particu-
larly the distal phalanges.
Giant (tall) acromegalics usually have a kyphosis
which makes the arms look longer than they really
are, but many acromegalics are not tall or kyphotic.
Their joints are often enlarged by exuberant
osteoarthritis.
The big nose, protuberant jaw and large hands
have been compared to the facies of Punch of
‘Punch and Judy’.
The skin is greasy, not dry, and there is no loss of
mental faculties. These two features help distinguish
early acromegaly from myxoedema.
Marfan’s syndrome
Although this is a rare syndrome, you must know of
its existence because of the blindness, caused by lens
dislocation, and the vascular catastrophes, such as
dissecting aneurysm and aortic incompetence, that
often accompany it. It is caused by an abnormality
of the mucopolysaccharides that form the ground
substance of intercellular cement.
Patients with Marfan’s syndrome are tall and
thin, with very long fingers and toes (arachnodactyly)
and a high arched palate.
When this syndrome causes only minor skeletal
changes it is difficult to recognize.
FIG 8.5
Acromegaly. A heavy head with a prominent nose,
chin and lips. These patients also have long arms and large
hands and feet.
FIG 8.6
MARFAN’S SYNDROME.
The long, spindly fingers of a patient with Marfan’s syndrome.
Tall, slim, with a high-arched palate, long arms, and long
spindly fingers.
Chap-08.qxd 4/19/05 14:13PM Page 220
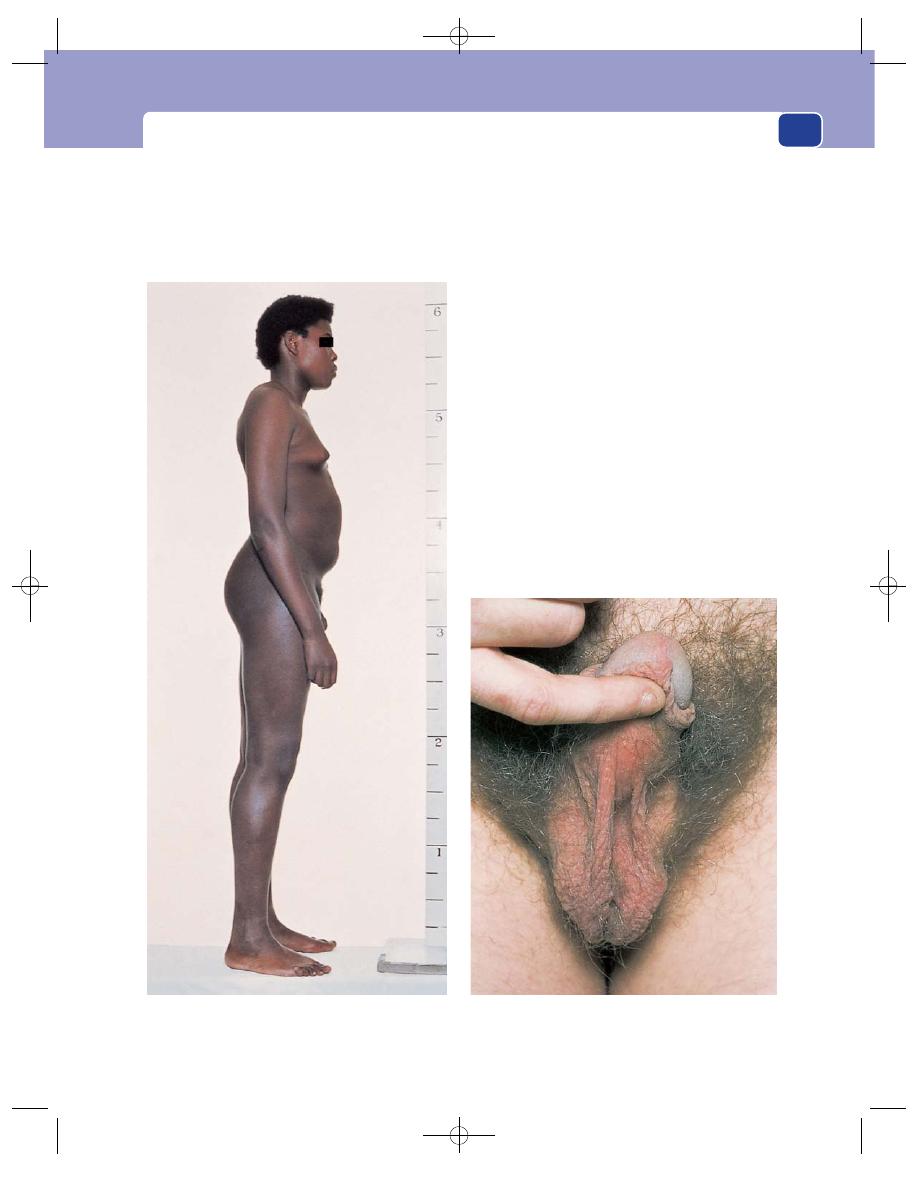
General appearance
221
Klinefelter’s syndrome
Klinefelter’s syndrome is a congenital abnormality
in which a male has an extra female (X) chromo-
some. Thus, instead of being a normal XY male, he
is XXY, and testosterone production is subnormal.
The patients are tall, with a female distribution
of fat around the breast and pelvis, but normal male
hair growth on the face and pubis.
The testes are very small and soft and do not pro-
duce spermatozoa, so the patients are sterile.
Turner’s syndrome
Turner’s syndrome is a congenital abnormality in
which a female has only one female (X) chromo-
some. Thus, instead of being a normal XX female,
she is XO.
There are no skeletal abnormalities, but the
patient has a masculine shape – wide shoulders and
narrow pelvis – and is invariably shorter than aver-
age for a woman.
The most distinctive feature, when present, is
‘webbing’ of the shoulders. This is a thickening of
the neck and a prominence of the skin folds that run
from the neck to the shoulders.
The breasts and pubic hair are usually under-
developed.
FIG 8.7
KLINEFELTER’S SYNDROME.
The small, underdeveloped scrotum, containing atrophic
testes, of a patient with Klinefelter’s syndrome.
A tall male with a female body shape, a female distribution
of body fat and hair, and atrophic testes.
Chap-08.qxd 4/19/05 14:13PM Page 221
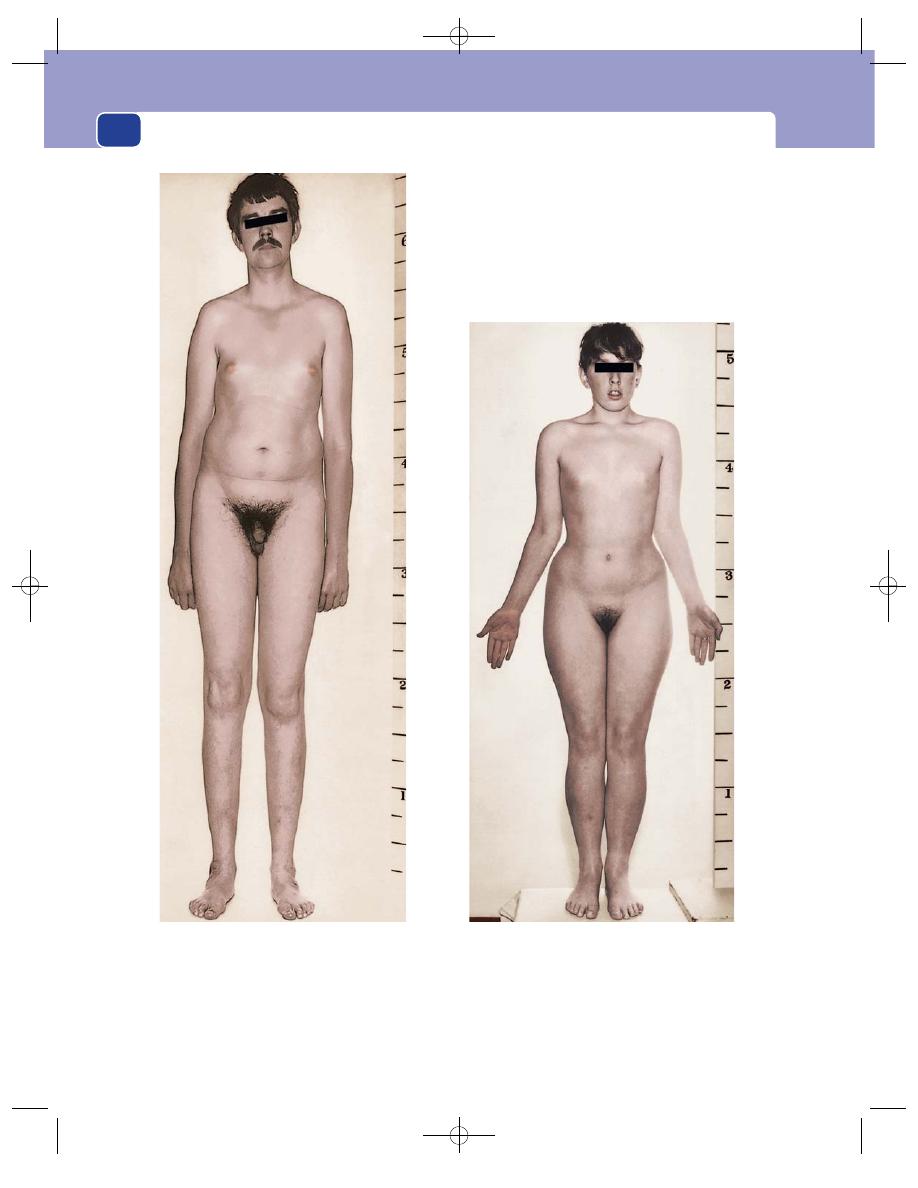
General and facial appearance
222
FIG 8.8
A comparison between the body build of a young
man with Klinefelter’s syndrome – a tall male with a female
distribution of body fat – and a young woman with Turner’s
syndrome – a short female with a masculine shape and
amenorrhoea. The ‘webbing’ of the shoulders is not very
pronounced in the female patient.
Chap-08.qxd 4/19/05 14:13PM Page 222
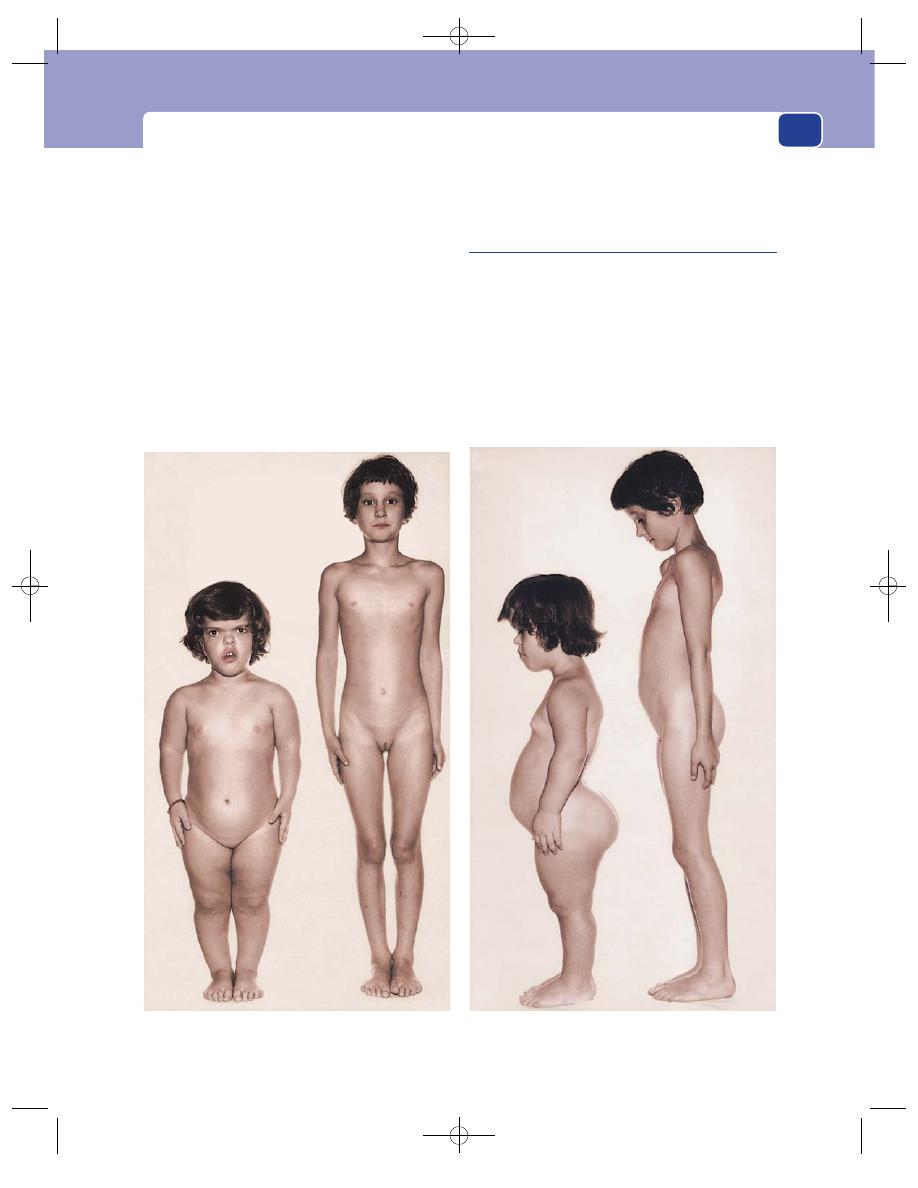
General appearance
Dwarfism
There is a multitude of causes of dwarfism, many
of which are obscure endocrine abnormalities. The
common causes are as follows.
■
Rickets. Bowed long bones. Scoliosis.
Prominent costochondral junctions (‘rickety
rosary’). Transverse groove across rib cage at
attachment of diaphragm (Harrison’s sulcus).
■
Achondroplasia (the circus dwarf). Large head.
Flattened bridge of nose. Stunted trunk, hands
and fingers. Waddling gait. Umbilicus below the
mid-point of vertical height.
■
Renal dwarfism.
■
Cretinism.
■
Pituitary deficiency.
Signs and stigmata of congenital syphilis
This is now a rare condition.
In infants
Signs of congenital syphilis rarely appear before 7
years of age. Any symptoms that do occur are usu-
ally similar to the symptoms of the secondary stage
of acquired syphilis: snuffles, condylomata around
the mouth and anus, and a ham-coloured, symmet-
rical, transient rash.
223
FIG 8.9
An achondroplastic child standing beside a normal child of the same age. The facial and skeletal abnormalities are all
obvious. Note that the umbilicus of the achondroplastic child is below the mid-point of the vertical height.
Chap-08.qxd 4/19/05 14:13PM Page 223
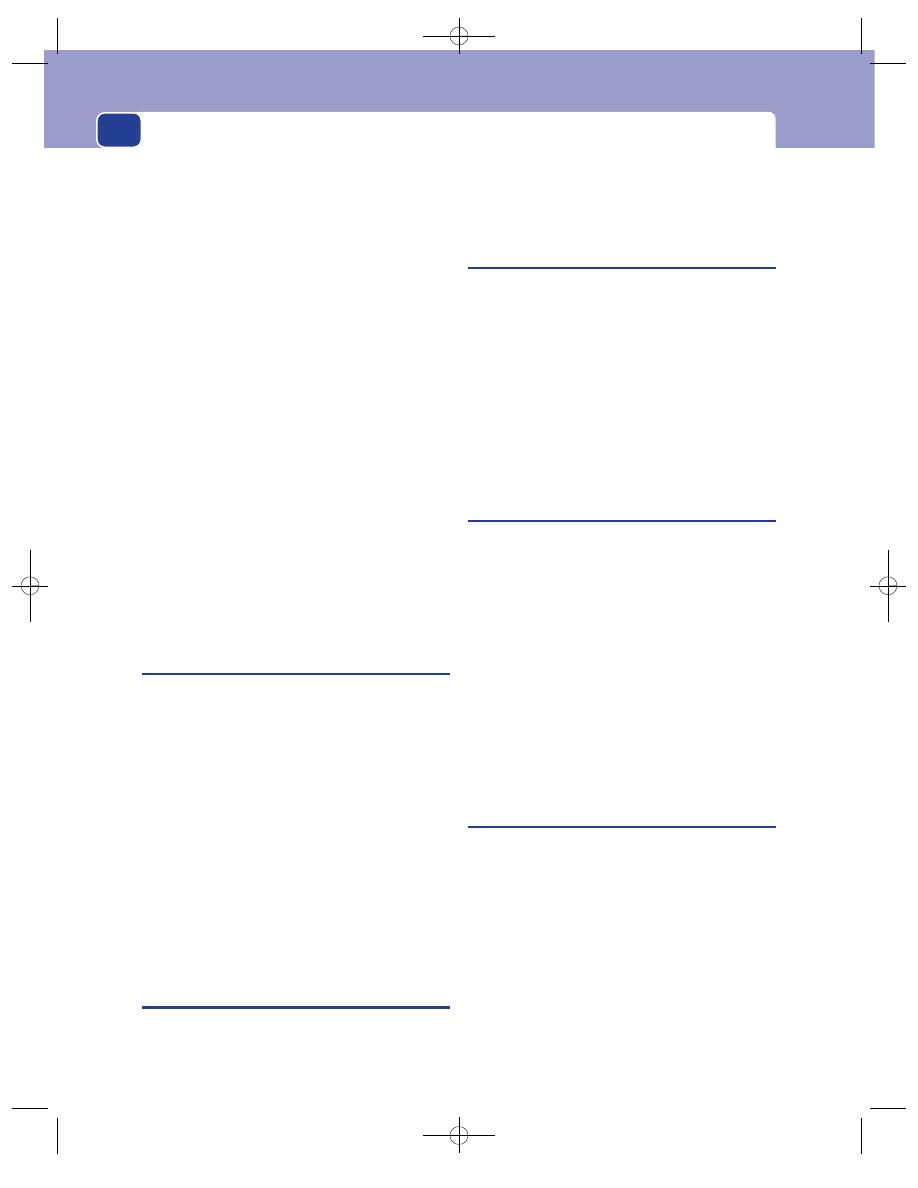
General and facial appearance
224
In children and young adults
Congenital syphilis causes:
■
interstitial keratitis
■
deafness
■
periostitis (sabre tibia)
■
synovitis (Clutton’s joints).
These conditions leave permanent defects, aptly
described as making the patient blind, deaf and lame.
The stigmata of the infection remain with the
patient for the rest of their life. They are:
■
remnants of interstitial keratitis (loss of vision)
■
nerve deafness
■
depressed bridge of nose (saddle nose)
■
perforated palate or nasal septum
■
radiating scars and creases around the mouth
(rhagades)
■
Hutchinson’s teeth (small permanent incisors
with a notched border)
■
sabre tibiae
■
painless joint effusions (Clutton’s joints)
■
retardation of growth.
Interstitial keratitis,
nerve deafness and
Hutchinson’s teeth are known as Hutchinson’s triad.
Hysteria
Beware of patients whose mental attitude to their
symptoms seems out of proportion – either over-
responding to them or ignoring them. The patient
whose symptoms do not fit any known pattern who
tells you with a big smile that they have severe pain,
or who, while complaining of severe symptoms,
appears quite unconcerned (‘la belle indifference’)
may well be neurotic, hysterical, or fabricating the
symptoms and the signs.
A diagnosis of hysteria should only be made
when all possible organic causes for the symptoms
have been excluded.
In this situation your clinical experience is your
greatest help.
DISEASES AFFECTING FACIAL
APPEARANCE
The appearance of the face has a major effect on the
patient’s general appearance. Those general conditions
that affect the face have already been described. This
section deals with diseases that particularly affect
facial expression and appearance.
Bell’s palsy
Bell’s palsy is a paralysis of the facial nerve affecting
the muscles of facial expression.
The absence of tone in the facial muscles makes
the affected side of the face look smooth and sloppy.
The corner of the mouth droops, the nasolabial
creases become asymmetrical and less noticeable,
and the lower eyelid droops. The asymmetry of the
mouth can be increased by asking the patient to bare
their teeth. If they are asked to shut their eyes, you
will see that the lids fail to close on the affected side.
Parkinson’s disease
(Paralysis agitans)
This condition is associated with an absence of
facial expression. The face becomes a fixed, unblink-
ing mask – the Parkinsonian mask.
In addition to the facial changes, all movements
become stiff and restricted. The patient walks with
short, shuffling steps, back bent, and head poked
forwards.
The hands, limbs and head develop a tremor.
The repetitive shaking of the thumb and index fin-
ger gives the appearance of ‘pill-rolling’.
In its florid state, Parkinson’s disease presents an
unmistakable clinical picture, but it can be detected
long before this if you look out for the loss of facial
expression.
Scleroderma
The progressive thickening of the skin of the face that
occurs with scleroderma can also reduce the patient’s
ability to use their muscles of facial expression. The
skin thickens and has a pale, waxy appearance.
The mouth gets small (microstomia) and jaw
movements may be restricted.
Telangiectases appear on the cheeks, around the
mouth and across the nose.
Fine, white, horizontal scars appear on the neck
in the lines of the transverse skin creases.
When the patient smiles and laughs the face does
not respond fully. This is different from Parkinson’s
Chap-08.qxd 4/19/05 14:13PM Page 224
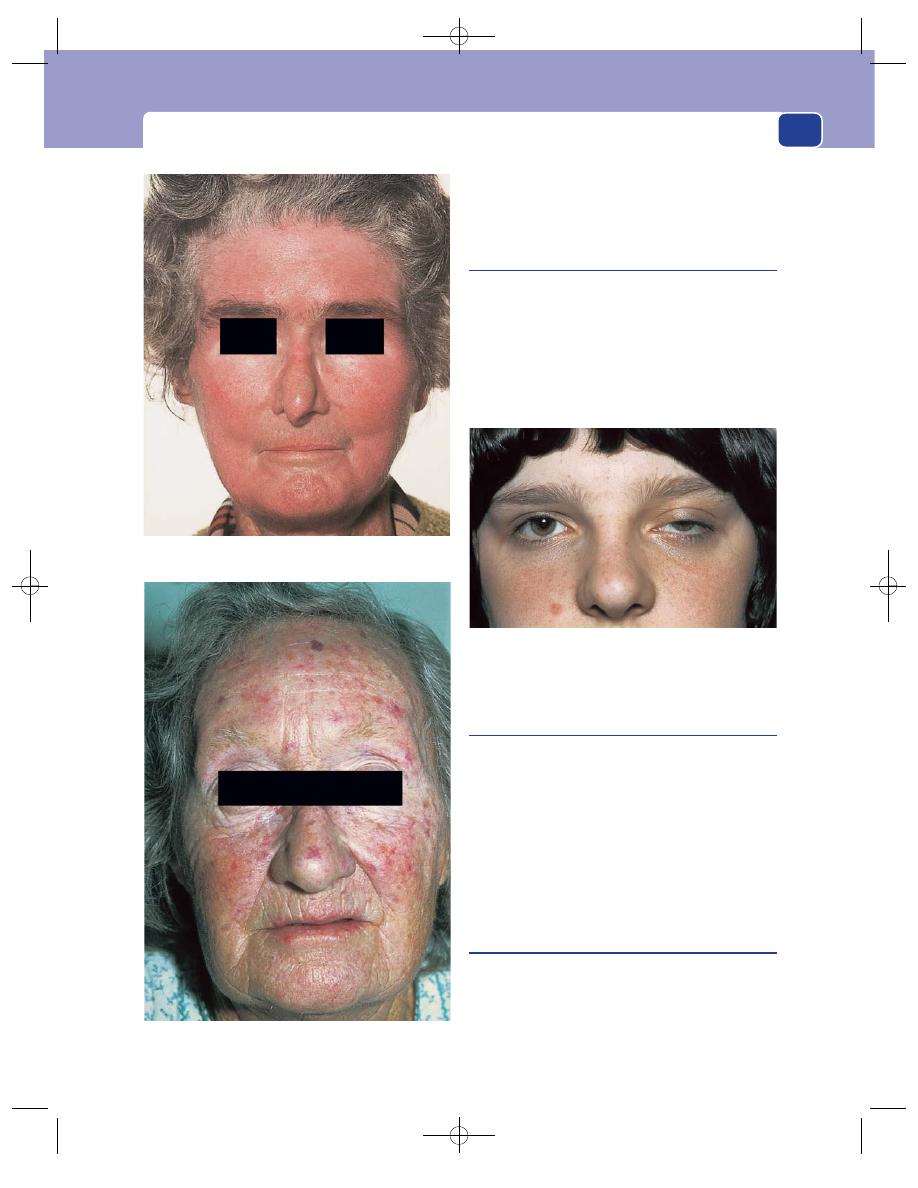
Diseases affecting facial appearance
225
disease, in which there is not a flicker of facial
expression even though the tissues of the face are
obviously normal.
Myasthenia gravis
Remember that myasthenia gravis causes weakness
of all muscles but particularly the muscles of the
eyelids. Suspect it in any patient who complains
of tired, drooping eyelids or weakness of the face
and jaw.
The weakness is transitory; power and move-
ment return if the muscles are allowed to rest.
Cretinism
A cretin is a child deficient in thyroid hormone. It is
a condition that should only be seen in neonates
because it should be recognized soon after birth and
cured by giving the child thyroid hormone.
In an advanced case, the face is broad and flat,
the eyes are wide apart and the tongue protrudes
from the mouth.
If the condition is not treated, growth is slowed,
so that the child is short, fat and mentally retarded.
Down’s syndrome
Down’s syndrome is a congenital abnormality usu-
ally associated with an extra chromosome 21.
Males and females and all races are equally
affected. The prime abnormalities are mental retard-
ation, floppiness and a short stature. The old name
FIG 8.10
SCLERODERMA.
The telangiectases of scleroderma.
Note the tight skin, small mouth, fine wrinkles around the
mouth and small telangiectases.
FIG 8.11
Myasthenia gravis: heavy, drooping eyelids, much
worse on the patient’s left side. The eye signs of generalized
diseases are often asymmetrical, even unilateral.
Chap-08.qxd 4/19/05 14:13PM Page 225
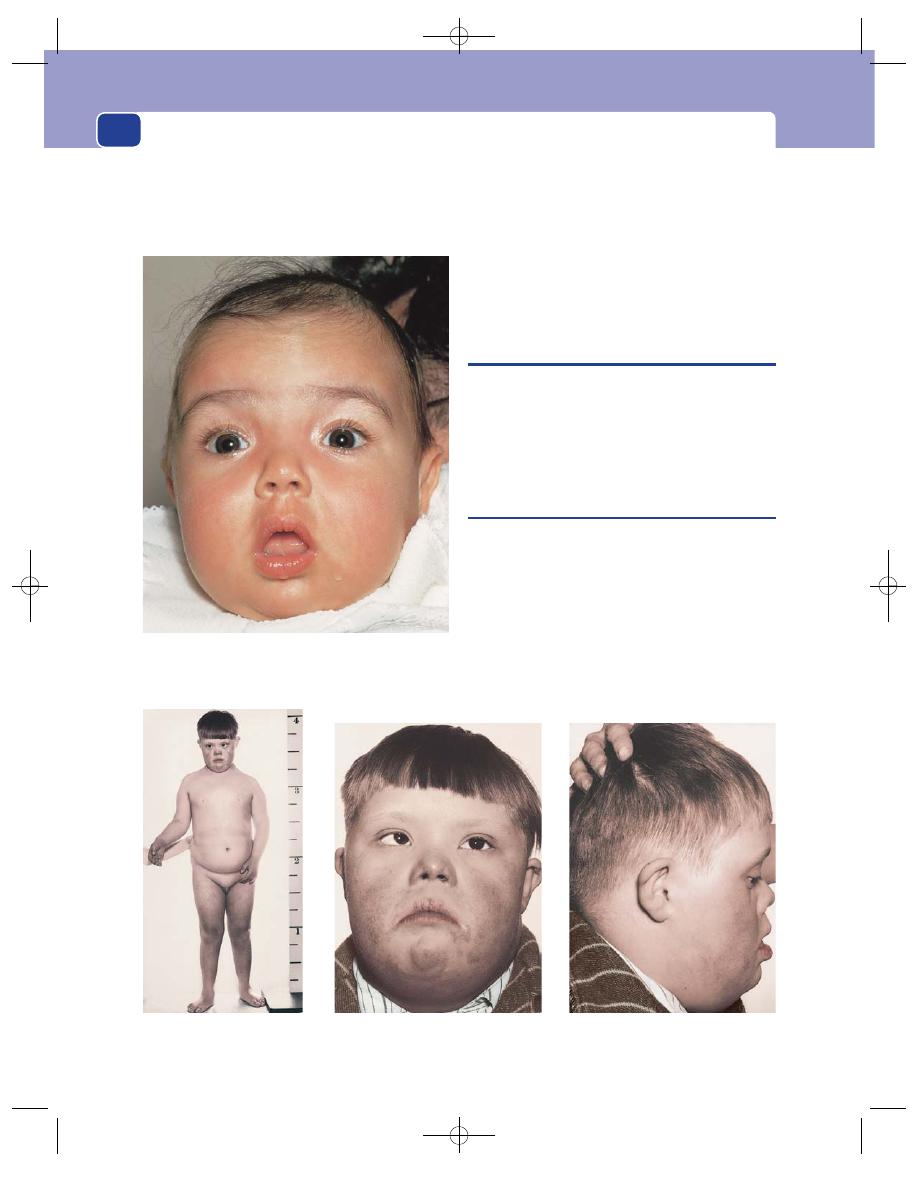
(mongolism) describes the dominant facial fea-
tures: the outer ends of the palpebral fissures slant
upwards and there are prominent epicanthic folds.
The face is flattened, and the tongue protrudes.
Affected children often have a squint and one-third
have congenital heart disease.
The Down’s baby is distinguishable from the
cretin because their skin and hair are smooth and
fine, not coarse and thick, and though they are more
floppy than a normal baby, they are not slow and
sluggish like a cretin.
THE EYES
This book cannot discuss the many diseases of the
eye that affect facial appearance, some of which are
part of generalized medical conditions, but does
present a few easily recognizable and surgically rele-
vant conditions.
Arcus senilis
This term is used to describe a white rim around the
outer edge of the iris. It is a rim of sclerosis and chol-
esterol deposition in the edge of the cornea and is
common in the elderly.
It has no great clinical significance, except in
patients below the age of 40, when it may be associ-
ated with hyperlipoproteinaemia. It is not associ-
ated with generalized degenerative arterial disease,
although both conditions often coexist.
General and facial appearance
226
FIG 8.13
Down’s syndrome. These three photographs show the short stature, floppiness and typical facial features of Down’s
syndrome.
FIG 8.12
Congenital hypothyroidism (cretinism). The head is
broad, the eyes wide apart, the tongue protrudes from the mouth
and all movements and responses are slow and sluggish.
Chap-08.qxd 4/19/05 14:13PM Page 226
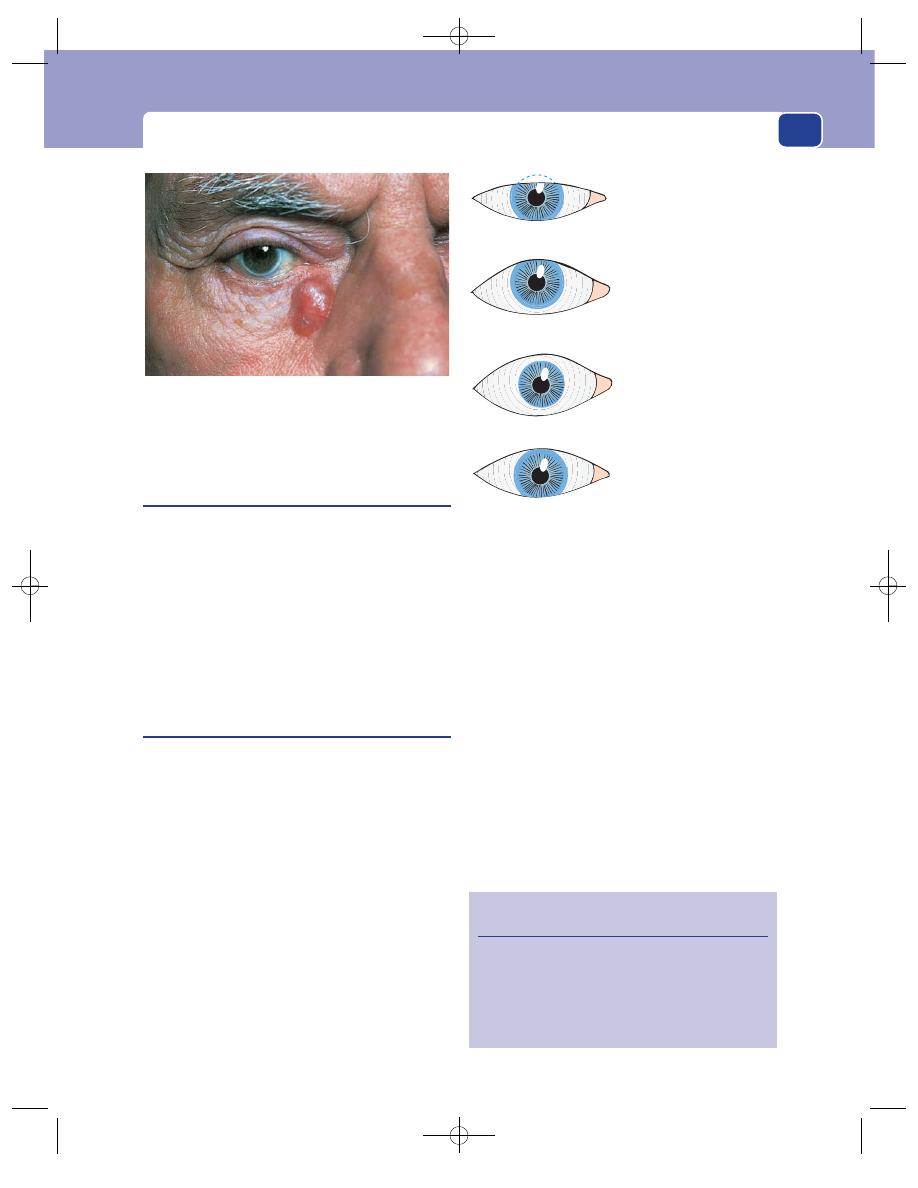
The eyes
227
Xanthelasma
(Xanthoma)
Xanthelasmata are fatty plaques in the skin of the
eyelids. They look like masses of yellow, opaque fat.
They are confined to the skin and are not painful or
tender.
Xanthelasmata are very common. One or two on
the eyelids do not indicate any underlying disease, but
if the patient has extensive, multiple, growing lesions,
you should exclude any underlying abnormality of
cholesterol metabolism, diabetes or arterial disease.
Exophthalmos
(Proptosis)
Exophthalmos is the forward protrusion of the eye
from its normal position in the orbit.
In the normal eye (Fig. 8.15), the lower eyelid
just touches the lower edge of the iris (the inferior
limbus), provided the lower lid is normal, while the
upper lid crosses the eye mid-way between the pupil
and the superior limbus.
The first sign of exophthalmos is the appearance
of sclera below the inferior limbus. The proptosis
has to be considerable before sclera is visible above
the superior limbus.
The position of the upper eyelid is also altered by
the tone of the levator palpebrae superioris muscle.
Retraction of the upper eyelid will reveal sclera
above the superior limbus, but you will not mistake
this for exophthalmos if you remember to check the
position of the lower eyelid.
When the eye is pushed forwards, four secondary
physical signs appear.
1. The patient can look up without wrinkling the
forehead.
2. Convergence for very close vision is restricted.
3. The patient blinks less often than normal.
4. The patient may not be able to close their eyes
and corneal ulceration may develop.
If the protrusion of the eye interferes with the
venous and lymphatic drainage of the conjunctiva,
it becomes oedematous and wrinkled. This is called
chemosis.
The causes of exophthalmos are listed in Revision
panel 8.7.
The commonest cause of both bilateral and
unilateral exophthalmos is thyrotoxicosis.
FIG 8.14
Arcus senilis: a thin white rim around the iris. It is a
common abnormality and does not indicate advanced arterial
disease. Note that the patient also has a basal cell carcinoma.
Normal
Mild exophthalmos
Sclera visible below
the inferior limbus
Severe exophthalmos
Sclera visible all round
the iris
Lid retraction
Elevation of the upper
eyelid
FIG 8.15
The relations of the eyelids to the iris.
Revision panel 8.6
The causes of ptosis
Inflammation
Tumours
Excess eyelid skin
Muscle weakness (myopathies, myasthenia)
Third nerve palsy
Chap-08.qxd 4/19/05 14:13PM Page 227
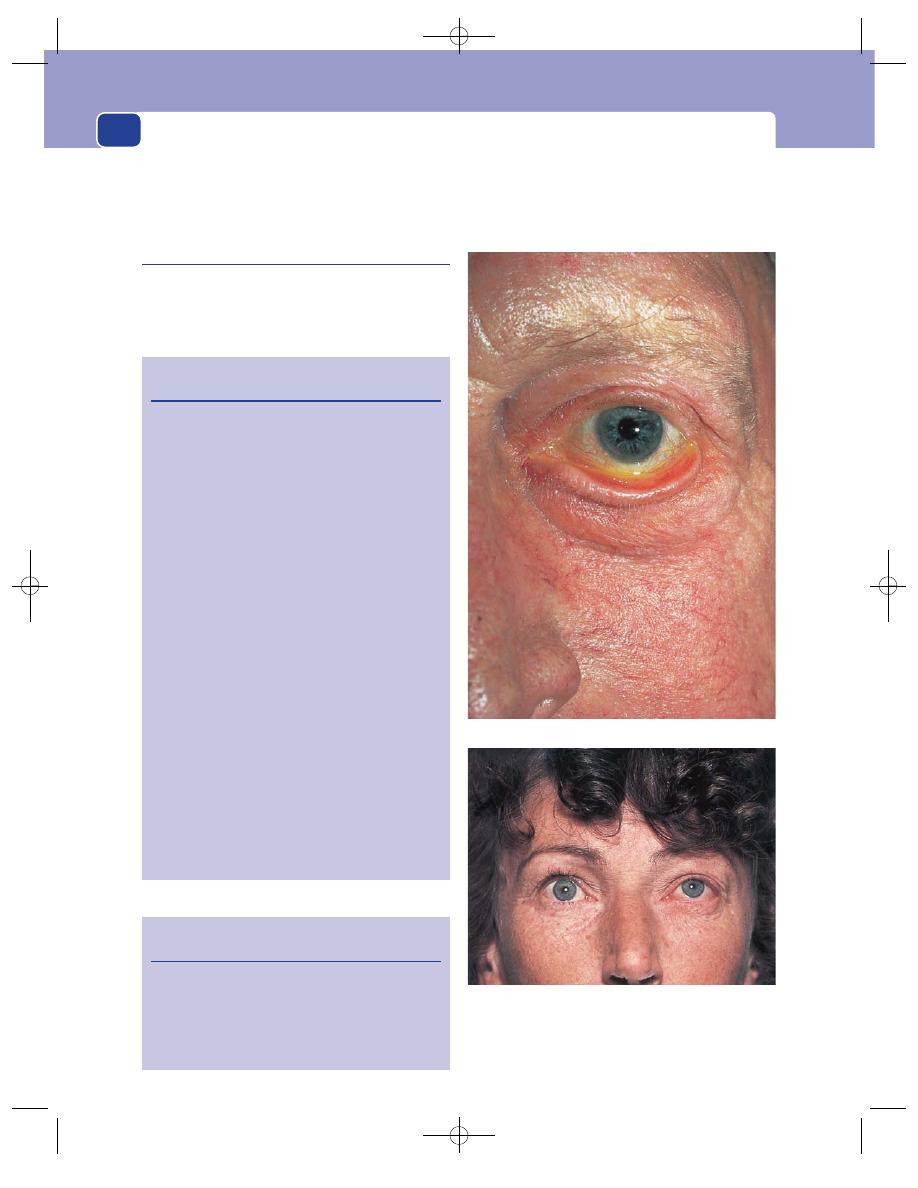
General and facial appearance
228
Revision panel 8.8 lists the causes of a pulsating
exophthalmos. This is a rare condition but easy to rec-
ognize. It is usually associated with severe chemosis.
Ectropion
Deformities of the lower eyelid often cause the lid to
evert. This reveals sclera below the inferior limbus
and so mimics exophthalmos, but should not lead to
a misdiagnosis because the eyelid looks deformed.
When the eyelid becomes everted, its inner surface
of shiny conjunctiva may become scarred, dull and
immobile.
Revision panel 8.7
The causes of exophthalmos
Endocrine
a
Thyrotoxicosis (before, during and after
its onset)
Cushing’s syndrome (rare)
Non-endocrine
Congenital deformities of the skull
a
(craniostenosis, oxycephaly, hypertelorism)
Orbital or peri-orbital tumours
Peri-orbital meningioma
Optic nerve glioma
Orbital haemangioma
Lymphoma
Osteoma
Pseudotumour (granuloma)
Carcinoma of antrum
Neuroblastoma
Inflammation
Orbital cellulitis
Ethmoid or frontal sinusitis
Vascular causes
Cavernous sinus arterio-venous fistula
Cavernous artery aneurysm
Eye disease
Severe myopia
a
Severe glaucoma (buphthalmos)
a
a
Likely to be bilateral.
Revision panel 8.8
The causes of pulsating exophthalmos
Carotid artery–cavernous sinus arterio-venous
fistula
Aneurysm of the ophthalmic artery
Vascular neoplasm in the orbit
Cavernous sinus thrombosis
Ectropion: eversion of the lower eyelid.
Proptosis: the sclera is visible between the inferior limbus
and the left lower eyelid, but the lower eyelid is normal. Thus
this is not ectropion but proptosis, caused, in this patient, by
a retro-orbital tumour.
FIG 8.16
Chap-08.qxd 4/19/05 14:13PM Page 228
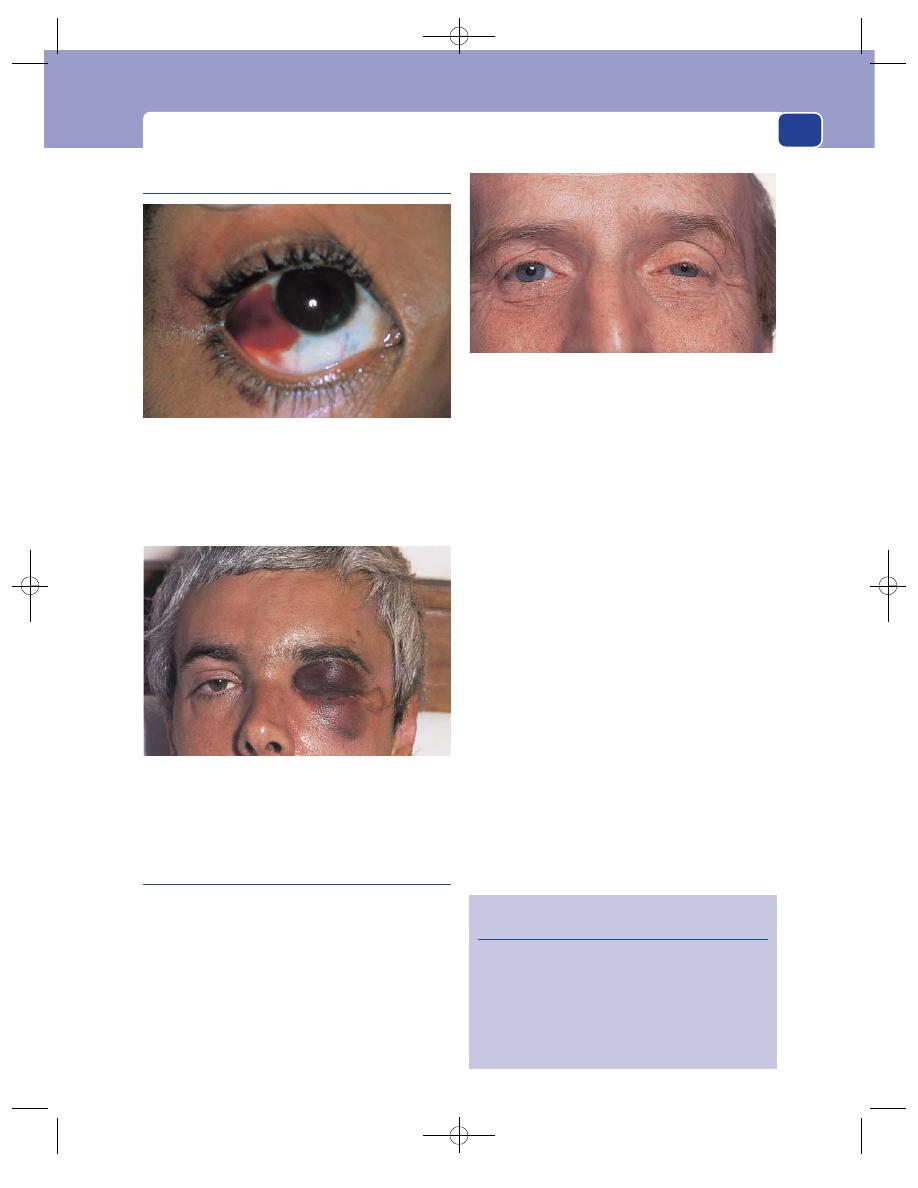
The eyes
229
Subconjunctival haemorrhage
Horner’s syndrome
Horner’s syndrome comprises the physical signs
that follow interruption of the sympathetic nerve
supply to the head and neck.
The pre-ganglionic sympathetic fibres of the head
and neck arise in the first and sometimes second
thoracic segments of the spinal cord. They synapse
with the cells in the three cervical sympathetic
ganglia whose fibres (post-ganglionic) are distrib-
uted to the structures of the head and neck along
the nerves and blood vessels.
The sympathetic pathway to the face and eye can,
therefore, be interrupted by trauma or disease any-
where between the appearance of the pre-ganglionic
fibres from the spinal cord and their termination.
Absence of sympathetic tone causes myosis, pto-
sis, vasodilatation and anhidrosis.
The causes of Horner’s syndrome are as follows
(the common causes are in bold type).
■
Brain lesions – posterior inferior cerebellar
artery thrombosis.
■
Spinal cord lesions – syringomyelia, tumours.
■
Injuries to the lower roots of the brachial
plexus.
■
Surgical excision of the inferior cervical
ganglion (cervical sympathectomy).
■
Tumours in the apex of the lung (Pancoast’s
tumour).
■
Tumours in the neck.
■
Aneurysm and dissection of the carotid artery.
When these nerve fibres are interrupted by dis-
ease there may be a period before the paralysis when
the sympathetic activity is increased. Stimulation
of the sympathetic nerves makes the pupil dilate,
the upper eyelid retract and the skin of the face pale,
FIG 8.17
A subconjunctival haemorrhage may arise from a
subconjunctival vessel or be blood which has tracked
forwards from behind the eye – usually from a fracture of the
base of the skull. When this patient looked to the left, white
sclera could be seen to the right of the haemorrhage,
confirming that the bleeding was solely from subconjunctival
blood vessels.
Extensive bleeding from a fracture of the base of the skull
may cause a large peri-orbital haematoma as well as a
subconjunctival haemorrhage.
FIG 8.18
Horner’s syndrome of the left eye. (See Revision
panel 8.9.)
Revision panel 8.9
Horner’s syndrome
A small pupil (myosis)
Drooping of the upper eyelid (ptosis)
A warm, pink cheek (vasodilatation)
Absence of sweating (anhidrosis)
Nasal congestion (nasal vasodilatation)
Apparent enophthalmos
Chap-08.qxd 4/19/05 14:13PM Page 229
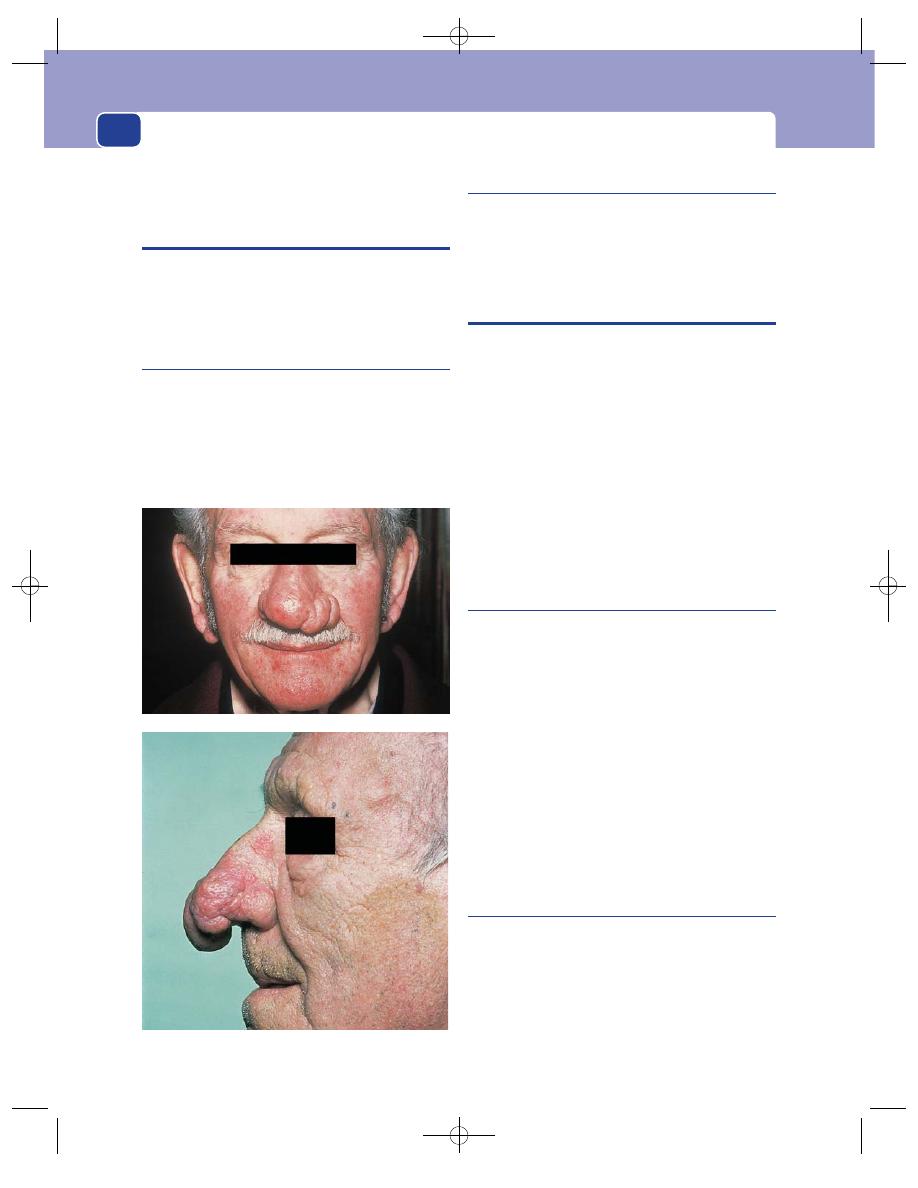
cold and sweaty. The causes of sympathetic nerve
irritation are the same as the causes of paralysis.
THE NOSE
The appearance of the face is affected by the shape
of the nose. In addition to the infinite variability of
the shape of the normal nose, there are two patho-
logical conditions which alter its shape.
Saddle nose
A nose whose bridge is depressed and widened is
called a saddle nose. This deformity is caused by
congenital abnormalities such as achondroplasia
and hypertelorism, or destruction of the nasal cartil-
ages, commonly caused by leprosy, cutaneous leish-
maniasis and congenital syphilis.
Rhinophyma
Rhinophyma is a thickening of the skin over the tip of
the nose caused by hypertrophy and adenomatous
changes in its sebaceous glands. It is not caused by
an excessive intake of alcohol.
SHAPE OF THE SKULL
There are a number of congenital deformities of the
skull, all with long names that describe the skull’s
shape, but they are all very rare.
The abnormality of shape that you should look
out for in neonates and young children is the pro-
gressive and disproportionate enlargement of the
skull caused by hydrocephalus.
The normal scalp consists of hairy skin, subcuta-
neous fat and a fascial aponeurosis. All these struc-
tures can give rise to the common lesions of the skin
and subcutaneous tissues described in Chapters 2
and 3, but some are so common on the scalp that
they deserve special mention.
Hydrocephalus
Hydrocephalus is a pathological accumulation of
cerebrospinal fluid within or around the brain –
internal or external hydrocephalus.
Congenital hydrocephalus is caused by a failure
of cerebrospinal fluid absorption, so that there is
distension of the ventricles within the brain and of
the subarachnoid space with which they communi-
cate. Congenital hydrocephalus is often associated
with a meningo-myelocele and spina bifida.
Acquired hydrocephalus is caused by a block of
the aqueduct of Sylvius or the foramina over the
fourth ventricle, by tumour or infection. In this type
of hydrocephalus the distended ventricles do not
communicate with the subarachnoid space.
Multiple sebaceous cysts
The scalp may be covered with sebaceous cysts of all
sizes. They are diagnosed by their spherical shape
and hard, tense composition (see also page 73).
They are by far the commonest cause of a lump on
the scalp. They rarely have a visible punctum.
A suppurating sebaceous cyst with granulation
tissue bulging out of it is sometimes called Cock’s
General and facial appearance
230
FIG 8.19
Two examples of rhinophyma.
Chap-08.qxd 4/19/05 14:13PM Page 230
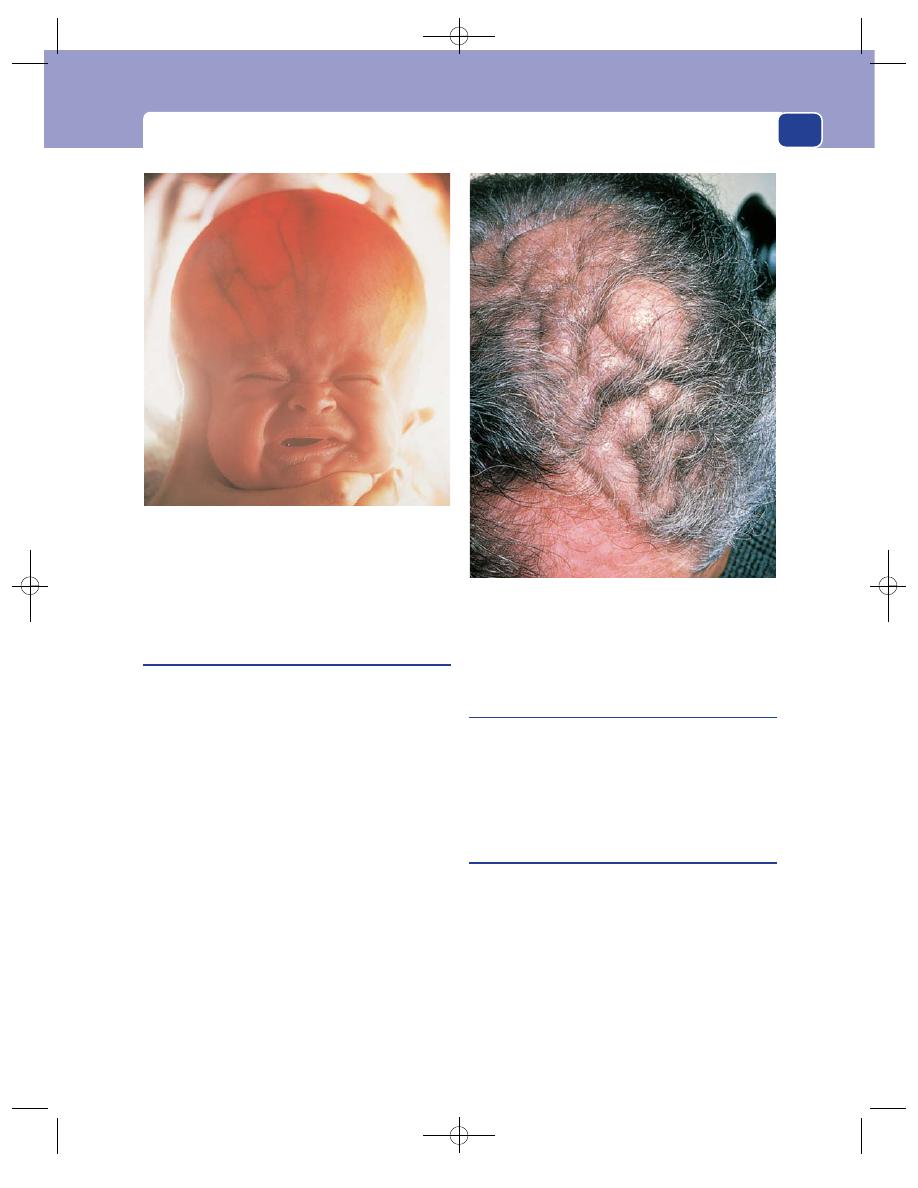
Shape of the skull
231
peculiar tumour (see page 73). It is easily mistaken
for a squamous cell carcinoma.
Turban tumour
There are four pathological conditions that can cause
multiple lumps on the scalp which grow steadily,
coalesce and eventually produce an irregular mass
that covers the whole scalp and looks like a turban.
All are rare.
As the term ‘turban tumour’ is purely descriptive,
it can be applied to all four conditions. However, it is
most often used to describe multiple cylindromata,
which present as firm, pink nodules in the skin.
Multiple nodular basal cell carcinomata may also
cover the scalp, but they are firm, retain their pearly-
white appearance and covering of fine blood vessels,
do not really look like a turban and can usually be
diagnosed by examining one of the smaller lesions.
Multiple sweat gland tumours (hidradenomata)
form soft, boggy swellings in the scalp. Although
very soft (they feel like lumps of oedematous skin),
they are not fluctuant and cannot be compressed or
indented.
Finally, and rarest of all, is subcutaneous plexi-
form neurofibromatosis of the scalp. This is usually
associated with neurofibromata in other sites and
café au lait patches.
Pott’s puffy tumour
Pott’s puffy tumour is a diffuse oedematous swelling
of the scalp over a patch of osteomyelitis in the
skull. It is most often seen in the frontal region over-
lying frontal bone osteomyelitis caused by frontal
sinusitis.
Cephalhaematoma
This is a subperiosteal haematoma. It occurs in
neonates following a traumatic delivery, and in
infants following direct trauma. The haematoma
spreads beneath the pericranium (periosteum) to
the fissures between the skull bones.
For a few days it forms a soft, fluctuant swelling
covering one of the bones of the vault of the skull,
but when the blood begins to resorb, the residual
blood clot forms a ridge around the edge of the
swelling. Ultimately all that is left of the swelling is
FIG 8.20
Congenital hydrocephalus. The bright light behind the
baby’s head reveals the thinness of the bones of the skull.
FIG 8.21
A ‘turban tumour’. This one was a cylindroma.
Chap-08.qxd 4/19/05 14:13PM Page 231
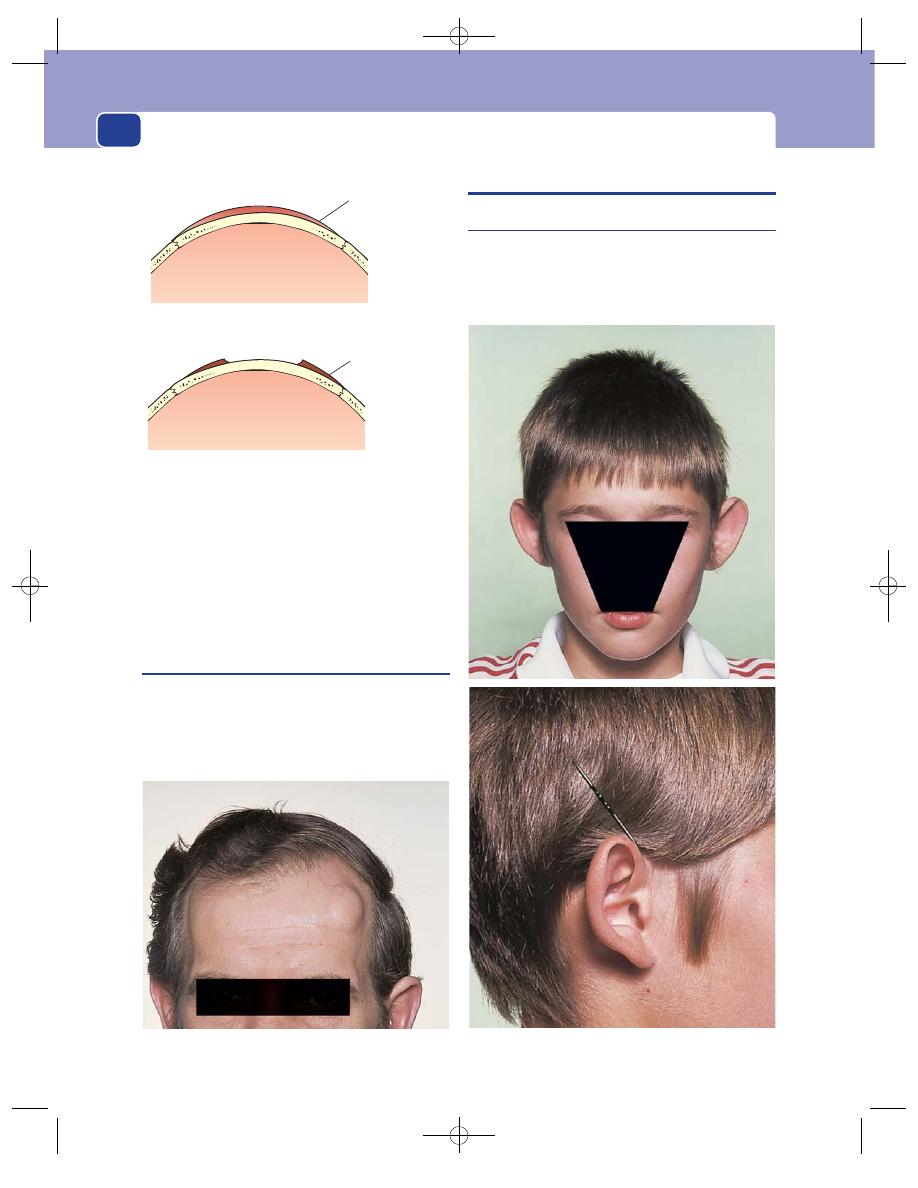
a hard, raised edge, which is often compared to a
dinner plate, and is easily mistaken for a depressed
fracture if you do not observe that its lip is above the
level of the rest of the skull.
Ivory osteoma
This is an osteoma of the cortical bone that forms
the outer table of the skull. Ivory osteomata appear
during adolescence and young adult life but cause
no symptoms and need no treatment.
THE EARS
Bat ears
Congenital bat ears are ears which jut out from the
side of the head rather than lying flat against it. Bat
ears are not associated with any mental abnormal-
ities. Cup-shaped ears that protrude from the side
General and facial appearance
232
FIG 8.24
Bat ears: antero-posterior and lateral views.
Subperiosteal
haematoma
Residual ridge of
clotted blood
FIG 8.22
A cephalhaematoma is a subperiosteal haematoma
limited by the fissures between the bones. When the blood is
absorbed, a ridge of clotted blood forms a rim around the
edge of the haematoma.
FIG 8.23
An ivory (cortical) osteoma on the forehead.
Chap-08.qxd 4/19/05 14:13PM Page 232
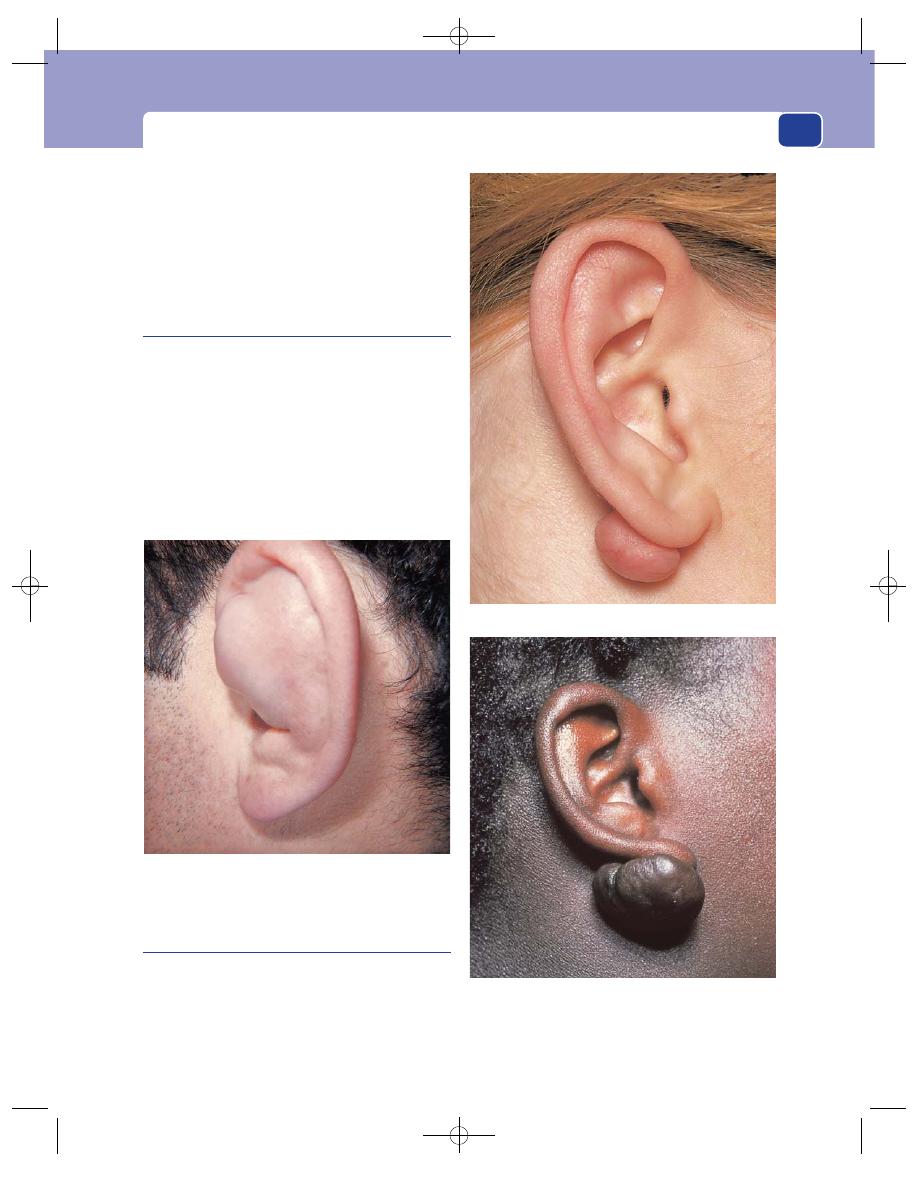
The ears
233
of the skull are a feature of Down’s syndrome, but
these are not true bat ears.
If a patient complains that one ear has become
prominent, look behind it for swellings in the sub-
cutaneous tissue or bone that may be pushing it
outwards. For example a mastoid abscess makes the
ear more prominent.
Cauliflower ears
Cauliflower ears are ears distorted by multiple sub-
perichondral haematomata. Unlike most other
haematomata, those beneath the perichondrium of
the ear are slow to resorb. Some actually absorb
fluid and swell. The patient complains of a flat-
tened, sometimes fluctuant, sometimes firm, swel-
ling fixed to the cartilage of the ear, which fills the
hollows of the ear and distorts its shape.
Cauliflower ears are common in boxers and
wrestlers.
Keloid nodules
Many women have their ears pierced. If the hole
becomes infected, or if the patient has an inherent
tendency towards keloid scarring, the scar tissue
may overgrow and produce a large nodule behind
the lobe of the ear. The nodule is soft, spherical
FIG 8.25
A ‘cauliflower ear’. The swelling is a subperichondral
haematoma and is almost blocking the external auditory
meatus.
FIG 8.26
Keloid scars at the site of ear piercing. The mass
of scar tissue usually protrudes from the posterior aspect
of the ear lobe. Keloid scars are more common in
black-skinned races.
Chap-08.qxd 4/19/05 14:14PM Page 233
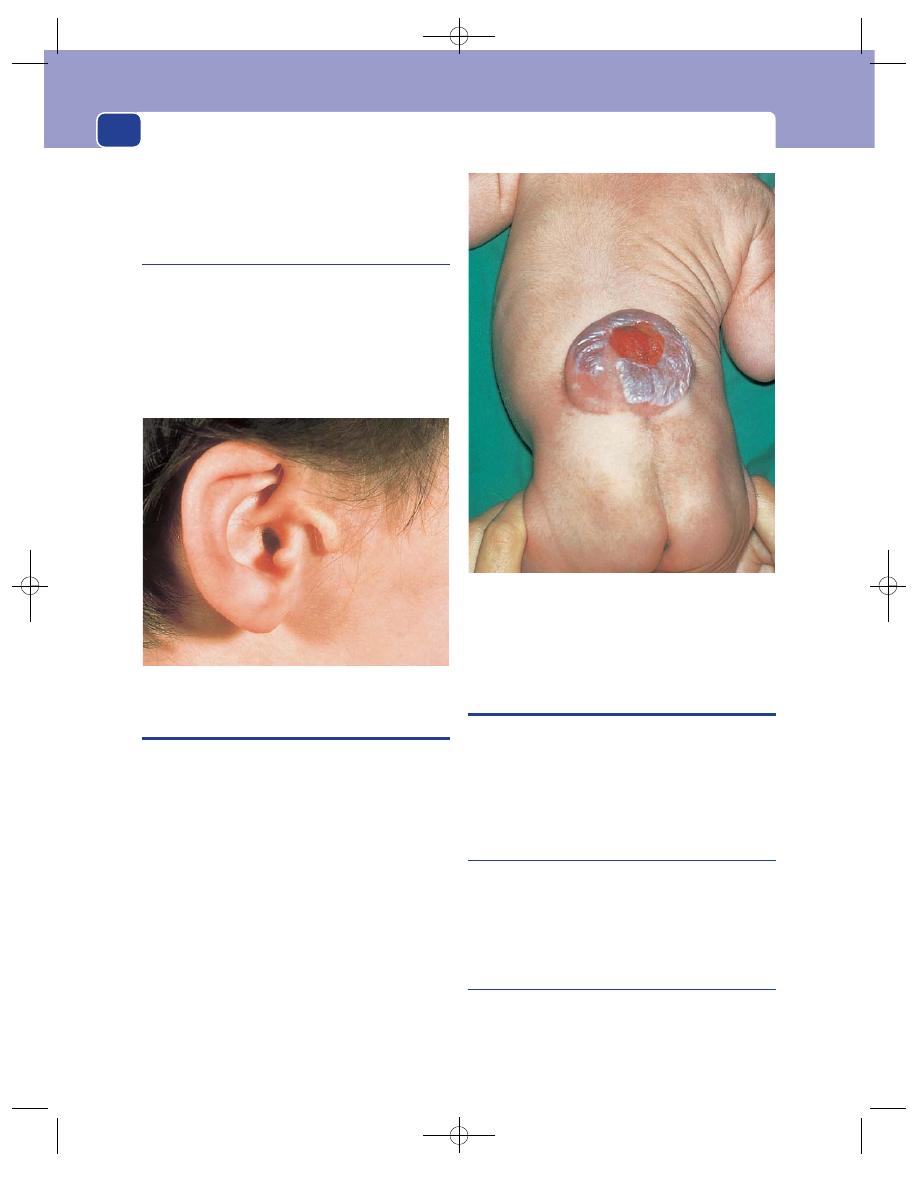
and sometimes pedunculated. It is often misdiag-
nosed as an inclusion dermoid cyst but is usually a
solid mass of keloid scar.
Accessory auricle
Accessory auricles are small pieces of cartilage separate
from the pinna. They are found on the side of the face
just in front of the tragus. They cause no symptoms
and can be differentiated from the other two lumps
that develop in front of the ear – an enlarged pre-
auricular lymph gland or a parotid gland tumour – by
the fact that they have been present from birth.
MENINGOCELE
A meningocele is a protrusion of the meninges
through a defect in the spinal canal or skull. It con-
tains cerebrospinal fluid and is covered by skin.
A meningo-myelocele is a protrusion of the
meninges plus part of the spinal cord or cauda
equina through a defect in the spinal canal. It is not
completely covered by skin, and the thin meninges
rupture a few days after birth.
There are two other, uncommon, congenital
abnormalities of spinal cord and canal develop-
ment. A myelocele is an open, exposed spinal cord.
The infant is stillborn or dies within a few days of
birth. A syringo-myelocele is the bulge of a dilated
spinal cord (hydromyelia) through the spinal canal.
The diagnosis of a meningocele, or meningo-
myelocele, is made on the basis of its composition –
soft, fluctuant and translucent; its site – in the mid-
line of the lower back, or the back of the skull; and
the presence of neurological abnormalities below
the level of the lesion.
THE CHEST WALL
There are a number of deformities and diseases
which alter the shape of the chest wall and which,
therefore, affect the general appearance of the
patient – hence their inclusion in this chapter.
Funnel chest
(Pectus excavatum)
Funnel chest is a congenital depression of the body of
the sternum. If it is deep, it may embarrass respira-
tion and cause recurrent respiratory tract infection.
Pigeon chest
(Pectus carinatum)
Pigeon chest is the opposite deformity to funnel
chest. The sternum sticks forwards like the keel of a
boat. It may be a congenital deformity or be caused
by chest disease in childhood, such as asthma.
General and facial appearance
234
FIG 8.27
An accessory auricle.
FIG 8.28
A meningo-myelocele of the spine.
Chap-08.qxd 4/19/05 14:14PM Page 234
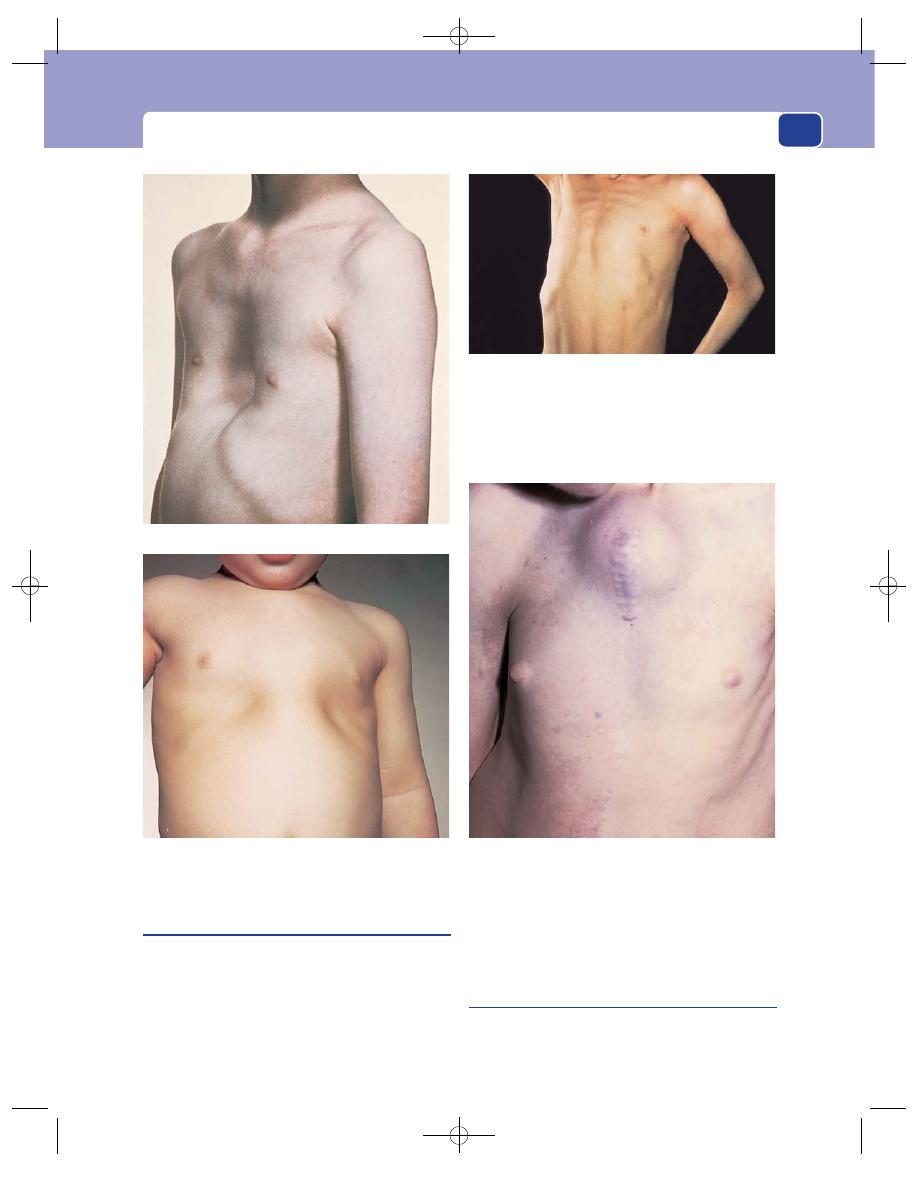
The chest wall
235
Harrison’s sulcus
This is a hollow in the thoracic cage, caused by the
depression of the costo-chondral junctions of the
fourth, fifth, sixth and seventh ribs.
This abnormality is a late effect of rickets. Rickets
first causes an enlargement of the costo-chondral
junctions – the rickety rosary – but later both
these and the ends of the ribs soften and sink
inwards. The resulting hollow is particularly notice-
able over the lower group of ribs attached to the
sternum.
Sprengel’s shoulder
Sprengel’s shoulder is caused by a congenital eleva-
tion of the scapula which distorts the whole shape
of the chest and shoulder.
FIG 8.29
DEFORMITIES OF THE CHEST WALL.
Funnel chest.
A rickety rosary.
Pigeon chest.
An aortic aneurysm eroding through the sternum.
Chap-08.qxd 4/19/05 14:14PM Page 235
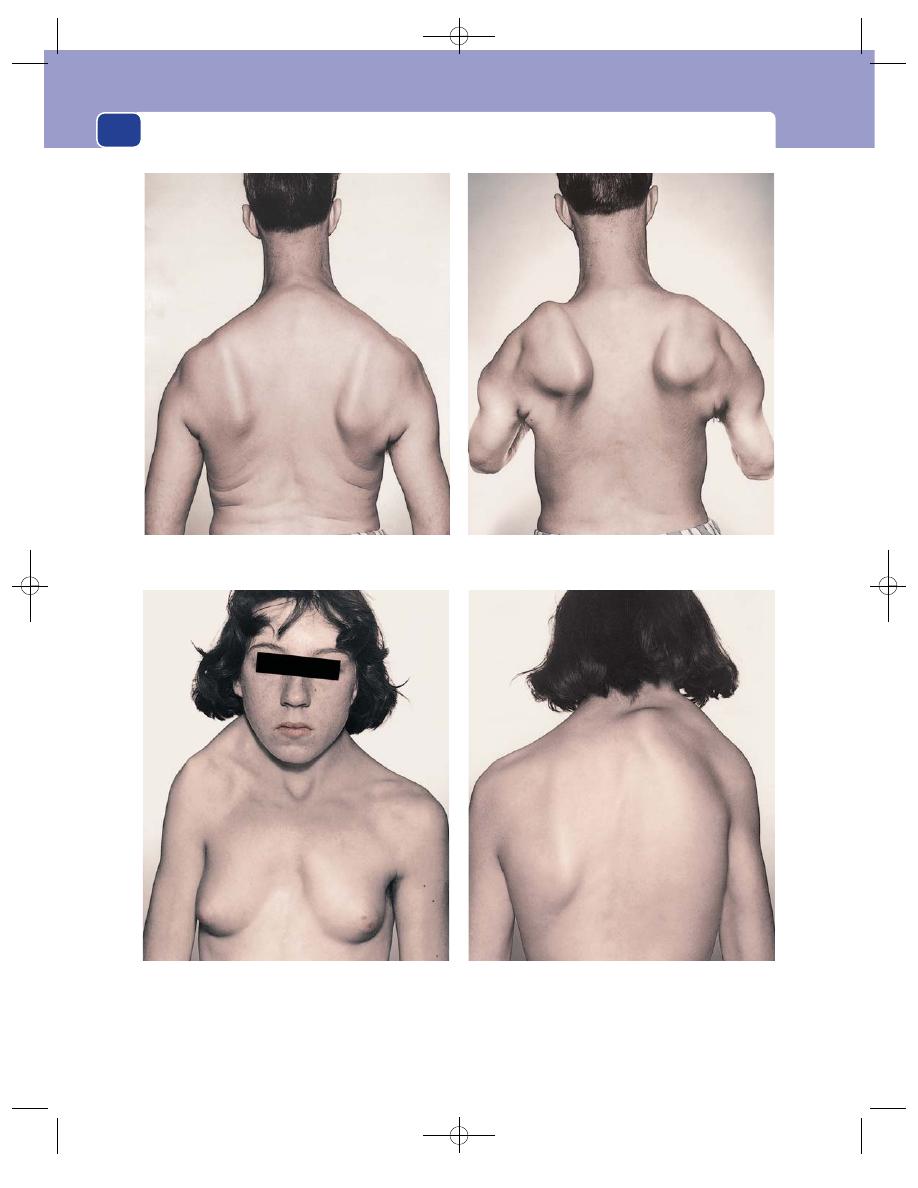
General and facial appearance
236
Winging of the scapulae, accentuated by asking the patient to hold out their arms in front of their trunk and press against a wall.
Sprengel’s shoulder: a congenitally high scapula.
FIG 8.30
SOME ABNORMALITIES AFFECTING THE APPEARANCE OF THE CHEST WALL.
Chap-08.qxd 4/19/05 14:14PM Page 236
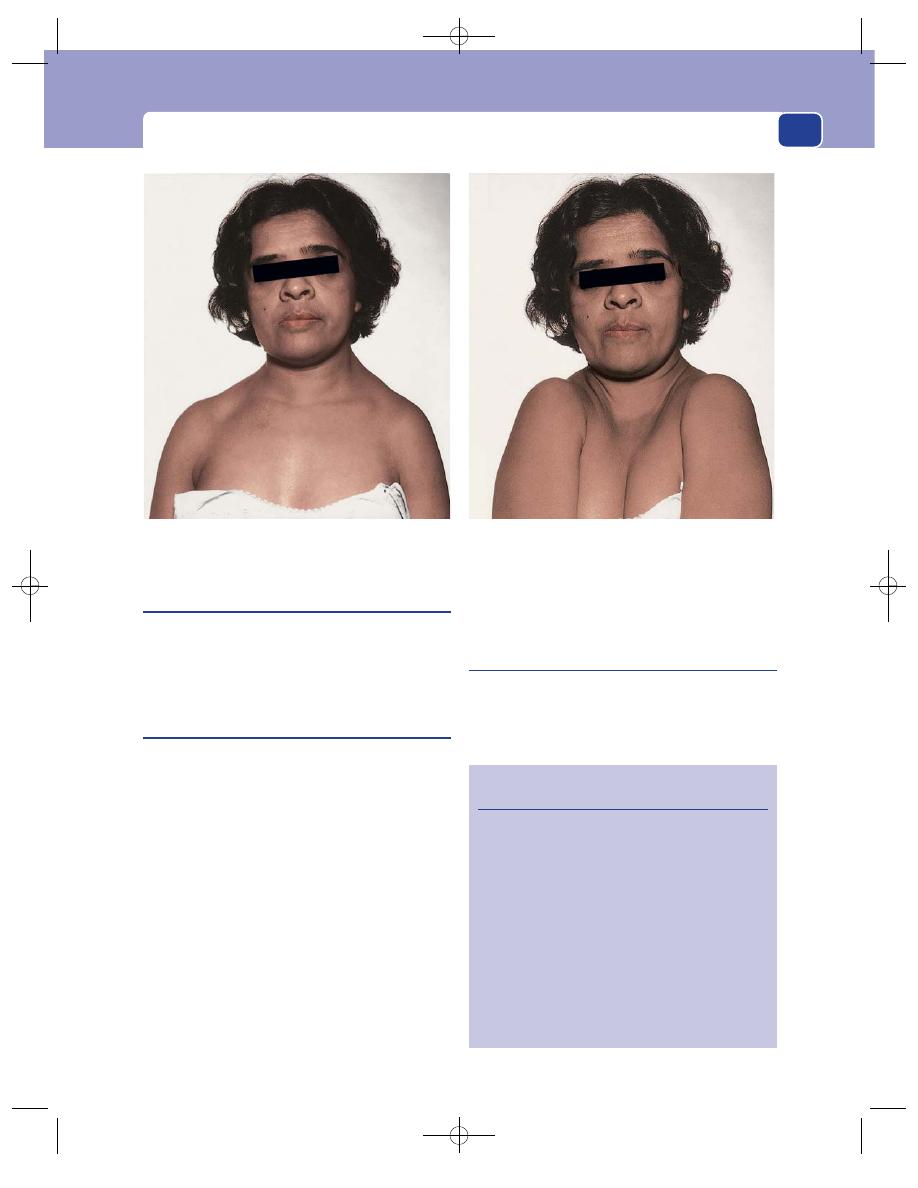
The chest wall
237
FIG 8.30
continued
Craniocleidodysostosis: congenital absence of the clavicles.
Craniocleidodysostosis
Craniocleidodysostosis is a rare inherited absence of
the clavicles. The patient is able to pull the shoulders
to the mid-line and distort the whole shape of the
chest.
Winging of the scapulae
The scapula is normally held against the chest wall
by the serratus anterior muscle. This muscle also
rotates and moves the scapula forwards around the
chest during those movements that involve holding
the arm out forwards.
The nerve to the serratus anterior (the long
thoracic nerve of Bell) may be divided or stretched
by direct trauma, carrying heavy weights or wear-
ing a knapsack, or be affected by a viral neuritis.
When the serratus anterior muscle is paralysed, the
scapula pokes out from the chest wall – a deformity
called ‘winging’. If a patient complains of weakness
of the arms or deformity of their back, remember
to ask them to put their hands and arms out
forwards and press against a wall. If the serratus
anterior muscle is paralysed, the scapula will pro-
trude backwards.
Myopathy affecting the serratus anterior muscle
will also cause ‘winging’.
Tietze’s syndrome
This is a condition which occurs in young women. It
is a painful swelling of the second, third and fourth
costal cartilages. The cause is unknown, but the
Revision panel 8.10
The causes of swellings of the chest wall
Bony hard
Secondary carcinoma
Chondroma
Osteoma
Exostosis (diaphyseal aclasis)
Myeloma
Fluctuant
Tuberculous abscess of rib or lymph gland
Empyema necessitas
Infected haematoma
Pulsatile
An eroding aortic aneurysm
Chap-08.qxd 4/19/05 14:14PM Page 237
symptoms, pain and swelling in or near the breast,
cause the patient great concern because she thinks
she has a carcinoma of the breast.
The diagnosis is based solely upon the clinical
detection of hard, immobile, tender swellings of
the costo-chondral junctions. It is a self-limiting
condition.
Lumps on the chest wall
The tissues that form the chest wall can give rise to
all the benign and malignant swellings that have
been described in Chapters 2, 3 and 4.
Chondromata and secondary tumours in the
ribs are quite common.
Aneurysms of the arch of the aorta eroding
through the sternum and causing sudden death by
rupturing are now extremely rare.
General and facial appearance
238
Chap-08.qxd 4/19/05 14:14PM Page 238
Saliva is produced by the paired parotid, sub-
mandibular and sublingual glands and many other
small, unnamed glands scattered beneath the buccal
mucous membrane.
The commonest surgical conditions affecting the
salivary glands are:
■
infection and calculus formation in the
submandibular gland,
■
tumours of the parotid gland.
Mumps is the commonest medical disease; all
other diseases of the salivary glands are uncommon.
THE SUBMANDIBULAR SALIVARY
GLAND
Submandibular calculi
Submandibular calculi are common because the
submandibular gland lies below the opening of its
duct on the floor of the mouth, and because the
secretion of the submandibular gland contains a
considerable quantity of mucus, two factors which
encourage stasis in the duct. Calculi in the parotid
gland are less common.
A salivary gland calculus is composed of cellular
debris, bacteria, mucus, and calcium and magne-
sium phosphates – a mixture similar to the ‘scale’
(tartar) that the dentist scrapes off our teeth.
History
Age
Most submandibular salivary calculi occur
in young to middle-aged adults. They are rare in
children.
Sex
Males and females are equally afflicted.
Symptoms
The main symptoms are pain and swelling
beneath the jaw, caused by obstruction of Wharton’s
duct.
These two symptoms vary in predominance.
Swelling is usually the principal complaint, because
it appears before, and persists after, the pain. The
pain is a dull ache, which occasionally radiates to
the ear or into the tongue.
Both symptoms appear, or worsen, before and
during eating. The swelling begins just before eating
and the pain develops as the gland enlarges. Both
symptoms last through the meal, but afterwards the
pain goes away before the swelling. If the gland
becomes irreparably damaged, the swelling persists
between meals and the dull aching pain may also
become constant.
Very rarely, the patient may notice discomfort
and a swelling in the floor of the mouth.
Patients may be able to relieve their symptoms by
pressing on the gland, and they may notice that this
action produces a foul-tasting fluid in their mouth
(purulent saliva).
Development
The symptoms may recur and remit for
periods of a few days or weeks if the stone moves
about in the duct, sometimes obstructing it, some-
times not.
If the stone passes through the orifice of the
duct, the symptoms disappear.
Persistent obstruction damages the gland, mak-
ing it harder and more tender.
Previous history
The patient may have had similar
symptoms on the other side of the face. Simultaneous
bilateral calculi are uncommon.
Examination
The lump
Position
The submandibular gland lies beneath the
horizontal ramus of the mandible on the mylohyoid
muscle. It is 2–3 cm in front of the anterior border
of the sternomastoid muscle and should not be
Chap-09.qxd 4/19/05 14:16PM Page 239
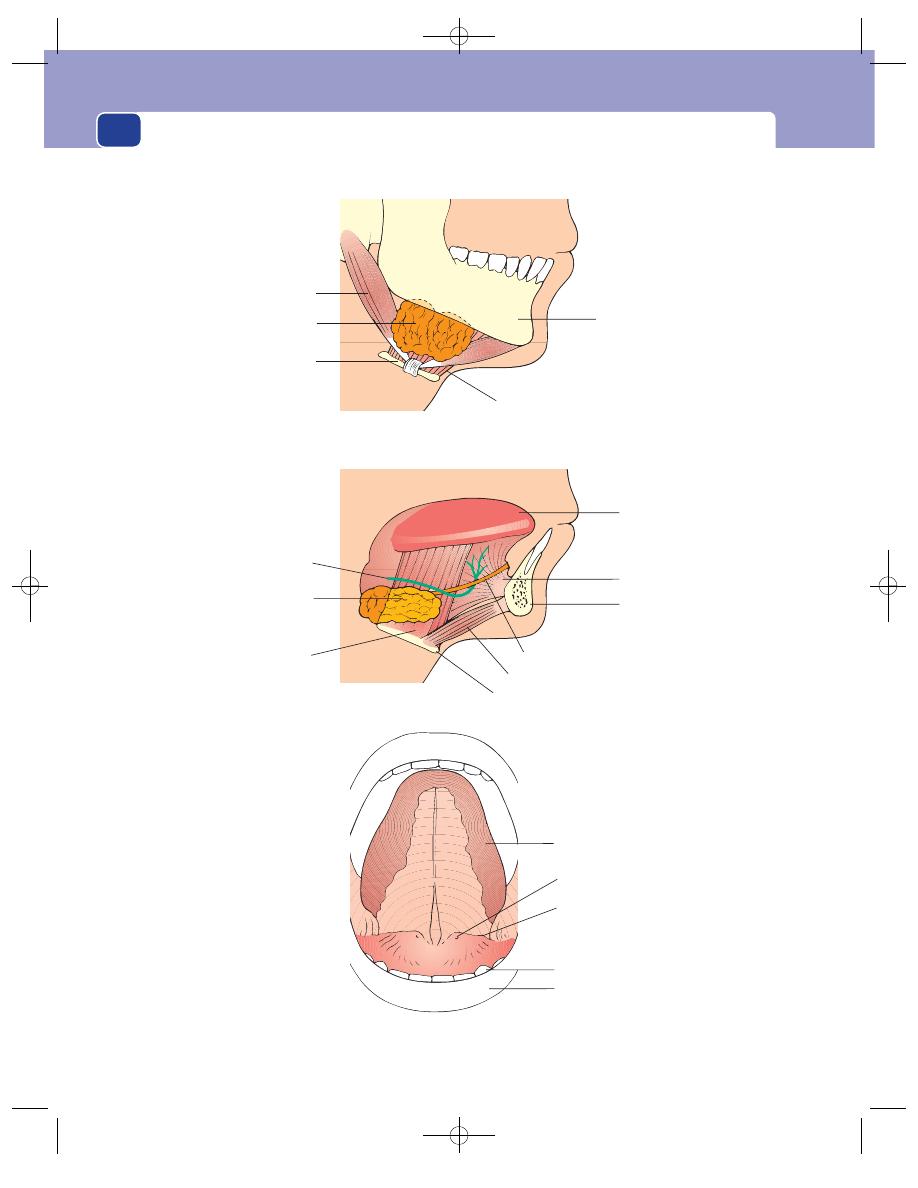
The salivary glands
240
Superficial part
Mandible
Mylohyoid
muscle
Hyoid cartilage
Digastric muscle
Superficial
part of gland
Tongue
Submucosal
course
of duct
Teeth
Lower lip
Orifice of duct
Deep part
Tongue
Jaw
Genioglossus
muscle
Geniohyoid muscle
Hyoglossus
muscle
Hyoid cartilage
Deep part
of gland
Lingual nerve
Duct
FIG 9.1
The anatomy of the submandibular gland.
Chap-09.qxd 4/19/05 14:16PM Page 240
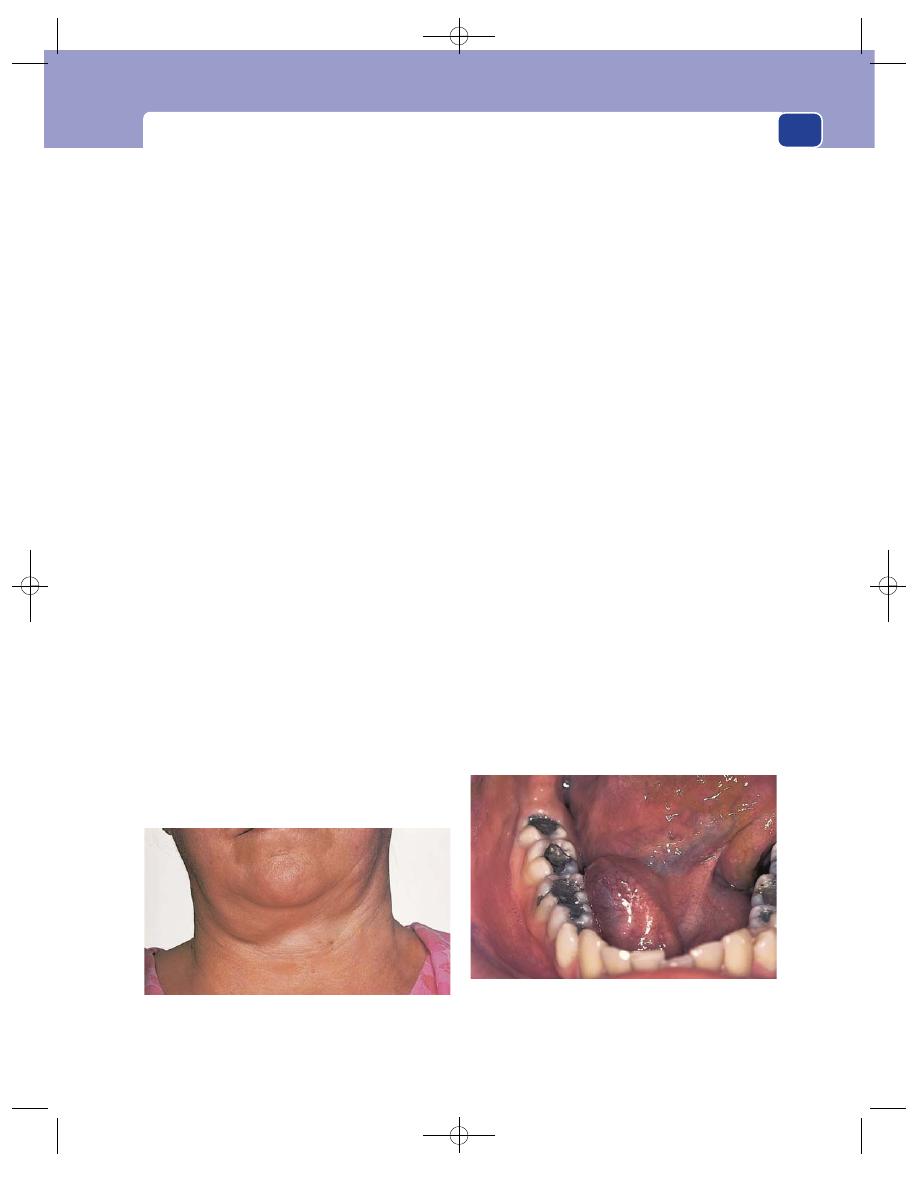
The submandibular salivary gland
confused with enlarged upper deep cervical lymph
glands, which are deep to the sternomastoid muscle.
Colour and temperature
If the gland is not infected, the
overlying skin will have a normal colour and tem-
perature. If the gland is infected, the skin becomes
red, oedematous and hot.
Tenderness
The gland is tender when it is tense
(before and during eating) but is not usually tender
between meals, unless it is infected.
Shape
The shape of the superficial part of the sub-
mandibular gland, and hence of the swelling, is a
flattened ovoid (almond shaped).
Size
If the gland is enlarged solely by obstruction of
its duct, it rarely becomes more than 3–5 cm across.
If it becomes infected, it may get much bigger.
Surface
Its surface is smooth but the lobules of the
gland may make it bosselated.
Edge
The anterior, posterior and inferior edges of
the gland are distinct and easy to define, but the
upper edge is wedged between the mandible and the
mylohyoid muscle and is impalpable.
Composition
A distended submandibular gland has a
rubbery, hard consistence and will not fluctuate,
transilluminate or reduce. It is dull to percussion
and has no bruit.
Occasionally, prolonged pressure on the gland
may make it a little smaller and produce a jet of
saliva from the orifice of the submandibular duct.
Relations
The skin is freely mobile over the swollen
gland. The gland itself can be moved a little from side
to side, but most movements are restricted by the
tethering of the gland to the underlying muscles.
When the muscles of the floor of the mouth are tensed
by asking the patient to push their tongue against the
roof of the mouth, the gland becomes less mobile.
It is important to ascertain the relations of the
lump to the floor of the mouth and the tongue by
bimanual palpation. Feel the lump between the
index finger of one hand inside the mouth (suitably
gloved), and the fingers of the other hand on the
outer surface of the lump.
It should be possible to appreciate that the lump
is outside the structures that form the floor of the
mouth. It should not be fixed to the mucosa of the
floor of the mouth or to the tongue.
Lymph drainage
The submandibular gland lymph
drains to the middle deep cervical lymph glands,
but there is also some lymphoid tissue within the
gland which can contribute to its enlargement.
The local lymph glands are usually not enlarged
unless the gland is infected.
Local tissues
The nearby tissues, except the sub-
mandibular duct in the floor of the mouth, should
be normal.
The floor of the mouth
Inspection
Ask the patient to open their mouth and
lift their tongue up to the roof of the mouth. This
displays the orifices of the submandibular ducts on
their small papillae on either side of the frenulum of
the tongue.
If a stone is impacted at the end of the duct, its
grey-yellow colour may be visible in the open orifice
of the duct.
241
FIG 9.2
A swollen right submandibular gland. Although some
of the swelling seems to spread over the jaw, the upper part
of the lump is actually deep to the mandible.
FIG 9.3
When a stone impacts at the end of the
submandibular duct, the floor of the mouth looks
asymmetrical. In this photograph there is a bulge over the
patient’s right duct. Palpation revealed a firm lump.
Chap-09.qxd 4/19/05 14:16PM Page 241
The salivary glands
The presence of a stone in the duct makes that
side of the floor of the mouth bulge upwards and
look pink.
Press the gland gently and watch for any discharge
from the orifice of the duct.
Palpation
Feel along the course of the duct in the
floor of the mouth for lumps and tenderness.
A stone in the duct will not feel stony hard if it is
small and surrounded by inflammatory oedema.
The lump caused by such a stone will feel soft with a
hard centre.
General examination
Examine all the salivary glands
in case the symptoms are due to a systemic disease
such as Sjögren’s syndrome (see page 249), not just
a stone.
Submandibular sialadenitis
Infection of a submandibular gland is invariably
secondary to the presence of a stone in its duct or
the damage done by a stone which has passed
through the duct. The infecting organism is usually
a staphylococcus.
The symptoms are identical to those caused by a
stone except that when the gland is infected the pain
is severe, throbbing, continuous and exacerbated
by eating.
The physical signs of the lump in the neck are
similar to those of the obstructed gland described
above, with the addition of heat and tenderness. An
infected gland may become quite big (5
⫻ 10 cm). If
the duct system becomes dilated (sialectasis), the
pus may pool in the gland and the whole structure
turn into a multilocular abscess, which may then
point externally onto the skin.
Submandibular salivary gland tumours
The tumours that often occur in the parotid gland –
pleomorphic adenoma, cylindroma and carcinoma –
may occur in the submandibular gland, but they
are rare.
The physical features of pleomorphic adenoma
and carcinoma in the submandibular gland are
identical to those of these tumours when they occur
in the parotid gland, apart from the site.
The pleomorphic adenoma forms a painless, slow-
growing, non-tender, hard, well-defined, spherical
mass within the gland. Carcinoma causes an indis-
tinct, hot, slightly tender, rapidly growing, painful
mass. Numbness of the anterior two-thirds of the
tongue indicates infiltration of the lingual nerve, and
is diagnostic of carcinoma.
It may be difficult to distinguish a pleomorphic
adenoma from enlargement of the lymph tissue
within the gland. A long history of slow, gradual
growth is the most useful distinguishing feature.
THE PAROTID GLAND
Acute bacterial parotitis
The commonest infection of the parotid gland is
mumps. This is an epidemic viral parotitis; when it
occurs in an epidemic with bilateral painful, swollen
glands and excessive oedema, which spreads down
into the neck, giving the child a double chin, it is
easy to diagnose.
When it causes unilateral gland enlargement, little
pain, no oedema, and there are no obvious contacts
with the infection, it can be much more difficult to
diagnose.
Remember, mumps is the commonest cause of
parotitis.
Non-specific parotitis, usually a staphylococcal
infection, is caused by:
■
poor oral hygiene
■
dehydration
■
obstruction of Stensen’s duct by stone or scar
tissue.
In the days before the fluid balance of sick patients
was properly controlled, fulminating parotitis with
a subsequent septicaemia was a common cause of
death.
History
Age
Acute parotitis is more common in the elderly
and the debilitated.
Symptoms
The patient complains of the sudden
onset of pain and swelling in the side of the face.
The pain is continuous and throbbing, and radi-
ates to the ear and over the side of the head.
Speaking and eating cause pain because any move-
ment of the temporo-mandibular joint is painful.
The patient feels hot, sweaty and ill and may
complain of shivering attacks (rigors).
242
Chap-09.qxd 4/19/05 14:16PM Page 242
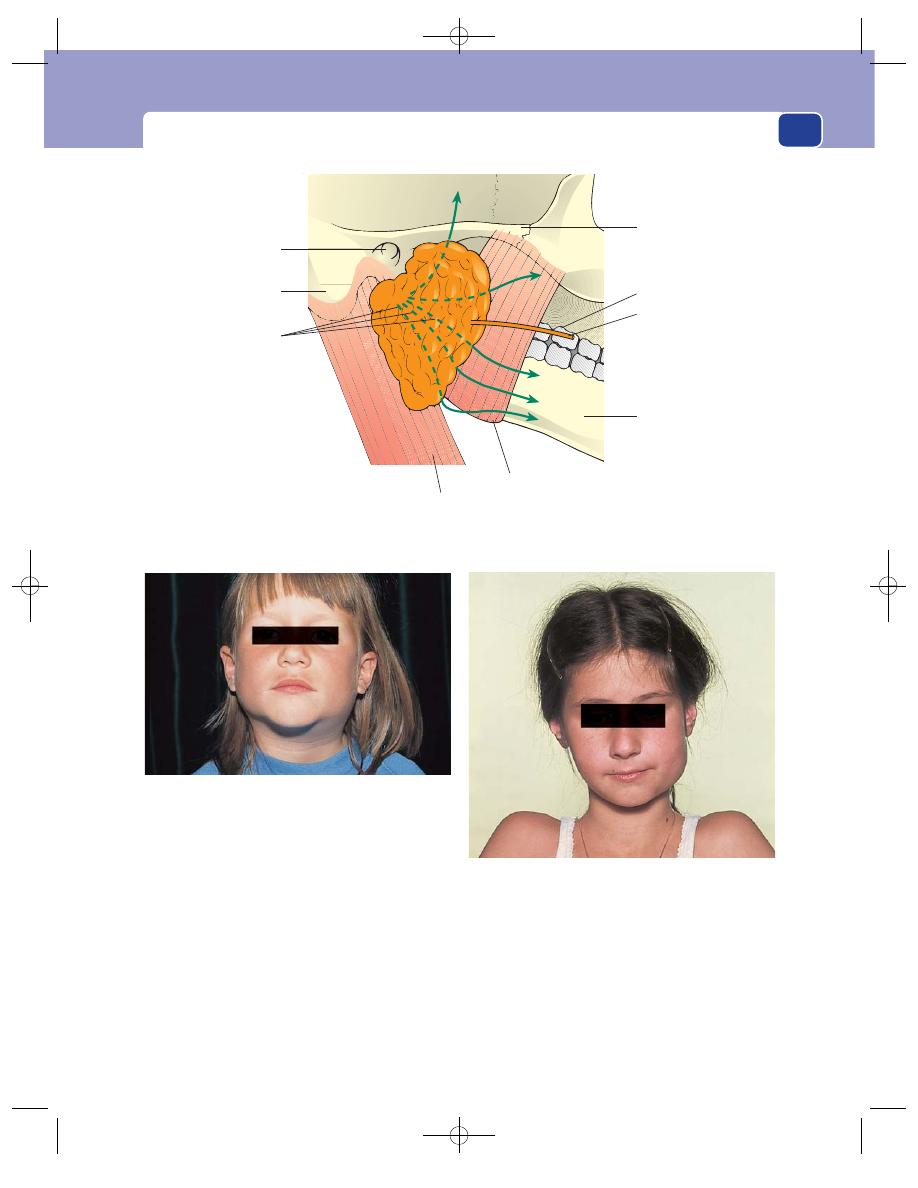
The parotid gland
Systematic questions
The answers to these questions
may reveal symptoms of another illness, such as a
bronchial carcinoma, which has caused the debility
and dehydration.
Previous history
The patient may have recently under-
gone a major operation or suffered a severe medical
illness.
Examination
The lump
Position
The parotid gland lies in front of and below
the lower half of the ear. It is wrapped around the
vertical ramus of the mandible, with its deep portion
in between this bone and the mastoid process.
In acute parotitis the whole gland is swollen, so
the whole of the face in front of the lower half of the
ear bulges outwards.
243
Zygoma
Stensen's duct
2nd upper molar
Mandible
Masseter muscle
Sternomastoid muscle
Branches of the
facial nerve
External auditory
meatus
Mastoid process
FIG 9.4
The anatomy of the parotid gland. N.B. The parotid gland extends below and behind the angle of the
mandible. Lumps in this part of the gland are easily mistaken for enlarged upper deep cervical lymph glands.
FIG 9.6
Unilateral mumps. A young girl with diffuse swelling
of the left parotid gland caused by mumps. Much of the
swelling is caused by oedema.
FIG 9.5
Bilateral mumps in a young girl.
Chap-09.qxd 4/19/05 14:16PM Page 243
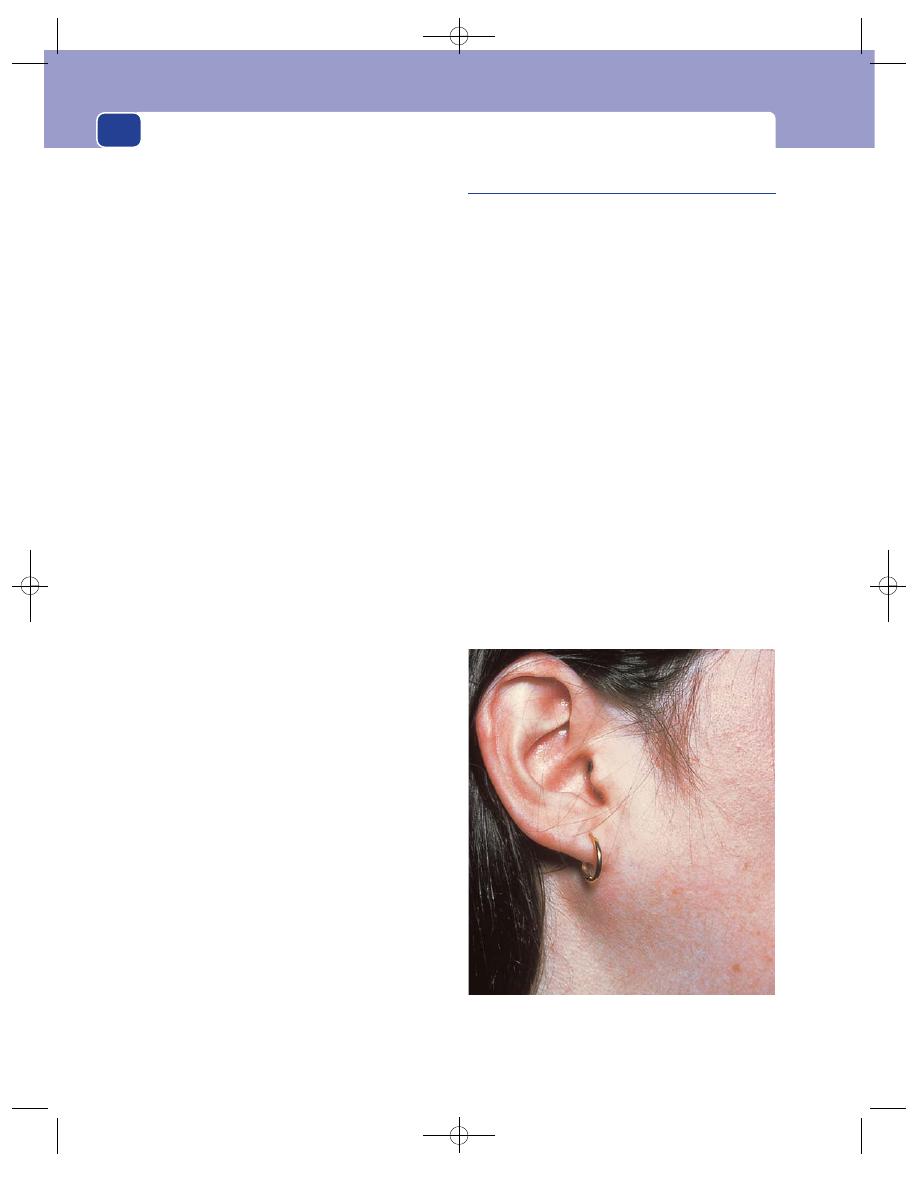
The salivary glands
Colour and temperature
The skin over the swelling is dis-
coloured a reddish-brown, feels hot, and is smooth
and shiny.
Tenderness
The swelling is very tender.
Shape
The mass has the shape of the normal parotid
gland: a semicircular anterior edge, a vertical edge
just in front of the ear, and a bulge running into
the gap between the mandible and the mastoid
process.
Size
The swollen gland may be three or four times
larger than a normal gland.
Surface
Its surface is smooth but difficult to define
because of the oedema, inflammation and tenderness.
Composition
The texture of the swelling is often
described as brawny. This means that it has a firm
consistence but is indentable. It is dull to percus-
sion, not fluctuant and not compressible.
Relations
If the overlying skin is red and oedematous,
it will be tethered to the swelling. The swelling cannot
be moved over the deep structures and becomes
more prominent when the patient contracts the
masseter muscles by clenching their teeth.
Lymph drainage
The upper deep cervical lymph
glands are usually enlarged and tender.
Local tissues
Apart from the changes in the skin, and
the restricted movements of the temporo-mandibu-
lar joint, the surrounding tissues are normal. The
function of the facial nerve is not impaired.
The mouth
Inspection
Remember that the orifice of Stensen’s
duct is opposite the second upper molar tooth.
The mouth of the duct may be patulous and the
buccal mucosa over the course of the duct slightly
oedematous.
Palpation
Feel the mouth of the duct for any thick-
ening or lumps.
The parotid gland cannot be palpated bimanu-
ally because it lies behind the anterior edge of the
masseter muscle and the vertical ramus of the
mandible.
Gentle pressure on the gland may produce a
purulent discharge from the orifice of the duct.
Chronic parotitis
Chronic parotitis is usually caused by a small calcu-
lus or a fibrous stenosis blocking the mouth of
Stensen’s duct.
History
The patient complains of recurrent swelling of the
parotid gland. The swelling is particularly noticeable
before eating and is associated with an aching pain.
In severe cases the gland becomes permanently
swollen, but the pain does not usually become
constant.
Chronic parotitis is sometimes bilateral.
Examination
The whole gland is easy to feel because it is slightly
bigger and firmer than a normal gland and its
edges are distinct. It is also tender and feels rubbery
hard.
If there is partial obstruction to the flow of saliva,
pressure on the gland may produce a copious squirt
of fluid through the orifice of the duct.
Examine all the other salivary glands to exclude a
general abnormality.
244
FIG 9.7
Chronic parotitis. A firm, slightly tender enlargement
of the whole of the parotid gland caused by recurrent
infection secondary to a stone in Stensen’s duct.
Chap-09.qxd 4/19/05 14:17PM Page 244
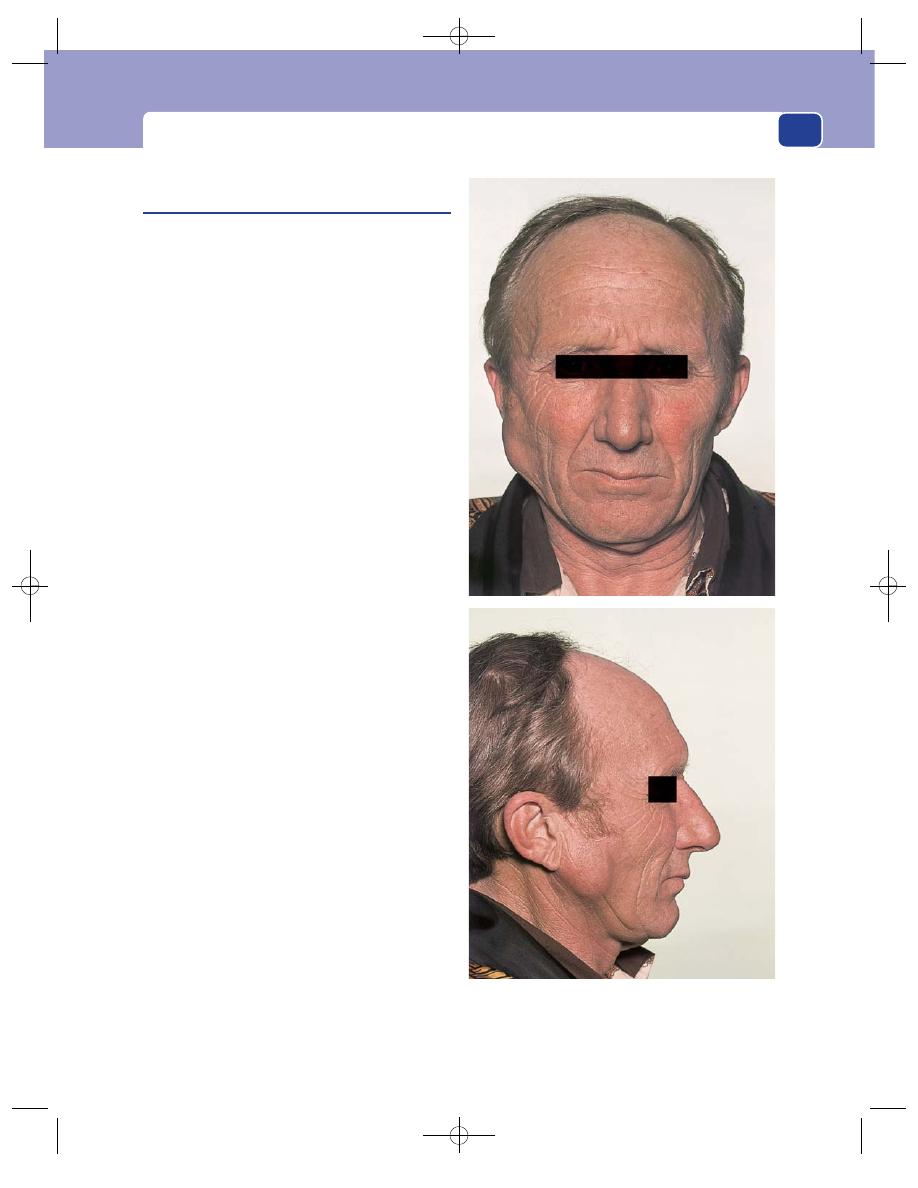
The parotid gland
Pleomorphic adenoma
(Mixed parotid tumour, sialoma)
This is a true adenoma of the parotid gland. Its mixed
histological appearance gave rise to its old name,
mixed parotid tumour, and its currently favoured
name, pleomorphic adenoma. It has also been called
a sialoma.
It is a slow-growing adenoma with an incom-
plete capsule. The small pieces of tumour that pro-
trude through the defects in its capsule limit its
treatment by enucleation and allow its rapid exten-
sion if it turns malignant. After many years of slow,
benign growth, a small proportion of adenomata
become locally invasive.
History
Age
These tumours appear in early and middle
adult life.
Sex
They occur more often in males than in females.
Symptoms
The patient complains of a painless
swelling on the side of their face which has been pres-
ent for months or years and which is slowly growing.
The lump may be more prominent when the
mouth is open, or when eating. The latter symptom
can cause confusion, so it is important to find out
whether the lump just becomes more prominent
because of contraction of the masseter muscle or
actually increases in size.
Examination
Position
The majority of parotid adenomata begin
in the portion of the gland that lies over the junction
of the vertical and horizontal rami of the mandible,
just anterior and superior to the angle of the jaw.
Why the majority begin here is not known, for
they can occur in any part of the gland.
Colour and temperature
The temperature and colour
of the overlying skin are normal.
Tenderness
The lump is not tender.
Shape
Most pleomorphic adenomata are spherical
when they are small, but as they grow they become
flat on their deep surface and slightly pointed super-
ficially. They may become lobulated when very large.
Size
These tumours can vary from pea-sized nodules
to large, almost pendulous, masses, 20 cm across.
245
FIG 9.8
A pleomorphic adenoma. These photographs show
the typical site, the healthy overlying skin, the absence of
facial nerve involvement and the lobulation that develops as
the tumour grows.
Chap-09.qxd 4/19/05 14:17PM Page 245
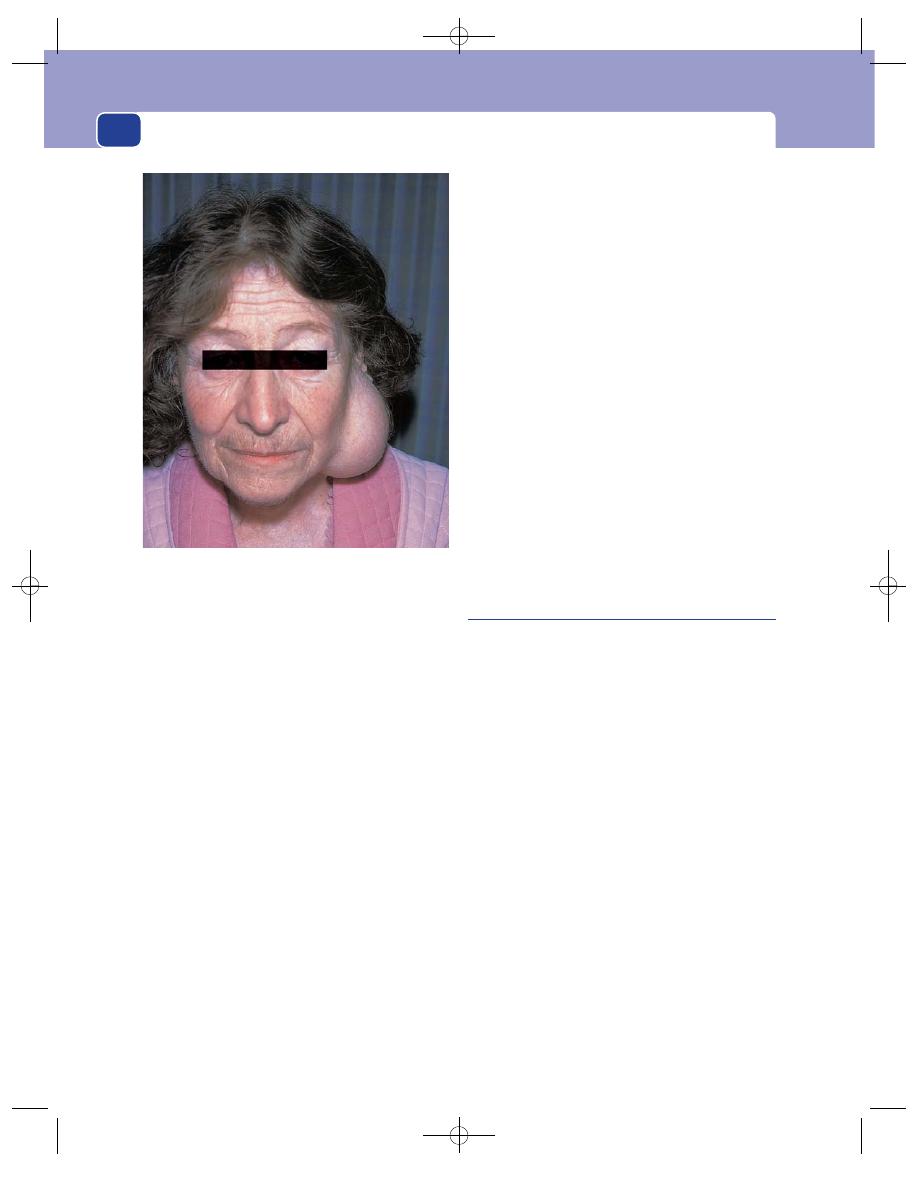
The salivary glands
Surface
Their surface is smooth, sometimes bosse-
lated, and occasionally crossed by deep furrows.
The surface of any deep extension between the
mandible and the mastoid process is impalpable.
Edge
The edge is quite distinct and easy to feel.
Composition
The tumour mass has a rubbery, hard
consistence, is dull to percussion, not fluctuant or
translucent, and not compressible.
Relations
The overlying skin and the ear are freely
movable, not attached to the lump.
Small tumours can be moved about over the
deep structures, but large tumours are less
mobile.
Lymph drainage
The cervical lymph glands should
not be enlarged.
Local tissues
Apart from any distortion caused by
the mass, the local tissues should be normal. In par-
ticular, the facial nerve should function normally.
Paralysis of any facial muscles indicates infiltration
of the nerve, which means that the lump is a car-
cinoma, not a benign adenoma.
Examine the inside of the mouth
A pleomorphic adenoma in the deep part of the
parotid gland will push the tonsil and the pillar of
the fauces towards the mid-line.
Differential diagnosis
Remember that the pre-auricular lymph gland may
be enlarged by secondary infection or metastases
from a tumour in the forehead, scalp, eyelids, cheek
or external auditory meatus. The resulting firm,
smooth swelling just in front of the tragus can be
indistinguishable from a pleomorphic adenoma if it
is not tender and there are no obvious abnormal-
ities in its drainage area.
The most distinctive physical sign of an enlarged
pre-auricular lymph gland is its mobility. Most
tumours in the parotid gland can only be moved a
short distance because they are tethered to the
gland; the pre-auricular lymph gland lies outside
the capsule of the parotid gland and is usually very
mobile.
Adenolymphoma
(Warthin’s tumour)
This is a cystic tumour which contains epithelial
and lymphoid tissues. The epithelial element is
believed to originate from embryonic parotid ducts
that have become separated from the main duct sys-
tem of the gland. The lymphoid element comes
from normal lymph tissue that happened to be close
to the developing gland.
The tumour arises on the surface of, or just
beneath, the capsule of the parotid gland.
History
Age
Adenolymphomata appear in middle and old age.
Sex
They are more common in men than in women.
Ethnic group
It does not occur in Negroes.
Symptoms
The patient complains of a slow-growing,
painless swelling over the angle of the jaw. The
swelling may be bilateral.
Examination
Position
The adenolymphoma usually develops in the
lower part of the parotid gland, level with the lower
246
FIG 9.9
A very large, almost pendulous, pleomorphic
adenoma of the parotid gland.
Chap-09.qxd 4/19/05 14:17PM Page 246
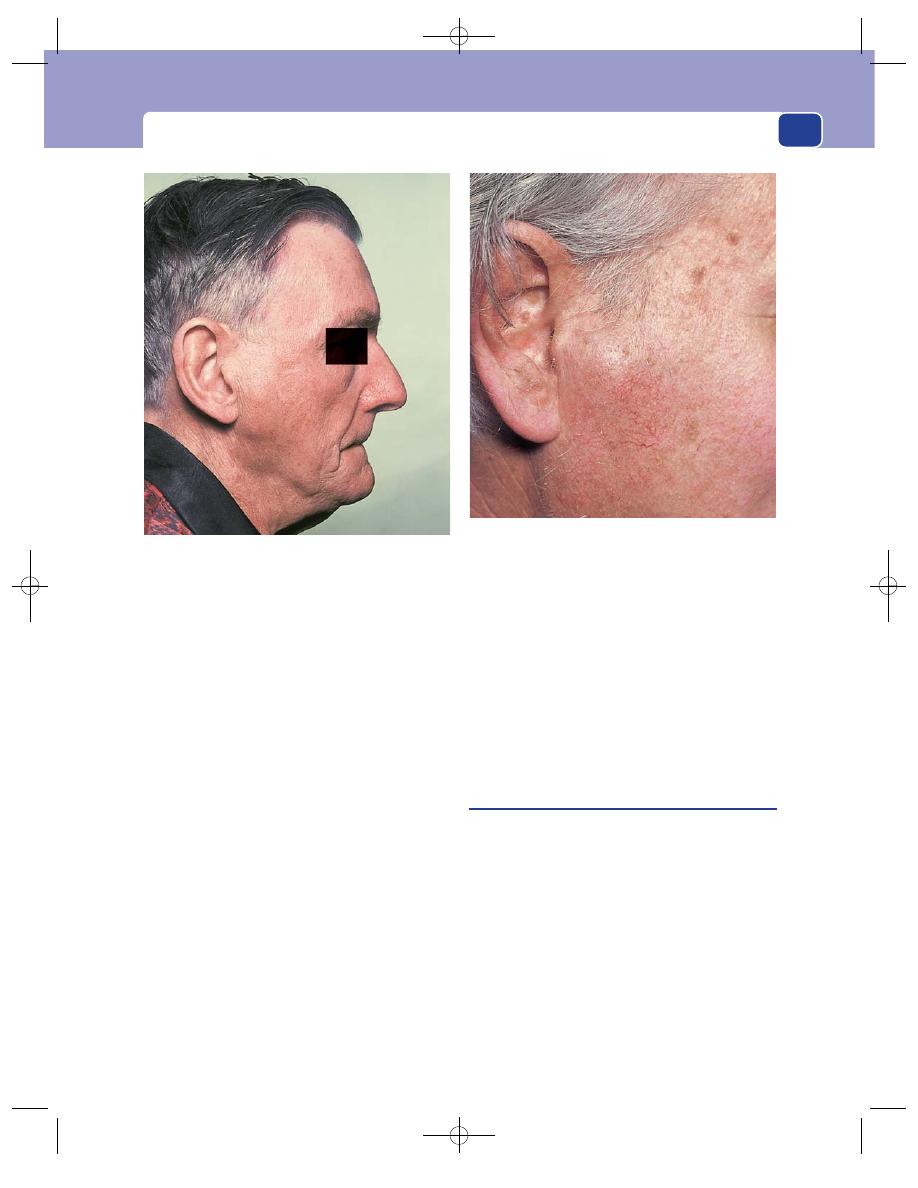
The parotid gland
border of the mandible. This is slightly lower than the
common site of origin of the pleomorphic adenoma.
Temperature and colour
The overlying skin looks and
feels normal.
Tenderness
The lump is not tender.
Shape
Adenolymphomata are spherical or hemi-
spherical.
Size
They are usually 1–3 cm in diameter.
Surface
The surface is smooth and well defined.
Edge
Its edge is distinct and sometimes makes the
lump seem separate from the parotid gland.
Composition
Adenolymphomata have a soft consist-
ence, are dull to percussion and not translucent, but
they often fluctuate. The fluctuation is sometimes a
true sign of the fluid content of the cysts, but more
often is a reflection of the soft, solid consistence and
strong capsule.
Relations
The lump can usually be moved a little in
all directions and is not attached to the skin.
Lymph drainage
The cervical lymph glands should
not be enlarged.
Local tissues
The adjacent tissues are all normal.
The site and consistence of the lesion are the fea-
tures which make one suspect that a parotid
swelling is an adenolymphoma.
Carcinoma of the parotid gland
Carcinoma of the parotid gland is uncommon, but
not very rare. It can arise de novo, or in a long-
standing pleomorphic adenoma.
History
Age
The patient is usually over the age of 50 years.
Sex
Males and females are equally affected.
Symptoms
The common complaint is of a rapidly
enlarging swelling on the side of the face. The
swelling is persistently painful, especially during
movements of the jaw. The pain may radiate to the
ear and over the side of the face. The patient may
247
FIG 9.10
Warthin’s tumour. An adenolymphoma of the
parotid gland. This photograph shows the typical site of an
adenolymphoma – just over the angle of the jaw. Although it
looks similar to the pleomorphic adenoma shown in Fig. 9.8,
it had a soft consistence.
FIG 9.11
Carcinoma of the parotid gland. This patient
complained of a painful swelling in front of his ear. The
swelling was hot and the overlying skin reddened. Although
the swelling was not very large, there was some weakness
of the muscles of facial expression.
Chap-09.qxd 4/19/05 14:17PM Page 247
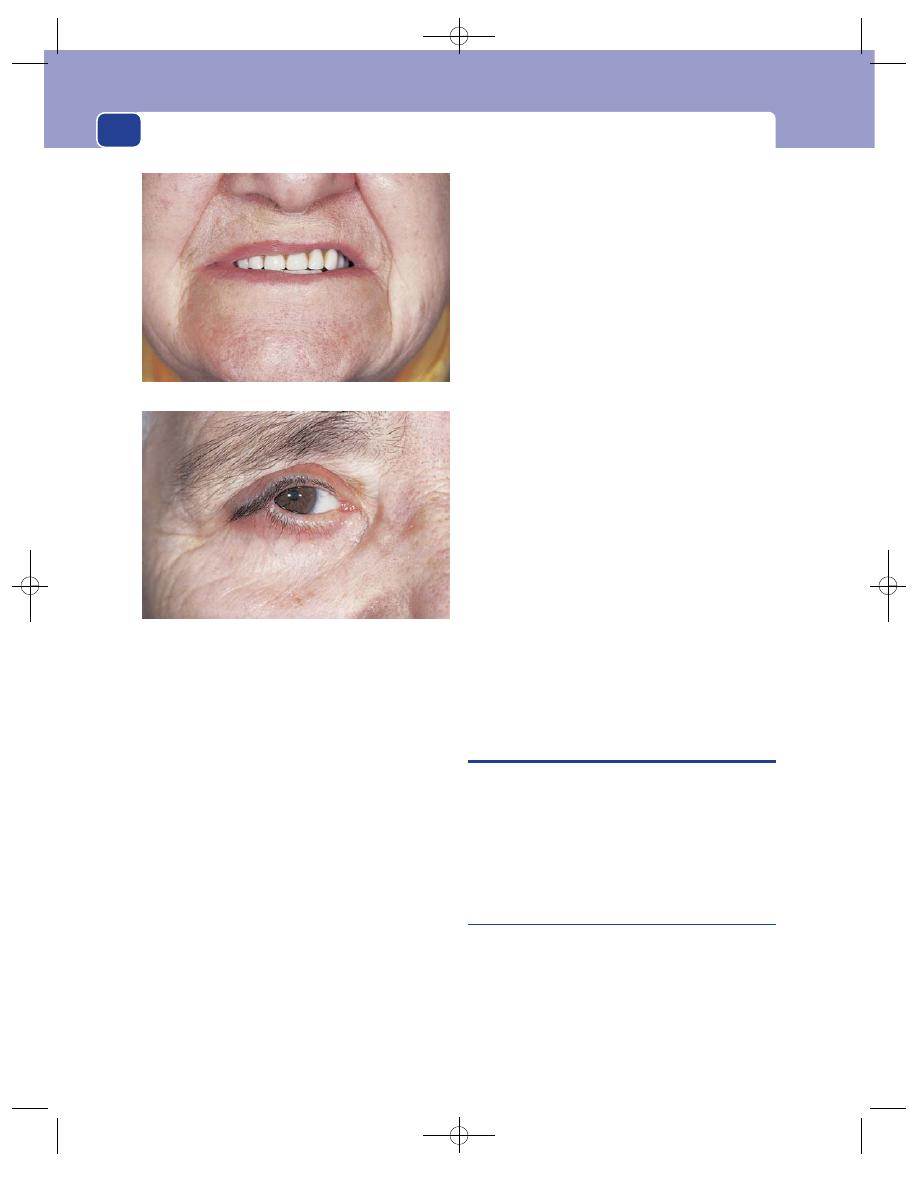
The salivary glands
give a history of a preceding painless lump that has
been present for many years.
The patient may also complain of asymmetry of
the mouth and difficulty in closing the eyes. When
this is marked, the patient may require a lateral tar-
sorrhaphy to protect the cornea from exposure and
ulceration.
Examination
Position
The swelling is in the site of the parotid
gland.
Colour
If the overlying skin is being infiltrated by the
tumour it may be reddish-blue.
Temperature
The skin and the mass are hyperaemic
and hot.
Tenderness
The mass is not very tender, an import-
ant difference from acute parotitis, which also pres-
ents with a hot swelling.
Shape
The tumour may be of any shape. It is basic-
ally a flattened hemisphere but, as it spreads in dif-
ferent directions, its shape becomes irregular.
Size
Its size increases inexorably.
Surface
The surface is smooth but irregular.
Edge
The edge is often indistinct.
Composition
The mass has a firm, sometimes hard
consistence, is dull to percussion, but is not fluctu-
ant or translucent. Although it may be very vascular,
it does not have an audible bruit.
Relations
Carcinoma of the parotid becomes fixed to
the deep structures early in its growth and may also
become fixed to, and infiltrate, the skin.
The thickening of the tissues around the tem-
poro-mandibular joint may restrict jaw movements.
Lymph drainage
The cervical lymph glands are likely
to be enlarged and hard.
Local tissues
If the facial nerve is infiltrated by
tumour, the patient will be unable to use the muscles
of facial expression. The signs may vary from mild
weakness of the lower lip when baring the teeth, to a
complete seventh nerve palsy.
If the tumour has infiltrated into the mandible,
the jaw may be swollen and tender.
General examination
There may be evidence of dis-
seminated blood-borne metastases.
AUTOIMMUNE DISEASE
There are two syndromes of slow, progressive, but
relatively painless enlargement of the salivary glands,
in which biopsy reveals that the swelling is caused
by replacement of the glandular tissue by lymphoid
tissue. Both conditions are believed to be auto-
immune diseases.
Mikulicz’s syndrome
Mikulicz’s syndrome is:
■
enlargement of the salivary glands: usually both
parotid and both submandibular glands enlarge,
but the syndrome can begin and remain in one
gland for quite a long time;
■
enlargement of the lachrymal glands: this
causes a bulge at the outer end of the upper
248
FIG 9.12
FACIAL NERVE WEAKNESS CAUSED BY A
CARCINOMA OF THE PAROTID GLAND.
Asymmetry of the mouth.
Lateral tarsorrhaphy to protect the cornea from ulceration.
Chap-09.qxd 4/19/05 14:17PM Page 248

Autoimmune disease
249
The submandibular swelling in this woman was a lymph gland
enlarged by secondary deposits from a carcinoma of the
tongue.
Pre-auricular lymphadenopathy is a condition which is
commonly mistaken for parotid gland enlargement. However, this
woman’s pre-auricular swelling was caused by a secondary
deposit of carcinoma in the ascending ramus of the mandible.
This ulcerating lesion over the parotid gland was initially
diagnosed as a parotid carcinoma. However, there was no
facial weakness and the lesion was actually in the skin.
A biopsy revealed that it was a squamous cell carcinoma of
the skin.
eyelids and narrowing of the palpebral
fissures;
■
a dry mouth, which may be the presenting
symptom: the patient is not thirsty.
It may be associated with lymphoma, leukaemia,
sarcoidosis and tuberculosis.
Sjögren’s syndrome
Sjögren’s syndrome is all the above conditions,
although the degree of salivary gland enlargement is
often not so gross, plus:
■
dry eyes
■
generalized arthritis.
Revision panel 9.1
Causes of swelling of a salivary gland
Acute infection
Viral (e.g. mumps)
Bacterial (e.g. Staphylococcus)
Duct obstruction
Sialectasis (chronic infection)
Tumour
Benign
Malignant
Sarcoidosis (Mikulicz’s syndrome)
Sjögren’s syndrome
FIG 9.13
NOT ALL SWELLINGS IN THE PAROTID AND SUBMANDIBULAR REGIONS ARE CAUSED BY SALIVARY GLAND ENLARGEMENT.
Chap-09.qxd 4/19/05 14:17PM Page 249
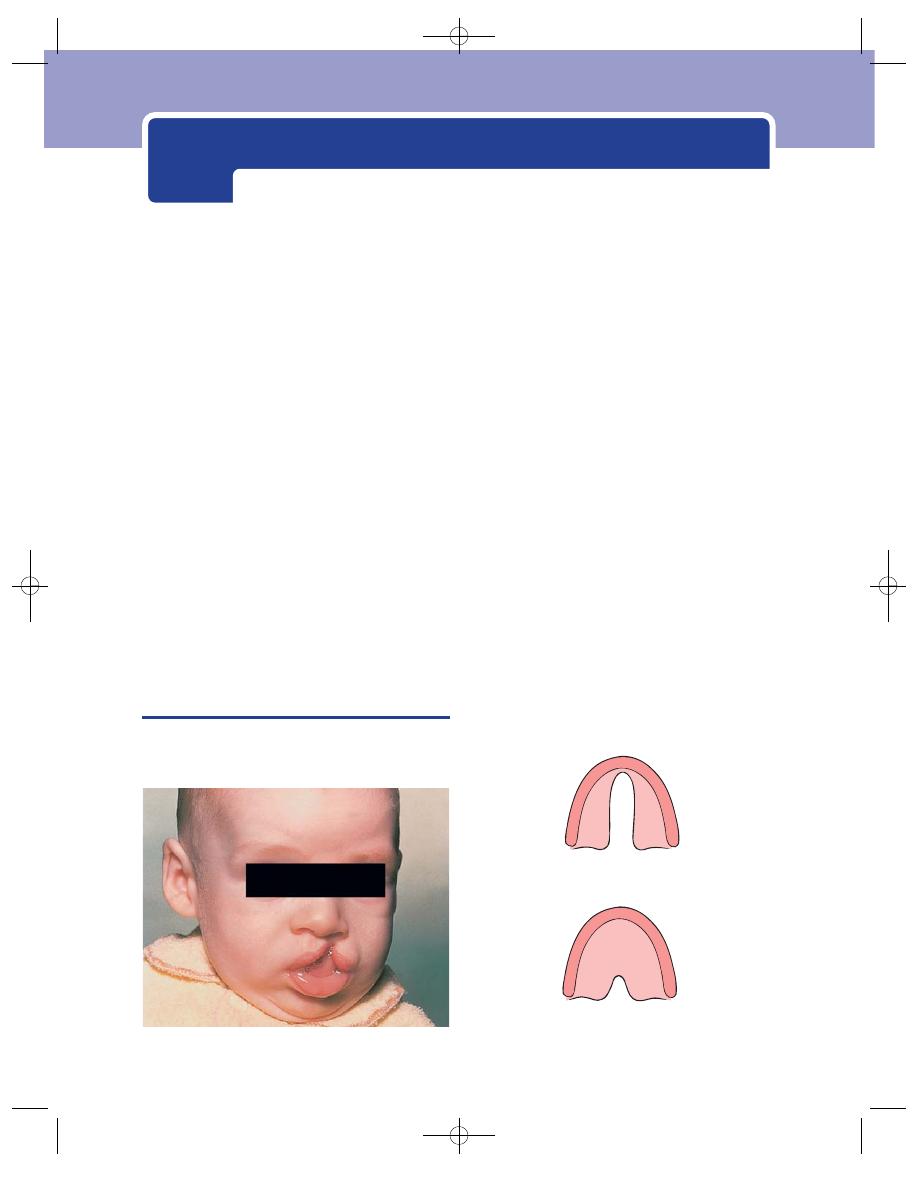
Always inspect the mouth with a good light and use
a spatula.
■
Inspect the external appearance of the lips.
■
Retract the lips to see the buccal mucosa.
■
Push the cheek outwards to see the buccal side
of the gum.
■
Push the tongue away from the inside of the
gum and the floor of the mouth.
■
Push the tongue to one side to see the lateral
aspect of its posterior third.
■
Depress the tongue to look at the fauces, tonsils
and pharynx.
Always remember to palpate the structures in
the mouth bimanually, one finger inside and one
outside. Always wear a finger cot or, if there is any
possibility that the lesion is contagious, a glove.
CONGENITAL ABNORMALITIES OF
THE LIPS AND PALATE
The face, jaw and palate are formed by the fusion of
the frontonasal, maxillary and mandibular processes.
■
The frontonasal process forms the nose, the
nasal septum, the nostrils, the philtrum of the
upper lip and the premaxilla.
■
The maxillary processes form the cheek, the
upper lip (except the philtrum), the upper jaw
and palate.
■
The mandibular processes form the lower jaw
and lip.
Failure of these processes to meet and fuse pro-
duces a group of congenital abnormalities: cleft lips,
cleft palates and facial clefts.
Half of the infants with a cleft lip also have a cleft
palate.
Complete failure of fusion causes a bilateral
cleft lip, a cleft palate and a protuberant premaxilla.
The diagnosis is apparent from inspection of the lip
and palate.
Partial failure of fusion causes unilateral cleft
lip and a unilateral cleft of the palate which may be
complete or partial.
FIG 10.1
A child with a simple cleft lip.
A partial cleft of the hard and soft palates
A partial cleft of the soft palate
FIG 10.2
The varieties of a simple cleft palate.
(Lips, teeth, tongue, tonsils, palate and jaw)
Chap-10.qxd 4/19/05 14:18PM Page 250
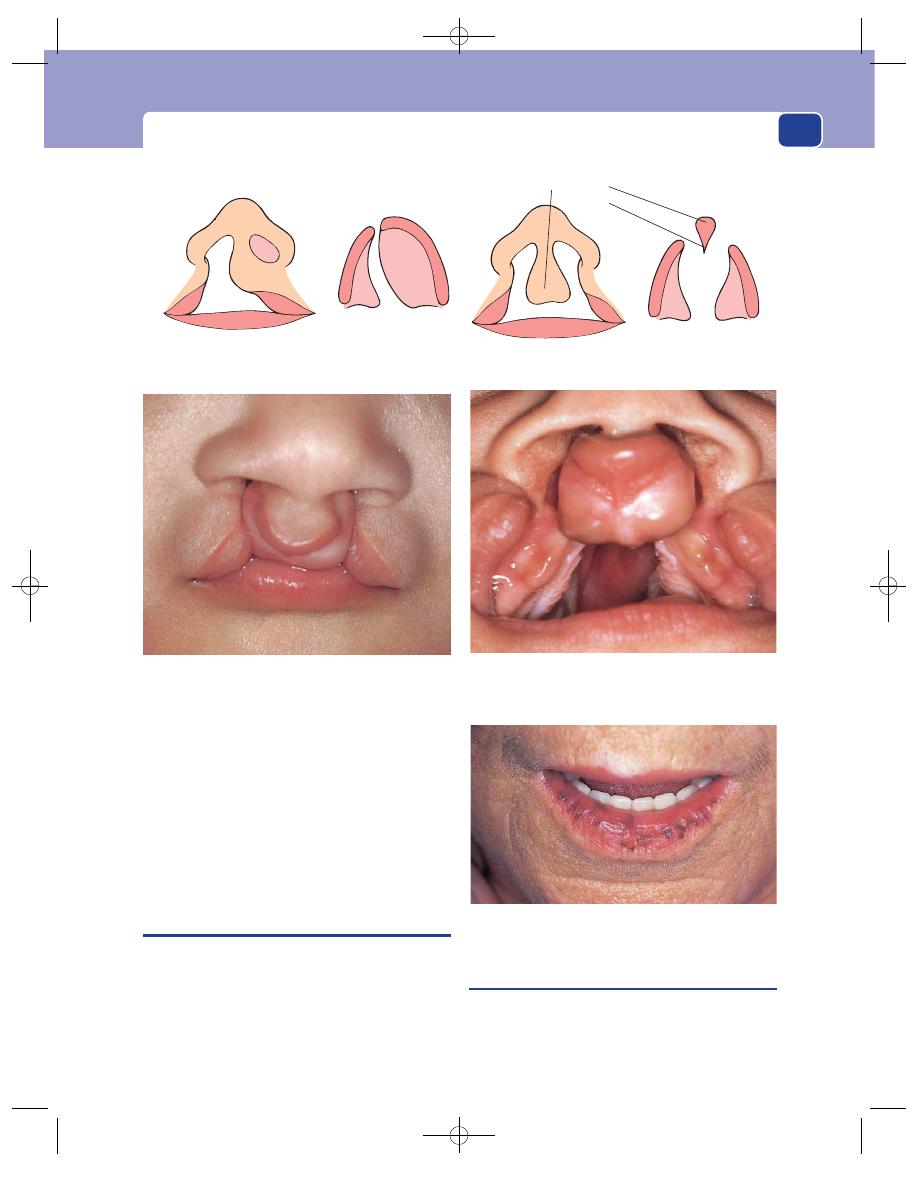
The lips, buccal mucosa and tongue
251
Rare varieties of failure of fusion may cause a
central cleft of the lower lip and jaw, and a facial
cleft between the maxilla and the side of the nose.
The symptoms of cleft lip and palate, apart from
the disfigurement, are an inability to suckle, inter-
ference with speech (particularly the formation of
consonants such as D, T and G) and distortion of
the dental arch.
THE LIPS, BUCCAL MUCOSA AND
TONGUE
Begin by inspecting the external appearance of the
lips for any discolouration, pigmentation such as that
of Addison’s disease or the Peutz–Jegher syndrome or
the telangiectasia of Rendu–Osler–Weber syndrome,
before looking for any swellings or irregularities in
the buccal mucosa lining the inside of the mouth.
