Chapter 5 – Cardiovascular disease
83
“” Functional Anatomy & Physiology “”
(Printed by Mostafa Hatim)
Anatomy
The heart lies in the middle of the chest, slightly to the left. It occupies about <50% of the
diameter of the transverse section of the chest. The heart diameter must be < 50% →
anything larger means cardiac enlargement. Ventricular hypertrophy occur if thickness
of left ventricle ˃ 1cm & right ventricle ˃ (2-3) cm
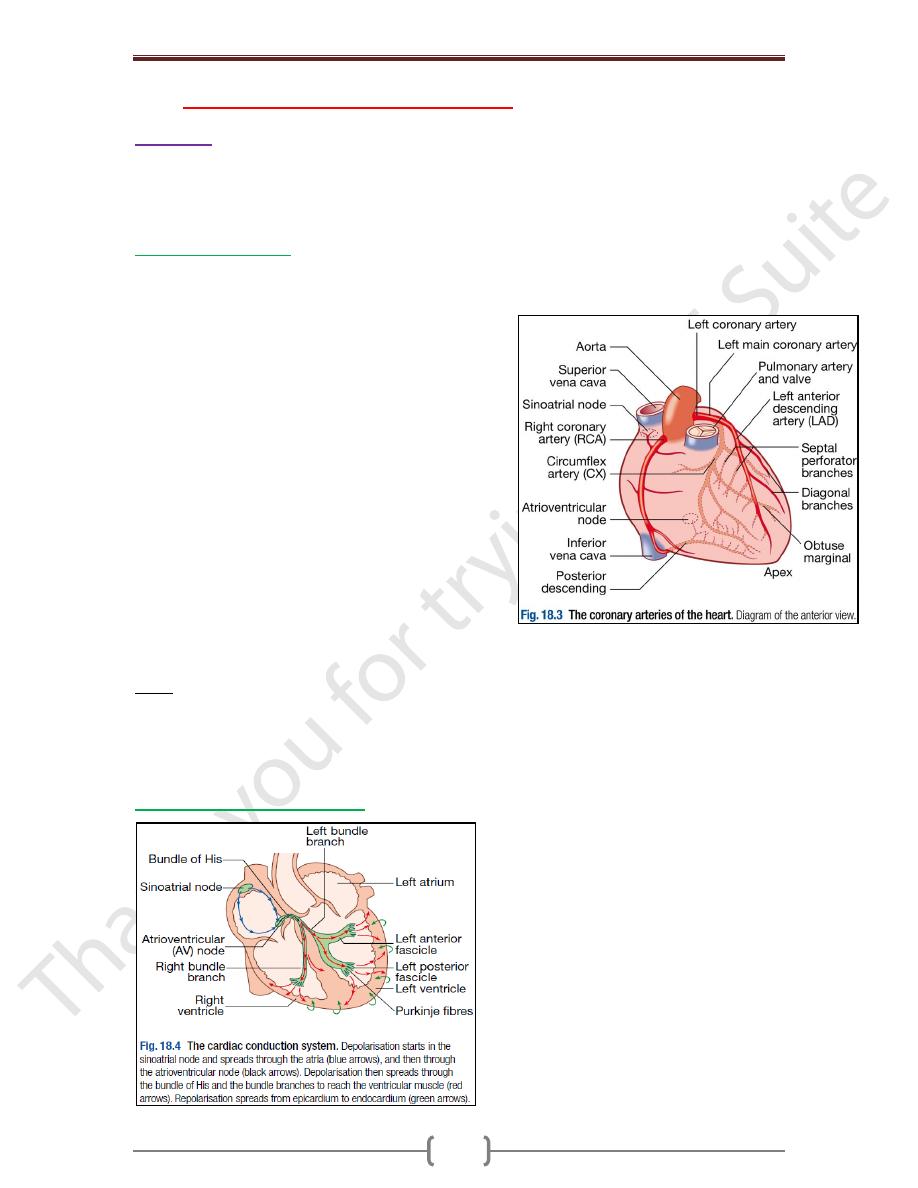
Coronary circulation
The left main and right coronary arteries arise from the left and right coronary sinuses of
the aortic root, distal to the aortic valve (Fig. 18.3). Within 2.5cm of its origin, the left
main coronary artery divides into the left anterior
descending artery (LAD), which runs in the anterior
interventricular groove, and the left circumflex artery
(CX), which runs posteriorly in the atrioventricular
groove. The LAD gives branches to supply the anterior
part of the septum (septal perforators) and the anterior,
lateral and apical walls of the LV. The CX gives marginal
branches that supply the lateral, posterior and inferior
segments of the LV. The right coronary artery (RCA) runs
in the right atrioventricular groove, giving branches that
sup- ply the RA, RV & inferoposterior aspects of the LV.
