Unit 2: Bacteriology
120
Lecture 9 – Legionellae, Bartonella
& unusual bacterial pathogens
Legionella
Outbreak of pneumonia in attending an American Legion
convention (1976). There are several species of Legionella:
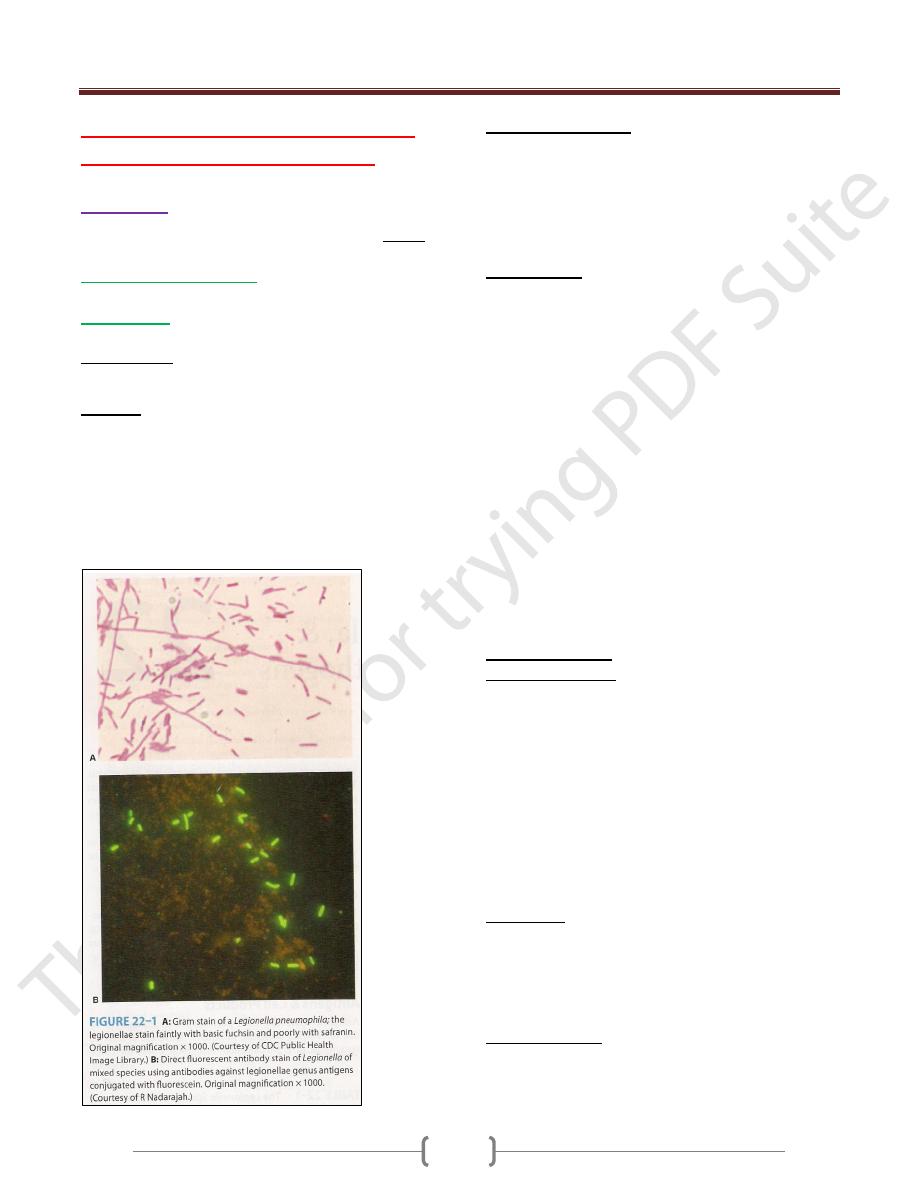
-Legionella pneumophila
: the most important, cause
Legionnaire’s disease & Pontiac fever.
-L. micdadei
: sometimes causes pneumonia.
Morphology:
Fastidious, aerobic G- rods stain poorly by Gram’s method
Culture:
Grown on complex media BCYE + α-ketoglutarate at pH
6.9, 35C˚ & humidity 90% →grow slowly, visible
colonies after 3 days (in blood culture require 2 weeks or
more) → variation in colony, round or flat with entire
edges, vary in color from colorless to iridescent pink or
blue & translucent.
Catalase +, L. pneumophila is oxidase + & others variable
Antigenic Structure:
There is more than 10 serogroups of L. pneumophila,
serogroup 1 the most common (complex antigenic
structure).
Legionellae produce: proteases, phosphatase, lipase,
DNase & RNase.
Pathogenesis:
Legionellae found in warm moist environments &
infection of immunocompromised humans follows
inhalation of the bacteria from aerosols (contaminated air-
conditioning systems, showerheads & similar sources).