Mucous retention/extravasation cysts
The inner surface of the lips, and the whole of the
inside of the mouth, are covered with an epithelium
that contains many small mucus-secreting glands.
Unilateral cleft lip
Complete unilateral
cleft palate
Bilateral cleft lip
Complete bilateral
cleft palate
Premaxilla
Vomer
A baby with a bilateral cleft lip and cleft palate. Note the way in which the premaxilla protrudes.
FIG 10.4
The pigmentation of the lips seen in the
Peutz–Jegher syndrome.
FIG 10.3
CLEFT LIP AND CLEFT PALATE COMBINED.
Chap-10.qxd 4/19/05 14:18PM Page 251
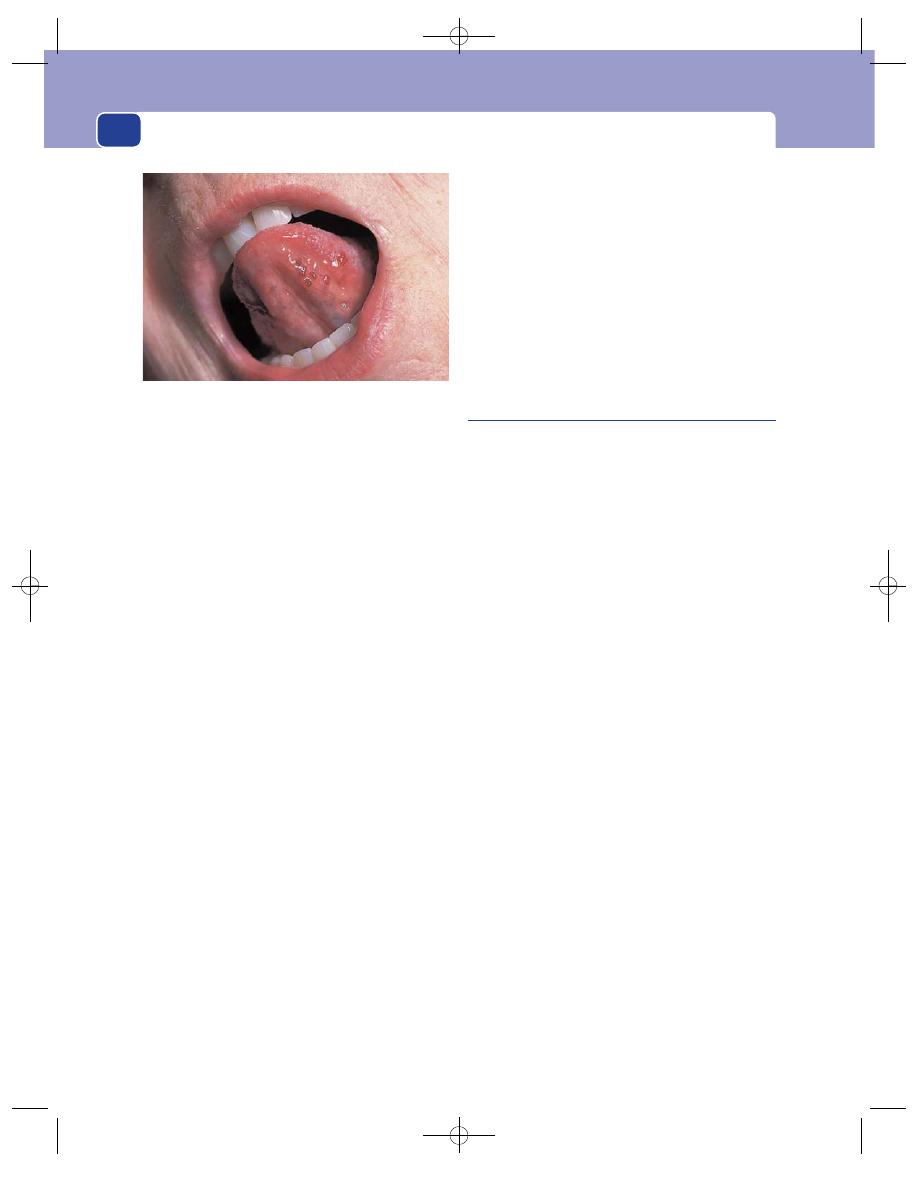
The mouth
252
Obstruction of the duct of one of these glands
may cause a mucous retention cyst or may cause the
gland to rupture and so initiate the formation of a
mucous extravasation cyst.
These cysts are common and often rupture spon-
taneously or get bitten through.
History
Age
Mucous retention cysts occur at all ages.
Symptoms
The patient complains of a lump on the
inner side of the lip or cheek. It is not painful, but
grows slowly and may interfere with eating and get
bitten.
Examination
Position
Mucous retention cysts are most common
on the lower lip and in the buccal mucous mem-
brane at the level of the occlusion of the teeth.
Colour
Their colour varies according to the state of the
overlying epithelium. If the epithelium is healthy, the
cyst will be pale pink, with the grey glairy appear-
ance of the mucus in the cyst just visible.
If the epithelium has been frequently damaged by
the teeth, it will be white, scarred and slightly boggy,
and will obscure the colour of the underlying cyst.
Shape
These cysts are spherical.
Size
They vary in size from 0.5 to 2 cm in diameter.
Surface
Their surface is smooth.
Composition
Their consistence varies from soft to
hard, depending on the tension of the fluid within
them.
Fluctuation and transillumination can be
detected if the cyst is large enough to grasp between
two fingers.
Relations
The mucous membrane can be moved
over the cyst, which is not fixed to the underlying
muscle (orbicularis oris or buccinator).
Lymph drainage
The local lymph glands should not
be enlarged.
Local tissues
The surrounding tissues should be
normal.
Stomatitis
Stomatitis is a general term used to describe an
inflammation of the whole lining of the mouth, but
the surface of the tongue is also often involved. It
can have a variety of clinical appearances and has
many causes.
History
Stomatitis occurs in all age groups and equally in
both sexes.
Symptoms
The patient complains of soreness in the
mouth. The mouth may feel dry.
Movements of the tongue and cheeks are painful
and individual ulcers are very painful. Mastication
is difficult.
The patient may also have the symptoms of a
generalized condition that is causing the stomatitis.
Examination
The physical appearances vary according to the
cause.
Catarrhal stomatitis
This is often associated with an acute upper respira-
tory tract infection and acute specific fever. The
whole of the mucous membrane of the mouth is
oedematous and red. Small ulcers may appear and
coalesce to become an ulcerative stomatitis.
Aphthous stomatitis
The inside of the mouth becomes covered with
small, tender vesicles which have a thickened hyper-
aemic base. When a vesicle breaks it leaves a small,
white, circular, deep, very painful ulcer. The cause of
these ulcers is not known.
FIG 10.5
Subglossal telangiectasia in a patient with
Rendu–Osler–Weber syndrome.
Chap-10.qxd 4/19/05 14:18PM Page 252
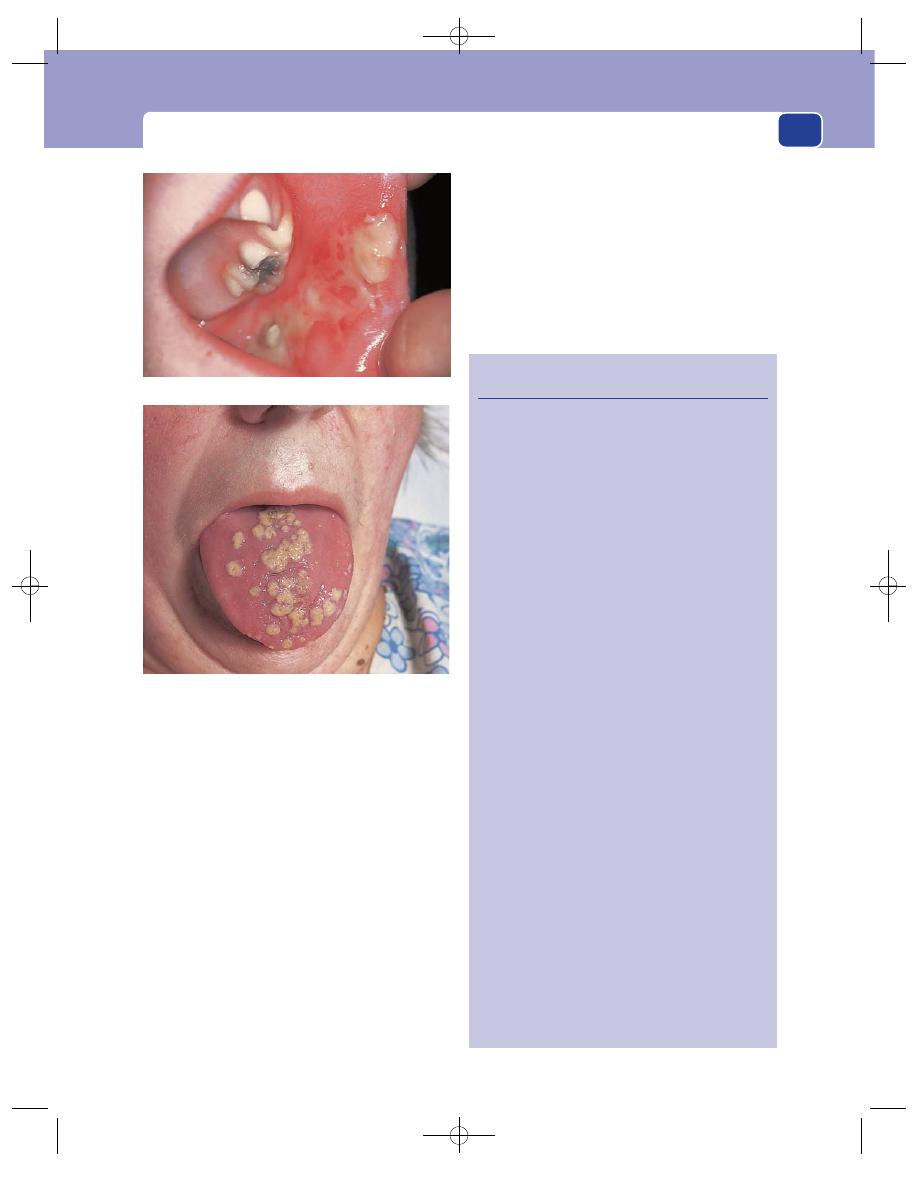
The lips, buccal mucosa and tongue
253
Recurrent solitary aphthous ulcers are com-
monplace in otherwise healthy people. Multiple
ulcers are very painful and often associated with a
generalized debilitating disease.
Acute monilial stomatitis
(Thrush)
Infection of the alimentary tract by the fungus
Candida albicans is common in children and in people
with debilitating disease, and as a complication of
any antibiotic therapy which changes the balance of
the bacteria in the alimentary canal.
Small red patches appear on the buccal mucosa
and tongue, which then turn white. The white appear-
ance is caused by a layer of oedematous desquamating
epithelium, heavily contaminated with the fungus.
The mouth is painful, and salivation is excessive.
This induces frequent swallowing, which is also
painful if the infection has spread into the pharynx.
Acute ulcerative stomatitis
(Vincent’s angina)
This usually follows a severe gingivitis, but may
complicate catarrhal stomatitis. It is caused by an
Revision panel 10.1
The causes of stomatitis
Local trauma
Poorly fitting dentures
Sharp teeth
Excessive smoking
Radiotherapy
Local infection
Herpes
Monilia
Vincent’s angina
Glandular fever
Foot and mouth disease
General conditions
Stevens–Johnson syndrome
Behçet’s syndrome
Aphthous ulceration
Vitamin deficiencies
Vitamin C (scurvy)
Vitamin B and C (coeliac disease, pellagra,
pernicious anaemia, kwashiorkor)
Blood diseases
Acute leukaemia
Agranulocytosis
Aplastic anaemia
Purpura
Immunosuppression
Acquired immunodeficiency syndrome (AIDS)
Chemotherapy
Drugs
Phenytoin
Lead, mercury and bismuth poisoning
Debility
Tuberculosis
Carcinomatosis
FIG 10.6
STOMATITIS.
Multiple aphthous ulcers of the buccal mucosa.
Monilial stomatitis. The colonies of Monilia on the tongue and
mucous membranes look like patches of cream-coloured paint.
Chap-10.qxd 4/19/05 14:18PM Page 253
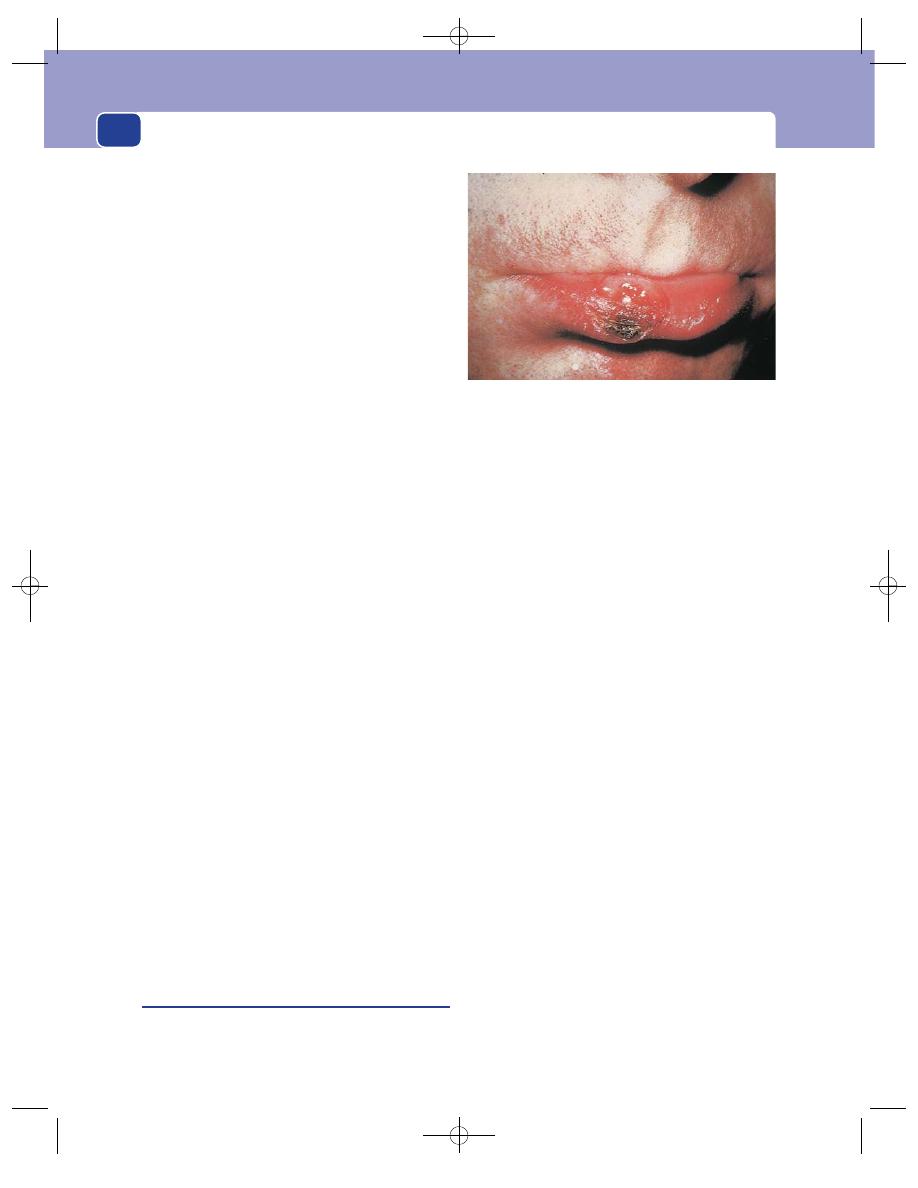
The mouth
infection (Borrelia vincenti) and is often known as
Vincent’s angina.
The gums are swollen, inflamed, painful and pep-
pered with small ulcers that are covered by a yellow
slough. These changes may spread to the tonsils, the
fauces and the buccal mucosa.
The gums bleed, there is excessive salivation and
a marked foetor oris.
The cervical lymph glands are enlarged and tender.
The patient feels ill, has a fever and loss of appetite.
Gangrenous stomatitis
(Cancrum oris)
Gangrenous stomatitis is now a rare condition
except in countries with a high incidence of starva-
tion. It is an uncommon but not rare complication
of measles and other specific fevers in malnourished
children, and it is occasionally seen in a child with
leukaemia.
It begins as an area of oedema and induration
on the lip, which becomes ischaemic and necrotic.
The area of necrosis spreads steadily, and as the
dead tissue separates so the contours of the mouth
and face are destroyed.
The process is extremely painful, and the patient
is very ill with anorexia, prostration and a pyrexia.
Angular stomatitis
(Perlèche)
This term describes inflamed, red-brown fissures at
the corners of the mouth. Its common cause is the
dribbling of saliva in this area, which follows over-
closure of the bite caused by loss of the teeth. Most
elderly edentulous patients have some degree of
angular stomatitis.
A similar condition occurs in children who rub
and lick the corners of their mouth.
The cracks may become infected by Candida
albicans.
Rhagades is the name given to the small radiat-
ing cracks in the corners of the mouth that develop
in patients in the secondary stage of syphilis (see
below). They are sore and uncomfortable, and when
they heal they leave fine linear scars.
Syphilis
All three stages of syphilis can cause abnormalities
in the mouth.
1. Primary syphilis: chancre on the lip or tongue.
2. Secondary syphilis: ‘snail-track’ ulcers, mucous
patches, Hutchinson’s wart.
3. Tertiary syphilis: gummata, chronic superficial
glossitis, gummatous parenchymal infiltration.
Primary (Hunterian) chancre
The features of a primary chancre on the lip are
similar to those of one on the genitalia (see also
page 338).
The initial lesion is an elevated but flat, pink,
painless macule. This grows slowly into a hemi-
spherical papule, the mucosal covering of which
breaks down to leave a superficial, slightly painful
ulcer. The ulcer may be covered with a thick crust.
The papule and its base are rubbery hard and
discrete.
The lymph glands in the neck become enlarged
and tender 1–2 weeks after the appearance of the
lump.
Ultimately, the ulcer heals, the lump dissolves and
the only permanent remnant is a fine superficial scar.
Chancres are highly contagious.
The mucous patch
Mucous patches are grey-white or pearl-coloured,
raised patches which appear on the inside of the lips
and cheeks and on the pillars of the fauces. They
vary in size from 3 to 20 mm in diameter. The white-
ness is caused by oedema and desquamation of the
epithelium. When the grey patch of dead epithelium
separates, the underlying mucosa is left raw and
bleeding.
Mucous patches are highly contagious.
The patient’s main complaint is of a sore throat.
254
FIG 10.7
Primary chancre of the lower lip.
Chap-10.qxd 4/19/05 14:18PM Page 254
The lips, buccal mucosa and tongue
‘Snail-track’ ulcers
‘Snail-track’ ulcers are long, narrow ulcers which
are covered with transparent glistening mucus or a
white boggy epithelium which makes them look like
snail tracks. They are commonly seen on the pillars
of the fauces.
They form from the coalescence of a number of
small mucous patches.
Gummata
Gummatous degeneration may be nodular or infil-
trating. A gumma of the tongue presents as a
painless, hard, discrete mass, while parenchymal
infiltration makes the tongue big, stiff and irregular.
Gummata in the hard palate and nasal septum can
cause perforation of these structures and collapse
of the bridge of the nose. Both varieties affect
the tongue. Gummata of the lips and cheeks are
uncommon.
Gummata also develop in the hard palate and
nasal septum, causing perforations and collapse of
the bridge of the nose.
A gumma in the tongue presents as a painless,
hard, discrete mass. It usually develops in the ante-
rior two-thirds of the tongue and, unless there is a
history of syphilis or other physical signs of the dis-
ease, is indistinguishable from an interstitial carci-
noma or a secondary deposit.
Gummatous parenchymal infiltration makes the
tongue big, stiff, thick and irregular.
Hutchinson’s wart
This is a mid-line condyloma of the tongue. A
condyloma is an area of hypertrophic epithelium,
broad based and flat topped. It is highly contagious.
Chronic superficial glossitis
This condition is commonly caused by syphilis. Its
final stage is leukoplakia, which is a pre-cancerous
condition. Its other causes are described below.
Chronic superficial glossitis
This is a condition in which a sequence of chronic
inflammatory,
degenerative and hypertrophic
changes occur in the tongue, which terminate in the
development of a carcinoma.
The causes of chronic superficial glossitis are
usually remembered as six Ss:
■
syphilis
■
smoking
■
sharp tooth
■
spirits
■
spices
■
sepsis.
However, the only conditions which can be defi-
nitely incriminated are syphilis and recurrent
trauma from a tooth or pipe. The role of the other
factors is open to doubt.
History
Age
The conditions which predispose to the devel-
opment of glossitis need to be present for many
years before they have any effect. Thus most patients
with this disease are over the age of 50 years.
Sex
More men are affected than women.
Symptoms
The patient has remarkably few symp-
toms. The condition is not painful and does not
interfere with eating. The common complaint is
that the tongue has become shiny or white, or devel-
oped a lump.
255
Revision panel 10.2
Chronic superficial glossitis
Causes
Syphilis
Recurrent trauma:
pipe smoking
sharp tooth
Spices
Spirits
Sepsis
Clinical features
Thin milky film
Thick white paint
(leukoplakia)
Nodules
Red, shiny
atrophic
Cancer
patches
←
←
←
←
Chap-10.qxd 4/19/05 14:18PM Page 255
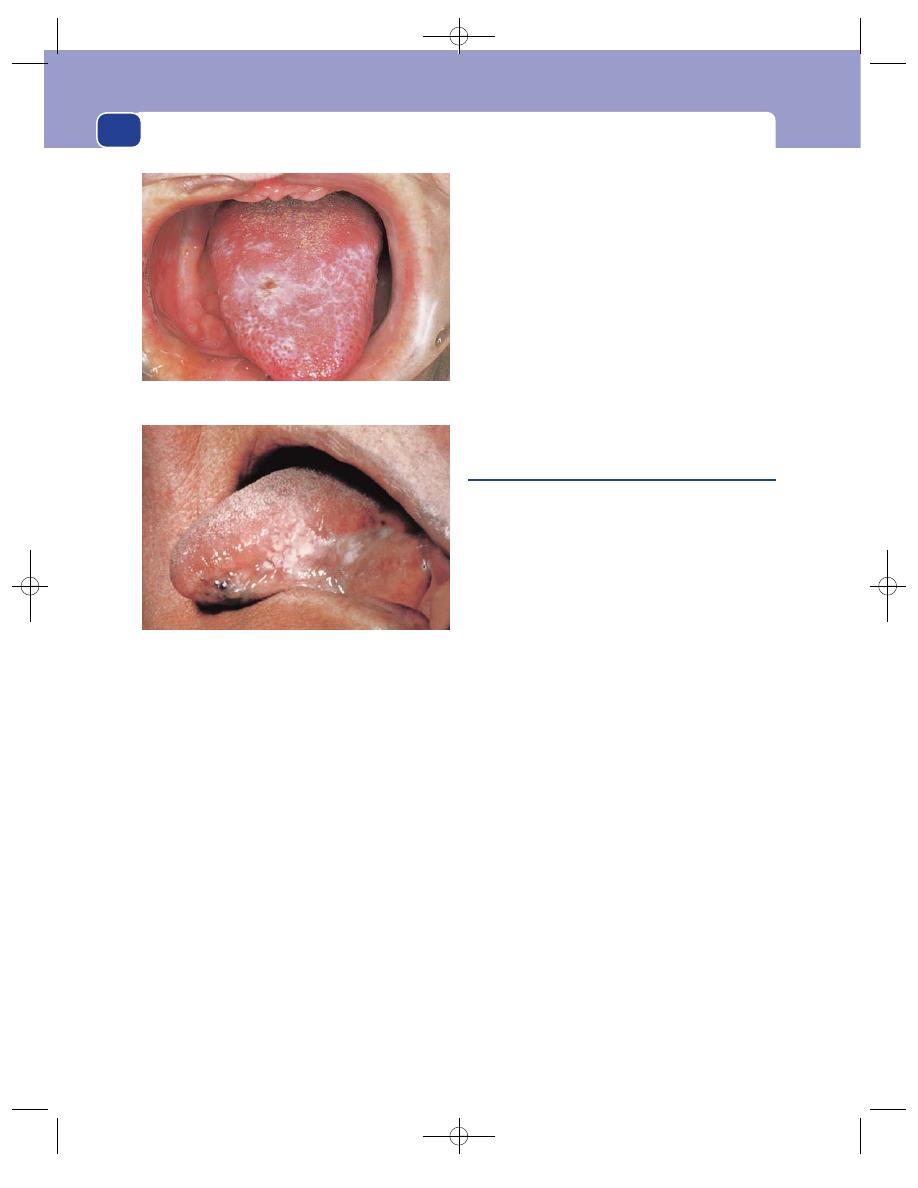
The mouth
Examination
The surface of the tongue passes through a series of
changes as the epithelium thickens. The prickle cell
layer hypertrophies (acanthosis) and swollen cells
with nuclei reach the surface (spongiosis and para-
keratosis). These changes are patchy, and all clinical
stages may coexist on different parts of the tongue.
First stage
The first abnormality is the appearance
of a thin, grey, transparent film on a part of the
tongue.
Second stage
This thin film turns opaque and white.
This is leukoplakia. Young leukoplakia looks like
fresh, soft, semi-matt paint. Old leukoplakia cracks,
fissures and gets slightly yellow so that it looks like
old, cracking, wrinkled, white gloss paint.
Third stage
Beneath the white patches the epithelium
becomes hyperplastic. Small nodules and warty
outgrowths appear, which may eventually become
overt carcinomata.
The areas of very active cellular division are visi-
ble as smooth, red, shiny patches.
Fourth stage
The fourth stage is the appearance of
clinically detectable carcinomata. The lesions have all
the features of a primary carcinoma of the tongue.
Many small cancers may appear together and the
cervical lymph glands may be enlarged. Change
identical to that of chronic superficial glossitis can
occur on the lips and any part of the buccal mucosa –
cheek, gums and palate. Leukoplakia of the lips and
cheeks is now more common than leukoplakia of
the tongue.
Carcinoma of the lip
Carcinoma of the lip is no longer common in Great
Britain since the reduction of the incidence of
syphilis and leukoplakia of the lip. The factors that
produce pre-malignant changes in the epithelium
of the lip are leukoplakia and its causes, and recur-
rent trauma from pipes and prolonged exposure to
sunlight.
Since the reduction in the incidence of syphilis,
exposure to sunlight, especially the ultraviolet part
of sunlight, is the commonest cause of carcinoma of
the lip.
History
Age
Most of the patients with carcinoma of the lip
are over the age of 60 years.
Sex
Men are affected more often than women.
Occupation
It is particularly common in men with
outdoor occupations and is sometimes called ‘coun-
tryman’s lip’; but remember that there are many
men with outdoor occupations living in towns.
Ethnic group
People with dark skin are less suscep-
tible to, but not exempt from, diseases induced by
sunlight.
Geography
All sunlight exposure conditions are
more common in countries with a tropical or semi-
tropical climate and populated by white Caucasians,
such as Australia.
Symptoms
When the pre-malignant changes are devel-
oping in the lip, the patient complains of blistering,
256
FIG 10.8
CHRONIC SUPERFICIAL GLOSSITIS.
The early stage, when the tongue is covered with a
transparent grey film and loses its papillae.
The advanced stage, with hard white plaques, nodules and
fissures.
Chap-10.qxd 12/21/10 6:36 PM Page 256
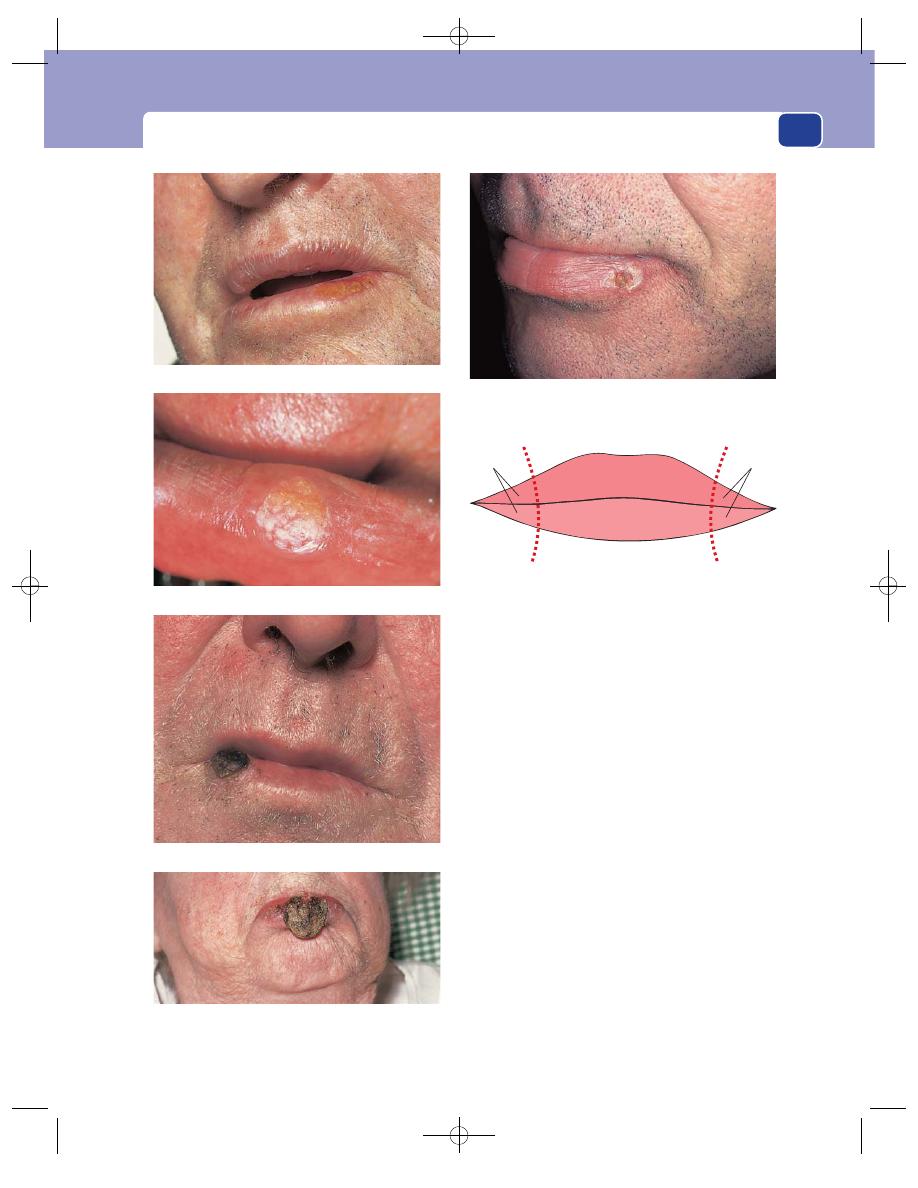
The lips, buccal mucosa and tongue
257
thickening (keratosis), and white patches (leuko-
plakia).
A carcinoma causes a lump, or an ulcer which
fails to heal.
As the ulcer grows it interferes with speech and
eating, bleeds and produces an offensive discharge,
but is not always painful.
The patient may notice lumps under their chin.
Although small lumps and sore spots on the lips are
common, be suspicious of any lump that does not
heal quickly.
Previous history
It is important to ask about previous
diseases, especially syphilis and conditions caused
by exposure to sunlight.
Habits
Ask if the patient smokes a pipe. Carcinoma of
the lip was common when clay pipes were popular.
Examination
Position
The lower lip is affected over ten times
more often than the upper lip. Carcinoma in the
angle of the lips is uncommon. The lesion is usually
to one side of the mid-line.
Solar keratoses on the lower lip – a pre-malignant change.
A small, early lesion that has just ulcerated.
An ulcerating lesion covered with a black slough.
A large proliferating and infiltrating carcinoma distorting
the whole lower lip.
FIG 10.10
Carcinoma of the lip in a habitual pipe smoker. The
lesion developed where he used to rest his pipe.
1%
1%
93%
5%
FIG 10.11
The distribution of carcinoma of the lips.
FIG 10.9
CARCINOMA OF THE LIP.
Chap-10.qxd 4/19/05 14:18PM Page 257
The mouth
258
Colour
The skin over the lump or round the ulcer
may show evidence of a pre-malignant condition:
blistering, thickening and pigmentation, or white
boggy patches.
Tenderness
A cancer of the lip, nodular or ulcerative,
is not always tender. The absence of tenderness
should alert your suspicions because most ulcers in
the mouth are very painful and tender.
Shape
The cancer starts as a small lump or nodule,
which ultimately ulcerates in its centre and develops
the typical everted edge of a carcinoma.
The initial lesion is small, just a few millimetres
across, but can become large if not treated.
Edge
Once the lump has ulcerated, the edges prolif-
erate and evert. They are red and, at their junction
with the base of the ulcer, bleed easily.
Base
The base is covered with a thin, soft, friable,
grey-yellow slough. It is a mixture of dying tissue
and inflammatory exudate. It is thin because the
ulcer is repeatedly rubbed by the tongue.
Depth
The ulcer is initially shallow, but can erode
deep into the lip, destroying the epithelium and the
underlying muscle.
Discharge
The discharge is thin, watery and slightly
blood stained. It is usually infected but rarely
purulent.
Relations
The lump is invariably fixed to the subcu-
taneous structures of the lip but can be moved, with
the lip, separately from the jaw. Only very advanced
lesions are fixed to the gum and jaw.
Lymph drainage
The lymph glands draining the dis-
eased portion of the lip are likely to be enlarged by
secondary infection, if not by tumour.
■
The lymph draining from the upper lip passes
across the face and over the angle of the jaw to
the upper deep cervical glands.
■
Lymph from the centre of the lower lip drains to
the submental glands and then to the lower
deep cervical glands.
■
Lymph from the lateral third of the lower lip
drains to the lymphoid tissue overlying and
sometimes within the submandibular gland, and
then to the middle deep cervical lymph glands.
■
Lymph from the angle of the mouth drains into
the lymphatics of both lips.
If the lymph glands contain metastases, they will
be hard and discrete. If the enlargement is caused by
secondary infection, they will be slightly tender.
Surrounding tissues
Away from the ulcer, the rest of
the lip is usually normal or mildly affected by the
predisposing causes of cancer already mentioned.
General examination
Disseminated distant metastases
are rare.
Carcinoma of the tongue
Like carcinoma of the lip, the prevalence of carci-
noma of the tongue has fallen in parallel with
the reduction in the prevalence of syphilis, and
there is no longer a high incidence of the disease in
males.
The important pre-malignant disease of the
tongue is chronic superficial glossitis, especially when
it has reached the leukoplakia stage. Thus the causes
of chronic superficial glossitis, already described,
are the causes of carcinoma of the tongue.
Carcinoma of the tongue spreads locally and
causes death through local complications and aspi-
ration or obstructive pneumonia. Distant blood-
borne metastases are a late and uncommon event.
History
Age
The patients are usually over the age of 50 years.
The peak incidence is between 60 and 70 years.
Sex
Males were affected far more than females when
syphilis and pipe smoking were common. Now there
are almost as many women affected as men.
Symptoms
The commonest complaint is of a painless
lump or irregularity on the surface of the tongue.
If the early lesion is ignored or not noticed, the
patient may not present until they have an enlarg-
ing ulcer causing pain in the tongue (sometimes
referred to the ear), excessive salivation, difficulty
with mastication and swallowing, and foetor oris.
If the lesion has spread extensively before it is
noticed, it may cause immobility of the tongue
(ankyloglossia) and difficulty with speech.
Lesions on the back of the tongue may alter the
quality of the voice.
Alternatively, the patient may present with a
lump in the neck (enlarged lymph glands) before
they notice any abnormality in the tongue.
Chap-10.qxd 4/19/05 14:18PM Page 258
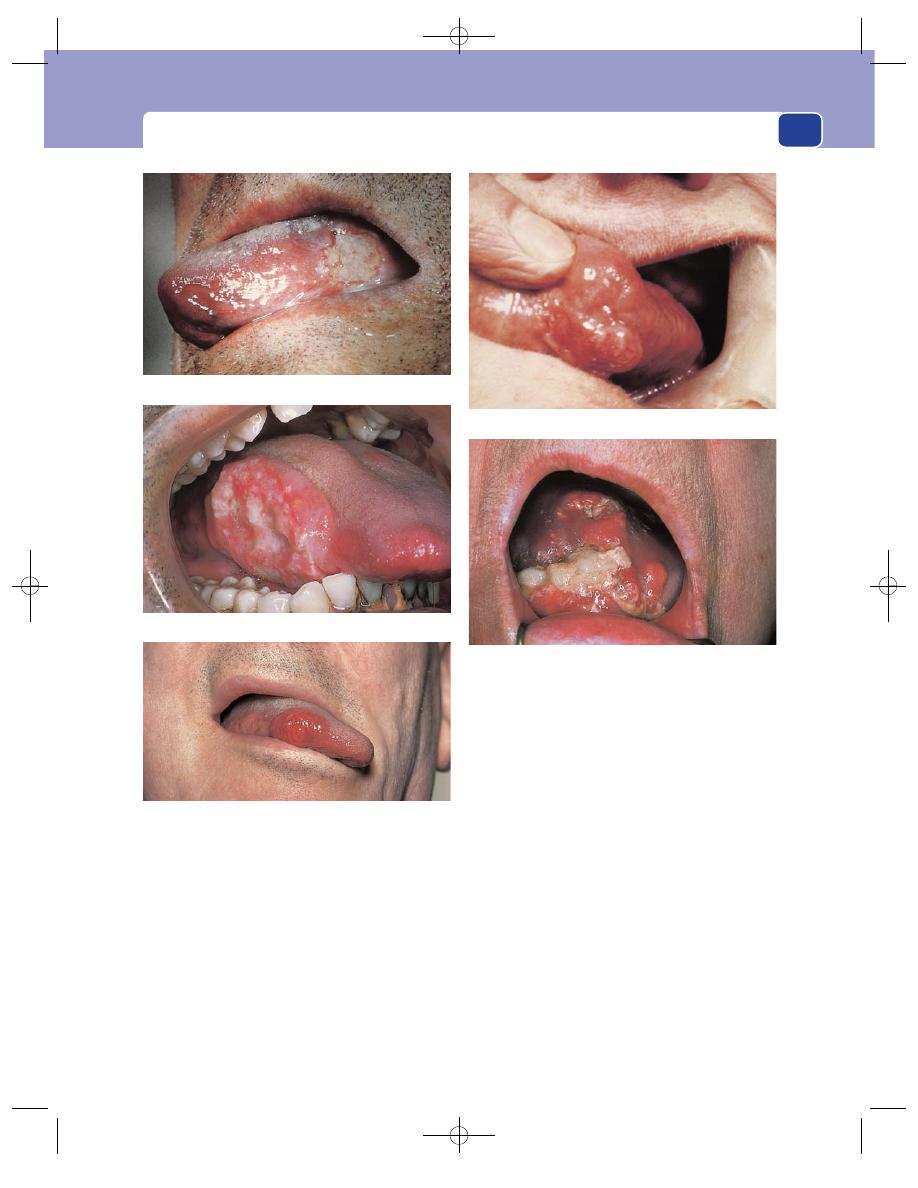
The lips, buccal mucosa and tongue
259
Previous history
Ask about previous venereal disease,
or any trouble with the teeth or dentures that may
have caused chronic trauma.
Habits
Ask if the patient smokes, or has smoked, a
pipe.
Examination
Position
Carcinomata of the tongue are most com-
mon on the edge and the lateral surface of the
tongue, 20 per cent occur in the posterior third,
20 per cent on the dorsum and tip, and 10 per cent
on the under-surface.
Colour
The epithelium and papillae over a deep-seated
lump look normal, but if the lesion is near the surface,
the epithelium loses its papillae and looks smooth,
shiny and stretched. Ulcers are usually covered with a
transparent, yellow-grey slough.
Tenderness
The lump, or ulcer, is not tender.
Shape, size and composition
Carcinomata of the tongue
may present in four forms: an ulcer, a nodule, a
FIG 10.12
CARCINOMA OF THE TONGUE.
An ulcerated nodule on the side of the tongue.
A nodular carcinoma of the tongue.
A large ulcer with an everted edge on the side of the tongue.
Not all nodules are primary lesions. This one was a
metastasis from a carcinoma of the bronchus.
A very advanced carcinoma of the tongue.
Chap-10.qxd 4/19/05 14:19PM Page 259
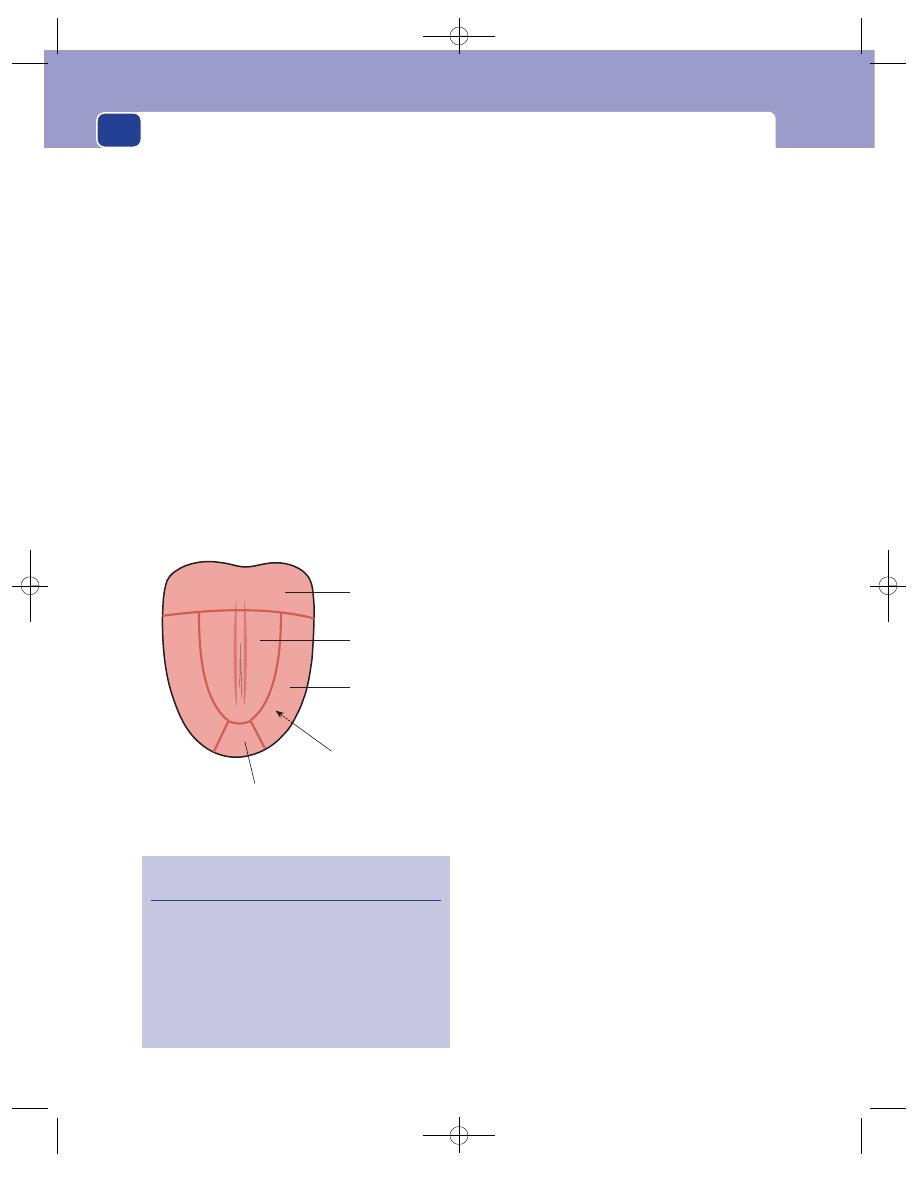
The mouth
260
papilliferous or warty nodule, or a fissure in an area
of induration.
A carcinomatous lump tends to be ovoid, with its
long axis parallel to the mid-line of the tongue. It may
vary in size from a small nodule to a mass 2–5 cm
across. It feels hard and has an indistinct edge
where it is spreading into the rest of the tongue.
A carcinomatous ulcer of the tongue usually has
the typical features of a carcinoma: a florid, friable,
bleeding, everted edge, a sloughing yellow-grey base,
a thin serous discharge and induration of the sur-
rounding tissues.
The papilliferous or warty carcinoma looks like
any other papilloma in that it is covered with an
excess of proliferating filiform epithelium, which is
usually paler than the surrounding pink epithelium,
but the base is broad and firm and the area of
tongue from which it arises is indurated. It may be
of any size, but rarely juts out far from the tongue
because of the restriction of the mouth.
The fissure in an area of carcinomatous indura-
tion is a rare form of tongue cancer. It is a modified
form of the nodule which has spread so diffusely
that it does not have a detectable edge. The fissure
may be a cleft in the tongue that has deepened and
lost its epithelium, or a deep linear ulcer.
Relations
It is very important to examine the floor of
the mouth, the gums, jaw, tonsils and fauces,
because a carcinoma can spread into any of these
structures, and once it has done so, its treatment
becomes much more difficult.
Lesions on the side or under-surface of the tongue
are more likely to spread into the floor of the mouth
than lesions on the dorsum.
Spread to the floor of the mouth causes thickening
of the tissues and reduces the mobility of the tongue.
Infiltration of the gum and jaw fixes the tumour to the
bone, and the jaw itself may be swollen. Tumours of
the posterior third of the tongue spread into the ton-
sil and the pillars of the fauces.
Lymph drainage
■
The lymph from the tip of the tongue drains to
the submental glands and then to either or both
jugular lymph chains.
■
The lymph from the rest of the anterior two-
thirds drains to the glands on the same side of
the neck, usually the middle and upper deep
cervical glands.
■
Lymph from the posterior third drains into the
ring of lymph tissues around the oropharynx
and into the upper deep cervical lymph glands.
More than half of the patients who present with
a cancer of the tongue have palpable cervical lymph
glands, but in some cases the enlargement is caused
by secondary infection, not tumour.
State of local tissues
Involvement of the lingual nerve
causes a pain that is referred to the ear, probably
through its connections with the auriculotemporal
nerve.
Infiltration of the mandible causes pain and
swelling of the jaw.
The surface of the tongue around the cancer may
be affected by leukoplakia, and there may be other
primary tumours.
Differential diagnosis
The causes of ulcers on the
tongue are given in Revision panel 10.3.
Posterior third
20%
Dorsum
10%
Under-surface
10%
Tip 10%
Lateral third
25% (
⫻2)
FIG 10.13
The distribution of carcinoma of the tongue.
Revision panel 10.3
The causes of ulceration of the tongue
Aphthous ulcer
Trauma (dental)
Non-specific glossitis
Chancre
Gumma
Tuberculosis
Carcinoma
Chap-10.qxd 4/19/05 14:19PM Page 260
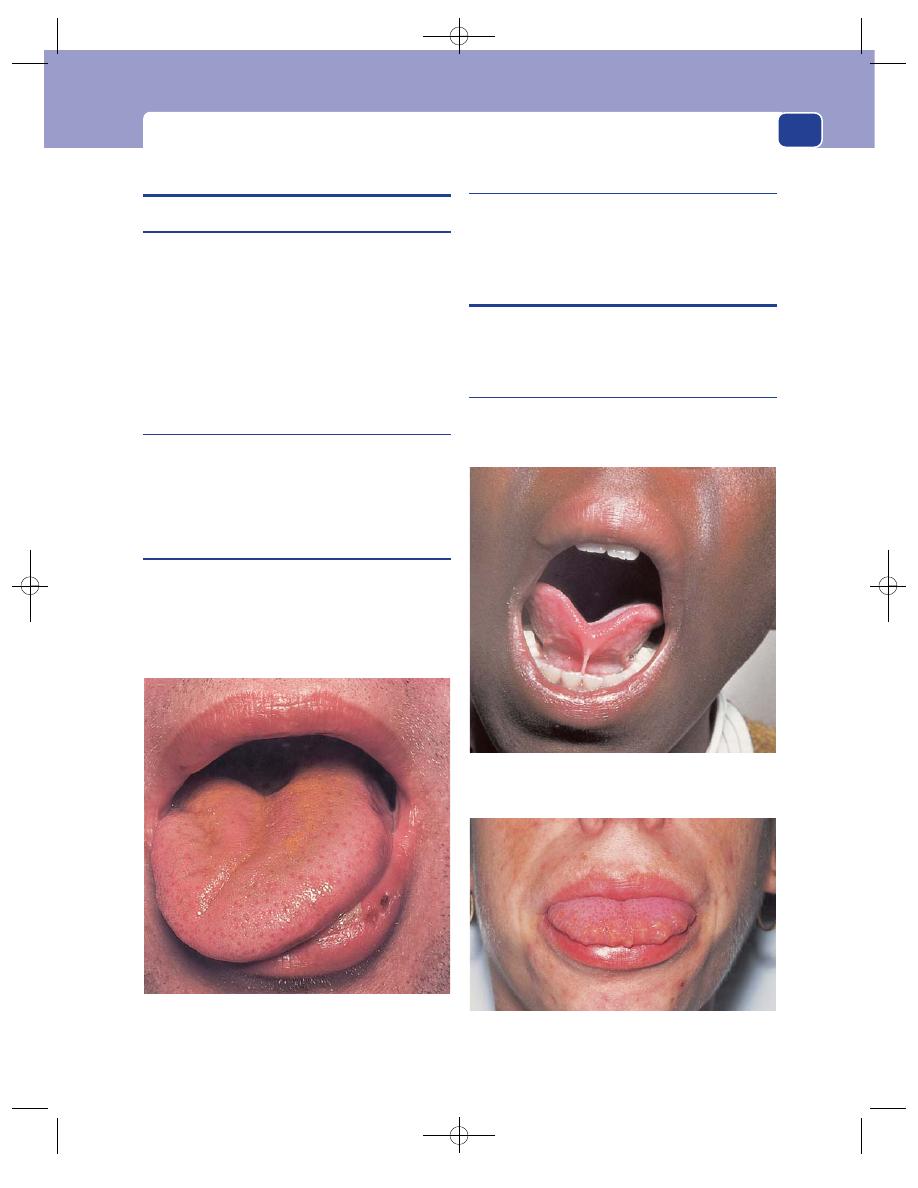
The palate
261
OTHER CONDITIONS OF THE TONGUE
Macroglossia
Macroglossia is a large tongue. The causes of macro-
glossia are:
■
multiple haemangiomata
■
multiple lymphangiomata
■
plexiform neurofibromatosis
■
amyloid infiltration
■
infiltrating carcinoma
■
muscle hypertrophy (cretins).
Wasting of the tongue
Paralysis of the 12th cranial nerve (the hypoglossal
nerve) causes disuse atrophy of one side of the
tongue. When the patient is asked to ‘put out your
tongue’, it deviates towards the paralysed side.
Tongue-tie
If the patient has a congenitally shortened frenu-
lum, this can lead to a degree of tongue-tie. This
rarely causes any significant impairment of speech,
but if it is severe and remains uncorrected into late
infancy, it can interfere with speech.
Mucosal neuromata
In the uncommon condition of multiple endocrine
neoplasia type 2b (MEN 2b), multiple mucosal neu-
romata can be seen, particularly on the tongue.
THE PALATE
The varieties of congenital cleft palate are described
on pages 250–1.
Perforation of the palate
A perforation in the palate can be acquired if disease
or trauma destroys the bones of the palate.
FIG 10.14
A right hypoglossal nerve palsy. When this patient
was asked to protrude his tongue, it could be seen to be
wasted on the right and deviated to the right.
FIG 10.15
Tongue-tie: a congenitally short frenulum. This
rarely causes any significant impairment of speech.
FIG 10.16
Multiple mucosal neuromata on the tongue of a
patient with MEN 2b.
Chap-10.qxd 4/19/05 14:19PM Page 261
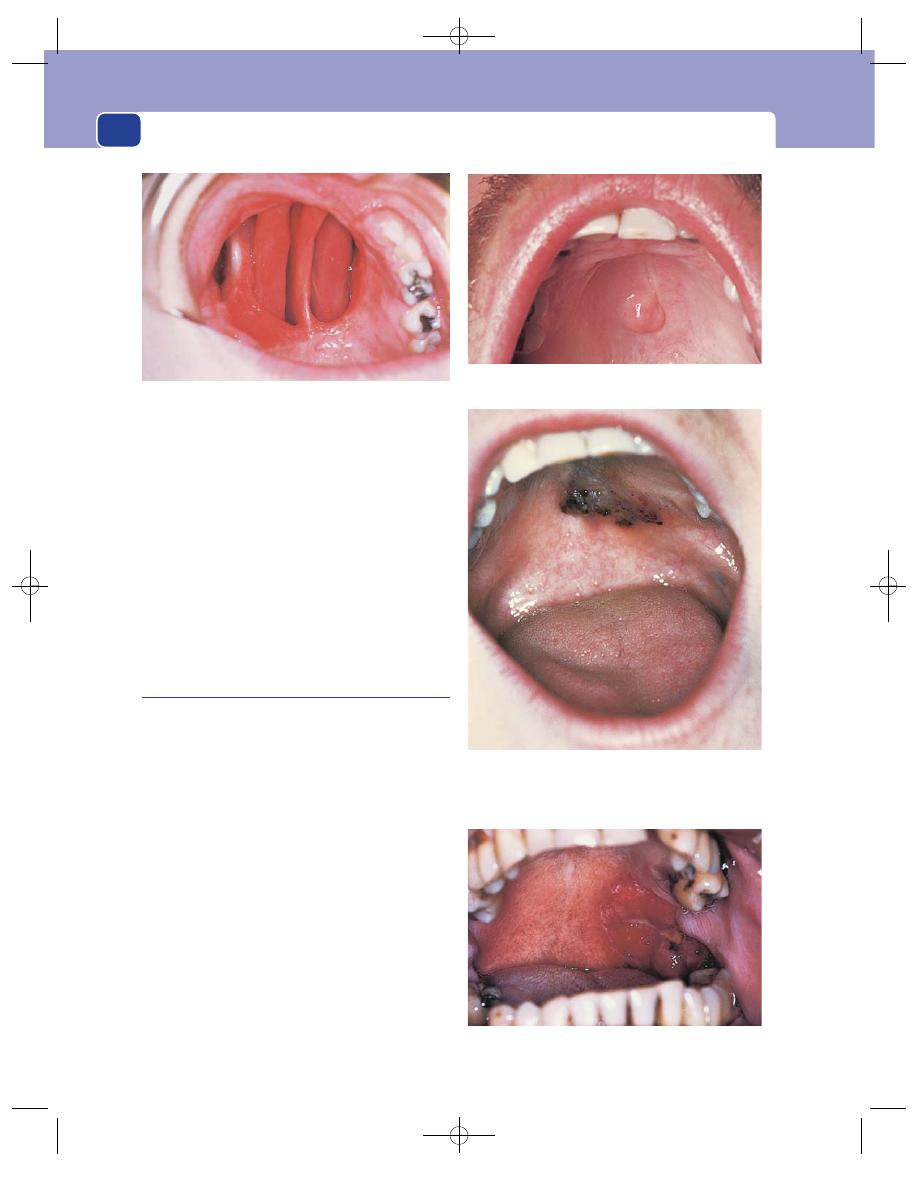
The mouth
262
When syphilis was common, perforation of the
hard palate following gummatous destruction of the
bone and mucosa was quite common. Nowadays
acquired perforation of the palate is rare. It can be
caused by:
■
an empyema or tumour of the maxillary antrum
bursting through the palate into the mouth,
■
repeated trauma from poorly fitting dentures,
■
surgical excision of the palate to approach the
maxillary antrum.
Tumours of the palate
The mucous membrane covering the hard palate is
identical to that of the rest of the buccal mucosa.
Retention cysts and carcinoma, similar to those of
the lips and buccal mucosa, are not uncommon.
The hard palate also contains many small glands
identical in structure and function to the salivary
glands.
A pleomorphic salivary adenoma (mixed sali-
vary tumour – see Chapter 9) is a common cause of
a lump on the palate.
The patient’s sole complaint is of a lump on the
palate which grows slowly but steadily.
If it is not treated, it can fill the arch of the palate
and make speech and eating difficult.
On examination, the lump feels smooth and hard.
The overlying mucous membrane is not attached to it
and if the lump is small, it can be moved over the
underlying palate. As the tumour grows it becomes
less mobile and more difficult to distinguish from a
tumour growing in or above the palate.
A carcinoma on the side of the hard palate.
FIG 10.18
TUMOURS OF THE HARD PALATE.
A small pleomorphic adenoma of a salivary gland on the hard
palate.
A malignant melanoma of the hard palate. This is a rare
condition, but is included as a reminder that malignant
melanoma can arise at the mucocutaneous junctions, i.e.
around the mouth and anus.
FIG 10.17
Large perforation of the palate. The nasal septum
and turbinate bones are clearly visible.
Chap-10.qxd 4/19/05 14:19PM Page 262
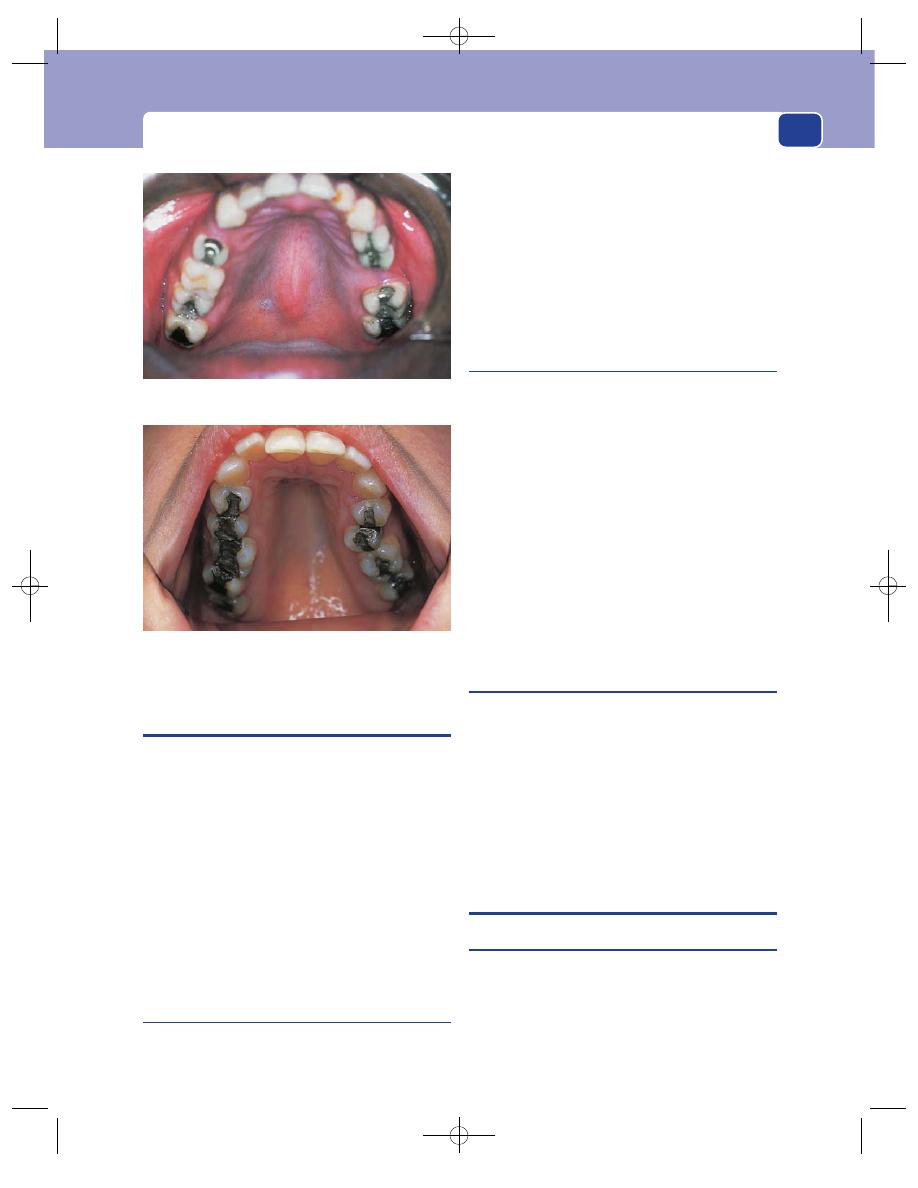
The floor of the mouth
263
THE TONSILS
Tonsillitis is a condition familiar to all because
almost everyone has suffered it. It causes a sore
throat and pain during swallowing. On examina-
tion, the tonsils are seen to be enlarged and red, with
pus exuding from their crypts. The surrounding pil-
lars of the fauces, soft palate and oropharynx are
also red and tender, and may be covered with small
yellow-based ulcers.
Bilateral enlargement of the tonsils, together
with the above signs, is diagnostic of tonsillitis.
Unilateral enlargement of a tonsil, even if it is red
and tender, is not always caused by acute tonsillitis.
Remember the other causes described below.
Carcinoma of the tonsil
Carcinoma of the tonsil occurs in the elderly. The
enlarging tonsil and deep infiltration by the tumour
cells may cause severe pain in the throat, which is
referred to the ear.
The surface of the growth eventually ulcerates to
form a deep indolent ulcer, rarely with everted edges,
which bleeds, causes severe dysphagia and a pun-
gent foetor oris. The cervical lymph glands often
become involved and enlarged at an early stage of
the disease.
Lymphoma of the tonsil
Lymphoma of the tonsil occurs in late-middle and
old age. In contrast to carcinoma it causes a painless
swelling. The patient’s only complaints are the sen-
sation of a lump in the back of the mouth and
throat and sometimes mild dysphagia.
Gross swelling may interfere with speech and make
the words indistinct.
Enlargement of the cervical lymph glands occurs
at a late stage of the disease.
Both carcinomatous and lymphomatous tonsils
can become infected. Acute tonsillitis in the elderly
is not common, so be on your guard and search for
an underlying cause.
Peritonsillar abscess
(Quinsy)
This is an abscess, lateral to the tonsil, which pushes
the tonsil towards the mid-line and makes it
look enlarged. It is a very painful condition. Opening
the mouth and swallowing saliva is particularly
painful.
The diagnosis rests on observing a red bulge in
the anterior pillar of the fauces, tender cervical lymph
glands, fever and tachycardia.
THE FLOOR OF THE MOUTH
Ranula
A ranula is a large mucus-containing cyst in the
floor of the mouth. The mucus probably comes
from acini of the sublingual gland which have rup-
tured in response to secretory back-pressure sec-
ondary to an obstruction of the sublingual duct, or
direct injury.
The high-arched palate of Marfan’s syndrome.
FIG 10.19
A mid-line bony spur of the hard palate, recognizable by its
mid-line cleft, known as a torus palatinus.
Chap-10.qxd 4/19/05 14:19PM Page 263
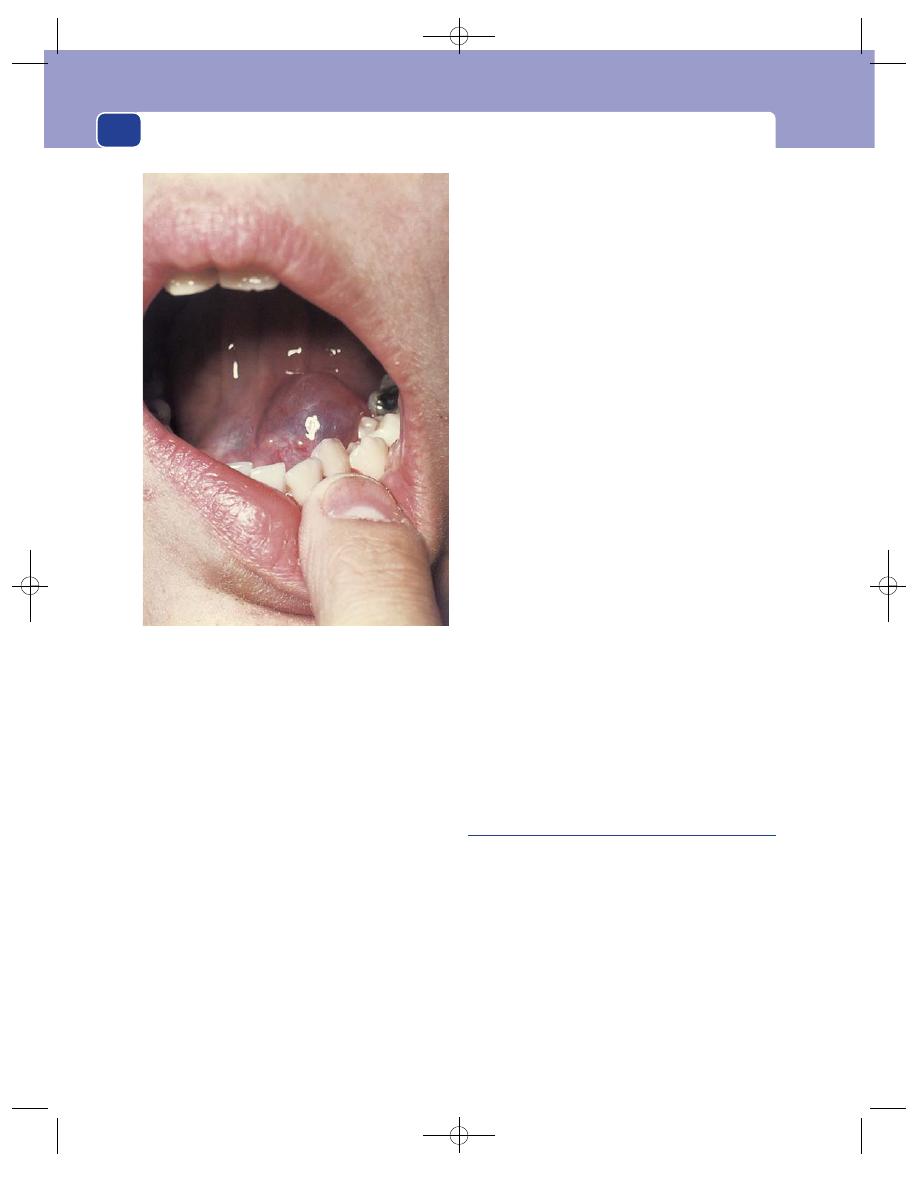
The mouth
264
Ranula is the Latin for a small frog. It is said that
the swelling was given this name by Hippocrates
because he thought it looked like the belly of a frog;
but when the patient opens their mouth and the
swelling bulges up under the tongue, it looks more
like the air-filled swelling under the jaw of a frog
when it croaks.
History
Age
Ranulata appear most often in children and
young adults.
Sex
Both sexes are equally affected.
Symptoms
The patient complains of a swelling in the
floor of the mouth, which has grown gradually over
a few weeks.
Some ranulata fluctuate in size, and some swell
suddenly and become painful, but they rarely get
big enough to interfere with eating or speech.
Examination
Position
The swelling lies in the floor of the mouth,
between the symphysis menti and the tongue, just
to one side of the mid-line.
Colour
The lump has a characteristic semi-transparent
grey appearance. The colour and the site are the
diagnostic features.
Tenderness
The swelling is not tender.
Shape
Ranulata form spherical cysts, but only the
top half is visible.
Size
They vary from 1 to 5 cm in diameter.
Surface
Their surface is smooth, but their edge is
difficult to feel because they are deep within the arch
of the mandible.
Composition
The swelling is soft, usually fluctuant
and transilluminates, but it cannot be compressed
or reduced.
Relations
The overlying mucosa is not fixed to the wall
of the cyst and the cyst is not fixed to the tongue or
the jaw.
The swelling is usually closely related to the duct
of the submandibular salivary gland (Wharton’s
duct), which may be seen running over its surface or
alongside it.
Ranulata occasionally extend through the mylo-
hyoid muscle into the neck. This variety is called a
plunging ranula.
Lymph drainage
The cervical lymph glands should
not be enlarged.
Local tissues
These should all be normal.
Sublingual dermoid cyst
When the face and neck are formed by the fusion of
the facial processes, a piece of epidermis may get
trapped deep in the mid-line just behind the jaw,
and later form a sublingual dermoid cyst.
Such cysts are in the mid-line, but may be above
or below the mylohyoid muscle.
History
Age
The swelling is usually noticed when the patient
is between the ages of 10 and 25 years.
Sex
Both sexes are equally affected.
FIG 10.20
A ranula: a tense, translucent, spherical swelling
just below the mucosa of the floor of the mouth.
Chap-10.qxd 4/19/05 14:19PM Page 264
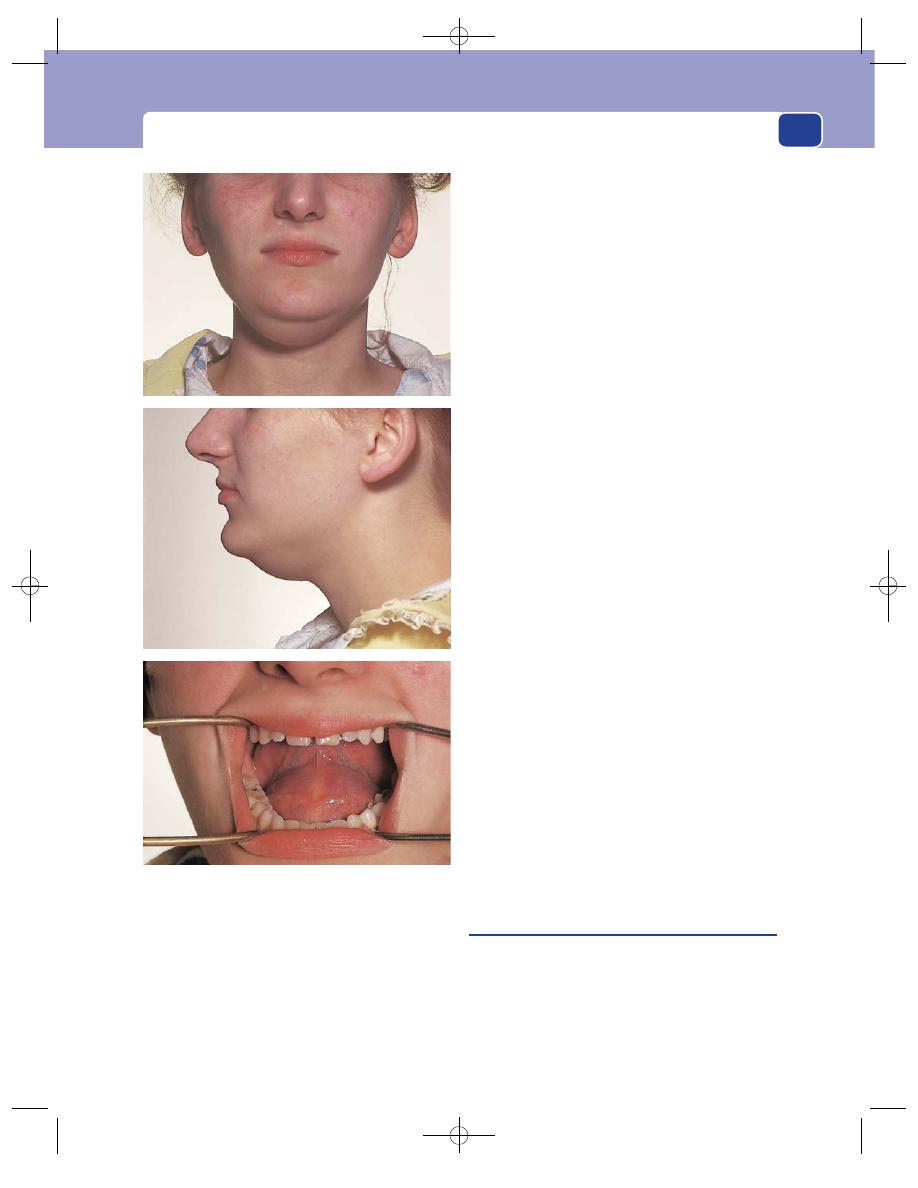
The floor of the mouth
265
Symptoms
The patient complains of a swelling
under the tongue or just below the point of the chin.
It may appear suddenly, when it is usually
painful, or gradually. It is otherwise symptomless.
Very rarely, the contents become infected and the
cyst becomes tense and painful.
Examination
Position
The lump is easily visible, either in the cen-
tre of the floor of the mouth between the tongue
and the point of the jaw, or bulging down below the
chin, looking like a double chin.
Colour
The mucous membrane of the mouth and
the skin beneath the chin overlying the lump are
normal.
Tenderness
Sublingual dermoid cysts are not tender.
Shape
The cyst is clearly spherical, even though its
whole surface cannot be felt.
Size
By the time these cysts are noticed they are
2–5 cm across.
Surface
The surface is smooth.
Edge
The edge is clearly defined.
Composition
The lump feels firm, but bimanual pal-
pation reveals that it fluctuates.
These cysts do not usually transilluminate, as
their contents are often opaque. They cannot be
compressed or reduced.
Relations
Sublingual dermoid cysts can be felt
bimanually, with a finger in the mouth and one
beneath the chin.
When the tongue is lifted up, the supramylohy-
oid variety bulges into the mouth.
If the tongue is pushed against the roof of the
mouth with the teeth clenched, the submylohyoid
variety bulges out below the chin.
Neither variety is attached to the covering buccal
mucosa or skin, or the tongue, but the proximity of
the tongue muscles and jaw limits their mobility.
Local tissues
The nearby tissues should all be normal.
Lymph drainage
The local lymph glands should not
be enlarged.
Stone in Wharton’s duct
Stones and infection in the submandibular gland
and duct are common (see page 239). When such a
stone migrates forwards to the mouth of the sub-
mandibular duct (Wharton’s duct), it forms a lump
in the floor of the mouth (see Fig. 9.3, page 241).
The lump bulges slightly into the mouth, is tender
FIG 10.21
A sublingual dermoid cyst. This cyst was above the
mylohyoid muscle but large enough to cause a visible
swelling below the chin.
Chap-10.qxd 4/19/05 14:19PM Page 265
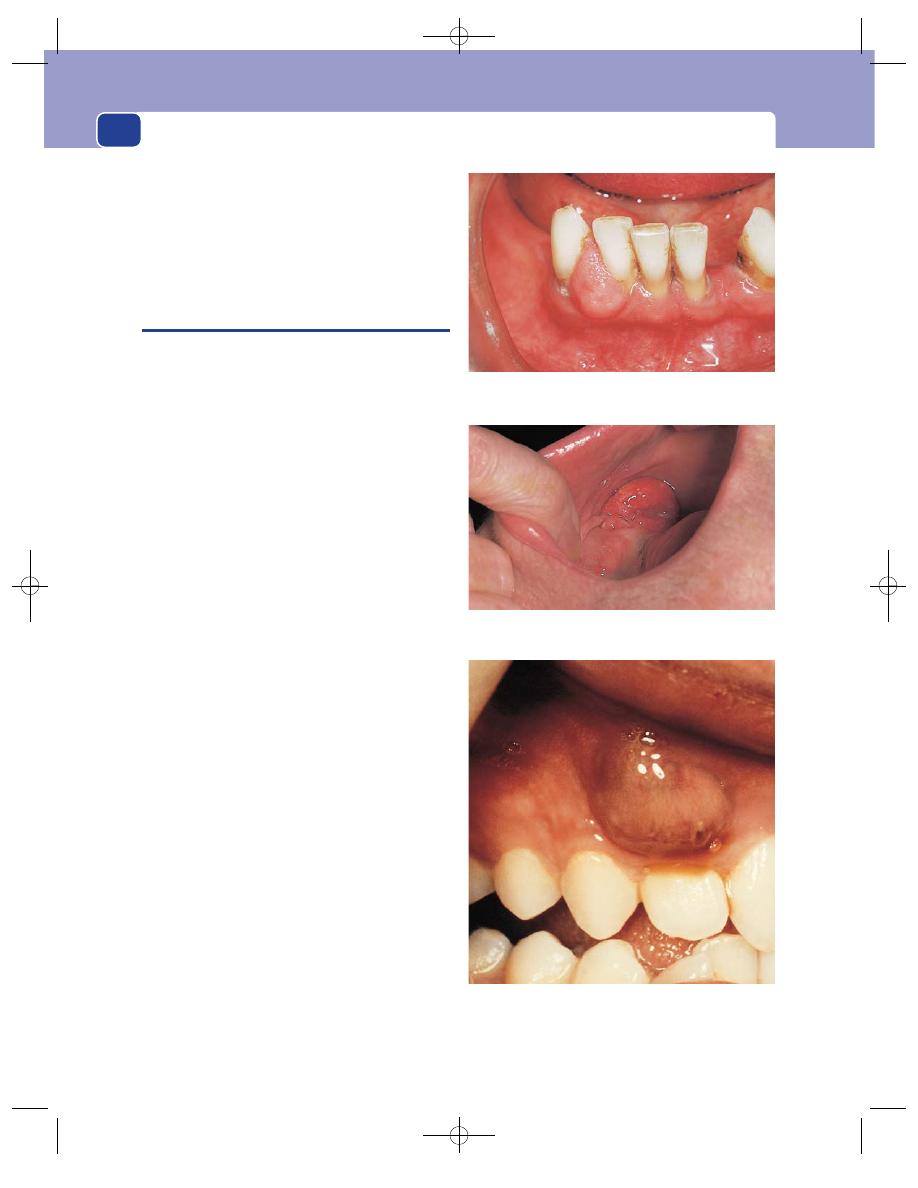
The mouth
266
and, through the surrounding oedema, the centre
may feel hard.
Sometimes the surface of the stone can be seen
through the open end of the duct.
The submandibular gland is usually swollen and
tender.
THE GUMS
Retention cysts, carcinomata and salivary tumours
can arise from the mucous membrane that covers
the jaw, but there are some swellings which are
peculiar to the gum. They are called epulitides, but
this is just a special name to indicate the site of the
lump, not its pathology.
An epulis is a swelling that arises from the alve-
olar margin of the jaw. It can originate from the
bone, the periosteum or the mucous membrane.
Fibroma
The commonest variety of epulis is the fibrous
epulis. This is a fibroma that arises from the gingi-
val tissues, so forming a firm nodule at the junction
of gum and tooth. It may bulge out and become
polypoid in shape.
Fibrosarcoma
A fibrosarcomatous epulis is the malignant variety
of the fibrous epulis. It grows rapidly, is soft and fri-
able, and very rare.
Granuloma
A granulomatous epulis is a pyogenic granuloma
of the mucosa of the gum. It is usually associated
with gingivitis or dental caries.
Bone tumour
A bony epulis is usually caused by an osteoclastoma
(giant cell tumour). Although the underlying
mass is hard, the gum covering the mass becomes
hyperaemic and oedematous, and may bleed and
ulcerate.
Carcinoma
Carcinoma of the gum presents as a lump or an
ulcer. It is usually recognizable as a carcinoma, so
the description used in some books – carcinoma-
tous epulis – is confusing and inappropriate.
A giant-celled epulis.
FIG 10.22
SWELLINGS OF THE GUM.
A fibrous epulis.
A pyogenic granuloma or granulomatous epulis.
Chap-10.qxd 4/19/05 14:19PM Page 266
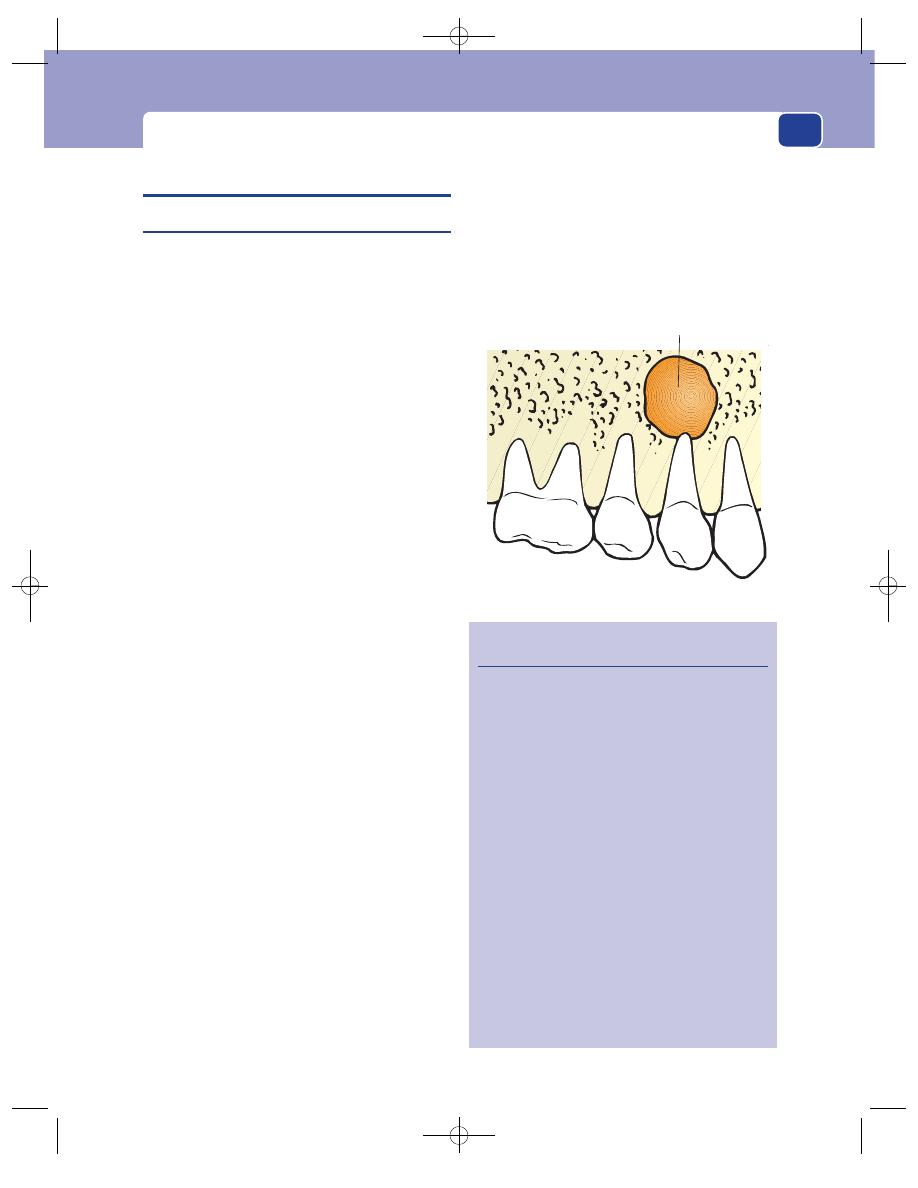
Swellings of the jaw
SWELLINGS OF THE JAW
Alveolar (dental) abscess
The commonest cause of swelling of the jaw is a dental
or alveolar abscess. This is an abscess which forms at
the base of the root of a decaying tooth and tracks out-
wards, through the external surface of the mandible or
maxilla, to form an abscess beneath the cheek or jaw.
History
Age
An alveolar abscess can develop at any age, with
the first or the second dentition.
Symptoms
The patient complains of a constant dull
ache in the jaw, which gets gradually worse and
becomes throbbing in nature.
Soon after the onset of the pain, a swelling
appears which is very tender.
There is often sweating, general malaise and loss
of appetite.
Previous history
The patient may know that they
have bad teeth, having had toothache and avoided
dental care.
Examination
Position
Most alveolar abscesses point to the labial
(outer) side of the jaw. Those in the lower jaw also
point downwards to the inferior margin of the
mandible.
An abscess which points to the lingual (inner)
surface causes a swelling on the palate or between
the mandible and the tongue.
Colour
The overlying skin or mucosa is reddened by
the inflammatory hyperaemia.
Temperature and tenderness
The swelling is hot and
acutely tender.
Shape
The abscess takes the form of a flattened
hemisphere, but its edges merge into the surrounding
tissues, so it does not have a clear-cut shape or edge.
Surface
The surface is indistinct.
Composition
It is difficult to assess the composition
of the swelling because it is so tender.
The deep part of the mass feels firm, but the
overlying tissues may be soft and boggy with oede-
matous fluid. Large abscesses may fluctuate.
Relations
The mass is clearly fixed to, and feels as if it
is part of, the underlying bone.
The skin and mucosa move freely over the lump
until they become involved in the oedema or the
inflammatory process. The precise relations depend
upon the site of the abscess. The commonest site is
267
Revision panel 10.4
The causes of swelling of the jaw
Infections
Alveolar (dental) abscess
Acute osteomyelitis
Actinomycosis
Cysts
Dental cysts
Dentigerous cysts
Other odontogenic cysts and cystic tumours
Neoplasms
Benign
Fibrous dysplasia
Giant cell granuloma
Odontogenic tumours
Locally invasive
Adamantinoma
Malignant
Osteogenic sarcoma
Malignant lymphoma (Burkitt’s tumour)
Secondary tumours (by direct invasion or
bloodstream spread)
Cyst attached to the
root of a tooth
FIG 10.23
The site of origin of a dental cyst.
Chap-10.qxd 4/19/05 14:19PM Page 267
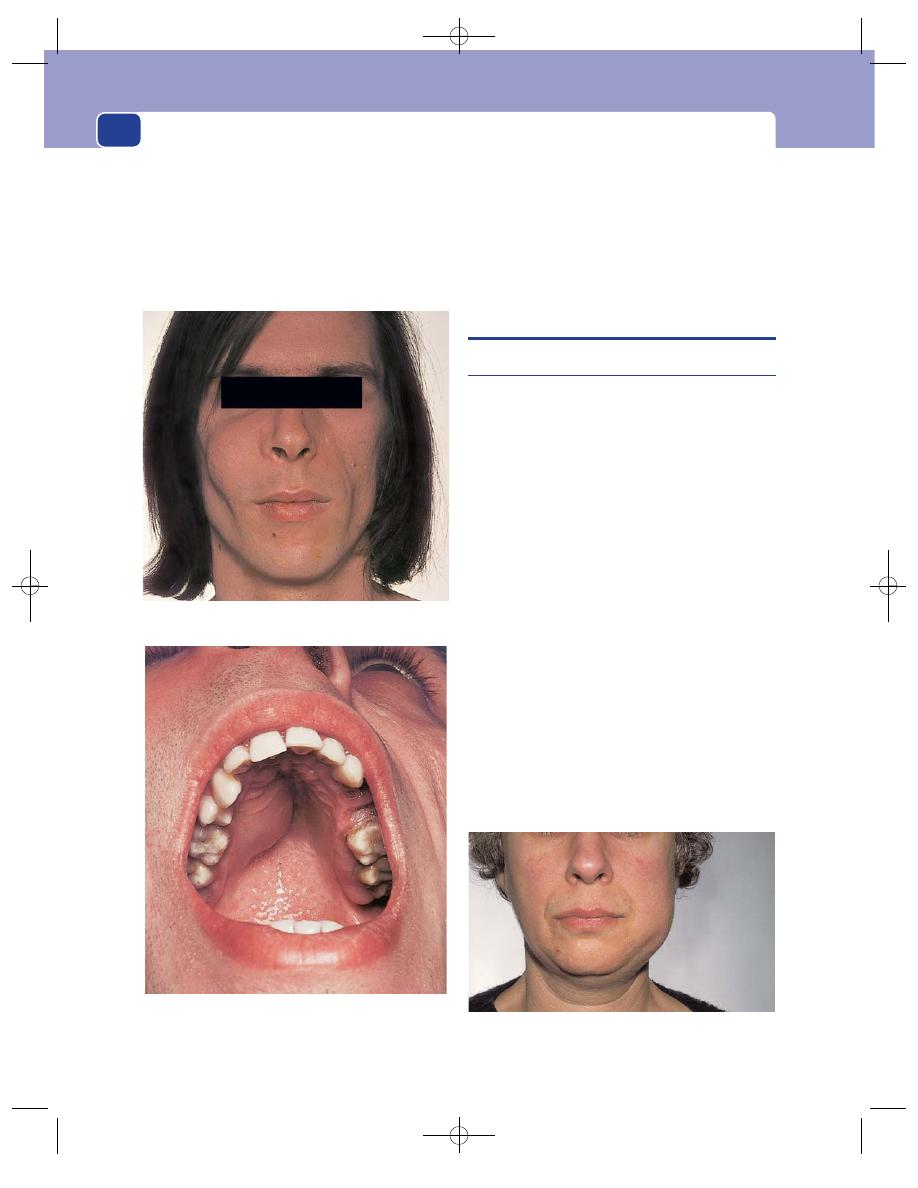
The mouth
268
the posterior part of the lower jaw in relation to
caries in the molar teeth or failure of their eruption.
An alveolar abscess in the upper jaw, pointing
medially, causes swelling of the palate and fauces.
Lymph drainage
The upper cervical lymph glands are
usually enlarged and tender.
Local tissues
The arteries and nerves of the face, jaw
and tongue should be normal. There may be visible
evidence of neglect of the teeth, such as caries and
gingivitis, and there may be unerupted teeth. If an
alveolar abscess points and discharges, it may
become a chronic discharging sinus.
THE JAW
Cysts of the jaw
Swelling of the whole jaw may be caused by infection,
a cyst or a tumour. These are classified in Revision
panel 10.4.
There are two common benign cysts of the jaw.
Dental cyst
This is a cyst attached to the root of a normally
erupted but usually decayed and infected tooth.
The epithelial cells that form the cyst are thought
to be derived from the enamel organ.
These cysts are more common in the upper jaw.
They grow steadily, expanding the jaw and filling
the maxillary antrum.
Clinical examination can get no further than
detecting that the swelling is in the bone. Sometimes
the bone is so thin that it ‘crackles’ when touched,
like a broken eggshell.
Dentigerous cyst
A dentigerous cyst is a cyst containing an unerupted
tooth.
The cyst can enlarge and cause swelling of the jaw.
The palate crackled when it was palpated because the bone
was so thin.
FIG 10.24
A large dental cyst expanding the maxilla and bulging into the
roof of the mouth.
FIG 10.25
A dentigerous cyst causing swelling at the angle of
the mandible.
Chap-10.qxd 4/19/05 14:19PM Page 268
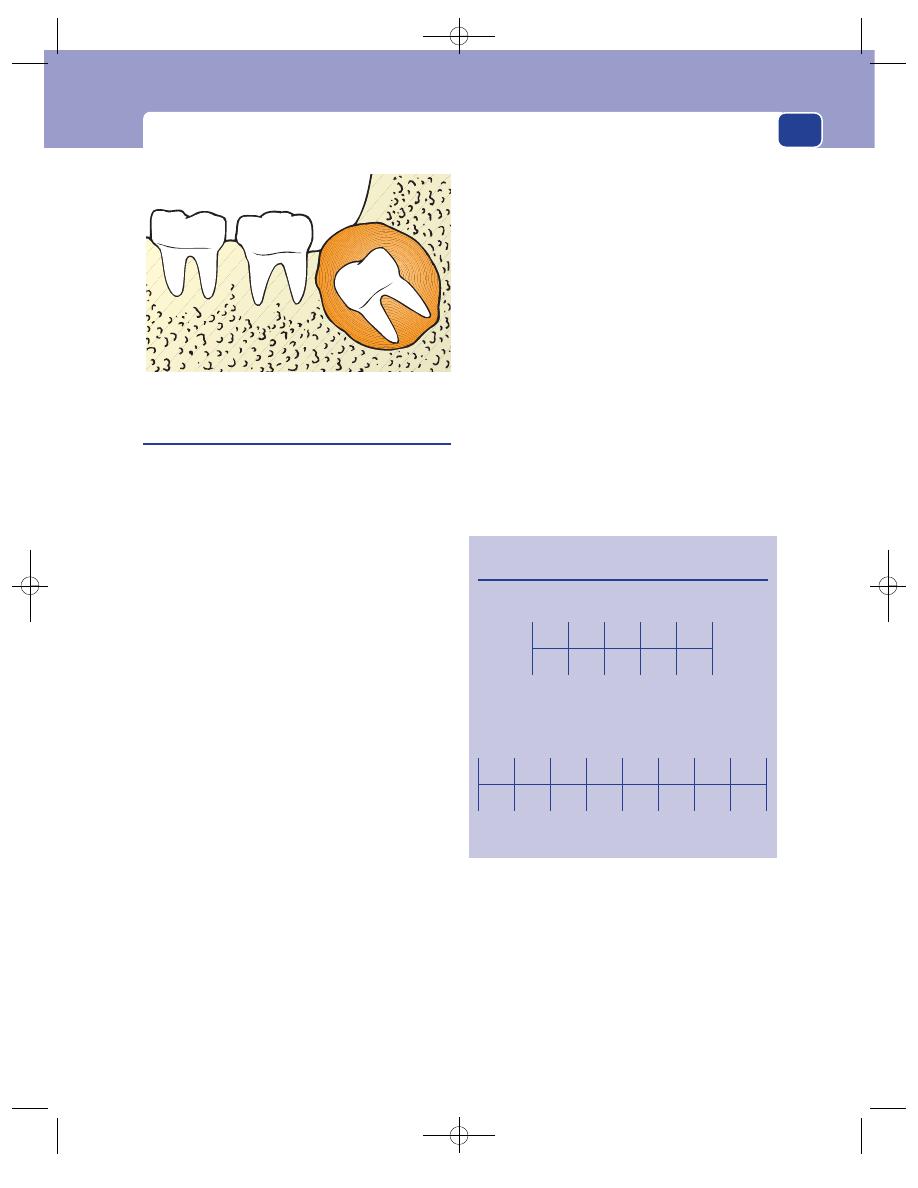
The jaw
Tumours of the jaw
Many types of benign and malignant tumours of
the jaw are listed in Revision panel 10.4. They all
present as a bony swelling that grows steadily, and
usually painlessly.
Four neoplastic causes of swelling of the jaw
deserve special mention.
Carcinoma of the antrum
Carcinomata of the antrum are much more com-
mon than primary bone tumours, and when they
invade downwards into the maxilla they cause
swelling of the upper jaw and palate.
Adamantinoma
Adamantinoma is a tumour which causes a painless,
progressive swelling of the jaw, but it is locally inva-
sive and tends to recur.
Osteosarcoma
Osteosarcomata can occur in both the upper and
the lower jaw.
Malignant lymphoma
(Burkitt’s lymphoma)
Burkitt’s lymphoma is a malignant tumour of B
lymphocytes associated with Epstein–Barr virus
infection. In 80 per cent of patients it presents as a
tumour in the jaw. In its endemic form it affects
children below the age of 12 years and occurs in
those areas of sub-Saharan Africa and the coastal
regions of New Guinea that have a warm, wet climate
and endemic malaria. It is believed that the latter
causes immune depression of T suppressor cells,
which permits the uncontrolled proliferation of
Epstein–Barr-virus-infected B cells to form the
tumour. Sporadic cases of Burkitt’s lymphomata
also occur throughout the world.
The child presents with a progressive, painless
swelling of the jaw which distorts the face, may dis-
place the eye and partially occludes the mouth.
Lymphomatous tissue may also be present in
the retroperitoneal tissues, kidneys, ovaries and
spine, where it may cause abdominal and skeletal
symptoms.
269
Revision panel 10.5
Remember when the teeth erupt
Primary dentition (months)
Incisors
Canine
Milk molars
Permanent dentition (years)
Incisors
Canine
Premolars
Molars
7
9
18
22
24
6
9
18
22
24
冦
冦
7
8
11
11
11
6
12
18
7
8
11
11
11
6
12
18
冦
冦
冦
FIG 10.26
A dentigerous cyst.
Chap-10.qxd 4/19/05 14:19PM Page 269
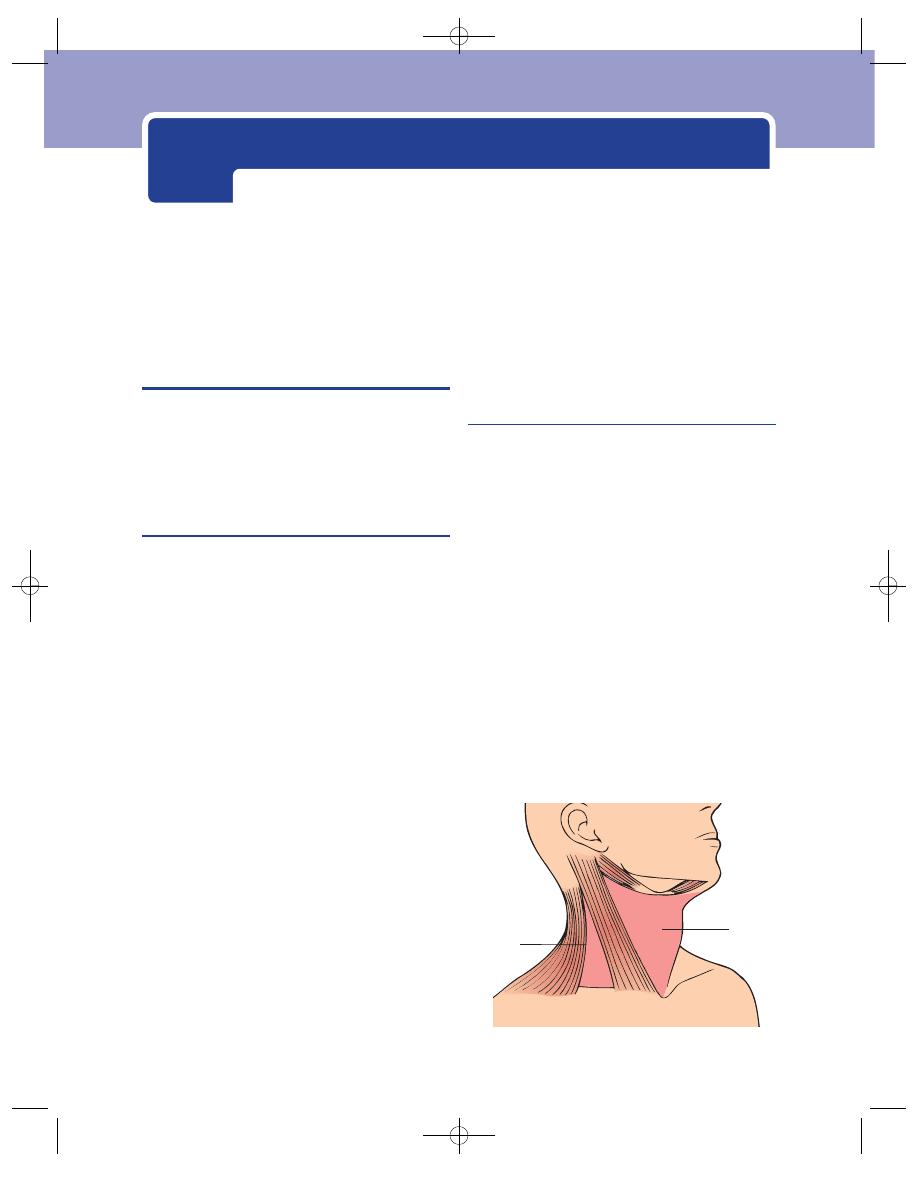
THE HISTORY AND EXAMINATION OF
SWELLINGS IN THE NECK
The majority of surgical conditions which arise in
the neck present as a swelling. Taking the history
and performing the physical examination should
follow the standard pattern, but there are some
important features that deserve special attention.
The history of swellings in the neck
Because the commonest cause of a swelling in the
neck is an enlarged lymph gland, and because the
commonest causes of enlarged lymph glands are
infection and secondary tumour deposits, you must
remember to ask about symptoms which might
help you identify the cause of the swelling.
Systemic illness
Symptoms such as general malaise, fever and rigors
and contact with people with infectious diseases
may indicate an infective cause of the swelling.
Loss of appetite, loss of weight, pulmonary, ali-
mentary or skeletal symptoms may suggest the site
of a neoplasm.
Irritation of the skin associated with enlarged
cervical lymph glands is often seen with lymphoma.
Head and neck symptoms
Ask about: pain in the mouth, sore throats or ulcer-
ation; nasal discharge, pain or blockage of the air-
way; pain in the throat, dysphagia, changes in the
voice and difficulty with breathing; and lumps or
ulcers on the skin of the head and face that have
changed size or begun to bleed.
The skin, mouth, nose, larynx and pharynx are
common sites for neoplasms, and although head
and neck cancers commonly present with metastases
in lymph glands, they are not usually associated
with the symptoms of distant metastases such as
general malaise and loss of weight.
The examination of swellings in the neck
Site
It is essential to define the site of a lump in the neck.
The neck is divided into two triangles. The ante-
rior triangle is bounded by the anterior border of
the sternomastoid muscle, the lower edge of the jaw
and the mid-line. In clinical practice, the structures
deep to the sternomastoid muscle are considered to
be inside the anterior triangle.
The upper part of the anterior triangle, below
the jaw but above the digastric muscle, is sometimes
called the digastric or submandibular triangle.
The posterior triangle is bounded by the poste-
rior border of the sternomastoid muscle, the ante-
rior edge of the trapezius muscle and the clavicle.
To define the triangles it is necessary to get the
patient to tense the neck muscles.
■
The sternomastoid muscle is made to contract
by putting your hand under the patient’s chin
Anterior
triangle
Posterior
triangle
FIG 11.1
The anatomical triangles of the neck.
Chap-11.qxd 12/11/07 9:49 AM Page 270
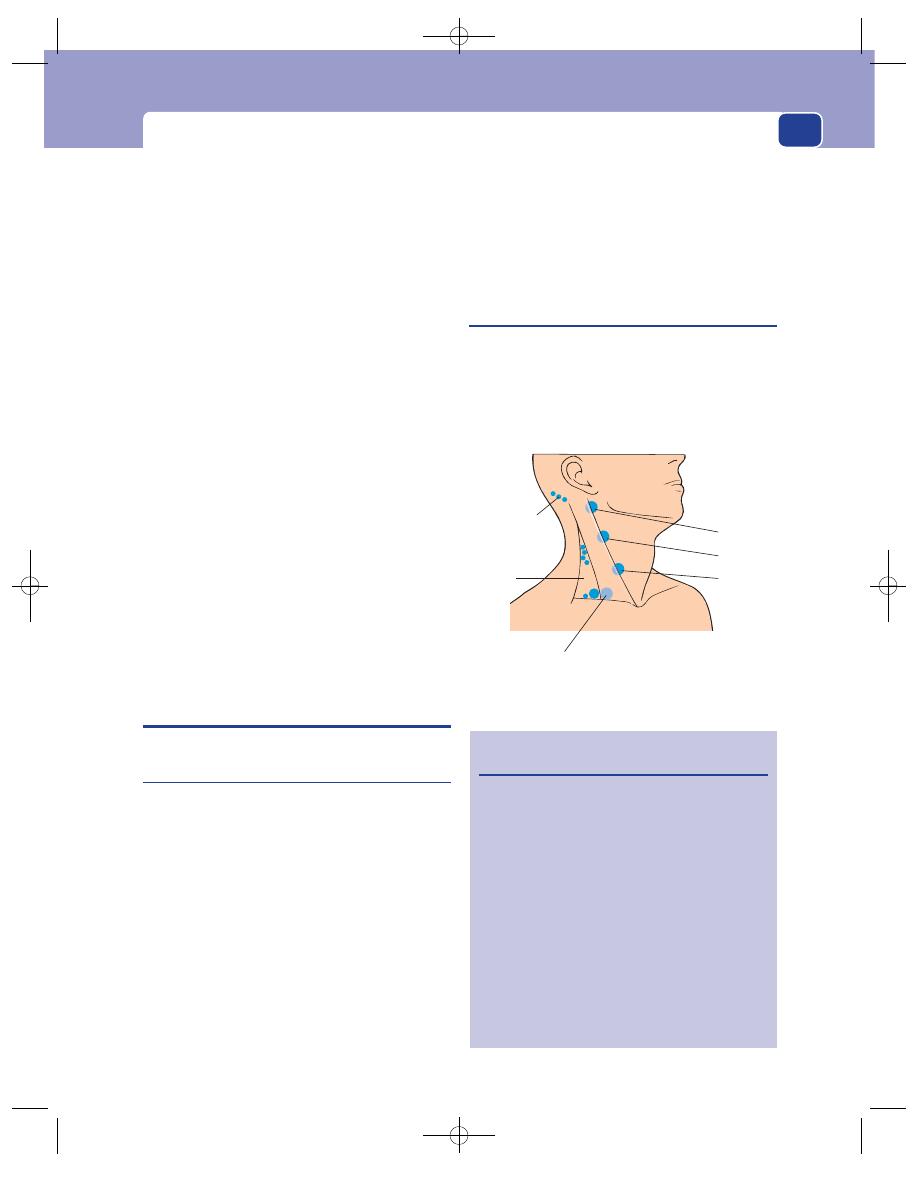
Cervical lymphadenopathy and other neck swellings
and asking them to nod their head against the
resistance of your hand. This tightens both
sternomastoids.
■
The trapezius muscle is made to contract by
asking the patient to shrug (elevate) their
shoulders against resistance.
Relation to muscles
Always feel lumps in the neck with the muscles
relaxed and then with them contracted. If the lump
is deep to a muscle, it will become impalpable when
the muscle contracts.
Relation to the trachea
Swellings that are fixed to the trachea will move when
the trachea moves. The trachea is pulled upwards
during swallowing. Assess the relationship to the
trachea of every lump in the neck by watching to see
if it moves with the trachea during swallowing.
Relation to the hyoid bone
The hyoid bone moves only slightly during swallow-
ing, but ascends when the tongue is protruded. Ask
the patient to open their mouth. When the jaw is
still, ask them to protrude their tongue. If the
swelling in the neck moves as the tongue protrudes,
it must be fixed to the hyoid bone.
CERVICAL LYMPHADENOPATHY AND
OTHER NECK SWELLINGS
Causes of cervical lymph gland
enlargement
Enlargement of the cervical lymph glands is the
most common cause of a swelling in the neck. Even
when only one gland is palpable, the adjacent glands
are invariably diseased.
The four main causes of cervical lymph gland
enlargement are as follows.
■
Infection: non-specific tonsillitis, glandular
fever, toxoplasmosis, tuberculosis, cat scratch
fever.
■
Metastatic tumour from the head, neck, chest
and abdomen.
■
Primary reticuloses: lymphoma,
lymphosarcoma, reticulosarcoma.
■
Sarcoidosis.
The diagnosis of lymphadenopathy caused by
systemic illnesses such as glandular fever, toxoplas-
mosis and sarcoidosis depends upon finding lympha-
denopathy elsewhere, other evidence of the underlying
disease, and special blood tests.
Non-specific cervical inflammatory
lymphadenopathy
Non-specific reactive lymphoid hyperplasia can fol-
low any inflammatory process or be associated with
skin conditions, particularly of the scalp, when it
is termed dermatopathic lymphadenopathy. How-
ever, non-specific inflammatory lymphadenopathy
271
Suboccipital
Supraclavicular
Posterior
triangle
Upper
Middle
Lower
Deep
cervical
FIG 11.2
The anatomy of the cervical lymph glands.
Revision panel 11.1
Causes of cervical lymphadenopathy
Infection
Non-specific
Glandular fever
Tuberculosis
Syphilis
Toxoplasmosis
Cat-scratch fever (Rochalimaea henselae)
Metastatic tumour
From head, neck, chest and abdomen
Primary reticuloses
Lymphoma
Lymphosarcoma
Reticulosarcoma
Sarcoidosis
Chap-11.qxd 12/11/07 9:49 AM Page 271
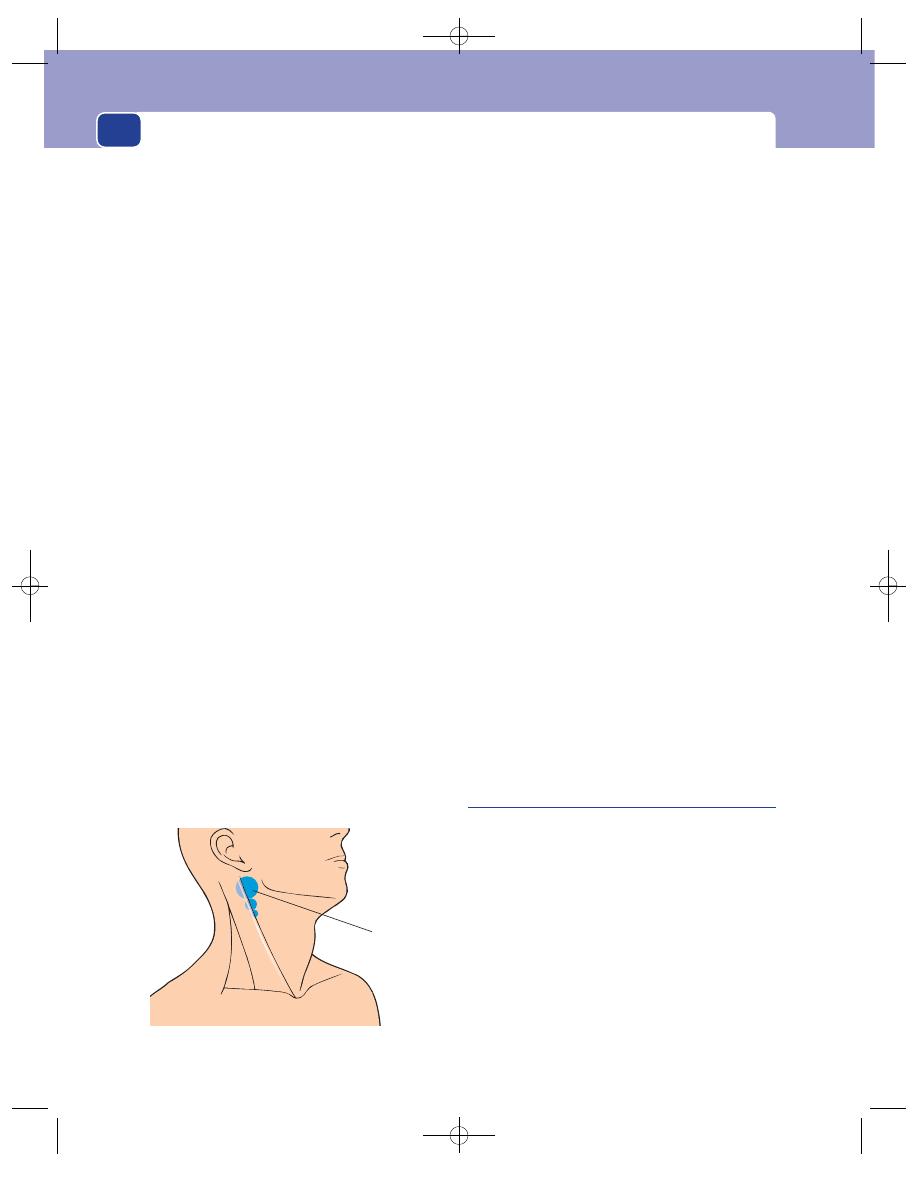
The neck
272
commonly follows recurrent bouts of tonsillitis,
especially if the attacks have been treated inade-
quately. The upper deep cervical glands are most
often affected.
In a healthy child, small normal lymph glands are
often palpable, especially in the posterior triangle.
History
Age
When associated with tonsillitis, the majority
of patients are below the age of 10 years. Other react-
ive conditions can occur at any age.
Symptoms
The common presenting symptom is a
painful lump just below the angle of the jaw.
The severity of the pain varies. It is usually a dis-
comfort, which becomes acute when the patient has
a sore throat.
The lump may be large enough to be visible or
felt by the child’s parent when washing the neck.
The child may snore at night, have difficulty in
breathing, have nasal speech because of tonsillar
and adenoid hyperplasia, and suffer from recurrent
chest infections.
Cause
The child and the parents frequently appreci-
ate the relationship between the appearance of the
lump and an episode of tonsillitis.
Systemic effects
When the lump is tender the patient
often feels ill, has a sore throat and pyrexia and does
not want to eat.
Recurrent severe episodes can cause loss of
weight and slow down the rate of growth and body
maturation.
Social history
Recurrent sore throats and upper
respiratory tract infections are more common in
malnurtured children living in substandard, cold,
damp houses.
Examination
Position
Lymph from the tonsils drains to the upper
deep cervical lymph glands. The gland just below
and deep to the angle of the mandible is often called
the tonsillar gland. This gland and those just below
it are likely to be enlarged.
Tenderness
If the infection is active, the enlarged
glands will be tender.
Shape and size
The tonsillar gland is usually spher-
ical and approximately 1–2 cm in diameter. It is
rarely bigger than this. The glands below it are usu-
ally smaller, even when inflamed.
Composition and relations
Each gland is firm in consist-
ence, solid and discrete, not fixed but not very mobile.
Local tissues
The tonsils are likely to be enlarged and
hyperaemic. Pus may be seen exuding from the sur-
face crypts.
The glands on the other side of the neck are often
just as large but may not have been noticed by the
parents.
General examination
Look for the presence of enlarged
lymph glands elsewhere. None should be enlarged.
Recurrent chest infections may have damaged
the lungs – look for collapsed lobes, bronchiectasis
and lung abscess. However, these are rare complica-
tions nowadays.
Tuberculous cervical lymphadenitis and
abscess
The human tubercle bacillus can enter the body via
the tonsils, and from there move to the cervical lymph
glands. The upper deep cervical glands are most often
affected. There is no generalized infection, so there
is little systemic disturbance of health. Infection
with bovine tuberculosis ceased in the UK when the
control and testing of dairy cattle was introduced.
History
Age and ethnic groups
Tuberculous lymphadenitis
is common in children and young adults, and in
the elderly. In the UK the incidence in the young
has diminished since the introduction of Bacilli
‘
Tonsillar’
lymph gland
FIG 11.3
The site of the ‘tonsillar’ lymph gland.
Chap-11.qxd 12/11/07 9:49 AM Page 272
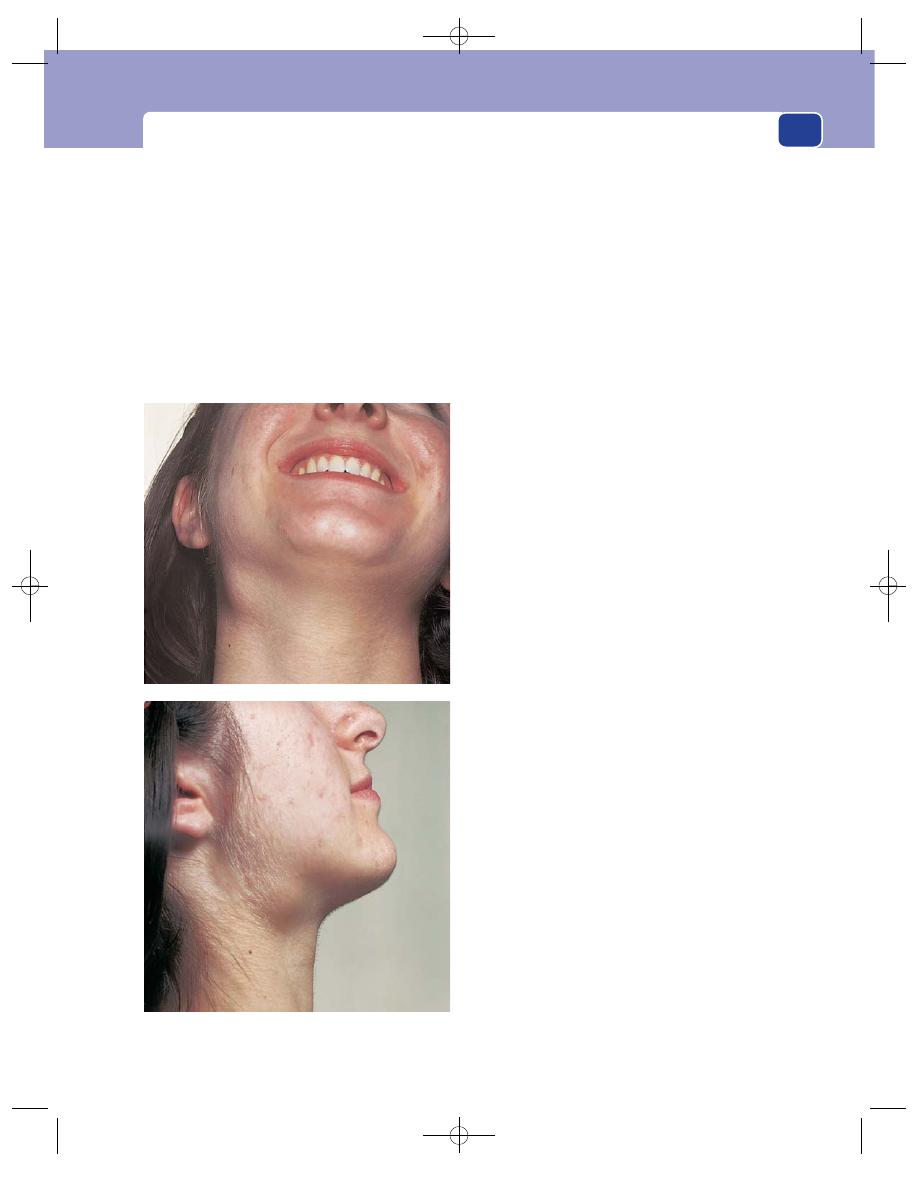
Cervical lymphadenopathy and other neck swellings
273
Calmette–Guerin (BCG) vaccination, mass radiog-
raphy screening and the discovery of effective anti-
tuberculosis antibiotics; but the prevalence of cervical
lymph gland enlargement caused by anonymous
mycobacteria is increasing. In the UK, tuberculous
lymphadenitis is found most often in young immi-
grant adults.
Symptoms
The patient complains of a lump in the
neck. This appears gradually, sometimes with, some-
times without, pain.
The pain can be intense if the glands grow rap-
idly and necrose.
Systemic symptoms are unusual in the young,
but the elderly sometimes have anorexia and slight
weight loss.
If the glands break down into an abscess, the
swelling increases in size, becomes more painful
and the patient notices discolouration of the over-
lying skin.
When the glands are very painful, neck move-
ments and swallowing may be painful.
Previous history
Elderly patients often have a history
of swollen neck glands when young – sometimes
treated at that time by surgical excision.
Immunization
Ask whether the patient has been vac-
cinated with BCG.
Family history
Check that no one in the family has
had tuberculosis.
Social history
Tuberculosis is more common in the
poor and socially underprivileged.
Examination
The signs of tuberculous lymphadenitis
Position
The upper and middle deep cervical glands
are most often involved.
Temperature
The mass of glands does not feel hot.
Tenderness
Although the temperature of the skin is
normal and the glands are often slightly tender, pain
and tenderness are not prominent features of tuber-
culous lymphadenitis.
Colour
If there is no abscess present, the overlying
skin should look normal.
Shape, size and consistence
In the early stages, the
glands are firm, discrete and between 1 and 2 cm in
diameter.
As caseation increases and the glands necrose,
the infection spreads beyond the capsules of the
glands. This makes the lumps enlarge and coalesce.
A typical patch of tuberculous lymphadenitis is an
indistinct, firm mass of glands which occupies the
upper half of the deep cervical lymph chain, partly
beneath and partly in front of the sternomastoid
muscle.
FIG 11.4
Enlargement of the upper deep cervical lymph
glands caused by tuberculosis.
Chap-11.qxd 12/11/07 9:49 AM Page 273
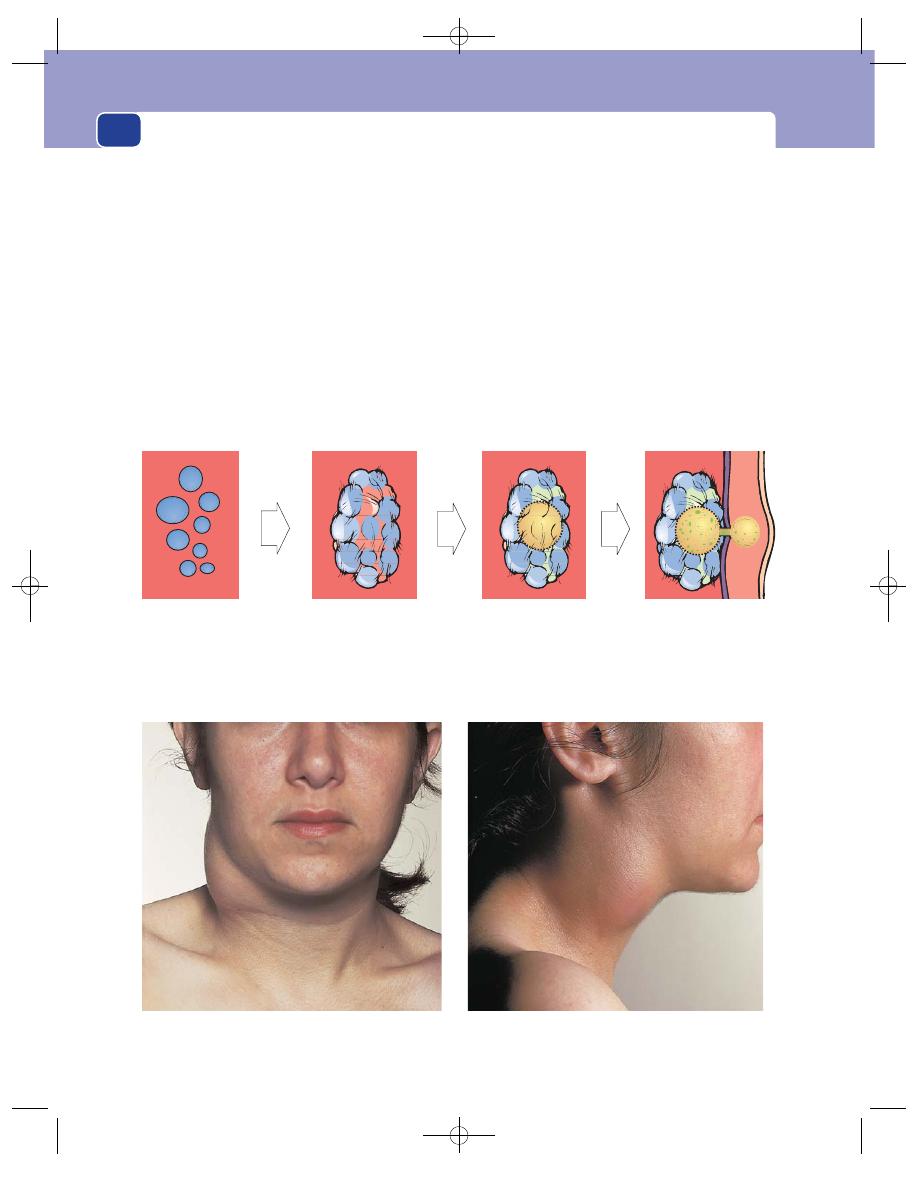
The neck
274
The glands are commonly described as matted
together, but there may be some discrete glands
above or below the matted mass.
Local tissues
Other cervical lymph glands may be
palpable. The tonsils and the other tissues in the
neck should be normal.
The signs of a tuberculous abscess
When an infected lymph gland caseates and turns
into pus, it becomes, by definition, an abscess. The
natural tendency of an abscess is to weaken the over-
lying tissues until it bursts through them, ultimately
to reach and burst through the skin. This is known
as pointing. At the stage when a tuberculous abscess
has burst through the deep cervical fascia into the
subcutaneous tissues, it has two compartments, one
on either side of the deep fascia, connected by a small
central track. This is called a collar-stud abscess.
Position
Because a tuberculous abscess forms in
tuberculous lymph glands, it is most often found in
the upper half of the neck.
Colour
When the pus reaches the subcutaneous tis-
sues, the overlying skin turns reddish-purple.
Temperature
The skin temperature is normal because
the process of caseation and pus formation is slow
and does not stimulate excessive hyperaemia –
hence the name cold abscess.
Enlarged discrete
glands
'Matted' glands
Abscess forms in the
centre of the glands
Abscess bursts
through the deep
fascia and becomes
'collar-stud' in shape
The development of a ‘collar-stud’ abscess.
FIG 11.5
THE TUBERCULOUS ABSCESS.
A large tuberculous ‘collar-stud’ abscess.
Chap-11.qxd 12/11/07 9:49 AM Page 274
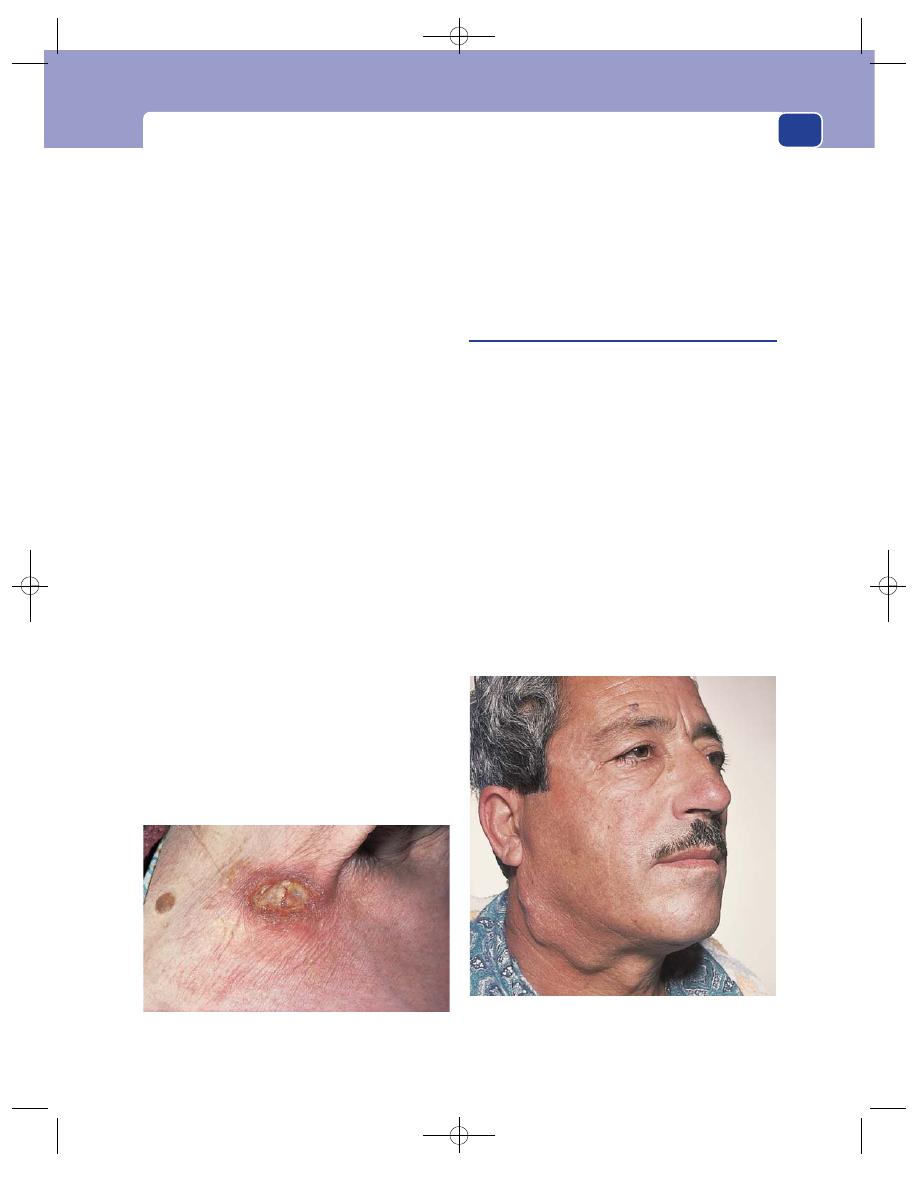
Cervical lymphadenopathy and other neck swellings
275
Tenderness
The mass is tender, sometimes exquis-
itely so if the abscess is tense.
Shape
The deep part of the abscess tends to be
sausage shaped, with its long axis parallel to the
front edge of the sternomastoid muscle. The super-
ficial pocket of the abscess is usually lower than the
deep part.
Size
Most tuberculous abscesses are 3–5 cm across,
but they can be much larger.
Surface
The surface is irregular and indistinct.
Edge
The edges are moderately well defined if the
abscess is tense, but you will not be able to feel a def-
inite surface or edge if the pocket of pus is lax.
Composition
The abscess feels firm and rubbery and
if there is sufficient pus present, it will fluctuate.
This latter sign cannot be elicited if the abscess is
small and deep to the sternomastoid muscle.
The subcutaneous part of a collar-stud abscess
should be clearly fluctuant, but it is not usually pos-
sible to reduce the superficial pocket of pus into the
deep pocket.
Relations
The original abscess is deep to the deep
fascia, partly under the sternomastoid muscle, and
fixed to surrounding structures. The superficial part
of a collar-stud abscess is immediately below the
skin and becomes more prominent when the ster-
nomastoid muscle is contracted. If spontaneous dis-
charge occurs, a chronic sinus may form. Tuberculous
sinuses are characterized by minimal erythema and
lack of pain, unless secondarily infected.
The other lymph glands in the neck near the
abscess may be enlarged.
General examination
When the patient has tuberculous
lymphadenitis there are often no systemic abnormal-
ities; but when a tuberculous abscess develops there
may be tachycardia, pyrexia, anorexia and general
malaise.
There may be signs of tuberculosis in the lungs,
in other lymph glands and in the urinary tract.
Carcinomatous lymph glands
Metastatic deposits of cancer cells in the cervical
lymph glands are the commonest cause of cervical
lymphadenopathy in adults.
The primary cancer is most often in the buccal
cavity (tongue, lips and mucous membrane) and lar-
ynx, but every possible primary site must be exam-
ined when cervical glands are thought to be enlarged
by secondary deposits.
History
Age
Most head and neck cancers occur in patients
over the age of 50. Most patients presenting with
metastatic deposits in their cervical lymph glands
are between 55 and 65 years.
The exception is papillary carcinoma of the thy-
roid, which occurs in children and young adults.
FIG 11.6
A chronic tuberculous sinus that has become
secondarily infected.
FIG 11.7
This patient presented with hard, enlarged lymph
glands in the neck. The primary lesion was the insignificant
mole above his right eyebrow.
Chap-11.qxd 12/11/07 9:49 AM Page 275
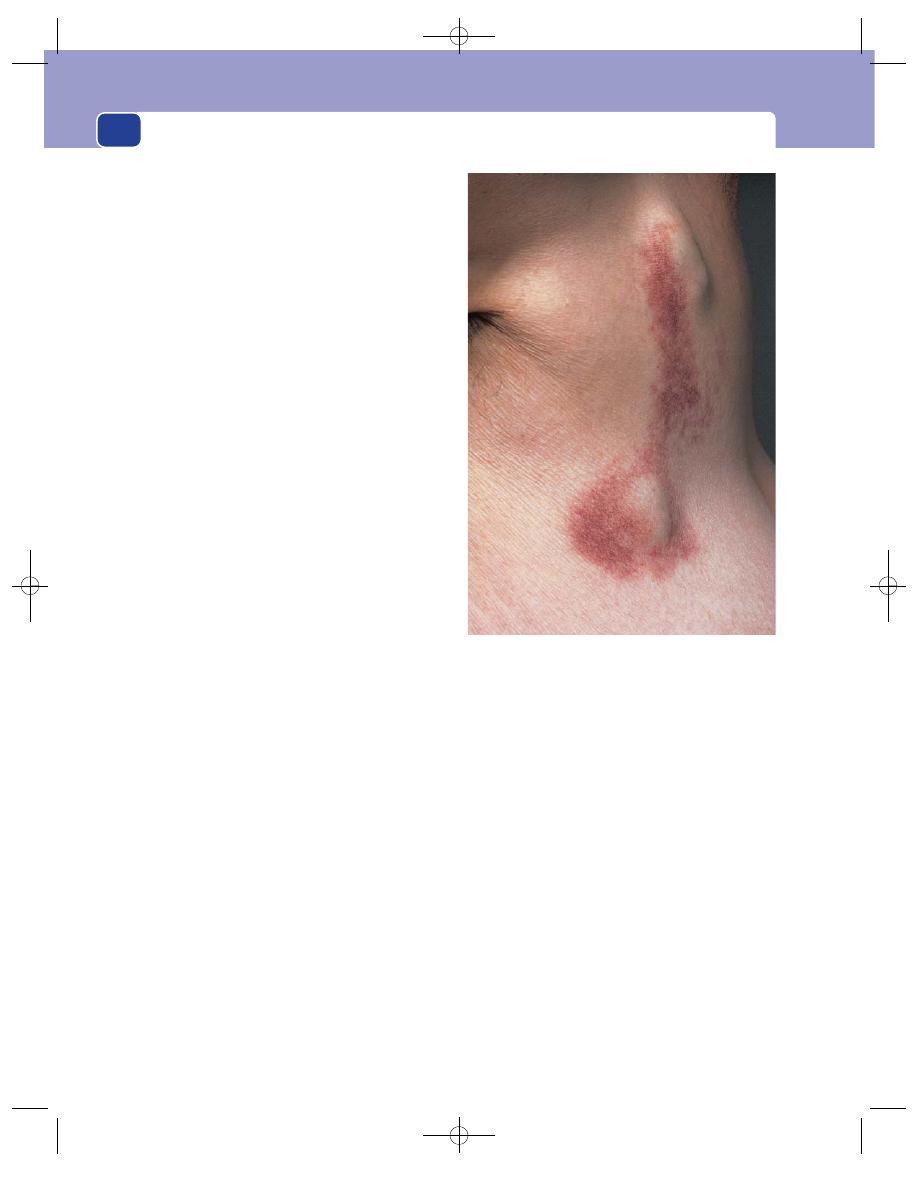
The neck
276
Sex
Most of the head and neck cancers are more
common in men than in women.
Local symptoms
The patient complains of a painless
lump in the neck, which they have seen or felt by
chance.
It is uncommon for carcinomatous glands to be
tender or to become so large that they interfere with
neck movements before being noticed.
The lump grows slowly, and new lumps may
appear.
General symptoms
The patient may have symptoms
from a primary lesion in the head or neck, such as a
sore tongue or a hoarse voice. If the primary is in
the chest, they may have a cough or haemoptysis; if
it is in the abdomen, they may have dyspepsia or
abdominal pain.
Generally speaking, head and neck cancers do
not cause anorexia and weight loss, whereas cancers
in the lungs and intra-abdominal organs do.
Examination
Site
The site of the affected glands gives a crude
indication of the site of the primary. Lesions above
the hyoid bone drain to the upper deep cervical
glands. The larynx and thyroid drain to the middle
and lower deep cervical glands. An enlarged supra-
clavicular lymph gland commonly indicates intra-
abdominal or thoracic disease. When enlarged by
metastases, this gland is called Virchow’s gland; its
presence is Troisier’s sign.
Colour
The overlying skin is a normal colour unless
the mass is so large that it stretches or infiltrates the
skin, which makes it pale or blotchy red.
Temperature
The skin temperature will be normal
unless the tumour is very vascular.
Tenderness
Glands containing secondary deposits
are not tender.
Shape and size
Glands containing metastases vary in
size and shape. Both features depend upon the
amount of tumour within them and the rate of its
growth. At first the glands are smooth, discrete and
a variety of sizes. As they grow, they may coalesce
into one large mass.
Composition
Glands containing tumour are hard,
often stony hard. Rarely, a very vascular tumour
deposit will be soft, pulsatile and compressible.
Relations
The glands are tethered to the surround-
ing structures, so they can usually be moved in a
transverse direction, but not vertically.
Their relation to the sternomastoid muscle varies
according to the group to which they belong. Sec-
ondary cancer is more common in the glands of the
anterior than the posterior triangle. These glands are
deep to the anterior edge of the sternomastoid.
If the tumour spreads beyond the capsules of the
glands, the mass becomes completely fixed.
Local tissues
The overlying skin and muscle may be
infiltrated with tumour, in which case the tumour
must be distinguished from secondary deposits
actually in the skin.
Lymph drainage
Other lymph glands on the pathway
between the primary lesion and the gland com-
plained of by the patient, and beyond it, may be
enlarged.
FIG 11.8
Secondary malignant deposits in the skin of the neck.
Chap-11.qxd 12/11/07 9:49 AM Page 276
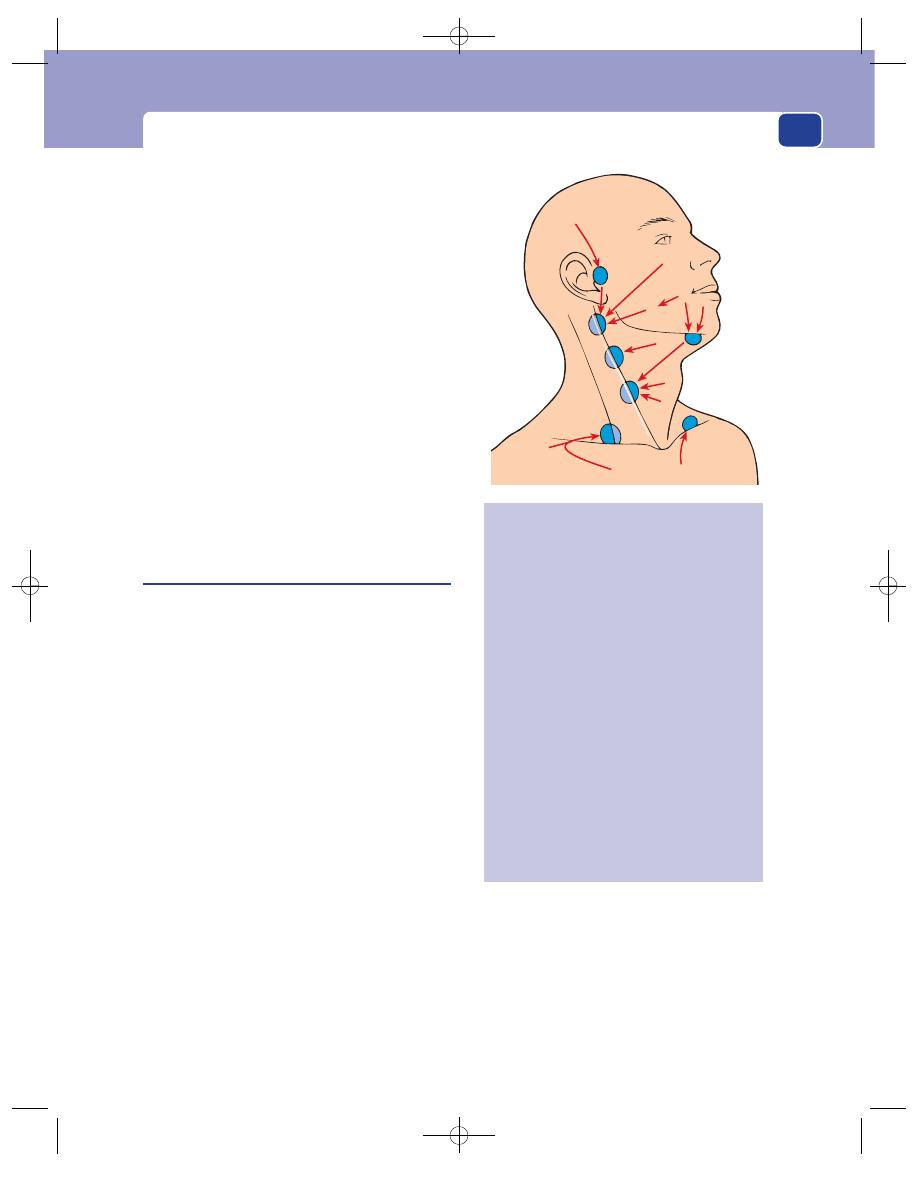
Cervical lymphadenopathy and other neck swellings
277
General examination
Examine all the sites which might
contain the primary lesion, in particular:
■
the skin of the scalp, the ear and the external
auditory meatus,
■
the lips, tongue, buccal mucous membrane and
tonsils,
■
the nose, maxillary antra and nasopharynx,
■
the thyroid gland,
■
the skin of the upper limb,
■
the breasts,
■
the lungs,
■
the stomach, pancreas, ovaries and testes.
The symptoms and signs of malignant disease
originating in these organs are discussed in the appro-
priate chapters.
Some of this examination requires special
instruments, for example a head mirror and light
and a laryngeal mirror.
Primary neoplasms of the lymph glands
(Reticuloses, lymphoma)
The most common primary tumour of lymphoid
tissue is the malignant lymphoma. There are many
histological varieties of lymphoma, but they are
often collectively and loosely divided into Hodgkin’s
and non-Hodgkin’s lymphoma.
History
Age
The reticuloses are common in children and
young adults.
Sex
Males are affected more often than females.
Symptoms
The most common presenting symptom
is a painless lump in the neck, which is noticed by
chance and grows slowly.
Malaise, weight loss and pallor are common
symptoms.
Itching of the skin (pruritus) is an unexplained
but distinctive complaint.
There may be fever with rigors, occurring in a
periodic fashion (Pel–Ebstein fever).
Lymphomatous infiltration of the skeleton may
cause pains in the bones, and there may be abdom-
inal pain after drinking alcohol.
If there are large masses of lymph glands in the
mediastinum, they may occlude the superior vena
cava, causing venous congestion in the neck and
the development of collateral veins across the chest
wall.
Large masses in the abdomen can obstruct the
inferior vena cava and cause oedema of both legs.
1
2
3 4
5
6
7
8
11
10
9
FIG 11.9
Sites of primary neoplasms that metastasize to the
cervical lymph glands.
1. Scalp (sometimes via the preauricular node)
Parotid gland
Upper face
Ear
2. Maxillary antrum and other air sinuses
Nasal cavity and nasopharynx
3. Tongue
Buccal mucosa
Floor of mouth
Mandible
4. Lips
5. Tonsil
Base of tongue
Oropharynx
6. Submandibular gland
Skin of neck
7. Larynx and laryngopharynx
8. Thyroid
Upper oesophagus
9. Upper limb and both sides of the chest wall
10. Breast
11. Lungs, stomach and all the viscera
Chap-11.qxd 12/11/07 9:49 AM Page 277
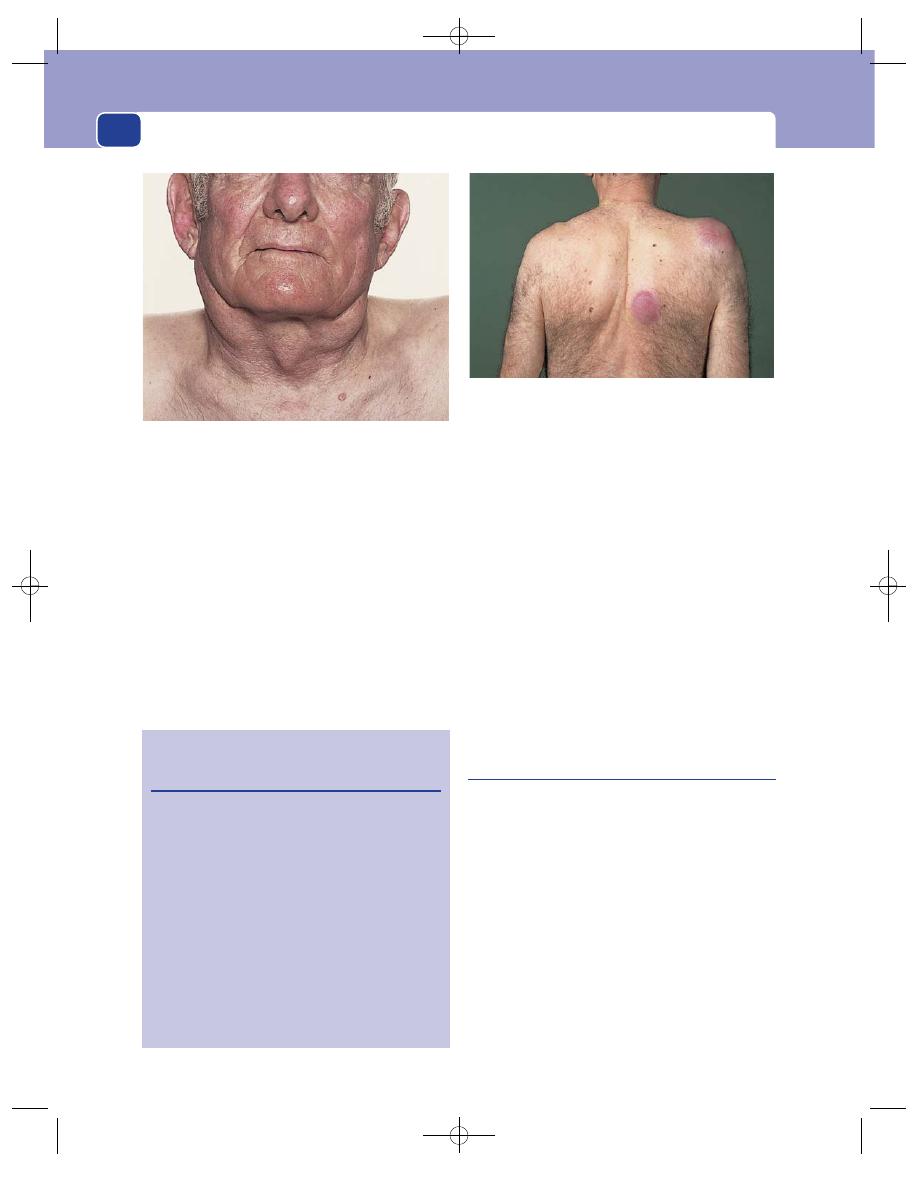
The neck
278
Examination
Site
Any of the cervical lymph glands can be
affected. Lymphoma is one of the few conditions,
apart from infection, that often causes lympha-
denopathy in the posterior triangle.
Tenderness
The glands are not tender.
Shape, size and surface
The lymph glands in Hodgkin’s
disease are ovoid, smooth and discrete.
It is possible to define individual glands even
when they become large. This is the opposite to
tuberculosis, in which the lymph glands become
matted and indistinct.
Consistence
Glands infiltrated by lymphoma are
solid and rubbery in consistence.
Relations
Although tethered to nearby structures,
these glands can usually be moved from side to side
and rarely become completely fixed.
Local tissues
The surrounding tissues should be
normal.
General examination
Other groups of lymph glands
may be enlarged. The liver and spleen may be pal-
pable. The patient is often anaemic and may be
jaundiced.
Spread to the skin produces elevated, reddened,
scaly patches of skin known as mycosis fungoides.
Branchial cyst
A branchial cyst is a remnant of a branchial cleft,
usually the second cleft. It is therefore lined with
squamous epithelium, but there are also patches of
lymphoid tissue in the wall which are connected
with the other lymph tissue in the neck and which
can become infected.
History
Age
Although these cysts are present at birth, they
may not distend and cause symptoms until adult
life. The majority present between the ages of
15 and 25 years, but a number appear in the 40s
and 50s.
Sex
Males and females are equally affected.
FIG 11.11
Cutaneous deposits of lymphoma.
Revision panel 11.2
Plan of examination for source of secondary
cervical lymphadenopathy
(Start at the top and work downwards.)
Examine the skin of the scalp, face, ears
and neck.
Look in the nose.
Look in the mouth at the tongue, gums, mucosa
and tonsils.
Palpate the parotid, submandibular and thyroid
glands.
Examine the arms and the chest wall – including
the breast.
Examine the abdomen and genitalia.
Transilluminate the air sinsuses.
Examine the nasopharynx and larynx with mirrors.
FIG 11.10
Bilateral cervical lymphadenopathy caused by
Hodgkin’s lymphoma.
