Unit 2: Bacteriology
116
Lecture 7 - Haemophilus
Small, G- pleomorphic bacteria. Identification of H.
group depends (in part) upon requirement for growth
factors (X & V factors).
X factor: heme
V factor: Nicotinamide-adenine dinucleotide
1. Haemophilus influenzae:
Found on the mucous membranes of upper R.T.
occasionally causes R.T. infections in children & adults.
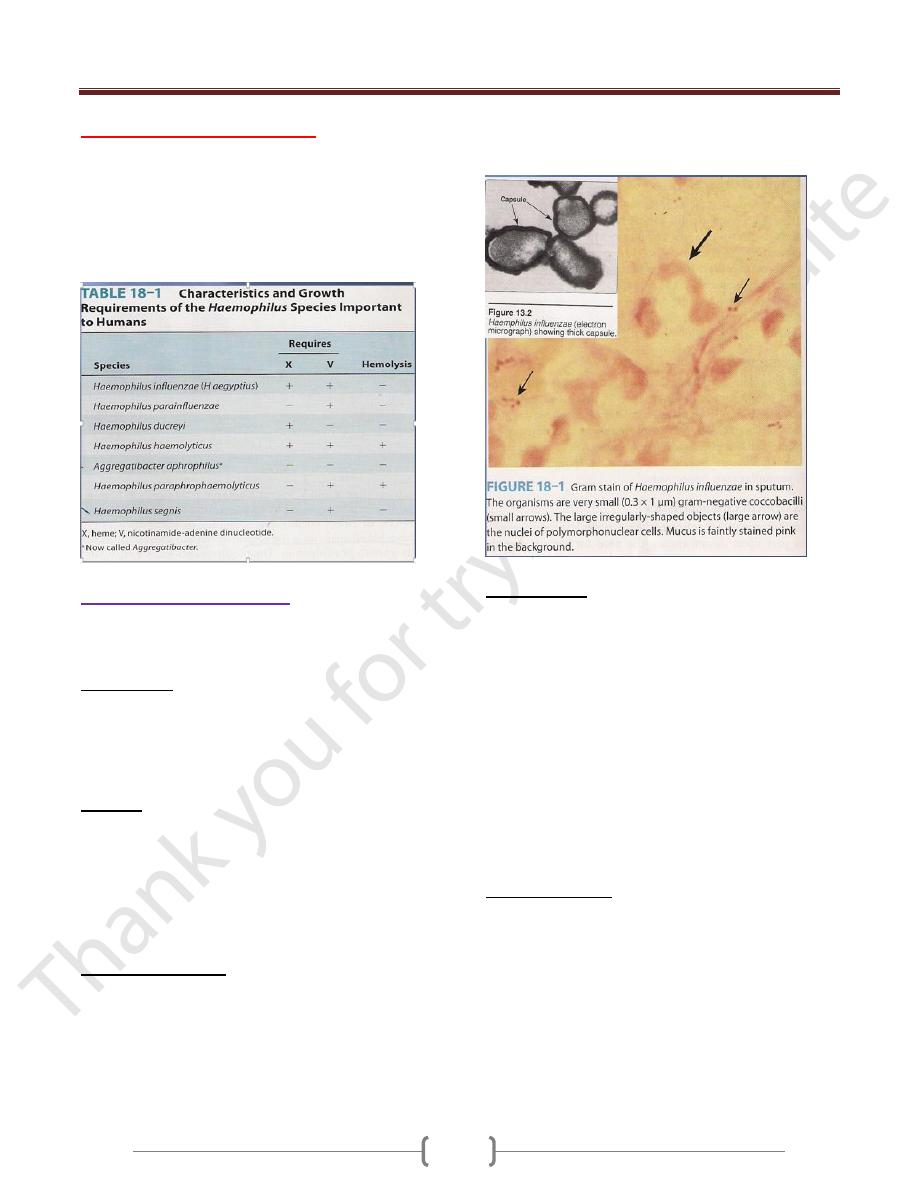
Morphology:
In specimens: coccoid bacilli, in pairs or short chain.
In young culture (6-8 hours): small coccobacilli & have a
finite capsule. Later become longer rods & very
pleomorphic form.