L. pneumophila causes a lobar, segmental or patchy
pulmonary infiltration, acute purulent pneumonia
involving the alveoli with dense intra-alveolar exudate of
macrophages, PMNs, RBCs & proteinaceous material.
There is interstitial infiltration & little or no inflammation
of the bronchioles & upper airways.
L. pneumophila enters & grows within human alveolar
macrophages & monocytes (phagocytosed but not killed),
so L. pneumophila in lesions found within phagocytic
cells. Ribosomes, mitochondria & small vesicles
accumulate around phagocytic vacuoles → the cells
destroyed → the bacteria released & infected other
macrophages.
Clinical Findings:
Legionnaire’s disease: asymptomatic infection is common
in all ages, highest in men over 55 years. Risk factors:
smoking, chronic bronchitis & emphysema, steroid &
other immunosuppressive drugs, cancer chemotherapy &
diabetes mellitus.
Infection may nondescript febrile illness of short duration
or sever, rapidly progressive illness with high fever,
chills, malaise, nonproductive cough, hypoxia, diarrhea &
delirium. Chest X-rays reveal patchy & multilobar
consolidation.
There are leukocytosis, hyponatremia, hematuria (even
renal failure) or abnormal liver function.
Pontiac fever: fever, chills, myalgia, malaise, headache
(6-12 hours), dizziness, photophobia, neck stiffness &
confusion. Respiratory symptoms are much less in
Pontiac fever than Legionnaire’s disease & include mild
cough & sore throat.
Diagnostic Lab.:
Specimens: bronchial washings, pleural fluid, lung
biopsy & blood.
Smear: Direct Ab tests (low sensitivity).
Unit 2: Bacteriology
121
Culture: BCYE agar then IF staining.
Specific tests: Legionellae Ags in patient’s urine by
immunologic method.
Serologic tests: detection Abs to Legionellae (outbreaks).
Treatment:
The drug of choice is erythromycin. Rifampin when
treatment delayed.
Ventilation & management of shock is essential.
Epidemiology & Control:
The natural habitats for Legionellae are lakes, streams,
rivers & thermally heated bodies of water & soil (survives
up to 63C˚). Cooling towers & evaporative condensers
heavily contaminated with L. pneumophila.
Contamination of residential water systems
community acquired inf.
Contamination of hospital water systems hospital
acquired or nosocomial infection.
Control of Legionellae in water & air-conditioning
systems by hyperchlorination & superheating of water.
Bartonella
Is a genus of Gram-negative bacteria. Faculative
intracellular parasite, Bartonella species can infect
healthy people but are considered especially important as
opportunistic pathogen. Bartonella are transmitted by
insect vectors such as ticks, fleas, sand
flies&mosquitoes
At least eight Bartonella species or subspecies are known
to infect humans. G- pleomorphic rods, difficult to
isolated but can be seen in infected tissues by Warthin-
Starry silver stain
3 medically important spp.:
1. B. bacilliforms:
2 stages of Bartonellosis or Carrion’s disease:
a) Oroya fever (initial stage):
serious infectious anemia
due to blood cells destruction, hemorrhage into the lymph
nodes & enlargement spleen & liver. Masses of
bartonellae fill the cytoplasm of cells lining the blood
vessels & endothelial swelling → vascular occlusion &
thrombosis → 40% mortality rate.
b) Verruga peruana (eruptive stage):
begins 2-8 weeks
later through verrugae (absence of Oroya fever), vascular
skin lesions no anemia & fatalities, lasts for 1 year.
• Diagnosis by stained smear & blood culture (28C˚ for 10
days or more).
• In Peru, Colombia & Ecuador, transmitted by sandflies
• Control: by insecticides.
• Treatment: penicillin, streptomycin or chloramphenicol.