Chap-11.qxd 12/11/07 9:49 AM Page 278
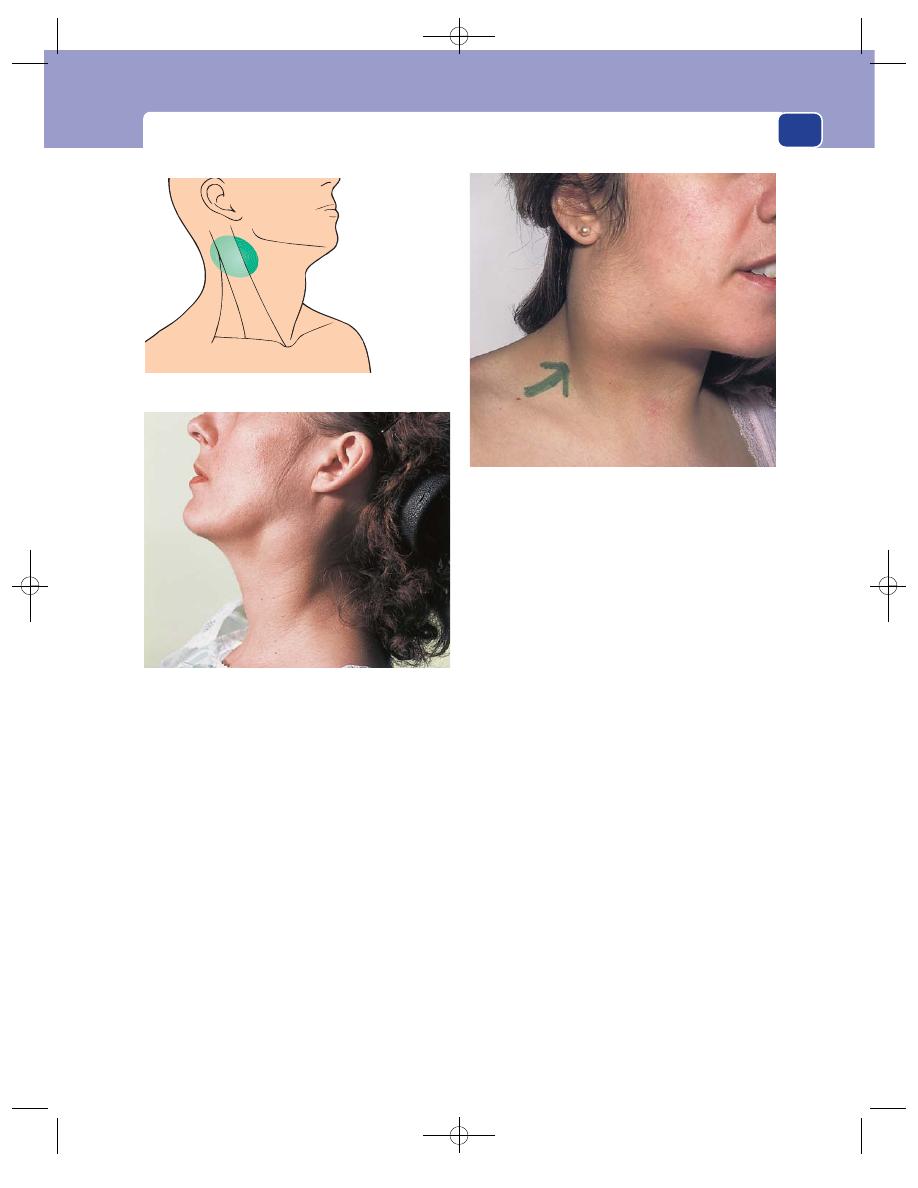
Cervical lymphadenopathy and other neck swellings
279
Symptoms
The common presenting complaint is a
painless swelling in the upper lateral part of the neck.
The lump may be painful when it first appears and
later cause attacks of pain associated with an increase
in the size of the swelling. The pain is usually caused
by infection in the lymphoid tissue in the cyst wall.
A severe throbbing pain, exacerbated by moving
the neck and opening the mouth, develops if the
contents of the cyst become infected and purulent.
General effects
These cysts have no systemic effects
and are not associated with any other congenital
abnormality.
Examination
Position
A branchial cyst lies behind the anterior edge
of the upper third of the sternomastoid muscle, and
bulges forwards. Very rarely, the cyst can bulge
backwards behind the muscle.
Colour and tenderness
The overlying skin may be red-
dened and the lump may be tender if the cyst is
inflamed.
Shape
The cyst is usually ovoid, with its long axis
running forwards and downwards.
Size
Most branchial cysts are between 5 and 10 cm
long.
Surface
Their surface is smooth and the edge distinct.
Composition
The consistence varies with the tension
of the cyst. Most cysts are hard, but a lax cyst feels
soft. They are dull to percussion.
The lump fluctuates. This sign is not always easy
to elicit, especially if the cyst is small and the sterno-
mastoid muscle thick.
The lump is usually opaque because it contains
desquamated epithelial cells that make its contents
thick and white. Sometimes the fluid is golden yel-
low and shimmers with fat globules and cholesterol
crystals secreted by the sebaceous glands in the epi-
thelial lining. Such cysts may transilluminate.
The cyst cannot be reduced or compressed.
Relations
It is important to ascertain that the bulk
of the mass is deep to the upper part of the
FIG 11.13
A branchial cyst which presented in adult life. The
back of the swelling is clearly deep to the sternomastoid
muscle.
FIG 11.14
A large branchial cyst which had become painful.
This commonly follows recurrent bouts of tonsillitis,
especially if the infection has been treated inadequately.
A branchial cyst
appears from
beneath the upper
third of the sterno-
mastoid muscle
FIG 11.12
The site of a branchial cyst.
Chap-11.qxd 12/11/07 9:49 AM Page 279
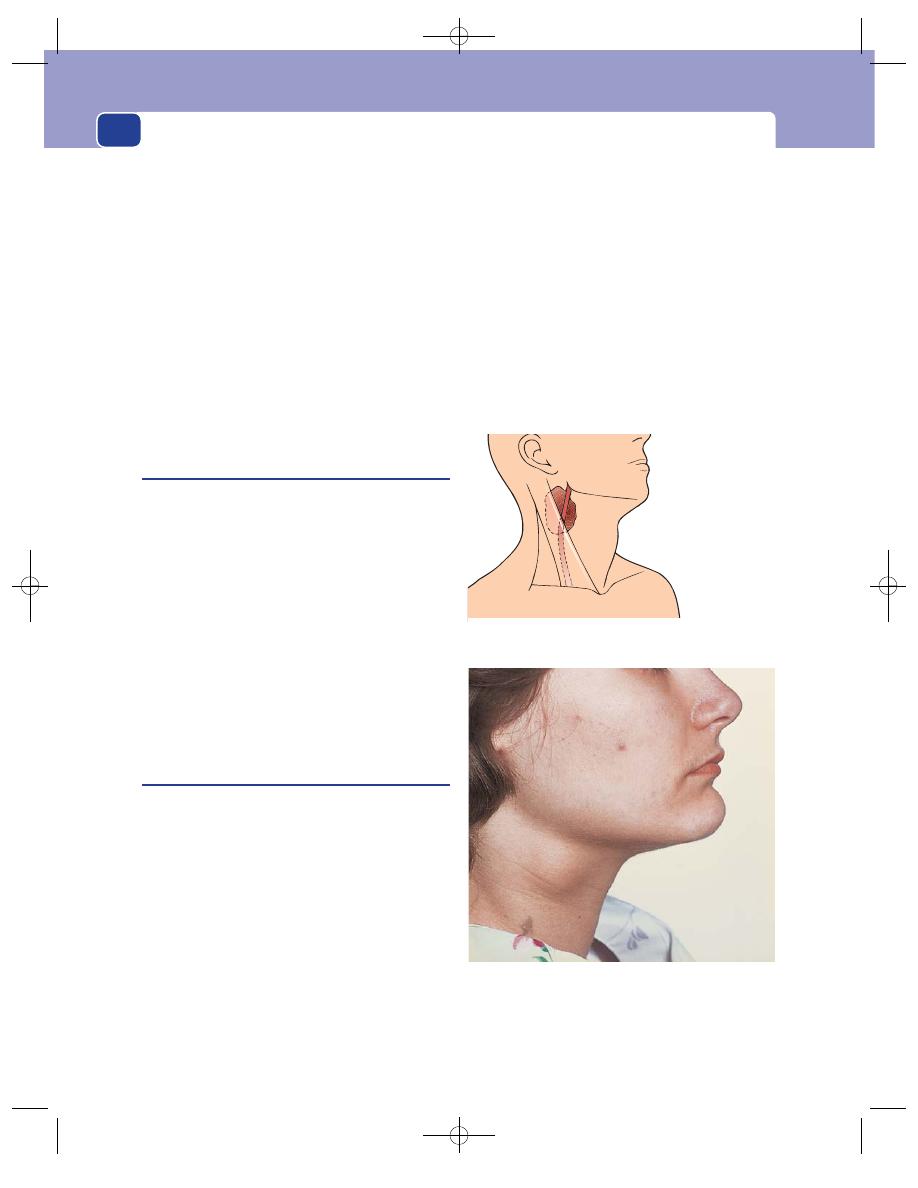
The neck
280
sternomastoid muscle. It is not very mobile because
it is closely tethered to the surrounding structures.
Lymph drainage
The local deep cervical lymph glands
should not be enlarged. If they are palpable, you
should reconsider your diagnosis in favour of an
inflammatory process such as a tuberculous abscess
rather than a branchial cyst. The other cystic lesions
that are often operated upon as presumed branchial
cysts are often secondary cystic lymph gland deposits
from a papillary carcinoma of the thyroid.
Local tissues
The local tissues should be normal.
If the cyst has turned into an abscess, the sur-
rounding tissues will be oedematous and the skin
hot and red.
Branchial fistula (or sinus)
This is a rare congenital abnormality. It is the rem-
nant of a branchial cleft, usually the second cleft,
which has not closed off.
The patient complains of a small dimple in the
skin at the junction of the middle and the lower
third of the anterior edge of the sternomastoid
muscle, that discharges clear mucus, and sometimes
becomes swollen and painful and discharges pus.
When the whole branchial cleft stays patent, the
fistula connects the skin with the oropharynx, just
behind the tonsil. In most cases the upper end is
obliterated and the track should really be called a
branchial sinus.
Swallowing accentuates the openings on the skin.
Carotid body tumour
This is a rare tumour of the chemoreceptor tissue
in the carotid body. It is therefore a chemodectoma.
It is usually benign, but can become quite large and,
occasionally, malignant.
History
Age
Chemodectomata commonly appear in patients
between the ages of 40 and 60 years.
Symptoms
The common presentation is a painless,
slowly growing lump. The patient may notice that
the lump pulsates, and may also suffer from symp-
toms of transient cerebral ischaemia (blackouts,
transient paralysis or paraesthesia). These symptoms
are unusual because the increasing compression of
the carotid artery by the tumour is a very slow
process.
Development
The lump grows so slowly that many
patients ignore it for many years.
Multiplicity
Carotid body tumours may be bilateral.
Examination
Always be especially gentle when palpating a lump
close to the bifurcation of the carotid artery. Pres-
sure in this area can induce a vasovagal attack.
Position
The carotid bifurcation is at, or just below,
the level of the hyoid bone. Carotid body tumours
FIG 11.16
A carotid body tumour. Note that the visible mass is
lower than that of a branchial cyst (see Fig. 11.13) but
indistinguishable on inspection from an enlarged cervical
lymph gland. Most carotid body tumours are initially mistaken
for enlarged lymph glands.
A carotid body
tumour should be
level with the
hyoid cartilage
The external
carotid artery may
cross the surface
of the tumour
FIG 11.15
The site of a carotid body tumour.
Chap-11.qxd 12/11/07 9:49 AM Page 280
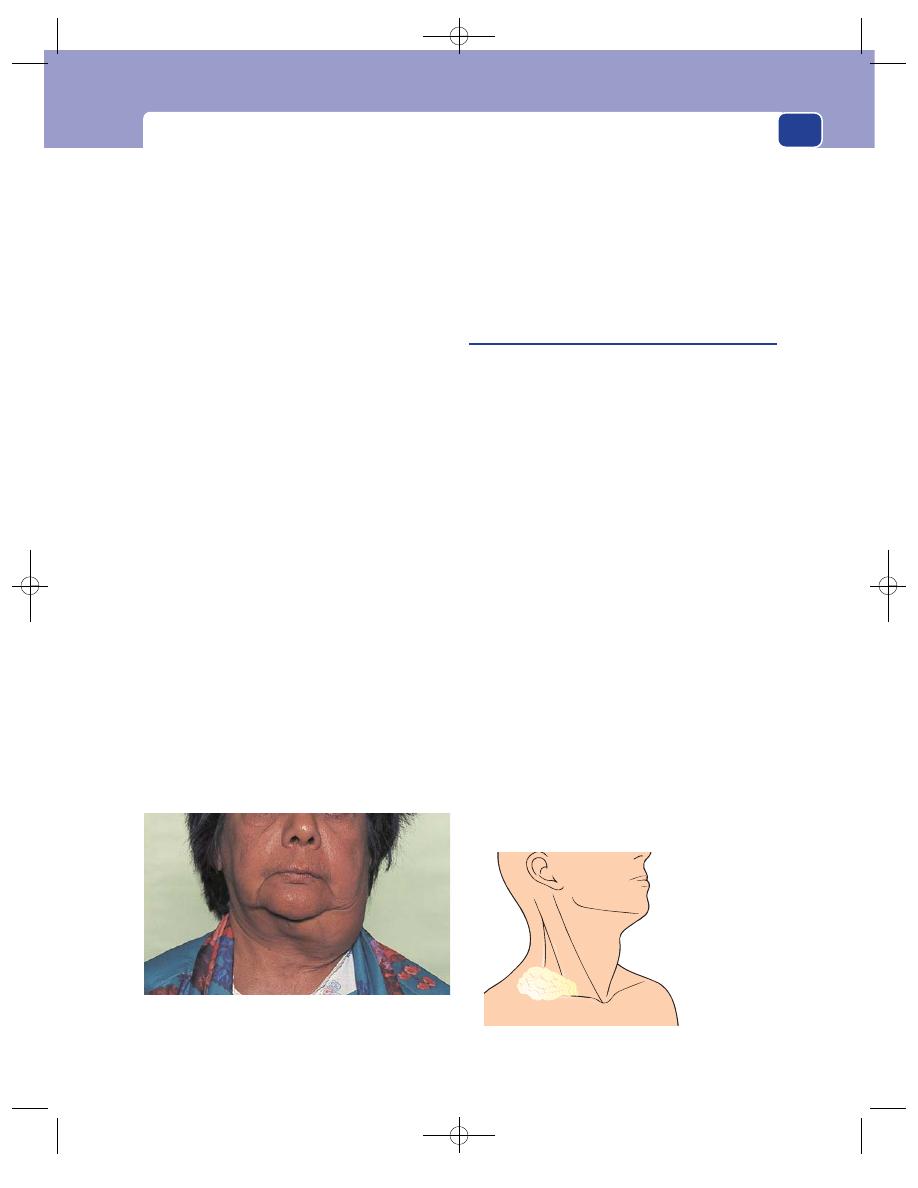
Cervical lymphadenopathy and other neck swellings
are therefore found in the upper part of the anterior
triangle of the neck, level with the hyoid bone and
beneath the anterior edge of the sternomastoid
muscle.
Tenderness, colour and temperature
These tumours are
not tender or hot, and the overlying skin should be
normal.
Shape
The lump is initially spherical but, as it
grows, it becomes irregular in shape, often narrower
at its lower end, where it is caught at the bifurcation
of the common carotid artery.
Size
Carotid body tumours may vary from 2–3 cm
to 10 cm in diameter.
Composition
The majority of these tumours are solid
and hard. They are dull to percussion and do not
fluctuate. They are often called potato tumours
because of their consistence and shape.
Sometimes these tumours pulsate. This is either
a transmitted pulsation from the adjacent carotid
artery, or a palpable external carotid artery running
over the superficial aspect of the lump, or a true
expansile pulsation from a soft or very vascular
tumour.
It is surprising that in spite of their vascularity
most of these tumours are hard. Those which are
soft and very vascular not only have an expansile
pulsation, but can also be compressed.
Relations
The lump is deep to the cervical fascia and
beneath the anterior edge of the sternomastoid
muscle.
The common carotid artery can be felt below the
mass, and the external carotid artery may pass over
its superficial surface. Without this close relation-
ship to the arteries, this tumour is indistinguishable
from an enlarged lymph gland.
Because of their intimate relationship with the
carotid arteries, these tumours can be moved from
side to side but not up and down.
Cystic hygroma
(Lymph cyst, lymphocele, lymphangioma)
A cystic hygroma is a congenital collection of lym-
phatic sacs which contain clear, colourless lymph.
They are probably derived from clusters of lymph
channels that failed, during intra-uterine develop-
ment, to connect with and become normal lymphatic
pathways. Lymph cysts commonly occur near the root
of the arm and the leg (i.e. in the anatomical junc-
tion between the limbs and head and the trunk).
History
Age
The majority of cystic hygromata present at
birth or within the first few years of life, but they
occasionally stay empty until infection or trauma in
adult life causes them to fill up and become visible.
Occasionally large lymphoceles can be seen in eld-
erly patients.
Symptoms
The only symptom is the complaint about
the lump, but the parents of an affected child are
usually more concerned about the disfigurement
caused by the cyst.
Family history
This condition is not familial.
Examination
Position
Cystic hygromata are commonly found
around the base of the neck, usually in the posterior
281
The cystic hygroma
is commonly found
in the subcutaneous
tissues at the base
of the posterior
triangle
It is brilliantly
translucent
FIG 11.18
The site of a cystic hygroma.
FIG 11.17
A large carotid body tumour. A very large, firm,
bosselated carotid body tumour – hence the term ‘potato
tumour’.
Chap-11.qxd 12/11/07 9:49 AM Page 281
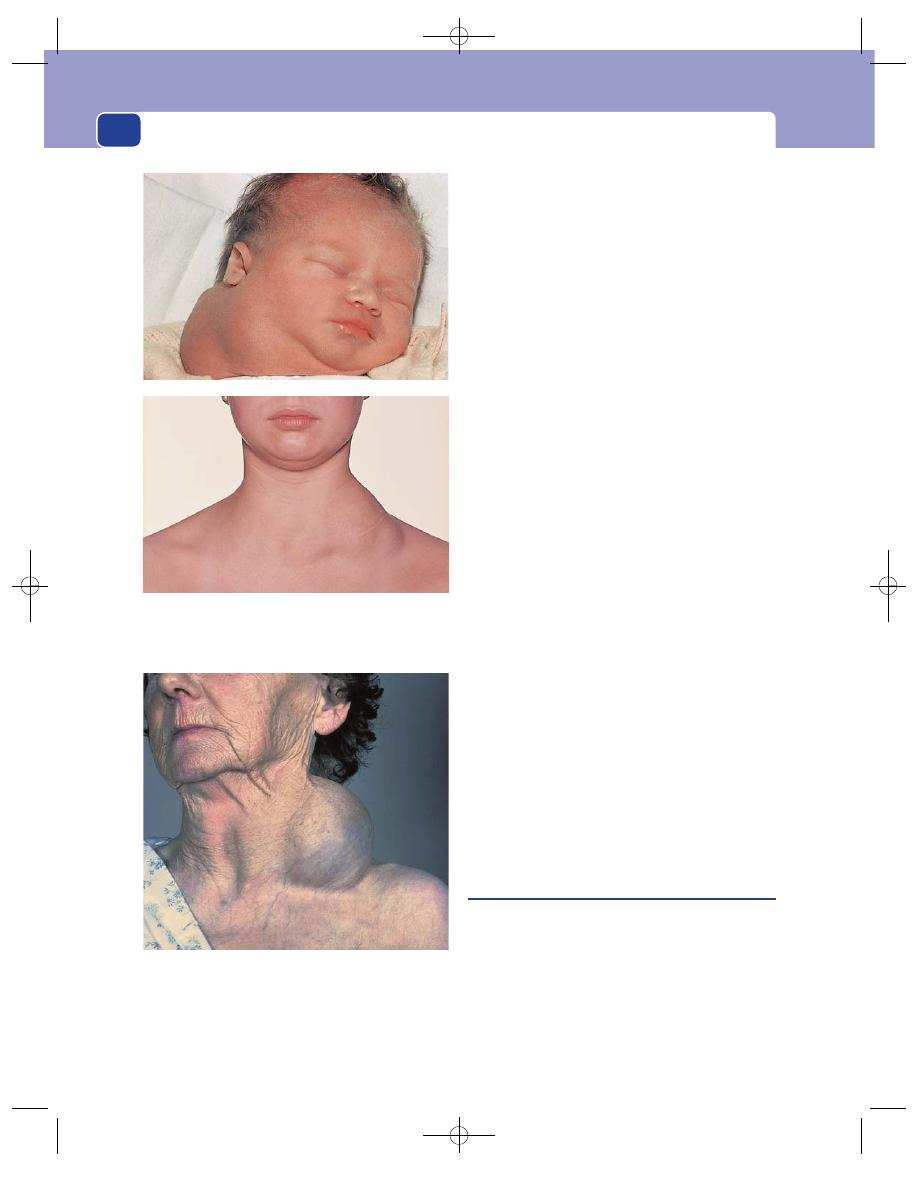
The neck
282
triangle, but they can be very big and occupy the
whole of the subcutaneous tissue of one side of
the neck.
Temperature and tenderness
They are not hot or ten-
der, and the overlying skin is normal.
Shape
A cystic hygroma is a mixture of soft uniloc-
ular and multilocular cysts, so the whole mass looks
lobulated and flattened.
Size
The small cysts are a few centimetres across.
Large cysts can extend over the whole of one side of
the neck.
Surface
If the cysts are close to the skin, it may not
be possible to feel a distinct surface. Deep cysts feel
smooth, but because they are lax their edges are
often indistinct.
Composition
Cystic hygromata are soft and dull to
percussion. They fluctuate easily but, because they
are close to the skin and contain clear fluid, their
distinctive physical sign is a brilliant translucence.
Large cysts will conduct a fluid thrill, and in some
multilocular swellings the fluid in one loculus can
be compressed into another.
They cannot be reduced.
Relations
Cystic hygromata develop in the subcuta-
neous tissues. Thus they are superficial to the neck
muscles and close to the skin but are rarely fixed to
the skin. However, it is essential to perform a thor-
ough examination of the oropharynx, as a cyst in the
posterior triangle may extend deeply beneath the ster-
nomastoid muscle into the retropharyngeal space.
Lymph glands
The local lymph glands should not be
enlarged and, as the lymph drainage of the tissues
around the cyst is normal, there is no lym-
phoedema. If there is associated lymphadenopathy,
reconsider the diagnosis, as cystic nodal metastases
of papillary thyroid carcinoma can present as large,
painless cystic swellings in the neck.
Local tissues
The local tissues are normal.
Pharyngeal pouch
A pharyngeal pouch is a pulsion diverticulum of the
pharynx through the gap between the horizontal fibres
of the cricopharyngeus below and the lowermost
oblique fibres of the inferior constrictor muscle
above. If swallowing is uncoordinated so that the
sphincter-like fibres of the cricopharyngeus do not
relax, the weak unsupported area just above these
fibres (known as Killian’s dehiscence) bulges out.
FIG 11.19
TWO EXAMPLES OF CYSTIC HYGROMA. In a very
young child – the common age of presentation, and in a
young adult.
FIG 11.20
A large lymphocele in an elderly lady.
Chap-11.qxd 12/11/07 9:50 AM Page 282
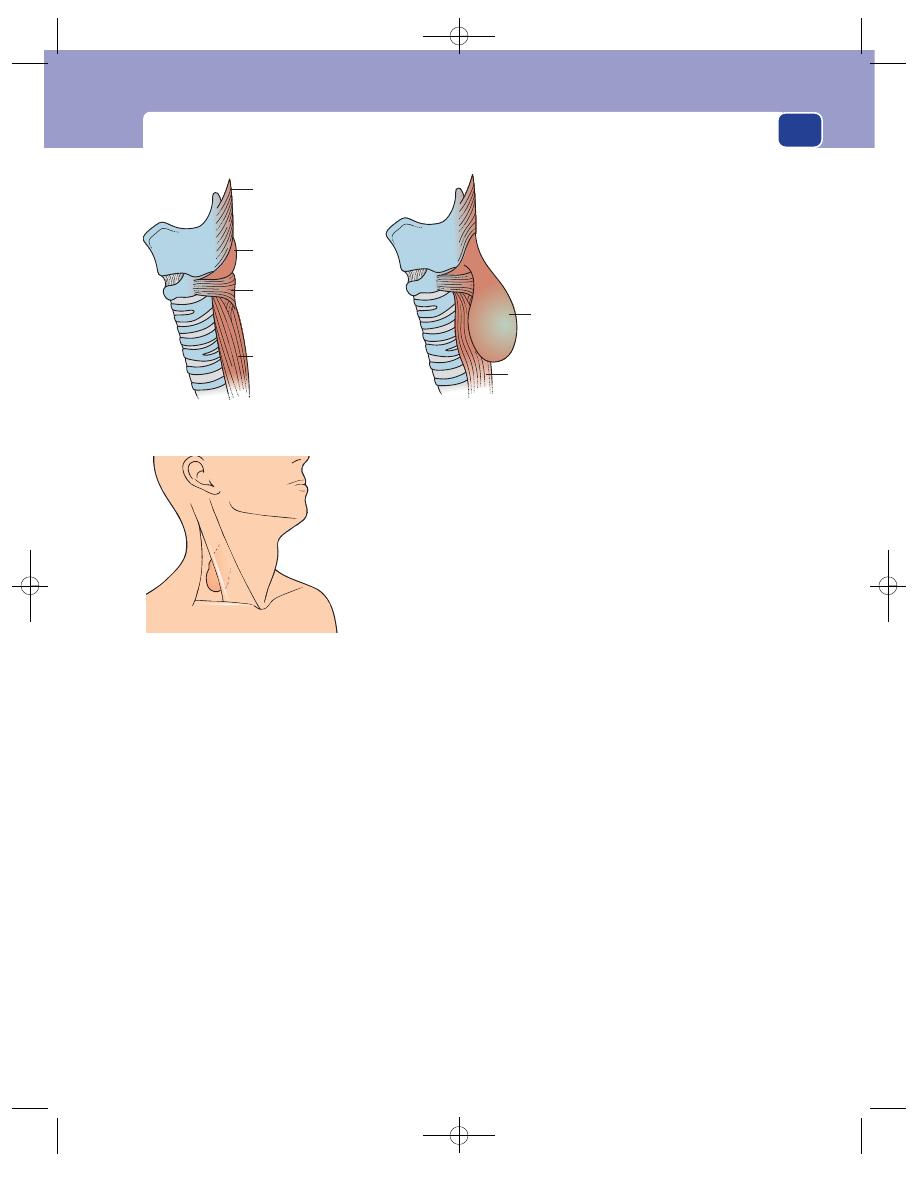
Cervical lymphadenopathy and other neck swellings
283
Eventually the bulge grows into a sac, which hangs
down and presses against the side of the oesophagus.
History
Age
Pharyngeal pouches appear in middle and
old age.
Sex
They are more common in men than in women.
Symptoms
Patients often have a long history of hali-
tosis and recurrent sore throats before noticing the
common presenting symptom of regurgitation of
froth and food. The regurgitated food is undigested
and comes up into the mouth at any time. There is
no bile or acid taste to it.
Regurgitation at night causes bouts of coughing
and choking, and if pieces of food are inhaled, a
lung abscess may develop.
As the pouch grows, it presses on the oesophagus
and causes dysphagia. Patients can sometimes swal-
low their first few mouthfuls of food (until the pouch
is full), but thereafter have difficulty in swallowing.
By the time these symptoms become severe, the
patient may have noticed a swelling in the neck,
and find that pressure on the swelling causes gurgling
sounds and regurgitation. The swelling changes in
size and often disappears.
If the dysphagia continues, the patient may
become malnourished and lose weight.
Examination
Position
In most patients there is no palpable swelling,
but when a swelling caused by a pharyngeal pouch
is apparent, it appears behind the sternomastoid
muscle, below the level of the thyroid cartilage.
Shape
Its shape is indistinct because only part of
its surface is palpable. It feels like a bulging deep
structure.
Size
Most pouches only cause a swelling of 5–10 cm
diameter. The pouch is not palpable when it is
smaller, so many patients have symptoms but no
abnormal physical signs.
Surface and edge
The surface is smooth, but the edge
is not palpable.
Composition
The lump is soft and sometimes
indentable. It is dull to percussion and does not
fluctuate or transilluminate.
It can be compressed and sometimes emptied.
Compression may cause regurgitation. Although
the mass may disappear with compression, not to
return until the patient eats again, it cannot be said
to have been ‘reduced’ according to the usual mean-
ing of the word.
Dehiscence
of Killian
Oblique fibres
of inferior constrictor
(thyropharyngeus)
Transverse fibres
of inferior constrictor
(cricopharyngeus)
Oesophagus
Normal
Pouch
Oesophagus
compressed
by pouch
Pharyngeal
pouch
FIG 11.21
The anatomy of a
pharyngeal pouch.
A pharyngeal pouch
rarely causes a
detectable swelling
If it does, the swelling
is behind the
sternomastoid muscle
FIG 11.22
The site of a pharyngeal pouch.
Chap-11.qxd 12/11/07 9:50 AM Page 283
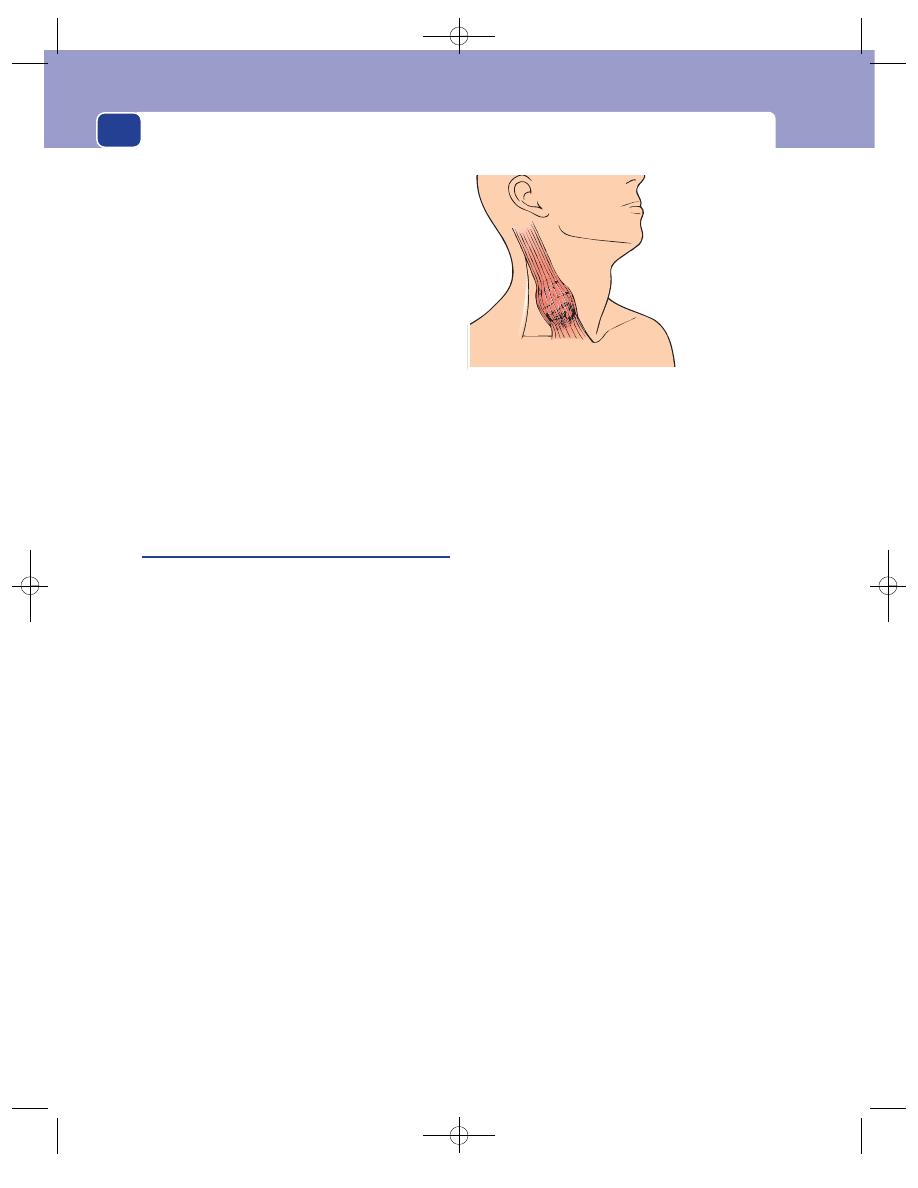
The neck
284
Relations
A pharyngeal pouch lies deep to the deep
fascia, behind the sternomastoid muscle, and is
fixed deeply. Its origin from a structure behind the
trachea can be appreciated during palpation, but
the neck of the pouch and its attachment to the
oesophagus cannot be felt.
It cannot be moved about in the neck.
Lymph glands
The cervical lymph glands should not
be enlarged.
Local tissues
The surrounding tissues feel normal.
Indeed, when the pouch is empty the whole neck
feels normal.
General examination
Pay special attention to the chest,
as there may be an aspiration pneumonia, collapse
of a lobe or a lung abscess.
Sternomastoid ‘tumour’
(Ischaemic contracture of a segment of the
sternomastoid muscle)
This is a swelling of the middle third of the ster-
nomastoid muscle. In neonates it consists of oedema
around an infarcted segment of the muscle, caused
by the trauma of birth. As the patient grows, the
lump disappears and the abnormal segment of
muscle becomes fibrotic and contracted.
History
Age
The lump is noticed at birth or in the first few
weeks of life.
Symptoms
The mother may notice the lump or that
the child keeps their head turned to one side –
torticollis. Attempts to turn the head straight may
cause pain or distress.
If the muscle is not extensively damaged, the
swelling slowly subsides, the muscle spasm relaxes
and the torticollis disappears. If the muscle damage
becomes an area of permanent fibrosis, the twist
and tilt of the head to one side becomes more
noticeable as the child grows.
Examination
The lump
Position
The swelling lies in the middle of the ster-
nomastoid muscle (i.e. in the middle third of the
neck on the antero-lateral surface).
Tenderness
The lump may be tender in the first few
weeks of life.
Shape and size
The swelling is fusiform, with its long
axis along the line of the sternomastoid muscle. It is
usually 1–2 cm across.
Surface
The surface is smooth.
Edge
The anterior and posterior edges of the lump
are distinct but the superior and inferior edges,
where the lump becomes continuous with normal
muscle, are indistinct.
Composition
At first the lump is firm and solid and
easy to feel, but as it gradually becomes harder it
begins to shrink and may become impalpable.
Surrounding structures and local lymph glands
These
should be normal.
The neck
Examine the movements of the neck. As the child
is too young to obey commands, you must watch
how they move their head when lying in their
cot, and then manipulate the head and neck very
gently.
The sternomastoid muscles rotate and tilt the
head. Contraction of the left sternomastoid turns
the head towards the right, but tilts the head to the
left. Both these deformities may be present. Forced
movement to correct the deformity may cause pain
and be resisted by the child.
Apart from the restriction of movement caused
by spasm of the sternomastoid muscle, the neck
movements should be normal.
A 'sternomastoid
tumour' is an area
of oedema and
necrosis in the
lower third of the
sternomastoid
muscle
FIG 11.23
The site of a sternomastoid tumour.
Chap-11.qxd 12/11/07 9:50 AM Page 284
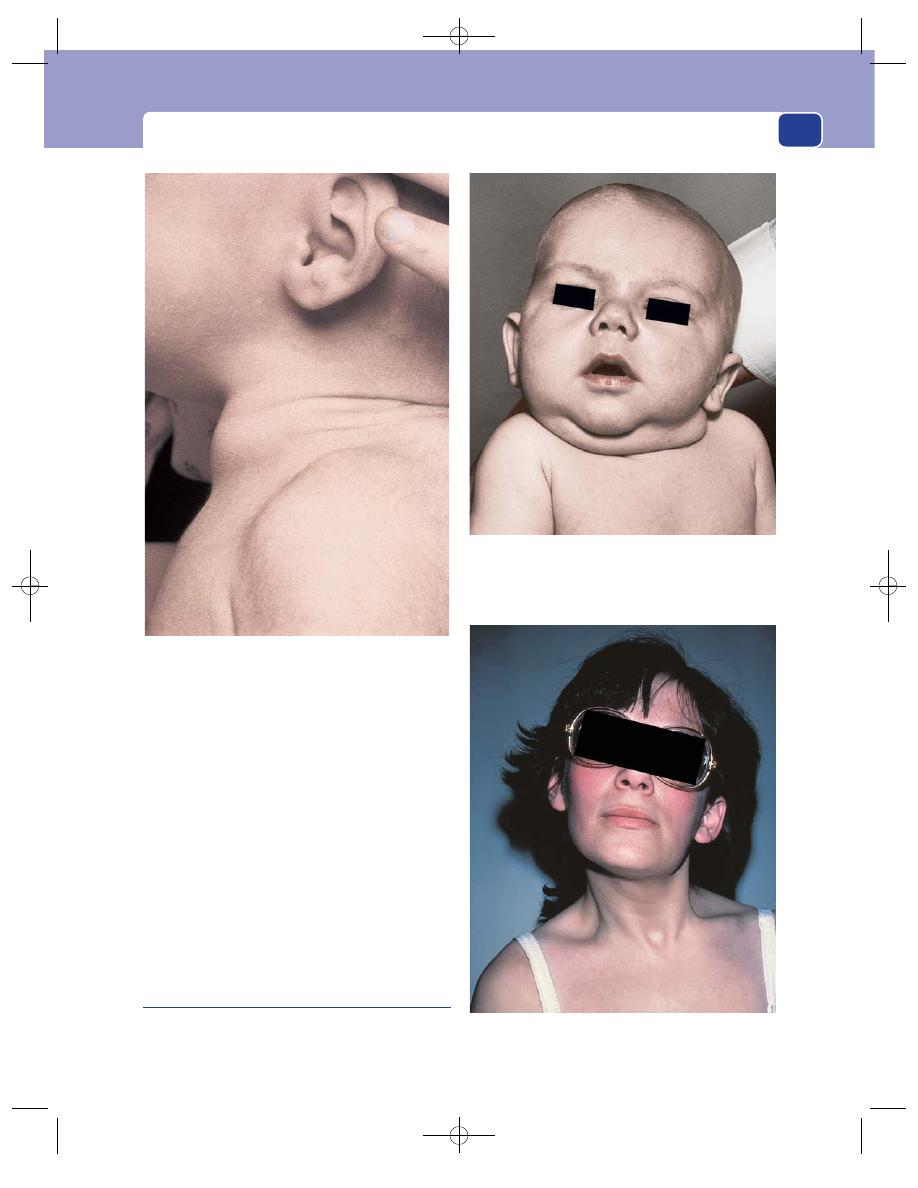
Cervical lymphadenopathy and other neck swellings
285
The eyes
Look at the eyes and watch their movements to detect
any squint. Torticollis can be a means of correcting a
squint. Move the head into a vertical and central
position and watch the eyes. If the torticollis is sec-
ondary to a squint and not a sternomastoid tumour,
the squint will appear as the head is straightened.
The head
An uncorrected torticollis may affect the growth of
the facial bones and cause facial asymmetry.
In adults, recent onset torticillis usually just rep-
resents muscle spasm.
Cervical rib
Although the cervical rib can cause serious neuro-
logical and vascular symptoms in the upper arm,
FIG 11.24
A localized swollen segment of sternomastoid with
a slight torticollis in an older child, caused by ischaemia and
fibrosis of the muscle after birth. A typical sternomastoid
‘tumour’.
FIG 11.25
An infantile torticollis caused by ischaemia of the
sternomastoid muscle.
FIG 11.26
An adult form of torticollis caused by muscular
spasm.
Chap-11.qxd 12/11/07 9:50 AM Page 285
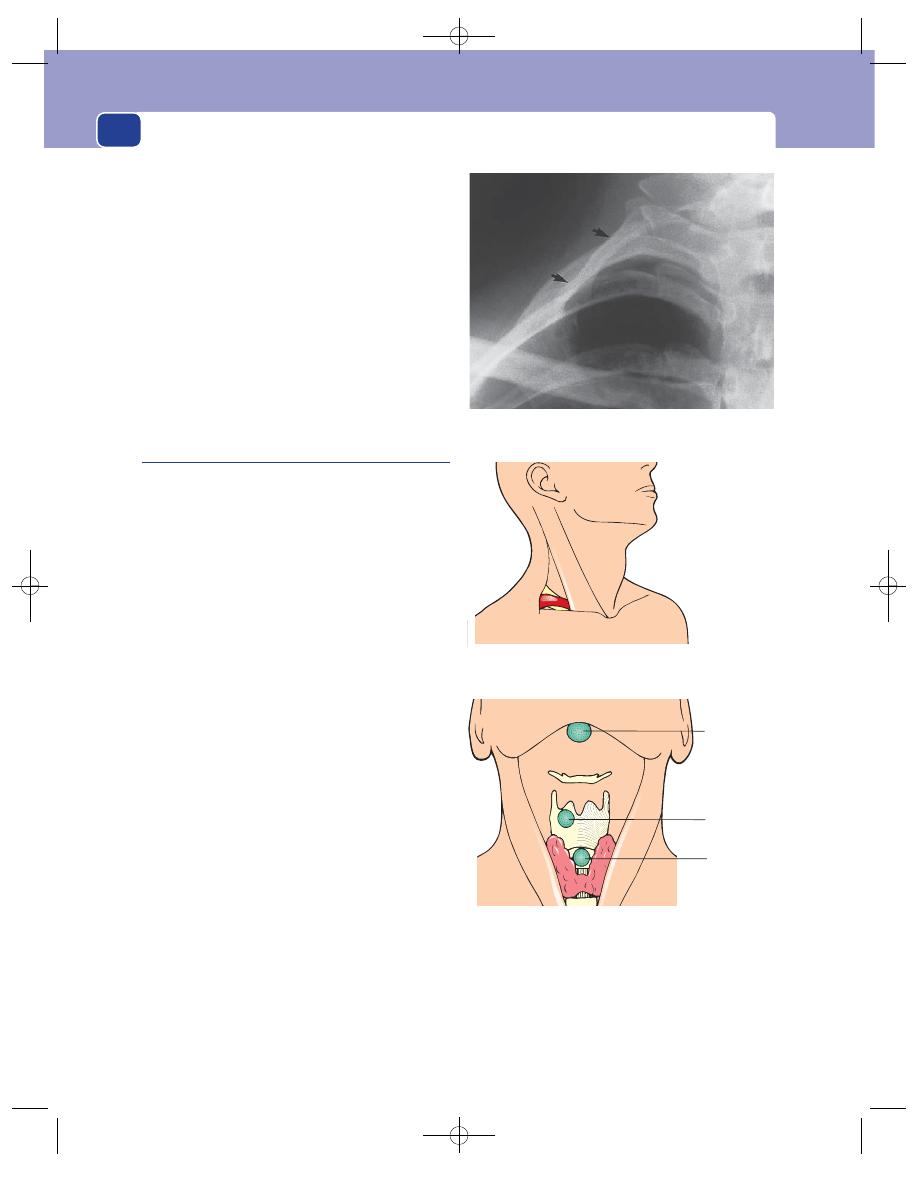
The neck
286
clinical examination of the neck does not usually
reveal any abnormalities. The abnormal rib is usu-
ally detected with an X-ray. Sometimes there is a
fullness at the root of the neck, but it is rarely dis-
tinct enough to justify a firm clinical diagnosis of
cervical rib. Occasionally it can be associated with
aneurysmal change in the subclavian artery.
The common neurological symptoms caused by
a cervical rib are pain in the C8 and T1 dermatomes,
and wasting and weakness of the small muscles in
the hand. Vascular symptoms such as Raynaud’s
phenomenon, trophic changes, even rest pain and
gangrene, may occur but are uncommon.
Thyroglossal cyst
The thyroid gland develops from the lower portion of
the thyroglossal duct, which begins at the foramen
caecum at the base of the tongue and passes down
to the pyramidal lobe of the isthmus of the thyroid
gland. If a portion of this duct remains patent, it can
form a thyroglossal cyst.
Theoretically, thyroglossal cysts can occur any-
where between the base of the tongue and the isth-
mus of the thyroid gland, but they are commonly
found in two sites: between the isthmus of the thy-
roid gland and the hyoid bone, and just above the
hyoid bone. Thyroglossal cysts within the tongue
and in the floor of the mouth are rare.
History
Age
Thyroglossal cysts appear at any age, but the
majority are seen in patients between 15 and 30
years old.
Sex
They are more common in women than in men.
Symptoms
The commonest symptom is a painless
lump in a prominent and noticeable part of the neck.
Pain, tenderness and an increase in size occur only
if the cyst becomes infected.
Duration of symptoms
The lump may have been pres-
ent for many years before an increase in its size
causes the patient to complain.
Systemic symptoms
There are no systemic symptoms
associated with this condition.
Examination
Position
Thyroglossal cysts lie close to the mid-line,
somewhere between the chin and second tracheal
ring. In the fetus the thyroglossal duct is in the
FIG 11.27
An X-ray demonstrating a cervical rib.
A cervical rib
rarely causes a
visible swelling
It may cause a
subclavian artery
aneurysm
FIG 11.28
The site of a cervical rib.
Suprahyoid
Subhyoid
Pretracheal
FIG 11.29
The sites of a thyroglossal cyst.
Chap-11.qxd 12/11/07 9:50 AM Page 286

Cervical lymphadenopathy and other neck swellings
287
mid-line, but when a cyst forms in adult life it often
slips to one side of the mid-line, especially if it devel-
ops in front of the thyroid cartilage.
Colour, temperature and tenderness
If the cyst is infected,
the overlying skin will be red, hot and tender. When
there is no infection, the overlying skin is normal.
Shape and surface
Thyroglossal cysts are spherical
and smooth, with a clearly defined edge.
Size
They vary from 0.5 to 5 cm in diameter. Because
a lump in the front of the neck is so noticeable,
patients often complain of these cysts when they are
very small.
Composition
Thyroglossal cysts have a firm or hard
consistence, depending upon the tension within the
cyst. Some cysts are too tense and others too small
to fluctuate, but the majority of thyroglossal cysts
are between these extremes and fluctuate with ease.
Some cysts transilluminate but many do not, either
because the contents have become thickened by
desquamated epithelial cells or the debris of past
infection, or because they are too small.
Revision panel 11.3
A scheme for the diagnosis of swellings
in the neck (deep to the deep fascia)
After your examination you should be able to
answer four critical questions:
1. Is there one or more than one lump?
2. Where is the lump?
3. Is it solid or cystic?
4. Does it move with swallowing?
Multiple lumps are invariably lymph glands
A single lump
In the anterior triangle that does not move with
swallowing
Solid:
■
a lymph gland
■
carotid body tumour
Cystic:
■
cold abscess
■
branchial cyst
In the posterior triangle that does not move with
swallowing
Solid:
■
a lymph gland
Cystic:
■
cystic hygroma
■
pharyngeal pouch
■
occasionally a secondary deposit of a
papillary thyroid carcinoma
Pulsatile:
■
subclavian aneurysm
In the anterior triangle that moves with
swallowing
Solid:
■
thyroid gland
■
thyroid isthmus lymph gland
Cystic:
■
thyroglossal cyst
Subhyoid cyst.
Pretracheal cyst.
FIG 11.30
TWO THYROGLOSSAL CYSTS.
Chap-11.qxd 12/11/07 9:50 AM Page 287
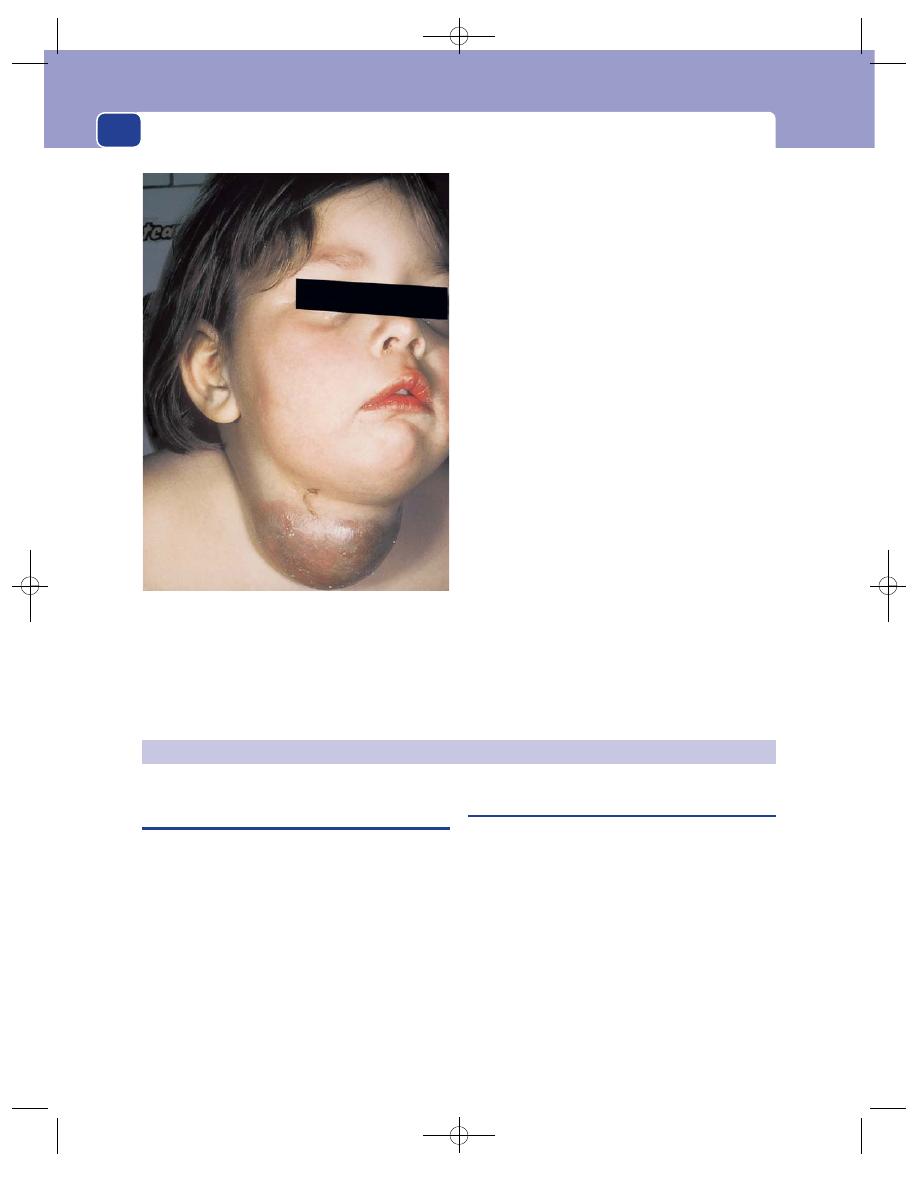
The neck
288
Relations
Thyroglossal cysts are tethered by the rem-
nant of the thyroglossal duct. This means that they
can be moved sideways, but not up and down.
The thyroglossal duct is always closely related,
usually fixed, to the hyoid bone. When the hyoid
bone moves the cyst also moves.
The hyoid bone moves upwards when the tongue
is protruded. First, ask the patient to open their
mouth and keep the lower jaw still; next hold the
cyst with your thumb and forefinger, and then ask
the patient to protrude their tongue. If the cyst is
fixed to the hyoid bone, you will feel it tugged
upwards as the tongue goes out. This is a difficult
sign to elicit.
Do not expect to see much movement. It is easier
to feel the tugging sensation than to actually see the
movement. Although this test is diagnostic of
attachment to the hyoid cartilage, the absence of
movement does not exclude the diagnosis. Indeed,
this sign is absent from most cysts that are below the
level of the thyroid cartilage.
Lymph glands
The local lymph glands should not be
enlarged unless there is secondary infection of
the cyst.
Local tissues
Whenever there is an abnormality of
thyroid gland development, examine the base of
the tongue for ectopic (lingual) thyroid tissue.
A lingual thyroid looks like a flattened strawberry
sitting on the base of the tongue.
THE THYROID GLAND
FIG 11.31
An infected thyroglossal cyst.
SYMPTOMS OF THYROID DISEASE
The thyroid gland can cause two groups of symp-
toms and signs: those connected with the swelling
in the neck, and those related to the endocrine activ-
ity of the gland. Therefore, in order to appreciate
fully the symptoms and signs that may be produced
by diseases of the thyroid, a clear understanding
of the physiology of the gland is essential. The his-
tory and examination should be directed towards
detecting both local and general symptoms and
signs that may be produced, either by any physical
abnormality in the configuration of the thyroid or by
any pathophysiological abnormality of its endocrine
activity.
Neck symptoms
A lump in the neck
The majority of thyroid swellings grow slowly and
painlessly. Quite often the patient will come across a
swelling coincidentally when washing, or a member
of their family or a close friend will point it out to
them. Other swellings may have been there for some
years before the patient suddenly decides to seek
advice concerning their nature and management. In a
few patients, a lump will appear suddenly and may be
painful, or a long-standing lump may enlarge quickly.
A rapid change in the size of part of the gland, or
of an existing lump, may be caused by haemorrhage
into a necrotic nodule, a fast-growing carcinoma,
Chap-11.qxd 12/11/07 9:50 AM Page 288
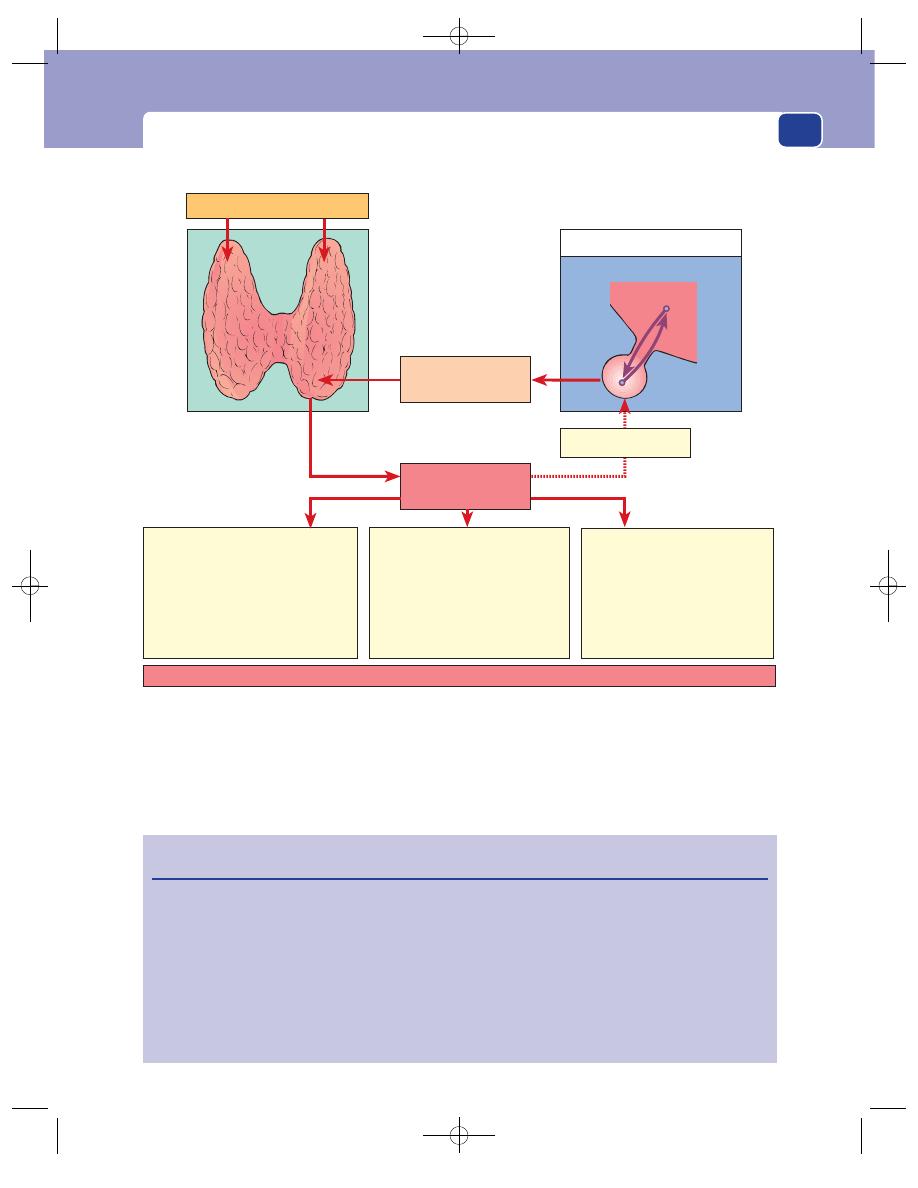
Symptoms of thyroid disease
289
or subacute thyroiditis. The sudden enlargement of
a lump caused by haemorrhage is usually painful,
whereas a fast-growing anaplastic carcinoma is not
usually painful until it invades nearby structures.
A special feature of papillary and follicular carci-
nomata of the thyroid gland is their very slow
growth. They may exist as a lump in the neck for
many years before metastasizing. Thus the length of
The active thyroid hormones are thyroxine (tetra-iodothyronine,T4) and probably tri-iodothyronine (T3)
1 Increase tissue metabolism
(by affecting the respiratory
enzymes in mitochondria)
2 Increase sensitivity of
β-adrenergic receptors
Tachycardia
Lid lag
Tremor
Nervousness
3 Increase tissue growth
(by increasing metabolism
and secretion of growth
hormone)
Increased growth and
early tissue maturation
Active hormones
(T3 and T4)
Circulating iodine and tyrosine
Pituitary and hypothalamus
Thyroid-stimulating
hormone (TSH)
Inhibitory feedback
Increased appetite
Decreased weight
Increased heat production
and oxygen consumption
PHYSIOLOGY OF THE THYROID GLAND.
FIG 11.32
Revision panel 11.4
Physiology of the thyroid gland
Changes in hormone activity can be assessed by:
Hormone secretion can be suppressed by:
■
clinical examination
■
iodine, which inhibits hormone release
■
measuring circulating tri-iodothyronine
■
potassium perchlorate, which interferes
(T3) and thyroxine (T4)
with iodine trapping
■
measuring the rate and quantity of
■
carbimazole and thiouracil, which inhibit
radioactive iodine taken up by the gland.
the iodination of tyrosine and the coupling of
tyrosines to make thyronines
■
destroying the gland surgically or with
radiotherapy.
Chap-11.qxd 12/11/07 9:50 AM Page 289
The neck
290
time that a lump has been present is no indication
as to its underlying nature.
Discomfort during swallowing
Large swellings may give the patient a tugging sen-
sation in the neck when they swallow. This is not
true dysphagia. Thyroid swellings rarely obstruct the
oesophagus because the oesophagus is a muscular
tube that is easily stretched and pushed aside. How-
ever, because the thyroid has to be pulled upwards
with the trachea in the first stage of deglutition, an
enlarged gland can make swallowing uncomfortable,
or even difficult.
Dyspnoea
Deviation or compression of the trachea by a mass
in the thyroid may cause difficulty in breathing.
This symptom is often worse when the neck is
flexed laterally or forwards and when the patient lies
down. The whistling sound of air rushing through a
narrowed trachea is called stridor.
Pain
Pain is not a common feature of thyroid swellings.
Acute and subacute thyroiditis can present with a
painful gland, and Hashimoto’s disease often causes
an uncomfortable ache in the neck.
Anaplastic carcinoma can cause local pain and
pain referred to the ear if it infiltrates surrounding
structures.
Hoarseness
A change in the quality of the voice of a patient with
a lump in the neck is a very significant symptom
because it is probably caused by a paralysis of one
of the recurrent laryngeal nerves, which means that
the lump is likely to be malignant and infiltrating
the nerve.
Symptoms and signs of endocrine
dysfunction
Every patient with any thyroid disorder should be a
carefully questioned and examined for any symp-
toms or signs of endocrine dysfunction.
Symptoms and signs of thyrotoxicosis
(see also pages 299–301)
Nervous system
Symptoms include nervousness,
irritability, insomnia and nervous instability, and
examination may reveal a tremor of the hands.
Occasionally a full-blown thyrotoxic psychosis may
be apparent.
Cardiovascular system
Symptoms include palpita-
tions, breathlessness on exertion, swelling of the
ankles and chest pain, which may be manifest as
tachycardia, auricular fibrillation dyspnoea and
peripheral swelling.
Metabolic and alimentary systems
There is an increase
in appetite but loss of weight, and sometimes a
change of bowel habit, usually diarrhoea. Proximal
muscle myopathies may occur with wasting and
weakness. The patient has a preference for cold
weather, and often complains of excessive sweating
and an intolerance of hot weather. Some women have
a change of menstruation, usually amenorrhoea.
Symptoms and signs of myxoedema
(see also pages 301–3)
There is an increase of weight, with deposition of
fat across the back of the neck and shoulders.
Symptoms also include: slow thought, speech and
action; intolerance of cold weather; loss of hair,
especially the outer third of the eyebrows; muscle
fatigue; a dry skin and ‘peaches and cream’ com-
plexion; and constipation.
EXAMINATION OF THE THYROID GLAND
Although this should be part of the general exami-
nation, the method of examining the neck is
described in detail because it is so important. The
important features of the general and eye examination
are also reiterated.
Concentrate upon both the nature of any gland
enlargement or abnormal configuration, as well as
any change in endocrine activity. It is best to assess
both aspects in a combined approach, rather than
try to assess each separately.
Look at the whole patient
First confirm that the swelling in the neck is in the thy-
roid gland by watching to see if it moves when the
patient swallows. Then look at the whole patient.
Are they sitting still and composed, or fidgeting
about, constantly moving their fingers and looking
nervous and agitated, or are they slow and ponderous
in their movements?
Chap-11.qxd 12/11/07 9:50 AM Page 290

FIG 11.33
EXAMINA
TION
OF THE THYROID
GLAND.
Try to decide if there is:
one lump
two lumps
diffuse enlargement
Look a
t the
eyes and the
neck and ask
the pa
tient to
swallo
w
.
P
alpa
te both lobes
and the isthmus with
the fingers fla
t.
Listen over the gland
for a systolic bruit.
Feel the trachea.
If one lobe is
difficult to feel,
make it more
prominent by
pressing firmly
on the opposite
side.
P
alpa
te the neck from
behind,
with the
thumbs pushing the
head forwards to flex
the neck slightly
.
P
ercuss the lo
wer limit
of the gland.
Chap-11.qxd 12/11/07 9:50 AM Page 291
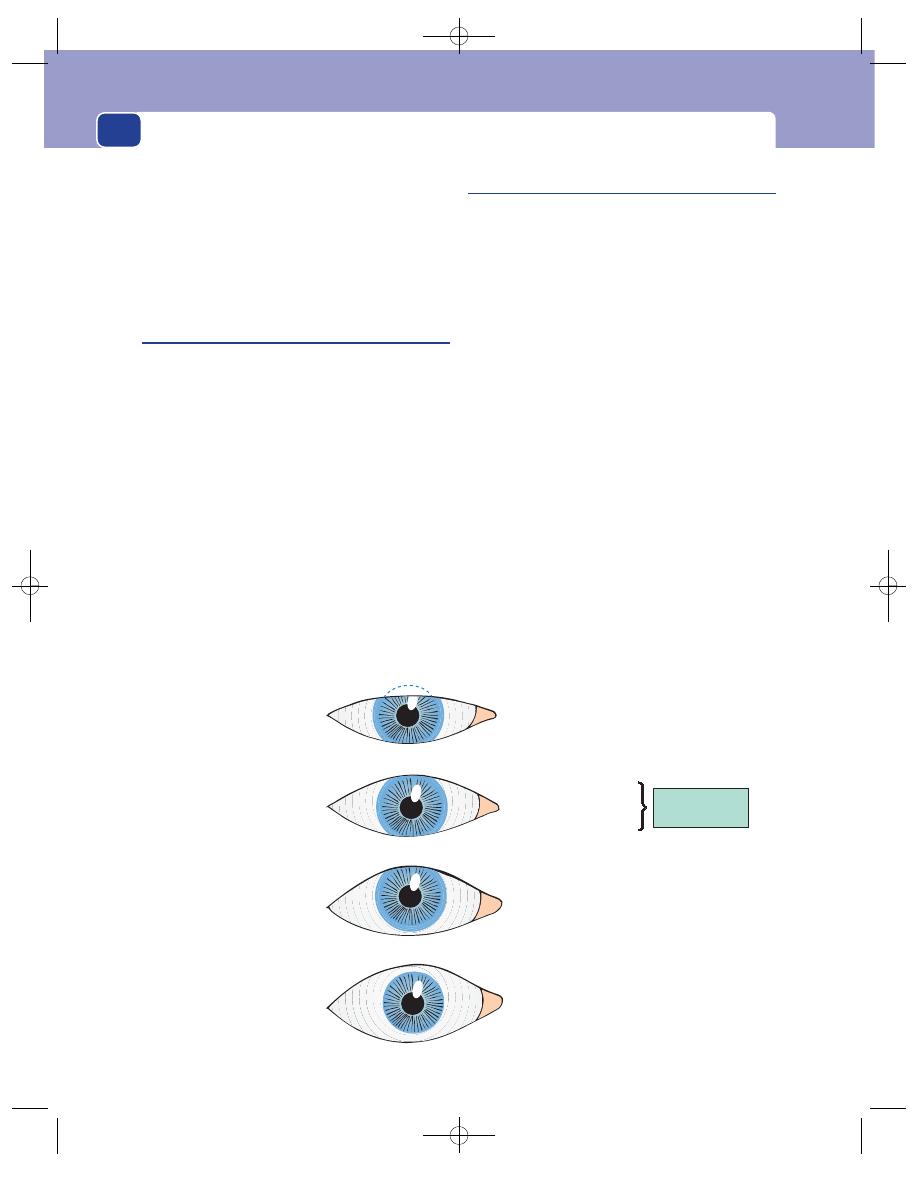
The neck
292
Lid retraction
Exophthalmos
Upper lid halfway between pupil
and superior limbus
Lower lid at a tangent to inferior limbus
Upper lid raised
Lower lid normal
Both lids moved away from centre with
sclera visible below or all round the iris
N.B. This is not
exophthalmos
Normal
FIG 11.34
The relations of the eyelids to the iris.
Are they thin or fat? Where is the wasting or the
fattening? Patients with thyrotoxicosis have a gener-
alized loss of weight, especially about the face, but
may also have localized wasting of their hands, face
and shoulder muscles.
Are they under-clothed and sweaty, or wrapped
up in a large number of jumpers but still cold?
Look at the hands
■
Feel the pulse Tachycardia suggests
thyrotoxicosis; bradycardia suggests
myxoedema. In middle-aged and elderly
patients thyrotoxicosis may cause atrial
fibrillation.
■
Are the palms moist and sweaty?
■
Is there a tremor? Test for a tremor by
asking the patient to hold their arms out in
front of them, elbows and wrists straight,
fingers straight and separated. Thyrotoxicosis
causes a fine, fast tremor. If in doubt, hold
out your own hand beside the patient’s
for comparison. A fine tremor may be
accentuated by placing a sheet of paper
over the fingers.
Examine the eyes
Eye symptoms
Patients who suffer from thyrotoxicosis may com-
plain of staring or protruding eyes and difficulty
closing their eyelids (exophthalmos), double vision
caused by muscle weakness (ophthalmoplegia) and
swelling of the conjunctiva (chemosis). They may
get pain in the eye if the cornea ulcerates.
There are four important underlying changes
that can occur in the eyes of patients with hyper-
thyroidism that produce the above effects (Figs 11.34
and 11.35). Each one may be unilateral or bilateral.
Lid retraction and lid lag
This sign is caused by over-activity of the involun-
tary (smooth muscle) part of the levator palpebrae
superioris muscle. If the upper eyelid is higher than
normal and the lower lid is in its correct position,
the patient has lid retraction. Do not be deceived
into thinking this abnormality is caused by exoph-
thalmos.
When the upper lid does not keep pace with the
eyeball as it follows a finger moving from above
downwards, the patient has lid lag.
Chap-11.qxd 12/11/07 9:50 AM Page 292
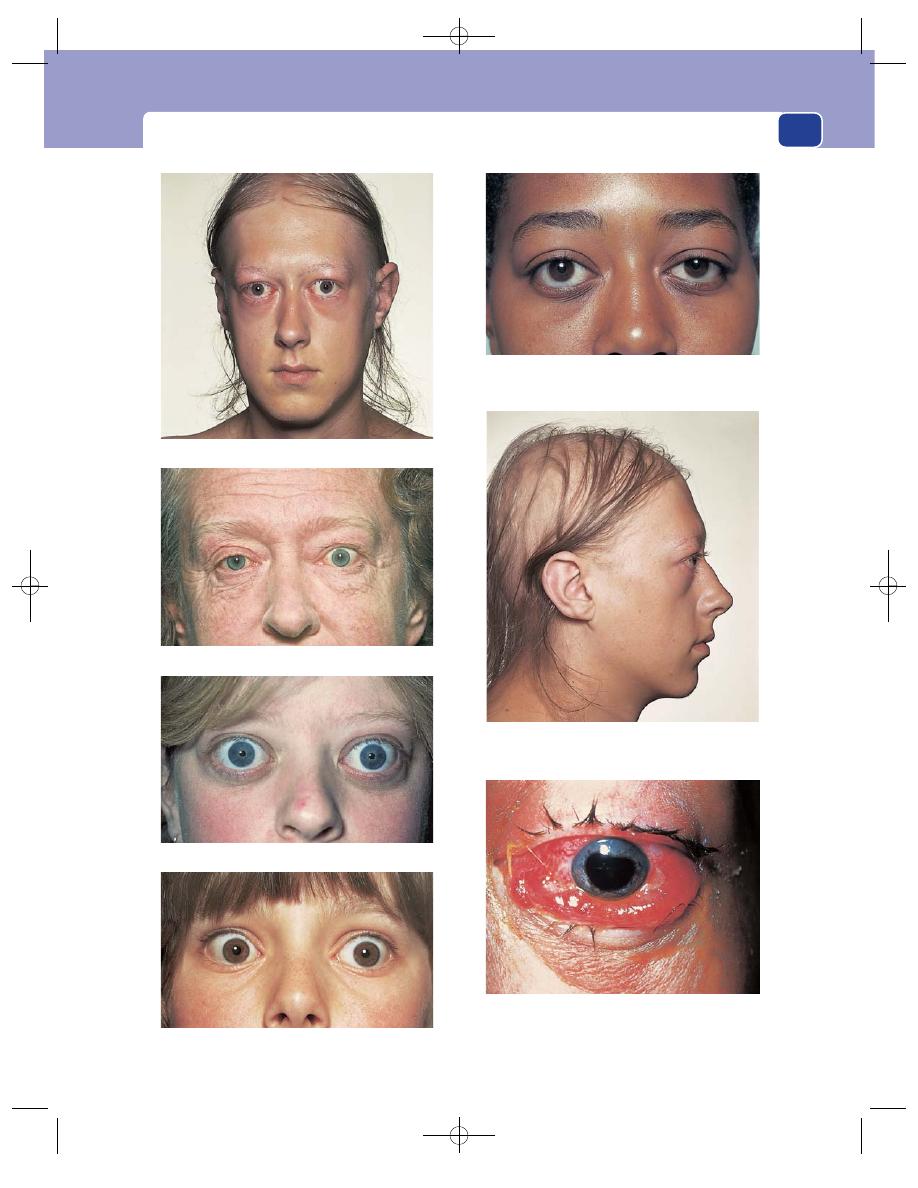
Examination of the thyroid gland
293
Exophthalmos.
Wasting and loss of hair (and exophthalmos).
Severe lid retraction but no exophthalmos.
Exophthalmos but no lid retraction.
Unilateral lid retraction.
Exophthalmos and lid retraction.
Chemosis. The conjunctiva is hyperaemic and bulging
over the eyelid. There is exophthalmos, lid retraction
and peri-orbital oedema.
FIG 11.35
SOME EYE SIGNS ASSOCIATED WITH THYROTOXICOSIS.
Chap-11.qxd 12/11/07 9:50 AM Page 293
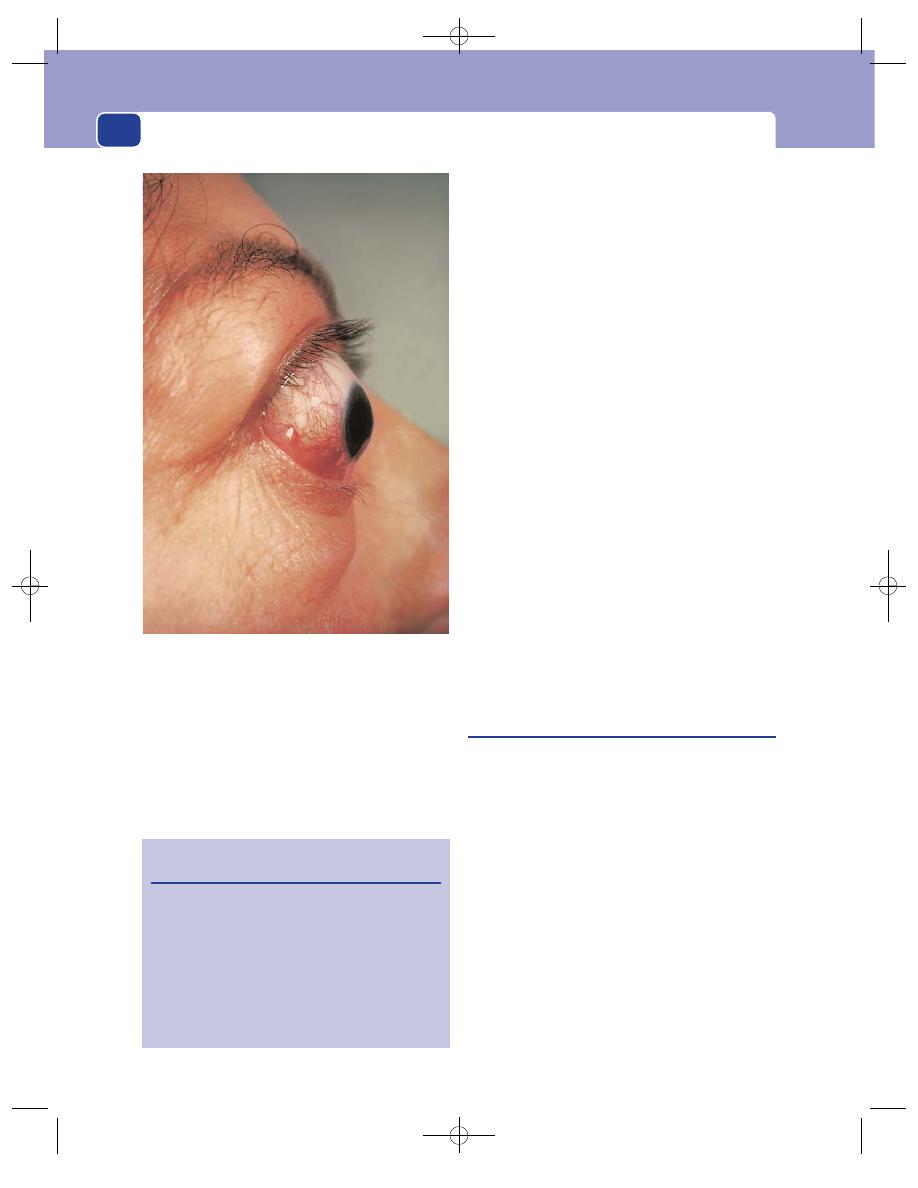
The neck
294
Exophthalmos
If the eyeball is pushed forwards by an increase in
retro-orbital fat, oedema and cellular infiltration,
the normal relationship of the eyelids to the iris is
changed. Sclera becomes visible below the lower
edge of the iris (the inferior limbus).
Because the eyes are pushed forwards, the patient
can look up without wrinkling the forehead, but
will have difficulty converging. In severe exoph-
thalmos the patient cannot close their eyelids and
may develop corneal ulceration.
Ophthalmoplegia
Although exophthalmos stretches the eye muscles, it
does not usually affect their function. The cause of
the weakness of the ocular muscles (ophthalmople-
gia) associated with severe exophthalmos is oedema
and cellular infiltration of the muscles themselves
and of the oculomotor nerves. The muscles most
often affected are the superior and lateral rectus
and inferior oblique muscles. Paralysis of these
muscles prevents the patient looking upwards and
outwards.
Chemosis
Chemosis is oedema of the conjunctiva. The normal
conjunctiva is smooth and invisible. A thickened,
crinkled, oedematous and slightly opaque conjunc-
tiva is easy to recognize.
Chemosis is caused by the obstruction of normal
venous and lymphatic drainage of the conjunctiva
by the increased retro-orbital pressure.
Inspect the neck
After checking that the lump is in the anatomical site
of the thyroid gland, ask the patient to swallow. The
patient may need a sip of water to help deglutition.
All thyroid swellings ascend during swallowing.
Observe the general contours and surface of the
swelling. The skin may also be puckered and pulled
up by swallowing if the patient has a thyroid carci-
noma which has infiltrated into the skin, although
this is uncommon.
Ask the patient to open their mouth and then to
put out their tongue. If the lump moves up as the
tongue comes out, it must be attached to the hyoid
bone, and is likely to be a thyroglossal cyst.
The neck veins will be distended if there is a mass
obstructing the thoracic inlet.
Look at the position of the thyroid cartilage. Is it
in the centre of the neck or deviated to one side?
FIG 11.35
continued
Revision panel 11.5
The eye signs of thyrotoxicosis
Lid retraction and lid lag
Exophthalmos, which also causes difficulty with
convergence and absent forehead wrinkling
when looking upwards
Ophthalmoplegia, particularly of the superior
rectus and inferior oblique muscles (cannot
look ‘up and out’)
Chemosis
This patient had gross chemosis and exophthalmos but the
eye was pulsating. The cause of these abnormalities was a
carotid artery–cavernous sinus fistula.
Chap-11.qxd 12/11/07 9:50 AM Page 294
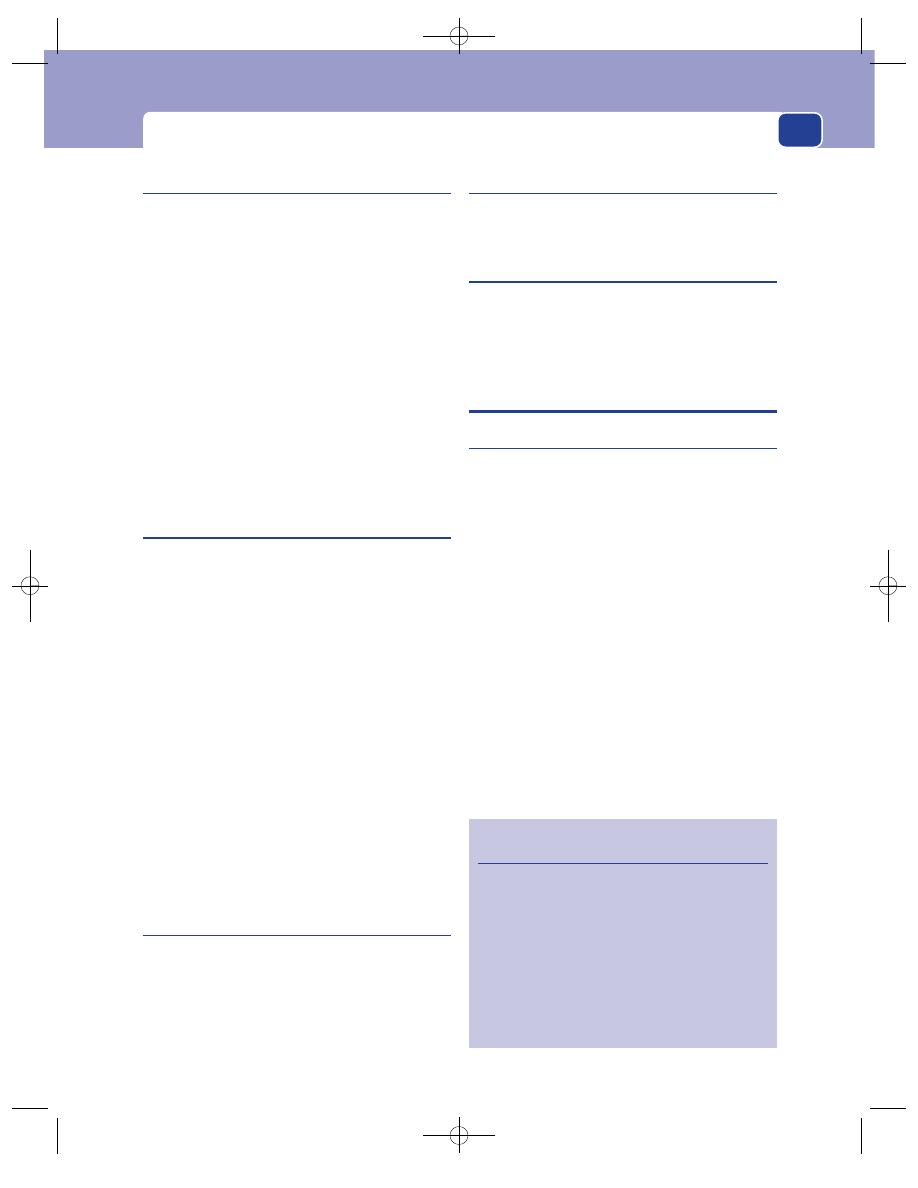
Different forms of goitre
295
Palpate the neck from the front
The most important part of palpation is done from
behind (see below), but it is worthwhile placing your
hand on any visible swelling while standing in front
of the patient, to confirm your visual impression of
its size, shape and surface, and to find out if it is
tender. It is sometimes helpful to measure and record
the circumference of the neck with a tape measure.
Check the position of the trachea. This is best
done by feeling with the tip of two fingers in the
suprasternal notch. The trachea should be exactly
central at this point. When a thyroid mass extends
below the suprasternal notch and obscures the
trachea, you must examine the thyroid cartilage. A
mass that is displacing the trachea will tilt the thy-
roid cartilage laterally.
Palpate the neck from behind the
patient
Stand behind the patient. Place your thumbs on the
ligamentum nuchae and tilt the patient’s head
slightly forwards to relax the anterior neck muscles.
Let the palmar surface of your fingers rest on each
side of the neck. They will be resting on the lateral
lobes of the thyroid gland. A small lobe can be made
prominent and easier to feel by pressing firmly on
the opposite side of the neck.
Ask the patient to swallow while you are palpat-
ing the gland to confirm that any swelling moves
with swallowing and is actually part of the thyroid.
This manoeuvre also lifts up lumps that are lying
behind the sternum into the reach of your fingers.
At the end of palpation you should know the fol-
lowing facts about the gland and/or the lump: ten-
derness, shape, size, surface and consistence.
A normal thyroid gland is not palpable.
Palpate the whole of the neck for any cervical
and supraclavicular lymphadenopathy.
Percussion
Percussion is used to define the lower extent of a
swelling that extends below the suprasternal notch
by percussing along the clavicles and over the sternum
and upper chest wall. This can be done when stand-
ing in front of or behind the patient. Percussion of
the lump in the neck itself is rarely helpful.
Auscultation
Listen over the swelling. Thyrotoxic and vascular
glands and lumps may have a systolic bruit.
General examination
Pay particular attention to the cardiovascular and
nervous systems for any evidence of hyperthy-
roidism or hypothyroidism, the signs and symp-
toms of which are described on pages 299–303.
DIFFERENT FORMS OF GOITRE
Simple hyperplastic goitre
Simple enlargement of the thyroid gland is invari-
ably caused by excess stimulation by thyroid-stimu-
lating hormone (TSH), the production of which is
stimulated by low levels of circulating thyroid hor-
mone. Relative iodine deficiency is the commonest
pathological cause for a low level of thyroid hor-
mone production. Physiological states that require
increased activity of the thyroid gland, such as
puberty and pregnancy, are also associated with
enlargement of the gland.
The term colloid goitre is used to describe the late
stage of diffuse hyperplasia, when all the acini are dis-
tended with colloid which has not been released
because the stimulation by TSH has dropped off.
History
Age
In areas where goitre is endemic (i.e. prevalent
in the local population), hyperplastic goitres appear
in childhood.
Revision panel 11.6
Plan for the examination of a patient with a goitre
Look at the whole patient for agitation,
nervousness or lethargy.
Examine the hands for sweating, tremor,
tachycardia.
Examine the eyes for exophthalmos, lid lag,
ophthalmoplegia, chemosis.
Examine the neck: always check that the lump
moves with swallowing.
Palpate the cervical lymph glands.
Chap-11.qxd 12/11/07 9:50 AM Page 295
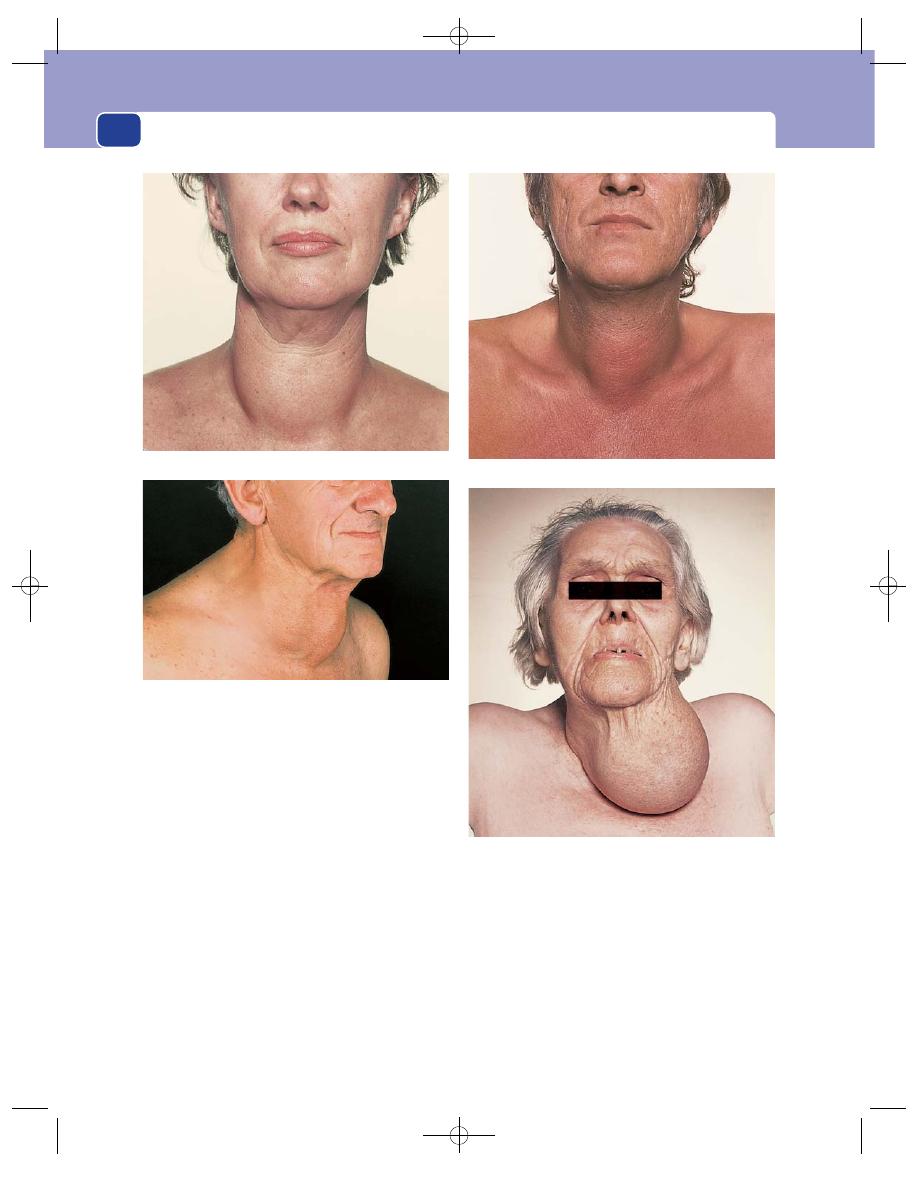
The neck
296
Sporadic physiological hyperplastic goitres appear
at puberty, during pregnancy, and during severe ill-
nesses and emotional disturbances, and so they are
commonly seen in puberty and young adult life.
Sex
Hyperplastic goitres are five times more common
in women than in men.
Geography
Endemic goitre is common in places where
the drinking water has a low iodine content, such as
the habitable valleys of the Alps, Andes, Himalayas and
Rocky Mountains, and the lowland areas that depend
upon water from mountain ranges, such as the Nile
Valley, Congo Delta and Great Lakes of the USA. The
rain that falls on the mountains has a normal iodine
content, but it is filtered out by the time it reaches the
springs and streams of the highland valleys.
Diet
Some vegetables contain chemicals which are
goitrogens (i.e. they interfere with hormone synthe-
sis). An excess dietary intake of the brassica family of
FIG 11.36
VARIOUS GOITRES.
A large colloid goitre. The patient was euthyroid.
A nodular goitre extending below the sternum and causing
venous obstruction. Distended veins are visible above the right
clavicle. The patient was euthyroid.
A large central solitary nodule.
Beware! Not all lumps in the neck are thyroid swellings. This
mass was soft and did not move with swallowing. It was a
lipoma. Never make a spot diagnosis. Examine every lump
carefully and thoroughly.
Chap-11.qxd 12/11/07 9:50 AM Page 296
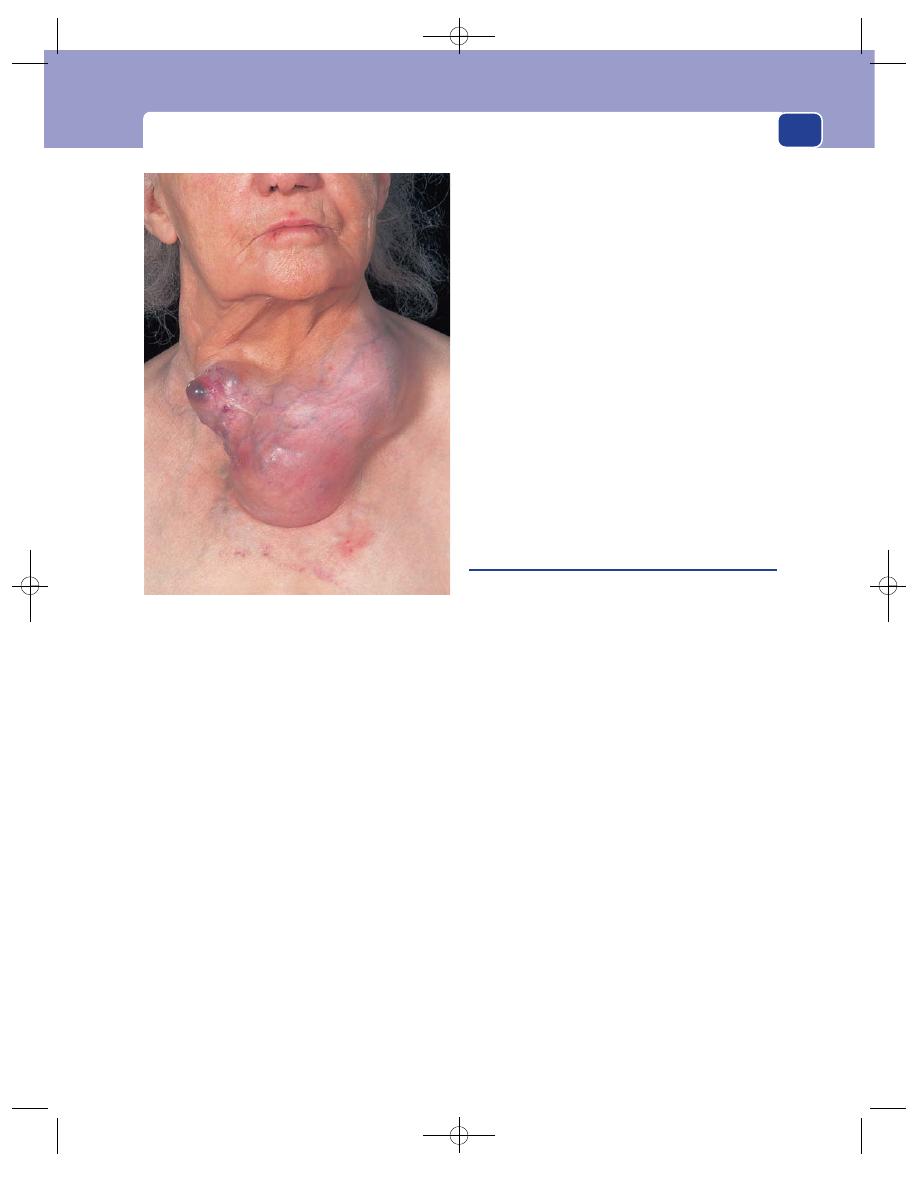
Different forms of goitre
297
foods (e.g. cabbage, sprouts and kale) can cause a
goitre.
Local symptoms
The principal complaint is of a
swelling in the neck. This appears slowly and with-
out pain.
If it becomes large – especially if it remains as a
colloid goitre after the initial stimulus has gone – it
can cause pressure symptoms such as dyspnoea,
venous engorgement and mild discomfort during
swallowing.
General symptoms
Diffuse hyperplastic goitres are not
usually associated with clinically significant hyper-
function or hypofunction of the gland.
Long-standing colloid goitres often become nodu-
lar goitres and occasionally secondary thyrotoxicosis
(Plummer’s syndrome) or myxoedema may develop.
Examination
Position
The swelling occupies the anatomical site of
the thyroid gland.
Tenderness
It is not tender.
Shape
The swelling usually follows the configuration
of the gland and can be seen to have two lobes and
an isthmus.
Size
Physiological goitres are only two or three times
larger than a normal gland, but iodine-deficiency
goitres can become very large.
Surface
The surface of a hyperplastic goitre is
smooth. If it turns into a colloid goitre, its surface
becomes bosselated and, in time, nodular.
Composition
The gland feels firm and is dull to per-
cussion. Hyperaemic physiological goitres may have
a very soft systolic bruit.
Relations
The gland moves upon swallowing. The
other tissues in the neck should be normal.
Lymph glands
The deep cervical lymph glands should
not be palpable.
The eyes
The eyes should be normal.
General examination
The patient is usually euthyroid.
Multinodular goitre
Multinodular goitres develop spontaneously and
in glands subjected to prolonged stimulation (i.e.
hyperplastic glands). They can therefore be endemic
(in iodine-deficient areas) or sporadic (occurring
haphazardly).
A nodular goitre results from a disorganized res-
ponse of the gland to stimulation, and contains areas
of hyperplasia and hypoplasia, side by side.
The cut surface of a nodular goitre reveals nodules
with haemorrhagic, necrotic centres, separated by
normal tissue. The normal tissue contains normally
active follicles; the nodules contain both hyper-
active and degenerate, involuting, follicles.
When the nodules are hyperplastic the patient
may develop secondary thyrotoxicosis.
In long-standing nodular goitres, most of the nod-
ules are inactive and the quantity of normally active
follicles may be so reduced that thyroid hormone
production is inadequate and myxoedema develops.
History
Age
In endemic areas, nodular goitres appear in early
adult life (15–30 years). Sporadic nodular goitres
appear later, between the ages of 25 and 40 years.
Sex
Nodular goitres are six times more common in
women than in men.
FIG 11.37
A large goitre causing skin changes and imminent
ulceration.
Chap-11.qxd 12/11/07 9:50 AM Page 297
The neck
298
Geography
These goitres are common in areas where
the drinking water is deficient in iodine (see hyper-
plastic goitre).
Symptoms
The commonest presenting symptom is
an enlarging, painless swelling in the neck, which
may cause dyspnoea, discomfort when swallow-
ing, stridor and engorged neck veins.
Sudden enlargement and pain can occur if there
is haemorrhage into a necrotic nodule. Necrotic
nodules are not cysts, and it is wrong to call this
event a haemorrhage into a cyst.
Thyrotoxicosis occurs in a significant proportion
(maybe as high as 25 per cent) of patients with long-
standing nodular goitres. The symptoms of thyro-
toxicosis are listed on pages 299–300.
Myxoedema: as the follicular hyperplasia and its
stimulation subside, the patient is left with a devas-
tated gland that has little normal tissue. Ultimately, its
endocrine secretions are inadequate and the patient
has a considerable chance of becoming myxoede-
matous by the time they reach 60 or 70 years of age.
The symptoms of myxoedema are described on
pages 301–2.
Examination
Position
The swelling is in the lower third of the
neck in the anatomical site of the thyroid gland and
is usually asymmetrical.
Tenderness
A nodular goitre is only tender when
there has been a recent haemorrhage into a nodule.
Shape and size
The nodules are asymmetrical and
the gland can become any shape. Nodules in the
isthmus are prominent. The nodules may extend
below the clavicles and the sternal notch, into the
superior mediastinum.
Surface
The surface of a nodular goitre is smooth
but nodular. Frequently, only one nodule may be
palpable, even though the rest of the gland is
grossly diseased. This is termed a ‘dominant nodule’
and malignancy must be excluded.
Composition
The consistence of the nodules varies:
some feel hard, others feel soft. There is an old saying
that ‘Solid lumps in the thyroid feel cystic, whereas
cystic lumps feel solid’. The explanation is that a
nodule composed of thyroid tissue is soft, whereas a
nodule full of blood and liquefied necrotic tissue
becomes tense and feels hard.
The nodules of a nodular goitre do not fluctuate,
or transilluminate, and are dull to percussion.
There should be no bruit over the gland.
Relations
The lump will move upwards during swal-
lowing, indicating that it is fixed to the trachea. It
should not be fixed to any other nearby structures.
Lymph drainage
The cervical lymph glands should
not be palpable.
State of local tissues
The trachea may be compressed
and/or deviated, depending on the site of the nod-
ules. Bilateral nodules will compress the trachea
into a narrow slit, causing dyspnoea and stridor –
especially during lateral flexion of the neck. Large
unilateral nodules will push the trachea laterally.
When the trachea is pushed to one side, the ‘keel’
of the larynx is tilted away from the mid-line.
If the gland is jammed in the thoracic inlet, it
may obstruct and distend the jugular veins.
Rarely, the goitre is so large that it starts to cause
pressure on the overlying skin, and on occasions
may even start to ulcerate through.
The eyes
The eyes should be normal. It is unusual to
get neurological or eye changes with secondary thyro-
toxicosis associated with a nodular goitre. These sys-
tems are affected more often in primary thyrotoxicosis.
General examination
There may be the general signs
of thyrotoxicosis – especially the cardiovascular
signs or, in elderly patients with very long-standing
nodular goitres, the signs of myxoedema.
The solitary nodule
Although only one nodule may be palpable, approx-
imately one-half of the patients who present with
a solitary nodule actually have a multinodular
goitre, i.e. a clinically dominant nodule in a macro-
scopical multinodular goitre.
Revision panel 11.7
Causes of a ‘solitary’ nodule in the thyroid gland
A dominant nodule in a multinodular goitre
Haemorrhage into a nodule
Adenoma
Carcinoma (papillary or follicular)
Enlargement of the whole of one lobe (usually
Hashimoto’s disease)
Chap-11.qxd 12/11/07 9:50 AM Page 298
Thyrotoxicosis and myxoedema
299
It is unusual to be able to determine the pathology
of a solitary nodule by clinical examination. Thus,
although the majority of solitary nodules are benign,
they must all be investigated, as many well-differen-
tiated carcinomata of the thyroid present as solitary
nodules. Fine-needle aspiration (FNA) to determine
the cytology of the nodule has become part of the
routine of clinical examination in many clinics.
Thyrotoxicosis caused by a solitary toxic/auto-
nomous adenoma is uncommon and is never (well,
hardly ever) caused by a solitary malignant nodule.
The causes of a solitary nodule in the thyroid
gland are:
■
dominant nodule in a multinodular goitre,
■
haemorrhage into, or necrosis of, a hyperplastic
nodule,
■
adenoma,
■
carcinoma (papillary or follicular),
■
enlargement of the whole of one lobe by
thyroiditis.
THYROTOXICOSIS AND MYXOEDEMA
(Hyperthyroidism and hypothyroidism)
Thyrotoxicosis
Thyrotoxicosis is caused by an excess of circulating
thyroid hormone. The gland may be diffusely hyper-
plastic (Graves’ thyroiditis), nodular, or the site of
disease such as thyroiditis or an adenoma, but rarely
a carcinoma.
The terms ‘primary’ and ‘secondary’ are used to
describe thyrotoxicosis arising in a previously normal
or previously abnormal gland, respectively. They can
be confusing terms, but usually primary thyrotoxi-
cosis (Graves’ disease) is caused by a form of autoim-
mune thyroiditis, whereas secondary thyrotoxicosis
(Plummer’s syndrome) usually occurs in a long-
standing multinodular goitre.
The thyroid hormones tri-iodothyronine (T3)
and thyroxine (T4) have three effects.
1. They increase the metabolic rate of all cells.
2. They increase the sensitivity of beta-adrenergic
receptors.
3. They stimulate all cells to grow, but the effect on
growth is only significant before natural growth
has finished.
The increased tissue metabolism causes an
increased appetite, a decrease in weight and an
increased heat production.
The increased adrenergic receptor sensitivity
causes tachycardia, extrasystoles, atrial fibrillation,
tremor and nervousness, and lid retraction and lid lag.
Stimulation of growth during childhood pro-
duces early maturation and a slight increase in the
rate of growth.
In myxoedema (hypothyroidism), all of these
symptoms are reversed. The lack of growth stimula-
tion in a child causes dwarfism.
History
Age
Primary thyrotoxicosis occurs most often in
young women, between 15 and 45 years of age.
Toxic autonomous nodules can occur at any age.
Secondary thyrotoxicosis (from a nodular goitre)
occurs in middle age – between 45 and 65 years.
Sex
Primary thyrotoxicosis is ten times more com-
mon in women than in men.
Geography
Secondary thyrotoxicosis is more com-
mon in those areas where simple hyperplastic goitre
(and nodular goiter) is endemic.
Metabolic symptoms
The patient complains of a rav-
enous appetite, but in spite of eating excessively,
tends to lose weight. Patients may also find that
they always feel warm, and therefore like cold
weather and dislike hot weather. There may be
excessive sweating.
Cardiovascular symptoms
The patient complains of pal-
pitations, shortness of breath during exertion,
missed and irregular heart beats (extrasystoles and
atrial fibrillation) and tiredness. Cardiovascular sym-
ptoms are often the presenting symptoms of second-
ary thyrotoxicosis, whereas atrial fibrillation may be
the only sign of thyrotoxicosis in an elderly patient.
Neurological symptoms
Symptoms such as nervousness,
irritability, insomnia, depression and excitement,
even mania and melancholia, may be noticed by close
relatives long before the patient is aware of them.
There may be hyperaesthesia, headaches, vertigo
and tremors of the hands and tongue.
The patient may complain that their eyes have
become more protuberant and that some eye move-
ments are difficult.
Chap-11.qxd 12/11/07 9:50 AM Page 299
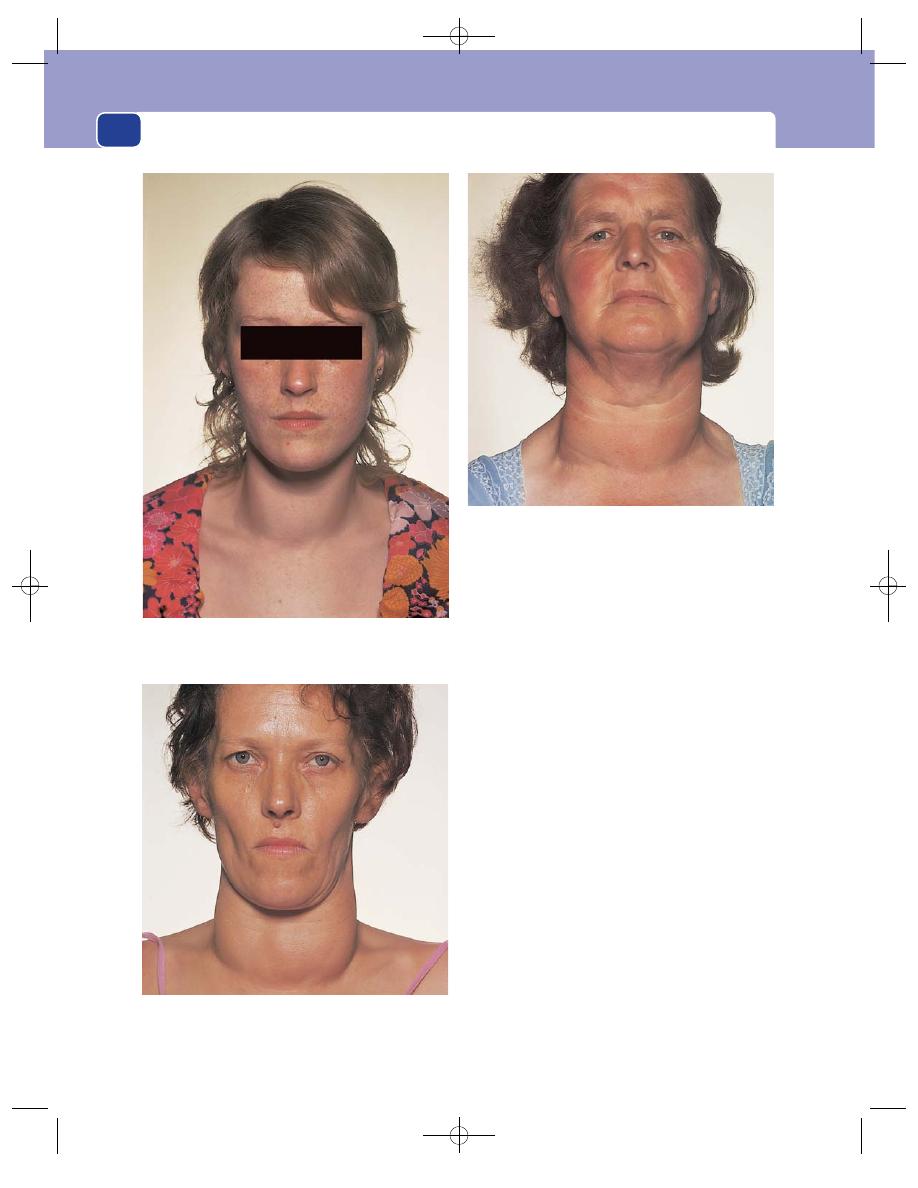
The neck
300
Alimentary symptoms
The changes in appetite and
weight have been mentioned under metabolic
symptoms. There is often a slight change in bowel
habit – usually mild diarrhoea.
Genital tract symptoms
Most women have a reduction in
the quantity of their menses; some have amenorrhoea.
Musculoskeletal symptoms
In addition to generalized
weight loss, there may be specific wasting and weak-
ness of the small muscles of the hand, shoulder
and face. These muscles rarely become completely
paralysed.
Cause
Patients with primary thyrotoxicosis may
relate the onset of their symptoms to puberty, preg-
nancy, an illness or a sudden emotional upset.
Although it is difficult to be certain that events of
this sort are the prime cause of hypersecretion of
the thyroid gland, they undoubtedly exacerbate any
hidden or developing abnormality. They are some-
times remembered as the three Ss – sex (puberty
and pregnancy), sepsis and psyche!
Examination
Signs in the neck
The thyroid gland is usually enlarged, but thyrotox-
icosis can be present without any enlargement of
the gland.
FIG 11.38
THE FACIES OF THYROTOXICOSIS.
A large goitre, increasing appetite but weight loss –
particularly of the face and shoulder girdle – no eye signs.
A small goitre, nervousness and agitation, beginning to lose
weight, left lid retraction and very early exophthalmos (sclera
visible below right inferior limbus).
A nodular goitre. No eye or nervous system signs, but
palpitations, breathlessness and atrial fibrillation.
Chap-11.qxd 12/11/07 9:50 AM Page 300
Thyrotoxicosis and myxoedema
301
The enlargement may be diffuse, nodular or ten-
der, depending on the local pathology.
A diffusely enlarged hyperaemic gland usually
has a systolic bruit audible over its lateral lobes.
Signs in the eye
Thyrotoxicosis is associated with four groups of
physical signs in the eyes.
LID RETRACTION AND LID LAG
These are common signs. In lid retraction the upper
eyelid crosses the eye above its usual level (mid-way
between the pupil and the superior limbus of the
iris) because the autonomic part of the levator
palpebrae superioris muscle is hypertonic.
Ask the patient to follow your finger as you move
it slowly from above downwards. If the upper eyelid
does not keep pace with the eye, the patient has lid
lag. This is also caused by the increased tone of the
levator palpebrae superioris muscle.
The patient may blink less frequently than normal.
EXOPHTHALMOS
Oedema of the retro-orbital tissues pushes the
eye forwards. The first abnormality is the appear-
ance of sclera below the inferior limbus, but when
the condition is extreme, the eye appears to be pop-
ping out and the eyelids cannot be completely
closed.
Exophthalmos makes convergence difficult and
allows the patient to look up without raising their
eyebrows or wrinkling their forehead. Corneal ulcer-
ation may complicate severe exophthalmos.
OPHTHALMOPLEGIA
Infiltration of the ocular muscles weakens the eye
muscles and diminishes the eye movements. The
muscles most often affected are the superior rectus
and inferior oblique muscles. As these muscles
normally turn the eye upwards and outwards, this is
the first movement to become weak.
CHEMOSIS
This is oedema of the conjunctiva. The conjunctiva
becomes thick, boggy and crinkled and may bulge
over the eyelids. The eyes water excessively.
General signs
These are best described in bodily systems.
METABOLIC SIGNS
The patient looks thin and their face and hands may
be particularly wasted. They may look hot and be
sweating, even in a cold room.
CARDIOVASCULAR SIGNS
There is usually a tachycardia of 90 beats/minute or
more at rest, which persists during sleep.
If there are extrasystoles or atrial fibrillation,
the pulse will be irregular.
If there is mild heart failure, there may be râles at
the bases of the lungs and oedema of the ankles.
NEUROLOGICAL SIGNS
The patient looks worried and nervous and moves
about in an agitated, jerky way. They will often twist
and twine a handkerchief between their fingers.
A fine tremor may be demonstrated when they
stretch out their hands with their fingers spread. A
similar tremor may be present in the protruded
tongue.
MUSCULOSKELETAL SIGNS
The muscles of the hands, shoulders and face may
be wasted and weak and the finger tips enlarged.
SKIN
In certain patients with Graves’ disease, red, blotchy,
raised areas may be seen over the shins. This is termed
pretibial myxoedema and is caused by deposits of
myxoid tissue within the skin.
Myxoedema
History
Myxoedema is the clinical state which follows a
severe lack of thyroid hormone (hypothyroidism).
The term means ‘mucous swelling’ and is used
because when it was first described it was believed
that the increase in weight and body swelling was
caused by a new form of oedema.
Age
Myxoedema tends to occur in middle and old age.
Sex
It is more common in women than in men.
Metabolic symptoms
The patient complains of tired-
ness and weakness, which become intense physical
and mental lethargy.
The patient always feels cold, and therefore likes
hot weather and dislikes cold weather. They gain
weight but have a poor appetite.
Chap-11.qxd 12/11/07 9:50 AM Page 301
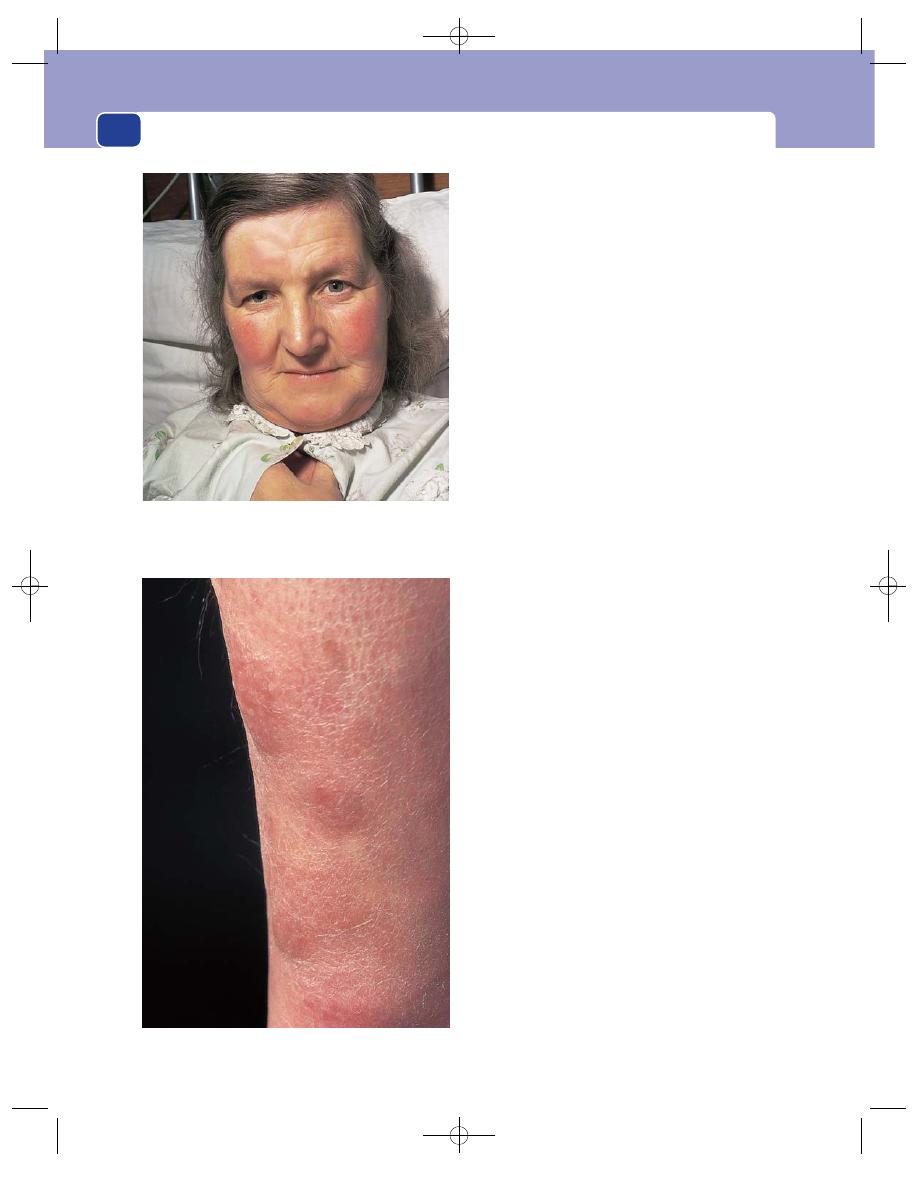
The neck
302
Cardiovascular symptoms
Breathlessness and ankle
swelling indicate the onset of cardiac failure.
Neurological symptoms
The patient finds it difficult to
think and to speak quickly and clearly. Hallucinations,
dementia (‘myxoedema madness’) and, in severe
cases, ‘myxoedema coma’ can occur.
Alimentary symptoms
Progressive and obdurate consti-
pation is common.
Genital tract symptoms
Menorrhagia is common when
myxoedema occurs before the menopause.
Examination
Signs in the neck
The thyroid gland may be enlarged by long-stand-
ing disease such as a nodular goitre, but in many
cases the neck is normal.
Signs in the eyes
The eyes are normal but the eyelids become swollen
and heavy, making the patient look sleepy and
lethargic.
The hair of the outer third of the eyebrows falls out.
General signs
General appearance and metabolic signs
The complex-
ion of a white-skinned patient with myxoedema is
said to resemble peaches and cream. The skin is
smooth and has a pale-yellow (the cream) colour.
The cheeks are often slightly flushed and have a
pink-orange tinge (the peaches).
The skin is dry and inelastic and does not sweat.
Although it may look oedematous, it does not pit
after prolonged pressure.
The patient is overweight, with excess connective
tissue and fat in the supraclavicular fossae, across
the back of the neck and over the shoulders.
The hair looks thin and ragged and falls out.
The hands are puffy and spade-like.
The tongue enlarges and seems to fill the mouth
during speech and interfere with the articulation of
words. The voice becomes deep and hoarse.
Cardiovascular signs
The pulse rate is slow (40–60 beats/
minute) and the blood pressure is low. Both these
changes may be reversed if heart failure develops.
The hands are cold and the finger tips blue.
FIG 11.40
Pretibial myxoedema.
FIG 11.39
The facies of myxoedema. Thinning of the hair, loss
of the outer third of the eyebrows, ‘peaches and cream’
complexion, thickening and heaviness of the eyelids.
Chap-11.qxd 12/11/07 9:50 AM Page 302
Carcinoma of the thyroid gland
303
Neurological signs
Mental alertness and the ability
to respond to questions and solve problems are
noticeably retarded. Conversation is also hampered
by the difficulty in articulation caused by enlargement
of the tongue.
All movements are slow and deliberate.
The reflexes are sluggish and their relaxation
period prolonged.
Cretinism
A cretin is a child whose mental and physical devel-
opment has been retarded by a lack of thyroid hor-
mone. Nowadays cretins are rare because the
hormone deficiency can be replaced.
Cretinism is likely to occur in those places where
goitre is endemic. The child may have a goitre.
The cretin has an underdeveloped skeleton (a
dwarf) and a large protruding tongue, the eyes are
wide apart, and the skull is also wide. The limbs and
neck are short and the hands spade-like.
The skin is dry and there are supraclavicular
pads of fat.
The abdomen is distended and protuberant and
there is often an umbilical hernia.
There is mental retardation, even imbecility.
When hypothyroidism occurs in older children,
they develop a mixture of the symptoms of cre-
tinism and myxoedema.
CARCINOMA OF THE THYROID
GLAND
The thyroid gland is a very vascular organ, and sec-
ondary tumour deposits from primary lesions in
the breast, stomach, colon and lung are often found
at autopsy. However, these secondary deposits rarely
become large and noticeable and rarely present
Revision panel 11.8
Correlation between clinical state of the thyroid gland, endocrine function and
pathological diagnosis
Hypothyroid
Euthyroid
Hyperthyroid
Diffuse enlargement
Thyroiditis
Iodine deficiency
Primary hyperthyroidism
Enzyme defects
(Graves’ disease)
Goitrogens
Thyroiditis
Amyloid
Physiological
(pregnancy, puberty)
Multinodular
Multinodular goitre
Multinodular goitre
Secondary
enlargement
with gross
Lymphoma
hyperthyroidism
degeneration
Anaplastic carcinoma
(Plummer’s syndrome)
Medullary carcinoma
Solitary nodule
Coincidental nodule
Cyst
Autonomous toxic
with myxoedema
Dominant nodule
nodule
Adenoma
Follicular or papillary
carcinoma
No palpable goitre
Thyroiditis
Normal gland
Primary hyperthyroidism
Primary myxoedema
Thyroxine overdose
Post-thyroidectomy or
post-radioactive iodine
Chap-11.qxd 12/11/07 9:50 AM Page 303
The neck
304
primarily as a thyroid swelling. The majority of the
neoplasms in the thyroid gland that present as a
lump in the neck are primary thyroid tumours.
There are three varieties of carcinoma of the thy-
roid follicles:
■
papillary carcinoma
■
follicular carcinoma
■
anaplastic carcinoma.
The parafollicular (C) cells can also undergo
malignant change, and this cancer is called:
■
medullary carcinoma.
The lymphoid tissue in the gland can also undergo
malignant change to become a lymphoma, but this
is not a true thyroid tissue neoplasm. Lymphoma is
more common in patients with Hashimoto’s disease.
Papillary carcinoma
This tumour contains a few formed follicles, but its
bulk consists of hyperplastic follicular epithelium
with a papilliferous configuration which sometimes
produces a small quantity of colloid. This tumour
spreads in the lymphatics. The cervical lymph
glands may be palpable long before the primary
lesion in the thyroid gland becomes palpable.
History
Age
Papillary carcinoma is a tumour of children
and young adults. Because it occurs in young chil-
dren, the metastases in the lymph glands were once
thought to be clusters of aberrant normal thyroid
tissue. They are not. They are true metastases and
may often be the presenting feature. Often these
enlarged nodes can present as large cystic swellings
and mimic a branchial cyst.
Sex
Females are affected three to four times more
often than males.
Symptoms
The common presenting symptom is a
lump in the neck. The lump may be in the region of
the thyroid gland or, if it is caused by secondary
deposits in the lymph glands, in the antero-lateral
part of the neck.
Distant secondary deposits or a change in thy-
roid function are very uncommon with papillary
carcinomata.
Duration of symptoms
The lump may have been pres-
ent for many years before the patient seeks advice,
because these tumours are slow growing and slow to
spread beyond the thyroid gland and its draining
lymph glands.
Cause
The patient will have no idea of the cause of
the lump, but it is important to ask them if they
have had any radiation to the neck or mediastinum.
There is a greater incidence of papillary carcinoma
in children who have had their neck or chest inten-
tionally irradiated for conditions such as asthma,
tuberculosis, enlargement of the thymus, tonsillitis
and acne (a form of treatment no longer practised),
and unintentionally following a nuclear reactor
accident.
Examination
The principal, and usually the only, abnormality is
the lump or lumps in the neck.
Position
The lump may be in the region of the thy-
roid gland or deep to the sternomastoid muscle.
Temperature and tenderness
The skin of the neck
should be normal, provided the tumour has not
infiltrated into it. The lumps are usually not tender.
Shape and size
The primary nodule in the thyroid
gland may vary in size from a minute, impalpable
nodule to a nodule 3–5 cm in diameter. When pal-
pable, it is usually spherical, smooth and clearly
defined, but its surface may be bosselated.
Lymph glands containing thyroid carcinoma
metastases are ovoid or nodular, and usually
smooth and clearly defined. Occasionally they can
be cystic, providing a diagnostic dilemma. The thy-
roid gland lymph first drains to the pretracheal and
paratracheal lymph glands and then to the lower
deep cervical lymph glands which lie beneath the
anterior edge of the lower third of the sternomastoid
muscle.
Composition
The consistence of both the primary
nodule and the secondary lymph glands is hard or
firm. Both are dull to percussion, do not fluctuate
and do not cause a bruit.
Relations
The primary nodule in the thyroid gland
will move upon swallowing and is not usually fixed
to superficial structures.
Chap-11.qxd 12/11/07 9:50 AM Page 304
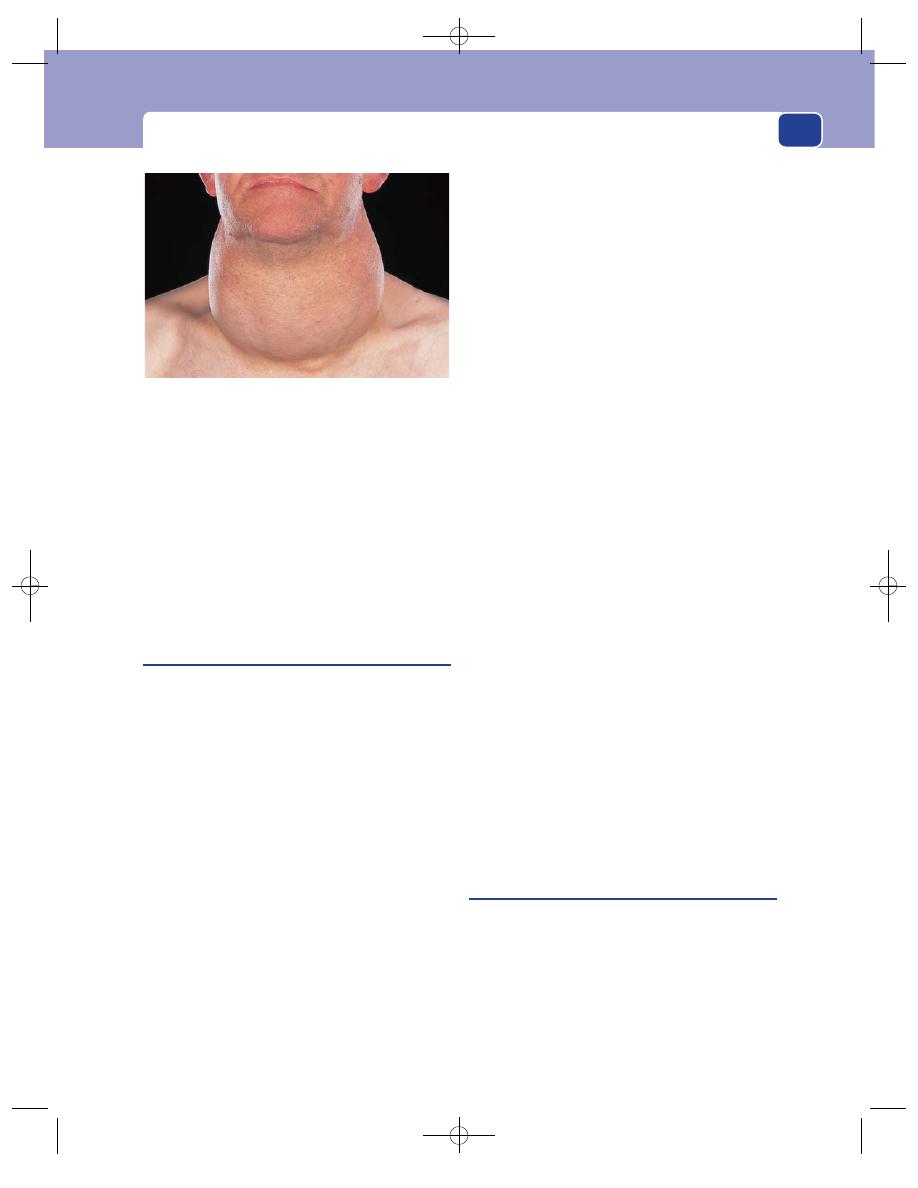
Carcinoma of the thyroid gland
305
Enlarged lymph glands move more easily in a trans-
verse than in a vertical plane and do not move with
swallowing. They are not usually attached to the skin.
Lymph drainage
If you feel a nodule in the thyroid
gland, examine all the lymph glands in the neck
with care.
General examination
The patient usually appears fit and
well, without any of the systemic signs which suggest
a disseminated neoplasm or thyroid dysfunction.
Follicular carcinoma
The cells in this well-differentiated thyroid cancer
retain their normal follicular configuration. Most of
the follicles contain a small amount of colloid, which
implies that the cells are synthesizing hormone. This
has an important bearing on treatment, because the
tumour cells will often take up radioactive iodine.
This tumour spreads by the bloodstream.
History
Age
Follicular carcinomata occur in adults between
the ages of 20 and 50 years.
Sex
Women are affected more often than men.
Symptoms
The common presenting symptom is a
lump in the neck, which may have been present for
many years.
If the tumour has spread beyond the thyroid, the
patient may complain of breathlessness, chest pain or
pain or swelling in a bone, caused by lung and bone
metastases, respectively. In these circumstances the
pathologist usually finds that the tumour has a thin
capsule and has spread into the substance of the
gland – the ‘invasive’ variety of follicular carcinoma.
Multiple lumps in the neck caused by metas-
tases in lymph glands do occur, but not as fre-
quently as with papillary carcinoma.
Systemic effects
These patients are euthyroid.
Examination
The principal, and often the only, abnormality is the
lump in the neck.
Position
Follicular carcinoma usually arises in one of
the lateral lobes of the thyroid gland.
Temperature and tenderness
The overlying skin is not
hot and the lump is not tender.
Shape and size
The lump is usually spherical and
smooth, with distinct edges. Even the invasive var-
iety feels as if it has a distinct surface.
Composition
The lump is firm to hard, does not fluc-
tuate, is dull to percussion and has no bruit.
Relations
The lump moves with swallowing, but is
not attached to overlying structures.
Lymph glands
The deep cervical lymph glands may
be enlarged and hard.
Local tissues
The local tissues are usually normal.
General examination
Examine the chest carefully for
any evidence of consolidation or collapse. Pulmonary
secondary deposits are quite common but may not
cause any abnormal physical signs.
Metastases in the skeleton are often painful and
tender. A bone near to the skin containing a metasta-
sis may be visibly deformed, swollen and hot. Some
thyroid cancer metastases are so vascular that they
are soft and pulsatile and have an audible bruit.
Anaplastic carcinoma
This is the worst variety of thyroid cancer because it
spreads rapidly. Most patients with this disease are
dead within 1 year of diagnosis. Its cells do not
synthesize thyroid hormone.
History
Age
Anaplastic carcinoma of the thyroid gland
appears between the ages of 60 and 80 years.
FIG 11.41
A poorly differentiated follicular carcinoma arising
in a long-standing multinodular goitre.
Chap-11.qxd 12/11/07 9:51 AM Page 305
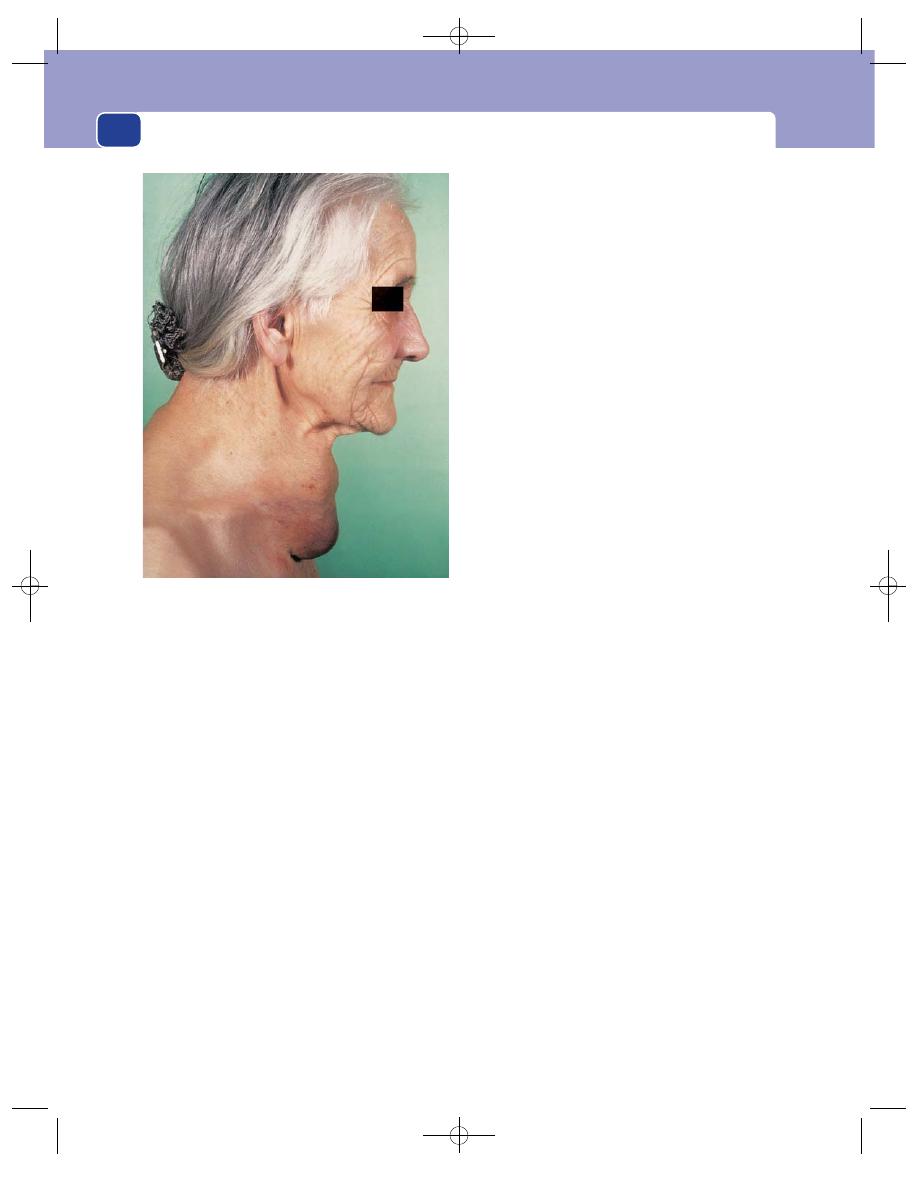
The neck
306
Sex
Females are affected more often than males.
Symptoms
The common complaint is a swelling of
the neck rather than ‘a lump’, which may be rapidly
growing. The patient complains of swelling because
the tumour is diffuse and infiltrating, not localized.
A dull aching pain in the neck is quite common.
Dyspnoea occurs when the tumour begins to
compress the trachea, especially when the neck is
flexed. It may also occur if there are multiple pul-
monary metastases.
Hoarseness or a change in the quality of the
voice is a diagnostic symptom because it implies
infiltration of the recurrent laryngeal nerve.
Pain in the ear, caused by infiltration of the
vagus nerve, is not uncommon.
There may be bone pain. Any bone can be the
site of a secondary deposit, and pathological frac-
tures can occur.
General malaise and weight loss appear when
there is disseminated disease.
Duration of symptoms
The symptoms of an anaplastic
carcinoma often develop rapidly as this carcinoma
grows quickly and is highly invasive. Local invasion
and compression of the trachea can lead to death
from asphyxia or precipitate a fatal pneumonia.
Examination
Position
The swelling in the neck is in the region of
the thyroid gland. At first this is in one lobe, but in
advanced cases the whole gland may be enlarged
and irregular.
Colour
The overlying skin often has a red-blue tinge
because the underlying infiltration interferes with
its venous drainage.
Temperature
The skin temperature is normal, or
slightly raised.
Tenderness
The mass often becomes tender as the
tumour infiltrates beyond the thyroid gland.
Shape
The mass in the neck has no definable shape
once it has spread beyond the thyroid gland, and
before this stage it is not easy to define because the
surface is so indistinct.
Size
The mass may become so big that it interferes
with neck movements.
Surface and edge
The surface is irregular and indis-
tinct and the lump often has no palpable edge.
Composition
The mass is hard and solid. It does not
fluctuate, is dull to percussion and has no bruit.
Relations
Provided the mass is not infiltrating the
whole neck, it will move during swallowing.
It may be fixed to one or both sternomastoid
muscles and the overlying skin as well as to the tra-
chea. When the sternomastoid muscle is contracted,
the movement of the lump during swallowing is
limited and the skin becomes puckered.
The skin may be infiltrated with tumour, making
it thick, nodular and a reddish-brown colour.
Lymph glands
Although the deep cervical lymph
glands are invariably involved in the disease, their
enlargement may be obscured by the primary mass
in the gland.
If the local lymph glands are palpable, they feel
hard and fixed. At first they are smooth and discrete,
but they become irregular and indistinct when the
tumour begins to spread through their capsules.
FIG 11.42
An anaplastic carcinoma of the thyroid.
Chap-11.qxd 12/11/07 9:51 AM Page 306
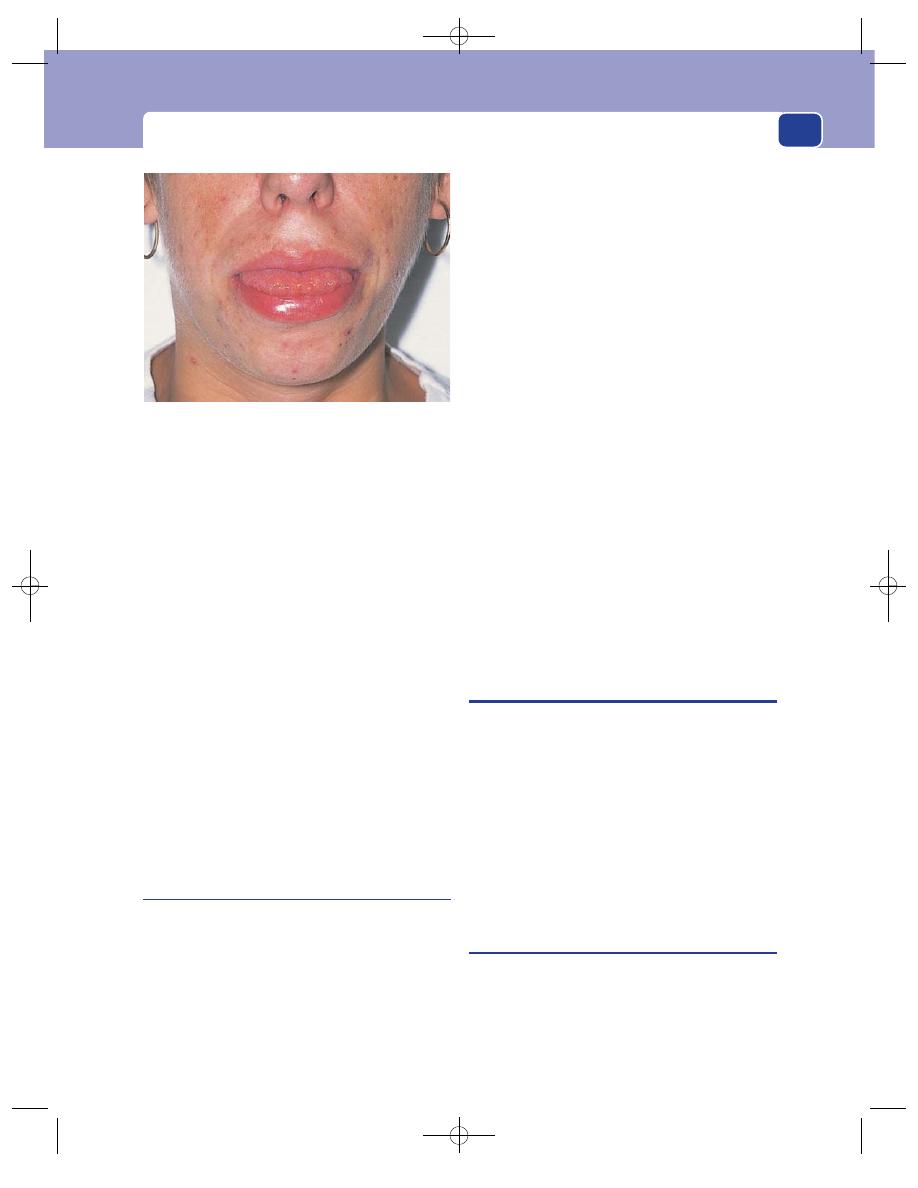
Thyroiditis
307
State of local tissues
The skin of the neck may be
tethered or fixed to the lump or even infiltrated with
tumour.
The trachea is often compressed and deviated,
causing stridor.
One vocal cord may be paralysed by infiltration
of the recurrent laryngeal nerve. This may be sus-
pected if the patient has a hoarse voice, but must be
confirmed by indirect laryngoscopy.
All the soft tissues of the neck may be fixed and
hardened by infiltrating tumour.
General examination
Patients often breathe with diffi-
culty and have stridor. There may be basal pneumonia
or collapse caused by pulmonary secondary deposits
or the restriction of lung expansion by the narrowed
trachea.
There is often wasting and anaemia.
There may be evidence of skeletal metastases –
even pathological fractures.
In advanced cases the liver may be enlarged, and
secondary deposits occasionally appear in the skin.
Medullary carcinoma
This is a rare condition but is mentioned because it
can sometimes be diagnosed before operation. It is a
neoplasm of the parafollicular (C) cells.
The common presentation is a firm, smooth and
distinct lump in the neck, indistinguishable from
any other form of thyroid solitary nodule.
The majority of patients are between the ages of
50 and 70 years when the tumour is sporadic in
nature. When the condition occurs in young adults
(20–30 years), often with a family history, it may be
a manifestation of the multiple endocrine neoplasia
syndrome (MEN) types 2a or 2b.
In these cases, the medullary thyroid carci-
noma may be accompanied by associated conditions
such as:
■
phaeochromocytoma
MEN 2a
■
parathyroid tumours
or
■
phaeochromocytoma
■
neuromata of the tongue,
lips and conjuctiva
■
pale-brown birthmarks
MEN 2b
■
megacolon
■
marfanoid habitus.
The symptoms which should make you think of
medullary tumour, apart from a lump in the neck
and the presence of the above lesions in the patient
or their family, are diarrhoea and flushing.
Diarrhoea occurs in one-third of the patients. The
fluidity of the stool and the frequency of defaeca-
tion are both increased.
If this tumour is suspected, it is important to
measure the serum calcitonin level.
THYROIDITIS
There are three varieties of thyroiditis which can
be diagnosed clinically: Hashimoto’s disease, de
Quervain’s thyroiditis and Riedel’s thyroiditis.
The term thyroiditis is a non-specific description
of the histological changes occurring in the gland.
Although the aetiology of these conditions is only
partly understood, the eponyms are useful because
they do not imply an aetiology but rather a clinical
description (provided you ignore the aetiologies pro-
posed by the three gentlemen who made the original
descriptions!).
Hashimoto’s disease
This is an autoimmune thyroiditis. The body fails to
recognize part of itself – in this case both the mito-
chondria of the thyroid cells and the thyroglobulin
they produce – and sets up an immune response
against its own tissues. The result is lymphocyte and
冧
其
FIG 11.43
Tongue neuromata in a patient with MEN 2b and
medullary carcinoma of the thyroid.
Chap-11.qxd 12/11/07 9:51 AM Page 307
The neck
308
plasma cell infiltration of the gland that ultimately
destroys the thyroid cells. In the first instance the
thyroid cells respond by becoming hyperplastic,
causing a degree of thyrotoxicosis, but eventually
and inevitably the gradual destruction of the thy-
roid cells causes myxoedema (hypothyroidism).
History
Age and sex
Hashimoto’s disease is most common in
middle-aged women, especially those near the meno-
pause; but it can occur in men, and at any age.
Symptoms in the neck
The patient usually complains
of a swelling or lump in the neck. This lump may
appear gradually or rapidly, and is often painful,
particularly when it appears rapidly.
The swelling, or lump, fluctuates in size, and the
pain is often intermittent. The symptoms are worse
when the patient is tired, or run down, or has an
intercurrent illness.
The voice should not alter.
Systemic effects
The symptoms of mild thyrotoxico-
sis or myxoedema may be present.
The common course of events is for the mild
symptoms of thyrotoxicosis, which appear at the
onset of the disease, to die out gradually and become
replaced by the opposite symptoms of myxoedema.
The majority of patients are euthyroid when they
complain of the lump, having ignored or not had
any symptoms of thyrotoxicosis, and not reached
the myxoedematous phase.
This variability of the local and systemic effects
of the disease makes the diagnosis difficult.
Family history
Other members of the family may have
suffered from the same or other forms of auto-
immune disease, such as pernicious anaemia and
autoimmune gastritis.
Examination
The main complaint is usually the lump in the neck.
Position
The swelling is in the region of the thyroid
gland and may be unilateral or bilateral.
Temperature
In the initial acute phase – if it occurs –
the overlying skin may feel warm.
Tenderness
The swelling is often slightly tender.
Shape
The swelling may be any shape – a solitary
nodule, the whole of one lobe, or the whole gland.
When one lobe or more is involved, the swelling is
usually lobulated.
Size
Hashimoto’s disease usually causes a moderate
swelling of the gland, easily visible but rarely gross.
Surface
The swelling has a smooth surface and the
edge is distinct.
Composition
The swelling has the texture of firm
rubber. This texture is homogeneous, in spite of the
lobulated shape, which helps distinguish the
swelling from a nodular or colloid goitre.
There is no bruit.
The composition and mild tenderness are the
features most likely to alert you to the possibility of
the diagnosis.
Relations
The swelling moves with swallowing but is
not fixed to any other structures.
Local tissues
All the local tissues should be normal.
Lymph glands
The nearby lymph glands should not
be enlarged.
General examination
The majority of patients are
euthyroid, but some will have the signs of mild thy-
rotoxicosis and others of early myxoedema.
De Quervain’s thyroiditis
This condition is a true subacute inflammation of
the thyroid gland, often associated with mild hyper-
thyroidism. It may be caused by a virus infection,
and sometimes occurs in epidemics.
History
De Quervain’s thyroiditis occurs in adults. The main
complaint is of the sudden appearance of a painful
swelling in the neck. The patient feels ill and may
notice that they are anxious, sweaty and hungry and
have palpitations.
Examination
Examination reveals a diffuse, firm, tender swelling
of the whole of the thyroid gland.
There may be signs of mild thyrotoxicosis –
nervousness and agitation, lid lag and tachycardia.
De Quervain’s thyroiditis is self-limiting. It dis-
appears in 1–3 months.
Chap-11.qxd 12/11/07 9:51 AM Page 308
Thyroiditis
309
Riedel’s thyroiditis
This is a very rare condition but is mentioned
because the changes in the gland can be mistaken
for the signs of a carcinoma.
It is a condition in which the gland is gradually
replaced by dense fibrous tissue, which may even infil-
trate beyond the gland into the nearby strap muscles.
The patient complains of a lump in the neck or,
very rarely, increasing dyspnoea caused by com-
pression of the trachea.
Examination reveals a stony hard swelling of the
thyroid gland, at first of one lobe, but eventually of
both lobes and the isthmus.
The lump moves with swallowing but may be
fixed to the surrounding tissues, which are other-
wise normal.
When both lobes are involved, the smooth, discrete
surface usually excludes the diagnosis of carcinoma,
but when one lobe is involved it is impossible to
make a firm clinical diagnosis.
Note
A scheme for diagnosing thyroid swellings is shown
in Figure 11.44 on pages 310–11.
Chap-11.qxd 12/11/07 9:51 AM Page 309
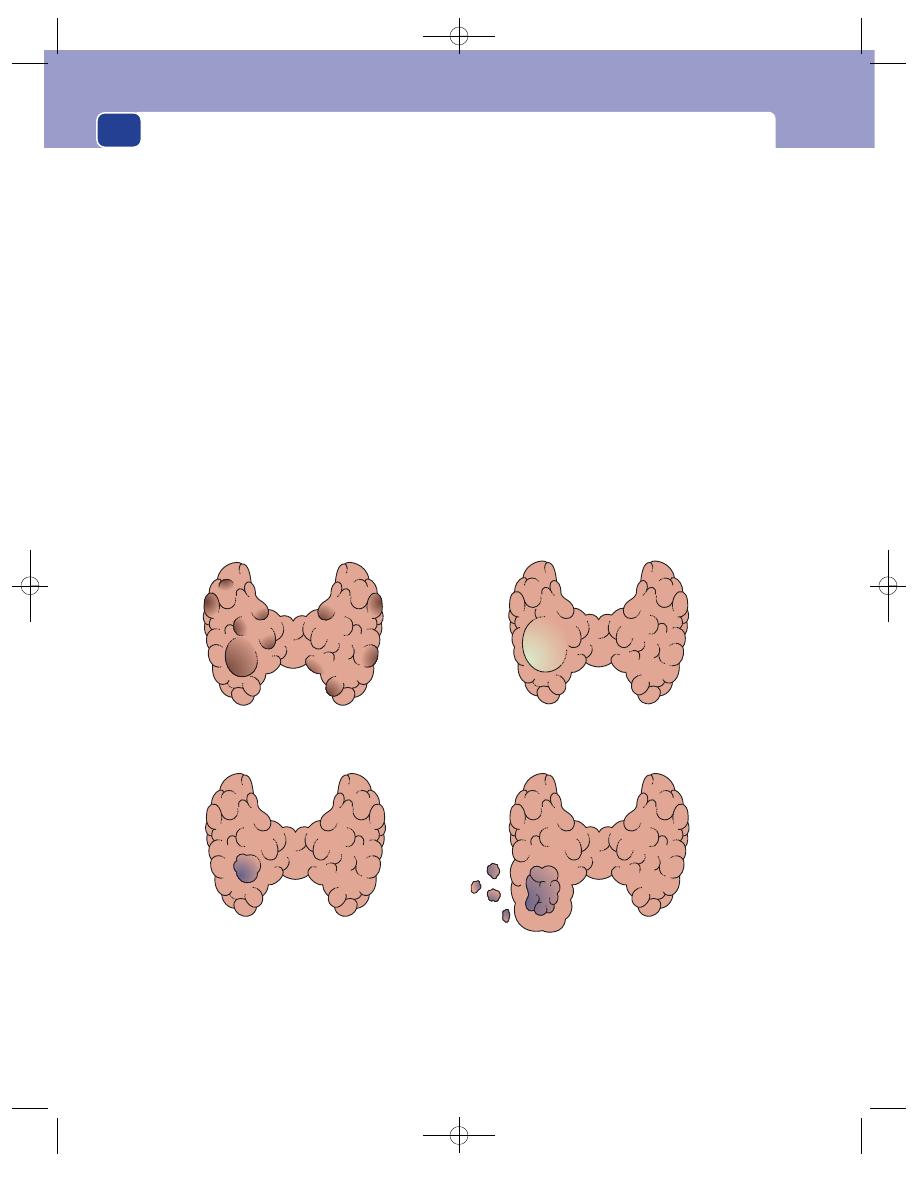
The neck
310
A SCHEME FOR THE DIAGNOSIS OF THYROID SWELLINGS
Once you have examined the patient you should be able to draw conclusions as to the nature and texture of the gland and as
to its endocrine activity.
