Dr.Abdulkarim September 5, 2016
Session 9
1
NGT Insertion
1-distance from nos to stomach(nasal-nasopharynx-oroph.=16-esophegaus=25cm-)
2-stethoscope on epigastium & air or fluid inj. 10cc
3-XR
4-gastric juice (green color)&sometime pyloric stenosis mislead U
-Colour of fluids which appear after putting of naso gastric tube :
1. Light green - gastric juice
2. Dark green - bile
3. Yellow - small bowel fluid
U/s in I.O
1-intussciption 2-stone 3-Panceatitis
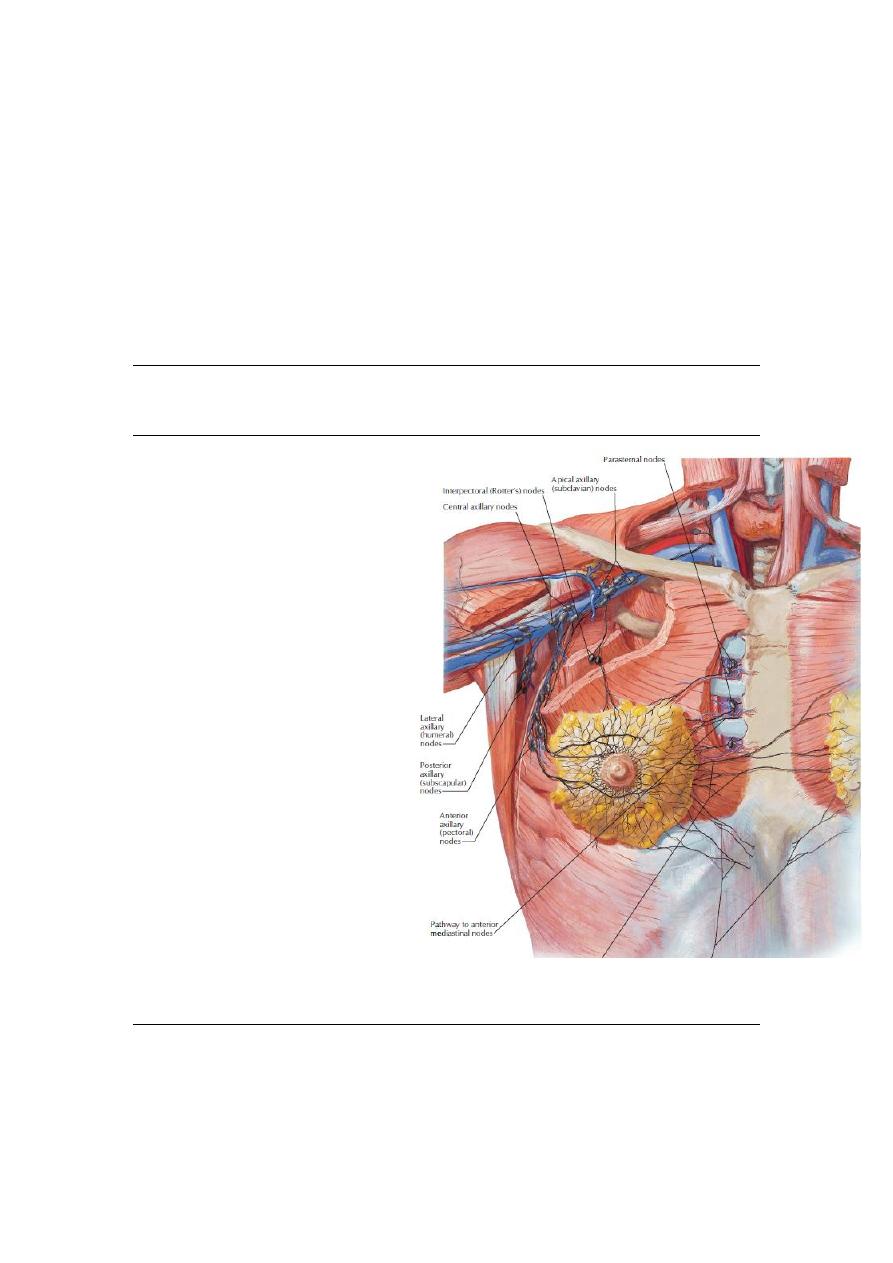
Axillary L.N
1- Lateral: along the Axillary vein.
2- Anterior: along the lat. Thoracic
vessels
3- Posterior: along the subscapular
vessels.
4- Central: embedded in the fat of
the axilla.
5- Interpectoral: between
pectoralis major & minor muscles.
6- Apical: lies above the level of
pectoralis minor tendon & it
receive the lymph of all other
groups. The apical group are in
continuity with the supraclavicular
LNs and drain into subclavian
lymph trunk which enter the great
veins directly or via thoracic duct or
jugular trunk.
