Respiratory diseases caused by fungi
Dr Ghazi Farhan HajiCardiologist
The majority of fungi encountered by humans are harmless , but in certain circumstances some species may infect human tissue, promoting damaging allergic reactions or producing toxins.
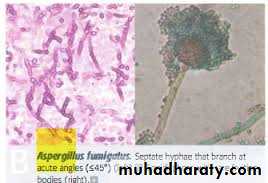
Mycosis' is the term used to describe disease caused by fungal infection. (Aspergillus fumigatus)
Other fungal infections:
Pulmonary mucormycosis .
Histoplasmosis,
coccidioidomycosis,
blastomycosis
cryptococcosis
Most cases of bronchopulmonary aspergillosis are caused by Aspergillus fumigatus
Classification of bronchopulmonary aspergillosis1-Allergic bronchopulmonary aspergillosis (asthmatic pulmonary eosinophilia)
2-Extrinsic allergic alveolitis (Aspergillus clavatus)3-Intracavitary aspergilloma
4-Invasive pulmonary aspergillosis
5-Chronic and subacute pulmonary aspergillosis


Factors predisposing to fungal disease
@ Diabetes mellitus@Chronic alcoholism
@HIV and AIDS
@Corticosteroids and other immunosuppressant medication
@Radiotherapy
Allergic bronchopulmonary aspergillosis (ABPA)
ABPA is a hypersensitivity reaction to fungal spores, which may complicate asthma and cystic fibrosis. It is a recognised cause of pulmonary eosinophilia .The prevalence of ABPA is approximately 1-2% in asthma and 5-10% in CF.
Clinical features and investigationsFeatures of allergic bronchopulmonary aspergillosis
1-Asthma (in the majority of cases) fever, breathlessness, cough productive
2-Proximal bronchiectasis
3-Positive skin test to an extract of A. fumigatus
4-Elevated total serum IgE
5-Peripheral blood eosinophilia
6-Presence or history of chest X-ray abnormalities
7-Fungal hyphae of A. fumigatus on microscopic examination of sputum
Management
1-Regular low-dose oral corticosteroids (prednisolone 7.5-10 mg daily)2-In some patients, Itraconazole (400 mg/day) allows to a reduction in oral steroids;
3-The use of specific anti-IgE monoclonal antibodies is under consideration.
Exacerbations, particularly when associated with new chest X-ray changes, should be treated promptly with prednisolone 40-60 mg daily and physiotherapy.
.
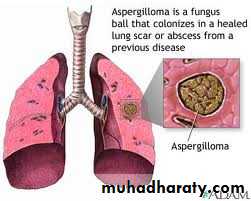
Aspergilloma
Inhaled Aspergillus may lodge and germinate in areas of damaged lung tissue forming a fungal ball or aspergilloma.The upper lobes are most frequently involved, and fungal balls readily form in tuberculous cavities..
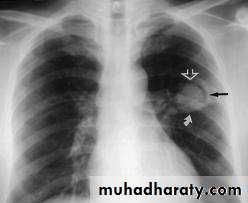

Clinical features and diagnosis
#often asymptomatic, and are identified incidentally on chest X-ray.The fungal ball produces a tumour-like opacity on X-ray (presence of a crescent ),they may cause recurrent haemoptysis
# HRCT is more sensitive
.#Elevated serum precipitins to A. fumigatus are found in virtually all patients.#Sputum microscopy typically demonstrates hyphal and is usually positive on culture.
#skin hypersensitivity to extracts of A. fumigatus.
Management
@Asymptomatic cases do not require treatment.
Specific antifungal therapy is of no value and steroids may predispose to invasion.
@Aspergillomas complicated by haemoptysis should be excised surgically.
@In those unfit for surgery, palliative procedures range from local instillation of amphotericin B to bronchial artery embolisation.Invasive pulmonary aspergillosis (IPA) Risk factors for invasive aspergillosis
1-Neutropenia2-Prolonged high dose corticosteroid therapy
3-Leukaemia and other haematological malignancies
4-Cytotoxic chemotherapy
5-Advanced HIV disease
6-Severe COPD
7-Critically ill patients on intensive care units
Clinical features
Acute IPA causes a severe necrotising pneumonia, and must be considered in any immunocompromised patient who develops :fever, new respiratory symptoms (particularly pleural pain or haemoptysis) or a pleural rub.
Invasion of pulmonary vessels causes thrombosis and infarction, and systemic spread may occur to the brain, heart, kidneys and other organs. .
Diagnosis
• @HRCT characteristically shows macronodules (usually ≥ 1 cm) Dense, well-circumscribed lesion(s) with or without a halo sign -Air crescent sign-Cavity@Culture or histopathological evidence of Aspergillus in diseased tissue gives a definitive diagnosis by bronchoscopy.
@detection of Aspergillus cell wall components in blood or BAL fluid, and Aspergillus DNA by PCR.
Management and prevention
$IPA carries a high mortality rate, especially if treatment is delayed.#The treatment of choice is -Itraconazole.
#Second-line agents include lipid-associated amphotericin
#Response is assessed both clinically and radiologically.
Patients at risk of Aspergillus should be nursed in rooms with high-efficiency particulate air filters OR wear a maskItraconazole (200 mg/day) may be prescribed for primary prophylaxis.
Thank you for attention
