


Plague
&Anthrax
Lecture No. 7/ General Medicine
Prof. Dr. Zainalabideen A. Abdulla

Plague
Plague (anciently called Black Death) is caused by Yersinia pestis and is transmitted between rodents by their fleas (Fig). If domestic rats become infected, it is transmitted to humans by bites with infected fleas, and between humans by droplets in late stages of human plague (pneumonic, see below). The first sign of plague is the appearance of dead rats. Furthermore, Y. pestis is a potential bioweapon (biological weapon) with high fatality from pneumonic plague.


Clinical features
The incubation period of plague is 3-6 days and is shorter in pneumonic type. Yersinia pestis is taken rapidly from the skin bite to the draining lymph nodes and causes severe haemorrhagic inflammation. Alveolitis develops in case of inhalation. Then septicaemia may start and lesions (nectrotic, purulent, or haemorrhagic) develop in many organs, followed by oliguria, shock and DIC with widespread haemorrhage. Plague can be categorized into three types:1. Bubonic
2. Septicaemic
3. Pneumonic
Bubonic plague
This form is the most common, starts suddenly with rigor, high fever, dry skin, and severe headache. The patients have rapid pulse, hypotension, and mental confusion with splenomegaly. At the site of infected lymph nodes there are aching and swelling, and “bubos” develop at the groin region from swollen lymph nodes and surrounding tissues.Septicaemic plague
The patient is toxic, and may have gastrointestinal symptoms such as nausea, vomiting, abdominal pain, and diarrhea. DIC and bleeding with ecchymoses may occur together with hypotension, shock, renal failure and acute respiratory distress syndrome (ARDS). Meningitis, pneumonia, and expectoration of blood-stained sputum containing Y. pestis could complicate the condition.Pneumonic plague
The onset is very sudden after respiratory infection with Y. pestis, with dyspnoea, and cough. The patient expectorates copious blood-stained frothy and highly infective sputum, and then becomes cyanosed and dies. The chest imaging shows bilateral infiltrates which may progress to ARDS.
Investigations
1. Stained smear by Gram’s, Geimsa or Wayson stains for rapid diagnosis.Y. pestis is gram negative coccobacilli with bipolar staining (safety pin) appearance (Figure).
2. Culture: Blood, sputum, and bubo aspirates
3. Immunofluorescence staining: Using F1 antigen-specific antibody (significant titre >1/128)
4. PCR: DNA detection of Y. pestis
Management
1. Start antibiotic immediately (even before sample collection):First choice: Streptomycin (1 g 12-hourly) or gentamicin (1mg/kg 8-hourly)
Alternative: Tetracycline (500 mg 6-hourly) and chloramphenicol (12.5 mg/kg 6-hourly)
Recently: Fluoroquinolones (ciprofloxacin and levofloxacin)
2. Treatment of acute circulatory failure, DIC, and hypoxia may be needed.
Prevention and control
1. Control of rats and flees2. Isolation of patients for the first 48 hours
3. Contacts with pneumonic plague: Prophylactic doxycycline (100 mg daily or ciprofloxacin 500 mg 12-hourly) for 7 days
4. Killed vaccine is available for those at occupational risk such as hunters and trappers. ** Recombinant subunit vaccine using F1 antigen is under trial.
Anthrax
Anthrax is an acute zoonotic disease caused by inoculation of spores of Bacillus anthracis (Figure) that can survive for years in soil mainly through contact with animals (herbivores). B. anthracis can also be used as a bioweapon.
Herbivores






Clinical features
The clinical features depend on the route of entry of spores to the body namely:1. Cutaneous anthrax
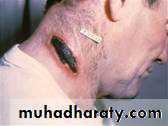
This is the most common type and is frequently occupational or due to bioterrorism. The spores enter into the skin, and a single lesion may develop as an irritable papule on an oedematous haemorrhagic base. This lesion progresses to a depressed black eschar (Figure) with infrequent pain.
2. Gastrointestinal anthrax
This type is associated with ingestion of contaminated meat food products. The caecum is the site of infection leading to nausea, vomiting followed in 2-3 days by severe abdominal pain and bloody diarrhea, with rapid development of toxaemia and death.3. Inhalation anthrax
This type is very rare, associated with bioterrorism, and carries a high mortality rate of 50-90%. After 3-14 days of exposure the patients develop fever, dyspnoea, cough, headache, and symptoms of septicaemia. The CXR shows widening of the mediastinum and pleural effusions (haemorrhagic, Figure). Meningitis may develop.
Management
Skin lesions are curable with early antibiotic therapy, and B. anthracis can be cultured from these lesions:1. Ciprofloxacin 500 mg 12-hourly, then change if susceptible, to benzyl penicillin 2.4 g I.V. 4-hourly or phenoxy-methylpenicillin (penicillin V) 500-1000 mg 6-hourly for 10 days. Addition of an aminoglycoside improves the outcome (synergism).
2. Ciprofloxacin or doxycycline 12-hourly orally is added for 2 months in case of possibility of inhalation form in bioterrorism.
3. Prophylactic ciprofloxacin is used for high risk exposure.