The gland
1.
Solitary palpable nodule
2.
Multinodular goitre
3.
Diffusely enlarged gland
Activity of the gland
1.
Normal (euthyroid)
2.
Hypersecretion (hyperthyroidism/thyrotoxicosis)
3.
Hyposecretion (hypothyroidism/myxoedema)
Having established the configuration of the gland and its endocrine activity, a table can be drawn up as to possible
differential diagnoses (see Revision panel 11.8 on page 303). This allows a degree of clarity in interpreting the presenting
clinical features and in arriving at a working diagnosis.
A benign adenoma
A cyst
Carcinoma (papillary, follicula or medullary).
The lymph glands may be palpable,
especially with the papillary type
The only palpable nodule of a
multinodular goitre
If only one lump is palpable it may be:
FIG 11.44
Chap-11.qxd 12/11/07 9:51 AM Page 310
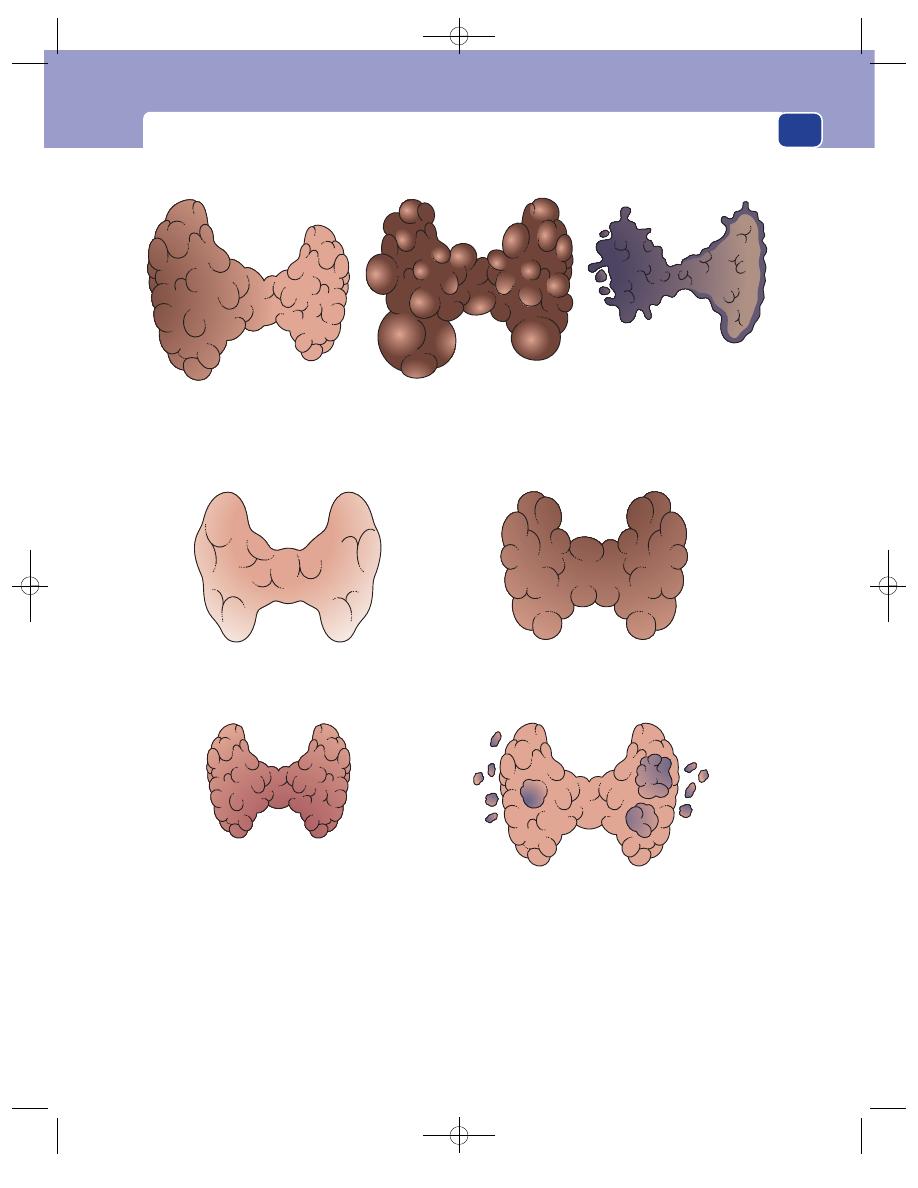
Thyroiditis
311
FIG 11.44
continued
A multinodular goitre
The whole of one lobe involved by
Hashimoto's thyroiditis
If more than one lump is palpable the swelling may be:
Hyperplastic (colloid) goitre.
Moderate to gross enlargement.
Bosselated. No bruit
Thyroiditis. Hashimoto's,
de Quervain's or Riedel's.
Moderate or small. Hard, tender
Grave's disease. Primary thyrotoxicosis.
Slight to moderate enlargement.
Soft, smooth with a bruit
If there is diffuse, homogeneous enlargement of the whole gland the swellling may be:
Multifocal carcinoma
An anaplastic carcinoma
especially if the voice is
hoarse and the mass is fixed
to the surrounding tissues
Chap-11.qxd 12/11/07 9:51 AM Page 311
More than a quarter of general surgical outpatient
referrals are females with breast symptoms, only a
small proportion of whom will have breast cancer.
Less than ten per cent of general surgical operations
are for breast disease.
Breast cancer has by far the best prognosis of the
common solid organ malignancies and, with con-
stantly improving treatments, up to 80 per cent of
sufferers are alive and well 10 years after diagnosis.
Nevertheless, public perception and constant media
attention ensure that women with breast symptoms
are significantly more anxious than other surgical
patients.
At first, students find the assessment of the breast
difficult but, with practice, a carefully taken history
and painstaking examination will yield an accurate
diagnosis in most cases. Most patients require no
more than reassurance, but rapid identification of
those few with malignant disease remains a challenge.
Development and physiology of
the breast
Breast development is occasionally seen in neonates
as a consequence of maternal oestrogens crossing
the placenta. Babies of both sexes may be affected
and lactation can occur (‘witches’ milk’), sometimes
complicated by abscess formation.
Normally the female breast develops shortly
before the menarche. Occasionally, the enlargement
is asymmetrical and causes great parental anxiety.
The breasts increase in size in the second half
of each menstrual cycle, following ovulation. Mild
pain and tenderness during this phase are common.
In pregnancy, the size and texture of the breasts
change profoundly in preparation for lactation. At
this time and during lactation, clinical assessment is
much more difficult.
HISTORY AND EXAMINATION OF
BREAST DISEASE
History
Age
Age is a simple but very important piece of diagnostic
information.
Young women will only very rarely have cancer,
but over the age of 70 most breast lumps turn out to
be malignant.
After taking the past medical history and the his-
tory of the presenting complaint, it is essential to ask
specific questions about the following.
Previous pregnancies
How many children has the patient had?
Were the children breast-fed and, if so, for how
long?
Parity and breast-feeding reduce the incidence of
breast cancer: a mother of five who fed all her chil-
dren is less likely to have breast cancer than a nulli-
parous woman of the same age.
Menstrual pattern
What is the menstrual pattern? (Regularity, dur-
ation and quantity of bleeding.)
Breast symptoms which alter with the menstrual
cycle are highly likely to be associated with benign
disease.
Medication
Is the patient taking drugs containing female sex
hormones? Oral contraceptives commonly reduce
the severity of cyclical change in the breasts. Hormone
replacement therapy taken by menopausal and post-
menopausal patients extends the age at which they
are likely to suffer from benign conditions such as
breast cysts.
Chap-12.qxd 4/19/05 14:26PM Page 312
History and examination of breast disease
313
Mental attitude
When taking a detailed history of the presenting
complaint, remember that patients are often fearful
of the consequences of breast lumps and hide their
symptoms with an impressive degree of self-delusion.
One may be told that a fungating cancer was only
noticed last week when it has clearly been present
for much, much longer. Never be censorious about
this facet of human nature – you do not know how
you would react in similar circumstances!
Your assessment of the way in which the patient
is reacting to her symptoms will help you decide
how to guide her through her subsequent treatment
and management.
Examination
Position
The patient must be fully undressed to the waist,
resting comfortably on an examination couch with
her upper body raised at 45° to the legs. This posi-
tion is the best compromise between lying flat,
which makes the breasts fall sideways, and sitting
upright, which makes the breasts pendulous.
Patients sometimes say that their lump can only be
felt when they adopt a certain posture, e.g. standing
or lying on one side, and they should therefore be
examined in this position as well.
Inspection
Stand or sit directly in front of the patient, inspect
both breasts and look for the following features.
Size
There is enormous variation, with individual
sensitivities at each extreme.
Symmetry
It is quite normal for there to be a differ-
ence between the sides. However, any marked size
difference of recent onset is likely to be caused by
significant pathology.
Skin
The skin may be pulled in or puckered by an
underlying cancer. There may be oedema caused by
obstruction of skin lymphatics by cancer cells, which
is commonly referred to as peau d’orange, an accur-
ate description. Other skin changes include nodules
of tumour or a malignant ulcer due to direct inva-
sion of the skin by a cancer.
The nipples and areolae
The colour of the nipples and
areolae changes with age, and there is darkening
during pregnancy. The areolar skin is naturally cor-
rugated with small nodules known as Montgomery’s
tubercles.
The nipple may be inverted. Is this bilateral, and
does it display the transverse slit pattern seen in
duct ectasia? There may be evidence of fluid leaking
from the nipple, or there may be eczematous skin
changes as in Paget’s disease.
Duplication
There may be accessory nipples along
the mammary line from axilla to groin, or visible
ectopic breast tissue in the anterior axillary fold.
Revision panel 12.1
Points to remember when examining the breast
History
Menarche, development, menopause,
changes during menstrual cycle,
pregnancies, lactation, family and
drug history.
Examination
Expose all of the top half of the trunk.
Inspect the breasts at rest and ask the
patient to raise her arms above her head.
Look at :
size
symmetry
skin:
■
puckering
■
peau d’orange
■
nodules
■
discolouration
■
ulceration
nipples and areolae
axillae, arms and neck.
Feel the normal side first.
Examine the axillae and arms.
Examine the supraclavicular fossae.
Palpate the abdomen for :
hepatomegaly
ascites
nodules in the pouch of Douglas.
Examine the lumbar spine:
percussion
movements
straight-leg raising
ankle jerks.
Chap-12.qxd 4/19/05 14:26PM Page 313
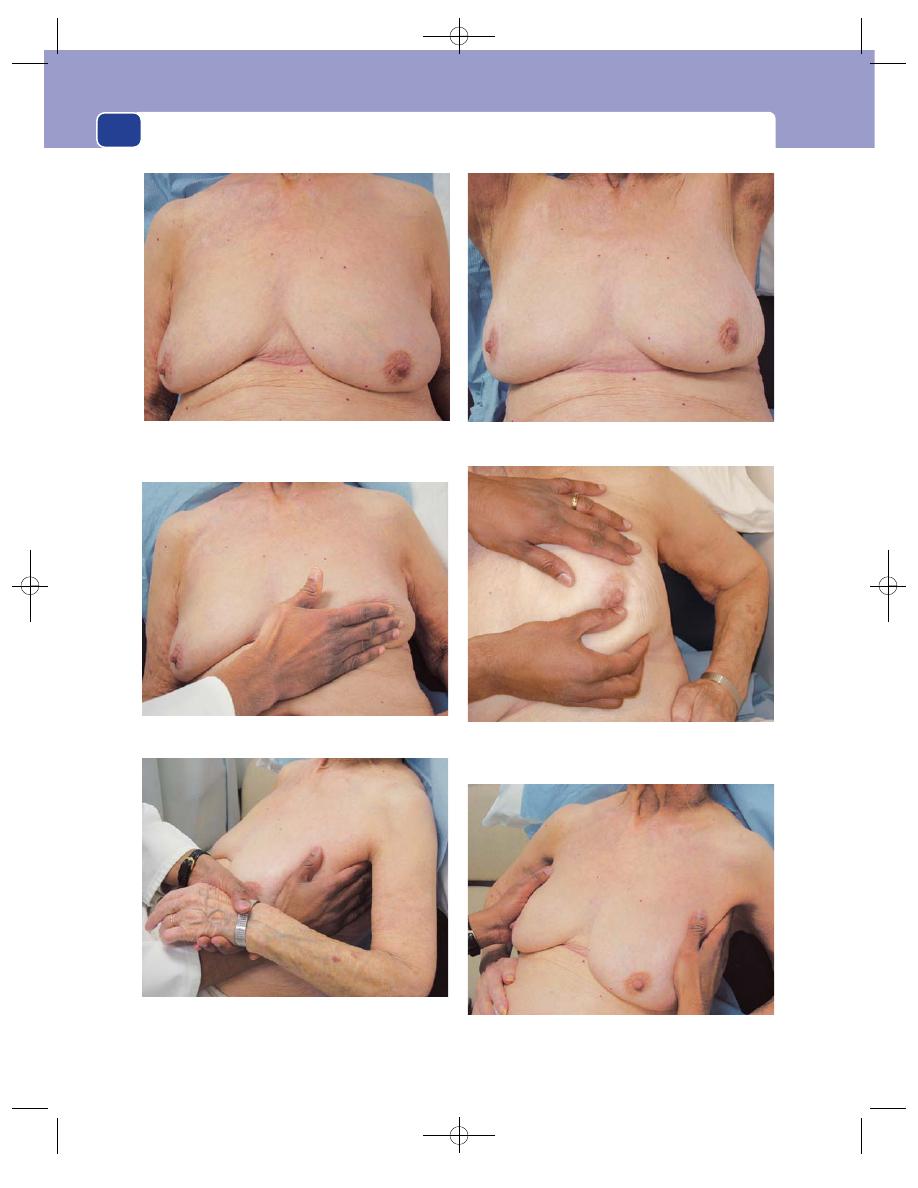
The breast
314
FIG 12.1
THE EXAMINATION OF THE BREAST.
Look at the breast for asymmetry and for changes in the skin
and nipple.
Feel the breast with the flat of your fingers.
If necessary, compare the axillae simultaneously.
When you palpate the axilla, hold the patient’s arm to relax
the muscles that form the axillary folds.
Test the mobility of every lump in two directions, with the
pectoralis muscles relaxed and tense. Tense the muscles by
asking the patient to place her hands on her hips and press in.
Ask the patient to raise her hands above her head. This
exaggerates asymmetry and skin tethering.
Chap-12.qxd 4/19/05 14:27PM Page 314
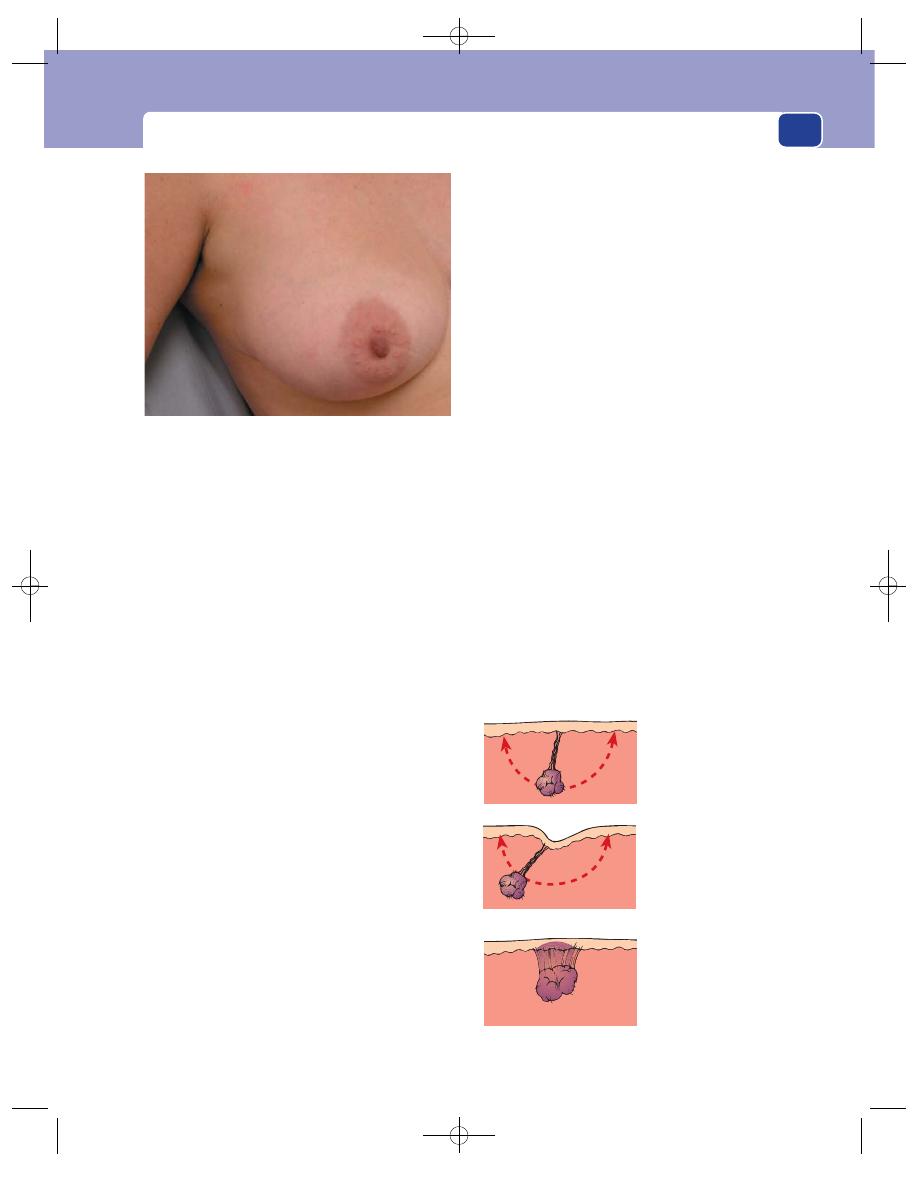
History and examination of breast disease
315
Ask the patient to slowly raise her arms above her
head. Skin changes may then become more apparent,
particularly tethering to a carcinoma. Exposure of the
underside of the breasts in an obese patient with
large breasts may reveal intertrigo.
Ask the patient to press her hands against her
hips to tense the pectoral muscles. This may reveal a
previously invisible swelling.
Inspect the axillae, arms and supraclavicular fos-
sae. Grossly enlarged lymph glands may be visible, and
distended veins or arm lymphoedema may be obvious.
Palpation
The breast should be palpated with the flat of the
fingers and not with the palm of the hand. Surgical
mythology says that the breast should be felt with
‘the flat of the hand’ – this is wrong: use the fingers,
which are far more sensitive.
With the patient sitting up at 45°, either begin
with the normal side or face the patient and feel
both breasts together. The texture of the breast is
enormously variable, more so than any other organ,
depending on age, parity, body mass and hormonal
activity. It may be quite soft and apparently feature-
less, or it may be firm and fibrous, with easily palp-
able nodules, which are in fact normal lobules. In a
menstruating woman and at the end of the second
half of the menstrual cycle, the breasts may be
engorged and tender. In a patient with pendulous
breasts and firm breast tissue, the edge of the breast
may be readily felt at its upper margin.
Do not forget to feel the axillary tail, which lies
over the anterior axillary fold. This may be very
obvious in a slim woman with firm breast tissue.
Occasionally this part of the breast seems to be
separate from the main breast and so presents as
an apparently axillary swelling.
Do not be discouraged by your initial difficulty
in differentiating normal from abnormal breast
tissue. Clinical examination remains an art, not a
science, and requires frequent practice.
If you find a lump, ascertain its site, shape, size,
surface, edge and consistence, as with a lump in any
other area of the body. This may require bimanual
examination, controlling movement of the lump
with one hand and feeling it with the other.
Not infrequently, even after a thorough palpation,
you may fail to find swelling. If so, ask the patient to
find it. Often she will then demonstrate to you a very
obvious abnormality! Do not consider this a per-
sonal affront – it happens to the most experienced!
Even if you still cannot feel the lump that the patient
can feel, take the symptom seriously and arrange
further investigations or a re-examination. Believe
the patient and not your inexperienced fingers.
Relations to skin
There is a difference between skin fixation and skin
tethering.
Most lumps can be
moved anywhere
within the arc
depicted, without
moving the skin.
If when a lump is
pulled outside the arc
the skin indents, it
is tethered.
If a lump cannot be
moved without
moving the skin,
it is fixed.
An ectopic mass of breast tissue in the axilla. This is easily
mistaken for a pathological abnormality.
FIG 12.1
continued
FIG 12.2
Tethering and fixation.
Chap-12.qxd 4/19/05 14:27PM Page 315
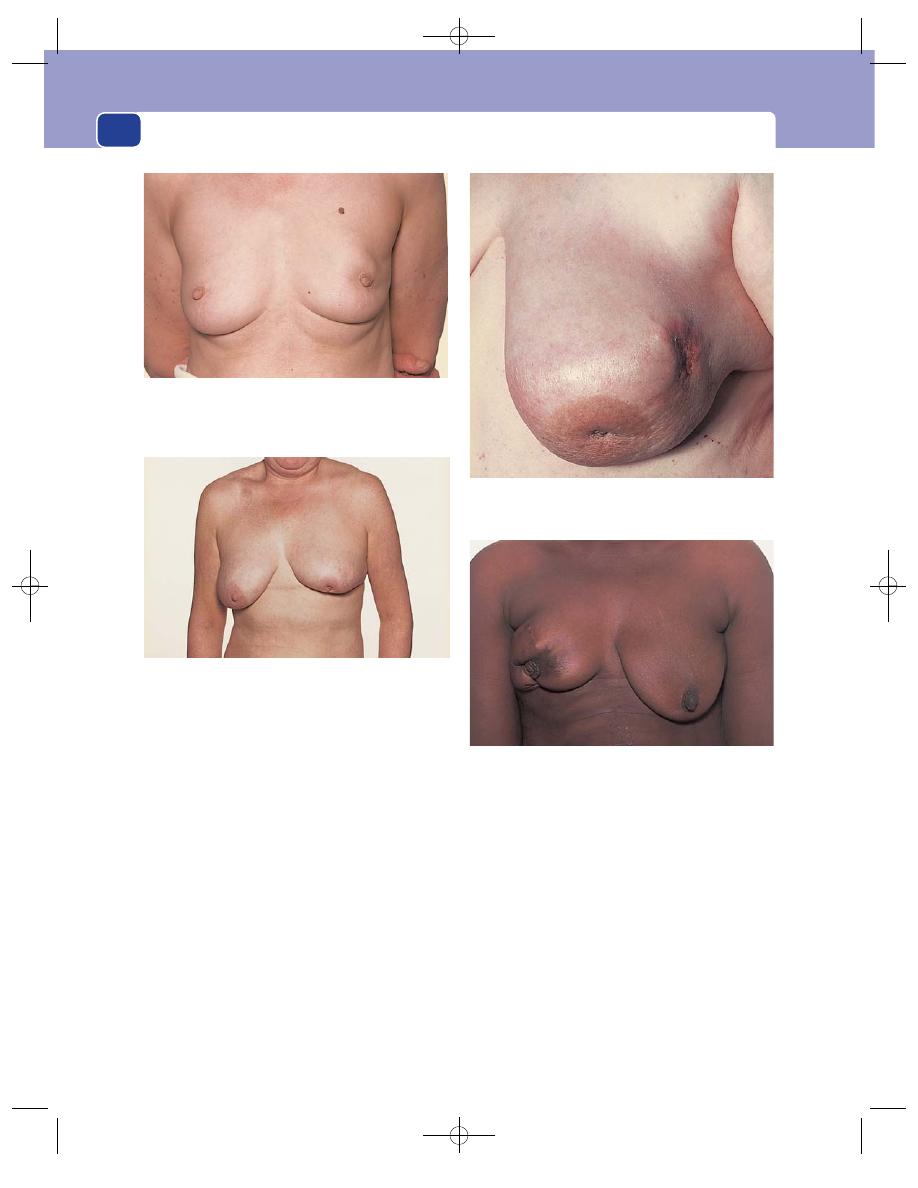
The breast
316
When a lesion is fixed to the skin it has spread into
the skin and cannot be moved or separated from it.
A tethered lesion is one which is more deeply situ-
ated and, by distorting the fibrous septa which sep-
arate the lobules of breast tissue (the ligaments of
Astley Cooper), puckers and pulls the skin inwards,
but remains separate from the skin and can be
moved independently.
Relations to the structures beneath
the breast
The difference between fixation and tethering to
deep structures is less obvious because the muscles
beneath the breast are invisible, soft and mobile. If
there is a deep-seated lump, ask the patient to press
her hand against her hip, thereby tensing the pec-
toral muscles. If the lesion becomes less mobile, it is
either fixed or tethered. The less the movement, the
more likely it is to be fixed.
The nipple
If there is nipple inversion, it may be possible to
evert it by gentle squeezing its base or by asking the
patient do it for you.
Nipple inversion that is easily everted is not an
abnormality.
FIG 12.3
CHANGES IN THE NIPPLE THAT MAY BE CAUSED BY
AN UNDERLYING CARCINOMA.
Displacement and deviation. The left nipple is elevated
(displaced) and pointing downwards and inwards, not
downwards and outwards (deviation). The tumour can be
seen just above the areola.
Retraction and peau d’orange. This carcinoma has invaded
the skin and ulcerated. The skin of the lower part of the
breast is oedematous and looks like the skin of an orange.
Destruction. The right nipple and areola have been invaded
and destroyed by the underlying carcinoma.
Retraction and displacement. The left nipple has been pulled
into the breast (retraction) and pulled upwards (displacement)
by the underlying carcinoma.
Chap-12.qxd 4/19/05 14:27PM Page 316
History and examination of breast disease
317
If the nipple will not evert, there is likely to be
underlying disease.
Unilateral inversion is more significant than
bilateral inversion.
If there is said to be a discharge, it may be possible
to express it by gently pressing the areola around the
base of the nipple and observing whether any fluid
comes from one or many duct orifices. The character
of the fluid should be noted. Nipple discharges may be
red, white, creamy yellow or watery (see page 326).
The axilla
Clinical assessment of the axilla in the absence of
gross pathology is difficult. Small, firm,‘shotty’ glands
can often be felt in thin patients, but this finding is
usually symmetrical. In the obese, it may be virtually
impossible to feel even significantly enlarged glands.
The axillary lymph glands form a three-sided
pyramid whose apex is in the narrow gap between
the first rib and the axillary vessels.
Stand on the patient’s right side. Take hold of her
right elbow with your right hand and let her forearm
rest on your right forearm. Persuade her to allow you
to hold the weight of her arm. (Patients always want to
help by holding their arm away from their side, but
this tenses the muscles in the anterior and posterior
axillary folds and makes palpation of the lymph glands
impossible.) Place your left hand flat against the chest
wall and feel for any glands that may lie in the central
or medial aspects of the right axilla by sweeping the
tips of your fingers across and from the top to the base
of the axilla to catch the glands against the chest wall.
To reach the apex of the axilla you will have to
push the tips of your fingers upwards and inwards.
Explain to the patient that you must push firmly to
examine the axilla thoroughly and that this may
cause discomfort. (Some patients find this ticklish!)
Next move your left hand anteriorly over the edge
of the pectoralis minor muscle and downwards into
the axillary tail and behind the edge of the pectoralis
major muscle. Turn your hand (or change hands) to
feel the subscapular glands on the posterior wall of
the axilla, and finally feel the lateral aspect of the
axilla in case there are any brachial glands level with
the neck of the humerus.
To palpate the left axilla, lean across the patient,
hold her left elbow with your left hand and use your
right hand to feel the axilla. If it is difficult to feel the
axilla in this way, move round to her left side.
With a cooperative patient who is able to relax
(and is not ticklish!), you may be able to obtain
good access to the axillae by asking her to place her
hands on her iliac crests and slacken her muscles,
and then approach from in front. This position is par-
ticularly useful for comparing the two sides when
glands are palpated but may not be pathological.
Finally, palpate the supraclavicular fossa and
the neck.
Record the number, size and consistence of any
glands that you feel.
General examination
Check the arms for swelling or any neurological or
vascular abnormalities, palpate the abdomen look-
ing for hepatomegaly or ascites, and examine the
lumbar spine for pain or restricted movements.
Triple assessment
In the UK, most patients with breast problems are
seen in dedicated breast clinics. Those with suspected
Revision panel 12.2
The changes that can occur in the nipple
Destruction
Depression (retraction or inversion)
Discolouration
Displacement
Deviation
Discharge
Duplication
Revision panel 12.3
The types of discharge from the nipple
Colour
Cause
Red (blood)
Duct papilloma
Pink (serum
⫹ blood)
Duct carcinoma
Clear pale yellow (serum)
Duct ectasia
Brown
(breast
Duct ectasia
Green
secretions
Cysts
Black
and debris)
Creamy white or yellow (pus)
Duct ectasia
Thin white (milk)
Lactation
}
{
{
Chap-12.qxd 4/19/05 14:27PM Page 317
The breast
318
cancer receive a triple assessment, which consists of:
1. history and examination,
2. diagnostic imaging by mammography and/or
ultrasound scanning,
3. cytology or histology.
Cytological examination looks at smears obtained
by aspiration of a lump with a fine needle (FNA).
Histological examination is based on biopsy
specimens obtained with special core-cutting nee-
dles, often with radiological guidance.
PRESENTATION OF BREAST DISEASE
Breast disease presents in three main ways:
■
a lump, which may or may not be painful,
■
pain, which or may not be cyclical,
■
nipple discharge or change in appearance.
The common conditions which cause these symp-
toms are described individually in the rest of this
chapter, but the likely diagnoses when the patient
presents with one or more of the above are as follows.
A painless lump
■
Carcinoma
■
Cyst
■
Fibroadenoma
■
An area of fibroadenosis
A painful lump
■
An area of fibroadenosis
■
Cyst
■
Periductal mastitis
■
Abscess (usually postpartum or lactational)
■
Sometimes a carcinoma
Pain and tenderness but no lump
■
Cyclical breast pain
■
Non-cyclical breast pain
■
Very rarely, a carcinoma
Nipple discharge
■
Duct ectasia
■
Intraduct papilloma
■
Ductal carcinoma-in-situ
■
Associated with a cyst
Changes in the nipple and/or areola
■
Duct ectasia
■
Carcinoma
■
Paget’s disease
■
Eczema
Changes in breast size and shape
■
Pregnancy
■
Carcinoma
■
Benign hypertrophy
■
Rare large tumours
The fact that many diagnoses are repeated in dif-
ferent sections explains why it is often difficult to
make a definite clinical diagnosis. Note carefully that
carcinoma, the only life-threatening disease of the
breast, can present in almost any way, to which must
be added, in recent years, cases discovered in asymp-
tomatic women by screening mammography.
CARCINOMA OF THE FEMALE BREAST
Cancer of the breast is an adenocarcinoma and the
commonest cancer in women. There are many
macroscopic varieties and histological types. A par-
ticular feature is the variable quantity of fibrous tis-
sue that surrounds the cancer cells. Sometimes 90
per cent of the mass is fibrous stroma, with just a few
cancer cells scattered through it, while at the other
end of the spectrum is the cancer with no fibrous
reaction. This variety may be so cellular, vascular
and fast growing that it is clinically indistinguish-
able from acute inflammation.
The cut surface of a carcinoma is classically con-
cave, rough, gritty and pale grey with prominent
yellow and white flecks, and is said to cut like ‘an
unripe pear’. The cut surface of a benign lesion bulges
out to become convex, is white rather than grey, and
feels smooth and rubbery, not gritty.
The designation ‘cancer’ for malignant tumours
originates from the Latin word for a crab. Certainly
the cut surface of some breast carcinomata, with an
indefinite edge and extending, infiltrating tentacles,
rather like crab claws, fits this description.
In a proportion of cases, the malignant cells
remain inside the ducts and there is no invasive
element. This is termed ‘ductal carcinoma-in-situ’
(DCIS). It may present as a lump in a manner simi-
lar to invasive cancer, or with nipple discharge, or
be picked up on screening because it is often associ-
ated with microcalcification, which is visible on
mammography.
Chap-12.qxd 4/19/05 14:27PM Page 318
Carcinoma of the female breast
319
When carcinoma cells migrate along the ducts to
the nipple, they produce the skin changes known as
Paget’s disease.
History
Age
Carcinoma of the breast is extremely rare in
teenagers and rare in the twenties. From the thirties
onwards there is a progressively increasing inci-
dence to which peaks in the late fifties. It remains
common into old age. There are unexplained geo-
graphical variations in its incidence, but it is pre-
dominantly a disease of Western civilizations.
Symptoms
The presenting symptoms may be related
to the primary lesion or, rarely, to the effects of
secondary deposits.
Classically the patient notices a painless lump,
often when washing or looking into a mirror. The
size of the lump when first noticed does not give an
accurate indication of how long it has been present.
Occasionally there is a pricking sensation in the breast
and the patient finds a lump when feeling the symp-
tomatic area. A lump may be found in the axilla if
there are lymph gland metastases.
The patient may notice a skin dimple caused by
tethering.
The nipple may become retracted, or even
destroyed.
The breast may be noticed to be harder or to have
changed shape.
Swelling of the arm, caused by lymphatic or
venous obstruction in the axilla, is an uncommon
but significant presentation.
Backache, caused by secondary infiltration and
collapse of lumbar vertebrae, with nerve root pains
radiating down the back of the legs, is a common
symptom of advanced disseminated disease, but an
uncommon mode of presentation, as are respira-
tory symptoms from pleural effusions or malignant
infiltration.
A cerebral metastasis may cause a fit.
A pathological fracture may be the first indica-
tion of the presence of the disease.
Curiously, the general symptoms commonly
associated with cancer, such as malaise, weight loss
and cachexia, are rare in patients with breast cancer.
Even those with disseminated fatal disease usually
feel well in themselves (apart from bone pain) until
the final stages.
Family history
Two per cent of women with breast
cancer have the BRCA gene. This declares itself before
the age of 40, and other members of the family will
have been affected, some of them with ovarian can-
cer as well.
Breast cancer is a common disease and so finding
several sufferers in one family is not unusual. Whether
there is a significantly increased risk in those with a
strong family history but without the specific gene
is not yet clear.
Parity
Carcinoma of the breast is more common in
nulliparous women, and less common in women
who have had many children and breast-fed them.
Examination
A technique for examining the breast is described
earlier in this chapter.
Site
Half of carcinomata of the breast occur in the
upper outer quadrant, which includes the axillary tail,
so do not forget to feel this when palpating the breast.
Colour
If the tumour is close to the surface, the over-
lying skin may be discoloured. Tumours fixed to the
skin first give the skin a smooth, reddened appear-
ance, but as the process advances and ulceration is
imminent, the skin becomes paler.
Tenderness
Most carcinomata are not tender, but
palpation may produce a mild discomfort, often
because of the patient’s fear of the consequences of
the surgeon finding a lump.
Temperature
Only the very rare ‘inflammatory’ type
of breast cancer feels warm.
Shape
A carcinoma of the breast may grow into any
shape but in the early stages it is roughly spherical.
The disease may also be multifocal, and it is not
that unusual to find two separate primary tumours.
Surface
The surface is usually indistinct, which
makes it difficult to define the shape except when
the lesion is small. However, a few cancers are
Revision panel 12.4
The cardinal signs of a late cancer of the breast
Hard, non-tender, irregular lump
Tethering or fixation of the lump
Palpable axillary lymph glands
Chap-12.qxd 4/19/05 14:27PM Page 319
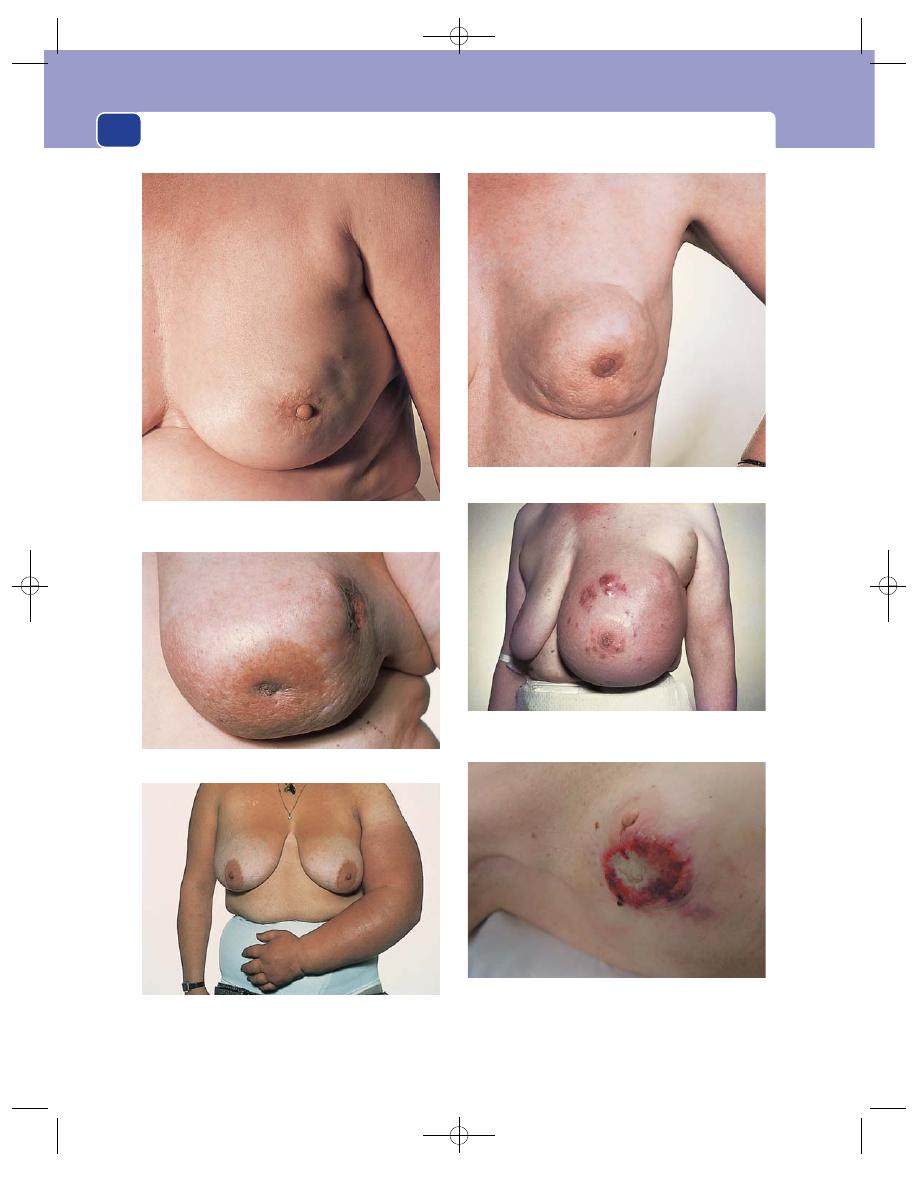
The breast
320
FIG 12.4
SOME DIAGNOSTIC FEATURES OF ADVANCED CARCINOMA OF THE BREAST.
Retraction, deviation and displacement of the nipple.
Puckering and tethering of the skin.
Fixation to the skin and the underlying muscle.
Peau d’orange.
Enlargement of the breast with secondary nodules of tumour
in the skin.
A fungating carcinoma with local secondary tumour nodules
in the surrounding skin. The axillary lymphadenopathy is
visible as well as palpable.
Secondary lymphoedema of the left arm caused by
metastases in the lymph glands.
Chap-12.qxd 4/19/05 14:27PM Page 320
Carcinoma of the female breast
321
encapsulated and have a smooth surface, mimicking
cysts and fibroadenomata.
Composition
Carcinomata are solid, so they do not
fluctuate, transilluminate or have a fluid thrill. Their
consistence is normally quite firm. However, some
tumours are soft, almost as soft as a lipoma, so do
not attribute too much significance to the absence
of a textbook ‘stony hard’ consistence.
Relations to surrounding structures
The terms fixation
and tethering have already been defined. If a lump is
tethered to the skin, it behaves as if it is tied to it by a
piece of string. It can move freely and independently
of the skin within the limits determined by the
length of the string, but pulls the skin when moved
beyond these limits. If a lump is fixed, it cannot be
moved independently.
Fixation of a lump to the skin is almost diagnos-
tic of a carcinoma. The only other condition produc-
ing fixation is traumatic fat necrosis (or, of course, a
pointing abscess, which should be obvious).
A cancer may also infiltrate through the under-
lying muscle into the chest wall. Such a lesion will be
fixed. If neglected, the tumour will invade and con-
sume the whole breast, leaving only a large malignant
ulcer on the chest wall. Such lesions are still seen.
When a tumour spreads along the fibrous septae
of the breast it blocks the lymphatics which run
alongside them. This causes oedema of the overly-
ing skin between the many small pits which mark
the openings of the hair follicles and sweat glands.
The result is an orange-peel appearance known as
peau d’orange.
Lymph drainage
The axillary lymph glands are often
palpable, but this does not necessarily indicate
tumour involvement except when the glands are
very large. They may sometimes be visible.
Lymph glands containing metastases are usually
hard and discrete. As they enlarge, they may mat
together and become adherent to nearby structures
such as the skin, axillary vessels and nerves. They
may eventually become tethered or fixed to the skin,
but by this stage the primary tumour is usually
obvious. Ulceration in the axilla is rare.
Glands may become fixed to the chest wall, par-
ticularly at the apex of the axilla where there is less
space for gland enlargement.
Nearby tissues
Extensive (but not necessarily palp-
able) involvement of the axillary lymph glands may
cause lymphoedema of the arm or venous throm-
bosis and oedema.
The other breast may contain a lump, which the
patient has not noticed. It may be a secondary deposit
or another primary lesion. Do not forget to examine
the axilla on the non-symptomatic side, both to make
a comparison and to look for separate pathology.
General examination
A full general examination is
essential to detect the presence of metastases, which
commonly occur at the following sites.
■
The skeleton – especially the lumbar spine,
causing back pain and reduced spinal movements,
and pathological fractures in long bones. There
may even be paraplegia from cord compression.
■
The lungs – causing pleural effusions. Lung
parenchymal involvement, in the form of diffuse
The International TNM classification
T = Tumour
N = Nodes
M = Metastases
T
1
2 cm diameter or less. No fixation or tethering
N
0
No palpable axillary nodes
N
1
Mobile palpable axillary nodes
N
2
Fixed axillary nodes
N
3
Palpable supraclavicular nodes. Oedema of the arm
M
0
No evidence of distant
metastases
M
1
Distant metastases
T
2
2–5 cm diameter (or less than 2 cm) with tethering or nipple retraction
T
4
Any tumour with infiltration or ulceration wider than its diameter. Tumours larger than 10 cm
T
3
5–10 cm diameter (or less than 5 cm) with infiltration, ulceration or peau d'orange
over the tumour, or deep fixation
FIG 12.5
The TNM classification.
Chap-12.qxd 4/19/05 14:27PM Page 321
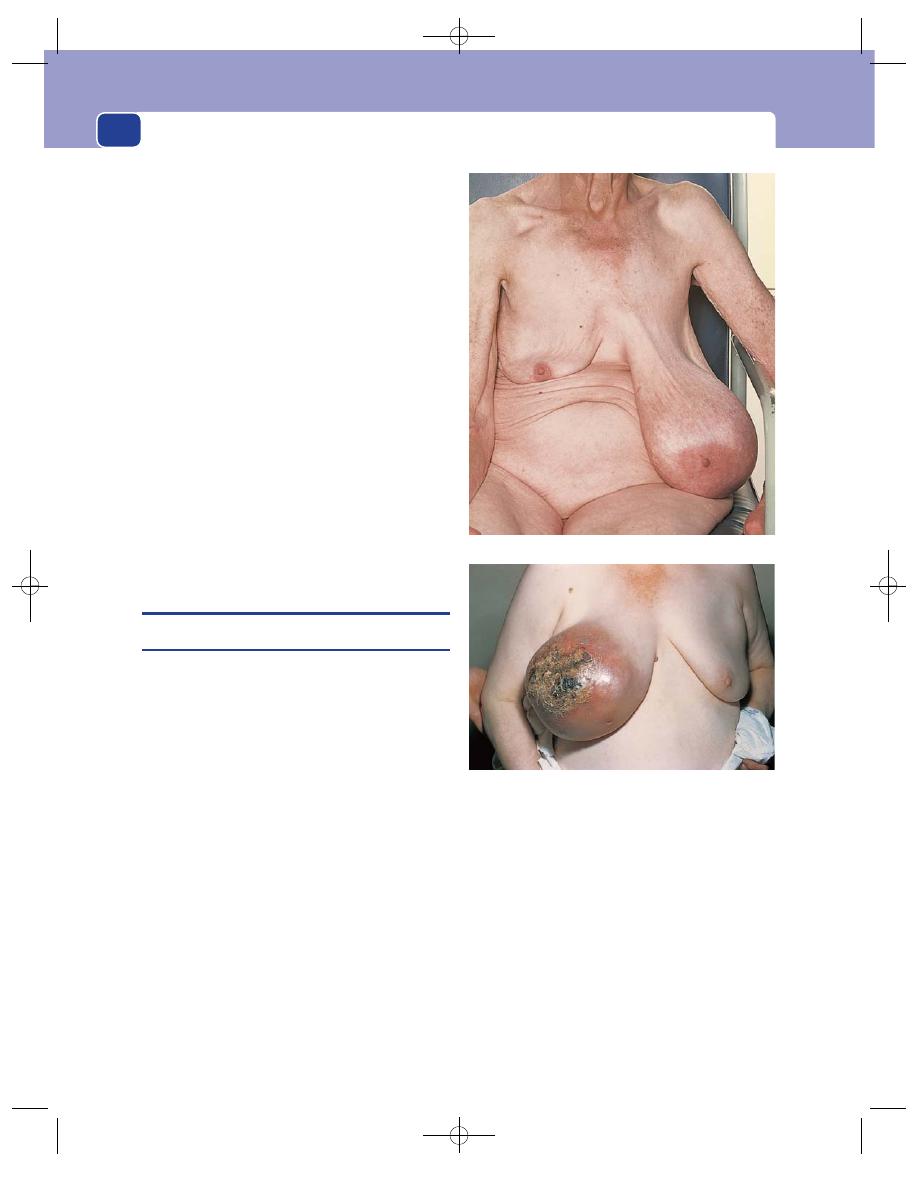
The breast
322
lymphatic involvement known as lymphangitis
carcinomatosa, may cause severe dyspnoea.
■
The liver – making it palpable and causing
jaundice and ascites.
■
The skin – producing multiple hard nodules
within the skin. These are usually in the skin of
the breast containing the cancer, but may be
seen in the neck, trunk and further away.
■
The brain – producing any variety of
neurological symptoms and signs.
Conditions mimicking breast cancer
Fat necrosis
Fat necrosis occurs in the elderly. After
an injury, not necessarily noticed by the patient,
there may be a focal necrosis of subcutaneous fat
with local scarring which causes skin tethering.
There may be a history of trauma or of bruising.
The condition resolves spontaneously.
Mondor’s disease
Mondor’s disease is a thrombo-
phlebitis of the lateral thoracic vein which produces
a cord-like, linear skin puckering that can alarm
patient and clinician. It resolves spontaneously.
BENIGN BREAST TUMOURS
Fibroadenoma
A fibroadenoma is a benign neoplasm of the breast
in which the fibromatous element is the dominant
feature. The cut surface of a fibroadenoma reveals
lobules of whorled, white fibrous tissue which bulge
out of their capsules.
There are two histological varieties of fibroade-
nomata, pericanalicular, which mainly consist of
fibrous tissue, and intracanalicular, which contain
more glands. The former tend to be harder and more
discrete. Clinically the distinction is unimportant.
Most fibroadenomata present in young women,
aged between 15 and the late twenties. They are
seen, however, into the forties and occasionally even
later, but not in the elderly. They grow slowly and
may become quite large. They are then termed ‘giant
fibroadenoma’, but the histological appearance does
not change.
History
The patient presents with a painless lump in the
breast, usually noticed by accident. Occasionally
there is more than one lesion.
Examination
Look out for a mobile, very discrete lump.
Position
It may be anywhere in the breast.
Shape and size
Fibroadenomata are usually spherical or
ovoid, but sometimes lobulated, and may be any size.
Surface
The surface is smooth, the edge definite and
the consistence like firm rubber.
Mobility
Classically the fibroadenoma is the most
mobile of all breast lesions and fully merits the
description of ‘breast mouse’.
A large phylloides tumour (Brodie’s tumour) causing necrosis
of the overlying skin.
FIG 12.6
A giant fibroadenoma of the left breast.
Chap-12.qxd 4/19/05 14:27PM Page 322
Benign breast disease
323
The breast swelling most like a fibroadenoma is a
breast cyst, but cysts are found in a different age
group and are not usually mobile.
Phylloides tumour
This is a rare lesion, first described as cystosarcoma
phylloides or Brodie’s sarcoma. It is not a sarcoma
but may recur locally after simple excision. It does
not metastasize.
It presents as a slow-growing, smooth swelling in
the middle aged, rather like a large fibroadenoma,
from which it is usually only distinguished on hist-
ology. It can be big enough to cause skin necrosis.
Intraduct papilloma
This uncommon condition is a papillary neoplasm
arising from duct epithelium and enlarging into the
duct system. It usually presents with a bloodstained
discharge from the nipple, although there may be a
soft swelling near the areola.
Lipoma of the breast
Lipomata may occur anywhere in the body where
there is fat, which includes the breast, both subcuta-
neously and more deeply seated between the lobules.
Subcutaneous lipomata are just like lipomata else-
where, and there may be others on the trunk or limbs.
If more deeply seated, they may have clinical fea-
tures similar to those of cysts and fibroadenomata.
BENIGN BREAST DISEASE
Most of the conditions which lead women of repro-
ductive age to seek medical advice in relation to their
breasts are not truly a disease process, but reflect or
are exaggerations of the normal pattern of life in
Western civilizations, where women have relatively
few children, relatively late in life, and frequently do
not put their breasts to the purpose for which they
are designed, namely feeding babies.
Biologically, women are able to have children at
regular intervals from the menarche onwards and
could be almost constantly breast-feeding until the
menopause (should they survive that long!). In these
circumstances it is unlikely that so-called benign
breast disease would occur, or perhaps be noticed.
For many years the term chronic mastitis was used
to describe the various symptom complexes seen in
benign breast disease. This is an inappropriate name
because there is no clinical or microscopic evidence
of an inflammatory process; but the term is still heard.
The same is true for many other names used for the
same condition, such as fibroadenosis, fibrocystic dis-
ease and cystic hyperplasia. These names are derived
from the histological features of breast biopsies,
such as fibrosis, adenosis, microcyst formation,
epithelial hyperplasia and lymphocytic infiltration.
Studies of normal breasts have shown that all these
changes are non-specific and are commonly present
in women without breast complaints. They are the
histological manifestations of the dynamic changes
that occur throughout normal reproductive life
during breast development, cyclical menstrual
change, pregnancy and menopausal involution.
It is best when considering the manifestations
of so-called benign breast disease not to apply a
histopathological label to the various symptom pat-
terns seen in clinical practice, but to use simple clin-
ical descriptions.
Most patients’ symptoms fall, with considerable
overlap, into three categories:
■
lumps and nodularity
■
pain
■
cysts.
Lumps and nodularity
History
The symptoms of lumps and nodularity occur dur-
ing the years of ovarian activity, from menarche to
menopause, beginning in the early twenties and
reaching a peak in the thirties.
Revision panel 12.5
The causes of massive enlargement of
the breast
Benign hypertrophy (usually bilateral)
Giant fibroadenoma
Phylloides tumour (Brodie’s disease)
Sarcoma
Colloid carcinoma
Filarial elephantiasis
Chap-12.qxd 4/19/05 14:27PM Page 323
The breast
324
Most patients present complaining of more than
one lump in the breast, which are commonly tender.
It is often the tenderness that draws the patient’s
attention to the lump. The swelling may be inter-
mittent and clearly related to the menstrual cycle,
usually being more obvious in the premenstrual
phase and resolving when the menses begins. The
history is often quite long, as patients are not unduly
concerned by an intermittent swelling which they
correctly conclude is unlikely to be malignant.
Examination
Benign breast lumps can vary from a diffuse nodu-
larity to quite discrete lesions which mimic a cancer.
Begin by assessing the asymptomatic breast to
get some idea of its consistence. There is enormous
variability. In thin women, the lobular structure is
often clearly discernible and the breast tissue may be
picked up and palpated. In women with large
breasts, gravity stretches the breast downwards and
outwards, and the axillary tail may be readily palp-
able as a nodular ridge on each side. Sometimes the
upper border of the firm breast tissue is easily felt
separate from the subcutaneous fat.
Nodular benign lumps tend to be in the upper
outer quadrants and have a moderate hardness,
sometimes described as rubbery. Sometimes the
nodularity is so obvious as to resemble a bunch of
small grapes.
They are not fixed or tethered to skin or muscle.
Comment
Experience is needed to differentiate dis-
crete lesions which might be malignant and require
further investigation, from diffuse swellings which
only require reassurance and perhaps re-assessment
at a different phase of the menstrual cycle. Do not
become discouraged by this difficulty, but try to see
patients with obvious real pathology before attempt-
ing to interpret the more subtle physical signs of
benign breast disease.
Breast pain
Breast pain falls into various patterns and may be
cyclical or non-cyclical.
Cyclical breast pain
Cyclical breast pain is very common. Almost all
women experience it to some degree during their
Revision panel 12.6
A comparison of the clinical features of four common breast lumps
Type of lump
Age (years)
Pain
Surface
Consistence
Axilla
Solitary cyst
35–55
Occasionally
Smooth
Soft to hard
Normal
Nodularity
20–55
Occasionally
Indistinct
Mixed
Normal
Fibroadenoma
15–55
No
Smooth and
Rubbery
Normal
bosselated
Carcinoma
35
⫹
No
Irregular
Stony hard
Glands may
be palpable
Revision panel 12.7
A simplified plan for the diagnosis of the common breast lumps
Define the surface and shape and then define the consistence
Irregular and indistinct
Smooth and well defined
Hard
Rubbery
Hard
Rubbery
Carcinoma
Nodularity
Cyst
Fibroadenoma
Chap-12.qxd 4/19/05 14:27PM Page 324
Benign breast disease
325
reproductive life. It comes on during the second half
of the cycle and is relieved, sometimes dramatically,
when menstruation commences. It is unusual before
the age of 30 and resolves spontaneously in the forties.
Curiously, as it is clearly of hormonal origin, it is
quite commonly unilateral. It may be felt through-
out the breast, or more in the upper outer quadrants.
There may be associated tenderness, sometimes to
the extent that the sufferer cannot bear any pressure
on the breasts at that time in the cycle, even from a
brassiere. The pain is usually reduced by the use of
oral contraceptives.
On examination, there may be tenderness but
no discrete lump. Diffuse nodularity is common,
particularly in the upper outer quadrants.
It is important to appreciate that cyclical breast
pain is never a symptom of cancer. Several large
studies have shown that women with breast pain are
no more likely to have an impalpable carcinoma
than women who do not complain of it, and so no
special investigations are necessary.
Non-cyclical breast pain
Non-cyclical breast pain is less common than cyc-
lical breast pain and has many causes.
Girls at the menarche sometimes experience dis-
comfort during very early breast development.
Women in their twenties may present with a per-
sistently painful, tender area in one breast, but this
usually resolves spontaneously.
Non-cyclical breast pain without any physical
signs is also seen around the menopause and again
resolves on its own.
Elderly women sometimes complain of unilat-
eral breast pain, many years after hormonal activity
has ceased. Careful examination is essential, as very
occasionally there is an underlying cancer, especially
when the pain is described as ‘prickling’.
Breast pain in the elderly is often skeletal in ori-
gin, arising from conditions such as frozen shoulder
and osteoporosis of the spine.
Conversely, very large painful breasts may pro-
duce skeletal symptoms in the neck and shoulder
region, from both abnormal posture and pressure
from brassiere straps.
Tietze’s syndrome is an uncommon condition
in which pain and tenderness arise from a costo-
chondral junction lateral to the sternum. The patient
complains of pain that is exacerbated by movement
and finds what she thinks is a breast lump. Careful
examination will demonstrate that the lump
noticed by the patient is in fact behind the breast
and is part of the chest wall.
Breast cyst
Breast cyst is probably the commonest of the dis-
crete breast swellings.
In pathological terms, a fluid-filled cavity appears
in the breast, without a demonstrable endothelial
lining or a capsule. The condition is age related and
occurs at times when the patient’s hormone environ-
ment is changing, usually around the menopause.
Cysts may be multiple and recurrent.
History
Age
Breast cysts are unusual before the age of 40.
The peak incidence is in the forties and early fifties.
Hormone replacement therapy has extended the age
range, and cysts are sometimes seen in women in
their seventies.
Presentation
They may develop suddenly, the patient,
to their surprise, finding a large swelling that was not
there the day before, and naturally assumes the worst
if this is the first cyst she has had. Moderate pain and
tenderness are common.
Past history
Many patients have had previous cysts
and will be aware that it is worth waiting for a while
before consulting their doctor, as most cysts will
eventually resolve.
Examination
Shape and surface
A solitary cyst is smooth, spherical
and of variable consistence, from soft and cystic to a
hardness equal to cancer. The clinical diagnosis of a
cyst usually rests upon its smooth, spherical shape,
but the swelling may be more diffuse.
Size
Large breast cysts may be visible and even
appear blue or green through the skin, but there will
never be tethering or fixation to skin or muscles.
Consistence
It is rarely possible to elicit fluctuation
or a fluid thrill or to transilluminate the lesion.
Comment
The experienced clinician, having made a
confident clinical diagnosis of a cyst, will proceed
immediately to needle aspiration, the appropriate
treatment. The fluid that emerges is variable in
colour and clarity, varying from very dark green,
Chap-12.qxd 4/19/05 14:27PM Page 325
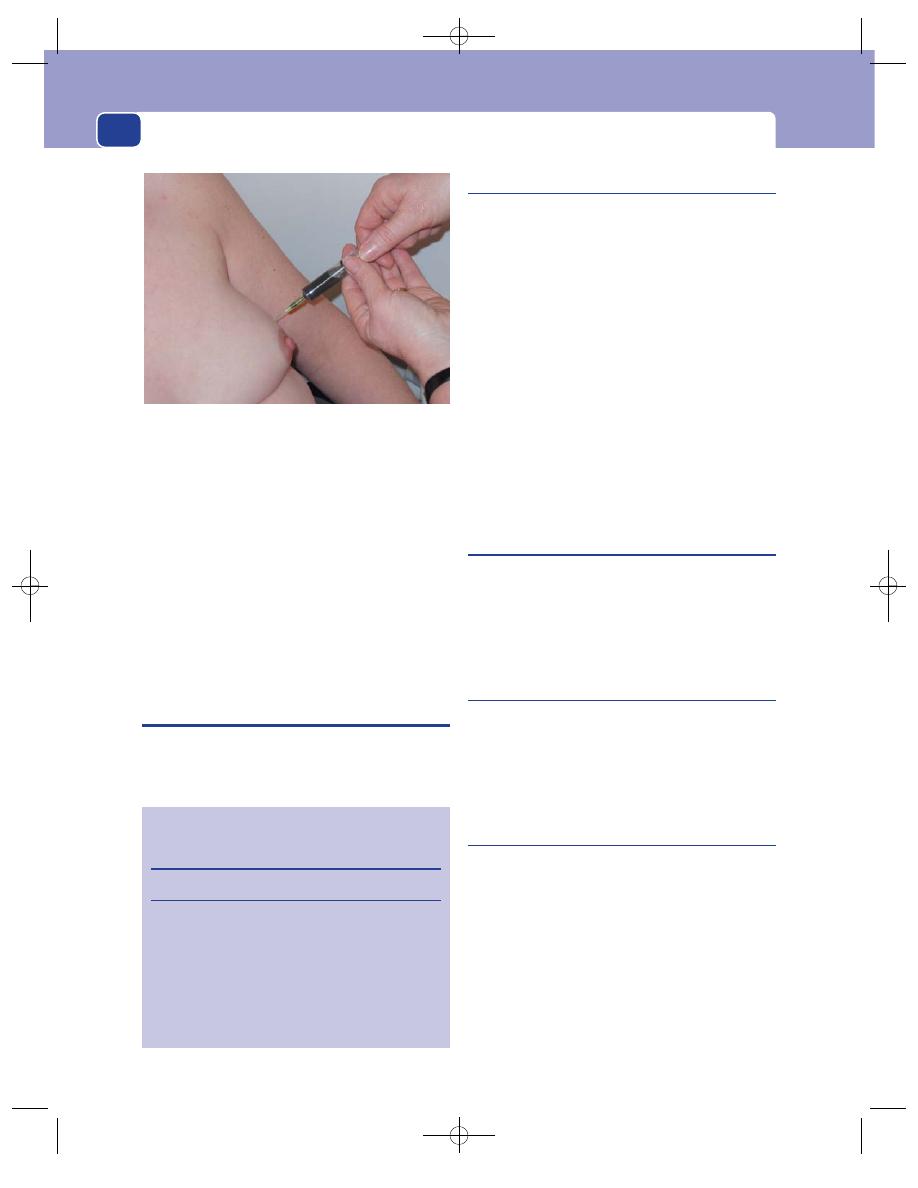
The breast
326
almost black, to clear yellow. There are few more
rewarding (or simpler) surgical procedures than the
aspiration of a breast cyst in a concerned woman.
Occasionally a breast cyst communicates with
the duct system and there is concomitant nipple
discharge. This resolves when the cyst is aspirated or
settles spontaneously.
A galactocele is a milk-containing cyst and
occurs during or shortly after lactation. It presents
as above and the physical signs are similar. Aspiration
produces milk, but the cyst rapidly refills and reso-
lution must await cessation of breast-feeding.
THE NIPPLE
The symptoms associated with the nipple are dis-
charge, inversion and skin changes.
Nipple discharge
Considering that the breast is designed to produce
milk, it is hardly surprising that a fluid discharge is
a common symptom.
It may occur in any age group, but is commonest
during reproductive life. Most women who have
breast-fed can express fluid on request for some
time afterwards, and in most patients seen with this
symptom no cause is ever demonstrated.
The fluid may be thick or thin, cloudy or clear, or
bloodstained. The discharge may be unilateral or
bilateral.
Endocrine causes of nipple discharge are very rare.
Significant causes of nipple discharge include
ductal carcinoma-in-situ (DCIS), duct papilloma
and, most commonly, duct ectasia.
Nipple discharge is rarely associated with inva-
sive cancer.
Nipple inversion
Unlike nipple discharge, this condition is frequently
associated with significant disease and always merits
full assessment. The commonest cause by far is duct
ectasia, but it is a regular presentation of breast
cancer, with or without a palpable lump.
Nipple skin changes
It is fixed in the minds of the public and the profes-
sion that an eczematous rash on the nipple indicates
the presence of a cancer. In fact most patients with a
rash on or around the nipple have a skin disease, not
Paget’s disease of the nipple.
Paget’s disease of the nipple
Paget’s disease of the nipple is caused by cancer cells
migrating or spreading along the duct system from
a carcinoma situated deeply in the breast, which in
the early stages is usually confined to the epithelium
(DCIS).
The presence of carcinoma cells in the skin of the
nipple produces a clinical appearance similar to that
of eczema. Patches of skin first become red and then
encrusted and oozy. The edges of these lesions are
distinct, unlike eczema, and they do not itch,
although the patient may complain of abnormal
FIG 12.7
Aspiration of a breast cyst, a simple clinic procedure.
The aspirant has the typical green colour of a benign cyst.
Revision panel 12.8
The differences between eczema and Paget’s
disease of the nipple
Eczema
Paget’s disease
Bilateral
Unilateral
Commonly occurs
Occurs at menopause
at lactation
Itches
Does not itch
Vesicles
No vesicles
Nipple intact
Nipple may be destroyed
No lumps
May be an underlying lump
Chap-12.qxd 4/19/05 14:27PM Page 326
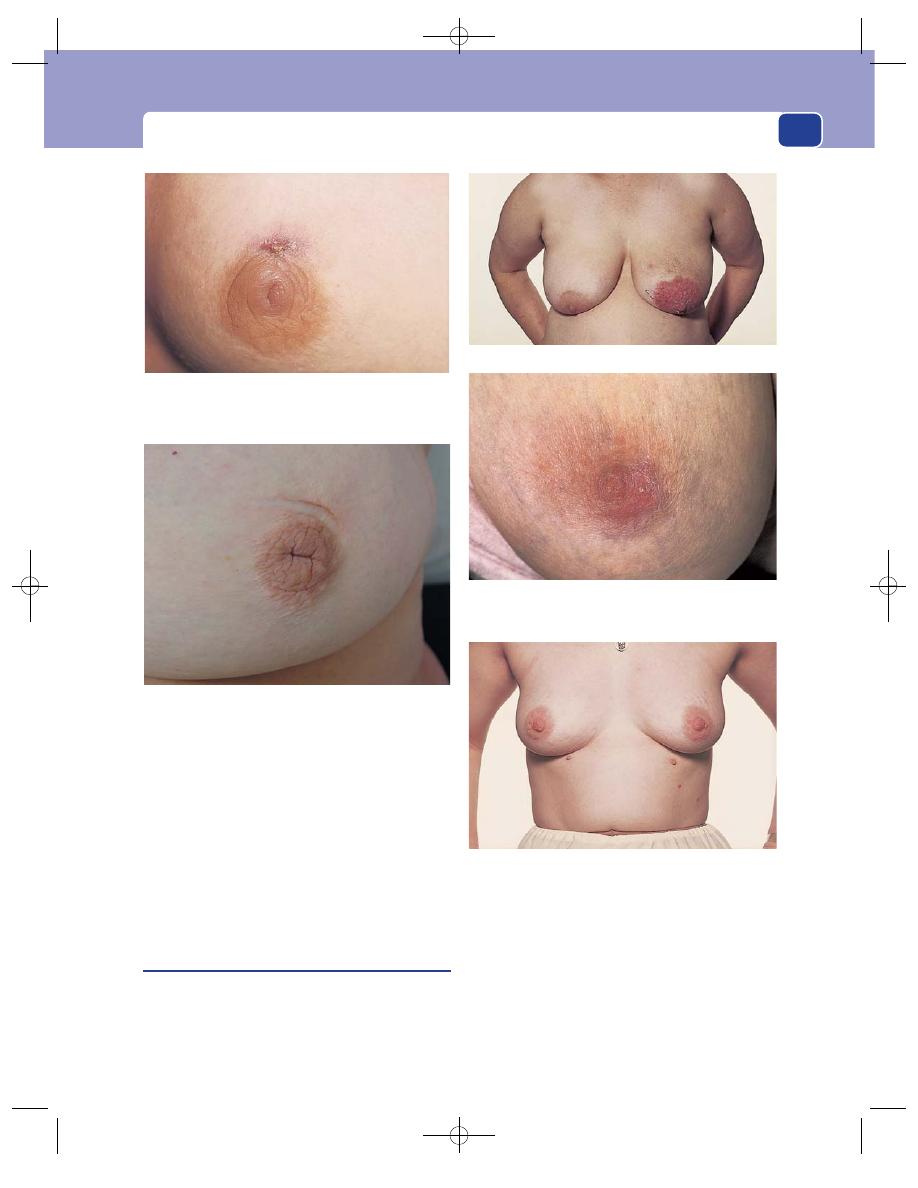
The nipple
327
sensations and prickling. In time the nipple is
destroyed, and replaced by a malignant ulcer.
In the early stages of the disease there may be no
palpable abnormality in the breast, but ultimately
the in-situ carcinoma becomes invasive and a lump
appears.
Never forget that Paget’s disease of the nipple
always indicates an underlying malignant process
in the breast itself.
Duct ectasia
This is a common condition of unknown aetiology
and, as the name implies, the characteristic patho-
logical feature is dilatation of the mammary ducts,
which are full of inspissated material containing
macrophages and chronic inflammatory debris. It
has the following presenting features.
■
Nipple inversion, which is at first mild and
readily everted. There is a characteristic
transverse slit appearance. In many patients this
is the only feature, and as it is mild and
long-standing, it is ignored.
FIG 12.8
A mammillary duct fistula. This tract connects with
a mammary duct. Recurrent infection causes recurrent
acute breast abscesses.
FIG 12.9
The typical appearance of the nipple in duct ectasia.
Note the transverse slit. The scar above the areola is the
aftermath of an incision made to drain an abscess caused by
periductal mastitis.
Florid exudative eczema of the left nipple and areola.
Paget’s disease of the left nipple. The skin of the outer lower
quadrant of the areola is red and slightly thickened. Careful
palpation revealed the mass of a small underlying carcinoma.
Supernumerary nipples.
FIG 12.10
THE NIPPLE.
Chap-12.qxd 4/19/05 14:27PM Page 327
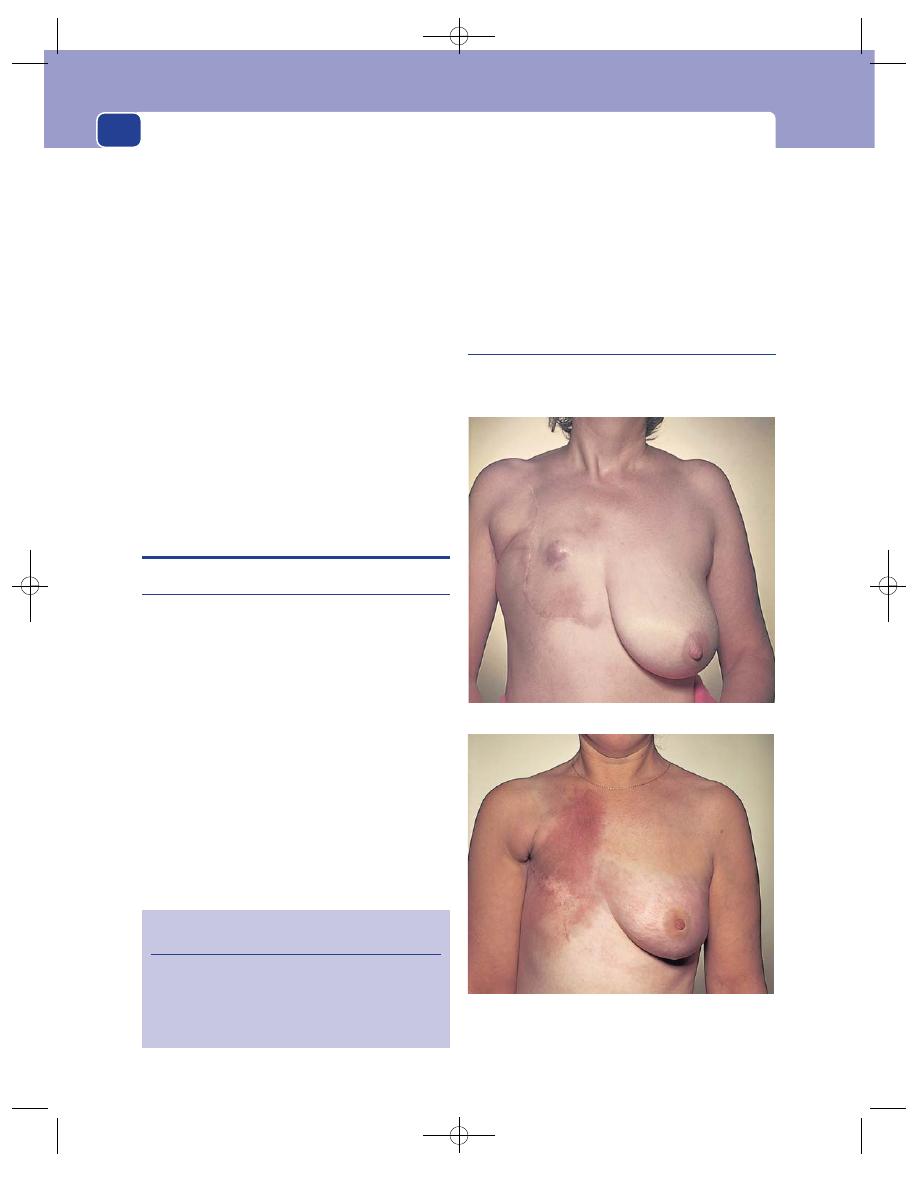
The breast
328
■
Difficulty in breast-feeding because the infant
is unable to apply suction to the partly inverted
nipple.
■
Nipple discharge of sometimes purulent
material from the dilated ducts.
■
Chronic low-grade infection of the
peri-areolar area, with tender thickening around
the nipple, going on to abscess formation, known
as periductal mastitis. This is genuine
inflammation and merits the description
mastitis (unlike the outdated expression
‘chronic mastitis’ mistakenly applied to the
changes of benign breast disease).
■
A periductal abscess that may rupture (or be
drained externally) and stay in communication
with the duct system. This results in a
mammillary fistula and the pathogenesis is
identical to that of the analogous anal fistula
and requires similar principles of treatment.
BREAST ABSCESS
Acute breast abscess
History
Acute breast abscess is often associated with lacta-
tion. Bacteria may gain access to the engorged breast
lobules, an excellent medium for bacterial culture,
via the nipple and duct system or via the circulation.
The patient develops malaise and fever accom-
panied by an ache in the breast which progresses to
an inexorable throbbing pain.
Examination
The infected breast prominently displays the signs
of Celsus, namely rubor, calor, tumour and dolor.
Eventually the abscess will point and discharge
through the skin. There may be very obvious tender
lymphadenopathy in the ipsilateral axilla.
Note: it is safe to continue breast-feeding, even
from the breast containing the abscess. Had the
inflamed area communicated with the duct system,
the infection would have discharged this way and
the abscess would have not have formed.
When a breast abscess occurs in a women who is
not lactating there is often a predisposing risk factor
such as diabetes mellitus or immunocompromise.
Recurrent and chronic breast abscess
Recurrent and chronic breast abscess is usually asso-
ciated with duct ectasia, described above.
Revision panel 12.9
The varieties of true mastitis
Neonatal (caused by maternal hormones)
Milk engorgement during lactation
Diffuse infection during lactation
Mumps
Telangiectases caused by radiotherapy.
FIG 12.11
TWO COMMON APPEARANCES AFTER
MASTECTOMY.
Recurrent nodules in the skin flaps.
Chap-12.qxd 4/19/05 14:27PM Page 328
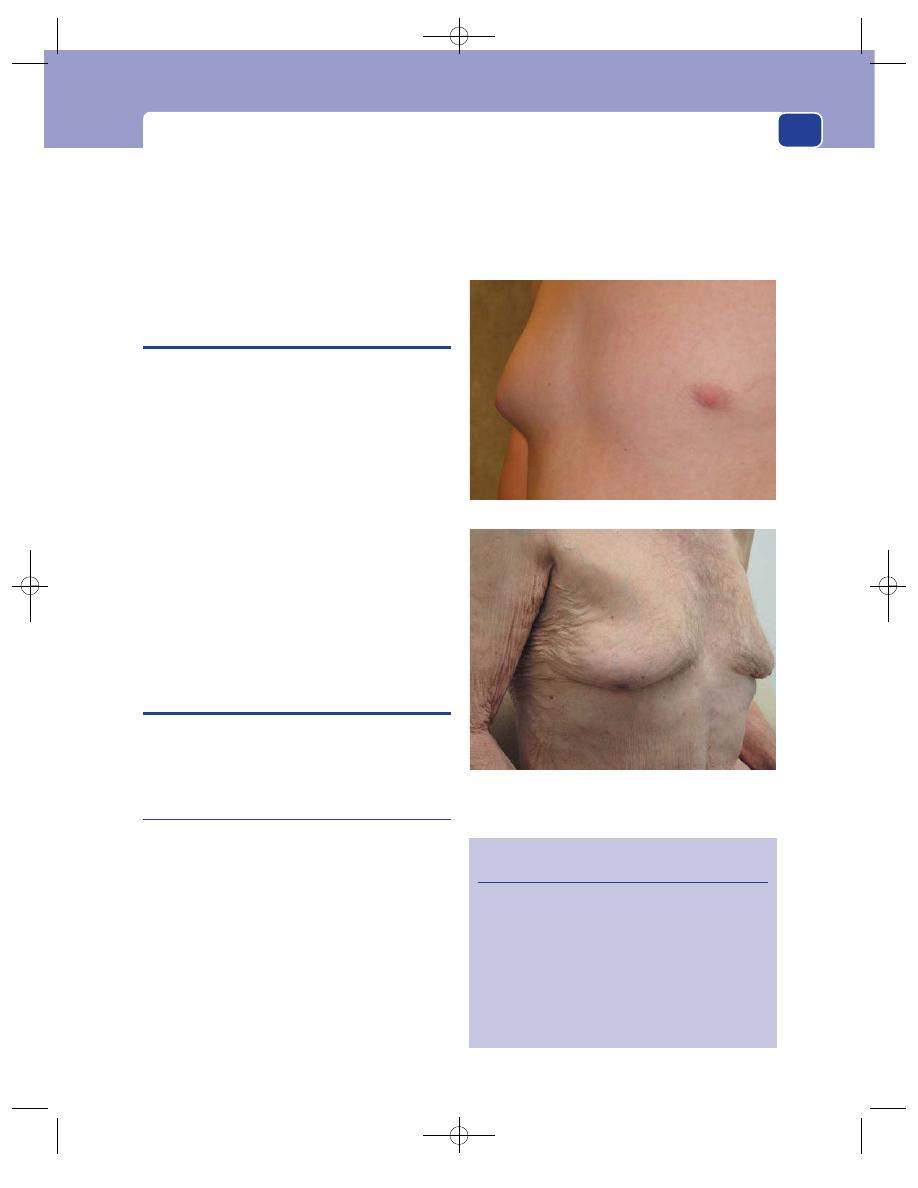
The male breast
329
Tuberculosis of the breast remains common in
some parts of the world and is occasionally seen in
the UK in immigrants.
Granulomatous infections of the breast caused by
atypical mycobacteria are rare but on the increase.
Both forms of infection present with a painless
mass and mimic carcinoma.
PREGNANCY
Pregnancy is always associated with changes in the
breast.
Within a few weeks of the ovum being fertilized,
the breasts become tense, heavy and slightly uncom-
fortable. Many women notice pricking sensations
deep inside the breast.
By 2 months the breasts are enlarged and feel
granular – even ‘lumpy’ – in texture. The subcuta-
neous veins dilate and become prominent, and the
skin of the breasts is warm. The nipples enlarge and
the areolae become darker. The skin around the
areolae may also become slightly pigmented. The
sebaceous glands of the areolae become larger and
the skin over them appears stretched and pale. The
lumps they form are called Montgomery’s tubercles.
By the fourth month, a thin, clear secretion may
sometimes exude from the nipple.
THE MALE BREAST
There are two causes of enlargement of the male
breast: gynaecomastia, which is benign and com-
mon, and carcinoma, which is malignant and rare.
Gynaecomastia
All males have rudimentary breasts. Gynaecomastia is
an abnormal development of both ductal and stromal
elements, with the following patterns of presentation.
■
Transient breast enlargement in male infants
due to ingestion of maternal oestrogens.
■
Early breast development in adolescents,
presumably caused by a temporary imbalance of
adrenal and testicular steroid hormones.
Testicular atrophy and hormone-secreting
testicular tumours are rare causes.
■
Breast enlargement in middle-aged adults is
usually idiopathic, but in some cases is caused
by repeated minor trauma from belts and
harnesses. It is usually bilateral.
■
Breast enlargement in elderly men, almost
invariably caused by drugs. This is often an
expected part of the action of the drug, as in the
Revision panel 12.10
The breast changes of pregnancy
Fullness and pricking sensations
Enlargement
Distended subcutaneous veins
Increased nipple and areolar pigmentation
Circumareolar pigmentation
Hypertrophy of subareolar sebaceous glands
(Montgomery’s tubercles)
A clear, expressible secretion (colostrum)
Bilateral gynaecomastia in an old man.
FIG 12.12
GYNAECOMASTIA.
Unilateral gynaecomastia in a young man.
Chap-12.qxd 4/19/05 14:27PM Page 329
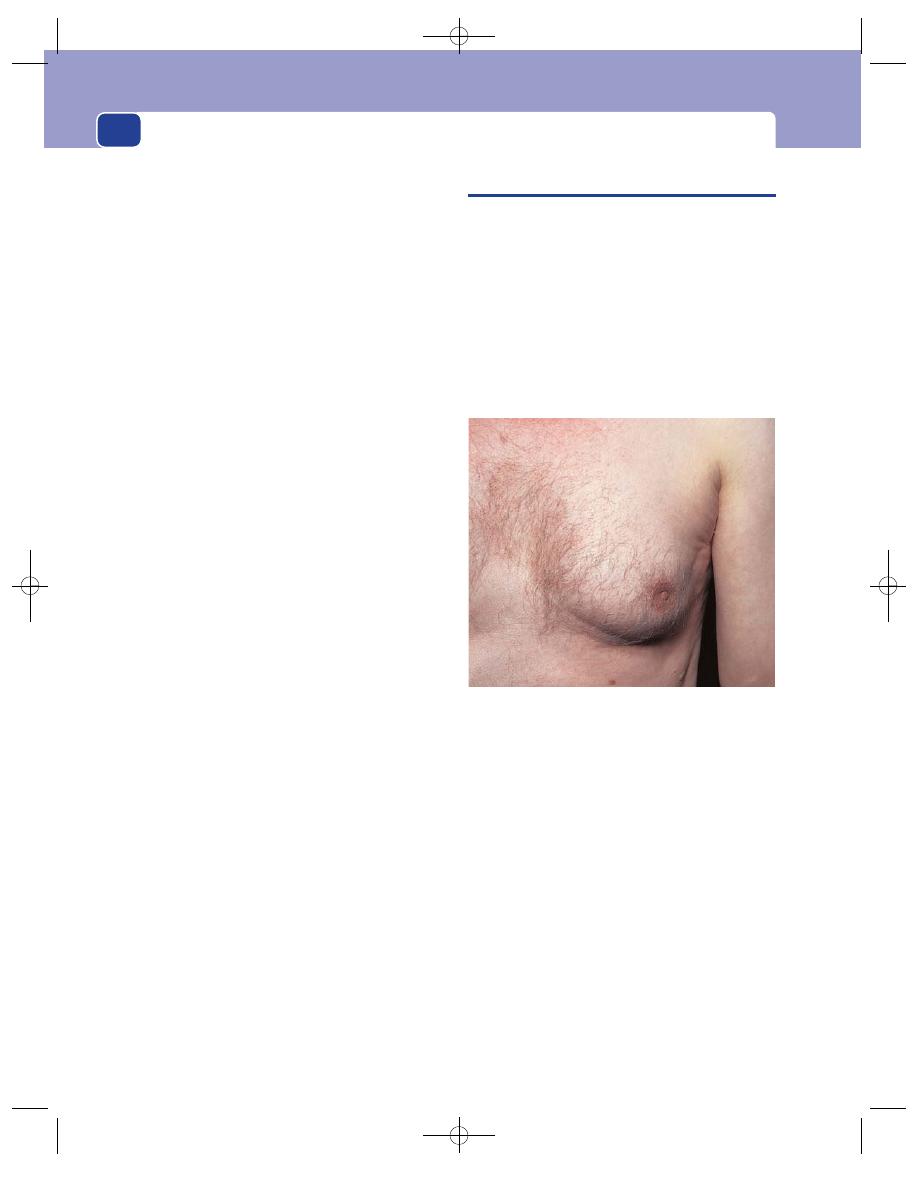
The breast
330
use of oestrogens for prostatic carcinoma.
(A similar effect occurs in younger males
abusing anabolic steroids.)
Gynaecomastia may also be a true side-effect
of histamine antagonists, diuretics and cardiac
drugs. Curiously, it tends to resolve without the
offending agent having to be stopped.
■
A few cases are caused by inappropriate
hormone secretion or metabolism, as may
occur in cirrhosis of the liver and bronchial
carcinoma.
History
The patient complains of painless, or slightly tender,
enlargement of one or both breasts. Schoolboys with
gynaecomastia are often teased by their (so-called)
friends.
There may be a history of a recent illness.
Taking a drug history is essential.
Examination
Sometimes there is a clearly palpable disc of firm
breast tissue behind and attached to the areola and
this is the usual form of gynaecomastia seen in
younger men. Drug-induced breast enlargement
tends to be more diffuse, with a fatty element.
Tenderness is unusual and the axillary lymph glands
will not be enlarged.
A general examination, especially of the abdomen
(liver) and scrotum (testes), may yield information
that indicates the likely cause.
CARCINOMA OF THE MALE BREAST
This is an uncommon condition, usually of elderly
men. Its symptoms and physical signs are identical
to those of carcinoma of the female breast except
that there is little public awareness of the condition
and presentation may be late.
Because the male breast is small and not covered
by a thick layer of subcutaneous fat, the disease
spreads rapidly. Physical signs such as skin and mus-
cle fixation, ulceration and axillary lymphadenop-
athy are often present by the time of presentation.
FIG 12.13
Carcinoma of the male breast. Although the mass
of tumour is relatively small, it has already caused retraction
of the nipple and is fixed to, and dimpling, the skin.
Chap-12.qxd 4/19/05 14:27PM Page 330
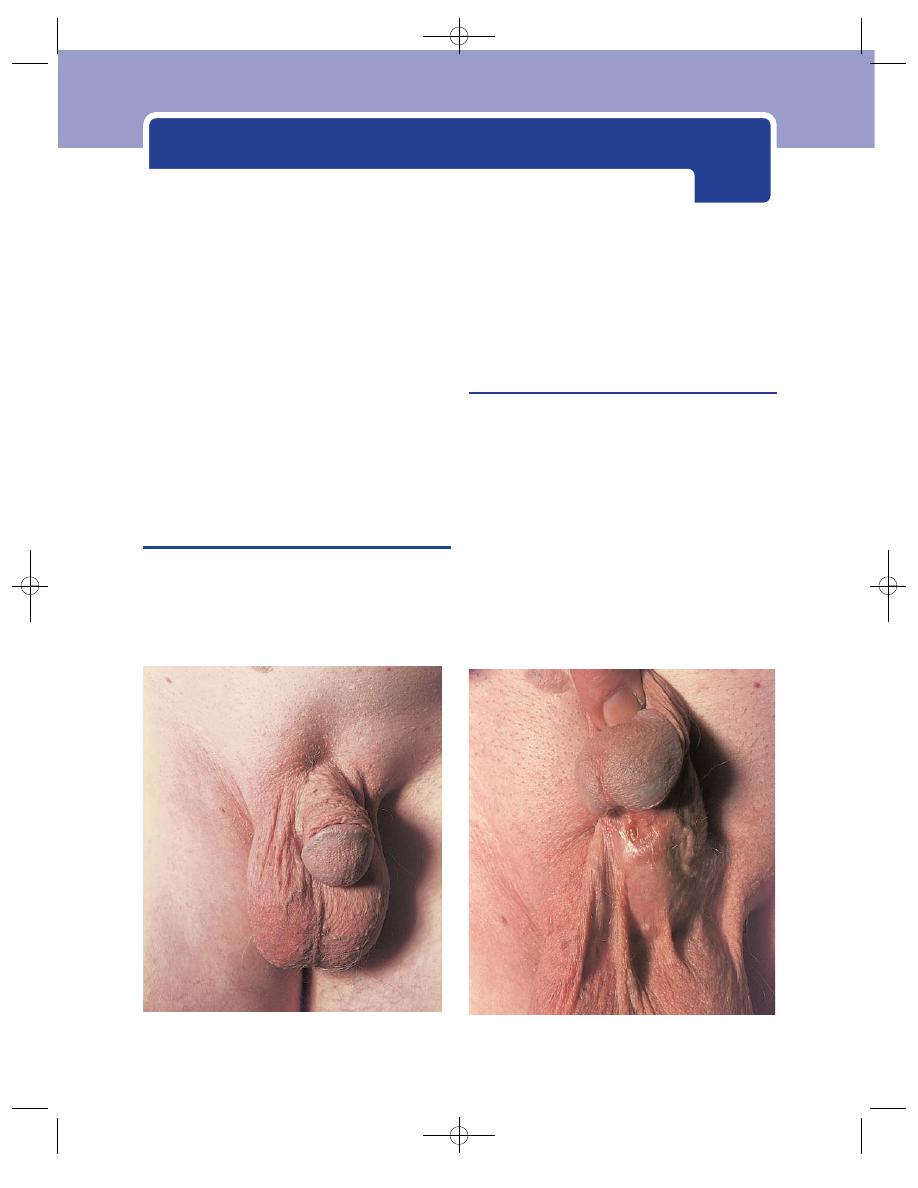
The penis and testes are sensitive organs and diffi-
cult to examine when they are tender. This is espe-
cially true of the testes. You must be very gentle and
careful when examining a tender testis if you wish
to gain your patient’s confidence and elicit all the
abnormal physical signs.
EXAMINATION OF THE MALE
GENITALIA
Always put on protective gloves, especially if there is
any urethral discharge or if you have any suspicion
that the patient is suffering from a communicable
disease.
The penis
Inspection
Note the size and shape of the penis, the colour of the
skin, the presence or absence of the foreskin and any
discharge, scaling or scabbing around its distal edge.
Palpation
Assess the texture of the body of the penis and the
whole length of the urethra right down to the peri-
neal membrane.
Always ask the patient to retract the prepuce to
examine the skin on its inner aspect, the glans penis
and the external urethral meatus. Some patients are
FIG 13.1
Examination of the penis. Always look at the ventral surface of the penis. In this patient it revealed a
hypospadias.
Chap-13.qxd 4/19/05 14:29PM Page 331
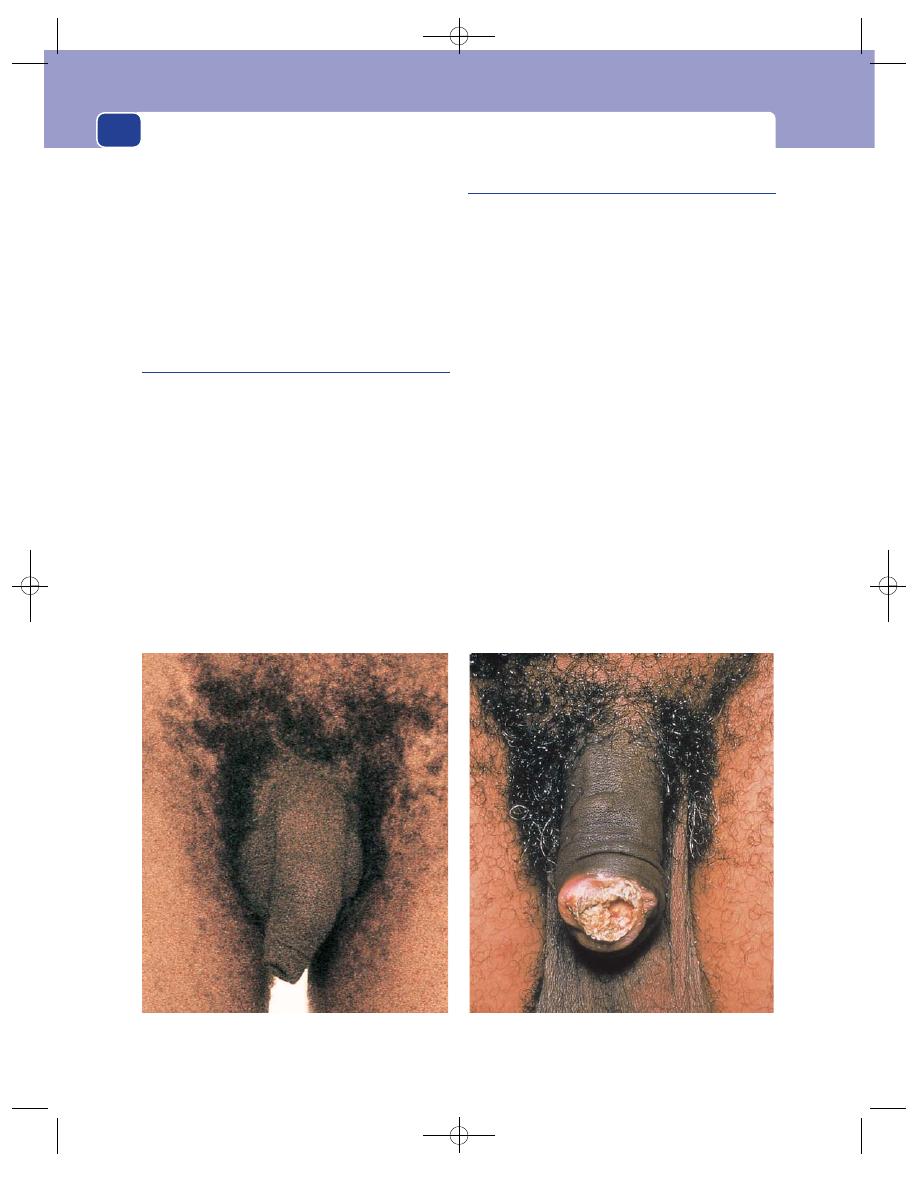
The external genitalia
332
unable or unwilling to do this and the examiner must
take over. This is commonly the case with children.
At birth the foreskin is tethered to the glans penis
with only a small meatus. Do not expect, therefore,
to be able to retract the foreskin of a small child.
Phimosis is a narrowing of the distal rim of the
prepuce, which also prevents retraction. It is seen in
all age groups and, when tight, prevents proper
examination.
The scrotal skin
The skin of the scrotum is usually wrinkled and
freely mobile over the testes. If it is reddened, tethered
or fixed, there is probably a deep abnormality,
but do not forget that the conditions which affect
hair-bearing skin on any other part of the body –
sebaceous cyst, infected hair follicle, and squamous
carcinoma – may affect the scrotal skin.
The scrotum is two-thirds of a sphere. Remember
it has a back and front and do not forget to examine
its posterior aspect.
Should you find a lesion in the scrotal skin, pro-
ceed methodically through your examination of any
lump or ulcer found elsewhere.
The scrotal contents
The shape of the scrotum and the position of the
testes within it can only be observed properly when
the patient is standing up, but it is more comfort-
able for patient and student to perform the major
part of the examination with the patient lying
supine.
Inspection
Note the size and shape of the scrotum, particularly
any asymmetry.
Palpation
The scrotal contents are examined by gently sup-
porting the scrotum on the fingers of one or both
hands, while feeling the testis and any other lumps
between your index finger, which is behind the scro-
tum, and your thumb, which is in front. Do not
squeeze the testis or a lump between your thumb
and index finger – let it slip from side to side so that
you can feel its shape and surface.
First, check that the scrotum contains two testes.
Next, decide the position and nature of the body
of each testis, epididymis and spermatic cords.
FIG 13.2
Examination of the penis. Always retract the prepuce and inspect its inner surface, and the glans penis. In this
patient it revealed a carcinoma.
Chap-13.qxd 4/19/05 14:29PM Page 332
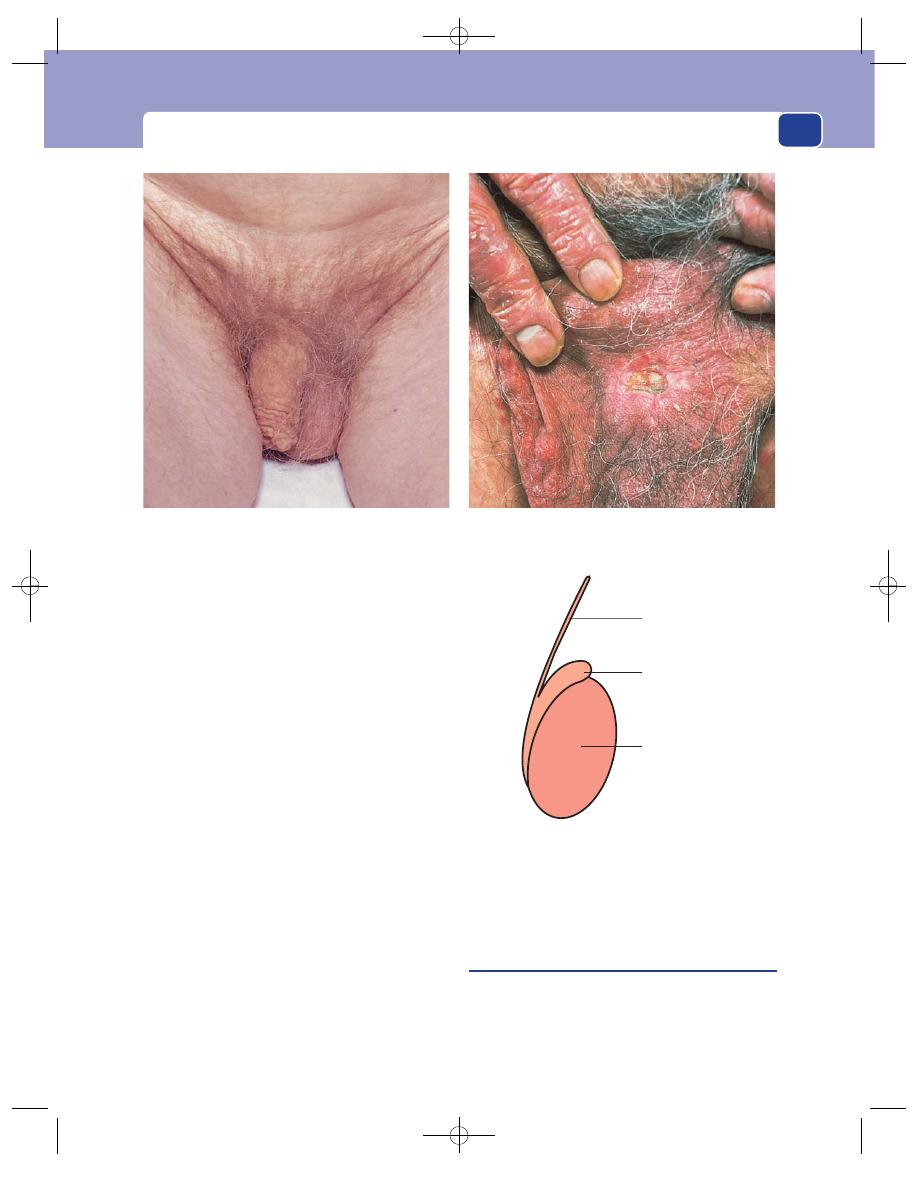
Examination of the male genitalia
333
If you are unsure that what you are feeling is indeed
the testis, ask the patient. The testis has unique sen-
sation and, even with gentle palpation, the patient
will know when you are holding the testis rather
than a similarly sized and shaped swelling.
Assessment of the scrotal contents is one of the last
refuges of clinical assessment alone, without investi-
gation. Armed with knowledge of the anatomy and
the pathology of the scrotal conditions, it is possible
to make an accurate diagnosis in nearly every case.
There are three main characteristics of any scro-
tal lump which you must determine, and which will
be mentioned time and time again in the descrip-
tions of individual diseases.
1. Is the lump confined to the scrotum? (Can you
get above it?)
2. Does the lump transilluminate?
3. Does the lump have an expansile cough
impulse?
If you have established the answers to these three
questions and have defined the physical characteristics
of the lump and its relations to each testis and
epididymis, you will have no difficulty making the
diagnosis. Record your findings on a diagram simi-
lar to that in Figure 13.4.
The perineum and rectum
Examination of the perineum is an essential part of
the examination of the genitalia. Rectal examina-
tion to feel the prostate and seminal vesicles is
obligatory.
FIG 13.3
Examination of the scrotum. Always look at the posterior surface of the srotum. In this patient it revealed a carcinoma.
Cord
Epididymis
Body of testis
FIG 13.4
If you think of the way in which you will draw
the testes, and any abnormality you find, in your notes, it will
help you define the anatomy. Do not stop your examination
until you have defined the position and condition of the cord,
the epididymis and the body of the testes.
Chap-13.qxd 4/19/05 14:29PM Page 333
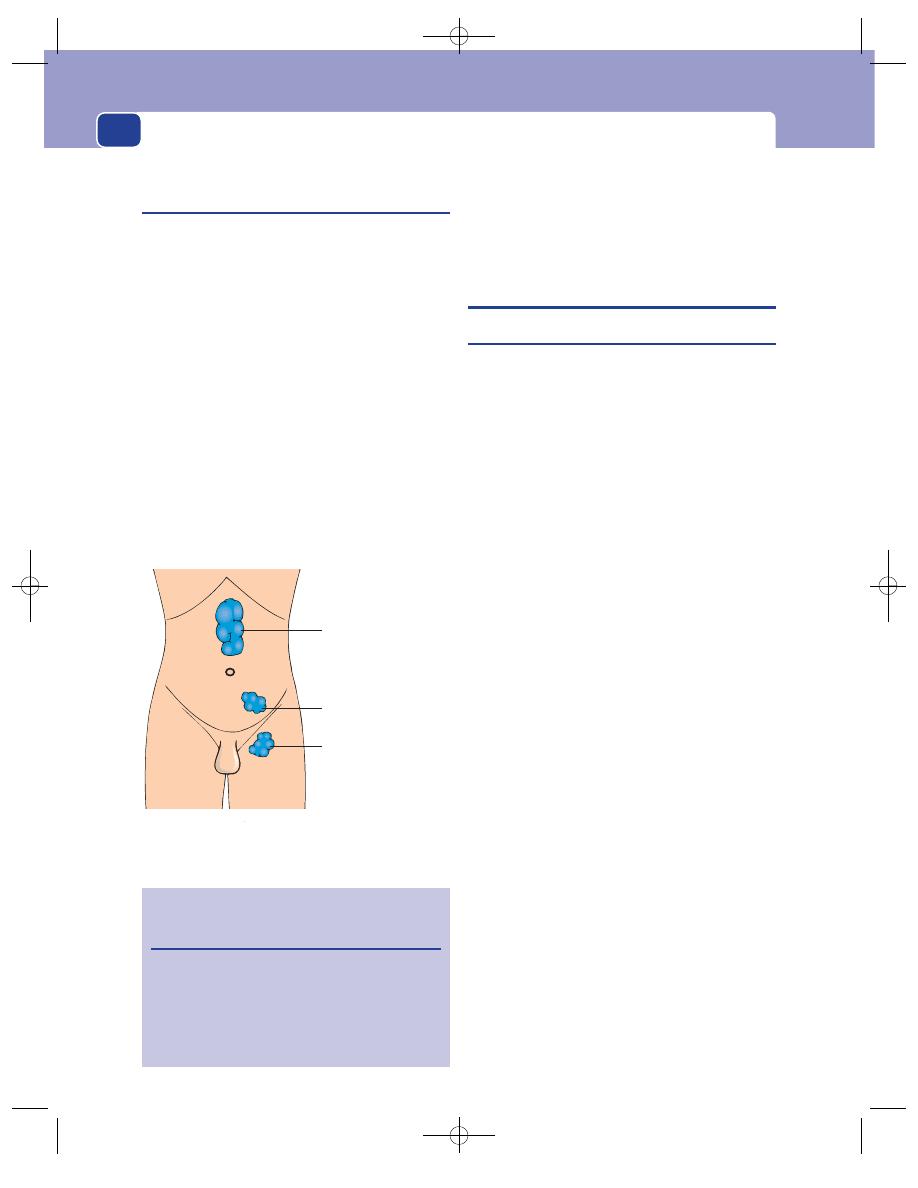
The external genitalia
334
Lymph drainage
(Fig. 13.5)
The skin of the external genitalia drains to the
inguinal lymph glands. The scrotal contents, how-
ever, develop in the para-aortic area in the back wall
of the abdomen. During descent into the scrotum,
the arterial blood supply and venous and lymphatic
drainage follow the testicle. In consequence:
■
lymph from the skin of the penis and scrotum
drains to the inguinal glands,
■
lymph from the coverings of the testis and
spermatic cord (i.e. the tunica vaginalis and
the cremasteric and spermatic fasciae) drains
to the internal and then to the common iliac
glands,
■
lymph from the body of the testis drains to the
para-aortic glands.
The aortic bifurcation is at the level of the
umbilicus; therefore, the abdominal aorta is above
the level of the umbilicus. Thus, enlarged para-aortic
glands are felt in the upper half of the abdomen, in
the epigastrium.
THE PENIS
Phimosis
Phimosis is a narrowing of the end of the prepuce
(foreskin), which prevents its retraction over the
glans penis. It may be congenital, or it may develop
due to scarring of the skin following infection or
trauma.
Natural history of the foreskin
At birth, the foreskin covers and is adherent to the
glans penis. The opening may initially be very nar-
row, like a pinhole. In the first few years of life, the
foreskin gradually separates and widens so that by
the age of 5 approximately 90 per cent of boys are
able to retract it freely and easily. The mechanism by
which this happens is uncertain. Certainly the nor-
mal skin secretions that build up between foreskin
and glans (smegma) play a part, and there is also
stretching from erections and patient curiosity.
It is normal to have a non-retractile foreskin in
early childhood. Even when the foreskin retracts,
adhesions between the foreskin and glans may persist
into the early teens. There is no ‘normal’ age beyond
which failure to be able to retract the prepuce may
be termed abnormal and require treatment, but full
retraction should be possible in all adults.
It could therefore be said that phimosis is the
normal state of affairs in infants but not in adults; so
when does failure to be able to retract become a dis-
ease? This is a grey area, and can cause considerable
parental concern.
There is one variety of phimosis that is clearly
pathological from the beginning, and that is balani-
tis xerotica obliterans (BXO). In this condition,
there is scarring of the tip of the foreskin, presum-
ably due to minor tearing and healing with scarring,
perhaps with some element of low-grade infection
caused by skin organisms. The appearance is char-
acteristic. On gently attempting retraction, whitish,
irregular scarring is seen. The process begins at the
tip of the foreskin but may spread on to the glans
and even narrow the urinary meatus.
The testis drains to
the para-aortic
lymph glands
The coverings of the
testis and the vas
drain to the iliac
lymph glands
The scrotal skin drains
to the inguinal lymph
glands
FIG 13.5
The lymph drainage of the testis, its coverings
and the scrotum.
Revision panel 13.1
Age-related incidence of separation/
retractability of the foreskin
At birth
4%
At 1 year
50%
At 5 years
90%
Note that the majority of non-retractable
foreskins in children do not have a phimosis.
Chap-13.qxd 4/19/05 14:29PM Page 334
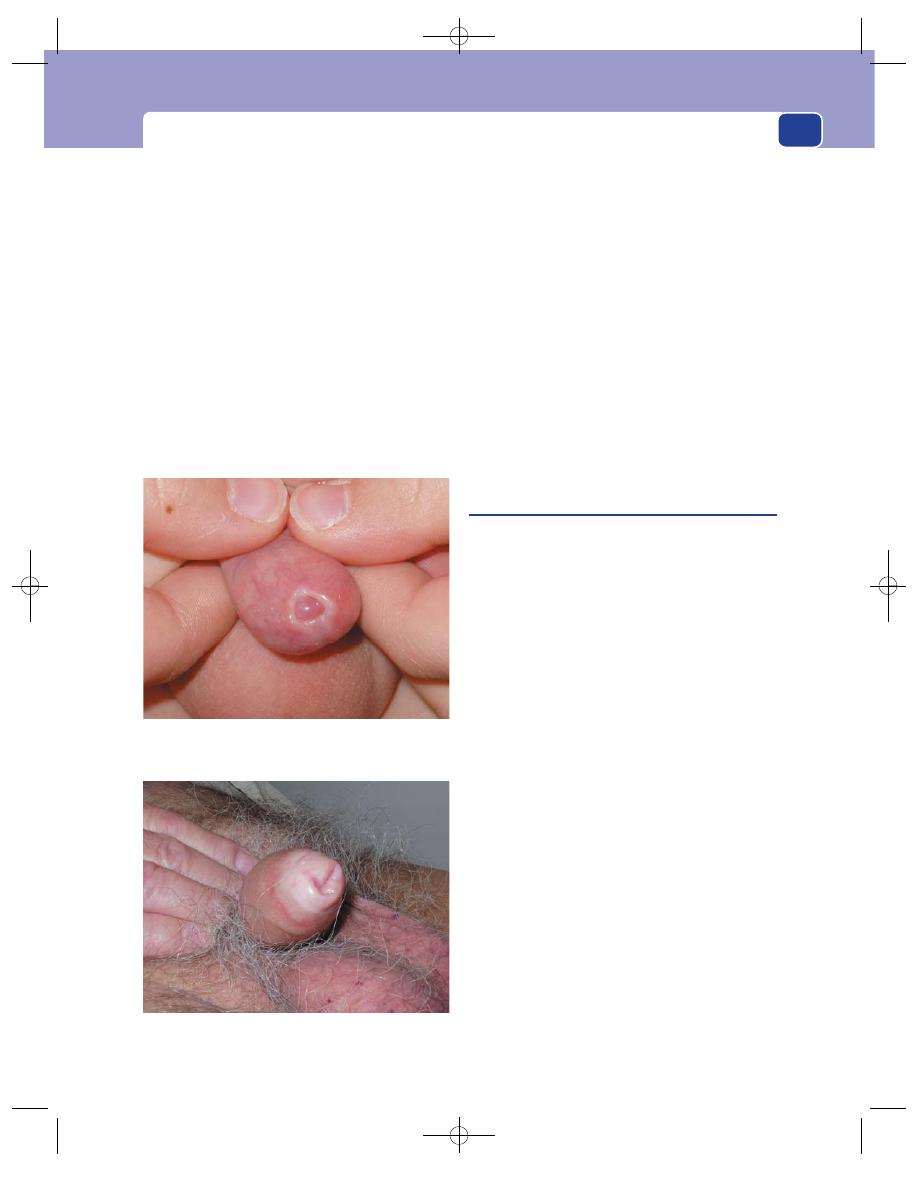
The penis
Symptoms
Ballooning of the prepuce on mictur-
ition may not be abnormal in a young child. It can
only occur when there are no preputial adhesions.
Therefore ballooning is only a sign of phimosis
when there are no preputial adhesions.
Recurrent balanitis (see below) causing pain and
a purulent discharge is a common complication,
but actual urinary tract infection is uncommon,
although sometimes attributed to phimosis.
Similar symptoms may occur in the adult, but
the commonest complaint is of discomfort with
erection and during sexual intercourse. If a tight
foreskin does get retracted, it may not be possible to
pull it forwards again; the patient then has a para-
phimosis (see below).
Examination
In a child, gently draw back the foreskin and look at
the tip. In a normal but narrow foreskin in a small
child, the orifice will be small but the skin will appear
normal. Sometimes as you continue to retract, the
foreskin will not come back completely but skin on
the inside of the prepuce will appear. It is pinker and
more delicate than the skin on the outside, which
has been exposed to friction from clothing. If there
is any balanitis xerotica obliterans (BXO), you will
see a narrow ring of white scar tissue and will be
unable to retract the skin at all.
In children, smegma may build up as yellow
masses visible and palpable through the foreskin.
This appearance may alarm parents and referring
physicians.
Paraphimosis
This occurs when the narrowing of the prepuce is
just sufficiently tight to get stuck behind the glans
penis during an erection, although not necessarily
at other times. In this position it impedes venous
blood flow and causes oedema and congestion of
the glans, which in turn makes reduction of the pre-
puce more difficult.
History
Age
Paraphimosis usually occurs in young men and
is very rare in children. It is a common complication
of urethral catheterization at any age. It is always
preventable by the simple expedient of always
pulling the foreskin forwards over the catheter.
Symptoms
Shortly after the failure of the foreskin to
return to its normal position, there is swelling and
discomfort of the glans penis with a tender, tight
band in the coronal sulcus. It is uncommon for the
urethra to be so compressed that micturition is
obstructed.
Past history
The patient will not usually have been
circumcized, but note that some religious circumci-
sions do not involve removal of the whole of the
prepuce, so recurrent phimosis and hence paraphi-
mosis may occur.
Examination
The diagnosis is usually obvious. The glans penis is
swollen and oedematous and there is a deep groove
335
FIG 13.6
TWO EXAMPLES OF BALANITIS XEROTICA
OBLITERANS (BXO) AND PHIMOSIS.
Phimosis and BXO in an adult.
Phimosis in a child with a ring of BXO. Note the white
scar tissue made prominent as the patient tries to retract
his foreskin.
Chap-13.qxd 4/19/05 14:29PM Page 335
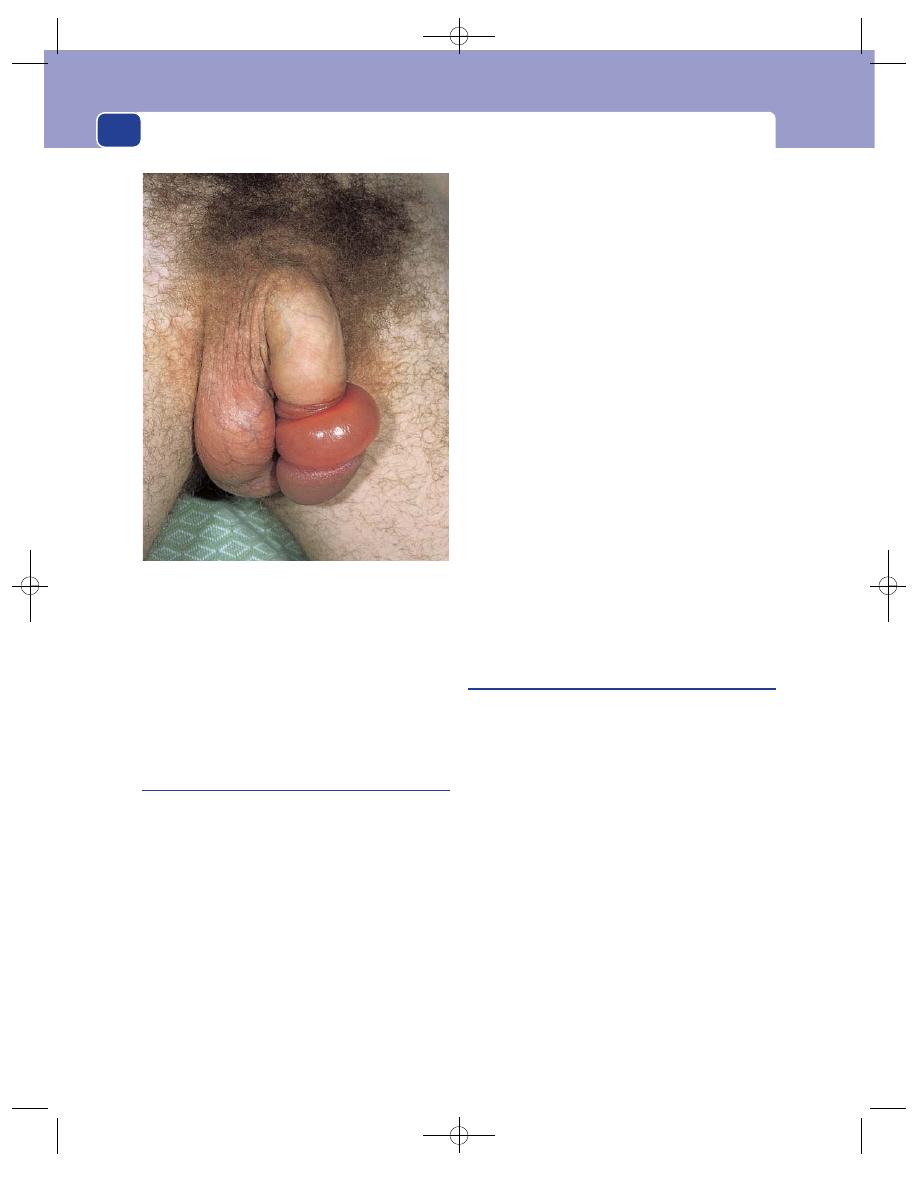
just below the corona where the skin looks tight,
and may be split and ulcerated.
The condition may be chronic, in which case
there may be superficial ulceration and infection of
the skin of the glans penis.
Hypospadias
Hypospadias is a congenital abnormality in which
the urethra opens on the ventral surface of the penis
(i.e. proximal to its usual position at the tip of the
glans penis).
The opening may be anywhere along the line of
the urethra, from a few millimetres from the usual
position at the tip of the penis, to the perineum. If
the urethral opening is in the perineum, the scro-
tum is bifid. The site of the opening may be classi-
fied as glandular (on the glans), penile (on the
shaft) or perineal.
Glandular hypospadias is easy to miss because it
causes no symptoms and there is a deceptive vertical
slit at the normal site of the urethral opening. The
actual meatus may be quite small and a common site
is in the coronal sulcus. Sometimes the parents
notice that during micturition, urine is coming from
this ectopic opening and not the end of the penis,
but quite commonly they do not.
The prepuce has a hooded appearance in hypo-
spadias, because it is deficient ventrally where the
urethra emerges. It is vital never to carry out circum-
cision in a child with any degree of hypospadias, as
the preputial skin may be needed for corrective
plastic surgery.
Chordee is commonly associated with hypospa-
dias. It is a descriptive term for a curved penis.
The curvature is convex dorsally and is more pro-
nounced the further the urethral meatus is away
from the end of the organ. It is caused by the cor-pus
spongiosum being shorter than the corpora caver-
nosa when the urethral opening fails to reach the
end of the penis. It may only be visible on erection.
Chordee in the other direction, convex ventrally,
is seen in adults with Peyronie’s disease.
Epispadias
Epispadias is the opposite of hypospadias. The
urethral opening is on the dorsal surface of the
glans penis. This condition is extremely rare.
Balanitis
Strictly speaking, balanitis is inflammation of the
prepuce, and the correct term for inflammation of
the glans is posthitis. Many patients have inflam-
mation of both prepuce and glans, and therefore
have balanoposthitis, but in practice the only term
used is balanitis.
Symptoms
The patient may complain of itching,
pain or discharge, almost invariably with difficulty
in retracting the foreskin.
Examination
The foreskin appears reddened and there may be a
purulent discharge. In children there will usually be
collections of smegma, which may be visible. Look
for signs of BXO.
In elderly males, remember the possibility that
balanitis may be caused by a carcinoma hidden
beneath the prepuce, so retract it if possible.
Palpate the glans and the inguinal lymph glands.
The external genitalia
336
FIG 13.7
Paraphimosis. The retracted, tight, constricting
ring of preputial skin is causing oedema of the skin distal to
it and congestion of the glans penis.
Chap-13.qxd 4/19/05 14:29PM Page 336
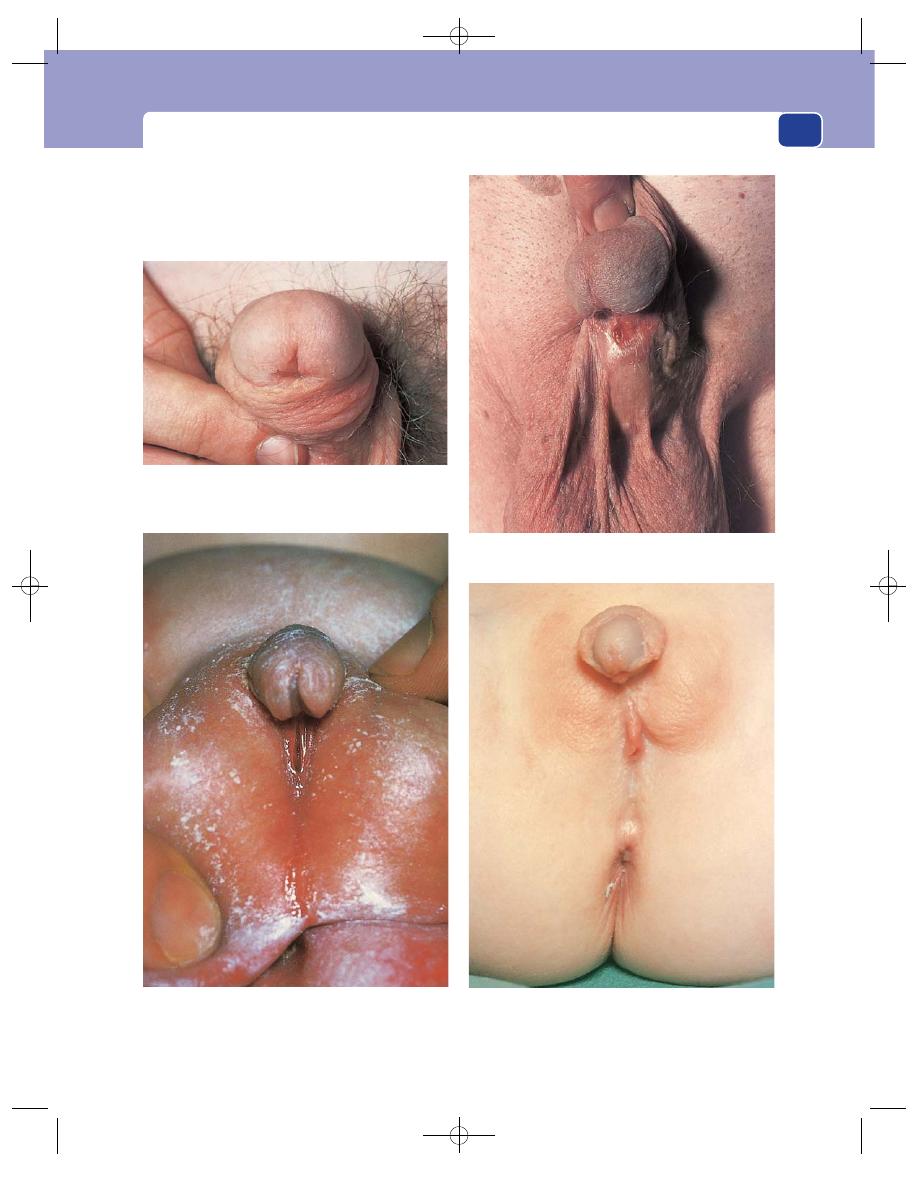
The penis
337
Glandular hypospadias. The urethral opening is on the edge
of the glans penis. The pit where the opening should be is
also visible.
Penile hypospadias. The urethral opening is 1 cm below the
edge of the glans.
Penoscrotal hypospadias. The urethral opening is at the
junction between the shaft of the penis and the scrotum.
Perineal hypospadias. The urethral opening is in the
perineum. The scrotum is bifid.
FIG 13.8
HYPOSPADIAS. Note that the external urethral meatus may be on the glans penis, the shaft of the penis or the perineum.
Chap-13.qxd 4/19/05 14:29PM Page 337
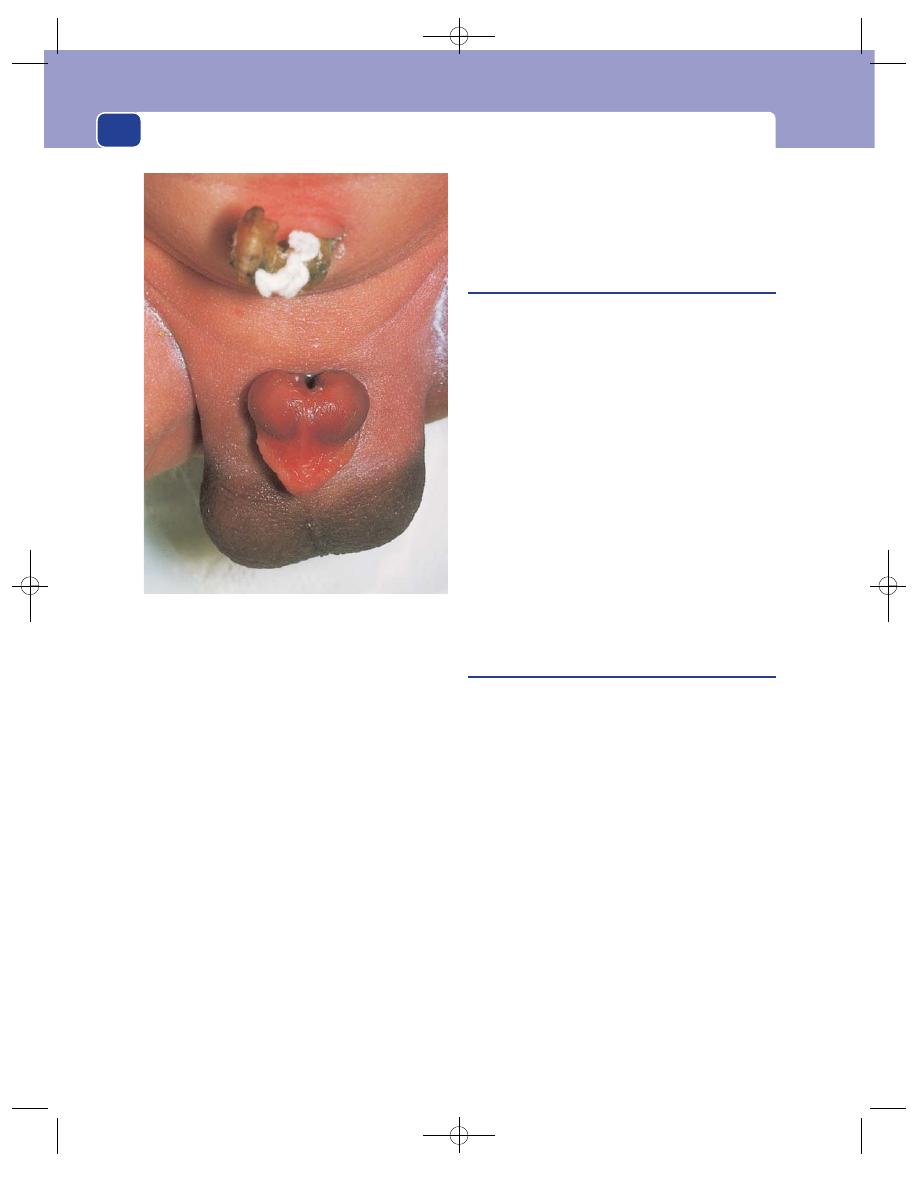
The external genitalia
338
Special types of balanitis
Candidal balanitis is seen in diabetics and in
immunosuppressed patients. The glans penis will
show red patches, which may be itchy. The foreskin
has a white appearance with longitudinal fissuring,
particularly at the tip.
Genital herpes can involve the shaft, glans
or foreskin. The vesicles, initially itchy, are soon
replaced by shallow, painful erosions. Particularly
in the first attack, there may be painful inguinal
lymphadenopathy.
Reactions to drugs
Drug eruptions are usually pain-
less discolourations, most often seen on the glans
penis, and are sometimes the only manifestation of
drug hypersensitivity.
Dirt
Poor personal hygiene with failure to wash
behind the foreskin, particularly in surroundings
with a high concentration of dust and dirt, can
encourage the accumulation of debris beneath the
prepuce. The resulting irritation may cause non-
specific inflammation. Coexisting diseases, such as
diabetes, which render patients more susceptible to
infection, increase the risk of secondary infection.
Syphilitic chancre
In many parts of the developed world, syphilis is
now rare.
The primary sore, known as a chancre, is soli-
tary and always painless. It usually occurs in the
coronal sinus, the prepuce or the frenulum, and
produces a serosanguinous discharge.
Beneath an area of superficial ulceration is an
indistinct, indurated lump, 5–10 mm in diameter.
The ulcer is covered with a slough and has a sloping,
indolent edge. It is not fixed to deeper structures.
The inguinal lymph glands are invariably
enlarged, often mainly on one side. They are rub-
bery and discrete, but not tender.
General examination may reveal no other abnor-
malities, but a primary sore may still be present
should the patient present with the secondary
manifestations of the disease 4–6 weeks after the
appearance of the chancre.
Carcinoma of the penis
Carcinoma of the penis is a squamous cell carcin-
oma. It is exceedingly rare in men who have been
circumcized at birth or in adolescence, as is com-
mon in Jewish and Muslim communities.
It may be preceded by a number of pre-malignant
conditions described below. It invades from the
penile skin into the tissues of the shaft of the penis
and spreads via the lymphatics.
History
Age
Carcinoma of the penis commonly presents in
middle or old age, but can, rarely, occur in young men.
Ethnic group
Carcinoma of the penis is more common
in cultures that do not practise ritual circumcision.
Symptoms
Most patients present with a lump or an
ulcer. The lesion may be painful, especially if it is
infected.
There is usually a purulent discharge, which
may be blood stained.
FIG 13.9
Epispadias. The urethra opens on the dorsum of the
glans penis, almost on the dorsal aspect of the shaft of the
penis.
Chap-13.qxd 4/19/05 14:29PM Page 338
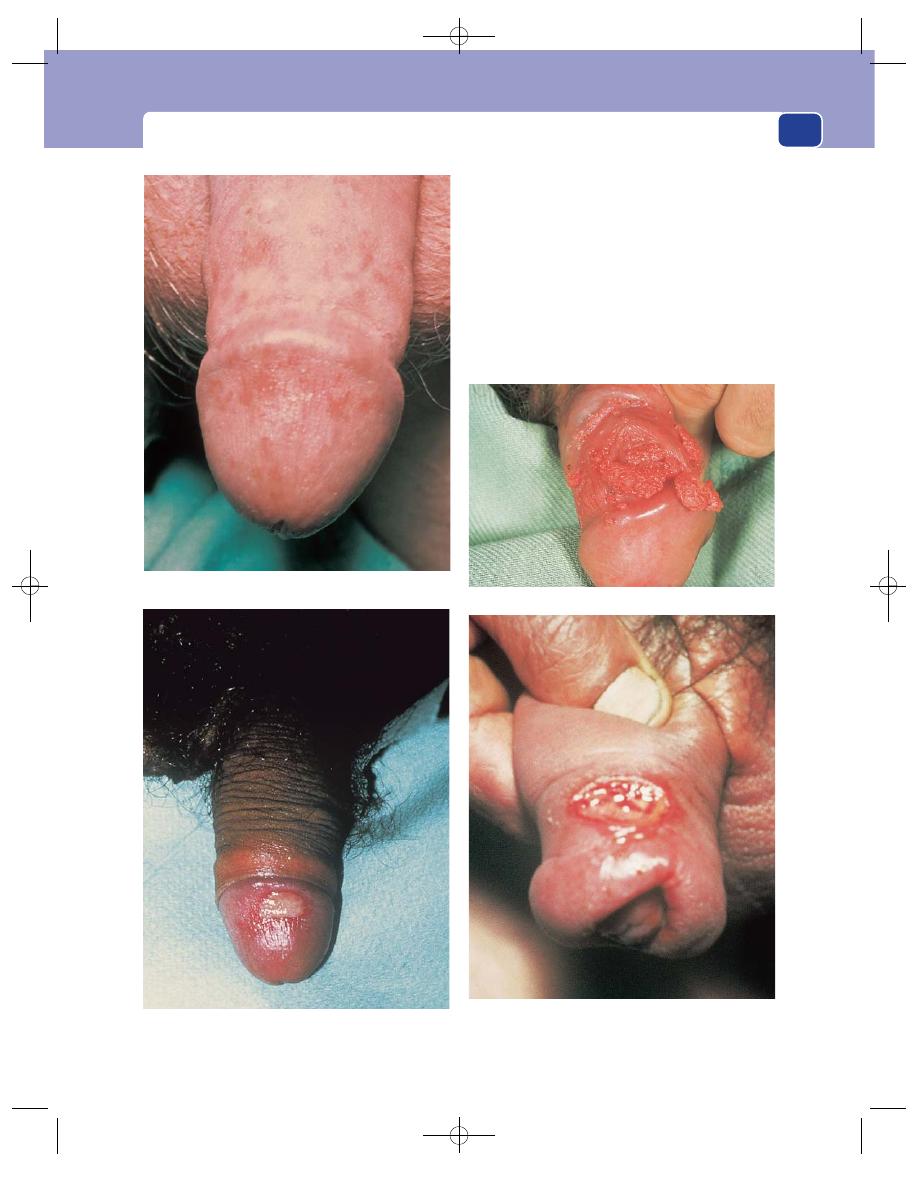
The patient may also complain of phimosis. In
these circumstances the primary lesion can become
quite advanced before it is detected.
The inguinal lymph glands may be enlarged by
secondary infection or secondary deposits and may
be the first abnormality noticed by the patient.
Presentation with distant metastases is rare.
The occasional patient ignores his symptoms
until the tumour compresses or invades the urethra
and urinary retention occurs.
The penis
339
A syphilitic chancre on the inner surface of the prepuce. (The
ungloved hand is that of the patient.)
FIG 13.10
FOUR COMMON PENILE CONDITIONS.
Monilial balanoposthitis.
A drug eruption. This ulcer was part of a reaction to Septrin.
Penile warts.
Chap-13.qxd 4/19/05 14:29PM Page 339
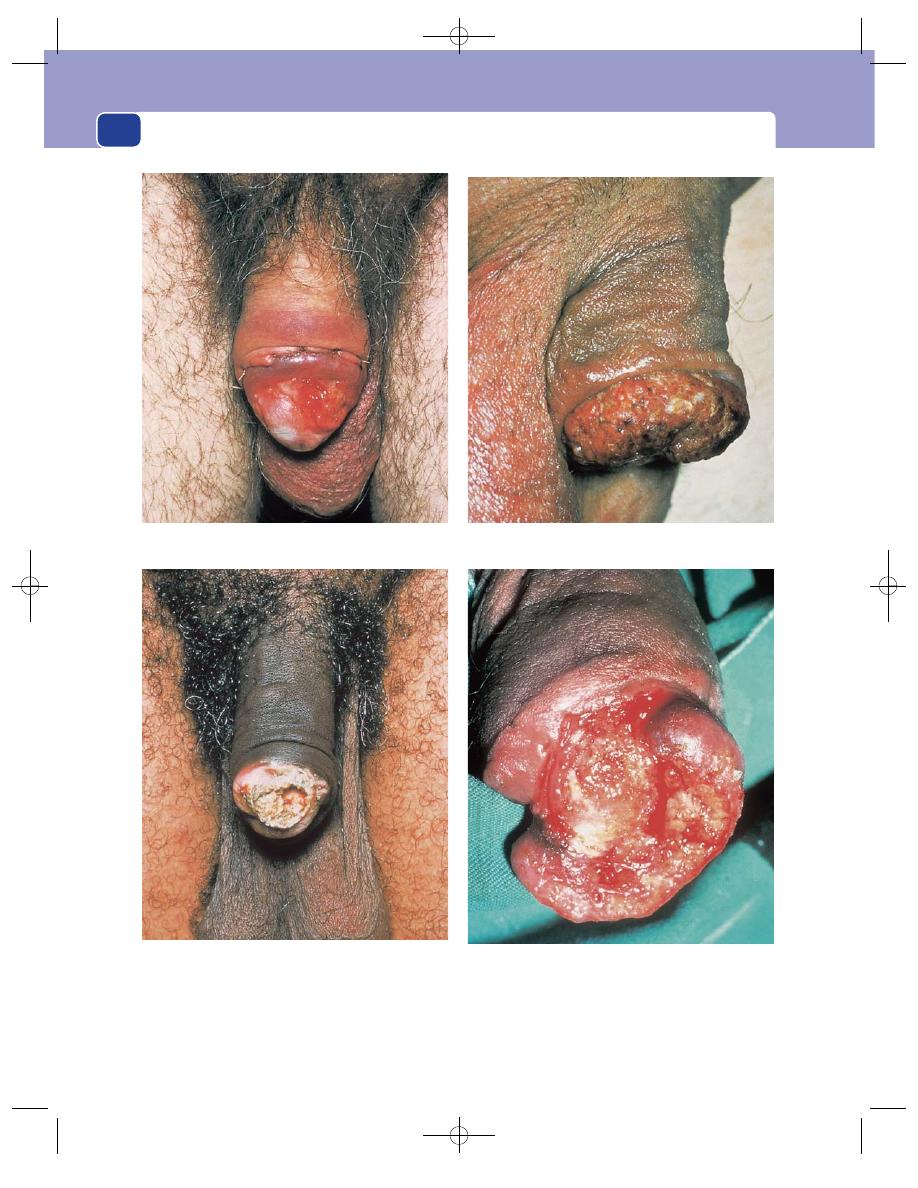
The external genitalia
340
FIG 13.11
CARCINOMA OF THE PENIS.
An early carcinomatous ulcer on the glans penis, exposed by
a circumcision.
An advanced infiltrating carcinoma which has invaded the
whole thickness of the prepuce.
A papilliferous carcinoma arising in the coronal sulcus.
An ulcerating carcinoma that has destroyed half of the glans
penis.
Chap-13.qxd 4/19/05 14:30PM Page 340
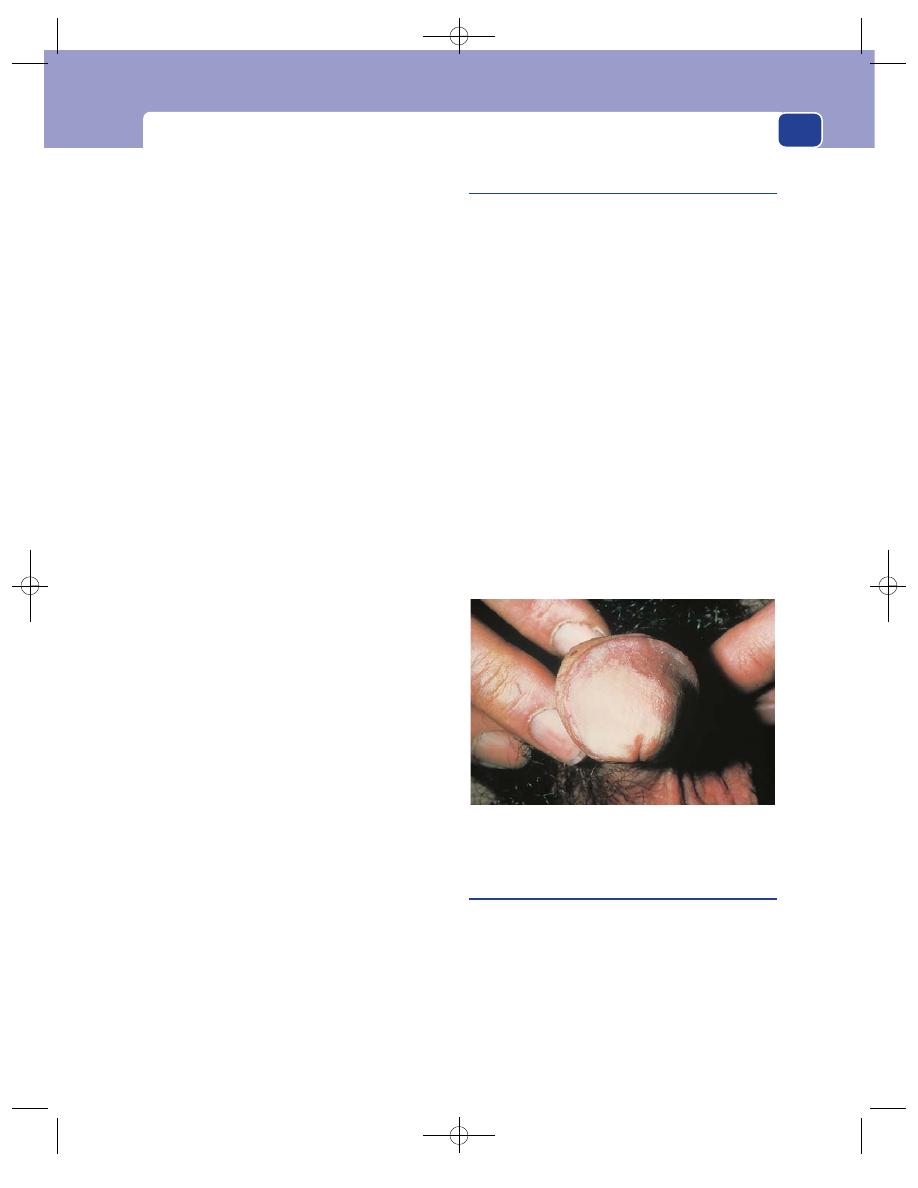
The penis
341
Examination
Prepuce
The patient is most unlikely to have been
circumcized, and in the UK is commonly elderly
and self-neglected. There may be a serous, purulent
or sanguinous discharge coming from beneath the
prepuce. If the foreskin cannot be retracted, full
examination of its inner surface and the glans penis
may require a surgical slit.
Deformity
The penis may be swollen at its tip
owing to the mass beneath the prepuce. In the
advanced stages the tumour may appear through
the opening in the prepuce or erode through the
preputial skin.
Position
The lesion may be anywhere on the skin of
the prepuce or the glans penis.
Tenderness
The lump or ulcer is not usually tender,
except when secondarily infected.
Shape
Carcinoma of the penis tends to adopt one
of two macroscopic forms: a classic carcinomatous
ulcer with a raised everted edge and necrotic base,
or a papilliferous tumour with a wide sessile pedi-
cle and an indurated base. The microscopic patho-
logy is the same.
The shape simply reflects the degree of tumour
necrosis.
Size
Most patients appear early in the course of the
disease provided they can retract their foreskin. If
they have phimosis, and have grown accustomed to
an occasional discharge, they may not present until
the tumour is large or visible.
Composition
The tumour has a hard consistence,
especially at its base. Any part of the penis that is
infiltrated also feels hard. The surface of the papillif-
erous variety is soft and friable. It often looks like
granulation tissue, and bleeds easily.
Relations
In the early stages the tumour is confined
to the skin, but it may invade and spread through
the whole corpus cavernosum, making it indurated
and hard, and if it begins on the inner side of the
prepuce, it may spread to and through the outer
layer of skin.
Lymph drainage
The inguinal lymph glands of both
groins are likely to be enlarged, by infection or sec-
ondary deposits.
Skin conditions of the penis
Various skin conditions are associated with an
increased incidence of carcinoma of the penis, and
the underlying pathological condition is called
intraepithelial neoplasia. This is the same as that
seen in the female genital tract in the cervix and
vulva, and also in the peri-anal skin.
It is now appreciated that various clinical
appearances, often classified by their colour (e.g.
leukoplakia) or the name of the physician who fist
described them (e.g. Paget’s disease or the erythro-
plasia of Querat), have essentially the same patho-
logy. The student needs to remember that any
chronic skin eruption on the penis might be penile
intraepithelial neoplasia (PIN) and should be
assessed and treated accordingly.
Clinical diagnosis is difficult because any skin
disease may occur on the skin of the penis. Lichen
sclerosis particularly mimics intraepithelial neo-
plasia.
Viral warts are common and behave as they do
elsewhere in the body.
Priapism
Priapism is a persistent, usually painful erection.
There are two varieties, primary and secondary.
Secondary priapism is caused by a haematological
disorder which triggers thrombosis of the corpora
cavernosa, such as leukaemia or sickle-cell disease,
or by obstruction to the venous and lymphatic
drainage of the penis by pelvic malignancy. Presenta-
tion is part of a generalized advanced illness.
FIG 13.12
An example of penile intraepithelial neoplasia
(PIN). This variety is commonly called leukoplakia.
Chap-13.qxd 4/19/05 14:30PM Page 341
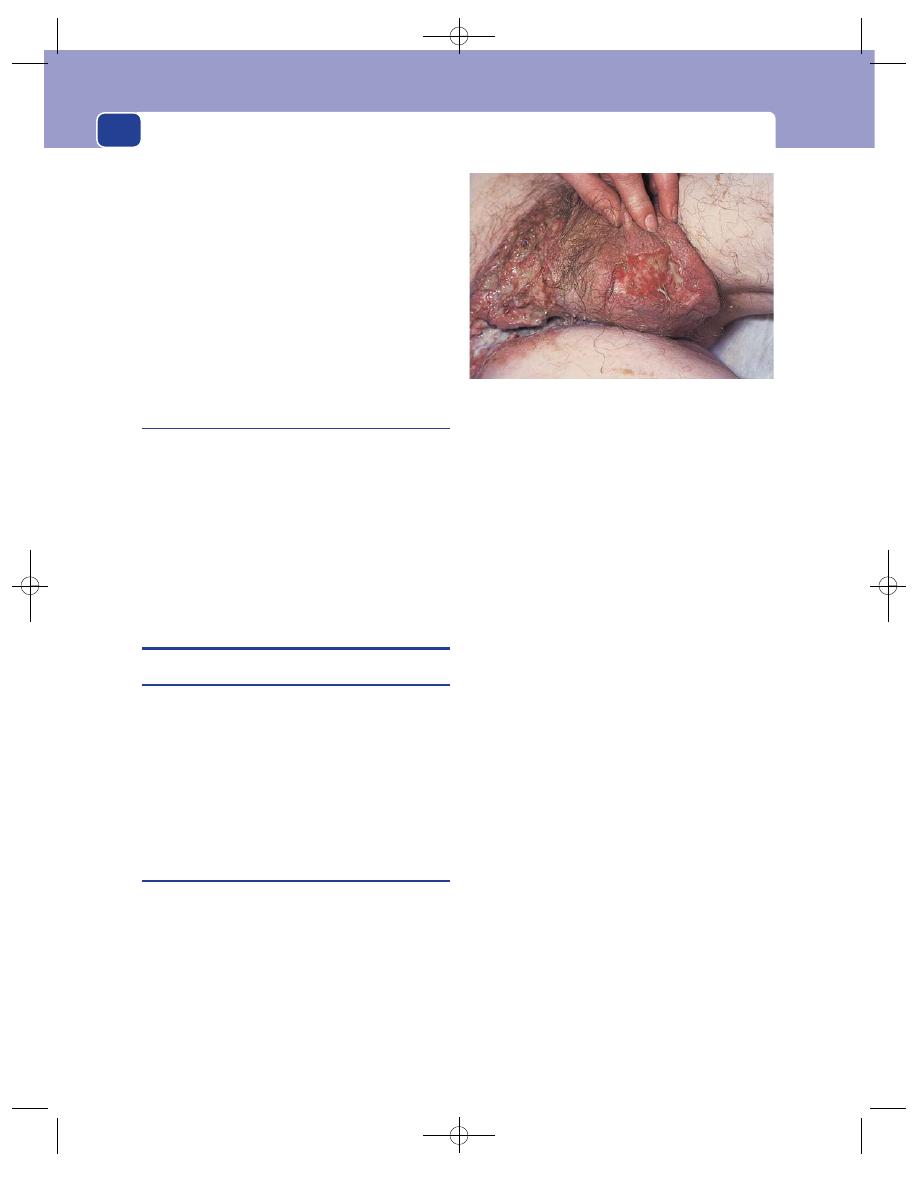
The external genitalia
Primary idiopathic priapism is seen in previ-
ously fit men after sexual activity. It is usually
caused by a failure of the venular spasm that sus-
tains the erection to relax. Because of embarrass-
ment, presentation may be late.
