Chapter 12 - Labour
166
“” Obstructed labour “”
Definition
Labour is said to be obstructed when there is absence of progress in the presence of
efficient uterine contractions. Absence of progress: - Failure of the cervix to dilate
- Failure of the presenting part of the fetus to descent the birth canal
Etiology
A. Maternal conditions
1) Contracted pelvis or deformity of the pelvis
2) Tumors of the uterus or ovary – Fibromyoma of lower uterine segment
3) Tumors of rectum or bladder
4) Tumors of pelvic bones
5) Pelvic kidney
6) Stenosis of cervix or vagina
7) Congenital Septum of vagina
8) Contraction ring of uterus
B. Fetal conditions
1) Malposition of the fetus
- Persistent posterior position of the occiput
- Deep transverse arrest of the fetal head
2) Malpresentations of the fetus
- Breech presentation - Face presentation - Brow presentation
- Shoulder presentation - Compound present. - Locked twins
3) • Fetal congenital abnormalities - Large fetus - hydrocephalus - Hydrops fetalis - Fetal
abdominal tumors or ascites
Clinical picture
The patient is exhausted by pain and the demands of over contracting uterus.
Pulse rate rise. Temperature may also rise
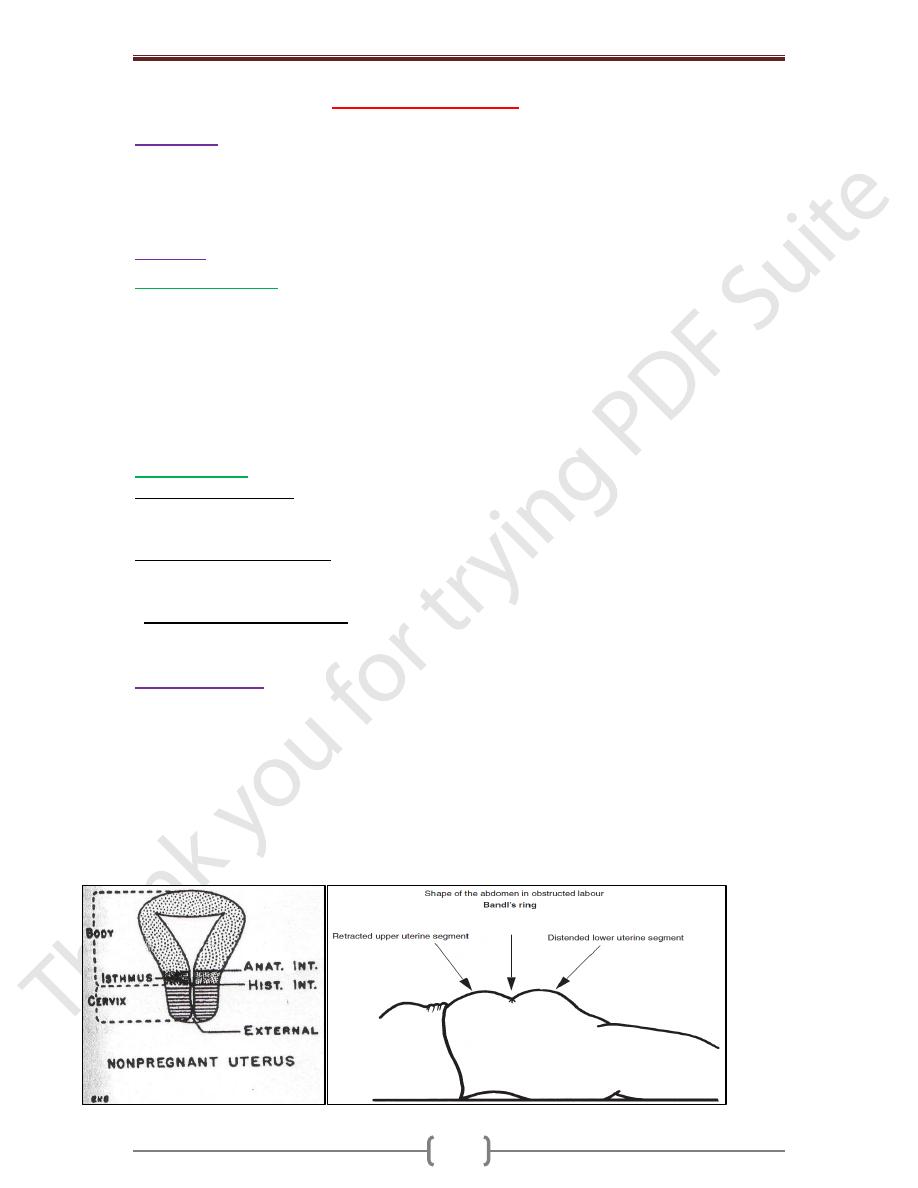
The upper part of the uterus is hard. The lower part (segment) is tender and distended
The line of junction between the two areas is clearly visible on the abdominal wall as an
oblique groove or furrows “The retraction Ring”.
In obstructed labour the presenting part has become arrested inspite the strong contractions.
There is over thickening of the upper segment and over thinning of the lower segment
Pathological retraction ring or “bandls ring” is diagnostic
Chapter 12 - Labour
167
During labour
The upper segment actively contracts & retracts while the lower segment is relatively passive
The upper segment contracting almost instantly and retracting becomes hard and its walls
become very much thicker and shorter as it forces fetus down and draws the lower segment
and cervix up.
As times goes on more and more of the fetus is driven down into the relaxing lower
segment which becomes dangerously and will rupture if urgent helps not given.
The uterine contractions usually increase in force & frequently often accompanied by
strong bearing efforts. The mother becomes exhausted usually restless & haggard.
Pains are severe and continuous and her tongue and lips becomes dry and discolored; the
pulse rate is 120/minute or over. The temperature also rises.
Obstruction always occurs in the cavity or just below the pelvic ring serious obstruction at
the pelvic outlet is uncommon. Death of the fetus results from compression of the placental
site circulation.
The vagina and vulva are edematous and the birth canal feels hot and dry. The edematous
cervix may be felt below the presenting part and a large caput and marked molding of
cranial bones are felt.
Management of obstructed labour
IV line for Rehydration
(a) Cross match blood (b) Haemogram (c) Urea/Electrolyte
Catheterize the bladder if the urine is blood stained – remember to have continuous bladder
drainage for 10 days postnatally.
Arrange for delivery of the baby by c/s to relieve the obstruction.
Give antibiotics – broad-spectrum.
Delivery- by cesarean section
Notes:
Most of the abnormalities should be detected antenataly & planned delivery can be arranged
No labor should be allowed to reach a stage of obstruction