The posterior descending artery runs in the
posterior inter- ventricular groove and supplies the
inferior part of the interventricular septum. This vessel is
a branch of the RCA in approximately 90% of people
(dominant right system) and is supplied by the CX in the
remainder (dominant left system). The coronary anatomy varies greatly from person to
person & there are many ‘normal variants’.
Notes
Blockage of the left main coronary artery will cause immediate death.
The RCA supplies the sinoatrial (SA) node in about 60% of individuals and the AV node
in about 90%. Proximal occlusion of the RCA therefore often results in sinus bradycardia
and may also cause AV nodal block.
Conducting system of the heart
Chapter 5 – Cardiovascular disease
84
Nerve supply of the heart
The heart is innervated by both:
Sympathetic: Adrenergic nerves from the cervical sympathetic chain supply muscle
fibers in the atria and ventricles and the electrical conducting system. Positive inotropic
and chronotropic effects are mediated by β1-adrenoceptors, whereas β2-adrenoceptors
predominate in vascular smooth muscle and mediate vasodilatation. Adrenergic
stimulation associated with exercise, emotional stress, fever and so on causes the heart
rate to increase.
Parasympathetic: pre-ganglionic fibres and sensory fibres reach the heart through the
vagus nerves. Cholinergic nerves supply the AV and SA nodes via muscarinic (M2)
receptors. Under resting conditions, vagal inhibitory activity predominates and the heart
rate is slow.
In disease states the nerve supply to the heart may be affected. For example, in heart
failure the sympathetic system may be up-regulated, and in diabetes mellitus the nerves
themselves may be damaged (autonomic neuropathy) so that there is little variation in
heart rate.
Physiology
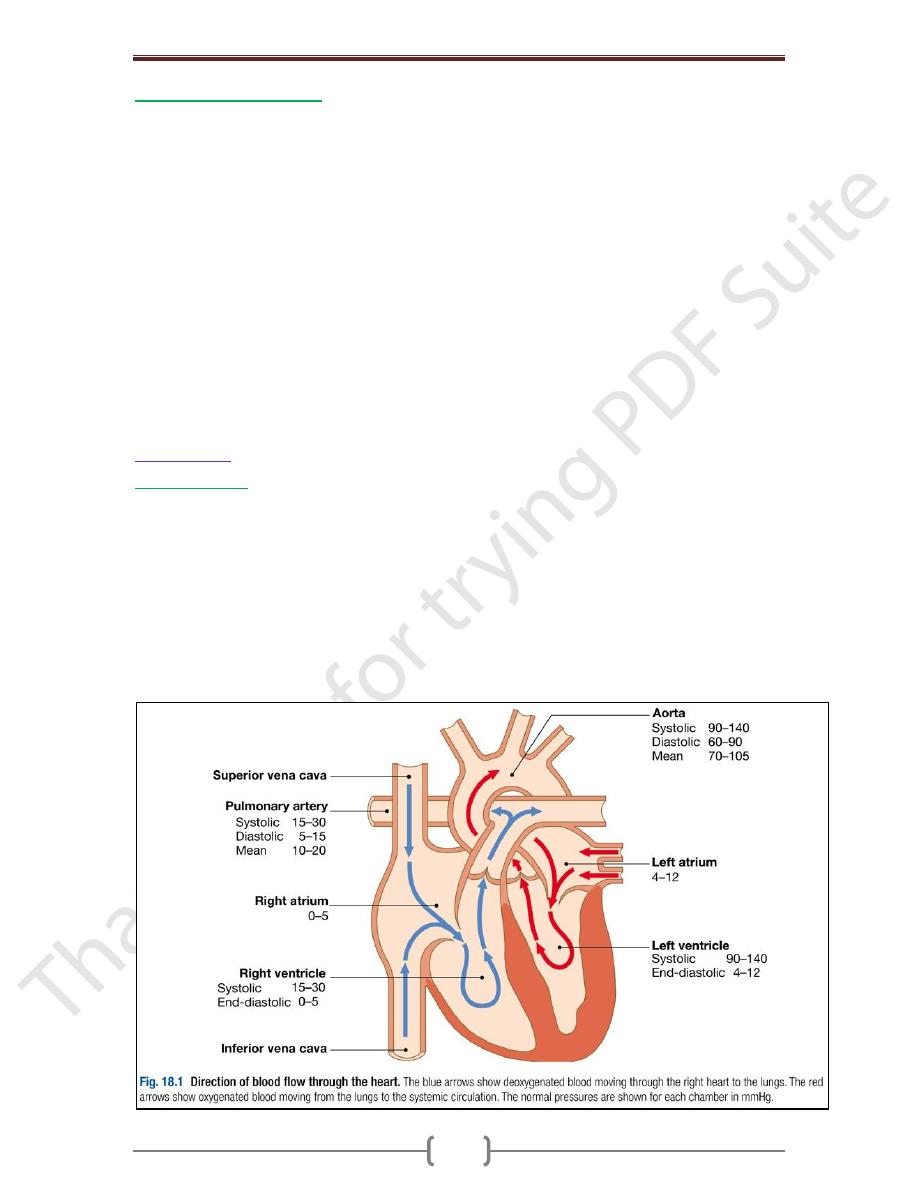
The circulation
The RA receives deoxygenated blood from the superior and inferior venae cavae and
discharges blood to the RV, which in turn pumps it into the pulmonary artery. Blood
passes through the pulmonary arterial and alveo- lar capillary bed where it is oxygenated,
then drains via four pulmonary veins into the LA. This in turn fills the LV, which delivers
blood into the aorta. During ventricular contraction (systole), the tricuspid valve in the
right heart and the mitral valve in the left heart close, and the pulmonary and aortic
valves open. In diastole, the pulmonary and aortic valves close, and the two AV valves