The erection seen in priapism is not of the
normal pattern and shape. It is confined to the cor-
pora cavernosa and may affect only one side, pro-
ducing a lateral chordee. The corpus spongiosum
remains soft.
Without immediate surgical treatment, impo-
tence will result.
Peyronie’s disease
This is an idiopathic plaque of fibrosis in one of the
corpora cavernosa, usually on the dorsal side. It
occurs in middle-aged men. The symptoms are pain
and a curvature of the penis when erect. It rarely
interferes with sexual intercourse. The plaque may
be palpable when the penis is flaccid.
The differential diagnosis includes metastatic
tumour deposits, but this is a rare event and the
patient will usually be clearly unwell.
THE SCROTAL SKIN
Sebaceous cysts
Sebaceous cysts are common in the scrotal skin
and are often multiple. They have all the fea-
tures described in Chapter 3 but are mentioned
here because it is surprising how often they are
misdiagnosed.
Occasionally they can become infected, dis-
charge and produce so much granulation tissue that
they look like a carcinoma.
Carcinoma of the scrotal skin
This is a squamous carcinoma. It can be caused by
frequent contact with soot (chimney sweep’s can-
cer), tar or oil (mule spinner’s cancer). The skin
must be exposed to these irritants for many years
before a cancer develops.
History
Age
Carcinoma of the skin of the scrotum is
uncommon below the age of 50 years.
Occupation
The patient’s occupation may be respon-
sible for frequent soiling of the scrotal skin with oil
and other carcinogenic hydrocarbons. Even today,
the clothes of garage mechanics and machine oper-
ators become soaked in oil, which percolates
through to their underclothes.
Symptoms
Most patients present with a lump or an
ulcer or a lump. A purulent discharge may appear,
and if the ulcer is hidden in the cleft between the
scrotum and leg, the discharge may be noticed
before the ulcer.
The patient may notice lumps in the groin if the
inguinal lymph glands are involved.
Examination
Position
A carcinomatous ulcer can occur on any
part of the scrotal skin, but industrial cancers are
often high up in the cleft between the leg and
the scrotum, where there is repeated friction and
persistent traces of oil.
Tenderness
The ulcer is usually painless and not
tender.
Shape
In its early stages the ulcer is small and cir-
cular, but it usually enlarges in an irregular fashion
and develops an irregular outline.
Edge
The edge is reddish, friable and typically
everted.
Base
The base is covered with yellow-grey, infected,
necrotic tumour.
Discharge
There is often a purulent, bloody, offen-
sive discharge.
342
FIG 13.13
A carcinoma of the scrotal skin. Note that it is
on the postero-medial surface of the scrotum.
Chap-13.qxd 4/19/05 14:30PM Page 342
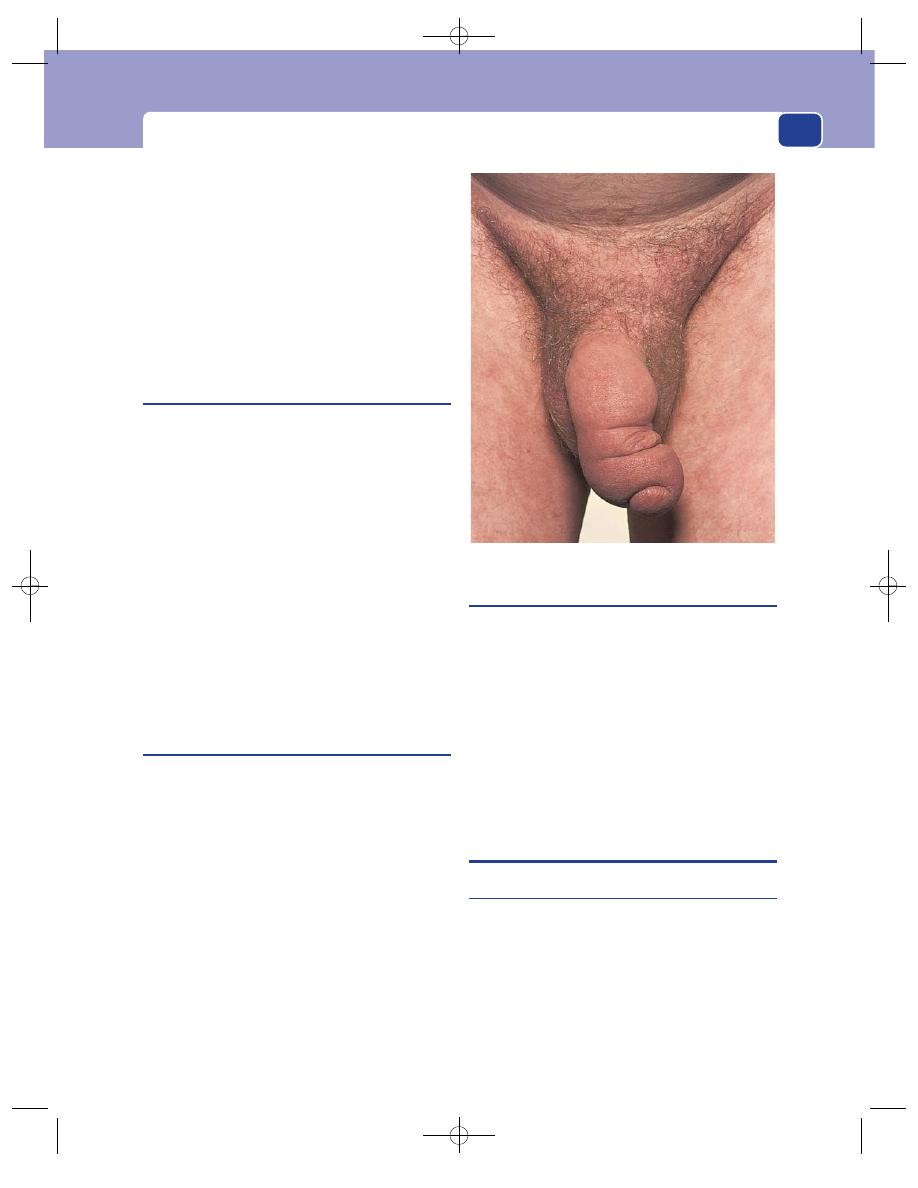
The testes
Relations
In the early stages the skin and ulcer are
freely mobile, but if the tumour cells spread deep to
the skin, the ulcer may become tethered to the
underlying testicle.
Lymph drainage
The inguinal lymph glands may
be enlarged by tumour metastases or secondary
infection.
General examination
Distant metastases are unusual
with scrotal cancer.
Tinea cruris
Common conditions present in diverse clinics.
Tinea cruris is a fungal infection of the skin of the
upper medial aspect of the thigh and the adjacent
scrotal skin.
The first symptom is itching, but this is soon fol-
lowed by the appearance of a dry erythematous
rash with a sharply defined edge on the thigh and
scrotum.
If the patient perspires heavily, the rash may
become macerated and ooze serum, which forms
pale-brown crusts.
The patient may present to a surgical clinic
because of the changes in the scrotal skin, or you
may notice the distinctive skin changes when exam-
ining the patient’s scrotum for another complaint,
such as a hernia.
Lymphoedema
Swelling of the penis and scrotum caused by excess
fluid in the subcutaneous tissue (oedema) is seen
commonly in patients confined to bed with heart
failure or fluid retention. It may also occur after sur-
gery in the groin.
True lymphoedema of the genitalia – oedema
caused by retention of protein-rich lymph in the
subcutaneous tissues – is uncommon. It may be
associated with lymphoedema of one or both limbs.
The usual cause is obstruction of the inguinal and
iliac lymph pathways by secondary or primary
malignant disease or, in tropical areas, by worms
(Wuchereria bancrofti, filariasis).
Primary genital lymphoedema is very rare and
caused by hypoplastic lymphatics. It is not known if
it is a congenital or an acquired condition.
Sinuses of the scrotum
Disease of the testis or epididymis may occasionally
spread to, and through, the scrotal skin to create
a sinus between the primary lesion and the skin
surface.
Provided the testis is lying in the normal posi-
tion, disease of the body of the testis tends to spread
to the antero-lateral surface of the scrotum, whereas
disease of the epididymis spreads to the posterior
surface. Both are rare occurrences requiring gross
intrascrotal pathology. Most sinuses in the scrotal
skin are discharging sebaceous cysts.
THE TESTES
Failure of normal testicular descent
The testis develops in utero in the posterior abdom-
inal wall from nephric tissue. Its blood supply comes
from the aorta and its veins drain into the inferior
vena cava, on the left via the renal vein. Lymph
drainage is to the para-aortic glands.
Guided by the gubernaculum, the testicle descends
into the scrotum, the left before the right. Most tes-
ticles have reached the scrotum by the time of birth
343
FIG 13.14
Lymphoedema of the penis.
Chap-13.qxd 4/19/05 14:30PM Page 343
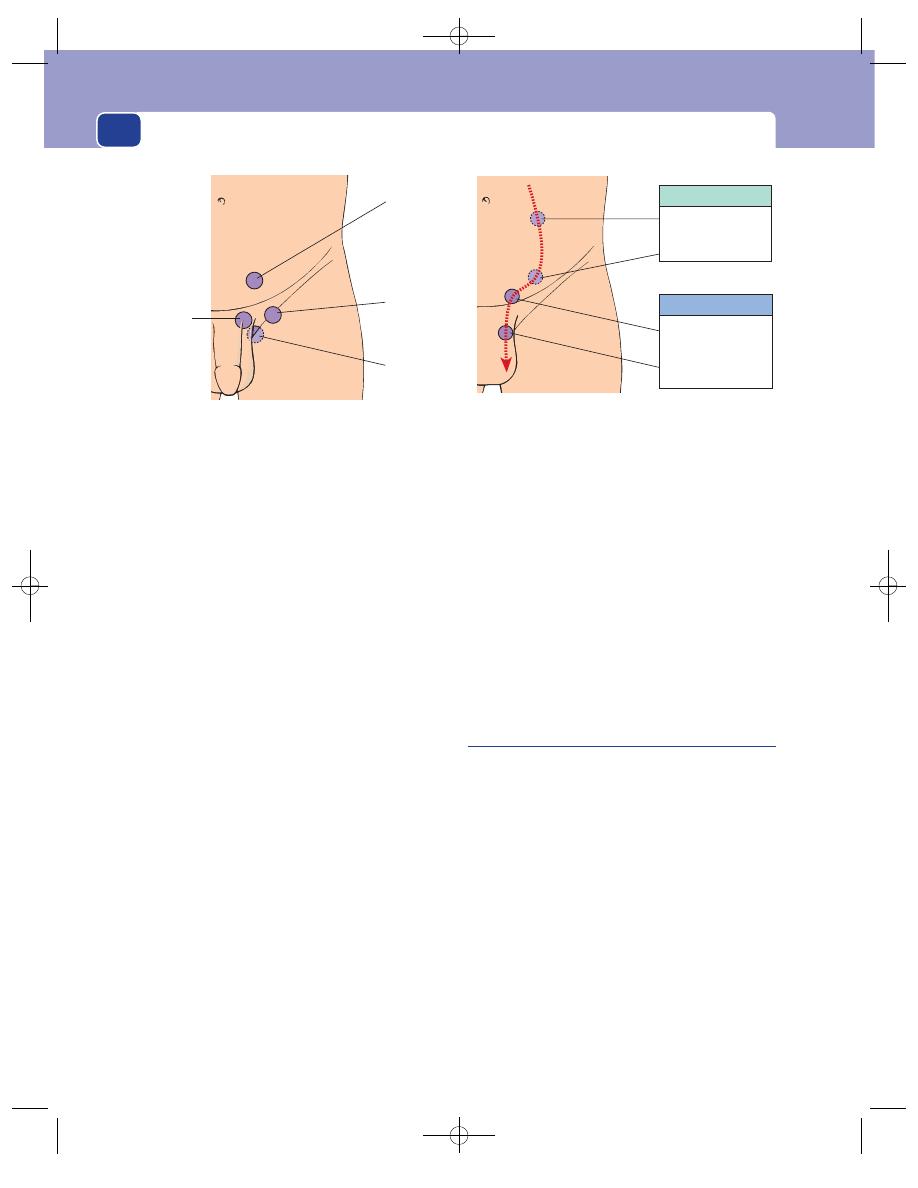
The external genitalia
344
and it is unlikely that any natural descent occurs
thereafter.
Examination of the scrotum and groin can be
difficult in small babies.
You can only confirm the presence or absence
of the testes by careful palpation. A quick glance at
the scrotum is not good enough.
By 3 months, only 1–2 per cent of testicles can-
not be found by an experienced examiner.
If a testis has never descended into the scrotum,
the scrotal skin on that side will be underdeveloped.
If a testis is not in the scrotum, it may either have
stopped somewhere along its line of normal descent
or have found its way to an abnormal site. The aeti-
ology of these two abnormalities is different and
there is no standardization of the names used to
describe them. A simple classification is as follows.
■
A testis which has descended to an abnormal
site is an ectopic testis. There is no confusion
about this term. The testis may be in the
superficial inguinal pouch, the femoral triangle
or the perineum. The mechanism causing
descent is normal but the guidance system has
gone wrong. The testicle itself is normal.
■
A testis which is in its correct anatomical path
but has failed to reach the scrotum is best
called a truly undescended testis. Although this
is a cumbersome name, it is better than
‘undescended’ or ‘maldescended’ because both
these names could reasonably be used to
describe the two sorts of missing testicle.
The truly undescended testicle is small and
abnormal, with a separated epididymis and often an
associated indirect inguinal hernial sac. We do not
know whether the testicle is abnormal because it
fails to descend, or fails to descend because it is
abnormal.
Absence of both testes from the scrotum caused
by a failure of descent is known as cryptorchism.
True congenital absence of a testicle is rare and is
usually on the left. The testicle is sometimes missing
because it has met with a vascular accident, usually
torsion (see below) in early or even intrauterine life.
Examination of a child with a missing
testicle
This can be difficult with a child who does not want
to be examined and frequently anxious parents.
Make sure the room and your hands are warm. The
child has to be persuaded to lie down. Do not be
downhearted if you cannot persuade the child to let
you carry out the necessary careful examination. Try
again later, or accept that more experienced help on
another occasion will be needed.
Inspection
The child must be undressed from the
waist downwards in a good light. An empty scro-
tum, with very little development of the scrotal skin
because it has never had the testicle within it, is usu-
ally obvious. However, a prominent gubernaculum
may look like a testis but it will not feel like one.
If the testicle is in the superficial pouch, it may be
visible in the inguinal region in a thin patient.
Base of
penis
(‘penile’)
Superficial
inguinal
pouch
(‘inguinal’)
Femoral
triangle
(‘femoral’)
Perineum
(‘perineal’)
FIG 13.15
The sites where you may find an ectopic testis.
Not palpable
Posterior
abdominal wall
Inguinal canal
Palpable
External
inguinal ring
Neck of
scrotum
FIG 13.16
The line of normal testicular descent. An
incompletely descended testis may be found anywhere on
this line. If it is above the external inguinal ring, it will be
impalpable.
Chap-13.qxd 4/19/05 14:30PM Page 344
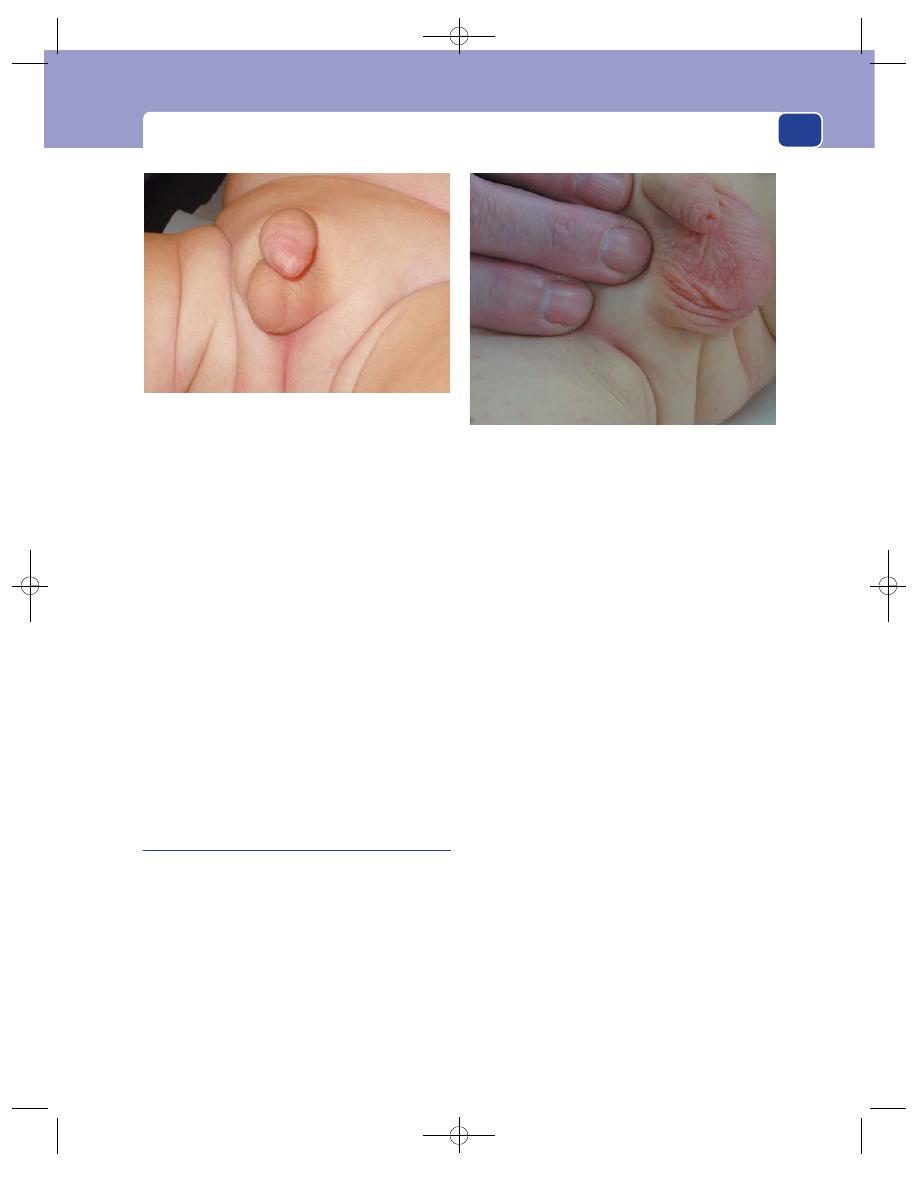
The testes
345
Palpation
You must try to get the child to relax, as
muscular activity makes the dartos muscle contract
and draw the testicle up towards the groin.
Examine the groin before palpating the scrotum.
If you cannot see or feel the testis in the subcuta-
neous tissues, find out if it is in the inguinal canal by
gently sweeping your fingers from the anterior
superior iliac spine obliquely across the groin to the
pubis, along the line of the inguinal canal, towards
the neck of the scrotum, to ‘milk’ the testis, if pres-
ent, through the external ring. If the testis becomes
palpable, catch it gently with the thumb and index
finger of your other hand and draw it down to the
scrotum. If it is a retractile testis, it will move down
easily.
Should you get the testicle down into the scro-
tum, show it to the parents before you remove your
fingers and the testicle retracts!
Ectopic testis
History
Age
Children in developed countries will usually be
routinely examined at birth and again in the first
year of life. Examination requires experience. An
ectopic testis may readily be missed, a prominent
gubernaculum being mistaken for the testicle. Not
all parents notice that their infant child has one or
both testes missing from his scrotum.
The patient may not discover the abnormality
himself until adolescence.
Symptoms
Absence of a testis is the common pre-
senting symptom, but the patient may also com-
plain of pain or discomfort if the testis is in a site,
such as the superficial inguinal pouch, likely to be
rubbed or compressed during normal physical
activity. Note that the pain pathway is via auton-
omic afferent nerves and for developmental reasons
may be experienced in the groin or even loin.
Systemic effects
If both testes are ectopic, the patient
may be subfertile but rarely lacks secondary sex
characteristics.
Examination
The side of the scrotum without the testis may be
poorly developed, but not so obviously as with a
truly undescended testicle.
Site
An ectopic testis is nearly always palpable,
although with difficulty in a fat child. A truly undes-
cended testis lying in the inguinal canal or abdomen
is not palpable. If the testis is not in the scrotum,
you must search for a smooth, sensitive, ovoid
swelling in those sites where ectopic testes are known
to settle.
■
Superficial inguinal pouch. This is by far the
commonest site in which to find an ectopic
testicle. It is also the place to which the retractile
testicle retreats. An ectopic testicle in this site
has emerged through the external ring but,
having failed to enter the scrotum, turns
FIG 13.17
This baby has a truly undescended and impalpable
left testis. The scrotal skin is very poorly developed compared
to the right side, where the testis has fully descended.
FIG 13.18
A perineal ectopic testis. As the testicle was
milked downwards and medially, it did not enter the scrotum,
but passed backwards into the perineum.
Chap-13.qxd 4/19/05 14:30PM Page 345
The external genitalia
346
upwards and laterally to lie in a pouch deep to
the superficial fascia. This may be caused by
some obstruction at the neck of the scrotum
from tight fascia. The testis can be palpated in
the subcutaneous tissue just above and lateral to
the crest of the pubis and the pubic tubercle.
■
Femoral triangle. If the testis moves laterally
after leaving the external inguinal ring, it can
come to rest in the upper medial corner of the
femoral triangle. A testis in this site is easy to
feel and easily misdiagnosed as a lymph gland
or even a femoral hernia, although the latter is
very rare in children. This variety is sometimes
termed crural, as it lies in the thigh.
■
Base of the penis. If the testis moves medially, it
will lie at the base of the penis, where it can be
easily felt against the underlying pubic bone.
■
Perineum. Occasionally, the testis passes over the
pubis and then backwards, instead of downwards,
to lie in the perineum just to one side of the
corpus cavernosum of the penis. An ectopic testis
cannot be manipulated into the scrotum.
The lump
An absent scrotal testis and a lump in one
of the four sites described above make the diagnosis
of ectopic testis very probable, but it is important to
confirm that the lump has the features of a testis.
It should be ovoid, smooth, slightly tender and
soft-solid in consistence. It should be mobile within
the subcutaneous tissues, and gentle pressure should
cause the mild sickening sensation recognized by
most males as testicular sensation.
It is unusual to be able to define the separate fea-
tures of the body of the testis and the epididymis.
Any enlargement, irregularity or immobility
should make you suspect the presence of malignant
change in the testis, or make you look for another
diagnosis.
Truly undescended testis
History
Truly undescended testes are usually noticed in
early life but occasionally not until adolescence.
Symptoms
An absence of one or both testes from
the scrotum is the presenting symptom. The par-
ents may first notice that the scrotum has not
developed – unaware of the absence of the testes. A
small proportion of patients present in adult life with
infertility. Although failure of testicular descent is
invariably associated with abnormal spermatogenesis,
the hormone-producing cells are usually normal
so the boy has a normal puberty and secondary sex
characteristics.
All truly undescended testes are associated with
an indirect inguinal hernia, and a groin swelling
may be the presenting complaint.
Examination
The scrotum
When both testes are undescended the
scrotum is small and hypoplastic. If only one testis
has descended, it is markedly asymmetrical.
Site
A truly undescended testis lies somewhere in
the line of normal descent (i.e. at the neck of the
scrotum, in the external inguinal ring, in the inguinal
canal or in the posterior abdominal wall).
The testis only becomes palpable when it reaches,
or is outside, the external inguinal ring.
Within the inguinal canal it cannot be felt because
the tense overlying external oblique aponeurosis con-
ceals it and it tends to slip back through the internal
ring into the abdomen. Thus, if you can feel a testis
lateral to the external inguinal ring, it must be super-
ficial to the external oblique and is therefore an
ectopic testis not a truly undescended testis.
Some testes which lie in the inguinal canal can be
milked down to the external ring by gently stroking
along the line of the canal as described above.
The lump
A truly undescended testis is usually
smaller than normal but otherwise has all the
expected characteristics of a testis.
In an adult, the appearance of a mass in the line
of testicular descent, whether within the abdomen
or the inguinal canal, and an empty scrotum should
make you suspect malignant change in a truly unde-
scended testicle. The risk of malignant change is
many times greater than in a normally descended or
ectopic testis. Fixing the testis in the scrotum
(orchidopexy) does not eliminate this risk.
The truly undescended testis is also more likely
to undergo torsion than a normally descended testis.
Retractile testes
The cremaster is a strong active muscle during
childhood, and the testes of many young children
Chap-13.qxd 4/19/05 14:30PM Page 346
The testes
move freely up and down between the scrotum and
the inguinal canal or the superficial inguinal pouch.
A cold examining hand may be sufficient stimulus
to cause retraction. If the patient is seen when the
testis is retracted, it may be misdiagnosed as a truly
undescended testis and surgical treatment advised.
This will be an unnecessary operation because all
retractile testes ultimately descend properly, before
or at puberty.
History
The parents notice that the testicle (frequently
both) is absent from the scrotum. This situation is
often intermittent, and it may be noticed that every-
thing appears normal when the child is warm and
relaxed, typically in the bath.
The testicles may have been reported in the scro-
tum at previous routine examinations.
Examination
When the testes are retractile, the scrotum is nor-
mally developed.
You should always attempt to manipulate the
testis into the scrotum, as described above. If the tes-
ticle can be persuaded into the scrotum and it rests
there when you let go, it is a retractile testicle. A testis
should only be classified as truly undescended or
ectopic if you cannot manipulate it into the scrotum.
However, experience is required to be certain of
this physical finding.
The ascending testicle
Many boys are referred to the surgical clinic with a
missing or intermittently absent testicle, a normal
scrotum, and a testicle that is palpable in the super-
ficial inguinal pouch. On examination, the testicle
may or may not be placed in the scrotum. However,
a single assessment is not reliable. A testicle that
cannot be placed in the scrotum one day may be
persuaded to go there on another, perhaps by a dif-
ferent examiner.
There is also a group of patients in whom the tes-
ticle has been found and placed in the scrotum to
the satisfaction of all, but, some while later, the par-
ents notice that the testicle is no longer visible and
seek further advice. On this occasion, the testicle
may be palpable in the superficial inguinal pouch
and cannot be persuaded into the scrotum, even by
the examiner who was successful on the previous
occasion.
The testicle has, on our clinical criteria, changed
from being retractile to ectopic. This is termed the
‘ascending testicle’ or sometimes ‘acquired unde-
scended testicle’, a confusing term.
Thus there is often uncertainty in differentiating
between superficial pouch ectopic and superficial
pouch retractile testicles. The only solution to the
dilemma is to repeat the assessment until puberty is
attained, when any testicle not resting in the scro-
tum should be considered to be abnormal and in
need of surgical treatment. Note, however, that the
truly undescended testicle may be diagnosed defini-
tively because it is impalpable and the scrotum is
poorly developed.
Hydrocele
A hydrocele is an abnormal quantity of fluid within
the tunica vaginalis. There are two varieties:
■
primary, of unknown cause,
■
secondary, caused by trauma, infection or
neoplasm.
Most secondary hydroceles appear rapidly in the
presence of other symptoms associated with their
cause, are not tense, and contain some altered
blood. They are much less common than primary
(idiopathic) hydroceles, which develop slowly and
progressively and become large and tense.
History
Age
Primary hydroceles are most common over
the age of 40 years. In children, although the phys-
ical signs are the same as in adults, the condition is
always associated with a patent processus vaginalis
and is a variety of inguinal hernia.
Secondary hydroceles are more common between
20 and 40 years because trauma, infection and tes-
ticular neoplasms are more common in this period.
Symptoms
The patient complains of an increase in
the size of the testis, or a swelling in the scrotum.
There may be pain and discomfort if there is under-
lying testicular disease, but idiopathic hydroceles
reach a considerable size without causing pain. The
patient may complain of the social embarrassment of
his large scrotum, which shows through his trousers.
347
Chap-13.qxd 4/19/05 14:30PM Page 347
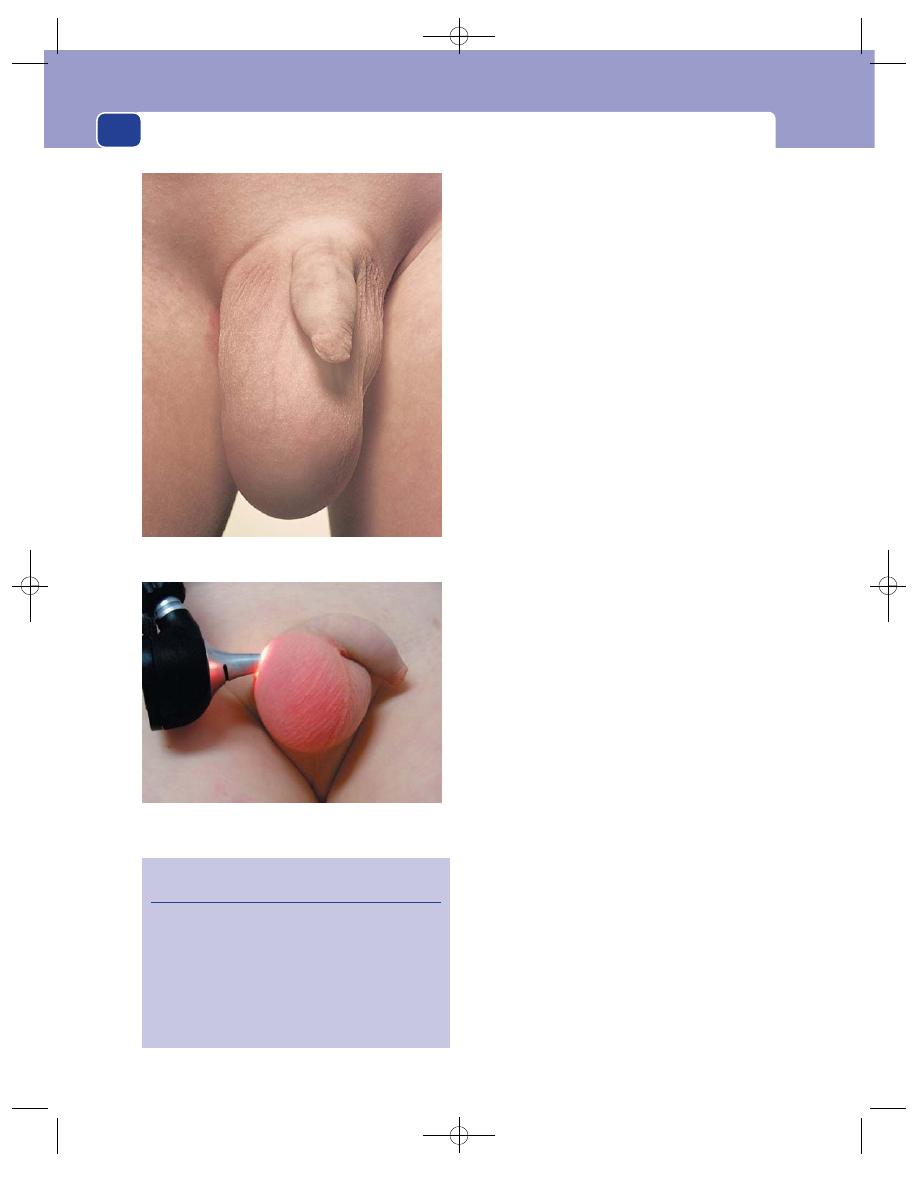
The external genitalia
348
Hydroceles do not affect fertility, although a large
one may cause problems during sexual intercourse.
Examination
Position
The swelling fills one side of the scrotum
but is within the scrotum and you can feel the sperm-
atic cord above the lump. The testis cannot be pal-
pated separately because it is within the swelling.
This is the cardinal physical sign that distinguishes a
hydrocele from an epididymal cyst.
Hydroceles may be bilateral.
Colour and temperature
The colour and temperature
of the overlying scrotal skin are normal.
Tenderness
Primary hydroceles are not tender.
Secondary hydroceles may be tender if the under-
lying testis is tender.
Shape and size
When the tunica vaginalis first fills
with fluid, the resulting hydrocele is just a little
larger than the testis. As time passes, the volume of
fluid increases.
Hydroceles can become 10–20 cm in diameter
and contain as much as 500 mL of fluid. They are
ovoid in shape.
Surface
The surface is always smooth and well
defined. Occasionally a weak spot in the wall gives
way to form a small fluctuant bump, a hernia of the
hydrocele fluid through its coverings.
Composition
Hydroceles contain a clear yellow fluid
which is protein rich. They are therefore fluctuant,
have a fluid thrill if they are large enough, are dull
to percussion and usually transilluminate.
They do not pulsate and are not compressible.
They may be tense or lax, depending on the
pressure of the contained fluid.
The wall of a long-standing hydrocele may become
calcified, making the mass hard and opaque.
Reducibility
Hydroceles cannot be reduced.
Relations
The fluid of a hydrocele surrounds the
body of the testis, making the testis impalpable.
This is its most important relationship. If you can
feel the testis separate from a scrotal swelling, the
swelling cannot be a hydrocele.
When a hydrocele is lax, a feature almost invariably
seen only in secondary hydroceles, it may be possible
to feel the surface of the testis through the fluid.
FIG 13.19
HYDROCELE.
Revision panel 13.2
The causes of hydrocele
Primary
Idiopathic
Secondary
Trauma
Epididymo-orchitis
Tumour
Lymphatic obstruction
A large hydrocele. The swelling is confined to the scrotum, not
tender, fluctuant, translucent, and the testis is not palpable.
A transilluminated hydrocele.
Chap-13.qxd 4/19/05 14:30PM Page 348
The testes
349
The testis produces an opaque area in an other-
wise highly translucent swelling, but it is usually too
small to see clearly.
The spermatic cord can be felt coming down to
and running into the swelling. The skin of the scro-
tum is freely mobile over the swelling.
Lymph drainage
The para-aortic lymph glands, which
receive lymph from the testis, should be carefully
palpated if you think the swelling is a secondary
hydrocele, because they may be enlarged if there is
an underlying testicular tumour.
Epididymal cyst
Epididymal cysts are fluid-filled swellings arising
from the epididymis. Their aetiology has not been
satisfactorily explained, but they are derived from
the collecting tubules of the epididymis.
An epididymal cyst usually contains clear fluid.
The variety that contains slightly grey, opaque, ‘bar-
ley water’-like fluid and a few spermatozoa is some-
times termed a spermatocele. This distinction can
only be made after aspiration, and there is no clinical
way of differentiating between the two types. As the
large majority of cysts connected with the epididymis
contain clear fluid, it is best to call them all epididy-
mal cysts and not use the term spermatocele.
History
Age
Most epididymal cysts occur in men over the age
of 40 years, but they are occasionally seen in children
and adolescents.
Symptoms
The main complaint is of swelling in the
scrotum, with the occasional patient believing that
he has developed a third testis.
In older age groups the swelling is usually painless.
Small epididymal cysts in men in their thirties
and forties may be painful and tender.
Development
Epididymal cysts enlarge very slowly,
over many years, but rarely become gigantic. A
really big, fluid-filled scrotal swelling is likely to
be a hydrocele.
Multiplicity
They are often multiple or multilocular,
and are frequently bilateral.
Fertility
Epididymal cysts do not interfere with fer-
tility. However, surgery to remove such cysts may
have an effect equivalent to that of a vasectomy.
Examination
Position
The swelling lies within the scrotum, usually
above and slightly behind the testis. The testis can
be felt separately from the swelling. If the swelling
is similar in size to a testicle, ask the patient which of
the lumps is which. He will always be able to tell you!
The spermatic cord can be felt above it.
Tenderness
Small cysts of the epididymis in younger
men may be tender, but larger cysts in older men
are not.
Shape
Because the cysts are usually multilocular,
the swelling is rarely a perfect sphere. It is usually
elongated and bosselated, and individual loculi may
be palpable.
Size
Epididymal cysts may vary in size from a few
millimetres to 5–10 cm in diameter. They rarely
reach the size of the large hydroceles.
Surface
The surface is smooth but the contours of
individual loculi may be palpable.
Composition
These swellings are fluctuant, have a
fluid thrill, are translucent if large enough to trans-
illuminate, and are dull to percussion.
Epididymal cysts cannot be reduced.
All the signs mentioned in this section on com-
position are identical to those for hydrocele. The
difference between a hydrocele and an epididymal
cyst lies in the relation of the swelling to the testis.
Relations
Epididymal cysts are separate from the
testis, therefore the testis remains palpable.
Most epididymal cysts are connected to the head
of the epididymis and so lie above the testis with the
spermatic cord descending into or behind them.
They occasionally lie at the lower pole.
Lymph drainage
The regional lymph glands should
not be palpable.
General examination
This should be quite normal.
Differential diagnosis
The normal epididymis is usu-
ally palpable and may be noticed by concerned
young men who think they have a testicular
tumour. It may on occasion be difficult to say if a
swelling is a normal palpable organ or a small cyst.
A period of observation will provide the answer.
Tumours of the epididymis itself are so rare as to
be virtually non-existent. Any swelling that is clearly
in the epididymis is therefore benign.
Chap-13.qxd 4/19/05 14:30PM Page 349
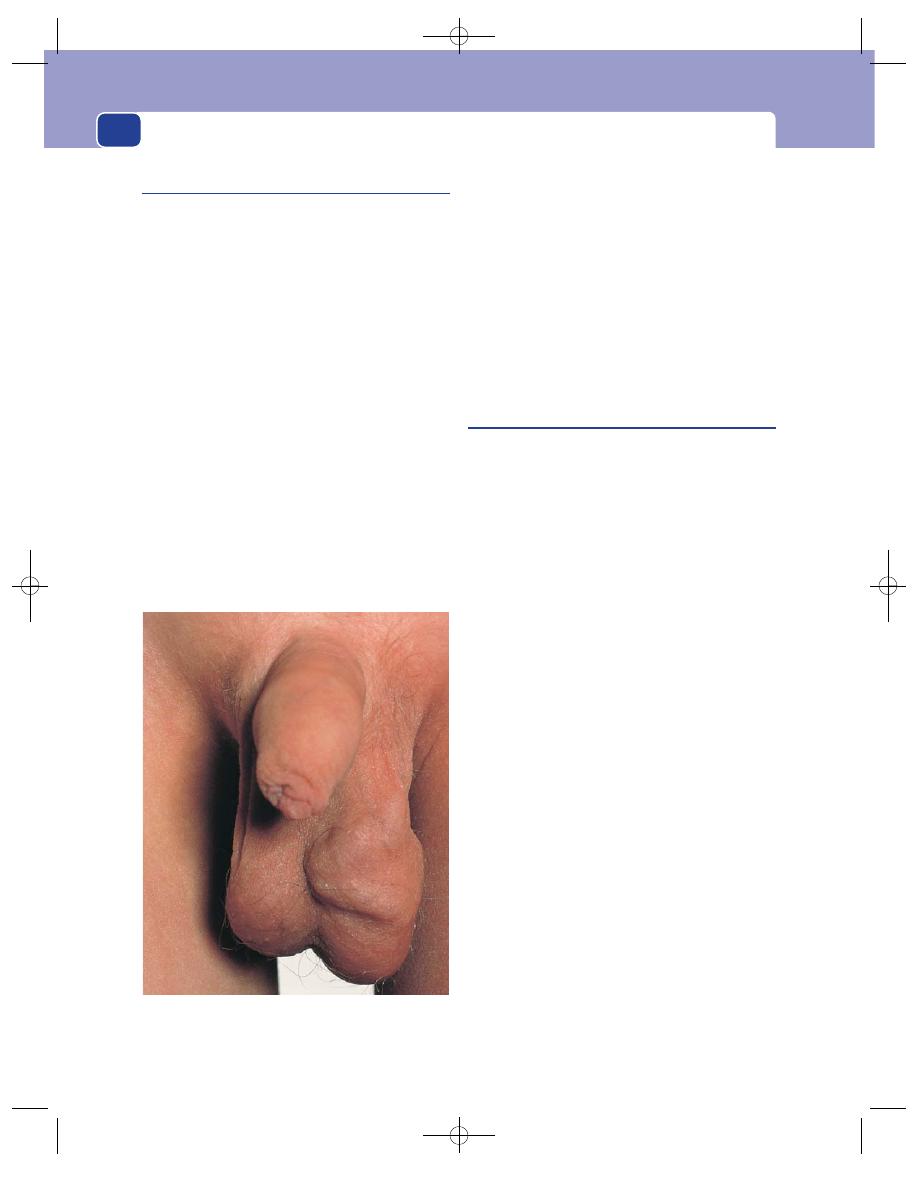
The external genitalia
Varicocele
A varicocele is a bunch of dilated and tortuous veins
in the pampiniform plexus. The condition could be
renamed varicose veins of the spermatic cord. It is
almost invariably on the left. The right testicular
veins drain into the inferior vena cava, but on the
left they drain into the left renal vein. The left testicu-
lar vein (or veins) is thus a long vessel and it is
hardly surprising that its valves often fail and pro-
duce a varicocele.
Small symptomless varicoceles occur in 25 per
cent of normal men, on the left side. When the
veins become large, they may cause a vague, drag-
ging sensation and aching pain in the scrotum or
groin. The appearance may embarrass adolescents
and young men.
The sudden appearance of a varicocele in middle
or old age may be caused by a renal neoplasm spread-
ing along the renal vein and obstructing the testicu-
lar vein. This is a very rare presentation of carcinoma
of the kidney but should not be forgotten, particu-
larly if there are other urinary tract symptoms.
You cannot feel a varicocele when the patient is
lying down because the veins are empty. This is one
of the reasons why you must always examine the
scrotum with the patient standing up. The dilated,
compressible veins above the testis are then palpable
and often visible. They feel like a ‘bag of worms’, an
accurate description.
The testis below a large varicocele may be smaller
and softer than the testis on the normal side.
The effect of a varicocele on spermatogenesis is
controversial.
Haematocele
A haematocele is a collection of blood within the
tunica vaginalis. The bleeding is usually caused by
trauma or underlying malignant disease.
In the acute phase the mass has the same physical
signs as a hydrocele, except that it is not translucent
and may be tender. When the blood clots, it con-
tracts and forms a small, hard mass, which can
cause diagnostic problems.
Acute haematocele
The patient usually but not always gives a clear his-
tory of an injury, or of vague discomfort in the
testis, followed by a painful, rapid swelling of the
scrotum. It is a condition particularly associated
with cycling.
The swelling, which is in one side of the scrotum,
is tense, tender and fluctuant, but does not transillu-
minate. The testis cannot be felt separate from the
swelling.
Chronic haematocele
If the acute episode is ignored and not treated, or if
the bleeding occurs without the patient’s know-
ledge, the blood in the tunica vaginalis will clot. As
time passes, the clot that surrounds the testis con-
tracts and hardens. The result is a hard mass, which
is no longer tender and is not fluctuant. Normal tes-
ticular sensation may be lost if the contracting clot
causes ischaemic necrosis of the testis.
These changes make a chronic haematocele diffi-
cult to distinguish from a testicular tumour, and the
testis may need to be explored before the final diag-
nosis can be made.
350
FIG 13.20
A varicocele. When standing, the tense, tortuous,
distended veins are said to feel like a ‘bag of worms’. When
supine, they collapse and are almost impalpable.
Chap-13.qxd 4/19/05 14:30PM Page 350
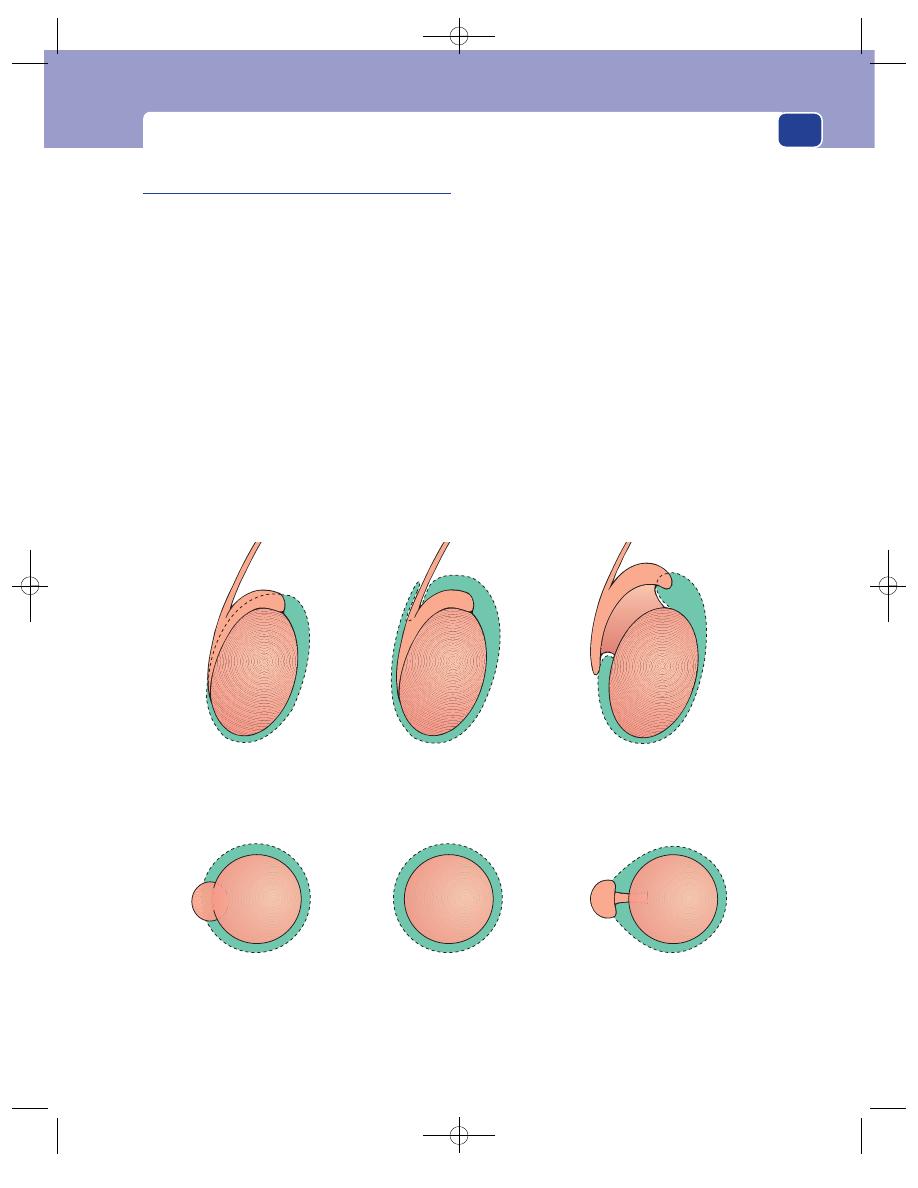
The testes
351
Torsion of the testicle
The tunica vaginalis covers the sides and anterior
aspect of the testis. The back of the epididymis and
the posterior surface of the testis covered by the
epididymis are not covered by the tunica vaginalis.
A normal testis is, therefore, fixed within the tunica
and cannot twist.
However, there is variability in the extent to which
the tunica vaginalis covers the body of the testis. In
one variation, the testicle is suspended in the tunica
like the clapper in a bell, and is thus able to twist on
its attachment. This process can be aided by con-
traction of the spiral fibres of the cremaster muscle.
In another variety, the testis is separated from the
epididymis by a long mesorchium, long enough to
allow a twist to occur between the testis and the epi-
didymis. This is less common.
Extravaginal torsion – torsion of the spermatic
cord itself – is another rarer possibility.
The anatomical abnormality that allows torsion
is invariably bilateral.
The condition may resolve spontaneously or
progress to testicular infarction.
History
Age
Torsion presents most commonly in teenagers,
but as the cause is a congenital abnormality, it can
occur in young children, neonates and even in utero.
It is very uncommon in men over 25 years of age and
unknown over 40.
Symptoms
The initial symptom is an uncomfortable,
poorly localized pain, which may initially be felt in
the abdomen or loin because it is autonomically
modulated and so referred to the embryological site
The tunica invests the
body of the testis and
part of the epididymis
The tunica invests the
testis, epididymis and
part of the cord
The mesorchium is long
and narrow. The tunica
is normal
The testis cannot twist
The testicle hangs like
the clapper in a bell
and can twist with ease
The body of the testis
can twist, but the
epididymis stays fixed
Normal
‘
Clapper in a bell’
Long mesorchium
FIG 13.21
The congenital anatomical abnormalities that permit torsion of the whole or the body of the testis.
Chap-13.qxd 4/19/05 14:30PM Page 351
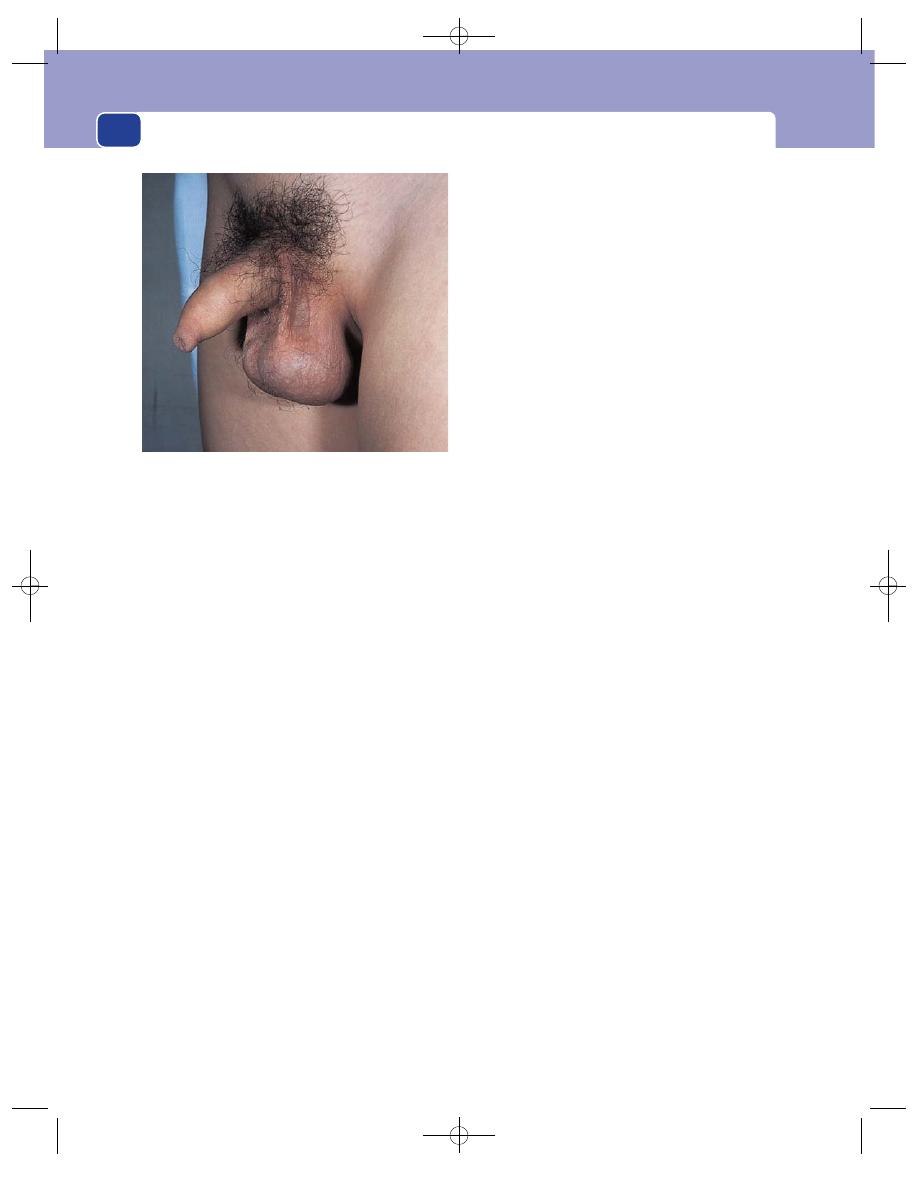
The external genitalia
of origin of the testis. Severe pain and tenderness
in the testicle follow the abdominal pain, but the
abdominal component may be absent or forgotten.
Nausea and vomiting are common.
In a baby there may be restlessness and a failure
to eat.
Previous attacks
The patient may have had similar
mild attacks of pain, which subsided spontaneously,
or an episode on the other side which required sur-
gery. Recurrent torsion is possible if the testicle has
not been securely fixed.
Cause
Although the majority of torsions seem to
occur spontaneously, often in the early hours of the
morning, some follow minor trauma, one of the
commonest being a blow on the scrotum as the boy
jumps on to his bicycle.
Examination
Position
The swelling is confined to the scrotum.
The affected testis lies higher in the scrotum than the
normal testis. This is a most important physical sign.
Colour
The scrotal skin may be normal, or red and
oedematous. Although the latter changes are more
commonly associated with epididymo-orchitis,
their presence must not dissuade you from making
a diagnosis of torsion.
Temperature
The skin will feel hot if it is red and hyper-
aemic.
Tenderness
The testis is exquisitely tender, making
palpation very difficult.
Shape
The whole of the testis is swollen and it is
usually impossible to distinguish the contours of
the epididymis from those of the body of the testis.
Surface
The surface of the testis is smooth, but it
may be obscured by scrotal oedema.
Composition
It is usually impossible to elicit the
signs which will reveal the composition of the mass
in the scrotum because of tenderness. The mass may
be the testicle, or the testicle surrounded by an acute
secondary hydrocele.
Surrounding tissues
Apart from the scrotal skin, which
may be red and oedematous, the other nearby tissues,
including the other testis, will be normal.
Differential diagnosis
Torsion of a testis within the
scrotum may be indistinguishable from acute
epididymo-orchitis, particularly if there are no
urinary symptoms. However, epididymo-orchitis
usually occurs in an older age group. Torsion of a
truly undescended testicle in the groin may be indis-
tinguishable from a strangulated inguinal hernia.
■
Torsion of a testicular appendage is the
commonest condition mimicking torsion.
There are two appendages (the appendix of
the testis and the appendix of the epididymis)
and either may tort. Their initial symptom
(abdominal pain) may be identical. The testicle
is not usually so tender, and sometimes the torted
appendage is palpable as a tender nodule.
However, a secondary hydrocele may obscure this.
■
Idiopathic scrotal oedema is a condition in
which the skin and subcutaneous tissues of the
scrotum become oedematous, red and inflamed,
in most cases as a result of a streptococcal
infection.
The swelling is confined by the attachments of
the scrotal fascia and sometimes unilateral. A clinical
diagnosis can usually be made, as the testicle itself is
not tender.
Warning: when in doubt about a painful scrotal/
testicular swelling, make a diagnosis of torsion,
because failure to explore the scrotum and reduce
the torsion will result in death of the testicle. The
window of opportunity during which the testicle
352
FIG 13.22
A testis hanging horizontally and susceptible to
torsion.
Chap-13.qxd 4/19/05 14:30PM Page 352
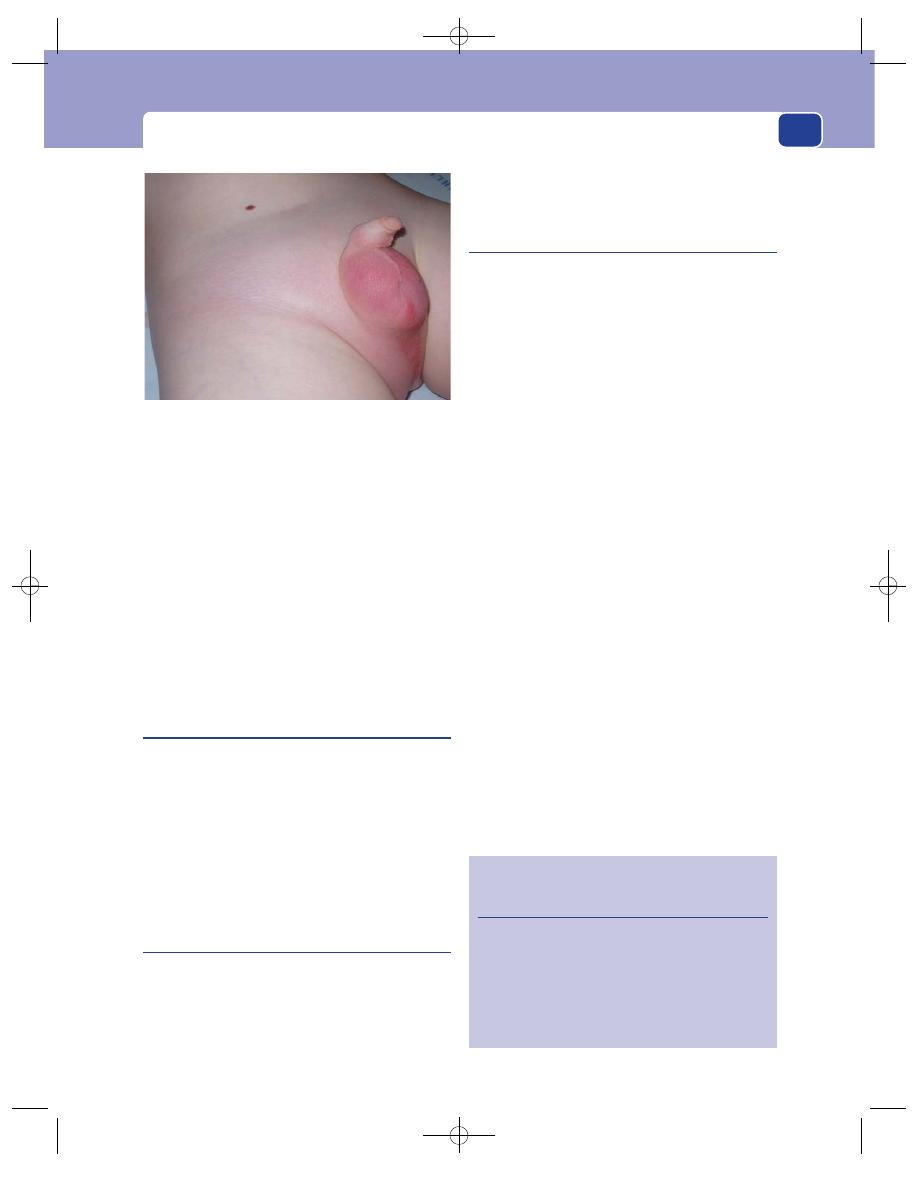
The testes
353
can be saved is only a few hours. If the diagnosis turns
out to be wrong and the patient has an epididymo-
orchitis, the surgical exploration will have done no
harm and the decompression of the tunica vaginalis
will have relieved painful pressure from the second-
ary hydrocele.
There are reports from experienced school med-
ical officers describing manipulative reduction of
testicular torsion. While undoubtedly successful at
times, this is for experts only.
Gumma
This is now a very rare condition in Europe.
Congenital syphilis causes testicular atrophy, but in
adult life the same interstitial inflammation turns
the testis into a round, hard and insensitive mass –
the ‘billiard ball testis’.
A gumma of the testis is painless and therefore
presents either as a lump felt by chance on the sur-
face of the organ or as an enlargement of the whole
organ. It is usually indistinguishable from a tumour.
Orchitis
Acute orchitis, in the absence of epididymitis, is
invariably due to a virus infection, commonly the
mumps virus. The damage caused by a bilateral
orchitis may leave the patient with a painful testis
or, rarely, make him subfertile. Mumps orchitis may
occur without enlargement of the salivary glands,
but there is usually a history of contact with mumps.
Acute epididymo-orchitis
This is primarily an infection of the epididymis, but
some oedema and inflammatory changes spread
into the testis. There is usually an associated urinary
tract infection, often prostatitis.
The common infecting organism in patients
under 40 years old is Chlamydia trachomatis, and in
older patients Escherichia coli, and do not forget the
possibility of gonorrhoea.
History
Age
This condition can affect all age groups but is
commonest in young and middle-aged men. It is
rare in children.
Symptoms
There is often an initial flu-like illness,
with malaise and fever, and sometimes deep-seated
pelvic pain caused by inflammation of the prostate.
The patient then develops severe pain and swelling
in one side of the scrotum, which usually come on
quite quickly over 30–60 minutes and are sometimes
relieved by supporting the scrotum. Frequency of
micturition and painful micturition may indicate
the presence of a urinary tract infection.
Examination
Position
The swelling is confined to one side of the
scrotum.
Colour
The scrotal skin is red and shiny. After a few
days it turns a bronze colour and the superficial lay-
ers of skin desquamate.
Temperature
The scrotal skin is hot.
FIG 13.23
A very severe case of idiopathic scrotal
oedema. The scrotal skin has lost its wrinkled appearance.
Unusually, the oedema has tracked into the groin, perineum
and the other side of the scrotum. The attachment of
Scarpa’s fascia in the thigh is clearly visible.
Revision panel 13.3
The causes of a solid single mass in one side
of the scrotum
Tumour
Orchitis (mumps)
Haematocele
Gumma
Epididymo-orchitis (when the epididymis is
large and the testis is small)
Chap-13.qxd 4/19/05 14:30PM Page 353
The external genitalia
354
Tenderness
The scrotal skin is not tender but the
testis and epididymis beneath it are extremely tender.
You must be patient and gentle. Careful palpa-
tion will reveal that the tenderness is in the swollen
epididymis and that the body of the testis itself is
not so tender.
Shape and size
The whole testicle may be enlarged
and tender and you may be unable to distinguish
epididymis from testis. This is more likely in the
presence of a small secondary hydrocele. If a hydro-
cele does not form, you should be able to distin-
guish the testis from the epididymis, which is
commonly enlarged to about 1 cm or so in width.
In mild cases the inflammation may be localized
to the head or tail of the epididymis.
Surface
The surface of the epididymis remains
smooth but will probably be too tender for this to be
obvious.
Composition
If there is a small hydrocele, the swelling
may be fluctuant, with the testis palpable through
the fluid.
If there is no hydrocele, you may be able to detect
that the body of the testis feels a little more tense
than normal. Initially the epididymis is soft, but as
the inflammation subsides, it becomes hard and
craggy.
Relations and local tissues
The skin over the involved
testicle is oedematous and mobile. Should there be
no antibiotic treatment, the infection may spread
beyond the epididymis to the surrounding tissues
and the skin becomes fixed. If an abscess develops in
the epididymis, nowadays a rare event, it may point
and discharge through the area of skin fixation. As
the epididymis normally lies behind the testis, epi-
didymal disease involves the skin of the back of the
scrotum, so always remember to look at its posterior
aspect.
The spermatic cord is always thickened and ten-
der because epididymal infection spreads distally
from the urinary tract along the vas deferens.
The other testis should feel normal.
General examination
Pay particular attention to the
lower urinary tract. Rectal examination may reveal
tenderness of the prostate and seminal vesicles.
There may also be a fever and a tachycardia.
The para-aortic glands will not be tender.
Tuberculous epididymo-orchitis
History
This condition is now uncommon in the UK, but is
still seen in many other parts of the world. The tuber-
cle bacillus reaches the epididymis via the blood-
stream or by travelling along the vas from the lower
urinary tract. The infection develops slowly without
causing severe or acute pain or tenderness. There
may be systemic symptoms of tuberculosis, or only
the urinary tract may be involved.
Most patients complain of a lump in the scro-
tum, and an associated dull, aching pain.
Examination
On examination, the epididymis is hard, knobbly
and two or three times its normal size. A secondary
hydrocele is unusual. The spermatic cord is thickened
as far as you can feel. The vas deferens is often irreg-
ular and swollen and feels like a string of beads. This
physical sign is rare but is diagnostic of tuberculosis.
Tumours of the testis
There are two main varieties of testicular tumour:
■
seminoma – a carcinoma of the seminiferous
tubules,
■
teratoma – a malignant germ cell tumour.
There are some clinical features which help dif-
ferentiate between the two types, but usually the
diagnosis is made by the histopathologist.
History
Age
Teratoma commonly occurs between the ages
of 20 and 30 years but seminoma may occur a few
years later. Both are very rare in childhood and the
teenage years.
There is now high public awareness of this quite
uncommon condition, and the anxiety engendered
by a recently noticed scrotal swelling, particularly in
younger men, approaches that found in women
with a breast lump. The chance of malignancy in
these circumstances is substantially lower than with
the breast, and the swelling found is usually a nor-
mal epididymis.
Symptoms
The commonest presentation is a swell-
ing of the testicle, which is not usually painful.
Chap-13.qxd 4/19/05 14:30PM Page 354
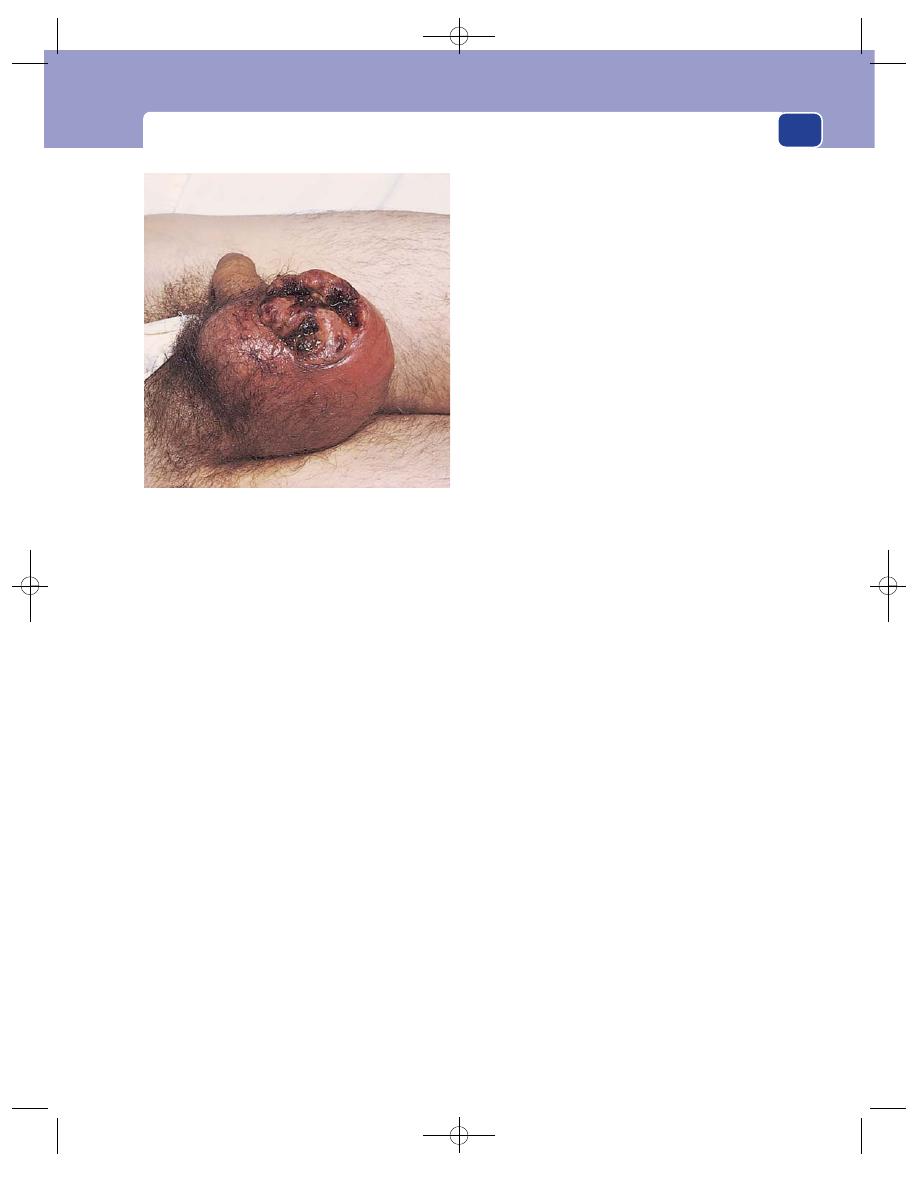
The testes
355
However, the occasional patient presents acutely
with a painful, tender testicle, and diagnosis is not
always straightforward.
Dull, aching, dragging pains in the scrotum and
groin occur in some patients, particularly if the
testis becomes significantly enlarged. An important
symptom to enquire about is whether the testicle
feels heavy. This is almost diagnostic of a testicular
tumour.
Presentation with distant metastases may occur
in many different ways, such as general malaise, loss
of appetite, wasting, abdominal pains and dyspnoea.
Cause
Many patients will state that their scrotal
symptoms followed an injury. Ignore this view unless
there is an obvious haematocele. It is better to explore
a testis for benign disease than to miss a tumour.
There is a considerably higher incidence of malig-
nant change in the incompletely descended testis. As
an incompletely descended testis will not, by defini-
tion, be in the scrotum, diagnosis will be difficult.
Examination
Position
The swelling is confined to the scrotum.
Temperature and colour
The scrotal skin should be
normal, except in the rare circumstance in which
the tumour has invaded and ulcerated through it.
Tenderness
Testicular tumours are not tender except
in the unusual acute presentation.
In many instances, normal testicular sensation
is lost. Ask the patient about this, as it is an import-
ant symptom of a testicular tumour, rarely associ-
ated with other conditions.
Shape
The majority of testicular tumours are not
noticed until they occupy the whole testis. Rarely,
you may be able to feel a nodule that is clearly in the
testis and not in the epididymis. A nodule that is in
the epididymis is never a tumour.
Testicular tumours are irregular and variable in
shape but are basically spherical.
Size
Tumours are noticed by the patient when the
testicle is clearly larger than its companion. Large
swellings are now uncommon in the UK because of
heightened public awareness.
Surface
This is usually smooth, but can be irregular
or nodular.
Composition
Testicular tumours feel harder than a
normal testis, are dull to percussion, not fluctuant
and not translucent.
Heaviness is an important physical sign. With
the patient lying on his back, place your fingers
underneath the testicle and lift it up. Compare it
with the normal side. A feeling of heaviness is char-
acteristic of a tumour.
Relations to surrounding tissues
The other testis should
be normal, but bilateral tumours occur in 2 per cent
of cases. The spermatic cord and the vas deferens
should be normal. Once the tumour breaks through
the tunica albuginea, it infiltrates the skin of the
scrotum.
Lymph drainage
Lymph from the testis drains to the
para-aortic lymph glands. Remember that these
glands lie in the centre of the abdomen above the
level of the umbilicus.
Seminomata commonly metastasize to the
para-aortic lymph glands, sometimes producing a
palpable abdominal mass. The inguinal glands will
only be enlarged if the tumour has spread to the
scrotal skin, a rare event.
General examination
Pay particular attention to all the
lymph glands, especially the para-aortic and supra-
clavicular groups.
FIG 13.24
A testicular tumour fungating through the
anterior surface of the scrotum. Note that the edge of the
scrotal skin is sloping and trying to heal.
Chap-13.qxd 4/19/05 14:30PM Page 355
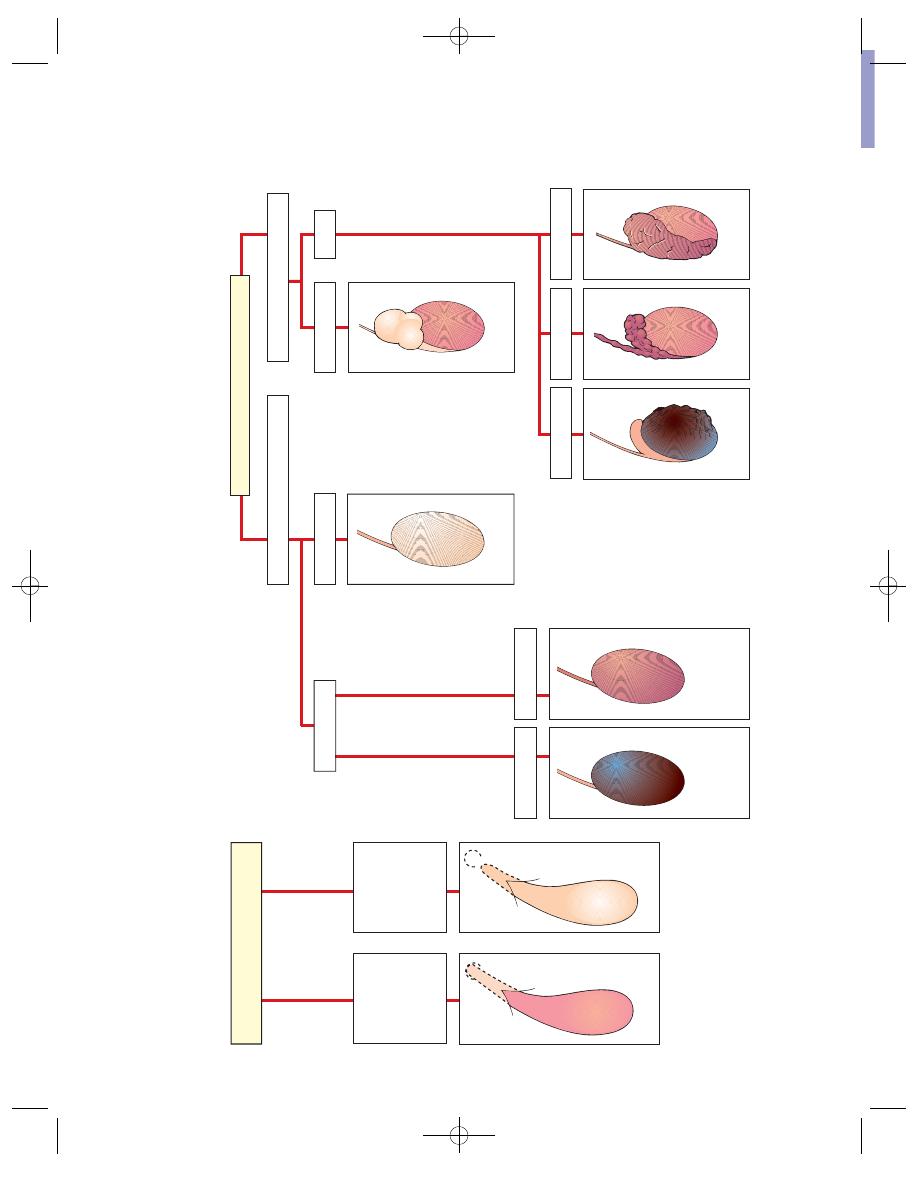
FIRST DECIDE THE ANSWERS TO THESE FOUR QUESTIONS
1 Can you get above the swelling?
2 Can you identify the testis and epididymis?
Cough impulse
Reducible
Testis palpable
Opaque
Hernia
Tender
Not tender
To
rsion
Severe epididymo-
orchitis
Acute haematocele
Chronic
haematocele
Gumma
Tumour
Infantile hydrocele
No cough impulse
Not reducible
Testis not palpable
Tr
anslucent
Testis and epididymis not definable
Opaque
Vaginal hydrocele
Acute epididymo-
orchitis
Tumour
Not tender
Tuberculous
epididymis
Tender
Not tender
Cyst of epididymis
SWELLINGS NOT CONFINED
TO THE SCROTUM
SWELLINGS CONFINED TO THE SCROTUM
Tr
anslucent
Tr
anslucent
Opaque
Testis and epididymis definable
3 Is the swelling translucent?
4 Is the swelling tender?
FIG
13.25
A plan for the dia
gnosis of scrotal s
wellings.
A PLAN FOR THE DIAGNOSIS OF SCRO
TAL SWELLINGS
Chap-13.qxd 4/19/05 14:30PM Page 356
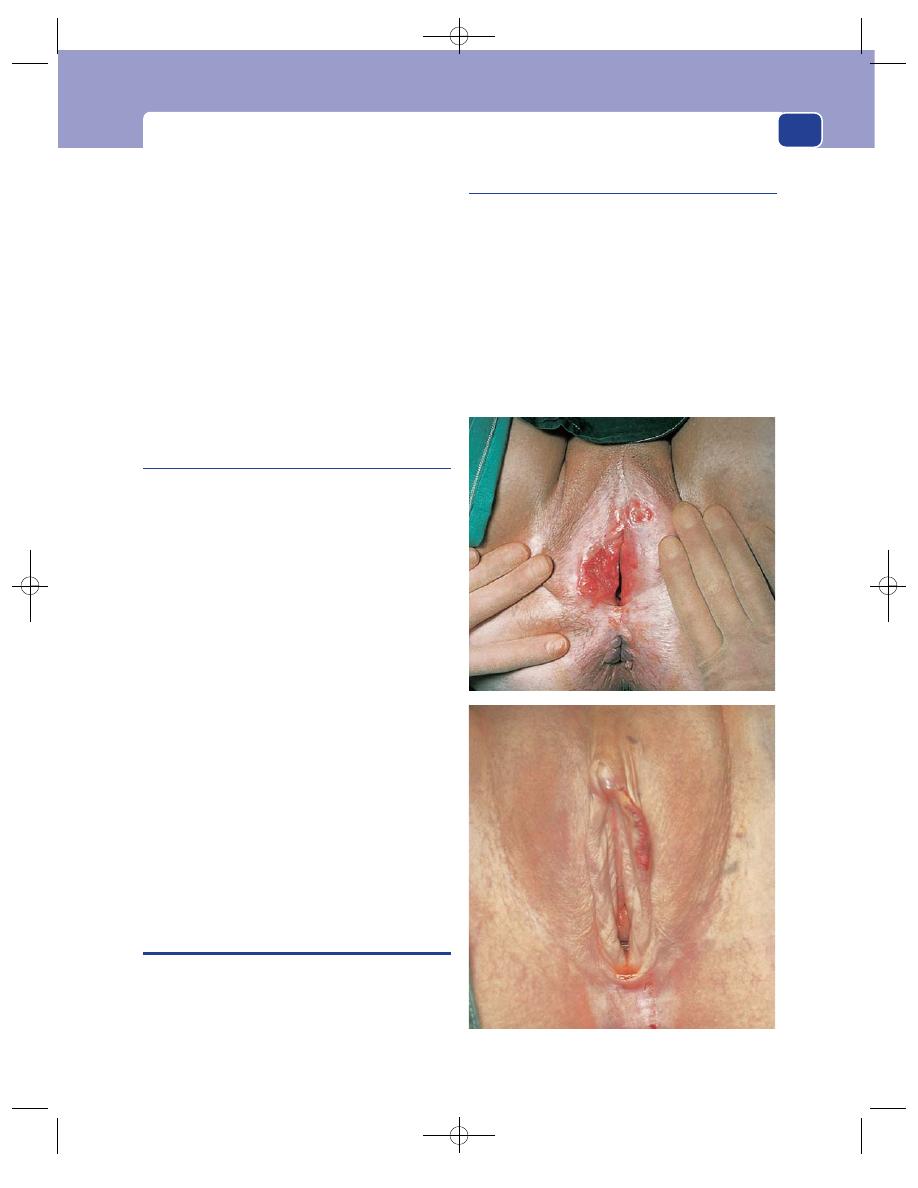
The female external genitalia
357
Testicular tumours may metastasize to any tissue
in the body. Unusual swellings may be detected on
general examination. Lung metastases are usually
peripheral and not detectable on clinical examin-
ation, but are readily visible on a chest X-ray.
Differential diagnosis
The testicular swellings likely
to be confused with tumours are acute and chronic
epididymo-orchitis, and haematocele. However, if
the patient tells you that his testicle feels heavy,
you find that testicular sensation is lost, and the
enlarged testis feels, to you, heavier than the other
side, the diagnosis of testicular tumour is almost
certain.
Chronic testicular pain
This is a common reason for referral to a surgical
clinic. The patient is a young or middle-aged
man. The pain may be localized to the testicle or
it may radiate to the groin. It may be associated
with exercise and movement, or sitting in certain
positions.
Common findings are:
■
a mildly tender but otherwise normal
epididymis, occasionally associated with a
chlamydial urinary tract infection;
■
a small epididymal cyst: differentiation from a
normal epididymis may be difficult;
■
an inguinal hernia: the skin of the scrotum is
supplied by the genito-femoral nerve, which
may be compressed in the groin by a hernia,
causing discomfort referred to the testicle;
■
rarely, but significantly, a testicular tumour;
■
nothing abnormal.
The possibilities are many, but frustratingly for
both patient and doctor, there may be no physical
signs and a diagnosis cannot be made. In this case,
the symptom usually settles with time.
THE FEMALE EXTERNAL GENITALIA
Most complaints about the external genitalia are
referred to gynaecologists and are described in
detail in their textbooks, but there are three com-
mon conditions that quite often appear in a general
surgical clinic.
Bartholin cyst
Bartholin’s glands are a pair of small glands that lie
at the sides of the lower end of the vagina, and
whose ducts open on to the inner side of the poster-
ior part of the labium minus. They are normally
impalpable. When the duct of a gland is distended
by obstruction or infection, it forms a cystic
swelling in the posterior part of the labium majus.
The site betrays the diagnosis.
FIG 13.26
Two examples of carcinoma of the vulva.
Chap-13.qxd 4/19/05 14:30PM Page 357
The external genitalia
358
Urethral caruncle
This is a bright-red, polypoid granuloma that arises
from the mucosa of the urethral orifice in post-
menopausal women. It is very tender and causes
painful micturition, dyspareunia and occasional
bleeding.
The differential diagnosis is urethral prolapse,
which is purple in colour and not so tender.
Carcinoma of the vulva
Carcinoma of the vulva usually takes the form of a
chronic ulcer with an everted edge.
The patient complains of pain, a purulent or
bloody discharge and sometimes of a lump in the
labia. Very small carcinomata can metastasize early
and present with enlargement of the inguinal
glands. The primary ulcer can be small and hidden
in the folds of the labia.
There will usually be evidence of pre-malignant
changes in the surrounding skin (vulval intra-
epithelial neoplasia).
Chap-13.qxd 4/19/05 14:30PM Page 358
The abdominal wall, herniae and
The abdominal wall has a complex structure and
many of the surgical conditions affecting it are
embryological in origin. It develops laterally from
the vertebral column, later than the intestinal tract,
and ultimately fuses in the mid-line to form a seam-
like fibrous cord, the linea alba. This is pierced at the
umbilicus by the umbilical cord, which in early
embryonic life contains the yolk sac and the entire
mid-gut. The testes develop in the peritoneum of
the posterior abdominal wall and migrate through
the muscles just above the inguinal ligament into the
scrotum followed by the spermatic cord. It is thus
hardly surprising that there are many weak areas in
the abdominal wall.
The abdominal wall is also afflicted by many of
the common skin, subcutaneous, fascial and muscle
tissue lesions described elsewhere, which can be just
as difficult to diagnose as when they appear in other
sites.
It is important to decide whether any abdominal
swelling is deep to, or part of, the abdominal wall.
This may be established by palpating the lump with
the abdominal wall relaxed and then with it tense. A
lump deep to the abdominal wall becomes impalp-
able when the abdominal muscles contract. A lump
superficial to the muscles becomes more prominent.
Do not forget to apply this simple reliable test to all
abdominal swellings.
Contracting the abdominal muscles
If you ask a patient to lift their head and shoulders
off the couch, they will contract their abdominal
muscles – provided they do not lever themselves up
with their elbows, which the elderly tend to do.
Another way to achieve contraction of the abdominal
muscles is to lift the patient’s heels yourself and then
ask the patient to hold them in that position. This
tenses the rectus abdominis muscle very effectively
and any mass deep to it will become impalpable
unless it is huge. However, frail elderly patients may
be unable to maintain a sustained contraction of
their abdominal muscles, whatever method you try.
Swellings in the rectus sheath
Acute
The inferior and superior epigastric arteries lie deep
to, or within, the rectus abdominis muscles. If these
muscles contract suddenly and violently, the epigas-
tric arteries may be torn. The haematoma which then
develops within the muscle causes pain and swelling.
Rupture of the inferior epigastric artery occurs
in athletes and during coughing in elderly patients
with chronic obstructive airways disease, especially
if they are taking steroid medication. The blood
spreads within the muscle, but as there is no poster-
ior rectus sheath below the arcuate line (the lower
edge of the posterior rectus sheath, mid-way between
the pubis and the umbilicus), the blood spreads out
into the extraperitoneal area of the iliac fossa.
The patient complains of pain and tenderness in
the iliac fossa, right or left, which is made worse by
contracting the abdominal muscles. Examination
reveals a diffuse, tender mass in the iliac fossa, deep to
the abdominal wall. Skin discolouration may appear
a few hours after the onset of the pain. If the pain is
not made worse by contracting the rectus abdominis
muscle, and if there is no bruise in the skin, the
condition may be confused with acute appendicitis,
but there will be none of the systemic features of
the latter.
Rupture of the superior epigastric artery may
follow a bout of violent coughing, and cause pain and
tenderness in the upper abdomen, made worse by
Chap-14.qxd 4/21/05 12:54AM Page 359
The abdominal wall, herniae and the umbilicus
360
tensing the abdominal muscles and by deep breath-
ing. A bruise may appear below the costal margin
12–24 hours later. When this condition occurs on the
right-hand side it can be confused with cholecystitis.
Tears of the muscle fibres alone, with no major ves-
sel disruption, may also cause rectus sheath haema-
tomata.
Chronic
Chronic haematomata
Patients occasionally present
with a painless mass which examination reveals to
be in the rectus sheath. The most likely cause is a
chronic rectus sheath haematoma with the acute
phase forgotten or not noticed. Discrete swellings
are more likely to occur in the upper abdomen, con-
fined by the fibrous intersections in the upper part
of the muscle.
The swelling will be firm to hard, clearly in the
abdominal wall and without a definite edge because
it is deep seated.
Sarcomata
The rare desmoid tumour and other
sarcomata may arise in the rectus sheath.
Lipomata
The most common swelling found in the
anterior abdominal wall, superficial to the rectus
sheath, is the subcutaneous lipoma. This is clearly in
the subcutaneous fat and displays the smooth sur-
face, rolled edge and pseudo-fluctuant consistence
characteristic of the condition. Such lipomata are
either solitary or multiple. Multiple lipomata are
rarely bigger than 2–3 cm across and are also found
in the chest wall and limbs (but never below the
knee). They may be familial and tender, a condition
sometimes called Dercum’s syndrome.
ABDOMINAL HERNIAE
A hernia is the protrusion of an organ through its
containing wall. The term can be applied to the her-
niation of a muscle through its fascial covering, to
the herniation of brain through a fracture of the
skull or through the foramen magnum into the
spinal canal, as well as to the protrusion of an intra-
abdominal organ through a defect in the abdominal
wall, pelvis or diaphragm.
Before an organ can herniate through its retain-
ing wall there must be a weakness in that wall. This
may be a normal weakness, found in everyone, and
related to the anatomical configuration of the area
such as a place where a vessel or viscus enters or
leaves the abdomen. Alternatively, the weakness may
be due to a congenital abnormality, or acquired as a
result of trauma or disease.
This chapter deals with abdominal herniae,
excluding those through and around the oesophageal
hiatus. There are a few common varieties and a larger
number of rarities. The common ones in order of
frequency in adult life are:
■
inguinal
■
umbilical
■
incisional
■
femoral
■
epigastric.
In childhood, umbilical hernia is more common
than inguinal hernia.
You seldom need to remember rarities, but it is
important to have some knowledge of the rare types
of abdominal herniae, because failure to diagnose
any type of strangulated hernia, common or rare,
may lead to the patient’s death. They are:
■
spigelian
■
obturator
■
lumbar
■
gluteal
Herniae occur frequently in both sexes. Inguinal
hernia affects 9 per cent of men at some time in
their lives and 1 per cent of women.
Although the femoral hernia is found more often
in women than in men, the commonest hernia in
women is the inguinal hernia.
Certain physical signs are common to all herniae
but are not always present:
■
they occur at congenital or acquired weak spots
in the abdominal wall;
■
most herniae can be reduced;
■
most herniae have an expansile cough impulse.
The last two signs may be absent, especially if the
hernia is tightly constricted at its neck, so their
absence does not exclude the diagnosis of hernia.
The diagnosis of a hernia is therefore made ini-
tially by the site and confirmed by the presence of
reducibility and an expansile cough impulse. It may
also be made when these signs are absent, by the
exclusion of other causes of a lump.
Chap-14.qxd 4/21/05 12:54AM Page 360
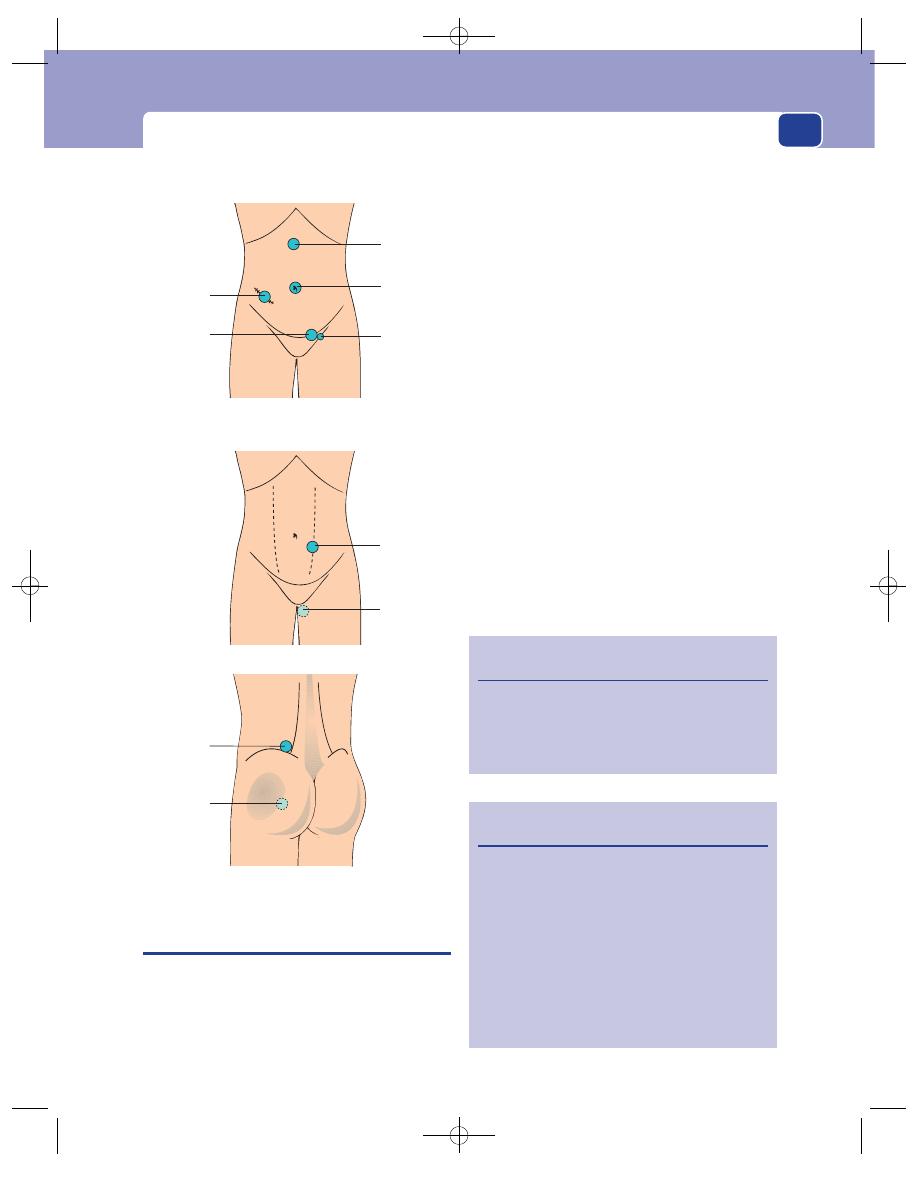
Inguinal hernia
361
INGUINAL HERNIA
An inguinal hernia is the protrusion of part of the
contents of the abdomen through the inguinal region
of the abdominal wall. To understand inguinal her-
niae it is necessary to understand the anatomy of
the inguinal canal (Fig. 14.2).
Surface anatomy
The inguinal ligament stretches between the anterior
superior iliac spine, which is easy to see and feel, and
the pubic tubercle, which is not. A skin crease runs
across the lower abdomen, convex downwards, sep-
arating the abdomen from the triangle known as the
mons veneris. The centre of this crease lies over the
upper edge of the pubic bones. The pubic tubercles
lie beneath this crease, approximately 2–3 cm either
side of the mid-line. To find a pubic tubercle, put
your finger on the centre of this skin crease, push
gently inwards until you feel the crest of the pubis,
and then slide your finger sideways until you reach
the tubercle. You can practise this on yourself.
Muscles
Beneath the skin and subcutaneous tissue lies the
aponeurosis (a word meaning a flat tendon) of the
external oblique muscle. The lower inwardly folded
edge of this aponeurosis, which runs between the
anterior superior iliac spine and pubic tubercle, forms
the inguinal ligament. The fibres of the aponeurosis
run parallel to the inguinal ligament in the direction
taken by a hand when placed in a trouser pocket,
The rare herniae
The common herniae
Epigastric
Umbilical
Inguinal
Femoral
Incisional
Spigelian
Obturator
Lumbar
Gluteal
FIG 14.1
The sites of herniae.
Revision panel 14.1
The basic features of all herniae
They occur at a weak spot
They reduce on lying down, or with direct
pressure
They have an expansile cough impulse
Revision panel 14.2
The causes of abdominal herniae
An anatomical weakness where:
■
structures pass through the abdominal wall
■
muscles fail to overlap
■
there are no muscles, only scar tissue (e.g.
umbilicus)
An acquired weakness following trauma
High intra-abdominal pressure from:
■
coughing
■
straining
■
abdominal distension
Chap-14.qxd 4/21/05 12:54AM Page 361
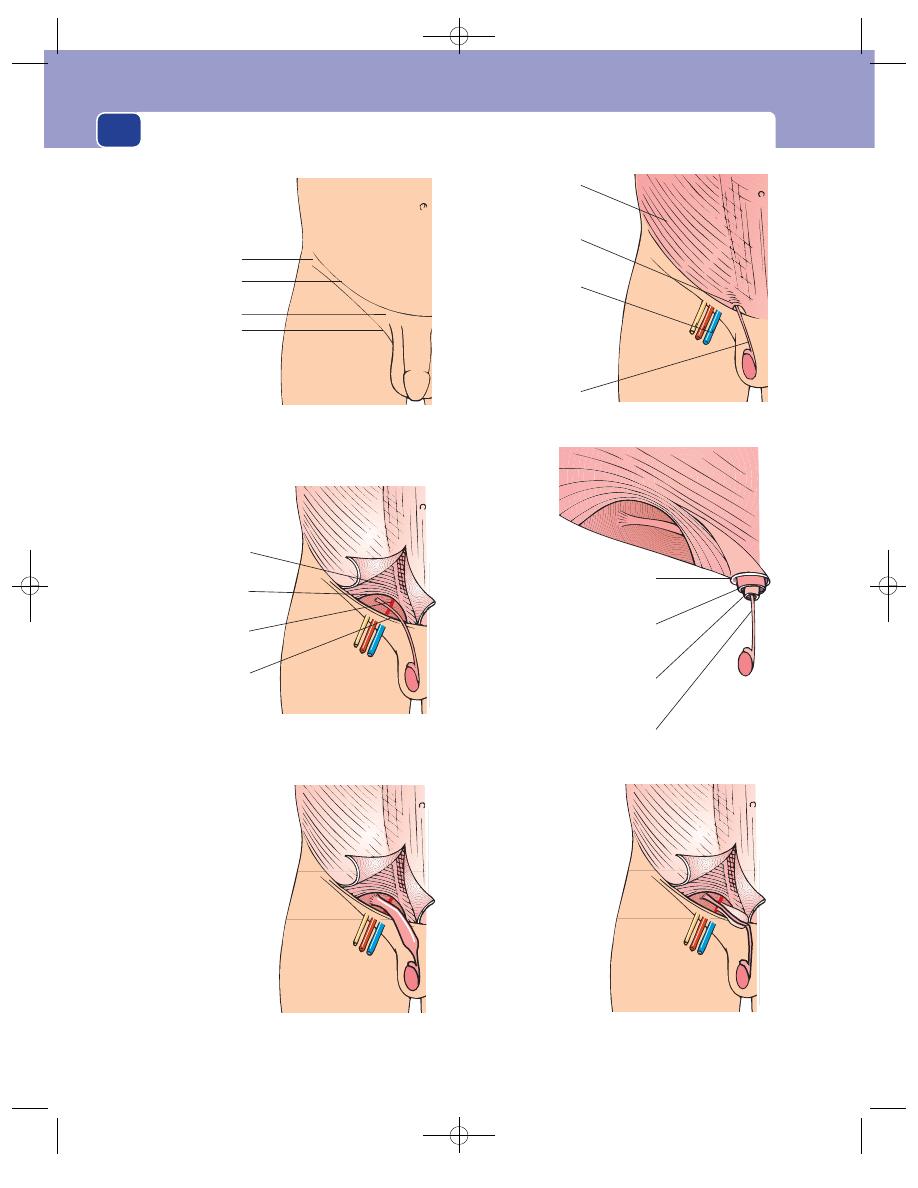
The abdominal wall, herniae and the umbilicus
362
The internal oblique muscle
The coverings of the spermatic cord
External spermatic
fascia from external
oblique
Cremasteric fascia
and muscle from
internal oblique
Internal spermatic
fascia from
transversalis fascia
Vas deferens
Internal oblique
muscle
Internal inguinal
ring
Inferior epigastric
artery
Transversalis
fascia
Anterior superior
iliac spine
Abdominal
crease
Pubic tubercle
Groin crease
Surface landmarks
External oblique
aponeurosis
External
inguinal ring
Femoral vessels
and nerve
Spermatic cord
The external oblique muscle
An indirect
inguinal hernia
Sac begins at the
internal ring and
is inside the
spermatic cord
A direct inguinal
hernia
Sac appears medial
to the inferior
epigastric artery
and is outside the
spermatic cord
FIG 14.2
The anatomy of the inguinal region.
Chap-14.qxd 4/21/05 12:54AM Page 362
Inguinal hernia
363
and separate above the crest of the pubis to form the
external inguinal ring.
Deep to the external oblique aponeurosis are the
lowermost fibres of the internal oblique muscle aris-
ing from the lateral half of the inguinal ligament.
They run medially in an arch, convex upwards, to
the edge of the rectus abdominis muscle, where they
join the aponeurosis of the transverse abdominal
muscle to form the anterior rectus sheath. At this
point the fused aponeuroses are known as the
conjoined tendon.
The half-moon gap beneath the arch of the inter-
nal oblique muscle is the weak spot of the inguinal
region. The tissue filling the gap is not very strong
and is called the transversalis fascia. This area is
crossed by the inferior epigastric artery as it runs
upwards (from the femoral artery), curving medi-
ally towards the rectus sheath. The point where the
vas deferens and testicular artery pierce the trans-
versalis fascia is lateral to the inferior epigastric
artery and known as the internal inguinal ring.
Indirect inguinal hernial sacs leave the abdomen at
this point. Direct inguinal herniae push through the
weak area of the posterior wall medial to the inferior
epigastric artery. Remember that the exit point of an
indirect hernia is lateral to this artery and that of
a direct hernia medial to it. You cannot palpate the
inferior epigastric artery, but the femoral pulse,
which can be felt at the mid-inguinal point (halfway
between the anterior superior iliac spine and the
mid-line pubic symphysis), will tell you where it
begins. The important clinical point is that the exit
point of an indirect hernia is lateral to that of a
direct hernia.
As the vas deferens enters the inguinal canal it
takes with it a thin layer of fascia derived from the
transversalis fascia called the internal spermatic fascia.
Further down the canal it collects a covering of
muscle fibres and fascia from the internal oblique
muscle. These coverings are called the cremaster
muscle and cremasteric fascia. Finally, as the vas
passes through the external ring, it acquires another
thin layer of fascia derived from the external oblique
aponeurosis called the external spermatic fascia.
Because the sac of an indirect inguinal hernia
comes down obliquely alongside the vas deferens
inside the spermatic cord, it has an easy path of lit-
tle resistance down into the scrotum. The three
fascial layers of the cord funnel the peritoneal sac
towards the scrotum. By contrast, the sac of a direct
inguinal hernia begins medial to the epigastric artery,
outside the spermatic cord with its three external
layers of tissue, and so has no easy path to the scro-
tum, which in consequence it rarely enters.
Technique for the examination of an
inguinal hernia
Ask the patient to stand up
It is not possible to see the true size of a hernia, exam-
ine it properly or even detect it at all when the patient
is lying down. If you suspect the diagnosis from the
history, start the examination with the patient stand-
ing. If, during a routine supine abdominal examin-
ation, you discover a lump that looks like a hernia,
complete the routine examination and then ask the
patient to stand up in order to examine it properly.
Always examine both inguinal regions.
Look at the lump from in front
It is essential to see the exact site and shape of the
lump. With practice you will be able to distinguish
an inguinal from a femoral hernia at sight because
the bulge of an inguinal hernia begins well above
the crease of the groin, whereas a femoral hernia is
more medial and related to the medial end of the
groin crease.
Inspection will also reveal whether the lump
extends down into the scrotum, if there are any
other scrotal swellings and if there are any swellings
on the ‘normal’ side.
Feel from the front
1. Examine the scrotum and its contents. It is
not unusual to find an epididymal cyst or a
hydrocele as well as a hernia because they are
all common conditions.
2. In men, first decide if the lump is a hernia or a
true scrotal lump by examining its upper edge.
If you can ‘get above it’ (i.e. feel its upper edge
between your thumb and index finger and a
normal spermatic cord above it), it must be a
scrotal swelling and not a hernia. If you cannot
feel the upper edge of the lump because it passes
into the inguinal canal, it is likely to be a hernia,
except in children, when it might be an encysted
hydrocele of the cord (page 372).
Chap-14.qxd 4/21/05 12:54AM Page 363
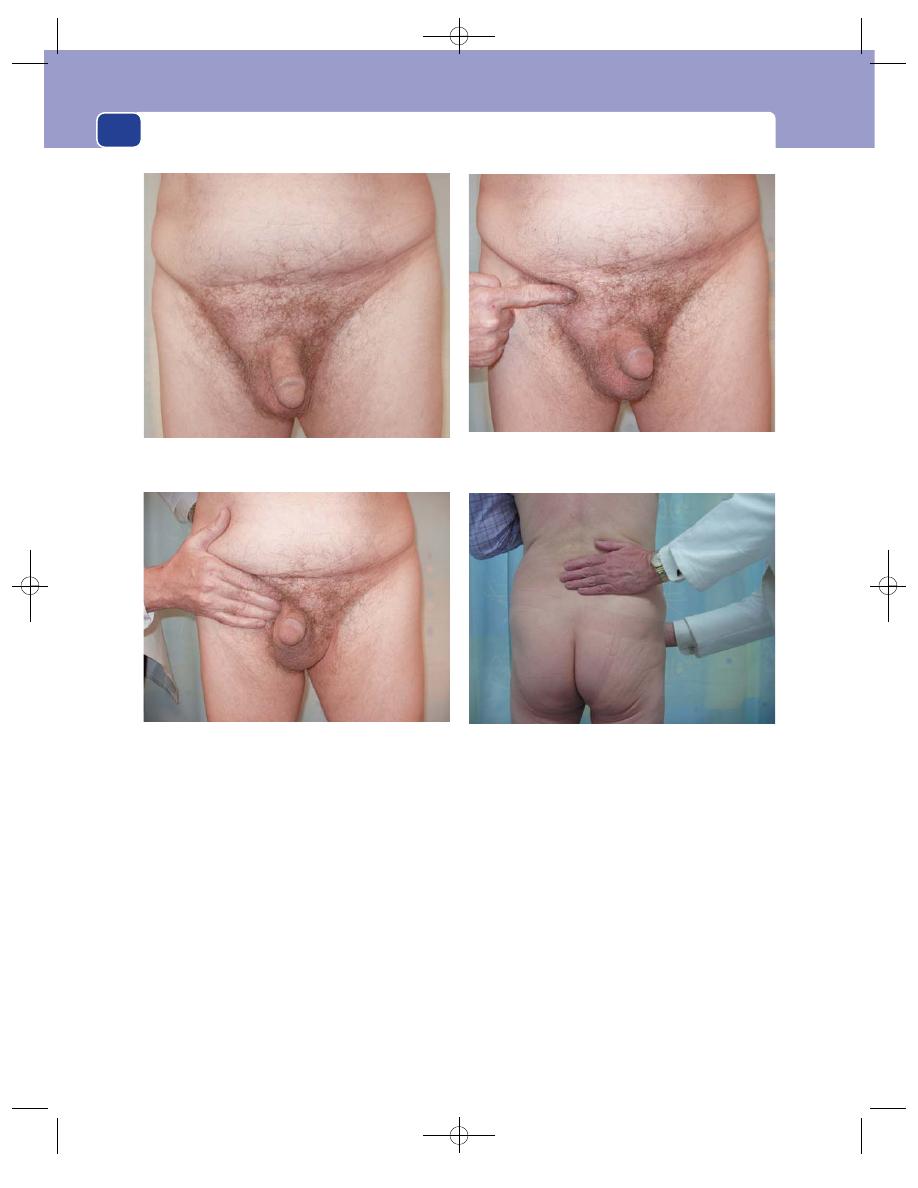
The abdominal wall, herniae and the umbilicus
364
3. Do not examine the external ring or palpate
the pubic tubercle by pushing a finger up along
the spermatic cord into the neck of the scrotum.
This is a painful, unnecessary method of
examination that very rarely yields useful
information.
Feel from the side
Having examined the scrotal contents and decided
that you cannot get above the lump, you can make a
provisional diagnosis of inguinal hernia and pro-
ceed to examine the lump itself.
Stand at the side of the patient, on the same side
as the hernia. Place one hand in the small of the
patient’s back to support him, and your examining
hand on the lump with your fingers and arm
roughly parallel to the inguinal ligament.
You must now ascertain the following facts about
the lump:
■
position
■
temperature
■
tenderness
■
shape
■
size
FIG 14.3
TECHNIQUES FOR THE EXAMINATION OF AN INGUINAL HERNIA.
Place your examining hand flat on the groin parallel to the inguinal ligament and your other hand on the patient’s back to stop
you pushing him over. You will then be able to manipulate and probably reduce the hernia with ease.
The upper crease of the mons veneris indicates the crest of
the pubis and the level of the pubic tubercle. Note that it is
not low down in the crease of the groin.
Ask the patient to stand up. When palpating the groin, stand
at the patient’s side.
Chap-14.qxd 4/21/05 12:54AM Page 364
Inguinal hernia
365
■
tension
■
composition (solid, fluid, or gaseous)
■
reducibility.
Expansile cough impulse
Compress the lump firmly with your fingers, then
ask the patient to turn his head towards the opposite
side, and then to cough. If the swelling becomes
tense and expands with coughing, it has a ‘cough
impulse’. Movement of the swelling without expan-
sion or an increase in tension is not a cough impulse.
A localized swelling in the spermatic cord or an
undescended testis will sometimes move down the
inguinal canal and come out through the external
ring during coughing, and look exactly like a hernia,
but neither will get bigger or more tense during
coughing. The presence of an expansile cough impulse
is diagnostic of a hernia, but its absence does not
exclude a diagnosis of hernia because the neck of
the sac may be blocked by adhesions, which prevent
the movement of additional viscera into the sac
during coughing.
Is the swelling reducible?
The main reason for standing at the side of the
patient is to be able to place your hand in exactly the
same position as the patient places his own hand
when he is reducing or supporting the hernia. He
puts his hand on the lump and lifts it upwards and
backwards. You must do the same. You can only do
this if your arm comes from a position above and
behind the hernia.
First, press firmly to reduce the tension of the
lump. Then gently compress the lower part of the
swelling. As the lump gets softer, lift it up towards
the external ring. Once it has all passed in through
this point, slide your fingers upwards and laterally
towards the internal ring to see if the hernia can be
controlled (kept inside) by pressure at this point.
If the lump reduces into or through the abdom-
inal wall at a point above and medial to the pubic
tubercle, it is an inguinal hernia. If the point of
reduction is below and lateral to the pubic tubercle,
it is a femoral hernia.
Note that this method of differentiation refers to
the point where the lump reduces, not the position
of the unreduced hernia, because once a hernia
reaches the subcutaneous tissue it can expand and
spread in any direction.
If the hernia can be held reduced only by pressure
over the external inguinal ring, it is a direct inguinal
hernia. If it can be controlled by pressure over the
internal ring, it is an indirect inguinal hernia.
If there is any difficulty in reducing the hernia,
ask the patient to lie down and try again. This will
also allow you to examine the abdomen (see below).
Remove your hand and watch the hernia
reappear
The direction of movement of the swelling and the
way in which it reappears will help to confirm your
deductions about its site of origin.
A reappearing indirect hernia will seem to slide
obliquely downwards along the line of the canal,
whereas a direct hernia will project directly forwards.
Comment. It may be impossible, particularly in
the obese, to differentiate between these two types
of hernia with any certainty, but attempting to do so
ensures that you conduct a thorough examination.
Percuss and auscultate the lump
If there is gut in the sac, it may be resonant and
there may be audible bowel sounds.
Feel the other side
Move to the other side of the patient and examine
that inguinal region. Inguinal herniae are com-
monly bilateral, particularly when they are direct.
Even when you cannot see or feel a lump, ask the
patient to cough whilst you are palpating the inguinal
canal. There may be a small bulge that is only made
detectable by the raised intra-abdominal pressure
produced by coughing.
Examine the abdomen
Look particularly for anything that may be raising
the intra-abdominal pressure, such as a large blad-
der, an enlarged prostate, ascites, chronic intestinal
obstruction or pregnancy.
With the patient lying flat, ask the patient to cough
as you observe the groin. Particularly in a slim adult,
you may see the contents entering the sac, which
will help you to decide if the hernia is direct or indir-
ect. With a direct hernia, the swelling will advance
directly upwards towards you. With an indirect her-
nia, you may be able to see oblique motion from the
internal ring to the neck of the scrotum. Indirect
herniae are sometimes referred to as oblique herniae.
Chap-14.qxd 4/21/05 12:54AM Page 365
The abdominal wall, herniae and the umbilicus
With the patient in this position, it is easier to
decide if a hernia is femoral. Femoral herniae rarely
reduce into the abdomen on lying down, and will be
found to be below the inguinal ligament and rather
more lateral than an inguinal sac extending down-
wards to the same level.
Cardiovascular and respiratory assessment
Assess the cardiovascular and respiratory systems
with the patient’s fitness for operation in mind.
Symptoms and signs of an
inguinal hernia
History
(elective presentation)
Age
Inguinal herniae may appear at any age. They
may be present at birth or appear suddenly in an 80
year old. The peak times of presentation are in the
first few months of life, in the late teens and early
twenties, and between 40 and 60.
Occupation
Heavy work, especially lifting, puts a
great strain on the abdominal muscles. If there is an
underlying weakness, the appearance of a hernia
may coincide with strenuous physical effort, or it
may be first noticed at such a time. Despite the fact
that herniae are no more common in manual work-
ers than in office workers, compensation law in many
countries accepts that a hernia may be an industrial
injury.
Local symptoms
The commonest symptoms are dis-
comfort and pain. The patient complains of a drag-
ging, aching sensation in the groin, which gets worse
as the day goes on.
If the hernia becomes very painful and tender, it
is probably strangulated. There may be pain long
before a lump is noticed.
On the other hand, many herniae cause no pain
and the patient presents having noticed a swelling in
the groin or in the scrotum. The lump gets smaller
on lying down and the patient may have noticed that
the swelling can be pushed back into the abdomen.
Symptoms may be bilateral.
Other abdominal symptoms
A loop of bowel in the sac
of a hernia may become obstructed. Obstruction is
associated with a colicky pain caused by bowel dis-
tension because bowel pain is mediated via sympa-
thetic afferent nerves and hence felt, not in the
groin, but in the mid-line of the abdomen, at a level
which depends on which part of the intestine is
involved. The pain occurs when the bowel is trapped
in the sac of the hernia and resolves when the bowel
is reduced into the abdomen.
Large herniae may interfere with bowel activity
and cause a change in bowel habit.
However, beware: patients with a carcinoma of
the left colon, or diverticular disease, may experi-
ence progressive constipation and hence increased
straining during defaecation. The increase in abdom-
inal pressure that accompanies straining may make
a coincidental hernia more prominent, and lead the
patient to attribute their symptoms to the hernia.
Therefore you must enquire of all patients present-
ing with a hernia whether their bowel action has
recently changed and investigate any significant
bowel symptoms in their own right before dealing
with the hernia.
It is also usual to ask about other diseases which
may have cause increased abdominal pressure, such
as chronic bronchitis with persistent coughing, and
difficulty with micturition.
History
(emergency presentation)
Herniae, pre-existing or just discovered, often pres-
ent as a surgical emergency. The patient may notice
that the groin swelling will not reduce or that it is
painful and tender. This may be associated with the
cardinal symptoms of intestinal obstruction – colicky
abdominal pain, vomiting, distension and absolute
constipation. The hernial orifices of any patient with
intestinal obstruction must always be carefully exam-
ined, as the patient may not have noticed a small
lump in their groin. This is particularly common
with femoral herniae.
The definitions of the terms irreducible, incar-
cerated, obstructed and strangulated, which are
freely used in the description of herniae, must be
understood.
Irreducible means simply what it states, that the
contents of the hernia sac cannot be replaced into
the abdomen. An irreducible hernia may be associ-
ated with three other categories of complication –
incarceration, obstruction and strangulation.
Incarcerated means that contents are literally
imprisoned in the sac of the hernia (usually by adhe-
sions) but are alive and functioning normally. An
incarcerated hernia is not tender.
366
Chap-14.qxd 4/21/05 12:54AM Page 366
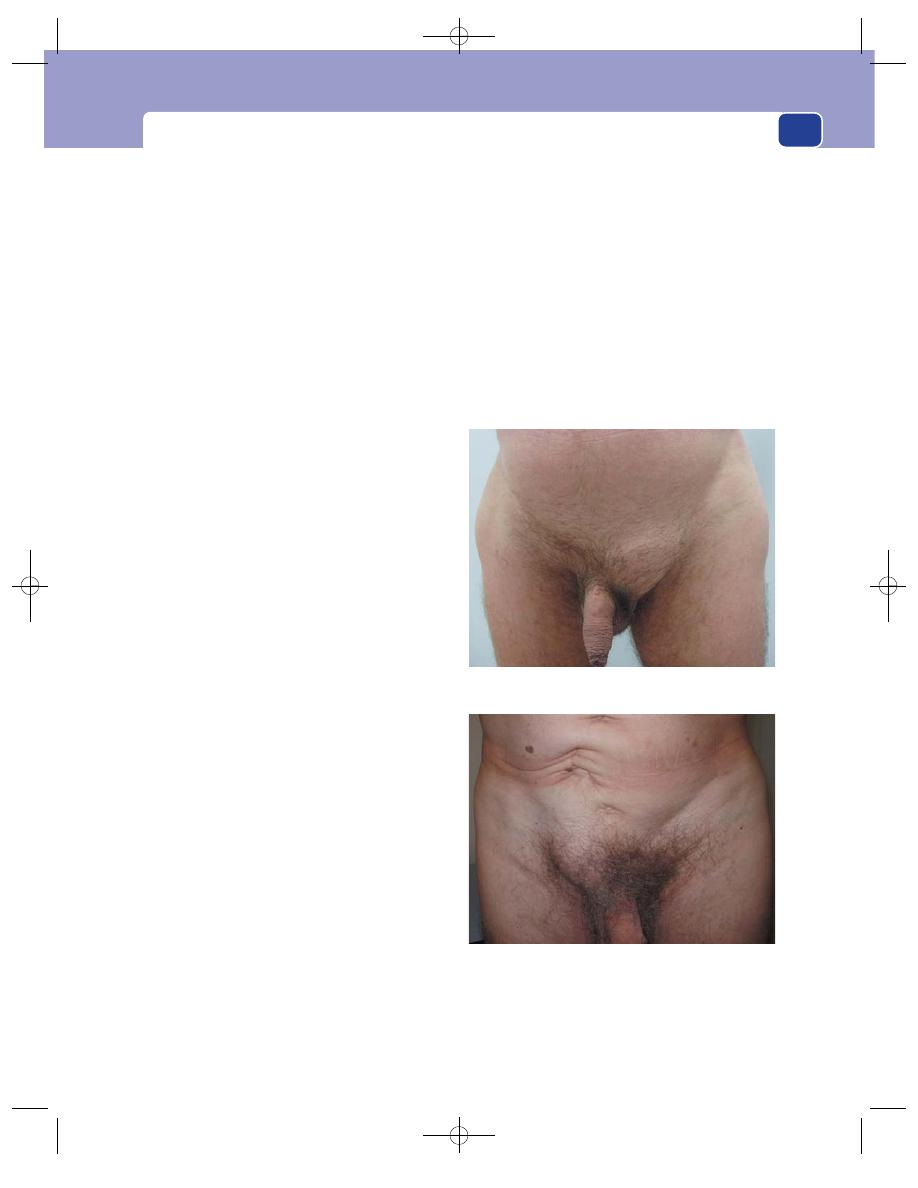
Inguinal hernia
367
Obstructed means that a loop of bowel is kinked
or trapped within the sac of the hernia in such a way
that its lumen but not its blood supply is obstructed.
The bowel is therefore alive and the patient has the
signs and symptoms of intestinal obstruction but
not of strangulation. The hernia will not be unduly
tender.
Strangulation means that the blood supply to the
contents of the sac has been cut off and they are
dead or dying. The patient will usually be obviously
unwell and the swelling will be acutely tender. An
entrapment that interferes with the blood supply to
the bowel wall will usually obstruct its lumen, so
most strangulated herniae containing bowel have
intestinal obstruction.
However, there is variety of strangulated hernia
in which only a segment of the bowel wall is trapped
and the lumen remains patent. The strangulation
makes the hernia very tender but there are no symp-
toms or signs of intestinal obstruction. This is called
Richter’s hernia.
Examination
The principal features to be determined are the site,
size and constituents of the lump, together with the
two diagnostic signs, reducibility and the presence
of an expansile cough impulse.
Position
An inguinal hernia will be visible in the
groin in all but the obese. The anatomical land-
marks and the site and line of direction of indirect
and direct hernias are described above.
Note that once a hernia has passed through the
external inguinal ring it can spread out into the loose
subcutaneous tissue under the membranous layer of
the superficial fascia and, if it is indirect, descend to
fill the scrotum. The oft-quoted description that the
inguinal hernia is found ‘above and medial to the
pubic tubercle’ refers not to the position of the whole
hernia, but to the point at which the hernia reduces
into the abdominal wall (the external inguinal ring).
Colour
The skin colour over an inguinal hernia
should be normal. If the hernia is strangulated, the
skin may be reddened. If the patient has worn a
truss for many years, the skin over the external
inguinal ring may be scarred and pigmented.
Temperature
The temperature of the skin overlying
a hernia will be the same as the surrounding skin
except when the hernia is strangulated. In this event
the skin may be warm.
Tenderness
A hernia may contain any viscus and, as
all abdominal structures have a visceral sensory
innervation, manual pressure is uncomfortable but
not truly painful. By contrast, a strangulated hernia
is very tender. An irreducible, non-strangulated
hernia is not tender to light pressure, but any attempt
at reduction by excessive pressing and squeezing can
cause considerable pain.
Shape
An indirect hernia moving obliquely along
the inguinal canal towards the scrotum is sausage
This is a right direct recurrent inguinal hernia. The original
inguinal hernia probably developed because of the disruption
and distortion of the abdominal wall caused by the previous
abdominal operation. Always look for a scar in the groin. The
bulge is coming out directly towards you.
FIG 14.4
INGUINAL HERNIAE.
A left indirect inguinal hernia, moving obliquely down towards
the scrotum.
Chap-14.qxd 4/21/05 12:54AM Page 367
The abdominal wall, herniae and the umbilicus
368
shaped, but when it extends beyond the external
inguinal ring it widens out to become pear shaped.
A direct hernia is usually round, like a plum in the
groin.
Size
Inguinal herniae vary from very small bulges
which are just detectable, to large masses descend-
ing almost to knee level. The larger a hernia is, the
more likely it is to be irreducible.
Surface
The surface will vary according to the nature
of the contents but is usually smooth. In a large
hernia it is sometimes possible to palpate indentable
faeces inside an incarcerated segment of colon.
Composition
Herniae that contain gut should be soft,
resonant and fluctuant, and you may be able to hear
bowel sounds. If the contents within the sac are tense,
the hernia will feel hard, but if it contains bowel, it
should still be resonant and fluctuant. Visible peri-
stalsis may be observed with a large scrotal hernia
containing small intestine.
Many herniae contain omentum, which makes
them feel firm (rubbery), non-fluctuant and dull to
percussion.
Cough impulse
A hernia will nearly always become
larger and more tense in all directions during cough-
ing, which is referred to as an expansile cough
impulse. Most lumps in the groin move up and down
with coughing, an impulse transmitted from the
abdominal wall. Only herniae and vascular tumours
expand in all directions.
Compressibility
A hernia can be compressed by steady
pressure but, unlike vascular tumours displaying the
same physical sign, it will not expand immediately
the compression is released unless some force, such
as gravity or coughing, forces it out.
Reducibility
A cardinal physical sign of a hernia is
reducibility. This means that it is possible to return
the contents of the hernia to their normal anatom-
ical site – the abdomen.
Unlike a compressible swelling, a hernia which
has been reduced does not immediately reappear
when the pressure is removed, unless forced to do so
by gravity or muscle tone. When you reduce a hernia
you move all parts of it to another place. When you
compress a lump you just move its fluid contents to
another place.
Relations
The relations of the lump will have already
been defined when deciding the site and nature
of the hernia.
State of local tissues
As acquired inguinal herniae are
caused by weakness of the tissues of the inguinal
canal, bulging of both inguinal regions with cough-
ing is common. Minor bilateral bulging of the
inguinal canal in slim individuals is normal and
known as Malgaigne’s bulges.
Look carefully for any scars near the hernia. It
may have been repaired in the past.
There is an increased incidence of direct right
inguinal hernia in patients who have had an appen-
dicectomy through a right iliac fossa incision because
this incision weakens the adjacent muscles and
occasionally divides the iliohypogastric or ilioin-
guinal nerves.
General examination
Look for the common causes of
a raised intra-abdominal pressure, namely chronic
bronchitis and coughing, chronic retention of urine,
difficulty in micturition, ascites and intra-abdominal
masses. These factors may have exacerbated or even
caused the hernia.
Look for any signs of intestinal obstruction,
such as distension, increased bowel sounds and visible
peristalsis.
Special varieties of inguinal hernia
The differences between a direct and an indirect
inguinal hernia are listed in Revision panel 14.3.
Distinction between the two is not totally irrelevant.
When an inguinal hernia strangulates, the usual site
of constriction is the external ring. Hence a direct
hernia, which does not pass through this ring, is
much less likely to place the patient’s life at risk by
becoming strangulated. This may influence man-
agement in a poor-risk patient.
It is important to try to differentiate between the
two varieties because it makes you examine the her-
nia more carefully.
Bilateral herniae are more likely to be direct than
indirect.
It is not uncommon to find both a direct and an
indirect hernia in the same groin. When this does
occur, the two sacs are straddled by the inferior
epigastric artery and the hernia is sometimes called
a pantaloon hernia.
Chap-14.qxd 4/21/05 12:54AM Page 368
Inguinal hernia
A sliding hernia is a hernia of a piece of extraperi-
toneal bowel (the caecum or terminal ileum on the
right and the sigmoid colon on the left), which slides
down into the inguinal canal, pulling a sac of peri-
toneum on its surface. The viscus involved is part of
the wall of the sac. It is sometimes possible to guess
that a hernia is of the sliding variety by the slow way
in which it reappears after reduction and the manner
in which it slithers down into the scrotum. The clini-
cal differentiation of this variety is never certain, but
it is far more common on the left, and involvement
of the sigmoid colon may produce disproportionate
pain and even symptoms of bowel dysfunction.
Sliding herniae are occasionally diagnosed during
the investigation of bowel symptoms when contrast
X-rays demonstrate colon in a hernial sac.
Maydl’s hernia (hernia-en-W) is a rare condi-
tion in which there are two loops of bowel in the
sac, with strangulation of the loop of bowel in the
abdomen which connects them. Diagnosis is made
at operation.
Recurrent herniae
Inguinal hernia is a common condition and not all
of the many surgical repairs that are performed are
successful.
Recurrent herniae are more likely to present with
local pain than new herniae. They tend to be direct
and, because of the scarring from the previous sur-
gery, are unlikely to be large. They are very rarely
scrotal. The hernia may consist of extraperitoneal
fat without a peritoneal sac, infiltrating itself into
the defects that have arisen in the previous repair.
Recognition is important because strangulation is
more likely than with a new hernia.
Differential diagnosis
There are very few conditions which can be mis-
taken for an inguinal hernia provided you remember
to check the scrotum, feel for a cough impulse and
test reducibility.
Confusion may occasionally be caused by swellings
which occur in the line of the spermatic cord that
can pop in and out of the external ring, such as an
undescended testis and a hydrocele of the cord. In
the former event, routine examination of the scro-
tum should reveal an absent testis. Neither has an
expansile cough impulse.
Inguinal herniae in women
In females there is a rudimentary testicular analogue
which descends through the muscles of the groin
as in males. The equivalent of the spermatic cord
is the round ligament, which, inside the abdomen,
joins the uterus just as the vas deferens joins the
prostate. Herniae in women nearly always follow the
369
Revision panel 14.4
The differential diagnosis of inguinal hernia
Femoral hernia
Vaginal hydrocele
Hydrocele of the cord or the canal of Nuck
Undescended testis
Lipoma of the cord
Revision panel 14.3
The features of inguinal herniae
Features of an indirect inguinal hernia
Can (and often does) descend into the
scrotum
Reduces upwards, then laterally and
backwards
Controlled, after reduction, by pressure
over the internal inguinal ring
The defect is not palpable, as it is behind
the fibres of the external oblique muscle
After reduction, the bulge reappears in the
middle of the inguinal region and then flows
medially before turning down to the neck of
the scrotum
Features of a direct inguinal hernia
Does not (hardly ever) go down into the
scrotum
Reduces upwards and then straight
backwards
Not controlled, after reduction, by pressure
over the internal inguinal ring
The defect may be felt in the abdominal
wall above the pubic tubercle
After reduction, the bulge reappears
exactly where it was before
Uncommon in children and young adults
Chap-14.qxd 4/21/05 12:54AM Page 369
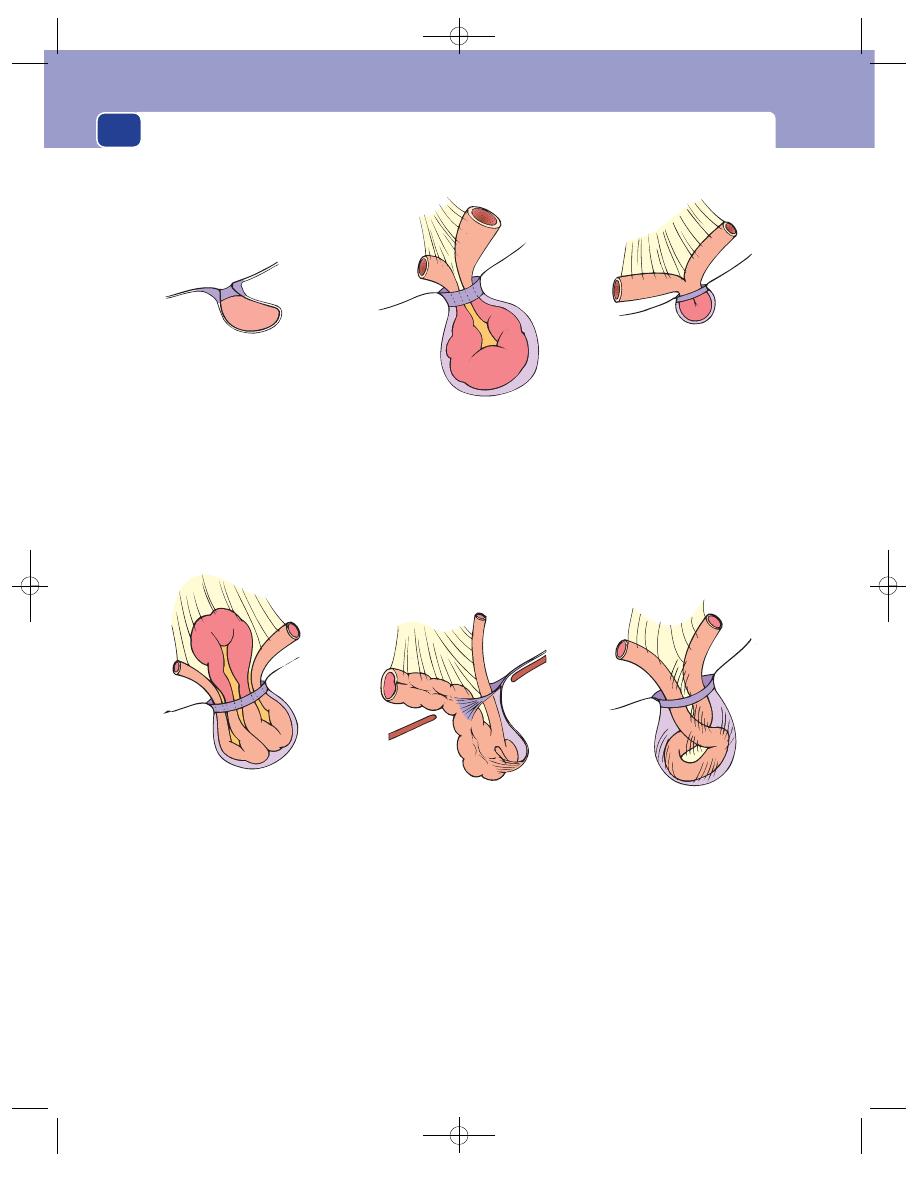
The abdominal wall, herniae and the umbilicus
370
Neck of sac
This tight ring of peritoneum
is usually the site of any
strangulation.
A strangulated hernia
The blood supply of the
contents of the hernia is cut
off. When a loop of gut is
strangulated there will also
be intestinal obstruction.
A strangulated hernia
If the sac is small, a knuckle
of bowel can be caught in
the sac and strangled
without causing intestinal
obstruction. This is called a
Richter's hernia.
Sliding hernia
If bowel which is normally
extraperitoneal forms one
side of the sac, it is thought
to have slid down the canal
pulling peritoneum with it,
hence the name hernia-
en-glissade. The sac can
contain other loops of
bowel, and the gut forming
the wall of the sac can be
strangled by the external ring.
Incarceration
The contents are fixed in the
sac because of their size
and adhesions. The hernia
is irreducible but the bowel
is not strangulated or
obstructed.
Maydl's hernia
When two adjacent
loops of bowel are in the
sac, the intervening portion
in the abdomen is the first
to suffer if the neck of the
sac is tight, because it is the
centre of the whole loop
involved. Thus the
strangulated piece is
intra-abdominal. This is a
rare variety of strangulation.
FIG 14.5
SOME DEFINITIONS
Chap-14.qxd 4/21/05 12:54AM Page 370
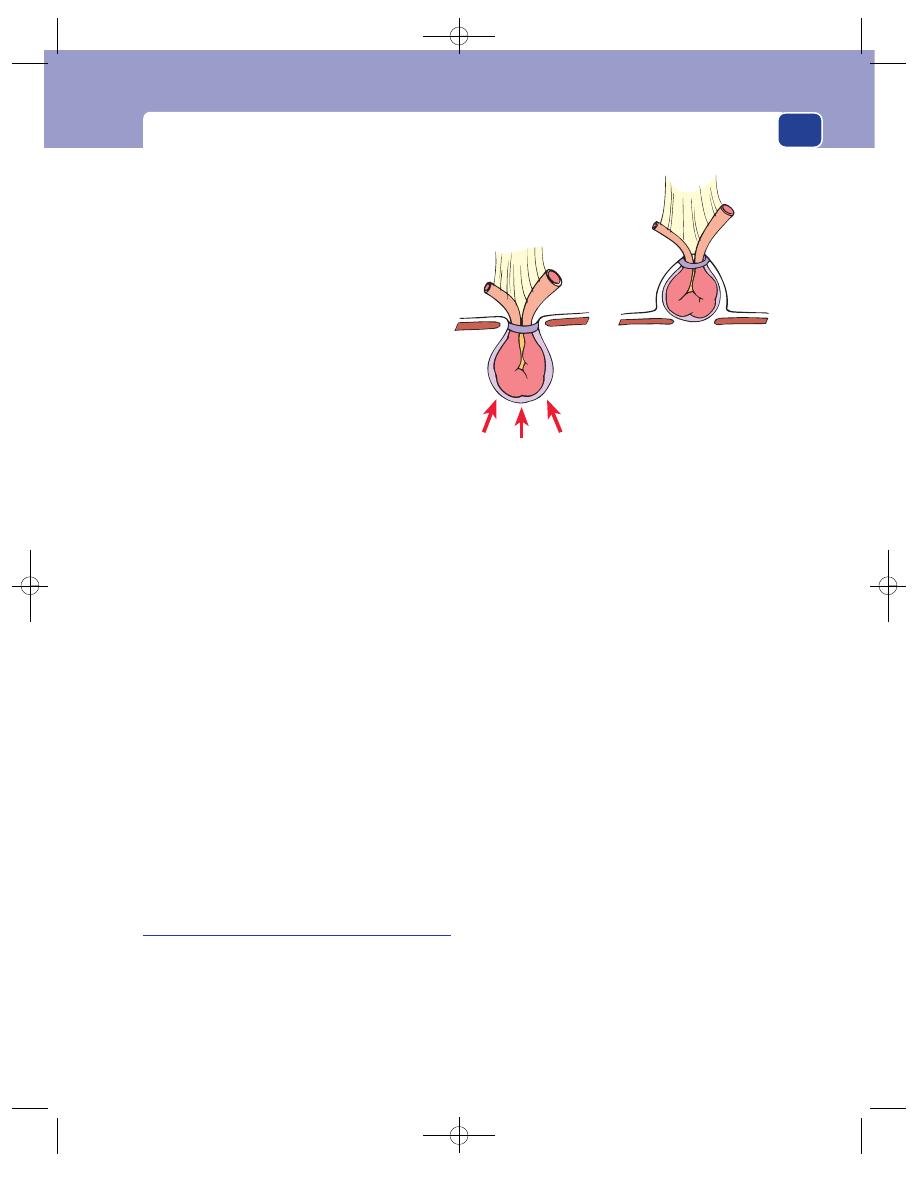
Inguinal hernia
371
round ligament and are therefore indirect. The sac
passes obliquely towards the labium in the same way
as it would pass towards the scrotum in the male.
There are two conditions of the groin peculiar to
women.
Hydrocele of the canal of Nuck is a fluid-filled
distal part of the sac of an indirect hernia. The prox-
imal part of the sac is too narrow to admit bowel or
other abdominal contents. It is analogous to the
encysted hydrocele of the cord seen in children. It
presents with a smooth, fluctuant swelling without
a cough impulse, which will transilluminate.
Haematocele of the round ligament is a curious
condition in which the round ligament becomes
distended with multiple small sacs containing blood-
stained fluid. It presents in pregnancy with a soft,
sausage-like swelling in the groin extending into the
labium. This may have a weak cough impulse and
when gently squeezed it feels spongy and reduces in
size. It is commonly confused with a hernia, but it
resolves when the pregnancy is over, which herniae
certainly do not.
Inguinal herniae in children
Groin herniae in male children are, for practical
purposes, always indirect and are caused by failure
of the processus vaginalis to obliterate after the tes-
ticle enters the scrotum. There are three clinical mani-
festations of this abnormality, but it is important to
appreciate that the pathological process in all three
is identical, namely a patent processus vaginalis. The
three clinical manifestations are:
■
an infantile hydrocele,
■
an obvious hernia,
■
an encysted hydrocele of the cord.
An infantile hydrocele is a fully patent processus
vaginalis (i.e. one extending right down to the scro-
tum) which is too narrow to admit bowel but which
allows fluid from the peritoneal cavity to accumu-
late within it. The condition may present at birth or
shortly afterwards as a scrotal swelling which is usu-
ally large, tense, brilliantly translucent and often
bilateral. It is should be possible to get above the
swelling, i.e. to feel or see that its upper limit is at or
below the external inguinal ring. It is rarely possible
to squeeze the fluid back into the abdomen, as the
narrow neck of the processus acts as a non-return
valve. It does not have an expansile cough impulse.
When the child cries, intra-abdominal pressure is
raised and the scrotal swelling may become harder.
It is important to reassure the parents that the
child is not crying because the hydrocele is tense,
but that the swelling is tense because the child is
crying.
The usual natural history is spontaneous reso-
lution during the first year of life as the processus
slowly obliterates, but once the child begins to walk
this is less likely. In ambulant children the swelling
often increases in size during the day, presumably
exacerbated by gravity.
Reduction-en-masse
It is possible to push a hernia back through the
abdominal wall, so apparently reducing it, without
actually pushing the contents out of the sac. If they
were strangulated in the first position they will still be
strangulated in the second. Never push hard when
trying to reduce a hernia.
FIG 14.5
continued
Chap-14.qxd 4/21/05 12:54AM Page 371
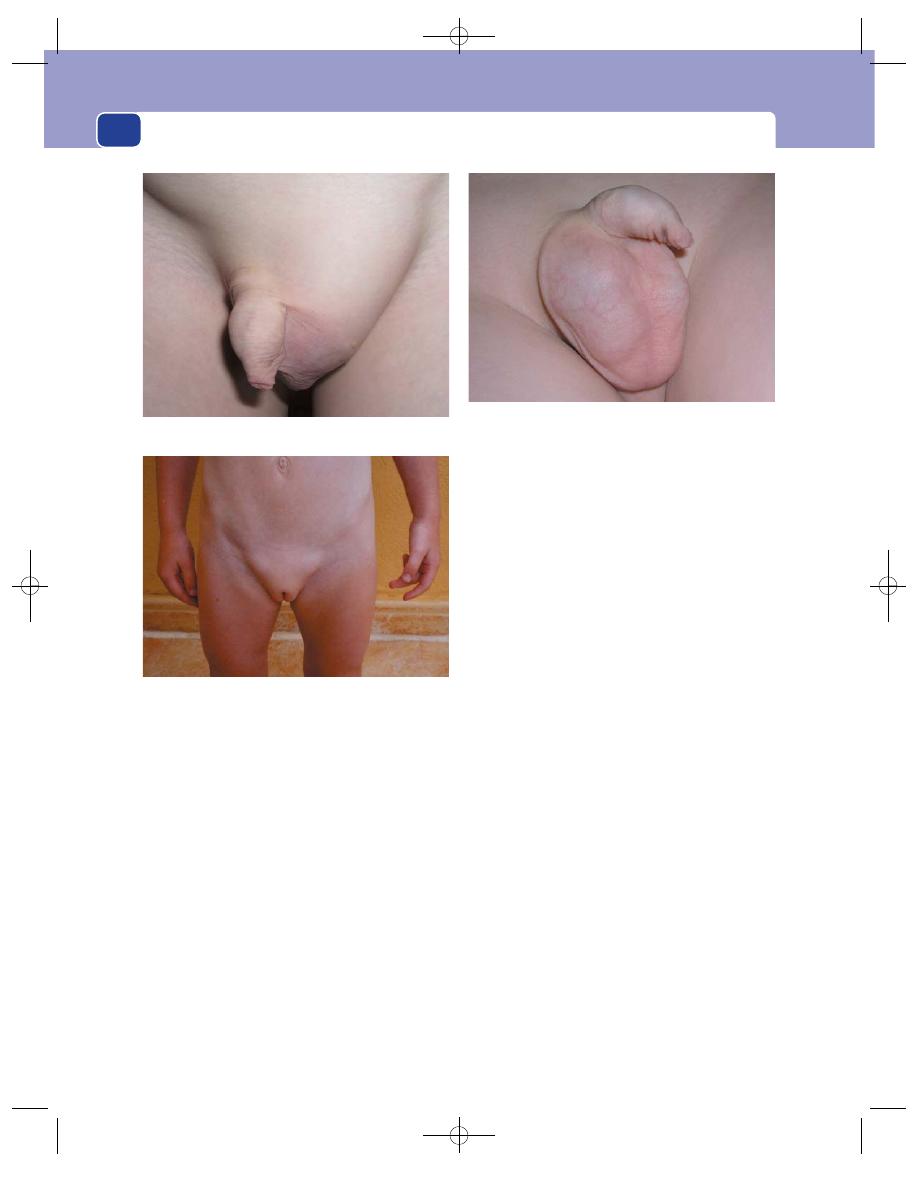
The abdominal wall, herniae and the umbilicus
372
An inguinal hernia in a child displays the phys-
ical signs listed above for an indirect inguinal hernia.
The contents reduce easily and the swelling does not
transilluminate.
Children’s groin herniae occasionally become
irreducible, but strangulation is rare. If strangulation
does occur, the gonadal vessels are more likely to be
damaged than the vessels of the bowel, so testicular
infarction is more common than bowel infarction.
Direct herniae do occur in children but are
very rare.
Children’s herniae may only appear intermittently.
The swelling that the parents have definitely seen
obstinately refuses to appear in the presence of the
examining physician. If the site of the swelling indi-
cated by the parents is the inguinal canal, exploration
is justified on the history alone and an indirect sac is
invariably found.
In girls, the wall of the sac may include the ovary
and Fallopian tube. When the contents are reduced,
there may remain a small mass, which is tender to
touch. The child may also complain of pain in the
area.
An encysted hydrocele of the cord is the least
common variety of patent processus vaginalis in
which a narrow patent processus, which extends
down to a level just above the testis and becomes
dilated and filled with fluid. It presents as a discrete
swelling in the spermatic cord below the external
inguinal ring, above or near the top of the scrotum,
separate from the testicle, which transilluminates
brilliantly and has no cough impulse.
Comment. Do not confuse the infantile with the
adult hydrocele.
In children the condition is really a fluid-filled
congenital inguinal hernia with a narrow sac which
communicates with the peritoneal cavity on every
occasion.
The adult hydrocele is an acquired condition in
which fluid accumulates around the testicle, within
the tunica vaginalis, in response to a local abnormal-
ity. It has no communication with the peritoneum.
FIG 14.6
A large left inguinal hernia in a child.
FIG 14.7
This young lady’s parents gave a history of an
intermittent left groin swelling and pointed to the inguinal
canal, but nothing was visible when she came to the clinic.
Nevertheless, the history was good enough for an operation
to be planned. But, when on holiday in Spain, a lump
appeared in the other groin and the parents took this
photograph confirming the presence of bilateral inguinal
herniae.
FIG 14.8
A right encysted hydrocele of the cord. It is clearly
separate from the testicle. You can get above it and there is
no cough impulse in the swelling or in the groin above it.
Chap-14.qxd 4/21/05 12:54AM Page 372
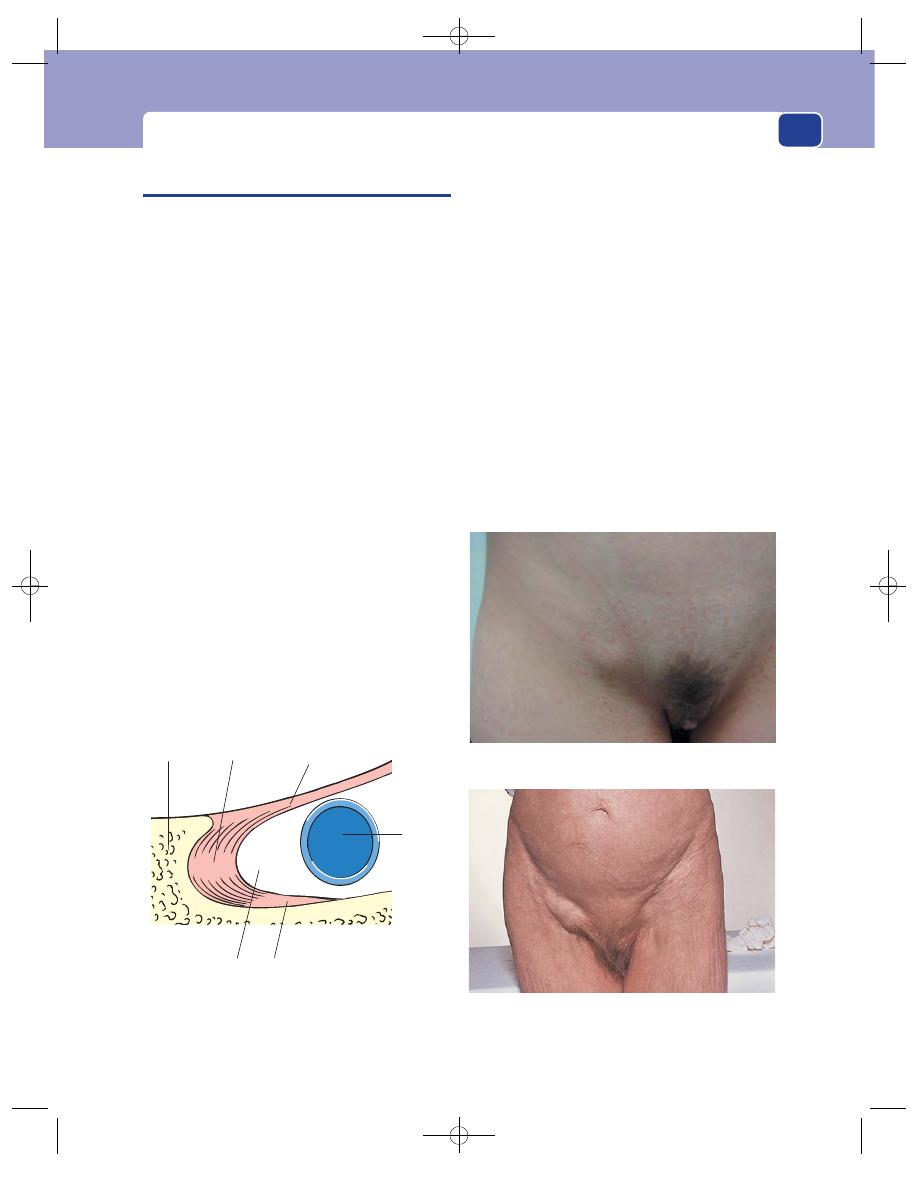
Femoral hernia
373
FEMORAL HERNIA
Anatomy
A femoral hernia is a protrusion of extraperitoneal
fat, a peritoneal sac and sometimes abdominal con-
tents through the femoral canal. The anatomical
margins of this canal are the inguinal ligament anter-
iorly, the pubic ramus and pectineus muscle poster-
iorly, the lacunar ligament and pubic bone medially,
and the femoral vein laterally.
The femoral canal provides a space into which
the femoral vein can expand. It normally contains
loose areolar tissue and a lymph gland known as the
gland of Cloquet. With bone or ligament on three
sides and a major vessel on the fourth, the femoral
canal cannot distend easily. A peritoneal sac coming
through it therefore has a stiff, narrow neck and any
contents are at risk of strangulation.