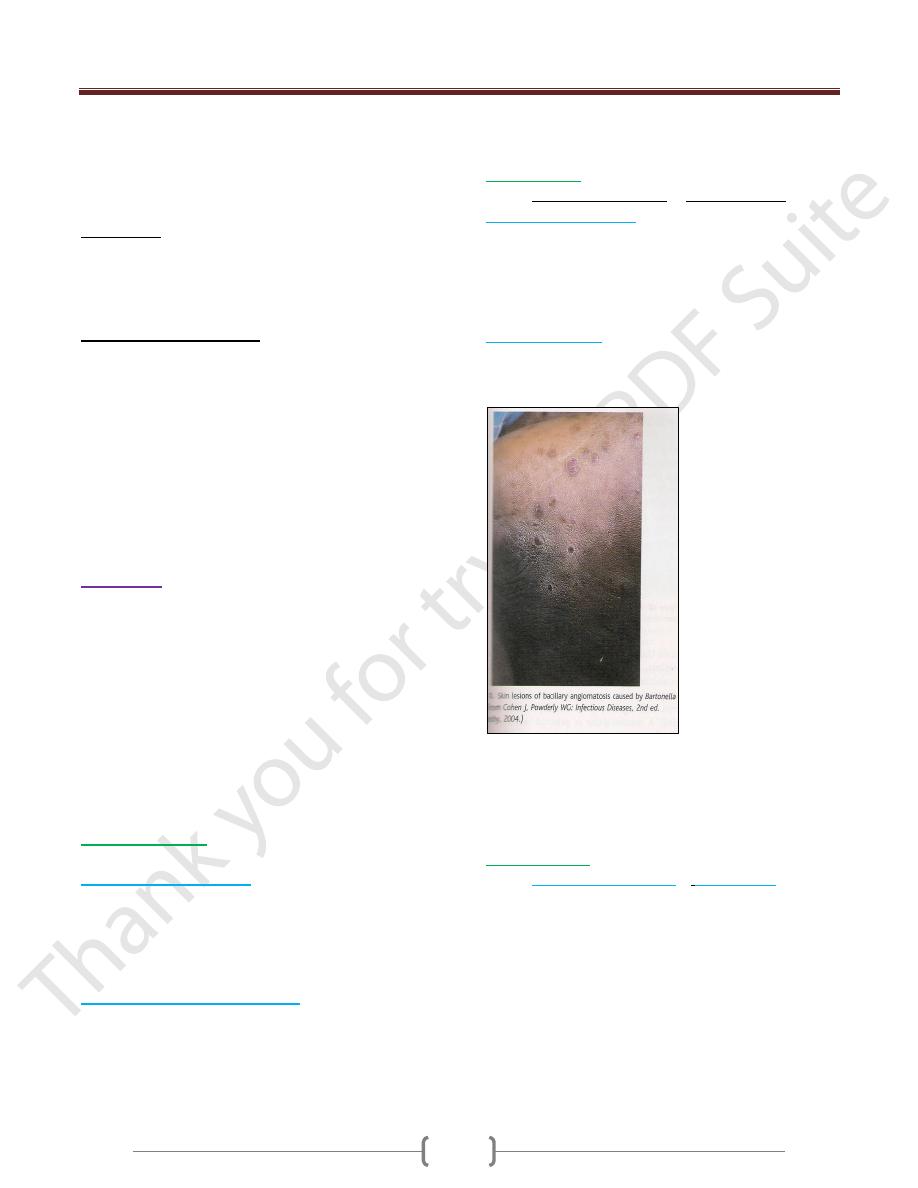
2. B. henselae
:
Causes bacillary angiomatosis & cat-scratch fever.
Bacillary angiomatosis:
proliferative, vascular lesions in the skin & visceral
organs (immunocompromised &
ADIS patients).
Treated with doxycycline or erythromycin.
Cat-scratch fever:
transmitted by cat scratch or bites &
cat fleas bites, after 3-10 days, skin lesions at the site of
scratch with low-grade fever, headache, sore throat or
conjunctivitis.
2 weeks later → lymphoadenopathy (regional lymph
nodes enlarged, tender & may discharge pus). Self-limited
illness (many weeks or months).
Treated by tetracycline or erythromycin.
3. B. quintana
:
Causes
bacillary angiomatosis
&
trench fever
(World
War I in trenches), transmitted by body lice → sudden fever
for 5-7 days, headache & sever pains in trunk & limbs.
Unit 2: Bacteriology
122
Unusual Bacterial Pathogens
* Calymmatobacterium granulomatis:
G- rods, causes granuloma inguinale, a sexually
transmitted disease → genital ulceration & soft tissue &
bone destruction. Diagnosis by stained smear from the
lesion → Donovan bodies (stained organism within large
macrophages).
-Treated by tetracycline.
* Tropheryma whippelii:
G+ bacilli related to actinomycete, causes Whipple’s
disease: fever, abdominal pain, diarrhea, weight loss &
migratory polyarthralgia. Diagnosis by periodic acid-
Schiff stain.
Gardnerella vaginalis:
Isolated from the normal female genitourinary tract &
associated with vaginosis (nonspecific vaginitis) → no
inflammatory cells & absence of common causes of
vaginitis, but in wet smear there are a clue cells (epithelial
cells covered with many Gram-variable bacilli. Vaginal
discharge has a fishy odor & contains many anaerobes
with G. vaginalis. Treatment: oral metronidazole.
Mobiluncus: motile, curved, Gram-variable or G-,
anaerobic rods isolated from bacterial vaginosis may be
part of the normal vaginal anaerobic flora in women.
Streptobacillus moliniformis:
Aerobic, G- highly pleomorphic forms irregular chains of
bacilli with fusiform enlargements.
Causes:
Rat-bite fever:(normal habitant of this bacteria the throats
of rats, humans infected by rat bites), a septic fever,
blotchy & petechial rashes & very painful polyarthritis.
Diagnosis by cultures of blood, joint fluid or pus & by
serum agglutination test.
Haverhill fever: infection after ingested contaminated
milk with these bacteria. Penicillin & other antibiotics as
effective therapy.