Culture:
On brain-heart infusion agar with blood (requires X & V
factors), after 24 hours → small, round, convex colonies.
Chocolate agar (36-48 hours) →larger colonies (1 mm,
not hemolytic).
Satellite phenomenon: H. influenzae grow much larger
colonies around staphylococcal or other colony.
Antigenic Structure:
Encapsulated H. influenzae contains capsular
polysaccharides (6 types Ags a-f), H. influenzae type b
an important human pathogen may lose its capsule & the
type specificity. H. influenzae in the normal flora of
upper R.T. are not capsulated.
Somatic Ags: outer membrane proteins.
LPS (endotoxin): share many structures with those of
neisseriae.
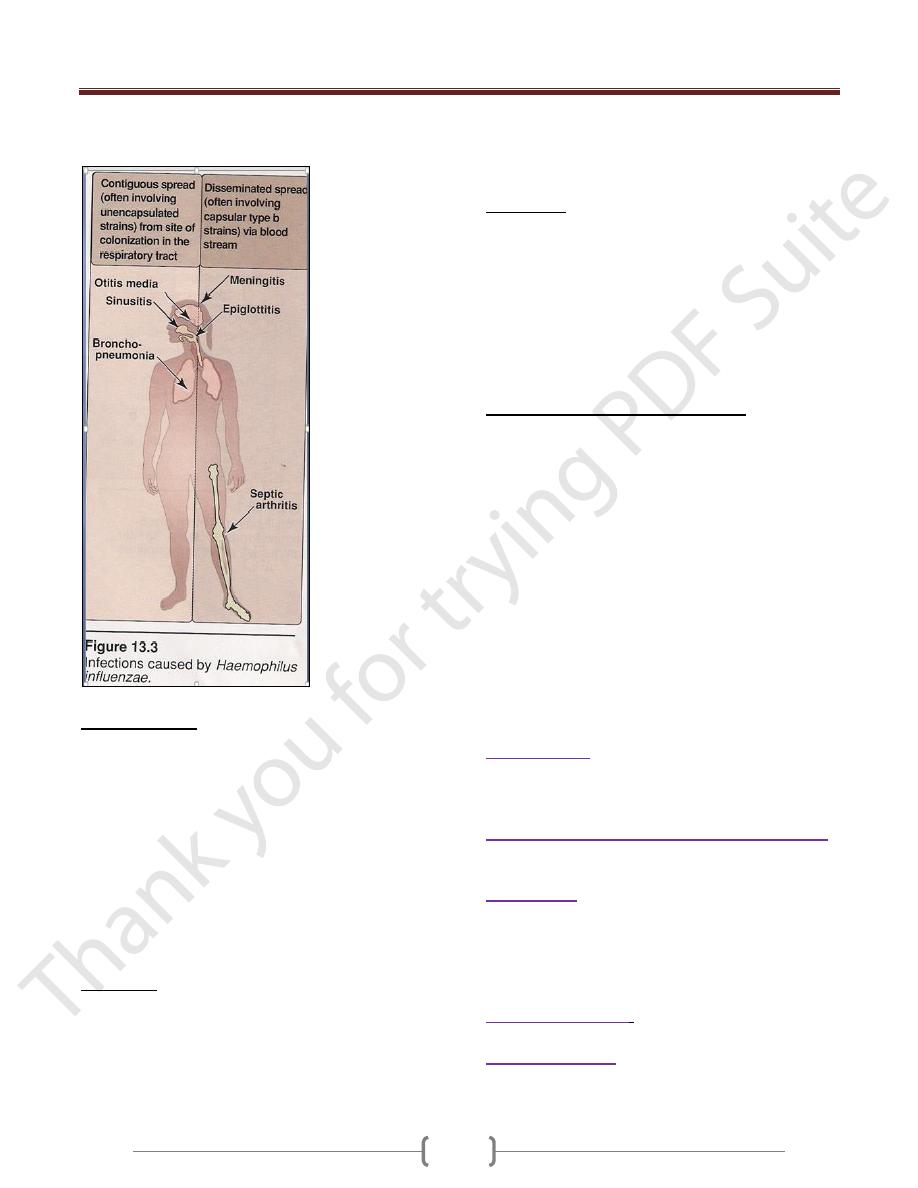
Pathogenicity:
The capsule is antiphagocytic, type b capsule (PRP=
polyribose ribitol phosphate) is the major virulence factor
of H. influenzae (causes meningitis, pneumonia &
empyema, epiglottitis, cellulitis, septic arthritis & other
invasive infections). H. influenzae types c-f rarely cause
disease.