A characteristic but not invariable feature of the
sac of a femoral hernia is that it is thick walled with
layers of fat and connective tissue, which when cut
across looks like an onion. This means that the sac
remains palpable even when empty and so seems to
be irreducible.
History
Age
Femoral herniae are rare in children and do
not become common until over the age of 50, with
no upper age limit.
Sex
Femoral herniae are much more common in
women than in men. Nevertheless, do not forget
that even in women the commonest hernia in the
groin region is the inguinal hernia, and that a man
can have a femoral hernia.
Symptoms
The symptoms of this variety of hernia are
similar to those described above for inguinal hernia:
■
local – lump in the groin, pain and discomfort,
■
general – if causing obstruction: colic,
distension, vomiting and constipation.
The femoral hernia is able to strangle a part of the
wall of the bowel without occluding the lumen and
causing intestinal obstruction – Richter’s hernia.
Femoral herniae are occasionally bilateral.
Examination
All the comments made about the examination of
inguinal herniae apply to femoral herniae. Ask the
Inguinal ligament
(Poupart's ligament)
Gimbernat's
ligament
Body of
pubis
Cooper's ligament
Pectineus muscle
Superior ramus of
pubis
Femoral
canal
Femoral
vein
FIG 14.9
The boundaries of the left femoral canal.
A larger femoral hernia, in an elderly woman, with a wide
neck stretching laterally over the femoral vein.
FIG 14.10
FEMORAL HERNIA.
A right femoral hernia. Note that the femoral hernia bulges
into the crease of the groin.
Chap-14.qxd 4/21/05 12:54AM Page 373
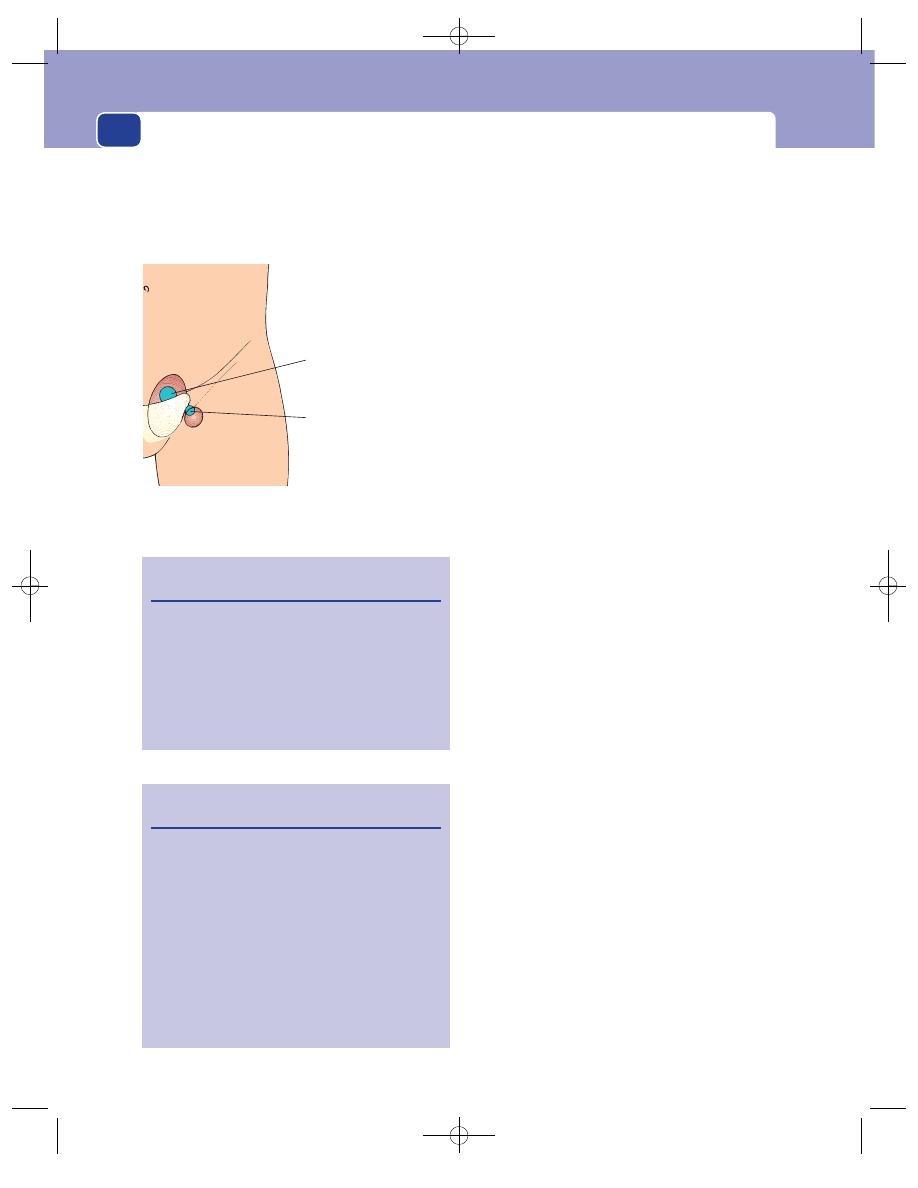
The abdominal wall, herniae and the umbilicus
374
patient to stand up, try to determine the exact ana-
tomical relations of the lump to the inguinal ligament
and pubic tubercle, and then decide if the lump has a
cough impulse and whether it is reducible.
The easiest way to confirm that a hernia is com-
ing through the femoral canal is to examine the
patient lying down, because it is easier in that posi-
tion to find the pubic tubercles and other related
anatomical landmarks.
Most femoral sacs are thick walled and remain
palpable, even when empty – a diagnostic clue in itself.
Position
The femoral canal is lateral to the body
of the pubis and inferior to the tip of the pubic
tubercle. Therefore, the neck of a femoral hernia, or
the point at which it disappears into the abdomen,
is below and lateral to the pubic tubercle. The main
sac of the hernia may expand in any direction. It
usually points downwards and laterally, but it can pass
medially and may bulge up and over the inguinal
ligament. Normally the bulge appears to be directly
behind the skin crease of the groin, whereas the
inguinal hernia bulges out above the groin crease.
With experience, this feature allows correct spot
diagnosis.
Feel the lump and, if it appears to have a neck
tethered deeply, palpate around this area very care-
fully to determine its exact position.
A small hernia in a fat person is very difficult to
feel, so take great care when examining this region
in a patient with intestinal obstruction.
Colour
The overlying skin should be of normal
colour. The skin may become red and oedematous if
the hernia is strangulated.
Temperature
The skin temperature is normal unless
there is hyperaemia caused by an underlying inflam-
matory response to strangulation.
Tenderness
Femoral herniae are not usually tender
unless strangulated, but you may cause pain if your
attempts at reduction are too vigorous.
Shape and size
The lump is almost spherical, with
an area above and deep to it which is difficult to
define, corresponding to the site of the neck in the
femoral canal.
Most femoral herniae are small. If they do enlarge,
they tend to flatten and spread upwards towards the
fold of the groin because downward extension is
limited by the attachment of the membranous layer
of the superficial fascia (Scarpa’s fascia) to the deep
fascia of the upper thigh.
Surface
The surface of the sac is usually smooth.
Revision panel 14.5
The differential diagnosis of femoral hernia
Inguinal hernia
Enlarged lymph gland
Sapheno-varix
Ectopic testis
Psoas abscess
Psoas bursa
Lipoma
Revision panel 14.6
The differential diagnosis of a lump in the groin
Inguinal hernia
Femoral hernia
Enlarged lymph glands
Sapheno-varix
Ectopic testis
Femoral aneurysm
Hydrocele of the cord or hydrocele of the canal
of Nuck
Lipoma of the cord
Psoas bursa
Psoas abscess
Inguinal herniae
Appear through the
external inguinal ring,
above and medial to the
pubic tubercle
Femoral herniae
Appear through the
femoral canal below
and lateral to the pubic
tubercle
FIG 14.11
The sites of appearance of inguinal and femoral
herniae.
Chap-14.qxd 4/21/05 12:54AM Page 374
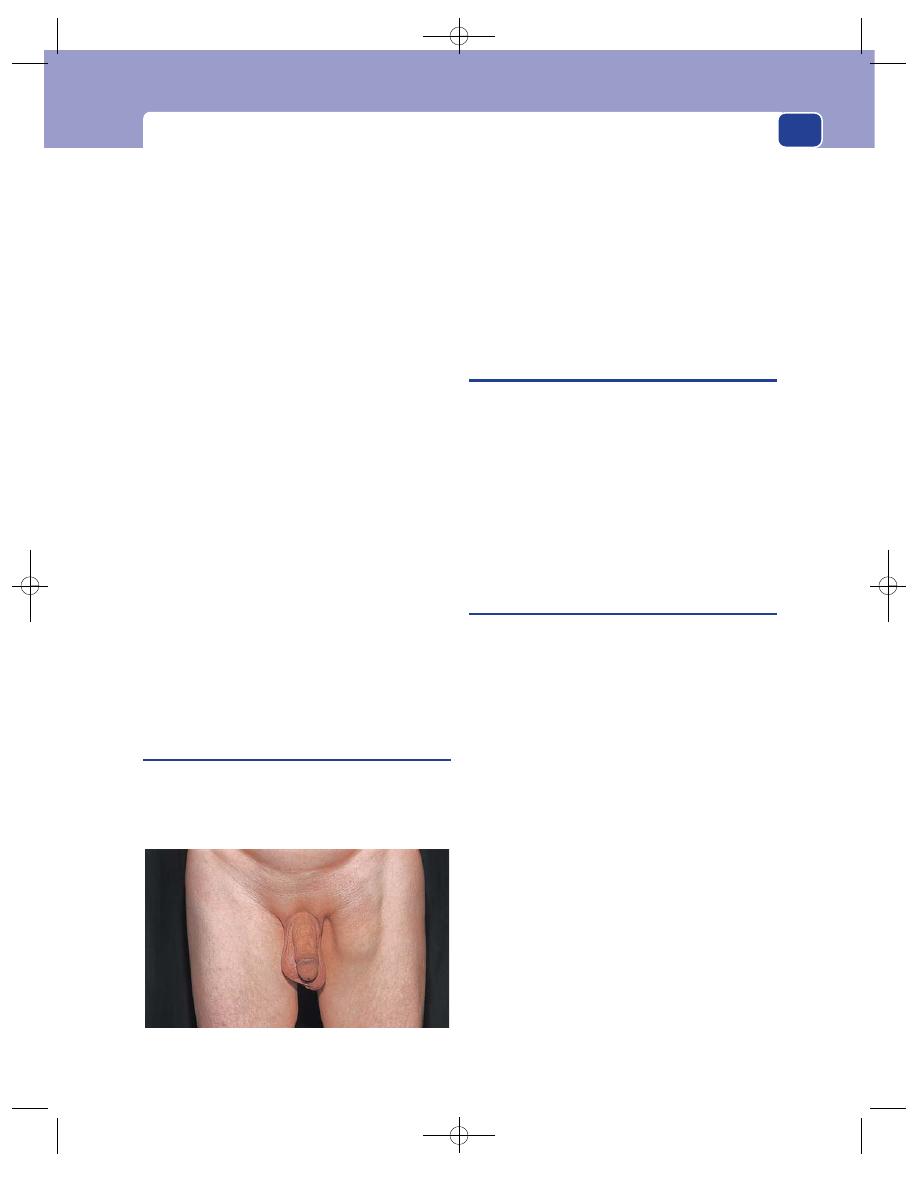
Umbilical hernia
375
Composition
The majority of femoral herniae feel
firm and are dull to percussion because they consist
of a small, empty sac surrounded by a lot of extraperi-
toneal fat and usually just contain omentum. They
occasionally contain bladder.
Reducibility
The size of most femoral herniae can
be reduced by firm pressure but can rarely be com-
pletely reduced, for the reasons given above.
Cough impulse
For the same reason that many femoral
herniae do not reduce easily – adherence of the con-
tents and a thick-walled sac – many do not have a
cough impulse. This may make the diagnosis difficult.
Relations
Because many femoral herniae do not have
the two signs diagnostic of herniae – reducibility and
a cough impulse – the diagnosis depends primarily
upon the site of the lump, hence the importance of
clearly defining its relations to surrounding structures.
State of local tissues
Femoral herniae develop because
the femoral canal is a naturally weak spot in the
abdominal wall, but the region may have been weak-
ened by injury, the commonest of which is the surgical
repair of an adjacent inguinal hernia. Look out for
other scars near the hernia and always examine the
other groin.
General examination
Look for causes of raised intra-
abdominal pressure, namely chronic bronchitis,
retention of urine and constipation, and for signs of
intestinal obstruction.
Prevascular femoral hernia
This is the only special variety of femoral hernia
that you need remember. It is rare, but usually easy
to diagnose. Instead of the sac coming through the
narrow femoral canal, it bulges down underneath
the whole inguinal ligament, in front of the femoral
artery and vein. This means that it has a wide neck
and a flattened wide sac, which bulges downwards
and laterally.
Prevascular herniae are usually easy to reduce, and
have a cough impulse. They rarely strangulate. They
are difficult to repair by open techniques because the
femoral vessels form the posterior wall of the defect.
UMBILICAL HERNIA
All herniae which appear to be closely related to the
umbilicus may be called umbilical herniae. They may
be congenital or acquired. All congenital umbilical
herniae come through the umbilical defect itself.
In adults, most umbilical herniae are acquired and
come through a defect adjacent to the umbilical cic-
atrix, and not through the umbilical scar itself, and
should be termed para-umbilical. In practice, the
distinction is academic and the simple expression
‘umbilical hernia’ is commonly used for both varieties.
Congenital umbilical hernia
In early fetal life the whole of the mid-gut protrudes
through the umbilicus. As it returns into the abdomen,
the gap in the abdominal wall gradually closes, leav-
ing a small central defect through which the umbil-
ical vessels connect the fetus with the placenta.
Congenital umbilical herniae appear at this site if
the process by which scar tissue closes the gap, once
the umbilical vessels have atrophied after birth, fails.
A congenital persisting protrusion of bowel
through the umbilical defect without a covering of
skin is called an exomphalos. This is not a true her-
nia and is discussed below.
History
Age
Although the weakness is present at birth, the
hernia may not be noticed until the umbilical cord
has separated and healed. Even then, it may be very
small and not noticed until it enlarges months later.
Ethnicity
Congenital umbilical herniae are more com-
mon in the Afro-Caribbean races.
Symptoms
The swelling rarely causes any symptoms
for the patient, but parental anxiety is common.
Intestinal obstruction is extremely rare.
FIG 14.12
A prevascular femoral hernia.
Chap-14.qxd 4/21/05 12:54AM Page 375
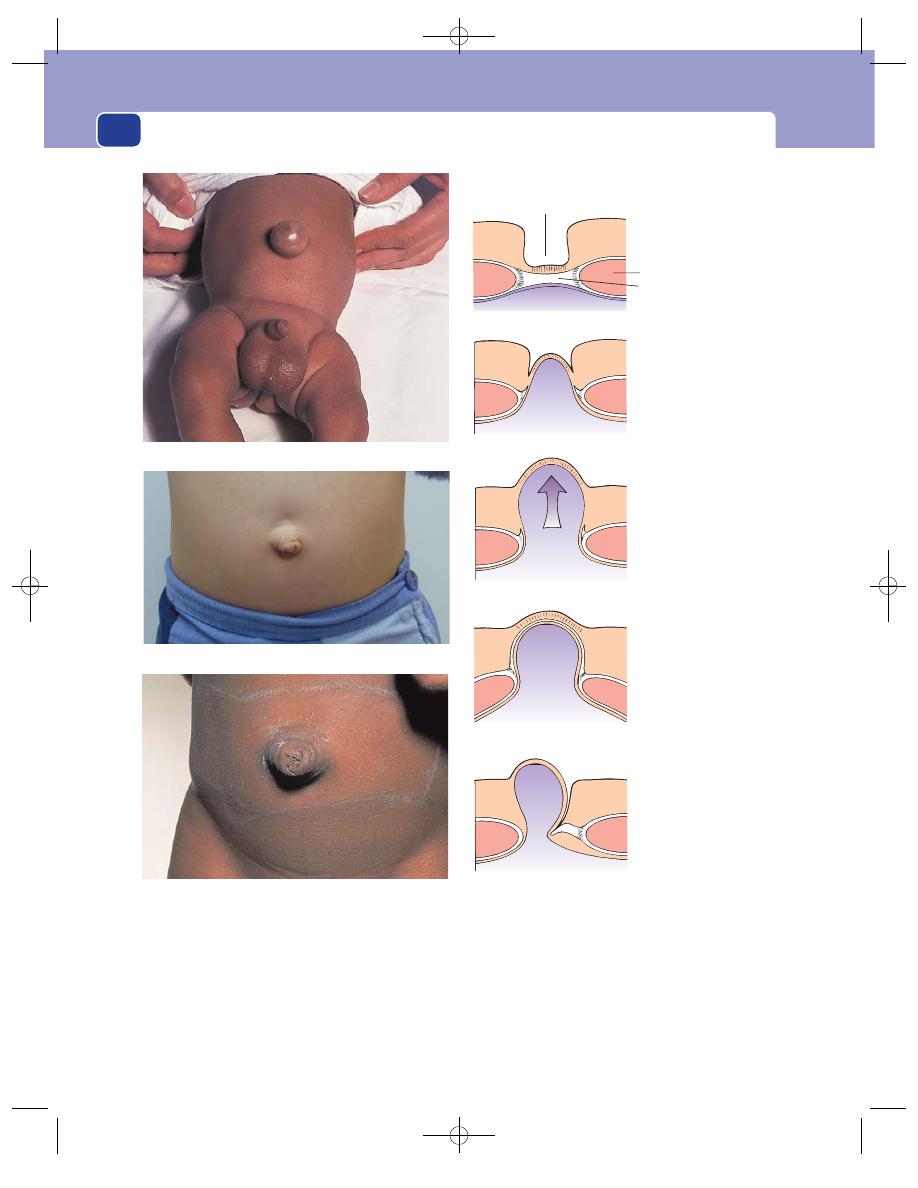
The abdominal wall, herniae and the umbilicus
376
A visible hernia may be embarrassing to a child,
when noticed by others.
‘Tummy ache’ in children may be attributed to
the hernia, but it is unlikely that there is ever a genu-
ine association.
Natural history
The vast majority of congenital umbil-
ical herniae disappear spontaneously during the
first few years of life. It is difficult to believe that a
large defect will close over in an active child, but this
is the usual course of events. The hernia becomes
The normal
umbilicus
Skin dimple
Rectus abdominis
muscle
Scar in linea alba
tethered to the skin
The umbilical scar fails
to form or is weak.
The abdominal
contents bulge through
the weak spot and
evert the umbilicus.
The umbilical scar is
stretched by a raised
intra-abdominal
pressure and the
umbilicus everts.
The hernial orifice is
at the side of the
umbilical scar so the
sac bulges out
beside the umbilicus,
turning it into a
crescent-shaped slit.
A paraumbilical
hernia
A congenital
umbilical hernia
An acquired true
umbilical hernia
FIG 14.14
ANATOMY OF UMBILICAL HERNIA
FIG 14.13
CONGENITAL UMBILICAL HERNIAE.
This baby also has a left inguinal hernia and a right hydrocele.
An umbilical hernia in a 3-year-old girl.
A regressing congenital umbilical hernia. The defect has
almost closed and the overlying skin is collapsing inwards to
become a normal umbilicus.
Chap-14.qxd 4/21/05 12:55AM Page 376
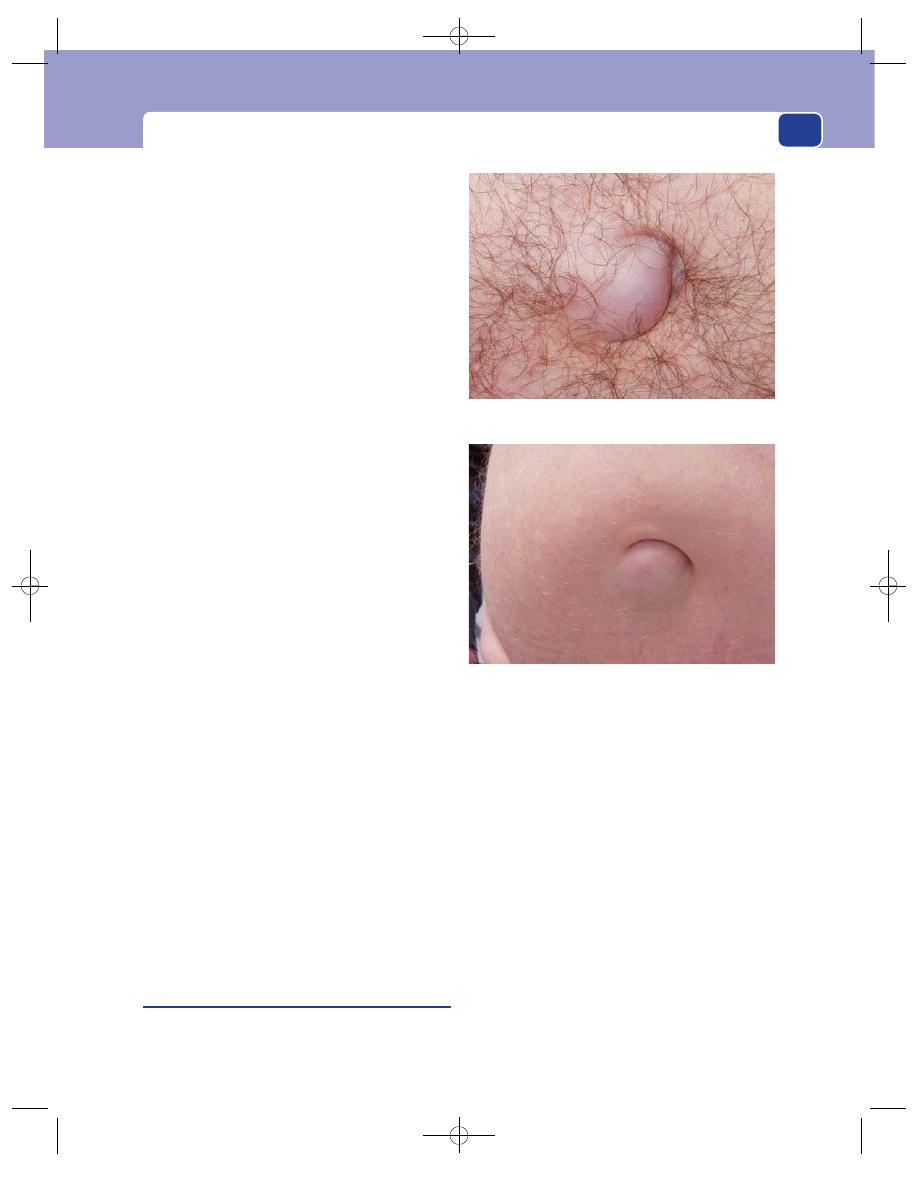
Umbilical hernia
377
gradually smaller, and then disappears. If there is
still a defect at the age of 4, it is unlikely to seal itself
and operation is required.
Examination
Shape and size
Congenital umbilical herniae are
usually hemispherical and overlie an easily palpable
defect in the abdominal wall. The size of the lump
can vary from very small (0.5 cm diameter) to very
large (10 cm diameter). Very small herniae can only
be diagnosed by carefully exploring the depth of the
umbilicus with the tip of a finger to find the defect
in the abdominal wall.
Although there may be quite a large visible
hernia, the palpable defect is often very small.
Sometimes, however, it is easy to insert a finger into
the hole.
In neonates, the remnants of the umbilical cord,
and sometimes a chronic granuloma, may be visible.
Composition
Congenital umbilical herniae are soft,
compressible and easy to reduce. They usually con-
tain bowel and so may be resonant to percussion, if
you can elicit this sign in a small child. They reduce
spontaneously when the child lies down and become
tense when the child cries.
Cough impulse
An expansile cough impulse is invari-
ably present.
UMBILICAL HERNIA IN ADULTS
A true umbilical hernia comes through the umbil-
ical scar and has the umbilical skin tethered to it. It is
not common in adults and usually secondary to
raised intra-abdominal pressure, so clinical examin-
ation should concentrate on finding the cause of the
raised intra-abdominal pressure.
The causes of abdominal distension are discussed
in detail in Chapter 15, but the common causes of
an acquired umbilical hernia are pregnancy and
ascites. The local physical signs of the hernia are
identical to those described for the congenital
variety.
Para-umbilical hernia
This is the common acquired umbilical hernia. It
appears through a defect that is adjacent to the
umbilical scar. That it is beside the umbilicus (para-
umbilical) rather than coming through the umbili-
cus is clinically apparent because it does not bulge
into the centre of the umbilicus, and the umbilical
skin is not attached to the centre of the sac. Why the
linea alba should give way so often just adjacent to
the umbilical scar is not known.
History
Age
Para-umbilical herniae usually develop in middle
and old age. They are more common in women than
in men, especially parous and obese women.
Symptoms
The commonest symptoms are discom-
fort and a swelling. Sometimes the swelling is so
small that it is not noticed by the patient, even when
Note that the hernia is clearly coming out alongside the true
umbilical scar.
A large para-umbilical hernia, partially obscured by a very fat
abdominal wall. Note the classical crescentic shape of the
umbilicus.
FIG 14.15
PARA-UMBILICAL HERNIAE.
Chap-14.qxd 4/21/05 12:55AM Page 377
The abdominal wall, herniae and the umbilicus
378
they present complaining of pain or discomfort and
tenderness around the umbilicus, made worse by
prolonged standing or strenuous exercise.
Strangulation of an umbilical hernia, whether or
not it has been previously noticed by the patient, is
common. The usual contents in this case are
extraperitoneal fat or omentum, so even though the
hernial contents may be strangulated, the bowel is
not obstructed.
Examination
Position
The main bulge of the hernia is beside
the umbilicus, which is pushed to one side and
stretched into a crescent shape. With a large hernia
in a fat patient there may be a crescent-shaped
pit, with the attachment of the skin to the umbilicus
at the bottom. This pit may be so deep that it can-
not be cleansed, and in consequence there may be
a foul-smelling discharge and even a collection of
dried-up sebaceous secretions, an ompholith (see
below).
Surface and edge
The surface is smooth and the edge
easy to define, except when the patient’s abdominal
wall is very fat.
Composition
The lump is firm as it usually contains
omentum. If it contains bowel, it is soft and reso-
nant to percussion. It will be reducible unless the
contents are adherent to the sac or the defect is very
narrow.
Cough impulse
Most of these herniae have an expan-
sile cough impulse.
Relations
The skin at the centre of the umbilicus is
not attached to the centre of the sac as in the true
umbilical hernia, but the umbilical skin is usually
firmly applied to the side of the sac and may be fixed
to it.
If the hernia can be reduced, the firm fibrous
edge of the defect in the linea alba is easy to feel. It
may vary in size from a few millimetres in diameter
to a defect big enough to admit your hand.
General examination
The patient is quite likely to be
obese and may have other herniae and generalized
abdominal wall laxity. There may be an apron of
pendulous fat across the lower abdomen.
Although abdominal distension usually causes a
true umbilical hernia, it can cause a para-umbilical
hernia, so examine the contents of the abdomen
with care.
EPIGASTRIC HERNIA
An epigastric hernia is a protrusion of extraperi-
toneal fat, and sometimes a small peritoneal sac,
through a defect in the linea alba somewhere between
the xiphisternum and umbilicus.
The patient complains of epigastric pain which is
localized exactly to the site of the hernia, but often
does not notice the underlying lump.
The pain is often associated with eating, so the
patient calls it ‘indigestion’ and makes a self-diagnosis
of peptic ulceration. A likely explanation for this is
that the fatty hernia is ‘nipped’ by the linea alba on
leaning forward in the sitting position adopted at
the dining table. Thus when a patient complains of
epigastric discomfort, palpate the abdominal wall
very carefully before concentrating on deep palpation,
because all the symptoms may be caused by a small,
fatty, epigastric hernia.
On examination, these herniae feel firm, do
not usually have a cough impulse and cannot be
reduced. It is sometimes impossible to distinguish
them from lipomata, only the typical position sug-
gesting the correct diagnosis. However, although the
defect is always exactly in the mid-line, the sac and
hence the palpable swelling may lie to the side of the
mid-line.
Epigastric hernia in children
This condition is reasonably common in childhood,
sometimes associated with divarication of the rec-
tus abdominis muscles. A small hernia may only be
visible intermittently, leading to diagnostic uncer-
tainty. As strangulation of such a sac in a child
rarely, if ever, occurs, it is safe to wait until the her-
nia is seen before recommending surgery, unlike
inguinal herniae in children, for which an operation
may be indicated on the history alone.
INCISIONAL HERNIA
An abdominal incisional hernia is a hernia through
an acquired scar in the abdominal wall, caused by a
Chap-14.qxd 4/21/05 12:55AM Page 378
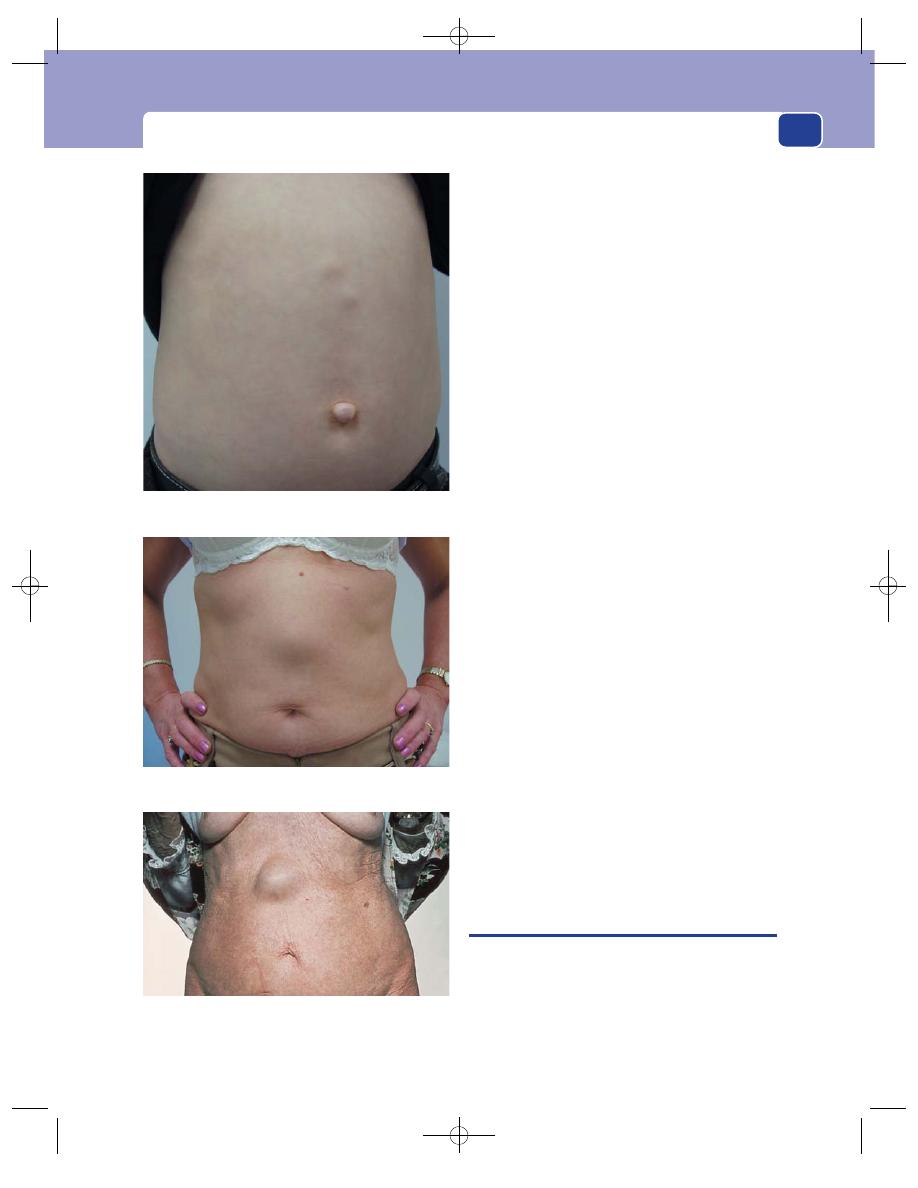
Divarication of the recti
379
previous surgical operation or injury. Scar tissue is
inelastic and stretches progressively if subjected to
constant stress.
History
Patients usually remember the operation or
wound that caused the scar, but may not recall any
complications in the original wound such as a
haematoma or infection, which weakened it and
made it more susceptible to the development of a
hernia.
There may be a history of factors likely to weaken
the abdominal musculature, such as chronic cough,
obesity or steroid therapy.
Age
Incisional herniae occur at all ages but are more
common in the elderly.
Symptoms
The commonest symptoms are a lump
and pain. Intestinal obstruction can occur, causing
distension, colic, vomiting, constipation and severe
pain in the lump.
Examination
The common findings are a lump with an expansile
cough impulse, beneath an old scar. The defect in
the abdominal wall may be palpable. Incisional her-
niae are not infrequently irreducible, the defect being
plugged with adherent omentum.
If the lump does not reduce and does not have a
cough impulse, it may not be a hernia, but rather a
deposit of tumour, a chronic abscess or haematoma,
or a foreign-body granuloma. All these lesions, except
recurrent tumour, appear shortly after the initial
surgery.
Incisional herniae usually appear in the first year
after surgery but may develop many years later.
The local tissues may be thin and weak because
of local damage or general cachexia.
DIVARICATION OF THE RECTI
This is separation of the rectus abdominis muscles
with extenuation of the linea alba, from xiphister-
num to umbilicus and occasionally below.
It may be seen in children in the first few years of
life. It is only noticeable when the abdominal wall is
tensed. Children have a relatively larger abdominal
FIG 14.16
THREE PATIENTS WITH EPIGASTRIC HERNIAE.
An elderly lady with an epigastric hernia. This reduced easily
and caused no symptoms.
A 3-year-old boy with two epigastric herniae and an umbilical
hernia. These small herniae can be the source of epigastric pain.
A lady with a large epigastric hernia, which was
misdiagnosed as a lipoma and ignored for 5 years.
Chap-14.qxd 4/21/05 12:55AM Page 379
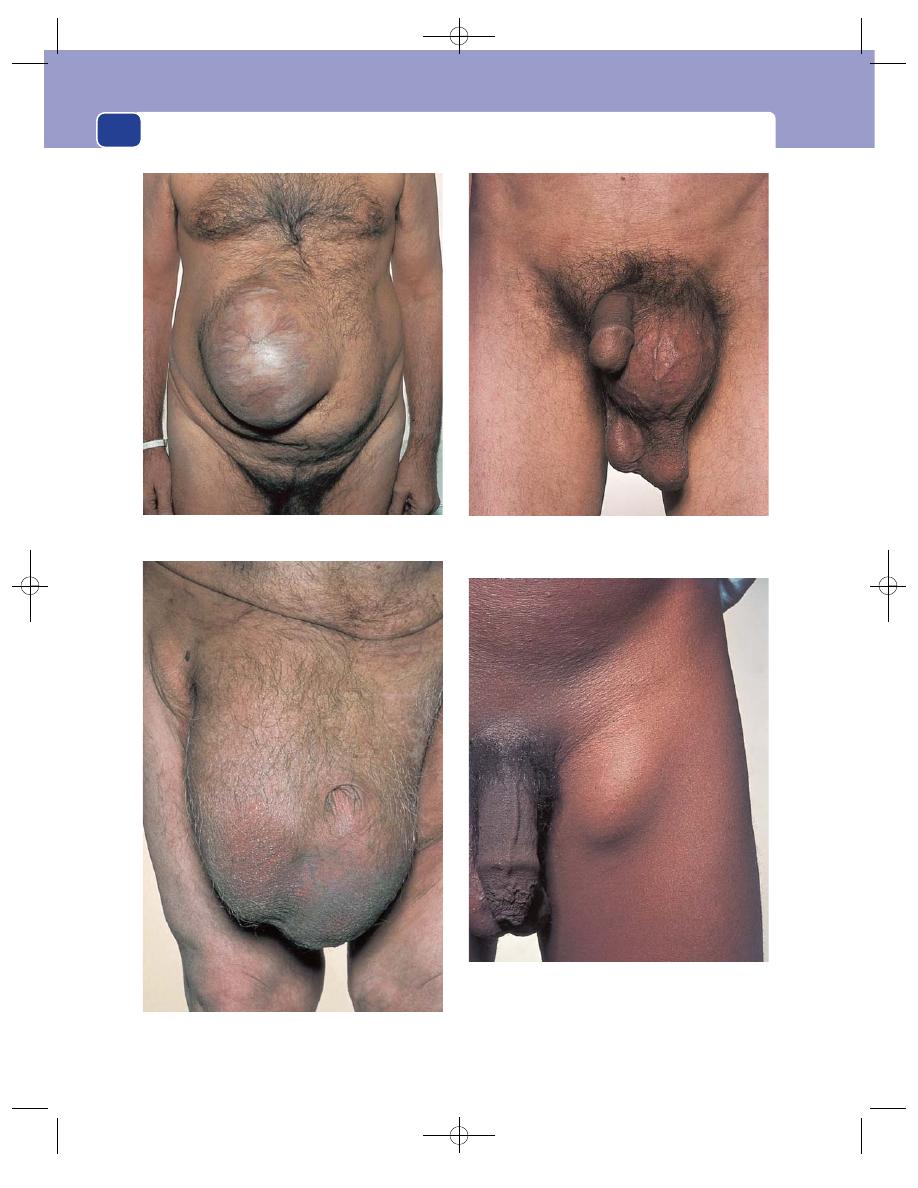
The abdominal wall, herniae and the umbilicus
380
FIG 14.17
HERNIAE: THE OBVIOUS AND THE DECEPTIVE.
A large incisional hernia.
Is this a hernia? No, because it was possible to feel the
spermatic cord above the lump and it had no cough impulse.
It was a hydrocele of the cord.
Very large, bilateral, irreducible herniae.
Is this a hernia? No, because it was firm, tender, not reducible
and distant from both the inguinal and femoral canals. It was
a mass of enlarged inguinal lymph glands caused by
lymphogranuloma.
Chap-14.qxd 4/21/05 12:55AM Page 380
The umbilicus
381
cavity than adults; even the slimmest appear some-
what ‘pot bellied’.
The condition usually improves and eventually
disappears as the child grows, but occasionally per-
sists into adult life. There may be a coincidental
umbilical hernia or an epigastric hernia.
The only clinical concern is the cosmetic disfig-
urement, as strangulation is impossible with such a
wide-necked bulge.
Divarication of the recti is also seen in adults, in
women during and immediately after childbirth.
There may be a wide separation of the muscles, with
stretched overlying abdominal skin. The examiner
may be able to push a hand into the abdominal cavity.
(Ask permission to do this!)
As abdominal tone recovers, the defect closes,
although it may become permanent after multiple
pregnancies.
Although strictly speaking an incisional hernia,
iatrogenic divarication may follow repeated surgery
through a long mid-line incision.
Divarication is best observed with the patient
lying supine. If asked to raise the head and legs
together, the recti are fully tensed and the abdom-
inal pressure rises. The thinned-out linea alba then
bulges, producing a visible swelling. Patients of all
ages learn the best way to produce the swelling.
RARE ABDOMINAL HERNIAE
Spigelian herniae occur at the edge of the rectus
sheath, below the umbilicus and above the inguinal
area. They are seen in obese patients and may be dif-
ficult to diagnose.
Obturator herniae come through the obturator
foramen, and the small sac is concealed among the
adductor muscles of the thigh. Only on very rare
occasions will there be a palpable mass. The usual
presentation is small bowel obstruction of unknown
cause. The sac may compress the obturator nerve
and cause pain in the medial side of the thigh.
Lumbar and gluteal herniae are extremely rare.
They are commonly associated with previous sur-
gery near to the defect, such as a loin incision or an
excision of the rectum. Diagnosis is difficult and often
requires imaging by magnetic resonance imaging
(MRI) scanning.
An interstitial hernia is a variety of inguinal
hernia in which the sac of the hernia spreads between
the muscles that form the inguinal canal, above the
groin, and emerges through a defect in the internal
oblique and transverse muscles rather than the exter-
nal inguinal ring. It may be suspected when the sac,
though clearly in the groin, appears more laterally
and looks flatter than usual.
THE UMBILICUS
The commonest abnormality of the umbilicus is an
umbilical hernia, described above.
The important congenital abnormalities of the
umbilicus are exomphalos and fistula, and the com-
mon acquired conditions (apart from herniae) are
inflammation and invasion by tumour.
Exomphalos
This condition, which is present at birth, represents
an intrauterine failure of the intestines to return to
the abdomen combined with a failure of the two
sides of the laterally developing abdominal wall to
unite to cover the embryonic defect.
The intestines protrude through a central defect
of all layers of the abdominal wall. Their only cover-
ing is a thin, transparent membrane formed from
the remnant of the coverings of the yolk sac. Once
this membrane is exposed to the air, it rapidly loses
its thin, transparent appearance, becoming thicker
and covered with an opaque, fibrinous exudate.
If this membrane ruptures, death from peritonitis
may follow.
Umbilical fistulae
Four structures pass through the umbilicus during
fetal development: the umbilical vein, the umbilical
arteries, the vitello-intestinal duct and the urachus.
If either of the last two tubes fails to close properly,
there will be an intestinal or a urinary fistula.
A patent vitello-intestinal duct produces an
intermittent discharge of mucus and sometimes
faeces from the umbilicus in the neonate. It is a rare
abnormality. Sometimes there is visible small intes-
tinal mucosa lining an obvious fistula, but on other
occasions there may only be a small fluid leak and
the condition mimics an umbilical granuloma. The
duct connects to the ileum at the site of a Meckel’s
diverticulum.
Chap-14.qxd 4/21/05 12:55AM Page 381
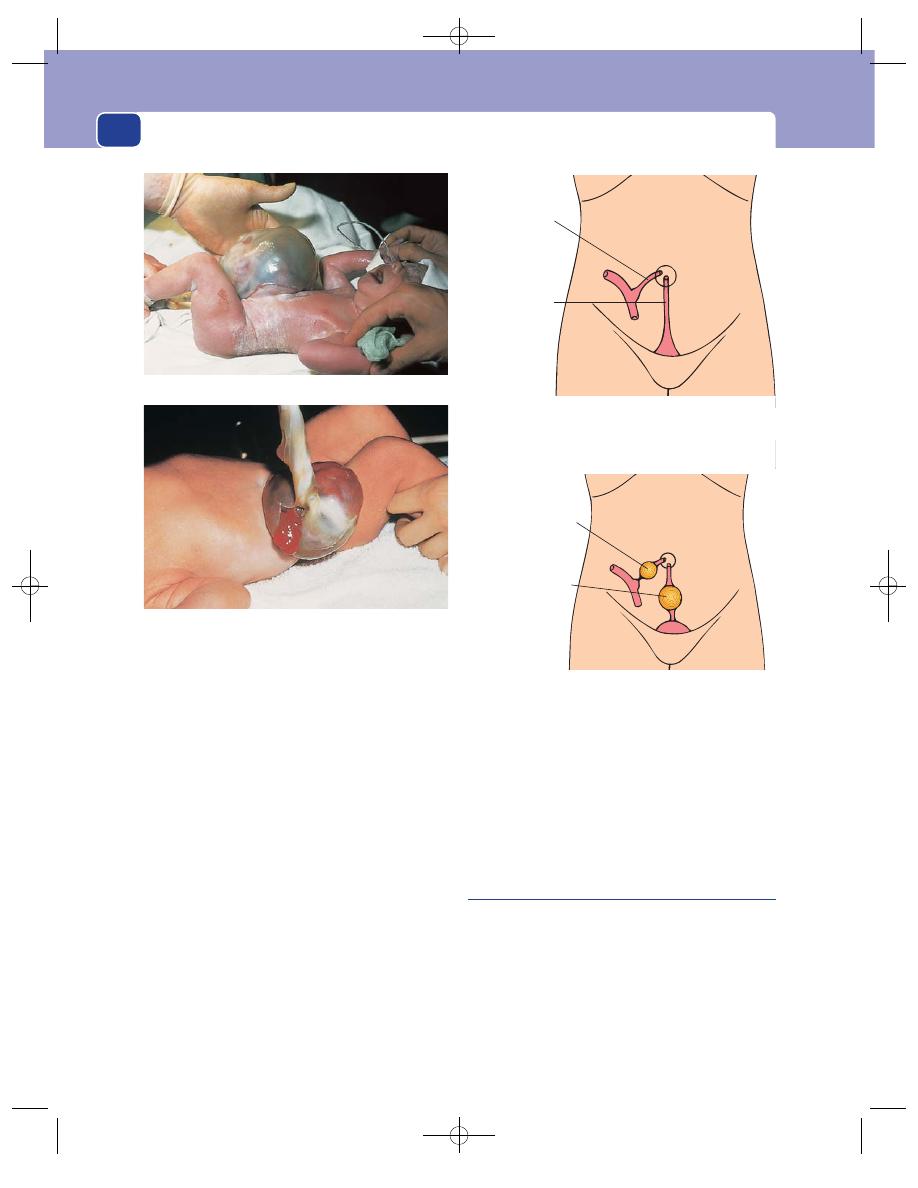
The abdominal wall, herniae and the umbilicus
382
A patent urachus can become a track through
which urine can leak onto the external surface of
the abdomen through the umbilicus. This rare
condition occasionally presents in childhood, but
more commonly in adult life in association with
chronic retention of urine caused by disease of the
prostate.
The patient complains of a watery discharge from
the umbilicus.
A watery umbilical discharge is nearly always
caused by infection in the umbilicus; nevertheless,
remember the possibility of a urachal fistula, particu-
larly if there are symptoms of urinary obstruction or
a palpable bladder.
Both these embryonic tracts may partially close,
leaving a patent segment that becomes a cyst.
A vitello-intestinal duct cyst is a small, spher-
ical, mobile swelling deep to the umbilicus that is
tethered to the umbilicus and to the small bowel by
a fibrous cord. It is usually impalpable.
A urachal cyst is an immobile swelling below the
umbilicus deep to the abdominal muscles. It may
become large enough to fluctuate and have a fluid
thrill. If it is still connected to the bladder, it may
vary in size and be difficult to distinguish from a
chronically distended bladder.
Umbilical granuloma
After the umbilical cord has been severed and tied,
the proximal remnant shrivels and separates spon-
taneously. This leaves an area of chronic inflamma-
tion at the line of demarcation, which is quickly
covered by epithelium. If the inflammatory process
becomes florid, with associated infection, excess
granulation tissue is formed which prevents the raw
area becoming epithelialized.
A patent
vitello-intestinal
duct
A patent
urachus
FIG 14.19
A persistent vitello-intestinal duct or patent urachus
can become an intestinal or urinary fistula, respectively.
A vitello-intestinal
duct cyst
A urachal cyst
FIG 14.20
If the vitello-intestinal duct or urachus are not
completely obliterated, they may turn into cysts.
FIG 14.18
TWO EXAMPLES OF EXOMPHALOS.
The bowel can be seen through the thin membrane.
The thin membrane is covered with fibrin but has,
nevertheless, ruptured. The umbilical cord is still present.
Chap-14.qxd 4/21/05 12:55AM Page 382
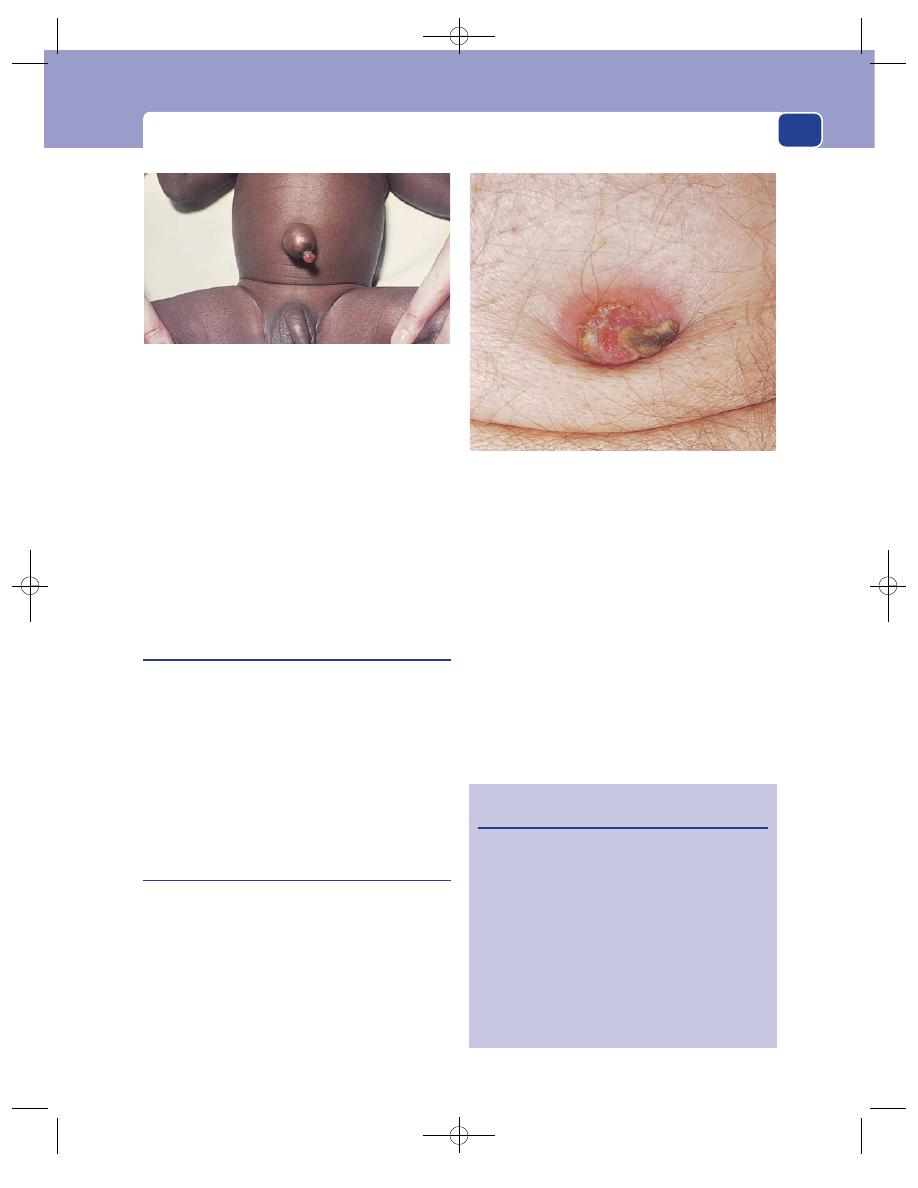
The umbilicus
The baby presents with a pouting umbilicus sur-
mounted by a bright-red, moist, friable, sometimes
hemispherical mass of bleeding granulation tissue.
This condition is similar to the pyogenic granuloma
seen in other parts of the skin. It usually regresses
spontaneously in the first month or so of life. If the
condition persists longer than this, the possibility of
a patent vitello-intestinal duct or an umbilical aden-
oma should be considered.
Umbilical adenoma
An umbilical adenoma is a patch of intestinal epithe-
lium left behind when the vitello-intestinal duct
closes. It may produce a discharge from the depths
of the umbilicus, but more often protrudes from the
umbilicus and looks like a raspberry. Although it
resembles an umbilical granuloma, the cause is
quite different. It will not resolve spontaneously.
The mother complains that the baby has a lump
at the umbilicus and a mucous discharge.
Omphalitis
Infection within the umbilicus is not uncommon in
adults. It is usually associated with inadequate hygiene
and a sunken umbilicus caused by obesity. The con-
dition is similar to the intertrigo that occurs between
the folds of skin associated with obesity and sweating,
which frequently becomes secondarily infected with
skin organisms that produce an unpleasant smell.
The patient complains of umbilical discharge,
pain and soreness.
On examination, the skin within and around the
umbilicus is red and tender, and exuding a seropu-
rulent discharge with a characteristic foul smell.
The whole umbilicus may feel indurated, espe-
cially if there is an ompholith or a tumour deposit.
Although simple dermatitis or skin infection is
by far the commonest cause of a discharge from the
umbilicus, it is essential to exclude the other causes
of an umbilical discharge, which are listed in
Revision panel 14.7.
True omphalitis is infection of the stump of the
umbilical cord following inadequate post-natal care
and cleanliness.
383
FIG 14.21
An umbilical granuloma. This is an excessive
amount of granulation tissue at the point where the umbilical
cord separated. These granulomata are often associated with
an umbilical hernia.
FIG 14.22
Omphalitis. A protruding mass of infected
granulation tissue caused by a large ompholith, the brown
tip of which is just visible.
Revision panel 14.7
The causes of a discharge from the umbilicus
Congenital
Intestinal fistula
Patent urachus
Umbilical adenoma
Acquired
Umbilical granuloma
Dermatitis (intertrigo)
Ompholith (umbilical concretion)
Fistula (intestinal)
Secondary carcinoma
Endometriosis
Chap-14.qxd 4/21/05 12:55AM Page 383
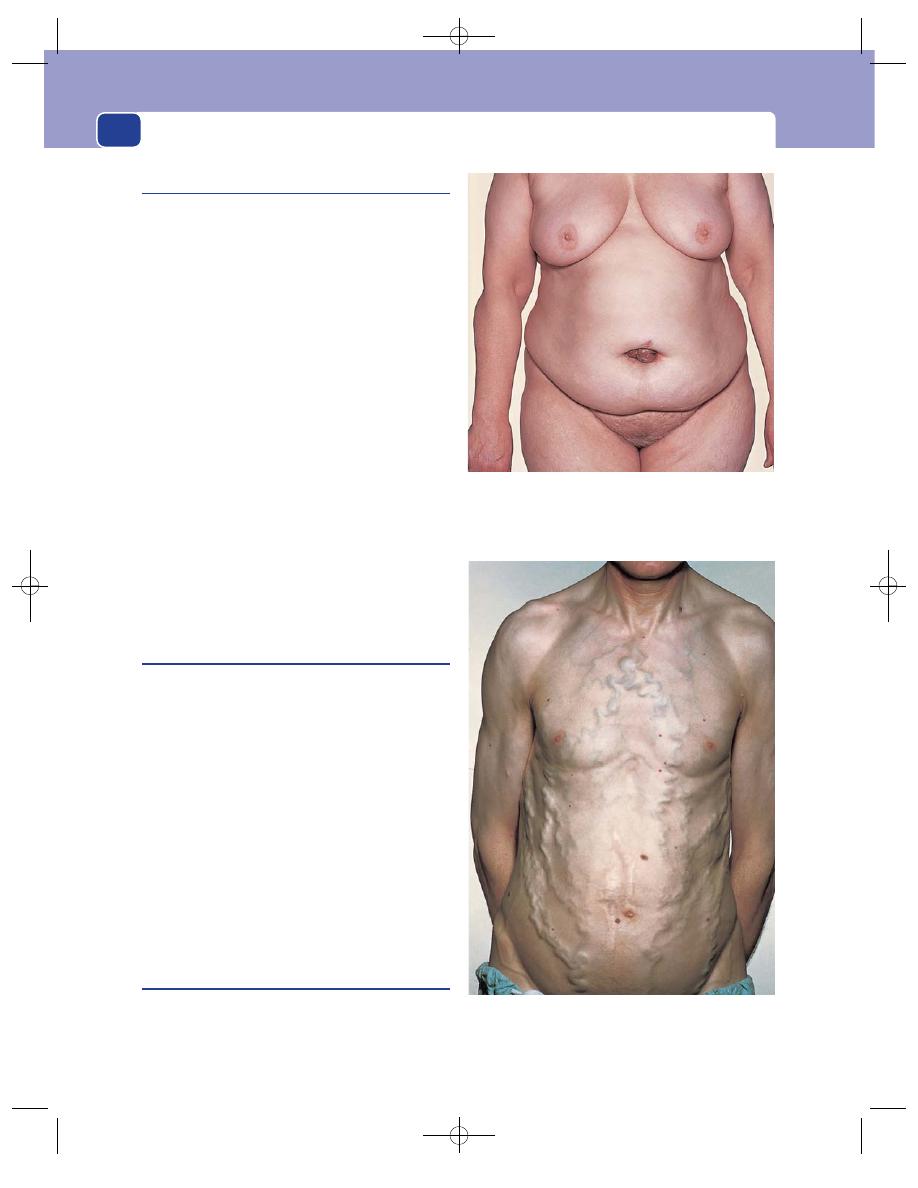
The abdominal wall, herniae and the umbilicus
Ompholith
When the sebaceous secretions which accumulate
in the umbilicus are mixed with the broken hairs
and fluff from clothing that become sucked into the
umbilicus, the mixture can form a firm lump, worthy
of the name umbilical stone or ompholith. The
outside tip of the concretions dries out and may
protrude like a sebaceous horn. In certain parts of
the UK there is an old wives’ tale that if this stone is
removed, the sufferer will bleed to death!
Routine personal hygiene will usually prevent
the formation of an ompholith, but this is not
always as simple as it sounds, for the umbilicus can
be deep and narrow, particularly in the obese.
Small concretions are common and uncompli-
cated. Occasionally an abscess will develop in a
narrow-necked umbilicus containing an ompholith.
The patient feels unwell and has a very painful,
throbbing, swollen umbilicus which may be difficult
to distinguish from a strangulated umbilical hernia.
Pus tracking from an intra-abdominal abscess
may occasionally point at the umbilicus, the com-
monest cause being diverticular disease.
Secondary carcinoma
(Sister Joseph’s nodule)
A firm or hard nodule bulging into the umbilicus,
underneath the skin or eroding through it, in a
patient who is losing weight and looks unwell is
likely to be a nodule of metastatic cancer. This pre-
sentation always indicates advanced, widespread
intra-abdominal disease, and the primary tumour is
usually in the abdomen.
The tumour cells reach the umbilicus via lymph-
atics that run in the edge of the falciform ligament
alongside the obliterated umbilical vein, or by trans-
peritoneal spread.
Nodules of secondary carcinoma may ulcerate,
bleed and become infected. Rarely, the tumour
deposit is in continuity with bowel and there may be
an acquired intestinal fistula.
Endometrioma
If, in a female patient, the umbilicus enlarges, becomes
painful and discharges blood during menstruation,
it may contain a patch of ectopic endometrial tissue.
384
FIG 14.23
A nodule of metastatic carcinoma bulging through
the umbilicus causing a serosanguinous discharge. This is
known as Sister Joseph’s nodule.
FIG 14.24
Inferior vena caval obstruction may present
with dilated subcutaneous veins in the abdominal and
chest walls.
Chap-14.qxd 4/21/05 12:55AM Page 384
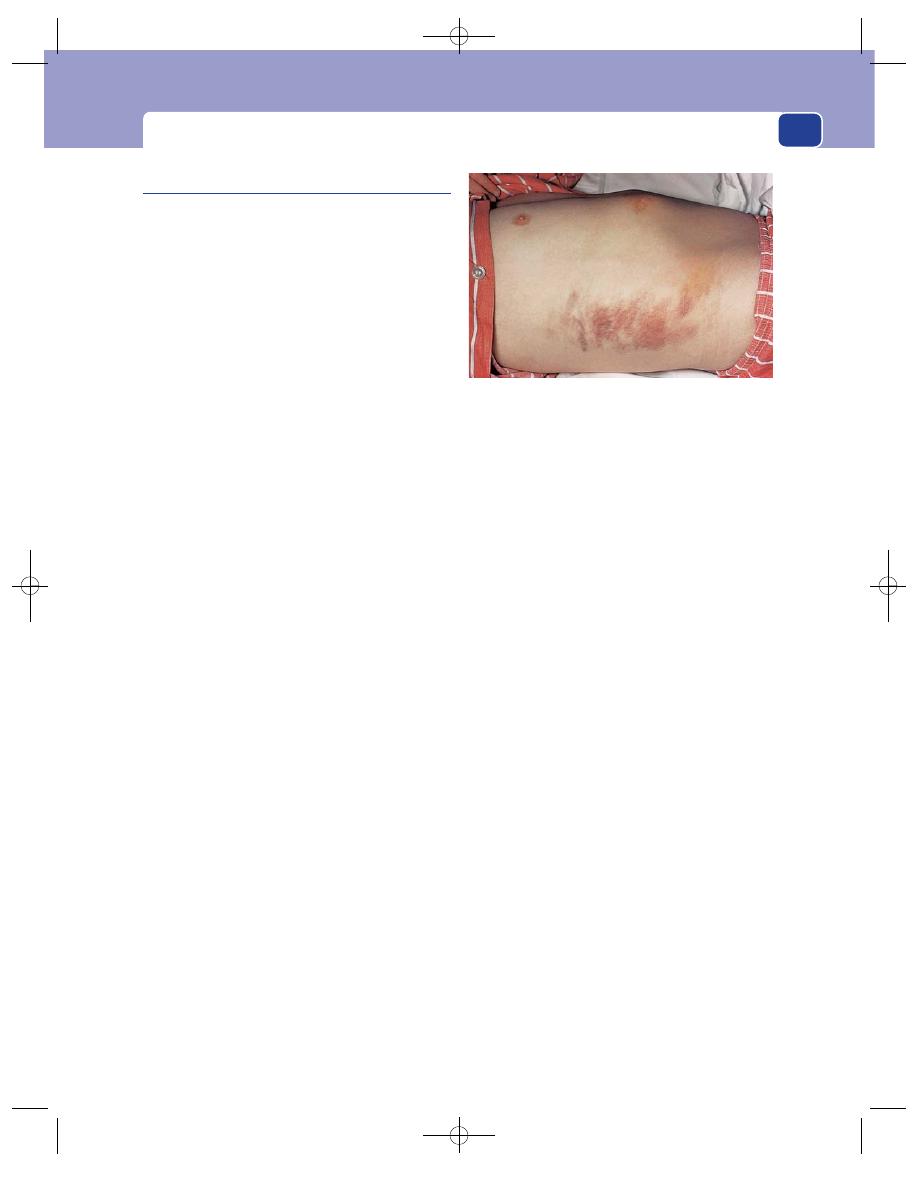
The umbilicus
385
Discolouration of the umbilicus
The following physical signs are rare, but the diseases
that cause them are common and serious.
A blue tinge around the umbilicus, caused by
dilated, tortuous, sometimes visible, veins, is called a
caput medusae, after Medusa, the mythical Gorgon
who had small snakes on her scalp instead of hair.
The dilated veins are collateral vessels that have
developed to circumvent portal vein obstruction.
There will be other signs of portal hypertension and
liver failure.
Yellow-blue bruising around the umbilicus
(Cullen’s sign) and in the flank (Grey Turner’s sign)
may be caused by pancreatic enzymes which have
tracked along the falciform ligament to the umbil-
icus or across the retroperitoneal space to the loin
and digested the subcutaneous tissues following an
attack of severe acute pancreatitis. Both appear a
few days after the beginning of the acute symptoms.
Bruising at the umbilicus can also be associated
with intra-abdominal bleeding, particularly when it
is extraperitoneal. Causes include ruptured ectopic
pregnancy and accidental peri-uterine bleeding in
pregnancy.
FIG 14.25
Grey Turner’s sign. Bruising in the left flank
caused by acute haemorrhagic pancreatitis.
Chap-14.qxd 4/21/05 12:55AM Page 385
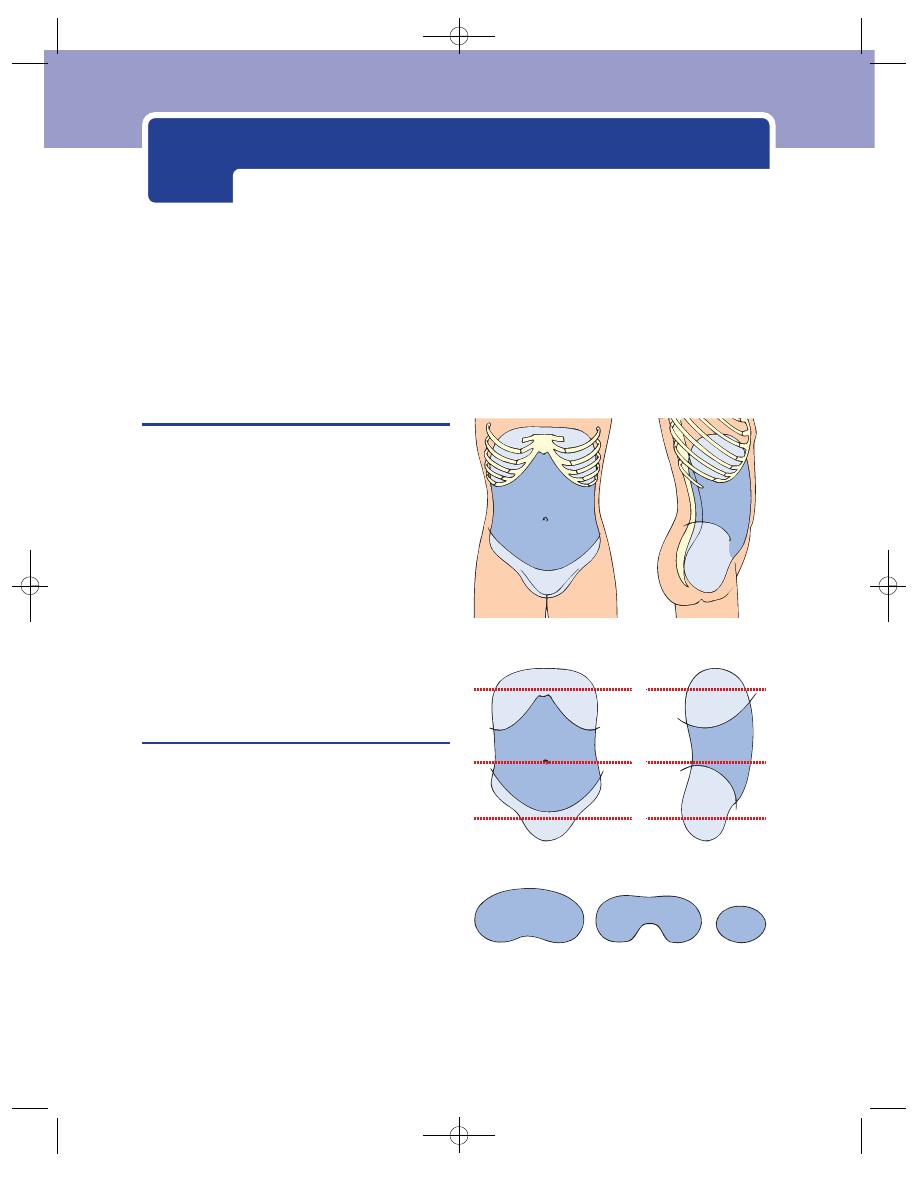
THE EXAMINATION OF THE ABDOMEN
The abdomen contains the stomach, duodenum,
small and large bowel, liver, gallbladder, spleen, pan-
creas, kidneys, uterus, bladder, aorta and vena cava
and, in women, the uterus, ovaries and Fallopian
tubes. This relatively small cavity therefore contains
a number of vital organs, all of which are susceptible
to disease or malfunction but many are inaccessible
to palpation, being hidden behind the lower ribs or
inside the bony pelvis (Fig. 15.1).
Because the abdominal organs are so close
together, the brain is often incapable of distin-
guishing which of them is the source of a pain, but
other symptoms and signs may help to distinguish
the likely organ and the pathology responsible for
the pain.
Preparation
The environment
The examination room must be warm and private if
the patient is to lie undressed and relaxed. A cold
couch placed in a draught or in the view of other
patients makes proper examination impossible. A
good light is essential, with, ideally, daylight coming
obliquely from the side of the patient to emphasize
the shadows. Artificial light obliterates the soft
shadows that often give the first indication of asym-
metry, and many neon lights falsify colours, particu-
larly the yellows and blues.
The examination couch or bed
A hard, flat couch makes the patient lie absolutely flat
and opens the gap between the pubis and the xiphis-
ternum, but unfortunately stretches and tightens
A
A
B
C
B
C
FIG 15.1
These drawings show the extent of the
abdominal cavity. The paler lavender areas indicate the parts
of the abdomen protected by the ribs and the pelvis. The
levels of the three cross-sections are indicated on the
central diagram.
Chap-15.qxd 4/19/05 14:34PM Page 386
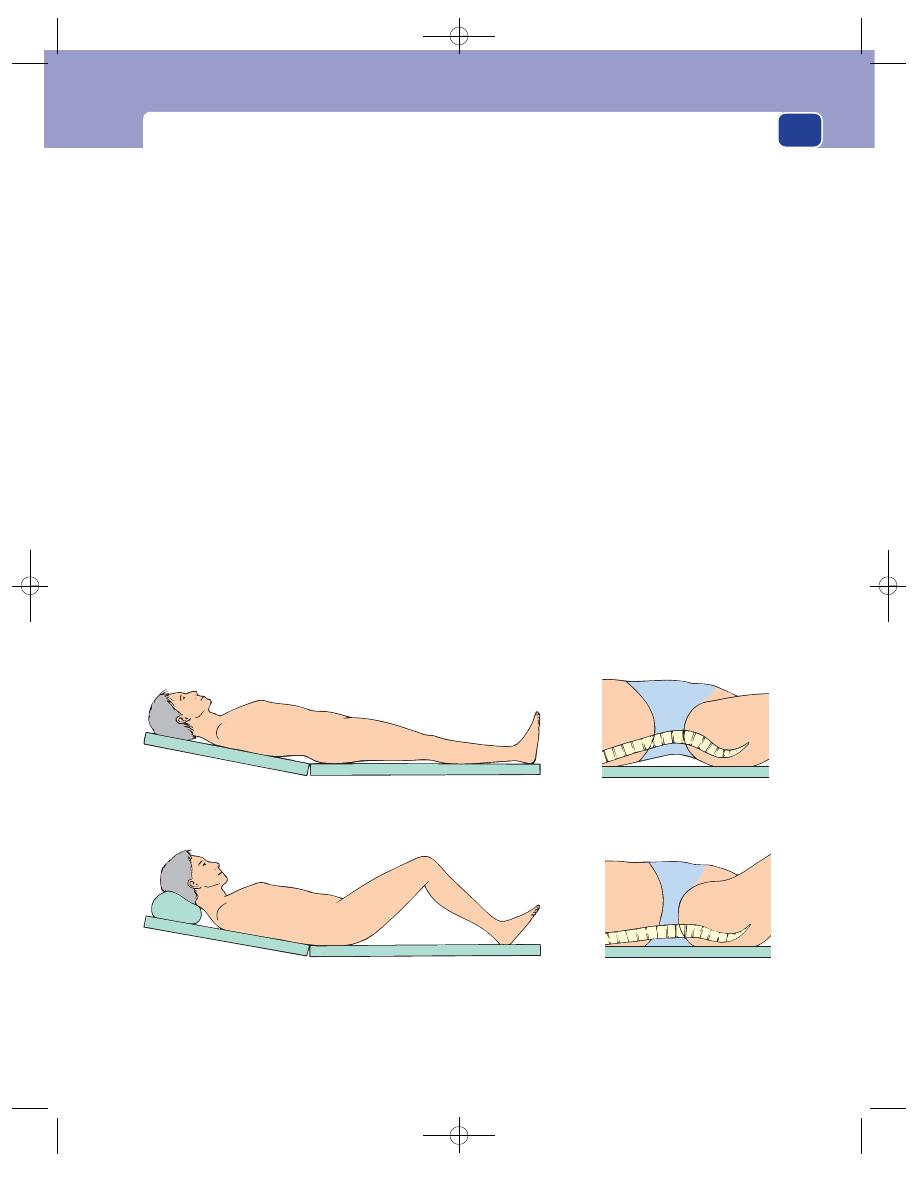
The examination of the abdomen
387
the abdominal muscles. A soft bed lets the lumbar
spine sink into a deep curve and closes the gap
between the pubis and the ribs. The best compromise
in the office or outpatients is a hard couch with a
backrest that can be raised by 15–20°. The hard couch
ensures that patients retain their lumbar lordosis,
opening access to the abdomen and pushing the cen-
tral contents anteriorly. The elevation of the thoracic
cage relaxes the anterior abdominal wall muscles.
Exposure
The full extent of the abdomen must be visible and,
ideally, patients should be uncovered from nipples to
knees. Many find this embarrassing and a comprom-
ise is to cover the lower abdomen with a sheet or blan-
ket while palpating the abdomen, but never forget to
examine the genitalia and the hernial orifices.
Getting the patient to relax
It is not possible to feel anything within the abdomen
if the patient is tense. There are several ways in
which relaxation can be encouraged.
■
Ask the patient to rest their head on the couch
or a pillow to avoid tensing the rectus
abdominis muscles.
■
Ask the patient to place their arms by their
sides, not behind their head.
■
Encourage the patient to sink their back into the
couch and breathe regularly and slowly.
■
Only press your hands into the abdomen during
expiration as the abdominal muscles relax.
If these manoeuvres do not work, ask the patient to
flex their hips to 45° and their knees to 90° and place
an extra pillow behind their head. Although these
manoeuvres tilt up the pelvis and reduce access to the
abdomen, they usually relax the abdominal muscles.
The position of the examiner
The examiner’s hands should be clean and warm
with short nails. It is impossible to palpate deeply
with long nails and it is an insult to the patient to
have dirty hands.
The whole hand should rest on the abdomen by
keeping the hand and forearm horizontal, in the same
plane as the front of the abdomen. To achieve this
the examiner must sit or kneel beside the bed. Do
not examine the patient from a standing position by
leaning forwards and dorsi-flexing your wrist.
Sitting or kneeling beside the patient with your
forearm level with the front of the abdomen puts your
(a)
(c)
(b)
(d)
FIG 15.2
EXAMINATION OF THE ABDOMEN. (a) Examine the abdomen with the patient on a firm couch or bed with just sufficient
support beneath the shoulders and head to stop the anterior abdominal wall being stretched tight. (b) If the abdominal wall is
tight, raise the head and flex the hips. (c) and (d) These figures show the reduction in the area of abdomen available for
palpation if the patient lies on a soft bed that allows the lumbar lordosis to straighten.
Chap-15.qxd 4/19/05 14:34PM Page 387
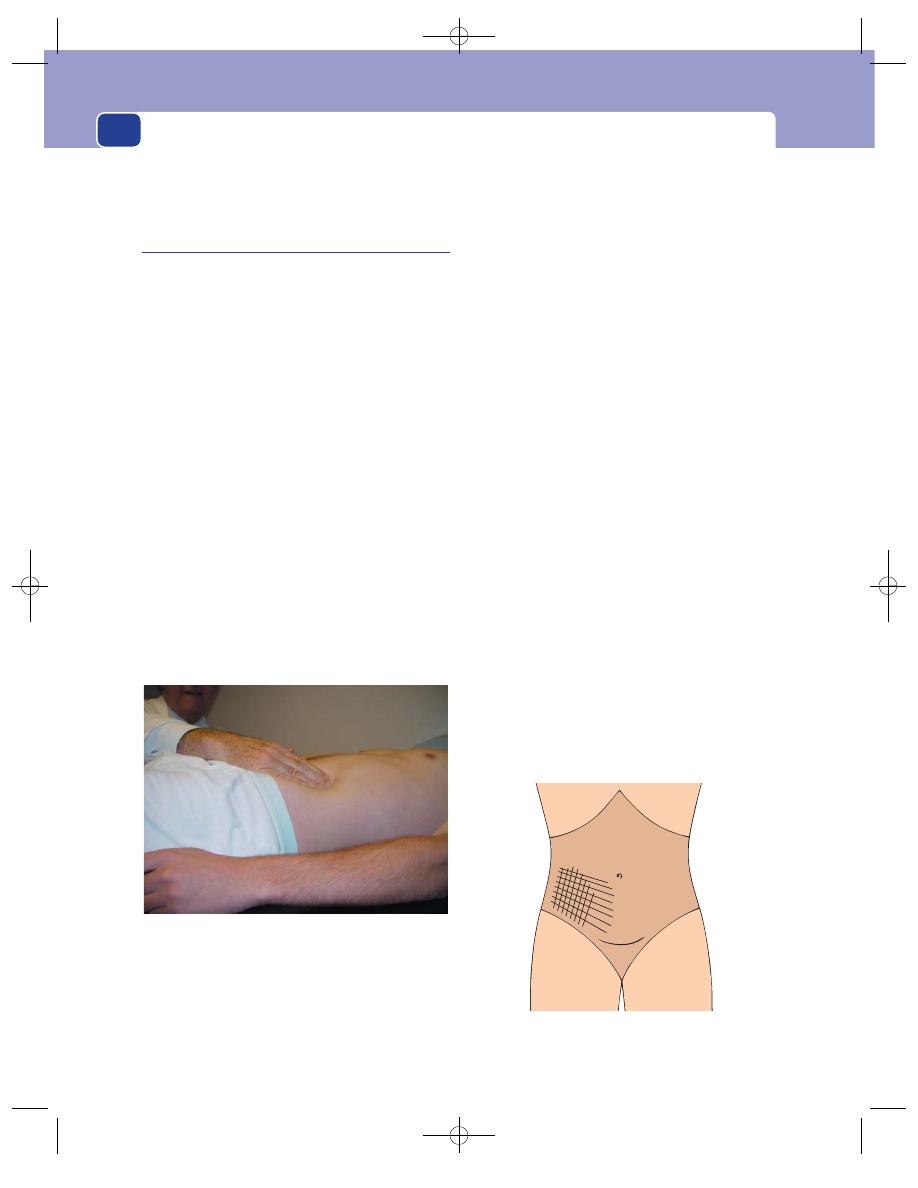
The abdomen
388
eyes about 50 cm above your hand, an ideal level for
seeing any soft shadows caused by lumps and bumps.
Examination
This should follow the standard routine of inspec-
tion, palpation, percussion and auscultation.
Inspection
Look at the whole patient. Look for any general
abnormality indicative of intra-abdominal pathology
such as cachexia, pallor or jaundice.
Inspection of the abdomen from the end of the
bed will reveal if there is any asymmetry or distension.
Note the position, shape and size of any bulge,
any changes in its shape, and whether it moves with
respiration or increases with coughing.
Observe the reaction of the patient to coughing
or moving. Patients with peritonitis find movement
extremely painful and, consequently, tend to lie very
still, whilst patients with colic roll around with each
bout of pain.
Record the presence of any scars, sinuses or fistulae.
Dilated surface veins may indicate the possibility
of portal hypertension or inferior vena caval occlu-
sion (see Fig. 14.24, page 384).
Palpation
Palpate gently but deliberately, firmly and with pur-
pose. Rapid, jerky or circular movements reminiscent
of kneading dough are distressing for the patient and
cause them to lose confidence. Keeping your hands
still and feeling the intra-abdominal structures mov-
ing beneath them gives more information than rapid
and thoughtless palpation.
Finish (or begin) by feeling the areas that might
otherwise be forgotten.
1. Feel the supraclavicular fossae and neck for
lymph glands.
2. Feel the hernial orifices at rest and when the
patient coughs.
3. Feel the femoral pulses.
4. Examine the external genitalia.
5. Look at the hands, nails and facies.
General light palpation for tenderness
This should be done by gently resting a hand on the
patient’s abdomen and pressing lightly. The hand
should be systematically moved over the whole of
the abdomen. If you are right handed, start in the
left iliac fossa and move round in an anti-clockwise
direction to finish in the right iliac fossa.
When a patient complains of pain, asked them to
indicate its site before you begin your palpation, so
that you can start over a non-tender area and move
towards the tender spot. Carefully define the area of
tenderness so that you can depict it as a hatched area
on a drawing of the abdomen (Fig. 15.4).
FIG 15.3
When you palpate the abdomen, sit or kneel so that
your forearm is horizontal and level with the anterior
abdominal wall, and your eyes are 50 cm above this level.
If you are higher, your wrist will be extended and you will
not be able to palpate comfortably and firmly. In this
illustration the abdomen is inadequately exposed. The
patient’s pants should have been removed or lowered down
to the level of the pubis.
FIG 15.4
Indicate areas of tenderness by oblique lines on a
sketch like this. Masses are depicted by outlining their shape.
Chap-15.qxd 4/19/05 14:34PM Page 388
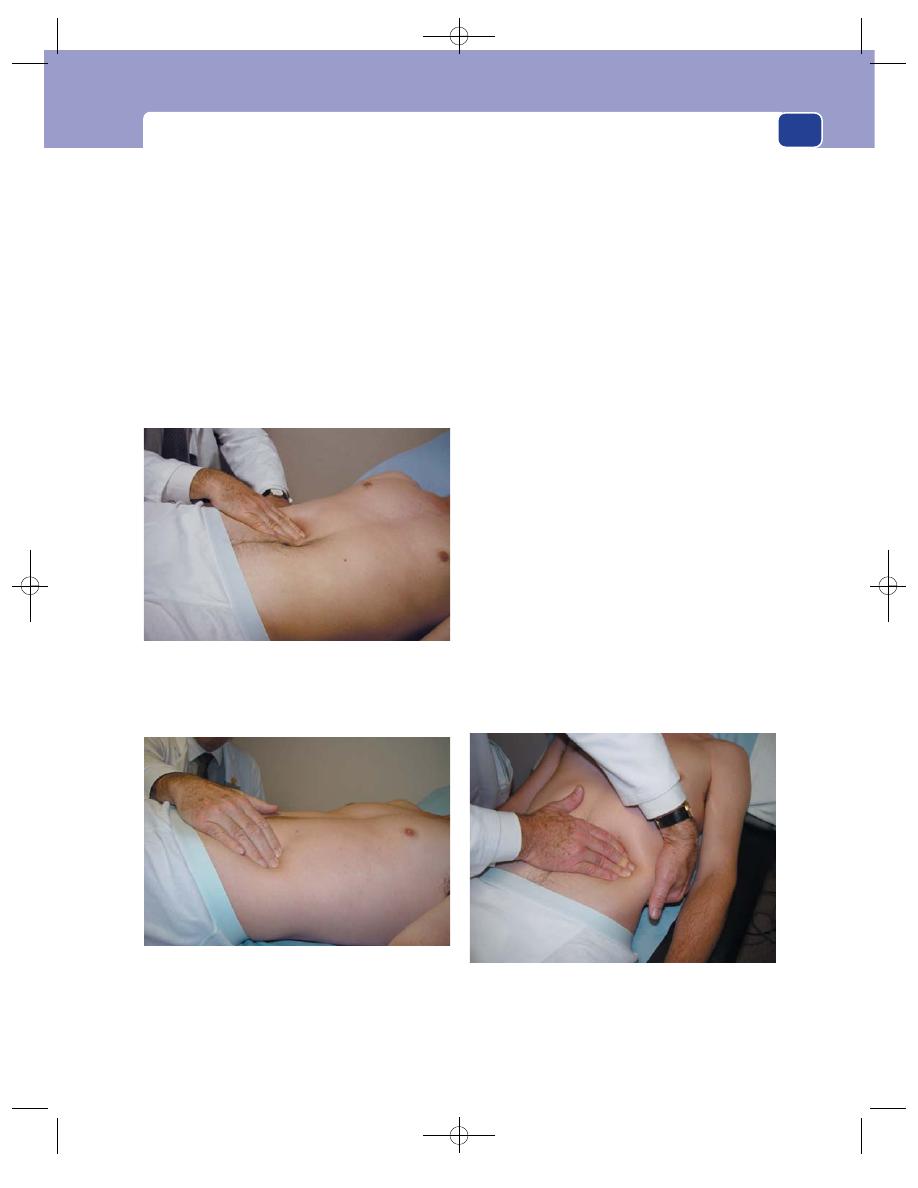
The examination of the abdomen
389
Assess the degree of tenderness. Palpation over
an area of mild tenderness just causes pain. Guarding,
the tightening of the patient’s abdominal muscles in
response to pressure, indicates severe tenderness.
The sudden withdrawal of manual pressure may
cause a sharp exacerbation of the pain, which is
known as rebound or release tenderness. This test
may be distressing for the patient and it is preferable
to assess rebound tenderness by the patient’s response
to light percussion.
Sometimes, release of pressure on a distant non-
tender part of the abdomen may cause pain in a ten-
der area.
General palpation for tenderness
When no pain is elicited by systematic light palpa-
tion over the whole abdomen, repeat the process,
pressing more firmly and deeply to see if there is any
deep tenderness.
Palpation for masses
The whole abdomen must be carefully palpated for
the presence, position, shape, size, surface, edge,
consistence, fluid thrill, resonance and pulsatility of
any masses.
Tender masses in the abdomen are very difficult
to feel because of the protective guarding of the
abdominal wall muscles. A good idea of the surface
and size of a tender mass may be obtained by resting
your hand gently on the tender area and pressing a
little deeper during each exploration and feeling the
mass as it moves beneath your hand.
Rapid, hard pressure achieves nothing under
these circumstances because the patient just tight-
ens their abdominal muscles.
Palpation of the normal solid viscera
The liver
To feel the liver, place your right hand
transversely and flat on the right side of the abdomen
at the level of the umbilicus, parallel with the right
costal margin. Then ask the patient to take a deep
breath. If the liver is grossly enlarged, its lower
edge will move downwards and bump against the
Palpate the liver by resting your fingers on the abdomen
almost parallel to the right costal margin and asking the
patient to breathe in. The liver edge can be made more
prominent by putting your left hand under the lower ribs and
lifting them forwards.
FIG 15.5
PALPATING THE ABDOMEN.
Palpate the kidneys by pressing firmly into the lumbar region
during inspiration while lifting the kidney forwards with your
other hand in the loin. (The exposure is inadequate for a proper
examination of the whole abdomen in these three illustrations.).
Palpate the spleen with your fingers lying transversely across
the abdomen so that its tip will hit the tips of your index and
middle fingers when the patient breathes in. You can make
the spleen more prominent by lifting the lower ribs forwards
with your left hand as you do when palpating the left kidney.
Chap-15.qxd 4/19/05 14:35PM Page 389
The abdomen
390
radial side of your index finger. If nothing abnormal
is felt, repeat the process after moving your hand
upwards, inch by inch, until the costal margin is
reached.
The liver edge may be straight or irregular, thin
and sharp, or thick and rounded. Palpation begin-
ning just below the costal margin can easily miss a
large liver. Gross hepatomegaly may fill the whole
abdomen so, if in doubt, begin your palpation in the
left iliac fossa.
The spleen
An enlarged spleen appears below the tip
of the tenth rib along a line heading towards the
umbilicus and, if really large, may extend into the
right iliac fossa. A normal spleen is not palpable.
To feel the spleen, place the fingertips of your
right hand on the right iliac fossa just below the
umbilicus. Ask the patient to take a deep breath. If
nothing abnormal is felt, move your hand in stages
towards the tip of the left tenth rib. When the costal
margin is reached, place your left hand around the
lower left rib cage and lift the lower ribs and the
spleen forwards as the patient inspires. This man-
oeuvre occasionally lifts a slightly enlarged spleen
far enough forward to make it palpable.
The spleen is recognized by its shape and site
and, when present, the notch on its supero-medial
edge. It is dull to percussion as it lies immediately
beneath the abdominal wall with no bowel in front
of it, unlike a renal mass (see below).
The kidneys
Normal kidneys are usually impalpable,
except in very thin people, but both lumbar regions
should always be carefully examined.
To feel the patient’s right kidney, place your left
hand behind the patient’s right loin between the
twelfth rib and the iliac crest, so that you can lift the
loin and kidney forwards. Then place your right
hand on the right side of the abdomen just below
the level of the anterior superior iliac spine. As the
patient breathes in and out, palpate the loin between
both hands. The lower pole of a normal kidney may
be felt at the height of inspiration in a very thin per-
son. If the kidney is very easy to feel, it is either
enlarged or abnormally low. To feel the left kidney,
lean across the patient, place your left hand around
the flank into the left loin to lift it forwards, then
place your right hand on the abdomen and feel any
masses between the two hands.
An enlarged kidney can be pushed back and forth
between the anterior and posterior hands. This is
called balloting. It feels like patting a ball back and
forth in a pool of water. Balloting is also used to pal-
pate a fetus in a pregnant uterus.
Percussion
The whole abdomen must be percussed, particu-
larly over any masses. A dull area may draw your
attention to a mass that was missed on palpation
and indicate a more detailed and careful palpation
of the area of dullness. When there is a circum-
scribed mass, a tap on one side while feeling the
opposite side with the other hand may reveal that it
conducts a fluid thrill. Any area of dullness should
be outlined by percussion with the abdomen in two
positions to see if it moves or changes shape. Free
fluid (ascites) changes shape and moves (shifting
dullness, see pages 433–4).
Percussion causes pain if peritonitis is present
and is a useful method for mapping out a tender
area (see above).
If a part or the whole of the abdomen is dis-
tended, the patient should be held at the hips and
the abdomen shaken from side to side. Splashing
sounds, a succussion splash, indicate that there is
an intra-abdominal viscus, usually the stomach, dis-
tended with a mixture of fluid and gas.
Auscultation
Listen to the bowel sounds. Peristalsis produces gur-
gling noises because the bowel contains a mixture of
fluid and gas. The pitch of the noise depends upon
the distension of the bowel and the proportions of
gas and fluid. Normal bowel sounds are low-pitched
gurgles which occur every few seconds. The absence
of bowel sounds indicates that peristalsis has ceased.
Revision panel 15.1
Never forget to examine
Supraclavicular lymph glands
Hernia orifices
Femoral pulses
Genitalia
Bowel sounds
Anal canal and rectum
Chap-15.qxd 4/19/05 14:35PM Page 390
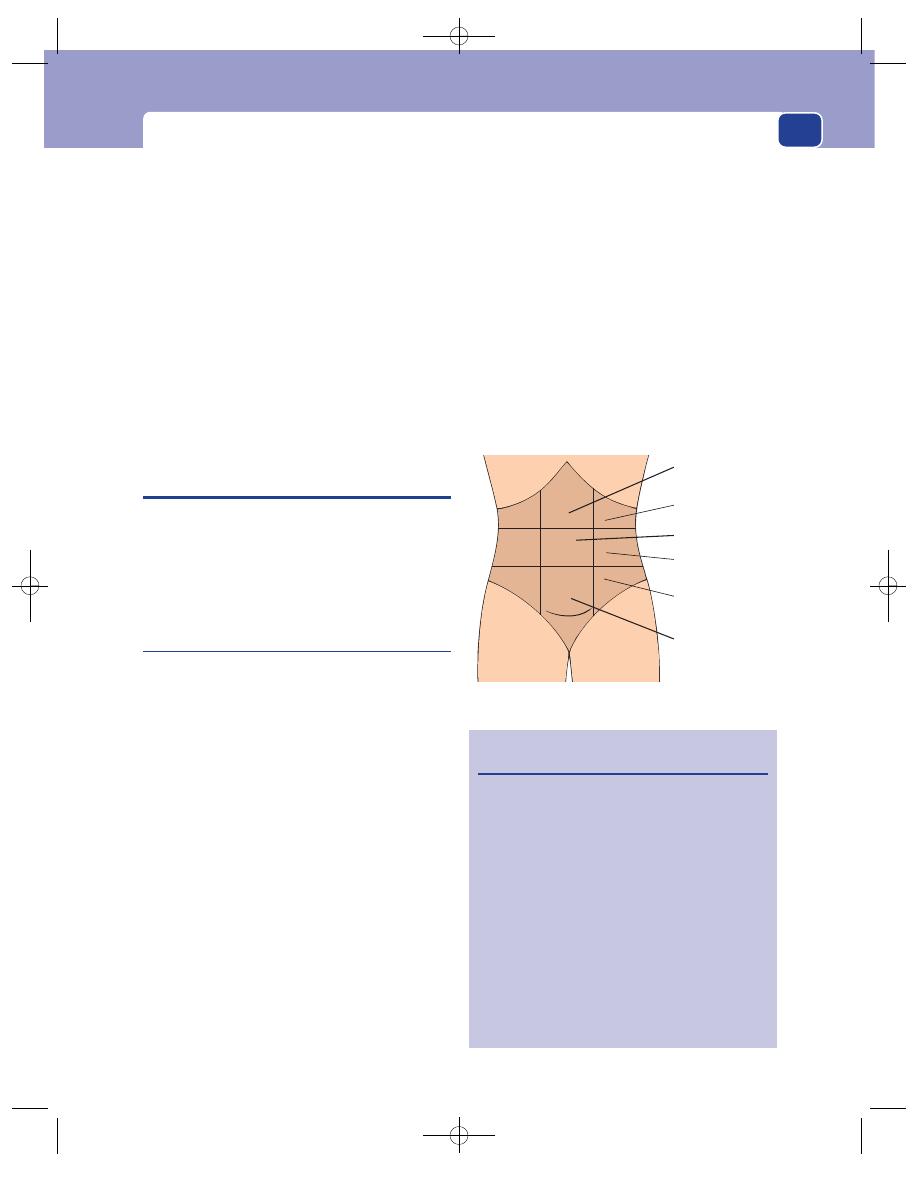
Abdominal pain
391
This may be either a primary or secondary phenom-
enon. If you can hear the heart and breath sounds
but no bowel sounds over a 30-second period, the
patient probably has a paralytic ileus.
Increased peristalsis increases the volume and
frequency of the bowel sounds. Distension of the
bowel caused by a mechanical intestinal obstruction
is associated not only with increased bowel sounds
but also with a change in the character of the
sounds. They become amphoric in nature with runs
of high-frequency gurgles, sounding like sea water
entering a large cave through a narrow entrance,
often described as ‘tinkling’.
Having assessed the quality of the bowel sounds, it
is important to listen for any systolic vascular bruits.
ABDOMINAL PAIN
Time spent taking a careful history is never wasted, as
abdominal pain is the only symptom of many intra-
abdominal diseases. The two most significant proper-
ties of an abdominal pain are its site and its character.
The significance of the site of
abdominal pain
The abdomen can be divided into three horizontal
zones – upper, central and lower – by two horizon-
tal lines. These are the transpyloric plane (a line cir-
cling the body mid-way between the suprasternal
notch and the symphysis pubis) and the transtuber-
cular plane (a line circling the body that passes
through the two tubercles of the iliac crest) as
shown in Figure 15.6. Each of these three zones can
be further vertically subdivided into three regions –
central, right and left – by the two mid-clavicular
lines.
The anatomical names of these nine regions are:
■
the epigastrium
■
the right hypochondrium
■
the left hypochondrium
■
the umbilical region
■
the right lumbar region
■
the left lumbar region
■
the hypogastrium or suprapubic region
■
the right iliac fossa
■
the left iliac fossa.
Sometimes patients are only capable of localizing
pain to the upper or lower half of the abdomen
and/or to the left or right side.
Colicky pain is referred to the centre of the
abdomen whatever its source, as it is a visceral sen-
sation, whereas the pain from the parietal peritoneum
is felt over the inflamed area (somatic sensation).
Pain in the upper abdomen is most likely to arise
from the biliary tree, stomach, duodenum or pan-
creas. These structures produce right-sided, central
and left-sided pain respectively. The pain from these
three organs radiates in different directions.
■
Gallbladder pain may radiate through to the
back and to the right to reach the tip of the
Epigastrium
Hypochondrium
Umbilical region
Lumbar region
Iliac fossa
Hypogastrium
FIG 15.6
The names of the regions of the abdomen.
Revision panel 15.2
The features of a pain that must be elicited
Time and nature of onset
Site
Character (burning, throbbing, stabbing,
constricting, colicky, aching)
Severity
Progression
Duration
End
Radiation
Relieving factors
Exacerbating factors
Associated symptoms, e.g. vomiting,
diarrhoea, painful micturition, missed or
absent periods
Chap-15.qxd 4/19/05 14:35PM Page 391
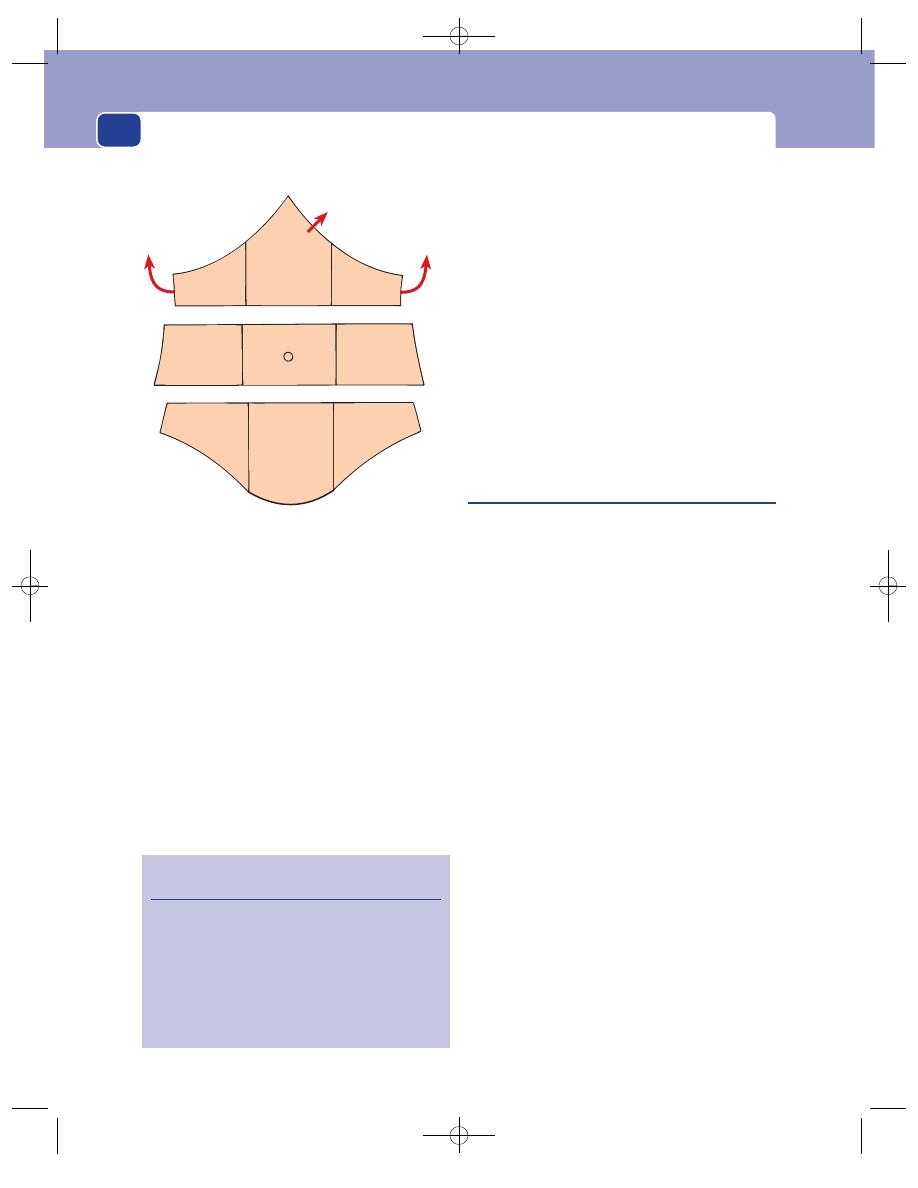
The abdomen
392
scapula. When felt in this area, it often seems to
the patient to be a separate, independent pain.
■
Ulcers in the posterior wall of the stomach or
duodenum cause a pain that radiates through to
the back.
■
Pancreatic pain also tends to go through to the
back and sometimes to the left.
Pain in the centre of the abdomen is most likely
to arise from the small bowel, caecum and mid-line
retroperitoneal structures such as the aorta. Pain from
retroperitoneal structures often radiates through to
the back. Pain in the lateral zones of the central
region is most likely to come from the kidneys. Pain
from the kidney is also felt in the loin and may radi-
ate down to the groin. All visceral pain may move
and become localized if the inflammatory process
in the viscus involves the parietal peritoneum.
Pain in the lower abdomen is most likely to
come from the appendix, caecum, colon, bladder,
uterus, ovaries and Fallopian tubes. Pain in the
hypogastric region usually arises from the bladder,
rectum, uterus and its adnexae. Pain in the right
iliac fossa usually comes from the caecum and the
appendix. Pain in the left iliac fossa usually comes
from the sigmoid colon.
Lower abdominal pains rarely radiate, but pain
from pelvic structures may be referred to the lower
back or perineum.
The significance of the character
of abdominal pain
It is possible to subdivide the character of the pain
of the majority of the painful conditions that occur
within the abdomen into two large categories: a
constant pain associated with inflammation and
neoplasic infiltration, and a colicky pain associated
with obstruction of a muscular conducting tube such
as the bowel or the ureter (colic).
The constant pain caused by inflammation or
infiltration, whether it is the mild inflammatory
response around a chronic peptic ulcer or the acute
response to a perforated appendix, is made worse by
any local or general movement and persists until the
underlying cause subsides. Inflammation within the
abdomen does not throb or burn in the same way
that inflammatory pains do elsewhere.
The colic caused by obstruction to a muscular
conducting viscus is a pain which fluctuates in sever-
ity at frequent intervals and feels griping in nature.
The source of bowel colic can be suspected from the
time interval between the peaks of the pain – short
in the jejunum, longer in the ileum, and longer still
in the colon. In biliary colic and renal colic, the
peaks of pain are short and the pain seldom goes
away completely between exacerbations. Prolonged
obstruction to the outflow of any hollow viscus ultim-
ately causes it to distend. This produces a constant
‘stretching’ pain, which is different from the ache of
inflammation but not colicky in nature. A similar
pain can come from conditions that stretch the
retroperitoneal tissues.
Gall bladder
Stomach and
duodenum
Pancreas
and straight through
to the back
and through to
the back and
the right
and through to
the back and
the left
Kidney
Small bowel
Caecum
Kidney
Retroperitoneal
structures
Appendix and
caecum
Sigmoid
colon
Transverse
colon
Bladder
Uterus and
adnexae
FIG 15.7
The structures that commonly cause pain in the nine
anatomical regions of the abdomen and often radiate through
to the back.
Revision panel 15.3
The principal causes of abdominal pain
Inflammation/infection
Perforation of a viscus
Obstruction of a viscus
Infarction/strangulation
Intraperitoneal/retroperitoneal haemorrhage
Injury
Extra-abdominal and medical causes
Chap-15.qxd 4/19/05 14:35PM Page 392
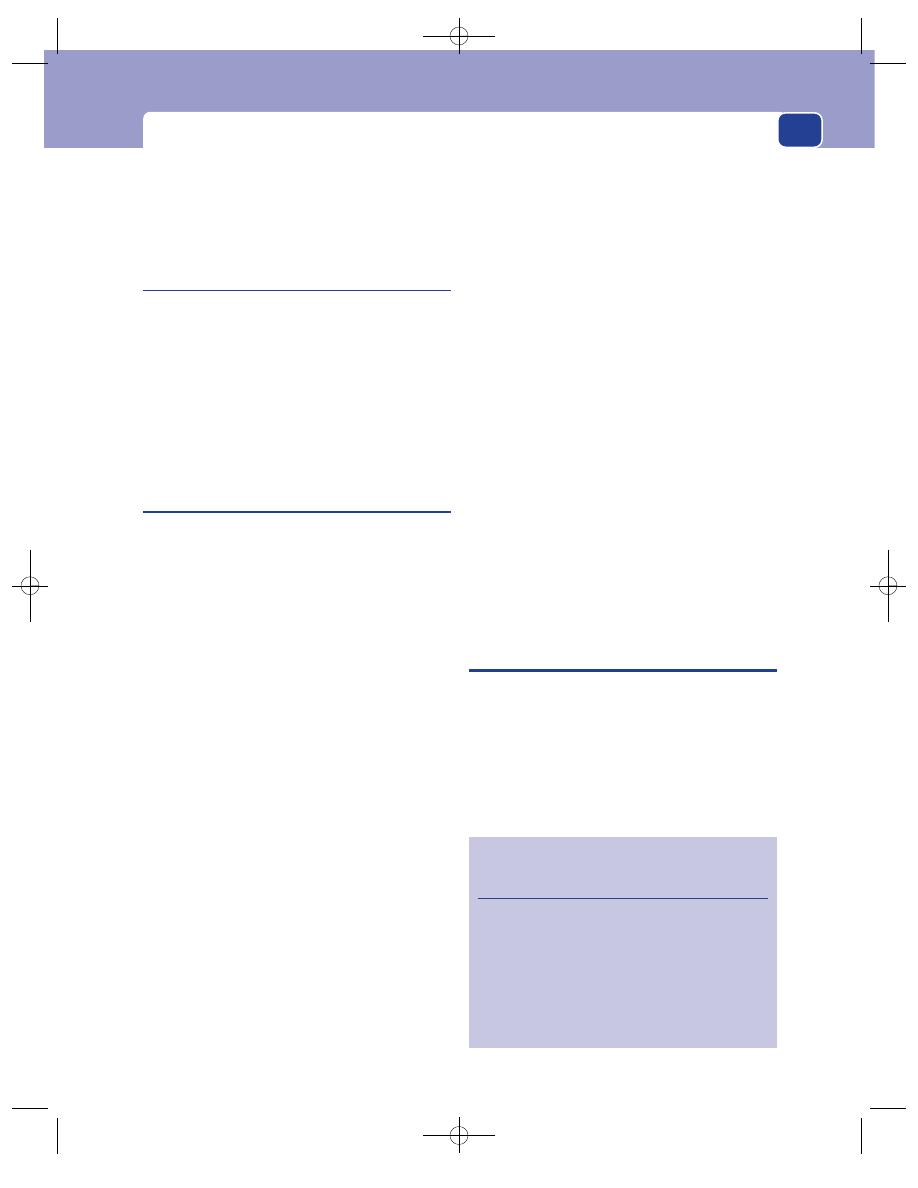
Upper abdominal pain
393
Colic can also be caused by muscular dysfunction,
i.e. disorders of gastrointestinal mobility such as the
irritable bowel syndrome, as opposed to true colic
which is secondary to obstruction.
The significance of radiation
Radiation of a pain signifies that other structures
are becoming involved. For example, when the pain
from a duodenal ulcer radiates through to the back,
it indicates that the inflammation has spread beyond
the duodenum into adjacent structures in the poster-
ior abdominal wall, such as the pancreas. Radiation,
therefore, not only indicates the source of the pain,
but may also hint at the extent of the disease.
The significance of the rate of onset
and severity
Patients with severe abdominal pain of acute onset
are usually collectively grouped as having an ‘acute
abdomen’. These patients usually consult their general
practitioner or seek emergency medical help once
their pain has persisted for more than an hour or so.
However, many will have had chronic symptoms over
the preceding months or years caused by the condi-
tion currently causing their acute symptoms, i.e. the
same condition can present acutely or chronically.
Therefore, although the rate and severity of pre-
sentation may indicate the urgency of the problem,
they do not always indicate the nature of the under-
lying pathology.
Whatever the urgency and underlying pathology,
a full history and clinical examination (as described
above) must be carried out so that a working diag-
nosis or differential diagnosis can be made and the
patient assigned to one of the following manage-
ment categories.
■
An acute abdomen, e.g. peritonitis, with a
known or unknown underlying cause requiring
urgent treatment.
■
An abdominal pain of known or unknown
cause requiring pain palliation pending further
investigation and treatment.
■
An abdominal pain with no evidence of any
clinically detectable intra-abdominal pathology
that can be observed and investigated later if
necessary, i.e. time to wait and see.
Put another way:
■
I may or may not know the diagnosis but the
problem needs urgent management.
■
I understand the problem but not necessarily its
cause and have time to investigate further in
order to decide what to do.
■
I do not think there is anything wrong and can
wait and see whether further investigations will
be required.
In almost every case, additional investigations are
likely to be required to refine the diagnosis and plan
treatment but, when the diagnosis is ‘uncertain’, care-
ful monitoring and repeated re-examination are
essential to detect any progression or resolution of
the problem and ensure that important new phys-
ical signs are not missed. Acute physical signs often
develop over several hours and become clear cut,
often diagnostic, by the time of a later examination.
In contrast, the signs of chronic conditions may take
months to develop.
UPPER ABDOMINAL PAIN – ACUTE
AND/OR CHRONIC – CAUSED BY
INFLAMMATORY AND MALIGNANT
CONDITIONS
The common sites of inflammation and malignant
disease in the upper abdomen causing upper abdom-
inal pain are in the stomach and duodenum, gallblad-
der and pancreas.
The conditions causing acute and/or chronic
upper abdominal pain are summarized in Revision
panels 15.4 and 15.5.
Revision panel 15.4
The common conditions that present with
acute upper abdominal pain
Oesophagitis
Boerhaave’s syndrome
Acute gastritis
Perforated peptic ulcer
Acute cholecystitis
Gallstone and biliary colic
Acute pancreatitis
Chap-15.qxd 4/19/05 14:35PM Page 393
The abdomen
Oesophagitis
This occurs when acid pepsin refluxes up out of the
stomach into the oesophagus through the lower
oesophageal sphincter onto the squamous epithe-
lium lining the oesophagus, which is not able to
resist these powerful chemicals. In many instances
the reflux occurs because of gastro-oesophageal
junction incompetence caused by a hiatus hernia.
Patients complain of heartburn, which is a
severe burning discomfort felt in the centre of the
chest behind the heart, often at night. The frequency
and severity of the heartburn is made worse by lying
flat, so patients sleep propped up on pillows to try to
reduce its occurrence. Heartburn is often initiated
by bending, stooping or heavy lifting. When reflux
occurs, patients may experience a bitter taste devel-
oping in the mouth, which is often accompanied by
flatulence and coughing if any of the refluxing acid
spills over into the lungs. Sometimes the burning
pain may only be experienced in the epigastrium.
After many years, patients may complain of diffi-
culty with swallowing and of food sticking in their
gullet. Although the presence of dysphagia suggests
the development of a stricture caused by the acid
reflux, achalasia or a carcinoma of the oesophagus
or cardia must be excluded.
Examination
This rarely reveals any diagnostic signs. The diagno-
sis relies on endoscopy and other investigations.
Boerhaave’s syndrome
This syndrome is caused by a full-thickness tear at
the oesophago-gastric junction, perhaps as a conse-
quence of attempting to suppress a vomit.
The patient complains of the sudden onset of a
severe pain in the upper abdomen or lower chest
after a bout of vomiting. The condition should be
suspected if, in addition to tenderness, guarding and
rigidity in the upper abdomen, there is supraclav-
icular subcutaneous emphysema.
Subcutaneous bubbles of air – emphysema – feel
like the little plastic air pockets in ‘bubble wrap’
which compress, crackle and pop beneath the fin-
gers during gentle palpation.
Acute gastritis/duodenitis/peptic
ulceration
Benign gastric and duodenal ulcers are classified
together as peptic ulceration. Mucosal infection
with Helicobacter pylorides is a major factor in the
development of both these conditions.
Gastric ulcers are now rare in the UK, so any
patient presenting with indigestion, non-specific
upper abdominal pain and the recent onset of weight
loss should be suspected of having a gastric cancer.
Duodenal ulcers are still common everywhere
and affect both sexes in equal numbers. They can
occur at any age, but do so most often in middle-
aged patients.
History
Symptoms
Patients with acute peptic ulceration pres-
ent with acute pain of short duration but may have
had previous similar episodes interspersed with peri-
ods of relief lasting for many months or even years.
The main symptom of acute peptic ulceration is
an epigastric discomfort or pain, which is related
to meals and described as indigestion. It can vary
from a mild discomfort to a very severe pain that
forces the patient to lie down. The severity and ten-
derness may equal those of a perforated peptic ulcer.
Patients with acute gastric ulcers are typically
afraid to eat because the pain is induced by food.
Vomiting often relieves the pain.
Patients with duodenal ulcers typically have a
good appetite and rarely lose weight because they
eat frequently to relieve their pain. Acid brash,
water brash and heartburn are rare symptoms. They
are more frequent in patients with duodenal than
gastric ulceration.
Haematemesis and melaena may complicate all
forms of peptic ulceration.
394
Revision panel 15.5
The common conditions that present with
chronic upper abdominal pain
Chronic peptic ulceration
Carcinoma of the stomach
Chronic cholecystitis
Chronic pancreatitis
Liver metastases
Splenomegaly
Chap-15.qxd 4/19/05 14:35PM Page 394
Upper abdominal pain
Drugs
Many drugs, but especially aspirin and the
non-steroidal anti-inflammatory drugs that are used
to treat arthritis, irritate the gastric mucosa and
cause ulceration, even perforation, so it is essential
to ascertain the precise details of any drug ingestion.
Social history
Cigarette smoking and periods of stress
may be important risk factors.
Examination
Abdominal examination usually reveals epigastric
tenderness, with guarding if the pain is severe. The
patient may be anaemic if there has been chronic
silent bleeding before the acute episode.
Chronic peptic ulceration, gastritis
and duodenitis
History
Age
Peptic ulceration tends to occur between the ages
of 20 and 60 years.
Sex
Both gastric and duodenal ulcers are more
common in men than in women.
Occupation
There is a higher incidence amongst the
professional and executive classes.
Symptoms
Although a few patients present to hospital
with an acute, sometimes very severe upper abdom-
inal pain of short duration as described above, the
great majority of patients with chronic peptic ulcer-
ation present with a chronic, less severe and more
intermittent pain, which they usually call ‘indiges-
tion’ or dyspepsia because it is directly related to
the ingestion of food. Nevertheless, some experi-
ence continuous pain over many hours or days
which is unaffected by food.
Night pain, which wakes the patient and seems
to be unrelated to food, is a common symptom of
duodenal ulceration. This is thought to be caused by
the drop of pH in the stomach at night, when the
acid secretions are no longer buffered by the pres-
ence of food. The pain is usually experienced in the
epigastrium and may radiate into either the back
or the right hypochondrium if the ulcer is situated
in the posterior part of the stomach or the second
part of the duodenum. The pain is usually described
as a continuous gnawing or boring ache and is
rarely very severe. It is usually episodic, occurring
for two or three weeks at a time before resolving
spontaneously, only to recur a few months later – a
feature known as periodicity. The rapid onset of
pain after food, causing food fear and loss of weight,
suggests the presence of a gastric ulcer. Pain that is
relieved by eating indicates the probability of a duo-
denal ulcer.
The pain is usually relieved by the commercially
available antacids, H2 receptor blockers and proton
pump inhibitors.
Peptic ulcers commonly arise in middle-aged
smokers, but are also common in middle-aged and
elderly patients on long-term non-steroidal anti-
inflammatory drugs.
Vomiting is rare unless a pyloric stenosis has
developed.
Excessive salivation (water brash) and acid brash
are highly suggestive of duodenal ulceration. Some
patients develop heartburn.
Haematemesis and melaena are important
complications which occur in a small proportion of
patients with chronic, and acute, peptic ulceration.
Chronic blood loss may cause an iron deficiency
anaemia, which presents with tiredness and short-
ness of breath.
Chronic peptic ulceration must be differentiated
from other causes of chronic abdominal pain. A
clear history of weight loss suggests a gastric carcin-
oma, whereas acid heartburn and reflux (see below)
suggest oesophagitis. Gallstones and chronic chole-
cystitis may coexist and are important differential
diagnoses (see below).
Examination
General
Anaemia and cervical lymphadenopathy
with obvious cachexia should suggest the possibility
of carcinoma of the stomach rather than peptic
ulceration.
Abdomen
Inspection. Epigastric distension and visible peri-
stalsis may be present if pyloric stenosis has developed.
Palpation. Minor tenderness in the epigastrium is
often the only abnormality. The presence of a succus-
sion splash indicates the presence of pyloric stenosis.
The diagnosis of chronic peptic ulcer is now
almost exclusively made on flexible endoscopy and
biopsy. The importance of Helicobacter pylorides as
395
Chap-15.qxd 4/19/05 14:35PM Page 395
The abdomen
a cause has already been described, and a breath test
is available to confirm its involvement.
Percussion and auscultation. These should be
normal.
Perforated peptic ulcer
Acid gastric juice will enter the peritoneal cavity if a
peptic ulcer erodes the wall of the stomach or duo-
denum at a point where it is only covered by visceral
peritoneum. This causes a chemical peritonitis,
which later becomes infected with bacteria.
History
Age and sex
Perforated peptic ulcers are most com-
mon between the ages of 40 and 60 years but also
occur in the very old because many old people are
given non-steroidal anti-inflammatory drugs. Men
and women are equally affected.
Symptoms
The perforation causes sudden severe
and constant pain. This usually begins in the epi-
gastrium, reaches its maximum intensity quickly and
remains severe for many hours. It gradually extends
to involve the whole of the abdomen. All move-
ment, including respiration, makes the pain worse,
causing the patient to lie immobile on the bed.
Many patients give no history of previous dyspepsia,
but it is important to ask if they have ever suffered
from indigestion in the past.
Drug history
It is important to enquire whether the
patient has taken steroids, non-steroidal anti-
inflammatory drugs or salicylates, because these dis-
pose to perforation.
Examination
General appearance
The patient looks ill and is obvi-
ously in pain, lying completely still. A tachycardia is
common and respiration is shallow, but the tempera-
ture is usually normal.
Abdomen
Inspection. The abdomen is flat and does not rise
and fall with respiration. The abdominal muscles
can be seen to be tightly contracted.
Palpation. In the early stages, tenderness and
guarding may be confined to the epigastrium and
right side, but eventually, when the whole peritoneal
cavity is contaminated, the whole abdomen becomes
very tender, with intense guarding, often described
as board-like rigidity. No intra-abdominal viscus
or masses can be felt because the abdominal muscu-
lature is permanently contracted.
Percussion. This is usually painful. If a large
quantity of air has escaped into the peritoneal cav-
ity, the liver dullness may be diminished or com-
pletely absent.
Auscultation. The bowel sounds disappear once
generalized peritonitis is established.
Beware: after 4–6 hours, the acid in the peritoneal
cavity becomes diluted and the pain and guarding
decrease. Patients think they are improving but
they are in fact getting worse. The peritonitis is
progressing and hypervolaemia is developing. An
increasing tachycardia and absent bowel sounds asso-
ciated with increasing abdominal distension and
sunken eyes indicate that the patient is becoming
extremely ill.
Carcinoma of the stomach
Carcinoma of the stomach is a common cause of
death in men. Pernicious anaemia, gastric polyps
and chronic gastric ulcers are known to be pre-
malignant conditions, but the majority of gastric
ulcers arise spontaneously. Helicobacter pylorides is
an important predisposing factor.
History
Age
The incidence of gastric carcinoma reaches its
peak between 50 and 70 years but can arise at an
earlier age.
Sex
Gastric cancer is two to three times more com-
mon in men than in women.
Geography
There are unexplained variations in the
incidence of this disease. It is very common in Japan,
closely followed by Chile, Austria and Finland. In the
United Kingdom, it affects approximately 20–30 per
100 000 of the population. Genetic and dietary factors
may be important, as may be the ingestion of nitrites.
Symptoms
The onset of indigestion or epigastric
pain in a patient over 40 years of age, however
vague, should be treated very seriously. The pain
may be mild and related to food but, unlike the
indigestion associated with peptic ulcer, the pain of
a gastric ulcer is constant and not solely brought on
by eating. When patients have had symptoms of a
396
Chap-15.qxd 4/19/05 14:35PM Page 396
Upper abdominal pain
397
peptic ulcer for many years, they are usually aware
that the nature of the pain has changed. Often their
periodic pain becomes constant.
Patients with stomach cancer do not want to eat,
and loss of appetite is a cardinal symptom. The
inevitable consequence of a loss of appetite is loss of
weight. The patient may lose 10–20 kg in 1 or 2
months. The loss of appetite and weight often occur
long before any other symptoms.
Tumours near the cardia may cause oesophago-
gastric junction obstruction and cause the patient
to complain of difficulty in swallowing (dysphagia).
As the dysphagia increases, undigested food may be
regurgitated from the oesophagus.
Cancers in the pyloric region often obstruct
the outflow of food from the stomach. If so, the
patient may vomit large quantities of undigested
food (undigested because of the low acid produc-
tion associated with the accompanying atrophic
gastritis) and notice epigastric discomfort and dis-
tension. Some cancers grow to a considerable size
without producing symptoms, apart from mild
weight loss.
Systematic questions
A systematic review of the other
systems may reveal symptoms that suggest that the
tumour has metastasized, such as weakness, tired-
ness or dyspnoea.
Previous history
The patient may have a long history of
peptic ulceration or have had an ulcer some years pre-
viously which was cured with medicine. Pernicious
anaemia and atrophic gastritis predispose to gastric
cancers. The patient may have been taking vitamin
B12 supplements for their anaemia.
Examination
General appearance
The most noticeable features are
wasting and pallor. The wasting is often most
apparent in the face and hands. The pallor is usually
caused by an iron deficiency anaemia that is the
result of chronic bleeding and lack of iron in the
diet. Many patients present at an advanced stage
with multiple hepatic metastases or metastases in
the lymph glands around the porta hepatis. Mild
jaundice suggests the latter.
The neck
The supraclavicular fossa must be carefully
examined, as secondary deposits in the supraclavi-
cular lymph glands are common. A palpable supra-
clavicular gland in a patient with a carcinoma of the
stomach is called Virchow’s gland and its presence
is referred to as Troisier’s sign.
The lungs
The presence of a pleural effusion suggests
pulmonary metastases.
Abdomen
Inspection. The abdomen is often scaphoid as a
consequence of weight loss but, paradoxically, there
may be generalized abdominal distension if ascites
is present. Pyloric obstruction causes epigastric dis-
tension and visible peristalsis. These physical signs
can only be seen in thin patients. In the majority the
primary tumour is too small, too high or too deep
to be seen.
Palpation. In the majority of patients, the only
physical sign is epigastric tenderness. Deep palpa-
tion on full inspiration may reveal an epigastric
mass. In a thin patient with advanced disease, there
may be a hard, irregular, dull epigastric mass which
moves with respiration. The liver may be palpable
and its edge and surface knobbly and irregular. The
epigastrium may be distended and there may be a
succussion splash if there is pyloric obstruction.
Percussion. Shifting dullness may be present if
there is an associated ascites.
Auscultation. The bowel sounds should be normal.
Rectal examination
Metastatic nodules may be felt
in the pelvis and in the ovaries (Krukenberg’s
tumours).
FIG 15.8
Some cancers of the stomach may present as a
palpable mass in the epigastrium, but the majority are
impalpable.
Chap-15.qxd 4/19/05 14:35PM Page 397
The abdomen
398
Lymphoma of the stomach
Lymphoma presents with symptoms and signs
similar to those of a carcinoma of the stomach –
vague epigastric pain and weight loss. It may arise in
middle-aged patients.
Acute cholecystitis
Acute inflammation of the gallbladder is commonly
caused by obstruction of the cystic duct by a small
stone causing gallbladder distension, chemical inflam-
mation of its wall and, eventually, secondary infection.
History
Age
Patients are commonly 30 to 60 years of age
and female. Younger patients with sickle-cell disease
often form pigment stones, which may precipitate
an attack of acute cholecystitis.
Sex
Acute cholecystitis is more common in women
than in men.
Symptoms
The main symptom is a sudden pain,
often without any previous symptoms of chronic
indigestion. It is felt in the right hypochondrium
and often radiates through to the back close to
the tip of the right scapula. The pain is continuous,
lasting more than 6 hours, and is exacerbated by
moving and breathing. Nothing except analgesic
drugs brings relief. Some patients recognize the pain
as a severe version of their chronic indigestion pain
but, as stated above, it often occurs de novo. Patients
nearly always feel nauseated and often vomit. If
there is an associated obstructive jaundice, the urine
may be dark, the stools pale and the skin itchy.
Previous history
There may be a history of flatulent
dyspepsia or previous attacks of gallstone colic.
Examination
General appearance
The patient is distressed by the
pain and lies quietly, breathing shallowly. There is
usually a tachycardia and pyrexia, although in the
early stages of the attack the temperature is often
normal. Jaundice may be present (see Chapter 8)
and the patient may be sweating.
Abdomen
Inspection. There may be a fullness in the right
hypochondrium in the early stages of the inflam-
mation (Zackary Cope’s sign).
Palpation. There is almost always tenderness and
guarding in the right hypochondrium. Palpate the
abdomen just below the tip of the ninth costal cartil-
age and ask the patient to take a deep breath. When
the liver and the attached gallbladder descend and
strike the palpating hand, the patient will experi-
ence a sharp pain which prevents further inspir-
ation. This is called Murphy’s sign.
At an early stage before there is any guarding, an
enlarged gallbladder may be palpable. At a later stage
when the inflammation has been present for several
days and the tenderness is beginning to subside, an
inflammatory mass may become palpable. This will
still be very tender and moves little with respiration.
It usually indicates that there is an abscess in the
gallbladder (an empyema).
Occasionally, the contents of an obstructed gall-
bladder do not become infected, and a large muco-
cele may develop. This may reach down to the level
of the umbilicus.
Because gallbladder pain often radiates through
to the tip of the scapula, the affected dermatome
may be hyperaesthetic, a change detected by lightly
drawing a pin down the back of the patient’s chest.
This is called Boas’ sign.
Percussion. An inflammatory mass may be detected
when guarding prevents deep palpation, by finding
a dull area just beneath the costal margin.
Auscultation. The bowel sounds are normally
present unless the gallbladder has infarcted or rup-
tured and caused biliary peritonitis. This complica-
tion is rare.
Gallstone colic/biliary colic
There is an overlap between gallstone colic and
acute cholecystitis. Gallstone colic is a severe pain
caused by spasm of the gallbladder as it tries to force
a gallstone down the cystic duct, which is why ‘gall-
stone colic’ is a preferable term to ‘biliary colic’. About
a fifth of patients who present in this way become
jaundiced. Many cases of gallstone colic progress to
acute cholecystitis.
History
Symptoms
Gallstone colic begins suddenly across the
upper abdomen. Patients are often unable to indi-
cate which side is more affected. The pain is severe
and constant with excruciating exacerbations. It is
Chap-15.qxd 4/19/05 14:35PM Page 398
Upper abdominal pain
not a true colic because it does not remit between
exacerbations. The severe pain seldom lasts longer
than a few hours unless acute cholecystitis develops.
It is usually accompanied by nausea and vomiting
and is only relieved by strong analgesia.
Previous history
Many patients give a history of flatu-
lent dyspepsia and previous episodes of upper
abdominal pain.
Examination
General appearance
The patient is frightened and
becomes restless as a consequence of the intensity of
the pain. A mild tachycardia is often present in the
early stages, but the temperature is usually normal.
Jaundice may be detected.
Abdomen
The abdomen is often extremely tender,
with intense guarding in the upper abdomen.
Chronic cholecystitis
Chronic or recurrent infection in the gallbladder
is almost always associated with gallstones. The
combination of stones and infection may present
various clinical pictures: indigestion, flatulent
dyspepsia (chronic cholecystitis), acute pain (acute
cholecystitis), gallstone colic, obstructive jaundice
and, less commonly, ascending cholangitis, acute pan-
creatitis and intestinal obstruction. Most of these
complications are associated with abdominal pain.
History
Age
Gallstones can form at any age. The majority
of patients with symptoms are between 30 and 60
years old, but a number of women between the ages
of 15 and 25 develop gallstones. Younger patients
with sickle-cell disease develop pigment stones.
Sex
Gallstones are far more common in women
than in men.
Ethnic group
North American Indians are particu-
larly liable to develop gallstones.
Symptoms
The common complaint is of an upper
abdominal indigestion-like pain after eating. The
pain normally begins gradually, 15 to 30 minutes
after a meal, and lasts for 30 to 90 minutes. When it
becomes severe, it tends to move over into the right
hypochondrium and may radiate through to the
back. It is not relieved by anything except analgesic
drugs. The patients often notice that the pain is worse
after eating a fatty meal, such as bacon and eggs or
fish and chips. The attacks of pain are irregular, last-
ing for weeks or months, with pain-free intervals of
varying length. There is often post-prandial belch-
ing, hence the description flatulent dyspepsia. The
patient’s appetite remains good and their weight
steady, or increases. Nausea and vomiting can occur
during acute exacerbations.
Previous history
Apart from previous episodes of dys-
pepsia, the patient may have been jaundiced or
noticed their stools were pale, offensive and floated
on the water in the lavatory pan.
Examination
General appearance
Medical students believe that
almost every patient with gallstones is female, fair,
fat, fertile and forty. Many are, but enough are male,
thin, dark and of any age to make one pay scant
attention to the ‘five Fs’ as an aid to diagnosis. The
skin or sclera may show signs of jaundice, indicating
that there may be stones in the common bile duct.
Abdomen
Inspection. The abdomen usually looks normal.
Palpation. The patient is tender in the right
hypochondrium just below the tip of the ninth rib, the
point where the edge of the rectus abdominis muscle
crosses the costal margin. It may be necessary to pal-
pate deeply behind the costal margin as the patient
takes a deep breath to detect mild tenderness or a
small mass. A mass present in the right hypochon-
drium suggests that a stone is obstructing the cystic
duct and that a mucocele or empyema is developing.
Percussion, ausculation and rectal examination.
These should be normal.
Acute pancreatitis
Acute pancreatitis is a condition in which activated
pancreatic enzymes autodigest the pancreatic gland.
It may be caused by obstruction of the pancreatic
duct, usually by a small gallstone obstructing the
ampulla of Vater or, a peri-ampullary carcinoma or
alcohol abuse. The mechanism by which alcohol
abuse causes pancreatitis is not known.
399
Chap-15.qxd 4/19/05 14:35PM Page 399
The abdomen
400
Viral infections, trauma and a number of rarer
conditions may also cause acute pancreatitis. In
about one third of cases, a cause is never discovered.
Pancreatitis can vary from a very mild inflamma-
tion to an acute haemorrhagic destruction of the
whole gland – a condition with a high mortality.
History
Age and sex
Pancreatitis is equally common in men
and women. The peak incidence is in the fourth and
fifth decades of life, but it can occur at any age.
Symptoms
The common presenting symptom is pain
which begins suddenly, high in the epigastrium,
and steadily increases in severity until it is very
severe, causing the patient to lie still and breathe
shallowly. It usually radiates through to the back.
Nothing relieves the pain, which is exacerbated by
movement. Frequent vomiting and retching are very
common and are an important pointer to the cor-
rect diagnosis. There is persistent nausea between the
bouts of vomiting. Many patients have eaten an
unusually large meal or drunk some alcohol before
the pain began.
In severe cases the patient may complain of
muscle twitching and cramps.
Previous history
In Great Britain, nearly half the
patients who present with acute pancreatitis have
biliary tract disease. Many patients therefore have a
previous history of indigestion.
Social history
A careful history of the patient’s alco-
hol intake is important. Relatives may have to be
interviewed, as many alcoholics refuse to reveal the
true extent of their drinking habits. Mumps is a very
rare cause of pancreatitis, but ask about any recent
contacts with children or the disease.
Examination
General appearance
Patients lie still because the pain
is severe and, if they are pale and sweating, it is
likely that they have become hypovolaemic. When
respiration is impaired, they become grey, appre-
hensive, dyspnoeic and cyanosed. The sclera may
reveal a slight tinge of jaundice if the pancreatitis
has been caused by a stone lodged in the lower end
of the bile duct. Mild jaundice may also appear
on the second or third day of the illness if oedema
in the head of the pancreas is causing compression
of the bile duct. There is usually a tachycardia and,
if the patient has become hypovolaemic, the jugular
venous pressure and blood pressure may be low.
Pyrexia may be present, but the temperature is rarely
greatly elevated.
Abdomen
Inspection. There is always tenderness and guard-
ing in the upper abdomen but the signs may be mild.
Any patient with severe pain but minimal abdom-
inal signs may have acute pancreatitis.
If the pain is severe and the tone of the abdom-
inal muscles is increased, the abdomen will not move
with respiration. A paralytic ileus may develop,
causing mild abdominal distension.
Bruising and discoloration in the left flank (Grey
Turner’s sign) and around the umbilicus (Cullen’s
sign) only develop in patients with very severe haem-
orrhagic pancreatitis. These are rare and late signs,
and indicate extensive destruction of the gland.
Remember that they may also occur after a large
intraperitoneal or retroperitoneal haemorrhage from
another cause, such as a leaking abdominal aortic
aneurysm.
A number of patients develop a collection of
inflammatory exudate in the lesser sac. This is ini-
tially suggested by fullness in the epigastrium, which
may become a more prominent mass if a pseudocyst
or abscess develops.
Percussion. Percussion may cause pain if there is
peritonitis and be dull over any pseudocysts that are
developing.
Auscultation. Bowel sounds are usually present in
the first 12 to 24 hours but fade away if a paralytic
ileus develops.
Note. Acute pancreatitis can be extremely diffi-
cult to diagnose and, as it has no distinctive features,
is often forgotten and missed. Whenever you exam-
ine an acute abdomen and cannot find a obvious
cause, think ‘Could this be pancreatitis?’ – ‘Or a
mesenteric vascular infarction?’ Or a leaking abdom-
inal aortic aneurysm?’
Chronic pancreatitis
Chronic pancreatitis progressively destroys the
exocrine and endocrine tissues of the pancreatic
gland.
Chap-15.qxd 4/19/05 14:35PM Page 400
Central abdominal pain
History
Age and sex
Many patients are middle aged and 80 per
cent are men. It is a rare condition, affecting between
3 and 10 patients per million in Western countries.
Symptoms
Patients complain of severe, recurrent
episodes of upper abdominal pain which usually
radiates through to the back. The pain is a gnawing,
dull, persistent ache. The pattern and periodicity of
the attacks vary greatly, but they are often related to
episodes of excessive alcohol drinking. The condi-
tion can develop after multiple attacks of acute
pancreatitis (acute relapsing pancreatitis) but more
often develops de novo in patients who subject
themselves to chronic alcohol abuse.
Weight loss and nausea are common. Diabetes,
steatorrhoea and jaundice develop in about 10 per
cent of affected patients.
Drug addiction is common, as long-term opiate
analgesics are often required to relieve the persist-
ent, intolerably severe pain.
Examination
There are often few physical signs. Patients often
look distraught and dishevelled. Weight loss and
jaundice may be apparent. A mass (a pseudocyst)
may be palpable in the epigastrium. The diagnosis
ultimately relies on special tests.
Chronic pancreatitis can cause thrombosis of the
portal vein, in which case the signs of portal hyper-
tension will be present.
Carcinoma of the pancreas is an important dif-
ferential diagnosis (see below).
Carcinoma of the pancreas
Eighty-five per cent of pancreatic cancers arise in
the head of the pancreas. Although many present
with jaundice and weight loss, abdominal pain is
the presenting symptom in more than half and
occurs at some stage in over 90 per cent.
The pain is usually a continuous, dull, boring
pain, felt in the epigastrium and radiating through
to the back. It is often worse at night and may be
relieved by sitting forward.
Radiation of the pain to the right hypochondrium
is common with tumours of the head of the pancreas,
while radiation to the left hypochondrium indicates
an infiltrating tumour of the tail of the gland.
Jaundice develops in almost 90 per cent of
patients at some stage of the disease and is charac-
teristically progressive but rarely painless. Pale stools,
dark urine and skin itching indicate obstructive
jaundice. Weight loss is almost universal.
Steatorrhoea, epigastric bloating, flatulence,
diarrhoea, vomiting and constipation may all occur
in between 20 and 30 per cent of patients.
Ten per cent of patients present with thrombo-
phlebitis migrans (see Chapter 7, page 207).
Examination
Obstructive jaundice, a palpable gallbladder and an
enlarged liver indicate a carcinoma of the head of
the pancreas, but in the early stages, physical signs
are rarely present. Carcinomata of the tail or body
of the pancreas often present late with the symp-
toms and signs of distant metastases.
LIVER METASTASES/TUMOURS
Distension of the liver capsule stimulates pain fibres.
Liver metastases are a common complication of all
intra-abdominal malignancies. A constant dull ache
in the right hypochondrium, general malaise, weight
loss and sometimes mild jaundice may be the first
indication of their presence.
Patients with liver cirrhosis who develop a
hepatoma often complain of epigastric or right
hypochondrial pain. A hepatoma should be sus-
pected when severe pain and weight loss develop in
a patient who is known to have cirrhosis.
SPLENOMEGALY
The causes of splenomegaly are given on page 422.
A large spleen can cause dull, persistent left hypo-
chondrial pain. Splenic infarction, which is often
associated with sickle-cell disease, causes a more
severe pain which may be exacerbated by deep res-
piration.
CENTRAL ABDOMINAL PAIN – ACUTE
AND/OR CHRONIC
Acute Meckel’s diverticulitis
Meckel’s diverticulum is the remnant of the vittelo-
intestinal duct. It contains all layers of the bowel
401
Chap-15.qxd 4/19/05 14:35PM Page 401
The abdomen
402
Occasionally it causes severe colicky, cramping
pains which must be differentiated from the colic of
small bowel obstructions caused by diseases such as
Crohn’s disease (see below), Yersinia infections (see
below) or acute appendicitis.
There are usually few signs on abdominal exam-
ination.
The stool should be cultured to exclude Campy-
lobacter, Giardia, ova and parasites, particularly if
the patient has recently travelled to foreign lands.
Inflammatory bowel disease
Crohn’s disease and ulcerative colitis may present
with acute or chronic central abdominal pain together
with a variety of other gastrointestinal symptoms.
Acute Crohn’s disease may present with central or
right iliac fossa symptoms and signs similar to those
of appendicitis. A thick and tender terminal ileum
may be palpable in the right iliac fossa, and thickened
ileum and jejunum palpable in the umbilical region.
Acute fulminating ulcerative colitis may pres-
ent as acute abdominal pain, especially when com-
plicated by acute toxic dilatation or perforation of
the colon. The abdominal pain is invariably pre-
ceded by severe incessant diarrhoea accompanied
by the passage of blood, mucus and pus.
Acute Yersinia ileitis
This condition is indistinguishable from acute
Crohn’s disease and appendicitis on the history and
physical signs. A mass is rarely palpable. It is usually
incorrectly diagnosed as acute appendicitis.
Typhoid
Typhoid normally presents with toxaemia and diar-
rhoea, but if a typhoid ulcer in the small bowel
perforates, severe abdominal pain and all the signs
of peritonitis will be present.
Tuberculosis
Intra-abdominal tuberculosis is relatively rare in
Western countries but is still quite common in India
and Africa, where it may be associated with the
increasing incidence of acquired immunodeficiency
syndrome (AIDS). Ileocaecal tuberculosis may cause
Revision panel 15.6
The causes of acute central abdominal pain
Meckel’s diverticulitis
Acute gastroenteritis
Inflammatory bowel disease
Acute Crohn’s disease
Acute ulcerative colitis
Yersinia ileitis
Typhoid
Tuberculosis
Urinary tract infection
Revision panel 15.7
The causes of chronic central abdominal pain
Crohn’s disease
Tuberculosis
Radiation bowel damage
Tumours of the small bowel
Recurrent adhesive obstruction/malrotation
Ischaemia of the small bowel
Endometriosis
wall, occurs in about 2 per cent of the population
and causes abdominal pain if it becomes inflamed.
Inflammation of a Meckel’s diverticulum pro-
duces symptoms and signs that are indistinguishable
from those of acute appendicitis, although the pain
and tenderness are generally felt more towards the
centre of the abdomen than in the right iliac fossa.
It may give rise to central abdominal pain if
any ectopic gastric or pancreatic mucosa within it
becomes ulcerated or inflamed.
It may also cause colicky abdominal pain if it acts
as the head of an intussusception or if a congenital
band arising from its apex causes small bowel
obstruction or a volvulus.
Acute gastroenteritis
Gastroenteritis is usually caused by a Campylobacter
or virus infection, but must be differentiated from
food poisoning. The symptoms of vomiting and
diarrhoea usually predominate over the abdominal
pain, which may be non-existent or very mild.
Chap-15.qxd 4/19/05 14:35PM Page 402
General abdominal pain
403
colicky or continuous central abdominal pain, often
associated with abdominal distension and weight loss.
There may be a mass of matted glands in the right
iliac fossa, a dough-like feeling to the abdomen,
ascites or signs of chronic intestinal obstruction
together with evidence of tuberculous infection at
other sites such as the lungs or cervical lymph glands.
Urinary tract infection (cystitis and
pyelonephritis)
The symptoms and signs of urinary tract infections
are discussed in Chapter 16. Pain from pyelonephri-
tis is felt mainly in the lumbar region but may
spread to the centre of the abdomen. When patients
are asked to describe the site of their renal pain they
usually put their hands on their waist with their
thumbs pointing forwards and their fingers spread
backwards between the twelfth rib and the iliac crest.
It is easier to detect tenderness in the renal angle if
the patient is sitting up and leaning slightly forwards.
Deep abdominal palpation is essential to ensure
that there is not an enlarged kidney affected by
another pathology responsible for the infection, such
as a hydronephrosis. The bladder may be enlarged
and should be palpated and percussed. Examination
of the external genitalia and a rectal examination
are essential (see Chapters 13 and 17). The urine
should be examined for red and white cells and
organisms. The presence of red cells in the urine
suggests that the pain is more likely to be coming
from a calculus or a tumour than an infection.
GENERAL ABDOMINAL PAIN –
ACUTE AND/OR CHRONIC
Patients often find it difficult to distinguish between
a central and a generalized abdominal pain. The sep-
aration of the conditions described below from
those described above is therefore somewhat arbi-
trary and rarely clinically relevant.
Irritable bowel syndrome
The irritable bowel syndrome is a functional disor-
der of the bowel of unknown aetiology which causes
chronic intermittent abdominal pain that may be
associated with changes in bowel habit and abdom-
inal distension. Combinations of these symptoms
occur in at least 10 per cent of the population, sug-
gesting the possibility that the syndrome is simply a
variant of normality. Many aetiological factors have
been proposed, including the quantity of fibre in
the diet, food allergies, disorders of bowel motility,
abnormalities of visceral autonomic nerve percep-
tion, psychological disorders and social and behav-
ioural problems.
The diagnosis is based solely on the history, as
there are no physical signs except for an indefinite,
ill-localized abdominal sensitivity on palpation.
It is important to exclude all other causes of
abdominal pain, so enquire about any symptoms or
signs that might indicate the presence of organic
disease such as anaemia, bleeding, weight loss, fever
or a change in bowel habit.
Revision panel 15.8
The causes of generalized abdominal pain
Irritable bowel syndrome
Recurrent adhesive obstruction
Mesenteric ischaemia
Carcinomatosis
Chronic constipation
Radiation damage
Retroperitoneal tumours
Endometriosis
Pelvi-ureteric junction obstruction
Lumbar spine pain
Retroperitoneal fibrosis
Psychosomatic
FIG 15.9
Pain from the kidney is felt in the renal angle, which
is between the 12th rib and the edge of the erector spinae
muscle.
Chap-15.qxd 4/19/05 14:35PM Page 403
The abdomen
404
The following symptoms suggest the diagnosis of
irritable bowel syndrome:
■
continuous or recurrent abdominal pain or
discomfort for at least 3 months – relieved by
defaecation and/or
■
a change in the frequency of defaecation and/or
■
a change in the consistence of the stool.
These symptoms are diagnostic when present-
ing together with two or more of the following
complaints:
■
an altered frequency of defaecation
■
an altered stool consistence
■
problems with defaecation
(straining/incomplete evacuation)
■
bloated feelings of abdominal distension
■
the passage of mucus.
Recurrent adhesive obstruction
Adhesive obstruction is suggested when the signs
and symptoms of small bowel obstruction develop
in a patient with an abdominal scar. Congenital
bands and internal herniae may also cause recurrent
episodes of small bowel obstruction.
Adhesive obstruction is a difficult diagnosis to
make and is often applied incorrectly to any patient
who experiences pain after abdominal surgery. The
diagnosis can only be made with certainty when the
obstruction becomes acute and laparotomy confirms
the presence of adhesions obstructing the bowel.
Tumours of the small bowel
Small bowel tumours are rare and often found
incidentally at autopsy. They present late with
unexplained small bowel obstruction. Adenomata
which occur in association with familial polyposis
and Gardiner’s syndrome may cause intussusception
and acute small bowel obstruction. Lipomata and
hamartomata can also arise in the small bowel.
The latter are known to occur in the Peutz–Jeghers
syndrome.
Carcinoid tumours are common in the appen-
dix, where they are usually benign, but they can also
arise in the small bowel, where they are more likely
to be malignant.
Lymphomata can occur anywhere in the intes-
tine but quite commonly arise in the small intestine.
Adenocarcinomata of the small bowel are
extremely rare.
All these rare tumours can present with chronic
sub-acute small bowel obstruction causing a central
colicky abdominal pain, weight loss and a change in
bowel habit. Acute obstruction may develop and a
mass may be palpable.
Mesenteric ischaemia
Infarction of the bowel caused by a sudden mesen-
teric artery occlusion causes acute abdominal pain.
Less acute occlusions of the mesenteric vessels
may cause chronic central or general abdominal
pain. This pain is often brought on by eating and is
called intestinal angina. It begins insidiously with
umbilical epigastric cramping pains, vomiting and
diarrhoea, which lead to ‘food fear’, anorexia and
weight loss.
The patient is usually a middle-aged male
smoker with other signs of arterial disease such as
intermittent claudication, angina or a previous
myocardial infarction. An abdominal bruit from
a stenosed mesenteric artery may be the only
detectable physical sign but is often not present.
Chronic mesenteric ischaemia should be considered
in all patients with unexplained abdominal pain
associated with severe weight loss.
The vasculitides such as systemic lupus erythe-
matosus and conditions such as sickle-cell disease can
also cause acute and chronic abdominal pain which
is thought to be related to mesenteric ischaemia.
Mesenteric venous thrombosis can complicate
abdominal trauma, portal vein thrombosis, splenec-
tomy and other causes of a hypercoagulable state.
Radiation damage
Both the small and large bowel can be damaged
by the external beam radiation used to treat pelvic
malignancies such as cancer of the uterus, cervix
and bladder. Most patients develop transient diar-
rhoea at the time of the radiation, but some present
months or years later, when fibrosis and strictures
form, with colicky or continuous pain, vomiting,
weight loss, constipation or diarrhoea. Eventually,
the endarteritis in the small mesenteric vessels,
caused by the irradiation, may lead to ischaemia,
necrosis and perforation of the bowel. Radiation
Chap-15.qxd 4/19/05 14:35PM Page 404
Lower abdominal pain
405
bowel injury must be differentiated from a recur-
rence of the primary tumour and/or widespread
metastatic spread throughout the abdominal cavity
(see below).
Carcinomatosis
Patients with extensive ‘seedling’ metastases through-
out the peritoneal cavity may develop a non-specific
aching abdominal pain which they find difficult to
describe and which may be associated with few
physical signs. Eventually, clinical ascites, abdom-
inal masses, evidence of tumour at other sites and
generalized weight loss and cachexia make the diag-
nosis obvious. In the early stages, the nebulous
nature of the pain and the lack of physical signs can
lead the physician to give, mistakenly, calming reas-
surance or make an incorrect diagnosis of irritable
bowel syndrome.
Retroperitoneal fibrosis
Retroperitoneal fibrosis not only obstructs the
ureters, but may also involve the abdominal aorta
and inferior vena cava. It often causes a vague cen-
tral, persistent abdominal pain. The kidneys may be
enlarged by a hydronephrosis or there may be a ten-
der abdominal aneurysm. If the fibrosis obstructs
the vena cava, the patient may present with the
symptoms of an acute deep vein thrombosis or
oedema of the lower limbs (see Chapter 7).