open. Collectively, these atrial and ventricular events constitute the cardiac cycle of
filling and ejection of blood from one heartbeat to the next.
Chapter 5 – Cardiovascular disease
85
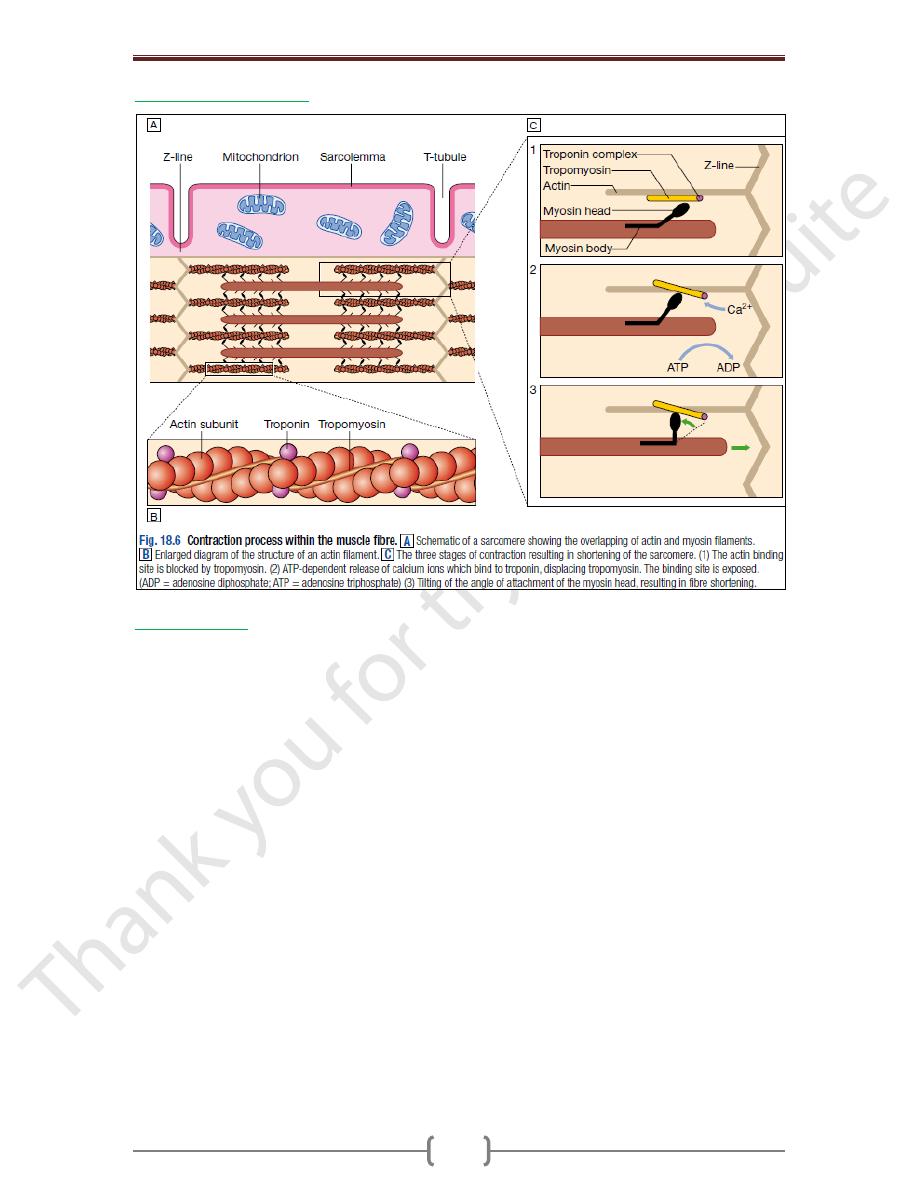
Myocardial contraction
Cardiac output
Cardiac output is the product of stroke volume & heart rate. Stroke volume is the
volume of blood ejected in each cardiac cycle & is dependent upon end-diastolic
volume & pressure (preload: amount of blood enter the heart), myocardial contractility &
systolic aortic pressure (afterload: amount of blood leaves the heart, it depends on
peripheral vascular resistance; in atherosclerotic patient will be decreased due to
collapsing of arteries & become resistant to CO of the heart).
Preload & afterload are two balanced power
CO = SV Χ HR. Normally → CO = 70 Χ 70 = 4900 cc/min ≈ 5 L/min
In stress, CO will increase to reach 10 L/min or even 15L/min
In heart failure, CO can’t exceed 5.5L/min. It is recommended that patient not to be
exhausted or they will die.
Stretch of cardiac muscle (from increased end-diastolic volume) causes an increase in
force of contraction, producing a greater stroke volume: Starling’s Law of the heart.