The internal mammary LNs: fewer
in No. & lie along the internal mammary vessels.
The Sentinal LN.: Is the first Axillary LN that drain breast.
Surgery for breast Ca
1. Conservative breast cancer surgery= Stage I, stage II, and sometime stage III carcinomas
QUART: Quadrentectomy+ Axillary dissection+ Radiotherapy

Dr.Abdulkarim September 5, 2016
Session 9
2
2.
Simple mastectomy(Treatment for non-invasive breast cancer)
3.
Modified radical mastectomy(patey) (for invasive breast cancer)
4.
Halsted radical mastectomy=Only indicated when pectoralis muscle involved
Chest tube
INdx:1-pantrating 2-non-pentrating 3-diseases
Presentation of tension pneumothorax?
Tension pneumothorax : one way valve lead to
Chest pain
Tachypnea
Tachycardia
Trachal deviation
Hyperresonance chest
Quite breath sounds
Rarely cyanosis
It is diagnosed clinicaly in which patients conditions worse in breath after breath
-Avoid chest tube insertion directly blow rib to avoid intercostal NV bundle inj.
Thoracotomy indx
hours through chest tube )
st
massive bleeding (>150ml/hr & >1000ml in 1
-
1
-----------------------
Goitre
Thyroid disease classification according thyroid enlargement
1-non-enlarged
a-no sign of thyrotoxicosis (euthyroid)
b-sign of thyrotoxicosis(1ry thyrotoxicosis =gravis )
c-apthy =hypothyroidism
2-enlarged
a-diffuse(smooth)-2ry thyrotoxicosis =gravis)
b-simple goiter =no signs of thyrotoxicosis
c-diffuse painful =subacute bacterial thyroiditis -hoshimato
Dr.Abdulkarim September 5, 2016
Session 9
3
d-diffuse non-painful
1-multinodular
e-soltory nodule
1-thyrotoxicosis (hot nodule )=plummer syndrome
2-neoplastic (cold nodule)
Complication of thyroid surgery
_complication of surgery
_bleeding
_nerve injury :
1. recurrent laryngeal
2.external branch of superior laryngeal(
المريض ما يقدر يصيح
)
3.superficial branch of transverse cervical (
المريض من يحلق وجهو ما يحس بالوجع
)
4.ansa cervicalis supply to strap muscles .
4.sympathetic chain injury(horner syndrome)