Endometriosis
This is a condition in which ectopic endometrial tis-
sue is present in sites in the abdomen other than the
uterus, such as the large and small bowel and the
lining of the abdominal cavity. It causes abdominal
pain at the time of menstruation.
Lumbar spine disorders
Pain caused by abnormalities in the spine may radi-
ate from the back to the front of the abdomen and
cause diagnostic difficulties. Any suggestion that an
abdominal pain is affected by movement and posi-
tion should indicate the possibility that the pain is
arising in the back. This can sometimes be con-
firmed by careful examination of the spine.
Constipation
Severe chronic constipation may cause a rather
indeterminate abdominal pain and general abdom-
inal distension. In these cases there are hard faeces in
the rectum and palpable, indentable masses in the
abdomen.
Psychosomatic pain
This is a dangerous diagnosis to make, especially
knowing how difficult it is to recognize the pain of
widespread intra-abdominal malignancy. There are,
however, some patients with profound psycho-
logical disturbances, severe anxiety or ‘cancer phobia’
who persistently present with abdominal pain for
which no cause can be found.
Beware of adopting the ‘cry wolf ’ attitude. Each
new episode of pain requires an open-minded new
history and examination.
LOWER ABDOMINAL PAIN – ACUTE
AND/OR CHRONIC – CAUSED BY
INFLAMMATORY AND/OR MALIGNANT
CONDITIONS
Acute appendicitis
Acute appendicitis is the commonest cause of acute
abdominal pain in the Western world. The cause of
appendicitis remains unknown, but obstruction of
the lumen by a faecolith, swollen Peyer’s patches,
a stricture or a carcinoid tumour at its base all play
Revision panel 15.9
The causes of acute and chronic lower
abdominal pain
Appendicitis
Crohn’s disease
Carcinoma of the caecum and right colon
Diverticular disease
Carcinoma of the left colon/rectum
Bladder outflow obstruction
Interstitial/irradiation cystitis
Pelvic inflammatory disease
Chap-15.qxd 4/19/05 14:35PM Page 405
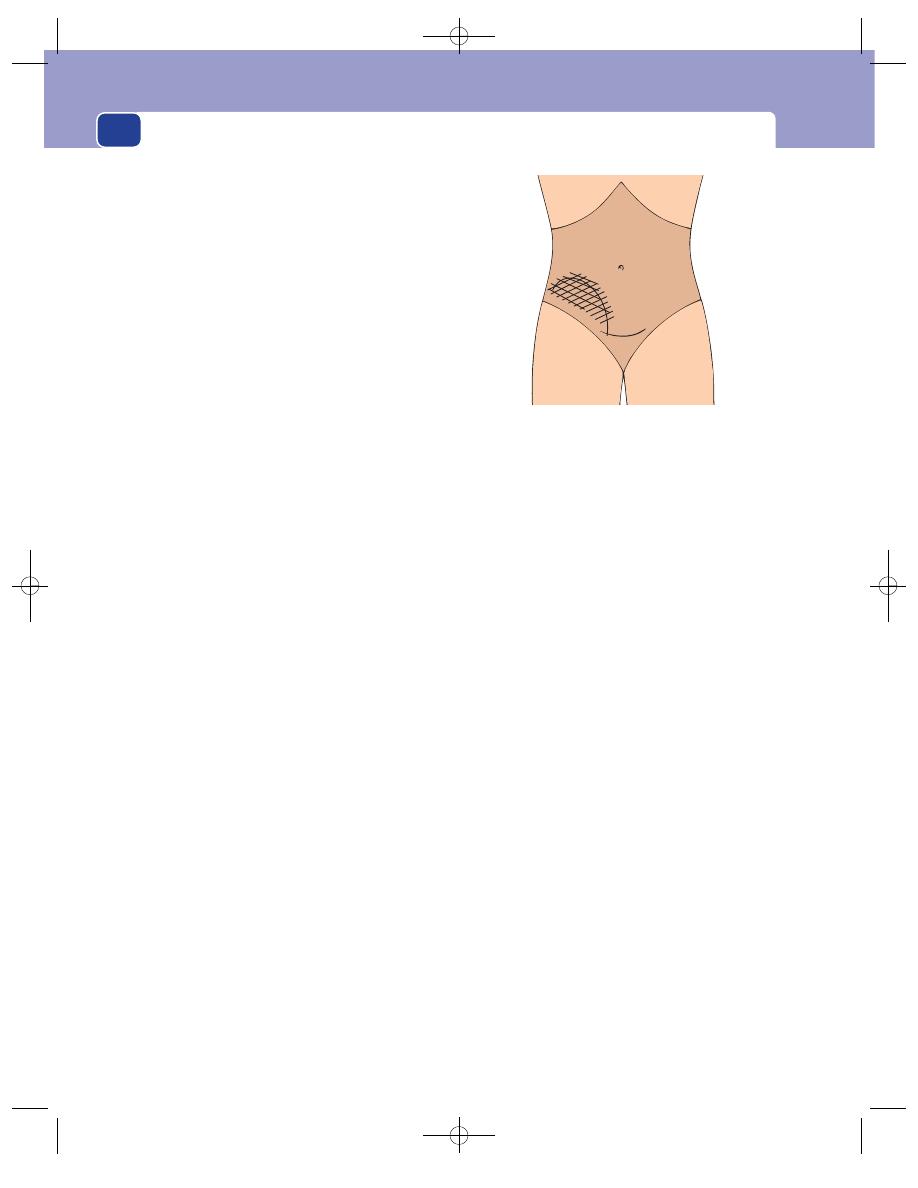
The abdomen
a part. Threadworms, which are often found in the
appendix, may be an aetiological factor, as may diet
and childhood infections.
History
Age and sex
Appendicitis can and does occur at any
age, but most often affects young adults or teenagers
of either sex.
Symptoms
The condition most often presents with a
vague pain which begins in the centre of the
abdomen. At first this is often thought to be indi-
gestion and ignored, but after a varying period, usu-
ally a few hours but sometime 2–3 days, the pain
shifts to the right iliac fossa and becomes more
severe. This ‘typical’ history is almost diagnostic of
appendicitis but only occurs in about half the
patients.
The remainder present with a variety of patterns
of pain. It may begin and remain in the right iliac
fossa or only be felt in the centre of the abdomen.
There may be pain in both sites simultaneously, and
a few patients have no pain at all.
The central pain is a referred pain. The normal
visceral innervation of the appendix comes from
the tenth thoracic spinal segment. The correspond-
ing somatic dermatome encircles the abdomen at
the level of the umbilicus. The mid-line pain is
higher if the spinal segment visceral innervation is
higher. Some patients have retrosternal pain which
shifts to the right iliac fossa. Therefore, the import-
ant feature of the initial pain is its central location
and not its precise level.
The inflamed appendix most commonly lies
behind the caecum (retrocaecal) and so causes pain
in the lateral part of the right iliac fossa and the
flank, but it may hang down into the pelvis and lie
against the bladder or a loop of large bowel. Under
these circumstances, the patient may present with
misleading bladder or large bowel symptoms.
Acute appendicitis may also present with intestinal
obstruction – colic and abdominal distension – if
the appendix lies too close to and inflames the ter-
minal ileum (pre-ileal or post-ileal).
A loss of appetite usually precedes the onset of
pain by a few hours and most patients feel slightly
nauseated. Many patients vomit once or twice. Most
patients with appendicitis state that they have been
constipated for a few days before the pain started,
but a few complain of diarrhoea, which may lead to
a mistaken diagnosis of gastroenteritis, especially in
children.
Some patients present with symptoms of general-
ized peritonitis – generalized abdominal pain, nau-
sea and vomiting, sweating and sometimes rigors –
especially if the initial stages of the disease are silent.
Atypical presentations are common in the very
young, in pregnant women and in the very old,
when the appendicitis may be related to obstruction
of its ostium by a carcinoma of the caecum.
Examination
General appearance
Patients often look unwell with
flushed cheeks. A low-grade pyrexia is usually pres-
ent, but a high temperature should suggest another
cause for the pain, or general peritonitis associated
with a ruptured appendix. The pulse rate is usually
elevated and rises as the infection spreads.
Head and neck
The tongue is usually furred and most
patients have a distinctive foetor oris. Palpable
lymph glands in the neck and enlarged tonsils indi-
cate that the patient may have mesenteric adenitis
rather than appendicitis, but beware – acute appen-
dicitis often follows a viral infection.
Chest
The lungs should be normal but be sure to
exclude any signs of a right-sided basal pneumonia,
because this can occasionally cause abdominal pain
and mimic appendicitis, especially in children.
406
FIG 15.10
An appendix mass or abscess. The continuous line
indicates the edge of the mass; the hatching is the area of
tenderness.
Chap-15.qxd 4/19/05 14:35PM Page 406
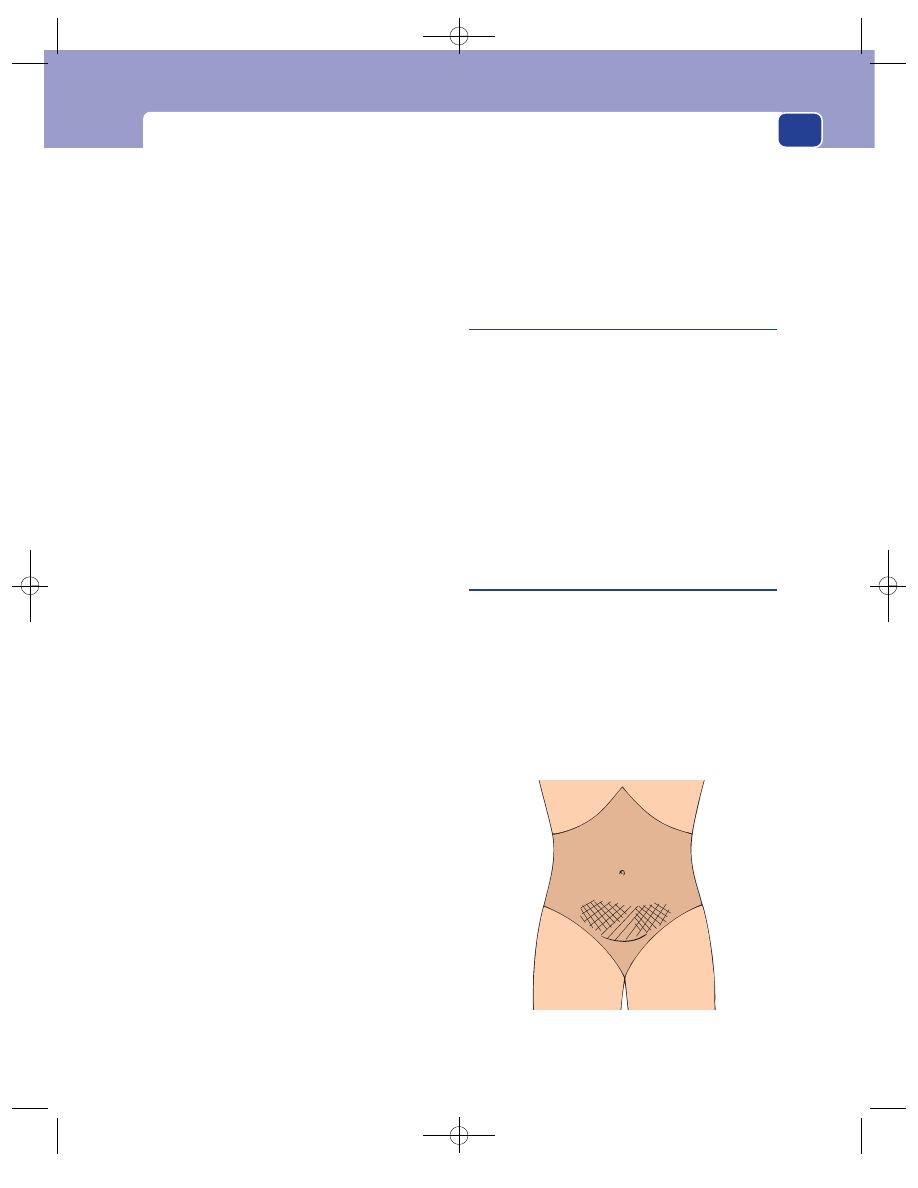
Lower abdominal pain
Abdomen
Inspection. The abdomen, though it may be
slightly distended, usually looks normal. The right
hip may be kept slightly flexed if the appendix is
lying against the psoas major muscle. Coughing and
sudden movements cause pain if peritonitis has
developed.
Palpation. The right iliac fossa is tender and the
overlying muscles guard. The maximum site of
tenderness must be carefully assessed by gentle
palpation. It is classically maximal over McBurney’s
point, but high or low tenderness may indicate that
the appendix is lying in an unusual position. There
may be release or rebound tenderness in the right
iliac fossa. Pressure on the left iliac fossa may cause
pain in the right (Rovsing’s sign). Release of pressure
on the left iliac fossa may cause pain on the right. All
these manoeuvres cause pain because they move the
inflamed appendix as it lies in the right iliac fossa
against the overlying peritoneum, which contains
many somatic pain fibres.
When the appendix is behind the caecum, the
tenderness may be experienced in the lateral part of
the lumbar region – the flank.
When a sub-hepatic appendix produces pain
and tenderness below the right costal margin, it
must be differentiated from acute cholecystitis (see
below).
A tender, indistinct mass may be felt in the right
iliac fossa. It is usually impossible to feel below it
because it is fixed posteriorly. It is dull to percus-
sion. An appendix mass usually takes a few days to
develop. An appendix abscess should be suspected
if the temperature is high and the mass very tender.
The features of an appendix mass and abscess are
described on pages 427–8.
Percussion. This causes pain if peritonitis is pres-
ent. Dullness on percussion may suggest the pres-
ence of an underlying mass that is obscured by
tenderness and guarding.
Auscultation. Bowel sounds are present unless
perforation and general peritonitis have caused a
paralytic ileus.
Rectal examination
There is considerable debate about
the usefulness of this examination, especially in
young children, but the presence of tenderness high
in the pelvis usually indicates an inflamed pelvic
appendix.
Hip movement
Extension of the right hip joint will
exacerbate the pain if the appendix is in a retro-
caecal position lying against the psoas muscle. Pain
on external and internal rotation of the hip indi-
cates that the appendix is lying against the obdura-
tor internis muscle.
‘Chronic’ appendicitis
Two forms of chronic inflammation may develop in
the appendix: the mucocele and the empyema. Both
follow an attack of acute inflammation and both
may cause recurrent pain in the right iliac fossa which
is sometimes colicky in nature. Worms and faecol-
iths may produce similar symptoms.
Recurrent episodes of mild acute infection, com-
monly classified as a ‘grumbling’ appendix, are
extremely rare. Do not make that diagnosis; look for
another cause for the patient’s pain.
Acute salpingitis/pelvic inflammatory
disease
Acute salpingitis is an infection in one or both
Fallopian tubes, but it is often associated with infec-
tion within the surrounding supporting tissues
around the adnexae – hence the term pelvic inflam-
matory disease. The common infecting organisms
are Gonococcus and Streptococcus. These organisms
usually reach the Fallopian tubes by direct spread
through the vagina and uterus, rarely from the
407
FIG 15.11
The areas of tenderness associated with
salpingitis.
Chap-15.qxd 4/19/05 14:35PM Page 407
The abdomen
408
bloodstream. Salpingitis is a well-recognized com-
plication of the puerperium and following abortion.
History
Age and sex
Salpingitis usually occurs in sexually
active women between the ages of 15 and 50 years.
Symptoms
A purulent, yellow-white vaginal dis-
charge usually precedes, by a few days, the gradual
onset of lower abdominal pain. The pain is con-
stant and can become severe. It may radiate to the
lower part of the back. Sometimes the abdominal
pain is preceded by a low backache. Menstruation
may have been irregular over the previous months
and patients often give a history of dysmenorrhoea.
Sweating and rigors are common, but there is usu-
ally no nausea, vomiting or change in bowel habit.
By contrast, urinary tract symptoms, such as painful
and frequent micturition, are common as the urin-
ary tract is often also infected.
Previous history
Patients may have had previous attacks
of infection or know that they have had or been
exposed to gonorrhoea.
Examination
General appearance
The patient looks flushed and
feverish. There is no distinctive foetor oris and the
oral temperature is often higher than in appen-
dicitis, being between 38 and 39.5°C.
Abdomen
Inspection. The abdomen moves normally and
looks normal.
Palpation. Tenderness and some guarding are
present across the lower abdomen. The tenderness
is often bilateral as both Fallopian tubes may be
infected, but can be asymmetrical if one tube is
more infected than the other. It is usually lower and
nearer to the mid-line than the tenderness of appen-
dicitis. A huge pyosalpinx is occasionally palpable,
but even large swollen tubes can often only be felt by
manual examination (see below).
Percussion. This seldom causes pain but may do
so if there is associated peritonitis.
Auscultation. The bowel sounds are usually
normal.
Vaginal examination
Examination of the vaginal introi-
tus may reveal a yellow-white discharge, a specimen
of which should be sent for culture. The cervix and
uterus should be normal sized, but bimanual palpa-
tion of the adnexae will cause pain, Moving the
cervix (cervical excitation) is also painful. Speculum
examination may demonstrate pus coming from
the cervical canal. If a pyosalpinx or tubo-ovarian
abscess is present, a mass may be felt to one side of
the uterus.
Chronic pelvic sepsis
A number of patients with acute pelvic inflamma-
tory disease proceed to develop lower abdominal
pain which is often related to the menstrual cycle.
Adnexal tenderness on bimanual examination in
association with a low-grade fever and a continuing
vaginal discharge indicates the diagnosis. There may
be associated urinary frequency and dysuria. Gono-
cocci and other pathogens found on a high vaginal
swab confirm the diagnosis.
Crohn’s disease
Acute Crohn’s disease presents with symptoms and
signs similar to those of appendicitis. The thickened,
tender terminal ileum may be palpable in the right
iliac fossa.
The symptom that helps distinguish acute Crohn’s
disease from appendicitis is the occurrence of
repeated episodes of diarrhoea in the weeks before
the acute attack. But Crohn’s disease usually runs
a chronic course. It generally presents with a long
history of colicky central or lower abdominal pain
coming on every 15–30 minutes, associated with
diarrhoea. Thickened segments of small bowel may
be palpable but some patients have no detectable
abdominal physical signs.
Anal complications – abscesses and fistulae – are
common (see Chapter 17).
The patient may show other stigmata of a chronic
inflammatory disease such as finger clubbing, ery-
thema nodosum, sacro-iliitis, episcleritis, pyoderma
gangrenosum, anal sepsis, sclerosing cholangitis, gall-
stones and renal stones. Fistulae of some description –
abdominal and anal – are present in 15 per cent of
patients, and anaemia and hypoproteinaemia are
also common.
Chap-15.qxd 4/19/05 14:35PM Page 408
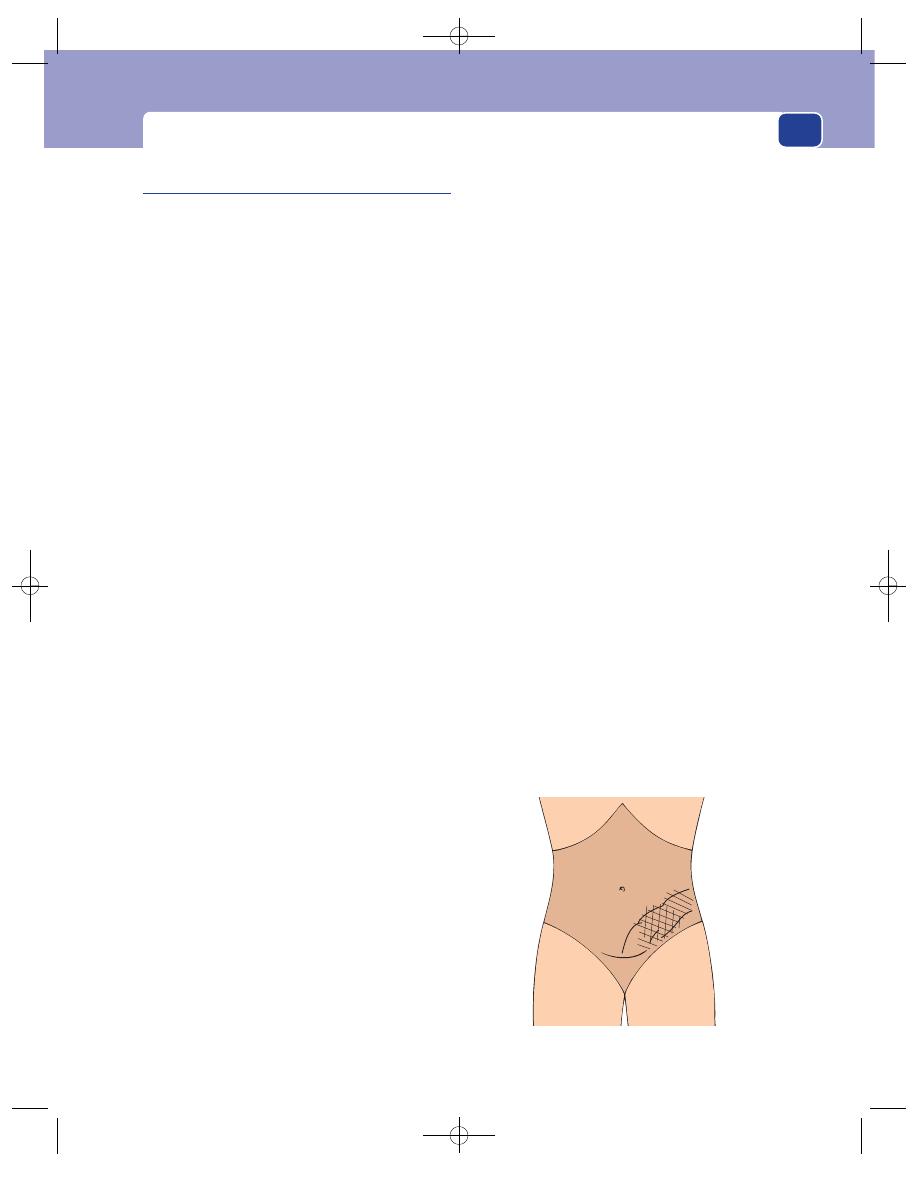
Lower abdominal pain
Acute diverticulitis of the colon
Acquired diverticula develop in the colon, especially
the sigmoid colon, probably as a result of changes
in bowel motility and the consistence of the faeces.
The condition may be related to the low roughage
diet popular in the USA and Europe. Diverticula
often cause no symptoms but they may become
obstructed and acutely inflamed – acute diverticuli-
tis. This may progress to a pericolic abscess situated
on the outside of the colon, which may then perfor-
ate causing generalized peritonitis (see below).
If a solitary diverticulum of the caecum becomes
inflamed, the signs are indistinguishable from
those of acute appendicitis or a carcinoma of the
colon.
History
Age, sex and ethnic group
Patients with divericulitis
are commonly between the ages of 50 and 70 years.
The condition is slightly more common in women
than in men. Native Africans and Asians are rarely
affected.
Symptoms
The first symptom is often a mild inter-
mittent lower abdominal pain which then shifts to
the left iliac fossa (for the same reasons as appen-
dicitis moves to the right), where it becomes a more
constant ache. The pain begins gradually before
becoming more severe and constant. It may become
colicky if the large bowel becomes obstructed. The
pain is often associated with nausea and a loss of
appetite, but rarely vomiting. Most patients are con-
stipated but a few develop diarrhoea. If the colon
lies against the vault of the bladder and the bladder
wall becomes inflamed, there may be increased fre-
quency of and painful micturition. Some patients
can relate their attacks to the type of food they have
eaten.
Previous history
Some patients give a history of chronic
diverticular disease, flatulence, distension and left
iliac fossa pain.
Examination
General appearance
Patients lie still because of the
pain and often look flushed. They are usually pyrex-
ial and have a tachycardia.
Abdomen
Inspection. The abdomen moves with respira-
tion. If there is a generalized peritonitis or intestinal
obstruction, the abdomen may be distended.
Palpation. There is tenderness and guarding in
the left iliac fossa, where there may be a palpable,
tender, sausage-shaped mass. Pressure on the right
side of the abdomen may induce pain on the left
(reversed Rovsing’s sign). Rebound tenderness will
be present if generalized peritonitis has developed.
In the latter stages of peritonitis or obstruction,
there may be considerable abdominal distension.
Percussion. Any palpable mass in the left iliac
fossa should be dull to percussion.
Auscultation. The bowel sounds may be normal,
hyperactive if there is intestinal obstruction, or
absent if a generalized peritonitis develops causing a
paralytic ileus.
Rectal examination
Pain may be experienced when
the finger is pushed high into the left side of the
pelvis. Rectal examination is important to exclude a
carcinoma of the rectosigmoid junction, which can
perforate and cause similar symptoms. Sigmoido-
scopy is indicated to exclude a carcinoma but often
causes pain when attempting to negotiate the recto-
sigmoid junction. The findings are rarely diagnostic
unless a carcinoma is seen.
Differential diagnoses
Acute diverticulitis must be dif-
ferentiated from carcinoma of the colon with a peri-
colic abscess, ischaemic colitis and occasionally
acute appendicitis or Crohn’s disease.
409
FIG 15.12
The mass and tenderness of acute diverticulitis.
Chap-15.qxd 4/19/05 14:35PM Page 409
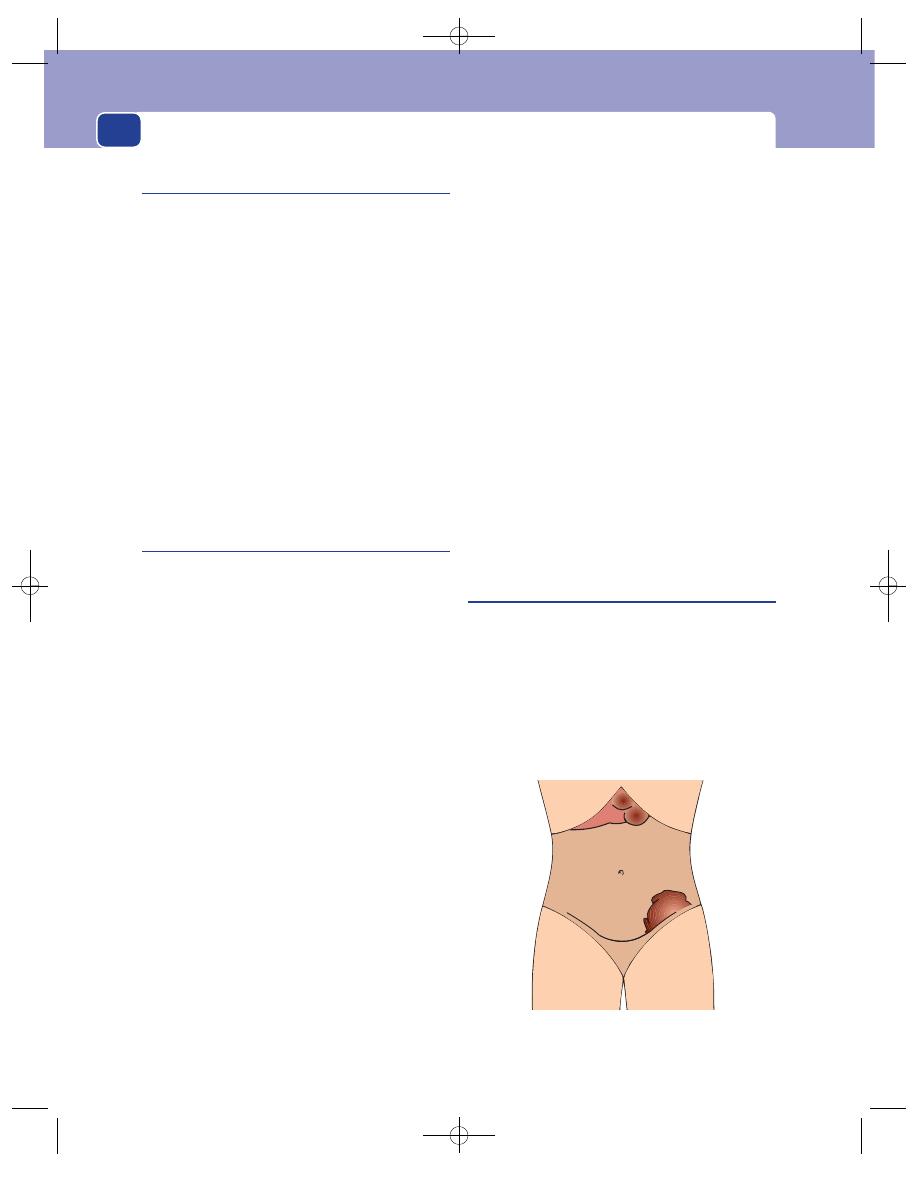
The abdomen
410
Chronic diverticular disease
Although diverticular disease may present with
acute abdominal pain or large bowel obstruction as
described above, it most commonly presents in mid-
dle-aged or elderly patients with episodes of central
or lower left-sided abdominal pain, often associated
with or preceded by constipation. The pain is dull or
colicky and there may be weeks, months or years
between attacks. The condition needs to be differen-
tiated from carcinoma of the colon, irritable bowel
syndrome and other causes of inflammatory bowel
disease. Examination of the abdomen may reveal
some tenderness in the left iliac fossa and, very occa-
sionally, a palpable mass. Rectal examination and
sigmoidoscopy are rarely helpful and the diagnosis is
made by special investigations.
Carcinoma of the caecum and
right colon
Cancer of the caecum is often silent until it has
grown to a considerable size.
History
Most right-sided colonic and caecal tumours pres-
ent with symptoms of anaemia (tiredness and
shortness of breath), weight loss and a mass. They
can also present with a dull pain in the right iliac
fossa or with the colicky pains of small bowel obstruc-
tion. Sometimes the symptoms closely mimic acute
appendicitis.
Examination
General appearance
Patients usually appear pale
and thin.
Abdomen
Inspection. The abdomen may be generally dis-
tended or full in the right iliac fossa. A mass may be
visible in a thin patient.
Palpation. The right iliac fossa is often tender,
with some guarding of the overlying muscles. A firm,
irregular mass may be felt in the right iliac fossa or
right lumbar region, which may be fixed or freely
mobile. The liver may be palpable, enlarged and
irregular.
Percussion. The mass is usually dull to percussion.
Auscultation. Bowel sounds are normal unless
obstruction or peritonitis is present.
Rectal examination
This is usually normal, as is sig-
moidoscopy, although the latter may show the pres-
ence of rectal polyps.
Occult blood may be detected in the faeces with
the appropriate test.
When a carcinaoma of the caecum causes appen-
dicitis, the physical signs are indistinguishable from
those of simple acute appendicitis. Even when a
mass is palpable, it is rarely possible to be certain
that this is not an inflammatory mass, and even if
the mass is very hard, discrete, knobbly and not very
tender, it may simply be caused by inflammation.
Consequently the possibility of a cancer of the cae-
cum must always be considered in a patient over 40
years old who presents with acute appendicitis.
Other possible diagnoses include an inflamed soli-
tary caecal diverticulum, Crohn’s disease and ileo-
caecal tuberculosis.
Cancer of the left colon
The symptoms of cancer of the left colon differ
according to the part of the colon involved. The
majority of colon cancers are found in the sigmoid
colon and at the recto-sigmoid junction, where they
are usually small, annular and ulcerated. They usu-
ally present with a change in bowel habit, often
with variable periods of constipation interspersed
FIG 15.13
The mass of a carcinoma of the sigmoid colon,
with liver metastases.
Chap-15.qxd 4/19/05 14:35PM Page 410
Symptoms and signs resulting from the perforation of a viscus
with episodes of explosive diarrhoea and the passage
of a number of loose stools.
History
Age
The majority of patients are over 50 years old,
but colon cancer can occur in young adults with
ulcerative colitis or familial polyposis.
Sex
Both sexes are equally affected.
Symptoms
Pain is a rare symptom and, when it is
present, it is usually a mild lower abdominal colic or
ache. After some weeks or months it usually becomes
a persistent pain in the left lower abdomen. Alternat-
ing constipation and diarrhoea is typical of the
annular variety of carcinoma of the left colon. The
constipation is caused by the intestinal obstruction,
and the diarrhoea by liquefaction of faeces above
the obstruction. The diarrhoea may be increased by
inflammation of the colonic mucosa and an exces-
sive secretion of mucus. The episodes of colicky
abdominal pain are accompanied by distension, but
early loss of weight and appetite is uncommon. The
weight loss often precedes the anorexia.
Thin patients may feel a lump in their abdomen.
Rectal bleeding is not a common symptom of a
tumour of the sigmoid or descending colon but,
when it occurs, the blood is dark and plum-coloured,
sometimes with clots of blood interspersed among
the faeces. When the tumour is at the recto-sigmoid
junction, it is more likely to cause bleeding and it
may prolapse into the rectum, causing tenesmus.
Painful frequent micturition indicates involvement
of the bladder.
Examination
General appearance
Weight loss may be apparent.
Abdomen
Inspection. In thin patients, there may be swelling
in the left iliac fossa. The colon, especially the cae-
cum, may be visibly distended with faeces.
Palpation. A large tumour may be palpable, often
in the left lumbar region or iliac fossa. Part of the
mass may be hard faeces above the tumour rather
than the tumour itself, in which case the mass is
indentable. The mass is tender if there is any sur-
rounding inflammation or a pericolic abscess asso-
ciated with a perforation.
The liver may be palpable with an irregular sur-
face and edge.
Percussion. A mass in the left iliac fossa will be
dull to percussion.
Auscultation. Loud, high-pitched continuous
gurglings can be heard during the attacks of colic,
but if the colon perforates, the abdomen becomes
silent and, of course, tender.
Rectal examination
A tumour in the apex of a loop of
the sigmoid colon hanging down into the pelvis may
be palpable on bimanual examination. Secondary
nodules may be felt within the pelvis and blood may
be visible on the fingerstall.
Tumours in the left side of the colon can present
with generalized peritonitis if the patient has ignored
the symptoms described above. In such cases, severe
generalized abdominal pain develops accompanied
by signs of shock with tachycardia, hypotension, dis-
tension, tenderness, loss of liver dullness and absent
bowel sounds. In many cases the peritonitis is caused
by a rupture of a distended caecum, not a rupture at
the site of the cancer.
SYMPTOMS AND SIGNS RESULTING
FROM THE PERFORATION OF A VISCUS
A perforation in the wall of a hollow viscus allows
its contents – acid, bacteria, small bowel contents,
faeces, bile or urine – to enter into the peritoneal
cavity, where they rapidly cause a chemical or
infected peritonitis. The history and physical signs
often indicate the site and cause of the perforation,
but whether they do or do not, it is usually necessary
to perform a laparotomy to confirm the diagnosis
and close the perforation. It is essential, therefore, to
recognize the signs of peritonitis.
Acute peritonitis
The clinical features of peritonitis are as follows.
Tenderness and guarding
The pain begins near the site of the perforation but
rapidly spreads across the whole abdomen. Guarding
is an excellent indication of the severity of the ten-
derness. If the whole abdomen is tense, there is
likely to be general peritonitis.
411
Chap-15.qxd 4/19/05 14:35PM Page 411
The abdomen
412
Rebound tenderness or tenderness on
percussion
This is just another way of detecting that the
abdomen is very tender. It can be a valuable sign
because the patient is not expecting pain when you
suddenly remove your hand, so the apprehension
which can cause guarding during direct palpation is
absent. However, it causes considerable discomfort
and should be used sparingly.
Localized pain during distant palpation
If a pain is experienced in a tender area when you
press on a distant non-tender part of the abdomen,
the structures in the painful area are likely to be very
inflamed.
Absence of bowel sounds
The absence of bowel sounds per se does not indi-
cate peritonitis, but their absence in a tender, rigid
abdomen makes it highly likely that there is general-
ized peritonitis.
An increasing tachycardia
If the pulse rate increases gradually during 1–2 hours
of observation, there is likely to be serious disease
within the abdomen.
Pyrexia
The temperature rises only when the peritoneal cav-
ity becomes heavily infected. Remember that steroids
damp down the inflammatory response. Patients on
corticosteroids with a severe peritonitis may have a
normal temperature.
When a peptic ulcer erodes through the wall
of the stomach or duodenum at a point where it is
only covered by visceral peritoneum, acid gastric
juice enters the peritoneal cavity. This causes a
chemical peritonitis, which later becomes infected
with bacteria.
Conditions likely to cause a perforation
■
Peptic ulceration (page 396)
■
Boerhaave’s syndrome (page 394)
■
Diverticulitis (page 409)
■
Carcinoma of colon (page 410)
■
Ulcerative colitis (page 402)
■
Acute cholecystitis and acute appendicitis
(pages 398 and 405)
■
A penetrating injury or rupture of the urinary
bladder
SYMPTOMS AND SIGNS CAUSED BY
AN OBSTRUCTED VISCUS
Intestinal obstruction
There are many causes of intestinal obstruction (see
Revision panel 15.12).
Although it is normally possible, on the basis
of the history aided by physical signs and plain
abdominal radiographs, to tell whether the site of
the obstruction is in the small bowel or large bowel,
the clinician must always attempt to answer these
three questions.
1. Is there intestinal obstruction?
2. Is the bowel strangulated?
3. Is the site of the obstruction in the small bowel
or large bowel?
Revision panel 15.10
The conditions likely to cause the perforation
of a viscus
Peptic ulceration
Boerhaave’s syndrome (violent vomiting)
Gangrenous appendicitis
A perforated gallbladder
Acute diverticulitis
Small bowel disease (Crohn’s disease,
strangulation, a foreign body, typhoid)
Ulcerative colitis (toxic megacolon)
Ischaemia
Radiation necrosis
Carcinoma of the colon
Ruptured bladder
Revision panel 15.11
The cardinal symptoms of intestinal obstruction
Pain
Vomiting
Distension
Absolute constipation
Chap-15.qxd 4/19/05 14:35PM Page 412
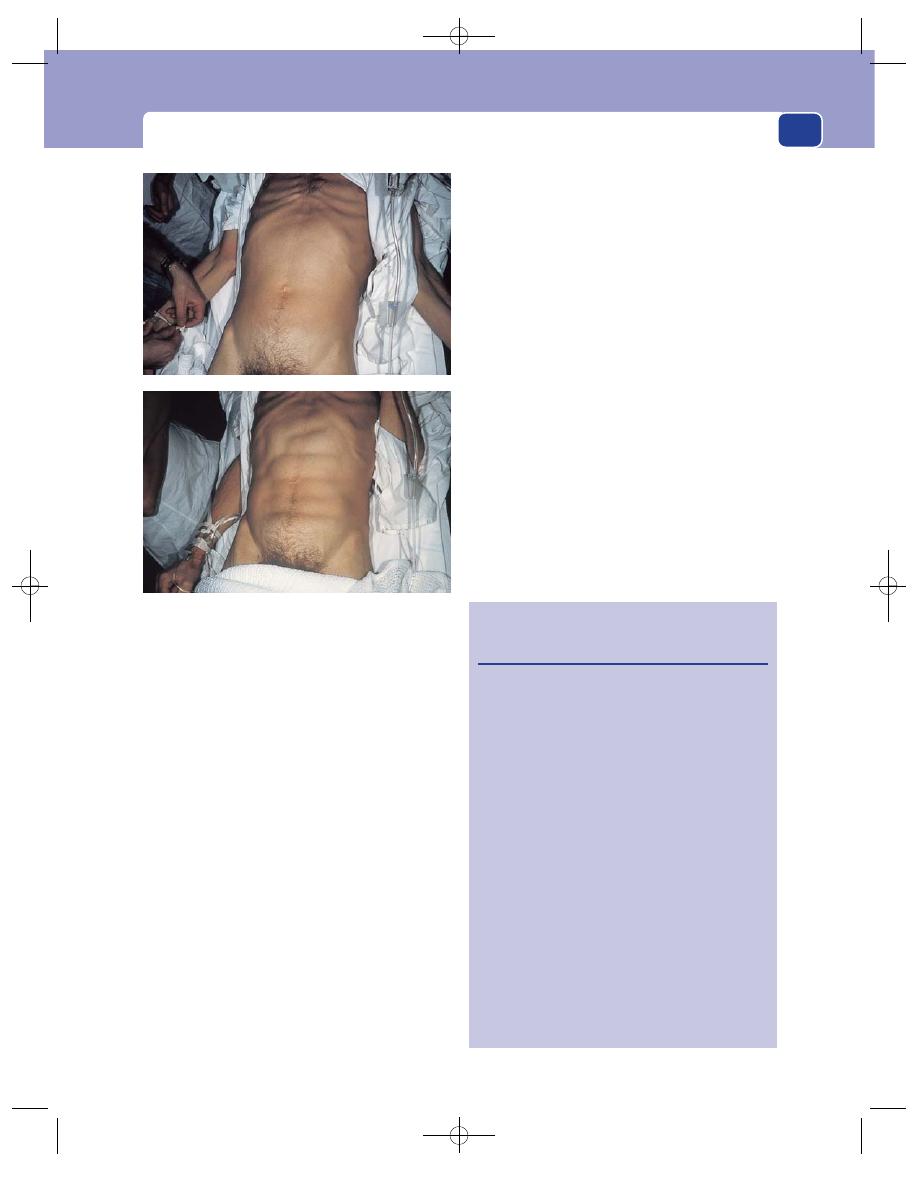
Symptoms and signs caused by an obstructed viscus
The signs of strangulation are the same as the
signs of local peritoneal inflammation, which have
been described above, namely, pain, tenderness,
guarding and rebound tenderness.
The cardinal symptoms of intestinal obstruc-
tion are pain, vomiting, distension and absolute
constipation, but the severity and time of onset of
each of these symptoms depend upon the level of
obstruction.
Pain
The pain of intestinal obstruction is true colic.
It occurs as a severe central griping pain inter-
spersed with periods of little or no pain. Colic is
uncommon with obstructions above the pylorus.
Small bowel colic is felt in the centre of the
abdomen, and large bowel colic in the lower third of
the abdomen. Small bowel colic occurs every 2–20
minutes, depending on the level of obstruction in
the small bowel. Large bowel colic occurs about
every 30 minutes or more.
Vomiting
Intestinal obstruction causes frequent vomiting. The
nature of the vomitus depends upon the level of the
obstruction. With pyloric obstruction, the vomitus is
watery and acid. High small bowel obstruction pro-
duces a greenish-blue, bile-stained vomit. Obstruc-
tion in the lower part of the small bowel is associated
with a brown vomit which becomes increasingly foul
smelling as the obstruction persists. It becomes so
thick, brown and foul that it is often called faeculent
vomit. Vomiting is unusual and usually a late symp-
tom in patients with large bowel obstruction.
Distension
The lower the site of the obstruction, the more
bowel there is available to distend. High obstruc-
tions are not associated with distension, particularly
if the patient is vomiting frequently. Obstruction
413
Revision panel 15.12
Age, and the common causes of alimentary
tract obstruction
Neonates
Atresia (duodenum, ileum)
Meconium obstruction
Volvulus neonatorum
3 weeks
Congenital hypertrophic pyloric
stenosis
6–9 months
Intussusception
Teenage
Inflammatory masses
(appendicitis)
Intussusception of Meckel’s
diverticulum or polyp
Young adult
Hernia
Adhesions
Adult
Hernia
Adhesions
Inflammation (appendicitis,
Crohn’s disease)
Carcinoma
Elderly
Carcinoma
Inflammation (diverticulitis)
Sigmoid volvulus
FIG 15.14
Visible peristalsis in a patient with a low small
bowel obstruction. Top: mild abdominal distension, surface
of abdomen smooth. Bottom: the abdomen 5 minutes
later – visible loops of peristalting small bowel.
Chap-15.qxd 4/19/05 14:35PM Page 413
The abdomen
414
of the colon causes the colon to distend around the
periphery of the abdomen. The distension then
extends into the small bowel if the ileocaecal valve is
incompetent. If this valve remains competent, the
right side of the colon, especially the caecum, can
become grossly distended, causing a visible bulge in
the right iliac fossa which is hyper-resonant. Small
bowel obstruction tends to cause distension in the
centre of the abdomen.
Absolute constipation
Once an obstruction is complete and the bowel
below is empty, absolute constipation develops. This
means that neither faeces nor flatus are passed.
This occurs early in lower large bowel obstructions
and late in high small bowel obstructions.
To summarize
A high small bowel obstruction causes frequent
colic and vomiting. The distension is slight and cen-
tral and absolute constipation is rare. A low large
bowel obstruction causes infrequent colic, absolute
constipation and peripheral abdominal distension.
Vomiting is absent or occurs very late on.
The bowel sounds in a patient with mechanical
obstruction are at first loud, frequent and obstruct-
ive in nature. As the bowel distends, the sounds
become more resonant and high pitched, before
eventually becoming amphoteric.
Strangulated herniae or adhesions are the com-
monest causes of small bowel obstruction. All the
hernial orifices must be carefully examined (see
Chapter 14).
Abdominal scars indicate the latter diagnosis.
Carcinoma, diverticulitis and volvulus are the
most common causes of large bowel obstruction.
Rectal examination and sigmoidoscopy are
essential before more detailed investigations are
carried out. It is important to remember that some
patients with large bowel obstruction have a pseudo-
obstruction (Ogilvie’s syndrome) in which large
bowel peristalsis disappears in association with
retroperitoneal pathology.
Ureteric colic
This is described in detail in the next chapter. It
presents with severe persistent pain radiating from
the loin to the groin.
Gallbladder colic
This is described on page 398.
Bladder colic
Bladder colic or retention is described in Chapter 16.
Uterine colic
This is always associated with pregnancy. The pres-
ence of a large pelvic mass should confirm the pres-
ence of a pregnant uterus.
INFARCTION OF A VISCUS CAUSING
ABDOMINAL PAIN
Revision panel 15.13 lists the abdominal organs that
may infarct and present with acute abdominal pain
together with the common pathological processes
responsible for infarction.
Acute pain develops when the blood supply of an
organ is obstructed. When the obstructing mechan-
ism is an external constriction or a torsion of a vas-
cular pedicle (e.g. a volvulus), the process is gradual
but the end result is the same – severe abdominal
Revision panel 15.13
The intra-abdominal organs that may infarct
Organ
Mechanism
Small and large bowel
Strangulation
Volvulus
Arterial thrombosis
Arterial embolism
Dissecting aneurysm
Venous thrombosis
Ovary
Torsion of pedicle
Omentum/appendix
Strangulation
epiploica
Stomach
Volvulus
Spleen/kidney/liver
Arterial occlusion
Chap-15.qxd 4/19/05 14:35PM Page 414
Abdominal pain caused by intra-abdominal or retroperitoneal haemorrhage
415
pain – as the nerve endings are damaged and die.
Pain is also experienced through the somatic nerve
endings of the peritoneal cavity if they are directly
stimulated by the proximity of the dead organ.
History
The pain of infarction is usually severe and
continuous and quickly develops all the hallmarks
of peritonitis. The patient often finds it difficult to
locate the site of the pain, which gets progressively
worse if left untreated and which is aggravated by
any movement and is only relieved by strong anal-
gesics. Vomiting may accompany the pain and most
patients are severely nauseated. Massive vomiting
and complete dysphagia occur in the few patients
who develop the rare condition of infarction of the
stomach caused by a gastric volvulus.
Some patients may describe a classical colic in
which the pain becomes continuous and much more
severe as the blood supply of an obstructed loop
is compromised by the process of strangulation.
Patients may know they have a hernia that has become
irreducible and painful, or they may provide a his-
tory of previous abdominal surgery, indicating the
possibility of adhesions as a cause of strangulation.
A history of angina, heart attacks, strokes or
intermittent claudication indicates coexisting athero-
sclerotic disease and increases the likelihood of a
mesenteric thrombosis.
Splenic infarction is common in patients with
sickle-cell disease, who may also develop bowel ischae-
mia, as may patients with autoimmune vasculitis.
Severe chest pain preceding the abdominal pain
indicates the possibility that an aortic dissection has
compromised the mesenteric vessels and led to
infarction.
Examination
General features
Patients with abdominal infarction
lie still and they are often pale and sweating from
the associated hypovolaemic shock. There is a
tachycardia, which increases during the period of
observation. An irregularly irregular pulse (atrial fib-
rillation) should suggest the possibility of a mesen-
teric embolus.
Pyrexia
The temperature may be mildly elevated at
first, but a high temperature only develops if
treatment is delayed and bowel wall putrefaction
begins to occur.
Tenderness and guarding
These signs may be mild at
first but become more pronounced as the condition
of the bowel wall deteriorates. The abdomen also
becomes more distended, and rebound or percus-
sion tenderness can be elicited.
Bowel sounds
These may be present whilst the infarc-
tion is beginning, but a major intra-abdominal infarct
always eventually causes a paralytic ileus.
The presence of an intra-abdominal bruit (see
Chapter 7) indicates the presence of atherosclerotic
disease in the intra-abdominal vessels.
The hernial orifices
These must be carefully examined
(see Chapter 14), together with all visible incisions,
and palpated for the presence of tender and irre-
ducible lumps.
Rectal examination and sigmoidoscopy
The presence of
a sigmoid volvulus is usually suspected from typical
appearances on plain abdominal radiographs, but
sigmoidoscopy may be both diagnostic and thera-
peutic in this condition. Gentle pressure of the sig-
moidoscope against a blind end of bowel, or the
passage of a flatus tube through the sigmoidoscope
usually leads to the passage of a massive flatus with
abdominal decompression and relief of pain, pro-
vided infarction has not developed.
Peripheral pulses
Absence of brachial or femoral pulses
indicates the possibility of a dissecting aneurysm,
especially in a patient whose pain began in the chest.
Summary
Infarction of the bowel must always be
considered in a patient with severe abdominal pain
and few signs. The most likely differential diagnoses
are a perforated viscus causing peritonitis, severe
acute pancreatitis, and a ruptured abdominal aortic
aneurysm.
ABDOMINAL PAIN CAUSED BY
INTRA-ABDOMINAL OR
RETROPERITONEAL HAEMORRHAGE
The common conditions that cause intra-abdominal
or retroperitoneal haemorrhage are a ruptured aortic
aneurysm, a ruptured spleen, and a ruptured ectopic
pregnancy.
Chap-15.qxd 4/19/05 14:35PM Page 415
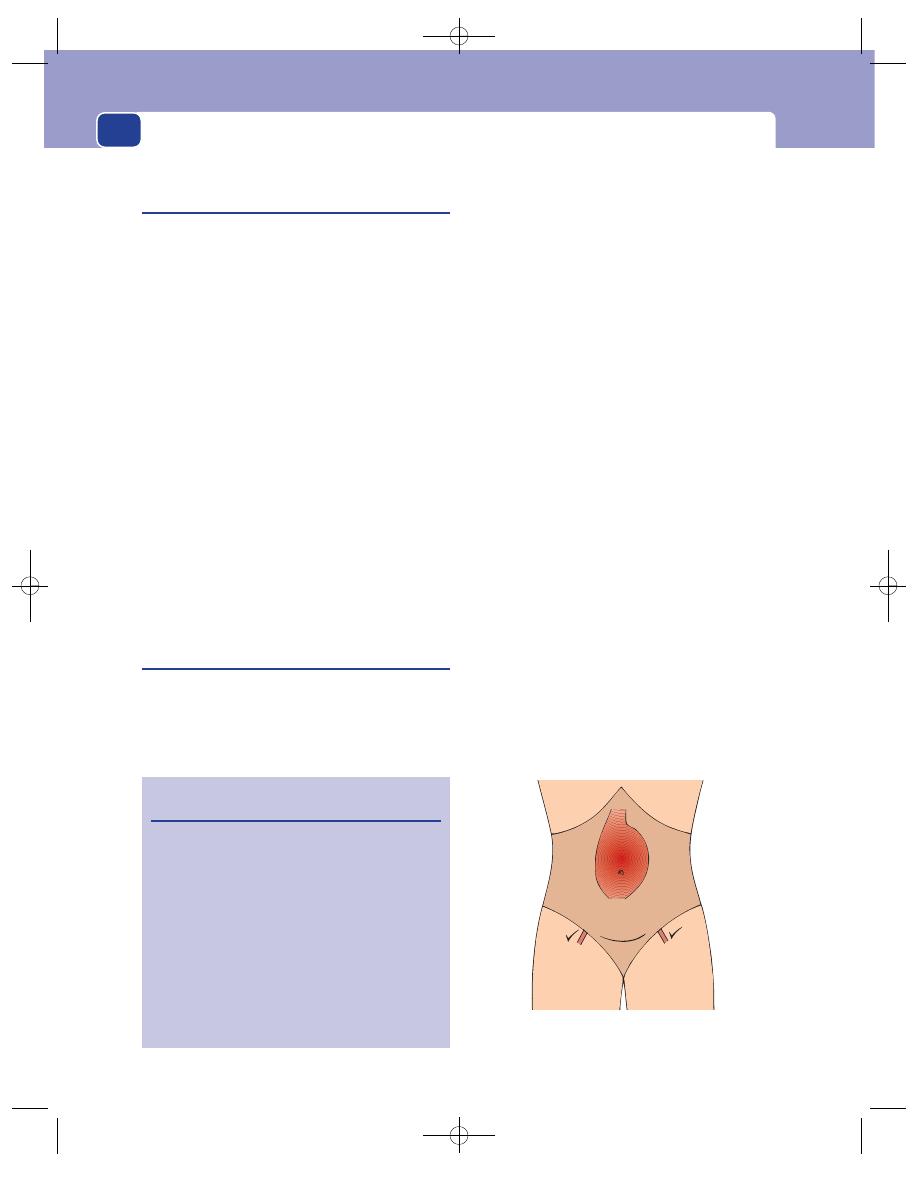
The abdomen
Common features of intra-abdominal
haemorrhage
History
The onset of pain is always rapid, but the signs of
shock and collapse may precede the pain and be the
predominating symptoms.
Although patients may die from untreated hypo-
volaemia, the accompanying hypotension some-
times reduces the bleeding, giving a false impression
of recovery but fortunately allowing time to transfer
the patient to hospital.
Examination
General appearance
The patient often looks very pale
and may be sweating, restless and breathless, a con-
dition known as ‘air hunger’. A tachycardia is invari-
ably present and this is often marked if the patient
is hypovolaemic. The blood pressure is maintained
at first, especially in fit young adults, but eventually
may fall suddenly and disastrously. The peripheral
circulation is shut down so that the extremities
of the limbs are pale and cold. The pupils may be
dilated. The jugular venous pressure is very low and
may not be visible even when the patient is lying flat.
Ruptured abdominal aortic aneurysm
History
Patients with abdominal aortic aneurysms invari-
ably are, or have been, smokers and may have a fam-
ily history of atherosclerotic aneurysms.
A previous history of angina, myocardial infarc-
tion, intermittent claudication, transient ischaemic
attacks or strokes will confirm the presence of gen-
eralized atherosclerosis.
Symptoms
The pain from a ruptured abdominal aor-
tic aneurysm begins in the centre of the abdomen
but commonly radiates to the back and may radiate
to the groin along the course of the genito-femoral
nerve.
Examination
Abdomen
Inspection. The abdomen is usually distended. If
the patient is thin, a large central pulsating mass may
be visible in the epigastrium or umbilical region.
Grey Turner’s sign and Cullen’s sign – bruising
around the umbilicus and in the flank respectively –
are late (3–4 days) indicators of a long-standing
rupture.
Palpation. The presence of an expansile pulsatile
mass may be confirmed. It is usually tender and
consists of the aneurysm and the surrounding
haematoma. The upper and lower limits of the
aneurysm should be defined. A clear separation
between the upper end of the aneurysm and the
costal margin indicates that the aneurysm is likely
to begin below the renal arteries. The finding of
additional pulsatile masses in the iliac fossae sug-
gests associated iliac aneurysms (usually in the
common iliac arteries). The femoral, iliac and foot
pulses must all be palpated. The presence of dilated
416
FIG 15.15
The site of an abdominal aortic aneurysm.
The femoral pulses are usually palpable.
Revision panel 15.14
The sources of intra-abdominal haemorrhage
Ruptured abdominal aortic aneurysm
Ruptured spleen
Ruptured ectopic pregnancy (tubal rupture)
Ruptured ovarian cyst
Haemorrhage from a liver adenoma
Ruptured visceral aneurysms
Splenic
Hepatic
Mesenteric
Torn mesentery
Retroperitoneal haemorrhage (over-
anticoagulation)
Chap-15.qxd 4/19/05 14:35PM Page 416
Abdominal pain caused by intra-abdominal or retroperitoneal haemorrhage
417
popliteal arteries strengthens the possibility that the
patient has an abdominal aneurysm. The peripheral
pulses may be absent.
Large amounts of free blood in the abdomen,
obesity, marked guarding and hypotension may all
conspire to render a leaking aneurysm impalpable.
Severe abdominal pain and collapse with clear
evidence of hypovolaemia are strongly suggestive of
a leaking aneurysm in an elderly male who is known
to be hypertensive and a smoker, but special investi-
gations may be needed to confirm the diagnosis.
Auscultation. The bowel sounds may be dimin-
ished as a consequence of the irritation caused by
intraperitoneal blood. Vascular bruits may be heard.
Rectal and vaginal examination
Rectal examination is
usually unhelpful, but occasionally an internal iliac
artery aneurysm can be palpated.
Special features of other abdominal
aneurysms
Aneurysms can arise in all the visceral arteries but
they are rare. Splenic artery aneurysms are the most
common.
Rupture of the spleen
The spleen may be ruptured by blunt or penetrating
injuries. When the spleen is ruptured by an external
injury, the left lower ribs are often fractured.
Splenic haemorrhage usually causes pain in the
left hypochondrium and upper abdomen. It may
be associated with left shoulder-tip pain if blood
or a haematoma is irritating the left hemidi-
aphragm. Shifting dullness and flank dullness may
be detected.
If the ribs are broken, there will be local pain and
tenderness and sharp pain on inspiration.
Occasionally, a ruptured pathologically enlarged
spleen is palpable in the right hypochondrium.
Abdominal trauma
Blunt and penetrating injuries can damage any of
the intra-abdominal viscera. The spleen and liver
are the most susceptible organs and both may bleed
profusely.
A history of blunt or sharp injury to the abdomen,
even if trivial, provides an important clue to the
diagnosis.
There may be signs of the external injury if the
patient has had blunt trauma to the abdomen, such
as cutaneous bruising or marks along the line of a
seat belt.
Ectopic pregnancy
When an ectopic pregnancy is the source of hae-
morrhage, the patient may know she is pregnant
(morning sickness, amenorrhoea, breast swelling or
a positive pregnancy test) and is likely to have experi-
enced some intermittent lower abdominal pain
before the sudden onset of severe pain in this area.
This is usually associated with faintness and col-
lapse, although less acute presentations are com-
mon. The lower abdominal pain becomes generalized
if left untreated.
A history of any abnormality in the menstrual
cycle in a woman of child-bearing age coupled with
the sudden onset of severe abdominal pain should
suggest the possibility of an ectopic pregnancy. A
previous history of pelvic inflammatory disease (see
above) or fertility problems also raises suspicions of
the diagnosis. If available, a rapid pregnancy test can
be very helpful.
Physiological rupture of ovarian
luteal cysts
These can cause minor episodes of bleeding and lower
abdominal pain when they rupture at the middle of
the menstrual cycle. This is called mittlesmertz.
Rupture of pathological ovarian cysts
Sometimes large pathological ovarian cysts can rup-
ture and bleed profusely. Patients may collapse from
the associated hypovolaemic shock or present with
lower abdominal pain and then develop the signs of
internal bleeding.
Rupture of liver adenomata
Liver adenomata can develop in young women taking
the contraceptive pill and may rupture spontaneously.
Chap-15.qxd 4/19/05 14:35PM Page 417
The abdomen
The pain is usually felt in the upper abdomen and
hypovolaemic collapse is common.
Summary
All the conditions described above present
with a combination of abdominal pain and haemor-
rhagic shock in varying proportions. Their presen-
tation needs to be distinguished from the symptoms
of intra-abdominal infarction and peritonitis caused
by a perforated viscus and acute pancreatitis, all of
which can produce a similar clinical picture.
EXTRA-ABDOMINAL AND MEDICAL
CONDITIONS CAUSING ACUTE
ABDOMINAL PAIN
The conditions described below are not unusual
causes of abdominal pain, a fact which emphasizes
the need to conduct a full clinical examination on
every patient however obvious it may seem that
their problem is in the abdomen.
The chest and heart must be examined and spe-
cial tests must be performed, such as chest X-ray and
electrocardiography (ECG), especially when there
are no or minimal signs in the abdomen.
The pain of spinal abnormalities can radiate to the
abdomen, so the back should be examined carefully,
especially if the pain is felt in the lumbar region.
Acute porphyria
This is associated with severe intestinal colic which
is particularly precipitated by barbiturates and alco-
hol. The urine is often dark and turns red/purple on
standing.
Mesenteric adenitis
This is associated with an upper respiratory tract
infection and cervical lymphadenopathy. It can
cause pain in the right iliac fossa which may be mis-
taken for appendicitis. The pain is caused by swollen
glands in the mesentery, so the area of tenderness
may move when the patient moves from side to side.
Infectious hepatitis/glandular fever
These conditions cause pain in the right hypochon-
drium. The pain is caused by swelling of the liver
stretching the liver capsule. Jaundice usually develops
within a few days.
Curtis–Fitz-Hugh’s syndrome
The pain of this syndrome is caused by a pericap-
sulitis around the liver that is related to pelvic
inflammation with Chlamydia. A preceding vaginal
discharge suggests the diagnosis, which has to be
differentiated from acute cholecystitis.
Herpes zoster
This causes pain in the abdomen if an appropriate
dermatome is involved. The diagnosis is only con-
firmed when the characteristic rash develops.
Diabetic keto-acidosis
This can cause marked abdominal pain. The diag-
nosis is confirmed by finding glycosuria and ele-
vated blood glucose levels. Patients are often very
thirsty and drowsy.
Syphilis
Syphilis can cause abdominal pain during a tabetic
crisis, but tertiary syphilis is uncommon nowadays.
418
Revision panel 15.15
Extra-abdominal and medical conditions
causing acute abdominal pain
Pneumonia/pleurisy
Pulmonary infarction
Acute Coxsackie infection (Bornholm’s
disease)
Myocardial infarction
Spinal disorders, e.g. prolapsed disc
Inferior epigastric artery haematoma
Acute porphyria
Mesenteric adenitis
Infectious hepatitis
Curtis–Fitz-Hugh’s syndrome
Herpes zoster
Diabetic keto-acidosis
Syphilis (lightening pains)
Henoch Schoenlein purpura
Acquired immunodeficiency syndrome (AIDS)
Collagen disease
Sickle-cell disease
Non-specific abdominal pain
Munchausen’s syndrome
Chap-15.qxd 4/19/05 14:35PM Page 418
Alimentary conditions presenting with dysphagia or vomiting
419
Argyll Robertson pupils and evidence of destruc-
tion of the dorsal columns of the spinal cord caus-
ing loss of deep pain and proprioception indicate
the diagnosis.
Henoch–Schönlein purpura
Purpura can present with intestinal colic. The diag-
nosis should be suspected in children who have a
purpuric rash over their thighs and buttocks.
Acquired immunodeficiency syndrome
Patients with AIDS have an increasing risk of
developing abdominal lymphomata which may
perforate or obstruct. Because of the compromised
state of their immune system, appendicitis and other
intra-abdominal infections can have a fulminating
course.
Collagen diseases
A number of collagen diseases, especially systemic
lupus erythematosus, can be associated with abdom-
inal pain and are associated with an increased risk
of intestinal infarction secondary to small vessel
obstruction.
Sickle-cell crisis
This can cause abdominal pain, usually from intes-
tinal and splenic infarction.
Non-specific abdominal pain
In some patients, no cause for acute abdominal
pain can be found, despite hospital admission, re-
examination and special investigations. These patients
are categorized as having non-specific abdominal
pain and represent a fair proportion of the many
patients admitted with abdominal pain as acute surgi-
cal emergencies. In the great majority, the pain disap-
pears spontaneously and does not recur. In some,
however, the cause eventually becomes apparent.
Munchausen’s syndrome
A very small group of patients with Munchausen’s
syndrome invent abdominal pain for their own
bizarre reasons. Many of these patients are psychi-
atrically disturbed. Some are attention seekers and
some are drug addicts who bluff their way into
being prescribed opiates. Beware the patient who
has come from many miles away, or even a different
country, whose abdomen bears the scars of many
incisions, especially if the pain is difficult to con-
trol and requires increasing quantities of analgesic
drugs. The physical signs are often minimal, but
some of these patients are very good at mimicking
guarding and rebound tenderness. A phone call to a
hospital that the patient claims to have previously
visited reveals either that the patient has never been
there or that the hospital also suspected the diagno-
sis of Munchausen’s syndrome.
ALIMENTARY CONDITIONS
PRESENTING WITH DYSPHAGIA
OR VOMITING
Some serious alimentary diseases do not cause
abdominal pain but do affect swallowing and may
cause retrosternal pain.
Revision panel 15.16
The causes of haematemesis and melaena
Chronic peptic ulceration (spontaneous,
steroids)
Acute gastric erosions (aspirin, phenyl-butazone,
steroids, trauma – especially burns)
Carcinoma of the stomach
Oesophageal varices
Purpura
Haemophilia
Revision panel 15.17
The causes of abdominal pain that are often
forgotten
Pancreatitis
Aneurysms (leaking or dissecting)
Mesenteric ischaemia
Herpes zoster (shingles)
Porphyria
Diabetes
Tabes dorsalis
Sickle-cell disease
Pneumonia
Chap-15.qxd 4/19/05 14:35PM Page 419
The abdomen
420
Carcinoma of the oesophagus
Carcinoma of the oesophagus rarely produces any
early physical signs apart from wasting and some-
times palpable supraclavicular lymph glands. The
diagnosis is suspected when the patient complains
of dysphagia. At first, large pieces of food stick, but
ultimately fluids cannot be swallowed.
Reflux oesophagitis
This causes a retrosternal burning sensation,
described by the patient as heartburn. Patients may
also develop dysphagia. Apart from the nature of the
pain, the clue to the diagnosis of reflux oesophagitis is
its relationship to posture. Bending, stooping, heavy
lifting and tight clothes all force acid up into the
oesophagus and cause heartburn. It is often worse at
night if the patient slips off their pillow. This is often
the only symptom of a hiatus hernia.
Pyloric stenosis
Pyloric stenosis occurs in neonates with congenital
hypertrophic pyloric stenosis and in adults with
cicatrizing peptic ulceration of their pylorus or
duodenum, or carcinoma of the antrum of the
stomach. The last two conditions may be associated
with symptoms of benign peptic ulceration or car-
cinoma of the stomach (see pages 395 and 396).
Neonates with congenital hypertrophic pyloric
stenosis present, when 2–6 weeks old, vomiting large
quantities of curdled and unpleasant-smelling milk.
The vomit is forcefully ejected, justifying the adjec-
tive projectile. The child becomes thin and dehy-
drated but retains its appetite. Careful abdominal
examination shortly after a feed may reveal a smooth
ovoid mass just below the right costal margin, some-
times called a pyloric ‘tumour’. This is the hyper-
trophied pylorus and is a diagnostic physical sign.
Adults with pyloric stenosis present with vomit-
ing. The vomit is usually large in volume, not bile
stained and, when the condition is long-standing,
not acidic because the chronic gastric retention
causes achlorhydria. The stomach contents are,
therefore, not digested and the patient may notice
that their vomit contains food that was eaten 24 or
48 hours previously. Epigastric distension, visible
gastric peristalsis and a succussion splash may be
present.
CONDITIONS PRESENTING WITH
DIARRHOEA
Some diseases of the large bowel cause diarrhoea
without any other symptoms. The nature of the
diarrhoea sometimes suggests the diagnosis, but
proof usually rests on the results of flexible sigmoid-
oscopy, biopsy, colonoscopy, barium enema and
stool cultures.
Infections of the gastrointestinal tract
Infections from food, such as typhoid and staphylo-
coccal toxins, are called food poisoning. The stools
are watery brown and passed with great frequency.
Abdominal colic is common and may be associated
with nausea, vomiting and thirst.
In tropical countries the most likely causes of
diarrhoea are bacillary dysentery, amoebic dysen-
tery, malaria, kala-azar and schistosomiasis.
Cholera presents with vomiting, cramps and
severe diarrhoea. The diarrhoea lasts up to 3 or 4
days. The patient passes colourless, opaque stools
(known as rice-water stools), which consist of an
inflammatory exudate, mucus, flakes of epithelium,
the casts of villi and the infecting organism.
Typhoid may also present as a surgical problem
with abdominal pain from the perforation of ulcers
in the small bowel.
Ulcerative colitis and Crohn’s disease
Patients with ulcerative colitis and Crohn’s disease
develop chronic frequent diarrhoea often associated
with diffuse intermittent abdominal pain. Sometimes
they pass a watery brown fluid, while at other times
they just pass mucus containing dark or red flecks of
blood or altered blood. Patients may have 20–30
bowel actions a day.
The presence of colicky abdominal pain suggests
Crohn’s disease.
Persistent pain may be the result of acute toxic
dilatation of the colon, especially if this is compli-
cated by perforation. The patient is then dehydrated,
thin, ill and feverish, with signs of abdominal disten-
sion and acute peritonitis, i.e. tenderness and guard-
ing with a loss of liver dullness and an absence of
bowel sounds.
Chap-15.qxd 4/19/05 14:35PM Page 420
The abdominal mass: causes and signs
421
Carcinoma of the colon and rectum
Most carcinomata of the left-hand side of the
colon cause a change in bowel habit which may be
associated with pain and bleeding, but persistent
copious diarrhoea is not a prominent feature.
A villous papilloma is a benign/malignant rectal
tumour which causes excessive mucus secretion.
Patients frequently pass stools of pure mucus. This
may cause dehydration and the loss of large quanti-
ties of sodium and potassium.
Spurious diarrhoea occurs when a very consti-
pated patient passes loose, watery stools around a
mass of faeces impacted in the rectum. Diagnosis is
by rectal examination.
Steatorrhea, the passage of pale, frothy and
offensive stools laden with fat, which float in the pan,
occurs in patients with inadequate fat digestion,
often a consequence of pancreatic or biliary disease.
THE ABDOMINAL MASS: CAUSES
AND SIGNS
The techniques for palpating the liver, spleen and
kidneys are described on page 389.
Hepatomegaly
The causes of enlargement of the liver, classified
according to their clinical presentation, are listed
below.
Smooth generalized enlargement, without
jaundice
■
Congestion from heart failure
■
Cirrhosis
■
Lymphoma
■
Hepatic vein obstruction (Budd–Chiari
syndrome)
■
Amyloid disease
■
Kala-azar
■
Gaucher’s disease
Smooth generalized enlargement, with
jaundice
■
Infective hepatitis
■
Biliary tract obstruction (gallstones,
carcinoma of pancreas)
■
Cholangitis
■
Portal pyaemia
Knobbly generalized enlargement,
without jaundice
■
Metastatic deposits
■
Cirrhosis
■
Polycystic disease
■
Primary liver carcinoma (hepatocellular and
cholangiocarcinoma)
Knobbly generalized enlargement,
with jaundice
■
Metastatic deposits
■
Cirrhosis
Localized swellings
■
Riedel’s lobe
■
Secondary carcinoma
Revision panel 15.18
Causes of hepatomegaly
Infection
Congestion
Bile duct obstruction
Cellular infiltration
Cellular proliferation
Space-occupying lesions
FIG 15.16
Hepatomegaly. The dotted line indicates the site
of Riedel’s lobe – a normal anatomical variation.
Chap-15.qxd 4/19/05 14:35PM Page 421
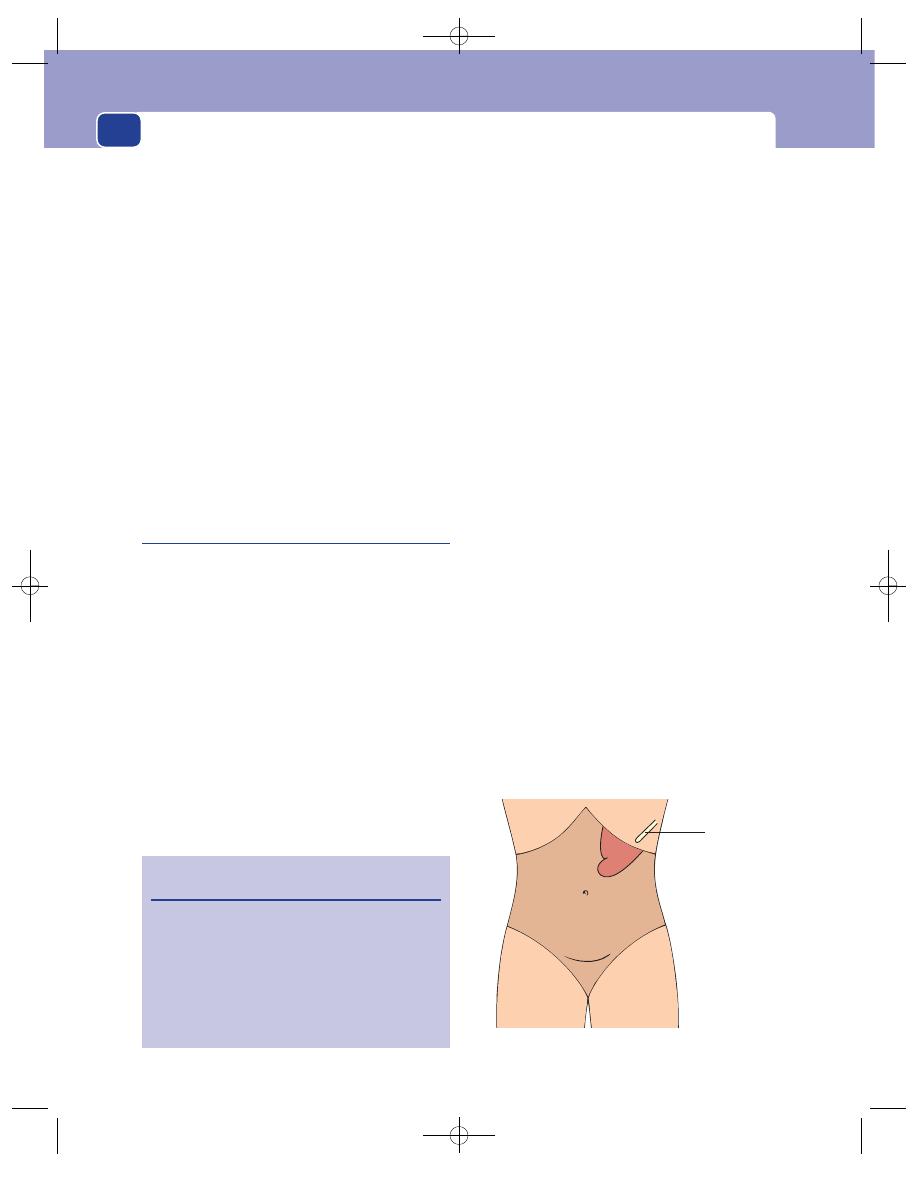
The abdomen
422
■
Hydatid cyst
■
Liver abscess
■
Primary liver carcinoma
■
Benign liver adenoma
The physical signs of an enlarged liver are:
1. it descends below the right costal margin,
2. you cannot feel its upper limit,
3. it moves with respiration,
4. it is dull to percussion up to the level of the
eighth rib in the mid-axillary line,
5. it may have a sharp or rounded edge with
a smooth or irregular surface.
Remember Riedel’s lobe. This is an extension of
the right lobe of the liver below the costal margin,
along the anterior axillary line. It is often mistaken for
a pathological enlargement of the liver or a gallblad-
der. It is a normal anatomical variation.
Splenomegaly
The spleen is almost always uniformly enlarged. The
causes of splenomegaly are classified according to
the underlying disease.
Infection
Bacterial
■
Typhoid
■
Typhus
■
Tuberculosis
■
Brucellosis
■
General septicaemia
Viral
■
Glandular fever
■
Epstein–Barr virus
Spirochaetal
■
Syphilis
■
Leptospirosis (Weil’s disease)
Protozoal
■
Malaria
■
Kala-azar
■
Schistosomiasis
Cellular proliferation
■
Myeloid and lymphatic leukaemia
■
Lymphoma
■
Pernicious anaemia
■
Polycythaemia rubra vera
■
Spherocytosis and other haemolytic anaemias,
e.g. sickle-cell disease, thalassaemia
■
Thrombocytopenic purpura
■
Myelofibrosis
■
Sarcoidosis
Congestion
■
Portal hypertension (cirrhosis, portal vein
thrombosis)
■
Hepatic vein obstruction
■
Congestive heart failure
Infarction and injury
■
Emboli from bacterial endocarditis, emboli
from the left atrium during atrial fibrillation
associated with mitral stenosis, emboli from
the left ventricle after myocardial infarction
■
Splenic artery or vein thrombosis caused by
polycythaemia or sickle-cell disease
■
Haematoma
Revision panel 15.19
Causes of splenomegaly
Infection
Cellular proliferation
Congestion
Infarction
Cellular infiltration
Collagen diseases
Space-occupying lesions
10th rib
FIG 15.17
Splenomegaly. The notch is not always palpable.
Chap-15.qxd 4/19/05 14:35PM Page 422
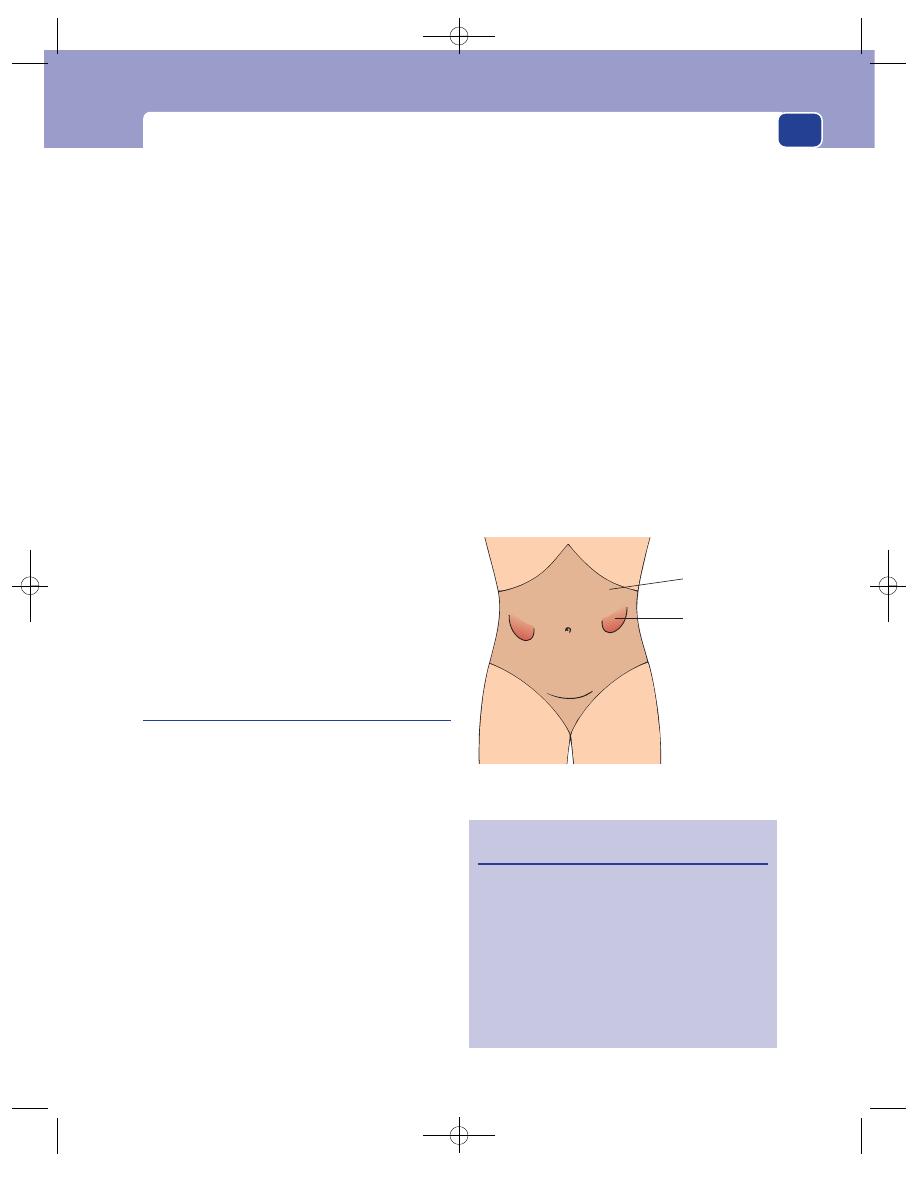
The abdominal mass: causes and signs
423
Cellular infiltration
■
Amyloidosis
■
Gaucher’s disease
Collagen diseases
■
Felty’s syndrome
■
Still’s disease
Space-occupying lesions
■
True solitary cysts
■
Polycystic disease
■
Hydatid cysts
■
Angioma
■
Lymphoma and lymphosarcoma
■
Secondary tumour (very rare)
The physical signs of an enlarged spleen are:
1. it appears from below the tip of the left tenth rib
and enlarges along the line of the rib towards
the umbilicus,
2. it is firm, smooth and usually spleen shaped; it
often has a definite notch on its upper edge,
3. you cannot get above it,
4. it moves with respiration,
5. it is dull to percussion,
6. although it may be possible to bring it forwards
by lifting the left lower ribs forwards, it cannot
be felt bimanually or be ballotted.
Enlargement of the kidney
One or both kidneys may be enlarged. The common
causes of enlargement of the kidney are:
■
hydronephrosis
■
pyonephrosis
■
malignant disease: carcinoma of the kidney and
nephroblastoma
■
solitary cysts
■
polycystic disease
■
hypertrophy.
A mobile or low-lying kidney may be easily pal-
pable and seem to be enlarged, especially if the patient
is thin.
Hydronephrosis may be bilateral if the obstruct-
ing lesion is in or distal to the neck of the bladder.
Nephroblastoma is occasionally bilateral.
Polycystic disease is very likely to affect both
kidneys.
The physical signs of an enlarged kidney are:
1. it lies in the paracolic gutter or can be pushed
back into this gutter – that is to say, it can be
reduced into the loin,
2. it is usually only possible to feel the lower pole,
which is smooth and hemi-ovoid,
3. it moves with respiration,
4. it is not dull to percussion because it is covered
by the colon; even when a large kidney reaches
the anterior abdominal wall, it has a band of
resonance across it,
5. it can be felt bimanually,
6. it can be balloted. This means that it can be
bounced between your two hands, one on the
anterior abdominal wall and the other behind
over the renal angle, rather like a ball being
patted between the hands. This sign is
diagnostic of a renal mass but can only occur if
the mass can be reduced into the loin.
Revision panel 15.20
Causes of enlargement of the kidney
Distension of the pelvi-calyceal system
Space-occupying lesions
Single
Cyst
Abscess
Tumour
Multiple
Polycystic disease
Compensatory hypertrophy
Resonant
Sometimes dull
FIG 15.18
Bilateral enlargement of the kidneys.
Chap-15.qxd 4/19/05 14:35PM Page 423
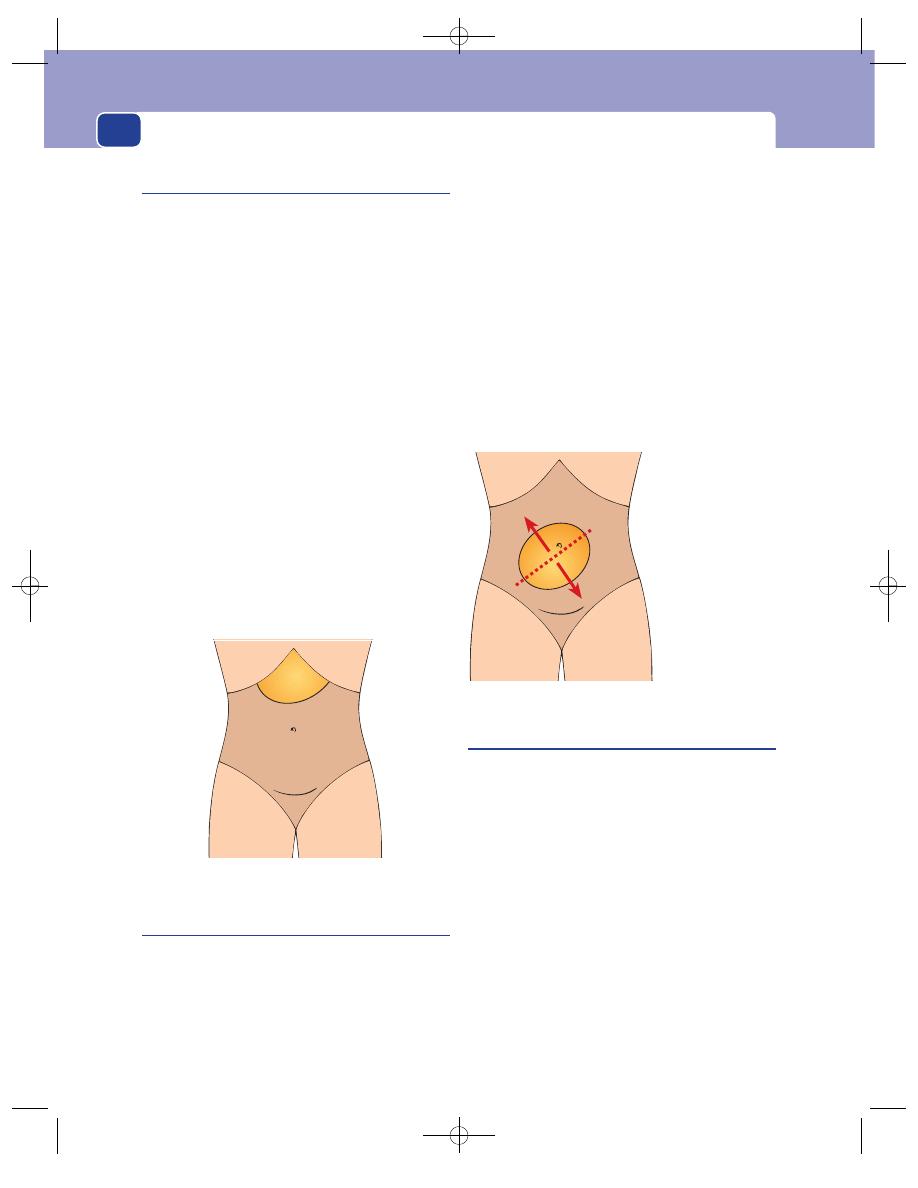
The abdomen
424
Pancreatic pseudocysts
This is a collection of pancreatic juice and inflam-
matory exudate, usually associated with acute
pancreatitis, which forms on the surface of the pan-
creatic gland or fills the lesser sac. The patient is
usually known to have just had an attack of acute
pancreatitis (see page 399) and then developed epi-
gastric fullness, pain, nausea and vomiting. If the
cyst becomes infected, the patient develops severe
pain, sweating and rigors.
The physical characteristics of a pancreatic pseudo-
cyst are:
1. the epigastrium contains a firm, sometimes
tender, mass with an indistinct lower edge; the
upper limit is rarely palpable,
2. it is usually resonant to percussion because it is
covered by the stomach,
3. it moves very slightly with respiration,
4. it is not possible to elicit fluctuation or a
fluid thrill.
These swellings can be very difficult to feel as
most of their bulk is beneath the costal margin.
Mesenteric cysts
These are cysts containing clear fluid that develop in
the mesentery. They arise from the vestigial rem-
nants of re-duplicated bowel and are usually found
by chance. They can, rarely, cause abdominal disten-
sion or recurrent colicky pain. Like all cysts, they
can rupture, twist and bleed from their lining.
Twisting is rare because they are fixed within the
small bowel mesentery.
The physical characteristics of a mesenteric
cyst are:
1. it forms a smooth, mobile, spherical swelling in
the centre of the abdomen,
2. it moves freely at right-angles to the line of the
root of the mesentery, but only slightly along a
line parallel to the root of the mesentery,
3. it is dull to percussion,
4. large cysts may be felt to fluctuate and have a
fluid thrill.
It is difficult to discriminate between a very large
cyst and tense ascites.
Retroperitoneal tumours
Apart from primary and secondary tumours of the
lymph glands, retroperitoneal tumours are rare. The
commonest variety is the liposarcoma. They grow
slowly and silently and usually become quite large
before they are noticed by the patient or become
palpable. The patient complains of distension, a
vague abdominal pain and sometimes anorexia and
weight loss.
They produce the following physical signs:
1. abdominal distension,
2. a smooth or bosselated mass with an indistinct
edge and a soft-to-firm consistence,
3. while they are covered with bowel they are
resonant, but when they reach the anterior
abdominal wall and push the bowel out to the
flanks they become dull to percussion,
Cyst moves freely
at right angles to
the root of the
mesentery
FIG 15.20
A mesenteric cyst.
FIG 15.19
A pancreatic, lesser sac, pseudocyst.
Chap-15.qxd 4/19/05 14:35PM Page 424
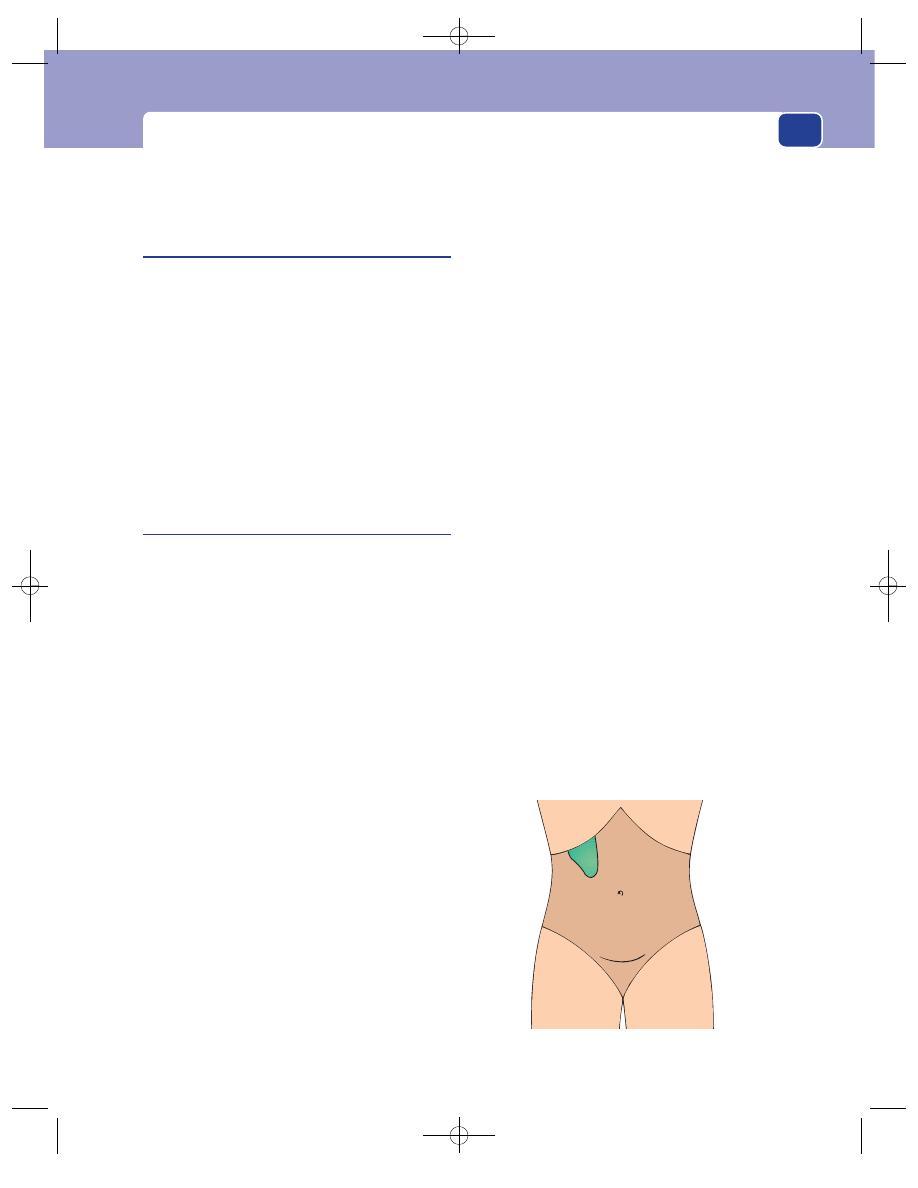
The abdominal mass: causes and signs
425
4. they move very little with respiration,
5. they may transmit aortic pulsation.
Carcinoma of the stomach
The symptoms of carcinoma of the stomach are
described on page 396. Although stomach cancers
can become large, hard masses, they are notoriously
difficult to feel because they are high in the
abdomen beneath the costal margin. A palpable
tumour is hard and irregular, disappearing beneath
the costal margin. It is rarely possible to feel its
upper edge. The symptoms of abdominal pain or
indigestion with loss of appetite and weight are far
more significant than the physical signs. Do not
expect to feel a mass in a patient with carcinoma of
the stomach.
The gallbladder
An enlarged gallbladder is usually easy to recognize
from its shape and position. The causes of enlarge-
ment of the gallbladder are as follows.
■
Obstruction of the cystic duct, usually by a
gallstone, rarely by an intrinsic or extrinsic
carcinoma. The patient is not jaundiced and
the gallbladder often contains bile, mucus (a
mucocele) or pus (an empyema).
■
Obstruction of the common bile duct,
usually by a stone or a carcinoma of the
head of the pancreas. The patient will be
jaundiced.
Courvoisier’s law states: ‘When the gallbladder is
palpable and the patient is jaundiced, the bile duct is
unlikely to be obstructed by a stone because previ-
ous attacks of inflammation will have caused the
gallbladder to become thick-walled, fibrotic and
non-distensible’.
This is a useful clinical rule but there are a num-
ber of exceptions.
■
Stones that form in the bile duct rather than
in the gallbladder may obstruct the duct
in the presence of a normal distensible
gallbladder.
■
There may be a double pathology – a stone in
the cystic duct causing gallbladder distension
and a carcinoma or a stone blocking the lower
end of the bile duct.
■
The converse of the law, jaundice without
a palpable gallbladder, does not mean that
jaundice is caused by stones. In such cases
the obstruction may be caused by a cancer
of the head of the pancreas, and the gallbladder
distension may be insufficient to be palpable.
Alternatively, the jaundice may be caused by
a carcinoma of the bile or hepatic ducts
above the entry of the cystic duct into the
bile duct.
■
Mirizzi’s syndrome: when the cystic duct is
closely applied to the common hepatic duct or
is very short, a stone impacted in it can inflame
and obstruct the bile duct and cause jaundice.
The gallbladder is often distended.
The physical features of an enlarged gall-bladder
are:
1. it appears from beneath the tip of the right
ninth rib,
2. it is smooth and hemi-ovoid,
3. it moves with respiration,
4. there is no space between the lump and the
edge of the liver,
5. it is dull to percussion.
When an acutely inflamed gallbladder becomes
surrounded by adherent omentum and bowel it
loses some of its characteristics. A gallbladder mass
is diffuse and tender, it lies in the right hypochon-
drium, and does not move much with respiration.
FIG 15.21
An enlarged gallbladder.
Chap-15.qxd 4/19/05 14:35PM Page 425
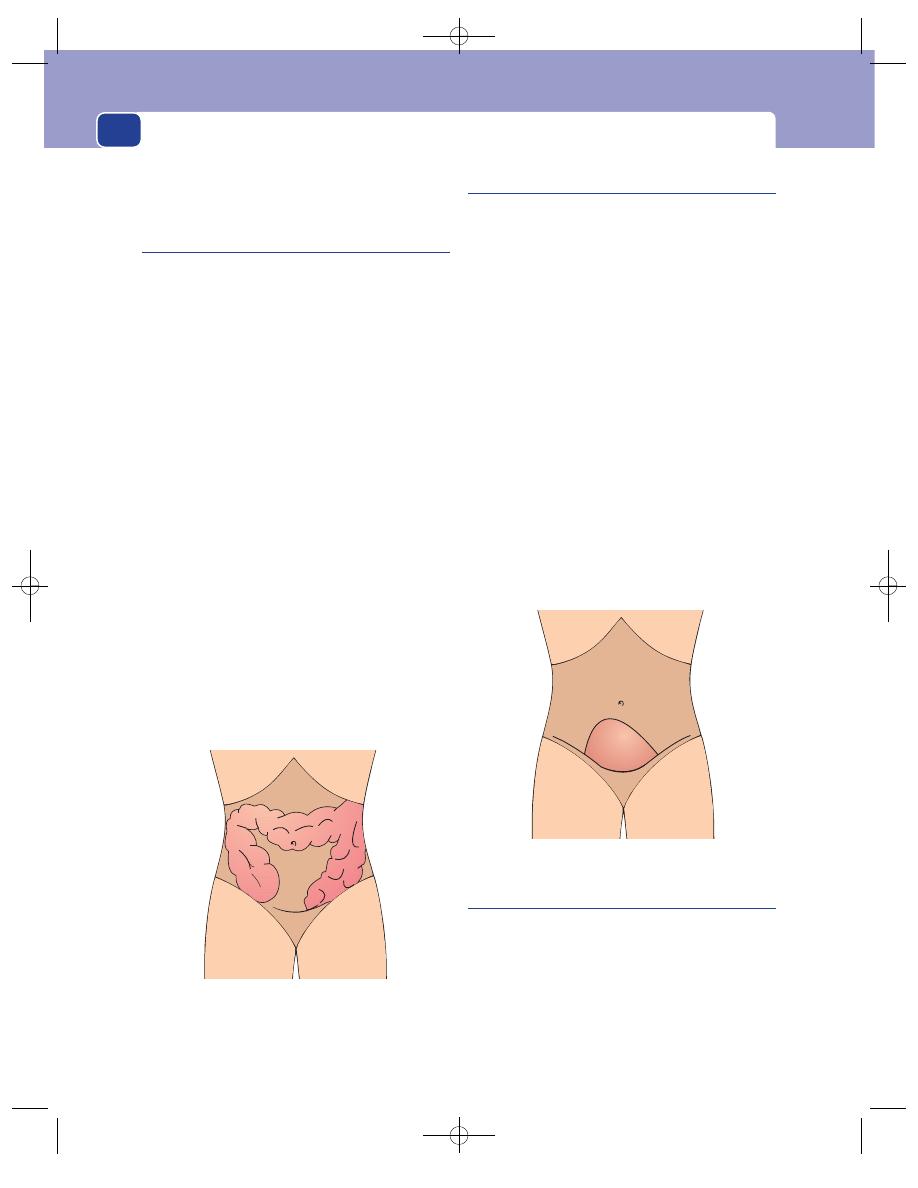
The abdomen
426
As the infection subsides it becomes more discrete
and mobile, and less tender.
Faeces
The colon can become grossly distended with faeces
as a result of a mechanical obstruction or chronic
constipation. The patient may complain of diar-
rhoea, but this is actually mucus and a little watery
faeces leaking out around the main mass of faeces
(spurious diarrhoea).
The physical characteristics of faeces are as follows.
1. The masses lie in that part of the abdomen
occupied by the colon – the flanks and across
the lower part of the epigastrium.
2. They feel firm or hard but are indentable – this
means that they can be dented by firm pressure
with the fingers and this dent persists after
releasing the pressure.
3. There may be multiple separate masses in the
line of the colon but in gross cases the faeces
coalesce to form one vast mass which is easy to
mistake for a tumour.
4. When there is no mechanical obstruction, rectal
examination confirms a rectum full of very hard
faeces, but if there is a blockage in the lower
colon, the rectum will be empty.
Do not forget that faecal masses can form above
an annular stenosing carcinoma of the colon.
The urinary bladder
The causes of retention of urine are listed on
page 442. The bladder may be tense and painful
(acute retention) or enlarged and painless (chronic
retention).
The physical features of an enlarged bladder are:
1. it arises out of the pelvis and so it has no
lower edge,
2. it is hemi-ovoid in shape, usually deviated a
little to one side,
3. it may vary in size: a very large bladder can
extend up to and above the umbilicus,
4. it is not mobile,
5. it is dull to percussion,
6. if it is large enough to permit the necessary
simultaneous percussion and palpation, it will
have a fluid thrill,
7. direct pressure on the swelling often produces a
desire to micturate,
8. it does not bulge into the pelvis and can only be
felt indistinctly on bimanual (combined rectal
and abdominal) examination.
Ovarian cyst
Small ovarian cysts are common and are impalp-
able. When they enlarge, they rise up out of the pelvis
into the lower abdomen and become palpable.
The physical features of a large ovarian cyst are:
1. it is smooth and spherical with a distinct outline,
2. it arises from the pelvis, so its lower limit is not
palpable, i.e. you cannot ‘get below it’,
FIG 15.23
A distended urinary bladder.
FIG 15.22
A colon distended with faeces. The masses
are indentable. Faecal impaction of this degree is likely
to be caused by Hirschsprung’s disease or gross
constipation.
Chap-15.qxd 4/19/05 14:35PM Page 426
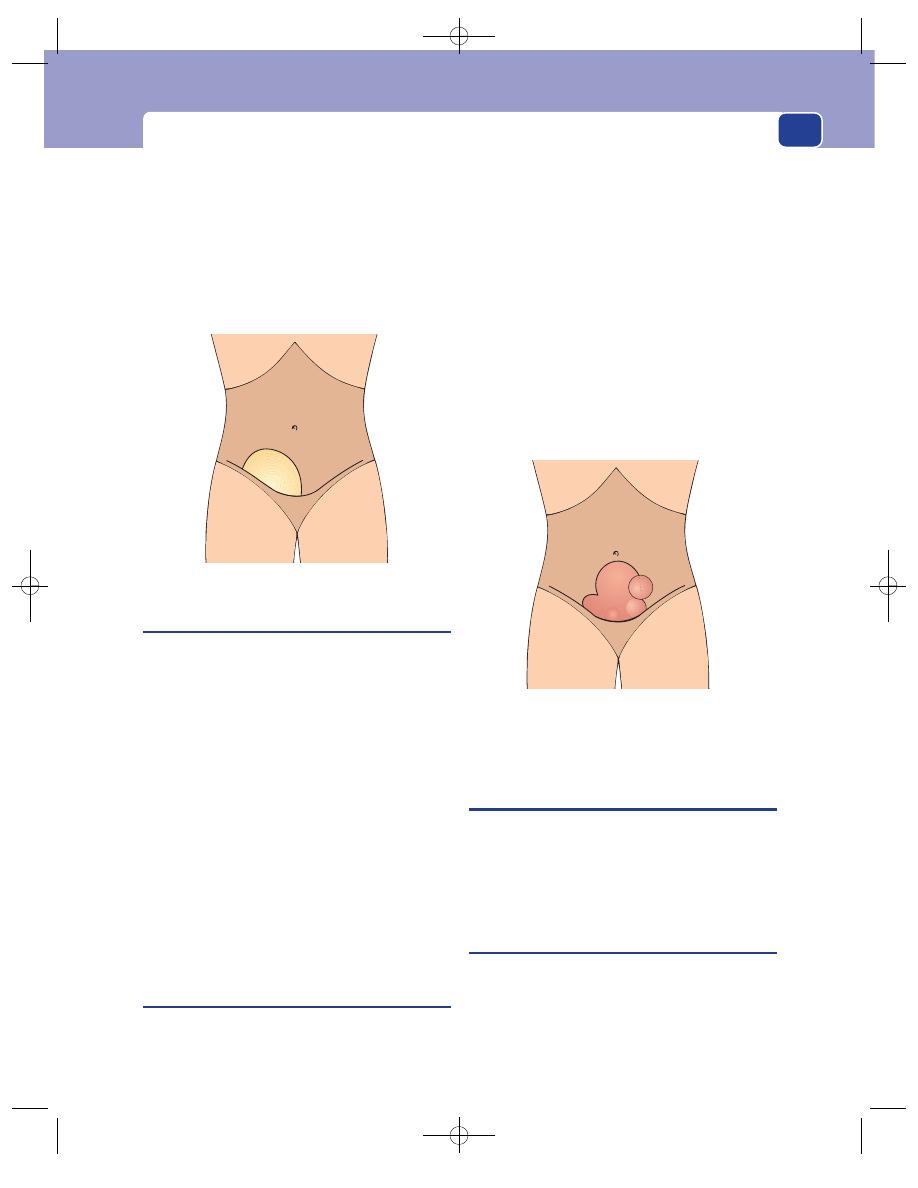
Causes of a mass in the right iliac fossa
427
3. it may be mobile from side to side but cannot be
moved up and down,
4. it is dull to percussion,
5. it has a fluid thrill,
6. its lower extremity may be palpable in the pelvis
during rectal or vaginal examination, and
movement of the cyst may produce some
movement of the uterus.
The pregnant uterus
Never forget that pregnancy is the commonest
cause of enlargement of the uterus, and of abdom-
inal distension.
The diagnosis of pregnancy is more difficult in
the first 20 weeks, when the uterus is still relatively
small and there are no fetal movements.
A pregnant uterus is a smooth, firm, dull swell-
ing arising out of the pelvis.
The uterus enlarges to the xiphisternum by the
36th week of pregnancy. At this stage the fetus is
palpable (ballotable) and moves.
The diagnosis of pregnancy is confirmed if
bimanual examination reveals that the mass cannot
be moved independently of the cervix and that the
cervix is soft and patulous.
An enlarged uterus must not be squeezed dur-
ing a bimanual examination, as this can cause the
patient to go into labour and abort the fetus.
Fibroids
Fibroids are benign fibromyomatous uterine tumours
which can grow to an enormous size and fill the
whole abdomen. They are usually multiple. They can
cause irregular and heavy periods, disturbed mic-
turition, lower abdominal pain and backache.
The physical signs of a fibroid uterus are:
1. it arises out of the pelvis and so its lower edge is
not palpable,
2. it is firm or hard, bosselated or distinctly
knobbly – each knob corresponding to a fibroid,
3. it moves slightly in a transverse direction and
any movement of the abdominal mass moves
the cervix,
4. it is dull to percussion,
5. it is palpable bimanually: a moderately enlarged
uterus can be pushed down into the pelvis.
CAUSES OF A MASS IN THE RIGHT
ILIAC FOSSA
A mass in the right iliac fossa is a common physical
finding. There are a number of conditions that may
be responsible. This section describes the important
features in the history and examination of each
cause.
Appendix mass
History
The patient usually complains of a period of
central abdominal pain followed by a pain in the
right iliac fossa. The pain often persists for several
days and is usually accompanied by malaise, loss of
appetite and pyrexia.
FIG 15.25
A large fibroid uterus.
FIG 15.24
A large ovarian cyst.
Chap-15.qxd 4/19/05 14:35PM Page 427
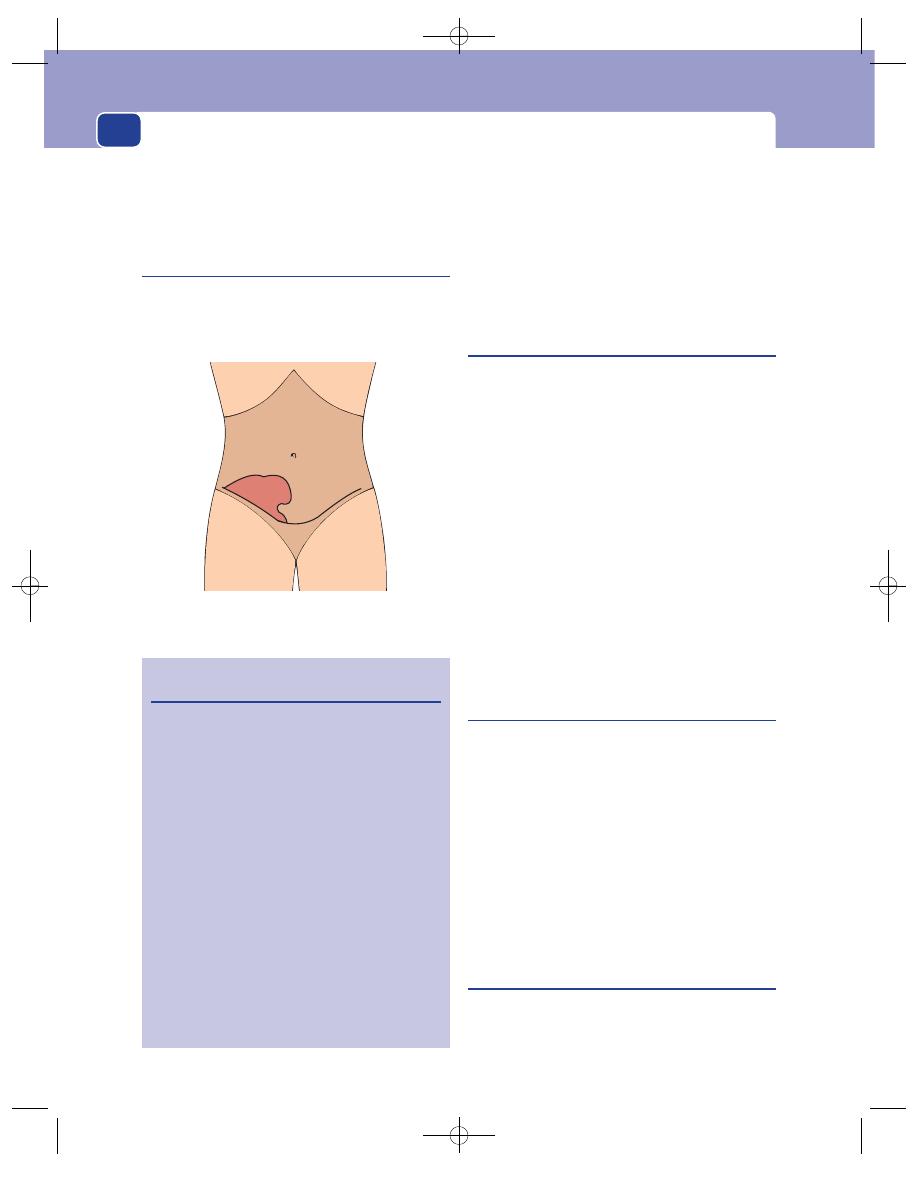
The abdomen
Examination
There is a tender, indistinct mass, which
is dull to percussion, fixed to the iliac fossa poster-
iorly, and accompanied by a persistent low fever and
tachycardia.
Appendix abscess
History
This is the same as for an appendix
mass, with the additional symptoms of an abscess,
namely, fever, rigors, sweating and increased local
pain.
Examination
There is a tender mass which, in its
late stages, may be associated with oedema and red-
dening of the overlying skin. The patient will have
a swinging, intermittent fever and an increasing
tachycardia.
Tuberculosis
In many parts of the world, tuberculosis is more
often the cause of an inflammatory mass in the right
iliac fossa than appendicitis. The mass consists of the
inflamed ileocaecal lymph glands and parts of the
caecum and terminal ileum that are also inflamed.
History
The patient often has a vague central pain for
months, with general ill-health, loss of weight, and
changes in bowel habit. The pain then becomes
intense and settles in the iliac fossa. An acute episode
of central abdominal pain moving to the right iliac
fossa, similar to appendicitis, is uncommon.
Examination
The mass is firm, tender and very indis-
tinct. The surface and the edge are difficult to define.
If there is a tuberculous peritonitis, the abdomen
will be swollen and less flexible – often described as
a ‘doughy’ abdomen.
Carcinoma of the caecum
History
Often there is no acute pain, just a dull
discomfort in the right iliac fossa. Some patients
present with anaemia, diarrhoea or intestinal
obstruction.
Examination
The mass is firm, distinct and hard. It is
usually fixed to the posterior abdominal wall, but
sometimes it is mobile. It is not tender and does not
resolve with observation. The patient’s temperature
and pulse are normal unless there is an associated
pericolic abscess.
Crohn’s disease
(Terminal ileitis)
History
The patient will have experienced recurrent
episodes of pain in the right iliac fossa, general
malaise, weight loss and episodes of diarrhoea.
428
FIG 15.26
A common diagnostic problem: a mass in the
right iliac fossa.
Revision panel 15.21
The causes of a mass in the right iliac fossa
Appendix mass
Appendix abscess
Tuberculosis
Carcinoma of caecum
Crohn’s disease (terminal ileitis)
Iliac lymphadenopathy
Iliac artery aneurysm
Psoas abscess
Chondrosarcoma or osteosarcoma of
the ilium
Tumour in an undescended testis
Actinomycosis
Ruptured epigastric artery
Spigelian hernia
Kidney transplant
Ovarian cyst/tumour
Fibroid
Malignant change in an undescended testis
Chap-15.qxd 4/19/05 14:35PM Page 428
Causes of a mass in the right iliac fossa
429
Examination
The swollen terminal ileum forms an
elongated sausage-shaped mass which usually lies
transversely in the right iliac fossa and feels rubbery
and tender.
Iliac lymph glands
History
The symptoms depend on the cause of
the lymphadenopathy. There may be a generalized
disease, or local disease in the limb, perineum or
genitalia.
Examination
Enlarged iliac lymph glands form an
indistinct mass, with no clear contours. The mass
follows the line of the iliac vessels and may bulge
forwards just above the inguinal ligament. It can be
easy to feel, or be no more than a fullness in the
depths of the iliac fossa.
All the other lymph glands must be examined, as
must the lower limb, to try to find the cause of the
lymphadenopathy.
Iliac artery aneurysm
History
The patient may have noticed a pulsating
mass or felt an aching pain in the right iliac fossa.
Examination
The common iliac artery dilates more
often than the external iliac artery, so the smooth,
distinct mass with an expansile pulsation is usually
in the upper medial corner of the iliac fossa.
Psoas abscess
History
The patient is likely to have felt ill for some
months, with night sweats and loss of weight. Back
pain and abdominal pain can also occur.
Examination
The iliac fossa is filled with a soft, ten-
der, dull, compressible mass. There may be a fullness
in the lumbar region which is accentuated by press-
ing on the mass in the iliac fossa. The swelling may
extend below the groin and it may be possible to
empty the swelling below the groin into the swelling
above, and vice versa.
Back movements may be painful and limited.
Chondroma and sarcoma of the ilium
Rarely, chondromata and chondrosarcomata arise
in the iliac bones. They grow slowly and may bulge
into the iliac fossa. They are large, hard, non-tender
and clearly fixed to the skeleton. They usually lie out
in the lateral part of the iliac fossa. Osteomata and
osteosarcomata of the ileum are equally rare.
Actinomycosis
This invariably develops as a complication of appen-
dicitis, but may present de novo as a mass in the iliac
fossa with a number of discharging sinuses. It is rare.
Spigelian hernia
These herniae appear at the outer edge of the rectus
abdominis muscle along the linear semilunaris. The
lump is still palpable when the abdominal wall mus-
cles are contracted and it is felt to lie above them.
Ruptured inferior epigastric artery
This occurs as a result of straining or coughing. The
haematoma tracks beneath the abdominal wall, extra-
peritoneally, to produce a mass in the iliac fossa. It is
diffuse and there may be discolouration of the skin.
It is attached to the anterior abdominal wall but, as
it is on its deep surface, it becomes impalpable when
the muscles contract. Contraction of the abdominal
muscles is usually painful.
A transplanted kidney
The mass is situated beneath the transplant scar
and a history of transplantation makes the diagnosis
easy. The lump is smooth, kidney shaped and
rubbery.
Ovarian cysts and fibroids
These can fall to the right into the right iliac fossa.
They will be felt to be connected to the uterus on
bimanual examination. A huge pyosalpinx may occa-
sionally be palpable in the right iliac fossa.
Malignant change in an undescended
testis
This is a rarity but is easily suspected provided you
remember your routine and always examine the
scrotum as part of the abdominal examination.
Chap-15.qxd 4/19/05 14:35PM Page 429
The abdomen
430
CAUSES OF A MASS IN THE
LEFT ILIAC FOSSA
Diverticulitis and carcinoma of the colon are the
common causes of a mass in the left iliac fossa. It
must be remembered that the normal sigmoid
colon is palpable in one out of three patients. An
appendix mass on the left side only occurs if the
patient has situs inversus. Tuberculosis and Crohn’s
disease only cause masses in the right iliac fossa. All
the other causes of a mass in the right iliac fossa
mentioned above can also cause a mass in the left
iliac fossa.
Diverticulitis
When sigmoid diverticula become inflamed, the
swollen colon and surrounding pericolic abscess may
be palpable.
History
The patient may have suffered from recur-
rent lower abdominal pains and chronic constipa-
tion for years. The acute episode starts suddenly with
a severe left iliac fossa pain, nausea, loss of appetite
and constipation.
Examination
The left iliac fossa contains a tender,
indistinct mass whose long axis lies parallel to the
inguinal ligament. There may be signs of general
or local peritonitis and intestinal obstruction. The
diagnosis depends upon the site of the tenderness.
There are very few other acute inflammatory condi-
tions that present with a mass in the left iliac fossa.
Carcinoma of the sigmoid colon
History
The patient may present with lower abdom-
inal pain, abdominal colic, intestinal obstruction, a
change in bowel habit, rectal bleeding and general
cachexia.
Examination
The mass is hard, easily palpable and not
tender. It may be mobile or fixed. The colon above
the mass may be distended with indentable faeces.
CAUSES OF A LUMP IN THE GROIN
The inguinal region is part of the iliac fossa and
swellings within it and just below it in the groin can
be confused with iliac fossa masses.
Hernia (inguinal or femoral)
(see page 374)
The diagnosis is made from the site and shape of the
lump and, if present, its reducibility and an expan-
sile cough impulse.
Lymph glands
Inguinal lymph glands present as hard or firm dis-
crete nodules, or an indistinct mass, spreading across
the groin, down the thigh along the line of the long
saphenous vein, and up into the iliac fossa. Look for
a local cause and examine all other groups of lymph
glands.
Saphena varix
(see page 202)
A saphena varix is a soft, compressible dilatation at
the top of the saphenous vein. It has an expansile
cough impulse. A fluid thrill will be felt when the
saphenous vein lower down the leg is percussed.
The swelling disappears when the patient lies down.
Revision panel 15.22
The causes of a mass in the left iliac fossa
Diverticulitis
Carcinoma of the colon
Carcinoma of caecum
Crohn’s disease (terminal ileitis)
Iliac lymphadenopathy
Iliac artery aneurysm
Psoas abscess
Chondrosarcoma or osteosarcoma of the
ilium
Tumour in an undescended testis
Actinomycosis
Ruptured epigastric artery
Spigelian hernia
Kidney transplant
Ovarian cyst/tumour
Fibroid
Malignant change in an undescended testis
Chap-15.qxd 4/19/05 14:35PM Page 430
Abdominal distension
431
Psoas abscess
A psoas abscess may pass down beneath the
inguinal ligament and present in the upper part
of the femoral triangle as a soft, fluctuant, com-
pressible mass. It is possible to elicit fluctuation
between the parts of the abscess above and below
the inguinal ligament, and empty one part into the
other.
Psoas bursa
A psoas bursa lies between the psoas tendon and the
lesser trochanter of the femur. When it becomes dis-
tended or inflamed, it bulges into the upper outer
corner of the femoral triangle, lateral to the femoral
vessels, where it causes a diffuse swelling. It is too
deep to have a distinct shape or to fluctuate. It is
painful when the hip joint is moved.
Femoral aneurysm
This presents as a mass with an expansile pulsation
lying in the line of the femoral artery.
Hydrocele of a femoral hernial sac
Hydrocele of the cord or canal of Nuck
(see page 371)
Ectopic testis
(see page 344)
ABDOMINAL DISTENSION
The causes of abdominal distension can be remem-
bered by repeating the letter ‘F’ six times: fetus, flatus,
faeces, fat, fluid (free and encysted), and fibroids and
other solid tumours.
Fetus
Pregnancy is the most common cause of abdominal
distension. The features of a pregnant uterus have
already been described on page 427.
Flatus
(Tympanites)
Gas in the intestine can cause considerable abdom-
inal distension.
In the early stages, the distension may be localized
to that part of the abdomen containing the distended
bowel, such as the epigastrium when the stomach is
distended, or the right iliac fossa when the caecum
is distended, but as the distension affects the whole
bowel, the whole abdomen swells.
The distension remains localized if the bowel
twists into a volvulus. This is a common complica-
tion of a long sigmoid colon combined with a nar-
row base of the mesocolon.
Distended bowel has no palpable surface or edge.
The only diagnostic features are hyper-resonance
and, when there is obstruction, visible peristalsis.
The bowel sounds may be hyperactive. Shaking the
patient causes a splashing sound as the thin layer of
fluid in the distended bowel splashes about. This is
known as a succussion splash and is particularly
common when there is gastric distension caused by
pyloric stenosis.
Acute dilatation of the stomach, mechanical intes-
tinal obstruction, paralytic ileus, aerophagy (air
swallowing) and massive amounts of free gas from a
perforation all cause hyper-resonance on abdom-
inal percussion.
Revision panel 15.23
The causes of abdominal distension
Fetus
Flatus
Faeces
Fat
Fluid:
free (ascites)
encysted
Large solid tumours such as:
fibroids
enlarged liver
enlarged spleen
polycystic kidneys
retroperitoneal sarcomata
Chap-15.qxd 4/19/05 14:35PM Page 431
The abdomen
432
Faeces
Faecal impaction may present as abdominal disten-
sion or an abdominal mass. The physical features
of faecal masses in the abdomen are described on
page 426. The diagnosis can usually be suspected
from the history of the patient’s bowel habits. The
common causes are Hirschsprung’s disease, chronic
intestinal obstruction, chronic constipation and anti-
depressant drugs.
Fat
Fat rarely causes distension, but frequently makes
the patient pot-bellied. A large fat abdomen may be
caused by a thick layer of subcutaneous fat or by
excess fat in the omentum and mesentery. These
two sites of fat deposition do not necessarily enlarge
together. A protuberant, round abdomen often has
a thin layer of subcutaneous fat but contains a
heavy, thick omentum.
Fluid: ascites
Free fluid in the peritoneal cavity is called ascites. It
is caused by a variety of conditions but they all fall
into one of four groups: those which raise the portal
venous pressure, those which lower the plasma
proteins, those which cause peritonitis, and those
which allow a direct leak of lymph into the peri-
toneal cavity.
Causes of an increased portal venous
pressure
Pre-hepatic
■
Portal vein thrombosis
■
Compression of the portal vein by lymph glands
Hepatic
■
Cirrhosis
Post-hepatic
■
Budd–Chiari syndrome
Cardiac
■
Constrictive pericarditis
■
Right heart failure caused by mitral stenosis,
tricuspid incompetence and pulmonary
hypertension
Pulmonary
■
Pulmonary hypertension and right heart failure
Causes of hypoproteinaemia
■
Kidney disease associated with albuminuria
■
Cirrhosis of the liver
■
The cachexia of wasting diseases, malignancy
and starvation
■
Protein-losing enteropathies
■
Malnutrition
Causes of chronic peritonitis
Physical
■
Post-irradiation
■
Starch granuloma
Infection
■
Tuberculous peritonitis
Neoplasms
■
Secondary peritoneal deposits of carcinoma
■
‘Mucus’-forming tumours (pseudomyxoma
peritonei)
Revision panel 15.24
Aetiology of ascites
Raised portal venous pressure
Pre-hepatic, intra-hepatic and post-hepatic
Cardiac
Pulmonary
Hypoproteinaemia
Renal
Hepatic
General
Peritonitis
Acute and chronic
Traumatic, chemical, infective, neoplastic
Lymphatic obstruction
(Chylous ascites)
Chap-15.qxd 4/19/05 14:35PM Page 432
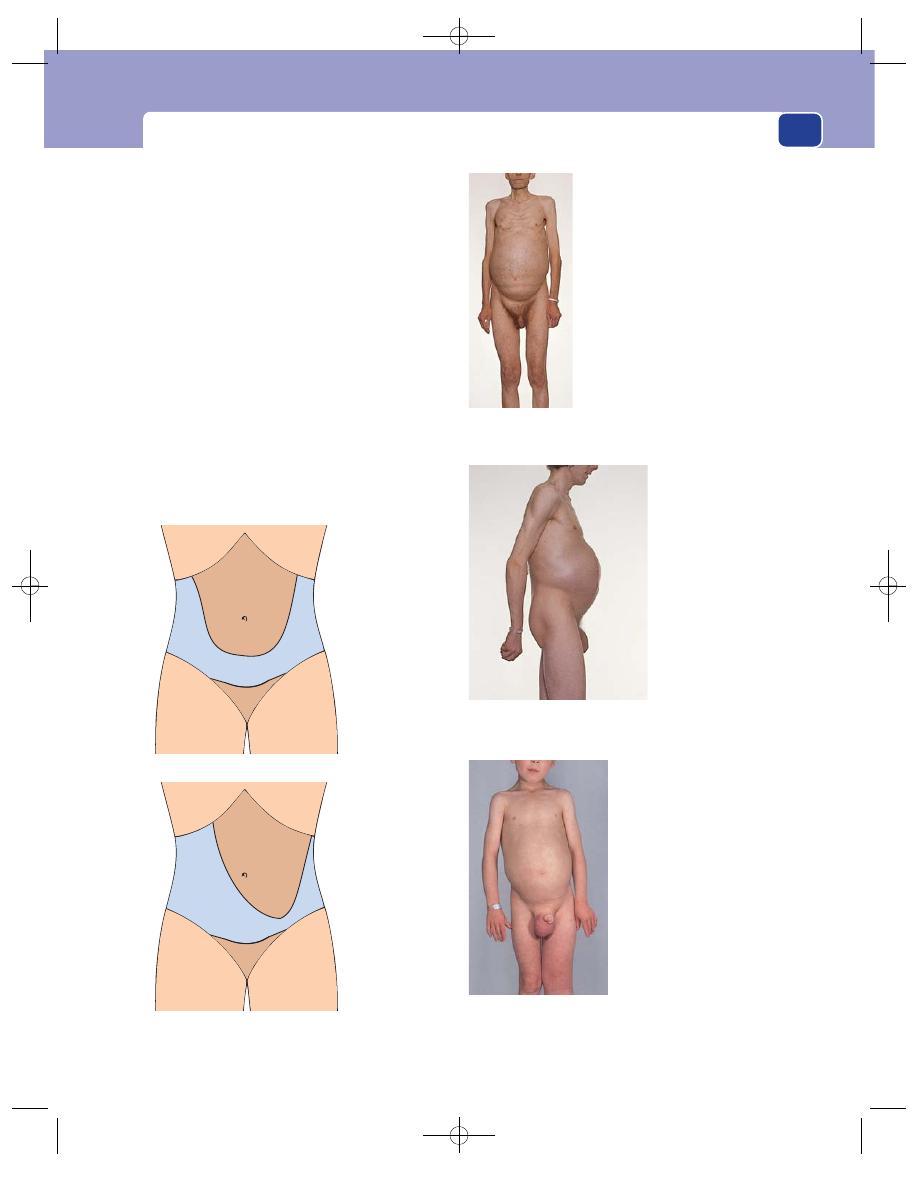
Abdominal distension
433
Causes of chylous ascites
Chylous ascites is caused by the leakage of lymph
from the lacteals or the cisterna chyli as a result of
congenital abnormalities, trauma and primary or
secondary lymph gland disease.
Physical signs of ascites
1. A fluid thrill
2. Shifting dullness
A fluid thrill is elicited by flicking one side of
the abdomen with the index or middle finger and
feeling the vibrations when they reach the other side
of the abdomen with your other hand. Before doing
this you must place the edge of the patient’s (or an
assistant’s) hand on the abdomen at the umbilicus
to prevent the percussion wave being transmitted
Distribution of
dullness caused
by ascites when
supine
Redistribution of
dullness when
patient is tilted
45
° to the right
FIG 15.27
Shifting dullness is diagnostic of free
intraperitoneal fluid (ascites).
Ascites secondary to carcinoma of the stomach. Note the
wasting and the right inguinal hernia full of ascitic fluid.
Abdominal distension caused by a retroperitoneal
liposarcoma in a young man.
Congenital chylous ascites. Note the lymphoedema of the
left leg, and the right hydrocele.
FIG 15.28
SOME EXAMPLES OF ABDOMINAL DISTENSION.
Chap-15.qxd 4/19/05 14:35PM Page 433
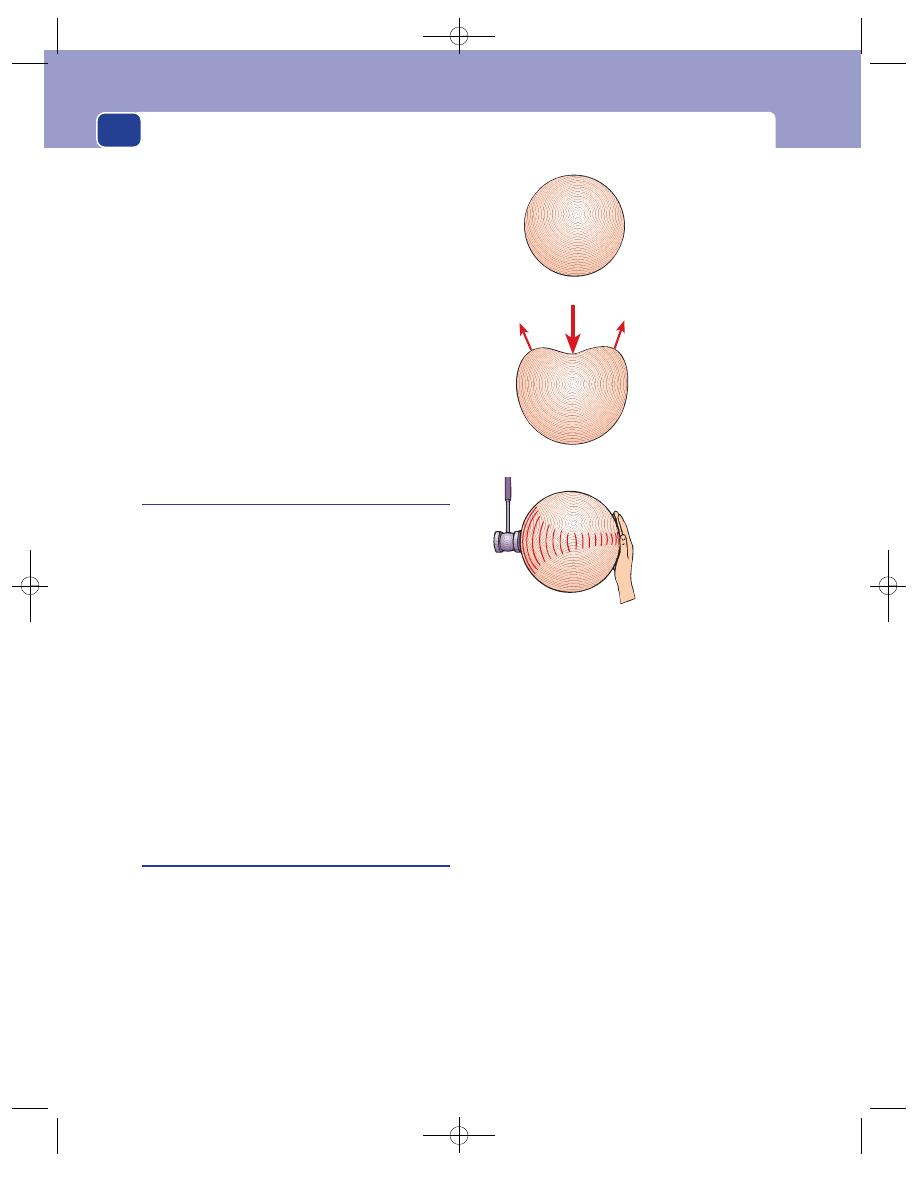
The abdomen
434
through the fat in the abdominal wall. A fluid thrill
is present in any fluid-filled cavity, so that the differ-
ence between free and encysted fluid depends upon
the recognition of shifting dullness.
Shifting dullness is a dull area which moves or
changes shape when the patient changes position.
The dullness of ascites is found in the flanks and
across the lower abdomen. Percuss the medial limits
of the flank dullness carefully and place vertical
marks on the abdomen with a felt-tipped pen. Then
ask the patient to turn onto one side to an angle of
approximately 45°. Wait a few seconds and percuss
again. The medial limits of dullness will have moved
towards the mid-line on the lower side of the abdo-
men and away from it on the upper side if there is
free fluid moving under the influence of gravity.
Fluid: encysted
Fluid trapped in a cyst, or in the renal pelvis, or
between adhesions, will have a fluid thrill, be dull to
percussion, but not shift.
The position and features of a cyst depend upon
its anatomical origin. The following cysts or fluid-
filled swellings may become large enough to present
as abdominal distension:
■
ovarian cysts
■
hydronephrosis
■
urinary bladder
■
pancreatic pseudocysts
■
mesenteric cysts
■
hydatid cysts.
A large aortic aneurysm can also distend the
abdomen. It is distinguished by the presence of an
expansile pulsation.
Fibroids and other solid tumours
Solid tumours which can become very large and
cause abdominal distension are, in approximate
order of frequency:
■
hepatomegaly (Budd–Chiari syndrome or
metastatic liver tumours)
■
fibroids
■
splenomegaly (myelofibrosis)
■
large cancers of the colon
■
polycystic kidneys
■
primary carcinoma of the liver
■
retroperitoneal sarcoma and lymphadenopathy
■
ganglioneuroma (in children)
■
nephroblastoma (in children)
■
neurofibroma/schwannoma.
The physical signs of most of these tumours are
described in the preceding parts of this chapter.
Tends to
become
spherical
Fluctuates
Has a fluid thrill
FIG 15.29
The features of encysted fluid.
Chap-15.qxd 4/19/05 14:35PM Page 434
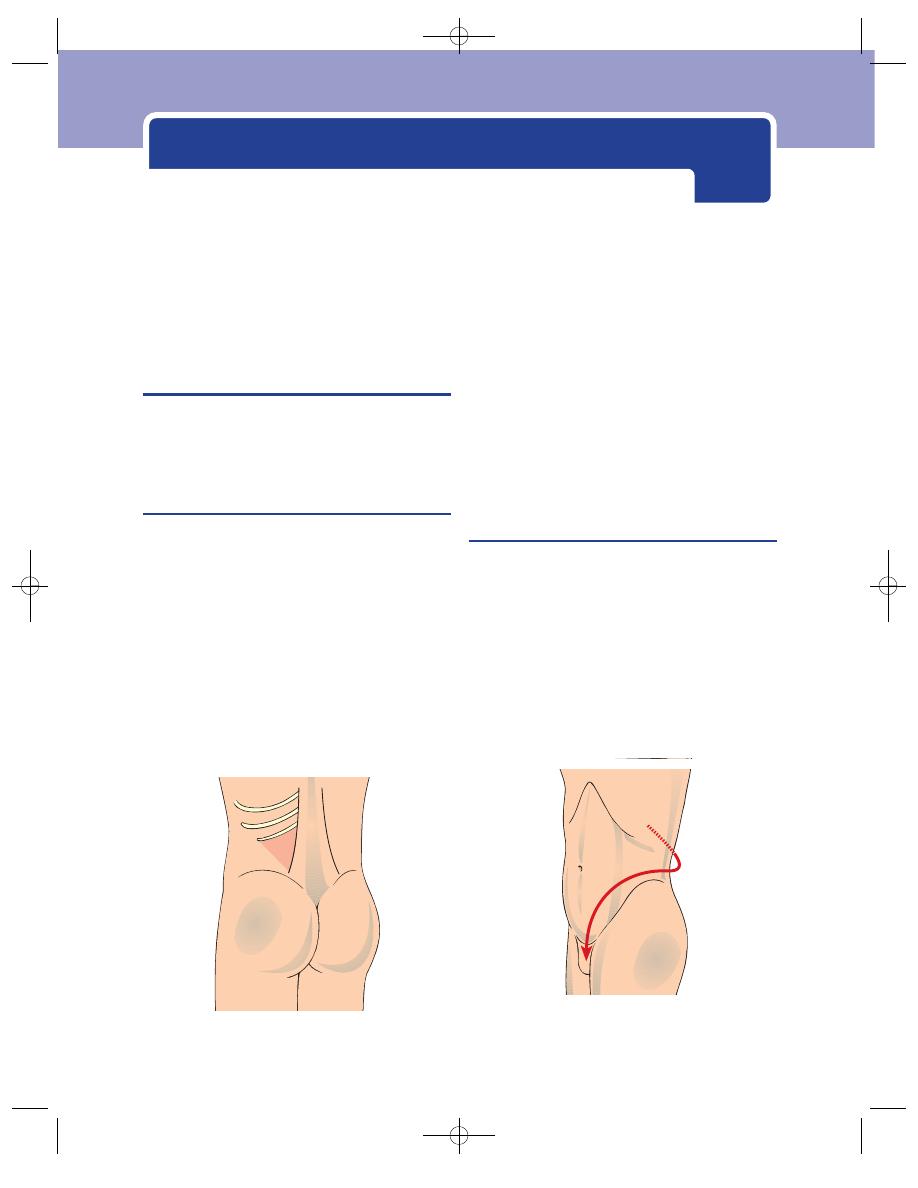
The kidneys, urinary tract and
SYMPTOMS OF RENAL AND URINARY
TRACT DISEASE
It is very important to obtain an exact history of the
symptoms of renal and urinary tract disease because
the kidney, ureter and bladder are not readily acces-
sible for physical examination.
Renal pain
Site
Pain from the kidney is felt in the:
■
loin – the space below the 12th rib and the iliac
crest
■
renal angle – the angle between the 12th rib and
the edge of the erector spinae muscle.
When you ask a patient with renal pain to show you
the site of the pain, he usually spreads his hand around
his waist with his fingers covering the renal angle and
his thumb above the anterior superior iliac spine.
Severity
Renal pain can vary from a constant dull
ache to a very severe pain.
Nature
Do not use the term ‘renal colic’. True colic
is autonomically modulated and can only come
from distension of the smooth muscle wall of a
conducting tube such as the ureter. Because the
severity of renal pain often fluctuates rapidly it gets
called renal colic, but patients rarely describe it as
griping, and it never disappears completely between
exacerbations.
Ureteric colic
Site
Colic from the ureter is felt along the line of
the ureter. The point where it begins is a reliable indi-
cator of the level of the obstruction.
In most cases the pain starts in the loin and then
radiates downwards, around the waist, obliquely
across the abdomen, just above the inguinal ligament,
to the base of the penis, the scrotum or the labia.
Severity
The exacerbations of ureteric colic are
extremely severe. The patient tries to relieve the pain
by rolling around the bed or walking about. Patients
FIG 16.1
The renal angle is the area in the loin between the
12th rib and the edge of the erector spinae muscle.
FIG 16.2
Ureteric colic radiates down from the renal angle,
along a line parallel to the inguinal ligament, into the base of
the penis, the scrotum or the labium majus.
Chap-16.qxd 4/19/05 14:35PM Page 435
The kidneys, urinary tract and prostate
often say that it is the worst pain they have ever
experienced, and women may say that it is as bad as
labour pain. It is accompanied by sweating and often
by nausea and vomiting.
Nature
Ureteric colic is a true colic. It is griping in
nature and comes in waves, with pain-free periods
between attacks.
Haematuria
Blood may be noticed in the urine during or after
micturition. Modest bleeding may have no visible
effect on urine colour or may make it look darker
than usual. If there is heavy bleeding, the urine may
resemble pure blood.
If the blood is coming from the bladder neck or
the lower part of the urinary tract, it may appear
only at the end of micturition.
The causes of haematuria are listed in Revision
panel 16.1.
Make quite sure that female patients have not
mistaken menstrual bleeding for haematuria, and
remember that there are other rare causes of a red/
brown discolouration of the urine, such as:
■
eating large amounts of beetroot
■
paroxysmal haemoglobinuria
■
porphyria.
Vesical pain
Pain from the bladder is usually a dull, suprapubic
ache, made worse by micturition.
Strangury (literally, squeezing urine) is one of
those many terms in medicine that means different
things to different people. Some use it to describe a
painful desire to micturate, which starts in the blad-
der and radiates into the urethra. Others use it
to describe pain felt at the end of micturition as
the patient squeezes out the last few drops of urine.
To avoid confusion, do not use it at all.
Frequency of micturition
An increased frequency of micturition may be
caused by a reduction in functioning bladder capacity
following incomplete emptying, or by irritation of
the bladder wall. It is of greater significance if it wakes
the patient from sleep, so remember to ask about the
436
Revision panel 16.1
The causes of haematuria
Kidney
Congenital
Polycystic kidney
Traumatic
Ruptured kidney
Stone
Inflammatory
Tuberculosis
Neoplastic
Carcinoma of the kidney
Carcinoma of the renal pelvis
Blood disorders
Anti-coagulant drugs
Purpura
Sickle-cell disease
Haemophilia
Scurvy
Malaria
Congestion
Right heart failure
Renal vein thrombosis
Infarction
Arterial emboli from:
a myocardial infarct, or
subacute bacterial endocarditis
Ureter
Stone
Neoplasm
Bladder
Traumatic
Stone
Inflammatory
Non-specific cystitis or ulceration
Tuberculosis
Schistosomiasis (bilharzia)
Neoplastic
Carcinoma
Prostate
Benign and malignant enlargement
Urethra
Traumatic
Rupture
Stone
Inflammatory
Acute urethritis
Neoplastic
Transitional cell carcinoma
Chap-16.qxd 4/19/05 14:35PM Page 436
Diseases of the urinary tract
frequency of nocturnal micturition and record a
day/night ratio.
Dysuria is commonly used to describe pain com-
ing from the urethra during the passing of urine.
Do not confuse it with, for example, the abdominal
pain experienced on micturition by a patient with
appendicitis, which has a totally different cause.
Prostatic pain
Pain from the prostate gland is felt deep inside the
pelvis, between the legs in the perineum and some-
times in the lower back. It is poorly localized and
patient often think it is coming from the rectum.
DISEASES OF THE URINARY TRACT
Hydronephrosis
Hydronephrosis is distension of the calyces and pelvis
of the kidney, caused by obstruction.
The causes of hydronephrosis are listed in Revi-
sion panel 16.2.
Hydronephrosis is often symptomless, but it may
produce renal pain, may present as renal failure, or
may be detected when investigating the symptoms
of the disease causing it.
History
Age
Hydronephrosis occurs at all ages.
Symptoms
The commonest symptom is pain in the
loin. This is a dull, persistent ache, which can be so
mild that it is accepted by the patient as backache and
ignored but which gets worse as the hydronephrosis
enlarges. If the enlargement is sudden, the pain can be
severe. As an autonomic pain, it may be poorly local-
ized and occasionally felt in unexpected sites such
as the epigastrium. A patient with this sort of pain
will never be able to localize the exact site with a fin-
ger, but will place their hand over quite a wide area.
The pain associated with hydronephrosis is made
worse or initiated by an increased production of
urine. Alcohol is a diuretic, so the pain may be asso-
ciated with drinking it. But patients who only get
pain after drinking quantities of beer or spirits are
often reluctant to admit to the association.
Pain is less frequent in bilateral hydronephrosis
as the cause lies in the lower urinary tract and dis-
tension of the renal pelvis tends to develop slowly
and progressively.
Congenital pelvi-ureteric junction obstruction
is often intermittent and associated with the most
severe pain.
Only a very large hydronephrosis will cause
abdominal distension.
There are usually no general symptoms unless
the back pressure damages both kidneys so severely
that renal failure and uraemia result.
Examination
The kidney is well hidden in the back wall of the
abdomen and only a large hydronephrosis will be
palpable. The features of a palpable kidney are des-
cribed in detail in Chapter 15.
An enlarged palpable hydronephrosis should:
■
arise from the loin
■
be reducible into the loin
■
be palpable bimanually
■
be ballotable.
437
Revision panel 16.2
The causes of hydronephrosis
Unilateral hydronephrosis
Pelvi-ureteric obstruction
Congenital pelvi-ureteric junction
stenosis
Pressure from aberrant arteries
Stones and tumours in the renal pelvis,
occluding the opening into the ureter
Ureteric obstruction
Stones
Tumour infiltrating the ureter from the
cervix, rectum, colon or prostate
Tumours of the ureter
Ureterocele
Schistosomiasis
Bladder tumour
Bilateral hydronephrosis
Retroperitoneal fibrosis
Prostatic enlargement – benign or
malignant
Carcinoma of the bladder
Schistosomiasis
Urethral strictures and valves
Phimosis
Chap-16.qxd 4/19/05 14:35PM Page 437
The kidneys, urinary tract and prostate
Acute pyelonephritis
Acute pyelonephritis (pyelitis) is an infection in the
upper part of the urinary tract caused by bacteria
which have come from the bloodstream or up the
ureter from the urethra or bladder. It is commoner
in women because the shortness of their urethra
makes the entry of bacteria into the lower urinary
tract more likely.
History
Sex
Pyelonephritis is much more common in females
than in males.
Age
It occurs in children, in women soon after the
initiation of sexual activity (honeymoon cystitis),
and during pregnancy.
Symptoms
The patient complains of the sudden
onset of a severe pain in one or both loins. The
pain may occasionally be felt anteriorly, and when it
is on the right-hand side can be mistaken for biliary
pain.
At approximately the same time as the onset of
the loin pain, micturition becomes frequent and
painful. Although there may be a vague suprapubic
ache, the main pain during micturition is felt as a
burning sensation along the length of the urethra.
The patient may also complain of a painful but
fruitless desire to micturate.
Headache, malaise, nausea and vomiting often
begin a few hours before the loin pain.
The urine may become cloudy and even blood-
stained. The patient feels ill, hot and sweaty and, in
severe cases, may suffer rigors.
Cause
The patient may have had similar attacks and
be aware of their relationship to sexual intercourse
or pregnancy.
Examination
General features
The patient looks ill and may be
flushed and sweating. The tongue is dry and furred.
The temperature is usually significantly elevated and
there is a tachycardia.
Abdomen
One or both kidneys are moderately
tender when palpated through the abdomen, and the
renal angle is very tender. Guarding and peritonism
will not be found. There may be mild suprapubic
tenderness.
The kidneys are not enlarged unless the infection
has arisen in a previously hydronephrotic kidney.
Urine
The urine may look cloudy and blood-stained.
Red blood cells and pus cells will be seen if the sedi-
ment is inspected with a microscope.
Carcinoma of the kidney
This tumour is also called a hypernephroma because
of its macroscopic appearance and site of occurrence.
This is an inappropriate name because it implies that
it is a lesion arising above the kidney, whereas it actu-
ally arises from renal parenchymal cells. However,
the term is still widely used. Its presentation is pro-
tean; few conditions produce such a range of pre-
senting symptoms.
History
Age
Carcinoma of the kidney is uncommon below
the age of 50 years.
Sex
It is twice as common in males as it is in females.
Symptoms
It can present in many ways, the most
common of which are described below.
■
Haematuria. This is the most common
symptom. The bleeding is usually sufficient to
stain the urine a pale-red colour and appears
intermittently. Occasionally, the bleeding is
heavy and the patient suffers ureteric colic as
blood clots obstruct the ureter (clot colic).
■
General debility. More than one-quarter of
patients with renal carcinoma have no
symptoms until secondary deposits or the
burden of the primary tumour cause general
malaise, loss of energy and loss of weight.
■
Carcinoma of the kidney is one of the cancers
which metastasizes to bone, and some patients
present with bone pain and pathological
fractures.
■
Pain in the loin. This is also a common symptom,
especially when the tumour breaks through its
false capsule and invades nearby structures.