The contractile state of the myocardium is controlled by neuro-endocrine factors, such
as adrenaline (epinephrine), and can be influenced by inotropic drugs and their
antagonists. The response to a physiological change or to a drug can be predicted on the
basis of its combined influence on preload, afterload and contractility
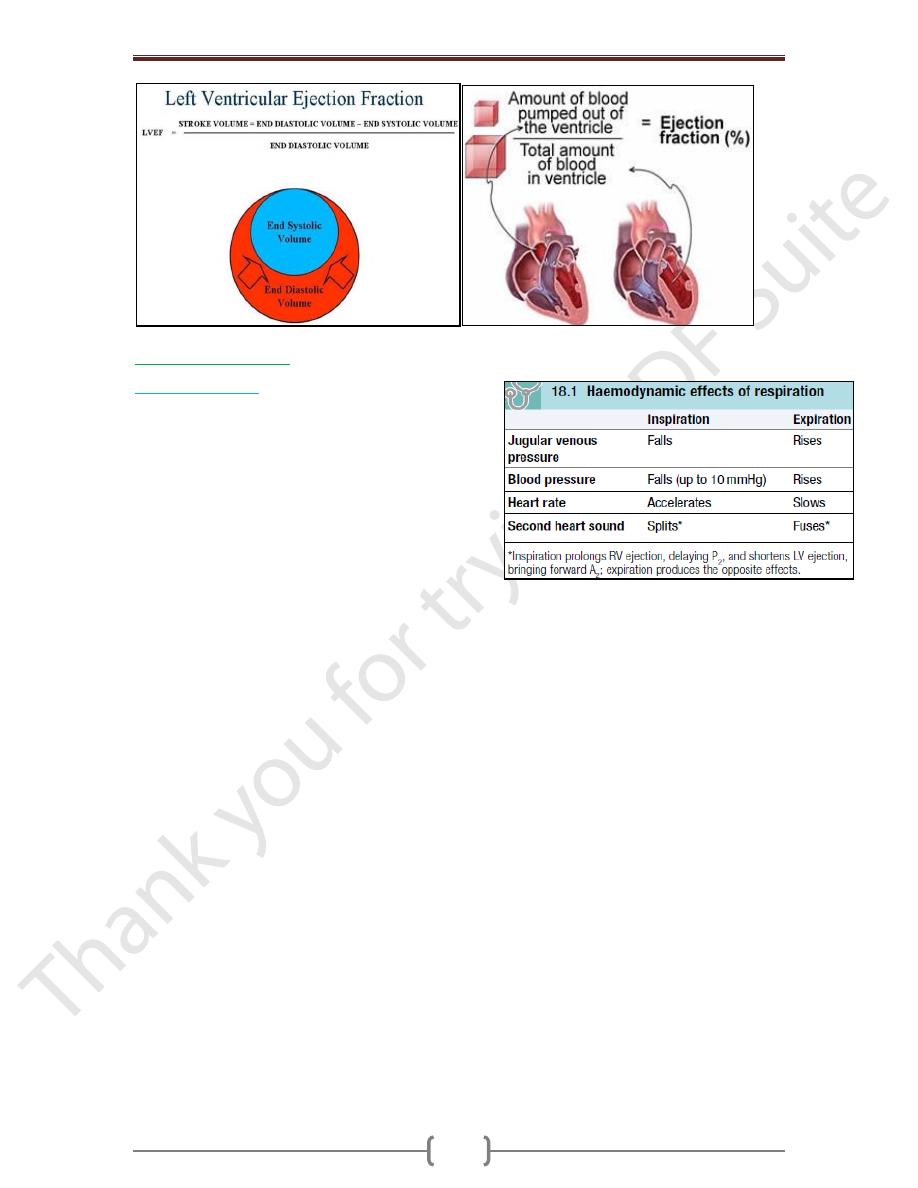
Ejection fraction: is the percent of end-diastolic ventricle volume that is ejected with
each stroke (stroke volume divided by end-diastolic volume. Normally is 50%; lower
volume indicate ventricular dysfunction)
End-diastolic ventricular volume: volume of blood in the left ventricle after diastole.
Note: when the ventricle contract, not all the blood will be pumped to the circulation →
about (30-40%) of the blood will stay in the ventricle after circulation.
Chapter 5 – Cardiovascular disease
86
Effects of respiration
Pulsus paradoxus
This term is used to describe the exaggerated fall in BP
during inspiration that is characteristic of:
Cardiac tamponade: compression of the right heart
prevents the normal increase in flow through the right
heart on inspiration, which exaggerates the usual drop
in venous return to the left heart and produces a marked
fall in BP
Severe airways obstruction: it is due to accentuation
of the change in intrathoracic pressure with respiration.