_Skin infection
_GIT problem
_hypocalcemia
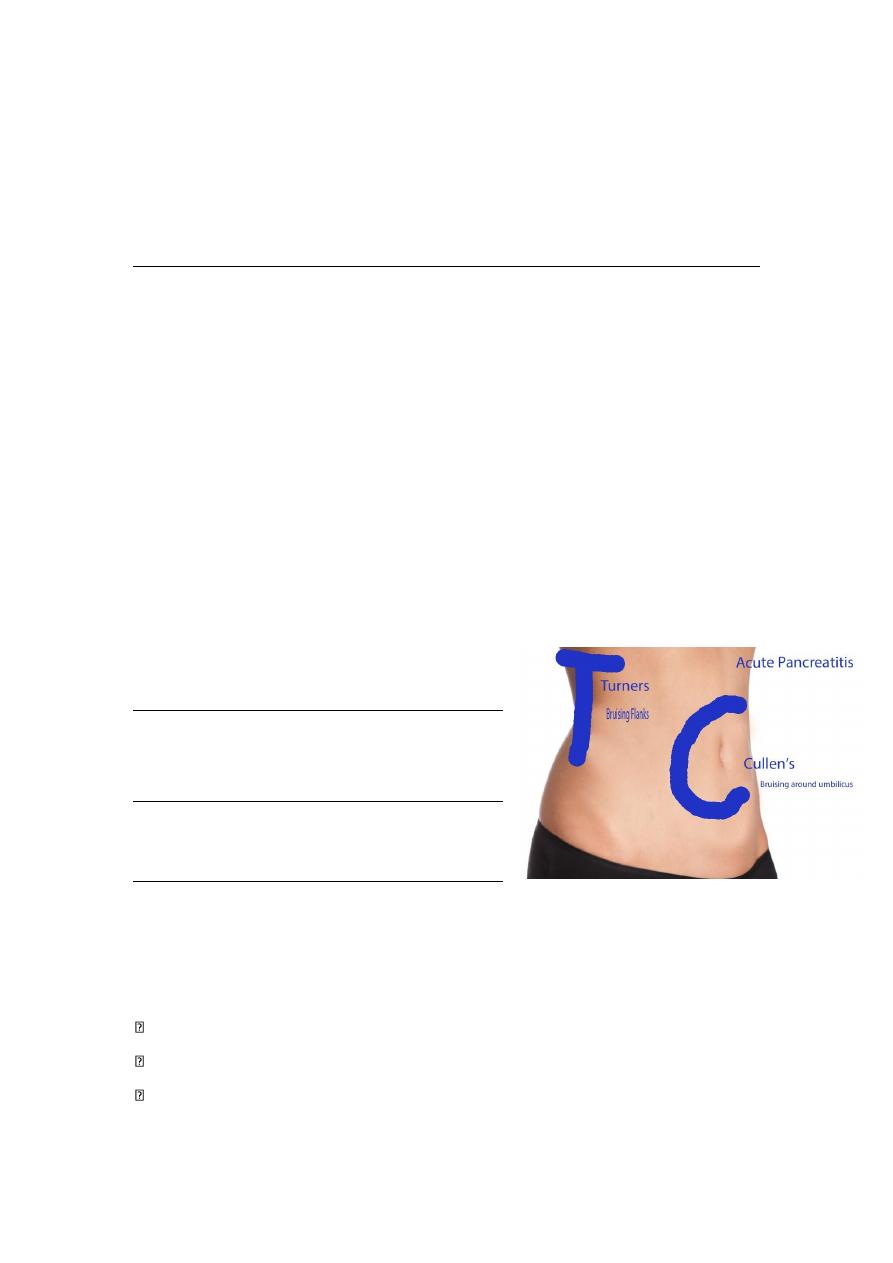
Bruising and discolouration in the left flank (Grey
Turner’s sign) and around the umbilicus (Cullen’s
sign) only develop in patients with very severe
haemorrhagic pancreatitis
*Bowel sound +ve, -ve
Normal, sluggish ,exaggerated
in paralytic ileus (borborygmi sound)
صوت النركيل
Painless progressive jaundice suggests carcinoma of the pancreas, especially in the presence
of a palpable gall bladder (Courvoisier’s law).
Stomach ca metastasis nomenclature
Lt supraclavicular LN. Virchow’s LN, Troisier’s sign.
Ovary (Krukenberg’s tumor)
Periumbilical region (“Sister Mary Joseph node”)
Peritoneal cul-de-sac (Blumer’s shelf): palpable on rectal or vaginal examination
Dr.Abdulkarim September 5, 2016
Session 9
4
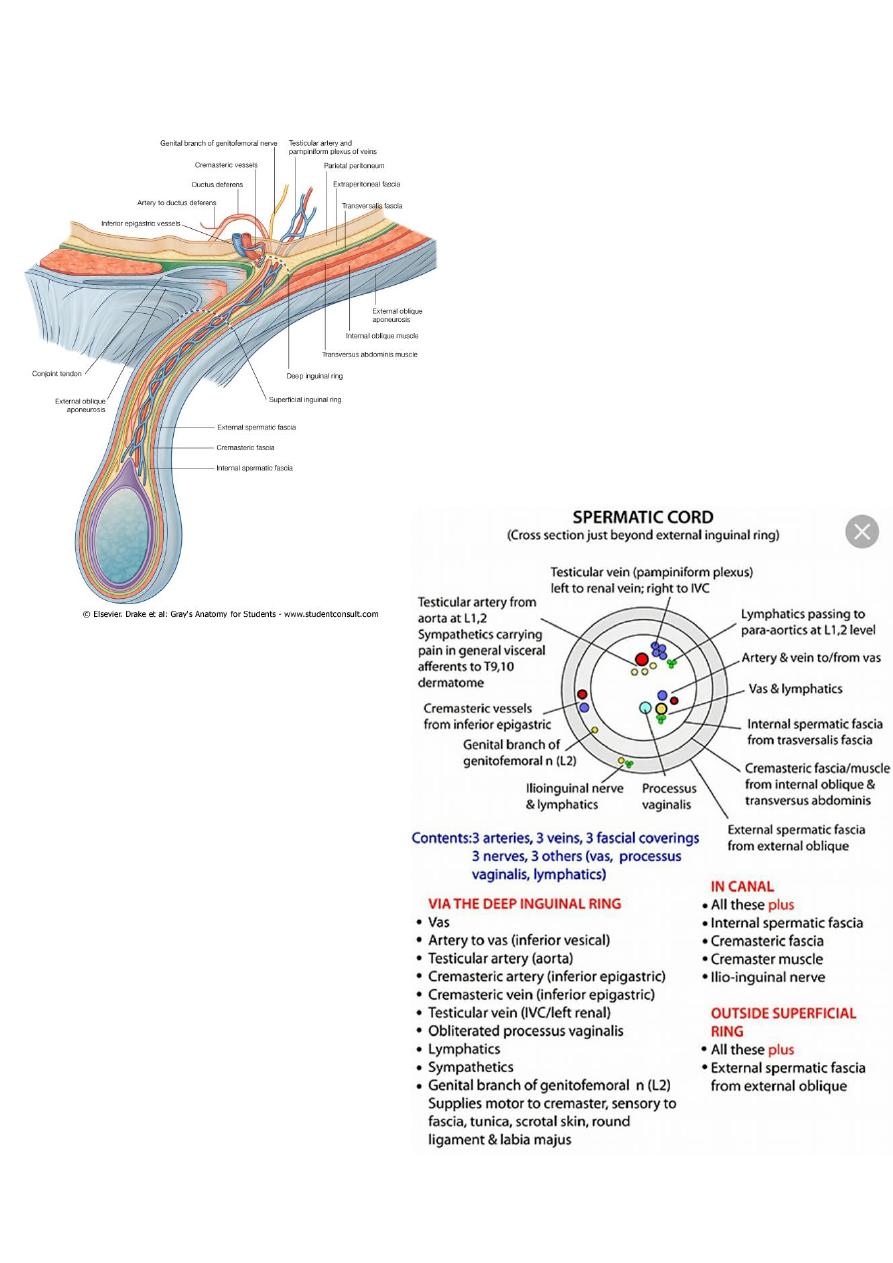
Inguinal canal contents
Dr.Abdulkarim September 5, 2016
Session 9
5
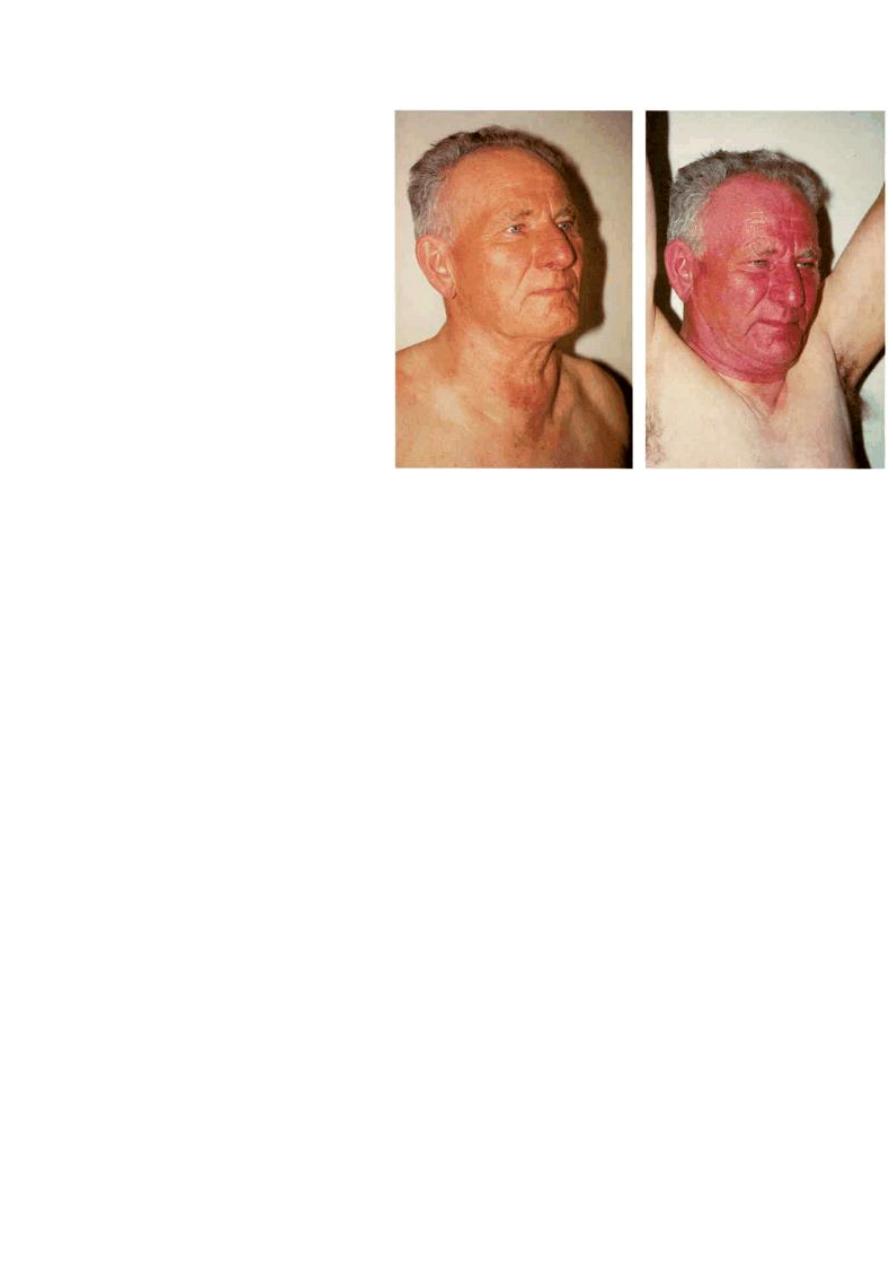
pemberton sign