■
A mass. A mass may be felt by chance at a
routine examination, or by the patient, or it may
cause abdominal distension.
The following are some of the less common
symptoms.
■
Pyrexia of unknown origin (PUO). Carcinoma
of the kidney should be excluded in every
438
Chap-16.qxd 4/19/05 14:35PM Page 438
Diseases of the urinary tract
patient who presents with a PUO, nowadays by
ultrasound scan.
■
Polycythaemia. The tumour cells produce
erythropoietin, resulting in polycythaemia.
This causes redness of the face and hands and
spontaneous venous and arterial thromboses.
To emphasize the multiplicity of symptoms of
renal cancer, other patients present with
anaemia from their haematuria!
■
Varicocele. Occlusion of the left renal and
testicular veins by direct spread of the tumour
along the renal vein can cause a varicocele.
There may even be inferior vena caval
obstruction, producing oedema of both legs
and the abdominal wall.
■
A sudden severe abdominal pain may indicate
acute haemorrhage into the tumour. The kidney
can also rupture spontaneously, producing
collapse and the signs of massive intraperitoneal
bleeding.
■
Hypertension, of renal origin, is a rare
complication of renal carcinoma.
Examination
General features
The patient may show signs of recent
weight loss.
Abdomen
Large tumours are palpable and demon-
strate the physical signs of an enlarged kidney, des-
cribed above. There is not usually any tenderness or
guarding.
Skeleton
There may be areas of swelling and tender-
ness in the bones, at the sites of secondary deposits.
Very rarely, such deposits of renal carcinoma can be
very vascular and feel soft, pulsatile and compres-
sible, and have an audible bruit.
Chest
There may be a pleural effusion on the side
of the tumour if it has spread up through the
diaphragm.
The usual type of lung metastasis produced by
carcinoma of the kidney has a ‘cannon ball’ appear-
ance on chest X-ray. This may be solitary.
Carcinoma of the renal pelvis
This is a transitional cell carcinoma of the urothe-
lium and is identical to the type commonly found in
the bladder and discussed below. It is often associated
with tumours elsewhere in the urinary tract, but may
be the only manifestation of uro-epithelial malignant
change.
These tumours present with haematuria. Occa-
sionally the patient has clot colic and passes blood
clots described as ‘stringy’.
They are often found during the routine investi-
gation of haematuria.
They cause no other physical signs.
Renal and ureteric calculi
Stones in the renal pelvis may lie silent for years and
not present until complications such as infection or
renal parenchymal damage occur. Stones in the ureter
invariably cause pain.
History
Age
Renal and ureteric calculi are found most often
between the ages of 30 and 50 years.
Sex
They are more common in men than in women.
Season
Urinary calculi develop more frequently in
the summer, perhaps initiated by the lower urine
flow in warm, dry weather and an abundance of soft
fruits which are rich in oxalates, an important consti-
tuent of calculi.
Symptoms
The principal symptoms are pain and
haematuria.
The pain depends on the site of the stone. A dull
ache in the loin is typical of a renal stone. A stone in
the ureter produces ureteric colic (described above),
moving down along the line of the ureter as the stone
makes its way to the bladder. All stones start in the
kidney. A large stone will not pass the pelvi-ureteric
junction. A stone small enough to enter the ureter will
normally pass through to the bladder, with much
patient discomfort as it intermittently becomes
jammed and produces a bout of colic.
A patient with ureteric colic invariably has micro-
scopic haematuria, but rarely visible haematuria.
However, stones occasionally ulcerate through the
uro-epithelium without causing pain, yet cause heavy
haematuria.
The first indication of the presence of a stone
may be the symptoms of acute pyelonephritis. If
the stone has damaged renal function, symptoms
of uraemia may develop – headaches, restlessness,
twitching, fits, convulsions, drowsiness, and coma.
439
Chap-16.qxd 4/19/05 14:35PM Page 439
The kidneys, urinary tract and prostate
Examination
Abdomen
It is not possible to examine the abdomen
properly when a patient is having an attack of
ureteric colic because he is rolling around and holding
his muscles tense. There may be secondary abdom-
inal distension, as occurs with other problems that
arise in the posterior abdominal wall.
The confirmation of the diagnosis rests on special
investigations which reveal the presence of the stone.
Nearly all urinary calculi show up on plain abdominal
X-ray. Dilatation of the urinary tract is best seen on
ultrasound scanning.
A few metabolic disorders predispose to the for-
mation of urinary calculi. The least rare (1 in 300) is
hyperparathyroidism. There may be symptoms of
hypercalcaemia (thirst, polydipsia, nausea, vomit-
ing and eventually drowsiness).
Bladder calculi
Stones may form in the bladder in association with
stasis, infection or tumour, or enter from the ureter.
There is always a degree of bladder outlet obstruction,
otherwise the stone would have been rapidly voided.
History
Age
Bladder stones are rare in Western countries
except in middle-aged and elderly males with pro-
static problems.
Symptoms
The most common symptom is an inc-
reased frequency of micturition, sometimes related
to posture. When the patient stands up the stone falls
onto the trigone, causing a stabbing pain and initiat-
ing a desire to micturate. During the night, the stone
rolls away and the frequent desire to micturate
abates.
There is sometimes a history of intermittent
sudden cessation of urinary flow, relieved by lying
down, for the same reason as given above.
There may be suprapubic stabbing pain, exacer-
bated by standing.
Haematuria, particularly at the end of mictu-
rition, is also a common symptom.
Many patients have chronic infection, with the
symptoms of cystitis.
The symptoms caused by the stone are often pre-
ceded by the symptoms of its cause, namely bladder
outlet obstruction, infection and bladder tumours.
Examination
There are rarely any physical signs, although very
large stones can sometimes be felt on bimanual
examination of the pelvis.
Sounding the bladder
Bladder stones were common in
past centuries and were diagnosed before X-rays
were available, by passing a metal instrument into
the bladder, via the urethra, and listening to the
sound made as it tapped on the stone. This proce-
dure is remembered in the name still used for the
instrument – a urethral ‘sound’.
Cystitis
Cystitis is an infection of the urine within the blad-
der, with a concomitant inflammatory reaction in
the bladder wall. The common predisposing factors
of cystitis are incomplete emptying of the bladder,
abnormalities within the bladder and, in women,
bacteria migrating up the urethra. In females, there
is often a clear relationship with sexual activity.
History
Age
Cystitis occurs often in young and middle-aged
women, in young men with urethritis and in elderly
men with prostatism and bladder tumours.
Symptoms
The most common symptoms are inc-
reased frequency and urgency of micturition, which
begin suddenly and persist through the night as well
as the day. The patient often wants to micturate
every few minutes.
Passing urine causes a burning or scalding pain
along the length of the urethra. It is often so bad
that the patient tries to avoid passing urine. There
may be a mild suprapubic ache.
Haematuria is common. The pattern is for there
to be a few drops of bloody urine at the end of mic-
turition, but it may turn the urine mahogany brown.
The urine may be cloudy, with a characteristic fishy
smell.
Examination
Apart from mild suprapubic tenderness, there are
rarely any physical signs.
Remember to look at the urine and examine the
sediment microscopically for pus cells.
440
Chap-16.qxd 4/19/05 14:35PM Page 440
Retention of urine
Urethral syndrome
Many women with the symptoms of recurrent cys-
titis never have bacteria demonstrated in the urine.
This collection of symptoms is termed the urethral
syndrome. Its cause is unknown and its manage-
ment difficult.
Carcinoma of the bladder
Bladder cancer is nearly always a transitional cell car-
cinoma, although there are several other rare types.
It rarely produces any physical signs, so the diagno-
sis must be suspected from the history.
History
Age
Bladder cancer occurs throughout adult life
but the peak incidence is between the ages of 60 and
70 years.
Sex
Males are afflicted more often than females and
smoking is a risk factor.
Occupation
Some industrial chemicals are excreted in
the urine and can stimulate malignant change in the
uro-epithelium. The better known ones are alpha-
naphthylamine and beta-naphthylamine, ben-
zidine and xylenamine, and artificial sweeteners
such as cyclamates. The industries that use these
chemicals (the rubber and cable industries, printers
and dyers) are now well aware of the relationship,
and chemically induced bladder cancer is now rare.
Predisposing conditions
Squamous cell carcinoma
may be induced by the chronic irritation caused by
bilharziasis.
Symptoms
In 95 per cent of cases, carcinoma of the
bladder presents with a degree of haematuria,
which turns the urine bright red. It may be inter-
mittent or occur every time the bladder is emptied.
The passage of blood clots may cause pain and dif-
ficulty with micturition.
If the urine becomes infected, the patient will expe-
rience a suprapubic ache and burning micturition.
Pain in the loin may occur, as bladder tumours
often begin near the ureteric orifice and obstruct
the lower end of the ureter.
Pain in the pelvis and lower abdomen, and nerve
root pain down the legs, can occur if the tumour
spreads through the wall of the bladder into the pelvis.
A small group of patients with bladder cancer
present with frequent and painful micturition,
without visible haematuria, but there will be micro-
scopic haematuria.
You must not forget that symptoms of cystitis
may indicate a bladder tumour, particularly when
they persist after treatment.
Examination
It is unusual to find any abnormality. If the tumour
is large, it may be felt bimanually, and if it has spread
beyond the bladder, the floor of the pelvis may be
indurated. Examination under anaesthetic is an
important part of the staging of a bladder tumour.
RETENTION OF URINE
There are two forms of retention of urine, acute and
chronic. They are usually easy to distinguish. Acute
retention is painful and sudden. Chronic retention is
painless and there is a chronically distended bladder.
As ever in medicine, things are rarely black and
white. Acute retention may develop in the presence
of chronic retention, when the expression acute on
chronic retention is sometimes used.
Acute retention in the absence of bladder outlet
obstruction is rare and occurs only after a surgical
operation, anaesthesia or an injury to the urethra.
Most patients with acute retention give a history of
progressive slowing of the urinary stream due to
narrowing of the bladder outlet or urethra. This is
termed bladder outlet obstruction.
441
Revision panel 16.3
Bladder carcinogens
Aniline dyes
␣ and  Naphthylamine
Xylenamine
Benzidine
Occupations associated with exposure to
bladder carcinogens
Dry cleaners
Leather workers
Painters and decorators
Paper and rubber manufacturers
Dental technicians
Chap-16.qxd 4/19/05 14:35PM Page 441
The kidneys, urinary tract and prostate
Patients with chronic retention may be symptom
free except for the abdominal swelling produced by
the large bladder.
Thus:
■
acute retention is the sudden, painful inability
to micturate,
■
chronic retention is an enlarged, painless
bladder, whether or not the patient is having
difficulty micturating.
The causes of retention are listed in Revision panel
16.4. It is a long list, but the commonest by far is pro-
static obstruction (benign or malignant) in middle-
aged and elderly men. In hospitals, an operation under
general anaesthesia is a common initiating factor.
Acute retention
History
Symptoms
The patient is likely to have symptoms
related to one of the causes listed in Revision panel
16.4, as well as suprapubic pain and an inability to
pass urine. The pain is severe and is described as a
gross exaggeration of the normal desire to micturate.
The patient is aware that the bladder is over-distended.
Examination
Usually the bladder has enlarged sufficiently to
become a palpable, tense, dull, rounded, tender mass
arising out of the pelvis to a point a few centimetres
above the pubis. Gentle pressure on the swelling exac-
erbates the patient’s desire to micturate. However, it
may be too tender for you to feel it properly, particu-
larly when the abdominal wall is tense or the patient
is overweight.
Percussion is useful in deciding whether a patient
is in acute retention, as the bladder is always dull.
If the patient has had chronic retention before
the acute episode, the bladder may reach up to, or
above, the umbilicus. A large bladder of this size
indicates previous chronic retention.
A rectal examination, if the patient is not too
distressed, will reveal that the prostate or uterus is
pushed backwards and downwards, with the cystic
mass of the bladder filling the front half of the pelvis.
You cannot assess the size of the prostate gland,
or the pelvis, when the bladder is full.
It is better to defer the rectal examination for
prostate assessment until after the retention has been
relieved with a catheter.
Remember to examine not only the prostate, the
urethra and the contents of the pelvis, but also the
central and peripheral nervous systems to exclude a
neurological cause.
Chronic retention
There are two varieties of chronic retention – high
pressure and low pressure.
442
Revision panel 16.4
The causes of retention of urine
Mechanical
In the lumen of the urethra, or overlying
the internal urethral orifice
Congenital valves
Foreign bodies
Tumour
Blood clot
Stones
In the wall of the bladder or the urethra
Phimosis
Trauma (rupture of the urethra)
Urethral stricture
Urethritis
Meatal ulcer
Tumour
Prostatic enlargement (benign and
malignant)
Outside the wall
Pregnancy (retroverted gravid uterus)
Fibroids
Ovarian cyst
Faecal impaction
Paraphimosis
Neurogenic
Post-operative retention
Spinal cord injuries
Spinal cord disease
Disseminated sclerosis
Tabes dorsalis
Hysteria
Drugs
Anti-cholinergics, anti-histamines,
smooth-muscle relaxants, some
tranquillizers
Chap-16.qxd 4/19/05 14:35PM Page 442
The prostate gland
In the high-pressure type, the cause is obstruc-
tion of the bladder outlet. Bladder pressure builds
up and, in a proportion of cases, produces dilatation
of the ureters and the renal collection systems as well
as the bladder. This ultimately results in renal fail-
ure, of the post-renal type.
In the low-pressure type, the fault seems to lie
with the bladder muscle, which is atonic. The vesico-
ureteric junctions remain competent and there is no
back-pressure effect on the kidneys.
If a patient in chronic retention has the symp-
toms and signs of renal failure, the retention is of
the high-pressure type.
History
Age and sex
Chronic retention is most common in
elderly men.
Symptoms
The patient may be unaware of his
chronic retention but complains of symptoms
related to the cause of the retention, such as an
increased frequency of micturition, and difficulty
micturating – delay on starting, a poor stream and
a dribbling finish.
Chronic retention is painless.
Many patients with chronic retention have drib-
bling overflow incontinence. The bladder becomes
so enlarged that the sphincters fail, yet, for some
mechanical reason not yet understood, the bladder
does not empty. Instead of functioning between
empty and full, it works between its residual volume
and an even greater volume. The patient may be able
to pass apparently normal quantities of urine but
the high residual volume persists. When the bladder
is at its fullest, any increase in abdominal pressure
such as that brought about by coughing or move-
ment causes a leakage of urine.
Examination
The bladder will be palpable. It is likely to reach at
least halfway up to the umbilicus. It is not tense or
tender, and supra-pubic pressure may not always
induce a desire to micturate.
The palpable bladder of chronic retention is dull to
percussion, and will fluctuate and have a fluid thrill if
the patient is thin enough to enable you to perform
the manoeuvres necessary to elicit these signs.
Look for the signs of the cause of the retention in
the pelvis, prostate, urethra and nervous system.
Bladder diverticulum
A bladder diverticulum is an out-pouching of blad-
der mucosa through a defect in all layers of the mus-
cle in the bladder wall.
Diverticula usually occur just above one or
both ureteric orifices. They are caused by outflow
obstruction.
Note. The small pockets between the hyper-
trophic strands of muscle that develop following
long-standing outflow obstruction are not true
diverticula, but saccules, as they have a muscle coat.
Bladder diverticula are rarely palpable because of
their position, but may give rise to a peculiar symp-
tom. When the patient needs to pass urine, the mus-
cle contracts and empties the bladder, but the
diverticulum does not empty because its orifice
closes as the bladder shrinks. When the patient has
finished and the detrusor muscle relaxes, the urine
in the diverticulum passes into the bladder and
within minutes the patient feels the need to mic-
turate again. This is sometimes called pis en deux.
THE PROSTATE GLAND
Benign hypertrophy of the prostate gland
The inner portion of the prostate gland hypertrophies
during late adult life. As it grows, it compresses the
outer layers into a false capsule, and bulges centrally
443
Revision panel 16.6
Symptoms of bladder and bladder neck irritation
Increased frequency of micturition
Urgency
Nocturia
Urge incontinence
Revision panel 16.5
Symptoms of bladder outflow obstruction
Hesitancy
Poor flow
Intermittent flow
Post-micturition dribbling
Pis-en-deux
Chap-16.qxd 4/19/05 14:35PM Page 443
The kidneys, urinary tract and prostate
into the urethra and the base of the bladder. The
cause of this hypertrophy is not known but it is
probably an involutional hypertrophy in response
to a changing hormone environment.
The majority of the symptoms result from
mechanical obstruction to the act of micturition.
History
Age
The prostate starts enlarging at the age of 40
years but the symptoms commonly appear between
the ages 50 and 70 years.
Symptoms
Poor stream. The cardinal symptom of
prostatic obstruction is a reduced rate of urine flow
during micturition, that is, a poor stream. However,
the condition develops slowly and intermittently
and the bladder compensates by muscular hyper-
trophy of its wall, which initially overcomes the
increased outflow resistance. In consequence, the
reduced rate of flow, which is very gradual, is not
noticed, or is accepted as part of growing older.
Increased frequency. What the patient complains
of most is an increased frequency of micturition,
often first noticed when it is necessary to pass urine
in the middle of the night.
Inadequate emptying of the bladder and there-
fore a reduction in the functional volume (the add-
itional volume needed to trigger the desire to
micturate) causes the frequency.
Urgency. In addition to the increased frequency
of micturition, the patient reports an urgent need to
start passing urine as soon as the desire arises. This
is called urgency and is caused by increased bladder
pressure.
All patients with significant prostatic hypertro-
phy have a reduced rate of urine flow and you must
enquire about this. Ask if the flow is as good as it was
20 years earlier.
Hesitancy. Associated with the reduced urinary
flow are two other symptoms, hesitancy and drib-
bling. Hesitancy is the inability to start to pass urine.
Straining does not help; it actually prolongs the
waiting time before the urine starts to flow.
Dribbling. Dribbling is the inability to finish
cleanly. A few drops continue to appear for some time
after the main stream has ceased. This goes on until
patience is lost, resulting in staining of underclothing.
Haematuria, in the form of a little dark blood at the
end of micturition, is not an uncommon symptom.
A proportion of patients first present with acute
or chronic retention, described above.
Examination
Abdomen
The bladder will be palpable if there is
acute or chronic retention.
Rectal examination
The features of the normal prostate
gland are described below. Benign hypertrophy causes
a diffuse enlargement. The gland bulges into the rec-
tum, its surface is smooth but the enlargement is often
slightly asymmetrical and the surface bosselated.
The consistence of the gland is firm, rubbery and
homogeneous.
The median sulcus usually remains palpable, even
when the gland is grossly enlarged, and the rectal
mucosa moves freely over the gland. It is not tender.
Note that there may be quite significant prostatic
obstruction without gross enlargement of the
gland. The key factor in the generation of symptoms
is the compression of the prostatic urethra, which
may occur with quite modest enlargement.
Remember that a full bladder pushes the prostate
downwards and makes it feel bigger.
Carcinoma of the prostate
Cancer of the prostate gland begins in its outer part,
so it does not develop a false capsule and can easily
spread into the floor of the pelvis. It is commonly
quite advanced before it causes symptoms.
History
Age
Carcinoma of the prostate is predominantly a
disease of elderly men. Its incidence increases from
the fifties onwards. By the late eighties and nineties
it can be found in nearly all males, but in the vast
majority produces no symptoms or signs.
Symptoms
The commonest presentation is with
symptoms similar to those caused by benign prosta-
tic hypertrophy and collectively called prostatism,
namely poor stream, urgency and frequency. With
prostatic cancer, these symptoms tend to progress
more rapidly and do not fluctuate in severity, as is so
often the case with benign hypertrophy.
A proportion of patients with carcinoma of the
prostate present with some form of retention of
urine.
If the tumour spreads outside the gland, it may
cause pain in the lower abdomen and perineum.
444
Chap-16.qxd 4/19/05 14:35PM Page 444
The urethra
Presentation with secondary deposits is com-
mon, with local symptoms absent or ignored. There
may be debility and loss of weight.
Prostatic cancer metastasizes to bone, particularly
the pelvis and lumbar spine. These bone deposits are
nearly always osteosclerotic, so tend to produce bone
pain rather than pathological fractures. Do not forget
to consider prostatic bony metastases in any eld-
erly man with skeletal pain.
Screening
Prostatic cancer may be detected by meas-
uring the serum levels of prostate-specific antigen
(PSA). There is controversy over the value of this
investigation as a screening tool, as it has been esti-
mated that, on the basis of this test, there are approx-
imately 1 million men with occult prostatic cancer in
the UK, but only 8000 die from the disease each year.
However, a positive PSA test is a mode of presenta-
tion that is becoming increasingly common.
Examination
The bladder will be palpable if there is retention of
urine.
Rectal examination
The prostate gland is asymmetric-
ally enlarged or distorted. It is irregular in contour
and heterogeneous in texture. Some areas are hard
and knobbly; others are soft. The median sulcus may
be absent and the rectal mucosa may be tethered to
the gland.
The tissues of the pelvis, lateral to the gland and
around the rectum, may be infiltrated by tumour.
Most prostatic carcinomata can be diagnosed by
rectal examination, but there are false positives and
false negatives.
The only other physical signs will be those caused
by metastases. Carcinoma of the prostate gland
sometimes gives rise to metastases in the skin and
other unusual sites as well as in bone.
THE URETHRA
Urethritis
This produces symptoms of painful micturition
with a purulent discharge from the external meatus,
which is easier to notice in men than in women. It is
almost invariably caused by a sexually transmitted
disease, commonly gonorrhoea. If not properly and
promptly treated, it heals with a scar, producing a
urethral stricture.
Urethral stricture
Urethral strictures occur as a result of damage or
destruction of the urethral mucosa followed by heal-
ing with fibrous scar tissue. The common causes of
urethral stricture are given in Revision panel 16.8.
History
Age
Urethral strictures occur at all ages. The most
common cause used to be gonorrhoea, which is a
disease of the sexually active, so the strictures that
445
Revision panel 16.8
The causes of urethral stricture
Congenital
Pinhole meatus
Urethral valves (not a true stricture)
Traumatic
Instrumentation (catheterization)
Foreign bodies
Prostatectomy
Amputation of the penis
Direct injuries
Inflammatory
Gonorrhoea
Meatal ulceration
Neoplastic
Primary and secondary neoplasms
Revision panel 16.7
Causes of a urethral discharge
Infection (urethritis) by:
Gonococcus
Chlamydia
Coliforms
Trichomonas
Candida
Lesions in the urethra
Warts
Herpes
Foreign bodies
Chap-16.qxd 4/19/05 14:35PM Page 445
The kidneys, urinary tract and prostate
follow it appeared in young and middle-aged men.
Better and quicker treatment of the infection has
reduced the incidence of post-gonorrhoeal strictures,
and the commonest cause nowadays is probably
catheterization or instrumentation of the urethra.
Symptoms
The key symptom is a poor urinary flow,
which, in contrast to the poor stream that occurs
with benign prostatic hypertrophy, is improved by
straining. The stream is thin and dribbles at its
end. Attacks of cystitis are common, but retention
of urine is rare unless there is added pathology such
as a bladder calculus.
There may be a urethral discharge, which is par-
ticularly noticeable in the morning.
An increasing frequency of micturition indicates
that the bladder is not emptying completely.
Examination
The bladder is sometimes palpable. Renal failure is
occasionally seen.
The penis and urethra usually feel normal because
the commonest site for stricture is where the urethra
passes through the perineal membrane. A stricture
caused by scarring of the penile urethra can some-
times be felt as an area of induration.
Meatal strictures, common following transurethral
operations, are usually visible if the edges of the
meatus are gently retracted.
446
Chap-16.qxd 4/19/05 14:35PM Page 446
Applied anatomy
The anus is the junction of the gut with the skin.
The ‘watershed’ is the mucocutaneous junction,
sometimes called Hilton’s white line. This is a wavy
white line, seen in the lower third of the anal canal
on proctoscopy (see below).
Above the mucocutaneous junction is the rec-
tum, which:
■
has autonomic sensation and is sensitive only to
stretching,
■
receives its arterial blood supply from the
mesenteric vessels,
■
drains venous blood into the portal circulation,
■
drains lymph into the mesocolic lymph glands.
Below the mucocutaneous junction is skin, which:
■
has somatic sensation and is as sensitive as skin
elsewhere,
■
receives its arterial blood supply from the iliac
vessels,
■
drains venous blood into the iliac veins,
■
drains lymph into the inguinal lymph glands.
This differentiation is useful in understanding
the generation of the various symptoms and in
understanding the spread of cancers.
SYMPTOMS OF ANO-RECTAL DISEASE
The principal symptoms of rectal and anal condi-
tions are bleeding, pain, tenesmus, change of bowel
habit, changes in the stool, discharge and pruritus.
These have been mentioned in Chapter 1, but
deserve more detailed consideration.
Bleeding
Blood passed per rectum may be fresh or altered.
When blood is degraded by intestinal enzymes and
bacteria, it becomes black and acquires a characteris-
tic smell. Such a black, tarry stool is called a melaena.
The blood must come from high in the intestinal
tract, usually from the stomach or duodenum, to
have time to turn black before it reaches the rectum.
Recognizable blood may appear in four ways:
■
mixed with the faeces,
■
on the surface of the faeces,
■
separate from the faeces, either after or
unrelated to defaecation,
■
on the toilet paper after cleaning.
Blood mixed with the faeces
This must have come from bowel higher than the
sigmoid colon, where the softness of the stool and
the time left for transit are still sufficient for mixing.
Blood on the surface of the faeces
This has usually come from the lower sigmoid
colon, rectum or anal canal.
Blood separate from the faeces
If the bleeding follows defaecation, it is probably
from an anal condition such as haemorrhoids.
If the blood is passed by itself, it has accumulated
in the rectum rapidly so as to give a desire to defae-
cate. Blood acts as a purgative, and the patient
passes blood and clots. Causes include diverticular
disease, a rapidly bleeding carcinoma, or inflamma-
tory bowel disease.
Occasionally, bleeding from the upper gastro-
intestinal tract is sufficiently rapid as to appear at
the anus as recognizable blood and not melaena.
However, as a rule, the brighter red the blood is, the
lower down is its source.
Blood on the toilet paper
This is usually caused by minor bleeding from con-
ditions in the lower part of the anal canal which are
Chap-17.qxd 4/21/05 12:58AM Page 447
The rectum and anal canal
at the anal margin, such as a fissure or haemor-
rhoids.
Pain
Pain from the anal canal is felt principally on def-
aecation, and is protracted, cramp-like and distres-
sing. There may be a background ache. Excessive
stretching of the anal canal may cause a sharp, split-
ting pain, sometimes described as if something is
tearing. If the patient has a fissure, something is!
The presence of pain may help you to make a
diagnosis, because haemorrhoids and rectal cancer
are not usually painful.
An annular lesion at the rectosigmoid junction
may obstruct the lumen of the bowel and cause
lower abdominal colic.
Pruritus
Peri-anal itching is a very common symptom. It
occurs with those peri-anal conditions that result in
leakage of mucus on to the peri-anal skin, but may
also be caused by a primary skin disease. In chil-
dren, the commonest cause is a worm infestation.
The symptom is frequently worse at night, per-
haps because there are no other sensory distractions.
Incontinence and soiling
This may be caused by sphincter failure, impaction
with overflow, extreme urgency or neurological
impairment.
Tenesmus
This is defined as a constant intense desire to def-
aecate. It may be painful, and when the patient tries
to evacuate the rectum, nothing appears, or just a
small amount of mucus and loose faeces. Tenesmus
is caused by a space-occupying lesion in the lumen
or wall of the rectum, which mimics the presence of
faeces, and is a symptom that should always be
taken seriously.
Bowel habit
Beware of the terms ‘diarrhoea’ and ‘constipation’.
When they use the word constipation, some patients
means that their bowels are opening less frequently
than usual, others that their motions are harder
than usual. Diarrhoea has a similar double mean-
ing, either frequent defaecation or loose motions.
Make sure that you find out what the patient means.
It is better to record the frequency of bowel
action and the consistence of the stool than to use
these lay terms.
Many patients complain of a change in bowel
habit, particularly the elderly, some of whom feel
that daily defaecation is a basic human right!
Picking out those with underlying bowel disease
requires much, often fruitless, investigation.
TECHNIQUE FOR ANO-RECTAL
EXAMINATION
This is commonly called a rectal examination, but
the prefix ‘ano’ has been added to remind you to
look at and feel the anal canal as well as the rectum.
Preparation
Position of the patient
Ensure adequate privacy and uncover the patient
from the waist to the middle of the thighs.
The patient should lie in the left lateral position
with the neck and shoulders rounded so that the
chin rests on the chest, hips flexed to 90° or more,
but knees flexed to slightly less than 90°. If the knees
are flexed more than 90°, the patient’s ankles will get
in your way.
If the patient is lying on a soft bed, ask them to
move towards you so that their buttocks are up to
the edge of the bed. This makes inspection easier
and tips the abdominal contents forwards, which
helps the bimanual examination.
You should never omit the rectal examination
from your routine examination.
Equipment
You need a plastic glove, some inert lubricating jelly
and a good light.
Tell the patient what you are going to do. Explain
that you are going to examine the ‘back passage’ and
the inside of the abdomen. Say that it will be uncom-
fortable but not painful, and ask the patient to relax
by breathing deeply and letting their knees go loose.
448
Chap-17.qxd 4/21/05 12:58AM Page 448
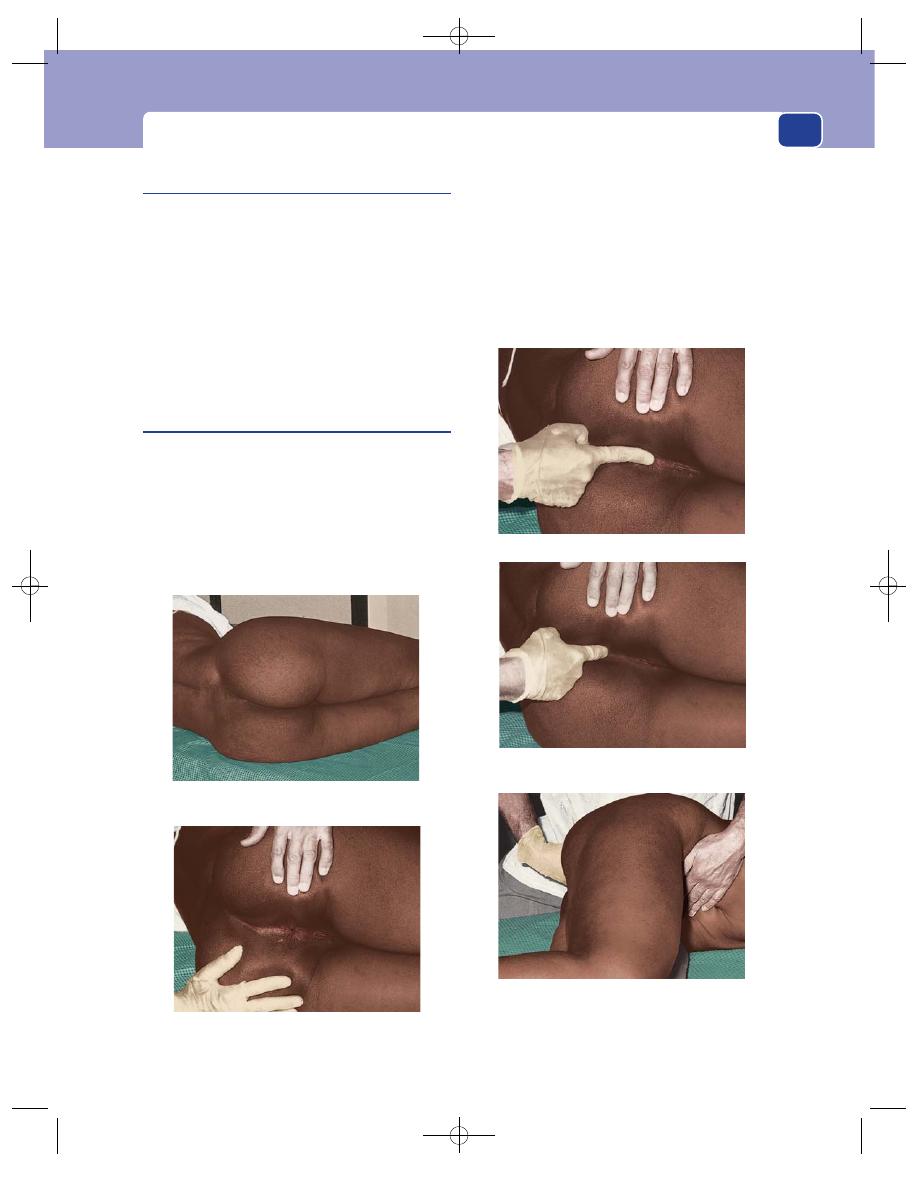
Technique for ano-rectal examination
Inspection
Lift up the uppermost buttock with your left hand
so that you can see the anus, peri-anal skin and peri-
neum clearly. Look for:
■
skin rashes and excoriation,
■
faecal soiling, blood or mucus,
■
scarring, or the opening of a fistula,
■
lumps and bumps (e.g. polyps, papillomata,
condylomata, a peri-anal haematoma, prolapsed
piles, or even a carcinoma),
■
ulcers, especially fissures.
Palpation
Before carrying out a digital examination, particularly
if there is a history of pain on defaecation, place your
fingers on either side of the anus and gently stretch
the anal orifice. This is to see if there is any spasm
associated with a fissure, which may be visible. If there
is spasm or a fissure, in no circumstances carry out
any instrumentation as this could cause severe pain.
Place the pulp of your gloved right index finger
on the centre of the anus, with the finger parallel to
the skin of the perineum and in the mid-line. Then
press gently into the anal canal, but at the same time
press backwards against the skin of the posterior
wall of the anal canal and the underlying sling of the
puborectalis muscle. This overcomes most of the
tone in the anal sphincter and allows the finger to
449
Place the patient in the left lateral position, hips
flexed to 90
⬚, knees less flexed to 110⬚.
Part the buttocks and inspect the anus and perineum.
FIG 17.1
THE TECHNIQUE OF ANO-RECTAL EXAMINATION.
As you insert your finger, pull backwards to
counteract the tone in the puborectalis muscle.
After examining the anal canal and rectum, place
your hand on the abdomen and examine the
contents of the pelvis bimanually.
Place the pulp of your finger on the anus.
Chap-17.qxd 4/21/05 12:58AM Page 449
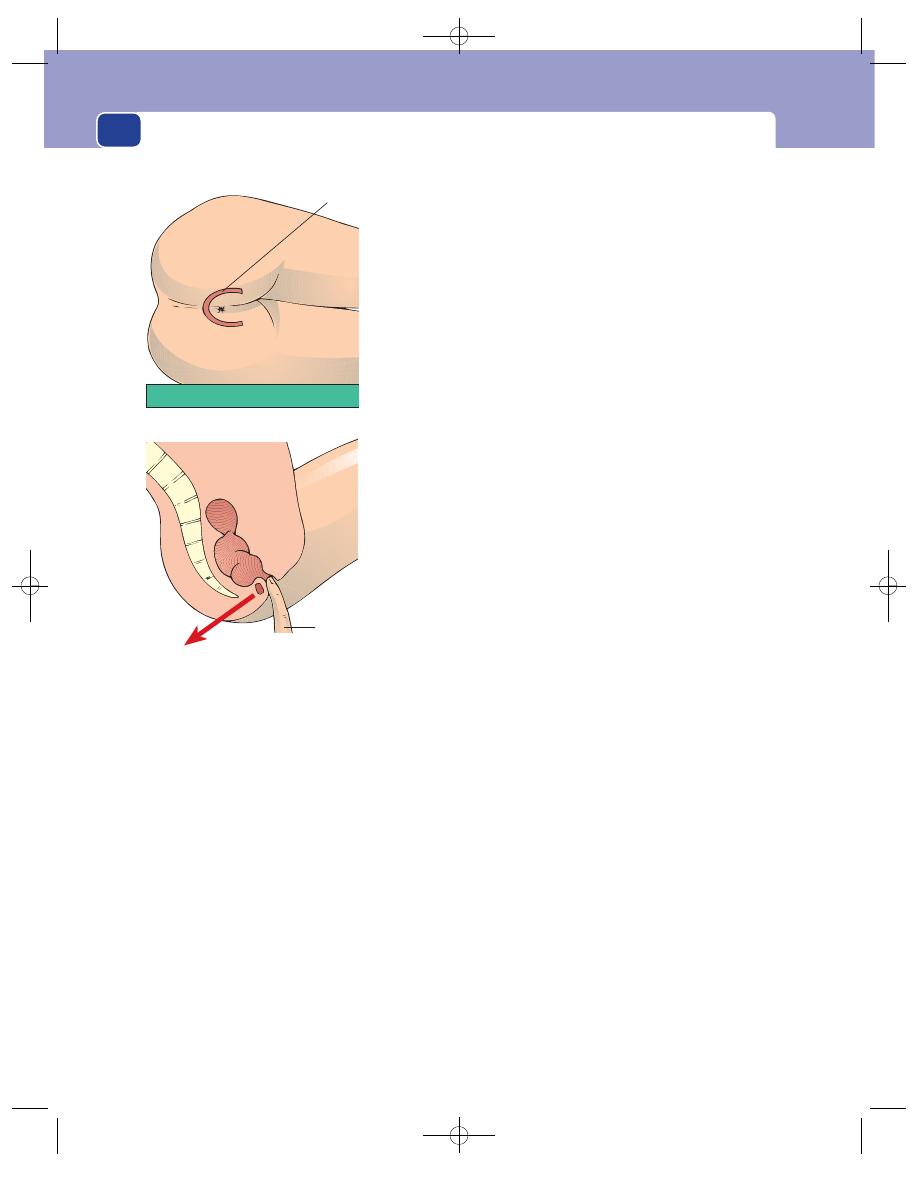
The rectum and anal canal
straighten and slip into the rectum. Never thrust the
tip of your finger straight in.
Look at your finger, when you remove it from
the rectum, to note the colour of the faeces and the
presence of blood or mucus.
The anal canal
As the finger goes through the anal canal, note the
tone of the sphincter, any pain or tenderness and
any thickening or masses.
Patients with fissures or abscesses may have so
much spasm that rectal examination is extremely
painful. In these circumstances, gently try to insert
your finger, and if there is any reaction from the
patient, abandon the procedure. A general anaes-
thetic may be needed for adequate assessment.
The rectum
Feel all around the rectum as high as possible. You
may have to push quite hard in a fat patient, and in
some it is difficult to feel much beyond the anal
canal. Note the texture of the wall of the rectum and
the presence of any masses or ulcers. If you feel a
mass, try to decide if it is within or outside the wall
of the rectum by testing the mobility of the mucosa
over it. This is a most important distinction.
Do not forget to feel the lower rectum, just above
the anal canal. Posteriorly, the rectum turns away at
a right-angle, and it is easy to miss a small swelling
in this area (and also at sigmoidoscopy).
Note the contents of the rectum. The rectum
may be full of faeces (hard or soft), empty and col-
lapsed, or empty but ‘ballooned out’. Faeces may feel
like a tumour but are indentable, the only rectal
mass that is.
If you can just detect a possible abnormality at
your fingertip, ask the patient to strain or push
down. This will often move the mass down 1 or
2 cm or so and bring it within your reach.
The recto-vesico/recto-uterine pouch
Turn your finger round so that the pulp feels for-
wards and can detect any masses outside the rectum
in the peritoneal pouch between the rectum and the
bladder or uterus. It takes practice to be able to tell
the normal prostate and cervix from an abnormal
mass. Do not be downhearted if you get it wrong at
first: experience and confidence are needed.
Bimanual examination
The examination of the contents of the pelvis is
helped if you place your left hand on the abdomen
and feel bimanually. This gives you a much better
idea of the size, shape and nature of any pelvic mass.
You will find this method of examination much
more difficult in an obese patient.
The cervix and uterus
These structures are easy to feel per rectum and,
with the help of bimanual palpation, you should be
able to define the shape and size of the uterus and
any adnexal masses. Do not call the hard mass that
450
The loop of
puborectalis
Pull backwards as you
insert your finger to
counteract the pull of
puborectalis
FIG 17.2
The puborectalis muscle forms a loop which helps to
keep the anal canal closed. As you insert your finger into the
anal canal, you must oppose this tone by pressing your finger
backwards.
Chap-17.qxd 4/21/05 12:58AM Page 450
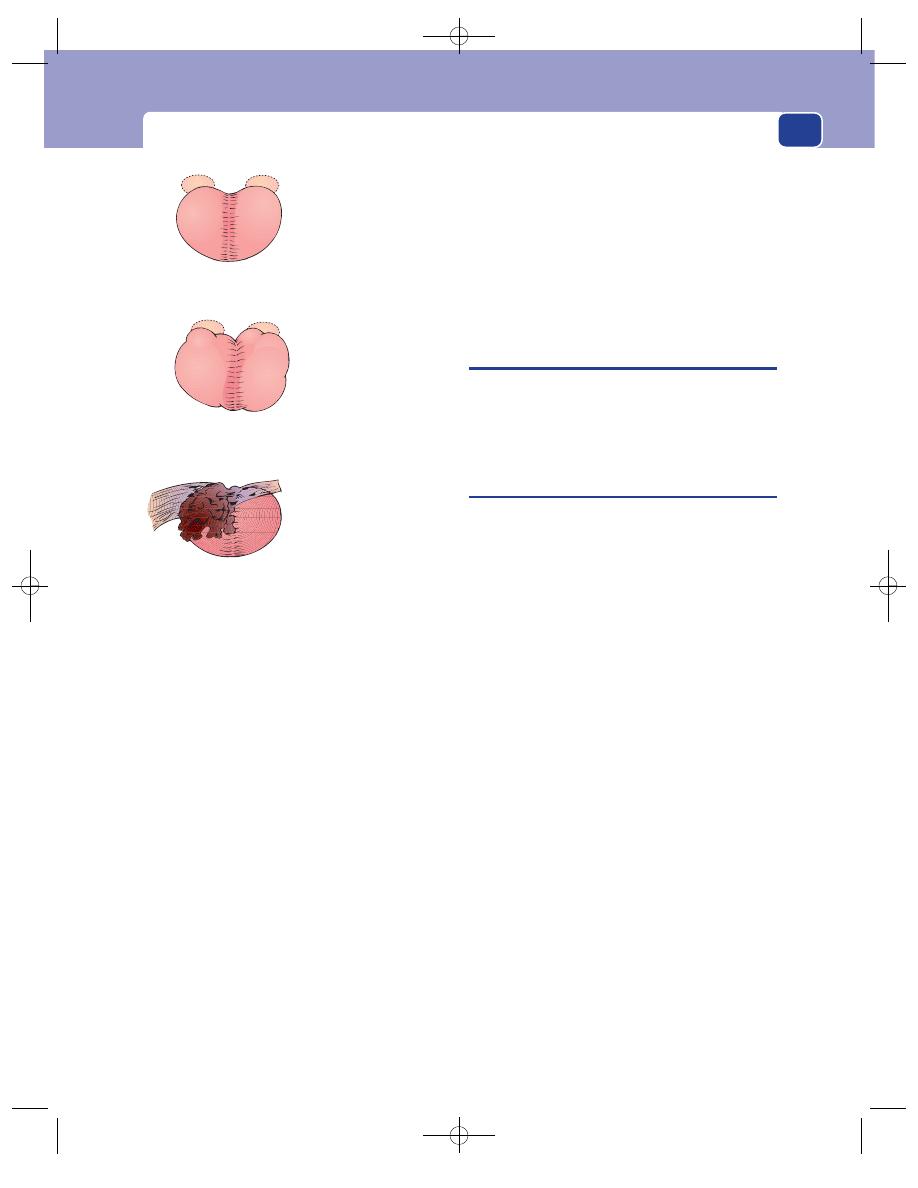
Sigmoidoscopy and proctoscopy
you can feel in the anterior rectal wall a carcinoma
until you are sure that it is neither the cervix nor a
tampon.
The prostate and seminal vesicles
The normal prostate gland is firm, rubbery, bilobed
and 2–3 cm across. Its surface should be smooth,
with a shallow central sulcus, and the rectal mucosa
should move freely over it. The seminal vesicles may
occasionally be palpable just above the upper lateral
edges of the gland (Fig 17.3).
Benign hypertrophy of the prostate causes
enlargement of the whole gland, which bulges back-
wards into the rectum. However, the central sulcus
is usually still there unless the gland is very large.
The gland may feel lobulated. The overlying rectal
mucosa remains uninvolved and mobile.
Carcinoma of the prostate may cause an irregu-
lar, hard enlargement which is often unilateral. The
edge of the enlarged area is indistinct.
If the tumour has spread out into the floor of the
pelvis, you will feel thickening either side of the
gland, which can sometimes encircle the rectum.
This lateral thickening is sometimes described as
‘winging’ of the prostate. The central sulcus may be
distorted or obliterated at an early stage of the disease
and the rectal mucosa fixed to the underlying gland.
When assessing the prostate, beware of the
incompletely emptied bladder, which pushes the
prostate downwards and makes it feel bigger than it
actually is.
SIGMOIDOSCOPY AND PROCTOSCOPY
In the hospital outpatient department, sigmoidos-
copy and proctoscopy, using simple rigid instru-
ments, have become part of the routine clinical
examination of every patient with bowel symptoms.
Sigmoidoscopy
The sigmoidoscope is basically a simple illuminated
tube, 20 or 30 cm in length, which is passed through
the anus to inspect the rectum and its lining. It has
an obturator with a rounded end to allow introduc-
tion, and a bellows attachment to allow insufflation
of air so that the rectum can be inflated and the
lining inspected. It should really be called a recto-
scope, but the term sigmoidoscope is invariably
used. It can usually be passed as far as the rectosig-
moid junction, but beyond this point most patients
experience significant discomfort.
Technique of rigid sigmoidoscopy
■
No bowel preparation is necessary.
■
Position the patient as for rectal examination,
making sure that they are lying as transversely as
possible on the couch, with their buttocks at the
edge or slightly overhanging. Elderly patients
may feel they are going to fall off, and need
reassurance.
■
Explain to the patient what you are going to do.
Tell them that they will experience discomfort
and a feeling of fullness as air is insufflated, that
you will release this pressure at the end to the
examination, and that you will stop at once if
there is any pain.
■
Inspect the anus to make sure there is no fissure
or other painful condition.
■
Warm the instrument, if it is metal, and apply
adequate amounts of lubricating jelly.
451
Smooth
Symmetrical
Median groove
Rubbery
Mobile mucosa
Smooth
Asymmetrical
Large
Median groove
Rubbery
Mobile mucosa
Irregular
Asymmetrical
Loss of median groove
Hard
Mucosa may be fixed
Lateral extension
Hypertrophic
Malignant
Normal
FIG 17.3
The prostate gland.
Chap-17.qxd 4/21/05 12:58AM Page 451
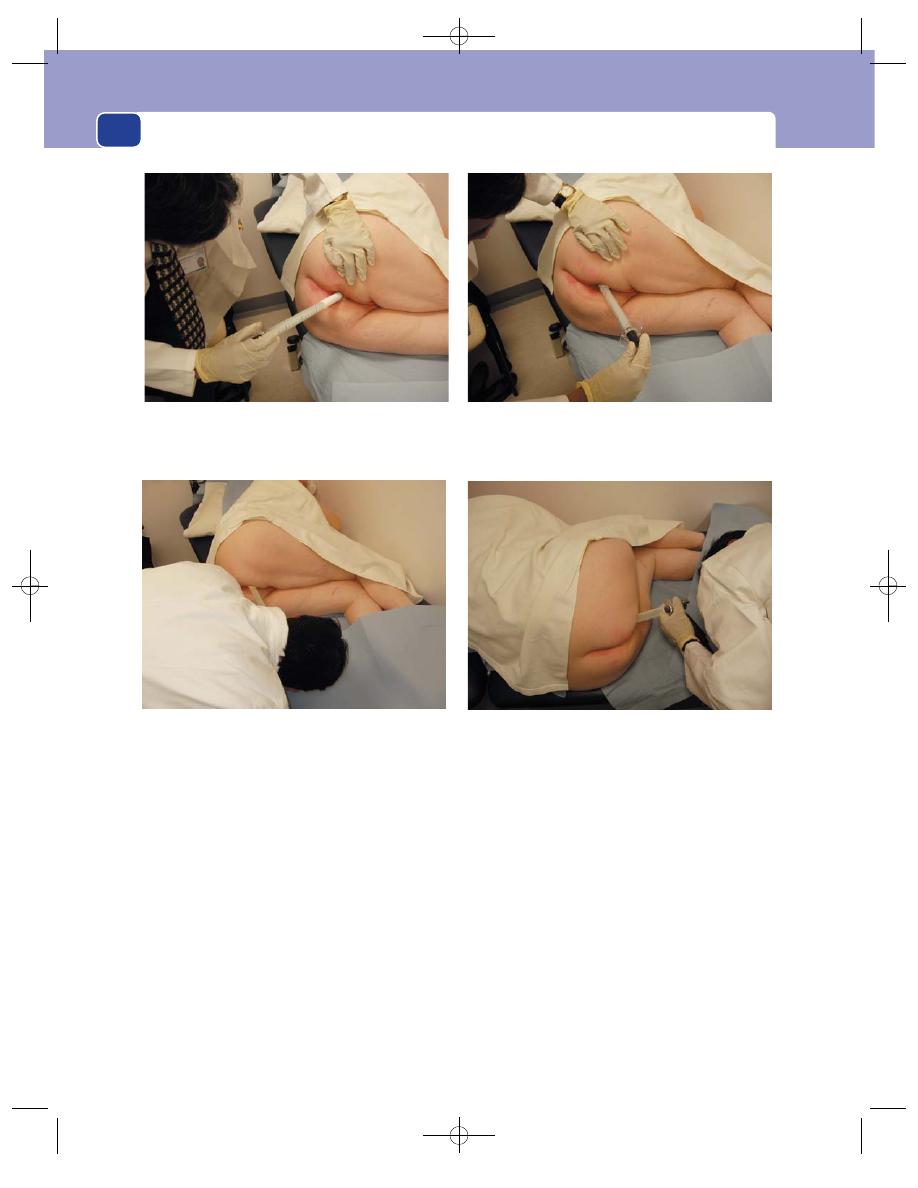
The rectum and anal canal
■
Insert the instrument in the direction of the
anal canal. This is achieved by pointing it
towards the umbilicus.
■
Once you have entered the rectum, remove the
obturator and attach the light source and
bellows. At this point, change the angle of
insertion backwards, to follow the course of the
rectum into the sacral hollow.
■
Under direct vision, insufflating enough air to
separate the rectal walls, negotiate the instrument
to the rectosigmoid junction. You will see and
work around the three semicircular folds known
as Houston’s valves. At the rectosigmoid junction
you will see the rectum narrowing down to the
diameter of the colon, which is normally smaller
than the calibre of the instrument you are using.
Do not attempt to go beyond this point in a
conscious patient, although you will occasionally
find a wide-open rectosigmoid junction, which
allows you to pass the instrument to its full length
without any problem.
■
Any gross pathology will be evident as soon as
you enter the rectum, but it is best first to
advance the sigmoidoscope to the rectosigmoid
junction, and inspect the contents and lining
during withdrawal.
■
There will be a variable amount of faecal
loading, but in most cases a reasonable
assessment of the rectum can be made. You must
note the character of the faeces. Are they solid or
452
Position the patient with the body as near transverse as
possible, with legs drawn up and buttocks at the edge of the
couch. Insert the well-lubricated instrument along the axis of
the anal canal by aiming it in the direction of the umbilicus.
Point the sigmoidoscope backwards to follow the course of
the rectum into the sacral hollow.
Under direct vision, insufflating air as you go, pass the
instrument up to the rectosigmoid junction.
FIG 17.4
SIGMOIDOSCOPY.
Carefully inspect the lining of the rectum as you withdraw the
instrument.
Chap-17.qxd 4/21/05 12:58AM Page 452
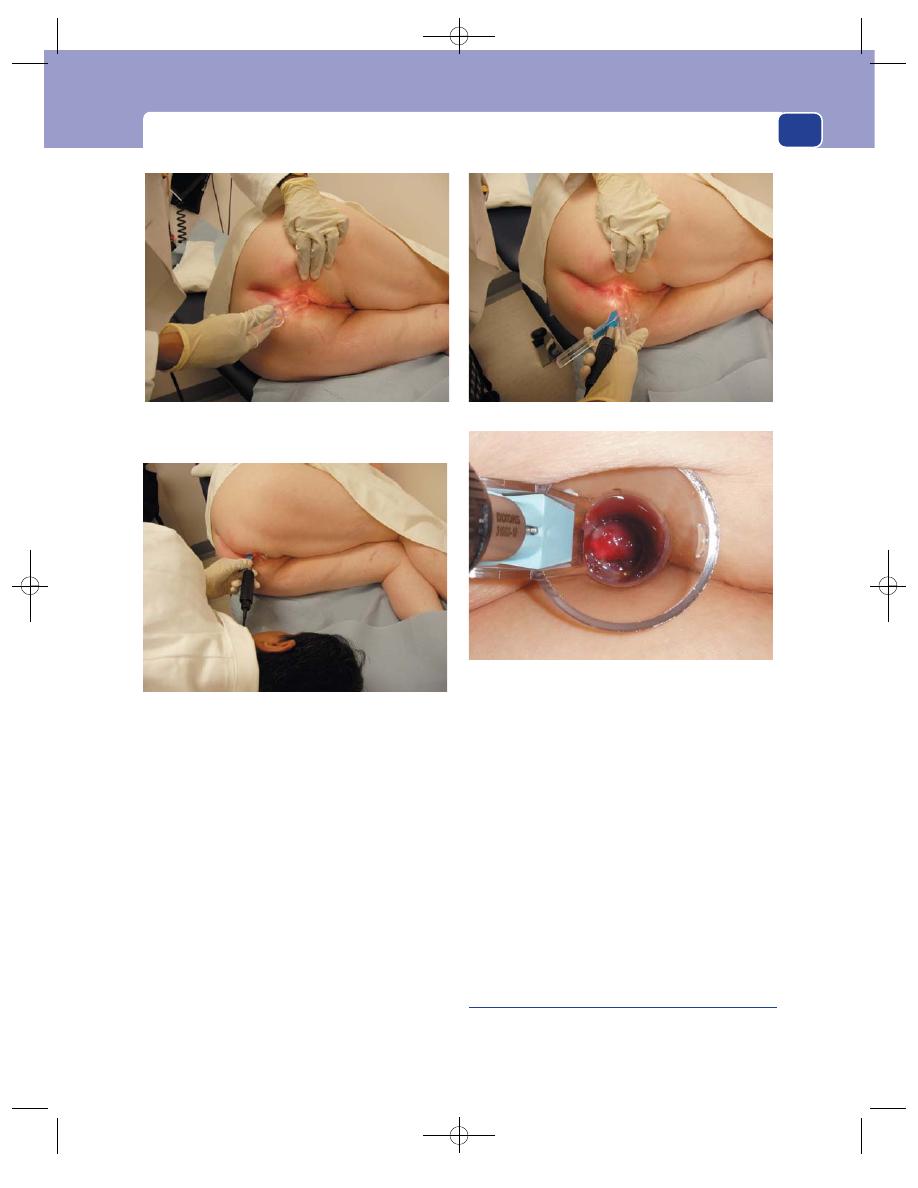
Sigmoidoscopy and proctoscopy
liquid? Is there any obvious blood or melaena? Is
there blood coming through the rectosigmoid
junction? Is there an excess of mucus?
■
Look at the whole of the rectal wall, searching
for tumours or polyps. Is the mucosa shiny,
smooth and the normal colour, or is it velvety,
granular and reddened as in proctitis?
■
Be careful to look at the posterior area just above
the anal canal. This is a potential blind spot on
sigmoidoscopy where it is easy to miss a small
lesion. (The same applies to rectal examination.)
■
When you have finished, make sure you release
all the air you have pumped in, and wipe away
any lubricating jelly around the anus.
■
Do not forget to add a digital examination.
Sigmoidoscopy will show you any pathology in
the lumen or wall of the rectum, but will not
show lesions outside the wall, or allow you to
assess any pelvic masses.
Sigmoidoscopy enables you to diagnose most
conditions of the rectum and some of the lower sig-
moid colon. Half of all colorectal cancers may be
seen with it.
Flexible sigmoidoscopy
Flexible fibre-optic instruments are increasingly
employed in specialized rectal clinics. Description
of their use is beyond the scope of this book. Bowel
preparation is required.
Proctoscopy
The proctoscope is a short illuminated tube,
employed to inspect the anal canal. Its principal use
453
FIG 17.5
PROCTOSCOPY.
Insert the proctoscope as you would the finger for a rectal
examination, obliquely and from behind, pulling backwards
against the puborectalis muscle.
Pass the instrument along the axis of the anal canal.
Inspect the anal canal as you slowly withdraw the proctoscope.
A large haemorrhoid will fall into the lumen of the proctoscope;
smaller ones just bulge over its end, an appearance that can
be enhanced by advancing the scope 5 mm.
Chap-17.qxd 4/21/05 12:58AM Page 453
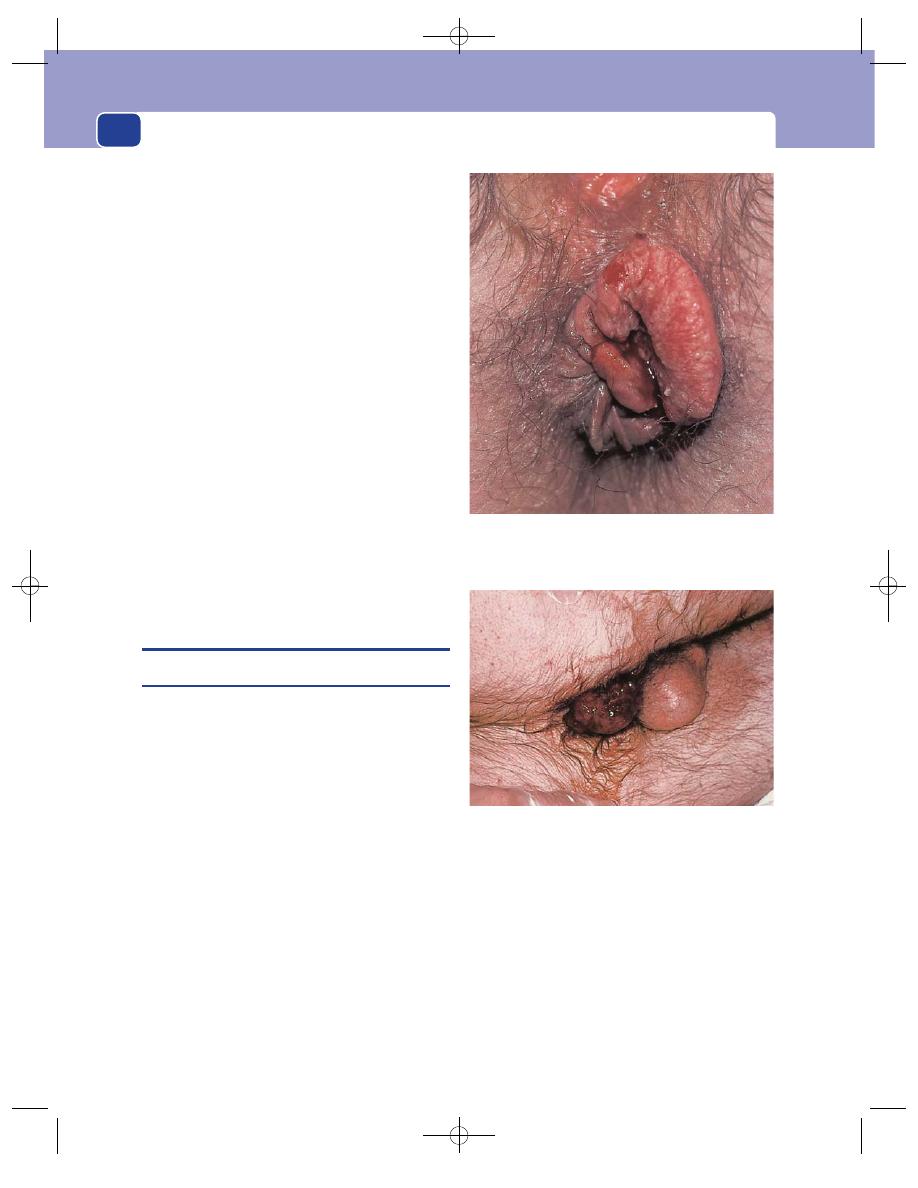
The rectum and anal canal
is for the diagnosis and treatment of haemorrhoids.
It should really be called an anoscope, but is always
called a proctoscope.
Technique of proctoscopy
■
Position the patient as for sigmoidoscopy.
■
No bowel preparation is necessary, and only
gross faecal loading will prevent adequate
assessment of the anal canal.
■
Make sure there is no painful external pathology
and prepare the patient generally as described
above.
■
Insert the instrument in the direction of the
anal canal, pointing at the patient’s umbilicus.
■
Remove the obturator and inspect the anal
canal as you withdraw the instrument.
If you suspect anal pathology, you will wish to
carry out a sigmoidoscopy in any event. Although the
anal canal may be inspected with the sigmoidoscope,
the view is not as good because of the greater length
of the instrument, so you will almost always need to
follow the sigmoidoscopy with a proctoscopy. Do
not forget to include a simple digital examination.
CONDITIONS PRESENTING WITH
RECTAL BLEEDING
Haemorrhoids
The anal canal contains three anal cushions, which
close it and help to provide an efficient gas- and
fluid-proof seal. If they enlarge, they can prolapse,
be damaged, bleed and even become pedunculated.
Such abnormal enlargements of the anal cushions
are called haemorrhoids. They consist of enlarged
congested patches of mucosa and submucosa.
Please note that they are not varicose veins! They
have no major vascular component other than the
normal small anal vessels, which are prominent on
their surface and in the submucosa.
If the condition is chronic, the process of pro-
lapse stretches the peri-anal skin below it, so that
the haemorrhoid is associated with an external skin
tag. The two together are sometimes termed a pile
mass. Skin tags may occur alone.
Doctors refer to haemorrhoids as ‘piles’, but the
general public use the term for any swelling near the
anus, and sometimes for anal pain. Remember this
when taking a history!
History
Age
Piles occur at all ages but are uncommon below
the age of 20 years. They are extremely rare in
children.
Symptoms
Uncomplicated piles do not cause pain.
The two common symptoms are bleeding and a pal-
pable lump or a sensation of prolapse after defaeca-
tion. They may also cause peri-anal discomfort and a
mucous discharge which leads to pruritus.
454
FIG 17.6
Third-degree (prolapsed) haemorrhoids. The
epithelium covering the 3 o’clock pile is becoming thick and
white. The 7 o’clock pile is bleeding.
FIG 17.7
Prolapsed, strangulated, thrombosed haemorrhoids.
Note the bloody serous discharge.
Chap-17.qxd 4/21/05 12:58AM Page 454
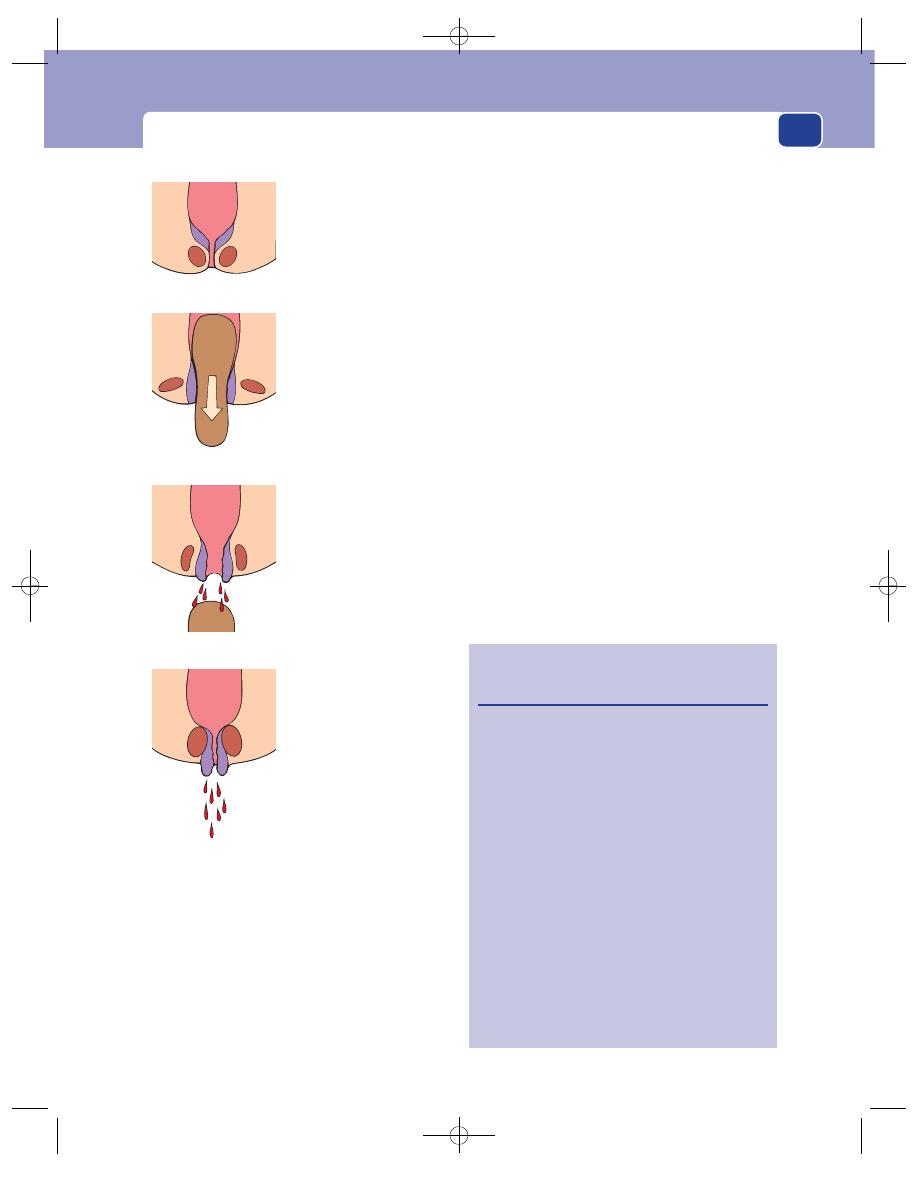
Conditions presenting with rectal bleeding
The bleeding, which is bright red, occurs after
defaecation. If it is a small quantity, it may just
streak the faeces or be noticed on the toilet paper. If
it is copious it may splash into the lavatory pan and
even cause iron-deficiency anaemia. Occasional
smears of blood on the lavatory paper are not
always abnormal. During normal defaecation there
is some degree of mucosal prolapse. If the patient
wipes vigorously, any protruding mucosa will bleed.
The patient notices the lump when cleaning after
defaecation. It may return to the rectum spontan-
eously or need to be pushed back. When the lump is
permanent, it may largely consist of the skin tag ele-
ment of the pile mass.
Pruritus is commonly associated with piles. It is
caused by exudation of mucus from the surface
mucosa leaking on to the peri-anal skin. This damp-
ness causes itching and maceration, which may
become secondarily infected.
Classification
Piles are categorized into three degrees
on the basis of the history:
■
first-degree piles bleed but do not prolapse,
■
second-degree piles prolapse but reduce
spontaneously,
■
third-degree piles prolapse and need reduction
or may not go back at all.
Although it is useful classifying piles in this way
as it helps decide the form of treatment, it is in some
ways an artificial classification. All piles are pro-
lapsed during defaecation and this is when they
bleed. If they return to their proper place when the
anal sphincter closes, they are never felt by the
455
The vascular pads
which become
haemorrhoids close
the anorectal junction.
During defaecation
the sphincter relaxes, the
anal canal everts and
the haemorrhoids are
compressed by the
faeces. The faeces
scratch the mucosa.
After the faeces have
passed, the haemorrhoids
are left scratched and
unsupported so they drip
blood onto the faeces.
If they do not retract
when the sphincter
begins to close, their
venous drainage is
obstructed and the
bleeding is made
worse so that it splashes
into the pan.
FIG 17.8
The way in which haemorrhoids are caused to bleed.
Revision panel 17.1
Diagnosis of conditions which present with
rectal bleeding
Bleeding but no pain
Blood mixed
=
Carcinoma of
with stool
colon*
Blood streaked
=
Carcinoma of
on stool
rectum*
Blood after
=
Haemorrhoids*
defaecation
Blood and
=
Colitis*
mucus
Blood alone
=
Diverticular
disease
Melaena
=
Peptic ulceration
Bleeding
=
Fissure
⫹ pain
(or carcinoma
of anal canal)
*Also proctitis caused by specific infections
(e.g. schistosomiasis).
Chap-17.qxd 4/21/05 12:58AM Page 455
The rectum and anal canal
patient and are therefore called first-degree piles.
Second-degree piles are vascular pads which remain
down below the sphincter when it contracts and
then return slowly but spontaneously, while third-
degree piles are so big and pendulous that they have
to be pushed back or are permanently down.
Cause
The incidence of haemorrhoids throughout
the world is inversely proportional to the stool vol-
ume, which depends on the amount of fibre in the
diet. They are rare in Africa, and common in the
industrialized developed nations. It is likely that
with lower stool volume there is more straining on
defaecation, which leads to elongation of the cush-
ions. Many patients with piles complain of straining
during defaecation. They commonly believe this is
the cause of their piles. However, some patients with
significant piles never have any difficulty defaecat-
ing and do not complain of straining at all.
Examination
First-degree and second-degree piles
First of all you
must examine the abdomen and then carry out an
external inspection of the anus and peri-anal skin
and perform a digital rectal examination.
You may see external skin tags.
All patients with rectal bleeding must then be
sigmoidoscoped. The history may be quite charac-
teristic of haemorrhoids, but you must make sure
there is no more serious pathology lurking in the
rectum. You may see the piles on sigmoidoscopy,
but you will then need to carry out a proctoscopy.
When a proctoscope is withdrawn through a
normal anal canal, the red-blue mucosa can be
seen collapsing over its end. Piles are darker, and
bulge so much that they protrude into the end of the
instrument. The multiple longitudinal corrugations
are lost and three deep clefts appear between the
bulging piles. The three usual places are at 3, 7
and 11 o’clock (with the patient in the lithotomy
position), the commonest sites of the three anal
cushions.
There is another classification of piles based on
the proctoscopic appearances which you must not
confuse with that which divides then into degrees,
given above.
■
Primary piles are those in the commonest
sites – 3, 7 and 11 o’clock.
■
Secondary piles are those seen at other
positions in the anal canal. They are usually
smaller and appear between the primary piles.
Do not confuse the two classifications.
Piles which are neither prolapsed nor thro-
mbosed cannot be felt on digital examination.
They are indistinguishable from normal mucosa.
Do not forget – you cannot diagnose haemorrhoids
with your finger.
Third-degree piles
. If you are fortunate (and the
patient unfortunate!) you may see the prolapsed
piles. They are bluish-purple swellings, usually
about 1 cm in diameter, in the 3, 7 and 11 o’clock
positions. Their distinguishing and diagnostic fea-
ture is their mucosal covering, recognized by its soft,
smooth, mucus-exuding surface.
Prolapsed piles are usually associated with skin
tags, which lie outside the true haemorrhoid.
If piles remain prolapsed, they ulcerate and
bleed. If the submucous veins thrombose, the pile
becomes tense, hard and oedematous. Palpation
and rectal examination in these circumstances are
painful and difficult because of spasm. Piles are
painful only when such complications occur.
However, you must not forget to do a sig-
moidoscopy and digital examination, if the patient
can tolerate it. There may be other rectal pathology.
The other common cause of a localized anal
swelling is a peri-anal haematoma. This lesion is
always covered by skin, which distinguishes it from
a mucosa-covered prolapsed haemorrhoid. It will
generally be exquisitely tender, more so than a pile.
Carcinoma of the rectum
Carcinoma of the rectum is diagnosed on the his-
tory, the findings on rectal examination and sigm-
oidoscopy and, finally, by biopsy.
Seventy-five per cent of carcinomata of the rec-
tum occur in the lower part of the rectal ampulla,
where they tend to be papilliferous or a simple ulcer
with an everted edge. The remaining 25 per cent are
in the upper part of the rectum and are often annu-
lar in shape. The pathology is the same, and the
shape reflects the diameter of the bowel and the pat-
tern of tumour necrosis.
About 90 per cent of rectal cancers can be felt
with the examining finger.
456
Chap-17.qxd 4/21/05 12:58AM Page 456
Conditions presenting with rectal bleeding
Every patient with any rectal complaint must
have a proper examination, either by sigmoidos-
copy or simple digital examination. You will be
considered negligent if you fail to perform a rectal
examination on a patient complaining of rectal
bleeding.
History
Age
Rectal carcinoma is common in middle and old
age but can occur in young adults.
Sex
It is equally common in both sexes.
Symptoms
Patients with rectal cancer usually have
multiple symptoms. One of the commonest is rectal
bleeding, usually a small amount of dark-red
blood streaked on the stool. Sometimes enough
blood accumulates in the rectum to be passed as
such without faeces, but this is uncommon.
The surface of the tumour produces mucus,
which may be reflected in progressively more liquid
motions, usually described as ‘diarrhoea’. Sometimes
the mucus pools, and is passed as liquid faeces. Any
patient complaining of ‘passing water through the
back passage’ usually has a rectal cancer (or villous
adenoma).
Paradoxically there may be a vague change in
bowel habit, usually towards constipation.
High cancers of the annular variety at the recto-
sigmoid junction may cause partial obstruction,
which presents as alternating episodes of diar-
rhoea and constipation. The constipation is caused
by the obstruction. The diarrhoea follows irritation
of the colon above the obstruction by the impacted
faeces, which gradually liquefy and, when they are
fluid, pass through the carcinomatous stenosis and
appear as diarrhoea.
Tenesmus occurs when a tumour in the lower
part of the rectum reaches a size large enough to be
mistaken by the patient’s rectal sensory mechanisms
for faeces. The patient has a persistent, sometimes
painful, desire to empty their rectum but cannot do
so, or just produces mucus, described usually as
‘slime’.
Weight loss is common, even if there has not
been distant spread.
Small primary lesions may be symptom-less but
associated with multiple metastases, particularly to
the liver. The patient presents with upper abdom-
inal pain and/or malaise, and has a palpable mass.
Pain is an uncommon symptom of carcinoma of
the rectum. There are three types:
■
colic, with distension and vomiting, caused by
high annular tumours obstructing the lumen of
the bowel;
■
local pain in the rectum, perineum or lower
abdomen, caused by direct spread of the
tumour to surrounding structures, especially
the sacral nerves;
■
pain on defaecation, which occurs if the tumour
has spread downwards below the mucocutaneous
junction into the sensitive anal canal. It can
mimic a fissure.
Previous history
Long-standing ulcerative colitis
increases the risk of malignant change in the colon
and rectum after 10 or more years of the disease.
Always ask about any previous large bowel symptoms,
particularly recurrent episodes of diarrhoea associ-
ated with the passage of mucus and blood. The fact
that the ulcerative colitis has been quiescent for many
years does not reduce the increased chance of malig-
nant change. In addition, the symptoms of a cancer
may be passed off as a recurrence of the colitis and
lead to late presentation.
Family history
Polyposis coli is a rare inherited condi-
tion in which the entire colon and rectum are car-
peted with adenomatous polyps, one or more of
which inevitably becomes malignant. It may also
arise sporadically. The family history may be denied
out of fear of cancer.
Examination
Rectal examination
There is usually nothing abnormal
to see around the anus, although occasionally a low
cancer may be visible, protruding through the anus.
In 90 per cent of cases the carcinoma is palpable
on digital examination of the rectum. What can
be felt depends upon the site of the lesion. If the
tumour is low in the ampulla, the finger can feel the
whole lesion. More commonly, only the lower edge
of a malignant ulcer is palpated.
A carcinomatous ulcer feels hard and bulges into
the lumen of the rectum. Its edge is usually everted
and its base is irregular and friable.
Try to decide if the tumour is fixed or mobile and
whether there is any local spread.
As you withdraw your finger, you will see blood
and mucus on the glove.
457
Chap-17.qxd 4/21/05 12:58AM Page 457
The rectum and anal canal
If the cancer is in the upper part of the rectum,
you may only be able to feel its lower edge. In these
circumstances it may be difficult to decide if the
lesion you are feeling is inside or outside the rec-
tum. This question is answered by sigmoidoscopy,
which should be carried out in all cases. Remember
also that rectal examination is not reliable in fat
patients, in whom you may hardly be able to insert
your fingertip further than the top of the anal canal.
General examination
By far the commonest site of dis-
tant metastases from rectal cancer is the liver, so you
must examine the abdomen carefully. Every patient
nowadays should have an ultrasound scan.
It is important to check all the other sites likely to
contain metastases, particularly the supraclavicular
lymph glands, the lungs and the skin.
Lung metastases are not uncommon but, as they
are small and peripheral, rarely produce symptoms
or physical signs. Chest radiography is therefore
mandatory.
Lymph from the rectum drains to the mesenteric
and then to the pre-aortic lymph glands. These
glands are rarely palpable. Meso-rectal glands are
occasionally palpable on rectal examination.
The inguinal lymph glands only become involved
when the tumour has spread below Hilton’s white
line to involve the skin. If the patient has palpable
inguinal lymph glands, the tumour is most likely to
be a squamous cell carcinoma of the anal skin.
Adenoma of the rectum
Benign neoplasms of the rectum are called adeno-
mata. They may be solitary or multiple throughout
the colon and rectum, rarely of the familial variety.
They adopt a polypoid form. The pathology is the
same wherever in the colon or rectum the tumour
arises, but the shape depends on the site. In narrow
parts of the bowel such as the sigmoid colon, peri-
stalsis draws the lesion out on a stalk. In the rectum,
the adenoma is usually sessile.
Initially the tumour is benign but, as time passes
and the lesion enlarges, dysplasia and malignant
change to invasive cancer occur. Malignant change
is unusual in a lesion smaller than 3 cm diameter,
but eventually it is likely that all true adenomata
turn into carcinomata.
The villous adenoma is a distinct variety of
rectal adenoma. It tends to occur in the elderly, is
solitary or multiple, and has a broad base with a
frondular (lots of villi) surface that exudes large
quantities of mucus. Growth is slow and the onset
of symptoms so gradual that presentation is often
late. Mucus is rich in potassium, and frail patients
with large villous adenomata may even present
with hypokalaemia. Malignant change at the base is
common.
History
Symptoms
A large adenoma produces a mucous dis-
charge and diarrhoea with a variable degree of
bleeding. A small adenoma may not alter the bowel
habit, but will occasionally bleed. When the lesion is
in the upper part of the anal canal it may also pro-
lapse, mimicking a haemorrhoid.
Examination
Adenomata are soft and often difficult to feel on
rectal examination. However, they will always be
visible on sigmoidoscopy. They are seen as small
polyps, but not all polyps in the rectum are truly
adenomatous. Metaplastic polyps are folds of nor-
mal mucosa which resemble small adenomata. Only
biopsy will confirm the diagnosis.
It is to be hoped that the student will now be
convinced that all patients with rectal bleeding
must be sigmoidoscoped. In most patients who
have cancer, there will usually be other symptoms.
However, by far the commonest cause of rectal
bleeding is piles, and it may be tempting to ignore a
single episode of bleeding, especially if there are no
other symptoms. But there may be an easily curable
adenoma, which will become a cancer if not
removed. Therefore all rectal bleeding must be taken
seriously and investigated with sigmoidoscopy.
Diverticular disease
Diverticular disease usually presents with chronic
left-sided abdominal pain and a change in bowel
habit, or acute abdominal symptoms (see Chapter
15). However, the disease may present with rectal
bleeding, hence its presence in this chapter.
The bleeding is typically acute, massive and
fresh. The usually elderly patient feels a little faint,
gets lower abdominal pain, and then has a desire to
defaecate. When they empty the rectum, they pass a
large volume of fresh blood and clots.
458
Chap-17.qxd 4/21/05 12:58AM Page 458
Conditions presenting with anal pain
This type of bleeding is a common reason for
emergency admission. Surprisingly, the patient is
rarely shocked and does not require transfusion. A
barium enema or colonoscopy is carried out and
diverticular disease is found.
Sometimes bleeding is seen to be coming from
an eroded artery in the mouth of a diverticulum.
However, in many patients, the diverticular disease
is incidental and the bleeding is caused by angiodys-
plasia of the colonic mucosa. Surgery is very rarely
needed.
CONDITIONS PRESENTING WITH
ANAL PAIN
Peri-anal haematoma
The name of this condition is well established, even
though it is not a true haematoma but a thrombosis
of a vein in the subcutaneous plexus. There is not
usually any precipitating factor, but there is prob-
ably some injury to the vein wall during the anal
stretching that occurs with defaecation.
The condition also occurs after childbirth, fol-
lowing the straining and stretching of the perineum
during the second stage of labour.
The thrombus causes a surrounding inflamma-
tory reaction of pain and oedema.
History
Age and sex
Peri-anal haematomata occur at all ages
and are equally common in both sexes.
Symptoms
The dominant symptom is pain, which
begins gradually, increases in severity over a few
hours and then subsides gradually over a few days. It
is a continuous discomfort, made worse by sitting,
moving and defaecation, and it is clearly localized to
the lump.
The swelling appears at the same time as the
pain. At first it is small and spherical, but it may
gradually enlarge and become more painful.
Bleeding occurs if the lump bursts through the
skin or if the skin over the lump ulcerates.
The patient often notices that the peri-anal skin is
moist and itchy. This is caused by leakage of mucus
as the swelling prevents the anus closing properly.
Peri-anal haematomata are occasionally multiple
and may be recurrent.
Cause
The patient may remember that the symp-
toms began after an uncomfortable episode of defae-
cation, but as the haematoma may take a few hours
to form, the connection is not always obvious.
Patients always think that they have an attack of
‘piles’. Do not be misled by this belief: peri-anal
haematomata are not piles in the medical sense of
the term.
Examination
Position
The lump may be anywhere around the anal
margin. More than one may be present.
Colour
When it is close to the skin and the skin is not
oedematous, the lump has a deep red-purple colour.
If the skin becomes oedematous, the redness of the
underlying blood clot cannot be seen.
Tenderness
The lump is tender, but disproportion-
ately less than you would expect from the pain felt
by the patient, which is due to tension rather like an
abscess. It is very tender if it becomes oedematous
and ulcerated.
Shape and size
The initial lump is spherical, and up
to 1cm in diameter. If the anal skin is lax, the lump
may become polypoid. This also happens when it
becomes oedematous.
459
Revision panel 17.2
Diagnosis of anal conditions which present
with pain
Pain alone
Fissure (pain after defaecation)
Proctalgia fugax (pain spontaneously
at night)
Anorectal abscess
Pain and bleeding
Fissure
Pain and a lump
Peri-anal haematoma
Anorectal abscess
Pain, a lump and bleeding
Prolapsed haemorrhoids
Carcinoma of the anal canal
Prolapsed rectal polyp or carcinoma
Prolapsed rectum
Chap-17.qxd 4/21/05 12:58AM Page 459
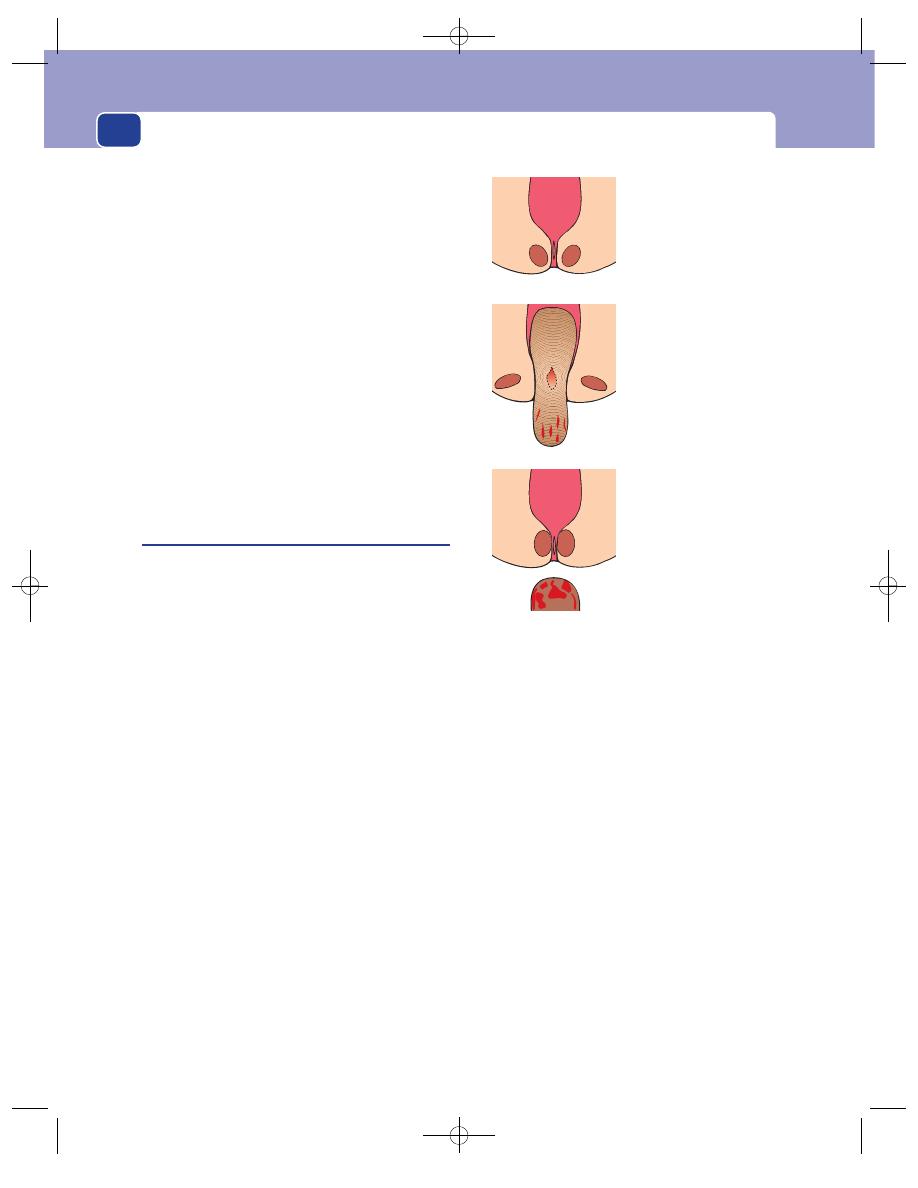
The rectum and anal canal
Surface
Peri-anal haematomata are covered by skin,
which may be normal or oedematous but is always
clearly recognizable as skin. The surface of the lump
beneath the skin is smooth.
Composition
The central lump can be felt as a solid,
hard, hemispherical mass.
Relations
The mass is under the peri-anal skin, and
superficial to the external sphincter. It is not fixed to
the skin or the deep structures and cannot be
reduced into the anal canal.
State of local tissues
The remainder of the anal skin
and anal canal are usually normal, but there may be
a palpable cord running up the anal canal from the
haematoma. This is probably caused by further
thrombosis in the vein that has been injured.
Lymph drainage
The inguinal glands will not be
enlarged.
Fissure-in-ano
An anal fissure is a longitudinal split in the skin of
the anal canal.
An acute tear is quite a common event and usually
heals quickly. Re-opening of the tear when the patient
next defaecates will cause further pain, which in turn
causes an increase in anal sphincter tone which pro-
gresses to spasm. This makes the tear more likely to
re-open at each subsequent episode of defaecation,
and leads to a vicious circle of tearing–pain–spasm
and more tearing. The base then becomes fibrous and
does not heal. It is, in fact, a chronic ulcer.
History
Age
Acute fissures are quite common in children,
who often pass bulky stools very quickly.
Chronic fissures are most common in patients
between the ages of 20 and 40 years. They frequently
begin in women after childbirth.
Sex
Fissure-in-ano is a little more common in men
than in women.
Symptoms
Both acute and chronic fissures are very
painful. The pain begins during defaecation and is
often described as tearing, which of course it is. It
persists for minutes or hours after defaecation and
is throbbing or aching in nature. It can be so severe
that the patient becomes afraid to defaecate. This
results in the development of large, hard masses of
faeces, which make the pain worse when the next
defaecation occurs.
The patient will also find that it is more difficult
to pass a stool, because of the spasm.
Acute fissures may bleed sufficiently to streak
the stool with blood and stain the toilet paper.
Chronic fissures bleed less and usually produce just
a little bloodstaining of the toilet paper, if that.
When parents notice bleeding in children, it
causes great alarm. The child rarely complains of
the pain, unless questioned directly.
A small skin tag (called a sentinel tag or some-
times a sentinel pile), which the patient may be able
to feel, may form at the lower end of a chronic fissure.
Some patients complain of ‘constipation’, by
which they mean that they pass hard stools associ-
ated with pain and aching. Remember that ‘consti-
pation’ (and ‘diarrhoea’) has many meanings to the
layman.
Pruritus may be the presenting symptom of a
chronic fissure. The fibrosis around the ulcer pre-
vents a good seal, and small amounts of mucus leak
460
The split in the anal
canal is closed when
the anal canal is shut.
The fissure is painful so
the sphincter closes
tightly. Any blood
remaining on the
perianal skin will be
wiped away on the
toilet paper.
Faeces split open the
fissure as they pass it
and make it bleed;
they become
streaked with blood.
FIG 17.9
The way in which a fissure is caused to bleed.
Chap-17.qxd 4/21/05 12:58AM Page 460
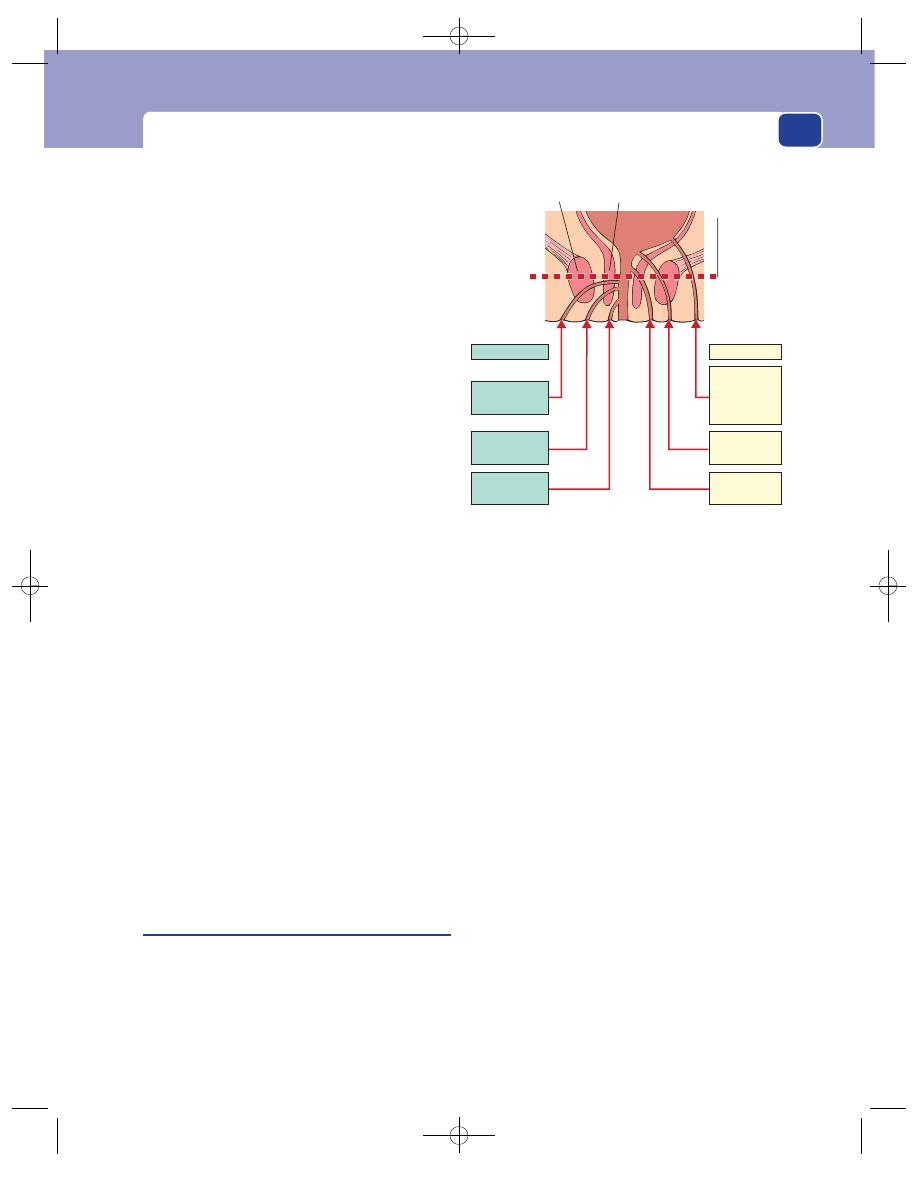
Conditions presenting with anal pain
on to the peri-anal skin and set up a reaction, which
is itchy. The same thing may happen with piles.
Persistence
The symptoms of a fissure are slow to
develop and become long-standing. There may be
periods of remission, and eventually the condition
either heals or becomes so chronic that the patient
lives with the discomfort. Many patients suffer for
months before going to see their doctor.
Cause
The patients either believe that their symp-
toms are caused by constipation or think that their
distressing pain must indicate some dreadful, incur-
able disease. In fact, the cause is unknown.
Examination
Position
The majority of fissures are in the mid-line
posteriorly, but some are anterior and a few are lateral.
The diagnosis is made by gently parting the skin
of the anus and looking for a split in the anal skin.
This may be all that you will be allowed to do,
because further examination is often prevented by
pain.
Tenderness
The anal sphincter is usually in spasm,
and any attempt to open it by firm traction on the
buttocks or inserting a finger into the rectum is
exquisitely painful. In these circumstances rectal
examination is contraindicated.
Rectal examination
If the pain and tenderness are not
severe, you may be able to perform a careful rectal
examination and feel the defect in the anal canal
skin and some surrounding induration. There will
often be a streak of fresh blood on the glove when
the finger is withdrawn.
Sigmoidoscopy and proctoscopy
Never attempt either
of these examinations in a conscious patient with
a fissure – they are much too painful. When these
examinations are carried out under anaesthetic, the
raw base of the fissure will be seen as the instrument
is withdrawn through the anal canal.
Fistula-in-ano
A fistula is a track, lined with epithelium or granu-
lation tissue, connecting two epithelial surfaces. It
may connect two body cavities or one cavity and the
body’s external surface.
A fistula-in-ano connects the lumen of the rectum
or anal canal with the external surface. It is usually
lined with granulation tissue. In most instances it is
caused by an abscess in the inter-sphincteric space
bursting in two directions – internally into the anal
canal, and externally into the skin.
Fistulae-in-ano may also be associated with
inflammatory bowel conditions, typically Crohn’s
disease. Rarely, a fistula is caused by direct infiltra-
tion and necrosis of a low rectal carcinoma.
Classification
Fistulae-in-ano can run through a
variety of anatomical planes, illustrated in Figure
17.10. The important distinction is between low-
level and high-level fistulae, as the surgical manage-
ment is completely different.
A low-level fistula has its internal opening below
the anorectal ring, the point where the puborectalis
muscle sling fuses with the external sphincter. The
anorectal ring is the major muscle involved in main-
taining continence. A fistula which is below this level
may be laid open without impairing continence.
A high-level fistula joins the rectum above the
anorectal ring. Laying this open would divide the
ring and make the patient incontinent. More com-
plex surgical procedures are required.
History
Age
Fistula-in-ano can occur at any time during
adult life. It is occasionally seen in children.
461
Trans
sphincteric
Extra
sphincteric
(pelvirectal
supralevator)
Low
High
Level of
anorectal
ring
External
sphincter
Internal
sphincter
Trans
sphincteric
Inter
sphincteric
Inter
sphincteric
Subcutaneous
or submucous
FIG 17.10
The varieties of fistula-in-ano.
Chap-17.qxd 4/21/05 12:58AM Page 461
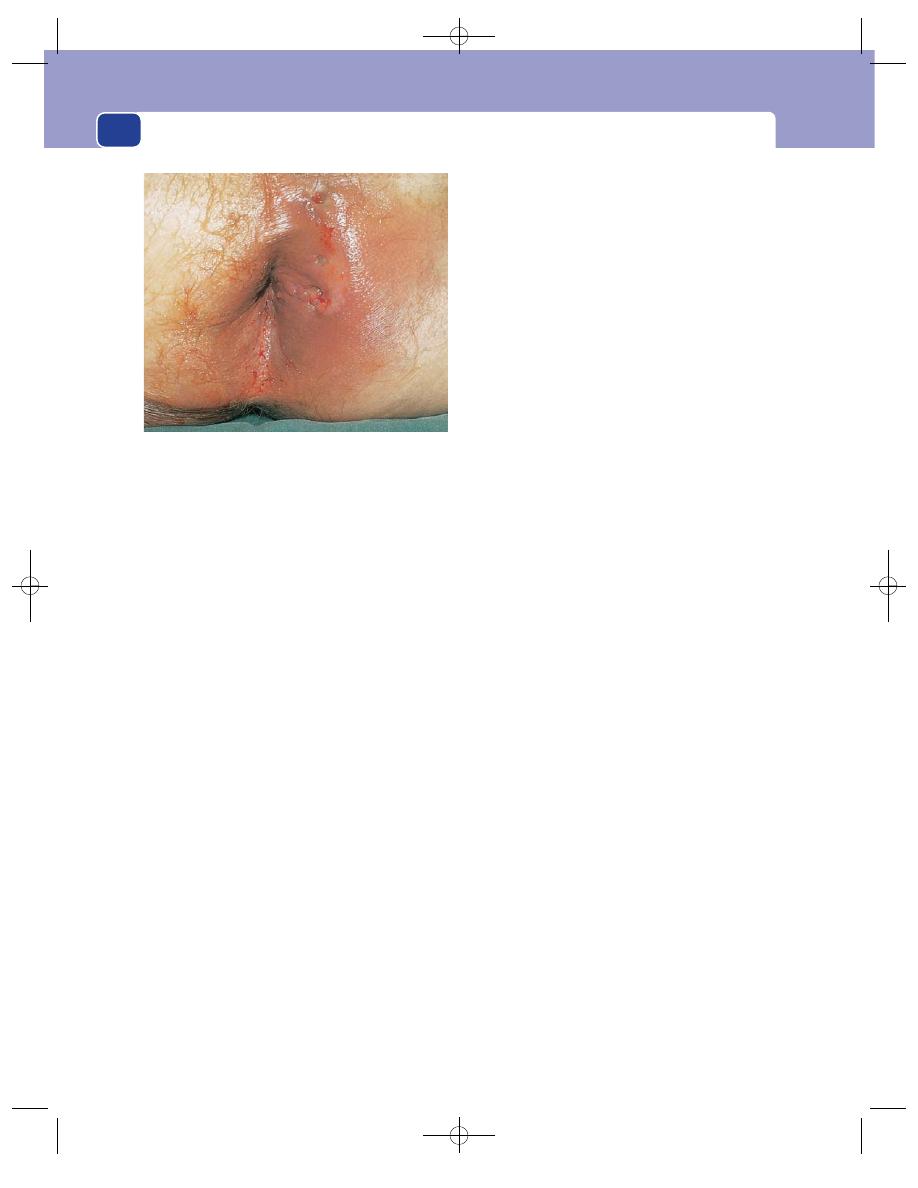
The rectum and anal canal
Symptoms
There may be a history of a peri-anal
abscess, which bursts spontaneously, followed by
the other symptoms. The abscess may also have
been drained surgically. However, many patients
with a fistula do not give a history of an abscess.
The commonest symptom is a watery or puru-
lent discharge from the external opening of the fis-
tula. The patient occasionally notices bubbling on
defaecation, as mucus is forced through the fistula
as the anal canal is stretched over the stool. This
forcing of mucus through the fistulous tract is the
mechanism that stops a fistula from ever healing.
There may be recurrent episodes of pain if the
centre of the fistula fills with pus. If the pus does not
discharge down the fistula, the pain becomes intense
and throbbing. There may be a story of the fistula
apparently healing but then becoming painful and
discharging again, with relief of the discomfort.
The discharge makes the peri-anal skin wet and
macerated and causes pruritus ani.
There is not usually any difficulty with defaeca-
tion, but there may be minor bleeding from the
external opening.
Persistence
The symptoms may be episodic as the
degree of infection in the fistula varies, but the con-
dition hardly ever cures itself, for the reasons given
above.
Other symptoms (direct questions)
The commonest
associated condition is Crohn’s disease, and it is
important to enquire about any bowel or abdominal
symptoms or systemic upset. Curiously, the fistulae
(commonly multiple) associated with this condi-
tion tend to be painless.
Examination
Position
The external opening of the fistula will be vis-
ible as a puckered scar or a small tuft of granulation
tissue anywhere around the anus, usually close to the
anal margin, but sometimes several centimetres away.
Goodsall’s rule states that the internal opening of
an anterior fistula lies along a radial line drawn
from the external opening to the anus, whereas the
internal opening of a posterior fistula lies in the
mid-line posteriorly. Although things are rarely cer-
tain in medicine, this rule is reliable.
There may be more than one opening, particu-
larly if the patient has Crohn’s disease.
Tenderness
The opening of the fistula is not tender,
but the tissues around it may be thickened and pal-
pation produces discomfort.
Discharge
The discharge, which can be serous or
purulent, may be visible on the skin.
Rectal examination
Rectal examination is not painful.
The internal opening of the fistula can often be felt
as an area of induration or a small nodule under the
mucosa. Two-thirds are posterior, one-third anter-
ior. Feel the anorectal ring and try to decide if the
internal opening of the fistula is below or above it,
i.e. at the low level or high level.
The indurated track of the fistula between the
internal and external openings will usually be palp-
able. If you cannot detect it by simply feeling with
the fingertip, bimanual examination may succeed.
Place your index finger in the rectum, and your
thumb (or a finger of the other hand) on the peri-
anal skin.
Take care to perform a careful rectal examin-
ation. Look for other diseases, such as a carcinoma,
which might be the cause of the fistula.
Sigmoidoscopy and proctoscopy are essential to
exclude underlying diseases such as Crohn’s disease,
carcinoma and even tuberculosis. Disappointingly,
the internal opening of the fistula, though palpable,
is rarely visible.
Local lymph glands
The inguinal lymph glands, which
receive lymph from the anal canal, should not be
enlarged unless the fistula is acutely inflamed or sec-
ondary to an infiltrating carcinoma.
462
FIG 17.11
Fistula-in-ano. There are multiple openings
behind and to the left of the anus. Although the opening
looks as if it is healing, there is a track leading through the
muscles to the anal canal.
Chap-17.qxd 4/21/05 12:58AM Page 462
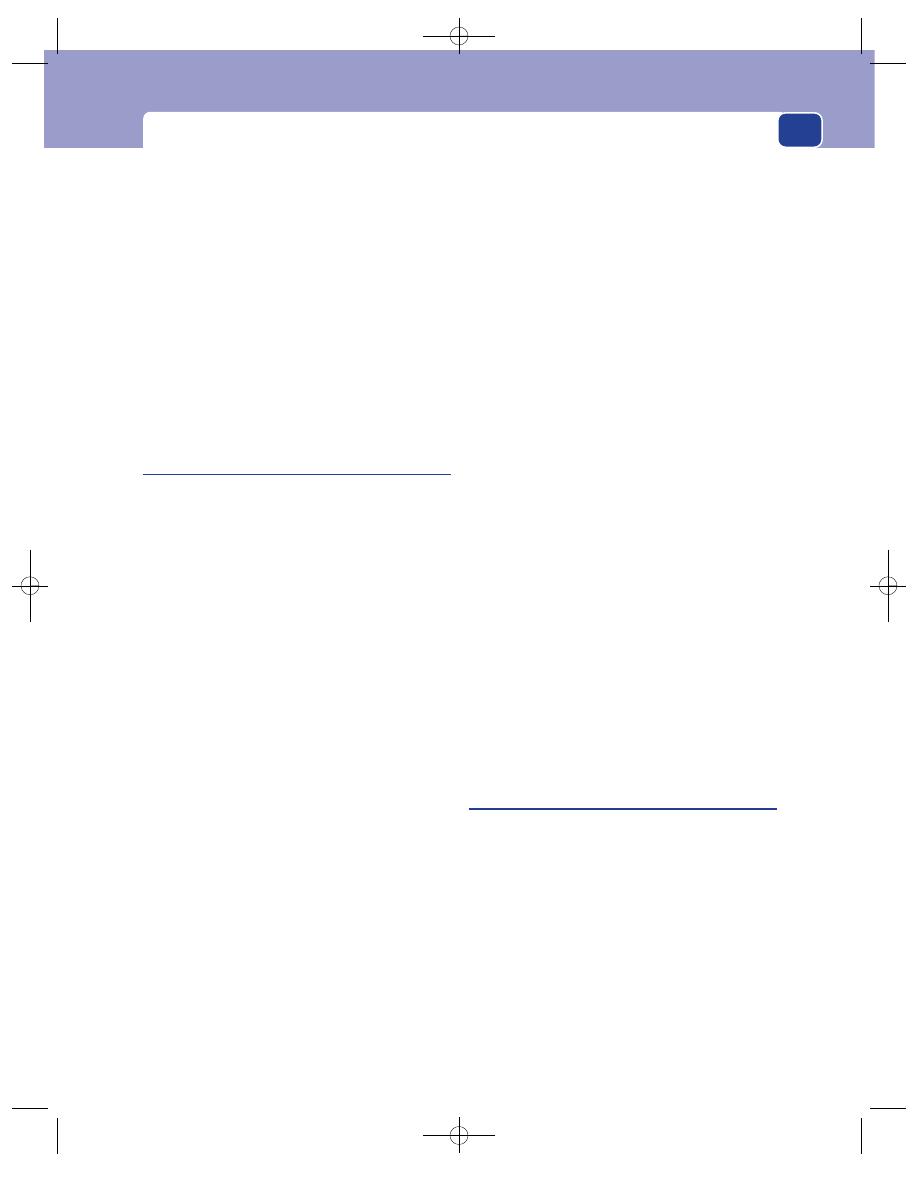
Conditions presenting with anal pain
State of local tissues
It cannot be repeated too often
that the anus and rectum must be carefully exam-
ined to exclude serious causes of the fistula. If the
fistula was caused solely by a simple peri-anal
abscess, the rest of the anus and rectum is likely to
be normal.
General examination
Many of the diseases mentioned
above may have associated abdominal and general
clinical signs, so never confine your examination to
the patient’s perineum.
Please note that in patients with Crohn’s disease
and an anal fistula, the primary bowel disease is
likely to be in the terminal ileum, not the rectum.
Examine the abdomen carefully.
Anorectal abscess
The term peri-anal abscess is widely used to
describe any abscess in the anorectal region. There
are, however, two distinct varieties. In the true peri-
anal abscess, the swelling is clearly at the anal mar-
gin, which it distorts. The ischiorectal abscess lies
lateral to the anus and occupies a much larger space.
The infection probably begins in an anal gland,
from which pus either tracks down to the perineum
between the sphincters to form a peri-anal abscess,
or penetrates the external sphincter to reach the
ischiorectal fossa. If the abscess is drained externally,
or bursts quickly, the anal gland is usually destroyed,
but if it continues to secrete, a fistula will develop.
History
Age
Anorectal abscess is commonest in patients
between 20 and 50 years old, but occurs at all ages
and, rarely, in children.
Sex
It is seen more often in men than in women.
Symptoms
The main symptom is a severe, throb-
bing pain which makes sitting, moving and defae-
cation difficult and is exacerbated by them all.
The patient may have felt a tender swelling close
to the anus.
Systemic effects
The general symptoms of an abscess –
malaise, loss of appetite, sweating and even rigors –
may be present. A patient with an ischiorectal
abscess is more likely to be systemically unwell, as
there is a large space to fill up with pus. Pain and
tenderness are greater with a peri-anal abscess, as
the space in which it can expand is more confined.
Examination
Position
The painful area over an ischiorectal abscess
is lateral to the anus in the soft tissues between the
anus and the ischial tuberosity. A peri-anal abscess
may be anywhere around the anal margin. It is not
always possible to decide which sort of abscess it is,
as the landmarks cannot be detected.
Tenderness
The whole area is exquisitely tender.
Colour and temperature
The overlying skin eventually
becomes hot and red, but the abscess has to be quite
big before these skin changes appear. A small
abscess may be very painful, with a lot of tender-
ness, but little to see externally.
Shape, size and composition
It is not possible to define
the features of the mass. Its surface is indistinct. Its
size can be crudely assessed by very gentle palpa-
tion. It will be far too tender to test for fluctuation.
Rectal examination
This is possible but very unkind,
and is best deferred until the patient is anaes-
thetized prior to drainage. The abscess may bulge
into the side of the lower part of the rectum, and the
rectum on the side of the abscess feels hot.
Lymph drainage
The inguinal lymph glands are some-
times enlarged and tender.
Local tissues. The nearby structures – the anus,
the rectum and the contents of the pelvis – may
show evidence of previous abscesses and fistulae,
such as scars and sinuses.
General examination
The patient tries not to move and
lies on their side. There is likely to be tachycardia,
pyrexia, sweating, a dry, furred tongue and foetor oris.
Pilonidal sinus
The word pilonidal means a nest of hairs. A
pilonidal sinus is a sinus that contains a tuft of hairs.
However, the condition can occur without hairs
ever being demonstrated.
These sinuses are commonly found in the mid-
line skin covering the sacrum and coccyx. They have
been found elsewhere, sometimes between the fin-
gers in hairdressers, and at the umbilicus.
There is a long-standing, unresolved argument
about the cause of the disease and the source of the
hairs. A pilonidal sinus is lined by granulation tissue
and not skin and there are no hairs growing within it.
In fact, the hairs in the sinus are short, broken pieces
of hair that often come from the scalp. A reasonable
463
Chap-17.qxd 4/21/05 12:58AM Page 463
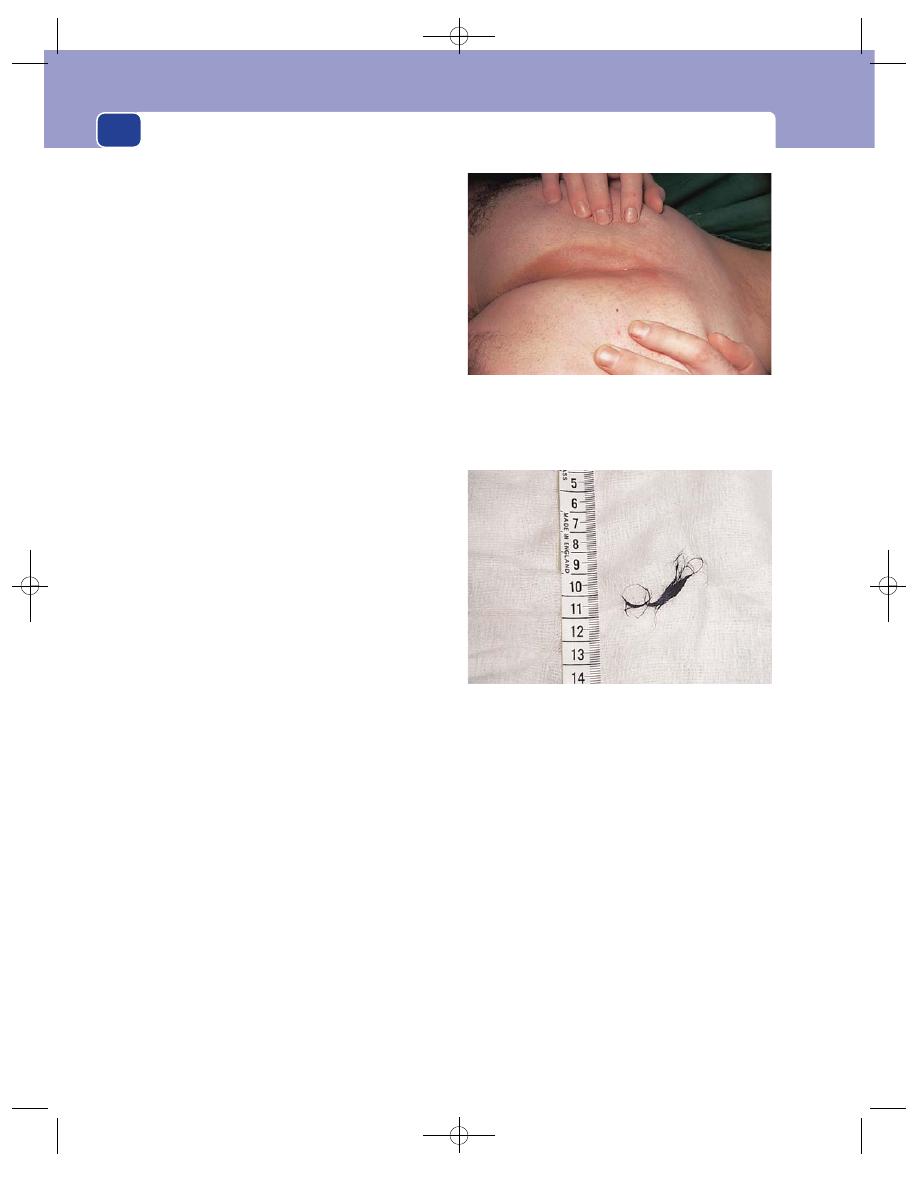
The rectum and anal canal
theory of the aetiology of pilonidal sinus is that the
mid-line skin in the buttock cleft is tethered to the
periosteum of the bone. In walking, the motion of
the buttocks on either side results in hairs getting
sucked into a pre-existing dimple in the skin or actu-
ally piercing the normal skin. They then act as foreign
bodies and cause chronic infection. The end-result is
a chronic abscess which contains hair and which
flares up at frequent intervals into an acute abscess.
History
Age
Pilonidal sinus is rare before puberty and in
people over 30 years of age. This suggests that it is a
self-limiting condition. Perhaps the strength of the
hairs and the likelihood of their pricking into the
skin varies with age.
Sex
It is more common in men than in women, and
classically, but by no means always, in dark-haired,
hirsute men.
Symptoms
The common symptoms are pain and a
discharge, which develop when an abscess forms in
the sinus tract. The pain may vary from a dull ache
to an acute throbbing pain, and the discharge will
vary from a little serum to a sudden gush of pus. An
acute abscess may be the first sign of the disease.
In between the acute exacerbations the sinus
produces few symptoms and patients often think it
has disappeared.
The acute exacerbations occur at irregular inter-
vals. If a sinus becomes chronically inflamed, it may
discharge continually.
Examination
Position
A pilonidal sinus is sometimes misdiag-
nosed as an anal fistula because of its proximity to
the anus. However, on careful inspection the diag-
nosis will become clear, because pilonidal sinuses
are always in the mid-line of the natal cleft and lie
over the lowest part of the sacrum and coccyx. The
opening of a fistula can be anywhere around the anus.
Also, it is very rare for a pilonidal sinus or abscess to
be closer to the anus than to the tip of the coccyx.
There may be one or many sinuses, some with a
smooth epithelialized edge, others with a puckered
scarred edge and some with pouting granulation
tissue. The last are usually those sinuses that are dis-
charging pus, and the orifices of the most recent
abscesses.
Temperature and tenderness
The skin around a pilonidal
sinus is normal except when the sinus is acutely
infected, when it becomes red and tender.
The sinus
The actual sinus openings are usually easy to
see as small mid-line pits with epithelialized edges.
You may be able to see protruding hairs. Gentle pres-
sure may produce a small quantity of serous dis-
charge and reveal more hair.
When a sinus is infected it becomes indistinguish-
able from any other form of subcutaneous abscess.
The pits will rarely be visible in the oedematous
skin. A patient with a pilonidal abscess finds some
relief from the throbbing pain by lying prone, in
contrast to patients with anorectal abscesses who
usually prefer to lie on their side.
Palpation of the skin and subcutaneous tissues
around the sinus reveals areas of subcutaneous
464
The hairs that were removed from the sinus shown above.
FIG 17.12
PILONIDAL SINUS.
The patient is lying on his right side with his buttocks held
apart to expose the bottom of the natal cleft. The sinus, which
is difficult to see, is the small, pale, central pit. The stiff black
hair that commonly covers the buttocks of these patients has
been shaved off.
Chap-17.qxd 4/21/05 12:58AM Page 464
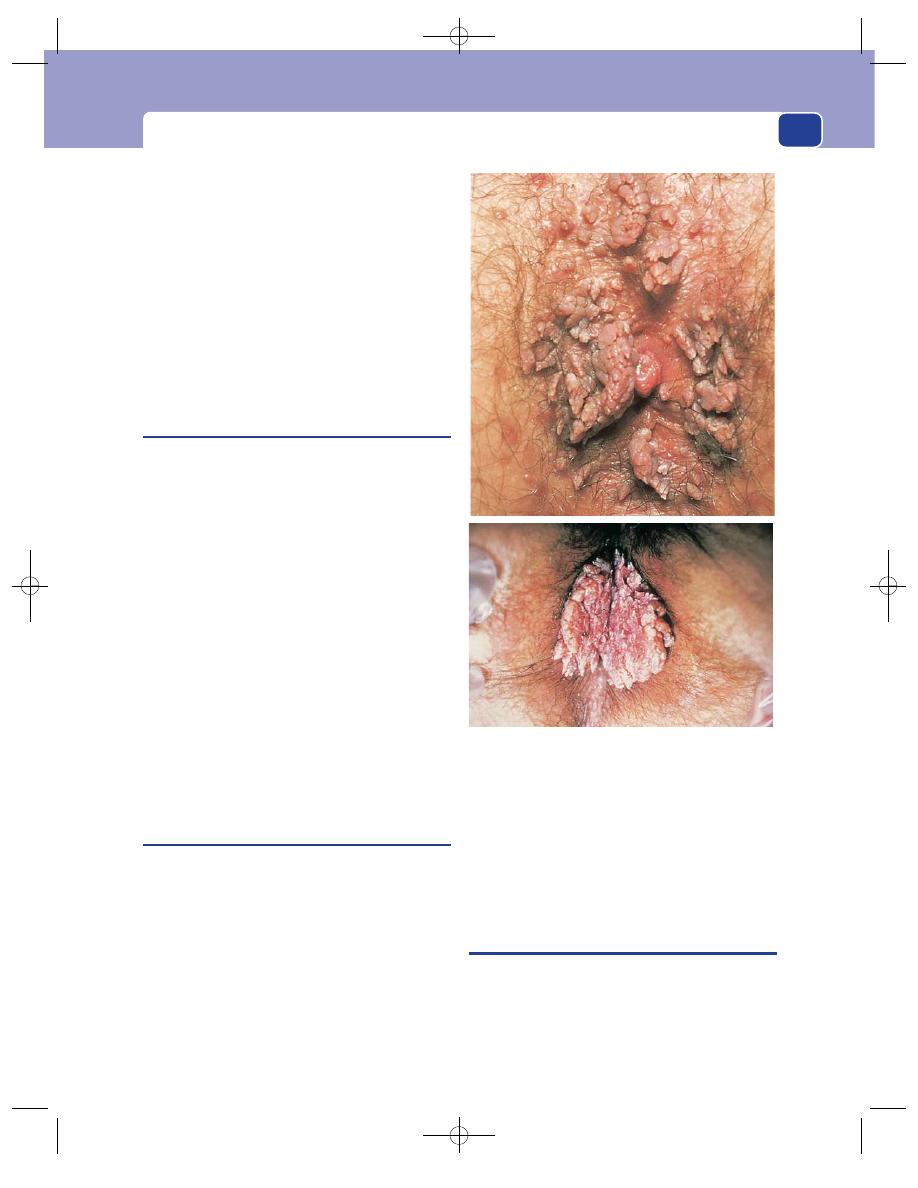
Conditions presenting as an anal lump with or without pain
induration, which correspond to the ramifications
of the sinus beneath the skin. There may be scars
well away from the mid-line, as high as the first
sacral vertebra, where previous abscesses have dis-
charged or been incised.
Lymph drainage
The inguinal lymph glands do not
enlarge, because the infection is mostly mild and
chronic.
Local tissues
The underlying sacrum, the skin of the
perineum, the anal canal and the ischiorectal fossae
should be normal.
Anal warts
(Condylomata acuminata)
Peri-anal warts (usually called simply anal warts)
are multiple, pedunculated, papilliferous lesions
which are easy to recognize as they resemble warts
anywhere else in the body. They may spread over the
whole perineum, including the labia majora and the
back of the scrotum.
They are caused by a virus and can be transmit-
ted by sexual contact. Consequently they are often,
but by no means always, associated with sexually
transmitted diseases.
They are also seen in patients whose immune
response has been depressed with steroids or cancer
chemotherapy, and in acquired immunodeficiency
syndrome (AIDS).
Condylomata lata are a manifestation of secondary
syphilis, but are broad-based, flat-topped papules
which are highly contagious.
All condylomata cause irritation, discomfort and
pain from rubbing, and may ulcerate and become
infected.
Proctalgia fugax
This condition is probably caused by a spontaneous
spasm (cramp) in the muscles of the pelvic floor or,
possibly, by a spasm at the rectosigmoid junction. It
is often associated with the irritable bowel syndrome.
It is mentioned here because the patient presents
complaining of severe rectal pain.
The pain comes on suddenly, often at night, is
severe, cramp-like and felt deep inside the true pelvis.
The site is described as a couple of inches inside
the anus. The duration is short, sometimes just a few
seconds and rarely longer than 5 minutes. Nothing
relieves it and it passes off spontaneously. There may
be other symptoms of functional bowel disorder.
General and rectal examination are normal, but
on sigmoidoscopy, as air is insufflated at the recto-
sigmoid junction, the patient may experience a
similar pain.
CONDITIONS PRESENTING AS AN ANAL
LUMP WITH OR WITHOUT PAIN
A number of the conditions already described pres-
ent with pain and a lump, but in the majority the
pain is the dominant symptom. The following
conditions are not necessarily painless, but the
lump is the dominant symptom.
465
FIG 17.13
Two examples of multiple perianal warts
(condylomata).
Chap-17.qxd 4/21/05 12:58AM Page 465
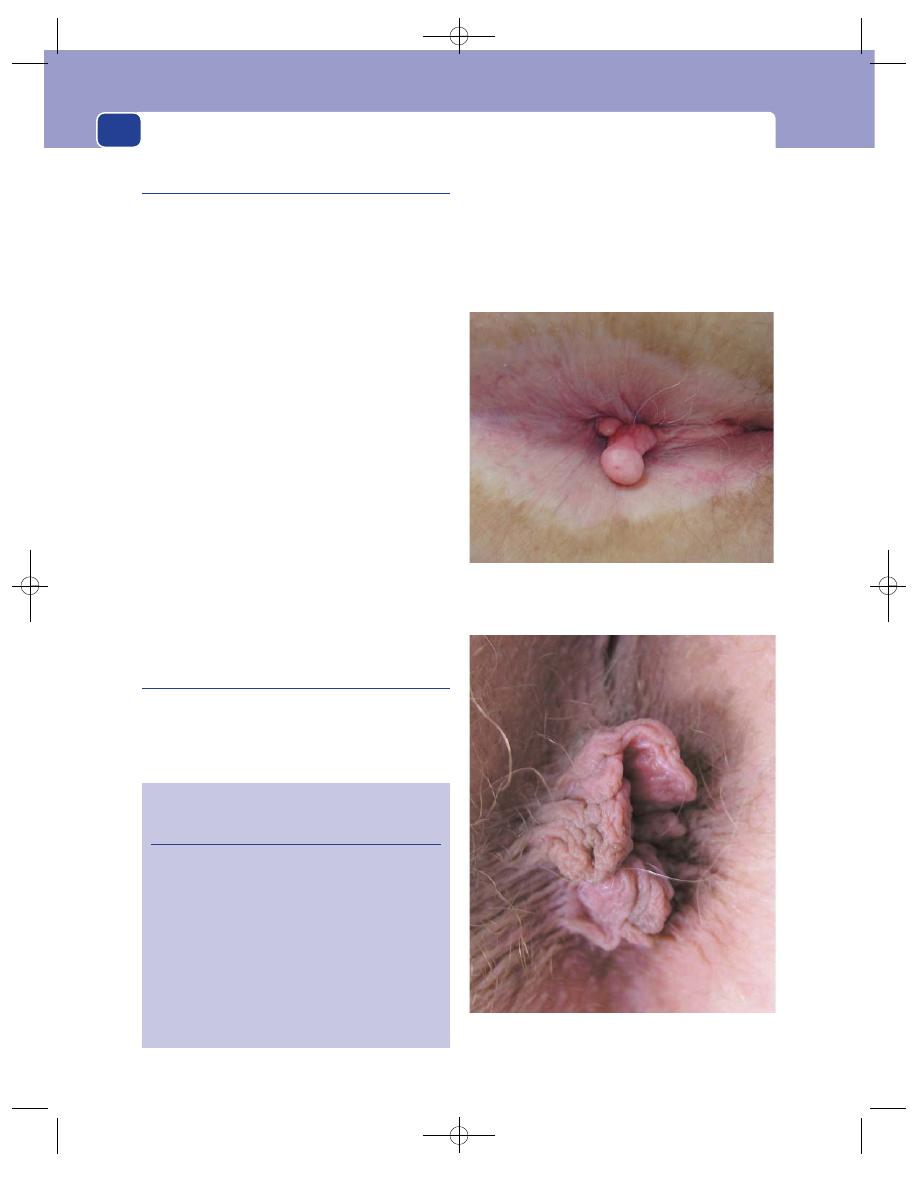
The rectum and anal canal
Prolapsed haemorrhoids
The symptoms of haemorrhoids have already been
described because their commonest symptom is
rectal bleeding. However, some piles do not bleed
(or the patient does not observe the bleeding) and
are therefore not noticed until the patient feels them
after defaecation. It may then be observed that the
lumps retract spontaneously, or can be pushed back
into the anal canal.
Piles which only prolapse during defaecation
(second degree) are not painful, but if they become
permanently prolapsed (third degree), strangulated,
thrombosed or ulcerated, they become very painful
and tender.
Examination then reveals two or three tense, ten-
der, red-purple mucosa-covered swellings protru-
ding from the anal canal. The covering of purple
mucosa and swellings at the 3, 7 and 11 o’clock pos-
itions (12 o’clock is anterior) make the diagnosis
easy. Associated oedematous skin tags, which are
part of the pile mass, have a surface that is clearly
skin and not mucosa. They lie outside the true piles.
If the piles have been prolapsed and thrombosed
for a long time, they may be so ulcerated and
infected that they resemble a prolapsing carcinoma
or other gross pathology.
Anal skin tags
Tags of skin, of varying size and shape, are com-
monly found in the peri-anal area. They represent
an exaggeration of the normal wrinkling of the lax
anal skin, which must be able to stretch enough to
allow defaecation. They are usually symptomless,
but may rub, catch or itch. A fastidious patient may
complain that skin tags prevent proper cleaning of
the peri-anal area.
Skin tags in the 3, 7, and 11 o’clock positions may
be part of a pile mass. However, there may be quite
466
Revision panel 17.3
Diagnosis of anal conditions which present
with a lump
A lump and no other symptoms
Anal warts
Skin tags
A lump and pain
Peri-anal haematoma
A lump, pain and bleeding
Prolapsed haemorrhoids
Carcinoma of anal canal
Prolapsed rectal polyp or carcinoma
Prolapsed rectum
FIG 17.14
An anal polyp. This is clearly fibrous and quite
different from an adenomatous polyp, in both level and
appearance.
FIG 17.15
Anal skin tags. Many patients call these tags
‘piles’, but they are not haemorrhoids.
Chap-17.qxd 4/21/05 12:58AM Page 466
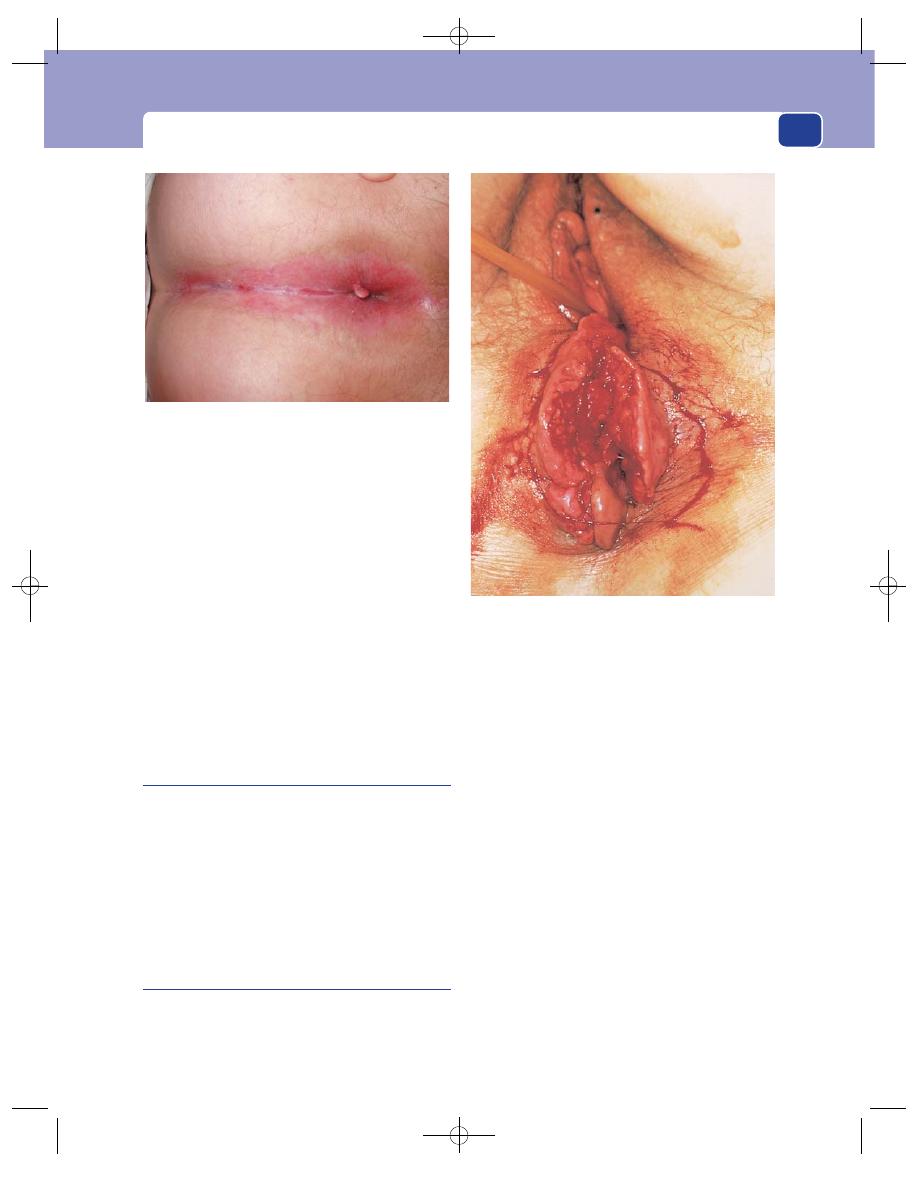
Conditions presenting as an anal lump with or without pain
large skin tags without piles and, of course, quite
large piles without skin tags.
Sometimes part of the lining of the lower anal
canal may develop into a smooth skin-covered pedun-
culated papilla, which prolapses or is seen on procto-
scopy. The common expression for this is an anal
polyp, or a fibrous polyp. Please note that this is using
the word ‘polyp’ in the generic sense of any swelling on
a stalk, and this condition must not be confused with
an adenomatous polyp which arises from mucosa, not
skin, and has a malignant potential. Fibrous polyps of
the skin of the anal canal are harmless.
A tag may develop at the lower end of an anal fis-
sure, often called a sentinel tag.
Carcinoma of the rectum
A carcinoma of the rectum or the anal canal may
present rarely as an anal lump if it prolapses
through the anus or spreads directly down the wall
of the anal canal to the peri-anal skin. When the
anal canal is invaded by tumour the patient usually
has pain on defaecation, as well as a lump. This is
one of the few circumstances in which a low rectal
carcinoma presents with pain.
Squamous cell carcinoma of the anus
This is a carcinoma of the anal or peri-anal skin,
and is identical to the squamous cell carcinoma
found anywhere else in the body. It may be associated
with pre-cancerous changes in the local skin known
as anal intraepithelial neoplasia.
Presenting symptoms depend on how far the
lesion is away from the mucocutaneous junction. If
the lesion is in the lower part of the anal canal, there
will be bleeding and pain on defaecation, which the
patient usually assumes are due to piles. If the lump
is away from the anal margin, the patient notices the
swelling without any bowel symptoms.
A low adenocarcinoma of the rectum and an
anal squamous cell carcinoma may appear very
similar. A squamous cell carcinoma does not exude
mucus. If there are palpable inguinal glands, the
lesion is likely to be an anal squamous carcinoma, as
a rectal adenocarcinoma drains to the mesorectal
lymph glands.
PROLAPSE OF THE RECTUM
This is an eversion of the lower part of the rectum
through the anal canal. There are two varieties.
467
FIG. 17.16
Severe pruritus caused by the leakage of
mucus from large second-degree haemorrhoids. There is a
small skin tag.
FIG 17.17
A carcinoma of the anal canal which has spread
into the skin of the perineum. The patient was still able to
defaecate. The patient is in the lithotomy position.
Chap-17.qxd 4/21/05 12:58AM Page 467
The rectum and anal canal
Full-thickness prolapse
Full-thickness prolapse means that the entire rectal
wall, muscle and mucosa become displaced through
the anus. It occurs when the structures in the floor of
the pelvis that normally hold the rectum in the curve
of the sacrum become weak and lax, and is always
associated with impaired continence because of
weakness and stretching of the anal canal.
History
Age
Prolapse of the rectum is commonly a disease
of the elderly. The majority of patients requiring
treatment are over 80.
Sex
Full-thickness rectal prolapse is more or less
confined to women who have had children. During
delivery, the anal canal is stretched and damaged.
The anal sphincters are thinner anteriorly in any
event in women compared with men, because of the
existence of the vagina. However, it is many years
before a prolapse becomes obvious, although contin-
ence problems occur sooner.
Symptoms
The patient complains of a large lump which
appears at the anus after defaecation, or sometimes
spontaneously when standing, walking or coughing.
The lump can usually be pushed back into the
rectum or may return spontaneously when the
patient lies down.
A prolapsed rectum is uncomfortable, often
slightly painful, and causes a persistent desire to
defaecate. The prolapsed rectal mucosa secretes
mucus and, if it remains prolapsed, ulcerates and
bleeds. Incontinence of faeces is coexistent.
Examination
Colour and shape
The prolapsed rectum forms a long
tubular mass protruding symmetrically through the
anus. The exposed mucosa is red and thrown into
circumferential concentric folds around a central
orifice, which is the lumen of the rectum.
Sometimes it is necessary to ask the patient to
strain down to produce the prolapse. The diagnosis
is made by inspection, and may be missed if this
essential manoeuvre is omitted.
The prolapse may be up to 20 cm in length. The
bowel is not tender and can be handled without
causing the patient discomfort.
Examine the junction of the mass with the anal
canal. If the lump is a rectal prolapse, its mucosal
covering and the anal skin will be continuous. If the
lump is an intussusception (extremely rare!), there
will be a gap between the mucosa covering the lump
and the anal skin. If you put your finger into this
gap, it will pass through the anal canal, into the rec-
tum, alongside the intussusception.
Intussusception of the sigmoid colon and upper
rectum occurs in adults when a polyp or carcinoma
forms the head of the intussusception. The causative
lesion will be visible at the apex of the swelling.
Reducibility
It is usually possible to reduce a prolapse
with gentle compression and cephalad pressure.
Local tissues
The rectum and anal canal are normal
but the anal sphincter is very lax.
Partial-thickness or mucosal prolapse
In this variety, only the mucosa prolapses. In adults,
the history is very similar to that of prolapsing
468
Revision panel 17.4
The causes of pruritus ani
Mucous discharge from the anus caused by:
Haemorrhoids
Polyps
Skin tags
Condylomata
Fissure
Fistula
Carcinoma of the anus
Vaginal discharge caused by:
Trichomonas vaginitis
Monilia vaginitis
Cervicitis
Gonorrhoea
Skin diseases
Tinea cruris
Fungal infections, especially monilial
infections in diabetics
Parasites
Threadworm
Faecal soiling
Poor hygiene
Incontinence
Diarrhoea
Psychoneuroses
Chap-17.qxd 4/21/05 12:58AM Page 468
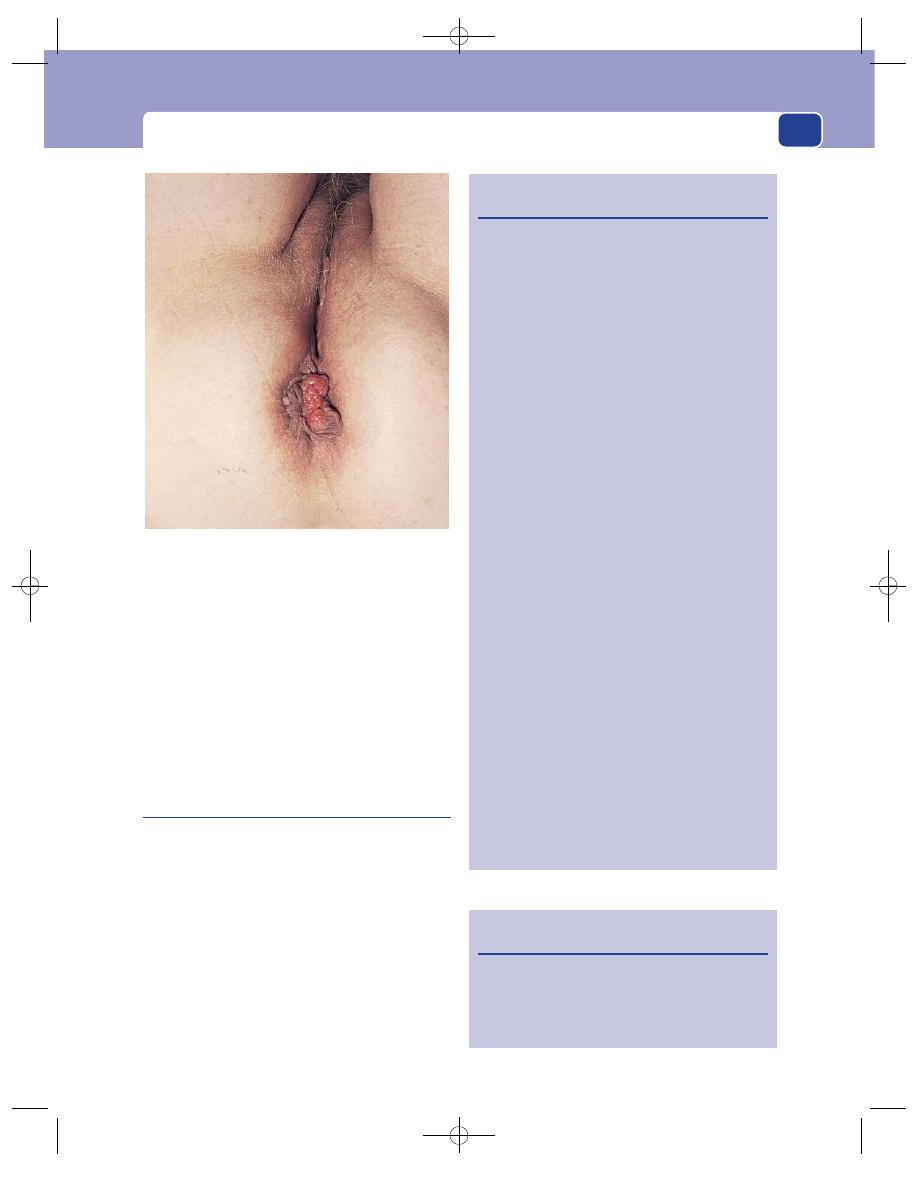
Conditions presenting as an anal lump with or without pain
(second-degree) piles. However, instead of there
being discrete anal cushions, there is a circular fold
of mucosa. There is an overlap between the two
conditions.
On examination, there will be a soft mass at the
anal margin. It is painless to palpate, and can be felt
as two thin mucosal layers. There will be a mucous
discharge, often the main symptom, and the redun-
dant mucosa is seen on proctoscopy.
Mucosal rectal prolapse in children
In children, the mucosa of the bowel is more loosely
attached to the muscle layer than in adults. In
addition, there is often hypertrophy of the submu-
cosal lymphoid aggregates known as Peyer’s patches.
This may result in prolapse of the anal mucosa.
History
Age
The condition usually presents at potty train-
ing, but occurs up to puberty.
Symptoms
Usually the parents notice a smooth,
soft swelling at the anal margin after defaecation.
The child may complain of discomfort, and older
469
FIG 17.18
Prolapsing rectal mucosa, part of which is
becoming fibrosed and papillomatous – a ‘fibrosed anal
polyp’. The patient is in the lithotomy position.
Revision panel 17.5
Some common causes of diarrhoea
Intestinal
Enteritis:
non-specific
staphyloccocal
typhoid
bacillary dysentery
amoebic
cholera
Worms
Ulcerative colitis
Crohn’s disease
Carcinoma
Irritable colon
Faecal impaction (spurious diarrhoea)
Tropical sprue
Gastric
Post-gastrectomy
Post-vagotomy
Gastrocolic fistula
Pancreatic
Pancreatitis
Carcinoma
Pelvic abscess
Drugs
Digitalis
Antibiotics
Laxatives
Endocrine
Uraemia
Thyrotoxicosis
Carcinoid syndrome
Zollinger–Ellison syndrome
Medullary carcinoma of thyroid
Hypoparathyroidism
Diet
Revision panel 17.6
Causes of pericoccygeal swellings
Pilonidal sinus
Postanal dermoid cyst
Chordoma
Sacrococcygeal teratoma
Chap-17.qxd 4/21/05 12:58AM Page 469
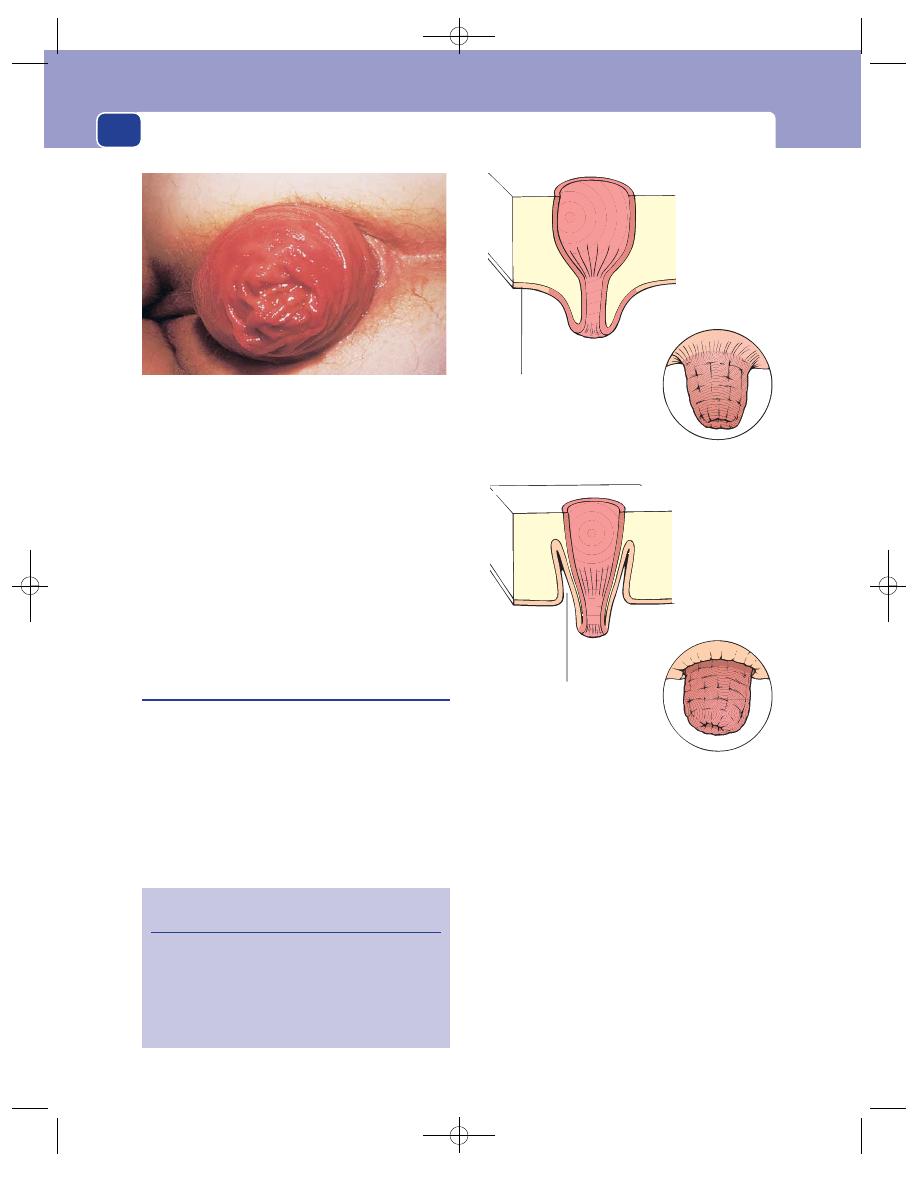
The rectum and anal canal
children may become frightened. There is no
bleeding, but there may be a mucous discharge.
Sometimes the child thereafter tries to avoid defae-
cation and becomes impacted with hard faeces.
Examination
Only rarely will the swelling be reproducible in the
clinic, and diagnosis must be made on the history.
The only differential diagnosis is the very rare juve-
nile polyp, and in this event there will be bleeding.
Course
The condition is self-curing with increas-
ing age.
Intussusception
It is rare for an ileocolic or caecocolic intussuscep-
tion in a child to present at the anus, but when it
does it appears as a sausage-shaped lump covered
with red-purple mucosa, similar to a rectal pro-
lapse. The only way to distinguish it from a rectal
prolapse is finding on rectal examination that the
anal canal is normal and that a finger can be passed
into it alongside the protruding bowel.
The history will give a clue to the diagnosis.
Intussusception in children occurs between the ages
of 9 months and 2 years, and is associated with
colicky abdominal pain and (rarely) the passage of
bloodstained mucus, often described as looking like
‘redcurrant jelly’.
In adults, the sigmoid colon and upper rectum
may intussuscept if the bowel contains a polyp or
carcinoma to act as the head of the intussusception.
In these circumstances the causative lesion will be
visible on the apex of the protruding bowel.
470
Revision panel 17.7
Causes of faecal incontinence
Diarrhoea
Faecal impaction
Nerve damage
Sphincter muscle damage
Dementia
Skin of anus and
mucosa of rectum
in continuity
Prolapse
Intussusception
Gap between the
bowel and anus,
which leads to
the rectum
FIG 17.20
The difference between a rectal prolapse (upper
panel) and an intussusception presenting through the anus
(lower panel).
FIG 17.19
A rectal prolapse.
Chap-17.qxd 4/21/05 12:58AM Page 470