Nontypeable H. influenzae causes invasive infections less
than type b (chronic bronchitis, otitis media, sinusitis &
conjunctivitis).
H. influenzae type b enters by way of the R.T →
extend to the sinuses or middle ear, may reach the
bloodstream →to the meninges (meningitis) or
establish in the joints (septic arthritis).
Clinical Findings:
Infant: fulminating obstructive laryngotracheitis with
swollen, cherry-red epiglottis (requires tracheostomy or
intubation as a lifesaving).
Small children & old or debilitated people: Pneumonitis
& epiglottitis may follow upper R.T. infections.
Adults: may have bronchitis or pneumonia.
H. influenzae the most common cause of meningitis in
children (age 5 months-5 years) resembles other forms of
childhood meningitis.
Unit 2: Bacteriology
117
H. influenzae type b & pneumococci are the most
common cause of otitis media & acute sinusitis.
Diagnostic Lab.:
Specimens: nasopharyngeal swab, pus, blood & csf.
Direct identification by immunofluorescence or by
specific rabbit antiserum for a capsule (type b) swelling
test. Commercial kits for immunologic detection of H.
influenzae Ags in csf.
Culture: IsoVital X enriched chocolate agar(24-48 hrs)
→ typical colonies.
Test for X & V factors can be done by placed strips or
disks containing these factors on the surface of agar,
growth of H. influenzae in the area between the strips
indicates requires both factors.
Immunity:
Infants (less than 3 months) have Abs transmitted from
the mother (rare infection). By age 3-5 years, many
children have naturally acquired anti-PRP Abs that
promote complement-dependent bactericidal killing &
phagocytosis.
Immunization of children with H. influenzae type b
vaccine induces the same Abs. Pneumonia or arithritis
due to H. influenzae can develops in adults with such Abs.
Treatment:
Untreated H. influenzae meningitis causes mortality rate
up to 90%. H. influenzae type b susceptible to ampicillin
(25% of strains are resistant by produce ß-lactamase
under control of a transmissible plasmid).More strains are
susceptible to chloramphenicol & all to the newer
cephalosporins (cefotaxime).
Influenzal meningitis may develop a subdural
accumulation of fluid, so requires surgical drainage.
Epidemiology, Prevention & control:
Encapsulated H. influenzae type b is transmissible from
person-person by the respiratory routes.
Infection can be prevented by administration of
haemophilus b conjugate vaccine (H. influenzae type b
with protein carrier either CRM, mutant C. diphtheriae
toxin protein or N. meningitidis outer membrane
complex) to children aged 2 months or older.
Children aged 15 months or older can receive H.
influenzae type b vaccine conjugated with diphtheria
toxoid (it is not immunogenic in younger children). The
vaccine reduces the incidence of meningitis & the carrier
rates for H. influenzae type b.
Contact with patients posses little risk for adults but
not to nonimmune children (less than 4 years), so can
use rifambin for them.
2. H. aegyptius
: Called the Koch-Weeks bacillus (H.
influenzae biotype III) causes conjunctivitis & it is the
cause of Brazilian purpuric fever, a disease of children
characterized by fever, purpura, shock & death.
3. H. aphrophilus (Aggregatibacter aphrophilus):
found as a normal oral & respiratory tract flora
causes infective endocarditis & pneumonia.
4. H. ducreyi
: Causes chancroid (soft chancre), a
sexually transmitted disease, a ragged ulcer on the
genitalia with marked swelling & tenderness, the regional
lymph nodes are enlarged & painful. Treatment with
ceftriaxone (IM), oral trimethoprime-sulfamethoxazole or
oral erythromycin.
5. H. parainfluenzae
: as a normal flora of the R.T.
causes infective endocarditis & urethritis.
6. H. haemolyticus
: as a normal flora of the
nasopharynx & associated with rare R.T. infections of
moderate severity in childhood.